Article Text

Statistics from Altmetric.com
COX-2 INDUCTION BY UNCONJUGATED BILE ACIDS INVOLVES REACTIVE OXYGEN SPECIES-MEDIATED SIGNALLING PATHWAYS IN BARRETT’S OESOPHAGUS AND OESOPHAGEAL ADENOCARCINOMA

Chronic exposure to both acid and bile leads to increased risk of Barrett’s oesophagus and oesophageal adenocarcinoma (OA). Bile acids can be both potent tumour promoters and carcinogens and are known to increase the expression of COX-2, which is involved in the development of Barrett’s oesophagus and OA. Song et al investigated the detailed molecular mechanisms by which bile acids regulate COX-2 expression in the oesophagus. They analysed the effects of bile acids on COX-2 expression in immortalised Barrett’s and OA cells and used several molecular techniques to identify relevant signalling pathways. Flow cytometry and reactive oxygen species (ROS) scavengers were used to examine ROS involvement. Immunohistochemistry was performed on oesophageal mucosa obtained from an established rat model of bile reflux. The authors showed that unconjugated bile acids induce cAMP response element-binding and AP-1-dependent COX-2 expression in Barrett’s oesophagus and OA through ROS-mediated activation of PI3K/AKT and ERK1/2 (see fig). This study enhances our understanding of the molecular mechanisms by which bile acids promote the development of OA and offers the potential for developing novel chemopreventive strategies for this important cancer.
See pages 1512
IMPAIRED ENTEROCYTE PROLIFERATION IN AQUAPORIN-3 DEFICIENCY IN A MOUSE MODEL OF COLITIS
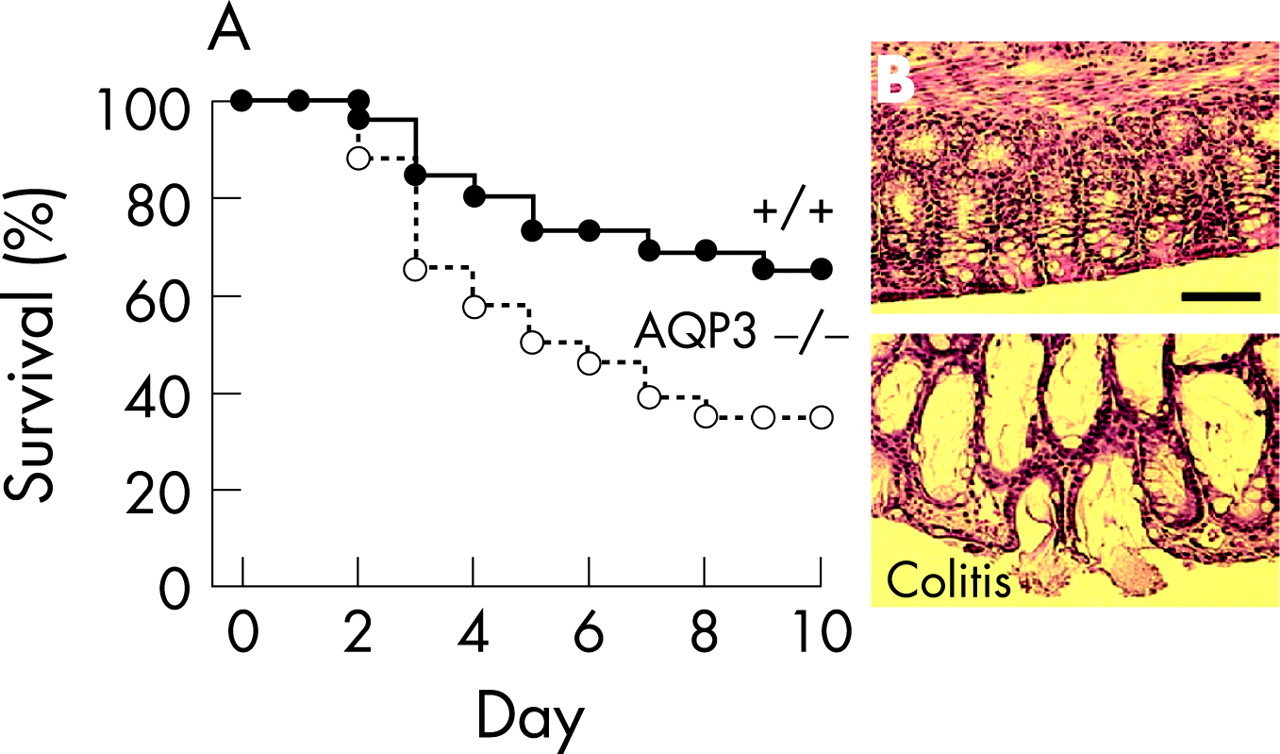
