Article Text

Statistics from Altmetric.com
Inflammatory bowel disease
THE USE OF ADALIMUMAB IN THE MANAGEMENT OF CROHN’S DISEASE: SCOTTISH SOCIETY OF GASTROENTEROLOGY AUDIT 2007
G. Ho1, L. Smith1, S. Aitken1, H. Lee1, D. Ting1, J. Fennell1, C. Lees1, K. Palmer1, I. Penman1, A. Shand1, I. Arnott1, M. Priest2, R. Boulton-Jones3, R. Russell4, C. Mowat5, D. Wilson6, J. Satsangi1. 1Gastrointestinal Unit, Western General Hospital, Edinburgh, 2Gastrointestinal Unit, Gartnavel General Hospital, 3Gastrointestinal Unit, Victoria Infirmary, 4Gastrointestinal Unit, Yorkhill Hospital, Glasgow, 5Gastrointestinal Unit, Ninewells Hospital, Dundee, 6Gastrointestinal Unit, Royal Hospital for Sick Children, Glasgow, UK
Introduction: Adalimumab is a humanised monoclonal antibody targeting tumour necrosis factor-α. Recent clinical trials have demonstrated its efficacy in Crohn’s disease, however experience in clinical practice remains limited.
Aims & Methods: We present the experience on the efficacy and safety of Adalimumab in a Crohn’s disease (CD) cohort in Scotland over a 4-year period (2003–7). All members of the Scottish Society of Gastroenterology were approached and data extraction was performed from case notes using a standard proforma form.
Results: 42 (26 females; age at therapy: 28.6 years, IQR 19.5–40.2 including 5 paediatric cases) patients were treated with Adalimumab from 7 hospitals. 34 (80.9%) patients were treated using an 80/40 mg induction regime followed by fortnightly 40 mg treatment (6 and 2 patients had 160/80 mg and 24/24 mg induction respectively). 38 (90.5%) patients had had previous infliximab infusions and 11 (26.2%) were primary infliximab non-responders. Over a median period of 0.57 year (IQR 0.26–1.71), 23 (54.7%) patients achieved and were maintained in steroid-free remission (survival curve analyses 56.3% at 1-year follow-up). Two (40%) paediatric CD cases achieved steroid-free remission (range 0.44–0.49 years). 19 of 34 (55.9%) patients on fortnightly therapy required dose escalation to 40 mg weekly (0.65 years IQR 0.13–1.44). 7 (63.6%) primary non-responders to infliximab achieved and maintained steroid-free remission (median 0.80 years follow-up IQR 0.44–1.87). There were 4 (9.5%) serious complications requiring permanent discontinuation of Adalimumab therapy: 2 patients developed serious infective complications (severe facial cellulitis and psoas abscess secondary to colonic perforation, after 8 weeks and 2.6 years of therapy), one patient developed lung cancer and one with central demyelinating illness (after 1.7 years and 9 weeks of therapy respectively). No patients developed infusion reactions.
Conclusion: Adalimumab is efficacious in the treatment of patients with refractory CD, with particular benefit in patients who have lost response or developed adverse reaction to infliximab. In this audit, we also present data for the first time in paediatric Crohn’s disease. However, many patients require escalation of dosing regime. Moreover, the treatment carries definite risks of serious adverse events, and careful patient selection, and continuous monitoring is needed.
ONCE- VERSUS TWICE-DAILY MESALAZINE (PENTASA) GRANULES FOR THE MAINTENANCE OF REMISSION IN ULCERATIVE COLITIS: RESULTS FROM A MULTINATIONAL RANDOMISED CONTROLLED TRIAL
A. Dignass1, H. Veerman2. 1Head Department of Medicine I, Markus-Krankenhaus, Frankfurter Diakonie-Kliniken, Frankfurt-Main, Germany, 2Medical, Ferring Pharmaceuticals, Hoofddorp, The Netherlands
Introduction: Patients with quiescent ulcerative colitis (UC) do not frequently adhere to prescribed mesalazine treatment. This is, in part, due to the low acceptability of currently available mesalazine formulations, which often require multiple-daily dosing regimens and a high number of tablets. Non-compliance is directly linked to relapse and disease exacerbation. This study investigated remission and relapse rates in patients with UC in remission receiving once daily (od) a single 2 g mesalazine granules sachet or twice daily (bd) a 1 g mesalazine granules sachet.
Aims & Methods: A 12-month, multicentre investigator-blinded randomised controlled trial. Patients with mild to moderate UC in remission who had had a relapse within the past year were randomised to receive either mesalazine granules 2 g/day given od or bd. Clinical evaluations were undertaken at 0, 4, 8 and 12 months. Primary objective was to demonstrate non-inferiority (defined as not more than 10% less efficacy below the od treatment) of the two regimes in terms of probability to remain in clinical and endoscopic remission during one year defined by an UCDAI score of <2, or an UCDAI of 2 without any adjustment of therapy. Treatment difference was calculated using Kaplan-Meier methodology.
Results: 362 patients were randomised. At end-of-study, 73.8% and 63.6% of patients in the od and bd groups were in clinical and endoscopic remission, respectively. The difference between the two treatment groups after one year was significantly above the non-inferiority limit with a treatment difference of 11.9% in favour of od (p = 0.024). Once daily dosing had a higher compliance than bd dosing in terms of % sachets used. Patient questionnaires yielded higher compliance scores for od than bd (p<0.05) and patient acceptability of treatment was significantly better for od (96.3% vs 85.6%, p<0.001) at end-of-study.
Conclusion: Once-daily 2 g mesalazine granules sachets (PENTASA) are an effective maintenance therapy in patients with mild to moderate UC. A once daily dosing regimen using a single 2 g sachet is not only non-inferior but even superior to twice daily dosing. Mesalazine granules taken once daily (2 g) ensure better remission rates, patient compliance and acceptability than twice-daily (2×1 g) administration.
Endoscopy free papers
CAN DEATH FOLLOWING ERCP BE PREDICTED? RESULTS OF A LARGE SCALE PROSPECTIVE STUDY
E. J. Williams. On behalf of the BSG audit of ERCP Steering Committee, British Society of Gastroenterology, London, UK
Introduction: The incidence of early mortality (from all causes) following endoscopic retrograde cholangiopancreatography (ERCP) is rarely described in prospective studies, though retrospective analyses of deaths suggest patient selection could be improved.
Aims & Methods: The aims are to examine 30-day mortality following ERCP, and identify independent predictors of early death. Results are derived from a prospective multicentre study of ERCP complications, based in 5 English regions. Where patients consented to follow-up, death within 30 days of ERCP was identified through contact with carers and interrogation of hospital electronic records. Where patients did not consent to follow-up mortality was calculated from death registrations. Binary regression analysis of participating patients’ first recorded procedures identified independent risk factors for early mortality.
Results: A total of 6910 ERCPs were performed in 66 centres during the study period. Consent for detailed follow-up was acquired for 5264 procedures, performed on 4561 patients. A therapeutic intervention was attempted in 3447/4561 (76%) of these patients as part of their first recorded ERCP. In total 121 participating patients (2.7%) died within 30 days of first recorded ERCP. Thirty-day mortality among non-participating patients was calculated to be higher (92/1646; 5.6%). Closer examination of participating patients revealed 18/121 deaths were directly attributable to the patient’s first recorded ERCP, with a further 2/121 deaths attributable to a second ERCP performed within 30 days of the first procedure. The remaining 101/121 deaths resulted from progression of the underlying disease process (which was carcinoma in 82 cases). Risk factors for death (OR, 95% CI) among participating patients were: ASA score (120.1, 24.5 to 588, when ASA 5 patients were compared to ASA 1 patients); a malignant indication for ERCP (2.94, 1.67 to 5.15); lower albumin (1.05, 1.02 to 1.08 for every g/l decrease); ln bilirubin (1.49, 1.18 to 1.88) and ln white cell count (1.54, 1.09 to 4).
Conclusion: The extrapolated 30-day mortality following ERCP, based on participating and non-participating patients is 3.4%. While detailed analysis was limited to 5264/6910 procedures, results suggest that most deaths arise from progression of underlying disease, rather than as a result of ERCP itself. ASA score and pre-ERCP diagnosis are identified as important predictors of outcome.
VALIDITY AND RELIABILITY OF AN ACCREDITATION ASSESSMENT FOR COLONOSCOPY
R. Barton. For the Joint Advisory Group on Gastrointestinal Endoscopy and NHS Bowel Cancer Screening Programme, Newcastle University and Northumbria Healthcare NHS Trust, Newcastle upon Tyne, UK
Introduction: After national audit demonstrated very variable quality of colonoscopy, the introduction of the NHS Bowel Cancer Screening Programme prompted the introduction of a searching assessment to select the screening programme’s future colonoscopists. Leading endoscopists, trainers and the JAG collaborated to develop an appropriate assessment tool after consultation with clinical educationalists in 3 countries. This comprised performance data, a knowledge test (MCQ), and a DOPS (Direct Observation of Procedural Skills) assessment.
Aims & Methods: The aims of this study are to determine the validity and reliability of the assessment. A true/false 30 item × 5 answer MCQ was devised covering key issues. To ensure both professional and educational input, DOPS forms from two centres were reviewed by the Trainers Group appointed under the NHS National Endoscopy Training Programme, and important colonoscopy skills were identified and amalgamated into domains. Detailed descriptors for all skill levels were written for each domain. An outline curriculum was published, and assessors underwent both the assessment and further assessor training. Self-reported, verified, performance and demographic data, as well as assessment data both from the MCQ and DOPS over two cases by two assessors were collected prospectively from 76 candidates. Semi-structured questionnaires were collected from candidates and 17 assessors on the validity of the assessment.
Results: Colonoscopists submitted performance data and attempted the assessment. In 2284 paired judgments over 76 candidates during a total of 151 cases, overall there was 96% congruence of agreement across the pass/fail divide (98% for major domains), and high absolute congruence between assessors in many domains, for example 72.4% for “communication”, 69% “maintains luminal views”, 73% “uses torque steering” and 81% “adequate mucosal visualisation”. The expert global opinion agreed with the grading system in 74/76 (97%) of cases. Gradings correlated weakly with self-reported caecal intubation rates and MCQ scores (r = 0.24 and 0.27, p<0.01) respectively. No correlation was seen between the grading and colonoscopies in previous year. Overall 27/30 candidates felt the DOPS assessment was fair/very fair, while 27/32 felt the MCQ was fair/very fair. Of the assessors, 12/16 felt the DOPS was valid/very valid, while 17/17 overall felt the process was fair/very fair.
Conclusion: The DOPS accreditation has good face and content validity, and very high reliability across the crucial pass/fail divide. There is ongoing work improving the MCQ.
BOWEL CANCER SCREENING PROGRAMME ONE YEAR IN: EXPERIENCE OF A SINGLE FIRST WAVE CENTRE
M. R. Tighe1, M. G. Phillips1, W. S. L. Stebbings2, B. Brett1, A. Cook1. 1Department of Gastroenterology, 2Department of Surgery, Norfolk and Norwich University Hospital, Norwich, UK
Introduction: The Norfolk & Norwich University Hospital was one of the first centres to launch the national bowel cancer screening programme, commencing in July 2006. The NNUH started covering a population of 550 000 based in mid Norfolk, with an estimated 68 000 falling into the 60–70-year-old age group. In June 2007, the population covered by screening in Norwich was expanded to the whole county of Norfolk with a population of 900 000.
Aims & Methods: A year on, we have reviewed our work to date to see if our results reflect the experience drawn for the large scale FOB trials and the pilot sites.
Results: Uptake for the programme has been high at 67%. In the first year, 53 711 invitation FOB kits were sent out, with 2933 over 70-year-olds requesting additional kits. 35 592 FOB kits have been returned with a positivity rate of 1.65% (584). Among these 584, 71 FOBT +ve were over the age of 70. 99% of patients attended pre-assessment and only 4 were deemed unsuitable for colonoscopy and underwent CT colonography instead. Colonoscopy was complete in 98.9% and 6 cases went on to have a CT colonography to complete the examination. Pathology detected: In year one 84 cancers have been detected (14.8% of colonoscopies)—23 were polyp cancers, an additional 10 cases were staged as Dukes A, 15 cases as Dukes B and 19 cases as Dukes C. 17 patients are awaiting final staging and surgery. All 23 polyp cancers were removed endoscopically. Six went on to have a segmental resection for poor prognostic features with no evidence of residual disease being found. Overall, 56% of cancer detected in screening population were Dukes A, 21% Dukes B and 23% Dukes C. Among over 70-year-old self-referrers, 14.6% with FOBT +ve had cancer, staged as Dukes A 18%, Dukes B 27% and Dukes C 55%, mirroring the symptomatic service. 49% of patients had adenomas at colonoscopy, subdividing into 13% high risk adenomas, 54% intermediate risk and 34% low risk adenomas. 35% of colonoscopies were normal. Complications: One patient has died following surgical removal of a caecal adenoma. Two patients have bled post large polypectomy, one of whom required surgery—the other settled spontaneously.
Conclusion: The first year experience of the screening programme supports the trial and pilot study data. The detection of predominant early stage disease amongst the screened population infers that the trial benefits in terms of mortality from colorectal cancer will be seen in our population. The programme has been very well received by the public. We are targeting publicity to those geographical areas of lower take-up.
COMPARISON OF HIGH RESOLUTION MAGNIFICATION ENDOSCOPY, NARROW BAND IMAGING WITH MAGNIFICATION AND CHROMOENDOSCOPY WITH MAGNIFICATION IN THE DIAGNOSIS OF COLORECTAL NEOPLASIA: A FEASIBILITY STUDY
R. Singh1, A. Shonde1, P. Kaye2, C. J. Hawkey1, K. Ragunath1. 1Wolfson Digestive Diseases Centre, 2Department of Histopathology, Nottingham University Hospitals Trust, Nottingham, UK
Introduction: With the emergence of colorectal cancer screening, the distinction between non-neoplastic from neoplastic colorectal polyps during colonoscopy is paramount. A suitable technique which allows this differentiation could increase the efficiency of treatment by eliminating additional cost associated with unnecessary biopsies. Although chromoendoscopy (CHR) has been propagated as a technique that improves prediction of polyp histology, it has failed to be incorporated into routine practice. Narrow band imaging (NBI) is a novel endoscopic imaging technique which is relatively simple to use and simulates CHR during the procedure.
Aims & Methods: We evaluated the positive predictive value (PPV), negative predictive value (NPV) and accuracy (Acc) of three different techniques: conventional high resolution white light endoscopy (WLE), NBI and CHR, all with magnification in differentiating adenocarcinomas, adenomatous and hyperplastic colorectal polyps. Each lesion was sequentially assessed first by WLE, followed by NBI and finally by CHR. Digital images of each polyp with each modality were taken. Biopsies or polypectomies were then performed followed by blinded histopathological analysis. Each image was then blindly graded based on the Kudo’s pit pattern (KPP). In the assessment with NBI, the meshbrown capillary network pattern (MBCN) of each polyp was also described. The PPV, NPV and Acc of differentiating hyperplastic (Type I & II - KPP, Type I - MBCN) adenomatous (Types III, IV - KPP, Type II - MBCN) and carcinomatous polyps (Type V- KPP, Type III- MCBN) were then compared with reference to the final histopathological diagnosis.
Results: A total of 50 colorectal polyps (5 adenocarcinomas, 38 adenomas, 7 hyperplastic) in 37 patients (25 men, mean age 68.5 years) were assessed. Morphologically, 19 were classified as type Is, 6 type Ip, 24 type IIa and 1 type IIa-c polyps. The PPV, NPV and Acc of the various modalities are depicted in the table.
Conclusion: NBI was superior to WLE and CHR if both the KPP and MBCN criteria were combined and applied in the prediction of non-neoplastic and neoplastic colorectal polyps. This feasibility study demonstrated that this combined classification for NBI could potentially be useful in routine clinical practice, allowing the endoscopist to predict histology with higher accuracies.
CONFOCAL ENDOMICROSCOPIC LASER SCANNING IN VIVO CELLULAR IMAGING OF BARRETT’S OESOPHAGUS: FIRST PROOF OF ENDOSCOPIC CONCEPT IN THE UK
D. P. Hurlstone, N. Tiffin, S. S. Cross. Endoscopy, Royal Hallamshire Hospital, Sheffield, UK
Introduction: Confocal laser scanning endomicroscopy permits cellular resolution imaging in vivo during ongoing video endoscopy. Microvascular architecture and connective tissue stroma can be visualised to a depth of 250 μm. In Barrett’s oesophagus, specialised columnar epithelium presents in a “patchy” distribution. Previous studies assessing magnification +/− chromoscopy have failed to show a definitive clinical advantage compared to quadrantic biopsies alone.
Aims & Methods: To evaluate the efficacy of live cellular endomicroscopic imaging for the in vivo diagnosis of Barrett’s epithelium during ongoing video endoscopy. Consecutive patients with long-term reflux, known Barrett’s oesophagus or patients with known complicating IN were recruited. Endomicroscopy following methylene blue 0.1% chromoscopy was performed using topical acroflavin for surface mucosal nuclear imaging in addition to 5 ml of iv 10% sodium fluorescene for deep z-axis vascular imaging. Endomicroscopy was performed at 10 mm quadrantic segmental intervals and targeted to focal mucosal defects unmasked by chromoscopy—classified according Paris guidelines. Confocal greyscale macro data were collected at 1.6 frames/sec/optical z-axis sectioning 0.7 μm—field view 500 μm×500 μm, minimum 12 macros per segment. The in vivo endomicroscopic diagnosis (according to Mainz criteria) was then compared to targeted biopsies equating to the raster scanned mucosal segment taken as the gold standard.
Results: 48 patients completed the endomicroscopy protocol-median duration of procedure 18 min (range 10–32)/median Barrett’s length 3.4 cm (range 1–12). A total of 9216 endomicroscopy images from 243 target sites were analysed. The in vivo diagnosis of Barrett’s oesophagus using endomicroscopic vascular and cell architecture criteria was predicted with a sensitivity 94.3%/specificity 91.8%/PPV 94.8% and NPV of 96.4%. Basement membrane integrity loss, sub-epithelial vascular tortousity +/− leakage and irregular dark epithelial cell architecture were highly predictive of high-grade dysplasia in vivo (sensitivity 88.1%/specificity 94.1%)/K = 0.88.
Conclusion: Endomicroscopy permits live cellular, sub-cellular and deep vascular imaging of high quality during ongoing video endoscopy. In vivo cellular-vascular architecture has a high correlation with ex vivo histopathology and may prove a novel tool in the rapid diagnosis of Barrett’s oesophagus and associated neoplasia. Multiple optical biopsy sites can be obtained in vivo without white light “field loss” due to biopsy site bleeding. Targeted high quality specimens can improve histopathological processing and patient “flow” in endoscopy.
CATCHING THE BIT IN BETWEEN: ENDOSCOPIC ULTRASOUND-GUIDED MURAL TRUCUT BIOPSIES IN THE DIAGNOSIS OF THICKENED OESOPHAGOGASTRIC WALL
T. Thomas1, P. Kaye2, K. Ragunath1, G. Aithal1. 1Gastroenterology, 2Histopathology, Nottingham University Hospitals NHS Trust, QMC Campus, Nottingham, UK
Introduction: A thickened oesophagogastric wall (OGW) in patients with alarm symptoms raise the possibility of malignancy, but establishing a tissue diagnosis may be difficult as mucosal biopsies are usually negative. Using linear array endoscopic ultrasound (EUS) it is possible to target and biopsy the thickened part of the gut wall.1
Aims & Methods: We aimed to evaluate the efficacy and safety of EUS-guided transmural biopsies in detecting underlying malignancy in patients with thickened oesophagogastric wall and negative mucosal biopsies. Patients were referred for EUS guided sampling as a part of their clinical management. Linear array echoendoscope (GF-UCT240-AL5, Olympus- KeyMed) and 19 G Trucut needle (Wilson Cook, Quickcore) were used for sampling. A previously described technique was used for mural biopsy.1 Clinical and investigatory data were collected prospectively from 2004 to date.
Results: Thirty one patients (19 men) aged 60–74 years (median 68) were included. All patients had thickened oesophageal wall (n = 10), gastric wall (n = 20) or both on CT scan. Prior to EUS, patients had 1–5 (median 1.2) endoscopies and 2–8 mucosal biopsies. The mean oesophageal and gastric wall thickness was 12 and 18 mm respectively. During sampling 1–5 (median 3) needle punctures were made. On EUS trucut biopsy, adequate specimen was obtained for histology in 25/31 (80.6%) although biopsies were fragmented in 16/31 (51.6%) patients. The size of the samples were 4–10 (median 6) mm. Malignancy was confirmed in 17/31 patients (54%) on histology and in 11/31 patients (35.5%) an underlying malignancy was excluded (confirmed at a median follow-up 12 months). There was no significant correlation between wall thickness and biopsy size (Rho, 0.11, 95% CI −0.25 to 0.45, two sided p = 0.53). Transmural biopsies have a sensitivity and specificity of 85% and 94% respectively. The positive and negative predictive value was 94% and 77% respectively. There were no major immediate or late complications
Conclusion: EUS-guided trucut biopsy is a safe and useful technique in the investigation of thickened oesophagogastric wall with a high sensitivity and specificity for the diagnosis of cancer.
DEDICATED BLEED UNITS: SHOULD THEY BE ADVOCATED?
R. Sidhu, P. V. Sakellariou, M. E. McAlindon, D. P. Hurlstone, S. A. Riley, M. T. Donnelly, S. Johal, J. M. Hebden, K. K. Basu, A. J. Lobo, D. S. Sanders. Department of Gastroenterology, Sheffield Teaching Hospitals NHS Trust, Sheffield, UK
Introduction: Upper gastrointestinal haemorrhage (UGH) is a common emergency, however dedicated bleed units with 24-hour endoscopy are still only available in selected hospitals. A previous study from this unit supported a lower case mix adjusted mortality rate in a specialised bleed unit.
Aims & Methods: To evaluate the re-bleeding and mortality rate of patients admitted with UGH to the Sheffield Bleed Unit in comparison to the National Audit and previous performance. Notes of patients admitted between January 2005 and December 2006 were reviewed retrospectively for demographics, Rockall and Child Pugh scores and outcome. Multiple logistic regression was performed.
Results: 66% were emergency admissions, while 23% were tertiary referrals and 11% were current inpatients. 29% of gastroscopies were done out of hours while 82% were within 24 hours. The table tabulates results with a comparison to the previous study and the National Audit. In the 2005–6 cohort, pre and post-endoscopy Rockall scores were predictive of re-bleeding (p = 0.013, p = 0.045) and mortality (p = 0.003, p = 0.01) while only the Child Pugh was predictive of mortality in liver patients (p = 0.002). Compared to the previous cohort, a reduction in the number of bleeding points identified at endoscopy and the number of patients requiring surgery may reflect the vigorous use of intravenous proton pump inhibitors pre-endoscopy and the aggressive endoscopic intervention performed in our unit.
Conclusion: This study has shown that in comparison to the National Audit, the re-bleeding rate and mortality is consistently lower in both cohorts of patients admitted to our bleed unit over time. This further supports the evidence to encourage the development of dedicated bleed units across the UK.
PATIENT POSITION CHANGES DURING COLONOSCOPE WITHDRAWAL INCREASE ADENOMA DETECTION: A RANDOMISED, CROSSOVER TRIAL
J. E. East1, P. Bassett1, M. Stavrinidis1, N. Arebi1, S. Thomas-Gibson1, T. Guenther2, B. P. Saunders1. 1Wolfson Unit for Endoscopy, 2Academic Department of Cellular Pathology, St Mark’s Hospital, London, UK
Introduction: Colonoscopy has a miss rate for adenomas which may partly relate to poor visualisation of the colonic surface. Position changes during colonoscope withdrawal can improve luminal distension.1
Aims & Methods: We aimed to assess whether position changes during colonoscope withdrawal improve adenoma and polyp detection. 130 patients attending for routine colonoscopy underwent back-to-back segmental examination of the colon proximal to the sigmoid-descending junction, randomised to have the first examination in either left lateral position alone or with position changes (cecum to hepatic flexure, left lateral; transverse, supine; splenic flexure and descending colon, right lateral) followed by examination in the other position. After both examinations, polyps were removed for histopathology. Luminal distension was measured in each position on a scale of 1–5: 1, total collapse; 5, fully distended.
Results: At least one adenoma was detected in 34% of patients in colonic areas where position change differed from left lateral (transverse, splenic, descending) compared to 23% examined in left lateral alone, p = 0.01. At least one polyp was detected with position changes in 52% versus 34% respectively, p<0.001. Both adenoma and polyp detection were positively correlated with improved distension score, correlation coefficient 0.12, p<0.001. Adenomas were detected in 16% of colonic areas with an adequate distension score (4 and 5) compared to 7% of those with a borderline or non-diagnostic score (1–3), p<0.001.
Conclusion: Position changes during colonoscope withdrawal, a cost-neutral intervention, significantly improved adenoma detection between hepatic flexure and sigmoid-descending junction. The effect appears to relate in part to improved luminal distension. This intervention could improve efficacy of colonoscopy in cancer prevention without additional resources.
ClinicalTrials.gov Identifier: NCT00234650.
PREDICTING OUTCOMES FOLLOWING GASTROSTOMY INSERTION USING THE SHEFFIELD GASTROSTOMY SCORE. A PROSPECTIVELY DEVISED SCORING SYSTEM WITH A VALIDATION COHORT
J. S. Leeds1, M. E. McAlindon1, S. R. Morley2, R. Marr2, H. E. Robson1, J. Grant1, F. K. T. Lee3, M. T. Donnelly4, D. S. Sanders1. 1Gastroenterology, 2Clinical Chemistry, 3Radiology, Royal Hallamshire Hospital, 4Gastroenterology, Northern General Hospital, Sheffield, UK
Introduction: Several scoring systems are used in the field of Gastroenterology. Although previous studies have demonstrated the substantial risk of death following gastrostomy insertion and some risk factors have been identified, no previous investigators have described a scoring system for gastrostomy insertion. We undertook a prospective, unselected, dual centre study in order to establish the relative importance of risk factors for mortality after gastrostomy insertion. We then formulated a simple numerical scoring system to categorise patients’ risk of death. We then sought to validate our scoring system on an independent second cohort of patients.
Aims & Methods: All patients referred for gastrostomy are prospectively included in a database along with demographic, biochemical and outcome data. We analysed gastrostomy insertions from two teaching hospitals from February 2004 to February 2007. There were 887 referrals resulting in 837 gastrostomy insertions. The largest cohort was at site A and was used to construct a risk stratification scoring system. Site B was used to validate the scoring system.
Results: Site A received 552 referrals and 403 new gastrostomies were inserted (median age 64, 268 males). Overall 30-day mortality rate was 51/403 (12.7%) with the highest risk in those with dementia (40%) followed by stroke (22.2%). Univariate analysis identified that 30 day mortality was associated with age (OR 3.4), albumin (OR 5.6), cardiac comorbidity (OR 2.0) and neurological comorbidity (OR 1.7). On multivariate analysis only age and albumin remained significant (both p<0.001) and were then modelled and attributed scores with age scoring 0 or 1 and albumin scoring 0, 1 or 2 giving composite scores from 0 to 3. Scores of 0, 1, 2 and 3 gave 30-day mortalities (95% CI) of 0% (0 to 2.1), 7% (2.9 to 13.9), 21.3% (13.5 to 30.9) and 37.3% (24.1 to 51.9) respectively. Kaplan-Meier curves stratified by total score showed a significantly increased mortality at 7 (p = 0.0003), 30 (p<0.0001) and 90 (p<0.0001) days. Site B (validation cohort) received 335 referrals and inserted 153 new gastrostomies (median age 77, 64 males) with a 30-day mortality of 24/153 (15.7%). Application of the scoring system in this validation cohort gave comparable 30-day mortality figures of 0%, 7.7%, 15.6% and 29.3% for scores 0, 1, 2 and 3 respectively.
Conclusion: The gastrostomy score can be used to categorise patients being considered for gastrostomy insertion and to calculate risk of death at 30 days. Further external validation is required.
NATURAL ORIFICE TRANSLUMINAL ENDOSCOPIC SURGERY (NOTES) VERSUS LAPAROSCOPY FOR COLON PERFORATION AND REPAIR: FEASIBILITY AND RISK OF ADHESIONS
J. Morris, J. Romagnuolo, K. Morgan, S. Palesch, R. Hawes. Digestive Disease Center, Medical University of South Carolina, Charleston, USA
Introduction: Natural orifice transluminal endoscopic surgery (NOTES) has evolved as a novel endoscopic approach to surgery with the potential to offer scarless procedures and minimise adhesion formation. Postoperative adhesions are an important cause of morbidity in the USA each year. Case reports suggest that NOTES procedures are feasible but little is known of the pathophysiological response to transluminal procedures.
Aims & Methods: To determine if colon perforation repair is feasible with NOTES and to assess adhesion severity with NOTES transgastric colon perforation repair (TGCR) compared with laparoscopic colon repair (LCR) 40 25 kg male pigs were randomly assigned to either TGCR or LCR. TGCR involved a trangastric needleknife puncture with a double channel therapeutic endoscope, peritoneal cavity entry after balloon dilatation, pneumoperitoneum with CO2 and performance of a 2 cm perforation of the spiral colon with a needleknife, and repair of the perforation with clips. The gastric perforation was then closed with a detachable snare and clips using a purse string technique. Pigs were given colon prep preoperatively and antibiotics during the procedure followed by standard chow the next day. Necropsy was performed at 21 days. Adhesion score was a 9 point composite score of (a) density and vascularity of adhesions (1 = filmy, avascular, 2 = dense or vascular, or 3 = dense and vascular) (b) breadth of adhesions (0 = <4 cm, 3 = >4 cm) and (c) extent of adhesions (1 = 1×2 organ pairs, 2 = 2×2 organ pairs, 3 = 3 or more 2 organ pairs). Final score was a mean of the necropsy surgeon and 2 independent reviewers of necropsy video. Mann-Whitney and Fisher’s exact test were used.
Results: Preliminary composite adhesion scores were analysed for 13 TGCR and 14 LCR pigs. Mean scores were 4.8 (TGCR) and 4.5 (LCR) p = 0.7. Subscores were similar. No pigs had significant procedure-related adverse events. Weight gain and postoperative behaviour were normal in both groups. All colon perforation sites were well healed.
Conclusion: NOTES colonic perforation repair is feasible. Preliminary data show similar adhesion score with TGCR compared with LCR.
Service development free papers
PROVIDING A REGIONAL SMALL BOWEL ENDOSCOPIC SERVICE: THE SHEFFIELD EXPERIENCE
R. Sidhu1, M. E. McAlindon1, D. P. Hurlstone1, M. Thomson2, I. C. Cameron3, D. S. Sanders1. 1Department of Gastroenterology, Royal Hallamshire Hospital, Sheffield Teaching Hospitals NHS Trust, 2Department of Gastroenterology, Sheffield Children’s Hospital, 3Department of Surgery, Royal Hallamshire Hospital, Sheffield Teaching Hospitals NHS Trust, Sheffield, UK
Introduction: The small bowel is an important area for diagnosis, but endoscopic access has historically been limited. Our centre provides push enteroscopy (PE), capsule endoscopy (CE) and double balloon enteroscopy (DBE). However the clinical utility and impact of these modalities on service provision (in the UK) is unknown.
Aims & Methods: To evaluate the diagnostic rates of PE, CE and DBE as well as the impact on patient management, in a tertiary setting in the UK. Data were collected on patients that underwent PE (since January 2002), CE (since June 2002) and DBE (since July 2006). Case notes were reviewed for age, sex, indication of referral, comorbidity, previous investigations and diagnosis obtained including follow-up data. The initial choice of investigation performed depended on the referral indication and the suspected anatomical location of the pathology. The demand for each modality was also assessed since the inception of the service.
Results: Eight hundred CEs, 182 PEs and 30 DBEs have been performed over 70 months. Forty per cent of the referrals originated from outside the region. The commonest indication for all three procedures was obscure gastrointestinal bleeding (OGB). Patients underwent a mean of 4.3 tests prior to CE or DBE. The overall diagnostic yield was 39% for CE, 33% for PE and 43% for DBE respectively. The diagnostic yield was highest for the indication of overt bleeding for both PE (p<0.01) and CE (p<0.001) when compared to other referral indications. Management was altered in 26% of patients that underwent CE, 22% for PE and 43% for DBE respectively. Importantly there were no cases where PE or DBE recognised a lesion that had not already been detected at CE. When comparing CE and DBE, complete small bowel examination was more likely with CE; p<0.001, however, there was no significant difference in the diagnostic yields of the two groups (p = 0.41). DBE allowed intervention in 38% of patients who had a lesion identified by CE. Referrals for either a therapeutic DBE or PE have occurred in 11% of all CE undertaken. There has been a year by year increase in demand for CE. The increasing demand for CE has resulted in a relative decline in the number of diagnostic PEs performed while the demand for DBE is rising particularly for lesions considered beyond the reach of PE.
Conclusion: As part of the regional service, CE should be used as a first-line investigation for the small bowel. PE and DBE should be used as an adjuvant to CE for therapeutic intervention, depending on the location of pathology seen at CE. This ensures efficient use of the small bowel service.
TRANSFUSION IN ACUTE UPPER GASTROINTESTINAL BLEEDING: PRELIMINARY RESULTS FROM THE UK COMPARATIVE AUDIT
S. A. Hearnshaw1, D. Lowe2, R. F. Logan3, S. P. L. Travis1, K. R. Palmer4, M. F. Murphy5. 1Gastroenterology, John Radcliffe Hospital, Oxford, 2CEEU, Royal College of Physicians, London, 3Epidemiology and Public Health, University of Nottingham, Nottingham, 4Gastroenterology, Western General Hospital, Edinburgh, 5NHS Blood and Transplant, John Radcliffe Hospital, Oxford, UK
Introduction: More than 60% of red blood cells (RBC) are now transfused to medical patients. Patients with acute upper gastrointestinal bleeding (AUGIB) are one of the main groups of medical patients using blood (∼14% of all RBC transfusions).1 However, there are no large randomised controlled trials showing transfusion in AUGIB improves outcome. Every transfusion carries risk, and inappropriate transfusion is also a waste of a scarce and costly resource. The BSG guidelines recommend transfusion in patients with a haemoglobin (Hb) <10 g/dl with acute bleeding, or ongoing haematemesis with shock.2 UK transfusion guidelines exist for the use of RBC, platelets and FFP in bleeding patients.3–5 This comparative audit of AUBIG provides the opportunity to review current practice in these patients where transfusion is common. The audit data will be provided to each participating hospital with recommendations for avoidance of inappropriate transfusion.
Aims & Methods: To audit current transfusion practice in AUGIB against published guidelines, and to investigate the relationships between transfusion and patient outcomes including re-bleeding and death. All UK acute NHS hospitals were invited to participate. Enrolled hospitals identified all new admissions and inpatients presenting with suspected AUGIB between 1/5/07 and 30/6/07. Endoscopy, laboratory and transfusion data were entered online.
Results: Data were received from 6750 patients from 208 UK hospitals treating patients with AUGIB. 43% received RBC transfusion for AUGIB. 10% of all initial transfusions were to haemodynamically stable patients with Hb>10 g/dl, and 5% were given to stable patients with no recorded Hb. FFP was transfused to 503 (7%) patients, 29% of whom had normal coagulation studies. 189 patients received a platelet transfusion, 39% being given to patients with a platelet count >50 ×10*9/l. 23% of patients who received RBC transfusion had ongoing or further bleeding following transfusion. For all Rockall scores, the rate of re-bleeding was lower in patients who did not receive RBC transfusion.
Conclusion: RBC transfusion remains common in patients with AUGIB, with the majority of RBC transfusions being given according to published guidelines. 15% did not appear to be justified. Inappropriate transfusion of platelets and FFP was higher.
30-DAY MORTALITY AUDIT USING A LATE QUALITY AND SAFETY OUTCOME IT SYSTEM
S. Hebbar, E. Nowell, K. Dowler, R. Valori, P. Dunckley. Gastroenterology, Gloucester Royal Hospital, Gloucester, UK
Introduction: Following an endoscopic procedure, the capture of immediate outcomes is relatively easy compared to that of late outcomes. Locally, we have set up an automated late quality and safety outcome IT system to identify patients who have died within 30 days of an endoscopic procedure, thus facilitating the systematic audit of these procedures and their appropriateness.
Aims & Methods: The aim of the audit was to identify the number of cases assigned to the clinical governance review, the number of days from the endoscopic procedure to death and the percentage of deaths in community. The average time to review each case note was also identified. The late quality and safety outcome IT system obtains 30-day mortality data by linking the PAS and Patient Administration System’s (PAS) theatre module, SwiftOp. An endoscopist was assigned to review the notes who, on signing into the system, can open a data entry screen for each case which displays full details of the endoscopic procedures, into which the outcomes and comments from the notes review are entered. Date of procedure and death and any adverse events are also displayed in the system. Cases where it was determined that the procedure was inappropriate or contributed to death, or where the reviewer was unsure about either of these, were assigned to a clinical governance review.
Results: Between January 2006 and October 2007, 17 744 endoscopic procedures were performed and 341 patients died within 30 days. 138 notes have been reviewed to date. The average time to review each notes was 3 min. The average number of days to death from the time of endoscopic procedure was 14.53. 25 patients (18.1%) died in the community. Nine (0.05% of total endoscopic procedures) cases are assigned to clinical governance review, of which 7 cases possibly and 2 (0.01% of total endoscopic procedures) cases definitely contributed to death. The deaths in all the 9 cases have been within 8 days of procedure and all died within the hospital.
Conclusion: The late quality and safety outcome IT system is user-friendly and quick. The audit has identified 2 cases whereby the endoscopy directly led to patient death. These cases will be reviewed as part of the endoscopic clinical governance framework in order to further enhance the quality and safety of our endoscopic practice. The 9 cases where the endoscopic procedure possibly or definitely contributed towards death all died within 8 days of the procedure and within the hospital. Although this is only a small number of cases, these initial data suggest that reducing the late outcome mortality audit data from 30 to 10 days, in patients who have died in hospital only, may still capture the majority of late deaths and reduce the workload associated with collecting this data.
CAN WE ACHIEVE THE 18 WEEK PATHWAY TARGET? EFFECT OF DIFFERING PATIENT PRESENTATIONS
P. Sakellariou, D. A. Elphick, G. Toy, D. S. Sanders, D. P. Hurlstone, M. E. McAlindon, A. J. Lobo. Gastroenterology Unit, Royal Hallamshire Hospital, Sheffield, UK
Introduction: Investigation of out-patients with a wide range of presenting features is a major part of a gastroenterologist’s workload. Few data exist on the extent to which different units investigate similar presentations. This is of critical importance in provision of an 18 week (126 day; from referral to initiation of treatment) patient pathway—a key objective for the NHS.
Aims & Methods: This study aimed to quantify the investigative load of newly referred patients to the Gastroenterology clinic of a single University Teaching Hospital and to evaluate performance against the local Trust’s 18 week “clock rules”. 306 new out-patients were reviewed by 4 consultant teams over a 62-day period (16/08/06–16/10/06). All case notes were reviewed. Referral category, main and additional symptoms, time to first appointment and outcome at 18 weeks were recorded. Time and reason for stopping the clock were identified.
Results: Median age (range) was 56 (18–94) years and 61% were female. Referrals were from GPs (240, 78%) or another consultant (66, 22%). 77 (25%) referrals were through the “suspected cancer” system. Median time to first appointment was 56 (1–192) days. The commonest main symptoms were diarrhoea (74, 24%), dyspepsia (43, 14%), iron deficiency anaemia (IDA) (53, 17%). At 18 weeks the clock had been stopped in 164 (54%) patients while 60 (19%) were undergoing further investigation, 53 (16.7%) awaiting treatment to be agreed, 22 (8%) awaiting first appointment, 6 (2%) referred to another specialty and 1 (0.3%) had a new clock started. The clock had been stopped for 268 (87%) patients with a median time 111 (7–499) days (68 (25%) offered treatment; 112 (43%) decision not to treat; 20 (7%) declined treatment or investigation; 68 (25%) commenced active monitoring). With administrative changes, the pathway could have been accelerated to stop the clock at median 77 (7–499) days compared to actual time (p<0.01, Wilcoxon test). Median time to stopping the clock was 41 (11–249) days for the “suspected cancer” pathway, and 130 (7–499) days for the remainder. Those with diarrhoea had median 2 (1–6) further investigations (dyspepsia 2 (0–5); IDA 3 (0–5)). Median time to stopping the clock for patients with diarrhoea was 120 (13–491) days (dyspepsia 78(7–499); IDA 103 (12–494)) and proportion of patients with completed investigation by 18 weeks was 42% (diarrhoea), 70% (dyspepsia) and 47% (IDA).
Conclusion: The investigative practice of one hospital unit is described allowing comparison with others and benchmarks to be set. To achieve the March 2008 milestone with 90% of patients having received initial treatment by 18 weeks from referral, our audit highlights the requirement for a transformation of services and for the complexity of investigative pathways to be considered in delivering that objective.
USING THE 13C-UBT TO PROMOTE NICE GUIDELINES FOR SIMPLE DYSPEPSIA: AN 8-YEAR FOLLOW-UP COHORT STUDY
A. J. Norman, S. Din, N. J. Taylor, S. Swain, R. P. H. Logan. Department of Gastroenterology, King’s Mill Hospital, Mansfield, UK
Introduction: The 2004 NICE guidelines advise that in patients with dyspepsia, gastroscopy (OGD) should be reserved for patients with alarm symptoms. However there is continued demand for OGD, often as a means of providing reassurance. This study evaluates the long-term effectiveness and safety of an alternative management pathway in minimising the use of OGD in patients with uncomplicated dyspepsia.
Aims & Methods: Observational cohort study of patients 65 years old and under with uncomplicated dyspepsia routinely referred to a district general hospital between 11/08/98 and 1/11/03 with follow-up to 1/11/07. Hospital activity and pathology database analysis for death, cancer diagnosis, OGD (out-patient and in-patient) and case note review. Ascertainment bias (for OGDs performed elsewhere) was evaluated by review of GP records in a subset of referred patients (n = 30). The two-step pathway was a 13C-UBT and a subsequent 20 min out-patient consultation in all patients with a negative result.
Results: Between 11/08/1998 and 28/10/2003, 242 patients (median age 41 years, range 14–65 years, 130 male, 112 female) with uncomplicated dyspepsia were referred, had a negative 13C-UBT and were reviewed as an out-patient. The clinical diagnoses were GORD (74%) and non-ulcer dyspepsia (14%). During the period of follow-up (median 78 months, range 45 to 111 months), 39 patients had an OGD either within one year (n = 15; indication for OGD: severe/atypical symptoms (n = 7), pre-fundoplication (n = 4)) or subsequently (n = 24, 24/227 (11%), median follow-up 33 months, range 14–92 months). In the latter group, a normal OGD was the most common endoscopic diagnosis (n = 20) followed by oesophagitis (n = 6). During a total follow-up of 1593 patient years, there were 3 deaths (lung cancer and LVF. One patient’s cause of death could not be found). From a subset of GP records (n = 30), only one patient had an OGD performed elsewhere.
Conclusion: These data show that uncomplicated dyspepsia can be safely managed without performing OGD in up to 90% of cases referred to secondary care. The alternative pathway exploits the reassurance value of a negative 13C-UBT reinforced by out-patient clinic review. This strategy may allow endoscopy resources to be used more appropriately.
A TEMPLATE PROFORMA AND OPERATIVE INFORMATION IMPROVES THE QUALITY OF HISTOPATHOLOGY REPORTING IN COLORECTAL CANCER
P. N. Siriwardana1, A. Pathmeswaran2, J. S. D. E. Hewavisenthi3, K. I. Deen1. 1University Surgical Unit, North Colombo Teaching Hospital, 2Department of Community Medicine, 3Department of pathology, Faculty of Medicine, Ragama, Sri Lanka
Introduction: The histopathology report is vital to determine the need for adjuvant therapy and prognosis in colorectal cancer (CRC).1 We and others have highlighted the inadequacy of histopathology reports in paragraph prose.2 3 To improve the completeness and quality of histopathology reports, the Royal College of Pathologists (RCP), UK has formulated a proforma to include a minimum dataset required for accurate assessment of a colorectal cancer specimen.4
Aims & Methods: The aim of this prospective study is to assess the robustness of the histopathology report following introduction of a template proforma based on RCP, UK guidelines, which had 19 items for rectal cancer (RC) and 15 items for colon cancer (CC). A total of 150 reports were evaluated; 68 consecutive histopathology reports in proforma format were prospectively analysed and compared with 82 consecutive histopathology reports in text format. The percentage of reports containing a statement for each data item in the dataset in template proforma format was obtained and compared with the series in paragraph format. Completeness (%) of each report classified <80% or >80%.
Results: Eleven data items common to CC and RC had a comment in all proformas compared to only 2 in text format reports. The completeness of reports in text and template format is shown in table 1. Except for comments on presence of “histologically confirmed liver metastases” in CC and RC, “distance from dentate line” (information provided by surgeon) and “distance to circumferential margin” in RC, all other items were reported in more than 90%, where 71% of the items based on the minimum dataset were present in all. Mean percentage completeness of all reports in template format for RC was 91% (SD±4%) and 99% (SD±1%) for CC, whilst a text report had completion rates of 74% (SD±8%) and 81% (SD±5%) respectively.
Conclusion: A checklist of report items improves the quality of the histopathology report in CRC which can be further enhanced by the surgeon’s contribution of operative findings.
PRELIMINARY RESULTS OF THE UK COMPARATIVE AUDIT OF ACUTE UPPER GASTROINTESTINAL BLEEDING: ORGANISATION OF CARE
S. A. Hearnshaw1, D. Lowe2, R. F. Logan3, M. F. Murphy4, S. P. L. Travis1, K. R. Palmer5. 1Gastroenterology, John Radcliffe Hospital, Oxford, 2CEEU, Royal College of Physicians, London, 3Epidemiology and Public Health, University of Nottingham, Nottingham, 4NHS Blood and Transplant, John Radcliffe Hospital, Oxford, 5Gastroenterology, Western General Hospital, Edinburgh, UK
Introduction: Prompt assessment, investigation, resuscitation (including appropriate transfusion), and endoscopic therapy are required to manage optimally patients with acute upper gastrointestinal bleeding (AUGIB). BSG guidelines state that patients with major bleeding should undergo urgent endoscopy, and that therapeutic endoscopy should be provided by skilled endoscopists 24/7.1 2 A dedicated space on routine endoscopy lists should be provided daily for patients presenting with AUGIB.3
Aims & Methods: To survey the current organisation of care for patients admitted with AUGIB against published guidelines. To examine the availability of emergency endoscopy, endoscopic therapies, and skilled medical and nursing staff in hospitals admitting patients with AUGIB. Organisational questionnaires were sent to the clinical lead for endoscopy in the 217 hospitals that participated in the audit.
Results: 190 hospitals provided organisational data. 91% provide level 2 care beds on site, with 15 hospitals having a dedicated AUGIB unit. 99% provide endoscopy on site, and 89% have out of hours endoscopy. 99% have facilities for endoscopic therapy in patients with AUGIB, with 57% ensuring a dedicated slot for emergency endoscopy. Only 55% of hospitals have a consultant on call rota for out of hours emergency endoscopy; 75% of these have 3–8 consultants on the rota. 41% of hospitals have an endoscopy nurse assistance on-call rota. In 14% of sites, out of hours emergency endoscopy is provided by unsupervised junior doctors. 5% of hospitals treating patients with AUGIB do not have a transfusion laboratory on site. 82% of hospitals have written guidelines for the management of AUGIB in the hospital, and 85% audit their practice.
Conclusion: There is wide variation in service provision for patients with AUGIB in the UK, with many hospitals not having a named consultant on call for endoscopy out of hours. The use of out of hours emergency endoscopy and its appropriateness needs to be reviewed both at national and local levels, and will be evaluated in this audit. The impact of the current service provision on patient outcomes needs to be assessed, before recommendations of “best practice” can be made.
“STRAIGHT TO TEST” UPPER GASTROINTESTINAL CANCER SERVICE: EFFICIENCY, SAFETY AND COST EFFECTIVENESS
R. Madhotra1, P. Steer2, A. Ignjatovic2, C. Akubuine2. 1Gastroenterology, Milton Keynes Hospital Foundation Trust, Milton Keynes, 2Gastroenterology, Milton Keynes General Hospital, Milton Keynes, UK
Introduction: Rapid access to diagnosticvs is essential for early diagnosis of upper gastrointestinal (GI) cancer. In the UK, Cancer Plan 2000 requires all suspected cancer patients to be seen in two weeks and diagnostics must be completed within 31 days. These targets put huge service delivery challenges for most NHS hospitals with limited resources. We, therefore, started a “Straight to Test” STT service to reduce access times, and rapid diagnosis and staging suspected cancer patients. There were no extra cost for setting up the service. The patients were followed up for 6 months after endoscopy by telephonic interview and/or review of medical records.
Aims & Methods: We conducted a prospective audit of the new STT service over the first 12 months to study the efficiency, safety and cost effectiveness. All consecutive patients referred by the GPs for urgent cancer assessment were studied. Data were collected to include the demographics, presenting symptoms, endoscopy findings, follow-up plan and 6-month outcome. Cost savings were calculated using Outpatient Mandatory Tariff Coding system.
Results: A total of 241 patients (116 males, 125 females) were studied. Ninety five per cent patients had endoscopy within two weeks of referral. Majority had multiple symptoms. the commonest presenting symptoms were dyspepsia (68%), dysphagia (48%) and weight loss (40%). The endoscopy diagnoses were gastritis (32%), hiatus hernia (26.9%), oesophagitis (16.8%), duodenitis (12%) and gastric ulcers (2.4%). Cancers were detected in 27 (11.2%) patients. Cancers included 11 oesophageal, 4 gastric, 3 pancreas, 2 liver and 3 colon. One hundred and seven (44.3%) patients were discharged back to the GP after endoscopy, 134 (55.7%) were followed up in hospital. Excluding cancer patients there were no significant difference in presenting symptoms, endoscopy findings and clinical outcomes at 6 months in the two groups. No missed cancers were detected at 6-month follow-up. STT service saved 107 new patient appointments (£188 each) and reduced 134 follow-up appointments (£88 each) for the remaining. The net saving was £32,576.
Conclusion: Our audit shows that STT service for upper GI cancer assessment is efficient, safe and highly cost effective. The audit also shows that more patients could be safely discharged to their GPs, hence there is scope more cost saving. This model of cancer assessment service in the NHS has potential for widespread use in upper GI as well as other cancers.
LIVER HISTOPATHOLOGY IN THE YORKSHIRE REGION: A NETWORK MODEL
J. I. Wyatt1, G. Reall1, R. Jones2. 1Histopathology Department, 2Hepatology, St James’s University Hospital, Leeds, UK
Introduction: The national plan for liver services UK 2004 envisages that “each hepatology centre should have access to a specialised liver pathologist. Ideally this would be in the site of the lead centre providing expertise and training for the local pathology departments within the managed clinical network.”1 This arrangement has evolved informally in West and North Yorkshire.
Aims & Methods: The aim of this study was to investigate the volume and provision of liver histopathology in our region originating outside Leeds, as a potential model for a hepatopathology network. A questionnaire was sent to all pathologists in west and north Yorkshire, covering 11 hospital trusts, referring into the main centre at Leeds. It covered departmental statistical data on liver biopsy workload, and attitudes of individual pathologists to reporting liver biopsies. Individual attitudinal responses to statements were on a scale of 1 (strongly disagree), 3 (neutral), to 5 (strongly agree).
Results: Replies were received from all 11 hospitals: 23/31 (74%) pathologists in non-specialised DGH departments and 3/4 liver pathologists in larger specialised departments (Bradford, Hull). The DGH departments receive on average 70 biopsies/year (range 30–150; 67% medical, 33% for tumour) representing 0.55% (0.33–1.1%) histology requests. Reporting is shared by all 2–6 pathologists/department. On average estimated 35% (5–100%) cases are discussed with the clinician during a CPC (5/9) and/or by phone (5/9). About 10% biopsies are reviewed in Leeds. The two larger departments receive 120 and 170 biopsies/year reported by 2 named subspecialist pathologists out of the 10–11 consultants/department. <5% biopsies are reviewed in Leeds. Of 23 DGH pathologists expressing a view (>16 not neutral for each question), >90% enjoyed liver work, often read up about biopsies, and discussed them with their colleagues. 94% said they would like to do liver CPD, 62% had done liver CPD in the last 3 years. 7/23 would like to refer more biopsies centrally. Only one said they would prefer not to do any liver work.
Conclusion: In Yorkshire, liver biopsies account for 0.5% DGH histopathology specimens. Most pathologists enjoy the challenge of this work, and would like more opportunity for CPD. A minority would like a more centralised service. This indicates support for a more formalised network, providing support, training and guidelines to pathologists to work with their local clinical hepatologist.
A DECADE AFTER ROCKALL: A 12-MONTH SINGLE-CENTRE STUDY OF CLINICAL OUTCOME IN NON-VARICEAL UPPER GASTROINTESTINAL BLEED
R. Arulraj1, I. Khan1, S. Pathmakanthan1, K. Kane1, R. Boulton1, M. Hallissey2, J. Goh1. 1GI Unit, 2Surgery, University hospital Birmingham NHS Trust, Birmingham, UK
Introduction: A decade following the publication of the Rockall risk score have seen significant medical and endoscopic advances in treatment of non-variceal upper gastrointestinal (GI) bleed (NVGIB) and also a change in the epidemiological pattern of NVGIB. Many gastroenterologists feel there has been a progressive fall in the incidence of bleeding and endoscopic therapy is useful in control of bleeding.
Aims & Methods: We report a 12-month (2006) study of clinical outcome of patients presenting to the emergency department in a single centre with a 24/7 consultant-led GI bleed service. All patients admitted with acute NVGIB were included (GI bleed in our tertiary services including transplant units were excluded). Case/electronic record of all patients were reviewed and discussed at weekly bleed audit meeting.
Results: 202 patients were identified as true NVGIB (mean age 67±18; M:F = 125:77). Medication: Aspirin (n = 54), Clopidogrel (2), NSAID (22) and Warfarin (15). Endoscopy was performed within 24 h in 90 (45%; mean Rockall: pre 2.9 post 4.6); 24–48 h in 46 (23%; mean Rockall pre 2.3 post 3.7) and >48 h in 59 (29%; mean Rockall pre 2.3 post 3.5). 23 (11%) were performed out-of-hours (Rockall pre 3.2; post 5.8). The top 4 diagnoses were duodenal ulcer (56; 28%), gastric ulcer (32; 16%), oesophagitis (32; 16%) and gastritis (32; 16%). In total, 15 (7%) underwent emergency surgery. The overall mortality was 9% (18/202). Endoscopic interventions were carried out in 35 (18%; Rockall pre 3.4 post 6.1). Mortality in the intervention and non-intervention groups were 5.7% (2/35) versus 8.9% (15/169) respectively (p = NS; χ2 test).
Conclusion: NVGIB remains a significant workload for gastroenterologists both in and out of hours and is still associated with significant morbidity and mortality. The Rockall score continues to be useful in risk stratification despite the shift in epidemiological pattern from Helicobacter to increasing anti-platelet therapy usage.
BSG pancreatic/radiology section joint symposium
A COMPARISON OF CAPSULE ENDOSCOPY WITH SMALL BOWEL MRI IN THE MANAGEMENT OF PEUTZ-JEGHER’S SYNDROME
A. J. Postgate1, A. Fitzpatrick1, D. Burling2, A. Gupta2, C. Fraser1. 1Wolfson Unit for Endoscopy, 2Intestinal Imaging Department, St Mark’s Hospital, London, UK
Introduction: Capsule endoscopy (CE) is more accurate and better tolerated than barium follow through x ray for small bowel polyp surveillance in patients with Peutz-Jegher’s Syndrome (PJS).1 2 However polyp size estimation and localisation is difficult at CE. Small bowel MRI is an evolving modality which may have a role for this indication.
Aims & Methods: We compared the accuracy of CE with MRI follow through for the detection of significant (>10 mm) small bowel polyps in adults with PJS. Study patients underwent an MRI and a subsequent CE. Each test was reported by different reviewers, blinded to the results of the other modality. A visual-analogue scale documenting patient comfort was completed. The results were confirmed at double balloon enteroscopy (DBE) or operative enteroscopy (IOE) when clinically appropriate.
Results: An interim analysis of 9 patients was performed. 705 polyps of all sizes were identified by both modalities: 681 by CE and 24 by MRI (table). CE identified significantly more diminutive polyps (6 mm or less) than MRI (643 vs 2, p = 0.008), and more 6–10 mm polyps (24 vs 8, p = 0.07). Six patients had significant (>10 mm) polyps: 5 were identified at MRI and CE, and 1 at MRI only. Each modality identified 14 significant polyps. To date confirmation of the results by DBE has been performed in 1 patient (no 1, table 1), at which 3 significant polyps were noted: two 12 mm polyps in the jejunum, and one 22 mm polyp in the proximal ileum. CE identified a 15 mm and 20 mm polyp in the jejunum and two 12 mm polyps in the ileum, while MRI found a 16 mm polyp in the jejunum and a 13 mm polyp in the ileum. Patients found CE more comfortable than MRI (78% vs 52%) but of equal convenience (77% vs 77%). Patient preference was split between the two tests.
Conclusion: CE is superior for identifying small (10 mm or less) polyps but MRI is comparable in performance for clinically significant (>10 mm) polyps. Further data from DBE or IOE are required to examine which modality most accurately localises and sizes significant polyps. Although patients rate CE as more comfortable than MRI, neither test was preferable overall. In conclusion, MRI follow through is a promising alternative to CE for small bowel polyp surveillance, and it is likely that the two modalities will complement each other in the management of difficult cases prior to organising invasive polypectomy.
Neurogastroenterology/motility free papers
SYMPATHETIC AND PARASYMPATHETIC SYSTEM CO-ACTIVATION UNDERLIES HEART RATE INCREASE IN BOTH HUMAN VISCERAL AND SOMATIC PAIN
P. Paine1, J. Kishor2, L. Gregory1, Q. Aziz2. 1Department of Gastroenterology and Translational Imaging Unit, Manchester University, Manchester, 2Wingate Institute of Neurogastroenterology, Queen Mary University of London, London, UK
Introduction: Somatic pain animal models have recently identified novel, seemingly paradoxical, sympathetic (SNS) and parasympathetic (PNS) co-activation in pain evoked heart rate (HR) increase. It is not known whether this can be seen in humans or for visceral pain.
Aims & Methods: To compare brainstem selective autonomic nuclei outputs for visceral and somatic pain. Methods: 18 healthy volunteers (2 males), mean age 35.4 (range 18–59 years) underwent serial nail bed (NB) pressure stimuli; 16 of whom also had serial oesophageal balloon (O) distension. Both stimuli were delivered to pain tolerance threshold. In addition to HR, selective cardiac PNS (cardiac vagal tone (CVT)) and SNS responses including cardiomotor (Cardiac Sympathetic Index (CSI)); sudomotor (skin conductance (SCR)) and vasomotor (mean blood pressure (MBP)) were acquired pre- and post-stimulation using a novel beat to beat technique.
Results: There were comparable ratings between sites of pain intensity (O = 7.9 + 0.2, NB = 8.1 + 0.2; p>0.05) and unpleasantness (O = 7.9 + 0.2; NB = 7.8 + 0.3; p>0.05). HR increased during both somatic (71.02 + 2.1 bpm pre-stimulus; 73.9 + 2.05 post-stimulus, p<0.05) and visceral pain (72.3 + 2.05 bpm pre-stimulus, 76.9 + 2 bpm post-stimulus, p<0.05). This was accompanied by CVT increases for both somatic (pre-stimulus 8.11 + 1.06, post-stim 8.50 + 1.12, p<0.05) and visceral pain (pre-stimulus 8.15 + 1.4, post-stimulus 8.84 + 1.32, p<0.05). CSI also increased for visceral (pre-stimulus 2.38 + 0.19; post-stimulus 3.33 + 0.31, p<0.05); p<0.01) and somatic (pre-stimulus 2.36 + 0.15, post-stimulus 2.91 + 0.26) pain. SCR increased for somatic (pre-stim 6.86 + 0.97 uS, post-stim 8.35 + 1.05, p<0.05) and visceral (pre-stimulus 6.25 uS + 0.96, post-stimulus 7.32 uS+1.08, p<0.05) pain. MBP fell however: somatic (pre-stim 99.1 + 2.5 mmHg, post-stim 95.5 + 2.24, p<0.05) visceral (pres-stim 95.8 + 3.5 mmHg post-stim 91.2 + 4.3, p<0.05). The pain related change was greater for SCR for NB than O (p<0.05) but there were no differences otherwise in magnitude of pain-related changes between sites.
Conclusion: For the first time, co-activation of SNS and PNS has been shown to accompany pain evoked HR increases in humans for somatic and visceral pain. This confirms recent similar findings in animal studies. The ANS is not a simple reciprocal system but its subcomponents are capable of nuanced patterned responses in pain. Visceral and somatic pain responses were qualitatively similar.
ANXIETY INDUCTION IS ASSOCIATED WITH GREATER SENSITISATION TO OESOPHAGEAL ACID IN A HUMAN MODEL OF VISCERAL PAIN HYPERSENSITIVITY
A. Sharma1, L. Van Oudenhove2, P. Paine1, Q. Aziz3. 1GI Sciences, Hope Hospital, Salford, UK, 2Department of Psychiatry, University Hospital Gasthuisberg, Catholic University of Leuven, Leuven, Belgium, 3Wingate Institute of Neurogastroenterology, Barts and the Royal London, Queen Mary University, London, UK
Introduction: Patients with stress or anxiety at the time of gastrointestinal injury/inflammation (for example, gastroenteritis) have a higher risk of developing subsequent functional gastrointestinal disorders (FGID). Patients with these disorders often display a heightened sensitivity to experimental gut stimulation, termed visceral pain hypersensitivity (VPH). We have previously shown that distal oesophageal acidification induces sensitisation of spinal dorsal horn neurones leading to the development of VPH in the non-acid exposed proximal oesophagus (PO).1 How anxiety modulates this VPH is unknown.
Aims & Methods: To determine whether anxiety induction affects the magnitude of acid-induced oesophageal pain hypersensitivity. 16 healthy volunteers (10 female, age 22–57 years, mean 35.7 years), were studied on two occasions. Pain thresholds (PT) to electrical stimulation (in milliamperes, mA) were determined in the PO and foot (somatic control) pre- and post a 30-min infusion of 0.15M HCl. During the infusion, all subjects randomly received a 10 min cognitive mood induction paradigm combining autobiographical recall of an anxiety-inducing life event with presentation of fearful faces or a neutral life event with neutral faces in a cross-over design. A Spielberger state anxiety inventory (SSAI) was recorded before and after the acid infusion. Subjects also completed unpleasantness ratings on a 10 cm Likert scale before, during and after the infusion.
Results: The mean change in SSAI score with infusion was significantly greater for anxiety versus neutral conditions (21.7 (12.6 SD) vs 3.6 (6.4 SD), p<0.0001 Wilcoxon). Anxiety induction increased unpleasantness scores compared to neutral (2.5 (2.0 SD) vs 0.63 (1.2 SD), p = 0.008 Wilcoxon). There was a greater reduction in PT in the PO during anxiety compared to neutral condition (−4.5 mA (6.4 SD) vs −2.1 mA (6.2 SD), p = 0.05 Wilcoxon). The mean maximum change in PT was also greater with anxiety than neutral mood induction (−7.6 mA (6.7SD) vs −3.8 mA (5.8SD), p = 0.02 Wilcoxon). There was no difference in the mean change in foot PT between the conditions (p = 0.14, Wilcoxon).
Conclusion: Combining anxiogenic autobiographical recall with fearful faces increases subjective anxiety, and unpleasantness scores during oesophageal acidification and the magnitude of subsequent visceral sensitisation. These findings provide objective evidence for the role of anxiety in the development of prolonged VPH, and provides a model for studying the biological reasons for the effect observed and will also allow testing of therapeutic strategies.
FAECAL LACTOFERRIN: A NOVEL TEST TO DIFFERENTIATE BETWEEN IRRITABLE OR INFLAMED BOWEL?
R. Sidhu1, L. Foye2, S. Morley2, P. Wilson2, A. C. Wright1, A. J. Lobo1, M. E. McAlindon1, D. S. Sanders1. 1Department of Gastroenterology, 2Department of Clinical Chemistry, Royal Hallamshire Hospital, Sheffield Teaching Hospitals NHS Trust, Sheffield, UK
Introduction: Irritable bowel syndrome (IBS) and inflammatory bowel disease (IBD) may not always be discriminated by using symptoms alone. Thus invasive tests may be performed. Lactoferrin is a glycoprotein expressed by activated neutrophils. Previous studies have demonstrated the presence of faecal lactoferrin (FEL) in patients with IBD, coeliac disease and infective diarrhoea. It has been proposed as a non invasive test to screen patients with gastrointestinal symptoms for the presence of inflammation. However there is paucity of data on the use of FEL in IBS.
Aims & Methods: To investigate the clinical utility of faecal lactoferrin (FEL) as a marker of GI inflammation when assessing patients with Rome II IBS, IBD and healthy controls. Patients with Rome II IBS and IBD were invited to participate in this study. Disease activity in IBD patients were assessed using the modified Harvey-Bradshaw Activity Index (HBI). Healthy volunteers acted as controls. Stool samples were analysed using an ELISA assay (Techlab). A two-tailed t test was used to compare means between groups and Kendall-Tau correlation calculations were performed between lactoferrin concentrations and disease activity.
Results: Eighty seven patients with IBS, 55 patients with IBD: 33 ulcerative colitis (UC) and 22 Crohn’s disease (CD) and 98 healthy volunteers were recruited. The mean +/− SE FEL concentration (μg/g faecal weight) was 1.63 +/− 0.44 for IBS patients, 39.3 +/− 16.6 for UC patients, 35.4 +/− 10.7 for CD patients and 2.43 +/− 0.72 for healthy controls. FEL levels were significantly higher in IBD patients compared to IBS patients (p = 0.001) and healthy controls (p = 0.002). There was no significant difference in mean FEL concentration between UC and CD patients (p = 0.8) and between IBS and healthy controls (p = 0.34). However, the mean FEL concentrations were significantly higher in active UC patents compared to inactive UC patients (mean FEL: 100 +/− 40.9 vs 4.67 +/−1.2, p = 0.04). This comparison was not significant for Crohn’s patients (p = 0.1). The correlation coefficient between disease activity and FEL concentrations for UC patients were 0.54 (p = 0.0001) and for CD patients was 0.4 (p = 0.02).The sensitivity and specificity of the FEL assay for distinguishing active IBD from IBS/healthy controls were 90.5% and 95.7% respectively. The positive and negative predictive values were 70.4% and 98.9%.
