Article Text

Abstract
Background: The human anti-tumour necrosis factor (TNF) antibody infliximab binds to the membrane TNF and subsequently induces apoptosis of activated lamina propria T lymphocytes in patients with Crohn’s disease in vitro.
Aim: To test whether the ability of rapid anti-TNF-induced apoptosis in the gut predicts the efficacy of anti-TNF treatment in inflammatory bowel disease.
Methods:99mTechnetium–annexin V single-photon emission computer tomography (SPECT) was performed in 2 models of murine experimental colitis and in 14 patients with active Crohn’s disease as assessed by the Crohńs Disease Activity Index (CDAI) to study the effect of anti-TNF treatment on apoptosis in the intestine during active colitis. Disease activity was evaluated 2 weeks after infliximab infusion using the CDAI (definition response: drop of >100 points).
Results: Colonic uptake of 99mTc-annexin V significantly increased in 2,4,6-trinitrobenzene sulphonate-induced colitis as well as in transfer colitis on administration of anti-TNF antibodies compared with a control antibody as determined with dedicated animal pinhole SPECT. In addition, uptake of 99mTc–annexin V significantly increased in patients with active Crohn’s disease responding to infliximab treatment. Colonic 99mTc–annexin V uptake ratio (mean (SEM)) increased from 0.24 (0.03) to 0.41(0.07) (p<0.01), 24 h after infliximab infusion (5 mg/kg). A mean increase of 98.7% in colonic uptake of 99mTc–annexin V could be detected in 10 of the 14 responding patients (CDAI >100 points at week 2) compared with 15.2% in non-responding patients (p = 0.03). Analysis of the mucosal biopsy specimens identified lamina propria T cells as target cells undergoing apoptosis.
Conclusions: These in vivo observations support the notion that colonic uptake of 99mTc–annexin V correlates with clinical benefit of anti-TNF treatment and might be predictive of therapeutic success.
- 7AAD, 7-amino-actinomycin D
- AZA, azathioprine
- CDAI, Crohn’s Disease Activity Index
- CRP, C reactive protein
- CUR, colon uptake ratio
- cVAM, chimaeric rat anti-mouse control antibody
- FACS, fluorescence-activated cell sorting
- LPMNC, lamina propria mononuclear cell
- mAb, monoclonal antibody
- PBS, phosphate-buffered saline
- SCID, severe combined immunodeficiency
- SPECT, single-photon emission computer tomography
- 99mTc-HYNIC, technetium-hydrazinonicotinamide
- TNBS, trinitrobenzene sulphonic acid
- TNF, tumour necrosis factor
Statistics from Altmetric.com
- 7AAD, 7-amino-actinomycin D
- AZA, azathioprine
- CDAI, Crohn’s Disease Activity Index
- CRP, C reactive protein
- CUR, colon uptake ratio
- cVAM, chimaeric rat anti-mouse control antibody
- FACS, fluorescence-activated cell sorting
- LPMNC, lamina propria mononuclear cell
- mAb, monoclonal antibody
- PBS, phosphate-buffered saline
- SCID, severe combined immunodeficiency
- SPECT, single-photon emission computer tomography
- 99mTc-HYNIC, technetium-hydrazinonicotinamide
- TNBS, trinitrobenzene sulphonic acid
- TNF, tumour necrosis factor
Tumour necrosis factor α (TNFα) is essential for the initiation and amplification of Crohn’s disease (reviewed by Papadakis and Targan 1 and van Deventer2). TNFα is first synthesised as a 26 kDa transmembrane form with an intracellular tail, which is cleaved to the secreted 17 kDa soluble form by the metalloproteinase TNFα-converting enzyme.3,4 The resulting 17 kDa form of TNFα then aggregates to form trimolecular complexes (trimers), which bind and activate their cognate receptors, either the p55 receptor or the p75 receptor.1 Soluble TNFα is predominantly synthesised by lymphocytes and activated macrophages.5 The number of lamina propria-soluble TNFα-producing T cells is increased in patients with Crohn’s disease, and high concentrations of soluble TNFα can be detected in the stool of patients with active immune responses.6,7
Anti-TNF neutralising strategies used in inflammatory disorders include etanercept (TNFα receptor 2 IgG1 invariant tail fusion protein) and infliximab (chimaeric IgG1 anti-TNF antibody). Etanercept is ineffective in the treatment of active Crohn’s disease,8 although it is beneficial for various other autoimmune disorders, including rheumatoid arthritis.9 Infliximab, however, is efficacious in both rheumatoid arthritis10,11 and Crohn’s disease.12,13 Infliximab, but not etanercept, causes apoptosis of monocytes14 and activated lymphocytes through the binding of membrane-bound TNF15 and subsequent reverse signalling.16 Crohn’s disease is characterised by mucosal T cell proliferation that exceeds T cell apoptosis,17 and infliximab has been shown to restore this inappropriate T cell accumulation by induction of apoptosis.18 This implies that it is not TNF neutralisation in itself, but an alternative mechanism that mediates the effect of infliximab in inflammatory bowel disease.
