Article Text

Statistics from Altmetric.com
ZINC CARNOSINE, A HEALTH FOOD SUPPLEMENT THAT STABILISES SMALL BOWEL INTEGRITY AND STIMULATES GUT REPAIR PROCESSES
There is great interest in “nutriceuticals” for disease prevention and treatment, but many commercially available products are sold without rigorous scientific validation. One such product is zinc carnosine (ZnC), which is sold as a dietary supplement with “added value for gastric health”. The authors assess the effect of ZnC on various models of gut injury and repair and in a clinical trial. In vitro studies showed that ZnC caused a threefold increase in cell migration and proliferation, which are surrogate markers of wound repair. ZnC reduced indomethacin-induced gastric injury by 75% in a rat model (see fig) and reduced small intestinal injury by 50% in a similar mouse model. In the clinical study, healthy volunteers undertook a randomised, crossover trial comparing changes in gut permeability before and after 5 days of indomethacin with ZnC or placebo coadministration. Indomethacin caused a threefold increase in gut permeability, while coadministration of ZnC protected subjects from this increase. ZnC appears promising as a stabiliser of gut mucosa but further studies are warranted.
See p 168

Effect of zinc carnosine (ZnC) on rat model of gastric damage, **p<0.01 v saline control.
KEY ROLE OF INTESTINAL MACROPHAGES IN POSTOPERATIVE ILEUS
Considerable expense and morbidity results from postoperative ileus, which appears to be due, in part, to the activation of normally quiescent macrophages resident within intestinal muscle. Their importance has been further demonstrated by this study of rodents, in which intestinal macrophages had been depleted either chemically, by exposing rats to liposomal clodronate and gadolinium, or genetically in mice by a mutation of the colony stimulating factor-1 gene. Both types of depletion reduced macrophage populations in the muscle layer and inhibited the early rise in macrophage inflammatory protein-1 (MIP-1) and inflammatory cytokines such as interleukin (IL) 1β (see fig), IL6 and the expression of the cellular adhesion molecule (ICAM-1). These effects were most striking in the genetically deficient mouse. Similarly, there was a marked reduction of the inhibitory effect of surgical manipulation on jejunal contractility and transit of an insoluble marker. This study confirms the key role of activated macrophages in ileus, which remain an attractive target for treatment of this common clinical problem.
See p 176

Reduced levels of IL1β mRNA in macrophage-depleted rats(DI) compared with normal rats 3, 12 and 24 h after surgery. There was no difference between groups before surgery. CTL, controls.
ACTIVATION OF JEJUNAL MAST CELLS IN DIARRHOEA-PREDOMINANT IRRITABLE BOWEL SYNDROME (D-IBS)
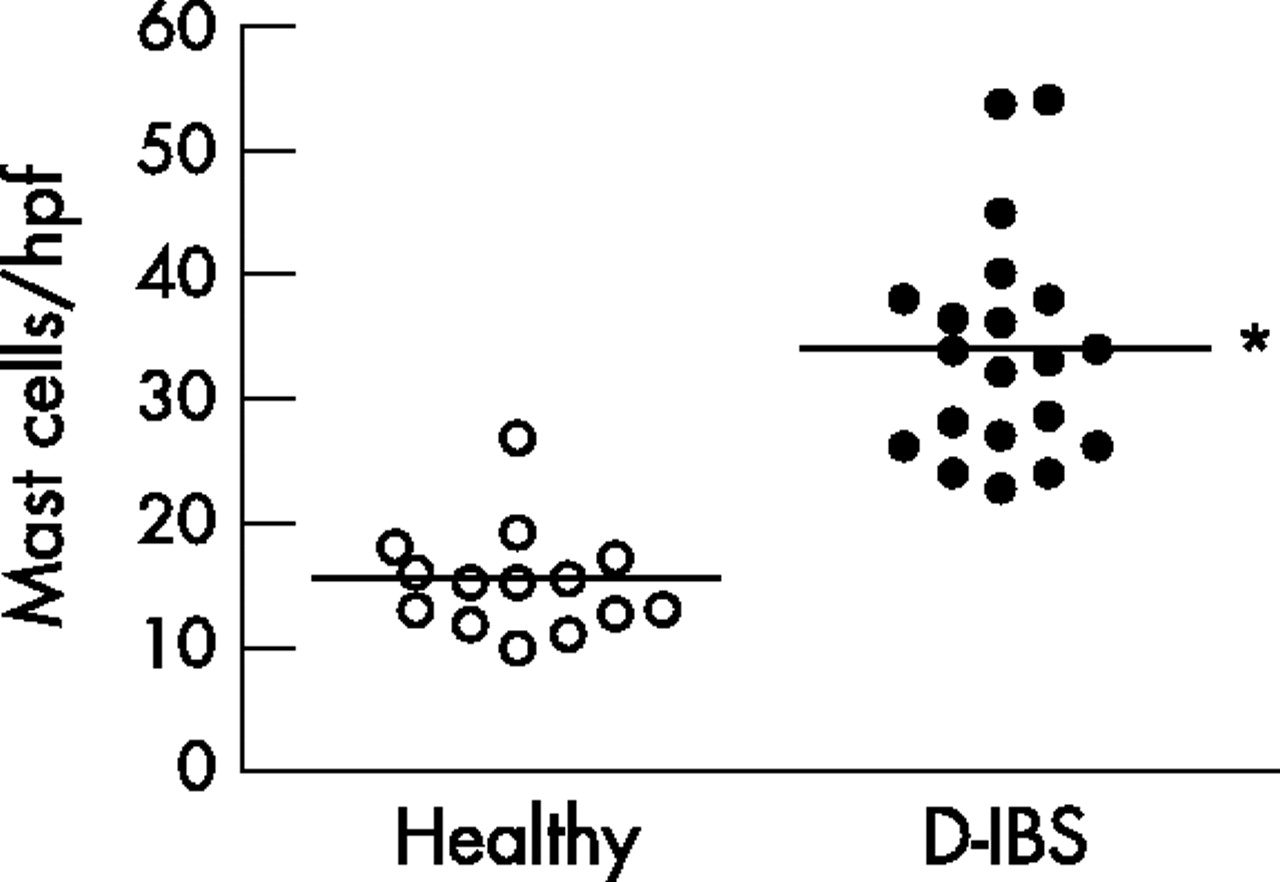
Recent studies have shown increased numbers of mast cells in the descending colon of unselected patients with IBS whose pain correlated with the proximity of mast cells to nerve endings. Mast cells secrete a range of mediators including mast cell tryptase (MCT) that could sensitise afferent nerves, thereby contributing to visceral pain. Stress is known to aggravate IBS symptoms and the Barcelona research group have previously shown that the stress of cold pain causes release of MCT in normal subjects, which is associated with increased water secretion and could contribute to diarrhoeal symptoms. This study extends these observations to D-IBS patients and shows increased numbers of jejunal mast cells and increased levels of MCT in jejunal aspirates. More patients with D-IBS also had stress and depression compared with controls but whether this increase in mast cells is specific to IBS or a feature of depression remains to be established. Furthermore, proof that this is of aetiological significance requires demonstration that mast cell stabilisers improve symptoms in IBS, something which has yet to be shown in a high-quality, randomised, placebo-controlled trial.
See p 203