Conclusion: FEL is an inexpensive and non invasive test that can provide the clinician with a marker to differentiate between IBD and IBS. These preliminary data suggest that FEL could be used as a non-invasive marker for determining whether patients who have IBS should have endoscopic investigations.
REVERSING A VIRTUAL LESION IN HUMAN SWALLOWING MOTOR CORTEX WITH CORTICAL STIMULATION: A MODEL FOR DYSPHAGIA AFTER STROKE?
S. Jefferson1, S. Mistry1, L. Hancock1, J. Rothwell2, S. Hamdy1. 1GI Sciences, University of Manchester, Salford, 2Sobell Department of Neurophysiology, Institute of Neurology, UCL, London, UK
Introduction: We have previously shown that transcranial magnetic stimulation (TMS) delivered at 1 Hz to pharyngeal motor cortex can unilaterally suppress cortical excitability (virtual lesion) which can transiently alter swallowing behaviour.1 Here we examine if an excitatory intervention (5 Hz repetitive TMS (rTMS)) applied to the contralesional hemisphere can reverse a virtual lesion as a prelude to applying such neurostimulation in the treatment of dysphagia after stroke.
Aims & Methods: Healthy volunteers (n = 12, 5 male, mean age 39 years) underwent single pulse bi-hemispheric TMS measurements of cortico-pharyngeal excitability via a swallowed intraluminal catheter, before and for 60 min after 10 min of 1 Hz rTMS delivered to unilateral pharyngeal motor cortex. Five Hz rTMS (250 pulses over 90 seconds) or sham was then applied to the contralesional hemisphere randomised to different sessions, 1 week apart. Post-lesional cortical excitability following active intervention vs. sham was compared using ANOVA.
Results: As expected, sham rTMS had no effect on the suppression of excitability induced by the virtual lesion, with both lesional and contralesional hemispheres decreasing by a maximum of −35% and −16% respectively. By contrast, active 5 Hz rTMS completely abolished the virtual lesion, reversing the direction of excitability both in the lesional and contralesional hemispheres by +35% and +25%, respectively (p = 0.035, fig).

Conclusion: Fast rTMS applied to the contralesional hemisphere completely reverses a unilaterally induced virtual lesion in pharyngeal motor cortex. These data support the notion that rTMS might be usefully applied in stroke patients, as a therapeutic intervention for dysphagia.
AUTONOMIC EFFECTS OF OESOPHAGEAL ACIDIFICATION AND THEIR RELATIONSHIP TO THE DEVELOPMENT OF HUMAN VISCERAL PAIN HYPERSENSITIVITY
A. Sharma1, P. Paine1, Q. Aziz2. 1GI Sciences, Hope Hospital, Salford, 2Wingate Institute of Neurogastroenterology, Barts and the Royal London, School of Medicine and Dentistry, Queen Mary University, London, UK
Introduction: Visceral pain hypersensitivity (VPH) is a common feature of functional gastrointestinal disorders (FGD). We have shown previously that distal oesophageal acidification induces sensitisation of spinal dorsal horn neurones leading to the development of VPH in the non-acid exposed proximal oesophagus (PO).1 Variability exists in the degree to which individuals sensitise but factors that modulate this are unknown. As the parasympathetic (PNS) and sympathetic nervous systems (SNS) have been proposed as pro-nociceptive and anti-nociceptive respectively we decided to study their influence on sensitisation in our model.
Aims & Methods: To determine whether differential autonomic reactivity predicts the degree of VPH to oesophageal acidification. Methods In 25 healthy volunteers, pain thresholds (PT) to electrical stimulation (in milliamperes, mA) were determined in the PO pre- and post a randomised double-blind 30-min distal oesophageal infusion of either 0.15M HCl or saline. All subjects had autonomic monitoring before and during the infusion. Selective PNS (cardiac vagal tone (CVT) and cardiac sensitivity to baroreflex (CSB)) and SNS (cardiac sympathetic index (CSI)) measures were derived.
Results: There was a significant difference between the mean change in PT in the PO between acid (−3.9 mA (5.5 SD)) and saline 2.6 (4.9 SD)) suggesting the development of VPH with acid (p<0.0001 Wilcoxon, n = 25). Of the 25, 16 had a fall in PO PT of ⩾5 mA with acid and thus sensitised. End-infusion heart rate (HR) and mean arterial pressure (MAP) were significantly higher with acid than saline (73.4 (9.9 SD) vs 67.7 (7.6 SD), p = 0.0001 for HR, paired t test) and (100.4 (13.4 SD) vs 95.0 (13.5 SD), p = 0.0007 for MAP, paired t test). End-infusion CVT and CSB were significantly lower with acid than saline ((p = 0.01, Wilcoxon; CVT) and (p = 0.0038, Wilcoxon; CSB). End-infusion CSI was greater for acid than saline (p = 0.0016, paired t-test). In the 16 sensitisers, the degree of sensitisation was related to increasing heart rate (r = −0.66, 95% CI −0.87 to −0.25, p = 0.005), and fall in CVT (r = 0.54, 95% CI 0.06 to 0.82, p = 0.031) and CSB (r = 0.54, 95% CI 0.06 to 0.82, p = 0.030). A trend was also apparent that increasing CSI might be associated with increasing sensitisation (r = −0.43, 95% CI −0.76 to 0.08, p = 0.09).
Conclusion: Oesophageal acidification is associated with SNS activation and PNS withdrawal. In turn greater PNS withdrawal is associated with greater sensitisation. These data suggest the PNS may have anti-hyperalgesic properties in the human viscera. Future studies using pharmacological modulation of the autonomic nervous system may be beneficial in modulating VPH.
Plenary session
PRELIMINARY RESULTS OF THE UK COMPARATIVE AUDIT OF OVER 6500 PATIENTS WITH ACUTE UPPER GASTROINTESTINAL BLEEDING
S. A. Hearnshaw1, D. Lowe2, R. F. Logan3, M. F. Murphy4, S. P. L. Travis1, K. R. Palmer5. 1Gastroenterology, John Radcliffe Hospital, Oxford, 2CEEU, Royal College of Physicians, London, 3Epidemiology and Public Health, University of Nottingham, Nottingham, 4NHS Blood and Transplant, John Radcliffe Hospital, Oxford, 5Gastroenterology, Western General Hospital, Edinburgh, UK
Introduction: In 1993, Rockall et al reported a large audit of patients presenting with acute upper gastrointestinal bleeding (AUGIB) to 4 health regions in England.1 Mortality overall was 14%, with in-patient bleeding mortality 33%. A risk-score developed from this audit (Rockall score) has been shown to predict re-bleeding and death.2 Guidelines recommend early endoscopy for those at high risk.3 Considerable changes have occurred in the presentation and management of AUGIB in the 14 years since Rockall. These include differences in demography, resuscitation, endoscopic therapy and use of specific drugs. At the same time there is concern that inadequacies in service provision may have adversely affected outcomes in some hospitals.
Aims & Methods: To audit current care in UK hospitals for managing AUGIB against published recommendations.3 To look at aetiological factors, diagnoses and mortality in AUGIB, and to audit the use of risk stratification and early endoscopic therapy in high risk patients. All UK acute NHS hospitals were invited to participate. Enrolled hospitals identified new admissions and in-patients presenting with suspected AUGIB between 1/5/7 and 30/6/7. Endoscopy, laboratory and transfusion data were entered online.
Results: 6750 patients were included for analysis from 208 hospitals; 82% new admissions and 16% in-patients. 37% of patients were aged <60 yrs and 28% >80 years with mean (SD) age 64.4(19.7) years. 50% had at least one comorbidity, with 9% having documented cirrhosis. 29% were taking aspirin, 12% an NSAID. 26% had a history of alcohol excess. Risk assessment scores were calculated by hospitals for 19% of cases. Scores calculated from submitted data showed 28% had final Rockall score 0–2, 44% score 3–5, 24% score 6–8 and 3% score >8. 50% had endoscopy within 24 h of presentation, including 50% of those with a pre-endoscopy Rockall score of >2. Varices or portal hypertensive gastropathy were found in 12%; peptic ulcer disease was the commonest diagnosis (36%). Endoscopic therapy was undertaken in 19% of non-variceal and 65% of variceal cases. 64% received iv PPI after endoscopic therapy (excluding varices). 2% had surgery for AUGIB. Postoperative mortality was 30%. Unadjusted mortality was 10% overall—7% in new admissions and 26% in in-patients.
Conclusion: Despite a population with increasing medical comorbidity and a marked increase in the proportion of patients with varices, the unadjusted mortality of patients with AUGIB has significantly improved in the UK. This could be due to improvements in general health, supportive care, endoscopic haemostasis and acid suppression.
DEFINING THE IMPACT OF ORGAN DYSFUNCTION IN CIRRHOSIS: SURVIVAL AT A COST?
D. L. Shawcross, M. J. Austin, R. D. Abeles, M. McPhail, A. Yeoman, A. J. Portal, W. Bernal, G. Auzinger, E. Sizer, J. A. Wendon. Institute of Liver Studies, King’s College Hospital, London, UK
Introduction: Cirrhosis kills more men than Parkinson’s disease and more women than cervical cancer. The incidence of cirrhosis is increasing exponentially and it is projected that there will be a fivefold increase in demand for liver transplantation in the next 6–10 years. Historically, the perception of cirrhosis with organ dysfunction as having a poor prognosis has fuelled a self-fulfilling prophecy with iniquitous access to intensive care (ICU). However, recent data to support this view is lacking. We report the 7-year experience of the outcome, physiological disturbance and resource utilisation of 658 emergency admissions with cirrhosis and organ dysfunction to a specialist liver ICU at King’s College Hospital.
Aims & Methods: We prospectively collected and analysed physiological and biochemical variables on day 1 and 3 of admission. Outcome variables, organ scores (Child Pugh, MELD, SOFA and APACHE II) and number of days requiring vasopressors, ventilation and renal replacement therapy (RRT) were recorded. The Therapeutic Intervention Scoring System (TISS) score, validated as a tool for estimating cost in ICU, was calculated.
Results: Alcohol was the most common aetiology (47%) and variceal bleeding the most common reason for admission (35%). 51% required inotropes, 72% invasive ventilatory support and 49% RRT during their ICU stay. Despite this, ICU admission for many of these patients with cirrhosis was not futile, with 55% surviving their ICU stay and 41% surviving to discharge. Variceal bleeders had a 30-day survival of 53% versus 33% with a non-variceal indication for admission (p<0.0001). 19% of survivors subsequently underwent liver transplantation. Survival was at a significant cost to the NHS (median cost per patient: £12,403 (4636–27,283) for a median 7-day admission (3–15)). Admissions with multi-organ failure (with and without requirement for RRT) cost significantly more (multi-organ failure p<0.001; RRT p<0.0001) and had more prolonged lengths of stay compared to those that did not (p<0.0001). There was no difference in cost, length of stay or outcome (p = 0.2) between patients with alcoholic liver disease and other aetiologies. RRT was well tolerated and facilitated stability and/or recovery in 23/59 (39%) patients who were subsequently transplanted.
Conclusion: More than 50% of patients admitted as emergencies will survive their ICU stay with the majority of these surviving to hospital discharge. These data challenge the widely held prejudice that patients with cirrhosis requiring emergency admission to ICU inevitably die. This endorses the establishment of managed clinical care networks and demands the engagement of all levels of critical care and ward based care models in the treatment of organ dysfunction in cirrhosis.
Gastrointestinal physiology associates group
THE EFFECT OF ARGON PLASMA COAGULATION ABLATION ON OESOPHAGEAL MOTILITY AND CHEMORECEPTOR SENSITIVITY
K. Elghellal, A. Smythe, R. Ackroyd. Surgery, Royal Hallamshire Hospital, Sheffield, UK
Introduction: Barrett’s oesophagus is of clinical importance because of the strong association with oesophageal adenocarcinoma. The use of endoscopic argon plasma coagulation (APC) ablation to eliminate intestinal metaplasia combined with oesophageal acid control has been shown to minimise if not remove the cancer risk.
Aims & Methods: Oesophageal motility and sensitivity appear to be disturbed in Barrett’s oesophagus. As ablation treatment is a thermal technique causing superficial damage, the aim of this study therefore was to look at any further effect of APC on both oesophageal motility and mucosal sensitivity. APC was used to treat 20 patients with Barrett’s oesophagus (16 males and 4 females, median age 56 (range 51–81) years) confirmed at endoscopy and histologically, median Barrett’s segment length 4 cm (range 2–10 cm). Station pull through manometry was carried out 1 week before APC treatment. The lower oesophageal sphincter pressure (LOSP), proximal and distal wave amplitude, primary peristalsis with 5 ml water swallows and secondary peristalsis with air and water bolus was measured. To assess oesophageal sensitivity, acid (0.1NHCl) and alkaline (0.1N NaOH ) provocation was carried out. Lag time to initial discomfort (t), sensory intensity rating (i) (no discomfort = 0, intense pain = 20) and acid perfusion sensory score (t × i/100) were obtained. These tests were repeated 4–6 weeks following successful APC.
Results: Using the Wilcoxon Rank Sum test for statistical evaluation, no significant differences were seen in any of the motility parameters comparing before and after APC. Sensitivity intensity rating and acid perfusion sensory score were significantly higher after APC treatment (pre-APC sensory score for acid = 1.6 (1.8), post-APC sensory score for acid = 0.5 (0.3), p<0.01. Pre-APC sensory score for alkali = 1.5 (1.7), post-APC sensory score for alkali = 0.9 (1.0).
Conclusion: Following reversal of Barrett’s epithelium using APC, no changes in oesophageal motility are seen but a decrease in oesophageal sensitivity occurs. Longer term studies are needed to see if sensitivity improves.
THE EFFECTS OF GLUCOSE, FRUCTOSE AND TAGATOSE ON GASTRIC EMPTYING
A. McGlone, T. J. Little, D. G. Thompson. Section of GI Sciences, University of Manchester, Salford Royal NHS Foundation Trust, Salford, UK
Introduction: The mechanisms by which nutrients, in the small intestine, signal to the CNS to alter gastrointestinal function are poorly understood. It has been suggested that sugars slow gastric emptying (GE) (a proxy measure of brainstem activation) by stimulating “osmoreceptors” in the small intestine; however, at a low osmolality, solutions of glucose and fructose appear to empty differently,1 suggesting that the potency of the feedback may also depend on the sugar molecule per se. It is known that the length of intestine exposed to nutrient is important for the regulation of GE. In dogs, slowing of GE by glucose is dependent on exposure of at least 15 cm of the small intestine to nutrient, and the intensity of the feedback increases as the length of exposure is increased.2 Differences in the absorption of hexose sugars may, therefore, be an important determinant of their effects on GE.
Aims & Methods: This study therefore aimed to determine whether tagatose, a poorly absorbed hexose sugar (used as a non-caloric sweetener), would slow gastric emptying to a greater extent than glucose or fructose. 12 non-obese subjects (7F, 5M; BMI 23 (0.76) kg/m2) drank 500 ml solutions of 250 mOsmol glucose, fructose or tagatose, and water (non-osmotic control for volume), each labelled with 100 mg of 13C-acetate. Gastric emptying was assessed over 45 min (breath samples collected every 5 min) using a 13C-acetate breath test; the lower the cumulative 13CO2:12CO2, the slower the rate of gastric emptying.
Results: There was a significant effect of hexose type on gastric emptying (p<0.05). The mean cumulative 13CO2:12CO2 values for tagatose were 139.5 (18.2) units lower than those for water, 123.8 (23.4) units lower than those for glucose, and 99.4 (17.5) units lower than those for fructose (p<0.05, for all), whereas there was no difference between glucose, fructose and water. There was, however, substantial interindividual variation in the gastric emptying response, particularly for tagatose and fructose. In general, those individuals who were most able to slow their GE in response to tagatose, had a tendency to slow the GE of fructose.
Conclusion: The poorly absorbed hexose sugar, tagatose, slows GE more potently than fructose and glucose, both of which would be expected to be absorbed more completely in the proximal small intestine, thus limiting the length, and duration, of exposure of the small intestine. However, there was substantial phenotypic variation in the gastric emptying responses to hexose sugars. Since the rate of GE closely correlates with ingested meal volume, this observation may have implications for the regulation of food intake.
Oesophageal free papers
AN IMPROVED STAGING SYSTEM FOR OESOPHAGEAL ADENOCARCINOMA BASED ON THE NUMBER OF INVOLVED LYMPH NODES
C. J. Peters1, R. H. Hardwick2, J. R. E. Rees3, S. L. Vowler4, P. M. Safranek2, V. Save5, N. Carroll6, S. Dwerryhouse2, N. Imrit7, N. Maynard7, G. W. B. Clark8, R. C. Fitzgerald1. 1MRC Cancer Cell Unit, Hutchison MRC Research Centre, Cambridge, 2Cambridge Oesophago-Gastric Centre, Addenbrooke’s Hospital, Cambridge, 3Department of Surgery, Bristol Royal Infirmary, Bristol, 4Cancer Research UK, Li Ka Shing Centre, Cambridge, 5Department of Histopathology, Addenbrooke’s Hospital, Cambridge, 6Department of Radiology, Addenbrooke’s Hospital, Cambridge, 7Oxford Oeosphago-Gastric Unit, Oxford Radcliffe Hospital, Oxford, 8Department of Surgery, University Hospital of Wales, Cardiff, UK
Introduction: The incidence of oesophageal adenocarcinoma has quadrupled in the last 30 years and outcomes remain poor. Oesophageal adenocarcinoma is now the commonest oesophageal malignancy yet is staged using a system originally developed for squamous cell carcinomas. This system does not take into account the number of involved lymph nodes despite increasing evidence this is prognostic. There is a growing consensus in the literature that a new staging system is required.
Aims & Methods: The aim of this study was to develop a new staging system for GOJ adenocarcinoma based on the number of involved lymph nodes. A systematic retrospective database was created of 280 patients diagnosed with GOJ adenocarcinoma in whom outcome data were available from 3 UK tertiary referral centres. We collected detailed information on lymph node status and found the association with outcome using SPSS and Prism. We developed a new N-stage using recursive partitioning with the R Statistical package.
Results: T-stage (p<0.0001), current N-stage (p<0.0001), differentiation (p = 0.0002), presence of neurovascular invasion (p<0.0001) and resection margin status (p<0.0001) were all prognostically significant on univariate analysis. Recursive partitioning of nodal positive patients generated the following revised N-stage: N0 = No involved nodes (from present system), N1 = 1–2 involved lymph nodes, N2 = 3–5 involved lymph nodes, and N3 = 6 or greater involved lymph nodes. This new system was highly prognostically significant on univariate analysis (p<0.0001) and outperformed the current N-stage on multiple regression analysis. Furthermore it identified a subgroup of nodal positive patients (N3) with a dismal prognosis (0% 5-year survival), equivalent to that of M1 disease.
Conclusion: We have developed a new N-stage for GOJ adenocarcinoma, based on the number of involved lymph nodes, which outperforms the existing system on multiple regression analysis and provides the ability to discriminate between nodal positive patients. We are in the process of validating our findings on an external dataset but this system has the potential to vastly improve our ability to make management decisions. We feel it is time to change the way we stage GOJ adenocarcinoma.
PRELIMINARY RESULTS OF A RANDOMISED CONTROLLED TRIAL INTO THE SAFETY AND EFFICACY OF ALA VERSUS PHOTOFRIN PHOTODYNAMIC THERAPY FOR HIGH GRADE DYSPLASIA IN BARRETT’S OESOPHAGUS
G. D. Mackenzie, J. M. Dunn, M. R. Novelli, S. Mosse, S. M. Thorpe, S. G. Bown, L. B. Lovat. National Medical Laser Centre, University College London, London, UK
Introduction: Photodynamic therapy (PDT) using Photofrin is a licensed minimally invasive treatment for Barrett’s high grade dysplasia (HGD). Photofrin PDT affects the entire oesophageal wall and causes strictures in 18–50% of patients. Patients must also avoid bright light for 3 months to prevent sunburn. 5 aminolaevulinic acid (ALA) is preferentially concentrated in the oesophageal mucosa. The risk of stricture is therefore very low. Light sensitivity for ALA lasts for only 36 hours. The aim of current RCT is to determine if PDT for HGD using ALA is safer and more effective than Photofrin.
Aims & Methods: Patients with HGD in Barrett’s oesophagus confirmed on at least two occasions by at least two independent pathologists were offered participation in the above RCT. Any visible nodules of HGD were removed and patients only treated if residual HGD was proven to still be present. To ensure length of Barrett’s and extent of HGD were similar in each treatment group patients were stratified for these two factors prior to randomisation. Patients received either Photofrin PDT with the standard licensed protocol or as previously shown to be the most effective 60 mg/kg of ALA activated by 1178 J/cm of red laser light. Follow-up was quadrantic biopsies every 2 cm throughout the treated area of Barrett’s at 6 weeks, 4 months and 1-year post therapy. All side effect data were collected.
Results: Forty patients (out of a planned 66) have so far been recruited and 32 treated; 16 with ALA and 16 with Photofrin. Five patients are undergoing repeat therapy (3 with photofrin and 2 with ALA) and 27 patients are in follow-up. Remission rates are 14/14 (100%) in the ALA group and 9/14 (64%) in the photofrin group (Fisher’s exact test, two-sided p value<0.05). Strictures developed in 6/16 patients treated with Photofrin and 1/16 with ALA, the latter is thought to relate to uncontrolled and significant acid reflux at the time of therapy measured on 24-h pH monitoring (Fisher’s exact test, one-sided p value<0.05). Skin photosensitivity developed in 7/16 patients treated with Photofrin, one of whom was briefly admitted to hospital. There were none with ALA (Fisher’s exact test, one-sided p value<0.05). There are no significant differences to date between groups with respect to other side effects.
Conclusion: The preliminary data are encouraging and suggest that ALA PDT is both safer and potentially more effective than Photofrin PDT but follow-up is short and only half the planned number of patients have been treated to date.
NARROW BAND IMAGING WITH MAGNIFICATION IS SUPERIOR TO WHITE LIGHT ENDOSCOPY WITH MAGNIFICATION IN STUDYING THE MUCOSAL MORPHOLOGY IN BARRETT’S OESOPHAGUS
R. Singh1, V. Owen2, H. Karageorgiou1, G. K. Anagnostopoulos1, K. Garsed1, P. Fortun1, E. Fogden1, V. Subramaniam1, A. Shonde1, P. Kaye1, C. J. Hawkey1, K. Ragunath1. 1Wolfson Digestive Diseases Centre, Nottingham University Hospitals Trust, 2Trent Research and Development Support Unit, University of Nottingham, Nottingham, UK
Introduction: Narrow band imaging with magnification (NBI-Z) can reliably predict histology in Barrett’s oesophagus (BE). Although available in a single unit, the utility of white light endoscopy with magnification (WLE-Z) in BE has not been assessed in prior studies.
Aims & Methods: The aim of the study was to see if there is any appreciated difference in imaging characteristics between WLE-Z and NBI-Z in BE and if this translated into clinically relevant benefit in the prediction of histology, specifically looking at dysplasia detection. This was a prospective cohort study involving 21 patients (75 areas with corresponding NBI-Z and WLE-Z images) with BE. Mucosal patterns were evaluated for its image quality on a visual analogue scale (VAS) of 1–10 by 5 expert endoscopists specifically looking at the pit pattern and microvascular morphology. The endoscopists then predicted the histology based on four subtypes which can be visualised in BE: Type A: round pits with regular microvasculature (columnar mucosa without intestinal metaplasia); Type B: villous/ridge pits with regular microvasculature (specialised intestinal metaplasia); Type C: absent pits with regular microvasculature (specialised intestinal metaplasia); Type D: distorted pits with irregular microvasculature (high grade dysplasia). The sensitivity (Sn), specificity (Sp), positive (PPV), negative predictive values (NPV) and accuracy (Acc) compared to the final histopathological analysis and the interobserver variability among the 5 assessors were then calculated.
Results: The overall pit quality was significantly higher for NBI-Z compared to WLE-Z (VAS: NBI-Z = 6, WLE-Z = 4.5; z = 11.0, p<0.001). The overall vasculature quality was also significantly better for NBI-Z (VAS: NBI-Z = 7.3, WLE-Z = 4.9, z = 14.1, p<0.001). This translated into a superior prediction of histology in BE with higher Sn, Sp, PPV, NPV and Ac for NBI-Z compared to WLE-Z (table). Looking specifically at the prediction of dysplasia, NBI-Z was superior to WLE-Z (χ2 = 10.3, df = 2, p = 0.006). The overall kappa agreement amongst the 5 endoscopists for NBI-Z and WLE-Z were 0.59 and 0.31 respectively (p<0.001).
Conclusion: NBI-Z is superior to WLE-Z in the prediction of histology in BE with good reproducibility. This novel imaging modality could be an important tool for surveillance in patients with BE.
IMPROVING OUTCOME IN PATIENTS WITH OESOPHAGEAL CANCER
A. K. Saha, C. Sutton, S. P. L. Dexter, A. I. Sarela, H. M. Sue-Ling. Academic Division of Surgery, The General Infirmary at Leeds, Leeds, UK
Introduction: The management of oesophageal cancer has changed significantly over the past 30 years. Improved preoperative and postoperative care, sub-specialisation and increasing use of chemotherapy and radiotherapy have all contributed to improved survival. Our unit has previously reported how these changes had begun to improve overall outcomes1 and suggested that they could be further improved by continuing these changes.
Aims & Methods: Using a prospectively maintained database, all patients who underwent oesophageal resection between January 2000 and December 2006 were reviewed. The results were analysed and compared with previously published and presented audits of oesophagectomy from our unit between 1975–88 and 1990–9.
Results: Results are summarised in the table. In-hospital mortality has improved from 27% to 2.9% and 5-year survival has improved from 7% to 52%.
Conclusion: These results are encouraging and suggest that the outlook for patients with oesophageal cancer can be greatly improved by earlier diagnosis, greater specialisation and a multi-disciplinary approach to the management of oesophageal cancer.
EOSINOPHILIC OESOPHAGITIS: RARE DISEASE OR A DIAGNOSIS FREQUENTLY MISSED?
V. Kanakala1, C. Lamb2, R. W. Stirling3, S. E. Attwood1. 1General Surgery, 2Gastroenterology, 3Pathology, North Tyneside General Hospital, North Shields, UK
Introduction: The diagnosis of eosinophilic oesophagitis (EO) is relatively rare although there has been a dramatic rise in the frequency of case reports and case series over the past 10 years.
Aims & Methods: This study aimed to identify the frequency of diagnosis of EO in our community, how the diagnosis was made or suspected and the outcome of specific interventions once the diagnosis was made. The pathology records of gastroscopies performed (62 437) in all the hospitals in Northumberland during years 2001–Oct 2007 were reviewed for patients with a diagnosis of EO (>20 per HPF) on any biopsy sample. The clinical details were obtained from the case notes and hospital electronic database.
Results: Eighteen patients who were diagnosed as having EO were all male with a median age of 46 years (range 17–85 years). There was a median time delay of 2 years between onset of symptoms and diagnosis (range 1–>10 years). Our results show that the endoscopic findings rarely directed the decision to biopsy as most patients had the suspicion of the disease raised beforehand (13/18). In 5 the endoscopic appearances prompted a biopsy not previously planned. 17 patients presented with intermittent dysphagia which is the characteristic symptom of EO. Only two patients had definite response to PPI therapy. In three we felt that treatment was not necessary due to mild symptoms. Treatment outcomes >6 months are available in 13 with good response to oral systemic steroids, ingested topical steroids and oral montelukast. Stricture dilatation was indicated in two patients with good results.

Conclusion: It is very likely the infrequent diagnosis of eosinophilic oesophagitis is due to a lack of clinical suspicion and failure to biopsy rather than there being a true low incidence. The presentation of frequent bolus obstruction, intermittent or continuous dysphagia refractory to routine PPI therapy should prompt oesophageal biopsies to look for eosinophils, as this condition can be effectively treated by medical management.
RISK FACTORS FOR THE DEVELOPMENT OF OESOPHAGEAL CANCER IN BARRETT’S OESOPHAGUS: A PRIMARY CARE NESTED CASE-CONTROL STUDY
S. C. Cooper1, P. Graham2, N. J. Trudgill1. 1Department of Gastroenterology, Sandwell General Hospital, West Bromwich, 2Information Department, Worcester Acute Hopsitals, Worcester, UK
Introduction: The annual risk of Barrett’s oesophagus (BO) progressing to oesophageal cancer (OC) is estimated between 0.5–2%. Previous studies examining risk factors for OC in BO have been limited to surveillance patients, with inherent selection biases.
Aims & Methods: The Health Improvement Network (THIN) and General Practice Research Database (GPRD) collects information from UK primary care patients. Patients with BO with at least two years of follow-up were identified. The influence of age, gender and drugs potentially associated with OC development was examined. Cox regression analysis, adjusted for age and gender, generated hazard ratios for association with OC development.
Results: 4571 BO patients were eligible for the study providing 20 703 years of follow-up, median 4 (IQR 3–6) years. 70 developed OC (0.3% pa). Median age (IQR) in OC patients was 67 (62–72) and in BO without OC 63 (52–72) and, hazard ratio (95% CI) 1.03 (1.01–1.05) p = 0.001, for each increasing year. Male gender was associated with developing OC (OC 81% male, BO 63% male); 2.64 (1.44–4.8) p = 0.002. After adjusting for age and gender, inhaled steroids (OC 30% vs BO 19%), 1.79 (1.07–2.99) p = 0.025 were the only drug associated with progression to cancer. Use of PPIs was negatively associated with progression to cancer 0.42 (0.18–0.98) p = 0.045, while aspirin showed a non-significant trend towards a negative association 0.68 (0.4–1.15). Cumulative addition of drugs for COPD/asthma led to increasing association with OC (1 drug 0.83 (0.37–1.84), 2 drugs 1.38 (0.74–2.57), 3 drugs 2.84 (1.27–6.34) p = 0.011).
Conclusion: Male gender and increasing age in BO patients were associated with progression to OC. Inhaled steroid use, and cumulative use of respiratory drugs was associated with the development of OC, suggesting a potential role for COPD or asthma in the aetiology of oesophageal cancer in BO.
ANALYSIS OF SUPINE GASTRO-OESOPHAGEAL REFLUX VARIABILITY DURING 96 HOURS MONITORING USING BRAVO CAPSULE
K. P. Basavaraju1, A. Anggiansah2, M. Fox1, T. Wong1. 1Gastroenterology, 2Oesophageal laboratory, St Thomas Hospital, London, UK
Introduction: Bravo catheter-free oesophageal pH monitoring allows prolonged monitoring of gastro-oesophageal acidic reflux (GOR) up to 96 hours. The day-to-day concordance of upright GOR data during 48-hour recordings has been reported as fair, but poor for supine data. There are very few data available regarding the variability of supine GOR in patients with 96-h recording.
Aims & Methods: This study aimed to evaluate inter- and intrapatient variability for supine GOR over 96 h and determine the effect of meal to bedtime (MBT) on the supine GOR.
We analysed 80 consecutive oesophageal pH studies that completed 96-h recordings between October 2004 and October 2007 in our unit. 34 (42.5 %) of these patients with abnormal supine GOR (pH>3.45%) were included in the study. The main recumbent period for each 24-h period was divided into two halves (H1 and H2). The two halves were compared on reflux time (%) and total number of refluxes (TNR) across the 96-h period. Cumulative diagnostic yield using prolonged pH monitoring for each 24 h was analysed. Reflux time (%) was compared for patients with MBT cut-off of 2 and 3 h during both H1 and H2 across the 96-h period.
Results: Within-individual variability for supine GOR for H1 and H2 across the 96-h period was high (intraclass correlations only 0.091, 0.146 respectively). Median values for reflux time (%) and TNR for each of the halves across the 96-h period are shown below (table 1). Measurements of % GOR for H1 were significantly higher than those for H2 (Wilcoxon signed-rank test, p<0.001). There was a similar decrease for TNR (p<0.001). The cumulative diagnostic yield for pathological supine GOR was 73.5%, 88.23%, 88.23% and 100% at 24 h, 48 h, 72 h and 96 h respectively. The median for MBT was 3.53 h. During H1, MBT of <2 h (n = 29.4%) was significantly associated with increased supine reflux compared to MBT >2 h (n = 70.6%) (Wilcoxon rank sum test, p = 0.02), but not during H2 (p = 0.21). There was no significant difference in supine reflux with patients retiring to bed <3 h (n = 47.8 %) vs >3 h (n = 52.2%) in either H1 (p = 0.38) or H2 (p = 0.79).
Conclusion: Variability in the supine position showed little day-to-day diagnostic reproducibility with resulting increased diagnostic yield with prolonged recording up to 96 h. The supine GOR is greatly reduced in the second half of the night compared to the first half. Patients going to bed within 2 h, but not 3 h, of a meal are at a higher risk of experiencing increased supine GOR.
Health service research and IT free papers
DEEP CLEAN: THE WAY FORWARD IN CONTROLLING C DIFFICILE INFECTION?
A. Malik1, D. W. Bullimore2. 1Medicine, Nevill Hall Hospital, Abergavenny, 2Medicine, Barnsley NHS FT, Barnsley, United Kingdom
Introduction: Because of concerns about hospital acquired infection the Government has proposed a “Deep Clean” programme of wards in all NHS hospitals. Alan Johnson1 has expressed this as: “This deep-clean programme will give hospitals a one-off blitz so walls, patient equipment and ventilation ducts are disinfected and scrubbed clean, a ward at a time.” It is noted the total cost could be £50m. Our Trust undertook a similar process in 2006. We have examined the results of the Deep Clean on subsequent infection rates with C difficile on eight medical wards to see what benefits resulted.
Aims & Methods: A microbiology database of all C difficile positive samples recorded during 2006 was analysed. The file was filtered for in-patients only, ranked by date, duplicates removed and further sub-filtered by ward. The Deep Clean took approximately 4 weeks/ward. The return date for the ward and the subsequent 3-month period was plotted on the spreadsheet against the year’s cases of C difficile, so that for each ward the number of cases in this period could be compared against the number for the whole year. Figures for 8 medical wards were analysed. The Medical Admissions Unit and a decanting/overspill ward were excluded from analysis. Ward infection rates were similarly derived for 2005 and January–April 2007.
Results: A total of 209 c.difficile infections were identified on the 8 wards in 2006, this was an increase from 81 infections in 2005. Of the 209 infections 53 (observed 25% vs expected 25%, no significant difference) occurred during the 3-month period immediately following return of patients to the cleaned ward. The number of cases/ward was highly variable, despite 7 of the wards being broadly similar in size. The ranking of number of cases between wards also varied considerably for the periods 2005, 2006 and January–April 2007. In the longer term 70 cases of C difficile occurred during the first 4 months of 2007. This gave a projected annualised rate for 2007 of 210 cases, compared with 209 cases for 2006, demonstrating no significant difference. (The closeness of observed and expected figures is itself a statistical aberration.)
Conclusion: The Deep Clean process did not alter subsequent infection rates in the short term or longer term. This perhaps suggests that infection via spore transmission is not common in the hospital setting. Patient to patient transmission may occur and/or use of antibiotics in debilitated patients may lead to auto-infection in a suppressed bowel flora. The use of communal toilet facilities needs to be investigated as a factor in patient to patient transmission. Deep Clean policies are unlikely to control C difficile infections on hospital wards.
A RETROSPECTIVE RECORD-LINKAGE STUDY TO FOLLOW UP PATIENTS WITH NO CLINICALLY OBVIOUS LIVER DISEASE FROM THEIR FIRST LIVER FUNCTION TESTS IN PRIMARY CARE
D. J. McLernon1, P. T. Donnan1, J. F. Dillon2. 1Tayside Centre for General Practice, 2Pathology and Neurosciences, University of Dundee, Dundee, UK
Introduction: Liver function tests are routinely performed in primary and secondary care and often lead to further invasive and expensive investigations. The aim of this study was to follow up individuals with LFTs initiated in primary care with no obvious liver disease and to ascertain their outcomes.
Aims & Methods: A population-based retrospective cohort study followed up these patients in Tayside from 1989 to 2003 to subsequent diagnosed liver disease, mortality from liver disease and all-cause mortality. Record linkage of datasets including biochemistry, hospital admissions, psychiatric admissions, death registry and prescriptions enabled ascertainment of risk factors and outcomes. Sensitivity, specificity, positive predictive value and negative predictive value analyses were carried out and Weibull regression analysis from initial LFT date was performed on outcomes of mortality and liver disease by level of LFT abnormality.
Results: 95 977 patients had 364 194 incident initial LFTs taken during the 15-year period 1989 to 2003, with median follow-up 3.7 years. At initial tests, 21.7% had at least one abnormal LFT and 1213 (1.3%) developed liver disease. Elevated transaminases were strongly associated with diagnosed liver disease, HR = 4.20 (3.54, 4.98) for mild levels and HR = 11.99 (9.26, 15.52) for severe levels vs. normal. For GGT these hazards were 2.46 (2.12, 2.86) and 13.21 (10.60, 16.46) respectively. Low albumin was strongly associated with all cause mortality, 2.65 (95% CI 2.47 to 2.85) for mild levels and 4.99 (95% CI 4.26 to 5.84) for severe levels. Sensitivity for predicting events over 5 years was low and specificity high. For liver disease the sensitivity and specificity values were: albumin (9%, 98%), alkaline phosphatase (32%, 90%), transaminase (35%, 93%) and GGT (62%, 85%).
Conclusion: All LFTs were predictive markers for liver disease as well as general ill health, although sensitivity was poor. Many patients with abnormal LFTs detected in this study had no later formal diagnosis of liver disease but may be alcohol abusers on the road to liver problems. That liver disease takes time to develop illustrates a window of opportunity to intervene in these patients with lifestyle advice, alcohol therapies or drugs.
DIVERTICULAR DISEASE HOSPITALISATIONS HAVE A RAPIDLY INCREASING IMPACT ON THE HEALTH SERVICE AND AFFECT YOUNGER PEOPLE AND DEPRIVED SOCIOECONOMIC GROUPS
S. Jeyarajah1, P. P. Tekkis2, P. Aylin3, I. Bjarnason4, S. Papagrigoriadis1. 1Department of Colorectal Surgery, King’s College Hospital, 2Department of Biosurgery and Surgical Technology, St Mary’s Hospital, 3Department of Epidemiology, Imperial College, 4Department of Gastroenterology, King’s College Hospital, London, UK
Introduction: Diverticulosis of the colon is common in the Western world with a prevalence of approximately 33% in patients over 60 years of age. In the UK, there are few data on the epidemiology of diverticular disease (DD) particularly with regards to the effect of social deprivation on disease presentation and clinical management.
Aims & Methods: This was a population-based study across the UK of all hospital episodes reporting on clinical outcomes of patients admitted with diverticular disease as the primary or secondary diagnosis between 1996–2006. The Hospital Episode Statistics and the general population 2001 Census databases were used for data extraction. Social deprivation was evaluated using quintiles of socioeconomic deprivation based on the Carstair’s classification. Logistic regression analysis was used to evaluate the study end points.
Results: Over the study period there were 1 219 480 admissions with the diagnosis of DD; 567 423 patients with DD as a primary cause for admission and 652 057 as a secondary diagnosis (comorbidity). Primary admissions increased from 0.6 to 1.2/1000 population (p<0.001). The mean age of primary DD decreased from 67.8 to 66.8 years (p<0.001). 732 493 (60.1%) of all admissions with DD were female patients. The median in-patient length of stay (LOS) was 6 days (range 0–2,283, 75th percentile 12 days). 179 426 (31.62%) patients were emergency admissions. 38 796 (6.8%) patients with primary DD underwent a laparotomy and 560 (0.1%) required admission to ITU. There were 29 168 (5.1%) in-hospital deaths. The admission rate within 28 days and at one year was 4.9% and 46.8% respectively. 101 688 (17.9%) patients were in the fifth Carstairs quintile (most deprived). In-hospital mortality following admission for DD was highest in the lowest socioeconomic group (OR 1.2, p<0.01). Emergency re-admission within 28 days (OR 1.4, p<0.01) and at 1 year (OR 1.7, p<0.01) were more likely in the lowest socioeconomic groups. In-hospital LOS >12 days was more likely in the least deprived patient group (OR 1.4, p<0.01). The need for surgery was most likely in the most affluent patients.
Conclusion: The study suggests an increasing incidence of diverticular disease hospital admissions across all socioeconomic groups with disease migration to younger patients. In-hospital mortality, length of stay and re-admissions were more likely to occur in the most deprived patients. Diverticular disease has a large financial and social burden to the NHS. New research and management strategies are required for prevention in the community thus minimising in-hospital complications.
AN OPEN-SOURCE BROWSER-BASED ENDOSCOPY MANAGEMENT SYSTEM THAT MAPS TO SNOMED CT
J. L. Brown1, A. MacDonald2, J. Davies2, P. Ryder2. 1Department of Gastroenterology, Gloucestershire Royal Hospital, Gloucester, 2Beaumont-Colson Ltd, Software Developers, Newcastle, UK
Introduction: European, American and Japanese Gastrointestinal Endoscopy Societies have worked collaboratively to devise an international lexicon of terms and attributes (with definitions) to be used for endoscopy reporting (Minimal Standard Terminology for Digestive Endoscopy V2.0 – OMED 2002). Since April 2003, SNOMED CT was identified as the preferred clinical terminology for NHS information systems. A project to map MST to SNOMED CT was commissioned in 2002 by the former NHS Information Authority and this was undertaken with representation from the BSG IT subcommittee. The dataset is freely available for BSG members to review on the society’s website and may also be obtained from Connecting for Health. With the exception of the National Bowel Cancer Screening software, we are not aware of any clinical implementations of the endoscopy subset.
Aims & Methods: In order to demonstrate that this dataset is fit for purpose we have built a web application (Endoplex) that allows clinicians to aggregate terms in a browser to generate a clinical report. Open Source materials (comprising an Apache web server, MySQL database server and PHP scripts) have been used throughout. The application, supported by AJAX (asymmetric javascript XML) methods, permits client sided processing of the SNOMED CT dataset from within the browser cache.
Results: The result is a remarkably fast reporting tool which can write coded clinical data to multiple server-sided database tables without the delay of sequential post operations and screen refreshes. Reports can be printed onto paper in portable document format or can be viewed as a web page containing embedded multimedia.
Conclusion: We believe our platform-independent solution to be scalable for use within large organisations such as the NHS because the only client-sided requirement is for a web browser and the server PHP scripts allow SQL connections to all the major commercial database engines. Furthermore, inevitable developments in endoscopic technique and reporting syntax merely require a modification to the database reference tables with new SNOMED codes which automatically update the client browser cache. The architecture of Endoplex has been designed to support tariff price calculations, quality assurance monitoring, accessory stock control, HL7 messaging and translation of reports into foreign languages that map to SNOMED CT.
AN INTERACTIVE POLYP DETECTION TRAINING TOOL: DEVELOPMENT AND INITIAL VALIDATION
P. L. Youd, A. Haycock, S. Preston, S. Thomas-Gibson. Wolfson Unit for Endoscopy, Imperial College London, London, UK
Introduction: Cancer prevention depends on the detection, safe removal and post-procedure surveillance of colonic polyps. NHS Bowel Cancer Screening accreditation requires colonoscopists to have an adenoma detection rate (ADR) of at least 20%. Adenoma miss rates of up to 22% have been reported and vary considerably amongst colonoscopists. Colonoscopy trainees receive little specific training in polyp detection and lesion recognition. Self-directed learning material in this area is limited. We describe the first interactive e-learning tool designed specifically for the training and assessment of polyp detection (PDTT).
Aims & Methods: The objectives of this study were: (1) To determine construct validity of a video-based polyp detection assessment tool, and (2) To determine whether a self-directed learning package improves polyp detection. During the initial self-assessment part of the PDTT, trainees watch eleven 10–15 second video clips and are scored based on their ability to accurately detect colonic polyps. The second part is a self-directed, computer-based learning package covering topics such as the importance of polyp detection, improving ADR and newer optical modalities for polyp detection. To confirm construct validity, the self-assessment exercise was undertaken by expert colonoscopists, colonoscopy trainees, endoscopy nurses and clerical staff. Secondly, as part of a pilot study, candidates at the St Mark’s Basic Therapeutic Endoscopy Training Course (BTEC) performed the self-assessment exercise before and after using the learning package. Endoscopy nurses without access to the learning tool were used as a control. Candidates completed feedback questionnaires.
Results: There was a statistically significant difference between the scores on the self-assessment exercise for the four groups (p<0.001, Kruskal-Wallis test). The median score for expert colonoscopists (⩾500 procedures) was 88% (n = 6, range 82–100); trainees (<500 procedures) 45% (n = 18, range 27–64); endoscopy nurses 45% (n = 12, range 18–77) and clerical staff 36% (n = 6, range 23–41). The 14 BTEC candidates demonstrated an average improvement in score of 8.1% after using the learning tool. The 8 endoscopy nurses who undertook the self-assessment exercise twice, without access to the learning material, demonstrated an average improvement of 2.2%, although the difference was not statistically significant (p = 0.18). Candidate feedback described the training module as excellent, fun and useful.
Conclusion: This first dedicated training and assessment tool for polyp detection, employing specifically-designed e-learning technology, has been very well received by trainees. The interactive, self-assessment tool has been shown to have construct validity. The results from the initial pilot study in the use of the teaching tool show promise and require further validation.
Small bowel and nutrition free papers
OUTCOMES FOLLOWING GASTROSTOMY: RADIOLOGICALLY INSERTED VERSUS PERCUTANEOUS ENDOSCOPIC GASTROSTOMY
J. S. Leeds1, M. E. McAlindon1, J. Grant1, H. E. Robson1, S. R. Morley2, F. K. T. Lee3, D. S. Sanders1. 1Gastroenterology, 2Clinical Chemistry, 3Radiology, Royal Hallamshire Hospital, Sheffield, UK
Introduction: Gastrostomy insertion has been demonstrated to be of benefit in selected patients. Percutaneous endoscopic gastrostomy (PEG) using the pull through technique is the most widely used insertion method, but it is recognised to have significant complications particularly in patients with respiratory risk factors. An alternative is a radiologically inserted gastrostomy (RIG). It has been suggested that RIG may be advantageous in patients who are potentially ‘high risk’ from respiratory complications. However there are no large studies comparing PEG against RIG.
Aims & Methods: All patients referred for a gastrostomy are prospectively included in a database along with demographic, biochemical and outcome data. Analysis of gastrostomy insertions over the period February 2004 to February 2007 was performed with reference to method of insertion and outcome at 30 days. Selection for method of insertion is left to the discretion of the referring clinician. Patients were subgrouped into cognitive impairment (n = 5), dysphagic stroke (n = 36), nasopharygeal cancer (n = 175), neurological (n = 116) and other (n = 71).
Results: Over the study period 170 RIGs and 233 PEGs were inserted (mean age 62, 268 males). There were no differences in age between the RIG and PEG group and case mix was comparable except in the nasopharyngeal cancer group (proportionally more RIGs). The RIG 30 day mortality was 26/170 (15.3%) and the PEG 30-day mortality was 25/233 (10.7%) (p = 0.17). One year mortality was 92/170 (54.1%) for RIG and 131/233 (56.7%) for PEG (p = 0.60). Within subgroups the only significant difference in 30-day mortality was in those patients with nasopharyngeal cancer; 14/106 (13.2%) for RIG and 1/69 (1.4%) for PEG (p = 0.005). However, patients referred for RIG were significantly older than those referred for PEG (mean age 59.7 vs 64, p = 0.019) and had a higher prevalence of significant comorbidities (21.1% in the PEG group and 37.7% in the RIG group).
Conclusion: Overall RIG and PEG appear to have similar 30-day mortality rates. In patients with nasopharyngeal cancer there was a higher mortality in those referred for RIG however pre-selection by the referring clinician due to perceived risk of endoscopic insertion may have biased the outcome. A randomised trial comparing both methods in this subgroup is needed.
TWO-YEAR PROSPECTIVE AUDIT OF USE OF LIQUID DIETS AS “BRIDGE” THERAPY FOR ACTIVE CROHN’S DISEASE
T. Demetriou1, C. Gawad2, C. Kok2, A. W. Harris1. 1Gastroenterology, 2Nutrition, Kent and Sussex Hospital, Tunbridge Wells, UK
Introduction: Liquid diets may be used to induce remission as an alternative to corticosteroids in active Crohn’s disease.1–3 In our practice liquid diets, high dose mesalazine or antibiotics may be used as “bridge” therapy to allow thiopurine or methotrexate to work. Steroids are used rarely, if at all. The tolerability of such diets may be a significant limiting factor.
Aims & Methods: To compare the efficacy and tolerability of 28 days’ therapy with either E028 or Modulen IBD in patients with active Crohn’s disease while starting treatment with mercaptopurine or methotrexate. Prospective study of all patients treated with liquid diets between April 2005 and August 2007. E028 was prescribed for the first 8 months of the audit and thereafter Modulen IBD was used. Liquid diets were started following dietetic advice; no other form of nutrition was allowed and patients received weekly dietician input. Clinical response (defined as decrease in stool frequency, pain and lethargy) was assessed in clinic around day 28 (or sooner if liquid diet failed).
Results: E028 was used in 13 patients (10 females; median age 41 (range 21–78) years); 7 (54%) completed 28 days treatment. Modulen IBD was used in 13 patients (9 females; median age 33 (range 16–63) years); 9 (69%) completed 28 days treatment. Clinical response occurred in 6 of 7 patients and in all 9 patients (p>0.05) who completed treatment with E028 or Modulen IBD, respectively. Overall, 15 of 16 patients who completed 28 days treatment with liquid diet achieved clinical response. By contrast, by intention-to-treat analysis, only 6 of 13 (46%) patients treated with E028 & 9 of 13 (69%) patients treated with Modulen IBD achieved a clinical response (p = 0.15; Fisher’s exact test).
Conclusion: In our cohort of well-motivated and supported patients 28 days treatment with liquid diet was completed in only 16 of 23 (65%) patients. Clinical response was achieved in 15 of 23 patients—a similar outcome after treatment with steroids where 35–40% achieve a partial or complete response to 30 days treatment.4 This audit has shown that the use of liquid diet to avoid the use of steroids and to act as a “bridge” to allow the onset of action of thiopurine or methotrexate appears practical and effective.
Acknowledgement: Dr R Loke for allowing us to access data on his patients.
OPTIMAL LEVELS OF PERIOPERATIVE PARENTERAL NUTRITION SUPPORT: A DOUBLE-BLIND RANDOMISED CONTROLLED TRIAL
T. R. Smith, P. Austin, S. Harding, Z. Leach, S. A. Wootton, M. A. Stroud. Institute of Human Nutrition, Southampton University Hospitals NHS Trust, Southampton, UK
Introduction: Optimal levels of energy and protein provision in perioperative patients requiring parenteral nutrition (PN) support are not known. There is considerable debate as to whether PN should be started at rates likely to meet all a patient’s metabolic needs immediately, or whether slower provision during the first few days is safer in terms of metabolic upset and refeeding risks. NICE guidelines (2006) favoured the latter approach, recommending the introduction of PN at 50% of estimated requirements. We have therefore investigated the effect of higher or lower rates of PN provision on biochemical parameters and clinical outcomes.
Aims & Methods: Patients referred for peri-operative PN were randomised to a lower (17.5 non-protein kcal/kg and 20.3 total kcal/kg, 0.12 gN/kg) versus higher (29.9 non-protein kcal/kg and 35.0 total kcal/kg, 0.22 gN/kg) regimen for the first 5 days of their nutrition support, with recording of both biochemical and clinical outcomes. Patients at very high risk of refeeding syndrome were excluded (BMI <16, >20% weight loss, >2 weeks with no nutritional intake).
Results: 60 patients (57% male, mean age 66 years (sd 15)) were recruited to the trial. 28 received the lower and 32 received the higher feeding regimens. Clinical outcome and glucose data are shown in the table. There were no significant differences between groups in the need for insulin infusions or biochemical measures indicative of refeeding syndrome (potassium, magnesium or phosphate). 13% of patients developed worsening oedema during PN support but with no significant difference between the two feeding regimens.
Conclusion: Although our data show clinical outcome trends that appear to favour introduction of PN feeding at lower levels, possibly related to significantly improved glycaemic control, standard deviations were extremely variable in both groups and hence differences in clinical outcomes were not significant. The introduction of nutrition support at lower levels may therefore be unnecessary if patients are not at very high refeeding risk, although a much larger, probably multicentre, trial is needed to confirm this. Our data permit the power calculations needed to plan such a trial.
THE “CUT AND PUSH” METHOD OF PERCUTANEOUS ENDOSCOPIC GASTROSTOMY TUBE REMOVAL IN ADULT PATIENTS
D. Kejariwal, D. Bromley, Y. Miao. Gastroenterology, Ipswich Hospital NHS Trust, Ipswich, UK
Introduction: The standard method of removing percutaneous endoscopic gastrostomy (PEG) tubes is by repeat gastroscopy and retrieval of the PEG bumper by the oral route. Most PEG manufacturers recommend the endoscopic method of removal except in those tubes with balloon or flexible ends designed for removal by external traction. Modern PEG design has made the ‘bumpers’ of the tubes softer and more malleable. We believe that the endoscopic removal method is not always necessary and use a non-endoscopic approach. “Cut and push”, is a simpler and cheaper alternative to endoscopic PEG removal and has been reported in 19911 and 20002 for tubes of 15 Fr or less. This involves cutting the tube at skin level and allowing the internal bumper to pass spontaneously.
Aims & Methods: The files of PEG tube removals by the cut and push method over a 5-year period at Ipswich Hospital were reviewed.
Results: Between February 2002 and May 2007, 80 Fresenius Freka 15Fr tubes were removed by the cut and push method. The age range of patients was 19–98 years (mean of 62, median of 63). The average duration of the tube in-situ before removal was 6.7 months (range 1–28). No reported hospital re-admissions or mortality occurred within 30 days of removal. No reports of minor complications occurred either. The original indications for the PEG tubes that were removed were head and neck malignancy (44), cerebrovascular accident (14), other neurological illness (15) and supplementary feeding (7).
Conclusion: The necessity to endoscopically remove PEG tubes is based on reported complications in a few case reports.3 4 The complications were principally small bowel perforation and obstruction. However these reported complications occurred in either children or those with tube sizes of more than 15 Fr. In our hospital, none of our patients with the “cut and push” method of tube removal suffered any complications. We believe that this provides further evidence that PEG tubes can be safely removed using this method. Elderly and neurologically impaired patients are spared an often-long and tedious journey to the Endoscopy unit as well as the hazards of an endoscopy. The saving in resources, in an already overworked system, by reducing endoscopies is also considerable.
BILE ACID MALABSORPTION: TWO DECADES ON
P. Basumani1, M. J. Smith2, M. Srinivas1, B. F. Dawson2, P. J. A. Willemse1, B. Höeroldt1, B. A. Mason1, C. Royston1, K. D. Bardhan1. 1Gastroenterology, 2Medical Physics, Rotherham General Hospital, Rotherham, UK
Introduction: Chronic diarrhoea, a common problem, often results in protracted negative and frequently repeated investigations and unsatisfactory outcome. While bile acid malabsorption (BAM) as a cause of diarrhoea is well known in specific settings, such as ileal resection, it is now recognised more often in patients with diarrhoea associated with other conditions.
Aims & Methods: We wish to draw attention to the simplicity of BAM diagnosis by the SeHCAT retention test and the benefits this brings. The procedure is simple, non-invasive and measures retention of an isotope-tagged synthetic bile acid (75-Seleno homo-taurocholic acid). BAM was diagnosed when retention was <10% at day-7. 1076 patients with chronic diarrhoea underwent SeHCAT test 1988–2007. Of these, 1028 could be grouped into five broad categories (see table) based on information on the structured referral form. BAM patients who failed treatment with conventional anti-diarrhoeals were treated with bile acid sequestrants (BAS), principally colestipol or cholestyramine. We reviewed the response in a subset of 56 patients treated in 2004.
Results: Treatment response (n = 56; 2004): number treated = 44; 18/25 (72%) D-IBS patients and 11/19 (58%) of the other groups showed good response to therapy with BAS (consistent with previous experience). BAM is commonly encountered in expected conditions such as ileal resection but is also common in post-cholecystectomy diarrhoea. Surprisingly, one third of patients with D-IBS have BAM; this proportion has remained constant over two decades. SeHCAT in our centre is now done among initial investigations in patients with chronic watery diarrhoea but with otherwise good general health, particularly where D-IBS is suspected, a common condition and our largest patient group. The early and definitive diagnosis of BAM by the readily available SeHCAT test frequently concludes investigations speedily; treatment with bile acid sequestrants is often more effective than conventional anti-diarrhoeals.
Conclusion: (1) BAM is common in many diarrhoeal conditions; the largest group is D-IBS. (2) The SeHCAT retention test allows rapid and definitive diagnosis. (3) Treatment with BAS often improves the patient’s quality of life.
MIDGUT NEUROENDOCRINE TUMOURS WITH LIVER METASTASES. RESULTS OF THE UKI NETS SURVEY
A. Ahmed1, G. Turner2, B. King1, L. Jones3, C. Bouvier4, D. McCance2, J. Ardill2, B. Johnston5, M. Rees6, G. Poston3, M. Buxton-Thomas7, M. Caplin4, J. Ramage8. 1Gastroenterology Department, North Hampshire Hospital, Basingstoke, 2Northern Ireland Neuroendocrine Tumour Group, Royal Victoria Hospital, Belfast, 3Department of Surgery, Royal Liverpool University Hospital, Liverpool, 4Neuroendocrine Tumour Unit, Royal Free Hospital, London, 5Neuroendocrine Tumour Unit, Royal Victoria Hospital, Belfast, 6Department of Surgery, North Hampshire Hospital, Basingstoke, 7Department of Nuclear Medicine, 8Institute of Liver Studies, King’s College Hospital, London, UK
Introduction: Midgut neuroendocrine tumours (NET) encompass tumours arising in the jejunum, ileum and proximal colon. Prediction of prognosis and guiding patients about the most appropriate course of action is difficult. This is partly due to the variation in the natural course of the disease but also due to the lack of robust evidence on the many available treatment options
Aims & Methods: We intended to identify the prognostic factors and the effect of interventions on patients with liver metastastic midgut carcinoids across UK and Ireland. Five institutions which are part of UK and Ireland NET group took part in this study. Clinical and biochemical data were collected from hospital charts, pathology reports, radiology reports and biochemistry records for each patient retrospectively, with entries onto a database for each year of each patient under follow-up.
Results: Data was collected on a total of 360 patients. The mean duration of follow-up from diagnosis was 5.29 years. 159 patients died during follow-up. The median survival from time of diagnosis of liver metastases was 5.95 years (SE 0.476). Increasing age at diagnosis, raised urinary HIAA levels, raised plasma Chromogranin A levels, high Ki67 and size of largest liver metastases >4 cm at presentation were identified as factors associated with poor outcome. Resection of liver metastases, Resection of small bowel primary, treatment with Somatostatin analogue therapy and treatment with targetted radiotherapy was associated with improved prognosis. Multivariate analysis using a Cox’s proportional hazards model revealed that age at diagnosis (sig 0.014), Ki67 level (sig 0.039) and resection of primary (sig 0.015) were independent predictors of survival.
Conclusion: This is the largest study to our knowledge specifically looking at the prognosis and clinical course of patients with liver metastatic midgut NETs. For the first time we have shown that Ki67 and resection of primary are independent predictors of survival. In the absence of randomised controlled trials for established therapies this gives evidence that will be useful in the management of these patients.
FIBROBLAST GROWTH FACTOR 19 MAY HAVE A ROLE IN THE PATHOGENESIS OF IDIOPATHIC BILE ACID MALABSORPTION
A. M. Tasleem1, G. W. Brydon2, T. Dew3, S. Balesaria1, C. W. LeRoux4, J. R. F. Walters5. 1Gastroenterology, Imperial College London, London, 2Clinical Biochemistry, Western General Hospital, Edinburgh, 3Clinical Biochemistry, Kings College Hospital, 4Metabolic Medicine, 5Gastroenterology, Imperial College Healthcare, London, UK
Introduction: Idiopathic bile acid malabsorption (IBAM) is an under-recognised syndrome where excess colonic bile acids produce chronic diarrhoea, which responds to sequestrants such as colestyramine. Bile acids are absorbed in the ileum and undergo enterohepatic circulation. Unlike the situation in secondary bile acid malabsorption, evidence suggests that the ileal uptake of bile acids is normal in IBAM. Recently Fibroblast Growth Factor 19 (FGF19), produced by the ileum, has been suggested to have a role in regulating bile acid synthesis.
Aims & Methods: We hypothesised that disordered signalling of FGF19 from the ileum to the liver could be a factor leading to IBAM. FGF19 transcripts in mucosal biopsies of human intestine were investigated in archived samples by quantitative RTPCR. Fasting serum levels of FGF19 and 7α-hydroxy-4-cholesten-3-one (C4), to quantify bile acid synthesis, were measured in 14 patients with chronic diarrhoea, where IBAM had been diagnosed by SeHCAT testing and who had been screened for secondary causes of BAM, and also in 8 controls without diarrhoea, also screened for symptoms of malabsorption. C4 was determined using HPLC and FGF19 by commercial ELISA.
Results: FGF19 mRNA was abundantly expressed in human ileum with wide variation in IBAM patients and in controls, but was undetectable in duodenum. In the IBAM patients, the mean bowel frequency was 3.1 vs 1.6/24 h in controls (p = 0.04, Mann-Whitney U test). The mean C4 was significantly higher in patients than in controls (59.0±9.5 vs 18.1±3.7 ng/ml; p = 0.0006). FGF19 was easily detected in human serum and median fasting values were lower in patients then in controls, with borderline significance (128 vs 222 pg/ml, p = 0.056). FGF19 and C4 showed a significant inverse relation overall (r = −0.415; p = 0.027, Spearman rank).
Conclusion: This is the first study of FGF19 in IBAM. The results obtained indicate that disordered signalling from the ileum to the liver by FGF19 could play a role in the pathogenesis of IBAM.
PRELIMINARY DOUBLE BALLOON ENTEROSCOPY EXPERIENCE FROM A TERTIARY CENTRE IN THE UK
R. Sidhu1, M. E. McAlindon1, D. P. Hurlstone1, M. Thomson2, I. C. Cameron3, S. Hardcastle1, D. S. Sanders1. 1Department of Gastroenterology, Royal Hallamshire Hospital, Sheffield Teaching Hospitals NHS Trust, 2Department of Gastroenterology, Sheffeld Children’s Hospital, 3Department of Surgery, Royal Hallamshire Hospital, Sheffield Teaching Hospitals NHS Trust, Sheffield, UK
Introduction: Double balloon enteroscopy (DBE) is a novel technique that has revolutionised small bowel (SB) examination. This technique has the potential to allow pan-endoscopic visualisation of the SB, with the ability to perform therapeutic intervention. Since its introduction in 2003, the use of DBE has surged internationally. Despite this, there is still no published literature from the UK
Aims & Methods: To assess the diagnostic yield of DBE and impact on patient management in a tertiary UK setting. Data were collected prospectively on all patients referred for DBE over 15 months. Case notes were reviewed for patient demographics and referral indications. All patients had capsule endoscopy (CE) prior to DBE and the route for DBE was based on location of abnormality on CE (that is, capsule reader described findings as proximal or distal small bowel). DBE findings, therapeutic intervention performed and subsequent change in management were noted.
Results: Thirty DBE procedures were performed in 21 patients between July 2006 and October 2007. 66.7% of the referrals originated from outside the region. Sixteen patients had DBE via the oral route and 14 patients had DBE via the anal route. 62% were female with a mean age of 55 years (range 20–77 years). The indications were obscure gastrointestinal bleeding - overt bleeding (n = 6) and iron deficiency anaemia (n = 12), suspected Crohn’s disease (n = 2) and assessment of polyps (n = 1). Four patients were transfusion dependent whilst 19% had significant cardiovascular co-morbidity. The mean procedure time was 70 min (range 2–120) with no reported complications. The overall diagnostic yield was 43%. The diagnoses were angiodysplasia (n = 4/19%), ulcers (n = 4/19%) and tumour (n = 1/4.8%). DBE was normal in 57% and unsuccessful in 4 patients (3 anal route, 1 oral route) due to poor patient tolerance. Intervention was performed in 38% (biopsy 50%, argon plasma coagulation 50%) with a subsequent change in management in 33% of patients. The diagnostic yield was not significantly different when comparing referral indications (p = 1) or whether referred from outside the region (p = 0.4).
Conclusion: Our preliminary experience from the UK has shown that DBE is a useful modality for diagnostic and therapeutic intervention in patients with suspected small bowel pathology. DBE is feasible within the UK setting, with a high diagnostic yield, low complication rate and a positive impact on patient management. Larger studies are required particularly in high-risk patient groups before advocating its use in routine clinical practice.
WHAT ARE THE IMPLICATIONS OF NEWLY IDENTIFIED COELIAC DISEASE IN PATIENTS WITH TYPE 1 DIABETES MELLITUS? EFFECT UPON GLYCAEMIC CONTROL, QUALITY OF LIFE, CARDIAC RISK FACTORS AND PERIPHERAL NERVE FUNCTION
J. S. Leeds1, A. D. Hopper1, M. Hadjivassiliou2, S. Tesfaye3, D. S. Sanders1. 1Gastroenterology, 2Neurology, 3Diabetes, Royal Hallamshire Hospital, Sheffield, UK
Introduction: Previous work from our group has shown that the prevalence of coeliac disease (CD) in Type 1 diabetes mellitus is 33/1000 (3.3%). Those with newly identified CD had worse glycaemic control compared to age, sex-matched controls but similar quality of life scores. CD has also been associated with peripheral neuropathy but there are no data examining peripheral nerve function in patients with both CD and Type 1 diabetes mellitus. The effect of a gluten-free diet (GFD) on glycaemic control, quality of life, cardiac risk factors and peripheral nerve function are unknown.