To further elucidate whether apoptosis in the intestine underlies the clinical benefit of anti-TNF treatment in Crohn’s disease in vivo, we performed real-time imaging of in vivo apoptosis using 99mTc–annexin V single-photon emission computed tomography (SPECT). This technique has shown the feasibility of visualising and quantifying cell death in reperfusion after myocardial infarction,19,20 and in tumours with a high apoptotic index and chemotherapy-induced cancer cell death.21 We use this technology to characterise the effect of anti-TNF strategies, both in murine models of experimental colitis as well as in patients with Crohn’s disease, and correlate the effects seen with the eventual clinical efficacy of infliximab treatment.
METHODS
Animal models
The animal studies ethics committee of the University of Amsterdam, Amsterdam, The Netherlands, approved of all experiments. BALB/c mice (Harlan Sprague Dawley, Horst, The Netherlands) and CB17 severe combined immunodeficient (SCID) mice (Charles River, Someren, The Netherlands) were used. The BALB/c mice were housed under standard conditions, whereas the SCID mice were housed in filter-top cages under specific pathogen-free conditions at the animal care facility. The experiments were conducted in 8- and 10-week-old female BALB/c mice and in 7–10-week-old female CB17 SCID mice.
2,4,6-Trinitrobenzene sulphonate colitis
Acute colitis was induced as described previously.22 Two doses of 1 mg of 2,4,6-trinitrobenzene sulphonic acid (TNBS; Sigma Chemical, St Louis, Missouri, USA) dissolved in 40% ethanol (Merck, Darmstadt, Germany) were rectally administrated (separated by a 7-day interval, ie, on days 0 and 7) using a vinyl catheter that was positioned 3 cm from the anus. During the instillation, the mice were anaesthetised using isoflurane (1-chloro-2,2,2,-trifluoroethyl-isoflurane-difluoromethyl-ether; Abbott Laboratories, Queenborough, Kent, UK). They were kept vertically after the instillation for 60 s. In total, 30 mice were used, which were divided into three groups.
Transfer colitis
Chronic CD45RBhigh transfer colitis was induced as described previously.23 BALB/c splenocytes were first enriched for CD4 cells by red-cell lysis and negative selection by using the following rat anti-mouse monoclonal antibodies (mAbs): B220 (clone RA3-6B2), Mac-1 (clone M1/70) and CD8α (clone 53-6.7) (gift from Dr R Mebius, Vrije Universiteit Medical Center, Amsterdam, The Netherlands). mAb-stained cells were removed in a magnetic field by using sheep anti-rat IgG-coated magnetic beads (Dynal, Hamburg, Germany). The resulting CD4 cells were stained with cytochrome-conjugated CD4 and fluorescein isothiocyanate-conjugated CD45RB (both BD Biosciences-Pharmingen, San Diego, California, USA) mAbs. Subpopulations of CD4 cells were generated by two-colour sorting on the FACS Vantage (BD Biosciences). Populations were found to be >95% pure on reanalysis. To induce colitis, only CD45RBhigh CD4 cells (1–4×105) were transferred to two groups of CB17 SCID mice. In all, 13 mice were used, divided into 2 groups. Animals were either injected with a chimaeric murine/rat monoclonal anti-TNF-α antibody (clone cV1q, gift from D Shealy, Centocor, Horsham, Pennsylvania, USA) as a single intraperitoneal injection (1 mg/mouse), or with a chimaeric murine/rat monoclonal cVaM negative control antibody, or vehicle, 64 days after the transfer model or 1 day after the second TNBS administration. For injection and scintigraphy, mice were sedated by a single intraperitoneal administration of 0.5 ml/10 g with FFD mix, consisting of 0.1 ml fentanyl/fluanisone (Hypnorm; Vetapharma, Leeds, UK), 0.1 ml dormicum (5 mg/ml, Roche Nederland BV, Woerden, The Netherlands) and 1.5 ml NaCl 0.9% (Fresenius Kabi Nederland BV, Hertogenbosch, The Netherlands). After 24 h of treatment, mice were injected intravenously with 50 MBq 99mTc-hydrazinonicotinamide (99mTc-HYNIC) annexin V (provided by Theseus Imaging, Cambridge, Massachusetts, USA) and after 1 h, scintigraphy was performed.