Aquaporin-3 (AQP3) is a water / glycerol transporter expressed at the basolateral membrane of colonic epithelial cells but its importance is not clear. Thiagarajah et al investigated the role of AQP3 in enterocyte proliferation using wild-type and AQP3 null mouse models of inflammatory bowel disease induced by administration of either oral dextran sulphate or intracolonic acetic acid. They measured clinical disease severity, survival, pathology and cellular responses. Glycerol was administered to mice to test whether disease progression could be altered. AQP3 null mice given dextran sulphate developed severe colitis after 3 days while wild-type mice, which had comparable initial colonic damage as assessed by cell apoptosis, developed remarkably less severe colitis, surviving >8 days. Cell proliferation was greatly reduced in AQP3 null mice. Survival was also reduced in AQP3 null mice in the acetic acid model (see fig). Oral glycerol administration significantly improved survival and reduced the severity of colitis in AQP3 null mice. The findings support a novel function for AQP3 in enterocyte proliferation and provide the first evidence for a major gastrointestinal phenotype associated with AQP deficiency.
See pages 1529
PROGRESS IN THE DEVELOPMENT OF GENETICALLY MODIFIED ENTEROTOXIGENIC ESCHERICHIA COLI VACCINE

Enterotoxigenic Eschericia coli (ETEC) diarrhoea is an important cause of childhood mortality and traveller’s diarrhoea. Immunity develops rapidly with antibodies to colonisation factor antigens (CFAs), which allow adherence to the gut mucosa. This