Aims & Methods: From the initial 1000 patient cohort 4 specific groups were identified and studied; Group 1 Type 1 diabetes and new CD (n = 12), Group 2 Type 1 diabetes and established CD (n = 12), Group 3 Type 1 diabetes alone (n = 20), Group 4 Type 1 diabetes with positive coeliac antibodies but normal duodenal biopsy (n = 17). Patients with CD alone were recruited to comprise group 5 (n = 15). HbA1c was used to assess glycaemic control and SF-36v2 was used to assess quality of life. Peripheral nerve function was assessed by nerve conduction velocities in the right radial, sural, tibial and common peroneal nerves. Cold, vibration and heat-pain detection threshold was determined using the CASE IV machine and cardiac autonomic function was assessed using the O’Brien protocol.
Results: There were no differences in age, gender distribution or body mass index between the groups. In group 1 median HbA1c was 8.2% prior to starting a GFD and 8.6% after 1 year (p = 0.45) and SF-36v2 scores did not change significantly. There were no changes in total cholesterol or triglyceride levels but cholesterol: HDL ratio increased from 3.7 to 3.2 (p = 0.033). On cardiac autonomic testing, mean resting heart rate was significantly lower in group 5 vs the other groups (65.5 vs 75.5, p = 0.028) but mean systolic and diastolic blood pressures were comparable. Radial and common peroneal nerve conduction velocities were significantly reduced in group 1 and 2 compared to the other groups (p = 0.007 and p = 0.0001 respectively). However, there were no differences in cold, vibration and heat-pain detection thresholds between the groups.
Conclusion: Following identification of CD in Type 1 diabetes and subsequent treatment with a GFD glycaemic control and quality of life are not altered however there appears to be improvement in HDL cholesterol levels. Resting heart rate was lower in non-diabetic coeliac patients but blood pressure was similar. Patients with Type 1 diabetes and CD have a higher prevalence of peripheral nerve dysfunction compared to controls.
CHANGES IN LIPID PROFILE WITH EXPOSURE TO A GLUTEN-FREE DIET IN INCIDENT CASES OF COELIAC DISEASE: A PROSPECTIVE COHORT STUDY
N. R. Lewis1, D. S. Sanders2, R. B. Hubbard1, R. F. A. Logan1, J. West1. 1Division of Epidemiology and Public Health, University of Nottingham, Nottingham, 2Gastroenterology and Liver Unit, Royal Hallamshire Hospital, Sheffield, UK
Introduction: Undetected coeliac disease is associated with 0.5 mmol/l reduction in mean serum cholesterol in comparison to the general population.1 A review of incident coeliac disease patients that had happened to have their lipid profile measured observed a significant increase in total cholesterol and HDL cholesterol with exposure to a gluten-free diet.2 Since each 0.03 mmol/l increase in HDL cholesterol is associated with a 2–3% reduced risk of future coronary heart disease,3 we prospectively observed the effect of a gluten-free diet on the lipid profile of a contemporary cohort of incident coeliac disease patients.
Aims & Methods: Lipid profile has been prospectively collected on incident cases of coeliac disease starting a gluten-free diet at the Royal Hallamshire Hospital since October 2004, at diagnosis and followed up for 12 months (n = 51). We compared measures at diagnosis and 12 months after using paired t tests
Results: There were twice as many female as male incident cases but the mean age at diagnosis was 47 years (SD 15) and similar between men and women (p = 0.45). 28% had partial villous atrophy; 40% had subtotal villous atrophy and 23% had total villous atrophy. The median tTG at diagnosis was 223 IU (range 5–300) and 90% (n = 80) were EMA positive. The mean value of HDL cholesterol and total cholesterol: HDL significantly increased with exposure to a gluten-free diet (table) as did folate. These changes did not vary by gender or by age. However, on stratifying according to severity of disease as measured by tTG titre and Marsh grading, HDL cholesterol and total cholesterol: HDL only significantly increased in those people with more severe coeliac disease.
Conclusion: Our data confirm HDL-cholesterol increases in people with celiac disease after starting a gluten-free diet. Improved intestinal absorption or some other reason may be responsible. We conclude that gluten-free diet treatment does not have an adverse effect on lipid profile and may be beneficial with regard to risk of coronary artery disease.
Joint IBD/paediatric/nutrition symposium
SINGLE-CENTRE EXPERIENCE OF EXCLUSIVE ENTERAL NUTRITION FOR INDUCTION OF REMISSION IN MORE THAN 100 CHILDREN WITH CROHN’S DISEASE
R. K. Russell, E. Buchanan, T. Cardigan, K. Hassan, D. Young, P. McGrogan. Paediatric Gastroenterology, Yorkhill Hospital, Glasgow, UK
Introduction: Enteral nutrition achieves remission rates between 20–84% in Crohn’s disease (CD) patients. We describe our experience of treating CD with a primary course of enteral nutrition and factors effecting treatment outcome.
Aims & Methods: Patients treated with enteral feeds over the past 3 years were studied. CD was diagnosed by standard criteria. Standard treatment was 8 weeks of exclusive enteral nutrition. Disease remission was assigned by a combination of clinical parameters (patient well being, weight gain, stool frequency and inflammatory markers). Disease phenotype was assigned using the Vienna classification and a paediatric classification that examined disease activity throughout the GI tract. Inflammatory markers were assessed at treatment start and end. Anthropometry (z scores) were calculated on starting treatment and at 2, 3 and 6 months later.
Results: 114 children were treated (4 were excluded from further analysis). There were 65 males (59%), median age at diagnosis 11.6 years (IQR 9.5–13.0) and median age at treatment of 12.1 (IQR 9.8–13.5). 57 (52%) took feeds orally, 48 (44%) via n-g tube and 4 (4%) via a PEG. Median length of treatment was 55.5 days (IQR 49.0–58.0) with 83 (75%) completing at least 7 weeks of treatment. Modulen IBD (Nestle) was used in 105 and EO28 (SHS) in 5. Median energy delivered was 107% of EAR (105–108) and protein 212% (IQR 204–220). Clinical remission was achieved in 88 (80%). In patients in clinical remission there was a significant reduction in both the median ESR and CRP at the start and end of treatment (38 vs 13 and 21 vs 6, respectively p<0.0001 for both). Patients in clinical remission gained a significant amount of weight (median weight gain 4 kg, p = 0.009 95% CI 1 to 7) reflected in a significant improvement in weight z score at the start and end of treatment (−0.93 vs 0.35, p<0.0001) but not in height z-score (p = 0.32). Unifactorial analysis examining sex, age, method of feeding, disease location and disease behaviour did not demonstrate any significant difference in patients achieving clinical remission. There were 19% of patients who had isolated colonic disease. The clinical remission rate in patients with isolated colonic disease was no different compared to other disease locations (79% vs 84%, p = 0.56). This was reflected in a significant drop in ESR in these patients at the start and end of treatment (46 vs 16 p = 0.001).
Conclusion: This large study demonstrates enteral nutrition is well tolerated and results in clinical remission, normalisation of inflammatory markers together with significant improvement in weight/BMI z-score in most patients. Importantly this study demonstrates clinical remission is not influenced by CD location suggesting enteral nutrition should be offered to all patients regardless of disease phenotype at diagnosis.
Gastroduodenal free papers
INFLUENCE OF ASPIRIN AND NON-STEROIDAL ANTI-INFLAMMATORY DRUG USE ON THE OUTCOMES OF BLEEDING PEPTIC ULCERS: 10-YEAR EXPERIENCE OF A SPECIALISED BLEEDING UNIT
U. Basavaraju, J. M. Thomson, D. Armour, N. A. G. Mowat, A. Fraser. Gastroenterology, Aberdeen Royal Infirmary, Aberdeen, UK
Introduction: The use of Aspirin, non-steroidal anti-inflammatory drug use (NSAID) and Warfarin has steadily increased over the past decade. Their use is amongst the main contributors to peptic ulcer bleeding requiring hospital admission. Since its inception in 1991, the Gastrointestinal Bleeding Unit (GIBU) has accepted all suspected bleeding admissions from a stable population of 485 600. We previously reported that while taking warfarin is associated with an increased incidence of having a significant bleed, an ulcer with stigmata of recent haemorrhage (SRH) and need for endotherapy, there is no statistically significant difference in the rebleeding, surgery or mortality rates. Here we analyse the effects of Aspirin and NSAID use on the outcomes of peptic ulcer bleeding.
Aims & Methods: From October 1991–2001, data were prospectively collected for all admissions with peptic ulcer bleeding to the GIBU. Patients were assigned to 4 groups: the “Aspirin” group were taking Aspirin alone; the “NSAID” group were taking NSAID alone; the “Combined” group were taking both Aspirin and NSAID; the “Control” group were taking neither drug. Statistical analysis with χ2 test was used and p value of <0.05 was considered significant.
Results: There were 1978 admissions with peptic ulcer bleeding, of whom 476 (24%) were on Aspirin alone, 336 (17%) were on NSAID alone, 137 (6.9%) on both Aspirin and NSAID and 1018 (51%) were taking neither drug. The use of these drugs has steadily increased over the 10 year period. Significant bleeding (Hb<10 g/dl, haemodynamic compromise) was more common in both the Aspirin (65%) and NSAID (69%) groups compared to 61% in the control group, but only statistically significant in the NSAID group (p<0.05). 73% in Aspirin and 74% in NSAID group required blood transfusion to maintain Hb>10 g/dl compared with 59% in Control group (p<0.001 for both). Use of these drugs made these patients more likely to have SRH at endoscopy (Aspirin 46% (p = 0.04), NSAID 50% (p = 0.002), Control 41%). Endotherapy rates were higher in the Aspirin (29%) (p<0.02) and NSAID groups (23.2%) (p = NS) compared to the Control group (22.9%).The rebleeding rate was significantly higher in Aspirin (19%) (p<0.02) and NSAID (20%) (p<0.01) groups than in the Control group (14%). Surgery rates were not significantly different among these groups. The 30-day mortality was 6.5% in the Aspirin group (p = NS), 8.9% (p<0.05) in the NSAID group and 13% (p<0.01) in the Combined group compared to 6% in the Control group.
Conclusion: Patients taking Aspirin or NSAID prior to admission with peptic ulcer bleeding were more likely to have a significant bleed, require blood transfusion and have SRH at endoscopy. Although these patients were no more likely to require surgery, they had an increased mortality suggesting that deaths were as a result of comorbid disease rather than bleeding.
THE EFFECT OF NATURAL POLYMORPHISMS UPSTREAM OF THE HELICOBACTER PYLORI VACUOLATING CYTOTOXIN GENE, VACA, ON VACA TRANSCRIPTION LEVELS
C. G. Masters, D. P. Letley, N. C. Doherty, J. C. Atherton. Wolfson Digestive Diseases Centre and Institute of Infections Immunity and Inflammation, University of Nottingham, Nottingham, UK
Introduction: The vacuolating cytotoxin is an important H pylori virulence factor, and different strains produce different amounts. This is due mainly to differences in vacA transcription. A vacA promoter and a transcriptional start point (TSP) have been identified between the upstream housekeeping gene, cysteinyl-tRNA synthase (cysS) and the vacuolating cytotoxin gene, vacA. Sequence analysis revealed that −35 (TTTATG) and −10 (TAAAAA) motifs are well conserved. Mutations made in this region by Forsyth et al (1999)1 resulted in a decrease in vacA transcription in vitro. In 2004 Ayala et al identified an inverted repeat upstream of the −35 motif present in strains transcribing high levels of vacA.2
Aims & Methods: Biopsies were taken from 30 patients attending for endoscopy in Nottingham. H pylori strains were isolated then grown in broth culture. RNA was extracted both from broth cultures and directly from biopsy specimens, vacA transcription levels were analysed by real-time PCR. The cysS-vacA intergenic region was sequenced for each strain, and natural polymorphisms correlated with vacA transcription in vitro and in vivo.
Results: Analysis of the cysS-vacA intergenic region revealed that differences between strains in the −35 and −10 regions were not significantly associated with levels of vacA transcription, and that regions within the promoter associated with differences in vacA production between strains differed in vitro and in vivo. Sequence alignment revealed that strains with a fully palindromic inverted repeat upstream of the −35 motif expressed more vacA than other strains in vitro (p = 0.01). Analysis of vacA transcription from the same strains in vivo revealed that strains with an A within the second stem of a different stem loop near the transcriptional start site expressed more vacA than those with a G at this position (p = 0.006).
Conclusion: Naturally occurring polymorphisms in two stem loops upstream of vacA are associated with differences in vacA transcription level. Mechanisms remain to be determined: effects on regulator binding or mRNA stability are possible. Different and opposing effects in vitro and in vivo imply in vivo regulation of vacA transcription. Differences in toxin production between H pylori strains could help explain why only some infections result in disease.
GHRELIN INCREASES NUCLEAR FACTOR-KAPPA B EXPRESSION IN A HUMAN LYMPHOCYTE CELL LINE
E. Z. H. Sung1, N. F. da Silva1, S. J. Goodyear1, R. Prajapati1, P. J. McTernan2, C. U. Nwokolo1. 1Gastroenterology, University Hospital Coventry, 2Unit for Diabetes and Metabolism, Warwick Medical School, Coventry, UK
Introduction: Ghrelin is a 28 amino acid orexigenic peptide produced predominantly by the stomach. Interest has increased in its other putative roles including immune-modulation. There is some evidence that ghrelin can affect the release of cytokines from primary lymphocytes and monocytes. The aim of this study was to assess the effects of octanoyl-ghrelin on the p65 subunit of nuclear factor-kappa B (NFκB) (a nuclear transcription factor involved in cellular inflammatory response) in a human B-lymphocyte cell line.
Aims & Methods: A B-lymphocyte cell line (WILCL) was cultured in RPMI 1640 media enriched with L-glutamine, fetal bovine serum and penicillin/streptomycin. Expression of ghrelin receptors (GHSR 1A and 1B) was confirmed by western blotting. The cells were incubated in an atmosphere of 5% CO2 at 37°C and cell density was maintained between 1–3×106 cells/ml. Cells were then transferred to smaller flasks maintaining a density of 1×106 cells/ml. There were 4 starting cell groups which were treated with either control solution or 3 concentrations of octanoyl ghrelin (1 nM, 10 nM and 100 nM). Cell aliquots from each group were cultured for 6, 24 and 48 hours with or without phyto-haemagglutinin (PHA). The cells were then washed in PBS, protein extracted and NFKB activity and concentration estimated using the Trans Am NFKB activity assay. Experiments were done in triplicate.
Results: After 6 hours of culture, for PHA treated (activated) cells mean (±SEM) NFKB activity for control cells was 0.31±0.083, and was increased to 0.35±0.102, 0.43±0.133, 0.32±0.062 for 1 nM, 10 nM and 100 nM ghrelin concentrations respectively. After 6 hours of culture, for non-PHA activated (resting) cells a similar trend was observed with mean (±SEM) NFKB activity for control cells of 0.3±0.044 and 0.3±0.055, 0.37±0.121, 0.32±0.063 for 1 nM, 10 nM and 100 nM ghrelin concentrations respectively. Octanoyl ghrelin was associated with a stepwise increase in NFKB activity at 1 nM and 10 nM concentration in activated cells but NFKB expression at 100 nM concentration of ghrelin was less than at 10 nM concentration. In all experiments PHA activated cells express more NFKB than resting cells.
Conclusion: Octanoyl-ghrelin seems to up regulate NFKB activity in the WILCL B lymphocyte cell line which expresses the ghrelin receptor. This should lead to the transcription of various cytokines involved in inflammatory responses. Our observation is contrary to the data from some recent studies which suggest an immune-inhibitory role for ghrelin. The reason for the tailing-off of the ghrelin effect at 100 nM concentration is uncertain.
GASTRIC CANCER CELL MIGRATION IS REDUCED BY NOVEL MIGRASTATIN ANALOGUES
G. Horgan1, D. Murray2, A. Madden2, G. Bennett2, G. Anquetin3, P. Murphy3, J. Lennon1, P. MacMathuna1, P. Doran2. 1Gastrointestinal Unit, Mater Misericordiae University Hospital, 2UCD School of Medicine and Medical Sciences, UCD/Mater Clinical Research Centre, Mater Misericordiae University Hospital, 3UCD Centre for Synthesis and Chemical Biology, Belfield, Dublin, Ireland
Introduction: Gastric cancer (GC) aetiology is unclear, its prognosis is poor and effective chemotherapy regimes have yet to be developed. We have previously reported NET1 to be increased in GC, whereby it facilitates cell migration and invasion via RhoA activation and subsequent cytoskeletal re-arrangements. Migrastatin analogues (MA) have been shown to reduce tumour cell migration and metastasis in a range of malignancies but have yet to be investigated in GC.
Aims & Methods: In this study we assessed the effect of seven novel MAs on: (A) GC cell proliferation and migration and (B) NET1 mRNA expression and cytoskeletal re-arrangements. GC cells were treated with varying doses of the seven novel MAs. Cell proliferation was assessed using an MTS assay. GC cell migration was investigated using a fluorescent trans-well assay and also using a scratch “wound-healing” assay. NET1 mRNA expression was quantitated using real-time PCR. F-actin assembly was assessed by immuno-fluorescently staining.
Results: 5 of the 7 compounds caused reduced tumour cell migration as assessed using the transwell assay over 24 h (p<0.001). The IC50 migration values for these compounds for were; Compound A; 17 uM, Compound B; 29 uM, Compound D; 32 nM, Compound F; 1 uM, Compound G; 2 uM. 5 of the compounds caused reduced tumour cell migration as assessed using the scratch “wound-healing” assay. (p<0.05). Treatment with Compound E resulted in 65% decreased NET1. No changes in cytoskeletal architecture were observed upon treatment with the compounds. No significant effect on GC cell proliferation was observed upon treatment with the compounds.
Conclusion: We have demonstrated for the first time that novel MAs significantly inhibit GC migration while exhibiting no cytotoxic effects. Furthermore, the reduced NET1 expression upon treatment with Compound E is promising and worthy of further study. Ongoing studies into the underlying mechanism of these compounds may very well establish them as ideal therapeutic agents in GC.
ASSESSMENT AND OUTCOMES IN GASTRIC CARCINOID
L. Marelli1, C. Toumpanakis1, R. Srirajaskanthan1, T. Eves1, J. Watkins2, M. Caplin1. 1Centre for Gastroenterology, 2Department of Histopatology, RFH, London, UK
Introduction: Gastric carcinoid tumours are rare, but increasing in number.1 There are three types: Type I associated with autoimmune atrophic gastritis and hypergastrinemia, which are indolent in nature; Type II associated with multiple endocrine neoplasia (MEN I) and sporadic Type III with poor prognosis.
Aims & Methods: To evaluate clinical, biochemical, endoscopic and histological features of patients with gastric carcinoid. 37 consecutive patients with gastric carcinoid (mean age: 58±13 years; M/F: 23/14) were referred to our Unit between 1998 and October 2007. 31 patients with type I (84%), 3 with type II (8%) and 3 with type III (8%). Data collected retrospectively in 31 patients (n/a in 6 patients with type I).
Results: Median follow-up was 52 months (1–200). 3 patients, all with type III, died for metastatic carcinoid. Symptoms at presentation were: anaemia (55%), dyspepsia (23%), abdominal pain (16%) and GI bleeding (6%). In type I: chromogranin A (CgA) was normal in 65%, increased <×2 normal in 26% and >×2 normal in 9%; all patients had high gastrin (>400 pg/ml in 61%); antiparietal cell antibody positive in 63%. At endoscopy, there was gastritis only in 13%, <3 polyps in 50% and multiple small polyps in 37%. Size of largest polyp (n = 15) was <1 cm in 11, 1–2 cm in 3 and >2 cm in 1. At histology, 20% were micro-carcinoid and 80% low grade carcinoid; MIB-1 proliferation index (n = 18) was <2% in 13, 3–5% in 4 and 5–10% in 1. 79% had atrophic gastritis. EUS (n = 11) showed no infiltration beyond the muscolaris mucosae. OctreoScan (n = 10) showed abnormal uptake only in 1 patient with liver metastases. 2 patients had partial gastrectomy (lymph node involvement in 1 with 25 mm polyp), 3 mucosectomy and 1 polypectomy. In type II: both CgA and gastrin were increased; 2 patients had low grade (MIB-1<2%) and 1 had high grade (40–70%) carcinoid. In type III: gastrin was normal, no atrophic gastritis, all high grade (MIB-1: 35–60%) carcinoid and all developed metastases. One patient died for post-embolisation complication, 1 had total gastrectomy, chemotherapy and died after 19 months and 1 had liver transplant but died of disease recurrence 3 years later.
Conclusion: Management of patient with gastric carcinoid is based on careful identification of tumour type—endoscopy with biopsy (MIB-1), CgA, gastrin, CT scan, OctreoScan, EUS. Type I have good prognosis (at 5 years all patients were alive and only 1 of 31 patients had metastases); polyp >2 cm may be more aggressive. Type II are similar to type I, management depends on the associated MEN1. Type III are more aggressive—in our series, mean survival time was 29 months despite treatment.
Pancreatic section meeting
AZATHIOPRINE IN THE MANAGEMENT OF RELAPSING AUTOIMMUNE PANCREATITIS/IGG4 SCLEROSING CHOLANGITIS
N. S. Sandanayake, G. J. Johnson, C. M. Smyth, N. I. Church, L. Ayaru, M. H. Chapman, A. R. Hatfield, S. P. Pereira, G. J. Webster. Gastroenterology, University College London Hospital, London, UK
Introduction: A rapid clinical, biochemical and radiological response to steroids is a diagnostic feature of autoimmune pancreatitis/IgG4 sclerosing cholangitis (AIP/SC). However, disease relapse may occur, and its clinical importance and management has not been well defined. The use of maintenance immunosuppression, including Azathioprine (AZA), has not been reported in a case series of AIP/SC.
Aims & Methods: Aim of the study was to report our experience of disease relapse and its management in patients diagnosed with AIP/SC between 2004–7, following an initial course of steroids. Disease activity was assessed prospectively on clinical, biochemical, serologic and radiological criteria. Patients with post-steroid relapse, or failed remission, were the focus of this study.
Results: Of 26 AIP/SC patients followed for a median 24 months (range 2–46) from start of initial steroid course, relapse/failed remission occurred in 11 (42%). All were male, median 55 years (range 27–81). Two patient groups were defined: (1) Post-steroid relapse: 7/11 (64%) patients relapsed after initial steroid course, a median 3 months (range 1–7) after stopping steroids, following achieved remission. Indicators of relapse included jaundice and new/worsening hilar +/− intrahepatic biliary stricturing in all patients, and renal failure in one patient with renal IgG4-positive plasma cell infiltrates. Serum IgG4 was elevated in 3/7 patients, with a mean level of 2.31 (normal 0–0.3). All 7 patients received a second tapering course of 30 mg prednisolone daily, while 5/7 patients commenced AZA 2 mg/kg/day. Objective evidence of disease control was seen in all patients, including resolution of jaundice and removal of biliary stents following improvement of strictures. Of the 5 patients maintained on AZA, 3 remained in remission 3, 14 and 19 months after stopping steroids respectively, and the rest were clinically improved on a tapering steroid regimen. 1 patient needed dose reduction of AZA due to persistent nausea. (2) Failed weaning: 4/11 patients responded to initial steroid course, but failed steroid weaning and cessation, at a median 10 months (range 3–22). 3/4 patients commenced AZA 2 mg/kg/day (one declined AZA) with subsequent cessation of steroids in 2/3, and slow weaning of steroids in the remaining patient on AZA.
Conclusion: More than 40% of patients with AIP/SC fail to achieve stable remission after initial short-course steroids, with progression of intrahepatic biliary stricturing commonly seen. Elevated serum IgG/IgG4 titres may predict relapse. Maintenance therapy with AZA, as used in autoimmune hepatitis, appears to be effective, and merits further study.
Colorectal/anorectal free papers
COULD SURVEILLANCE PROTOCOLS BE ALTERED DUE TO LOW YIELD OF SIGNIFICANT COLORECTAL NEOPLASIA IN A HIGH RISK COHORT? INITIAL FIVE YEARS EXPERIENCE OF A COLLABORATIVE HIGH RISK FAMILIAL CANCER SCREENING INITIATIVE IN IRELAND
G. Horgan1, G. Lawlor1, L. O’Brien1, J. Leyden1, N. Ullah1, V. Sibartie1, M. O’Riordain2, G. O’ Sullivan2, J. Lennon1, P. MacMathuna1. 1Gastrointestinal Unit, Mater Misericordiae University Hospital, Dublin, 2Department of Surgery, Mercy University Hospital, Cork, Ireland
Introduction: Identifying and removing significant polyps is the rationale underlying both an average and high risk colorectal cancer screening strategy. However significant variation has been observed in polyp yield which may question current surveillance intervals.
Aims & Methods: To critically evaluate advanced neoplasia yield from a cohort of high risk asymptomatic individuals identified at two dedicated family cancer clinics in Dublin and Cork. In 637 individuals undergoing screening colonoscopy, we analysed the polyp characteristics according to number and pathology subset in relation to age (<50, >50) and risk stratification (medium risk n = 487 and HNPCC n = 103). Colonoscopy results in 47 low (but above average) risk were also included. Fisher’s exact two-tailed t test was used for statistical analysis.
Results: Tubular adenoma rates were statistically significant between individuals aged <50 compared to those aged >50 in: (a) low risk cohort (5.6% vs 37.9%; p<0.02) and (b) all risk groups combined (16.4% vs 24%; p<0.02). Tubulovillous adenoma yields were statistically significant between individuals aged <50 compared to those aged >50 in: (a) medium risk cohort (1.6% vs 6.2% p<0.01); (b) HNPCC cohort (0% vs 9.5% p<0.03) and (c) all risk groups combined (1.2% vs 6.7% p<0.03).
Conclusion: Advanced neoplasia in all at risk groups less than 50 years of age is low. Our results raise the possibility to delay initiation of screening in low and medium risk groups until the age of 50. It is worth considering delaying initiation of screening of HNPCC until the 5th decade and widening the screening intervals below the age of 50 as currently recommended.
STROMAL CELL CYCLOOXYGENASE-2 PROMOTES COLORECTAL TUMORIGENESIS IN THE APCMIN/+ MOUSE MODEL OF FAMILIAL ADENOMATOUS POLYPOSIS
M. A. Hull1, D. J. Scott1, R. J. Cuthbert1, S. Ko1, S. L. Perry1, E. Cartwright1, C. Bonifer2, A. F. Markham1, L. Coletta1. 1Section of Molecular Gastroenterology, 2Section of Experimental Haematology, Leeds Institute of Molecular Medicine, Leeds, UK
Introduction: Cyclooxygenase-2 (Cox-2) plays an important role in the early stages of intestinal tumorigenesis. However, the mechanism(s) underlying the pro-tumorigenic activity of Cox-2 remains unclear. In human and ApcMin/+ mouse intestinal adenomas, Cox-2 is localised predominantly to stromal macrophages. We have previously demonstrated that paracrine macrophage Cox-2 activity drives tumorigenic behaviour of intestinal epithelial cells in vitro. Therefore, we tested the hypothesis that stromal cell Cox-2 promotes intestinal tumorigenesis in vivo using a transgenic mouse model of macrophage-specific Cox-2 over-expression.
Aims & Methods: A complete mouse genomic Cox-2 clone was expressed under the control of the chicken lysozyme (cLys) locus, which directs macrophage-specific transgene expression in mice. Transgenic C57Bl/6 (B6) x 129Sv cLys-Cox-2 founders were generated by pro-nuclear injection and one line (termed GC25) chosen for further experiments based on Southern blot analysis and transgene expression studies in bone marrow-derived macrophages. cLys-Cox-2 mice underwent a N6 backcross to the B6 background before crossing with B6 ApcMin/+ mice. Intestinal phenotype analysis was performed in a blinded manner at day 100.
Results: As expected, cLys-Cox-2 ApcMin/+ mice exhibited increased Cox-2 expression in the brain, spleen and intestine compared with non-transgenic ApcMin/+ mice. There was elevated macrophage-specific Cox-2 expression in adenomas and histologically normal (HN) intestinal mucosa, along with increased intestinal tissue prostaglandin (PG) E2 levels (9.1±1.0 ng/mg total protein vs 6.2±1.1 ng/mg for HN colon), in cLys-Cox-2 ApcMin/+ mice compared with non-transgenic ApcMin/+ animals. There was a significant increase in colorectal adenoma multiplicity in cLys-Cox-2 ApcMin/+ mice (n = 12; median 5, IQR 2–11) compared with ApcMin/+ controls (n = 11; 3, 1–6; p = 0.03, Mann-Whitney). There was also a significant increase in tumour size in cLys-Cox-2 ApcMin/+ animals (p = 0.03 for the difference in number of polyps of 4.1–6 mm diameter; Student’s t test). However, there was no significant difference in small intestinal tumour number between cLys-Cox-2 ApcMin/+ mice and non-transgenic controls.
Conclusion: This is the first demonstration that mucosal Cox-2 activity (as opposed to models of exogenous PGE2 administration or Cox-2 inhibition/deletion) drives ApcMin/+ mouse intestinal tumorigenesis. Macrophage Cox-2 activity increases adenoma multiplicity and size in the colon, but not the small intestine. The cLys-Cox-2 mouse model will be useful for future studies of paracrine mucosal Cox-2 signalling as a specific target for colorectal cancer chemoprevention.
ABERRANT CRYPT FOCI FORMATION IS INHIBITED BY PEROXISOME PROLIFERATOR-ACTIVATED RECEPTOR/ALPHA IN APCMIN+/- MICE
A. Shonde1, N. Mandir2, D. Bell3, R. Goodlad2, A. Bennett4, C. Hawkey1. 1WDDC, University Hospital Notingham, Nottingham, 2Histopathology Unit, London Research Institute, Cancer Research, London, 3Biology, 4Biological Sciences, University of Nottingham, Nottingham, UK
Introduction: We have reported that ligand activation of peroxisome proliferator activated receptor (PPAR)-α reduces tumour burden in APCmin+/- mice while deletion of PPAR-α increases formation of colonic tumours.1 We investigated whether aberrant crypt foci (ACF) which are thought to be precursors of sporadic colorectal cancer, played a role in this process.
Aims & Methods: Our initial aim was to investigate ACF formation in APCmin+/- and APCmin+/- PPAR-α-/- mice. Once weaned C57BL/6J APCmin+/- mice (n = 20) and C57BL/6J APCmin+/- PPAR-α-/- mice (n = 20) were fed standard chow (rat and mouse standard diet, BEEKAY, Humberside) throughout the study. These mice were sacrificed when they showed signs of anaemia or lost >20% of weight (term). To investigate ACF formation over time five mice from each genotype were sacrificed at weeks 12, 18, 24 and term. The colons were opened and laid out before being soaked in 0.2% methylene blue. ACF were then analysed using a dissecting microscope.
Results: Tumours developed sooner in APCmin+/- PPAR-α-/- mice (from 12 weeks) than in APCmin+/- mice (from 18 weeks). ACFs were seen in APCmin+/- PPAR-α-/- mice from 12 weeks but never in APCmin/+ mice. Among mice sacrificed because of anaemia or weight loss there was an increase in both ACFs and colonic tumours in APCmin+/- PPAR-α-/- mice. There were no ACF in APCmin+/- mice at term, while in APCmin+/- PPAR-α-/- the mean number of ACF was 1.95 (SEM 0.16) in the mice sacrificed at term. The mean number of large bowel polyps in APCmin+/- mice at term was 0.75 (0.25) and 2.43 (0.30) in APCmin+/- PPAR-α-/-. There were no ACF found in APCmin+/- mice sacrificed at week 12, 18 and 24. However, the mean number of ACF at week 12, 18 and 24 in APCmin+/- PPAR-α-/- was 0.80 (0.36), 0.80 (0.2), 1.80 (0.37) respectively.
Conclusion: Tumours in APCmin+/- mice may not develop from ACF but these appear to be the source of the additional polyps that develop as a result of PPAR-α deletion. PPAR-α may be a key target for chemo prevention of sporadic polyps and cancers.
WITHDRAWN
INCIDENCE OF PERFORATED COLONIC DIVERTICULAR DISEASE AND ITS ASSOCIATED MORTALITY: A UK GENERAL POPULATION BASED STUDY
D. J. Humes1, M. Solaymani-Dodaran2, K. Fleming2, J. Simpson1, R. C. Spiller1, J. West2. 1Wolfson Digestive Disease Centre, Nottingham University Hospital NHS Trust, 2Division of Epidemiology and Public Health, The University of Nottingham, Nottingham, UK
Introduction: Perforated colonic diverticular disease (PCDD) represents one of the most serious complications of diverticular disease and is thought to be associated with high levels of mortality. However, little is known regarding the occurrence and consequence of the disease. We aimed to determine the incidence and mortality associated with PCDD in the UK.
Aims & Methods: Computerised general practice records from the General Practice Research Database were analysed. The patients were registered in the database from 1987 to 2006. Each case was matched to 10 age, sex and practice matched controls. The outcomes measured were incidence and mortality rates by calendar period, age group and gender using Poisson and Cox regression modelling to provide adjusted estimates.
Results: We identified 894 incident cases between 1990 and 2005. The overall incidence of PCDD was 2.49 (95% CI 2.33 to 2.66) per 100 000 person years, and this was highest in older age groups (>85 years 12.27 per 100 000 person years 95% CI 9.88 to 15.23). The incidence rates increased 2.17-fold (95% CI 1.70 to 2.77) when corrected for age and gender between 1990 and 2005 (Graph 1). A total of 312 (34.90%) PCDD patients died compared to 1822 (20.41%) controls. The crude mortality rates for the PCDD and control cohorts were 90.29 (95% CI 80.53 to 101.25) and 46.06 (95% CI 44.00 to 48.23) per 1000 person years. Over the time period of the study PCDD patients were twice as likely to die compared to the general population when corrected for age and sex (HR 2.22 95% CI 1.96 to 2.51).
Conclusion: We found that the incidence of PCDD has increased twofold during the 15 years of our study. Those at older age are more at risk and the mortality associated with the condition is high. There is a high early mortality following PCDD how much of this relates to the perforation or to concomitant disease remains to be determined. With the ageing demographic in the UK we would expect this condition to be a large future burden on health services.
ONCOLOGICAL MEDIUM TERM OUTCOME OF LOCAL ENDOLUMINAL RESECTION OF LOW RISK PTIM/T1 RECTAL CANCER: CAN WE CHANGE THE MANAGEMENT PARADIGM?
D. P. Hurlstone1, S. R. Brown2, S. Amin2, I. Adam2, A. J. Shorthouse2, P. Skinner2, L. Hunt2, W. Baraza3, S. S. Cross3, N. Tiffin2. 1Endoscopy, Royal Hallamshire Hospital, 2Colorectal MDT Working Group, STH NHS Foundation Trust, 3Colorectal MDT Working Group, Royal Hallamshire Hospital, Sheffield, UK
Introduction: Local excision of early rectal cancer is controversial, despite the non-inclusion of locally draining lymph nodes. Limited resection of low risk pTim/T1 disease can potentially achieve an adequate oncological outcome with lower morbidity and mortality compared with radical resection. We have previously shown R0 resection is achievable (both for Paris 0-II/Is morphology tumours) using EMR +/- combination endoscopic submucosal dissection (ESD) with full thickness excision achievable using the latter technique. Furthermore, overall 30-day mortality, procedure related complications and in-patient stay were superior to conventional transanal approaches in our previous series. Concern regarding local recurrence, nodal disease positivity and overall medium/long-term oncological outcome has limited practice of these techniques in the UK due to the lack of this mandatory evidence base.
Aims & Methods: Single centre, prospective cohort analysis of pTim/T1 rectal cancer resected using endoscopic local excision with curative intent. Outcome measures: post-dissection mortality/morbidity, local recurrence rates, tumour free and overall survival. 43 patients underwent local endoscopic excision using EMR+/-ESD. All lesions were staged pre-resection using triple modality imaging (magnification chromoscopy/EUS/pelvic MRI). Patients with T2 disease or node “+” were referred for surgery. Post-resection follow-up: 1. Chromoscopic colonoscopy + 12.5/20 MHz EUS at 3, 6, 12 months post-resection and annually thereafter. Higaki and Chak criteria were used to define recurrent disease at colonoscopy and EUS respectively.
Results: Data were available for analysis on 41 patients (2 lost to follow-up). 30-day re-admission/death rate = 0%. Early/delayed bleed rates = 3/41 (7%), haemastasis achieved in all using an endoscopic approach. Perforation rate = 1/40 (2.5%). Median in-patient stay = 8 hours (range 2–76). Resection status: R0 28/41(68%)/Rx 7/41(17%)/R1 6/41(15%). Of the 6 patients defaulting to R1 all underwent a R0 endoscopic dissection. Local recurrence rates = 2/41 (4.8%) – 1 patient Higaki criteria “+”/1 patient Higaki “−”(poorly differentiated mucinous compared to well-differentiated adenocarcinoma with TVA at index resection). Median follow-up 38 months (range 10–66): tumour free survival = 39/41 (95%)/overall survival 40/41 (97%).
Conclusion: This is the first UK study to show endoscopic resection of low-risk early rectal neoplasia can result in an oncological acceptable outcome in the medium term. Survival results are comparable to conventional transanal/transanal endoscopic microsurgical dissection.
MICRODISSECTING THE CARCINOGENESIS PATHWAYS IN SPORADIC AND COLITIS-ASSOCIATED COLON CANCER
S. J. Leedham1, T. Graham2, M. Rodriguez-Justo3, R. Harrison4, M. Novelli3, J. A. Jankowski5, N. A. Wright1. 1Histopathology Unit, 2Molecular and Population Genetics, Cancer Research UK, 3Pathology Department, University College Hospital, 4Pathology Department, Leicester General Hospital, London, 5Clinical Pharmacology, University of Oxford, Oxford, UK
Introduction: The adenoma-carcinoma sequence in sporadic colon cancer is the most established and best studied carcinogenesis pathway. It is thought that founder mutations in adenomatous polyposis coli (APC) are followed by K-ras lesions as polyps grow. p53 mutations occur late as an adenoma progresses to a cancer. The pathway to cancer in ulcerative colitis (UC) is less clearly understood.
Aims & Methods: We aimed to investigate these carcinogenesis pathways by assessing the mutation load of individual crypts at different stages of the dysplasia-carcinoma sequence in sporadic and colitis-associated cancer. Individual crypts were microdissected across 4 colitis-associated and 4 sporadic colectomy blocks containing carcinoma arising from dysplasia, as well as 15 sporadic polyps of varying sizes and 5 colitic dysplasias. APC, K-ras and p53 mutation load of normal, dysplastic and malignant crypts were then analysed. Individual lesions were also assessed for aneuploid change.
Results: Sporadic pathway: a small minority of sporadic polyps appeared to be polyclonal for APC. K-ras mutations, when present usually affected the entire adenoma, and p53 mutations were present in adjoining dysplastic as well as malignant crypts. Colitis-associated: p53 mutations were founder lesions in about 40% of cases, however one patient had a founder K-ras mutation. Dysplastic plaques are clonal lesions but synchronous tumours are usually made up of different clones. There was an increased frequency of aneuploidy in colitis-associated lesions.
Conclusion: Sporadic pathway: K-ras mutation may occur earlier or sweep through polyps more quickly than expected. p53 mutations do not always appear to be directly responsible for malignant change as they can be present in adenomatous crypts as well as their malignant counterparts. Colitis-associated: dysplastic plaques appear to be clonal as they shared identified founder mutations. Localised field cancerisation does appear to occur, probably as a consequence of increased crypt fission. No encompassing mutation sequence could be established and multiple carcinogenesis pathways are likely.
EXTRACELLULAR GALECTIN-3 INTERACTS WITH CELL SURFACE MUC1 TO PROMOTE CANCER CELL AGGREGATION, ADHESION AND TRANS-ENDOTHELIAL INVASION: AN IMPORTANT MECHANISM FOR METASTASIS
Q. Zhao1, M. Barclay1, J. Hilkens2, J. M. Rhodes1, L. G. Yu1. 1School of Clinical Science, University of Liverpool, Liverpool, UK, 2Divison of Cancer Biology, Netherlands Cancer Institute, Amsterdam, The Netherlands
Introduction: Cancer cell homotypic aggregation, heterotypic adhesion to and invasion through the endothelium are three key steps in the cancer metastasis cascade. Molecular mechanisms underlying these steps are not fully understood. We recently showed that the human lectin galectin-3, which can show up to fivefold increased serum concentration in cancer patients, interacts with the oncofetal Thomsen-Friedenreich (TF) (Galβ1,3GalNAc) carbohydrate antigen on MUC1 to promote cancer cell adhesion to endothelium by cross-linking cell surface MUC1 to reveal underlying adhesion molecules (Yu et al, J Biol Chem, 2007). We have now assessed the effects of this interaction on homotypic cancer cell aggregation and trans-endothelial invasion.
Aims & Methods: The aim of this study is to investigate the effects of MUC1-galectin-3 interaction on homotypic cancer cell aggregation and trans-endothelial invasion.
Results: Human colon cancer HT29-5F7 cells, a sub-population of HT29 cells that strongly express MUC1, in comparison with parent HT29 cells show less cell-cell aggregation (3.79±0.79%, mean ±SE vs 8.64±0.1%, p<0.01) assessed by FACS and less adhesion to human umbilical vein endothelial cells (HUVEC) either unstimulated: (8.6±0.77% vs 14.3±1.17%, p<0.01) or pre-stimulated with TNFα (15.5±2.75% vs 21.9±3.44%, p<0.05). MUC1-transfected human breast epithelial cancer cells (HCA1.7+) and human melanoma cells (ACA19+) also show much less cell-cell aggregation and adhesion to HUVEC than MUC1-negative transfectants (HCA1.7− and ACA19−). Recombinant galectin-3, at concentrations (0.1–1 μg/ml) similar to that found in the sera of cancer patients, caused cell surface clustering of MUC1 and increased cell aggregation and adhesion of high MUC1-expressing HT29-5F7 and HCA1.7+ cells, but not of HT29 and HCA1.7− cells. Recombinant galectin-3 increases invasion of ACA19+ (164±24%, p<0.05), but not ACA19−, through HUVEC monolayer. These effects of galectin-3 were largely prevented by the presence of lactose and also by anti-E-cadherin (in aggregation) or anti-CD44H or –E-selectin antibody (in adhesion).
Conclusion: These results suggest that circulating galectin-3 in patients with epithelial cancers including colon cancer may promote metastasis by interacting with MUC1/TF and revealing underlying adhesion molecules that allow homotypic aggregation and trans-endothelial invasion. Prevention of this interaction might plausibly prevent cancer metastasis.
INCIDENCE AND IMPLICATIONS OF PRE-POUCH ILEITIS IN PATIENTS FOLLOWING RESTORATIVE PROCTOCOLECTOMY
S. D. McLaughlin1, S. K. Clark2, A. J. Bell3, P. P. Tekkis1, P. J. Ciclitira4, R. Nicholls1. 1Department of Biosurgery and Surgical Technology, Imperial College, 2Department of Surgery, St Mark’s Hospital, London, 3Department of Gastroenterology, Weston-Super-Mare General Hospital, Weston-Supermare, 4Department of Gastroenterology, Nutritional Sciences Research Division, King’s College, London, UK
Introduction: Pouchitis following RPC for ulcerative colitis (UC) is common. Inflammation proximal to the pouch; pre-pouch ileitis (PI) has recently been described,1 its incidence and implications are unknown. Some authors have suggested it may indicate missed Crohn’s disease (CD).
Aims & Methods: The aim of this study was to identify the incidence of pre-pouch ileitis at pouchoscopy and correlate this with symptoms, diagnosis and outcome. It is routine practice at our institution to intubate the pre-pouch ileum at pouchoscopy. We searched the endoscopy database for the terms “pouchitis” and “ileitis” in all pouchoscopy procedures performed at our institution between April 2004 and September 2007, hospital records were then reviewed. Those with CD were excluded.
Results: 1448 pouchoscopies were performed on 754 patients (polyposis 179), (UC/indeterminate colitis (IC) 568), (CD 5). Pouchitis was diagnosed in 254 (34%) patients. 35 patients were identified with endoscopic signs of pre-pouch ileitis (UC/IC), (FAP 1). 1 patient took NSAIDs and was excluded from further analysis. All had concurrent pouchitis. 3 had ileal stricturing. PI length was recorded in 32 procedures (65%), mean PI length = 13.3 cm. Of the 35 patients with PI 25% were asymptomatic. Histology of the terminal ileum at the time of colectomy was available in 17 patients, 6 (35.4%) had histological backwash ileitis. At follow-up (mean 13 months) n = 0 were reclassified as Crohn’s disease, and no patient required an ileostomy for poor function. Histology of the terminal ileum at time of colectomy was available in 19 patients, 6 (34%) had histological backwash ileitis.
Conclusion: 34 of 568 patients with an ileo-anal pouch for UC/IC and 1 of 179 patients with polyposis were found to have PI. All had associated pouch inflammation, however not all patients were symptomatic. The incidence of backwash ileitis in this group was twice that expected (18%) at colectomy for UC;2 this may suggest a similar disease process. Our results demonstrate that PI is more common than previously thought; it does not imply missed Crohn’s disease or predict an increased rate of pouch failure at least in the short term.
MOST BOWEL CANCER SCREENING COLONOSCOPIES ARE UNDERTAKEN FOR WEAK POSITIVE FAECAL OCCULT BLOOD RESULTS
C. J. Rees1, M. Ritchie1, I. Ward2, D. Nylander3, J. Painter3, J. Singh2, L. Hurst4, M. Rutter4. 1South of Tyne Bowel Cancer Screening Centre, South Tyneside General Hospital, South Shields, 2South of Tyne Bowel Cancer Screening Centre, Queen Elizabeth Hospital, Gateshead, 3South of Tyne Bowel Cancer Screening Centre, Sunderland Royal Infirmary, Sunderland, 4Tees Screening Centre, University Hospital of North Tees, Stockton, UK
Introduction: Individuals who participate in bowel cancer screening complete 6 faecal occult blood (FOB) testing windows on 3 separate stool samples (2 windows for each day). If 5 or 6 windows are positive the result is classed as abnormal and they are invited to attend for colonoscopy. If 1–4 windows are positive this is classed as an unclear result and individuals undergo repeat FOB testing. Two further sets of 6 normal windows are then required to classify a result as normal. If any windows on the two repeat kits are positive the individuals are invited to attend for colonoscopy. This is classed as a weak positive result.
Aims & Methods: Data from the South of Tyne and Tees bowel cancer screening centres were collected from March to early October 2007. These centres serve 1.5 million people. Analysis of data was undertaken to identify the % of screening kits returned with an abnormal FOB result; those with a weak positive result and those with an unclear result that was subsequently classed as normal. Positive results (abnormal and weak positive) were compared to the pathology diagnosed at colonoscopy.
Results: 1.6 % of FOBs returned in the screening population served were classed as positive (abnormal (0.16%) or weak positive (1.44%)) and individuals were subsequently invited for colonoscopy. 521 colonoscopies were undertaken in 2 centres by 5 colonoscopists. 469/521 (90%) of patients undergoing colonoscopy had weak positive FOB results and 52/521 (10%) had abnormal FOB results. The table demonstrates the pathology diagnosed. Patients diagnosed with cancer were more likely to have an abnormal FOB result when compared to patients with a normal colonoscopy (p<0.05). 2.1% of FOBs returned demonstrated an unclear result initially with 2 subsequent FOB kits normal. These patients were classed as normal and did not undergo further investigation.
Conclusion: The overwhelming majority of colonoscopies undertaken as part of bowel cancer screening are on individuals with weak positive FOB results. High levels of pathology are diagnosed. Cancer patients were more likely to have an abnormal FOB result when compared to patients with normal colonoscopies however most cancers were still diagnosed in patients with weak positive FOBs.
Research submitted on behalf of the Northern Region Endoscopy Group.
Endoscopy free papers
ENDOSCOPIC MUCOSAL RESECTION FOR HIGH-GRADE DYSPLASIA AND EARLY CANCERS IN THE UPPER GASTROINTESTINAL TRACT: PORTSMOUTH EXPERIENCE
M. Duku1, R. Mead1, D. Poller2, S. Somers3, S. Toh3, P. Goggin1, R. Ellis1, H. Duncan1, C. Archer4, P. Bhandari1. 1Gastroenterology, 2Pathology, 3Surgery, 4Oncology, Portsmouth Hospitals Trust, Cosham, UK
Introduction: Endoscopic mucosal resection (EMR) is as an alternative treatment option to radical surgery in selected patients with early neoplasia of the upper GI tract. The risk of invasive cancer and lymph node metastasis in these patients has been cited as reasons to advocate radical surgery for these lesions. In addition to its therapeutic role, EMR also serves as a staging tool.
Aims & Methods: To evaluate effect of EMR on the histopathological staging and the rate of recurrence and/or development of metachronous lesions following EMR. We analysed a prospective series of 45 EMR cases performed on 35 consecutive patients with early oesophago-gastric neoplasia (non-squamous) by a single endoscopist between 2004 and 2007 in Queen Alexandra Hospital Portsmouth. All patients had a staging CT scan and a selected group had EUS as well. A staging chromoendoscopy, with acetic acid was carried out on all patients before EMR. Different EMR techniques (cap and snare, duette, strip biopsy, and insulated tip knife) were used either alone or in combination depending on the size and location of the lesions. Patients were followed-up with chromoenoscopy and biopsies of the EMR site and any remaining Barrett’s segments every three months for one year then every six months.
Results: 28/35 patients underwent only one EMR while 7/35 had two or more EMR sessions to achieve complete clearance. 29/35 patients (82.9%) had curative EMR. 6/35 patients had submucosal invasion (SM-cancer), of whom 4 had oesophagectomy and 2 (unfit for surgery) were referred for palliative therapy. There was one delayed bleeding at 48 hours, which was controlled endoscopically, and one stricture, managed by endoscopic dilation. 8/30 (26.7%) patients with HGD pre-EMR were up-staged to cancer post-EMR. After a median follow-up of 11.5 months, recurrent/metachronous lesions were identified in 6 (17.1%) patients on surveillance (5 HGD & 1 IM-cancer). 4/6 have had repeat EMRs and are now in remission, 2/6 are awaiting EMR.
Conclusion: Our series show that: (1) EMR is an excellent therapeutic tool in selected patients. However, following curative EMR patients need regular surveillance to identify and treat recurrent/metachronous lesions. (2) EMR has no mortality and low morbidity. (3) It is the best available staging tool for early gastrointestinal cancers.
CONTRAST ENHANCED ENDOSCOPIC ULTRASOUND FOR DISCRIMINATION OF FOCAL CHRONIC PANCREATITIS AND PANCREATIC CANCER
M. Hocke1, T. Topalidis2, C. F. Dietrich3, A. Stallmach1. 1Internal Medicine II, Friedrich Schiller University Jena, Jena, 2Private practice, Cytological laboratory, Hannover, 3Internal Medicine II, Caritas Hospital, Bad Mergentheim, Germany
Introduction: Recognising malignant neoplasia in chronic inflammatory pancreatic lesions has always been difficult. However, the introduction of endoscopic ultrasound guided fine needle aspiration made this much easier. Nevertheless, a non-invasive method for detecting pancreatic malignancy would still be preferable.
Aims & Methods: In 192 patients with suspected chronic pancreatitis (age 62±12 years) pancreatic lesions were examined by conventional endoscopic B-mode, Power Doppler ultrasound and contrast enhanced power mode (Hitachi EUB 525 or Aloka-Olympus UCT 160, SonoVue, 2.4 ml, Bracco) using the following criteria for malignant lesions: no detectable vascularisation using conventional power Doppler scanning, irregular appearance of arterial vessels over a short distance using SonoVue contrast enhanced technique, and no detection of venous vessels inside the lesion. A malignant lesion was assumed if all criteria were fulfilled (gold standard EUS-guided fine needle aspiration cytology with 1-year follow-up or operation). The criteria for chronic pancreatitis without neoplasia were defined as no detectable vascularisation before injection, regular appearance of vessels over at least a distance of 20 mm after injection of SonoVue and detection of arterial and venous vessels.
Results: Using conventional EUS-criteria sensitivity was 82.2% and specificity of 87.8 % for pancreatic cancer. Using contrast enhanced EUS 108 of 118 patients with malignant pancreatic lesion displayed all criteria (increasing sensitivity to 91.5%). In 70 of 74 patients with chronic inflammatory pancreatic disease, the diagnosis was correctly recognised, giving a specificity of 94.6%.
Conclusion: Contrast enhanced endoscopic ultrasound improves the differentiation between chronic pancreatitis and pancreatic carcinoma.
IS ENDOSCOPIC ULTRASOUND WITH FINE NEEDLE ASPIRATION NOW ESSENTIAL FOR THE MANAGEMENT OF PANCREATICOBILIARY MALIGNANCY?
G. C. Bennett1, S. O’ Riordan1, R. Sugrue1, R. Bambury1, S. Sengupta1, E. Clarke1, N. Mulligan2, J. Lennon1, T. Kelleher1, G. McEntee3, P. MacMathuna1. 1Gastrointestinal Unit, 2Department of Pathology, 3Department of Surgery, Mater Misericordiae University Hospital, Dublin 7, Ireland
Introduction: Endoscopic ultrasound (EUS) with fine needle aspirate +/− biopsy (FNAB) is increasingly used in the loco-regional staging, and pathological diagnosis of pancreaticobiliary malignancy. Prior to its introduction, CT was the modality of choice for staging, and a tissue diagnosis was often difficult to obtain preoperatively.
Aims & Methods: To evaluate our experience of EUS-FNA in the management of suspected pancreaticobiliary malignancy. All procedures were conducted over a 5-year period on a national referral basis. In 107 patients, we examined demographics, imaging, pathology and clinical follow up. FNA was performed on pancreas, ampulla, abdominal nodes, ascites. We examined the indication for FNA, diagnostic yield and complication rate.
Results: An adequate sample for diagnosis was obtained in 94/107 cases (88%). Complete follow up was available for 76/94 (81%). Malignancy was confirmed in 57/76 (75%) (sensitivity 100%, specificity 100%). The diagnosis was benign in 19/76 (25%). In 7 (36%) cases, the diagnosis was subsequently shown to be incorrect following surgery. (sensitivity 63%, specificity 100%) One major complication (perforated duodenum) was encountered.
Conclusion: EUS with FNA provides a safe, effective “one stop shop” approach to loco-regional staging and tissue diagnosis in pancreaticobiliary malignancy, with a high PPV. Benign histology, in the context of a high clinical suspicion for malignancy, must be interpreted with caution, since sampling error is a generic phenomenon, regardless of modality.
“UPSIDE DOWN” COLORECTAL ENDOSCOPIC DISSECTION FOR RETROFOLD AND HEMI-CIRCUMFERENTIAL INTRAEPITHELIAL NEOPLASTIC DISEASE: EXPANDING THE ENDOSCOPIC TECHNICAL PARADIGM
D. P. Hurlstone1, W. Baraza2, S. R. Brown2, N. Tiffin3, S. S. Cross4. 1Endoscopy, Royal Hallamshire Hospital, 2Colorectal Surgery, 3Histopathology, STH NHS Foundation Trust, 4Histopathology, Royal Hallamshire Hospital, Sheffield, UK
Introduction: Retrofold disease, hemi-circumferential luminal involvement and consecutive haustral fold expansion have historically been contraindications to endoluminal resection therapy for Paris type I, 0-II, LST (G/F) and stage N0/Tim/T1 carcinoma. Intraluminal access using conventional colonoscopes is often impossible due to limitations in acute tip angulation. Retroflexion can be achieved at any anatomical location in the colorectum with retrofold access using a GIF-XQ240 gastroscope.
Aims & Methods: To prospectively assess the technical efficacy and medium term clinical outcome of lesions resected using retroflexion assisted dissection as salvage endoscopic therapy. Patients were recruited for endoscopic retroflexion assisted dissection following an index diagnostic colonoscopy that precluded conventional en face endoscopic resection. Exclusion criteria were pre-resection high-frequency 12.5 MHz EUS suggestive of T1/N1 disease, index histopathology suggestive of invasive neoplasia and non-correctable coagulopathy. Endoscopic mucosal resection (EMR) and endoscopic submucosal cap assisted dissection (ESCA) was performed in all eligible cases. Primary end point: Curative excision rates. Secondary end points: 1. Complications 2. Intraepithelial neoplasia recurrence 3. Procedure time analysis.
Results: 188 patients with 188 lesions fulfilled eligibility for salvage therapy. Caecal/neoterminal-ileal intubation using the GIF-XQ gastroscope was achieved in 184/188 (98%). Median post resection inpatient stay 24 hours (1–72), Median intubation time 16.5 min (range 8–39). Median resection times for Paris class Is, 0-II, LST-G and LST-NG were 89 min (range 20–240), 32 min (15–64), 148 min (22–242) and 64 (10–119) respectively. LST-G morphology was significantly associated with prolonged resection time (as compared with all other morphologies, p<0.04) and a high median submucosal dissection volume requirement (p<0.01). 159/188 patients completed the post dissection surveillance programme to 36 months. Primary end point: Higaki criteria for recurrence/remnant disease = 9/159 (5.6%), 2 undergoing R0 revision ESD, 7 surgical intervention. Overall “cure” rate at 36 months = 95%. 30-day mortality rate 0%, 30-day readmission rate 2/188 (1%), delayed/acute bleed rates 7/188 (4%), perforation rate 2/188 (1%)—both not requiring laparotomy.
Conclusion: This is the largest prospective study to address the technical feasibility and clinical outcomes using retroflexion assisted endoluminal resection. Retroflexion assisted resection using EEMR and ESCA for complex intraluminal adenoma and early stage cancer is a safe, efficacious technique at medium term follow-up and an alternative to surgical excision.
NARROW BAND IMAGING FOR LESION CHARACTERISATION IN THE COLON, OESOPHAGUS, DUODENAL AMPULLA AND LUNG: A META-ANALYSIS
J. E. East1, E. Tan2, J. J. Bergman3, B. P. Saunders1, P. P. Tekkis2. 1Wolfson Unit for Endoscopy, St Mark’s Hospital, 2Department of Biosurgery and Surgical Technology, Imperial College London, London, UK, 3Department of Gastroenterology, Academic Medical Center, Amsterdam, The Netherlands
Introduction: Narrow band imaging (NBI) is a new endoscopic technology which can highlight mucosal surface structures and microcapillaries. Abnormal surface structure and microvasculature are predictive of neoplastic change. We aimed to assess the diagnostic precision of NBI for diagnosis of epithelial neoplasia compared to conventional histology.
Aims & Methods: We performed a meta-analysis of studies which compared NBI based diagnosis of neoplasia with histopathology, using the search keywords “narrow band imaging” and “endoscopy” published before 8 August 2007. Sensitivity, specificity, diagnostic odds ratios (DOR) were calculated for each study. Study quality and heterogeneity was assessed. Summary receiver operator characteristics (ROC) and subgroup analyses were performed. Meta-regression was used to compare subgroups.
Results: 51 studies were identified, of which 11 had extractable data (colon 5, oesophagus 3, lung 2, duodenal ampulla 1). Results for overall analysis, by organ, by assessment method, and by study quality are presented (table). Significant heterogeneity was found overall, and for studies in the colon and oesophagus. Meta-regression showed no significant difference between, colon versus oesophagus, mucosal pattern (pit pattern) versus microvascular measures, or magnification versus non-magnification for diagnostic accuracy. Studies with more than 50 patients (>100 lesions) had a higher DOR compared to those with <50 patients, relative DOR 7.0 (95% CI 1.1 to 44.5), p = 0.041, and NBI was more accurate than chromoendoscopy, relative DOR 3.6 (95% CI 1.2 to 11.1), p = 0.024.
Conclusion: NBI, a simple, push-button technology, appears highly accurate, with narrow confidence intervals, for in vivo diagnosis of neoplasia across a range of organs, using simple microvessel based measures. It has the potential to increase the yield of targeted biopsies or could even potentially replace formal histopathology for assessment of low-risk lesions.
Endoscopy videos
DOUBLE BALLOON ENTEROSCOPY: REACHING THE DEPTHS OF THE SMALL BOWEL
E. Despott1, S. Preston1, E. Tripoli1, A. Polecina1, K. Konieczko2, C. Fraser1. 1Wolfson Unit for Endoscopy, St Mark’s Hospital, 2Department of Anaesthesia, St Mark’s and Northwick Park Hospitals, London, UK
Introduction: The advent of double balloon enteroscopy (DBE) has advanced the investigation and management of small bowel disease to a higher level. In addition to complementing the findings of capsule endoscopy (CE), it has the capability of being a useful therapeutic device in areas of the small bowel which were previously inaccessible outside the operating theatre.
Aims & Methods: Since the DBE service began at our unit in February 2005, all DBE procedures have been recorded on digital video. This short film taken from these recordings, shows amalgamated video footage that exemplifies the diagnostic and therapeutic capabilities of DBE.
Results: The viewers will be shown cases where DBE was instrumental in making a diagnosis that led to definitive patient management. This is illustrated by video clips showing a selection of small bowel tumours, mucosal ulceration and a large vascular lesion. The therapeutic ability of DBE will be highlighted by video footage of direct percutaneous endoscopic jejunal feeding tube insertion, coagulation of bleeding vessels and balloon dilatation of Crohn’s disease related strictures.
Conclusion: Double balloon enteroscopy is highly effective for the diagnosis and treatment of small bowel pathology.
ENDOSCOPIC SUBMUCOSAL DISSECTION OF EARLY GASTRIC CANCER IN UK SETTING
M. Duku1, R. Mead1, D. Poller2, P. Bhandari1. 1Gastroenterology, 2Pathology, Portsmouth Hospitals Trust, Cosham, UK
Introduction: Endoscopic submucosal dissection (ESD) is an established therapeutic modality for early gastric cancers in Japan. Although the incidence of antral gastric cancer is low in the Western world, the incidence of gastric cardia cancers is rising. Traditionally, all these patients have been treated by radical surgery. There is increasing enthusiasm about using EMR. En bloc endoscopic resection of early gastric cancer is essential for accurate histological staging and reducing the recurrence rate. Unfortunately, simple EMR techniques do not allow en bloc resections of lesions more than 2 cm. ESD is a new, technically challenging technique which is used for en bloc resection of early gastric cancers of more than 2 cm.
Aims & Methods: We have been performing ESD for early gastrointestinal cancers since 2005 and have developed a good understanding of its principles, problems and role in Western settings. We have found that gastric lesions smaller then 4 cm, situated in antrum, incisura and O-G junction are less challenging and are the type of lesions that Western endoscopists can attempt to resect with ESD after suitable training. We aim to show video clips to illustrate the basic principles of ESD: Role of chromoendoscopy in lesion identification; Pre-marking the margins; Submucosal injection; Circumferrential incision; Submucosal dissection; Specimen retrieval and fixation; Post-ESD plans; Risks and management of ESD associated complications.
Results: It is technically feasible to perform ESD in Western settings but it requires training, good understanding of the basic principles, risks and skills in managing complications.
Conclusion: En bloc resection is the main principle of onco-surgery and ESD enables us to meet this principle when dealing with lesions larger then 2 cm. We have demonstrated that ESD is feasible in the Western settings but its exact role in the West needs further clarification.
EN BLOC RESECTION OF EARLY GASTRIC NEOPLASIA USING THE ENDOSCOPIC SUBMUCOSAL DISSECTION TECHNIQUE: WEST MEETS EAST!
K. Ragunath1, R. Singh1, P. Kaye1, M. Ilyas1, K. Yao2. 1Wolfson Digestive Diseases Centre, Queens Medical Centre, Nottingham University Hospital, Nottingham, UK, 2Department of Gastroenterology, Fukuoka University Chikushi Hospital, Fukuoka, Japan
Introduction: Endoscopic mucosal resection (EMR) is now a well established technique to excise early gastrointestinal neoplasia. The efficacy of the procedure is directly related to the ability of the endoscopist to achieve complete resection. Until recently, single piece resection of lesions larger than 10 mm was technically difficult. This resulted in piecemeal resections being performed with high recurrence rates. However, yet another Japanese innovation in this field, endoscopic submucosal dissection (ESD), has resulted in overcoming this shortfall.
Aims & Methods: To report our experience in ESD for en bloc resection of early gastric neoplasia by (1) demonstrating the identification of early gastric neoplasia and the technique of ESD, (2) elucidating common complications and their management, (3) discussing learning curve and training issues. The first author (KR) undertook a period of sabbatical in Japan observing advanced endoscopic imaging in identifying early GI neoplasia and endoscopic resection techniques. The procedure was registered and performed as per Safety and Efficacy Register of New Interventional Procedures (SERNIP) guidelines. KR then performed all the procedures in Nottingham with guidance and hands-on technical advice by a senior Japanese endoscopist (KY). High definition zoom endoscopy with Autofluorescence Imaging and Narrow Band Imaging were done in addition to Chromoendoscopy to identify and delineate the lesion. The Insulated Tip Knife and Hook Knife from Olympus, Tokyo were used for the resections. High frequency EUS was performed prior to resections. All the procedures were digitally recorded and this presentation will include short edited clips.
Results: Four male patients (mean age: 72, range: 63–80) had undergone en bloc resection by ESD for early (Paris Type IIa or IIb) gastric neoplasia under intravenous sedation (pethidine 50–100 mg, diazemules 10–20 mg). The mean procedure time was 53 min (45–180). Three patients developed brisk bleeding during the procedure which was controlled with hot biopsy graspers. All patients recovered well without any immediate or delayed complications. Complete resection was achieved in all cases and the mean size of the resected specimen was 2.5 cm (1.7–3.5). Histopathology demonstrated high grade dysplasia, low grade dysplasia, intramucosal carcinoma and carcinoid tumour respectively. Follow-up endoscopy with detailed examination of the resected sites and biopsies were performed at 3 months, 6 months then yearly. To date after a mean follow-up of 16 months, there were no recurrences in this cohort of patients.
Conclusion: ESD is a safe technique for en bloc resection of early gastric neoplasia and can be adopted in the Western world provided it is done under optimal conditions. It is technically challenging and requires systematic hands-on training.
A 7 CM G-TYPE LATERALLY SPREADING TUMOUR OF THE RECTUM EXCISED EN BLOC USING ENDOSCOPIC SUBMUCOSAL DISSECTION WITH THE FLUSH KNIFE
N. Suzuki1, B. P. Saunders2. 1Wolfson Unit for Endoscopy, 2Endoscopy, St Mark’s Hospital, Harrow, UK
Introduction: Endoscopic submucosal dissection (ESD) is recognised in Japan as an effective therapeutic modality for the clearance of gastrointestinal neoplasms, providing an en bloc specimen to confirm lateral and deep resection margins and minimising the risk of recurrence. However, due to the technical complexity and risk of complications, few European centres have introduced this technique. This video shows how an ESD technique can be safely applied to resect a 7 cm laterally spreading tumour (LST) in the rectum.