Assessment of inflammation
Mice with chronic colitis (transfer model) were weighed twice a week and mice with acute colitis (TNBS model) were weighed daily. Weight loss (percentage of baseline body weight) of 25% in transfer colitis was considered adequate. After killing the mouse, the colon weight was used as an index of disease-related intestinal wall thickening. The longitudinally divided colons were rolled up and fixed in 4% buffered formalin. Fixed tissues were embedded in paraffin wax, and 4–6 μm sections were stained with H&E for histological grading. In the transfer model, inflammation was scored on a scale of 0–4, representing no inflammation to severe inflammation. A different scoring system was used for the TNBS colitis model by using the following parameters: (1) percentage of colon involved, (2) fibrosis, (3) oedema, (4) erosions and ulcerations, (5) crypt loss, (6) infiltration of mononuclear cells or (7) polymorphonuclear cells.22 The total score ranged from 0 (normal colon) to a maximum of 20 points (most severe inflammation). Tissue slides were analysed by a pathologist blind to the study, and scored accordingly.
Treatment interventions and radiolabelling
For injection and scintigraphy, mice were sedated. A chimaeric rat/mouse monoclonal anti-TNF-α antibody (clone cV1q; gift from D Shealy, Centocor) was administered as a single intraperitoneal injection (1 mg/mouse). As negative control groups, age-matched mice were treated with either intraperitoneal 1 ml saline or injection of an irrelevant IgG1 isotype chimaeric antibody cVam (1 mg/mouse; gift from D Shealy, Centocor). 99mTc-HYNIC annexin V in kit formulation was prepared according to the guidelines provided by the manufacturer (Theseus Imaging). After 24 h of treatment, mice were injected intravenously with 50 MBq of the radiopharmaceutical compound 99mTc-HYNIC annexin V (further referred to as 99mTc annexin V) followed by scintigraphy after 1 h. 99mTc-HYNIC annexin V component is renally fully excreted with neither hepatic nor intestinal clearance.
Patients
Patients were recruited from the clinical department and outpatient clinic of the Department of Gastroenterology and Hepatology, University of Amsterdam, Amsterdam, The Netherlands. Disease activity was determined using the Crohn’s Disease Activity Index (CDAI). Patients were required to be taking stable drugs: no initiation or change in dosages was allowed within 8 weeks for thiopurine treatment or methotrexate, and within 2 weeks for corticosteroids. Patients who received infliximab within 8 weeks before the initiation date were excluded. After written informed consent was obtained, patients underwent a baseline colonoscopy and scintigraphy. Endoscopy included assessment of disease activity and collection of biopsy specimens. Severity of endoscopic disease was categorised according to the Simple Endoscopy Score.24 Mucosal specimens were placed in formalin and prepared for H&E staining at the site of inflammation for confirmation of disease activity. After concluding both the endoscopic and scintigraphic procedures, patients received a 2 h intravenous infusion of infliximab (Remicade, 5 mg/kg body weight) at the day care centre. Repeated endoscopy and scintigraphy was performed 24 h after infliximab dosing. Response to infliximab was defined as a drop of >100 points in the CDAI 2 weeks after infliximab treatment. This study was approved by the local medical ethical review board of the Academic Medical Center, Amsterdam, The Netherlands.
Mucosal T cell isolation and analysis
Mucosal biopsy specimens were collected from three patients during endoscopy and immediately placed in ice-cold phosphate-buffered saline (PBS). To isolate lamina propria mononuclear cells (LPMNCs), biopsy specimens were mechanically destroyed using an automated mechanical tissue-disaggregation device (Medimachine System, Dako, Glostrup, Denmark). The obtained cell suspensions were washed twice in PBS. To prevent changes in the studied surface markers, no collagenase step was used during isolation. Cell suspensions were centrifuged with Ficoll (Pharmacia, Uppsala, Sweden) and the mononuclear cells were subsequently passed through a 40 μM filter cell strainer (Becton/Dickinson Labware, Franklin Lakes, New Jersey, USA). Cells were then washed with FACS buffer (PBS, containing 0.5% bovine serum albumin, 0.3 mmol/l EDTA and 0.01% sodium azide) and were kept on ice for the rest of the procedure. After washing, LPMNCs were placed in FACS buffer and stained with CD4 PE antibody for 30 min on ice. Subsequently, LPMNCs were washed twice with PBS and placed in annexin-binding buffer and incubated 15 min with annexin V—fluorescein isothiocyanate, and then with 7-amino-actinomycin (7AAD, Via-Probe BD Bioscience) for 5 min, both on ice in the dark, and analysed by flow cytometry (FACS Calibur). 7AAD was used to exclude necrotic cells. The LPMNC population was gated according to the localisation on the forward/side scatter, and further analysis of the percentage of CD4 apoptotic cells was performed in the 7AAD-negative subpopulation—that is, necrotic cells. Data shown are representative for three patients.
Scintigraphy
Scintigraphy in animals was performed using a dedicated animal pinhole γ-camera SPECT as described earlier.25 A tungsten pinhole insert of 3 mm aperture was used. All studies were acquired with a 15% energy window on the 140 keV 99mTc photo peak. An operating workstation (Hermes, Nuclear Diagnostics, Stockholm, Sweden) was used to control both the camera and the step motor. The SPECT acquisition was performed 1 h after intravenous injection of 50 MBq 99mTc–annexin. In all, 50 projections of 30 s in a 64×64 matrix were acquired in a 360° orbit. SPECT reconstruction was performed using an application program (Hermes, Nuclear Diagnostics,) adapted to pinhole SPECT, using filtered back-projection. A Butterworth post reconstruction filter (order, 5; 0.8 cycle/cm) was applied.
