Article Text

Statistics from Altmetric.com
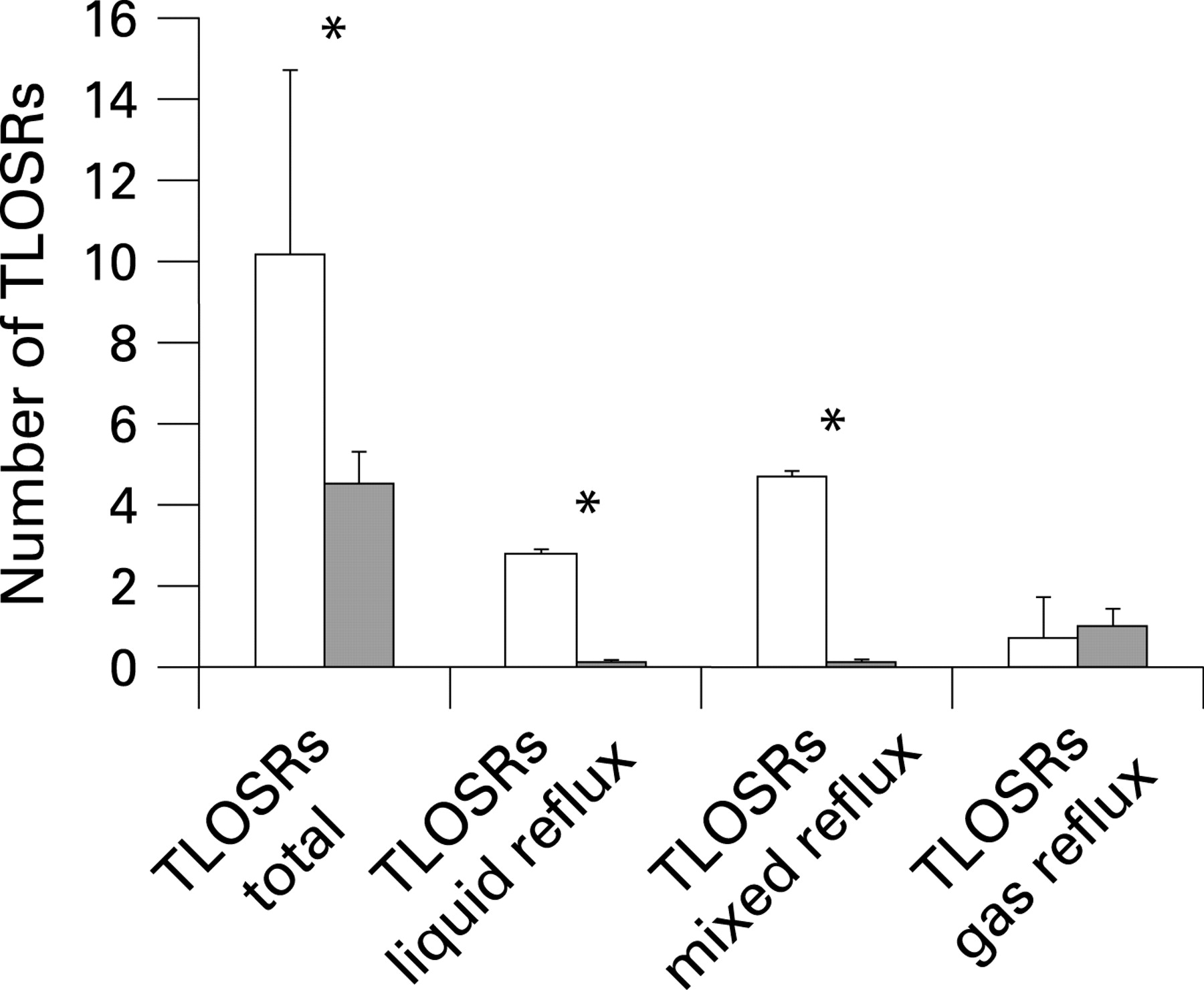
Mechanisms of acid, weakly acidic and gas reflux after anti-reflux surgery
Fundoplication reduces oesophageal acid exposure and reflux symptoms in patients with gastroesophageal reflux disease (GORD). The mechanisms behind this are incompletely understood and the effects on non-acid and gas reflux have not been fully evaluated. In this study, 14 patients with GORD were investigated before and three months after fundoplication. The patients underwent impedance pH monitoring to assess the reflux pattern and high-resolution manometry to evaluate the morphology of the oesophagogastric junction and the occurrence of transient lower oesophageal sphincter relaxations (TLOSRs), the main mechanism behind gastroesophageal reflux. Fundoplication was found to greatly reduce both acid and weakly acidic reflux, whereas gas reflux was reduced to a lesser extent. Abolition of the double high-pressure zone profile at the oesophagogastric junction (hiatal hernia), a reduced incidence of TLOSRs and a decreased percentage of TLOSRs associated with reflux were found to be important mechanisms involved in the reduction of reflux events after fundoplication. Unfortunately, no clear mechanisms explaining persistent symptoms or development of gas–bloat symptoms after fundoplication were detected.
See pages 10.1136/gut.2007.133298