Aims & Methods: The margins of the rectal LST were lifted by injection of sodium hyaluronate using a 23 gauge injection needle. The first incision was made through the mucosa adjacent to the lesion to gain access to the submucosal plane with a 1.5 mm flush knife (Fujinon), followed by cutting around the edge to enable a flap of mucosa to be lifted. The submucosal dissection was performed with the help of a distal attachment, which was fitted at the end of the scope to achieve optimum retraction and visualisation, helping to expose the submucosal layer by creating a counter traction effect. Any bleeding during the procedure was treated with an electrosurgical haemostatic forceps (Cograsper (Olympus)). The electrosurgical unit used was ICC200 (ERBE) using the following settings, “endocut 80W”, “soft coagulation 35W” and “forced coagulation 60W” for the mucosal incision, submucosal dissection and haemostasis, respectively.
Results: The patient received conscious sedation with midazolam (1.25 mg) and pethidine (25 mg). En bloc resection was achieved with a procedure time of 180 min. No early or late complications were encountered. The resected specimen was 65 by 70 mm in size. Histologically the lesion was a tubulovillous adenoma with high grade dysplasia with clear lateral and deep margins (R0 resection).
Conclusion: ESD was effective for the excision of this large rectal LST. Large sessile polyps and some T1 cancers are potentially best treated by this technique which provides definitive histology and very low risk of local recurrence. With the advent of bowel cancer screening and an increased detection of such lesions this new minimally-invasive approach is becoming more applicable and with careful training can be performed safely at specialist endoscopic centres in the UK.
SINGLE OPERATOR PERORAL CHOLEDOCHOSCOPY SYSTEM: A SINGLE CENTRE EXPERIENCE
M. A. Zubir, M. L. Wilkinson, R. J. Ede, T. Wong. Deparment of Gastroenterology, Guy’s And St Thomas Hospital NHS Foundation Trust, London, UK
Introduction: The SpyGlass (Boston Scientific) peroral choledochoscopy system provides 4-way deflected steering by a single operator which allows direct visual examination of bile ducts, visually guided intraductal biopsies, and therapeutic procedures.
Aims & Methods: To report our experience with using SpyGlass in 8 consecutive ERCP cases referred for choledochoscopy. ERCP with SpyGlass examinations with or without biopsy were performed in 8 patients. The patients selected were in those whom direct visualisation of intraductal pathology was indicated following previous investigations including ERCP which were inconclusive.
Results: Eight patients underwent ERCP with SpyGlass. The mean age of the patients was 68 years (range 34–84). The mean time taken for the whole procedure including ERCP was 43 minutes (range 28–56). Primary indications for SpyGlass were to biopsy indeterminate strictures (n = 5) and confirm intraductal abnormalities (n = 3). The primary SpyGlass visual diagnoses were strictures (n = 5), bile duct stone (n = 2) and normal findings (n = 1). Intraductal biopsies were taken in 4 patients. In patients in whom biopsies were not taken, one was due to technical difficulties and 3 others were not clinically indicated. No complications were identified post procedure.
Conclusion: Our early experience with SpyGlass suggest that it is safe, well tolerated, technically feasible and useful in the diagnosis and management of duct diseases. More experience of the procedure will be needed to the determine the accuracy of diagnosis with the Spyglass system.
ENDOSCOPIC MUCOSAL RESECTION OF HIGH GRADE GASTRIC DYSPLASIA USING THE DUETTE MUCOSECTOMY DEVICE
A. Dhar1, A. Allan1, E. Millington2. 1Department of Gastroenterology, Bishop Auckland General Hospital, County Durham, 2Endoscopy, Cook Medical (UK) Ltd, Hertfordshire, UK
Introduction: Endoscopic mucosal resection (EMR) is a relatively new technique for resection of early cancer in the oesophagus and stomach. It has been widely used in Japan for some years but has been incorporated into practice in the Western world for less than a decade. It can be done using conventional saline injection and snare resection using the Cap-EMR technique or by lift and cut technique using a dual channel scope. The Duette mucosectomy device is a new accessory developed by Cook Medical, using a combined multi-band ligator device and snare without the need for saline injection. In the UK, it has been used predominantly for resection of high grade dysplasia and intramucosal carcinoma of the oesophagus, in patients with Barrett’s oesophagus.
Aims & Methods: We present a patient with a 15 mm lesion in the stomach, histologically high grade gastric dysplasia, who was treated successfully with EMR using the Duette mucosectomy device.
Results: A 78-year-old gentleman with chronic obstructive airways disease, atrial fibrillation and heart failure underwent an upper GI endoscopy for new onset dyspepsia. At endoscopy, there was a 15 mm reddish, slightly elevated lesion in the distal body of the stomach on the lesser curvature which was better delineated with 1% indigo carmine dye spray. Multiple biopsies taken on 2 separate occasions, 3 months apart were reported to show high grade dysplasia, but no cancer. CT scan was normal. The patient underwent Endoscopic Mucosal Resection of the gastric lesion using the Duette mucosectomy device after marking and the entire lesion was removed in 4 separate pieces. Post-resection histology was reported to show dysplasia in only the superficial half of the mucosa with complete excision, and free margins. A 6 monthly endoscopic surveillance is planned for early 2008.
Conclusion: It is possible to safely resect early gastric cancer using the Duette mucosectomy device and the technique is easier to learn than the Cap-EMR resection and can be performed through a standard single channel therapeutic endoscope.
ENDOSCOPIC PAPILLECTOMY FOR AMPULLARY NEOPLASIA
R. J. Mead, M. D. Duku, P. Goggin, R. D. Ellis, H. Duncan, P. Bhandari. Gastroenterology, Portsmouth Hospitals Trust, Cosham, UK
Introduction: Management of benign ampullary tumours remains controversial due to the uncertainty in diagnosis and risks associated with various treatment options. We believe that endoscopic papillectomy (EMR) is technically feasible and safe. EMR can serve as a final diagnostic step or an ultimate therapeutic option for these patients.
Aims & Methods: We have been performing endoscopic resections of all benign ampullary tumours which has given us a good insight into the principles of endoscopic papillectomy. We aim to illustrate the following principles of endoscopic papillectomy: Role of chromoendoscopy; Role of submucosal injection; Snaring techniques; Billiary and pancreatic stents and their timings; Adjunctive treatment.
Results: We have recently performed 10 endoscopic papillectomies in last one year at our centre with very good outcome. We have had one patient with mild self-limiting pancreatitis and no cases of bleeding, perforation or mortality. These encouraging results have influenced the management of these patients in our region.
Conclusion: We have found that endoscopic papillectomy is technically feasible, safe and potentially curative. Our video clips illustrate some basic principles of the procedure including submucosal injections, snaring techniques, pancreatic and billiary stenting. We aim to discuss other controversies and principles of management of complications associated with this procedure.
Gastrointestinal pathology free papers
THE FIXATION OF MUTATIONS AND CLONAL EXPANSION IN INTESTINAL METAPLASIA: FIELD CANCERISATION IN THE HUMAN STOMACH
S. A. C. McDonald1, L. Gutierrez-Gonzalez1, M. Rodriguez-Justo2, S. J. Leedham1, M. Novelli2, I. Mitchell3, D. Stoker3, J. A. Jankowski4, N. A. Wright5. 1Histopathology Unit, London Research Insitute - Cancer Research UK, 2Histopathology, 3Department of Surgery, University College London, London, 4Department of Clinical Pharmacology, University of Oxford, Oxford, 5Histopathology, Barts and the London School of Medicine and Dentistry, London, UK
Introduction: The clonal origins and mechanisms of spread of intestinal metaplasia (IM) within the human stomach are poorly understood. Mihara et al1 suggested that IM is a polyconal disorder with distinct crypts having different methylation patterns. We have previously shown, using mitochondrial DNA (mtDNA) mutations as a marker of clonal expansion, that normal gastric glands are clonal: all cells within a gland contain the same mtDNA mutation. We have also shown that clonal patches occur with multiple glands each containing the same mutation.
Aims & Methods: Here we investigate the clonality of IM crypts in the human stomach and reveal a mechanism by which they spread. Double enzyme histochemistry was performed on frozen sections of human gastric resections with IM for reactivity of Cytochrome c oxidase (CCO) in along with the nuclear-encoded enzyme succinate dehydrogenase (SDH), the principle being that a mutation in the mtDNA that leads to inactivity of the CCO enzyme will result in only SDH activity being detected. Immunostaining for CD10, MUC2 and chromogranin was used as markers of differentiated epithelial cells.
Results: Entirely CCO −ve IM crypts were observed indicating that such crypts are clonal. Immunostaining revealed that all the major differentiated lineages (enterocyte, neuroendocrine and goblet cells) were present in such crypts. Partially mutated glands were also present suggesting that multiple stem cells reside in these crypts. We observed frequent patches of CCO −ve crypts which all contain the same mtDNA mutation suggesting that there is one founder crypt which has expanded by fission.
Conclusion: We propose that IM has its origins as a clonal disorder and that fission is a method by which it spreads in the stomach. Furthermore, the presence of partially and completely mutated crypts suggests that monoclonal conversion occurs—the process by which one stem cell takes over the entire stem cell compartment eventually leading to all their progeny becoming mutated. This is in conflict with previous studies which argue that IM is polyclonal and that “mixed” IM crypts are a separate classification of IM. We would suggest that mtDNA mutations are a more reliable method of showing clonal expansion as they take many years to accrue to detectable levels, whereas methylation is a far more rapid process and that patterns diverge quickly. We therefore conclude that in IM, crypt fission fixes mutations, enables the clonal expansion of mutated stem cells, and thus is responsible for field cancerisation in the human stomach.
IRON MEDIATED CELLULAR PROLIFERATION, MIGRATION AND COLONY FORMATION IS DEPENDENT ON ADENOMATOUS POLYPOSIS COLI STATUS IN COLORECTAL ADENOCARCINOMA
M. J. Brookes, K. Roberts, T. Iqbal, C. Tselepis. Cancer Studies, University of Birmingham, Birmingham, UK
Introduction: There is emerging evidence suggesting increased cellular iron is important in the development of colorectal cancer. Colorectal cancer is characterised by mutations in adenomatous polyposis coli (APC); a tumour suppressor gene crucial in Wnt signalling. We have previously demonstrated that iron can activate Wnt signalling in the background of an APC mutation. However, the effect of iron on cell phenotype to date has not been addressed. Thus the aims of this study were to determine if iron could enhance cellular proliferation, migration and colony formation and establish if these effects were APC dependent.
Aims & Methods: Human colorectal APC wild type (HEK-293 and RKO) and APC mutant containing lines (Caco-2, SW480) were challenged with either ferrous sulphate (FeSO4) (100 μM) or hemin (50 μM) in the presence or absence of the GSK-3β inhibitor lithium chloride (LiCl) (20 mM) for 24 h. Cellular iron loading was confirmed using the ferrozine assay. Cellular proliferation was determined by BrdU incorporation and FACS analysis. Cellular migration was assessed using a wound healing assay, and in vitro anchorage independent colony forming determined using a soft agar colony forming assay. To further test the dependency of APC SW480 cells transfected with or without full length wild type APC were also used in these studies.
Results: Challenging APC mutant containing lines with FeSO4 or hemin significantly increased cellular proliferation, wound healing and anchorage independent growth. Conversely, wild type APC containing cell lines only responded to FeSO4 or hemin when co-cultured with LiCl. The dependency for APC was exemplified by the inhibition of iron mediated cellular proliferation in SW480 cells transfected with human wild type APC.
Conclusion: This study demonstrates that iron can induce cellular proliferation, migration and anchorage independent growth and we believe this is a consequence of iron mediated Wnt signalling. Interestingly iron could only induce these cellular effects in the background of abrogated β-catenin degradation, such as a truncating mutation in APC or inhibition of GSK-β.
THE AETIOLOGY OF HYPERPLASTIC POLYPOSIS SYNDROME IN A LARGE FAMILY FROM THE WEST OF IRELAND
K. J. Monahan1, L. Carvajal-Carmona2, T. Guenther3, T. O’Gorman4, J. Cazier2, I. P. Tomlinson2, H. J. W. Thomas1. 1Family Cancer Clinic, St Mark’s Hospital, 2Molecular and Population Genetics Lab, Cancer Research UK, 3Academic Department of Pathology, St Mark’s Hospital, London, UK, 4Department of Medicine, University College Hospital, Galway, Ireland
Introduction: We have identified a family with a dominantly inherited predisposition to mixed histology multiple polyps and colorectal cancer. The family meet WHO criteria for hyperplastic polyposis. We have attempted to elucidate the gene which predisposes to this condition.
Aims & Methods: Mutations in APC, MYH, SMAD4 and genes which cause HNPCC were excluded by direct sequencing and other methods. Somatic mutations were screened in genes often mutated in colorectal cancers. Genome wide genotypes were obtained for over 10000 SNPs using Affymetrix 10k plus 2 arrays and linkage analysis was performed. Genome wide copy number variation analysis was also performed using the Goldengate SNP platform. Whole genome expression analysis profiles were obtained on cell line RNA using the Affymetrix U133 Plus 2.0 GeneChip oligonucleotide arrays.
Results: The polyps appear to follow a hyperplastic/serrated polyp to mixed serrated/adenomatous (see fig) to adenocarcinoma sequence. Linkage analysis shows a maximum parametric LOD score of 2.71 at 8p22–21.3. Genome wide copy number and loss of heterozygosity (LOH) studies reveal LOH at 8p and 17p in the cancers. A number of genes at that locus including BMP1 and MTUS1 have been screened, the latter gene having more than a fivefold up-regulation in expression.

Conclusion: We have identified a locus on chromosome 8p which predisposes to hyperplastic polyps and colorectal cancer in a large family from the West of Ireland. This is the first time such an association has been identified and may be useful in screening families at risk of colorectal neoplasia.
INHIBITING EGFR AND VEGR REDUCES SMALL INTESTINAL AND COLONIC POLYP FORMATION IN A DSS ENHANCED APCMIN/+ MOUSE MODEL
D. Alferez1, R. W. Wilkinson2, A. J. Ryan2, R. A. Goodlad1. 1Histopathology, CRUK, London, 2Departments of Cancer and Infection Research, AstraZeneca Pharmaceuticals, Macclesfield, UK
Introduction: The ApcMin/+ mouse is a well-characterised model of intestinal tumorigenesis, and animals with this genetic mutation develop macroscopically detectable adenomas from approximately 6 weeks of age. Most of the polyps are found in the small intestine (SI) so that the resolution of events in the colon is limited. Inducing colitis with dextran sodium sulphate (DSS) can enhance the development of lesions in the colon.1 The contribution of VEGFR- and EGFR-dependent signalling pathways to the development of polyps in DSS treated or untreated ApcMin/+ mice was examined using a selective inhibitor of the tyrosine kinase activity of these receptors (ZD6474).
Aims & Methods: 8-week-old ApcMin/+ mice were given 1.8% DSS or water for 4 days followed by a 2 day pause, after which they were given ZD6474 or vehicle for 28 days. Intestines were opened2 and fixed in Carnoy’s fluid and then stored in 70% ethanol before polyp number and size were measured.3
Results: ZD6474 reduced the number of polyps in the SI by 76% in the water group and by 65% in the DSS treated (p<0.025). ZD6474 reduced the number of polyps in the colon by 60% (from 3.9 to 1.4 (p = 0.1)) of the non-DSS mice and in the DSS pre-treated by 78% (from 13.8 to 3.1, p<0.001). Multivariate analysis demonstrated that the effects of ZD6474 were similar in both DSS treated and untreated, as there were no interaction effects.
Conclusion: The DSS model thus does not alter the response of the colon; it only increases the resolution of the model. VEGF/VEGFR-2-dependent angiogenesis and EGFR-dependent tumour cell proliferation and survival are thus key mechanisms in polyp development. Targeting VEGFR- and EGFR-dependent signalling is a promising therapeutic strategy in intestinal tumours.
THE DELTA-SAMP MOUSE: A NOVEL EXPERIMENTAL MODEL FACILITATING ASSESSMENT OF THE ROLE OF C TERMINUS OF APC IN INTESTINAL TUMORIGENESIS
M. G. Deheragoda1, A. Lewis2, E. Nye3, N. Wright1, I. Tomlinson2. 1Histopathology Unit, 2Molecular and Population Genetics unit, 3Experimental Pathology Unit, Cancer Research UK London Research Institute, London, UK
Introduction: Mutation of the adenomatous polyposis coli (APC) gene is an initiating step in colonic carcinogenesis. APC is a multifunctional protein involved in the Wnt signalling pathway which controls proliferation and differentiation in the intestine. The C terminus of APC has been proposed to have significance in tumourigenesis through cytoskeletal interactions. We previously presented our data on a novel experimental model of intestinal tumourigenesis, the APC1322 mouse,1 which carries a mutated APC allele analogous to that most commonly found in patients with familial adenomatous polyposis (FAP), the APC1309 mutation. We used a modified version of the APC 1322T gene construct, to develop a novel model of intestinal tumorigenesis, the delta-SAMP mouse. The mutant APC protein in the delta-SAMP mouse has the same APC N terminus as the APC1322T (lacking SAMP repeats involved in beta catenin interactions) but retains the C terminus of APC.
Aims & Methods: To develop and characterise a novel experimental model, the delta-SAMP mouse, with which to assess the relative contribution of N terminal effects versus C terminal effects of mutant APC in intestinal tumorigenesis. A novel APC knockout model of intestinal tumorigenesis, The delta-SAMP mouse, was developed following homologous recombination in ES cells. The phenotype of the delta-SAMP mouse was characterised and mechanisms of tumour growth were assessed relative to the APC1322T model. Any differences in tumorigenesis were attributed to the presence of the C terminus of APC.
Results: Western blotting confirmed the presence of a mutant APC protein of the expected length in delta-SAMP mice. Intestinal tumour numbers, site of polyp development, cellular composition of polyps, parameters of tumour growth such as crypt fission, and levels of Wnt signalling, as measured with immunohistochemistry for nuclear beta catenin levels, were comparable with those seen in the APC1322T mouse, with no significant differences between the two models.
Conclusion: The C terminus of APC does not appear to have a significant effect on intestinal tumorigenesis. The action of the N terminus of mutant APC appears sufficient to account for the effects of mutant APC on tumorigenesis.
Inflammatory bowel disease free papers
SUSTAINED FISTULA HEALING AND RESPONSE WITH ADALIMUMAB FOR UP TO 2 YEARS IN PATIENTS WITH FISTULISING CROHN’S DISEASE: 12 MONTHS OF OPEN-LABEL MAINTENANCE WITH ADALIMUMAB FOLLOWING THE CHARM TRIAL
J. F. Colombel1, M. A. Kamm2, D. Schwartz3, W. J. Sandborn4, J. Li5, K. G. Lomax5, P. F. Pollack5. 1Hepatogastroenterology, CHU Lille, Lille, France, 2Gastroenterology and Medicine, St Mark’s Hospital, Harrow, UK, 3Inflammatory Bowel Disease Center, Vanderbilt University Medical Center, Nashville, TN, 4Gastroenterology, Mayo Clinic, Rochester, MN, 5Immunology Development, Abbott, Parsippany, NJ, USA
Introduction: Adalimumab (ADA), a fully human monoclonal antibody targeting tumour necrosis factor, is effective in the induction and maintenance of remission in patients with Crohn’s disease (CD). Fistulising disease complicates the course of CD in 20%–30% of patients and frequently leads to surgical resection. The efficacy of ADA in fistula closure and response was previously seen in the CHARM trial.1
Aims & Methods: We assessed the long-term efficacy of ADA in sustaining fistula healing and response in patients with fistulising CD. In the CHARM trial, patients were randomised to receive placebo, ADA 40 mg every other week (EOW), or 40 mg every week (EW). At or after Week 12, patients experiencing flare or non-response could receive open-label (OL) ADA. At the end of CHARM (56 weeks), patients were eligible to enrol in an OL extension during which they received ADA EOW OL or remained on ADA EW OL. In the extension trial, escalation from EOW to EW therapy was permitted for flares or non-response. Data from the two ADA dosage groups were pooled and evaluated using both non-responder imputation (data not shown) and last observation carried forward (LOCF) analyses. Endpoints were defined as complete healing or ⩾50% reduction of draining fistulas at time points since CHARM baseline.
Results: The percentage (%) of patients with healed fistulas and the % with ⩾50% fistula response at 6 and 12 months in the blinded study and at 6 and 12 months of the OL extension (up to 24 total months of ADA therapy) are presented in the table (LOCF analysis). Months 18 and 24 in the table represent 6 and 12 months in the OL extension after up to 12 months of blinded therapy in the CHARM trial.
Conclusion: Adalimumab has sustained fistula healing and response through 2 years of therapy. Nearly two thirds of the patients in the OL extension who had fistulas at baseline of CHARM showed continued response with ADA maintenance treatment, and more than half of ADA-treated patients experienced sustained fistula closure.
A RETROSPECTIVE ANALYSIS OF SMALL BOWEL MRI IN EVALUATION OF DISEASE ACTIVITY IN ILEAL CROHN’S DISEASE
C. W. Lees1, C. Parisinos1, D. Subedi2, A. G. Shand1, I. D. R. Arnott1, S. Glancy2, J. Satsangi1. 1Gastrointestinal Unit, 2Radiology Department, Western General Hospital, Edinburgh, UK
Introduction: Crohn’s disease (CD) patients frequently have ileal involvement (70%). Barium follow-through has been the standard investigation of the small bowel (SB), but is limited by lack of discrimination between inflammatory and fibrotic strictures and high radiation exposure. Small bowel magnetic resonance imaging (SBMRI) has recently been introduced as a tool for assessment of disease activity, and may impact on the therapeutic decision pathway of CD patients.
Aims & Methods: We aimed to assess the reliability of SBMRI in detecting disease activity and its influence on subsequent management. 186 patients had SBMRI performed at WGH from 2004–7. Patients were asked to drink 1.5 l hyper-osmolar water solution pre-MRI. 103/186 had SBMRI to investigate possible ileal CD. 75/103 had either known CD (Lennard-Jones criteria) or proven ileal CD at SBMRI and were included in the main analysis. A total of 86 SBMRIs were performed in these 75 CD patients. There were significantly more females in this cohort (73.4%, p<0.001). Case-notes were reviewed in detail with documentation of serum and faecal inflammatory markers and histopathology pre- and post-SBMRI. Agreement between inflammatory markers and SBMRI findings was determined with Cohen’s kappa statistic.
Results: 32/86 (37.2%) of SBMRIs showed active ileal CD and 41/86 (47.6%) quiescent CD, while 11/86 (12.7%) were suboptimal (inadequate ileal distension secondary to limited contrast ingestion). There was substantial agreement between active ileal CD on SBMRI and CRP (κ = 0.61, p = 0.0004), faecal calprotectin (κ = 0.72, p = 0.047) and histopathology (κ = 0.66, p = 0.0006). SBMRI had 75% sensitivity and 93% specificity for active CD when compared with histopathology. Management was influenced by SBMRI reports following active (29/34, 75% treated medically) or quiescent (19/27, 85.3% managed conservatively) disease. Fibrotic strictures were predominantly treated surgically (5/6, 83.3%). 3/8 patients with inflammatory ileal strictures required surgery; only 1/3 did not have a trial of medical therapy. Active colonic CD was identified on 6/86 (7.0%) SBMRIs. In addition, a total of 26 extraintestinal findings were detected in the 103 SBMRIs performed for possible ileal CD.
Conclusion: SBMRI provides accurate information on ileal CD activity, with close correlation to inflammatory markers and histopathology. It represents a substantial advance in the staging of CD, with the potential to direct medical and surgical management, while avoiding harmful radiation exposure in young patients.
GENE SPECIFIC HYPERMETHYLATION IN COLORECTAL MUCOSA OF PATIENTS WITH ULCERATIVE COLITIS
R. P. Arasaradnam1, K. T. J. Khoo1, D. M. Commane1, J. Mathers1, M. Bradburn2. 1Human Nutrition Research Centre, School of Clinical Medical Sciences, Newcastle University, 2Department of Surgery, Northumbria Healthcare NHS Trust, Newcastle, UK
Introduction: We have previously shown evidence of global DNA hypermethylation in patients with ulcerative colitis (UC) and accompanying low folate status.1 Epigenetic modifications such as gene specific methylation are thought to occur early in the multi-step pathway of colorectal carcinogenesis. For example, p16INK4a a tumour suppressor gene (inactivated in most human cancers including colon cancer) has been shown to be silenced as a result of promoter methylation.2 Similarly, ESR-1 a putative tumour suppressor gene has been shown to be hypermethylated in both colon cancer as well as UC3 but few studies exist on gene specific (tumour suppressor) methylation in UC.
Aims & Methods: To assess gene specific methylation of ESR-1 (oestrogen receptor-1) and N-33 (tumour suppressor candidate-3) in the macroscopically normal mucosa of UC patients. 68 subjects were recruited (24 UC patients and 44 age- and sex-matched controls). Colorectal mucosal biopsies were obtained and DNA extracted. Gene specific methylation was quantified using the COBRA method described by Xiong et al.4
Results: Mean duration of UC was 9 years with on average 1 flare-up/year and mean SCCAI score was 2. Percentage methylation of both ESR-1 and N-33 were significantly (p = 0.015 and p<0.001 respectively) higher in UC subjects compared with age and sex matched controls.
Conclusion: In this study, we have confirmed the observation of ESR-1 hypermethylation but in addition, demonstrated a novel finding of hypermethylation of another putative tumour suppressor gene, N-33, in UC subjects. This preliminary finding suggests perhaps an alternative pathway for colorectal carcinogenesis in UC—that is, inactivation through methylation of putative tumour suppressor genes. Ongoing work is being undertaken to determine if lifestyle factors such as smoking and diet influence gene specific methylation.
This study is funded by the Food Standards Agency (N12015).
PROSPECTIVE MRI TO GUIDE PERINEAL CROHN’S FISTULA TREATMENT WITH INFLIXIMAB, ADALIMUMAB AND THALIDOMIDE
S. C. Ng1, S. Plamondon1, A. Swatton1, A. Gupta2, M. A. Kamm1. 1Gastroenterology, 2Radiology, St Mark’s Hospital, London, UK
Introduction: Anti-tumour necrosis factor (TNF) therapies are effective in treating perineal fistulising Crohn’s disease. We prospectively evaluated the efficacy of infliximab, adalimumab and thalidomide in treating perineal fistulising Crohn’s disease, and assessed the value of MRI to determine deep healing and influence duration of treatment.
Aims & Methods: Infliximab naïve patients received infliximab, while patients who had previously failed infliximab received adalimumab or thalidomide. Clinical fistula evaluation was performed at baseline and each 8 weeks. MRI was performed at baseline and weeks 34 and 52. Clinical healing, MRI assessment of fistula track healing, Crohn’s Disease Activity Index (CDAI), and Perianal Crohn’s Disease Activity Index (PCDAI) were prospectively assessed.
Results: 34 patients with perineal fistulas (29 anorectal and 5 anovaginal) were included. Median follow-up to date was 44 weeks (range 22–93). 19 patients received infliximab, 7 had adalimumab and 8 had thalidomide. 30 patients had concurrent luminal disease. Concurrent thiopurine was used in 17 of 19 infliximab, 1 of 7 adalimumab, and 3 of 8 thalidomide- treated patients. Adalimumab-treated patients had previously failed infliximab: 4 lost response, 2 anaphylaxis, 1 no response. At week 22, response (more than 50% reduction draining fistulas) and complete fistula closure, respectively, was seen in 16 (84%) and 10 of 19 (53%) infliximab-treated patients, 4 (57%) and 1 of 7 (14%) adalimumab-treated patients, and 4 (50%) and 1 of 8 (13%) thalidomide-treated patients. Three patients on thalidomide stopped treatment at week 2 due to side effects. At week 34, 19 patients have had a repeat MRI. Of 15 patients with clinical response, MRI showed complete healing in 4, improvement in 8 and unchanged in 3 patients. Of 4 patients without clinical response, MRI showed improvement in 1 and unchanged in 3. At week 52, of 13 patients who have had a repeat MRI, fistulas remained healed in the same 4 patients who had healed at week 34, further improvement in 5, and unchanged in 4 patients, compared with MRI at week 34. Mean PCDAI reduced from 9 at baseline to 4 at last follow-up. Mean CDAI reduced from 257 at baseline to 152 at last follow-up (p<0.05).
Conclusion: Anti-TNF therapy is highly effective in treating perineal Crohn’s fistulas. Limited preliminary data suggest that MRI may indicate when treatment can cease. In keeping with previous findings in luminal disease, in fistulising disease the use of a second antibody is proportionally less effective than the first. Fistula tracks are slower to resolve than clinical remission. Prolonged treatment is often required to achieve internal track resolution.
THE SAFETY PROFILE OF INFLIXIMAB FOR INFLAMMATORY BOWEL DISEASE IN EDINBURGH: FINAL ANALYSIS OF OVER 200 PATIENTS
C. W. Lees1, A. Ali1, A. I. Thompson1, R. O. Forsythe1, L. Marquez1, S. Aitken1, J. Fennell1, P. Rogers2, A. G. Shand1, I. D. Penman1, K. R. Palmer1, D. C. Wilson2, I. D. R. Arnott1, J. Satsangi1. 1Gastrointestinal Unit, Western General Hospital, 2Department of Paediatric Gastroenterology and Nutrition, Royal Hospital for Sick Children, Edinburgh, UK
Introduction: The efficacy of infliximab therapy is established for Crohn’s disease (CD) and to a lesser extent ulcerative colitis (UC). However, serious adverse events have been reported. We therefore set out to review the short and long-term safety of all patients treated with infliximab at the Western General Hospital (WGH) and Royal Hospital for Sick Children (RHSC), Edinburgh from 1999 to 2007.
Aims & Methods: Data were available on 202 patients (182 WGH, 20 RHSC) comprising 157 (77.7%) CD, 42 (20.8%) UC, and 3 (1.5%) coeliac disease, who received a total of 718 infliximab infusions. The median age at diagnosis was 23 years, with median duration diagnosis to first infusion of 4.9 years. Patients had a median of 3 infliximab infusions (range 1–35), with a median 2.5 years follow-up. 59.4% of patients received induction therapy only, 20.7% induction plus episodic and 19.8% induction plus maintenance therapy. The primary outcome was the number of adverse events occurring in the 90 days following infliximab infusion. Serious adverse events were defined as fatal or life-threatening, or leading to/prolonging hospitalisation.
Results: There were a total of 95 adverse events in 58/202 (28.7%) of patients in the 90 days following infliximab, with 30/202 (14.9%) having a serious adverse event. Of a total of 7 deaths in this cohort, 6 were >1 year post-infliximab and considered unrelated. 42/202 (20.8%) had an infectious event of which 22 were serious. 6/202 (3.0%) patients were diagnosed with malignancy after infliximab therapy. There were 3 cases of lung cancer in current or ex-smokers, all >65 years at diagnosis. 27/202 (13.4%) of patients had an infusion reaction. 20 acute infusion reactions were recorded in 19 patients; 4/20 were serious, including 1 anaphylactic reaction requiring adrenaline. 8 serum-sickness reactions occurred; 3/8 were serious, requiring hospitalisation for iv steroids. The median longest duration between previous infusions was 895 days. One patient (15 years old, CD) developed severe drug-induced lupus.
Conclusion: Important safety considerations of infliximab were identified in this retrospective cohort and the risk/benefit analysis needs to be carefully assessed and discussed with patients before commencement of therapy.
COMMON POLYMORPHISM IN THE ALDEHYDE OXIDASE GENE IS A MARKER OF NON-RESPONSE TO AZATHIOPRINE THERAPY IN INFLAMMATORY BOWEL DISEASE
M. A. Smith1, T. Marinaki2, A. Ansari1, J. Sanderson1. 1Gastroenterology, 2Purine Research Laboratory, Guy’s and St Thomas’ NHS Foundation Trust, London, UK
Introduction: Azathioprine (AZA) and 6-mercaptopurine (6MP) remain the immunosuppressants of choice for inflammatory bowel disease (IBD). Their metabolism has been extensively studied and both are thought to be pro-drugs activated by conversion to 6-thioguanine nucleotides (6TGNs). There are reports of aldehyde oxidase (AOX) acting on AZA, 6MP and the products of their metabolism, but the role played by the metabolites produced has not been established. There is only one reported coding SNP in the AOX gene: 3404A>G (encoding the amino acid substitution Asn1135Ser) it has a reported gene frequency of 0.16. We set out to establish whether the presence of this SNP is associated with clinical outcome in IBD patients treated with AZA.
Aims & Methods: A cohort of 182 prospectively recruited patients starting 2 mg/kg AZA for IBD was divided into responders, non-responders and those discontinuing treatment due to side effects. The whole cohort was genotyped for the presence of the coding SNP in AOX using real-time PCR Taqman drug metabolism genotyping assay. Contingency tables, chi-squared testing, Fisher’s exact test and unpaired Student’s t test were used for statistical analysis. DNA sequencing was used to confirm the accuracy of the SNP probe.
Results: 58% of patients recruited had Crohn’s disease. 74 (41%) withdrew due to side effects, 66 (36%) had a complete response. The SNP AOX 3404A>G had an allele frequency of 0.12 in our population over all. The allele frequency in responders was 0.08, but in non-responders the allele frequency was 0.18. The presence of SNP AOX 3404A>G strongly predicted a lack of response to AZA treatment as a dominant effect (p = 0.007). Sequencing data has confirmed the accuracy of the SNP probe. Failure to respond to therapy could not be attributed to differences in TGN level which did not differ significantly between those with and without the SNP (p = 0.56). Likewise, TPMT was not significantly different between those with and without the AOX SNP (p = 0.27). Importantly patients with both AOX 3404A>G and a TPMT greater than 35 had the lowest chance of responding (27%) compared to 55% for those with one of these predictors of non-response and an 86% chance of responding for those with neither predictor (p = 0.0002).
Conclusion: We have identified a novel pharmacogenetic marker of non-response to AZA. Our findings suggest that the thiopurine metabolites generated by AOX action may be clinically significant and warrant further study. Furthermore and additive effect between AOX 3404A>G and high TPMT predicts a group unlikely to respond to thiopurine therapy.
CORTICOSTEROIDS INCREASE INTERLEUKIN-10 AND INHIBIT INTERLEUKIN-12P40 PRODUCTION BY INTESTINAL DENDRITIC CELLS IN ACUTE ULCERATIVE COLITIS: NOVEL MECHANISMS OF THERAPY
S. C. Ng1, S. Plamondon1, H. O. Al-Hassi1, M. A. Kamm2, S. C. Knight1, A. J. Stagg1. 1Antigen Presentation Research Group, 2Gastroenterology, St Mark’s Hospital, London, UK
Introduction: Intestinal dendritic cells (DC) interact with the luminal flora and play a key role in maintaining immune homeostasis. Altered DC function and dysregulated cytokine production contribute to the inappropriate recognition of bacteria that drives inflammation in inflammatory bowel diseases.1 2 Corticosteroids, widely used in the treatment of acute ulcerative colitis (UC), work in part by suppression of T cell activation,3 4 but their influence on DC, key inflammatory initiators, is unknown.
Aims & Methods: We assessed cytokine production by ex vivo colonic DC from patients with acute UC, and determined the effects of in vivo corticosteroids. Rectal biopsies were obtained from inflamed tissue of patients with active UC, symptomatic for less than four weeks (n = 30; sigmoidoscopy score more than 2) and healthy controls (n = 16). Myeloid DC were identified by multicolour flow cytometry as CD11c+ HLA-DR+ lineage- cells (lin = anti-CD3, 14, 16, 19 and 34) in lamina propria mononuclear cells extracted from collagenase digested intestinal tissue and compared with CD11c- cells within the same gate. “Spontaneous” interleukin (IL)-10, IL-12p40, IL-6, and IL-13 production by lamina propria DC was measured by intracellular staining of permeabilised cells in the absence of exogenous stimulation. In seven UC subjects, cytokine production by colonic DC was assessed before and after 8 weeks of oral steroid treatment.
Results: In acute UC a significantly greater proportion of colonic myeloid DC produced IL-10 and IL-12p40 than did equivalent cells from control tissue (p<0.05). In contrast, production of IL-6 and IL-13 by myeloid DC did not differ between UC patients and controls. Compared with myeloid DC, fewer CD11c- HLA-DR+ lineage-cells in UC patients and controls produced the cytokines examined. Following high dose corticosteroids, there was an increase in IL-10 production by colonic myeloid DC (p<0.05), and a reduction in IL-12p40 production by both colonic myeloid DC and CD11c- HLA-DR+ lineage-cells in UC patients (p<0.05). There were no significant differences in IL-6 and IL-13 production by DC before and after corticosteroids.
Conclusion: Acute UC is associated with enhanced colonic DC production of the regulatory cytokine, IL-10 and the proinflammatory cytokine, IL-12p40. Oral steroids suppress production of IL-12p40 and potentiate secretion of IL-10 by colonic DC. These findings provide new insights into the potential mechanism of glucocorticoid gut immunosuppression and therapeutic efficacy in inflammatory bowel disease.
EFFECTIVE PROBIOTIC TREATMENT (VSL#3), BUT NOT PLACEBO, IN ACUTE ULCERATIVE COLITIS IS ASSOCIATED WITH DOWN-REGULATION OF INFLAMMATORY INTESTINAL DENDRITIC CELLS
S. C. Ng1, S. Plamondon1, A. L. Hart1, M. A. Kamm2, S. C. Knight1, A. J. Stagg1. 1Antigen Presentation Research Group, 2Gastroenterology, St Mark’s Hospital, London, UK
Introduction: In active ulcerative colitis (UC) gut bacteria drive inflammation, and preliminary data suggest that probiotic bacteria are therapeutically effective. Gut dendritic cells (DC) are pivotal in early bacterial recognition and T cell signalling and probiotic bacteria cause decreased pro-inflammatory DC interleukin (IL)-12p40 and increased regulatory IL-10 production in vitro.1 2
Aims & Methods: As part of a double-blind, placebo-controlled, therapeutic study investigating the effect of the probiotic mixture VSL#3 (8 bacterial strains: 4 lactobacillus, 3 bifidobacteria, and 1 streptococcus) in acute UC, we studied for the first time how probiotics modify DC function ex vivo, and how this correlates with therapeutic efficacy. In patients with acute UC (UC disease activity index 3–8), rectal biopsies were taken at baseline and after 8 weeks of treatment with VSL#3 (n = 10) or placebo (n = 9). Using multicolour flow cytometry, myeloid DC were identified as CD11c+ HLA-DR+ lineage-cells (lin = anti-CD3, 14, 16, 19, 34) in freshly isolated lamina propria mononuclear cells from collagenase digested colonic tissue.3 Surface expression (level and proportion of positive cells) of the activation markers (CD40, CD86), pattern recognition receptors (Toll-like receptors (TLR), TLR-2 and TLR-4), and spontaneous IL-10, IL-12p40, IL-6, and IL-13 production by DC, measured by intracellular staining of permeabilised cells in the absence of exogenous stimulation, were measured before and after VSL#3 or placebo.
Results: More patients on VSL#3 responded to treatment, compared with placebo. In patients treated with VSL#3, proportion positive cells and level of CD86 expression by colonic myeloid DC was significantly reduced (p<0.05), TLR-2 expression on DC was downregulated (p<0.05), IL-10 positive colonic DC were significantly increased and IL-12p40 producing DC were significantly reduced (p<0.005). The level of expression of IL-12p40 was also significantly decreased (p<0.05). There were no significant changes in TLR-4, IL-6 and IL-13 after VSL#3. In patients who received placebo, colonic DC expressed significantly more TLR-2 on repeat sampling (p<0.05), but no significant changes were detected for CD40, CD86, TLR-4 or intracellular cytokines.
Conclusion: In acute UC, probiotic treatment with VSL#3 differentially modulates the function of human intestinal DC studied ex vivo, inducing regulatory cytokine and down-regulating co-stimulatory molecules and pro-inflammatory cytokines. These changes correlate with clinical improvement. Probiotic effects on DC may be central to their therapeutic effect in UC.
DIETARY N-3 POLYUNSATURATED FATTY ACIDS PROTECT AGAINST THE DEVELOPMENT OF ULCERATIVE COLITIS: A UK PROSPECTIVE COHORT STUDY
S. John1, R. Luben2, H. J. Kennedy1, A. Welch3, K. Khaw4, S. A. Bingham5, A. R. Hart1. 1Gastroenterology, Norfolk and Norwich University Hospital, Norwich, 2Department of Public Health, University of Cambridge, Cambridge, 3Population Health, University of East Anglia, Norwich, 4Clinical Gerontology, 5Cancer Sciences, University of Cambridge, Cambridge, UK
Introduction: The aetiology of ulcerative colitis is unknown, although it is plausible that dietary n-3 polyunsaturated fatty acids (n3-PUFAs) may have a protective role. Metabolites derived from these nutrients, which are found in the colonic mucosa of patients, are less proinflammatory than those derived from n-6 PUFAs.
Aims & Methods: As no prospective cohort studies have investigated this association, the aim of this study was to report the effects of both total dietary n-3 PUFAs and the specific n-3 PUFAs eicosapentaenoic acid (EPA)and docosahexaenoic acid (DHA) on the risk of ulcerative colitis. A total of 25 630 participants without ulcerative colitis, living in Norfolk UK, completed detailed 7-day food diaries. These were interpreted using a specifically designed computer programme which converted food items into nutrients including n-3 PUFAs. The cohort was monitored for participants who developed ulcerative colitis and the diagnosis was confirmed by experienced physicians. Each case was matched for age and gender with four controls and analyses performed using unconditional logistic regression.
Results: In the cohort, 22 cases of incident ulcerative colitis were identified after a median follow-up time of 4.2 years (range 1.8–8.3 years). Statistically significant protective odds ratios for trends across quartiles were found for: total n-3 PUFAs (OR 0.49, 95% CI 0.25 to 0.99), EPA (OR 0.52, 95% CI 0.28 to 0.99) and DHA (OR 0.40, 95% CI 0.20 to 0.79) after adjusting for age, gender, total energy intake and cigarette smoking. These protective associations persisted after adjusting for n-6 PUFAs which can affect the metabolism of n-3 PUFAs.
Conclusion: Total dietary n-3 PUFAS, EPA and DHA are significantly associated with protection from the development of ulcerative colitis. This association needs to be investigated in other cohort studies to see if the effect is consistent. If the association is causal, then increasing the intake of n-3 PUFAs in the population should be helpful in reducing risk of ulcerative colitis.
MONITORING AZATHIOPRINE TREATMENT IN INFLAMMATORY BOWEL DISEASE: RITUALS RE-VISITED—BUT NOT REVISED!
M. Walsh, C. Royston, M. Srinivas, B. Hoeroldt, P. J. W. Willemse, P. Basumani, K. D. Bardhan. Gastroenterology, Rotherham General Hospital, Rotherham, UK
Introduction: Inflammatory bowel disease (IBD) patients on long-term AZA routinely have their haematology (± biochemistry) monitored regularly,1 a time consuming process often inconvenient to patients otherwise well.
Aims & Methods: Our aim was to assess if such monitoring is effective. All patients with IBD were followed-up, their data prospectively updated at each visit and later transferred to our electronic database. AZA starting dose was generally 50 mg (n = 205). Full blood count (FBC) and liver function tests (LFT) were routinely checked at baseline, 1, 2, 4, 8 and 12 weeks and 3 monthly thereafter if in remission and whenever an untoward event or unscheduled visit occurred. The process was repeated whenever dosage was increased. Thiopurine methyl transferase (TPMT) levels (introduced 1999) were checked whenever possible before starting AZA.
Results: Numbers treated: Crohn’s disease 141/339 (42%), ulcerative colitis 103/393 (26%), indeterminate colitis 10/50 (20%), total 254/782 (32%). Adverse Events (AE) occurred in 122/254 (48%) of patients and usually led to the withdrawal of AZA. AE were independent of disease type hence pooled data are presented. Type of AE: 81/122 patients (66%) had constitutional disturbance (CONS) alone; 25 (20%) had silent FBC or LFT changes; 15 (12%) had both. CONS (total 96) included GI and/or influenza-like symptoms in 64. FBC changes (17) included falling total white cell or neutrophil count in 12; none had neutropenic crisis. LFT changes occurred in 24. 1 patient had FBC and LFT changes. Separately, 1 patient developed myeloma after 8 years. Dose vs time: 91 patients developed AE on the 50 mg dose and the majority of AE, irrespective of dose, occurred early (⩽3 m). Most late constitutional but only half of late FBC changes were associated with dose increase. TPMT: Tested in 157/254. Normal/high n = 134, intermediate/carrier n = 23. AE occurred in 56% and 57% respectively. None had severe deficiency.
Conclusion: (1) AZA associated AE were common, independent of starting dose, IBD type or TPMT levels (carrier or normal). (2) The majority of constitutional events and LFT changes occurred early in treatment. In contrast FBC changes were spread over time. (3) Most late AE followed dose increase. (4) The yield of clinically useful information from regular monitoring diminished markedly after a year of stable dose. The infrequency of late events gives us much reassurance. Nevertheless we are concerned with the unforeseen consequences of prolonged immunosuppression, therefore, our “ritual” of close monitoring remains unchanged.
Liver free papers
EUROPEAN LIVER FIBROSIS MARKERS CAN PREDICT CLINICAL OUTCOME IN PATIENTS WITH CHRONIC LIVER DISEASE
J. Parkes1, P. Roderick2, S. Harris2, C. Gough3, M. Wheatley2, G. Alexander4, J. Collier5, C. Day6, M. Lombard7, D. Mutimer8, J. Ramage9, G. Dusheiko10, A. Burt11, E. Sampson12, W. Rosenberg13. 1Public Health Sciences and Medical Statistics, University of Southampton, 2Public Health Sciences and Medical Statistics, University of Southampton, 3Wellcome Clinical Research Facility, Southampton General Hospital, Southampton, 4Department of Hepatology, Addenbrooke’s Hospital, Cambridge, 5Department of Gastroenterology, John Radcliffe Hospital, Oxford, 6Department of Hepatology, Freeman Hospital, Newcastle upon Tyne, 7Department of Gastroenterology, Royal Liverpool & Broadgreen Hospital, Liverpool, 8Department of Hepatology, Queen Elizabeth Hospital, Birmingham, 9Department of Gastroenterology, N Hants Hospital, Basingstoke, 10Department of Hepatology, Royal Free and University College School of Medicine, London, 11Department of Histopathology, Freeman Hospital, Newcastle upon Tyne, 12Siemens Diagnostics, Siemens, Tarrytown NY, United States, 13Institute of Hepatology, University College London, London, UK
Introduction: When attempting to predict clinical outcomes of liver disease clinicians use the surrogate of fibrosis in a liver biopsy as a reference standard. Performance of non-invasive tests as predictors of clinical outcomes has been evaluated against fibrosis on biopsy but use of clinical outcomes as the reference standard would be ideal. The ELF panel of markers (TIMP1, HA, PIIINP) was derived and validated in a cohort of patients recruited in 1998–9 and shown to have excellent ability to identify significant fibrosis on biopsy. To evaluate ELF performance in predicting clinical outcomes, the original ELF cohort was followed-up at 8–9 years.
Aims & Methods: Patients recruited to the ELF study at 7 English centres were followed up for liver morbidity and mortality by examination of clinical data. Those lost to follow-up were followed up for morbidity by questionnaires to the GP. All deaths were ascertained and death certificates were obtained. Primary outcome measure was liver related morbidity/death; secondary outcome was all-cause mortality.
Results: 498 patients were followed up after a median of 6.7 (0.3–9.1) years. The median age = 43 years (19–75), 66% male, 42% CHC. 41% were lost to follow-up/discharged. 85% of GP questionnaires were returned reporting no liver outcomes. There were 67 liver-related outcomes (39 liver-related deaths), 70 deaths overall. Kaplan Meier plots showed that tertiles of baseline ELF score can predict liver outcomes and all-cause mortality (log rank test p<0.001) Cox proportional hazards analyses show that ELF remains predictive when adjusted for age, gender and disease aetiology (p<0.0001); adjusted HR for the middle tertile ELF score versus lowest tertile ELF score = 6, and for highest tertile ELF score versus lowest tertile HR = 29. From logistic regression at 6 years follow-up the OR for liver related outcome was 2.14.
Conclusion: ELF score can predict clinical outcomes in patients with CLD and is likely to be a useful prognostic tool. A unit change in ELF score is associated with a doubling of the odds of getting a clinical outcome at 6 year follow-up.
HIGHLY EFFICIENT DIFFERENTIATION OF HUMAN EMBRYONIC STEM CELLS TO FUNCTIONAL HEPATOCYTES IN VITRO AND IN VIVO REQUIRES ACTIVIN A AND WNT3A SIGNALLING
D. Hay1, J. Fletcher1, C. Payne1, J. Terrace1, R. Gallagher1, J. Black1, A. Pryde1, C. Filippi1, S. Forbes1, K. Samuel1, J. Ross1, J. Iredale2, P. N. Newsome3. 1Centre for Regenerative Medicine, 2Centre for Inflammation Research, University of Edinburgh, Edinburgh, 3Institute of Biomedical Research, University of Birmingham, Birmingham, UK
Introduction: Human embryonic stem cells (hESC) are a potentially valuable source of human hepatocytes, although their homogeneous differentiation to specific germ layers/cell types has proven difficult to achieve. Wnt signalling pathways have been shown to play important roles in development and cellular differentiation in vivo.
Aims & Methods: Our aim was to define the role of Wnt signalling in hepatic development and its effect on the hepatocytic differentiation of hESC. Wnt3a expression was examined in first (T1) and second (T2) trimester liver sections by immunostaining. We used cytokine combinations of Wnt, Activin A and Sodium Butyrate to direct hESC towards the hepatocyte lineage. Hepatocyte phenotype was confirmed by immunofluorescent staining and metabolic assays. Hepatocyte-like cells (hESHs) were injected (1×106 cells) intrasplenically (IS) or intrahepatically into NOD-scid mice. Functionality was confirmed by histological analysis and measurement of human albumin in serum.
Results: T1 liver exhibited Wnt3a staining adjacent to developing portal structures, but was not detected in the parenchyma. However, in T2 livers the pattern of expression was both portal and parenchymal suggesting that Wnt3a parenchymal expression correlated with hepatocyte differentiation in the developing liver, and may play a role in early hepatocyte differentiation. After 10 days culture hESC expressed a wide range of hepatocytic genes (albumin, AFP, HNF4a, tyrosine aminotransferase, tryptophan oxygenase, apolipoprotein F and cytochrome p450 3A4) and proteins (Albumin, Glycogen storage). The final population of hESHs was 90% pure as assessed by albumin and HepPar1 expression. Metabolic function was confirmed by urea synthesis (0.9 μmol/h/g TP), Gluconeogenesis (1.5 μmol/h/g TP) and p450 metabolism. We have been able to direct the hepatocytic differentiation of hESC using standard culture methodology and also from clonal cell lines. After IS injection hESHs were seen in the murine liver and spleen, expressed albumin and cytokeratin 18/19 and were seen to be cycling (Ki67 expression). These cells produced albumin which was detected in murine serum (10 μg/ml).
Conclusion: (1) We demonstrate that Wnt3a is expressed at critical stages of human liver development in vivo, highlighting its important role in development. (2) Wnt3a directed differentiation of hESC results in a functional, highly homogenous population of human hepatocytes which function in vitro and in vivo studies.
HOSPITALISATION OF HEPATITIS C DIAGNOSED PERSONS IN SCOTLAND FOR DECOMPENSATED CIRRHOSIS: A POPULATION-BASED RECORD-LINKAGE STUDY
S. A. McDonald1, S. Hutchinson2, S. Bird3, P. Mills4, J. Dillon5, P. Hayes6, C. Robertson7, D. Goldberg2. 1BBV-STI Section, 2Health Protection Scotland, Glasgow, 3MRC Biostatistics Unit, Institute of Public Health, Cambridge, 4Gartnavel General Hospital, Glasgow, 5Ninewells Hospital & Medical School, Dundee, 6Edinburgh Royal Infirmary, Edinburgh, 7Department of Statistics and Modelling Science, University of Strathclyde, Glasgow, UK
Introduction: Few studies have examined progression to the decompensated stage of cirrhosis in hetereogenous populations of persons infected with the hepatitis C virus (HCV). We investigated hospitalisation for decompensated cirrhosis among all individuals who have been diagnosed with HCV in Scotland.
Aims & Methods: The population studied consisted of 20 969 individuals diagnosed with hepatitis C through laboratory testing in Scotland between 1991 and 30 June 2006. These data were linked to other national databases on (1) all in-patient hospital discharges to retrieve episodes with discharge diagnoses of cirrhotic complications or hepatic failure (ICD-10: R18, I850, I982, K721, K729, K704, K709), and (2) all HIV tests to determine HIV co-infection status.
Results: 1027 individuals were admitted to hospital for the first time with decompensated cirrhosis during the follow-up period. The number of first-time admissions increased over the period 1996–2005, with an average annual change of 10.3%. The relative risk of hospitalisation was significantly greater for males (hazard ratio 1.3, 95% CI 1.1 to 1.6), for those with a previous alcohol-related hospital admission (hazard ratio = 5.7, 95% CI 4.7 to 6.9), for HIV co-infected persons (hazard ratio 1.6, 95% CI 1.0 to 2.5), and for those aged over 30 years (30–39: hazard ratio 3.6, 95% CI 2.3 to 5.6; 40–49: hazard ratio 10.1, 95% CI 6.5 to 15.7; 50–59: hazard ratio 17.8, 95% CI 11.1 to 28.6; 60+: hazard ratio 29.5, 95% CI 17.7 to 49.1).
Conclusion: The burden to the Scottish healthcare system from HCV-infected persons developing cirrhotic complications is increasing, due to the advancing age of this Scottish HCV-diagnosed population. Of the epidemiological risk factors examined, a history of alcohol-related hospitalisation was most strongly associated with progression to decompensated cirrhosis. A greater proportion of HCV-infected individuals needs to be identified, treated and educated about the importance of minimal alcohol consumption to achieve a greater impact on the morbidity of this disease.
EARLY LIVER BIOPSY IS CRUCIAL FOR ACCURATE DIAGNOSIS OF ALCOHOLIC HEPATITIS AND PROVIDES INDEPENDENT PROGNOSTIC INFORMATION IN PATIENTS WITH DECOMPENSATED ALCOHOLIC LIVER DISEASE
R. P. Mookerjee1, C. Lackner2, V. Stadlbauer1, R. Williams1, R. Jalan1. 1Hepatology, Institute of Hepatology, UCL, London, UK, 2Institute of Pathology, University of Graz, Graz, Austria
Introduction: Severe alcoholic hepatitis (AH) has a high mortality and accurate diagnosis is essential to allow appropriate intervention. Selecting patients for anti-inflammatory therapy without increasing risk of sepsis has proved difficult through inaccurate diagnosis of AH.
Aims & Methods: This study questioned the importance of liver biopsy in diagnosing AH in decompensated alcoholic cirrhosis and applied a histological score to see if this would identify patients with the highest mortality. Methods: Patients were studied with an appropriate alcohol history presenting acutely with decompensated alcoholic liver disease, and excluded if they had known additional liver pathology or culture positive infection within 72 hours of admission. All patients had a liver biopsy within 3-days of admission, graded 1–5 for alcoholic steatohepatitis: (0: no AH; 1: ballooned hepatocyes comprising <5% of parenchyma and no inflammatory cells (mononuclear/neutrophils); ranging up to grade 5: ballooned hepatocytes comprising >50% of parenchyma and moderate to many inflammatory cells). Hepatocyte balloon degeneration was also verified immunohistochemically by loss of cytoplasmic keratin 8 and 18 staining.
Results: 37 patients were graded as having no significant steatohepatitis (score 0–1) despite 18 patients having elevated systemic inflammatory response syndrome components (SIRS- possibly reflecting underlying infection), and 62 had features of established cirrhosis. 19 patients died, 6 with no significant AH. Cytokeratin 8/18 staining to qualify balloon degeneration in a subset of 21 AH+ve patients, showed a good correlation with steatohepatitis grade (r = 0.83, p<0.0001). The odds ratio (95% CI) for mortality in patients with AH was 4.3 (1.4 to 13.6) and for SIRS 7.6 (1.9 to 30). There was a significant difference in mortality in patients with and without SIRS and AH (p<0.01). In SIRS positive patients, discriminant function and Child score had no significant association with outcome.
Conclusion: Liver biopsy is crucial for the diagnosis of alcoholic hepatitis. Clinical assessment and the use of SIRS overestimates AH, whilst its diagnosis is missed in a proportion of decompensated patients without SIRS. Histological grading of AH has prognostic value independent of SIRS, which may help define treatment strategy.
CURRENT MEASUREMENTS OF RENAL FUNCTION DO NOT REFLECT TRUE GLOMERULAR FILTRATION: A COMPARISON OF STANDARD AND NOVEL MARKERS OF RENAL FUNCTION IN PATIENTS UNDERGOING LIVER TRANSPLANT ASSESSMENT
A. J. Portal1, M. McPhail1, I. Coltart1, M. Bruce1, S. Hughes1, N. Taylor1, R. Sherwood2, J. O’Grady1, N. Heaton1, M. A. Heneghan1. 1Institute of Liver Studies, 2Department of Biochemistry, Kings College Hospital, London, UK
Introduction: Renal dysfunction in cirrhotic patients is associated with significant mortality both pre and post transplantation. Creatinine clearances of <70 ml/min/1.73 m2 are associated with decreased survival following liver transplantation. Serum creatinine (SCr) is a poor reflection of glomerular filtration rate (GFR) and therefore novel methods of assessing GFR using Cystatin C (CyC) and estimated GFR (eGFR) have previously been investigated. We compared these methods against SCr and a new biomarker, neutrophil gelatinase associated lipocalin (NGAL), in 79 patients undergoing assessment for liver transplantation.
Aims & Methods: Data from 79 patients undergoing LT assessment were prospectively collected at the time of assessment. Renal function was measured by 24-hour urinary creatinine clearance (CrCl). NGAL and CyC were retrospectively analysed on stored samples. eGFR was calculated using the MDRD equation. Renal dysfunction was defined as a CrCl of <80 ml/min/1.73 m2. Results are expressed as medians and interquartile ranges.
Results: There were significant (p<0.001) correlations between CrCl and 1/NGAL (r = 0.6), CyC and eGFR (r = 0.58). The relationship between SCr and CrCl was less apparent. In patients with renal dysfunction, median SCr was within normal laboratory limits (99 mmol/l (84–130)) and 85 mmol/l (73–97, p = 0.001) in those without. Median values in those with and without renal dysfunction were: eGFR were 62 ml/min/1.73 m2 (49–82) vs 94 (81–104), p<0.001; NGAL 121 ng/ml (59–246) vs 73(48–104), p = 0.016; CyC 1.32 mg/l (0.9–1.67) vs 0.95 (0.74–1.07), p<0.001. In patients with Childs B or C cirrhosis, median SCr remained within normal limits even when CrCl was reduced to <45 ml/min/1.73 m2 (102 mmol/l (99–177)). Both CyC and NGAL were elevated outside of normal reference ranges. In patients with a CrCl of <80 ml/min/1.73 m2, eGFR of <74 ml/min/1.73 m2 had the highest receiver operator characteristic area under the curve (AUC 0.83, sensitivity 66%, specificity 93%, p<0.001). However, in those with lower GFRs, CyC and NGAL more accurately predicted low GFR than eGFR or SCr (CrCl <ml/min/1.73 m2: CyC >1.45 mg/l AUC0.85, sensitivity 80%, specificity 82%, p<0.001; NGAL >101 ng/ml AUC 0.8, sensitivity 91%, specificity 69%, p<0.001; eGFR and SCr AUC 0.78).
Conclusion: Normal SCr values do not accurately represent glomerular filtration as measured by urinary creatinine clearance. Both CyC and NGAL have good predictive value especially in patients with more severely impaired renal function. They also have the advantage of being elevated prior to a rise in SCr, making them useful screening tests in both the pre- and post-transplant period.
SILENCING TIMPS WITH SIRNA: DEFINING A ROLE FOR TIMP-1 IN HEPATIC STELLATE CELL PROLIFERATION
A. J. Fowell1, W. M. C. Rosenberg2, R. C. Benyon1. 1Liver and Pancreas Research Group, Division of Infection, Inflammation and Repair, University of Southampton, Southampton, 2Institute of Hepatology, University College London, London, UK
Introduction: Tissue inhibitors of metalloproteinase (TIMP)-1 and -2 may play a key role in hepatic fibrogenesis both by protecting extracellular matrix from matrix metalloproteinase (MMP) mediated degradation and by supporting survival of fibrogenic myofibroblastic hepatic stellate cells (HSC) which are pivotal to liver fibrosis. HSC are the major source of TIMPs during chronic liver injury, and both TIMPs and HSC represent important potential therapeutic targets.
Aims & Methods: Our aim was to investigate the phenotypic effect of silencing TIMP-1 and -2 in HSC using small inhibitory RNA (siRNA). Culture-activated rat HSC were transfected with TIMP-1 and -2 siRNA or a negative control siRNA by electroporation. Cell lysates and culture supernatants were collected to quantitate TIMP-1 and -2 mRNA and protein by real-time PCR and ELISA, respectively. Potential toxicity of siRNA electroporation was assessed by lactate dehydrogenase activity assay. Conditioned media from siRNA treated HSC were tested for their ability to inhibit the activity of recombinant active matrix metalloproteinase-2 (MMP-2) using a collagenase activity assay. HSC proliferation following siRNA mediated TIMP silencing was determined by [3H]-thymidine incorporation in serum-containing media.
Results: TIMP-1 and -2 siRNA electroporation was an effective means of silencing HSC TIMP expression. At 24, 48, 72 and 192 hours after electroporation, TIMP-1 siRNA induced 91%, 92%, 86% and 45% knockdown of TIMP-1 protein expression respectively, compared with negative control siRNA (p<0.05 at 24–72 h). TIMP-2 siRNA induced 24%, 41%, 63% and 57% knockdown of TIMP-2 protein at the same time points (p<0.05 at 48–72 h). Similar silencing was seen at the mRNA level. There was no excess toxicity in TIMP-1 siRNA treated cells compared with electroporation alone and no effect on TIMP-2 protein. Conditioned media from TIMP-1 and TIMP-2 siRNA treated cells showed 40% and 25% less inhibition respectively of MMP-2 collagenase activity than media from negative control siRNA treated cells, verifying that TIMP silencing removed a functionally important MMP-suppressive effect in HSC cultures. TIMP-2 knockdown had no effect on proliferation, whereas silencing of TIMP-1 produced a significant (p<0.05) 40% reduction in HSC proliferation.
Conclusion: These data suggest that siRNA are an effective means of silencing functional TIMP-1 and -2 activities in HSC. A novel autocrine mitogenic effect of TIMP-1 on HSC has been defined, and this effect might promote liver fibrosis in addition to TIMP-1’s previously described anti-apoptotic effect on HSC. Furthermore, siRNA targeting TIMP-1 may offer potential as a hepatic anti-fibrotic therapy.
ADRENAL INSUFFICIENCY IN PATIENTS WITH AOCLF ADMITTED TO INTENSIVE CARE. A SINGLE UNIT EXPERIENCE
M. J. Austin, A. J. Portal, I. Coltart, L. Sizer, G. Auzinger, W. Bernal, J. Wendon. Liver Intensive Care Unit, Kings College Hospital, London, UK
Introduction: Adrenal insufficiency (AI) is common in critically ill patients with septicaemia, having significant impact on prognosis.1 Patients with acute on-chronic liver failure (AoCLF) have a marked systemic inflammatory response (SIRS), and increased susceptibility to infection.2–4 This study was designed to determine prevalence of adrenal insufficiency, vasopressor requirements, severity of illness, and survival in a large cohort of patients with AoCLF admitted to intensive care.
Aims & Methods: All patients with AoCLF admitted to liver ITU (LITU) between November 2000 and June 2007 were eligible for the study. Cirrhosis was confirmed by histological or clinical, biochemical and radiological evaluation. Routine admission biochemical and physiological parameters were recorded allowing calculation of APACHEII, SOFA, MELD and CP score. AI was determined by short synacthen test (SST). This involved measurement of serum cortisol at time 0 (T0), and at time 30 (T30) and 60 (T60) min following injection of 250µgs of ACTH (synacthen). Requirements for inotropic support, severity of illness and survival were noted. Results expressed as n (%) or median (IQR).
Results: 259 patients underwent SST on admission to LITU; 160 (62%) male and 119 (46%) admitted with alcohol-related chronic liver disease. Median age 49 years (40–58), 50 (19%) admitted with encephalopathy, 62 (24%) with sepsis and 66 (25%) with variceal bleeding (VB). Mortality 73%. Median T0 cortisol 370 nmol/l (250–541), T30 cortisol 531 nmol/l (382–702). 82 (32%) required inotropes. ApacheII score 24 (18–29), SOFA score 10 (8–13), Child Pugh score 12 (11–13) and MELD score 28 (20–34). Those with AI: 64 (25%) were more likely to be admitted with multi-organ failure (MOF) SIRS (p = 0.05), treated with steroids (p<0.001) and require inotropic support p = 0.014. Serum albumin and lipid profile were no different between those with or without AI. LITU and 3-month survival was not related to presence of AI.
Conclusion: Adrenal dysfunction is common in patients with AoCLF. Those with AI are more likely to present with MOF or SIRS and require inotropic support. Survival and severity of illness were no different between those with or without AI.
IDENTIFICATION OF BIOMARKERS THAT MEASURE DISEASE ACTIVITY IN PATIENTS WITH NON-ALCOHOLIC FATTY LIVER DISEASE
R. Malik1, M. Lai1, K. Bhaskar1, I. Nasser2, M. Curry1, D. Schuppan1, N. Afdhal1. 1Liver Center, Department of Medicine, 2Histopathology Department, Beth Israel Deaconess Medical Center Harvard Medical School, Boston, USA
Introduction: Non-alcoholic fatty liver disease (NAFLD) is a heterogenous group of disorders ranging from simple steatosis to non-alcoholic steatohepatitis (NASH).