Images were interpreted and scored by an experienced nuclear medicine physician, blinded to the cytological data. A colon uptake ratio (CUR) was determined semiquantitatively by regions-of-interest analysis as described before.26 Five consecutive transverse slices with the highest colon uptake were selected and added. Counts in each region were obtained for the colon, spinal bone marrow and abdominal (small bowel) area as background. The CUR was calculated by subtracting abdominal background activity from colon activity and subsequently dividing the corrected colon uptake by bone-marrow uptake (counts colon−counts background)/(counts bone marrow−background). Immediately after scintigraphy, the mice were killed by cervical dislocation and colons were removed through a midline incision.
Scintigraphy in patients was performed on a large field-of-view SPECT-CT camera (GE Infinia General Electric (GE) Medical, Den Bosch, The Netherlands) equipped with low-energy high-resolution collimators. Patients were positioned supine on the imaging table with the abdomen in the field of view. A 20 min SPECT scan (60 views, 35 s/view, 128 matrix) was performed 60 min after intravenous injection of 450 MBq 99mTc–annexin V. Immediately after scintigraphy, a low-dose CT for attenuation correction and anatomical mapping was performed on the same gantry without moving the patient. Similar to the animal studies, five consecutive transverse slices were added. On the basis of these images, the colon was divided into the segments ascending, transverse, descending colon and rectosigmoid. Guided by endoscopy, a background-corrected colon uptake was determined in a segment with active disease based on an uptake hierarchical supervisor-guided protocol. The CUR was expressed as a background-corrected ratio to bone marrow (CUR). Pre- and post-therapeutic scans were assessed in the same segments of colon or ileum.
Statistical analysis
Results are expressed as median (range) or as mean (SEM) where appropriate. All statistical tests were performed using SPSS v 2.01 for Windows. A p value of ⩽0.05 was considered to represent a significant difference. Differences in mice colorectal 99Tc uptake between the various treatment groups (NaCl, control antiserum and mαTNF) were analysed by the heteroscedastic one-tailed t test. Differences between treatment groups in time were tested by analysis of variance for repeated measures. Correlations between change in CDAI and CRP were analysed using Spearman’s correlation coefficient (r).
RESULTS
Experimental colitis
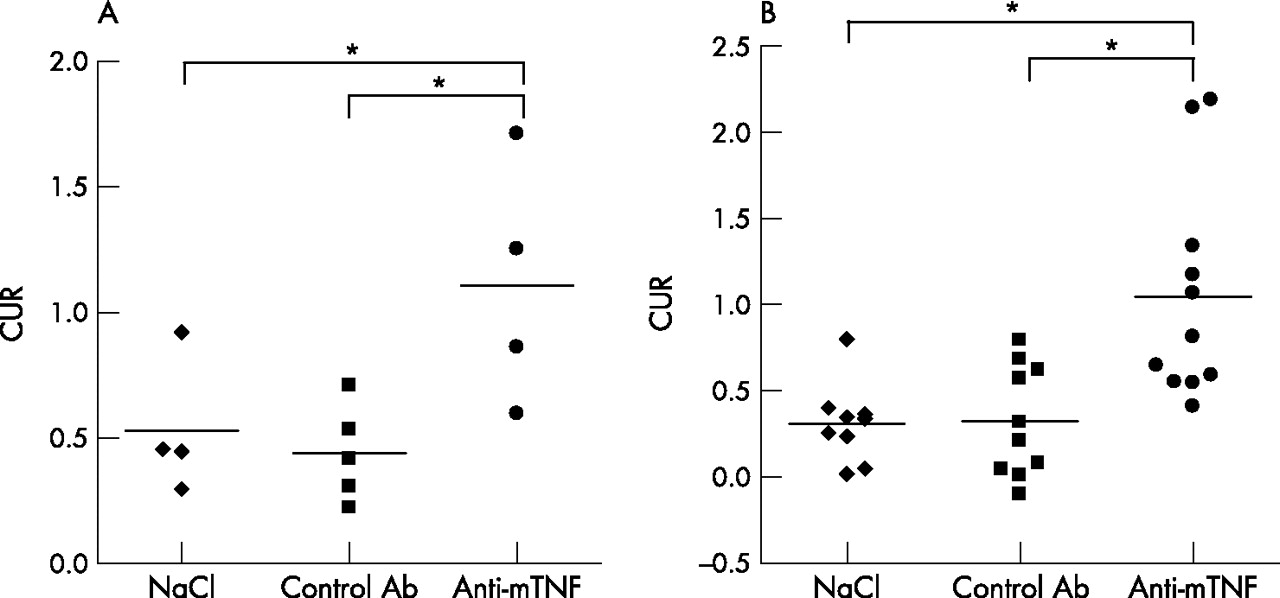
For the experiments in TNBS colitis, a total of 30 mice were used in 4 separate experiments. For the transfer colitis, CD45RBhigh CD4 cells (1–4×105) were transferred to two groups of CB17 SCID mice. In this experiment, a total of 13 mice were used, in two separate experiments. Both models were effective in inducing colitis: in the transfer model weight loss was observed 3 weeks after the transfer, whereas in the TNBS model, colitis was evident with mice demonstrating diarrhoea and rectal blood loss. BALB/mice had a baseline histopathological score of 0.3 (0.5), and normal SCID mice had a score of 0.2 (0.2). In TNBS-induced colitis, the histopathological score increased to 10.6 (2.8), whereas in the transfer colitis the histopathological score increased to 1 (0.6). Hence, all mice had colitis at time of collection of the colons, and this was confirmed by decreasing body weight curves and increasing colon weights (data not shown). In mice with either transfer or TNBS colitis treated with NaCl, 99mTc–annexin V was hardly detectable in the colon (figs 1⇓ and 2A,B⇓). The average colorectal 99mTc uptake was 0.53 (0.27) and 