pioneering study by Daley et al used oral administration of three strains of ETEC in which toxicity had been reduced by deleting a range of toxin genes. The vaccine was well tolerated with no significant episodes of diarrhoea and only a short-lived colonisation of the gut (<20 days). All strains elicited antibodies to CFAs in both serum, whole gut lavage fluid (WGLF) (see fig) and antibody in lymphocyte supernatant (ALS). There was good correlation between WGLF responses and serum IgA antibodies and ALS, which could be useful non-invasive assessments in future studies. Interestingly, there was no evidence of cytokine secretion into WGLF, suggesting that there was minimal enteric damage. The authors conclude that genetically attenuated organisms could be well-tolerated oral vaccines for many infectious diseases.
See pages 1550
SHORT TERM OUTCOMES OF THE FIRST ROUND OF A PILOT COLORECTAL CANCER SCREENING PROGRAMME WITH GUAIAC-BASED FAECAL OCCULT BLOOD TEST
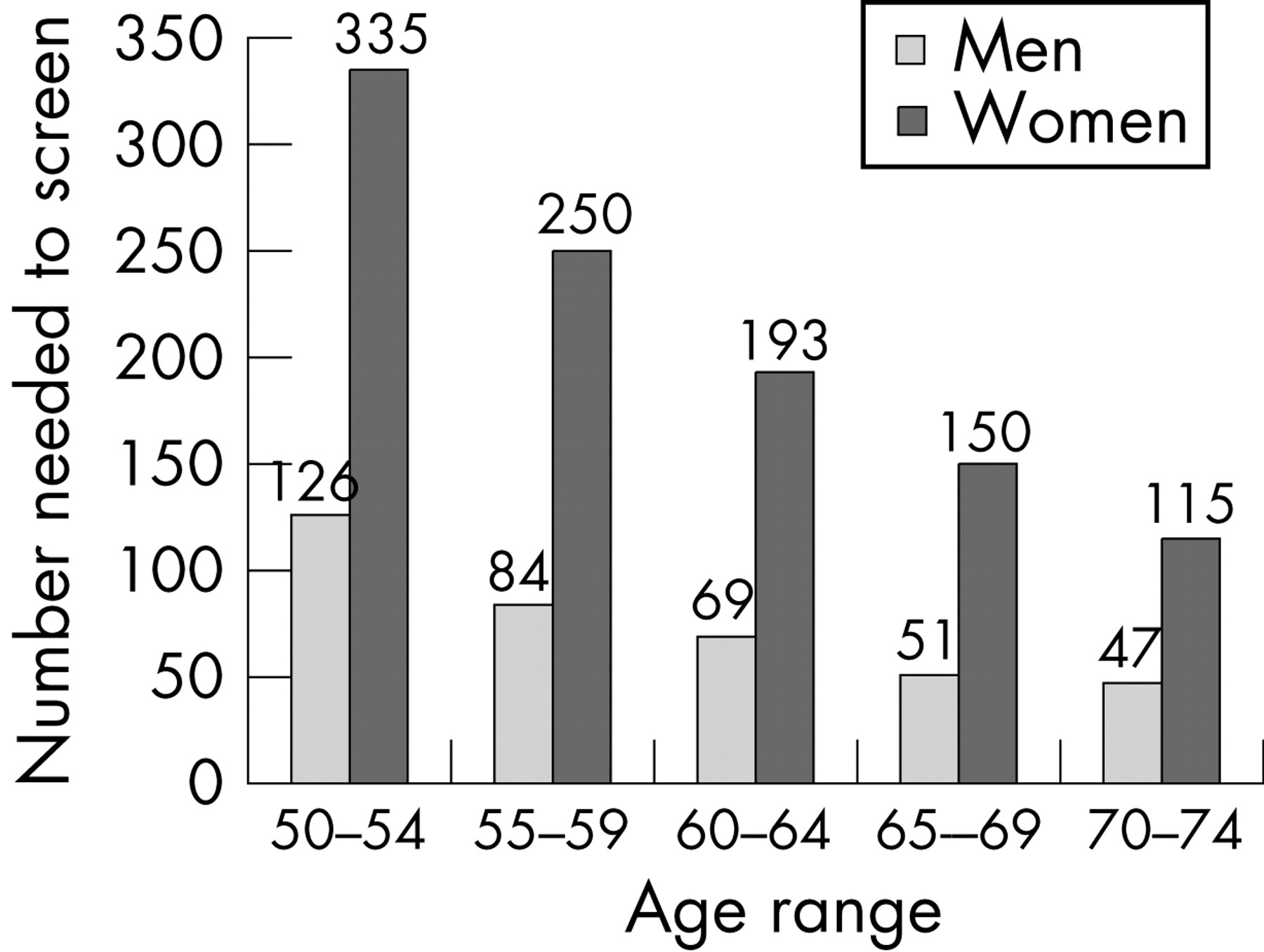
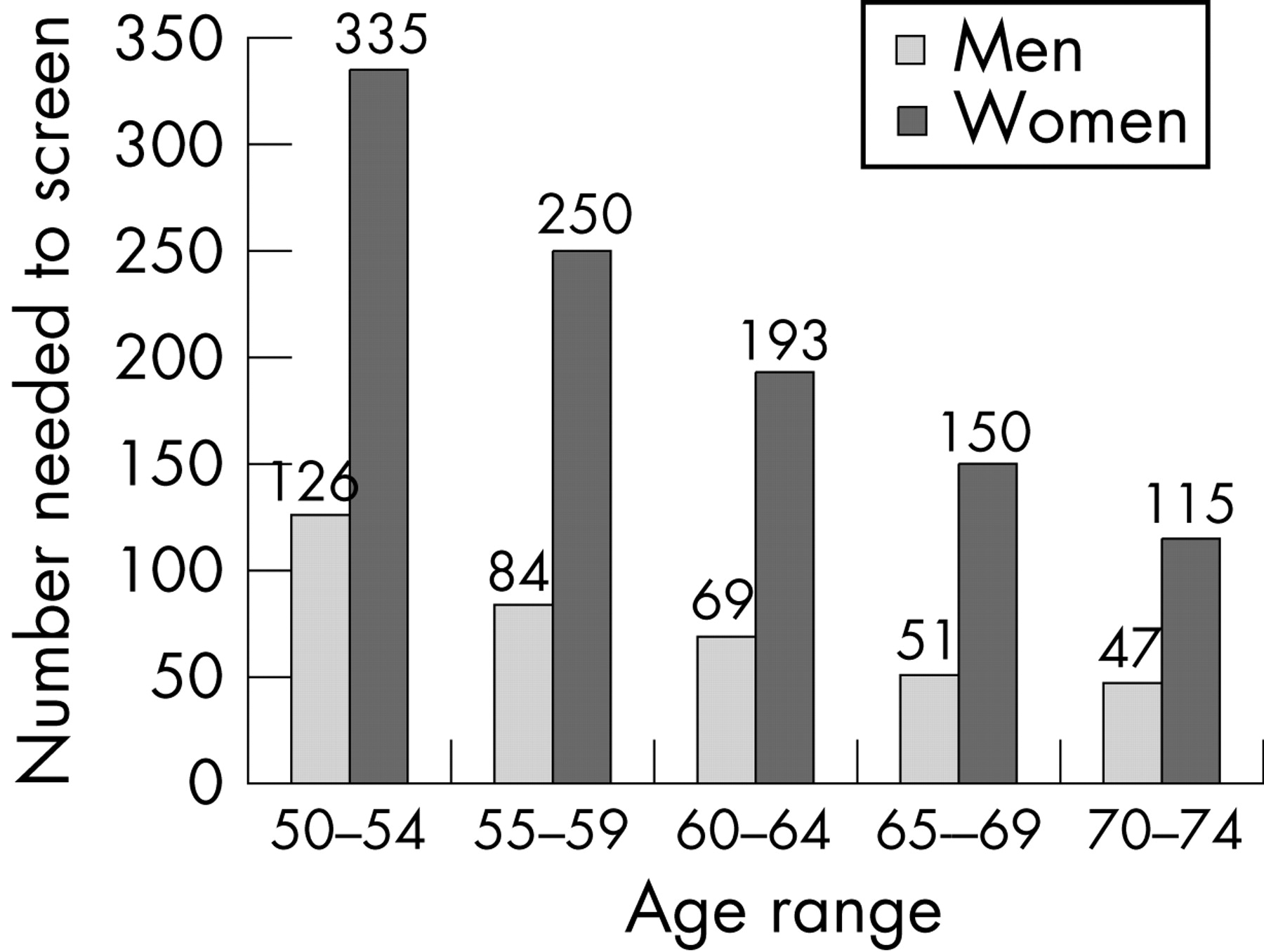
There is considerable interest in population screening for colorectal cancer (CRC). Denis et al report on the feasibility and effectiveness of a population-based CRC screening programme using a biennial guaiac-based faecal occult blood test (gFOBT) in the Haut-Rhin district of eastern France. A total of 182 981 residents aged 50–74 years were invited by their general practitioners to participate and 55.4% of eligible subjects completed a gFOBT. Subjects testing positive were offered a colonoscopy. The gFOBT positivity rate was 3.4%. The