Increased mast cell numbers per high power field in D-IBS patients compared with controls, p<0.001.
COMPARISON OF A GUAIAC-BASED AND AN IMMUNOCHEMICAL FAECAL OCCULT BLOOD TEST IN SCREENING FOR COLORECTAL CANCER IN A GENERAL, AVERAGE-RISK POPULATION
Colorectal cancer screening is becoming a national priority. The guaiac-based faecal occult blood test (G-FOBT) is a convenient screening tool but lacks sensitivity. The immunochemical (I-FOBT) test relies on specific human haemoglobin and has higher sensitivity. This study compared the performance of the G-FOBT (non-rehydrated Hemoccult II test) with the I-FOBT in a general, average-risk French population, with an automated reading process allowing comparison between different posititvity cut-off points for the I-FOBT. A sample of 10 637 patients completed the study and those with at least one positive test underwent colonoscopy (see table). Using the usual cut-off point of 20 ng/ml blood, the positivity rate for the I-FOBT was higher than that of the hemoccult test (6.9% vs 2.4%). The gain in sensitivity associated with the use of I-FOBT (50% increase for cancer and 256% increase for high risk adenoma) was balanced by a decrease in specificity. Automated reading allowed the use of two alternative thresholds (50 and 75 ng/ml) for the I-FOBT test. This produced a lower positivity rate and sensitivity, and an increase in the predictive positive value for both cancer and high risk adenomas.
See p 210
Colonoscopy findings according to the test results
ARTIFICIAL NEURAL NETWORK IS SUPERIOR TO MELD IN PREDICTING MORTALITY OF PATIENTS WITH END-STAGE LIVER DISEASE
The model for end-stage liver disease (MELD) score is used as a disease severity index to determine referral to transplant programmes and organ allocation priorities. Although quite accurate, it fails to predict the mortality of a considerable proportion of patients. Artificial neural networks (ANNs) perform better than conventional analysis and have the advantage of learning through training. In this study, the ANN was constructed using data from 251 consecutive, cirrhotic patients listed for liver transplantation in Bologna, Italy. The ANN was trained to predict 3-month survival for 188 of these patients, tested on the remaining 63 unknown by the system (internal validation group) and finally on 137 patients listed for liver transplantation at King’s College Hospital, London, UK (external cohort). The ANN performed significantly better than MELD, both for the internal validation group (area under the curve (AUC) = 0.95 vs 0.85; p = 0.032) and in the external cohort (AUC = 0.96 vs 0.86; p = 0.044, see table). ANN could better prioritise liver transplant candidates and may reduce mortality on waiting lists.
See p 253
Receiver-operating characteristic analysis of the artificial neural network in comparison with the model of the end-stage liver disease performance
PROGNOSIS IN LIVER TRANSPLANTATION IN THE UK FROM 1989 TO 2003
Liver transplantation has revolutionised the prognosis of patients with end-stage liver disease. Major advances in management have substantially improved mortality, with the biggest effect being seen in the reduction of early (<6 months) mortality, thereafter the slope of the survival curves become identical (see fig). However, as many patients are relatively young, future life expectancy becomes important when advising about employment and family planning. The current survey provides valuable information on which to base this advice. It describes the survival of 3600 adult liver allograft recipients from the UK National Transplant Database. Life expectancy after surviving 6 months postoperatively was found to be similar to the normal population in those patients selected for transplantation for primary biliary cirrhosis (PBC) and cryptogenic cirrhosis at 35.8 and 33.9 years. Life expectancy was slightly reduced for patients with autoimmune cirrhosis, sclerosing cholangitis and Hepatitis B (24.5, 26 and 24.5 years) but markedly reduced for those with hepatitis C, alcoholic liver disease and cancer (12, 15 and 5.3 years), conditions in which the original lesion often recurs.
See p 279

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier survival curves for adult liver allograft recipients in the UK from 1985 to 2003, the lowest curve being for 1985 to 89.
Linked Articles
- Small intestine
- Neurogastroenterology
- Irritable bowel syndrome
- Colorectal cancer
- Liver
- Liver