0.31 (0.23), respectively. On administration of negative control chimaeric antibody cVaM, the average colorectal 99mTc uptake was 0.44 (0.19) and 0.32 (0.32) for the transfer and TNBS models, respectively. Thus, chimaeric antibodies are not proapoptotic as such. Injection of the chimaeric murine/rat monoclonal cV1q caused an average colorectal 99mTc uptake of 1.11 (0.48) for the transfer model and 1.04 (0.63) for the TNBS model (fig 1 and 2A⇓⇓,B). The average colorectal 99mTc uptake ratio differed significantly between NaCl and anti-murine TNF antibodies in the transfer and TNBS colitis models, p = 0.016 and p = 0.01, respectively. Likewise, the average colorectal 99mTc uptake ratio differed significantly between control chimaeric antibodies and anti-murine TNF antibodies in the transfer and TNBS colitis models, p = 0.04 and p = 0.02, respectively. Healthy rodents show little annexin V binding in the mucosa of the intestine (not shown), demonstrating that such high annexin V binding is not a characteristic of the uninflamed mucosa. On the basis of the annexin uptake ratio in experimental colitis, we concluded that anti-TNF antibodies cause a rapid increase in apoptosis in the murine colon.

99m Technetium–annexin V single-photon emission computer tomography (SPECT) of murine colitis. Mice with trinitrobenzene sulphonate-induced colitis were treated with a saline, chimaerical rat-anti-mouse tumour necrosis factor (TNF) antibody (cV1q) or a chimaeric rat-anti-mouse control antibody (cVaM). Apoptosis was visualised using annexin V SPECT γ-camera. The results show relatively low intestinal annexin V uptake in saline and control antibody (Ab)-treated animals, and high uptake levels indicating increased levels of apoptosis in the intestine on treatment with a TNF-neutralising antibody. Representative coronal, transversal and sagittal sections are shown. Arrows have been electronically added, indicating the localisation of the colon and the 99mTc annexin V increased signal.

Quantification of annexin V single-photon emission computer tomography (SPECT) during experimental colitis. Transfer colitis (A) and trinitrobenzene sulphonate-induced colitis (B) was induced as described in the Methods sections and animals were treated with chimaeric rat-anti-tumour necrosis factor (TNF) antibody (cV1q) or a chimaeric rat-anti-mouse control antibody (cVaM). Apoptosis in the intestine was quantified using annexin V SPECT, a γ-camera and quantification software. Colorectal uptake ratio (CUR): 99m technetium–annexin V SPECT colonic uptake expressed as a background-corrected ratio to bone marrow. The results show relatively low intestinal annexin V uptake in saline and control antibody (Ab)-treated animals, but apparently high levels of apoptosis in the intestine are observed on treatment with a TNF-neutralising antibody. *p<0.05 and **p<0.01 as tested with a heteroscedastic one-tailed Student’s t test.
Patients with Crohn’s disease
Fourteen patients with active Crohn’s disease consented to participate in this study. Table 1⇓ summarises the patients’ characteristics. The mean CDAI was 381 (range 229–587) points, the mean CRP 55.9 (3–154) mg/l, and all except one patient had active distal disease accessible for endoscopy. One patient had a severe ileitis, and did not undergo endoscopy. All patients received corticosteroids and/or immunomodulators at baseline (table 1⇓). Three patients received episodic infliximab infusions before inclusion. These patients had shown a clinical response to their last infusion. Infliximab treatment did not result in any serious adverse event. All patients underwent uncomplicated dual SPECT scanning (at baseline and within 24 h after infliximab treatment).