positive predictive value was 42.7% for neoplasia, 23.6% for advanced adenoma and 7.6% for cancer. The number of normal colonoscopic procedures needed to be performed for each colonoscopy detecting an advanced neoplasia was 1.8 (1.2 in men and 3.4 in women) and decreased with age (see fig). Detection rates for neoplasia and cancer were 12.8 and 2.3 per 1000 people screened. Two hundred and six adenocarcinomas were detected: 47.6% were stage I and 23.8% stage II. The findings show that participation and diagnostic yield of controlled trials of gFOBT screening are reproducible in the real world.
See pages 1579
INCREASING RISK OF PROGRESSION FROM ADVANCED ADENOMA TO COLORECTAL CANCER WITH INCREASING AGE

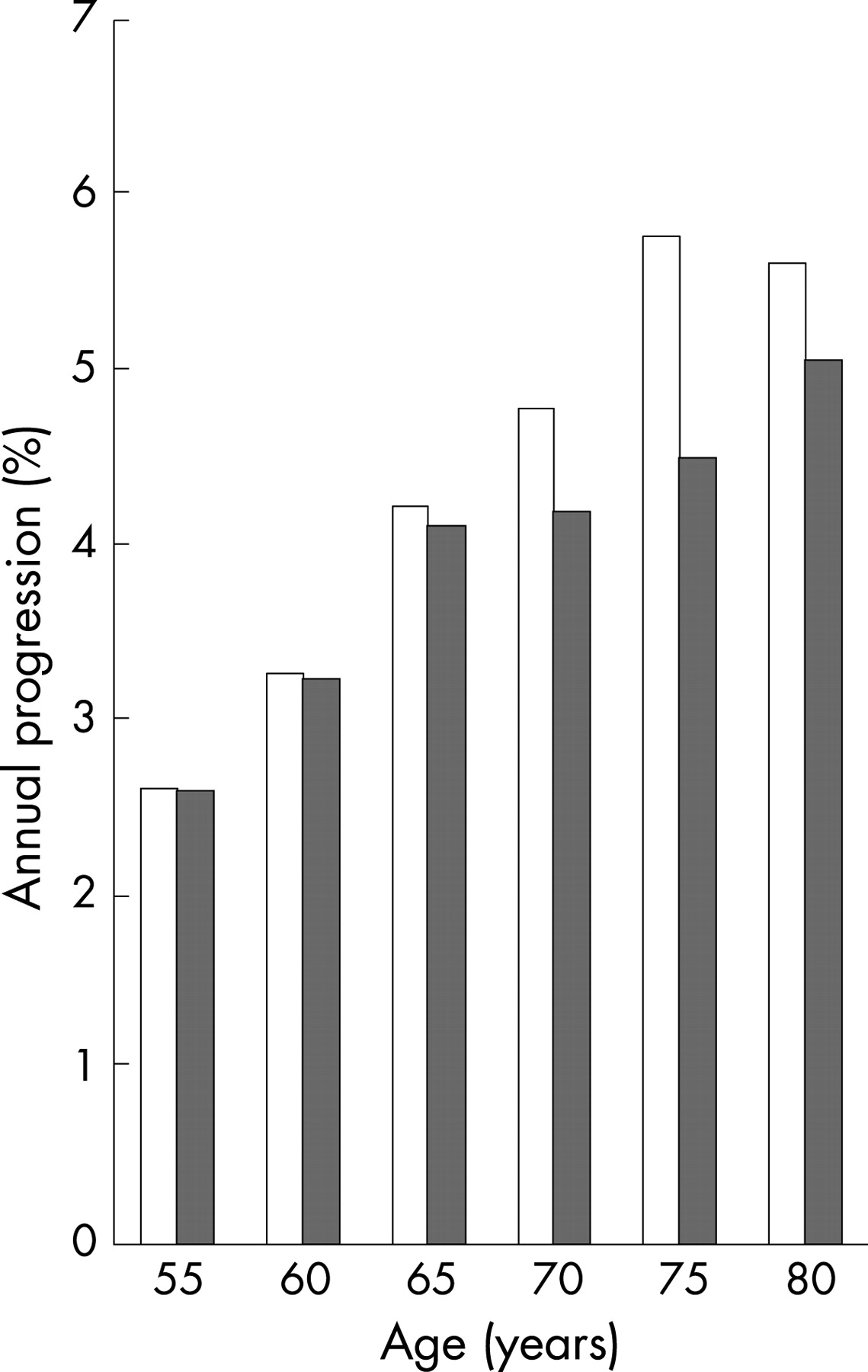
A vital component of any model assessing the cost effectiveness of colorectal cancer (CRC) screening is the rate of transition from advanced adenoma to CRC. A study by Brenner et al estimated this rate using the German national registry of 840 149 screening colonscopies performed in 2003 and 2004. The prevalence of advanced adenomas increased with age, rising from 3.4% in women aged 55–59 years up to 7.3% in women >80 years. The figures for men were higher at 6.2% and 9.5%, respectively. An estimate of transition rate to CRC was made from the incidence of CRC derived from a population-based cancer registry, assuming that 85% of CRC arises from advanced adenomas and clinical cancer takes 3.6 years to reach detection. The estimated annual transition rate was 2.6% in the youngest age group, increasing to 5.6% in the >80 years age group (see fig). These data will be important in optimising the timing and frequency of colonoscopy screening.