Aims & Methods: We characterised a group of NAFLD patients to determine the predictive value of serum markers to identify histological NASH. We assessed demographic, serological, radiological and histological variables on 95 consecutive patients with NAFLD. Diagnostic criteria for NAFLD included an alcohol intake less than 175 g/week, negative hepatitis serology and liver biopsy with greater than 10% lipid content. The serum markers assessed were CK 18 a marker of apoptosis and markers of liver fibrogenesis hyaluronic acid, TIMP 1 and YKL 40.The two tailed t test was used for parametric variables and the χ2 test for categorical variables with differences reported if p<0.05. The clinical performance of each significant variable was assessed using the area under the ROC curve.
Results: The NAFLD cohort of patients was initially stratified according to the degree of necroinflammation into simple steatosis (NAS 1–3) vs NASH (NAS score 4–8). Severe necroinflammation/NASH was associated with type 2 diabetes and high serum ALT levels. CK 18 levels were significantly higher in the NASH group compared to the simple steatosis group (394+53 u/l cf 194+26 u/l; p<0.05). There were no differences between groups in the levels of markers of liver fibrogenesis. CK 18 performed the best at identifying NASH patients yielding an AUC of 0.8, with a cut-off value of 350 u/l giving a PPV of 84% and NPV of 81%. Subsequently, we stratified the NAFLD cohort according to the degree of liver fibrosis into Metavir F0 vs F1–F4. Fibrosis was associated with advanced age, high BMI, type 2 diabetes and a high NAS score (NAS 4–8). There were significantly higher levels of CK 18 (372+49 u/l cf 206+31 u/l; p<0.05), hyaluronic acid (64+11 ng/ml cf 20+2.5 ng/ml; p<0.05) and YKL 40 (125+13 ng cf 79+10 ng/ml; p<0.05) in the fibrosis group compared to the control group. A high NAS score of 4–8 performed the best at predicting fibrosis yielding an AUC of 0.9.
Conclusion: These results indicate that CK 18 levels reflect both severity of inflammation and subsequent fibrosis in NASH, where as HA and YKL 40 exclusively mirror fibrosis/fibrogenesis. CK 18 can be used as a surrogate biomarker to assess disease severity in patients with non-alcoholic fatty liver disease.
PREVALENCE AND DETERMINANTS OF PRIMARY SCLEROSING CHOLANGITIS IN A COHORT OF PATIENTS WITH INFLAMMATORY BOWEL DISEASE AND NORMAL LIVER FUNCTION TESTS
H. K. Bungay1, O. C. Buchel2, F. Cummings2, S. P. L. Travis2, R. W. G. Chapman2. 1Radiology Department, 2Gastroenterology Department, John Radcliffe Hospital, Oxford, UK
Introduction: Primary sclerosing cholangitis (PSC) is the most frequent hepatobiliary disease associated with ulcerative colitis (UC), and is diagnosed in 2.1–4% of cases. Alkaline phosphatase is usually elevated, but may be normal in 8.5% of patients in large case series. Magnetic resonance cholangiopancreatography (MRCP) is the established method for the diagnosis of PSC. The prevalence of PSC in patients with IBD and normal serum liver enzymes is unknown.
Aims & Methods: The aim of this study was to investigate the prevalence and possible determinants of PSC in a cohort of patients with IBD and normal serum levels of liver enzymes. 58 patients with colitis and normal serum liver enzymes, recruited from the IBD clinic consented to having an MRCP. Of these, 51 had an MRCP. Demographic, lifestyle, medical and laboratory data were collected retrospectively from existing case notes. 9 volunteers without IBD and with normal serum liver enzyme levels, had MRCP examinations, and served as a control group. Variables analysed included age at MRCP investigation, duration of IBD at time of MRCP, gender difference, smoking status, Azathioprine use and presence or absence of extra-intestinal manifestations. Continuous data (age and disease duration) were compared using the student t test. Other variables were analysed using the χ2 test.
Results: All MRCP examinations in the control group were normal. The study group consisted of 32 men (63%) and 19 women (37%), aged 18 to 84 years (median age 48 years). 45 patients had pan UC, 2 Crohn’s colitis, 2 right sided colitis, 1 distal colitis and 1 pan colitis yet to be classified. Of the 51 patients, 9 (18%) had biliary abnormalities consistent with PSC on MRCP examination. There was no difference between the mean age of patients with and without PSC respectively (53.4 vs 48.4, p = 0.435). Similarly duration of IBD did not differ significantly between the two groups (17.7 vs 12.0 years, p = 0.390). The prevalence of PSC in females was 6/19 (32%) and 3/32 (9%) in males (p = 0.053, OR for males 0.224, 95% CI 0.048 to 1.038). 2/4 (50%) of active smokers had PSC as opposed to 6/41 (16%) of those not currently smoking (NS, p = 0.624). Only 2/19 patients (11%) who had ever been treated with Azathioprine had PSC, with those never receiving the drug having PSC in 7/28 (25%) of cases (NS, p = 0.197). 5/19 (26%) patients with extra-intestinal manifestations had PSC as compared to 3/26 (12%) without extra-intestinal manifestations (NS, p = 0.188). No patient has yet had a liver biopsy.
Conclusion: 18% patients with normal liver enzymes and colitis had appearances consistent with PSC on MRCP. There was a trend for more females to have the appearances of PSC, but this did not reach significance. This study suggests that PSC may be more prevalent than appreciated in patients with IBD.
STANDARDISED MORTALITY RATIO IN AUTOIMMUNE HEPATITIS
B. S. Höeroldt1, E. McFarlane2, M. Campell3, P. Basumani1, M. Karajeh2, D. Gleeson2. 1Gastroenterology, Rotherham General Hospital, Rotherham, 2Hepatology, Royal Hallamshire Hospital, 3Medical Statistics Group, School for Health and Related Research, Sheffield, UK
Introduction: The long-term outlook of autoimmune hepatitis (AIH) treated with immunosuppression is considered to be good, although follow-up data beyond 10 years are limited. We have previously reported substantial 20-year all-cause (45%) and liver-related (24%) mortality rates in AIH, despite >90% initial remission rate; however, age at presentation (median 57 years) was older than in other series. 222 patients with definite (n = 147) or probable (n = 75) AIH by International AIH Group criteria presenting to Liver Unit over 1971–2005. Capture of cases presenting since 1987 (n = 177) is thought to be near complete. 182 patients (82%) were referred directly from primary care.
Aims & Methods: To assess whether mortality in this cohort is higher than that expected for the general population. Standardised mortality ratios (SMRs), using age- (10 year blocks) and gender-specific life expectancy tables for the population of Yorkshire and Humberside were calculated.
Results: During follow-up for median (range) 9.2 (0.2–34) years, 9 patients had a liver transplant, 2 of whom subsequently died. 23 other patients died from liver disease without transplant and 1 from probable immunosuppressive drug toxicity. Reasons for not transplanting were: advanced age+cormorbidity (n = 9, age 72–79 years), major comorbidity (n = 8), advanced hepatoma (n = 2), cause unclear (n = 4). 35 other patients died, from non-liver related causes. 145 of the remaining 154 patients were alive without transplant on 31/12/05 and 9 were lost to follow-up. Overall SMR (n = 222), considering all-cause deaths and liver transplants was 1.88 (95% CI 1.42 to 2.33). SMR was similar: 1.87 (1.31 to 2.44) in patients presenting since 1987 (n = 177, presumed consecutive series). Overall SMR (n = 222) was not much reduced: 1.68 (1.22 to 2.13) when only actual deaths were considered (transplant not considered as death). SMR for non-liver-related death alone was close to unity: 0.97 (0.51 to 1.43); thus, most of the excess mortality is due to liver disease. The excess of all-cause deaths (including transplants) (A): persisted after the first decade of follow-up: SMR 1.92 (1.32 to 2.53) and 1.75 (1.02 to 2.49) for first and second decade respectively (B): was higher in patients presenting at a younger age: SMR 9.79 (3.9 to 15.7) if <45 years, 2.00 (1.24 to 2.75) if 45–65 years and 1.38 (0.87 to 1.89) if >65 years at presentation and (C): whilst higher in patients (n = 76) with cirrhosis at presentation (SMR 2.51 (1.62 to 3.40), was also present in patients (n = 145) without (SMR 1.53 (1.02 to 2.04).
Conclusion: Despite a good initial response to immunosuppression and despite the potential availability of liver transplantation, mortality in patients with AIH is higher than in the general population. This excess is due to liver disease and is relatively greater in those presenting at a younger age.
Interactive case presentations
AN UNUSUAL CAUSE OF RECURRENT CHEST PAIN
J. R. A. Skipworth1, A. Humphries2, B. Patel1, F. Hughes1. 1Department of Upper GI Surgery, Royal London Hospital, 2Research Fellow, Cancer Research UK, London, UK
Introduction: A 55-year-old man presented to the casualty department, with chest pain and vomiting. 8 months after this episode, he represented with similar symptoms. On both occasions, he was critically ill with clinical signs of septic shock. Further investigation revealed raised inflammatory markers, haemoconcentration, raised serum urea and positive chest radiograph findings (pneumothorax, pleural effusion, pneumomediastinum). We describe the strategies utilised in the multidisciplinary management of this patient’s recurrent condition.
Aims & Methods: Prospective assessment and collection of data, during the patient’s in-hospital stay, was undertaken, and combined with retrospective analysis of the patient’s notes, laboratory results and radiological images. A summary of the case is presented, together with a discussion of the literature.
Results: A combination of clinical, radiological, endoscopic and operative techniques were required to diagnose and manage recurrent, spontaneous oesophageal rupture and septic shock in this patient. During both admissions, the patient was treated operatively with direct closure of the oesophageal defect and conservation of the oesophagus, together with the insertion of mediastinal drains, drainage gastrostomy and feeding jejunostomy. Prolonged intensive care admission for cardiorespiratory organ support was crucial to ensure a successful outcome.
Conclusion: A multidisciplinary approach combining intensive care, radiological, endoscopic and surgical strategies is required in patients with recurrent Boerhaave’s syndrome, and patients with severe sepsis following late presentation. Literature searches reveal few detailed series of the diagnosis and management of Boerhaave’s syndrome, and only 3 descriptions of recurrence. Boerhaave described a transmural tear of the oesophageal wall, secondary to excessive vomiting, and occurring in association with excessive food and alcohol. However, clinical presentation can be misleading, and a high index of suspicion, combined with accurate radiological evaluation, is necessary to achieve a successful outcome. Swift diagnosis is crucial as the time elapsed between onset of symptoms and initiation of treatment correlates well with prognosis and hospital stay. Complications include mediastinitis, septic shock and death in up to 70%; and therefore patients commonly require prolonged intensive care admission and organ support. Management approaches include conservative, endoscopic and operative strategies, depending upon the patient’s condition, timing of presentation, and the site and size of the tear. Literature reviews of operative techniques that conserve the native oesophagus are usually associated with reduced morbidity and mortality, as compared to oesophageal replacement or resection approaches.
PRIMARY PANCREATIC LYMPHOMA: A DIAGNOSIS TO REMEMBER
K. E. Evans1, A. S. Mee2. 1Gastroenterolgy, Wycombe Hospital, High Wycombe, 2Royal Berkshire Hospital, Reading, UK
Introduction: This is a series of three cases of primary pancreatic lymphoma (PPL). PPL shares similar clinical and radiological features with the more common pancreatic adenocarcinoma. This series highlights the need to distinguish between the two because PPL is amenable to non-surgical treatment and carries a much better prognosis.
Aims & Methods: Case 1: A 51-year-old man presented with abdominal pain, fevers and obstructive jaundice. Ultrasound of the abdomen revealed pancreatic head mass. ERCP demonstrated a 10 mm stenosis in the pancreatic head. CT abdomen showed multiple cystic lesions within the pancreas, and multiple, large lymphnodes. Biopsy confirmed diffuse large B cell non-Hodgkin’s lymphoma. Case 2: A 74-year-old man presented with epigastric pain, weight loss, obstructive jaundice and a right upper quadrant mass. CT demonstrated a large pancreatic mass with large volume lymphadenopathy. ERCP demonstrated a distorted duodenum and a tight stricture in the common bile duct. The tumour and lymphnodes were PET negative. He then developed melaena and biopsy of the responsible gastric ulcer demonstrated a high grade non-Hodgkin’s lymphoma. Case 3: A 62-year-old man presented with symptoms of pancreatic insufficiency. This was confirmed by a pancreolauryl test. ERCP demonstrated irregular ducts in the pancreatic body, and common bile duct narrowing. CT abdomen showed a large soft tissue mass in the mesentery. A CT guided biopsy of the mesenteric mass confirmed a follicular B cell non-Hodgkin’s lymphoma.
Results: Two patients are in remission following chemotherapy. The third died of multiple complications within three months of diagnosis.
Conclusion: Primary pancreatic lymphoma is a rare extra-nodal lymphoma accounting for less than 0.5% of pancreatic tumours.1 As demonstrated here PPL often clinically and radiologically mimics the more common pancreatic adenocarcinoma. Nearly all PPLs are B-cell tumours.2 Most are treated with variants of CHOP (cyclophosphamide, doxorubicin, vincristine, prednisolone) chemotherapy. Tumour burden and LDH levels are the most important prognostic factors affecting outcome in primary gastrointestinal NHL.3 Multimodality treatment can give cure rates of up to 30% of PPL. This contrasts with the 5% 5-year survival for pancreatic adenocarcinoma.
BE AWARE OF THIS RISK WITH FEEDING
J. Mannath, I. Mohammed. Gastroenterology, Sandwell General Hospital, West Bromwich, UK
Introduction: Case report. A 57-year-old gentleman was recently admitted to gastroenterology ward with persistent vomiting and possibility of aspiration. He had an extradural haematoma in 2002 following trauma and underwent craniotomy. He was admitted under the gastroenterology team in 2003 with poor oral intake and was assessed by the SALT team. His swallow was poor and he was NG fed for 8 weeks before a PEG insertion was done. He was transferred to a nursing home after establishing PEG feed. In 2006 he was re-admitted with a PEG site infection and blocked PEG. He had a buried bumper for which he underwent laparotomy and removal. During laparotomy a gastric feeding tube was inserted. However he had persistent vomiting post gastrostomy insertion and a contrast examination through the PEG was done.
Aims & Methods: There were no signs of obstruction or reflux in the pegogram to account for persistent vomiting. However efforts to sustain his feed were futile due to vomiting. A jejunal extension tube (PEG-J) was thought to be the way forward and this was performed in July 2006 (Freka, ch-9). He settled well after this and his feed was gradually increased to 75 ml/h and he was discharged to nursing home. He tolerated the feeds well over the next 9 months and re-presented in April 2007. He had persistent vomiting and symptoms of aspiration. In view of his persistent vomiting a further pegogram and jejogram was done
Results: This showed that the jejunal extension tube has migrated to the oesophagus. The tube was probably displaced as a result of vomiting, causing further regurgitation and aspiration during feeding. The jejunal extension tube was removed and he was started on PEG feeds. He tolerated this well and was discharged with a plan to observe him and if he continues vomiting, a direct percutaneous endoscopic jejunostomy (DPEJ) or surgical jejunostomy will be considered.
Conclusion: Technical success of initial feeding tube insertion into the jejunum (PEG-J) can be achieved, but the function of these systems is often unsatisfactory due to frequent retrograde J-tube migration and dysfunction due to kinking and clogging. J-tube dysfunction is reported in 27–84% of cases and the average longevity of the jejunal extension tube is 3–6 months. DPEJs may be more dependable than PEG-Js and are being performed with increasing frequency, however some studies have shown a failure rate of around 30% due to lack of transillumination.
LATERAL THINKING AND GASTROINTESTINAL BLEEDING
E. Wesley1, R. Ali1, R. Ramnarace1, M. A. Puckett2, J. R. Lowes1. 1Gastroenterology, 2Radiology, Torbay Hospital, Torquay, UK
Introduction: Gastrointestinal bleeding is a common problem seen by gastroenterologists. We present a rare cause of this and discuss the possible causes and controversial treatment options available.
Aims & Methods: An 80-year-old man presented to our Accident and Emergency department with a short history of fresh haematemesis. He had not passed melaena and had no abdominal pain. Past medical history included atrial fibrillation, angina and deep vein thrombosis for which he was taking warfarin. There was no history of use of non-steroidal anti-inflammatory drugs, no history of excess alcohol consumption and no previous history of upper GI bleeding. On initial presentation he was shocked with a blood pressure of 90/70 mmHg and a pulse rate of 120. He had no stigmata of chronic liver disease and physical examination was otherwise unremarkable. His initial Rockall Score was 4. Initial blood tests showed a haemoglobin of 11.8 g/dl, platelet count of 302×109/l and INR of 2.9. His urea was normal at 6.4 mmol/l. He was resuscitated with intravenous fluids including blood and his coagulopathy was reversed with vitamin K and fresh frozen plasma. A gastroscopy was arranged and took place within six hours of admission. His stomach contained a large residue of altered and fresh blood and in the antrum an extensive adherent clot was noted. Adrenaline was injected around the edge of this and the heater probe used. Initially, this stopped the bleeding but the clot could not be removed to inspect underneath. A repeat gastroscopy and CT scan were arranged for the following day. Prior to this he received a pro-kinetic agent to improve mucosal views.
Results: The endoscopy and CT scan both showed a choledochogastric fistula.
Conclusion: This diagnosis is extremely rare. More common is fistulation between the gallbladder or bile ducts and other sites in the gastrointestinal tract. The main types of fistulae are cholecystoduodenal, cholecystocolonic and choledochoduodenal. Complications and therefore methods of presentation include gastrointestinal haemorrhage as well as gallstone ileus, ascending cholangitis and severe diarrhoea. Treatment of enterobiliary fistulae is controversial and often complex. Due to the extremely rare nature of the diagnosis, the area is lacking any firm evidence from randomised controlled trials. Some have advocated surgery in all patients because of the risk of carcinoma of the gallbladder which can be missed without surgery. However the mortality from such procedures is high. Our patient was treated conservatively. His bleeding stopped with the initial endoscopic therapy and correction of his coagulopathy. Given his age and comorbidity it was felt that surgical options to correct the fistula did not warrant the high risk of complications. He has so far not been readmitted and was asymptomatic at follow-up.
PYREXIA OF UNKNOWN ORIGIN: A DIAGNOSTIC CHALLENGE
A. Anand, R. Parmeshwar, A. K. Bohra. General Surgery, Royal Albert Edward Infirmary, Wigan, UK
Introduction: Pyrexia of unknown origin is an important clinical entity. It remains a diagnostic challenge because of the diversity and complexity of the clinical conditions it can represent.
Aims & Methods: We report a case of pyrexia of unknown origin where the lack of specific symptoms and signs and the absence of positive radiological findings presented a significant diagnostic challenge.
Results: A 45-year-old builder was admitted with a 3-week history of decreased appetite, fever and weight loss. The only positive examination findings were tachycardia and persistent pyrexia. Blood tests were unremarkable except for a low haemoglobin and albumin. Chest x ray and ECG were normal. An extensive infection screen and an autoimmune screen were negative. However, the patient developed diarrhoea and his general condition continued to deteriorate. A CT scan of the thorax, abdomen and pelvis was unremarkable. A bone marrow biopsy indicated depleted iron stores hinting at a gastrointestinal cause. However, before a gastroscopy and colonoscopy could be performed, he developed severe abdominal pain. On examination, he was shocked and his abdomen was peritonitic. He underwent an urgent laparotomy, which showed extensive small bowel thickening and patchy necrosis leading to perforation. He also had a partially obstructing lesion in the distal transverse colon. A resection-anastomosis of the worst affected segment of the small bowel was performed with fashioning of a loop colostomy. Although our patient went on to receive the recommended treatment for his disease, he developed neurological complications and succumbed to the disease barely five months after the onset of symptoms.
Conclusion: Our case illustrates the difficulties in the diagnosis and management of this clinical entity. We conclude that a high index of suspicion and appropriate early investigations are essential to improve the prognosis, which in general continues to be poor.
THE CONFUSING ALCOHOLIC
D. G. Craig1, I. Curzon2, K. Prasad3, N. Quinn4, J. Hancock1. 1Gastroenterology, 2Radiology, 3Histopathology, 4Endocrinology, Friarage Hospital, Northallerton, UK
Introduction: We report a rapidly fatal case of acute pancreatitis associated with severe hypertriglyceridaemia in an alcoholic admitted with newly diagnosed diabetic ketoacidosis. Serum amylase may be unhelpful in such cases and alternative diagnostic tests are required. The role of plasma exchange in hyperlipidaemic pancreatitis is discussed.
Aims & Methods: A 32-year-old Caucasian alcoholic was admitted with a 2-day history of progressive polydipsia and confusion. A diagnosis of diabetic ketoacidosis (DKA) was made after finding massive glycosuria and ketonuria along with a profound metabolic acidosis. Serum amylase was mildly elevated at 185 U/l. Liver function tests showed preserved synthetic function and serum lactate was normal. He was noted to have a milky, lipaemic serum with a cholesterol of 22.5 mmol/l and a hypertriglyceridaemia of 71.21 mmol/l. CT of chest and abdomen demonstrated marked peripheral infiltration of both lung bases but shortly afterwards the patient had a cardiorespiratory arrest culminating in his death 12 hours after admission. Postmortem examination revealed acute pancreatitis (AP) with fat necrosis.
Results: Coexistent diagnoses of DKA and AP present the physician with a complex diagnostic problem. The presence of abdominal pain is non-specific1 and the coexistence of AP with DKA is associated with more severe metabolic acidosis and hyperglycaemia, and a worse prognosis, than cases of isolated DKA. Hypertriglyceridaemia is a recognised consequence of DKA due to lipolysis of adipose tissue and severe hypertriglyceridaemia (>55 mmol/l) can cause chemical irritation around pancreatic acinar cells. Non-specific hyperamylasaemia is frequent in DKA while patients with hyperlipidaemic pancreatitis may have low initial levels of serum amylase2 and this provides a further diagnostic hurdle. Urinary trypsinogen-2 levels have high negative predictive values and may provide a more sensitive marker in hyperlipidaemic pancreatitis than serum amylase.3 Plasma exchange has been used successfully in hyperlipidaemic pancreatitis but its effectiveness has recently been called into question.4
Conclusion: This case demonstrates the continued diagnostic difficulties presented by patients with concurrent DKA and AP. Early recognition of the possibility of AP in patients with lactescent serum may allow earlier institution of intensive care input and radiological diagnosis.
SHORTNESS OF BREATH IN CROHN’S DISEASE
P. Ellul1, J. Mann2, E. T. Swarbrick1, D. C. Rowlands3, I. Morgan4. 1Gastroenterology, 2Respiratory, 3Histopathology, 4Cardiothoracic Unit, New Cross Hospital, Wolverhampton, UK
Introduction: A case of shortness of breath in Crohn’s disease.
Aims & Methods: To discuss the differential diagnosis and management of such pathologies.
Results: Our presentation is about an interesting case of a young man with Crohn’s disease, diagnosed 9 years ago who presented with weight loss, anorexia, nasal blockage, chest tightness and shortness of breath on exertion. He was having balsalazide and azathioprine as to keep his disease stable, although he had chronic perianal disease. In our case we first go through the investigations, differential diagnosis and treatment of his current medical pathologies. We demonstrate some interesting images of his chest x ray, computed tomography scan of his thorax and of histology samples. Then, we discuss the respiratory syndromes associated with IBD as well as the drugs used in the management of IBD. Finally we discuss the management of such challenging coexistant pathologies.
Conclusion: We discuss in detail, with the aid of images, the above differential diagnosis and the challenges in management of such pathologies.
AN UNUSUAL CAUSE OF GASTROINTESTINAL HAEMORRHAGE
C. E. Kober1, M. C. Gallagher1, S. de Sanctis2, C. Topham3, C. J. Tibbs1. 1Department of Gastroenterology, 2Department of Histopathology, 3Department of Haematology, Royal Surrey County Hospital NHS Trust, Guildford, UK
Introduction: A 59-year-old man presented with a 4-day history of malaena. His medical history revealed that he had undergone an anterior resection for colorectal carcinoma 36 months earlier. Postoperatively he received 12 cycles of adjuvant chemotherapy with Oxaliplatin and 5 Fluorouracil.
Aims & Methods: He had no prior history of gastrointestinal haemorrhage or bleeding diathesis, no known risk factors for chronic liver disease, and a modest alcohol intake (16 units per week).
Results: Laboratory tests revealed anaemia and thrombocytopenia (Hb 6.7, platelets 91), with normal renal function and liver biochemistry. Following resuscitation an upper gastrointestinal endoscopy was arranged. Multiple oesophageal varices with stigmata of recent haemorrhage were identified, and endoscopic band ligation performed. Ultrasound and CT examinations revealed splenomegaly, a structurally normal appearing liver and patent portal vessels. There was no evidence of recurrent colorectal carcinoma. Laboratory investigations for causes of chronic liver disease were negative (normal immunological profile and iron studies, and negative viral serology). Liver histology revealed features of hepatic venous outflow obstruction (veno-occlusive disease). Haematological studies for prothrombotic states were negative, and a bone marrow showed no evidence of a myeloproliferative disorder.
Conclusion: Although liver fibrosis and venocclusive changes have been reported in patients treated with oxaliplatin, this is the first report of a case of variceal haemorrhage secondary to oxaliplatin-induced liver injury.
A RARE COMPLICATION OF LIVER BIOPSY
M. Wireko1, S. Bridger2, C. Hovell2, R. Ward3. 1Gastroenterology, Poole Hospital NHS Trust, Poole, 2Gastroenterology, 3Radiology, Dorset County Hospital Foundation Trust, Dorchester, UK
Introduction: Case report. A 66-year-old man was admitted under the surgeons with abdominal pain and haematochezia. 7 days previously he had been diagnosed with autoimmune hepatitis with a pre-treatment score of 14.
Aims & Methods: His liver function tests (LFTs) were as follows: ALT 2442 IU/l,Alkaline Phosphatase 284 IU/l, GGT 195 IU/l, Bilirubin 383 μmol/l, Albumin 36 g/l and raised IgG of 24.4. His ultrasound guided liver biopsy was consistent with this diagnosis. He had been started on prednisolone 40 mg daily with rapid improvement in his LFT.
Results: On this admission, he was noted to be hypotensive, dropped his haemoglobin by 2 g/dl. Flexible sigmoidoscopy was negative. Gastroscopy revealed blood in the second part of the duodenum and a CT scan revealed an interesting abnormality. He responded successfully to a specific treatment and has now made a full recovery.
Conclusion: The symptomatic triad of gastrointestinal bleeding, biliary pain, and jaundice is characteristic of haemobilia and tends to occur about 5 days after liver biopsy. This complication is very rare occurring in only 4 out of 68 276 (0.006%) percutaneous liver biopsies.1 Most cases of haemobilia settles spontaneously, however significant cases causing symptoms will need embolisation. If the latter is unsuccessful, then surgical intervention would be required. This case highlights the need for vigilance and close follow-up of patients for rare but potentially serious complications post liver biopsy.
Plenary posters
MUCOSALLY-ADHERENT E COLI ISOLATES FROM HUMAN COLON CANCER INDUCE NUCLEAR TRANSLOCATION OF BETA-CATENIN AND CYCLIN D1 EXPRESSION IN HUMAN COLON CANCER EPITHELIAL CELLS
P. D. Collins, L. Yu, J. M. Rhodes. School of Clinical Science, University of Liverpool, Liverpool, UK
Introduction: Dysregulation of Wntβ-catenin signaling, nuclear translocation of β-catenin and subsequent T-cell factor/lymphoid-enhancing factor-mediated transcription are early events in colon cancer development.1 The Wnt target gene, Cyclin D1, is a major cell-cycle regulator. Non-virulent bacteria can influence β-catenin signaling in human epithelia.2 Mucosally-adherent E coli are found in increased numbers in colonic mucosa in patients with colon cancer.3 Bacterial involvement in cancer progression could explain the much higher rate of cancer in the colon than the small intestine.
Aims & Methods: DLD-1 cells, a colon cancer cell line with biallelic inactivation of APC gene, were cultured with E coli mucosal isolates from patients with colon cancer, isolates from control patients, heat-killed bacteria or bacterial supernatant. Cells were incubated with Prostaglandin-E2 (0.1 μM) as a positive control. Cellular localisation of β-catenin was assessed by immunofluorescence microscopy. Nuclear localisation of β-catenin was quantified and expressed as a ratio of the intensity of nuclear to whole cell fluorescence for over 100 cells from each blind-labelled sample. Expression of β-catenin and Cyclin D1 in whole cell lysates was analysed by western blotting.
Results: Colon cancer E coli isolate HM545 increased nuclear localisation of β-catenin (mean ratio of nuclear to whole cell fluorescence (N:WC) = 1.064; SD 0.406) compared to the negative control (no bacteria N:WC = 0.982; SD 0.087) (p = 0.017). Neither HM545 supernatant (N:WC = 0.983; SD 0.085) (p = 0.90) nor heat-killed HM545 (N:WC = 0.997; SD 0.117) (p = 0.25) increased nuclear localisation. Two E coli isolates from patients with normal colons did not induce nuclear localisation of β-catenin (HM452; N:WC = 0.983; SD 0.115 (p = 0.95) and HM455; N:WC = 0.973; SD 0.083 (p = 0.42)). Six of nine mucosal E coli isolates from colon cancer induced nuclear translocation. Western blotting showed that Cyclin D1 expression is increased in response to three of five E coli isolates (including HM545), but not in response to HM545 supernatant or heat-killed bacteria. The stimulatory effect of E coli HM545 on Cyclin D1 was inhibited when cells were pre-incubated with the cox-2 inhibitor NS398 (10 μM) or soluble plantain fibre (5 mg/ml), an inhibitor of E coli epithelial cell adhesion. Neither bacterial haemagglutination status nor phylotype corresponded with Cyclin D1 expression or β-catenin nuclear localisation. Bacterial isolates had no effect on total levels of β-catenin in whole cell lysates.
Conclusion: Mucosal E coli isolates from colon cancer induce nuclear localisation of β-catenin and activation of Cyclin D1 in human colon cancer cells. This effect requires whole, live bacteria. This is a plausible mechanism by which mucosa-associated bacteria may promote the development of colon cancer.
THE MISUSE OF THE FAECAL OCCULT BLOOD TEST UNDER THE LOWER GASTROINTESTINAL TWO-WEEK WAIT RULE
A. Shaw1, C. Longman2, J. N. Lund3, A. F. Goddard4. 1Gastrointestinal Surgery, University of Nottingham, 2Colorectal Surgery, Derby City General Hospital, 3Gastrointestinal Surgery, University of Nottingham, 4Gastroenterology, Derby City General Hospital, Derby, UK
Introduction: In July 2000 the two-week wait (2WW) referral system was introduced to reduce the delay in referral, diagnosis and subsequent treatment of patients with colorectal cancer. General practitioners are required to complete a proforma and state the necessary referral criteria for each patient. It is not part of the criteria for patients to have a FOB performed before referral. The NHS Bowel Cancer Screening Programme was introduced in England in July 2006 using the faecal occult blood (FOB) test. Screening demands a total of 6 samples be tested with 5 or 6 positive samples classified as a positive result.
Aims & Methods: To find the proportion of patients with an FOB performed as part of the referral for the lower gastrointestinal 2WW referral system, and whether this correlates with the cancer status. The last two thousand patients (from 01/08/05–31/07/07) referred as a 2WW were identified using the hospital’s cancer audit database. Performance of FOB and cancer status were recorded for each patient.
Results: A total of 2000 patients (F:M 1097:2000; median age 58; range 18–98) were referred by general practitioners. The FOB test was only performed on three samples in all cases. 1 positive (or more) FOB was classified as a positive result. In total, 169/2000 patients (8.5%) had an FOB performed prior to their referral, with 55/169 patients (32.5%) as part of the referral for 2WW. 16/169 patients (9.5%) had an FOB performed in the presence of overt rectal bleeding. In only 2/169 patients (0.01%) did the FOB correlate with a colorectal cancer (one of these had overt rectal bleeding). Unnecessary testing for FOB costs has cost £4001.92 in 2 years.
Conclusion: There is significant misuse of FOB testing. The detection rate, even in this symptomatic group of patients, is very low. FOBs are being performed in the community on three samples and not six, and those with one or two positive samples are being referred rather than being recalled for further testing, contrary to protocol. This, combined with the high false positive rate, leads to patients not only experiencing psycho-social consequences but could potentially lead to significant risks from unnecessary invasive investigation as well as the added financial burden of the test itself.
DOUBLE BALLOON ENTEROSCOPY IS HIGHLY EFFECTIVE: THE FIRST 100 CASES AT ST MARK’S HOSPITAL
E. Despott1, E. Tripoli1, A. Polecina1, K. Konieczko2, C. Fraser1. 1Wolfson Unit for Endoscopy, St Mark’s Hospital, 2Department of Anaesthesia, Northwick Park and St Mark’s Hospitals, London, UK
Introduction: The investigation and management of suspected small bowel pathology has been revolutionised by the introduction of double balloon enteroscopy (DBE). DBE is unique in that it provides the facility to biopsy lesions and to apply therapeutic procedures such as the coagulation of bleeding vessels and balloon dilatation of strictures, potentially averting the need for surgery.
Aims & Methods: We report our experience of DBE since its introduction to our unit in 2005. A comprehensive DBE database was collated and analysed for indications, concordance of capsule endoscopy (CE) and DBE findings, therapy applied at DBE, sedation practices and complications.
Results: 100 cases (56 males) were performed. Mean age was 58.8 years (16–92 years). 81 cases were performed via the oral route, 14 via the rectal route 4 cases via both the oral and rectal routes and 1 case through an ileostomy; 49 cases were done under general anaesthesia (mean age 49.1 years); 51 cases had conscious sedation (mean age 67.5 years). The indications and therapeutic interventions are shown (table). DBE was preceded by CE in 82 cases, the concordance of diagnoses at CE and DBE was 71%. Where there was divergence in the CE and DBE findings, abnormalities seen at CE were not confirmed at DBE in 15 cases. Conversely, DBE showed lesions that were not picked up by CE in 7 cases. Lesions missed at CE included small bowel ulceration, a GIST and a case of strongyloidiasis. The findings at DBE led to successful surgical management in 9 cases (small bowel tumours and a large vascular lesion). In cases referred for stricture dilatation, surgery was averted in 6 of 10 cases. In our cohort of patients the overall diagnostic and therapeutic yields (on an intention to treat basis) of DBE were 76% and 77% respectively. Limiting factors included bowel fixation by adhesions, scope looping, obesity and patient discomfort despite sedation. There were no clinically important complications.
Conclusion: DBE is a feasible, safe and reliable technique for the diagnosis and treatment of suspected small bowel pathology. Importantly, we confirm that in selected cases it offers an alternative to surgery. Our experience compares favourably to other results published in the literature to date.
DEFINING IN VIVO MUCOSAL INFLAMMATORY ACTIVITY AND DISEASE EXTENT IN ULCERATIVE COLITIS: DEVELOPING A CLINICALLY APPLICABLE MODEL USING LASER SCANNING CONFOCAL ENDOMICROSCOPY
D. P. Hurlstone1, N. Tiffin2, S. S. Cross3. 1Endoscopy, Royal Hallamshire Hospital, 2Histopathology, STH NHS Foundation Trust, 3Histopathology, Royal Hallamshire Hospital, Sheffield, UK
Introduction: Colonoscopy with mucosal biopsy is currently considered the “gold standard” for the assessment of disease activity and extent assessment in ulcerative colitis (UC). High-magnification Saitoh criteria are superior to Baron indices for all histopathological stages of disease but is complicated by complex classifications and significant inter/intra-observer variability. Using confocal laser scanning endomicroscopy we propose a novel, simple in vivo optical “biopsy” classification using combined surface cellular resolution and deep vascular architecture crypt imaging.
Aims & Methods: To evaluate the efficacy of live cellular endomicroscopic imaging for the in vivo diagnosis of disease extent and activity in UC. Consecutive patients with UC were recruited to ascertain current mucosal activity parameters and extent. Disease activity and extent was documented using conventional endoscopy (Baron indices), Sheffield endomicroscopy criteria with mucosal biopsy as the assumed “gold standard” from all 5 colonic segments and the rectum. Endomicroscopy was performed using topical acroflavin for surface mucosal nuclear imaging in addition to deep z-axis vascular imaging following 5 ml of iv. 10% sodium fluorescene. Endomicroscopy was performed at 10 mm quadrantic segmental intervals. Confocal greyscale macro data were collected at 1.6 frames/sec/optical z-axis sectioning 0.7 μm—field view 500 μm×500 μm, minimum 12 macros per segment. The in vivo endomicroscopic diagnosis (according to Sheffield criteria) was then compared to targeted biopsies equating to the raster scanned mucosal segment.
Results: 48 patients completed protocol. A total of 28-targeted biopsies were taken from each patient (in a segmental distribution) exacting to a 12 “slice” z-axis segmental endomicroscopy-scanning plane. A total of 1344 biopsies were subsequently compared to 18 816 endomicroscopy images graded according to Sheffield criteria. The K coefficient of agreement between the endomicroscopy indices (grade 0–2) and Matts grade 1/2, 3a–4 and 5 were 0.94, 0.82 and 0.79 respectively. Histopathological grade of disease was represented more accurately using endomicroscopy criteria as compared to conventional Baron scores for all clinical parameters (r = 0.91; p<0.01). Endomicroscopy was significantly better than conventional colonoscopy for predicting in vivo disease extent (p<0.001).
Conclusion: Endomicroscopy permits live cellular, sub-cellular and deep vascular imaging in UC which when interpreted using Sheffield criteria provide a high accuracy in vivo “virtual biopsy” and hence provide an instant biomarker for disease relapse. High-accuracy virtual biopsy can limit the number of biopsies required for the procedure with significant cost savings to pathology services.
“SALVAGE” ENDOSCOPIC SUBMUCOSAL DISSECTION AS AN ALTERNATIVE TO SURGICAL RESECTION FOR RESIDUAL OR LOCAL RECURRENT INTRAEPITHELIAL NEOPLASIA IN THE COLORECTUM: A PROSPECTIVE ANALYSIS
D. P. Hurlstone1, S. R. Brown2, W. Baraza2, N. Tiffin3, S. S. Cross4. 1Endoscopy, Royal Hallamshire Hospital, 2Colorectal Surgery, 3Histopathology, STH NHS Foundation Trust, 4Histopathology, Royal Hallamshire Hospital, Sheffield, UK
Introduction: Curative intent for residual or locally recurrent colorectal neoplasia following EMR is often not technically feasible due to submucosal fibrosis. Such cases often demonstrate false positive submucosal invasion status at high-frequency 20/12.5 MHz EUS and are associated with a conventional non-lifting sign at submucosal catheterisation. Primary ablative therapies preclude therapeutic efficacy confirmation histologically in this group. Endoscopic submucosal dissection may permit curative intent “salvage” therapy without the requirement for formal surgical resection as the technique permits endoluminal transection of fibrotic tissue.
Aims & Methods: A prospective technical feasibility study of cap assisted ESD for “curative intent” in patients with residual or local neoplastic recurrence following EMR. Primary end points were second stage R0 resection rate, safety and recurrence. Salvage endoscopic submucosal dissection was performed using the Olympus GIF-XQ240 gastroscope and KD-630L insulation tipped knife. Submucosal injection solute comprised sodium hyaluronic acid (10 ml) mixed with 1 ml 1/10 000 adrenaline and 1 ml of 0.5% indigo carmine solution for enhanced delineation of the muscularis at endoscopic dissection. 30-day mortality, re-admission rates, complications and histological resection status were collected prospectively up to 9 months following index resection.
Results: 30 patients met eligibility criteria. 29/30 (96%) demonstrated non-lifting or asymmetric lifting at index submucosal catheterisation. Index R0 resection was achieved in 25/30 (83%) lesions. 1 patient underwent surgical excision with a second receiving a curative second stage dissection. 96% (29/30) patients were discharged within 24 hours of the procedure with a 0% 30-day mortality and re-admission rate. Bleeding occurred in 5/30 (16%) treated successfully with endoluminal haemostasis. There were no perforations. Overall “cure” rates at short-term follow-up (median 6/12 (range; 3–18)) was 96%.
Conclusion: This novel application of endoscopic submucosal dissection for first line “salvage” therapy in treating residual or locally recurrent neoplastic disease may be a safe, minimally invasive and cost effective alternative to direct surgical resection in a select patient cohort.
PILLCAM COLON CAPSULE ENDOSCOPY COMPARED TO COLONOSCOPY IN DETECTION OF COLON POLYPS AND CANCERS. INTERIM ANALYSIS OF A PROSPECTIVE MULTICENTRE TRIAL
A. J. Postgate1, C. Fraser1, A. Fitzpatrick1, M. Munoz-Navas2, I. Fernandez-Urien2, M. Lapalus3, T. Ponchon3, G. Gay4, M. Delvaux4, H. Neuhaus5, M. Philliper5, G. Costamagna6, M. Riccioni6, C. Spada6, F. Haegenmuller7, M. Keuchel7, N. Schoofs8, A. Van Gossum8, J. Deviere8. 1Wolfson Unit for Endoscopy, St Mark’s Hospital, London, UK, 2Digestive Diseases Division, University of Navarra, Pamplona, Spain, 3Department of Digestive Diseases, Hôpital Edouard Herriot, Lyon, 4Department of Internal Medicine and Digestive Diseases, Hôpitaux de Brabois, Vandoeuvre les Nancy, France, 5Department of Gastroenterology, Evangelisches Krankenhaus, Düsseldorf, Germany, 6Digestive Endoscopy Unit, Catholic University, Rome, Italy, 7Department of Gastroenterology, Asklepios Klinik Altona, Hamburg, Germany, 8Department of Gastroenterology, Erasme University Hospital, Brussels, Belgium
Introduction: In pilot studies, PillCam colon capsule endoscopy (PCE) has been shown both feasible and able to demonstrate colonic polyps and cancers. An 8-centre prospective study with a target of 329 patients is ongoing in Europe. The primary objective is to assess the yield of PCE in detecting polyps and other pathologies in comparison to traditional colonoscopy. This study reports the first planned interim analysis.
Aims & Methods: Patients included in this study were known to have (age >18 years) or suspected of having (age >50 years) colonic disease and were referred for colonoscopy. Patients went through a traditional PEG colon prep and ingested the capsule in the morning. The procedure included prokinetic agents and additional small doses of laxatives. Independent physicians performed capsule imaging analysis and traditional colonoscopy (gold standard) after excretion. Significant findings were defined as at least one polyp ⩾6 mm or ⩾3 polyps of any size.
Results: One hundred and sixty six patients, mean age 60 (23–84) years, were included in this interim report. Capsules were expelled within 10 hours post-ingestion in 96% of patients, and remained in the stomach for the entire procedure in 2 (1.2%) patients who were excluded from the analysis. Quality of colon preparation in PCE was evaluated as excellent to good (68%), fair (24%) and poor (8%). A polyp of any size was found in 111 patients (68%) and 75 (46%) patients had significant findings detected by colonoscopy. The yield of PCE compared to colonoscopy is shown in the table. Fifteen polyps were detected only by PCE. No severe adverse events related to PCE were reported.
Conclusion: This interim analysis shows encouraging sensitivity and negative predictive values for the detection of significant findings compared to colonoscopy. If this data is further validated at the conclusion of this study, this new non-invasive technology might challenge colonoscopy for CRC screening and polyp detection.
ACCURATE QUANTIFICATION OF H PYLORI DENSITY IN HUMAN GASTRIC BIOPSIES USING REAL-TIME PCR
S. R. Patel, K. Robinson, D. P. Letley, J. C. Atherton. Gastroenterology, Wolfson Digestive Diseases Centre, Nottingham, UK
Introduction: The density of H pylori on gastric mucosa may be influenced by a number of factors, including the host immune response and virulence determinants expressed by the colonising strain. Current methods for assessing colonisation densities, however, are based on quantitative culture or histopathology scoring techniques, which have limited sensitivity and accuracy.
Aims & Methods: We aimed to develop a quantitative real-time PCR assay for measuring the colonisation density of H pylori in gastric biopsies. The H pylori 16S rRNA gene was selected as a target. Primers were designed and tested to ensure that they were specific for amplification of a product from diverse strains of H pylori. Standard curves were prepared using purified H pylori J99 genomic DNA. For greater accuracy, bacterial copy numbers were normalised against the human GAPDH housekeeping gene. The assay was validated by adding a known number of bacteria to a known number of AGS cells (a human gastric epithelial cell line), and also by spiking uninfected biopsy specimens with a known number of bacteria. The data were normalised against the copy number of human GAPDH, presenting the results as bacterial genome copy per human genome copy.
Results: Primers for the 16S rRNA gene were specific and could be used to amplify a product from 30 diverse H. pylori strains. Both bacterial and human standard curves demonstrated a high degree of fit (R2 = 0.99691 and 0.99582 respectively), and good reproducibility in the range of 20 ng/μl–10 fg/μl. Validation of the quantitative assay using known numbers of bacterial and AGS cells resulted in good accuracy with the ratio of number of bacteria/human cell detected almost exactly equal to the number added. We have examined antral and corpus biopsies from 10 patients and more are in progress. Mean ratios of bacteria to eukaryotic cells in the antrum were 0.3 (range 0.02–0.92), and in the corpus were 0.55 (range 0.009–3.78). There was no obvious association between bacterial numbers and neutrophil or lymphocyte scores. In preliminary results, all 3 patients with DU had an antral predominant colonisation with a mean antral: corpus bacterial ratio of 7.0. In contrast, 10 patients without ulcers had widely varying antral: corpus bacterial ratios.
Conclusion: The real-time PCR assay developed was highly sensitive and accurate for the quantification of H pylori. Preliminary results support antral predominant colonisation predisposing to DU. Further work is in progress.
UPREGULATION OF UROKINASE-TYPE PLASMINOGEN ACTIVATOR RECEPTOR IS ASSOCIATED WITH HELICOBACTER PYLORI IN PREMALIGNANT GASTRIC TISSUE
J. M. Mikhail1, P. Griffiths2, J. Manson3, L. Thomas4, L. Williams5, J. N. Baxter3, J. M. Parry1, G. J. S. Jenkins1. 1School of Medicine, Swansea University, 2Pathology, 3Surgery, 4Medicine, Swansea NHS Trust, Swansea, 5Medicine, Royal Glamorgan Hospital, Llantrisant, UK
Introduction: Helicobacter pylori (H pylori) associated gastritis, induces the production of reactive oxygen species (ROS) and has been associated with disease progression. ROS induced expression of IL-8, uPAR and PAI-1 has been described: NF-κB may be involved. It is unclear whether expression of these genes plays a role in gastric cancer progression.
Aims & Methods: We have investigated the expression of IL-8, uPAR and PAI-1 in gastric tumours and +/−H pylori infection in premalignant tissue to determine the stage in disease progression that changes occur. Tumours and adjacent normal mucosal tissue were obtained from surgical gastric resections. Gastric biopsies were isolated from consenting patients attending Endoscopy clinic. All samples were stored in RNA later, histology was confirmed and RNA extraction performed (Qiagen). Analysis of the gastric tumours using microarrays (Superarray) was followed by qPCR (Biorad). Premalignant biopsies were analysed using qPCR.
Results: In gastric tumours, IL-8 was upregulated >twofold in 17/19 (89.5%), PAI-1 was upregulated in 14/19 (74%) and urokinase-type plasminogen activator receptor (UPAR) was upregulated in 7/19 (37%), compared to the corresponding normal mucosal tissue. In the premalignant biopsy samples, IL-8 showed upregulation in chronic gastritis and gastritis associated with H pylori infection. Upregulation of uPAR was significant in samples with coexisting or previous H pylori infection. PAI-1 was not differentially expressed.
Conclusion: This study has shown upregulation of two ROS and NF-κB regulated genes, IL-8 and uPAR, in both gastric tumours and premalignant tissue. Further investigation, may show these genes to be markers of disease progression and NF-κB a potential therapeutic target.
THE COST-EFFECTIVENESS OF BIOLOGICAL THERAPIES FOR CROHN’S DISEASE: MARKOV COHORT ANALYSES INCORPORATING UK PATIENT-LEVEL COST DATA
K. Bodger1, T. Kikuchi2, D. A. Hughes2. 1Department of Medicine, Clinical Science Centre, University Hospital Aintree, Liverpool, 2Centre for Economics and Policy in Health, University of Bangor, Bangor, UK
Introduction: Anti-TNF-α agents for Crohn’s disease (CD) have good clinical efficacy but high acquisition cost compared to rival drugs. Previous modelling estimates of cost-effectiveness suggest an unacceptably high incremental cost per QALY compared to standard care. However, existing models were limited by a lack of primary data for costs of care and health state utility. The aim of the present study was to undertake an independent analysis incorporating data from recent trials and observational studies from the perspective of the UK National Health Service. The present analysis focuses on infliximab and adalimumab.
Aims & Methods: Lifetime Markov analyses constructed to simulate outcomes and costs. CD was represented by 5 disease states: Full Response (CDAI<150, remission); Partial Response (CDAI 150–220, mild-to-moderate activity); Non-Response (CDAI >220, moderate-to-severe activity); Surgery and Death. The course of CD under standard care was modelled from a transition matrix derived from a large population cohort.1 Systematic review identified ACCENT I (infliximab) and CHARM (adalimumab) as sources for efficacy data. We modelled an intention-to-treat strategy for biologics by including a non-responder cohort (representing patients excluded from the trials after failed induction). Surgical rates were based on observational data, cost estimates were taken from our UK dataset2 and utilities were derived for each state from an algorithm converting CDAI to EQ5D utilities.3
Results: In the base-case analysis (lifetime horizon; 1–2 years continuous therapy; discount rate 3.5%) both agents achieved acceptable incremental cost effectiveness ratios (ICERs) compared to standard care (table). Lifetime therapy was dominated by standard care.
Conclusion: We have taken advantage of recent studies to develop a model for estimating the cost-effectiveness of rival therapies for CD. Unlike earlier attempts, our model suggests acceptable ICERs for biological agents for periods of up to 2 years continuous therapy. Apparent differences between rival biological agents must be interpreted cautiously as head-to-head trial data are not available.
NICOTINE EXERTS ITS ANTI-INFLAMMATORY EFFECTS ON CELLS OF COLONIC PHENOTYPE VIA INHIBITION OF TRANSCRIPTION FACTOR, NF-κB
K. M. Khatab, W. Dhaliwal, D. S. Rampton. Centre for Gastroenterology, Barts and The London Queen Mary’s school of Medicine and Dentistry, London, UK
Introduction: Smoking is beneficial for ulcerative colitis, while the opposite is true for Crohn’s disease; the reason for this paradox is unknown. We have shown in previous work (Khatab, Gut 2005;54:A97) that nicotine significantly inhibits TNF-α-induced IL8 production by epithelial cells of colonic phenotype (HT29) while it has no effect on IL8 production by epithelial cells of small intestinal phenotype (Caco2). We have also shown that nicotine exerts its anti-inflammatory effects via α7-nicotinic acetyl choline receptors (nAChR) which are expressed by colonic epithelial cells (HT29) and myofibroblasts but not by those with small intestinal phenotype (Caco2) (Khatab, Gut 56(Suppl 2):A113–A114, April 2007). The exact intracellular signalling pathways involved in the anti-inflammatory potential of nicotine are not well established. Studies in different cell types including monocytes and macrophages have indicated that the anti-inflammatory potential of the alpha7-nAChR is mediated by the inhibition of the transcription factor, NF-κB.
Aims & Methods: We studied the hypothesis that the anti-inflammatory potential of nicotine by colonic intestinal cells is mediated by the inhibition of the transcription factor, NF-κB. Confluent Caco2, HT29 and myofibroblast cells were stimulated with TNF-α (50 ng/ml) or IL1 (10 ng/ml) in the absence or presence of nicotine (10−5 M). The nuclear extracts of these cells were collected after 24 hours. NF-κB (p65) levels were assayed using p65 NF-κB ELISA kit which detects the active form of NF-κB (p65).
Results: In all cell types used in these experiments; both TNF-α and IL1 stimulated p65 NF-κB. Nicotine had no effect on p65 NF-κB activation by Caco2 (fig 1) while it significantly inhibited p65 NF-κB activation by both HT29 (fig 2) and colonic myofibrolasts (not shown).

Conclusion: TNF-α and IL1 up-regulated the activation of NF-κB in gut cell lines. Nicotine inhibits activation of NF-κB in cell lines of cells of colonic phenotype that express α7-nAChR phenotypes (HT29 and myofibroblasts) while it had no effect on cells of small intestinal phenotype (Caco2) which do not express this receptor.
SAFETY OF ADALIMUMAB MAINTENANCE THERAPY IN CROHN’S DISEASE PATIENTS: OPEN-LABEL EXTENSION OF CHARM AND GAIN TRIALS
J. F. Colombel1, P. Rutgeerts2, W. J. Sandborn3, R. Panaccione4, W. Lau5, K. G. Lomax5, P. F. Pollack5. 1Hepatogastroenterology, CHU Lille, Lille, France, 2Gastroenterology, University Hospital of Gasthuisberg, Leuven, Belgium, 3Gastroenterology, Mayo Clinic, Rochester, MN, USA, 4Medicine, Health Science Centre, Calgary, AB, Canada, 5Immunology Development, Abbott, Parsippany, NJ, USA
Introduction: Approved in the EU for the induction and maintenance of remission in adults with severe Crohn’s disease (CD), adalimumab (ADA) has demonstrated efficacy and safety in patients with and without prior anti-TNF treatment.1–3
Aims & Methods: We assessed the safety of ADA maintenance therapy in patients who completed either of two Phase III, double-blind, placebo-controlled, ADA safety and efficacy trials, GAIN (4-week induction in infliximab failures) and CHARM (1-year maintenance). Patients had active CD (CDAI 220–450) and were naïve to prior anti-TNF therapy (approximately 50% of 854 patients in CHARM) or had lost response to/were intolerant of prior infliximab therapy (GAIN). Safety was routinely assessed and data were collected throughout CHARM, GAIN, and an open-label extension (OLE) trial following patients through 2 years since the start of CHARM and 1 year since the start of GAIN. Patients randomised to placebo in GAIN who discontinued prior to Week 4 with no exposure to ADA were not included in the safety analysis. Adverse events (AEs) were tabulated in events/100-patient-years (E/100-PY).
Results: In all, 1169 patients who received ADA in CHARM (n = 854) or in GAIN (n = 315) participated in the OLE. AEs of interest are presented in the table. Of the 28 opportunistic infectious AEs, 27 were non-systemic candidiasis, with 1 case of coccidiodomycosis. Of the 21 malignant AEs, there were 11 skin cancers and 1 lymphoma; the remainder varied in type.
Conclusion: Adalimumab was well-tolerated in this follow-up analysis of patients from CHARM and GAIN, with a safety profile consistent with those observed in previous ADA studies in CD and other indications.
AUDIT OF INFLAMMATORY BOWEL DISEASE CLINICAL RESEARCH ACTIVITY AND RESOURCES IN THE UNITED KINGDOM
B. A. Theis, S. L. Bloom. Department of Gastroenterology, University College London Hospitals NHS Foundation Trust, London, UK
Introduction: Results from the 2006 UK IBD Audit1 suggest that less than 1% of inpatients admitted with flares of IBD participated in clinical trials of treatments for their disease.
Aims & Methods: To try to determine the reasons behind such poor clinical trials recruitment an audit of current research activity, available research resources and perceived barriers to the successful conduct of clinical trials in patients with IBD in Gastroenterology units across the UK was undertaken. A questionnaire was sent via email to all members of the BSG IBD Section in September 2007. After two weeks a reminder was sent to non-responders.
Results: A total of 103 questionnaires from 99 units were returned: 85 (85.9%) were from England and 38 (38.8%) belonged to a teaching hospital. A median of 3 gastroenterologists with an “interest” in IBD (range 1–6) worked in the units. Only 7 (7.1%) units knew the size of the patient population they were treating, this despite 40 (40.4%) having a “regularly maintained database” of patients. The estimated median patient population for all respondents was 600 (range 50–3500). A specialist IBD Clinic was conducted in 66 (66.7%) units. Forty eight (48.5%) units were undertaking one or more clinical trials (median 2, range 1–5): in comparison units not currently doing so (over 60% of which reported past clinical trials experience) had a smaller estimated patient population (median 450 vs 800) and were less likely to conduct a specialist IBD Clinic (53.1% vs 81.3%), employ a clinical nurse specialist (57.1% vs 79.2%), research nurse (6.1% vs 33.3%) or research fellow (2.0% vs 44.7%), or have access to a clinical trials coordinator (14.3% vs 29.2%). While 9 respondents considered conducting clinical trials “easy”, 61 (61.6%) found it to be “difficult”. Forty eight (48.5%) respondents reported clinical workload to be a major barrier to clinical trials participation, with inadequate personnel (41.4%) and paperwork/bureaucracy, particularly in relation to LREC and R&D applications being cited as problematic. Measures that units felt would help support their clinical trials work included new/additional research nurse appointments (44.9%), clinical nurse specialists (15.3%) or a clinical trials coordinator (24.5%), along with extra funding (15.3%) and time for research being built into job plans (10.2%).
Conclusion: This audit has demonstrated the difference in availability of resources between research active and inactive units, as well as highlighting those factors identified by respondents as hampering the conduct of clinical trials and those deemed likely to be of most use towards developing clinical trials capability.
THE EFFECTS OF RIBAVIRIN OF DENDRITIC CELL MATURATION AND CYTOKINE PRODUCTION
S. J. Barker1, A. E. Semper2, W. M. Rosenberg2. 1Liver Group, Southampton University, 2iQur, Southampton General Hospital, Southampton, UK
Introduction: Hepatitis C is a major cause of liver related morbidity and mortality. Ribavirin in combination with interferon alpha (IFN\α) is currently the mainstay of treatment, leading to sustained viral eradication in 40–80% of infected patients. Ribavirin is a purine nucleoside analogue whose mechanisms of action are poorly understood although thought to include anti viral and immune modulatory effects. Dendritic cells (DCs) are potent antigen presenting cells and play a pivotal role linking innate and adaptive immunity and plasmacytoid DCs (pDCs) are the main producers of IFN\α in response to viral infection.
Aims & Methods: We tested the effect of ribavirin at different concentrations on expression of DC maturation markers (HLA-DR, CD83, CD86, CD40) and cytokine secretion from normal healthy donors and chronic hepatitis C patients (CHC) using ex vivo-isolated plasmacytoid DCs (pDCs) induced by CD40L, TLR9 or TLR7 agonists and cultured, monocyte-derived DCs (MoDCs) induced by CD40L.
Results: In pDCs, ribavirin upregulated the expression of CD86 (p<0.05) but had no effect on HLA class I expression in NHDs. CD40 ligation induced IFN-α production from NHDs and CHC patients was significantly reduced by ribavirin at all concentrations (p<0.05). In NHDs, ribavirin also caused a significant reduction in IL8 (p<0.05) and TNF-α (p<0.05). When a TLR9 agonist and a TLR7 agonist were used as alternative stimuli, the reduction in IFN-α production from pDCs by ribavirin was again seen in NHDs (p<0.005 and <0.05 respectively). The suppressive effects of ribavirin on cytokine production were not due to induction of pDC apoptosis or cell death, as assessed by cytometric staining for annexin V and PI. In MoDCs, ribavirin had no effect on maturation but was found to significantly suppress the production of TNF-α (p = 0.05).
Conclusion: The suppression of TNF-α seen from both MoDCs and pDCs treated with ribavirin may explain the reduction in hepatic inflammation seen with ribavirin monotherapy. The reduction of IFN-α from ribavirin treated pDCs may give some explanation as to why ribavirin alone has no beneficial effects on patients viral loads and does not lead to a sustained viral response and it underlines the importance of IFN in the treatment of HCV. The exact mechanisms causing the reduction in IFN-α production needs to be explored further.
RETINAL VASCULAR CHANGES IN PATIENTS WITH CIRRHOSIS
A. Mukhopadhya1, T. MacGillivray2, N. McAvoy1, P. C. Hayes1. 1Department of Gastroenterology, 2Clinical Research Facility, Royal Infirmary of Edinburgh, Edinburgh, UK
Introduction: The retinal microvasculature is unique in that it is the only part of the human circulation that can be directly visualised non-invasively in vivo and easily photographed. The subsequent application of digital image analysis to measure vascular topography in an automated and objective fashion is increasingly more common in modern ophthalmology and clinical research. Circulatory changes are common in cirrhosis and it is well known that vasodilatation worsens with worsening liver dysfunction. Study of retinal circulation may reflect severity of liver disease.
Aims & Methods: A digital fundus camera was used to take colour images of the human retina from patients with documented cirrhosis and compared with images from healthy controls. Post-processing, in the MATLAB environment, creates an enhanced grey-scale image for quantitative analysis. Vessel tracking describes the process of automatically searching along a vessel segment to detect centre positions and widths at regular intervals. Automatic segmentation of blood vessels enables the measurement of vascular tortuosity. We aimed to compare retinal vascular tortuosity in patients with cirrhosis and in healthy controls.
Results: The Lilliefors test confirmed that the tortuosity data of the arterioles and venules of cirrhotic patients did not come from a normal distribution. Median of veins tortuosity was 1.4 E-4 and the median of arteries tortuosity was 5.1 E-4. The tortuosity of veins was reduced and that of the arteries increased as compared to the normal controls. There was good correlation of indices from left and right eyes (correlation coefficient 0.7). The tortuosity of the arteries was significantly more in patients with Child’s C cirrhosis (11.3 E-4) as opposed to that with Child’s A (3.2 E-4) and Child’s B patients (4.0 E-4).
Conclusion: We show that liver disease increases tortuosity of arteries and lowers tortuosity of veins. We show that there is a relatively strong correlation between arterial tortuosity in left and right eyes in the presence of liver disease. We also demonstrate a strong correlation between arterial tortuosity and the stage of liver disease.
BILIARY EPITHELIAL TO MESENCHYMAL TRANSITION CONTRIBUTES TO PORTAL TRACT FIBROGENESIS IN PRIMARY SCLEROSING CHOLANGITIS
H. L. Marshall1, H. Robertson1, A. D. Burt1, D. E. J. Jones1, J. A. Kirby1, M. Hudson2. 1Institute of Cellular Medicine, University of Newcastle, 2The Liver Unit, Freeman Hospital, Newcastle upon Tyne, UK
Introduction: Damage and loss of intra-hepatic bile ducts are characteristic features of a range of chronic inflammatory liver diseases, including primary sclerosing cholangitis (PSC). Progressive cholestasis may predispose to portal fibrosis and biliary cirrhosis and is generally accompanied by an increase in bile ductules at the interface with the parenchyma, in turn thought to be a driver for periportal fibrosis. Intrahepatic biliary epithelial cells (IBEC) are obvious targets for immune-mediated injury since they bind leukocytes. Indeed, recent studies have shown immune cells induce IBEC to undergo phenotypic transition to myofibroblasts. Proteomic features of epithelial mesenchymal transition (EMT) include loss of epithelial markers and acquisition of mesenchymal markers such as S100A4. Importantly, induction of S100A4 occurs sufficiently early to visualise epithelial cells in situ during the initial phases of EMT.
Aims & Methods: The study was designed to quantify EMT at different stages of PSC. Tissue sections from all histopathological stages of PSC were labelled by immunohistochemistry to detect antigens associated with bile ducts (cytokeratin (CK)-19 and E-cadherin), EMT (S100A4, vimentin and matrix metalloproteinase-2 (MMP-2)) and myofibroblasts (α-smooth muscle actin: αSMA). S100A4/CK-19 dual-labelled cells were counted in biopsy sections and expressed as the number of S100A4+ IBEC per mm2 of portal tract. Biopsies from donor livers on the day of transplant provided normal controls.
Results: Normal bile ducts did not express S100A4, vimentin, MMP-2 or αSMA. IBEC in PSC expressed S100A4, vimentin, and MMP-2 but not αSMA; colocalisation of both S100A4/CK 19 and S100A4/E-cadherin was observed in bile ducts and the ductular reaction. There was loss of CK-19 and cell-surface E-cadherin in some S100A4-expressing IBEC and a tendency for these cells to migrate from the ductular structures. αSMA-expressing myofibroblasts were only observed in areas of established fibrosis. There was a positive relationship between number of S100A4+ IBEC per mm2 portal tract and PSC stages 1–3 (including normal, stage 0 p<0.02).
Conclusion: The association between EMT in both bile ducts and the ductular reaction and stage of PSC provides good evidence of a pathogenetic role for EMT in the development of portal tract fibrosis in this disease.
CORTICOTROPHIN RELEASING HORMONE INCREASES POSTPRANDIAL BLOATING BUT NOT DISTENSION IN PATIENTS WITH IRRITABLE BOWEL SYNDROME
A. Agrawal, R. Lea, P. J. Whorwell, L. A. Houghton. Neurogastroenterology Unit, University Hospital of South Manchester, Manchester, UK
Introduction: Corticotrophin releasing hormone (CRH) mediates the stress response causing increases in both visceral sensitivity and motility.1 2 The effect of stress on the symptom of bloating and abdominal distension (that is, change in girth) in patients with IBS, which are also modulated by changes in visceral sensation3 and gastrointestinal (GI) transit4 remain unknown.
Aims & Methods: To assess the effect of CRH on postprandial bloating and distension in patients with IBS compared with healthy volunteers. A randomised, double-blind, placebo controlled, cross-over study in which the effect of CRH on meal induced bloating and distension were compared between 17 female IBS (Rome II) patients with a history of bloating (aged 21–42 years) and 10 healthy female volunteers (21–32 years). Abdominal girth was measured using the validated technique of Ambulatory Inductance Plethysmography5 and bloating using a Likert Scale of 0–5 (5 = very severe) for one hour before and two hours after a standard meal (1114 kcal). CRH 1 μg/kg or placebo was intravenously administered immediately after the meal and patients were studied during the luteal phase of the menstrual cycle or while taking the contraceptive pill.
Results: In IBS patients, CRH significantly increased postprandial bloating (change fasting to fed: CRH, +1.35 (1.04 to 1.66) (mean (95% CI)) vs placebo, +0.53 (0.23 to 0.83); p = 0.001) but not distension (+2.02 cm (1.37 to 2.67) cm vs +1.28 cm (0.74 to 1.82) cm) compared with placebo control. No such effects were seen in healthy volunteers (bloating: +0.50 (0.1 to 0.9) vs +0.27 (0.09 to 0.45,), distension: +1.41 cm (0.30 to 2.52) cm vs +1.38 cm (0.85 to 1.91) cm). Thus, the postprandial bloating response to CRH compared with placebo was greater in IBS patients compared with healthy volunteers (p = 0.02).