Patients’ characteristics
Clinical response to infliximab
Figure 3A,D shows the clinical responses of the 14 included patients. The mean CDAI at baseline for all patients was 381 points (range 220–587), which decreased to 198 at week 2 (range 36–394, p<0.01). At week 2, the CDAI decreased >100 points in 10 patients (mean decrease 226 points, range 113–359), demonstrating a predefined clinical response. Four patients failed to show a response to infliximab, the mean change in CDAI was 12 points. In addition, responses were confirmed by changes in CRP. CRP levels decreased significantly on infliximab treatment when compared with baseline. The mean levels decreased from 50.4l to 7.5 mg/l (fig 3B⇓, p = 0.04). No significant correlation was observed between change in CDAI and change in CRP (r = −0.19, p = 0.517; −0.097%, p = 0.0742).

Quantification of annexin V single-photon emission computer tomography (SPECT) before and after infliximab treatment of patients with Crohn’s disease. (A) Clinical response to infliximab as measured by Crohn’s Disease Activity Index (CDAI). (B) Plasma C reactive protein (CRP) levels at baseline and after infliximab treatment. (C) Apoptosis as measured by annexin V SPECT just before (baseline) and 24 h after infliximab infusion, expressed as colonic uptake ratio (CUR; see Methods section). (D) Responders to infliximab have a higher CUR of 99mTechnetium–annexin V (98.6%) than non-responders (15.2%, p = 0.03). The results show a correlation between the occurrence of high amounts of apoptosis in the intestine 24 h after infliximab infusion and clinical response to infliximab, determined 2 weeks after infliximab treatment. (E) Influence of co-medication on infliximab-induced CUR responses. Azathioprine (AZA) did not influence the incorporation of 99mTc-annexin V in the gut mucosa in patients with Crohn’s disease receiving maintenance treatment. NS, not significant.
99mTc Annexin V uptake
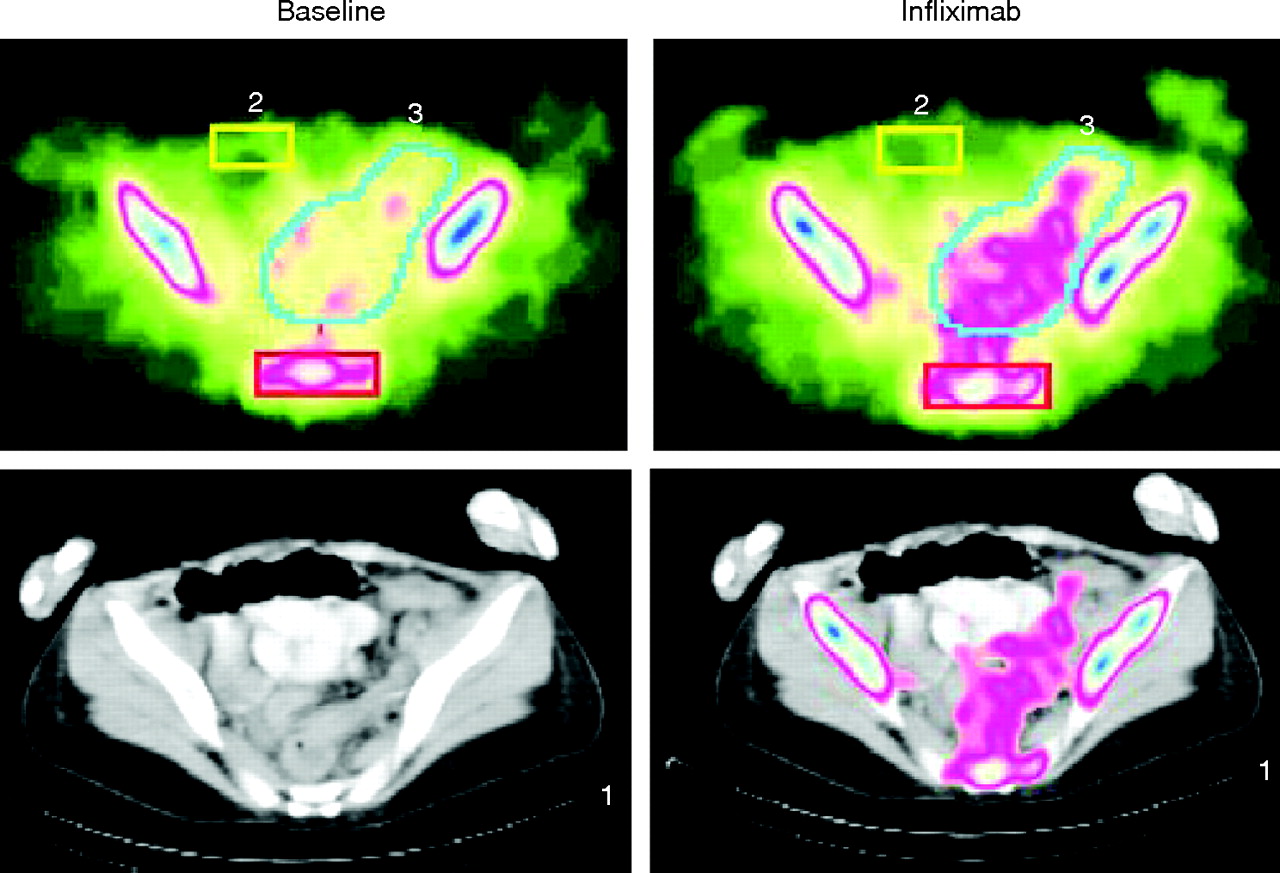
Baseline SPECT scanning displayed limited 99mTc–annexin V accumulation in the colon, and the CUR was 0.24 (0.03). An increase in CUR to 0.41 (0.07) was observed (p<0.01) 24 h after receiving 5 mg/kg infliximab (Fig 3C⇑; table 2⇓). Figure 5⇓ shows representative SPECT-CT images of the sigmoid colon before and after infliximab infusion. Subsequently, we investigated whether the accumulation of 99mTc–annexin V was different in patients exhibiting a favourable response to infliximab from those who did not display an objective response. The CUR increased in both responders and non-responders, but interestingly the increase in CUR was markedly higher in the group of responders (fig 3D⇑). In 10 responding patients, the mean increase in CUR was 98.6%, compared with 15.2% in the 4 non-responding patients (p = 0.03; fig 3D⇑). Endoscopic investigation of the patients involved, before experimentation, had shown that disease was present in the colon or both in the colon and small intestine. The scintigraphic signals obtained corresponded with these diseased regions, at least at this macroscopic level (table 2⇓), especially in the colon. The correlation with disease localisation and increased annexin V uptake was striking and held true for 13 of 14 patients (1 did not undergo endoscopy). These data suggest that higher levels of apoptosis correlate with clinical response to infliximab. 