See pages 1585
OPTIMISING THE SUCCESS OF ENDOSCOPIC TREATMENT OF POST SURGICAL BILE DUCT INJURY

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Bile duct injury following laparoscopic cholestectomy causes serious morbidity. The report by de Reuver and colleagues describes the outcome in patients referred to a tertiary referral centre for endoscopic treatment of leakage from the common bile duct / cystic duct (n = 93) or bile duct injury (n = 110). Successful outcome of treatment for bile leakage was achieved in 97% and 89%, respectively. Patients with bile duct strictures ran a more complicated course requiring multiple (1–7) stents and prolonged duration of stenting (median 11 months, range 1-69). Stent-related complications occurred in 33% (6% cholangitis, 14% clogging and 16% pain). Overall success was 74% and was 3.2 times more likely if more than one stent was inserted at the first endoscopic retrograde cholangiopancreatography and much less likely (OR 0.12–0.04) for injuries involving the bifurcation. A change in policy in 2002 to progressively increase the number of stents inserted during the period of stenting produced no significant change in any of the outcomes. The best strategy appears to be two stents at the first treatment aiming for up to four stents early in the course of treatment.
See pages 1599
Linked Articles
- Oesophagus
- Inflammatory bowel disease
- Intestinal immunology
- Colorectal cancer
- Colorectal cancer
- Pancreas and biliary tract