Conclusion: IBS patients exhibit an enhanced postprandial bloating response to CRH compared with healthy volunteers. This may be due to the sensation of bloating in IBS patients being in part related to visceral sensitivity3 which is increased by CRH.1 The lack of effect on distension, which has previously been shown to be directly related to transit time in IBS4 is probably explained by the fact that CRH increases motility and/or transit.
MEASUREMENT OF GLIADIN ALONE CANNOT PREDICT TOTAL GLUTEN CONTENT OF FOODS FOR COELIAC DISEASE SUFFERERS
H. J. Ellis1, M. C. Bermudo-Redondo2, M. L. Butero2, T. Suligoj1, C. K. O’Sullivan2, P. J. Ciclitira1. 1Nutritional Sciences King’s College London, Rayne Institute St Thomas’ Hospital, London, UK, 2Chemical Engineering, Universtidad Rovira i Virgili, Tarragona, Spain
Introduction: The gliadin fraction of wheat gluten has long been known to be coeliac disease (CD) activating. The other major wheat protein group, the polymeric glutenins, comprises low molecular weight and high molecular weight glutenin subunits (LMW-GS and HMW-GS). The latter was recently shown to exacerbate the CD. Less is known of the LMW-GS, but they are likely to be CD activating. Purified wheat starch is a standard constituent of many gluten-free foods for individuals with CD. Methods for gluten measurement have focussed on gliadins, whose content is multiplied ×2 to obtain total gluten content. However, this calculation is invalid, since high pressure liquid chromatography showed the ratio glutenin:gliadin varies from 0.2× to 5.8× in wheat starches. Draft legislation suggests the maximum permissible level of gluten in foods labelled as gluten-free should be 200 ppm gluten for rendered and 20 ppm for naturally gluten-free foods.
Aims & Methods: We previously developed monoclonal antibodies to HMW-GS and to the immunodominant gliadin epitope, α-2-57-75. Both antibodies recognised gluten from a wide variety of wheat cultivars. We used these antibodies in competitive ELISAs to measure HMW-GS and gliadin in a wide variety of gluten-free food types.
Results: In 5 wheat starches the ratio of HMW-GS to gliadin varied from 0.45× to 4.2×. The derived gluten content from gliadin ×2 in the last example would be 4.9 ppm, whereas gliadin plus HMW-GS was 12.4 ppm. In other foods the ratios of HMW-GS to gliadin were as low as 0.07×. Gluten-free pasta had 75 ppm gliadin, multiplied ×2 this would imply the product contained 150 ppm gluten, whereas gliadin plus HMW-GS comprised 88 ppm.
Conclusion: Within wheat varieties gliadin comprises 58–77% of total gluten and glutenins form 26–38%. Within glutenins LMW-GS comprise 19–25% of total gluten and HMW-GS 7-13%. However, owing to differing solubility characteristics of gluten protein fractions, huge variation in their final content may occur after processing. Thus the ratio of HMW-GS to gliadin in wheat starches varied 10-fold, and in other food samples variations of up to 68× were seen. We did not measure LMW-GS, however it is most unlikely that the proportion of these proteins varied inversely with HMW-GS sufficient to account for the wild fluctuations in the HMW-GS to gliadin ratio. Measurement of gliadin ×2 will lead to potential gross under and overestimations of total gluten content. If new guidelines are to be introduced with limits as strict as 20 ppm it will be essential to measure all of the toxic fractions independently rather than relying on the calculation gliadin ×2 = gluten.
A COMPARISON OF OUTCOME PREDICTIVE SCORES FOR ACUTE HAEMORRHAGE FROM OESOPHAGEAL VARICES
P. D. Dunckley1, N. Rajoriya2, K. Tweed2, J. Booth2. 1Gastroenterology Department, Gloucestershire Royal Hospital, Gloucester, 2Gastroenterology Department, Royal Berkshire Hospital, Reading, UK
Introduction: Several validated scoring systems have been developed to predict mortality from an acute upper gastrointestinal haemorrhage including the Rockall (RS) and Blatchford (BS) scores. Oesophageal variceal bleeding represented only 4% of the sample studied for the development of the RS and 6% for the BS. Whether these scores can be accurately used to predict outcome in suspected oesophageal variceal haemorrhage is less clear. The MELD and Child-Pugh (CPS) scores have also been shown to predict mortality in patients with acute variceal haemorrhage.
Aims & Methods: The aim of this study was to compare these four scores and their ability to predict inpatient mortality, 30-day re-bleed rates and transfusion requirements in patients with acute oesophageal variceal haemorrhage. Case notes of patients admitted to a single centre (RBH) were reviewed for the period between January 2000 and December 2006. Demographic, clinical, biochemical and haematological parameters were collected in order for the MELD, PS, CPS and BS scores to be calculated. Main outcome measures of in-patient mortality, 30-day re-bleed rates and transfusion requirement were documented.
Results: During the period of study, there were 86 admissions in 63 patients with proven acute oesophageal haemorrhage. The overall inpatient mortality was 17.4%; the 30-day re-bleed rate was 15.1% and the mean number of units of blood transfused was 5.1 units (SD-4.5). Receiver operating characteristic (ROC) curves were calculated to assess the performance of the scores. All four scores significantly predicted in-patient mortality (RS – area 0.71, 95% CI 0.57 to 0.84, p = 0.01; BS – area 0.76, 95% CI 0.64 to 0.87, p<0.01; CPS – area 0.74, 95% CI 0.61 to 0.87, p<0.01; MELD – area 0.73, 95% CI 0.58 to 0.88, p<0.01). Likewise all scores correlated with the total units of blood prescribed (RS – p = 0.001 (one-way ANOVA), CPS – p = 0.02 (one way ANOVA); MELD – Pearsons R –0.28, p<0.05; BS – Pearson’s R – 0.25, p<0.05). However, only the RS predicted 30-day re-bleed (RS – area 0.70, 95% CI 0.56 to 0.84, p = 0.03; BS – area 0.59, 95% CI 0.42 to 0.77, p = 0.29; CPS – area 0.55, 95% CI 0.37 to 0.73, p = 0.60; MELD – area 0.54, 95% CI 0.35 to 0.72, p = 0.69).
Conclusion: All four scores (RS, BS, CPS and MELD) predict in-patient mortality and correlate with the number of units of blood received by the patients suffering from acute oesophageal haemorrhage. The RS is the only score to predict 30-day re-bleeds. We propose therefore that the RS is the score of choice for predicting outcome in acute oesophageal haemorrhage, especially in light of its widespread use in upper gastrointestinal bleed integrated care pathways and its simplicity of use.
VIP ENDOSCOPY: THE RED CARPET TREATMENT?
C. W. Pritchard, P. M. Neville, M. J. Webberley. Department of Gastroenterology, Nevill Hall Hospital, Abergavenny, UK
Introduction: The VIP (virtual in-patient) system was introduced into our hospital in 2006. VIPs are patients who present to the acute hospital services or who are currently in-patients, who need urgent investigation, but do not necessarily require in-patient care. They are ‘admitted’ onto a virtual ward on the Clinical Work Station (CWS), but discharged from the hospital. Once their investigations are complete and their management plan decided, they are discharged from the virtual ward. The system has been used by both physicians and surgeons. It has allowed early discharge of patients from hospital but minimises their risk of being lost to follow-up.
Aims & Methods: VIP has successfully included many investigative modalities but here we have evaluated the patients referred for endoscopy.
Results: 103 procedures were performed over a 4-month period. Of this, 74 (72%) were OGDs, 10 (9.5%) were colonoscopies and 19 (18.5%) were sigmoidoscopies. 70% were booked within 48 hours of presenting and 30% were in-patients. The median time to procedure from booking, was 5 days, with 90% having been performed within 10 days. This amounted to 441 bed days saved over the study period (3.6/day). Of the gastroscopies, dyspepsia and abdo pain accounted for 50% of the indications, whereas upper GI bleed was only 22% (Rockall 1 or less), and a normal examination was found in more than 50% of patients. Of the colonoscopies, anaemia was the commonest indication (50%) and in 8 (70%) the procedure was normal. PR bleeding accounted for 60% of the indications for sigmoidoscopy and in 48% the procedure was normal. There were no adverse events recorded whilst patients were on the virtual ward and all patients were safely discharged to home following their procedure and no-one was lost to follow-up. 33 patients went on to have further investigations as out-patients.
Conclusion: We believe VIP to be a safe, popular and bed-efficient system for managing GI patients who would otherwise be admitted for investigation. It is easy and cheap to set up and requires little administration.
IS THERE A CASE FOR ROUTINE DUODENAL BIOPSY AT GASTROSCOPY OR IS A TARGETED APPROACH ADEQUATE? A RETROSPECTIVE AND PROSPECTIVE EVALUATION
A. D. Hopper, T. S. Chew, D. S. Sanders. Gastroenterology, Royal Hallamshire Hospital, Sheffield, UK
Introduction: Current UK recommendations advocate duodenal biopsy (DB) at the time of gastroscopy if there is evidence of anaemia or mal-absorption (weight loss or diarrhoea). However in “real” clinical practice DB rates have been reported as varying considerably (31–74%). For this reason routine DB has been suggested in order to avoid missing treatable disease—for example, coeliac disease or giardia.
Aims & Methods: We aimed to compare the diagnostic yield of routine DB against a policy of targeted DB using “high risk” indications. Initially, we retrospectively examined the endoscopy and histopathology database in our hospital from January 2003 to January 2004 to obtain data on our current practice. We obtained the number of gastroscopies and DB performed. Subsequently, consecutive adult patients referred for gastroscopy were prospectively recruited by a single endoscopist over a 26 month period (January 2004 to April 2006). All these patients had routine DB performed. In this prospective group patients were identified if they had target symptoms that should prompt an endoscopist to obtain DB. Patients were excluded if they had a coagulopathy, active gastrointestinal bleed or a suspected carcinoma observed during the examination (n = 220). We noted the number of new diagnoses of coeliac disease and giardia made from the DB in both groups.
Results: In the retrospective group 5979 gastroscopies were performed and analysed, 1464 with DB (DB rate 24.5%). In the prospective group 2220 gastroscopies were performed with routine DB taken in 2000 (DB rate 90.1%), 739 of these patients had target biopsy indication symptoms: a prevalence of 37.0%. The biopsy rates and diagnostic yields of the two groups are shown in the table. By performing routine DB, the DB rate increased by 3.7 (90.1/24.5)-fold. This was reflected by a similar and significant 4.17 (0.4/0.084)-fold increase in giardia prevalence and 3.9 (3.9/1.0)-fold increase in coeliac disease prevalence at gastroscopy (p<0.01). When comparing the prevalence of findings of targeted versus a routine DB policy there was a small non significant (p = 0.68) decrease in the prevalence of coeliac disease (3.9 to 3.6%) and also similar findings were observed in the giardia prevalence (0.4 to 0.1%) (p = 0.11). However there was a 2.7 (2000/739)-fold decrease in duodenal biopsy rates (p<0.0001) by adopting the targeted approach.
Conclusion: The diagnostic yield for coeliac disease and giardia is significantly increased by performing routine duodenal biopsies. However with accurate targeting of patients with anaemia or malabsorption, the number of DB can be significantly reduced without a significant reduction in the detection rate of small bowel disease.
Endoscopy posters
ENDOSCOPIC ULTRASOUND PREDICTS PATIENTS WITH OESOPHAGEAL CANCER WHO BENEFIT FROM NEOADJUVANT THERAPY
N. S. Balaji1, R. Melhado1, A. Fowler1, N. Wariach1, A. Goddard2, P. C. Leeder1, A. Cole2, S. Iftikhar1. 1Upper GI Surgery, 2Gastroenterology, Derby Royal Infirmary, Derby, UK
Introduction: Endoscopic ultrasound (EUS) remains the most accurate tool for staging of loco regional disease in oesophageal cancer. Neoadjuvant chemotherapy is proven beneficial in operable locally advanced T stages (>T2) and Nodal (N1) disease based on recent UK trials. The aim of this study was to assess the role of EUS in identifying patients with advanced locoregional disease who are likely to benefit from neoadjuvant treatment.
Aims & Methods: The study group included patients who underwent resection for carcinoma of the oesophagus following preoperative EUS over a 10-year period. Those who received neoadjuvant therapy were excluded. EUS stage was compared with pathologic staging. The accuracy of EUS in identifying patients who would benefit from neoadjuvant therapy (T2 N1, T3N0 or greater) was determined.
Results: 118 patients had EUS staging prior to resection. 31 patients underwent preoperative chemotherapy and were excluded. The mean age was 63 (SD 8.9) with an M: F distribution 4:1. Oesophagectomy was performed by an Ivor Lewis approach in 41 patients, left thoracotomy in 45 and a 3-stage approach in 1 patient. R0 resection was achieved in 66% of patients. The mean lymph nodal yield was 13 (SD 6). EUS predicted T stage was accurate in 55% of T1, 45% of T2, 66% in T1+T2 combined and 77% of T3 disease. T4 disease was excluded (unresectable). EUS predicted N stage was accurate in 56% of N0 and 60% of N1 disease. Locally advanced disease (T2N1, T3NO or greater) was predicted accurately in 89% of patients. The sensitivity of EUS for predicting the above group of patients who would benefit from neoadjuvant chemotherapy was 90% with a positive predictive value of 84%.
Conclusion: Although the sensitivity of EUS varies with T and N stage, the combined stage prediction of locally advanced disease is accurate. EUS remains a valuable tool in identifying this subset of patients in whom neoadjuvant chemotherapy offers a survival benefit following surgery.
OUTCOMES AND PERCEPTIONS OF A HIGH-STAKES COLONOSCOPY SKILLS ASSESSMENT: THE JOINT ADVISORY GROUP/BOWEL CANCER SCREENING PROGRAMME SCREENING COLONOSCOPY ASSESSMENT
R. Barton. For the Joint Advisory Group on Gastrointestinal Endoscopy and NHS Bowel Cancer Screening Programme, Newcastle University and Northumbria Healthcare NHS Trust, Newcastle upon Tyne, UK
Introduction: The introduction of an assessment of candidate colonoscopists wishing to provide the NHS Bowel Cancer Screening Programme created strong feelings in the endoscopy community, with concerns about the appropriateness and robustness of the process.
Aims & Methods: The aims of this study were to evaluate the performance and outcomes of candidates in the assessment, and their perceptions of the process. Data were collected as part of the accreditation process, and comprised quantitative data on performance in MCQ and DOPS assessments, and qualitative data on candidates’ perceptions of the assessment.
Results: Seventy six assessments were undertaken, by 67 candidates. Candidates had performed a mean (SD) of 2490 (1506) colonoscopies, range 500–7500, and detected polyps in a mean 29% (8%) of cases, range 18–53%. Mean MCQ score was 80% (6.3%), range 59–98%. Eight assessments were repeated, three for breach of process protocol with the DOPS assessment on the 1st or 2nd occasion, and 5 as a true re-sit assessment. Of 73 secure assessments, 54 (74%) candidates met the criteria. There were comments about the ambiguity of some MCQ questions “content fine but considerable ambiguity”, the clarity of the photographs “pictures unclear to make a measured judgement”, the relevance of some questions, and the inclusion of some controversial topics “There is some disagreement between experts on the management of depressed polyps”. Suggestions included using video clips rather than static photographs. There was confusion around whether or not the MCQ was negatively marked. With respect to the DOPS, candidates commented on the stress and anxieties provoked, “The process is hugely stressful. The examiners put me at ease but preassessment stress was very high” and “nerve racking but enjoyable”. They noted the luck involved in the cases encountered, “Very friendly and relaxed. Only problem it relies on individual patients having appropriate colons” and the lack of familiarity with the assessing unit, “Better in base hospital, could have been made less threatening.” They largely felt welcomed, “very relaxed non intimidating atmosphere” and that the assessment was fair “I think it is a fair assessment and very little improvement required” and “The process as written entirely fair, difficult two cases”. There have been five appeals against the results referred to the Accreditation Panel, with one upheld as a process breach.
Conclusion: Despite significant initial concerns, the overall process seems to have a reasonable level of acceptance. The MCQ clearly needs work and no-one has yet been failed on this basis. The DOPS, while nerve-racking in an unfamiliar environment, is generally well accepted. Further work on refining the process continues.
INITIAL EXPERIENCE OF THE NEW CYTOBRUSH IN THE ENDOSCOPIC ULTRASOUND MANAGEMENT OF PANCREATIC CYSTIC LESIONS- PROCEDURAL CHARACTERISTICS, CYTOLOGICAL YIELD AND SAFETY PROFILE
H. Karageorgiou, J. R. Bebb, K. Ragunath, G. Aithal. Gastroenterology, University Hospital, Nottingham, UK
Introduction: Endoscopic ultrasound (EUS) guided FNA of pancreatic cyst fluid is one of the most accurate methods of diagnosis of the nature of pancreatic cystic lesions but is still of limited sensitivity. A new through-the needle cytologic brush system has recently been approved for use during evaluation of cystic lesions of the pancreas. An initial study of 10 patients1 suggested use of brush was superior to standard FNA.
Aims & Methods: In a tertiary referral centre we have reviewed the clinical applicability of the cytobrush in the EUS evaluation of pancreatic cystic lesions in 38 consecutive EUS examinations.
Results: 38 EUS examinations were carried out on 32 patients with pancreatic cystic lesions over 30 months (median age 60, range 24–83, 53% male). 15/32 patients had a history of pancreatitis or EUS criteria for chronic pancreatitis on the day. The echobrush was used in 23 cases- on 15 occasions through the stomach. We were unable to use the echobrush in all cases for the following reasons: technically difficult or unable to use 19G needle, unable to puncture cyst wall, clinically inappropriate, technical malfunction. Cellularity yield was adequate in 19/23 (83%) cases. There were no major complications after any of the procedures. The final diagnoses (after minimum 6 months follow-up, including surgery) were pseudocyst (15), benign cyst (8), premalignant lesion (4) and malignant lesion (4). The cytobrush was used in all 4 malignant cases (adequate cells in 3 cases) with malignant cells (C5) seen in 2 of the patients.
Conclusion: This is the largest reported series of use of the cytobrush in routine EUS assessment of pancreatic cystic lesions. Our initial experience is that it is safe and technically feasible to use in most cases with good cellular yield. We feel that the cytobrush probably has a complementary role alongside other modalities in the management of cystic pancreatic lesions.
ENDOSCOPIC ULTRASOUND FINE NEEDLE ASPIRATION: A VALUABLE TOOL FOR EVALUATION OF MEDIASTINAL PATHOLOGY
G. C. Bennett1, R. Bambury1, S. O’Riordan1, R. Sugrue1, S. Sengupta1, E. Clarke1, J. Lennon1, N. Mulligan2, T. Kelleher1, P. MacMathuna1. 1Gastrointestinal Unit, 2Department of Pathology, Mater Misericordiae University Hospital, Dublin 7, Ireland
Introduction: Endoscopic ultrasound (EUS) with fine needle aspiration +/− biopsy (FNAB) is established in the diagnosis and staging of upper GI tract malignancy. Mediastinoscopy has been the usual method for sampling mediastinal nodes and masses. EUS FNAB provides a promising alternative in select cases.
Aims & Methods: We report our experience with EUS FNAB for mediastinal disease. In 35 patients referred for FNAB, we reviewed demographic information, radiology, surgical records, follow-up information, indication, diagnostic yields and complication rates.
Results: The indications were: mediastinal mass (n = 10), mediastinal nodes (n = 24) and oesophageal submucosal lesion (n = 1). A specimen adequate for diagnosis was obtained in 32/35 (91%). Follow-up data were available in 30 patients. Malignancy was identified in 15/30 (50%) (NPV 100%, PPV 100%). In 12/26 (46%), benign disease was found. No false negatives were identified. Post-procedure chest pain occurred in 2 patients.
Conclusion: EUS FNAB is a safe and reliable method for obtaining tissue from the mediastinum with high diagnostic accuracy. It provides a relatively non-invasive, safe and effective alternative to mediastinoscopy/CT guided biopsy in the management of mediastinal disease.
OUTCOME OF PATIENTS WITH UPPER GASTROINTESTINAL HAEMORRHAGE UNDERGOING DELAYED OUT-PATIENT ENDOSCOPY
S. Bhat, M. McLoughlin, T. C. K. Tham. Division of Gastroenterology, Ulster Hospital, Belfast, UK
Introduction: Ideally, all patients who present with an upper GI bleed should have an in-patient endoscopy. However, studies have shown that patients felt to be at low risk, according to a verified scoring system, could have the procedure as an out-patient without suffering any increase in morbidity or mortality. However, these studies were performed in healthcare systems where out-patient endoscopy can be performed within 48 hours. No studies have evaluated the outcome of such patients awaiting delayed outpatient endoscopy in a healthcare system with limited resources such as the NHS.
Aims & Methods: To determine if patients who were discharged for delayed out-patient endoscopy suffered adverse events while awaiting their procedure. We identified consecutive patients with upper GI haemorrhage who were discharged for out-patient endoscopy. A clinical Rockall score was generated retrospectively for each case. Those with a score of 0 were considered low risk for adverse events. Follow-up was obtained from the patients’ notes.
Results: 44 patients (27 males, 17 females), with a median age of 45 (range 17–91), were discharged for an out-patient endoscopy. The average delay from discharge to endoscopy was 85.5 days (range 1–318). 18 patients had a clinical Rockall score of 0, 12 had a score of 1, 5 had a score of 2 and 9 had a score of more than 2. The average length of stay for all patients was 3.6 days (range 1–21). In general, those with a Rockall score over 2 had longer hospital admissions (average 5.8 days). There were no deaths but 2 patients, with initial scores of 1 and 0, were re-admitted at 10 and 60 days respectively while awaiting OGD. The first required a blood transfusion and was diagnosed with a Mallory-Weiss tear. The second discharged himself after readmission without waiting for an inpatient endoscopy. Of the 33 patients who proceeded to out-patient endoscopy 14 had a normal OGD, 11 had either oesophagitis, gastritis or duodenitis, 6 had a hiatus hernia, 1 had Barrett’s oesophagus and 1 had a Mallory Weiss tear. 11 patients did not have an OGD. Of these, 8 did not attend, 1 patient was still awaiting endoscopy, intubation was not possible in 1 patient and in 1 elderly patient the family cancelled the procedure.
Conclusion: Despite a delay in out-patient endoscopy for those with upper GI haemorrhage, only 2 of 44 (4%) were re-admitted with an upper GI haemorrhage while awaiting their endoscopy. It is doubtful if an in-patient endoscopy in these cases would have changed their outcome. The decision to discharge patients before endoscopy on the basis of a low clinical Rockall score, or a length of stay of more than 3 days when there has been no rebleeding, appears to be associated with a satisfactory outcome in the majority of cases despite a delay in endoscopy.
MISSED DIAGNOSES IN PATIENTS WITH UPPER GASTROINTESTINAL CANCERS
D. H. Chowdhury, P. Bhandari, P. Goggin, R. Ellis, Q. Amanda, T. Trebble, S. Toh, S. Sommers, H. Duncan. Gastroenterology, Queen Alexandra Hospital, Portsmouth, UK
Introduction: Upper GI cancers are common and in spite of all the effects and improvements in the treatment modalities the overall survival is not improving. This is due to the cancer being diagnosed at a relatively advanced stage. There is evidence to suggest that most patients presenting with cancer have dyspeptic symptoms for many years predating these presentations with the increasing use of endoscopy and imaging techniques a lot of these patients would have had gastroscopies in the past. We believe that oesophageal and gastric cancers in their early stages are difficult to diagnose and could be missed at endoscopy.
Aims & Methods: The aim of our study was to: identify what percentage of patients have had imagings in the 3-year period prior to their presentation with cancer; to correlate the endoscopic findings with their current presentation; to identify the “missed early cancer” rate. Missed cancer was defined as a cancer patient who had a gastroscopy within 3 years prior to the index endoscopy (at which cancer diagnosis was made) and was found to have either normal or benign findings. We retrospectively analysed the patient records of 124 consecutive patients diagnosed with oesophageal and gastric cancers at our centre. We recorded timing of previous endoscopy, endoscopic findings, and surveillance or non-surveillance type of endoscopy, stage of the cancer and histological type of cancer. The reasons for failure or missed diagnoses were documented.
Results: Of the 124 patients, 14 (12%) had undergone a minimum of one endoscopy within the previous 3 years, 5 (36%) of these within the previous 1 year. 80% (11/14) of these patients had significant symptoms at the time of previous endoscopy. 12/14 of these patients with missed cancers had oesophageal cancers while 2/14 had gastric cancers. The endoscopy findings at the time of previous endoscopy (missed cancer) included normal (4/14), oesophagitis (8/14) and gastritis (2/14).
Conclusion: In our series endoscopic cancer miss rate is 12% for oesophago-gastric cancers. The exact reasons for this miss rate is not clear from our work but we believe that majority of these patients must have had very subtle endoscopic changes, the understanding of which lacks in western endoscopists. Advances in endoscopic imaging and increasing awareness of endoscopic appearances of early cancers should help reduce this miss rate.
LOCALISATION OF COLORECTAL TUMOUR AT COLONOSCOPY: DO WE KNOW WHERE WE ARE?
B. J. Colleypriest, P. F. Marden, A. Nicol, E. Griffiths, J. D. Linehan. Gastroenterology, Royal United Hospital, Bath, UK
Introduction: Quality and safety indicators for colonoscopy from the JAG have recently been revised and await ratification. It is suggested that suspected malignant polyps and that tumours if small, or the position unclear to the endoscopist are tattooed.1 Quality standards specific to colonoscopy in the National Bowel Cancer Screening Programme set as an objective in the planning of surgery the identification of tumour position in the correct segment of the colon in >95% of cases and tattooing of suspected malignant polyps in 100%. A previous American study has quoted a figure as high as 21% for endoscopist’s inaccuracy in correctly identifying tumour position at colonoscopy.2
Aims & Methods: This study aims to assess the ability of UK colonoscopists to identify the correct anatomical position of a colorectal tumour during the procedure. The endoscopy reporting system was interrogated for the findings of tumour or carcinoma on reports from June 2004 to August 2006. The endoscopically reported location of the tumour was recorded and compared with the pathology report of all patients proceeding to surgical resection. The colon was divided into segments as specified on the endoscopy reporting program (see table). The endoscopist was deemed inaccurate if there was discrepancy of more than one segment.
Results: 251 patients with a colorectal tumour found at colonoscopy were identified, 142 were male and 109 female. 200 of these had histologically confirmed cancers. 159 patients (87 male and 72 female) proceeded to surgical resection. 4 histology reports could not be found. Complete agreement between colonoscopy report and histology report was found in 94 (61%) cases. The endoscopic localisation was found to be inaccurate in 26 (17%) cases.
Conclusion: This study shows a significant inaccuracy in colonoscopy reporting of colorectal tumour location similar to figures published from North America.2 In 17% of cases there was a discrepancy of more than 1 segment and only 61% were accurate. Current BSG Quality and safety guidelines suggest tattooing colorectal tumours if small or the position is unclear and is an auditable outcome. Our data suggest that endoscopic localisation of tumours is unreliable and tattooing of all tumours should be mandatory.
COLORECTAL CANCER FOUND DURING COLONOSCOPY: HOW MANY BIOPSIES ARE NECESSARY?
B. J. Colleypriest, P. F. Marden, L. Ayres, B. Doshi, A. Nicol, E. Griffiths, J. D. Linehan. Gastroenterology, Royal United Hospital, Bath, UK
Introduction: Identification and diagnosis of colorectal tumours usually result from biopsies taken at colonoscopy. On occasions when the diagnosis is not clear from the first set of biopsies further sampling may necessitate a repeat colonoscopy with its inherent risks. Currently there are no guidelines recommending the number of biopsies that should be taken on the index colonoscopy. Studies asking the same question in oesophageal1 and combined upper GI cancer2 suggest 6 and 7 biopsies respectively. BSG guidelines for the management of oesophageal and gastric cancer reference a paper suggesting 6 biopsies.3
Aims & Methods: To suggest the optimal number of biopsies necessary. Data were collected on all colonoscopies with a diagnosis of suspected cancer over a 26-month period. Histological data were collected for initial and repeat biopsies and subsequent surgical specimens. The patients were divided into 2 groups, carcinoma correctly diagnosed at initial biopsy and those needing a second colonoscopy or surgery for diagnosis. Severe dysplasia was counted as a correct diagnosis unless this diagnosis was unsure and a repeat colonoscopy resulted.
Results: 217 patients were identified of whom 198 had a histological diagnosis of cancer. Of these 198 patients 182 were correctly diagnosed at index colonoscopy and 16 were diagnosed either on repeat colonoscopy (10) or at surgery (6). Nine patients with suspected cancer not confirmed on initial biopsies neither progressed to surgery nor were re examined endoscopically. 10 patients with suspected cancer were re-examined and diagnosed with non-malignant disease. The number of biopsies in the 16 patients with cancer “missed” at index colonoscopy were statistically lower when compared with the correct group (5.729±0.1392 vs 4.250±0.4031, p = 0.0025).
Conclusion: This study demonstrates that the sensitivity of diagnosis of a suspected cancer increases with the number of biopsies. A high degree of statistical significance was noted in the lower number of biopsies taken in the group of patients with an initial missed diagnosis. The combined sensitivity of taking 5 or fewer biopsies (85%) was significantly lower compared to more than 5 (98%) or 6 (99%). We suggest that at least 6 biopsies should be mandatory as a national auditable standard in the context of suspected cancer.
DOUBLE BALLOON ENTEROSCOPY: A LEAP FORWARD IN THE MANAGEMENT OF SMALL BOWEL CROHN’S STRICTURES
E. Despott1, E. Tripoli1, A. Polecina1, K. Konieczko2, C. Fraser1. 1Wolfson Unit for Endoscopy, St Mark’s Hospital, 2Department of Anaesthesia, St Mark’s and Northwick Park Hospitals, London, UK
Introduction: Small bowel strictures are a common, debilitating complication of Crohn’s disease (CD) that frequently result in the need for surgical treatment. Apart from the inherent risks of the morbidity and mortality associated with major surgery, afflicted patients also face the threat of resultant short bowel syndrome. Double balloon enteroscopy (DBE) with its unique ability to provide endotherapy to previously inaccessible parts of the small bowel, may make it possible to treat CD related strictures safely and at low risk to patients. We report our preliminary experience with DBE and CD stricture dilatation since the introduction of the service in February 2005.
Aims & Methods: A prospective proof of concept analysis of stricture dilatation by DBE in CD, assessing the feasibility of the procedure, symptom improvement and surgical requirements post procedure. Patients referred for stricture dilatation at DBE had the procedure done under general anaesthesia. Stricture dilatation was performed using controlled radial expansion (CRE) balloon dilators with fluoroscopic guidance. These patients remain under follow-up for recurrence of their symptoms and the need for surgical intervention.
Results: Eight patients (mean age 44.8, range 30–52 years) with CD related strictures were referred for DBE stricture dilatation due to obstructive symptoms. The strictures were diagnosed radiologically, were shown to be <5 cm in length and were refractory to medical therapy. Balloon stricture dilatation was performed successfully in 6/8 patients with a mean dilatation diameter of 15.4 mm (range 12–20 mm). In 2/8 patients, fixation of the small bowel due to adhesions, made reaching the strictures at DBE impossible. These 2 patients required surgical stricturoplasty. In the 6 patients where stricture dilatation was done at DBE, symptoms improved dramatically and to date there was no need for surgical intervention. The mean follow-up period was 8.8 months (range 2–28 months). There were no clinically important complications.
Conclusion: Our preliminary proof of concept experience regarding the use of DBE in CD related stricture dilatation shows promise. The procedure was feasible and safe and to date has had satisfying results. The potential for DBE to revolutionise the current management of CD small bowel strictures and avert surgical intervention, merits further evaluation in larger studies with more prolonged follow-up. The impact of this approach on patient quality of life, avoidance of surgery associated risks and small bowel saving potential could be significant.
A PROFILE OF COLONIC POLYPS IN THE NORTHEAST OF ENGLAND AND ITS IMPACT ON COLONOSCOPIC PRACTICE: THE SOUTH DURHAM POLYP PILOT STUDY
T. Wood1, C. Westwood1, K. Gunning1, A. Dhar2. 1Colorectal Surgery, Darlington Memorial Hospital, 2Department of Gastroenterology, Bishop Auckland General Hospital, County Durham, UK
Introduction: The clinico-epidemiological profile of colorectal polyps in the Northeast of England is not well described. The performance of colonoscopy and polypectomy in the region needs to be analysed particularly in preparation for bowel cancer screening, due to start in 2007 in the County.
Aims & Methods: To study the clinical characteristics of colonic polyps in the South of Durham, using a pilot cohort of approx 200 patients, and also analyse the performance of colonoscopic polypectomy and adherence to BSG guidelines. The histopathology database (SNOMED) was interrogated to identify a random set of 200 patients with colonic polyps between July 2005 and June 2006. Case notes and endoscopy reports were manually reviewed to include patient demographics, polyp characteristics, dysplasia grade, completeness of polypectomy and adherence to surveillance guidelines.
Results: 160 patients (M: F = 1.46, 55% over age 65 years) were included in this pilot study, with an adjusted caecal intubation rate of 93.8%. 213 polyps were found in these patients (mean 1.33 polyps/patient), with 78% having only one polyp and 22% having >2 polyps. 63% of all patients with polyps had adenomas. Of all polyps, 45% were metaplastic, 26% tubular adenomas and 21% tubulovillous, 4% villous and 1% had intramucosal carcinoma. Polyp sizes were as follows: <5 mm–68%, 6 to 10 mm–18%, 11 to 20 mm–6% and >20 mm–7%. Interestingly, 75% of the polyps were sessile or flat and only 20% were pedunculated. The base of the polyp was examined in only 16% patients after polypectomy. Histologically, the polyp removal was reported to be complete in 20%, incomplete in 14%, indeterminate in 34% and not commented in 32%. BSG guidelines for surveillance were adhered to in 85% of cases.
Conclusion: This pilot study shows that majority of the patients in this region have a single polyp, which is less than 10 mm in size but most of the polyps are sessile. This is likely to mean advanced saline lift polypectomy as the norm for most patients, but also a careful examination of the base to ensure complete excision. There is a need to improve adherence to BSG guidelines and improve our colonoscopy training by examining the base post polypectomy. The bowel cancer screening programme will give us more information as to whether the asymptomatic population has a different profile from the symptomatic population.
SAFE SEDATION IN ENDOSCOPIC PROCEDURES: IMPACT OF PETHIDINE ON 30-DAY POST-PROCEDURE MORTALITY
B. Doshi1, P. Marden1, B. Colleypriest1, G. Taylor2, D. Robertson1. 1Gastroenterology, Royal United Hospital, 2School for Health, University of Bath, Bath, UK
Introduction: Current endoscopy sedation protocols are based on the British Society of Gastroenterology guidelines issued in 2003. It recommends that minimum amounts of drug are used and that certain procedures may require a combination of benzodiazepine and opioid for adequate pain relief. The NCEPOD “scoping our practice” 2004 findings suggested that increased sedation may have contributed to 30-day post-procedure mortality (PPM). However, some studies have shown that reduced doses of midazolam did not result in a significant reduction in 30-day PPM.1
Aims & Methods: We retrospectively investigated the impact of a change in sedation practice on 30-day PPM in our unit. A total of 7122 endoscopic procedures performed over 12 months were identified on our electronic reporting system. Patients who died within 30 days of an endoscopic procedure were identified using the hospital IT system. The procedures were then assessed in two consecutive 6-month periods P1 (1/07/2006 to 31/12/2006) and P2 (1/01/2007 to 30/06/2007). Primary outcomes assessed were average dose (SD) of midazolam administered, frequency of pethidine use and 30-day PPM. Changes in sedation practice was assessed in different operator groups such as Consultants (Con), Non-Training Grade (NTG) such as associate specialist and general practitioners, Endoscopy Nurse Specialist (ENS) and Trainees.
Results: Total cases performed in P1 and P2 were 3509 (49.3%) and 3613 (50.7%) respectively. There was a significant increase in the percentage of cases who received pethidine in P1 compared to P2 (10% (223 cases) vs 19.1% (440 cases) (p<0.05)). This was accompanied by a reduction in average midazolam dose from P1 to P2 (3.5(1.2) mg vs 3.2 (1.2) mg (p<0.05)). The 30-day PPM remained similar in P1 and P2 (2% vs 2.5% (p = 0.23)). The Trainee group had the most significant increase in frequency of pethidine use (2.2% in P1 vs 14.3% in P2 (p<0.05)) and this was accompanied by a significant reduction in average midazolam dose (3.6 (1.3) mg in P1 vs. 2.9 (1.0) mg in P2 (p<0.05)). Their 30-day PPM did not alter significantly (2.6% in P1 vs 2.8% in P2 (p = 0.887)).The NTG group was the only other group to have had a statistically significant increase in frequency of pethidine use (5.9% in P1 vs 12.2% in P2 (p<0.05)). But the NTG group did not have a significant reduction in average midazolam dose (3.2 (0.9) mg in P1 vs 3.1 (0.9) mg in P2 (p = 0.46)). Interestingly, the 30-day PPM in the NTG group had a trend towards significance at 1.2% in P1 and 2.4% in P2 (p = 0.09).
Conclusion: Any interpretation of sedation related mortality should include analysis of both benzodiazepine and opioid administration. Despite a reduction in midazolam dose, a lack of improvement in 30-day PPM could be due to increased pethidine administration.
ENDOSCOPIC MANAGEMENT OF NON-VARICEAL UPPER GASTROINTESTINAL HAEMORRHAGE: RESULTS OF A QUESTIONNAIRE EVALUATING CURRENT PRACTICE
J. M. Dunn, A. McNair, V. Saxena. Gastroenterology, The Queen Elizabeth Hospital, London, UK
Introduction: Non-variceal upper gastrointestinal (UGI) haemorrhage is associated with a significant morbidity and mortality, which has remained unchanged for 50 years. There is good evidence that higher doses of 1:10 000 adrenaline (13–20 ml) and use of a second modality can improve outcome.1 Consultants should make trainees aware of this and ensure that they acquire these important endoscopic skills.
Aims & Methods: To evaluate current practice a questionnaire was sent to 38 specialist registrars in 16 acute hospitals across the South East Thames region. The questionnaire comprised of a clinical vignette describing a patient presenting with haematemesis, Rockall score = 8. A photograph showed a 1.5 cm duodenal ulcer with visible vessel. Questions on endoscopic management followed. A multinomial model of confidence in ability using 4 endoscopic therapies was evaluated. A 5-point quiz objectively assessed knowledge of UGI haemorrhage management. Training facilities were evaluated at each centre.
Results: Completed forms were returned from 15 hospitals (a 94% response rate) and from 29 trainees (an 80% response rate). The trainees were divided into two groups according to seniority; group A 3rd year or above; group B 1st and 2nd year. Results of multinomial model are shown (table). There was no significant difference in quiz scores (78% vs 68%, p = 0.12). 100% would use adrenaline as a first line. 69% of trainees would routinely use less than 10 ml of adrenaline, 71% in group A and 67% in group B (p = NS). There was considerable geographic variation in access to a second modality: heater probe (HP) or endoclip was available in 100% of hospitals inside M25, 78% outside. 50% of hospitals in the region had the choice of both. 73% of hospitals provided argon plasma coagulation (APC).
Conclusion: The majority of SpRs in South East Thames are not using high enough doses of adrenaline for treatment of bleeding ulcers. There was no significant difference in the proportion of senior trainees using higher doses of adrenaline, despite greater confidence and experience. As expected, senior trainees were significantly more confident in their ability to use a second modality. However 24% would use APC when not indicated and 76% did not know the energy setting for HP. Assuming the participants were representative of gastroenterology trainees in the UK, the quality and provision of training in the management of non-variceal UGI haemorrhage is currently inadequate.
GASTROINTESTINAL BLEEDING AND WARFARIN
P. Eadala, R. Crimmins, S. Dolwani, G. L. Swift, J. T. Green. Department of Gastroenterology, Llandough Hospital, Cardiff, UK
Introduction: Acute upper gastrointestinal bleeding (UGIB) is a common medical emergency with an incidence ranging from 50 to 150 per 100 000 of the population each year.1 Warfarin is commonly used to treat and reduce thrombo-embolic events. The GI tract is the most common site of bleeding in patients receiving anticoagulant therapy.2 Immediate endoscopy has been shown to have a lower yield in this group of patients and the group with negative findings have a favorable outcome.3
Aims & Methods: All patients presenting with acute UGIB between 1 June 2000 and 31 May 2005 to a single UK centre were identified. At the time of referral for endoscopy an initial proforma was completed as part of an ongoing audit and case notes were later retrieved to capture other data. Patients who were on warfarin were identified together with its therapeutic indications. They were subdivided on the basis of their target INR (International Normalised Ratio). Significant endoscopic findings were defined as: oesophageal ulcer, gastric ulcer, duodenal ulcer, carcinoma, angiodysplasia and varices. The presence of significant endoscopic findings and mortality was compared between the groups. Stastical analysis was performed using Fisher’s exact test.
Results: During this period 808 patients presented with UGIB, 80 (10%) were on warfarin. 47 (59%) had INR above their therapeutic range when compared to 33 (41%) whose INR was therapeutic/subtherapeutic at presentation. There is a lower yield of significant endoscopic findings (p<0.037) but no significant difference in mortality in those with INR above their therapeutic range when compared to those in the therapeutic/subtherapeutic range at presentation. Despite the above there was stastically demonstrable difference in mortality (p<0.049) but not in significant endoscopic findings in those on warfarin compared to those who are not.
Conclusion: Most of those who present with UGIB while on warfarin have an INR above their therapeutic range. Endoscopy in these patients has low yield but mortality is higher probably due to the fact that patients on warfarin tend to be older with significant comorbidities. Adequate resuscitation and correction of coagulopathy prior to endoscopy still form the mainstay of treatment.
A PROSPECTIVE STUDY TO DETERMINE FACTORS ASSOCIATED WITH INCREASED DISCOMFORT DURING COLONOSCOPY
D. A. Elphick, M. T. Donnelly, K. Smith, S. A. Riley. Department of Gastroenterology, Northern General Hospital, Sheffield, UK
Introduction: Colonoscopy can be an uncomfortable procedure. To increase safety, there is a trend towards lower levels of sedation and analgesia use during colonoscopy in the UK. In many endoscopy units, including our own, unsedated colonoscopy with or without use of inhaled nitrous oxide (entonox) is common practice and opiates are rarely used.
Aims & Methods: This study aimed to determine patient factors predictive of higher discomfort levels during colonoscopy. Patients undergoing outpatient colonoscopy were recruited. Patient age, sex, height, weight, surgical history, indication for colonoscopy, previous colonoscopy details were recorded. Patients were then asked to grade how uncomfortable they anticipated the test to be on a Numeric Rating Scale (NRS: zero (no discomfort) to 10 (maximal pain)). Scores were then recorded on the NRS for cannulation (22G), rectal examination, colonoscope insertion, every 2 minutes during the procedure, retroflexion in the rectum and extubation. An overall score for the procedure on the NRS was recorded on completion. The endoscopist graded procedure difficulty (0–10) and a hospital anxiety and depression score was filled by the patient. NRS scores of peak and overall discomfort were recorded between 2 and 3 months post procedure.
Results: 109 patients (44 male, 65 female; median age 61.5 (21–80) years) were recruited. 99 procedures were completed to caecal pole or terminal ileum, 44 received midazolam (median 2 (2–5) mg) and 88 used entonox. Mean overall NRS score was 4.72 (men 3.93; women 5.25; p<0.01) and mean peak score 6.97. Discomfort scores were higher in those with: irritable bowel syndrome (p = 0.03); diverticular disease (p<0.01); midazolam (p = 0.03), buscopan (p<0.001) or entonox (p<0.001) use; endoscope tracker use (p<0.01); incomplete procedures (p<0.001) or preceding gastroscopy (p = 0.02). Discomfort scores correlated with: anticipated discomfort rate (p<0.001), peak discomfort rate (p<0.001), endoscopist difficulty grade (p<0.001), patient anxiety (p<0.001) and depression (p = 0.02) scores. Discomfort during the procedure did not correlate to cannulation or rectal examination NRS score. Recollected overall discomfort scores 2–3 months following procedure were significantly lower than the originals (mean reduction 0.85) (p<0.001). However, this reduction was not influenced by the use of midazolam.
Conclusion: Colonoscopy can be an uncomfortable procedure. Factors indicative of difficult colonoscopy are associated with higher levels of discomfort, as are the presence of irritable bowel, high anxiety, depression and the anticipation of discomfort. Preceding gastroscopy worsens colonoscopy discomfort. Low dose midazolam neither relieves discomfort nor makes patients forget it. Selected patients may benefit from increased analgesia use.
ERCP TRAINING: WHAT HAS CHANGED IN THE LAST 5 YEARS?
A. D. Farmer, M. J. Brookes, P. G. Wilson. Department of Gastroenterology, City Hospital, Birmingham, UK
Introduction: Endoscopic retrograde choleangiopancreatography (ERCP) is perhaps the most difficult and skilled endoscopic procedure to learn. Despite less invasive diagnostic modalities being developed, demand for ERCP has remained static at a rate of 0.75–1 procedures per 1000 population.1 Training, and competency, in ERCP has long been a game of numbers and targets. In 1988, completion of 35 procedures deemed a trainee competent although this figure has risen to 300–450 procedures in 2007, with selective duct cannulation rates (SDCR) being a surrogate marker of the quality of training.2 The British Society of Gastroenterology ERCP survey in 20061 identified that only one third of trainees needed to become competent in ERCP to maintain the service.
Aims & Methods: The purpose of this survey was to assess trainees’ attitudes and exposure to ERCP training in the West Midlands and how this has changed over the last 5 years. All gastroenterology trainees in the West Midlands were approached to complete the survey. Trainees were surveyed in 2002 and 2007.
Results: The response rates were 23 out of 28 (82.3%) in 2002 and 36 out of 38 (94.7%) in 2007. The distribution of trainees through the training programme was similar. The table summarises the results.
Conclusion: It is apparent from this regional study that there has been a dramatic change in trainees’ attitudes and experience of ERCP training over the last five years. Because demand for training has decreased, with changing attitudes towards ERCP, smaller numbers of trainees are getting higher volume exposure to ERCP training. Training appears to have improved as reflected by the increase in SDCR, the reduction in major complications encountered and the total number of procedures completed and this is probably related to the numbers of ERCPs individual trainees are undertaking.
ENDOSCOPIC ULTRASOUND TRAINING: THE TRAINEES’ PERSPECTIVE
A. D. Farmer1, M. J. Brookes1, J. I. W. Jones2, P. G. Wilson1. 1Department of Gastroenterology, City Hospital, Birmingham, 2Department of Gastroenterology, Princess Royal Hospital, Telford, UK
Introduction: Endoscopic ultrasound (EUS) training within the UK is haphazard with piecemeal exposure. In addition, the lack of definitive guidance regarding curriculum and competence assessment from the Joint Advisory Group on Gastrointestinal Endoscopy serve only to compound this problem. These problems were highlighted as early as 2004 by the UK EUS Users group.1
Aims & Methods: The purpose of this survey was to assess trainees’ attitudes, and exposure, to EUS training in the West Midlands. Currently, there are 4 centres performing EUS in the region. All specialist registrars (SpRs) in gastroenterology in the region (n = 38) were approached either in person, by email or by telephone to complete the survey.
Results: 36 out of 38 SpRs responded to the survey (94.7%). 26 respondents (72%) were interested in pursuing training in EUS. 12 trainees (33.3%) intended to achieve accreditation in EUS prior to completion of training, although of these only 10 (27.7%) had done any EUS training. 5 respondents (13.8%) felt that obtaining accreditation in EUS was an essential part of training as a gastroenterologist. Indeed, 7 respondents (19.4%) felt that it would improve their job prospects if they were accredited in EUS. Experience of diagnostic EUS was limited with only 3 trainees having completed more than 40 procedures. Only 2 trainees had had any experience of interventional EUS. Of those intending to achieve EUS accreditation, they felt that training was hindered by the concomitant training of consultant staff (50%), other trainees (20%), lack of trainer availability (15%) and lack of time (15%). Only 1 respondent (2.7%) felt the current level of EUS training was adequate. No trainee had attended a national or international centre of excellence for specific EUS training. Trainees stated that the most important factor in improving EUS training should be the development of a dedicated training module (100%).
Conclusion: The experience of EUS among trainees in the West Midlands is low, although interest and enthusiasm is high. The reasons for this are several. These include the small numbers of centres performing the procedure, the relative low volume of procedures performed in the region and the concomitant training of local consultant staff. Training opportunities are likely to remain limited while capital costs of setting up EUS services remain high and the number of trainers small. If EUS is to grow as a diagnostic and therapeutic modality it is vital to have highly organised and coordinated training across the region. Clearly, provision needs to be made in terms of training courses and access for trainees to acquire EUS skills. We conclude that the establishment of a dedicated training module in EUS with defined goal orientated objectives and assessment, leading to accreditation, will improve the quality of EUS training and service within the region.
MORTALITY FOLLOWING PEG INSERTION IN A SCOTTISH DISTRICT GENERAL HOSPITAL
S. Ghosh, A. K. Ghosh, A. Roychoudhury, J. Rose. General Medicine, The Ayr Hospital, Ayr, UK
Introduction: Percutaneous endoscopic gastrostomy (PEG) is a widely used method for long term enteral nutrition whose appropriateness and safety have been critically examined in a recent report (Scoping our Practice. NCEPOD, 2004).1
Aims & Methods: To establish the safety of this technique as practiced in our hospital, we performed a retrospective case note analysis of the indications, risk factors, complications and mortality in patients with PEG insertion for the 10 years from 1996–2005. All patients were assessed by medical, dietetic and endoscopic unit staff and received parenteral antibiotics routinely before PEG insertion.
Results: Of 125 patients treated, adequate records were available for 109 (86%). Of these 36 were males and 73 females with a mean age of 65.4 years. The procedure was used in patients with CVA (60), dysphagia (41), aspiration (39), malnutrition (26) and MND or dementia (22) and was performed an average of 8.5 days after referral. Over 65% (71 patients) were alive at 28 days (cf: NCEPOD 75%) and a total of 58 (53%) were able to be discharged or transferred to long-term care. The common complications were chest infection (25), wound infection (11), peritonitis and sepsis (9) and pain (7). 35% (38 patients) died within 28 days, nearly three quarters (28 patients) of these within 14 days of the procedure. In a retrospective study of patients with multiple diseases it was not possible to ascertain the exact final cause of death. Although patients with aspiration may not benefit from PEG insertion, there was no excess of deaths of patients in this subgroup.
Conclusion: The majority of patients treated with a PEG tube in our hospital survived both the first month and to be discharged or transferred. Compared to the NCEPOD data early mortality (especially within the first two weeks) was higher in our audit (carried out on patient prior to NCEPOD) could probably be improved by better pre-assessment and stricter adherence to selection criteria. A prospective audit is essential to identify potential pitfalls in selection of patients and avoidance of complications related to PEG insertion.
USE OF ENDOSCOPIC ULTRASONOGRAPHY VERSUS OESOPHAGOGASTRODUODENOSCOPY IN ASSESSING INTESTINAL FAILURE ASSOCIATED LIVER DISEASE IN CHILDREN ASSESSED FOR INTESTINAL TRANSPLANTATION
P. McKiernan, K. Sharif, G. Gupte. Liver Unit, Birmingham Children’s Hospital, Birmingham, UK
Introduction: The severity of intestinal failure associated liver disease (IFALD) along with the presence/absence of portal hypertension determines the type of transplant recommended as per the international consensus criteria. The severity of IFALD is usually assessed histologically on liver biopsy and the presence of portal hypertension at esophagogastroduodenoscopy (OGD). Liver biopsy carries a risk of significant morbidity in this vulnerable group. Endoscopic ultrasonography (EUS) is a newer technique for detection of oesphagogastric varices (OGV) which can also detect extraluminal varices not seen by OGD. Using EUS in children being assessed for intestinal transplant might reduce the need for liver biopsy in this group.
Aims & Methods: To evaluate if EUS is more sensitive than OGD in detecting OGV in progressive IFALD. Children referred for liver and small bowel transplantation were assessed prospectively. 16 children (9M:7F, median age 13 months (range 7–88)) with progressive IFALD and splenomegaly were assessed by EUS and OGD to detect presence of GOV. EUS was performed with a high resolution endoluminal ultrasound miniprobe (UM-2R-3 20 MHz, Olympus UK) during conventional OGD. Results of EUS findings were compared with OGD examination.
Results: In 9 patients results of EUS and OGD were concordant, i.e., both positive (n = 2) or both negative (n = 7) for GOV. In 7 patients GOV were identified by EUS, but were not seen on OGD.Liver biopsy was avoided in 5 children by the use of EUS.
Conclusion: EUS can detect GOV not seen on OGD. EUS has changed our assessment strategy and is now used as the initial investigation method in evaluating the degree of IFALD.
MID-POINT RESULTS OF A RANDOMISED BLINDED CONTROLLED STUDY OF HANDS-ON THERAPEUTIC ENDOSCOPY TRAINING
A. V. Haycock, S. Thomas-Gibson. Wolfson Unit for Endoscopy, Imperial College London, London, UK
Introduction: Despite recent investment, there is limited evidence for the efficacy of intensive hands-on training courses in endoscopy. The St Mark’s Basic Therapeutic Endoscopy Course (BTEC) involves lectures and hands-on training in four therapeutic modalities: non-variceal upper GI bleeding, polypectomy and hot biopsy, oesophageal stricture dilatation and PEG insertion. Feedback from previous courses has shown it is considered to be an excellent training opportunity (mean rating 9.1 out of 10), but there has been no higher level evaluation of the benefits of the course.
Aims & Methods: The primary aim of the study is to evaluate the efficacy of the BTEC in delivering training in a range of basic therapeutic endoscopic techniques. Recruitment aims to enrol 32 delegates overall. Applicants to the course are randomised into subjects and controls. All delegates are initially assessed by blinded experts on procedural skills using procedure checklists and a global rating scale. They also complete a multiple choice questionnaire (MCQ) assessing knowledge of therapeutic endoscopy. Delegates are randomised to assessment before or after attending the lectures. The subjects then receive a half-day practical hands-on training as per the previous BTEC course, while the controls receive no hands-on training. All delegates are then re-tested on their procedural skills on each therapeutic modality.
Results: We report the mid-point results of the study (n = 17). There were no significant demographic differences between subjects and controls. There were no significant differences in initial practical assessment scores or MCQ score between delegates who had the lectures before or after testing. There was a significant improvement in the checklist score and overall score for subjects compared to controls for polypectomy and control of upper GI bleeding. There were differences for oesophageal dilatation and PEG insertion nearing significance.
Conclusion: There was no detectable benefit on practical skill or knowledge acquisition from the lectures. There were significant benefits from hands-on teaching on both skill at polypectomy and control of upper GI bleeding, with strong improvements in skill at oesophageal dilatation and PEG insertion. To confirm these results enrolment is continuing.
THE UK NATIONAL ENDOSCOPY TRAINING PROGRAMME HAS IMPROVED COLONOSCOPY TRAINING OVER A 5 YEAR PERIOD: CLOSING THE AUDIT LOOP
A. V. Haycock, J. H. Patel, S. Thomas-Gibson. Wolfson Unit for Endoscopy, Imperial College London, London, UK
Introduction: An audit in 20021 showed that colonoscopy training in the North West Thames deanery was poorly structured, with low levels of supervision and high complication rates. Since then, the UK National Endoscopy Training Programme introduced centrally funded, JAG accredited courses and new assessment tools to standardise training and raise the quality of practitioners. The primary aim of this study was to determine if this has had an impact on the standard of colonoscopy training in this region.
Aims & Methods: This was a cross-sectional survey. Questionnaires used in the previous study were updated and emailed to all gastroenterology and GI surgery trainees in the deanery and those who participated in the previous study. Trainees could complete the forms electronically and return them using an anonymous web-based secure upload portal.
Results: 37 out of 113 trainees responded (33%). 92% were aware of the JAG guidelines for training. Significantly more trainees said that they had been formally taught the principles of colonoscopy (89% vs 65%; p = 0.02), polypectomy (76% vs 53%; p = 0.04) and extubation (82% vs 55%; p = 0.02) than in 2002. Trainers are significantly more likely to be present in the room for a trainee’s first 100 colonoscopies (77% vs 49%; p = 0.04) and attempt explaining a solution to a problem before taking over (55% vs 23%; p = 0.03). Course attendance significantly increased (76% vs 45%; p = 0.006), and although most had to wait between 4–6 months to attend, all trainees were “quite” or “very” satisfied with the course. There was an increase in trainees who record their complication rate (51% vs 32%) although this was not significant (p = 0.11). Reported complication rates were lower, with 3 of 18 (16%) having had a perforation compared to 8 of 13 (61%) in 2002. 78% of trainees think that their training has been adequate or better than adequate, compared to 25% in 2002. The average caecal intubation rate, a surrogate marker of competence, did not change (90% vs 93%; p = 0.09).
Conclusion: There has been a significant improvement in colonoscopy training both at base hospitals and in access to specialist courses compared to 2002, although 83% of trainees believe that training can still be improved further. New technologies such as simulators and the 3D imager were considered by the majority to have contributed towards the improvement, but most trainees still feel they need greater regular access to dedicated training lists and courses. The central training programme and funding has made a significantly positive impact in this region. The loss of such investment may have a detrimental effect on future colonoscopy training.
GASTROINTESTINAL CANCER PREVALENCE IN IRON DEFICIENCY AND THE PREDICTIVE VALUE OF IRON INDICES
B. Hayee, S. Patel, J. O’Donohue, D. Reffitt. Gastroenterology, University Hospital Lewisham, London, UK
Introduction: In attempting to provide an efficient and cost-effective endoscopy service, “cut-off” criteria for investigating patients are useful tools to reduce the number of potentially inappropriate investigations. An audit of endoscopic investigation of patients referred for asymptomatic anaemia was carried out, changing local practice in terms of creating a new referral form with a mandatory requirement to enter iron indices to indicate the presence of true iron-deficiency anaemia (IDA). Concerns were raised regarding the validity of the use of such criteria to direct investigation. Results were therefore analysed further.
Aims & Methods: To determine the sensitivity, specificity and positive and negative predictive values of iron indices in the diagnosis of gastrointestinal (GI) cancer, data from an audit of endoscopic investigation of IDA were analysed over two three-month periods (2006–7). Iron deficiency (ID) was defined as a either mean cell volume (MCV) <76 fl or ferritin <15 μg/l (or <50 if ESR raised). With haemoglobin (Hb) level of <12.5 g/dl for men and <11.5 g/dl for women, these patients were termed “IDA”. Those with low Hb not fulfilling either of the two additional criteria were termed “non-IDA”.
Results: 221 patients (mean age 68.5 ± 16.9 years; 149 female) were analysed. 14 GI cancers were identified in the IDA group (n = 112) and 4 in the non-IDA group (n = 109): an overall prevalence of 8.1%. However, there were fewer cancers in the non-IDA group (3.5% vs 12.5%; two-tailed p = 0.025). Examination of the case-notes of this group revealed the presence of alarm symptoms in two of the four patients with GI cancer. Including these two patients, our results demonstrate a sensitivity (Sn) and specificity of iron-deficiency for detecting GI cancer of 77.8% and 51.7% respectively. Positive and negative predictive (NP) values were 12.5% and 96.3%. Raising the “cut-off” level for ferritin to 50 μg/l for all patients would increase the Sn and NP value to 94.4% and 99.1% respectively. There was no advantage comparing MCV to ferritin as the sole determinant of ID and insistence on both criteria being fulfilled would lead to a drop in Sn and NP values (55.6% and 93.3%).
Conclusion: The sensitivity and negative predictive value of the above criteria for GI cancer are high. Patients without true iron-deficiency are unlikely to have a sinister cause for their anaemia. While the possibility of GI cancer in patients without iron-deficiency should not be overlooked, a thorough evaluation and the presence of alarm symptoms should reduce the potential for missed diagnoses in this group. Defined criteria for IDA may be useful to determine whether endoscopic examination is warranted.
VIRTUAL CHROMOENDOSCOPY BY MEANS OF REAL-TIME ADAPTIVE HISTOGRAM EQUALISATION OF HD VIDEO WITH THE SONY CELL RSX GRAPHICS PROCESSING UNIT
S. Hebbar1, R. Beresford2, D. Lennon2, M. Williams2, J. Anderson3, N. Shepherd4, J. Brown1. 1Gastroenterology, Gloucester Royal Hospital, Gloucester, 2Broadcast & Professional Research Labs, Sony, Basingstoke, 3Gastroenterology, Cheltenham General Hospital, Cheltenham, 4Histopathology, Gloucester Royal Hospital, Gloucester, UK
Introduction: Accurate and early endoscopic diagnosis demands a precise assessment of mucosal detail. Chromoendoscopy, Narrow Band Endoscopy (Olympus) and Virtual Chromoendoscopy (Fujinon Intelligent Chromo Endoscopy) have been developed to supplement the information derived from white light illumination. The choice of techniques available to the clinician is often related to the availability of endoscopic equipment since many of the new technologies are device-specific. Our objective has been to devise a system that will generate real time, contrast-enhanced images to provide diagnostic information in a device and platform independent way.
Aims & Methods: We have undertaken Adaptive Histogram Equalisation on RGB images in each colour domain using matrix methods (MATLAB). This enhances contrast by stretching the pixel distribution in the original image across the entire dynamic range of the video monitor. We have also transformed RGB images to a novel endoscopy colour space and applied adaptive histogram equalisation to the luminance channel. A library comprising white light, adaptive histogram contrast enhanced, NBI and chromoendoscopy images has been accumulated for comparison.
Results: We have shown that it is possible to enhance endoscopic images using numerical methods which provide additional diagnostic information in a similar way to chromoendoscopy and NBI. Furthermore, real-time image processing can be accomplished by rewriting the MATLAB algorithms in C++ for compilation on the Sony Cell RSX graphics processing unit.
Conclusion: Numerical methods may provide enhanced diagnostic information for endoscopy and we have developed several candidate algorithms for real-time image processing. Further studies are planned to compare our numerical methods with the more established endoscopic techniques.
INTRAEPITHELIAL NEOPLASIA AND INTRAMUCOSAL CARCINOMA COMPLICATING BARRETT’S OESOPHAGUS: ENDOLUMINAL RESECTION IS POSSIBLE IN THE UK
D. P. Hurlstone1, N. Tiffin2, S. S. Cross3. 1Endoscopy, Royal Hallamshire Hospital, 2Histopathology, STH NHS Foundation Trust, 3Histopathology, Royal Hallamshire Hospital, Sheffield, UK
Introduction: Endoscopic mucosal resection (EMR) and now endoscopic submucosal dissection (ESD) using the insulation tipped needle knife for curative intent in intraepithelial neoplasia and Barretts associated intramucosal carcinoma could assume a “gold standard” therapy in comparison to primary ablative techniques. Definitive histopathology can be retrieved and if circumferential excision is achieved, buried gland phenomena abolished. No prospective studies from the UK have addressed the technical feasibility, safety or medium term efficacy of this technique.
Aims & Methods: To evaluate the efficacy of a staged pan-endoluminal resection for the treatment of Barretts associated intraepithelial neoplasia (IN) +/−intramucosal carcinoma in the UK. Patients were referred for consideration of curative intent endoluminal resection of Barretts oesophagus with biopsy proven complicating IN or mucosal carcinoma that had declined formal surgical excision or primary ablative techniques. Exclusion criteria were; pre-resection high-frequency 20 MHz EUS suggestive of T1/N1 disease or beyond, non-correctable coagulopathy or previous ablative PDT or APC endotherapy. Circumscribed lesions in addition to native Barretts epithelium were resected using extended EMR or ESD using sodium hyaluronic acid and an insulation tipped needle knife – 60W pure cut current. Circumferential lesions were resected in 2 or 3 sequential sessions. Primary end-point: histopathologically confirmed resection status; secondary end-points: (1) complication rates (2) intra-epithelial neoplasia recurrence; (3) stricture formation; (4) medium-term clinical efficacy.
Results: 24 patients met inclusion criteria (18;75% male). Pre-resection histopathology: IN–low grade:n = 16/high-grade n = 6/intramucosal carcinoma n = 2. Median number resection session 2.5 (range 1–4)/median procedure duration 68 min (range 32–146). Resection modality: ESD n = 15 (63%), EEMR n = 9 (37%). Primary outcome: post-resection histopathological IN resection status: R0 = 19/24(79%)/Rx: = 3/24(13%)/R1 = 2/24(8%). Secondary outcomes: post-resection stricture formation n = 1/24(4%)/perforation rate 0/24/bleed risk (immediate/delayed) 6/24 (25%)/successful endoluminal haemostasis n = 6 (100%)/IN recurrence n = 1 (4%)/endoscopic follow-up: median 39 months (range 6–68).
Conclusion: EMR and ESD with circumferential extension is a safe and efficacious therapeutic modality for the treatment of intraepithelial neoplasia complicating Barrett’s oesophagus with low complication rates and good medium term clinical efficacy. Definitive resection status can be objectively assessed histopathologically and the risk of dysplastic buried gland phenomena negated. Long-term efficacy and learning curve characteristics for this technique are now required.
THE ROLE OF STRAIGHT-TO-TEST ENDOSCOPY FOR TWO-WEEK WAIT REFERRALS SUSPECTED OF UPPER GASTROINTESTINAL MALIGNANCY
G. R. Irving1, F. Chikwanda1, P. Morowski2, K. Kapur3, M. Shiwani1. 1Upper Gastrointestinal Surgery, 2Clinical Audit, 3Gastroenterology, Barnsley District General Hospital, Barnsley, UK
Introduction: The two-week wait (2WW) system was introduced from July 2000. The impact of this with respect to Upper Gastrointestinal services and the management of malignancy has been reported. Originally, all 2WW referrals were provided with a clinical appointment following which a second appointment for endoscopy would be arranged. This has lead to the evolution of straight-to-test (STT) referrals for endoscopy with an aim to improve cancer waiting times. Referral criteria have been developed in an attempt to improve the service.
Aims & Methods: Data were obtained prospectively on patients referred via 2WW pathway to the Upper gastrointestinal specialists during the last financial year. Patients referred with dysphagia were automatically given STT appointment. Patients without dysphagia were given a clinical appointment. During the STT appointment clinical history, examination and endoscopy were conducted and further follow-up arranged as appropriate. Data were cross-referenced with the Open Exeter National cancer waiting time database and the 2WW referral office. Additional data were obtained retrospectively from all cases of upper gastrointestinal cancer. Origin of referral, diagnostic route, clinical outcome and the chronological data were recorded.