99mTc–annexin V uptake was analysed before and after infliximab treatment in the subgroup of seven patients using azathioprine (AZA; an apoptosis-inducing agent27) at baseline. Co-treatment with infliximab did not result in higher CUR in this subgroup receiving AZA (fig 3E⇑). Importantly, a volunteer not displaying colitis was infused with 99mTc–annexin V, and on analysis showed little annexin V binding in the intestine (not shown), demonstrating that the high annexin V binding is not a characteristic of the uninflamed mucosa, but is apparently an active representation of the clinical healing process.
Summary of disease localisation, endoscopic activity, colonic uptake ratio and severity of Crohn’s disease in patients

Infliximab administration increases apoptosis in CD4 lamina propria mononuclear cells (LPMNCs) isolated from fresh biopsy specimens obtained before or 24 h after infliximab treatment of patients with Crohn’s disease. The figure shows the relative proportion of apoptotic cells in the CD4 cell population at baseline and after treatment with infliximab. Freshly isolated LPMNCs were stained with annexin V, CD4 and 7-amino-actinomyocin (7AAD). The LPMC population was gated according to the localisation on the forward/side scatter and further analysis of the percentage of CD4 apoptotic cells was performed in the 7AAD-negative subpopulation. (Data shown are representative for the three patients analysed.) FITC, fluorescein isothiocyanate; PE, phycoerythrin.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Example of 99m Technetium-annexin V single-photon emission computer tomography (SPECT) of human Crohn’s disease. Apoptosis in the intestine of patients with Crohn’s disease was visualised just before (baseline) and 24 h after infliximab treatment. The picture shows a representative SPECT image in pseudocolours and a CT image with a superimposed SPECT image. The scintigraphic signals obtained corresponded with the diseased regions in the colon, indicating a correlation with disease localisation and increased 99mTc–annexin V uptake.
Mucosal T cell analysis
To test whether lamina propria T cells were indeed target cells for annexin V binding, LPMNCs were isolated from fresh biopsy specimens and the percentage of apoptotic cells in the CD4 positive subpopulation was analysed in three patients. The analysis of 7AAD-negative cells showed marked increase in apoptosis of CD4 cells 24 h after infliximab administration (fig 4⇑). This suggests that apoptosis of lamina propria T cells contribute to the increased level of apoptosis in the intestine.
DISCUSSION
Infliximab has become the mainstay for the treatment of steroid-refractory Crohn’s disease; however, the molecular mechanism underlying its beneficial effects remains unclear and it is difficult to predict the clinical success of this expensive treatment in individual patients. Recently, it was shown that in vitro infliximab can bind to membrane-bound TNF and cause apoptosis in activated T cells15 possibly through reverse signalling,16 but the in vivo clinical relevance of these findings remained unclear. In this study, we showed in vivo that apoptosis in the intestine is induced on chimaeric anti-TNF treatment in both experimental colitis and in human Crohn’s disease.