Endoscopic trimodal imaging for detection of early neoplasia in barrett’s oesophagus
Endoscopic surveillance of patients with Barrett’s oesophagus is recommended to detect neoplastic lesions at an early and curable stage. However, early neoplastic lesions (high-grade intraepithelial neoplasia or early cancer) are difficult to detect with standard endoscopic techniques and may be missed by random biopsies. In this multi-centre study the diagnostic potential of a new endoscopic system—endoscopic tri-modal imaging (ETMI)—which incorporates high-resolution endoscopy (HRE), autofluorescence imaging (AFI) and narrow-band imaging (NBI), was evaluated in 84 patients with Barrett’s oesophagus. Biopsies were obtained from all suspicious lesions found with the endoscopic techniques, followed by random biopsies. AFI almost doubled the number of patients detected with early neoplastic lesions relative to HRE. However, AFI was also associated with a high false-positive rate (81%). NBI could reduce this false-positive rate to 26% but also misclassified two lesions containing early neoplastic changes. Moreover, in three of the patients early neoplastic changes were not detected with any of the endoscopic techniques but only with random biopsy sampling. Further randomised studies of this promising technique are needed before incorporating it into Barrett’s surveillance.
See pages 10.1136/gut.2007.134213

Obesity and reflux independently increase the risk of oesophageal adenocarcinoma
Obesity and reflux both increase the risk of oesophageal adenocarcinoma (OA) and it has been assumed that reflux is the final common path. This case–control study attempted to examine the interaction between obesity and reflux in determining the risk of OA. This study compared 1191 patients with oesophageal cancer with controls from the electoral roll. Multivariate analysis showed a modest increased risk of OA in patients who were overweight with the biggest effect being found in those <50 years old in whom body mass index (BMI) >30 was associated with odds ratio (OR) of 10.2 (CI 2.7 to 40.9) (see table). When this was adjusted for reflux, the OR was still substantial at 7.5 (CI 1.7 to 33.0). Those with frequent reflux also had an increased risk of OA (OR 6.4 (CI 4.5 to 9.0). Obesity aggravated the risk, so that those with a BMI >30 had an OR of 16.5 (CI 8.9 to 30.6). The effect of obesity independent of reflux may be mediated through the increase in insulin and insulin-like growth factors and/or the products of adipose tissues themselves (adipokines).
See pages 10.1136/gut.2007.131375
Autologous haematopoietic stem cell transplantation without CD34+ cell selection in refractory crohn’s disease
A proportion of patients with Crohn’s disease are refractory to all available pharmacological treatment alternatives. Recently, promising results have been obtained with autologous haematopoietic stem cell transplantation (HSCT) with CD34+ cell selection in a limited number of patients with severe, refractory Crohn’s disease. In this Italian study, a protocol of autologous HSCT with unselected peripheral blood stem cells in an effort to reduce procedure-related toxicity was used in four patients with refractory Crohn’s disease. The primary endpoint of clinical remission at 3 months (Crohn’s disease activity index <150) was reached in all four patients and endoscopic and clinical remission was maintained after a median follow-up of 16.5 months in three of those four patients, despite withdrawal of all drugs. Moreover, the treatment was generally well tolerated and no life-threatening infections were observed. Whether autologous HCST in refractory Crohn’s disease adds to the effect of immunosuppression/granulocyte colony stimulating factor alone (used for the mobilisation of the peripheral blood stem cells and the conditioning) will hopefully be answered in an ongoing randomised European trial (ASTIC).
See pages 10.1136/gut.2007.128694

UK Bowel Cancer Screening Pilot shows decrease in emergency admissions for colorectal cancer
The rationale of the National Colorectal Screening Programme now being initiated in the UK is to increase the detection of early stage colorectal cancer (CRC). This study reports the effect of the pilot study for this programme, which ran in Coventry and Warwickshire from 2000 to 2004 and involved 187 777 subjects aged 50 to 69 years. Individuals were invited to submit faecal occult blood tests every 2 years. Uptake was 57% and those with positive results underwent colonoscopy with a yield of 1.6 CRC/1000 colonoscopies. Over the 5 years of study, total CRC presentations were constant but the proportion of emergency admissions declined (see fig). There was a 47% reduction in both emergency admission rates and emergency surgery. Furthermore, the 30-day CRC emergency operative mortality fell substantially from 48% in 1999 to 13% in 2004. These results indicate the potential substantial benefits of this programme.
See pages 10.1136/gut.2007.120253

Novel tumour suppressor in hepatocellular carcinoma
The protein melanoma inhibitory activity 2 (MIA2) is known to play a central role in early melanoma development and has been found in other tumours where low expression levels are associated with early tumour progression. This study examined its expression and function in both hepatocellular carcinoma (HCC) and HCC cell lines. An HCC tissue microarray was constructed from 85 HCC tumours and used to show, as predicted, a linear relation between mRNA expression for MIA2 and hepatocyte nuclear factor (HNF-1), which by binding to the MIA2 promoter is known to control MIA2 transcription. HCC samples showed marked down-regulation of both HNF-1 and also MIA2. The authors showed that transfecting HCC cell lines with an MIA2 expression vector could restore MIA2 expression and inhibit proliferation both in vitro and also in vivo, when tumour cells were implanted into nude mice (see fig). They also showed in their tissue array that those tumours with high MIA2 expression had a reduced proliferation rate and a lower tumour stage. The authors conclude that MIA2 can be considered a tumour suppressor in HCC and is, therefore, a potential marker for prognosis as well as a potential therapeutic target.
See pages 10.1136/gut.2007.129544

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Linked Articles
- Oesophagus
- Oesophagus
- Oesophagus
- Inflammatory bowel disease
- Colon cancer
- Hepatology