Results: 295 patients were referred via the 2WW system and underwent endoscopy of which 144 referred with dysphagia went STT. There were 53 gastro-oesophageal malignancies diagnosed (23 gastric and 30 oesophageal) in one year. 34 were diagnosed via 2WW pathway of which 10 were diagnosed at STT appointment. Median waiting time for patients referred for STT = 9 days (1–17) with 1 patient breeching the 14-day target before consultation. The median time before 2WW clinic appointment was 9 days (1–24) with no patients breeching the target. Patients referred from clinic to endoscopy had a median wait of 14 days (1–49). 1 cancer patient from the STT group exceeded 31 days until decision to treat date and 2 patients from this group exceeded the 62 day target for treatment. In 2WW patients not referred straight to test 4 exceeded 31 days until diagnosis and 5 exceeded 62 days until treatment.
Conclusion: Straight-to-test endoscopy service does improve cancer waiting times. It does not increase the incidence of diagnosing malignancy and proportionately more cancers were diagnosed in the patients not referred STT. Overall incidence was 11.5% in all 2WW patients but only 2% in STT group. Our criteria for immediate endoscopy do not provide good sensitivity, which may be a reflection of the referral practices and the interpretation of symptoms by primary care practitioners. However, fast-tracking endoscopies will still remain important with waiting times for non-malignant disease also becoming implemented in the near future.
INDICATIONS, SUCCESS AND COMPLICATIONS OF NEEDLE KNIFE SPHINCTEROTOMY IN A TERTIARY REFERRAL CENTRE
V. Jairath, S. P. Pereira, A. R. W. Hatfield, G. J. M. Webster. Department of Gastroenterology, University College Hospital London, London, UK
Introduction: Needle knife sphincterotomy (NKS) has been controversial since its introduction in the 1980s. There is a large variation in the published literature regarding the incidence of its use, ranging from 1% to 30%. Similarly, published complication rates vary from 5–30% in large series. NKS emerges as a multivariate risk factor for post-ERCP pancreatitis and overall complications of ERCP.
Aims & Methods: The aim of this study was to examine the frequency, indications, success and complication rates of NKS in our centre. We analysed data from 100 NKSs (38 prospective, 63 retrospective). Success was defined as deep biliary cannulation sufficient to allow further diagnostic/therapeutic measures. We recorded major complications as defined by Cotton et al (pancreatitis, bleeding, perforation, infection graded as mild/moderate/severe). Thirty-day post-procedure complication data were collected.
Results: We used NKS in 9.1% of ERCPs. Clinical scenarios in patients requiring NKS included: jaundice and dilated biliary tree (55%); abnormal LFTs and dilated biliary tree/bile duct stones (36%); postoperative bile leak (9%). Successful deep biliary cannulation was achieved in 80 patients (80%) requiring NKS, at first attempt at ERCP. Of the 20 initial failures, success was achieved on further ERCP in 6 cases within 7 days (that is, final endoscopic success in 86% of NKS cases), 5 had successful percutaneous transhepatic drains (all in the setting of malignancy), and 9 were managed expectantly. 30-day follow-up data were obtained for 87/100 patients with an overall complication rate of 11.5% (n = 10). Complications included pancreatitis in 4 cases (3 mild, 1 severe), bleeding in 5 cases (4 moderate, 1 severe), and 1 severe case of cholangitis leading to death in a patient with cholangiocarcinoma. There were no perforations.
Conclusion: In our analysis of 100 consecutive NKS the procedure was used in <10% of total ERCPs, with endoscopic success in 80% at first attempt. Overall 30-day complication rate was similar to data from other large series, with a pancreatitis rate lower than expected. Our data from a large volume centre suggest that NKS is an effective technique where biliary cannulation is difficult, with an acceptably low complication rate.
ASSESSMENT OF RAPID ON-SITE EVALUATION BY A BIOMEDICAL SCIENTIST IN ENDOSCOPIC ULTRASOUND GUIDED FINE NEEDLE ASPIRATIONS
S. Chaudhry1, V. Y. Kaushik2. 1Cytopathology, Tameside General Hospital, Ashton-under-Lyne, 2Gastroenterology, East Lancashire NHS Trust, Blackburn, UK
Introduction: Endoscopic ultrasound guided fine needle aspiration (EUS-FNA) is a technique that has achieved high sensitivities and specificities in the diagnosis of a range of malignancies many of which would otherwise require a more invasive and riskier procedure to allow confirmation. To aid the endosonographer in achieving a higher success rate, the laboratory can provide rapid on-site evaluation (ROSE) of the samples achieved. Other researchers have reported that the procedure time can be affected considerably by the presence of a cytopathologist, and therefore improving the overall benefits.1
Aims & Methods: The effectiveness of ROSE by a biomedical scientist (BMS) is evaluated in this study. During the study period of 6 months, a total of 24 patients had EUS-FNA performed. Data were gathered on the procedure times, the number of passes performed and the pass at which the biomedical scientist confirmed adequacy. The BMS staff had in-house training from a senior member of the technical staff, who accompanied them for the first 9 procedures.
Results: The data analysis showed a strong association between increasing numbers of procedures and a decrease in the overall procedure time. The average time for the pancreatic procedures decreased from 57 to 40 minutes, when comparing the first 7 procedures to the last 7 procedures performed (Pearson value = −0.911211). However, there was no correlation between procedures performed and the number of passes required for each patient, this remained at a median average of 2.5 passes with a range of 2–4. The overall inadequate rate achieved was 20%, while the FNA of pancreatic masses achieved an inadequate rate of 15%.
Conclusion: An improvement in the specific technical skills required by both the endosonographer and the liaising BMS leads to a decrease in the time required for each procedure. The absence of correlation between this and the number of passes can be explained by other underlying factors that were not accounted for in this study, for example the location and size of the mass and other clinical and pathological features of the patients. One of the other reasons was the cautious endosonographer’s desire to obtain a further sample after being informed on the adequacy of the FNA. The results achieved in this study prove that the use of ROSE in clinics by BMS is an effective method of reducing patient discomfort, and increasing diagnostic yield but there is a need to analyse the steps required to achieve proficiency in this technique.
BISPECTRAL INDEX MONITORING DURING ERCP
I. Khan1, M. Hegde1, A. Windsor2, J. Bateman1, M. Smith1. 1Gastroenterology, 2Anaesthetics, The Shrewsbury and Telford Hospital NHS Trust, Shrewsbury, UK
Introduction: In the UK most ERCP procedures are carried out using parenteral sedation, which carries risk of complications (for example, under/over sedation, aspiration). BIS gives an objective (EEG based) measure of the degree of sedation. Here data are shown from one unit where sedation was titrated using BIS during ERCP.
Aims & Methods: Data were collected prospectively during ERCP (at 5-min intervals): BIS scores (when used), heart rate, pulse oximetry, visible distress and sedative dose (midazolam and fentanyl). At the end of the procedure, the Observer’s Assessment of Alertness/Sedation (OAA/S) score (1, unresponsive to 5, responds to normal voice) was noted. When fully alert patient satisfaction with the procedure was assessed using visual analogue scales (VAS).
Results: 111 patients were studied in total: BIS (n = 77, 35 male, mean age 71.6 years, range 22–96 years); no BIS (n = 34, 15 male, mean age 65.1 years, range 27–90 years). Mean data shown in table. There were no serious sedation related complications and VAS analysis from both groups showed that most patients were satisfied with the procedure irrespective of whether BIS was used.
Conclusion: In our experience BIS provides a useful method for objective monitoring of parenteral sedation during ERCP, but the procedure can be safely and comfortably conducted without it. However, further case controlled data is required to fully evaluate this technique.
EARLY EXPERIENCE OF DIAGNOSTIC AND THERAPEUTIC SINGLE-BALLOON ENTEROSCOPY
S. C. Kong, A. J. Morris. Department of Gastroenterology, Glasgow Royal Infirmary, Glasgow, UK
Introduction: Capsule endoscopy has resulted in an increase in the pathology seen in the small bowel that requires further assessment or intervention. Push enteroscopy is limited to examination of the proximal jejunum. Recently encouraging results of the yield of double-balloon enteroscopes have been reported. A new single-balloon enteroscope (Olympus XSIF-260SB) has recently become available. We describe our initial experience with the new enteroscope.
Aims & Methods: The single balloon enteroscope was assessed by endoscopists trained in the use of push enteroscopes. The Olympus single-balloon enteroscope system was used. This comprised an EVIS LUCERA small intestinal video scope (XSIF-260SB), a balloon control unit (MAJ-1440) and a single use splitting tube (ST-SB1). The splitting tube is a silicone rubber overtube with an inflatable and deflatable balloon at one end. The inner surface of the tube has been treated with a hydrophilic lubricant coating which is activated by passing water over the inner surface of the tube. The technique of enteroscope advancement comprised of sequential push and pull manoeuvres combined with inflation and deflation of the balloon. Real-time radiological imaging confirmed the progress of the single-balloon enteroscope and the straightness of the shaft of the enteroscope.
Results: Over a three month period, 7 patients (5 females) were referred to our tertiary centre for single-balloon enteroscopy. All patients had been extensively investigated prior to referral. Mean age was 66 years old (range 42–80 years). 5 patients were referred due to recurrent symptomatic iron deficiency anaemia and 2 were referred for suspected complicated coeliac disease. The mean length of small bowel intubation was 182 cm from the incisors (range: 150–200 cm). 4 out of the 5 patients with recurrent iron deficiency anaemia had arteriovenous malformations (AVM) identified and ablated. In one of the cases, the lesion was actively bleeding on initial viewing and haemostasis was achieved at end of procedure. In one of the complicated coeliac cases, an ulcer was identified and biopsied at 150 cm. There was no complication in any of our patients.
Conclusion: Early experience with single-balloon enteroscope shows it is an effective instrument in diagnostic and therapeutic small bowel intervention. Initial experience suggests that the single-balloon enteroscope may be useful in treating lesions or obtaining biopsy from pathology identified by capsule endoscopy.
PATIENT INTOLERANCE DURING CONSCIOUS SEDATION IS A MAJOR CAUSE OF PROCEDURE FAILURE: A RETROSPECTIVE AUDIT OF ERCP IN A LONDON TEACHING HOSPITAL
N. Kumar, P. Kennedy, J. Mawdsley, M. Thursz, J. Teare, J. Hoare. Gastroenterology and Hepatology, St Mary’s Hospital, London, UK
Introduction: The BSG audit1 has provided a target for gastroenterologists performing ERCP. The society has also published sedation guidelines, recommending a maximum dose of midazolam of 5 mg.2 However, sufficiency of such low dose conscious sedation for successful ERCP is debatable, with deep sedation using propofol preferred for ERCP in the US.3 We undertook a retrospective analysis of ERCP practice in a London teaching hospital, assessing cannulation rates, technical success rates and complication rates and compared them to the BSG audit. We also examined adherence to sedation guidelines and recommendations.
Aims & Methods: Data were retrospectively collated from medical records of all ERCP procedures over a one-year period. ERCP indication, desired duct cannulation, diagnosis, therapeutic intervention and procedure failures were recorded. In addition, 30-day complication and mortality rates were calculated and sedation use recorded.
Results: 122 patients (52 male, 70 female, median age 63 years) underwent 171 procedures over 1 year. Completion of intended treatment was achieved in 99/122 (81%) undergoing their first recorded ERCP, compared with the national average (70%) in the BSG audit. Of the 122 first recorded procedures, 10 (8%) procedures were terminated prematurely due to failed sedation; 10 (8%) procedures failed duct cannulation, and only 3 (3%) procedures failed intervention. Hence with 102/122 (84%) successful duct cannulations at first recorded ERCP with 8/102 (8%) requiring pre-cuts, our overall cannulation rate of 84% is comparable to the BSG audit. There were 3 cases of ERCP related pancreatitis (3/171, 1.8%), 1 case of cholangitis (1/171, 0.6%) and one ERCP-related death of a patient with biliary sepsis, jaundice and advanced malignant disease (1/171, 0.6%). Midazolam was administered in 163/171 procedures. A median dose of 7 mg was used. In 85/163(52%) cases the recommended 5 mg limit was exceeded, compared with 33% of cases in the BSG audit. An inverse relationship between age and midazolam dose highlighted in the BSG audit was supported by our data.
Conclusion: Our cannulation rates, technical success rates, complication and mortality rates are comparable to those observed in the BSG audit. The commonest reason for an unsuccessful procedure was sedation failure. This was despite higher than the recommended dose of midazolam being used in more than 50% of cases. In response to this finding we propose more procedures to be performed under propofol sedation with anaesthetic support, with a view to improving patient experience and reducing failed procedures.
THE EFFICACY, ACCEPTABILITY AND SAFETY OF THE NEW 2 L MOVIPREP VS THE 4 L KLEANPREP IN PATIENTS UNDERGOING ELECTIVE COLONOSCOPIES
B. C. Lee, D. A. Moyes, J. C. McLoughlin, P. L. Lim. Gastroenterology, Mater Infirmorium Hospital, Belfast, UK
Introduction: Colonoscopy is an established diagnostic modality for colonic diseases and it has been increasingly utilised in colorectal cancer surveillance programme. A successful colonoscopy is very much dependent on the quality of bowel preparation. Although existing bowel preparation such as Kleanprep (Norgine Ltd, Harefield, UK) is widely used in most endoscopy units, its large volume remains a disadvantage. Therefore, there is a need for a bowel preparation with equivalent bowel cleansing properties but better patient tolerability.
Aims & Methods: To compare the efficacy, patient acceptability and safety of a new 2 l polyethylene glycol + electrolytes + ascorbic acid (Moviprep, Norgine Ltd, Harefield, UK) to the standard 4 l polyethylene glycol + electrolytes (Kleanprep, Norgine Ltd, Harefield, UK) in patients undergoing elective colonoscopies. A single-blinded randomised study was carried out at our unit over a 4-month period (May to August 2007). Patients referred for elective colonoscopy were invited to participate. Consenting patients were randomised to either Moviprep or Kleanprep for bowel cleansing. Endoscopists were blinded to the type of bowel preparation the patients had taken. The quality of bowel preparation was scored by the endoscopists at the time of colonoscopy. The acceptability and side effects of either bowel cleansing agent were recorded in a patient-filled questionnaire. Patient compliance was also reported.
Results: A total of 56 patients (28 males, 28 females) participated in the study, with a mean age of 57.9 years (age range 28–81 years). Twenty two patients were randomised to take Kleanprep while 34 patients to Moviprep. Gender distribution was comparable in both groups. The overall success rate in bowel cleansing was 82% with Moviprep and 77% with Kleanprep (p = NS). Moviprep has better taste acceptability compared to Kleanprep (70% vs 50%; p = NS). The compliance rate was significantly higher in the Moviprep group (91% vs 50%; p = 0.001). The proportion of patients taking either bowel preparation in the future, if required, is similar (85% Moviprep vs 75% Kleanprep; p = NS). Side effects were not significantly different between the two groups.
Conclusion: Moviprep has comparable bowel cleansing efficacy and safety with Kleanprep. With its higher patient compliance, due to its low volume, and better acceptability, Moviprep may be the new kid on the block in bowel preparation for elective colonoscopies.
IN CASES OF OBSCURE GASTROINTESTINAL BLEEDING, NEGATIVE CAPSULE ENDOSCOPY PREDICTS GOOD LONG-TERM OUTCOME
J. C. Macdonald, V. Porter, D. A. McNamara. Department of Gastroenterology, Aberdeen Royal Infirmary, Aberdeen, UK
Introduction: Capsule endoscopy (CE) is an established method for investigating obscure gastrointestinal bleeding (OGIB) with positive diagnostic yield reported at between 40–90%. There is little data available regarding the clinical implication and long-term outcomes for patients with a negative study in these circumstances.
Aims & Methods: Between April 2005–October 2006, 47 patients with OGIB underwent CE. All patients had previously undergone appropriate endoscopic examination of the upper and lower GI tract. 42 patients (89%) have been followed up over a mean period of 17.3±6.4 months (mean age 59.8±14 years; 45% female). 24/42 studies (57.1%) were performed in view of overt OGIB, 18/42 for occult OGIB. Case records were analysed for evidence of recurrent GI bleeding (re-investigation, blood transfusion, unexplained acute drop in haemoglobin >2 g/dl).
Results: Overall diagnostic yield was 57.1% (24 examinations), the remaining 18 studies (42.9%) being normal. Patients with a positive study tended to be older (65.7±14 years positive vs 53.8±14 years negative; p<0.01) but the nature of OGIB (overt vs occult) was not a predictor of study outcome. In the group with a positive study 19/24 (79%) were found to have angiodysplasia, and 7/19 (36.8%) of these patients underwent argon plasma coagulation. There was a re-bleeding rate of only 11.1% in the negative study group, while re-bleeding occurred in 11/24 (45.8%) following a positive study (p<0.01). Both individuals who re-bled following negative CE were anticoagulated with warfarin at the time of re-bleed. During the follow-up period there was one death amongst patients with a negative study (bacterial endocarditis), compared with 3 deaths in those whose CE had positive findings (1 renal failure, 1 gastrointestinal malignancy, 1 ischaemic heart disease). There was no statistical difference in period of follow-up for either group (16.2±4.6 months positive vs 18.6±5.9 months negative).
Conclusion: Patients with OGIB and a normal CE examination appear to be at low risk of subsequent re-bleeding. These results would indicate that this group of patients do not require further routine follow-up or additional gastroenterological investigations.
RATES OF CAECAL INTUBATION AS REPORTED IN THE ABSTRACTS OF THE BSG ANNUAL MEETING
M. R. Welfare1, S. J. Mills2, L. A. Macdougall3. 1Gastroenterology, North Tyneside General Hospital, 2Surgery, Wansbeck General Hospital, 3Foundation Year 2, North Tyneside General Hospital, Tyne and Wear, UK
Introduction: Individual colonoscopists frequently achieve the target of 90% crude completion rate but published data for whole units rarely do. We review the published completion rates in abstracts at the annual meeting of the BSG between 2000 and 2007.
Aims & Methods: We hand-searched for relevant abstracts, excluding all reports with <300 cases and <5 operators. The abstracts presented data in various formats and not all gave the absolute figures so we report only the percentage success. We ascribed the data to the year in which the colonoscopies were carried out, when possible, or to the last year of the audit if year by year breakdown was not given. As far as possible we reported crude completion rates, giving the range and the mode. We also looked for audit techniques used to improve performance.
Results: Before 2005 only one study reported completion rates of >90% and that was from St Mark’s (table). 50% of reports in 2005/6 achieved 90% or greater completion. The most effective audit techniques appear to be feedback on performance, although several units reported sequential improvement with no specific intervention. Improving bowel preparation also contributed. One report found that intensive education by outside experts and use of a magnetic imager did not improve completion rates.
Conclusion: There is clear evidence that general performance in colonoscopy is improving in the UK if these audits are representative of overall performance. Many units improved over time and several factors could be contributing to this including the standards promoted by JAG, the drive towards bowel screening and the threat of revalidation.
IS THE COLONOSCOPIC MEDICAL SURGICAL DIVIDE A REALITY?
L. A. Macdougall1, M. R. Welfare2, S. J. Mills3. 1Foundation Year 2, 2Gastroenterology, North Tyneside General Hospital, 3Surgery, Wansbeck General Hospital, Tyne and Wear, UK
Introduction: The Joint Advisory Group on Endoscopy (JAG) has set standards for training in colonoscopy since 1998. All trainees, regardless of discipline, should be trained to the same standards which include a 90% crude completion rate, a target which trained colonoscopists should also aim for. Previous studies have suggested a systematic difference in completion rates between physicians and surgeons. This study examines the completion rates in our institution over an 8-year period since the publication of standards.
Aims & Methods: Data were collected prospectively on endoscopy reporting systems (Endosoft and ERS) in 2 teaching District General Hospitals in Northumbria Healthcare NHS Trust from 2000–7. The discipline and grade of the endoscopist were recorded as were crude completion rates. Completion was defined as endoscopist reported caecal or terminal ileum intubation based on intention to complete with no adjustment for inadequate bowel preparation or impassable strictures.
Results: A total of 15 869 colonoscopies were recorded, the majority performed by consultants, but 1103 by clinical assistants, 318 by nurse endoscopists and 2567 by training grade doctors. The number of colonoscopies performed increased from 946 in financial year 2000/1 to 2850 in 2006/7 with an overall 8-year crude completion rate of 85.4%, improving from 78.5% in 2000/1 to 90.5% in 2007. The remainder of the analysis focuses on the 14 448 examinations performed by consultants and training grade doctors, excluding 52 cases for whom extent of examination was not recorded. Overall, consultant gastroenterologists intubated the caecum more regularly than consultant surgeons with completion rates of 4869/5550 (88.1%) and 5206/6237 (83.5%) respectively. However, the gastroenterologists started from a lower baseline, improving from 73.9 to 92.0% compared with the surgeons 80.1 to 88.1% over the same 8-year period. Completion rates of trainees improved from 79.1 to 91.6% between 2000 and 2007 and there was no overall difference between gastroenterology (1119/1409, 84.5%) and surgical trainees (983/1155, 85.1%).
Conclusion: The standard of colonoscopy in respect of completion rate has risen consistently over the last 8 years. Although the gastroenterologists performed better against this standard overall, the gap has narrowed in the most recent 2 years and there is no difference in performance amongst the training grade doctors. It may be that guidance on training from the JAG, with clearly defined objectives, joint training courses, and heightened awareness is raising and unifying standards. Examining the remaining shortfall in performance and enabling mentoring may improve colonoscopy performance as a whole.
USE AND SAFETY OF NEEDLE KNIFE SPHINCTEROTOMY AT ERCP: AN AUDIT OF 8 YEARS’ EXPERIENCE AT A DISTRICT GENERAL HOSPITAL
P. G. Mayhead, R. H. Loke, G. Greenhall, Y. Umebuani. Gastroenterology, Kent and Sussex Hospital, Tunbridge Wells, UK
Introduction: Needle knife sphincterotomy (NKS) is a method for achieving biliary access. It is used when standard cannulation is unsuccessful. Complications include hemorrhage, perforation and pancreatitis. NKS is a controversial technique due to the complications, but studies have shown it to be safe,effective and comparable to standard sphincterotomy (SS).1 2
Aims & Methods: We analysed the data of one doctor’s use of sphincterotomy techniques to detect differences in indications and complications between NKS and SS. Data were collected from 1999–2006 from reports. Patients who had a NKS were recorded and 1 in 3 patients who had SS were analysed. Complications were detected by using the hospital computer system to identify anyone who had ERCP with sphincterotomy who stayed more than or equal to two days following the procedure and the notes were examined for complications. Pancreatitis was defined using recent BSG Guidelines.3 Indications and findings were recorded from the documentation of each ERCP report.
Results: From January 1999 to December 2006, 1081 ERCPs were performed averaging 135 cases per year. 148 NKS and 546 SS were performed. Notes were reviewed for 80% of the NKS patients and 82% patients selected in the SS group. Repeat ERCP was required following NKS in 10 cases and was successful in 9. There was no difference in indication for ERCP between each group. The overall complication rate was 12.7% for NKS (5% pancreatitis, 2.5% bleeding) and 2.2% for SS (0.55% pancreatitis). There were 2 deaths within 10 days in the NKS group (1/540) from bleeding, both in their 80s.
Conclusion: Our complication rates are similar to previously published reports. In a similar study in 2004, complication rates from NKS were 7% for haemorrhage and 4% for pancreatitis.4 Our complication rate of 12.7% for NKS is comparable to other centres performing high volumes of ERCP (12% complication rate, 5.5% bleeding and 0.5% pancreatitis).5 There were very few complications in the SS group. Overall, the indications for ERCP in which each modality of sphincterotomy was used was similar implying that NKS is a safe alternative to SS and is a highly effective method of gaining biliary access in patients in whom deep cannulation proves difficult or impossible and biliary access is considered essential.
Gastrointestinal pathology posters
THE REGULATION OF CELLULAR IRON IS DEFECTIVE IN APC MUTANT COLORECTAL CARCINOGENESIS
M. J. Brookes, K. Roberts, T. Iqbal, C. Tselepis. Cancer Studies, University of Birmingham, Birmingham, UK
Introduction: The tight regulation of cellular iron levels in normal epithelial cells is mediated through the interaction of iron regulatory proteins (IRPs) with iron response elements found in many genes implicated in iron metabolism. In instances of excessive iron levels IRE/IRP signalling causes a repression in iron import proteins including TfR1 and DMT1. However, in colorectal cancers we have previously demonstrated high iron import protein expression in the face of high cellular iron levels suggesting an aberration in IRE/IRP signalling.
Aims & Methods: The aim of this study is to determine if iron mediated Wnt signalling is a crucial in the aberration of iron sensing and in particular address the impact of c-myc. Colorectal lines RKO and SW480 were cultured with or without iron; the expression of iron transport proteins and Wnt-targets examined by Q-RT-PCR and Western blotting. C-myc and IRP2 over expression studies were performed in RKO cells followed by ferrozine assays for iron determination.
Results: Our results demonstrate that in RKO cells (APC wild-type) iron does not induce Wnt signalling and cells behave in an IRE/IRP dependent manner. However in SW480 cells (APC mutant) iron loading results in Wnt signalling and inductions in iron import proteins (TFR1 and DMT1) which were associated with increased c-myc expression. This observation was verified by c-myc over expression studies where expression of the iron import proteins TfR1 and DMT-1 were both induced as a consequence of c-myc.
Conclusion: Wnt signalling and in particular c-myc is crucial in interfering with normal IRE/IRP signalling.
CELL SURFACE BINDING AND INTERNALISATION OF CLOSTRIDIUM DIFFICILE TOXIN A BY HUMAN INTESTINAL EPITHELIAL CELLS
K. Solomon, A. Robins, Y. R. Mahida. Institute of Infection, Immunity and Inflammation, University of Nottingham, Nottingham, UK
Introduction: C difficile causes colitis via secreted toxins A and B. Epithelial cells are likely to be the first host cells that bind the luminal toxins but the nature of these interactions are currently undefined.
Aims & Methods: To investigated binding and internalisation of toxin A. Purified toxin A was fluorescently labelled and unincorporated dye removed by size-exclusion chromatography. The labelled toxin retained biological activity (cell rounding) in Vero and Caco-2 cells. Specificity of fluorescence following application of labelled toxin was confirmed by its loss when pre-incubated with beads coated with toxin A-specific monoclonal antibody PCG-4. To control for batch-to-batch and experiment-to-experiment variation, beads with different (but known/defined) PCG-4 binding capacity were used in each experiment to create a standard curve of fluorescence, after application of labelled toxin A to PCG-4-coated beads. From the standard curve, fluorescence of cells after application of labelled toxin A was used to calculate toxin A fluorescence units (TAFU). Labelled toxin A binding to the surface of Caco-2 cells was studied on ice after 1 min exposure. Internalisation of labelled toxin A was studied by flow cytometry and confocal microscopy, after 2 h and 5 h continuous exposure at 37°C. Data are expressed as mean (±SEM).
Results: Caco-2 cell surface fluorescence was rapid (within 20 s) following application of labelled toxin A and was constant over the subsequent 5 min. When exposed to unfixed Caco-2 cells at 37°C, internalised toxin A was seen within the cell cytoplasm by confocal microscopy. Analysis by flow cytometry (table) showed a concentration-dependent increase in cell surface-associated TAFU (p<0.05). Internalised TAFU increased in a concentration and time-dependent manner. There was an inverse relationship between the concentration of labelled toxin A applied and the calculated proportion of cell surface-associated TAFU that was internalised at 2 h (2 µg/ml–60.7%, 5 µg/ml–33.9%, 10 µg/ml–24.2%) and 5 h (2 µg/ml–121.6%, 5 µg/ml–75.4%, 10 µg/ml–43.9%). Surface-associated TAFU was significantly greater than internalised TAFU after 5 h incubation with 5 and 10 µg/ml labelled toxin A (p<0.05).
Conclusion: (1) C difficile toxin A rapidly associates with the surface of human intestinal epithelial cells in a concentration-dependent manner. (2) There is an inverse relationship between the concentration of toxin A applied and the proportion of cell-associated toxin that is internalised. (3) The above could be explained by a concentration-dependent increase in non-specific binding of toxin A to the epithelial cell surface.
MALE PREDOMINANCE OF UPPER GASTROINTESTINAL CANCER IS RELATED TO INTESTINAL HISTOLOGICAL SUBTYPE NOT TUMOUR LOCATION
M. H. Derakhshan1, S. Liptrot2, J. Paul2, I. L. Brown2, K. E. L. McColl1. 1Medical Sciences, 2Division of Cancer Science and Molecular Pathology, University of Glasgow, Glasgow, UK
Introduction: Upper gastrointestinal adenocarcinomas show an unexplained male predominance which is more apparent in the oesophagus than stomach. We have conducted a population-based study to determine whether the gender phenomenon is primarily related to the anatomical site or the histological subtype of the tumour.
Aims & Methods: The study was based upon 3270 gastric and oesophageal cancers recorded in West of Scotland cancer Registry between 1998 and 2002. 812 of these cases were randomly selected for detailed analysis. Their records were reviewed for histological diagnosis and anatomical site of tumour using ICD-10 and ICD O-2. The Lauren histological subtype of adenocarcinoma was determined by reviewing 1204 original reports and 3241 biopsy and surgical slides. Logistic regression models were used to estimate relationship between male predominance and histological subtype, tumour location and age.
Results: 405 (51.5%) cancers originated from the non-cardia region of the stomach, 173 (22.0%) from the gastric cardia and 209 (26.6%) from the oesophagus. Regardless of anatomical subsite, the upper GI cancers were more common in males (502, 63.8%) than females (285, 36.2%). Regardless of anatomical site, the crude incidence rate of intestinal type upper GI adenocarcinoma was higher in males (23.86/100 000/year) versus females (9.00/100 000/year), giving M/F of 2.65. M/F ratio of intestinal type cancer was 3.41 at age <50, reached a peak of 7.86 at age 50–59, and then showed a progressive decrease with a minimum of 2.29 at age group ⩾80 years. In contrast, the crude incidence rate of diffuse-type adenocarcinoma was similar in males and females (5.58 vs 5.20/100 000/year) yielding M/F of 1.07. Male predominance was greatest in the oesophagus with M/F of 3.50, less in the cardia (M/F = 2.00) and least in the non-cardia cancer (M/F = 1.65). The relationship between tumour location and male predominance lost its significance in the multivariate analysis when histological subtype was added (OR 1.37, 95% CI 0.88 to 2.12). Multivariate analyses including histological subtype, tumour location and age indicated that the male predominance was related to the histological type rather than anatomical location. Intestinal type adenocarcinoma showed similar male predominance of incidence irrespective of its anatomical location (OR 2.6, 95% CI 1.78 to 3.9).
Conclusion: Male predominance in upper GI adenocarcinomas is not a function of tumour location (table) but rather related to histological subtype. The mechanism of the strong gender association with intestinal subtype requires elucidation.
MALE PREDOMINANCE OF UPPER GASTROINTESTINAL CANCER IS DUE TO A 17.2-YEAR DELAY OF INTESTINAL HISTOLOGICAL SUBTYPE IN FEMALES
M. H. Derakhshan1, S. Liptrot2, D. Morrison3, I. L. Brown2, K. E. L. McColl1. 1Medical Sciences, 2Division of Cancer Science and Molecular Pathology, 3Scottish Universities Environmental Research Centre, University of Glasgow, Glasgow, UK
Introduction: We have recently demonstrated that the male predominance of upper GI adenocarcinoma is associated with the intestinal histological subtype and is independent of anatomical location—that is, oesophageal versus gastric. We have undertaken kinetic analysis of age specific incidence trends to determine the effect of the gender phenomenon.
Aims & Methods: The study was based on 812 cases of upper gastrointestinal adenocarcinoma randomly selected from the West of Scotland Cancer Registry between 1998 and 2002. The Lauren histological subtype of adenocarcinoma was determined by reviewing 1204 original reports and 3241 biopsy and surgical slides. A regression curve modelling was used to calculate age-specific curve equations of both diffuse and intestinal subtypes of cancer.
Results: The analysis compromised 405 non-cardia cancer, 173 cardia cancer and 209 oesophageal adenocarcinoma. The crude incidence rate of intestinal type upper GI adenocarcinoma was higher in males (23.86/100 000/year) versus females (9.00/100 000/year), giving M/F of 2.65. M/F ratio of intestinal type cancer was 3.41 at age less than 50, reached a peak of 7.86 at age 50–59, and then showed a progressive decrease with a minimum of 2.29 at age group 80 years and over. In contrast, the crude incidence rate of diffuse-type adenocarcinoma was similar in males and females (5.58 vs 5.20/100 000/year) yielding M/F of 1.07. Curve modelling of the age-specific rates for diffuse subtypes showed similar equations, y = 0.016×mean age 2.007+32.98, R2 = 0.999 and y = 0.016×mean age 1.954+35.97, R2 = 0.989, for male and females, respectively. For the intestinal histological type, the age-specific incidence rates were different for males and females. Curve modelling indicated the same kinetic equation for rise in incidence with age, in males (y = 0.016×mean age 2.315+28.75, R2 = 0.990) and in females (y = 0.016×mean age 2.316+46.07, R2 = 0.998). However, the female curve was displaced to the right indicating a delay in the cancer onset. The estimated cancer onset delay for females was 17.2 years (that is, +46.07 minus +28.75 = 17.22).
Conclusion: Male predominance in upper GI adenocarcinomas is a reflection of approximately 2 decades delay of development of intestinal subtype adenocarcinoma in females. The mechanism of the marked delay in development of intestinal subtype requires elucidation.
SHOULD WE BIOPSY ANTRAL GASTRITIS TO DETECT INTESTINAL METAPLASIA?
S. S. Samji1, B. Nedjat-Shokouhi1, N. Alband2, A. D. Millar1. 1Gastroenterology, North Middlesex University Hospital, 2Gastroenterology, Queen Mary School of Medicine, London, UK
Introduction: Antral gastritis is a common finding at endoscopy often caused by H pylori.1 In NHS practice biopsies from mild-moderate antral gastritis are usually taken for CLO test but not histology, potentially missing intestinal metaplasia; which has proven carcinogenic potential.2 We reviewed results of 272 endoscopies comparing macroscopic appearances of the antrum, CLO test results and antral histology to establish the rate of intestinal metaplasia and associated gastric pathology.
Aims & Methods: We reviewed endoscopy reports from 1999–2007 in patients who had undergone endoscopy and were >18 with no previous gastric surgery, and if antral histology, a CLO test and an image of the antrum were available for analysis. Demographics, symptoms, diagnosis, antral appearance, histology and CLO-test results were recorded. The patients were drawn from a single endoscopist’s practice in two independent hospitals. In all patients at least two random antral biopsies were taken for CLO test and for histology.
Results: The age range was 17–93, median 53 years, with a male/female ratio of 1:1.2. 35 patients (13%) had a positive CLO test and 43 patients (16%) had gastritis on histology, of which only 13 had H pylori detected by CLO test or on histology; 3 had intestinal metaplasia, only 1 of which was positive for H pylori. As expected a positive CLO was strongly linked with GU or DU (p = 0.005) and dyspepsia (p = 0.04).
Conclusion: This study confirms that the common finding of gastritis is strongly linked with H pylori and GU or DU3 though ulcers were not commonly found probably because primary care practitioners follow national “test and treat” guidelines. CLO positive inflammation was therefore also uncommon in the study group. Three biopsies showed intestinal metaplasia which would not have been detected under common practice and many of these may be H pylori negative. Further studies are needed to establish the indication for antral biopsy to detect intestinal metaplasia and the effectiveness of surveillance of these patients.
ENHANCED BIOMEDICAL SCIENTIST CUT-UP ROLE IN COLONIC CARCINOMA: PRELIMINARY PERFORMANCE DATA AND COMPARISON WITH DEPARTMENTAL PERFORMANCE
E. J. V. Simmons1, D. S. A. Sanders1, A. Smith1, P. Murphy2, M. Osbourne2, K. Busby2, M. Stellakis2, J. Francombe2. 1Department of Histopathology, 2Department of Surgery, Warwick Hospital, Warwick, UK
Introduction: The extended Biomedical Scientist (BMS) role in surgical cut-up is increasing in importance and is likely to continue to do so. It allows more efficient use of Consultant time and resources and provides additional career progression for a highly skilled workforce. As the remit of BMS cut-up expands to include major cancer resection specimens, it becomes essential, on grounds of quality assurance, to apply the same performance criteria applied to specimens dealt with by Consultant and trainee pathologists. These are included in the recently published second edition of the RCPath colorectal cancer dataset.3
Aims & Methods: To compare performance data between colorectal cancer (CRC) cases trimmed by a pathologist, by our BMS in his extended practice role, RCPath guidelines and other published series. After preliminary review, CRC specimens of appropriate complexity are allocated to the BMS. The Consultant pathologist and the BMS then examine the specimen together, discussing block selection and any other areas of concern specific to the case. The Consultant is available for further advice and discussion at any point during trimming. The BMS then reviews the slides of the case plus their performance data in conjunction with the Consultant. Departmental figures are derived from 400 colorectal cases trimmed predominantly by a single Consultant Pathologist, with smaller numbers trimmed by trainee patholgists. The cases trimmed by our BMS are included in this series. At the time of abstract submission our BMS had trimmed 21 selected cases (colonic only).
Results: BMS cut-up performance meets RCPath guidelines and is comparable to overall departmental performance. Of note, our figures fall short of the exceptional results published by Peterson et al.2
Conclusion: The performance data from the cases handled by our BMS support the continuation of the BMS extended role within our department, with analysis of further data as it becomes available. The data collected, namely mean lymph node harvest and frequency of extramural vascular invasion and serosal involvement, have been demonstrated to be important in determining patient prognosis and appropriate adjuvant therapy.1 2 4
EGFR, HER-2, HER-3 AND HER-4 RECEPTOR EXPRESSION IN NEUROENDOCRINE TUMOURS
R. Srirajaskanthan1, T. Shah1, J. Watkins2, L. Marelli1, A. Quaglia2, K. Khan2, R. Sim2, M. Caplin2, D. Hochhauser3. 1Gastroenterology, 2Histopathology, Royal Free Hospital, 3Oncology, University College Hospital, London, UK
Introduction: The HER family is comprised of four distinct receptors: EFGR, HER-2, HER-3 and HER-4. These are transmembrane receptors composed of an extracellular ligand-binding domain and a cytoplasmic region with enzymatic activity. Over-expression of HER family receptors is associated with reduced survival in patients with breast cancer, colon and ovarian cancer.
Aims & Methods: In this study we sought to determine the pattern of expression and the prognostic significance of EGFR, HER-2, HER-3 and HER-4 in neuroendocrine tumours. Consecutive samples of formalin-fixed paraffin-embedded tumour tissue were available from 81 patients with a histologically confirmed diagnosis of neuroendocrine tumour (NET). The study population included all major NET subtypes including: foregut, mid-gut, hindgut, bronchial, paraganglionoma and NETs of unknown primary. Tumours were classified according to their site of origin, level of differentiation and their initial mitotic index. Scoring was based on intensity of staining whereby 0 = negative, 1 = weakly positive, 2 = moderate, 3 = strongly positive. Tumour staining was also scored, whereby, positive staining was marked as: 1 = <25%, 2 = 25–75% and 3 = >75%. The product of the density of staining and the percentage of tumour cells staining positive was used as the histological score, giving final values of 0, 1, 2, 3, 4, 6, 9. Score of ⩽2 were classed as negative.
Results: EGFR expression was identified in 69 of 81 (85.1%) samples, HER-2 was not expressed in any tissue, HER-3 was expressed in 7 samples (3 pancreatic, 3 paraganglionoma and 1 mid-gut), HER-4 was expressed 74 (91%). EGFR negative tumours were associated with a significantly worse prognosis than EGFR positive tumours (p = 0.014). There was no significant association between expression of HER-4 or HER-3 and survival. No significant correlation between EGFR and HER-4 expression.
Conclusion: EGFR and HER-4 are significantly expressed in NETs. EGFR and HER-4 share many the same ligands, this in part may explain the expression of these two receptors in NETs. The expression of EGFR does not appear to be a negative prognostic indicator.
THE ROLE OF ALPHA FETOPROTEIN AND HUMAN CHORIONIC GONADOTROPHIN-β; AS PROGNOSTIC TUMOUR MARKERS IN PATIENTS WITH NEUROENDOCRINE TUMOURS
R. Srirajaskanthan1, T. Shah1, M. Bhogal1, C. Toumpanakis1, T. Meyer2, A. Noonan1, T. Amin1, C. Witney- Smith1, S. Niroshan1, W. Ben1, D. Hochhauser3. 1Gastroenterology, 2Oncology, Royal Free Hospital, 3Oncology, University College Hospital, London, UK
Introduction: Serum chromogranin A is the best general tumour marker available for neuroendocrine tumour (NET) patients. The role for other tumour markers is less clear.
Aims & Methods: To determine the diagnostic and prognostic value of serum alpha-fetoprotein (AFP) and human chorionic gonadotrophin β (hCG-β) in NETs. A database containing biochemical, histological including Ki67 proliferation index, and survival data on 360 NET patients was constructed using an excel spreadsheet. These data were statistically assessed, using SPSS statistics package, to determine the utility of commonly measured tumour markers with particular emphasis on AFP and hCG-β.
Results: AFP and hCG-β were raised in 9.5% and12.3% of patients respectively. AFP levels associated strongly and positively with tumour grade, serum CgA, hCG-β levels and worse survival (mean 37.6 vs 69 months for AFP-high and control groups respectively; p = 0.001). hCG-β levels also associated strongly and positively with serum CgA, AFP levels and worsening survival (mean 48 vs 57.3 months for hCG-β high and control groups respectively; p = 0.037).
Conclusion: Both AFP and hCG-β are elevated in high-grade neuroendocrine tumours with a rapidly progressive course and poorer survival. They also correlate with chromogranin-A, which is known to be a marker of tumour burden and to have prognostic value. Thus AFP and hCG-β are clinically important in NETs and should be routinely measured.
TUMOUR GROWTH ASSESSMENT USING MINIMUM SPANNING TREE ANALYSIS IN PANCREATIC, AMPULLARY AND DISTAL BILE DUCT CANCER
C. S. Verbeke1, K. V. Menon2, J. Knapp3. 1Histopathology, 2Surgery, St James’s University Hospital, 3School of Physics and Astronomy, University of Leeds, Leeds, UK
Introduction: The definition of microscopic resection margin involvement (R1) in large bowel cancer (LBC) has been established as tumour cells <1 mm to the margin. This R1 definition is also used for the reporting of pancreatic head cancer specimens, but has never been validated. The Minimum Spanning Tree algorithm (MSTA) is a computer based method that analyses the topology of cancer growth patterns by determining the minimum distance between tumour cells.
Aims & Methods: To determine, using the MSTA, whether a similar growth pattern in LBC and cancer arising in the pancreatic head justifies the current R1 definition for reporting of the latter. In 10 cases of each LBC, pancreatic (PC), ampullary (AC) and distal bile duct cancer (DBC) a 200× picture was taken in the centre and periphery (at the invasive front) of the tumour as well as half way between both. For each picture, the distances between cancer cells were determined using the MSTA. The average minimum distance was compared between the 3 zones in the 4 cancer groups, as was the tumour cell density.
Results: In all cancer groups, the distance between cancer cells was comparable in the central zone, and larger in the periphery than in the centre of the tumour (p⩽0.02). However, this difference between centre and periphery was smaller in LBC than in PC, DBC and AC (p⩽0.03). Results were similar for PC and DBC, but differed from those of AC (p⩽0.03). On average, the tumour cell density dropped in the periphery of PC to 30% of that in the tumour centre, and only to 83% in LBC (p<0.0001), 62% in AC and 40% in DBC (p⩽0.01).
Conclusion: Tumour cell growth in PC, DBC and—to a lesser extent—AC is less dense than in LBC. Particularly in the periphery, tumour growth is more dispersed in PC, DBC and AD, and tumour cell density drops to as little as 30% at the invasive tumour front. This difference in tumour growth demands revision of the R1 definition for pancreatic head cancer. The MST algorithm is a useful tool to assess the topology of cancer growth patterns.
Gastrointestinal physiology posters
OVERWEIGHT AND WAIST CIRCUMFERENCE ARE RISK FACTORS FOR GASTRO-OESOPHAGEAL REFLUX DISEASE
R. Anggiansah1, R. Sweis2, T. Wong2, M. Fox1, A. Anggiansah1. 1Oesophageal Laboratory, 2Gastroenterology, St Thomas’ Hospital, London, UK
Introduction: The increasing prevalence of obesity and gastro-oesophageal reflux disease (GORD) strongly suggests an association between these two conditions. Previous studies indicate that waist circumference (WC) but not body mass index (BMI; kg/m2) is independently associated with oesophageal acid exposure.
Aims & Methods: This study aimed to examine the relationship between increasing WC and specific reflux parameters on 24-h pH monitoring to provide insight into the mechanism by which this occurs. A prospective study of 676 consecutive patients with suspected GORD referred for oesophageal investigation. Height, weight and waist circumference (WC) were measured. 24-h ambulatory pH studies were performed. The associations between demographic variables, reflux parameters (oesophageal acid exposure (%time-pH<4), number of reflux episodes (NR), longest reflux episodes (LR)) and the DeMeester score) was assessed in four time periods (total, upright, supine and postprandial) by univariate and multivariate analysis. In addition, symptom severity was assessed by a validated questionnaire.
Results: Complete 24-h pH data for 583 (86%) patients with M:F 44.%:56% were available. The prevalence of obesity was similar in both sexes. %time-pH<4 and LR were associated with increasing age in all time periods (all with p<0.001); however no such effect was seen for reflux symptoms (p>0.1). WC (adjusted for age and sex) but not BMI was independently associated with a significant increase in all reflux parameters during all four time periods (all p<0.001). There was a progressive increase in reflux parameters (%time-pH<4, NR and LR) from the low (WC <89 cm) through the medium (89–99 cm) to the high tertile group (WC >99 cm) which was significant in all time periods (all p<0.001). Similarly, the odds ratios for pathological reflux (DeMeester >14.7) adjusted for age and sex compared to patients with a low tertile WC was elevated in the medium tertile (OR 1.58, CI 1.02 to 2.44; p<0.001) and the high tertile groups (OR 3.36, CI 2.14 to 5.28; p<0.001). WC was not associated with the severity of reflux symptoms independent of oesophageal acid exposure (p = 0.1).
Conclusion: In patients referred for investigation of reflux symptoms WC is associated with increasing the number and duration of reflux episodes and overall oesophageal acid exposure, in all study periods. This indicates that obesity increases the severity of reflux disease both by increasing the frequency of reflux episodes in both the upright position likely by increasing the risk of reflux during transient lower oesophageal sphincter relaxation, but also in the supine position likely due to weak and incompetent reflux barrier and impaired clearance.
INTER-INDIVIDUAL VARIATIONS IN THE GUT-TO-BRAIN SIGNALLING RESPONSES TO HEXOSE SUGARS
A. Gopinath, T. Little, J. T. McLaughlin, D. Lassman, S. Rhodes, D. G. Thompson. GI Sciences, Hope Hospital, Manchester, UK
Introduction: The incidence of obesity is increasing rapidly. The increased consumption of fructose has been implicated in the pathogenesis of obesity. Therefore, understanding the mechanisms by which different sugars influence the gastrointestinal signaling to the brain, and thus the central regulation of appetite, is of paramount importance. Sugars are proposed to slow gastric emptying (GE), a proxy measure of brainstem activation, by stimulating osmoreceptors in the small intestine; however, glucose and fructose appear to empty differently.1 Furthermore, large inter-individual differences in the GE response to sugars were apparent.1 Previous studies have been unable to explore gastric emptying responses in detail within an individual due to limitations in methodology, therefore, it is unclear whether the reported differences are a true representation of an individuals responsiveness.
Aims & Methods: Primary aims of this study were, therefore, to determine: (1) the effects of hexose sugars, glucose, fructose and galactose on GE and (2) whether inter-individual differences in GE were consistent within individuals. 7 healthy subjects were studied after an overnight fast on 10 separate occasions to evaluate the effects of 500 ml solutions of glucose, galactose and fructose at 250, 500 and 1000 mOsmol, or water on GE (assessed using a 13C-acetate breath test). Subsequently, 3 subjects underwent 32 studies to evaluate intra-individual reproducibility in the GE of 250 mOsml hexose sugars.
Results: As the osmolality of the hexoses increased, GE was more potently slowed (p<0.001). At a low osmolality (250 mOsmol), a sugar-specific effect was apparent; the effects of fructose were more potent than those of glucose and galactose (p<0.05). After observing substantial inter-individual differences in the response to sugar ingestion at 250 mOsmol, we investigated whether the GE response within an individual was consistent. In Subject A, but not subjects B and C, fructose consistently slowed GE (p<0.05).
Conclusion: Hexose sugars slow gastric emptying in both an osmolality-dependent and sugar-specific fashion. At a low osmolality (250 mOsmol), fructose emptied from the stomach more slowly than both glucose and galactose; as the osmolality increased, the difference between the sugars decreased. Furthermore, while the effects of glucose and galactose on gastric emptying were relatively consistent between individuals, there was substantial inter-individual variation in fructose at 250 mOsmol; some individuals did not slow gastric emptying in response to fructose. Understanding the mechanisms underlying the inter-individual variations in the gastric emptying response to fructose may help to explain why some individuals are more susceptible to obesity in an obesogenic environment.
The below abstract is now an oral presentation in the Gastrointestinal Physiology Associates Group on Wednesday 12 March
DO PATIENT’S REPORTED FOOD TRIGGERS REALLY PROVOKE GASTRO-OESOPHAGEAL REFLUX AND HOW WELL ARE WE ADVISING THEM?
D. Vasant1, M. Deakin2, C. Cheruvu2, S. Evans1, F. C. Leslie1. 1Gastroenterology, 2Upper GI Surgery, University Hospital of North Staffordshire, Stoke-on-Trent, UK
Introduction: Different food intolerances and lifestyle practices are thought to trigger reflux. Foods act both as direct irritants or indirectly either pharmacologically or hormonally on the lower oesophageal sphincter—for example, fats. Lifestyle advice is important, but we hypothesised that there would be a wide variation in how effectively this was given.
Aims & Methods: A questionnaire was developed for gastro-oesophageal reflux disease (GORD) patients awaiting GI physiology appointments, asking about advice patients received, which foods precipitate their symptoms and nominated one food as a “test meal”. The post-prandial effect of the “test meal” on the oesophageal pH was analysed at 24-h pH/manometry.
Results: Data were obtained from 45 of 66 patients and 48 trigger foods identified. The top 4 trigger foods were fatty foods 76%, fried foods 71%, spicy foods 71% and pastry 69%. 75% (34) reported frequent heartburn (daily/several times/week), where the mean no of “trigger” foods was 14.0/patient, compared to those with infrequent heartburn (n = 11), mean 7.2. Despite referral for pH studies, only 71% recalled lifestyle advice. 63% to raise head of bed, 53% to eat regular small portions, 50% weight loss, 44% to avoid trigger foods, 25% to avoid late meals and 16% to reduce alcohol. In pH studies (n = 18), test meals chosen by patients included pastry (6), spicy food (4), chocolate, spearmint and muesli. Two patients had normal pH (Demeester <14.72). 88% (14/16) who had physiological reflux had increase in %time pH<4 2 hours post test meal, compared to total during 24-h study. Significant reflux was demonstrated in 5/6 patients who ingested pastry and 4/4 after spicy food test meals. Muesli and spearmint did not induce physiological reflux.
Conclusion: Reflux sufferers reported a large variety of “trigger” foods. Patients with more frequent reflux symptoms report double the amount of food triggers compared to those with infrequent heartburn. 88% of patients who ingested a food they believed to trigger their symptoms during 24-h pH testing, actually had a refluxogenic episode post-prandially. Better provision of consistent information about lifestyle and dietary measures could improve patient outcome.
WHAT DO GASTROENTEROLOGY TRAINEES KNOW ABOUT OESOPHAGEAL MANOMETRY AND PH MONITORING?
J. D. Shutt1, F. Robbie1, P. Boger2, A. Quine1. 1Gastroenterology, Queen Alexandra Hospital, Portsmouth, 2Gastroenterology, Southampton General Hospital, Southampton, UK
Introduction: Oesophageal manometry and pH monitoring is widely available for the investigation of oesophageal symptoms. However, trainees are frequently not exposed to these techniques. In November 2006 the BSG issued updated guidelines for oesophageal manometry and pH monitoring, acknowledging the advent of PPIs and their value in therapeutic trials.
Aims & Methods: We aimed to evaluate the knowledge of oesophageal manometry and pH monitoring against key recommendations made in the BSG guidelines, among gastroenterology SpRs in the Wessex region. All received a 25-point questionnaire that was completed electronically.
Results: 18/30 (60%) responded. One trainee worked in a hospital without oesophageal manometry and pH monitoring onsite. Knowledge of oesophageal manometry was good, although 22% considered it a first line investigation in patients with suspected oesophageal symptoms. Regarding ambulatory oesophageal pH monitoring: 44% wrongly considered it to have a very low false negative rate; 39% considered prior endoscopy necessary for accurate electrode placement; and while all knew that it allows correlation between reflux events and symptoms, only 41% understood the ideal time. Trainees overestimated normal oesophageal acid exposure, with mean total, upright, and supine times for oesophageal pH<4 for less than 11%, 7.6% and 13.4% respectively (5, 8 and 3% in the guidelines). Only 1 trainee was aware that the degree of supine reflux should be less than that upright, other responses ranged from 5–50%. The majority appreciated that pH monitoring should be the investigation of choice in patients with symptoms suggestive of gasto-oesophageal reflux disease (GORD) (89%) and in cases with atypical symptoms possibly due to GORD, a prolonged therapeutic trial of a PPI is considered more relevant (83%). The most confusion concerned having pH monitoring on or off a PPI in GORD: 44% correct in testing on a PPI in a failed therapeutic trial; 39% correct in testing off a PPI in endoscopy negative oesophagitis with a good response to PPI prior to anti-reflux surgery. In a patient with symptoms potentially due to GORD with a failed therapeutic trial, no trainee was correct in advising a pH study on a PPI prior to anti-reflux surgery. Knowledge of procedural issues were satisfactory, although only 33% and 11% appreciated the restrictions on diet and activity respectively, and only 44% were aware of the need for antibiotic prophylaxis if high risk of bacterial endocarditis.
Conclusion: The working knowledge of oesophageal manometry and pH monitoring among trainees was adequate at best, with limited in-depth knowledge and confusion regarding performing pH monitoring on or off PPIs. To ensure trainees refer patients appropriately, further training and exposure to these techniques is required.
Liver posters
ASSESSMENT OF “NUCLEATION TIME” AS A GOOD PREDICTOR OF CHOLELITHIASIS
V. Abeysuriya1, K. I. Deen1, S. K. Kumarage1, N. M. M. Navaratne2. 1Surgery, Faculty of Medicine, Ragama, University of Kelaniya, Sri Lanka, 2Medicine, National Hospital of Sri Lanka, Colombo, Sri Lanka
Introduction: In the formation of gallstones, crystal nucleation is the key step, which is followed by precipitation and gradual growth of cholesterol crystals.
Aims & Methods: A case control study was performed among 60 subjects (30 patients, 14 males: 16 females, median age 36 years, range 33–71 years, BMI = 25.1 +/−0.33 kg/m2, who underwent laparoscopic cholecystectomy; 30 controls, 15 males: 15 females, median age 38 years, range 33–70 years, BMI = 24.5+/−0.23 kg/m2, who underwent laparotomy and who had normal ultrasound scans of the gallbladder and no demonstrable stones). Bile aspirated from the common bile duct was ultrafiltered and anaerobically incubated at 37°C. Incubated bile was examined daily by polarised light microscopy (PLM), for appearance of cholesterol crystals. Nucleation time (NT) of bile was assessed as the time taken for the first crystals to appear under PLM.
Results: Controls were not different to cases studied. The overall mean NT was significantly shorter in patients versus controls (mean NT, patients: 1.76+/−0.2 SEM days; vs controls: 12.74+/−0.4 SEM days, p = 0.001). Of controls, females demonstrated a shorter NT compared with males (mean NT, females, 11.4 +/−0.36 SEM days; vs males, 14.1 +/−0.46 SEM days, p = 0.006). By contrast, there was no gender difference in NT in patients (mean NT, females: 1.7+/−0.24 SEM days; vs males: 1.8+/−0.2 SEM days, p = 0.7).
Conclusion: Overall, females tend to have shorter nucleation time compared with males. However, in those with demonstrable gallstones, there appears to be no significant difference in bile nucleation time.
EXPERIENCE OF A NURSE LED HEPATOMA SCREENING CLINIC
L. Bailey1, P. Dundas1, C. Clark2, A. Fraser1. 1Department of Gastroenterology, 2Department of Radiology, Aberdeen Royal Infirmary, Aberdeen, UK
Introduction: Hepatocellular cancer (HCC) is the fourth most common cancer in the world with the majority of cases having cirrhosis and/or chronic hepatitis B (HBV) infection. Once symptomatic, cure is seldom possible and prognosis is poor. Surveillance is recommended in high risk patients and aims to detect early tumours where curative therapy may be offered. Alphafetoprotein (AFP) is inadequate as a screening tool alone as the sensitivity is 60% and therefore ultrasonography with a sensitivity of between 65% and 80% may be used in combination with AFP. The ideal surveillance interval is unknown, an interval of 6–12 months has been proposed based on tumour doubling times.1 The clinic was established in September 2005. Patients with cirrhosis or at a high risk of HCC (with HBV infection) were referred to the clinic primarily from one consultant. The clinic operates twice monthly with 10 ultrasound appointments and nurse review/phlebotomy on the same day. A 6-month interval between appointments was selected. Although the clinic started in September 2005, there was an initial 6-month period before activity was monitored.
Aims & Methods: Details of patients with a diagnosis of cirrhosis were recorded prospectively into a database. An audit of all patients on the database and clinic attendance outcomes from March 2006–September 2007 were evaluated.
Results: As of September 07 there were 245 patients with cirrhosis or a diagnosis of chronic HBV infection on the database with 99 patients (40%) attending the clinic. Reasons for not offering appointments were; age >70 (depending on fitness) (30%), geographic distance from centre (23%), recurrent non-attender (20%), consultant discretion (primarily due to ongoing chaotic substance misuse) (19%) and lost to follow-up (8%). Of those being screened, the mean age is 54 years (range 21–76) and 68 (68%) are male. Since March 2006, there have been 270 appointments offered with 227 (85%) attending, 20 (6.5%) appointments were lost due to patients who could not attend giving prior notification and only 23 (8.5%) when the patient did not attend without prior notification. Since the clinic was established, there have been 3 new diagnoses of hepatocellular carcinoma. Patient A tumour size 1.5×6 cm required chemoembolisation awaiting transplant; Patient B tumour size 1 cm required surgery and chemoembolisation; Patient C tumour size 3.5×5.1 cm required surgery. All tumours have been diagnosed at the initial clinic visit with no tumours diagnosed through 6-monthly follow-up.
Conclusion: The clinic was well attended but this may be due to our selection criteria. The clinic has only operated for 2 years and the ability to identify tumours at an early stage requires further evaluation.
PHYSICAL ACTIVITY AND REDUCED RISK OF SYMPTOMATIC GALLSTONES: A PROSPECTIVE COHORT STUDY
P. J. Banim1, S. Bingham2, R. Luben2, N. Wareham2, A. Welch3, K. Khaw4, A. Hart3. 1Gastroenterology, Norfolk and Norwich University Hospital, Norwich, 2Institute of Public Health, University of Cambridge, Cambridge, 3School of Medicine, University of East Anglia, Norwich, 4Clinical Geronotology Unit, University of Cambridge, Cambridge, UK Kingdom
Introduction: Physical activity may protect against gallstone formation by reducing bile stasis and plasma triglycerides and by raising HDL levels. No prospective studies have previously investigated this hypothesis in both genders using a physical activity questionnaire validated against physiological measurements. The aim of this study was to investigate this relationship using a questionnaire to provide a simple global index of physical activity and to determine if physical activity predicts disease independently of known risk factors for gallstones.
Aims & Methods: A total of 25 639 men and women, aged 45–74, years were recruited into EPIC-Norfolk (European Prospective Investigation into Cancer) and completed a questionnaire which recorded both occupational and recreational physical activity. Participants were then ranked into four groups of physical activity, ranging from active to inactive. This questionnaire had been validated against both energy expenditure, as assessed by 4-day heart rate monitoring, and cardiorespiratory fitness, assessed by submaximal oxygen uptake. The cohort was monitored for the development of symptomatic gallstones and each case matched with four controls for age and sex. Odds ratios were calculated using unconditional logistic regression, adjusted for body mass index, alcohol intake, hormone replacement therapy and parity.
Results: In the cohort, 219 participants (67.6% women) developed symptomatic gallstones at a mean age of 61.3 (SD 9.0) years. Increased physical activity decreased the risk of symptomatic gallstones stones in a linear manner across the four categories of physical activity (odds ratio for trend 0.85, 95% CI 0.72 to 1.0, p<0.05). An active vs inactive level of physical activity gave an odds ratio of 0.48 (95% CI 0.26 to 0.89 p = 0.02). Physical activity was independently associated with a reduced risk of gallstones after multivariate adjustment for known risk factors (p<0.05).
Conclusion: Increased physical activity was associated with a decreased risk of symptomatic gallstones, a consistent finding in epidemiological studies, and now reported for the first time using a physical activity questionnaire validated against physiological measurements. If the level of physical activity in the population could be raised, then 33% of symptomatic gallstones could be prevented.
MYCOPHENOLATE MOFETIL IN PATIENTS WITH REFRACTORY AUTOIMMUNE HEPATITIS
A. T. Barnardo, U. Warshow, J. Mitchell, M. Cramp. Hepatology, Derriford Hospital, Plymouth, UK
Introduction: Autoimmune hepatitis has a prevalence of 16.9/100 000 in the European population and 65% respond to standard therapy of prednisolone and azathioprine by 18 months. However 15% are either intolerant of standard therapies or suffer long-term treatment failures.
Aims & Methods: A retrospective case study was performed for patients treated with mycophenolate mofetil (MMF) for autoimmune hepatitis (AIH) between 1999–2007. Eleven females and one male were identified all had definite autoimmune hepatitis on the International hepatitis scoring system with pre treatment scores greater than 15 (median 17, range 15–21).
Results: Patients had received MMF because of toxicity and intolerance to either azathioprine (n = 3) or 6-mercaptopurine (6MP) (n = 1); treatment failure with prednisolone, azathioprine and tacrolimus (n = 2); or intolerance and treatment failure (n = 5). One patient was commenced on MMF as the primary steroid sparing agent. While on MMF tranaminases normalised in 6/12 patients and prednisolone dosages were reduced in 10/12 and discontinued in a further case but 4 are now cirrhotic. Toxicity with Azathioprine caused Stevens-Johnson reaction and neutropaenia (normal TPMT) and 6MP toxicity caused haemolysis and presented with 4 weeks in all cases. Two further patients were intolerant with severe headaches and nausea. All 5 are in biochemical remission on lower doses of prednisolone and MMF, and one is off all treatment. One patient has features of NAFLD rather than AIH on their last biopsy. One patient had treatment failure on prednisolone and azathioprine and one was also refractory to the addition of with Tacrolimus. Both have persistent biochemical evidence of disease activity and prednisolone doses have not been reduced, and their biopsies reveal cirrhosis but no interface activity. One has now decompensated with jaundice and ascites. Five patients had treatment failure (prednisolone, azathioprine n = 4, prednisolone, azathiprine and tacrolimus n = 1) and severe intolerance. One has progressed to biopsy proven cirrhosis and one has stage 3 fibrosis and has had a variceal bleed. Three have entered biochemical remission on lower dose prednisolone but no histology is available. The patient who progressed to cirrhosis has had compliance difficulties. The patient treated with MMF as the primary steroid sparing agent because of pre-existing thrombocytopenia progressed to cirrhosis.
Conclusion: Patients in whom there was a drug intolerance but biochemical response were maintained in remission on MMF. Patients who did not respond to prednisolone and azathioprine/6MP were not controlled by MMF and progressed to cirrhosis. Response in patients with both intolerance and treatment failure had a variable outcome. Alternative immunosuppressive regimes should be considered for those patients refractory to prednisolone and azathioprine/6MP.
AUDIT OF MANAGEMENT OF ALCOHOL WITHDRAWAL AT DERRIFORD HOSPITAL
A. T. Barnardo, L. Walters, M. Cramp, J. Mitchell. Hepatology, Derriford Hospital, Plymouth, UK
Introduction: Alcohol-related morbidity and mortality is an increasing problem in the UK. Approximately 5% of males and 3% of females are drinking at hazardous levels. Hospital admissions for inpatient alcohol detoxification has dramatically increased from 49 in 2000 to 139 in 2006. Trust guidelines advise the use of Clinical Institute Withdrawal Assessment for Alcohol (CIWA) score for assessment of severity and only oral benzodiazepines for treatment.
Aims & Methods: Notes were reviewed for patients admitted in the last 12 months with alcohol withdrawal. Demographics and outcomes were recorded and their clinical management was compared to the trust guidelines.
Results: Fifty three men and 21 women, were identified. Chronic liver disease was evident in 19% men and 8% women and a previous recognised psychiatric diagnosis was present in 24% men and 12% women. CIWA score was recorded in the medical notes at admission in 77% patients and a repeat CIWA was recorded in 53% and 73% cases in the medical and nursing notes respectively. Diazepam was used in 54%, lorazepam 7% and a combination in 28%. Intravenously sedation was only administered in ITU. Pabrinex and oral vitamin supplements were given to 95%. Generalised seizures occurred in 38% of which 3% had a history of head trauma. Security was called for 14% patients and 7% were admitted to ITU for intravenous sedation and 3% required ventilation. Patients were managed on 17 wards and patients managed on surgical wards only had CIWA scores recorded in 3/12 cases. The median length of stay was 5.8 days (range 1–28) and 23% took their own discharge. Three patients with concomitant chronic liver disease died during their admission from PE, septicaemia and multi-organ failure respectively. A further 3 have died since discharge.