Apoptosis is a distinct mode of cell death and represents a crucial regulatory mechanism to remove redundant cells in many physiological events. Recently, the imaging of drug-induced apoptosis has generated enormous interest both in experimental and clinical research.28 Annexin V has been validated for in vivo scintigraphic imaging of apoptosis both in animals20,29–,32 and in humans.33,34 In the management of malignant disorders, this has proved a valuable tool for the accurate monitoring of apoptotic tumour response and chemosensitivity,35–,37 as well as the early prediction of chemoresistance in response to various pro-apoptotic interventions.35 As further evidence that the chronicity of inflammation in Crohn’s disease is largely due to apoptotic-resistant cells in affected Crohn’s mucosa, we have previously shown that infliximab exerts a pro-apoptotic effect on lamina propria or peripheral T cells from patients with active Crohn’s disease,18 which was subsequently shown by Di Sabatino et al38 to be caspase-dependent phenomenon. The increased accumulation of radioactivity after infusion of infliximab in the colonic region of patients with Crohn’s disease is certainly in agreement with this hypothesis, but this interpretation of our data critically depends on the assumption that the colonic scintigraphic signals obtained are derived from annexin binding to apoptotic T cells. To confirm this, T cells were isolated from biopsy specimens of three study patients and investigated with FACS for the presence of annexin V and the apoptosis status in the T cell compartment by co-staining with CD3 antibodies and 7AAD. 7AAD only enters membrane-compromised cells and binds to DNA. When the 7AAD-negative compartment was investigated (thus excluding necrosis), an increase in annexin V-positive cells was observed after infliximab infusion. Thus, the increased scintigraphic signals seem to include apoptosis in the T cell compartment and provide, to a certain extent, a bona fide representation of in vivo apoptosis. This observation correlates well with studies in which scintigraphic imaging was used for examining in vivo apoptosis, providing evidence that the signals obtained are truly generated by annexin V binding to apoptotic cells.20,30,39 To what extent other cell types (ie, macrophages and dendritic cells) contribute to the scintigraphic signals remains uncertain. Alternatively, high annexin V binding to the gut mucosa may be a characteristic of the uninflamed mucosa that is lost on inflammation. In this case, the observed increase in annexin V binding and its correlation with clinical efficacy would be an epiphenomenon of healing and not indicative of the remission process in itself. Healthy rodents and a healthy volunteer, however, show little annexin V binding in the intestine (RJB, data not shown), showing that such high annexin V binding is not a characteristic of the uninflamed mucosa. Thus, the increase in annexin V binding after infliximab treatment is a specific manifestation of the remission process. Together with the observation that this increase in annexin V uptake is at least partially dependent on the T cell compartment (although macrophages and monocytes also probably contribute to this signal40,41), and the correlation of annexin V uptake and clinical benefit of infliximab treatment, our data clearly indicate that annexin V uptake is a characteristic of remission induction, and that apoptosis might even be causative in this respect.
The observation that absolute levels of apoptosis correlate well with the clinical response in patients has important implications. Non-responders do not seem to have an intrinsic deficiency in their capacity to react to infliximab with apoptosis; rather, the levels of apoptosis induced in non-responders seem to be insufficient. To further support this notion, both in responders as well as non-responders, CRP levels are reduced in response to infliximab treatment hence, it seems that the magnitude of the infliximab-induced apoptosis is important, and non-responders’ reaction to the treatment by increasing apoptosis in the intestine is not sufficiently large to allow clinical recovery. A logical consequence of this notion is that when these patients are given apoptosis-inducing drugs along with infliximab, clinical responses may become apparent. We recently observed that methotrexate might act synergistically with infliximab by inducing apoptotic responses in activated T cells (unpublished observations). Also, AZA is known to induce apoptosis as a consequence of Rac1 inhibition27 and is thus an interesting candidate for co-application with infliximab. Interestingly, no significant increase was seen in baseline CUR in patients with AZA co-medication compared with the AZA-negative group. A possible explanation for this observation is that the low level of apoptosis might not be detectable in the maintenance setting. Finally, the observation that apoptosis levels in non-responders are lower than in responders requires validation in a larger cohort of patients, but, if confirmed, would provide a tool that can predict the response to infliximab and increase cost effectiveness.
In conclusion, infliximab rapidly induces apoptosis in the intestine of patients with Crohn’s disease. This is probably a key initiating event that triggers mucosal healing in patients. Further studies are warranted to study differences in the regulation of apoptosis in patients with Crohn’s disease and the possibilities of personalising biological treatment.
Acknowledgments
We thank Dave Shealy for the supply of chimaeric mouse antibodies, M Tanck, Department of Biostatistics, AMC, for the helpful discussions and Joost Daalhuisen for his expert technical assistance.
REFERENCES
Footnotes
↵* These authors equally contributed to this paper.
Published Online First 2 November 2006
Funding: MPP is supported by the Dutch Digestive Disease Foundation. DWH is a clinical fellow of the Netherlands Organisation for Health Research and Development.
Competing interests: None.