Conclusion: The assessment of severity of alcohol withdrawal was poor with documentation at admission in only 77% and in 27% no assessment was documented throughout the admission despite the dispensing of benzodiazepines. An unexpected high percentage of patients admitted with alcohol withdrawal have severe symptoms. Four of the admissions to ITU were unavoidable as oral sedation was not sufficient. Requests for security could have been obviated if the severity of withdrawal had been realised earlier and acted upon. Features of chronic liver were found only in a minority of patients with alcohol withdrawal but were present in all patients admitted to ITU. Diazepam was given inappropriately to patients with chronic liver disease and this led directly to one admission to ITU because of respiratory depression. The use of intravenous benzodiazepines was not identified outside of ITU and the nutritional aspects of the patients care were performed well. More education is required on assessment and treatment of alcohol withdrawal.
CHANGING EPIDEMIOLOGY AND TREATMENT DECISIONS IN CHRONIC HEPATITIS B
I. S. Bhattacharya, A. J. Bathgate. Liver Unit, Royal Infirmary of Edinburgh, Edinburgh, UK
Introduction: In recent years there has been a change in the numbers and demographics of chronic HBV patients attending the Liver Unit, Edinburgh. Treating chronic HBV infection can prevent cirrhosis, end stage liver failure and hepatocellular carcinoma (HCC), however one of the difficulties in chronic HBV management is deciding if and when it is appropriate to treat. High HBV DNA levels are associated with the development of cirrhosis. The normal levels for ALT and the ALT level which determines treatment remains controversial.
Aims & Methods: The aims of this study were to determine the clinical and demographic characteristics of patients attending the Liver Unit, to identify the predictors of treatment using both our current ALT Upper Limit of Normal (ULN) (45 IU) and recently proposed ALT ULN (30 and 19 IU for men and women respectively (rev ULN)) and to identify the predictors of cirrhosis. This was a retrospective case note study, which included patients aged ⩾18 years. Patient names were obtained from an existing HBV database, the Chinese HBV Clinic, and from Liver Unit out-patient clinics.
Results: 204 patients with chronic HBV were identified; 8 patients were co-infected with HCV, 3 co-infected with HIV and 1 with HCV and HIV. 67% patients were male, and 33% female. 45% patients were Chinese, 30% were Caucasian and 9% Pakistani. The most common “likely mode of transmission” was perinatal (54%). Of the 204 patients, 31% were HBeAg +ve, 30% were currently receiving treatment, 3% had HCC, 21% were cirrhotic and 2% had received liver transplant. Following exclusion of our 12 co-infected patients the following were found; 31% were HBeAg +ve and 27% were receiving treatment. Predictors of treatment were the presence of HBeAg (p<0.0005) and an HBV DNA level ⩾500 000 copies (p<0.0005). Predictors of cirrhosis were HBV DNA ⩾500 000 copies/ml (p<0.0005) and HCV co-infection (p<0.005). The table shows the relationship of present and revised ALT levels.
Conclusion: HBV demographics in the Liver Unit are changing with an increasing number of Chinese patients attending. An increasing HBV DNA level is a strong predictor of cirrhosis which emphasises the importance of regular monitoring and suppression of HBV DNA levels. ALT was not a predictor of treatment using either the present or proposed values. This study shows that our decisions regarding treatment have not been rigorously based on ALT levels.
CONCOMITANT PRIMARY SCLEROSING CHOLANGITIS DOES NOT INCREASE THE RISK FOR COLORECTAL DYSPLASIA IN PATIENTS WITH COLONIC CROHN’S DISEASE
B. Braden1, S. Aryasingha1, B. Warren2, T. Kitiyakara1, R. Chapman1. 1Gastroenterology, 2Pathology, John Radcliffe Hospital, Oxford, UK
Introduction: It is established that patients with ulcerative colitis and concomitant primary sclerosing cholangitis have an increased risk of developing colorectal dysplasia or cancer compared with those patients with ulcerative colitis alone. Therefore, annual surveillance colonoscopies are recommended.
Aims & Methods: We investigated whether primary sclerosing cholangitis is a risk factor for developing colorectal dysplasia/cancer in patients with Crohn’s disease of the colon. A retrospective review of 168 patients with primary sclerosing cholangitis was performed. 118 had concomitant ulcerative colitis and 50 Crohn’s disease. 109 patients with colonic involvement of Crohn’s disease served as controls. The primary outcomes were colorectal cancer and dysplasia. The secondary outcome was overall mortality.
Results: None of the patients with colonic Crohn’s disease developed dysplasia during follow-up of 9±6 years, neither the patients with concomitant PSC, nor with Crohn’s disease alone. In contrast, 2 cancers and 7 colorectal dysplasia were diagnosed in patients with ulcerative colitis and PSC during follow-up of 11±7 years giving a crude annual incidence rate of dysplasia or colorectal cancer of 1 in 144 patients. The general (p = 0.12) or PSC related (p = 0.20) mortality did not differ between PSC patients with ulcerative colitis or colonic Crohn’s disease.
Conclusion: The presence of primary sclerosing cholangitis in patients with colonic Crohn’s disease does not seem to increase the risk of devoloping dysplasia of the colon as it does in patients with ulcerative colitis.
PERIHEPATIC LYMPHADENOPATHY INDICATES AETIOLOGY IN ACUTE AND CHRONIC LIVER DISEASE
C. F. Dietrich1, D. Faust2, A. Ignee1, D. Schreiber1, A. Planner3, T. Hirche2, B. Braden4. 1Gastroenterology, Caritas Hospital, Bad Mergenteim, 2Gastroenterology, University Hospital, Frankfurt/Main, Germany, 3Radiology, 4Gastroenterology, John Radcliffe Hospital, Oxford, UK
Introduction: In chronic virus hepatitis C the total perihepatic lymph node volume reflects the underlying liver histology, viral load, and the host’s immunological response. Assessment of the perihepatic lymph node volume may represent an important diagnostic tool, and may help streamline the patient’s further management.
Aims & Methods: The purpose of this study was to prospectively assess whether perihepatic lymphadenopathy is associated with the aetiology of acute (and chronic) hepatitis. In 40 consecutive patients with transaminases >500 U/l without known liver disease the total perihepatic lymph node volume was assessed and compared to the ultrasound findings in 263 patients with known chronic liver disease and also 49 healthy controls.
Results: 31/40 patients were diagnosed with an acute viral hepatitis, while 9/40 patients were diagnosed with a toxic cause, resulting in acute liver damage. In all sonographically evaluated patients with acute viral hepatitis (29/31, 94%) perihepatic lymphadenopathy was found, whereas none of the patients with a toxic cause demonstrated lymphadenopathy. In chronic liver disease, perihepatic lymphadenopathy was present in 86% of viral, in 90% of autoimmune hepatitis, in 100% of primary sclerosing cholangitis, in 97% of primary biliary cirrhosis, but only in 6% of hemochromatosis, in 1% of fatty liver disease, and in 4% of cholecystolithiasis.
Conclusion: Perihepatic lymphadenopathy is found in infectious and autoimmune liver diseases, but not in metabolic or toxic liver damage. The absence of perihepatic lymph nodes in acute liver failure should lead to intensive search for a toxic or metabolic cause.
MISSED OPPORTUNITIES TO INTERVENE IN PROGRESSION TO ALCOHOLIC LIVER DISEASE
S. Benfield1, T. R. Card2. 1Gastroenterology, Kings Mill Hospital, Sutton in Ashfield, 2Department of Epidemiology and Public Health, University of Nottingham, Nottingham, UK
Introduction: Although the UK government’s alcohol harm reduction strategy of 2004 promised to “strengthen the emphasis on the importance of early identification of alcohol problems” it is far from clear that screening for alcohol problems has been widely adopted. If our patients are to receive benefit from intervention in their drinking behaviour, problem drinkers must first be identified.
Aims & Methods: To establish the efficacy of current practice (opportunistic case finding) in our trust we have audited the notes of those eventually referred to our drug and alcohol team. We have searched hospital records as well as their history provided to our drug and alcohol service to establish whether they have previously received any intervention for their drinking, and whether there had been an opportunity for their drinking problem to be detected at an earlier point.
Results: We requested records of the last 120 patients referred to the drug and alcohol service of our trust. Reasons for referral are given in the table. Of these we were able to obtain notes on 119 from which we abstracted information. 53 (45%) of these had previously been referred to alcohol services, but in 47 (40%) it was possible to identify clear evidence of problem drinking on a visit to the hospital prior to their first referral to alcohol services. On average failure to refer at the first opportunity resulted in a 1.6 year delay. Among the 23 finally referred with alcoholic liver disease (21 decompensated), 14 had had an opportunity for referral missed at an earlier stage, and in 11 the delay in referral exceeded one year. Of these 11 with a prolonged delay in referral only 1 had clear evidence of end organ damage at the first presentation (decompensated alcoholic liver disease). As can be seen in the table this high rate of delayed referral (61%) is greater in alcoholic disease patients than in any of the other groups we examined.
Conclusion: Although evidence of the benefit of strategies to intervene in problem drinking is not strong, we clearly cannot develop successful interventions until we identify those requiring them. At present, despite a well-funded drug and alcohol service in our trust, we are failing to do even this. We therefore plan to move from a system of case finding to one of screening.
ACUTE ALCOHOL WITHDRAWAL. IS IT TIME FOR NATIONAL GUIDELINES?
B. J. Colleypriest, P. F. Marden, A. Fard, J. Maltby. Gastroenterology, Royal United Hospital, Bath, UK
Introduction: Alcohol withdrawal is commonly encountered in all in-patient medical disciplines and carries a significant mortality. The psychiatric, psychological, forensic and medical problems of alcohol abuse/dependence are all well documented. Alcohol consumption, per person, has doubled since 1980 and continues to rise. Currently there are no national guidelines for the pharmacological management of acute alcohol withdrawal, although many hospitals have local policies.
Aims & Methods: This study aimed to answer the questions were local guidelines followed and was appropriate medication prescribed. Data for a 6-month period were retrospectively collected from the case notes of patients admitted through the medical admission unit at the Royal United Hospital. All patients treated for alcohol withdrawal were identified and pharmacological intervention recorded and compared to local guidelines.
Results: 51 patients were identified of whom 34 were male. The number of units of alcohol being drunk by each patient was recorded in 71% of cases. In addition to a regular decreasing dose, chlordiazepoxide was prescribed on a PRN basis for 63% of patients. Oral thiamine was prescribed in 79% patients but only according to guidelines in 16% of cases. Oral Vitamin B was prescribed in 59% patients of which only 14% followed guidelines. 37% of patients received multivitamins. Wernike’s encephalopathy (WE) was identified in 4 patients all of whom were prescribed parenteral B vitamins, but none according to guidelines. 47 patients, on review of notes, were deemed to be at risk of WE of whom 37 received parenteral B vitamins but only 4% followed guidelines.
Conclusion: This study demonstrates considerable variability and inadequacies in the treatment of alcohol withdrawal. Oral thiamine, vitamin B and PRN chlordiaxepoxide were only prescribed in 79%, 59% and 63% of patients respectively. Local guidelines were not followed in the vast majority of patients for thiamine, vitamin B, parenteral B vitamins or chlordiazepoxide prescription. Considering the rapid changeover of junior staff adherence to guidelines may be easier if national standardised guidelines were available.
LENGTH AND ADEQUACY OF HEPATITIS C VIRUS STAGING LIVER BIOPSY IMPROVE AS REGISTRARS SPEND MORE TIME IN POST
M. L. Cowan1, S. J. Thomson1, S. Musa1, M. Gess1, C. Finlayson2, S. Krishna3, S. Clark1, D. M. Forton1, T. M. Rahman1. 1Department of Gastroenterology and Hepatology, 2Department of Histopathology, St George’s Hospital, 3Division of Cellular and Molecular Medicine, St George’s, University of London, London, UK
Introduction: Liver biopsy is widely accepted as the gold standard for the staging of chronic liver disease secondary to infection with hepatitis C virus (HCV). Accuracy is reduced in small samples. A gold standard biopsy should be longer than 20 mm or contain 12 portal tracts. In our hospital, liver biopsy is performed by gastroenterology registrars who rotate in October.
Aims & Methods: We sought to determine the temporal trends in use of liver biopsy in patients with HCV and to assess the adequacy of tissue obtained for liver biopsy in our hospital. Patients with HCV undergoing liver biopsy between January 2001 and December 2006 were identified by a search of the histopathology database. Patient characteristics and biopsy findings were obtained by a search of the hospital electronic patient record.
Results: 258 percutaneous parenchymal liver biopsies were performed in patients with HCV. Eleven biopsies contained no liver tissue or were so small that the reporting pathologist described them as uninterpretable. The average patient was 46 years (range 10–78 years), 64% were male and 51% were infected with HCV genotype 1. 45% had minimal hepatic fibrosis (Ishak stage 0/1), 39% moderate fibrosis (stage 2–4) and 16% cirrhosis (stage 5/6). The average biopsy was 21.5 mm (range 3–57 mm) and contained 13.2 portal tracts (3–35). Sixty four per cent fulfilled the above criteria for biopsy adequacy. There were no differences in numbers of biopsies performed, viral genotype, fibrosis stage, biopsy size or adequacy when analysed by year between 2001 and 2006. There were significant differences in biopsy size and adequacy (p<0.05) depending upon the month that the biopsy was performed (but not in patient age, genotype or fibrosis).
Conclusion: Staging liver biopsy for assessment of HCV constitutes a significant workload for gastroenterologists and histopathologists. There has been no significant change in the numbers and findings of biopsies performed between 2001 and 2006. The adequacy of biopsies improves during the year that gastroenterology registrars spend in post, presumably reflecting increasing experience.
THE IMPACT OF CO-INFECTION OF HEPATITIS DELTA AND HUMAN IMMUNODEFICIENCY VIRUS ON THE NATURAL HISTORY OF CHRONIC HEPATITIS B
T. J. S. Cross, R. Dancer, M. Horner, P. M. Harrison, K. Agarwal. Institute of Liver Studies, King’s College Hospital, London, UK
Introduction: Background: Individuals with chronic HBV infection are at increased risk of developing cirrhosis, hepatic decompensation and hepatocellular carcinoma (HCC).
Aims & Methods: To assess the impact of co-infection with either hepatitis delta (HDV) or human immunodeficiency virus (HIV) on the natural history of chronic HBV infection. We performed a retrospective analysis of all chronic HBV infected patients attending our institution between 2000 and 2005. Patients were identified who were seropositive for anti-HDV antibody (HDV Ab), and anti-HIV Ab positive. Case records were reviewed for the presence of cirrhosis or HCC. Comparisons were made between HBV mono-infected patients against those co-infected with HDV or HIV. Statistical analysis was performed using χ2 tests and risk was calculated including 95% confidence intervals.
Results: 1026 patients were identified in whom HDV and HIV status was known in 941 patients. The median age for the entire cohort was 35 years (IQR 29–43). The median ages for the HBV mono-infected, vs HDV/HBV co-infected vs HIV co-infected, were 35 (29–43), 35 (28–46), and 42 (38–46) respectively (p = NS). 527 patients (56%) of patients were male. 841 patients had HBV mono-infection, 79 patients had HDV/HBV, and 22 patients had HIV co-infection. 1 patient had triple infection. HDV increased the risk of cirrhosis (22/78 (28%) vs 109/841 (13%), OR 2.64, 95% CI 1.55 to 4.49, p<0.0001), but did not increase the risk of HCC (8/78 (10%) vs 66/841 (8%), OR 1.34 95% CI 0.62 to 2.91, p = 0.46). The presence of HIV increased the risk of cirrhosis (13/21 (62%) vs 109/841 (13%), OR 10.91 95% CI 4.42 to 26.93, p<0.0001), and also increased the risk of HCC (7/21 (33%) vs 66/841 (8%), OR 5.87 95% CI 2.29 to 15.05, p<0.0001).
Conclusion: In our cohort, the presence of co-infection with HDV or HIV increased the risk of cirrhosis in chronic HBV patients. Interestingly, HIV but not HDV co-infection significantly increased the risk of HCC in our group. This may be due to lower HBV viral load often seen in HDV/HBV co-infection.
THE IMPACT OF STEATOSIS AND STEATOHEPATITIS IN TREATMENT RESPONSES IN PATIENTS WITH CHRONIC HEPATITIS C INFECTION
T. J. S. Cross, A. Quaglia, J. Nolan, I. Fletcher, K. Agarwal, P. M. Harrison. Institute of Liver Studies, King’s College Hospital, London, UK
Introduction: There is controversy regarding the impact that steatosis has on the rate of sustained virological response (SVR) amongst patients treated with pegylated interferon and ribavirin for chronic hepatitis C (CHC) infection.
Aims & Methods: To study the effect of pre-treatment liver biopsy steatosis and steatohepatitis on the likelihood of SVR with combination therapy. We studied liver biopsies and treatment responses in 204 consecutive patients treated for CHC between January 2001 to January 2005. Liver biopsies were graded according to the method described by Ishak. Steatosis and steatohepatitis were graded using the modified Brunt score. Patients were classified according to the presence or absence of steatosis and steatohepatitis. Patients were studied together and by their genotype. Patients achieving SVR were labelled as responders and those failing to achieve SVR as non-responders.
Results: 179 patients were included in the final analysis. 72% % were male, median age 46 years (interquartile range 40–52). 127 were Ishak Fibrosis grade 3 or less (71%), and 31 patients (17.3%) were cirrhotic (Ishak grade 5–6). The overall SVR rate was 59%, the SVR rates by genotype were: genotype 1 (35%), genotype 2 (82%), genotype 3 (79%), and genotype 4 (57%). 106 patients were responders (59%). Responders did not differ from non-responders in respect to gender, age, steatosis, necroinflammatory score or pre-treatment ALT. On univariate analysis reduced SVR was associated with non-genotypes 2 and 3 (p<0.0001), cirrhosis (p<0.0001), and steatohepatitis (p = 0.009). On multivariate analysis only non-genotype 2 and 3 (p<0.001), pretreatment weight (p = 0.002) were significantly associated with SVR. 98 patients had steatosis (51.9%). The Χ2 test for trend demonstrated a difference between the groups and the rates of steatosis (p = 0.14). Steatosis was lowest in genotype 2, 12/37 (32%) vs non-genotype 2, 81/142 (57%), p = 0.008. Genotype 3 had steatosis 34/54 (63%) vs non-genotype 3 59/125 (47%), p = 0.053. On exclusion of genotype 4 patients this reached statistical significance p = 0.028. Steatosis had no effect on the likelihood of being a treatment responder (p = 0.176). The presence of no or mild steatosis (grade 0–1) also had no effect on the SVR (p = 0.46). Steatohepatitis was present in 34 patients (19%). Patients with Steatohepatitis were older (49 years vs 44 years, p = 0.03), and were more likely to have more severe steatosis (grade 2–3 vs 0–1, p<0.0001), and cirrhosis (p<0.0001).
Conclusion: Steatosis has no effect on SVR. Steatohepatitis may predict poor outcome. SVR is mainly determined by genotype, patient weight, and the presence of cirrhosis. Therapeutic strategies aimed at treating steatohepatitis may improve SVR in at risk patients. Patients at risk should have liver biopsy to assess for steatohepatitis.
ALCOHOL INDUCED LIVER INJURY MOBILISES HAEMATOPOIETIC STEM CELLS THAT CONTRIBUTE TO HEPATIC FIBROSIS
E. Dalakas1, P. N. Newsome1, S. Boyle2, A. Pryde1, W. A. Bickmore2, P. C. Hayes1, D. J. Harrison3, J. N. Plevris1. 1Hepatology Department, Univesity of Edinburgh, 2MRC Human Genetics Unit, Western General Hospital, 3Pathology Department, Univesity of Edinburgh, Edinburgh, UK
Introduction: Haematopoietic stem cells (HSCs) can contribute to multiple epithelial lineages including myofibroblasts in the human liver. HSC mobilisation and migration to injured liver are essential components of this pathway.
Aims & Methods: Our aim was to study the effect of alcohol liver injury on HSC mobilisation, hepatic recruitment and differentiation into hepatic epithelial lineages. Peripheral blood samples were collected from patients with alcoholic hepatitis (AH, n = 15), paracetamol hepato-toxicity (n = 7) chronic liver injury (n = 17) and normal controls (NC, n = 12). Circulating CD HSC levels were quantified. Colony forming unit (CFU) assays were performed on CD34+ cells. Cross-sex (x-sex) liver biopsies with AH were analysed for HSC content (CD34+) and for markers of myofibroblasts (α SMA), hepatocytes and biliary epithelium using immunohistochemical and fluorescent in situ hybridisation techniques.
Results: (1) The AH group had higher circulating blood CD34+ cell levels (0.195±0.063%, p<0.05) and higher CFU counts (154±38, p<0.05) when compared with NC (0.058±0.008% and 44±28 CFUs). (2) There were increased numbers of recipient CD34+ cells in x-sex donor liver grafts with AH as compared with controls (1.834±0.605% vs 0.299±0.208%, p<0.05). 3) Increased numbers of recipient α SMA+ cells (7.9%–26.8%) were identified in the AH x-sex liver grafts. (4) There were increased numbers of co-staining α SMA+/CD34+ cells in x-sex donor liver grafts with AH as compared with controls (5.025±0.621% vs 0.690±0.290%, p<0.05). (5) No recipient hepatocytes or biliary cells were identified in the x-sex donor liver grafts with AH.
Conclusion: (1) In AH, CD34+ stem cells are mobilised into the circulation and display true stem cell potential. (2) Alcohol liver injury recruits CD34+ cells into the liver and contributes significantly to the hepatic myofibroblast population but not to parenchymal lineages.
PIG MEAT CONSUMPTION AND MORTALITY FROM CHRONIC LIVER DISEASE
H. R. Dalton1, C. Pritchard2, R. Bendall3. 1Cornwall Gastrointestinal Unit, Peninsula College of Medicine and Dentistry, and Royal Cornwall Hospital, 2Research and Development Research Unit, 3Clinical Microbiology, Peninsula College of Medicine and Dentistry, and Royal Cornwall Hopsital, Truro, UK
Introduction: In 1985 Nanji and French reported a correlation between pork consumption and mortality from chronic liver disease (CLD),1 based on data from the 1960s and 70s. This finding has never been confirmed nor adequately explained. This observation is currently of interest because of the emergence of locally acquired hepatitis E infection (HEV) in the developed world. Locally acquired HEV in developed countries is thought to be a zoonosis from pigs. It is much more common than previously realised, has a predilection for middle aged/elderly males, is caused by HEV genotype 3, and carries an adverse prognosis in CLD.2 Viable HEV has been isolated from retail pig meat in the USA,3 and HEV can survive cooking temperatures up to 60°C.4
Aims & Methods: To correlate the mortality from CLD with pork, beef and alcohol consumption and the seroprevalence of HBV and HCV in developed countries. Data from 1990–2000 in 18 developed countries for mortality from CLD, alcohol consumption, HBV and HCV seroprevalence were obtained from WHO databases, and pig meat and beef consumption from United Nations databases. Mortality from CLD was compared with the other variables using regression analysis.
Results: Bivariate regression showed that alcohol (t = 3.792, p = 0.002) and pig meat (t = 4.255, p = 0.001) consumption were associated with mortality from CLD, but beef consumption, HBV and HCV seroprevalence were not. Multivariate regression showed that alcohol (t = 3.403, p = 0.005) and pig meat (t = 4.691, p<0.001) consumption and HBV seroprevalence (t = 2.317, p = 0.037) were independently associated with mortality from CLD, but HCV seroprevalence was not.
Conclusion: Pig meat consumption is independently associated with mortality from chronic liver disease in developed countries. The reason for this observation is uncertain: it could be an epiphenomenon; a factor in pig meat (for example, pork fat) might cause cirrhosis; a factor in pig meat (for example, HEV) may cause increased mortality in patients with pre-existing chronic liver disease. The latter possibility is not as improbable as might at first be thought, as we have previously shown that 16% of blood donors in SW England are HEV IgG positive and up to 21% of US blood donors are seropositive. This suggests that unrecognised infection with HEV is common.
EVALUATION OF ABNORMAL LIVER FUNCTION TESTS IN PRIMARY CARE
T. Dickel, A. Sinha, M. Lancaster-Smith, H. Curtis. Gastroenterology, Queen Mary’s Hospital, Sidcup, UK
Introduction: Abnormal liver function tests (LFT) are a common finding in primary care. When significant underlying disease of the liver is suspected an ultrasound scan (USS) should be arranged in the clinical context together with additional blood tests, lifestyle and medication changes and referral to a specialist.1 2
Aims & Methods: 172 patients referred for open access USS to Queen Mary’s Hospital between February 2005 and January 2006 by their General Practitioner (GP) for investigation of abnormal LFTs had been identified. For 124 patients results were available from the pathology department. Data from GP notes were gathered for 78 patients by visiting the surgeries. The objective of this study is to assess the investigations arranged by GPs leading to and following open access USS for abnormal LFTs.
Results: USS for 93/124 (75%) patients showed fatty infiltration of the liver. Hepatitis A, B and C serology had been requested in 20/124 (16.1%), 43/124 (34.7%) and 39/124 (31.5%) patients respectively. Metabolic diseases had been screened for in 2/124 (1.6%) for Wilson’s disease, in 13/124 (10.5%) for α1-antitrypsin deficiency and in 33/124 (26.6%) patients for haemochromatosis. Antinuclear antibodies (ANA) were available in 20/124 (22.6%) patients. Smooth muscle antibodies (SMA) and antimitochondrial antibodies (AMA) were requested in 7/124 (5.6%) patients each. 17/124 (13.7%) and 11/124 (8.9%) patients had been referred to a gastroenterologist or surgeon. A liver screen including three groups of underlying liver diseases (viral, metabolic and autoimmune) was requested in 15/124 (12.1%), a screen including at least 1 or 2 groups in 46/124 (37.1%) and no further tests in 63/124 (50.8%) patients. 20/124 (16.1%) patients had LFTs higher than twice the upper limit of normal (ULN). Of this subgroup only 2/20 (10%) had further investigations and only 3/20 (15%) were referred to a specialist. Repeat LFTs were requested in 75/124 (60.5%) patients. 13/75 (17.3%) still had LFTs >2 ULN. For 78/124(62.9%) patients data from their GP notes was available. In 32/78 (41%) patients a potential cause was identified. Lifestyle advice was given in 16/78 (20.5%) cases. 7/78 (8.9%) and 9/78 (11.5%) patients were referred to a surgeon or gastroenterologist for further evaluation. In 38/78 (48.7%) cases no further investigations were arranged to follow up the results of the ultrasound.
Conclusion: Abnormal LFTs are often first diagnosed by the GP. Initial investigations and referral practice vary and are not always in line with current recommendations. The request for USS is often not accompanied by additional tests (screening for viral hepatitis, haemochromatosis and autoimmune disease). Implementation of guidelines for the evaluation of abnormal LFTs in primary care should be considered.
PROTEIN OXIDATION AND XANTHINE OXIDASE ACTIVITY IN HEPATITIS C VIRUS-RELATED HEPATOCELLULAR CARCINOMA: ROLE IN TUMOUR APOPTOSIS AND CYTOPROLIFERATION
H. A. El Aggan1, S. A. Mahmoud2, L. K. Younis3. 1Department of Medicine, Hepatobiliary Unit, 2Department of Medical Biochemistry, 3Department of Pathology, Faculty of Medicine, University of Alexandria, Alexandria, Egypt
Introduction: Hepatitis C virus (HCV) infection causes a state of chronic oxidative stress, which may contribute to hepatocarcinogenesis. The formation of reactive oxygen species (ROS) in the liver can promote oxidative damage of intracellular proteins, which tend to form high-molecular-weight aggregates and thereby influence a diverse array of cellular processes. Xanthine oxidase (XO) is a primary source of ROS and a key enzyme in protein oxidation.
Aims & Methods: The present work was designed to study the changes in protein oxidation and XO activity in patients with HCV-related hepatocellular carcinoma (HCC) in relation to the rates of tumour apoptosis and cell proliferation. To achieve this goal, the plasma levels of carbonyl proteins and advanced oxidation protein products (AOPP), as markers of protein oxidation, and plasma XO activity were determined in 50 patients with HCV-related cirrhosis (30 with histologically-proven HCC of different grades and stages and 20 without HCC) and in 20 healthy subjects. Core liver biopsies of hepatic tumours were examined for the rate of apoptosis using the terminal deoxynucleotidyl transferase-mediated deoxyuridine triphosphate nick-end labelling (TUNEL) method and for mutant p53 expression by immunohistochemistry. The proliferative activity of HCC was quantitatively assessed using proliferating cell nuclear antigen (PCNA) labelling.
Results: The plasma levels of carbonyl proteins and AOPP and plasma XO activity were significantly higher in cirrhotic patients with and without HCC than in healthy subjects and in patients with than in those without HCC (p<0.0001). The apoptotic rate was always less than the proliferative activity in HCC tissues and their ratio tended to decrease with higher tumour grade, size and stage and in p53-positive tumours (p<0.001). The markers of protein oxidation (but not XO activity) in HCC patients showed positive correlations with the proliferative activity and inverse correlations with the ratio between the apoptotic rate and the proliferative activity (p<0.05).
Conclusion: These findings suggest that enhanced protein oxidation and XO activity seems to play a role in the development and progression of HCV-related HCC with imbalance between rates of apoptosis and cytoproliferation. Better understanding of these processes might lead to the development of improved therapeutic approaches for the prevention and treatment of HCC.
WHICH SCORE FOR ALCOHOLIC HEPATITIS BEST PREDICTS MORTALITY?
P. Ellul1, K. M. Ashfaq2, R. Sekhar2, J. Keating2. 1Gastroenterology, New Cross Hospital, Wolverhampton, 2Gastroenterology, Furness General Hospital, Barrow-In-Furness, UK
Introduction: Alcoholic hepatitis (AH) is associated with a high mortality. With an alcohol-related mortality of 21.2 patients (UK −12.9) per year per 100 000 population, Barrow-in-Furness has one of the highest alcohol related mortality in the North West of England. There are various scores, which are used to risk stratify the patients. However, which score best predicts mortality?
Aims & Methods: Patients who died due to AH between January 2000 and December 2006 were identified. The modified Discriminant function (mDF), MELD score and the Glasgow AH score were retrospectively analysed. Data were obtained from the patients’ case notes. All patients had alcoholic liver disease and no other coexistent liver pathologies. The quoted 28-day mortality for patients with an mDF score >than 32 is 65%; MELD score >11 is 55%; Glasgow AH score >9 is 54%. Our aim was to assess which score best predicted mortality.
Results: We identified 62 patients and 51 were analysed. The others could not be analysed due to inadequate documentation. There were 37 male patients and 14 female patients. Mean age was 54 years (27–76 years). We calculated the scores by using the data on day 1 of admission. The scores were: 1. mDF >32; MELD>11; Glasgow score >9–25 patients; 2. mDF <32; MELD>11; Glasgow score <9–10 patients; 3. mDF >32; MELD>11; Glasgow score <9–14 patients; 4. mDF <32; MELD<11; Glasgow score <9–2 patients. The two patients with an mDF <32; MELD<11; Glasgow score <9 were admitted with alcoholic hepatitis but developed a gastrointestinal bleed (GI) and died from multiorgan failure after the GI bleed. From our results an mDF >32 was present in 39 patients who died (76.5%). The best predictor was the MELD score, as 49 patients (96%) with a score >11 died within 28 days. Only 25 patients (49%) with a Glasgow score >9 died within 28 days.
Conclusion: From our analysis the MELD score was the best predictor of 28-day mortality. An advantage of using the Glasgow AH score is that it is easy to calculate. However as information technology is easily accessible, it should be easy to calculate the MELD and mDF scores. Our limitation was that we could not calculate 3 month–1 year mortality. The obvious dilemma for the general clinician is which score to use for this common pathology with a high mortality. As if the above scores were not enough, recently the Lille prognostic model has been described. Its aim is the identification of patients at high risk of death at 6 months. Its accuracy should be higher than that of any of the other scores and is designed to predict survival in subjects with AH treated with corticosteroids. Above the ideal cut-off, the Lille model is able to predict 76% of the observed 6-month deaths. It suggests that it may be futile to treat patients for >7 days if the score is above the cut-off. What is definitely needed is more research on alternative treatments for patients with AH as this group of patients has a high mortality and a consensus for the best score is needed.
ALCOHOL-RELATED MORTALITY, SOCIOECONOMIC DEPRIVATION AND URBANICITY IN ENGLAND AND WALES
S. E. Erskine1, D. Gleeson2, R. Maheswaran1. 1School of Health and Related Research, University of Sheffield, 2Liver Unit, Sheffield Teaching Hospitals, Sheffield, UK
Introduction: Alcohol-related mortality is a serious problem in England and Wales. Alcohol-related mortality rates are increasing faster than in many other European countries. Such deaths are potentially preventable through education and regulation. It is important to identify groups of individuals who are most at risk of dying from alcohol-related disease to ensure that health interventions are effectively targeted.
Aims & Methods: Geographical ward level mortality data based on electoral wards for England and Wales from 1999 to 2003 were used to explore the association between alcohol-related mortality and socioeconomic deprivation by age and sex. The Carstairs index was used as an area based measure of deprivation. It is a standardised combination of four 2001 Census variables at ward level (male unemployment, overcrowding, residents in Social Class IV or V, no car access). Differences between urban and rural areas were also investigated. The Office for National Statistics definition of alcohol-related mortality was used. Deaths from liver cirrhosis accounted for 85% of the deaths. Other causes of death included in the definition were alcoholic gastritis, alcohol-induced chronic pancreatitis, alcohol poisoning, alcoholic neuropathies and alcoholic cardiomyopathy.
Results: People living in wards experiencing greater levels of deprivation had higher risks of dying from an alcohol-related cause. The rate ratios of mortality rates adjusted for age and urban-rural status for the most compared with the least deprived quintile of the population were 3.39 (95% CI 3.10 to 3.71) for males and 2.36 (2.16 to 2.57) for females. Rate ratios by age are as follows: 15–24 years: males: 1.45 (0.65 to 3.27) females: too few deaths to calculate; 25–44 years: males: 4.73 (4.00 to 5.59) females: 4.24 (3.50 to 5.13); 45–64 years: males: 4.18 (3.76 to 4.65) females: 2.67 (2.40 to 2.96); 65–79 years: males: 2.01 (1.75 to 2.32) females: 1.49 (1.29 to 1.71); 80+ years: males: 0.97 (0.75 to 1.26) females: 1.13 (0.86 to 1.48). The association peaked in the 25–44 years age category. People living in more urban areas experienced higher alcohol-related mortality rates. The rate ratios of mortality rates adjusted for age for urban relative to rural wards were 2.37 (2.05 to 2.75) for males and 1.68 (1.49 to 1.88) for females. After additional adjustment for deprivation, differences in mortality were attenuated but remained, with rate ratios of 1.35 (1.20 to 1.52) and 1.12 (1.01 to 1.25) for males and females respectively.
Conclusion: Alcohol-related mortality rates were found to be higher in more deprived areas and urban areas. The differences between the most and least deprived quintiles of the population were greatest between ages 25 and 44 years. Deprivation and urbanicity should be considered when designing alcohol-related health policies.
USING THE NEW AASLD-RECOMMENDED ALT RANGE INCREASES THE WORKLOAD FOR CHRONIC HEPATITIS B PATIENTS IN A CITY WITH A LARGE ETHNIC MINORITY POPULATION IN THE UK
N. Bholah, A. C. Ford, S. M. Moreea. Digestive Disease Centre, Bradford Royal Infirmary, Bradford, UK
Introduction: Bradford is a city with approximately 87 000 people from South Asia, in whom the prevalence of hepatitis B (HBV) is estimated at between 3 and 4%. In the latest AASLD guidelines1 the upper limits of normal for ALT at which to consider liver biopsy and treatment have been decreased from 40 IU/ml to 30 IU/ml for men, and from 40 IU/ml to 19 IU/ml for women. Treatment of HBV is based on eAg status, an ALT >1–2× the upper limit of normal (ULN), HBV viral load, and the degree of inflammation and/or fibrosis on liver biopsy.
Aims & Methods: We have prospectively collected data on all cases of HBV in Bradford between 2005 and 2007. Our database was analysed to obtain information concerning patient demographics, fluctuations in ALT and HBV viral load. The newly recommended ALT range and most recent viral load measurements were used to estimate any potential increase in the number of patients who would require a liver biopsy and possible treatment for their chronic HBV if the new AASLD guidelines were applied in our population. Patients were grouped according to HBe antigen (Ag) status and viral load.
Results: After excluding those individuals currently receiving anti-HBV therapy, and those with incomplete data, there were 147 patients available for analysis. There were 55 (37%) males with a mean age of 39 years (range 21 to 77.5), 35 (64%) of whom were Asian, and 92 (63%) females with a mean age of 34 years (range 17 to 83), 73 (79%) of whom were Asian. The results of our analyses are shown in the table.
Conclusion: Despite the fact that our current database does not reflect the expected prevalence of HBV in the large South Asian population in Bradford, adhering to the AASLD guidelines would significantly increase our workload, in terms of obtaining and interpreting liver histology, and treating patients with chronic hepatitis B infection. The majority of this increase in workload would be due to the alteration in the ULN of ALT in women. This must be taken into account for service development and provision.
WHEN CORTICOSTEROIDS DON’T WORK: RESCUE TREATMENT WITH PENTOXIFYLLINE FOR ALCOHOLIC HEPATITIS
E. Watson, H. Lafferty, E. H. Forrest. Gastroenterology, Glasgow Royal Infirmary, Glasgow, UK
Introduction: Corticosteroid (CS) treatment for alcoholic hepatitis (AH) remains controversial. Recent data have indicated that CS treatment can improve survival amongst patients with a Glasgow Alcoholic Hepatitis Score (GAHS) greater than or equal to 9 and a Discriminant Function (DF) greater than or equal to 32. However some patients do not appear to respond to CS, and these patients have a particularly poor outcome. Pentoxifylline (PTX) has also been suggested as a treatment of AH.
Aims & Methods: The aim of this study was to assess the effect of “rescue” PTX therapy in patients in whom CS was ineffective or had to be stopped. We retrospectively identified those patients with AH treated with CS who did not respond to such treatment, or in whom CS treatment (prednisolone 40 mg) was discontinued on account of contra-indications. Non-response was defined as a failure of serum bilirubin to fall by 25% from baseline after 7 days of CS treatment. Survival to 84 days was recorded relative to the use of rescue treatment with PTX (400 mg tds for 4 weeks).
Results: Thirty eight patients were identified: 34 were CS non-responders, 4 had CS therapy discontinued after developing sepsis. All patients had a GAHS greater than or equal to 9 and a DF greater than or equal to 32 at the start of treatment. Twenty one patients received PTX as treatment; 3 in addition to continued CS treatment, the remainder as alternative treatment. Six of the PTX-untreated patients discontinued CS treatment, the remainder continued for 4 weeks. The 28-day survival for PTX treated and PTX-untreated patients was 52% and 76% respectively (p = 0.24). The 84-day survival for PTX and PTX-untreated patients was 38% and 44% respectively (p = 0.97). There was no survival difference on Kaplan-Meier analysis (HR 0.655; 95% CI 0.28 to 1.52; p = 0.32). Multiple logistic regression analysis failed to identify PTX therapy, the discontinuation of CS treatment, or the 7-day change in bilirubin as independent predictors of outcome.
Conclusion: Rescue treatment with PTX had no survival advantage for patients with AH who did not respond to CS, or in whom such treatment had to be discontinued. The management of these patients remains difficult and new therapeutic approaches need to be explored.
HEPATITIS B: A SINGLE CENTRE STUDY OF PRACTICE
M. R. Foxton1, W. Tong2, S. Palmer2, J. Oben1, M. L. Wilkinson1, T. Wong1. 1Gastroenterology, 2Virology, St Thomas’ Hospital, London, UK
Introduction: The management of chronic hepatitis B (HBV) infection has undergone major changes recently, particularly with the greater accessibility to HBV DNA testing and an increasing number of therapies. Moreover, the Health Protection Agency (HPA) has issued standards regarding the follow-up of HBV infection. We wished to assess the practice of the management of HBV infection within our trust, which covers a population of 400 000 of whom 33% are from ethnic minorities, prior to the release of these guidelines.
Aims & Methods: All patients with a positive HBsAg test in the calendar year 2005 were identified along with the referring source and whether the patients were under follow-up by a team with expertise in the management of chronic HBV infection. All patients under the care of the gastroenterology department from June 2002 to June 2006 were identified from outpatient clinic letters. Data were collected for each patient including demographic, biochemical, virological, radiological, histological and therapeutic parameters.
Results: There were 21 683 hepatitis B surface antigen tests performed in 2005. Of these 938 (4.33%) were positive in 671 patients. In 167/671 (24.9%)patients, the test was ordered by gastroenterology or HIV/GU medicine teams. 356 tests (53%) were ordered from primary care. 65.4% of patients with a positive HBsAg test were not under the care of gastroenterology or GU/HIV medicine. 243 patients were seen in the out-patient gastroenterology clinic for further management with a median follow up of 464 days (IQR 154–922 days).The median number of appointments per patient was 5 (IQR 3–8). The median age was 35 years and the majority of patients were of Sub-Saharan Africa (44%) or Oriental (19%) origin. Fifty four patients were lost to follow-up and 11 patients died at a median 172 days after being first seen. There were 27 biopsies performed with 11 having significant fibrosis. Fifty five patients had abnormal ultrasound scans, 20 of which generated 33 CT scans. There were 6 cases of hepatocellular carcinoma. 27/35 eAg positive patients had abnormal ALT and 20/35 had HBV >5log IU/ml. 70/151 eAg negative patients had elevated ALT with 13 patients having an HBV DNA >5log. 42 patients were on anti-viral therapy. 38 patients were initiated on monotherapy. 4 patients were on dual therapy after monotherapy at a range of 15–26 months.
Conclusion: HBsAg testing is commonly performed but a significant proportion of positive tests are not referred to secondary care. Patients with chronic HBV require ongoing follow up, since a proportion will have advanced fibrosis. However, if all patients with positive HBsAg were referred to secondary care, as per HPA guidelines, there would be a considerable increase in resource utilisation in terms of biochemical, virological and radiological investigations.
INSULIN RESISTANCE PREDICTS RAPID VIROLOGICAL RESPONSE IN PATIENTS WITH GENOTYPE 1 CHRONIC HEPATITIS C TREATED WITH PEGINTERFERON AND RIBAVIRIN
A. Grasso1, F. Malfatti1, H. Martines1, P. De leo2, F. Toscanini2, A. De Ferrari3, E. Venturino4, M. Anselmo2, G. Menardo5. 1Internal Medicine and Gastroenterology Unit, 2Infectious Disease Unit, 3Immunohematology and Transfusion Medicine Unit, 4Pathology Unit, 5Internal Medicine and Gastroenterology Unit, San Paolo Hospital, Savona, Italy
Introduction: Several baseline factors have been identified as predictors of response to treatment in patients with chronic hepatitis C. Of these, genotype and on-treatment viral dynamics at week 4 and 12 are the most important. Aim of the study was to evaluate both the predictive capacity and the influence grade of pre-treatment variables on viral dynamics in patients with genotype 1 chronic hepatitis C (G1CHC) treated with peginterferon and ribavirin.
Aims & Methods: Sixty two patients (33 male, median age 46 years, range 30–67) with G1CHC consecutively treated with peginterferon alpha and ribavirin in our Department, were included. Determination of viral load was made (Cobas Amplicor 2.0, Roche) at baseline, week 4, week 12 and six months after therapy had finished. We defined rapid virological response (RVR) as undetectable plasma viral load at week 4, “complete” early virological response (cEVR) as undetectable plasma viral load at week 12 and “partial” early virological response (pEVR) as at least 2 logs reduction of viral load from baseline at week 12. In 52 patients viral load was also determined at week 1. Insulin resistance index (HOMA = insulin (mUI/l) × glucose (mmol/l)/22.5), body mass index (BMI), steatosis at histology (<5%/>5%), fibrosis (F0-F4; Scheuer) were also assessed. Univariate and multivariate analysis were carried out by means of a statistical software. Statistical significance was defined as an alpha error <0.05.
Results: Twenty nine patients (47%) experienced sustained viral response (SVR). All 21 RVR (100%), 6 of 11 cEVR (55%) and 2 of 6 (33%) pEVR had SVR. At multivariate analysis RVR was independently associated with HOMA (OR 0.22; 95% CI 0.06 to 0.81; p = 0.022) whereas cEVR was independently associated with steatosis (OR 0.045; 95% CI 0.002 to 0.92; p = 0.044). HOMA (<2 vs >2), steatosis (<5% vs >5%) and fibrosis (<2 vs >2) but not BMI (<25 vs >25) were able to influence viral dynamic assessed as decline of viral load (logs) from baseline to week 1 (HOMA p = 0.018; steatosis p<0.000; fibrosis p<0.000; BMI p = 0.74), decline of log HCV-RNA from baseline to week 4 (HOMA p = 0.008; steatosis p<0.000; fibrosis p = 0.001; BMI p = 0.75) and decline of log HCV-RNA from baseline to week 12 (HOMA p = 0.011; steatosis p<0.000; fibrosis p = 0.004; BMI p = 0.59).
Conclusion: HOMA is the only pre treatment predictor of RVR in patients with genotype 1 chronic hepatitis C candidates to antiviral treatment. The presence of insulin resistance, steatosis and fibrosis negatively influence early on-treatment viral dynamics during antiviral treatment.
CANCER IN AUTOIMMUNE HEPATITIS
B. S. Höeroldt1, N. Farquharson2, K. Shepherd2, E. McFarlane2, P. Silcocks3, D. Gleeson2. 1Gastroenterology, Rotherham General Hospital, Rotherham, 2Hepatology, Royal Hallamshire Hospital, 3Medical Advisor, Trent Cancer Registry, Sheffield, UK
Introduction: Autoimmune hepatitis (AIH) is an autoimmune liver disease, which may lead to cirrhosis and is often treated with long-term Azathioprine. Autoimmune diseases have been associated with lymphoproliferative cancers. In rheumatoid arthritis and following renal transplantation Azathioprine treatment has been associated with in increased risk of cancer. AIH has been associated with a low risk of hepatocellular carcinoma but a possibly increased rate of extrahepatic cancer; however published data are inconclusive.
Aims & Methods: To assess if cancer rates in a large cohort of patients with AIH are higher than those expected for the general population. Patients: 223 patients (186 female, mean age at diagnosis 57 years, mean follow-up 9.75 years) with definite (n = 147) or probable (n = 75) AIH by International AIH Group criteria presenting between 1971–2005. Patients with HCV-AB or HBsAg were excluded. Data were extracted from clinical records regarding site and time of diagnosis of first cancer after diagnosis of AIH. Cancer rates in AIH patients were compared with age- and gender-adjusted rates for the general population, using the Trent Region Cancer Registry. Follow-up was censored at diagnosis of cancer (n = 36), death (24 liver related, 19 non-liver, non-cancer), liver transplantation (9 patients), cessation of follow-up (9 patients) or at 31.12.2005. Cancers in 10 patients prior to the diagnosis of AIH were not included.
Results: 36 patients with AIH developed cancer: 5 HCC (all cirrhotic and female, mean age 73.3 yrs) and 31 other cancers including 7 GI tract, 6 breast, 4 lung, 3 GU tract and 3 maxillo-facial. Whether Azathioprine exposure was classified as (a) ⩽28/7 and >28/7 or (b) as no exposure and any Azathioprine exposure the relative risk was consistent to with up to a double risk of all malignancies (except non-melanoma skin cancer) but equally well with a halving respective relative risk; (a) RR 0.70 (95% CI 0.305 to 1.609) and (b) RR 1.00 (95% CI 0.458 to 2.148). By Cox multivariate analysis development of cancer in AIH was significantly associated with age at AIH diagnosis (p = 0.013) but not with duration of prior Azathioprine therapy.
Conclusion: The overall risk of cancer in AIH is slightly increased, but that for extrahepatic cancer not significantly so, relative to the local reference population. Cancer risk is unrelated to duration of Azathioprine treatment. These data do not suggest a substantially increased cancer risk in patients with AIH treated with Azathioprine. The risk of hepatocellular cancer is higher than in some previous reports.
PRIMARY SCLEROSING CHOLANGITIS IN PATIENTS WITH A DIAGNOSIS OF AUTOIMMUNE HEPATITIS
M. Hunter1, M. Loughrey2, M. Gray2, P. Ellis3, N. McDougall1, M. Callander1. 1Liver Unit, 2Pathology Department, 3Radiology Department, Royal Victoria Hospital, Belfast, UK
Introduction: Overlap syndromes between the autoimmune liver diseases (autoimmune hepatitis (AIH), primary sclerosing cholangitis (PSC), and primary biliary cirrhosis (PBC)) are well recognised although their frequency is not well established. We have reviewed our cohort of patients with AIH to determine how frequently a diagnosis of PSC was subsequently made and whether this might have been predicted
Aims & Methods: We reviewed clinical and laboratory data on all patients in whom a diagnosis of AIH was made at our Clinic from January 1979 to January 2007 (n = 118). We identified those in whom a subsequent diagnosis of PSC had been made. Those patients attending the Clinic whose liver function tests (LFTs) had an elevated alkaline phosphatase (ALP) or gamma glutamyl transpeptidase (GGT) (n = 16) underwent magnetic resonance cholangiogram (MRC). The features of this “cholestatic” group were compared with a randomly selected group of 25 patients who did not have cholestatic LFTs.
Results: Eight patients already had an additional diagnosis of PSC which was made one to 22 years from initial presentation. They were more commonly male (not statistically significant (NS)), younger (p<0.05), more often had ulcerative colitis (UC) (NS), had lower AST (p<0.05), and higher ALP (NS) at presentation than the controls. Four of the 16 patients with cholestatic LFTs had an MRC which showed PSC (table). These 16 tended to have lower AST at presentation than the control group (NS) but there were no other differences. The International Autoimmune Hepatitis Group (IAHG) scores (for autoimmune hepatitis) were calculated retrospectively. There were no significant differences between the groups.
Conclusion: At least 12 (10%) of 118 patients with an initial diagnosis of AIH subsequently developed evidence of PSC. IAHG scores at presentation did not predict those who would develop PSC. AIH patients who show cholestatic LFTs during follow-up should have MRC performed.
DIABETES AND ARTHROPATHY AS SURROGATE MARKERS OF IRON OVERLOAD AND LIVER FIBROSIS IN GENETIC HAEMOCHROMATOSIS
H. G. Jarvis, K. Hird, S. F. Stewart. Liver Unit, Freeman Hospital, Newcastle upon Tyne, UK
Introduction: Diabetes and arthropathy are classical features of haemochromatosis but debate exists over their association with the disease and the role of iron in their pathogenesis. It is also not clear whether these features are more prevalent in more advanced disease and if they could be useful in determining which patients to biopsy and which should undergo surveillance for the complications of cirrhosis.
Aims & Methods: We aimed to determine whether diabetes and arthropathy at diagnosis related to the degree of iron overload and liver fibrosis in a regional cohort of patients with genetic haemochromatosis. Case notes on 108 C282Y homozygotes or C282Y/H63D compound heterozygotes were analysed and data collected on ferritin at diagnosis, venesections and liver biopsy results. Univariate relationships between categorical variables were analysed by the χ2 test and differences in means by the Student’s t test.
Results: 17/108 (16%) were found to be diabetic at diagnosis. Diabetic patients had higher ferritins (3100.2±1571.9 vs 1673.4±328; p = 0.008) and required more venesections (39.23±20.2 vs 20.74±4.4; p = 0.008) to de-iron than non-diabetic patients. Although there was a trend towards more fibrosis this was not significant. 43/108 (40%) had arthropathy at diagnosis. Patients with arthropathy required more venesections to de-iron (29.43±10.2 vs 19.24±4; p = 0.04) but did not have statistically higher ferritins. There was a strong correlation between the presence of arthropathy at diagnosis and advanced fibrosis on liver biopsy (p = 0.03).
Conclusion: Diabetes in haemochromatosis relates to the degree of iron overload but does not help to determine which patients have advanced fibrosis. In contrast, patients with arthropathy do not have higher ferritins but are more likely to have advanced fibrosis. It may be reasonable to consider arthropathy as one of the factors influencing the decision to perform liver biopsy in these patients.
THE ROLE OF HEV TESTING IN DRUG INDUCED LIVER INJURY
M. Joseph1, H. R. Dalton1, H. Fellows1, W. Stableforth2, P. S. Thurairajah3, U. Warshow3, S. Hazeldine4, R. Remnarace5, S. Ijaz6, S. H. Hussaini1, R. P. Bendall7. 1Cornwall Gastrointestinal Unit, Royal Cornwall Hospital, Truro, UK, 2The New Zealand Liver Transplant Unit, Auckland City Hospital, Auckland, New Zealand, 3Gastroenterology, Derriford Hospital, Plymouth, 4Gastroenterology, Royal Devon and Exeter Hospital, Exeter, 5Gastroenterology, Torbay General Hospital, Torbay, 6Virus Reference Department, Centre for Infections, Health Protection Agency, London, 7Microbiology, Royal Cornwall Hospital, Truro, UK
Introduction: An accurate diagnosis of drug-induced liver injury (DILI) involves the application of the standard criteria for drug-induced liver injury.1 These criteria are based on a temporal relationship between the drug therapy and biochemical evidence of liver injury and the exclusion of alternative diagnoses. We have previously shown that locally acquired hepatitis E is an emerging infection in developed countries, is much more common than previously recognised, has a predilection for elderly males and can be misdiagnosed as DILI.2
Aims & Methods: To study the role of HEV testing in DILI. Retrospective review of a cohort of patients with suspected DILI (n = 69). The standard criteria for DILI were applied to this group. Patients with suspected DILI who met these criteria were retrospectively tested for HEV on stored sera taken at the time of presentation. Patients with confirmed DILI (HEV negative) were compared to a group of patients with locally acquired hepatitis E (n = 45) to determine variables that predicted either diagnosis.
Results: 47/69 had criterion-referenced DILI. 22/47 were HEV negative and thus had confirmed DILI. 6/47 were HEV positive and thus did not have DILI, but had hepatitis E infection. Compared to patients with confirmed DILI, patients with hepatitis E were significantly more likely to be male (OR 3.09, CI 1.05 to 9.08); less likely to present in November and December (0.03, CI 0.01 to 0.52); have lower serum bilirubin (p = 0.015); and higher serum alanine aminotransferase (p<0.001) and ALT/ALKP ratio (p<0.001).
Conclusion: The diagnosis of DILI is not secure without testing for HEV, particularly in elderly male patients with a predominant transaminitis.
ABNORMAL LIVER FUNCTION TESTS IN PATIENTS WITH TYPE 1 DIABETES MELLITUS: SEROPREVALENCE AND CLINICAL CORRELATIONS
J. S. Leeds1, E. M. Forman1, S. Tesfaye2, D. S. Sanders1. 1Gastroenterology, 2Diabetes, Royal Hallamshire Hospital, Sheffield, UK
Introduction: Abnormal liver function is well recognised in Type 2 diabetes mellitus and is associated with non-alcoholic fatty liver disease (NAFLD). There are no large studies examining the prevalence of abnormal liver function and its correlations in patients with Type 1 diabetes mellitus. The aim of this study was to determine the prevalence of abnormal liver function tests (particularly ALT) in a large cohort of patients with Type 1 diabetes and examine the clinical correlations and possible causes.
Aims & Methods: Patients were recruited from the Diabetes centre. Height and weight were measured and body mass index (BMI) calculated. Detailed drug history and other medical comorbidities were noted. Blood was taken for HbA1c, bilirubin, ALT, alkaline phosphatase, albumin and renal function.
Results: 614 patients were included in the study mean age 43.3 years (283 females). The prevalence of abnormal LFTs were bilirubin 29/614 (4.7%), ALT 13/614 (2.1%), ALP 43/614 (7.0%) and albumin 43/614 (7.0%). Males had higher ALT than females (p<0.001) but comparable age and HbA1c. There was no relationship between ALT and age group or BMI on univariate analysis but a significant correlation between ALT and male sex (p = 0.001), increasing HbA1c (p = 0.001) and creatinine (p = 0.006). Multivariate analysis using backwards stepwise logistic regression showed that ALT was significantly associated with creatinine (p = 0.027), male sex (p = 0.006) and HbA1c (p<0.001). Investigation of these patients revealed fatty liver on ultrasound scan in 5 patients (38.5%) and 1 patient admitted to alcohol excess. No biopsies were performed.
Conclusion: Abnormal liver function tests were common in Type 1 diabetes mellitus. Abnormal ALT appears to be associated with worse glycaemic control, male sex and higher creatinine levels. Age and BMI were not related to ALT in this cohort, however in those with raised ALT fatty liver was common.
THE SYSTEMIC INFLAMMATORY RESPONSE TO ACUTE LIVER FAILURE PREDICTS THE DEVELOPMENT OF RENAL FAILURE
J. A. Leithead, J. W. Ferguson, C. M. Bates, J. Davidson, A. J. Bathgate, P. C. Hayes, K. J. Simpson. Scottish Liver Transplant Unit, Royal Infirmary of Edinburgh, Edinburgh, UK
Introduction: Renal dysfunction is a common complication of acute liver failure. The current hypothesis is that the pathophysiological mechanisms are similar to those of hepatorenal syndrome in cirrhosis. However, we hypothesise that the systemic inflammatory response to acute liver failure plays a key role.
Aims & Methods: Our aim was to identify predictive factors for the development of renal failure in acute liver failure and, in particular, to assess the relationship with the systemic inflammatory response. A single-centre study of 454 patients admitted with acute liver failure between 01/92 and 06/07. Renal failure was defined as the need for renal replacement therapy (RRT). The 4 systemic inflammatory response syndrome (SIRS) components are temperature <36or>38°C, heart rate >90 bpm, WCC<4or>12×109/l, and PaCO2 <4.3 kPa.
Results: Mean age at time of presentation was 39.2+/−14.4 years (M:F = 1:1.3). The most common causes of liver injury were paracetamol (70%), viral (11.9%), idiosyncratic drug reactions (6.4%). 236 patients (52%) developed renal failure. The estimated 28-day survival for patients who did and did not develop renal failure was 15% and 58% respectively (p<0.001). The renal failure patients had a faster heart rate (p<0.001) and higher neutrophil count (p<0.001) at the time of hospital admission and were more likely to have a temperature <36or>38°C (p = 0.004). 41% of patients with renal failure had ⩾3 components of SIRS and only 20% of the non renal failure group (p<0.001). An increasing number of components of SIRS was associated with an increased probability of renal failure; 33%, 46%, 52%, 68% and 70% of the patients with 0, 1, 2, 3 and 4 components respectively required RRT (p = 0.004). The renal failure group were more likely to demonstrate infection (p = 0.001). Nevertheless, in both those with (p = 0.017) and those without infection (p = 0.002) the number of components of SIRS on admission was associated with the need for renal support. On multivariate analysis the factors associated with renal failure were fulfilled King’s College Hospital poor prognostic criteria (OR 4.84; 95% CI 2.62 to 8.93, p<0.001), paracetamol as the cause of liver injury (OR 2.75; 95% CI 1.42 to 5.33, p = 0.003), infection (OR 3.18; 95% CI 1.70 to 5.93, p<0.001), hypotension (OR 5.12; 95% CI 2.84 to 9.24, p<0.001) and the number of SIRS components on admission (OR 1.41; 95% CI 1.06 to 1.87, p = 0.017). A patient with 4 components of SIRS was 2.6 times more likely than a patient with no SIRS components to require RRT.
Conclusion: The systemic inflammatory response to acute liver failure is a predictor of renal failure requiring RRT. This supports previous studies linking the systemic inflammatory response with encephalopathy and poor prognosis, and the need for future targeted therapeutic intervention.
ESTIMATED GLOMERULAR FILTRATION RATE IS A PREDICTOR OF DEATH ON THE WAITING LIST FOR LIVER TRANSPLANTATION
J. A. Leithead, J. W. Ferguson, P. C. Hayes. Scottish Liver Transplant Unit, Royal Infirmary of Edinburgh, Edinburgh, UK
Introduction: Serum creatinine is a component of the MELD score, which in the USA is used to prioritise patients on the liver transplant waiting list. However, creatinine is influenced by gender, age and race and, as a result, MELD may be less accurate in some subgroups. Estimated glomerular filtration rate (eGFR) calculated using the MDRD4 equation takes into account these variables and may be a more useful prognostic indicator.
Aims & Methods: Our aim was to compare eGFR and creatinine as predictors of prognosis in patients awaiting liver transplantation. A single centre study of 464 patients listed for liver transplantation between 11/92 and 06/07. Patients listed for HCC, acute liver failure or combined renal transplant were not included. Logistic regression was used to assess the association of variables with 6-month waiting list mortality. The accuracy of traditional MELD (regression coefficients altered for our model) and MELD with eGFR substituted for creatinine in predicting mortality were assessed by the area under the ROC curve.
Results: Mean age at the time of listing was 55.4+/−11.5 years (M:F = 1:1). The main indications for transplantation were PBC (29%), alcoholic liver disease (24%), sclerosing cholangitis (15%). 65 patients (14%) died prior to transplantation. Median time to transplant was 64 (range 1–499) days. Median eGFR of the entire cohort at listing was 69 (IQ range 56–82) ml/min/1.73m2 and median creatinine was 90 (IQ range 77–109) μmol/l. 31% of patients had an eGFR<60 ml/min/1.73 m2 and only 10% had a creat>133 μmol/l. Despite having a lower eGFR than men (median 66 vs 74, p<0.001) women had a lower creatinine (median 82 vs 98, p<0.001) and lower MELD score (median 16 vs 17, p = 0.028). LogeGFR (p = 0.002) and logecreat (p<0.001) were associated with 6-month waiting list mortality on univariate analysis. The presence of an eGFR<60 was predictive of death in both men (p = 0.021) and women (p = 0.003), while creat>133 was not predictive in either sex (men p = 0.088, women p = 0.615). In the entire cohort the relative risk of death by 6 months post transplant in patients with an eGFR<60 was 3.01 (95% CI 1.08 to 8.36, p = 0.035). This association was independent of MELD and logesodium. The area under the ROC curve for predicting 6-month waiting list mortality based on MELD in men was 0.770 (95% CI 0.651 to 0.889) and in women was 0.740 (95% CI 0.593 to 0.887). When MELD was recalculated with logeGFR substituted for logecreat the c-statistic remained unchanged (0.771; 95% CI 0.653 to 0.889) and increased (0.789; 95% CI 0.659 to 0.918) in males and females respectively.
Conclusion: An eGFR<60 ml/min/1.73 m2 is an independent predictor of 6-month liver transplant waiting list mortality. eGFR substituted for creatinine may improve the accuracy of MELD in predicting death.
ANG 1–7 FAILS TO POTENTIATE ACETYLCHOLINE VASODILATATION IN THE PRECONSTRICTED IN SITU PERFUSED CIRRHOTIC RAT LIVER
J. S. Lubel, C. Herath, Z. Jia, L. M. Burrell, P. W. Angus. Department of Medicine, University of Melbourne, Melbourne, Australia
Introduction: Angiotensin 1-7 (Ang-(1-7)) is a vasoactive peptide of the renin-angiotensin system with properties that oppose that of Angiotensin II. In-vitro experiments have shown that Ang-(1-7) potentiates acetylcholine induced dilatation of aorta segments form cirrhotic rats.1 The aim of this study was to determine whether Ang-(1-7) could significantly alter the vaso-responsiveness of the cirrhotic liver to acetylcholine.
Aims & Methods: Male Sprague Dawley rats underwent bile duct ligation for 4 weeks. In-situ perfusion of livers was performed using oxygenated Krebs-Henseleit solution supplemented with 1% bovine serum albumin and 0.1% dextrose delivered at a flow rate of 30 ml/min. Animals were than randomly assigned to vehicle or Ang-(1-7) group (n = 4 each group). Liver viability was assessed by hepatic oxygen extraction, macroscopic appearance and stability of portal pressure. Following stabilisation, livers were perfused with either vehicle or 10-5 mol/l Ang-(1-7) for 20 minutes. Preconstriction was achieved using 10-4 mol/l Methoxamine. Portal pressure was measured using a manometer equilibrated to atmospheric pressure and recorded following cumulative bolus doses of acetycholine (10-8 mol/l–10-4 mol/l).
Results: There was no significant difference in body weight, spleen or liver weight between the two groups. The baseline and maximal portal pressures following methoxamine were similar in both groups. The portal pressures dropped in both groups following the initial two doses of Acetylcholine (10-8 mol/l and 10-7 mol/l), however subsequent doses were associated with increases in portal pressure reflecting altered epithelial responsiveness to these higher doses of acetycholine. Importantly, there was no evidence of an Ang-(1-7) enhanced vasoresponsiveness to acetycholine in cirrhotic livers as has previously been demonstrated in aortas of cirrhotic animals.
Conclusion: Although Ang-(1-7) has antifibrotic activity in the liver there is no demonstrable vasodilatory effect in cirrhotic rat livers either at basal conditions2 or preconstricted with methoxamine. Hepatic endothelial dysfunction is the probable reason for failure of a significant vasodilatory response.
POINT PREVALENCE AND CHARACTERISTICS OF CHRONIC HEPATITIS B IN THE SCREENED POPULATION OF PREGNANT WOMEN IN A CITY WITH A HIGH ETHNIC MINORITY
S. Mahmood1, F. Younis1, J. Rehman1, S. Moreea1, G. Chudasama2, V. Beckett2. 1Gastroenterology, 2Obstetric and Gynaecology, Bradford Royal Infirmary, Bradford, UK
Introduction: Bradford has a South Asian population of 18.5% (2001 census), with an unknown hepatitis B (HBV) prevalence. The Pakistan National Consensus Conference on Guidelines for Hepatitis B and C, Karachi, 2003, described the prevalence of HBsAg at 2.5% in pregnant women, of which 17% were eAg +ve and 61% anti HBe +ve1. As all pregnant women are screened for HBV we surmised that this would approximate the current prevalence of HBV in our local population.
Aims & Methods: The aim was to determine the prevalence and characteristics of HBV in pregnant women in relation to ethnicity between June 2005–September 2006. The method used was a retrospective analysis of the HBV databases from the Obstetrics/Gynaecology and Hepatology departments to obtain the following: demographics, percentage of women with a positive HBsAg test as well as their eAg/biochemical/virological status. Their attendance to clinic and requirement for anti-HBV treatment was also studied.
Results: During the study period there were 4817 pregnancies–53% Asians, 42% white Caucasians, 3% Africans and 2% unknown. 99% accepted screening for HBV. 42 women (0.88%) were HBsAg positive—29 Asians (prevalence in Asians = 1.1%), 8 white Caucasians (prevalence 0.4%), 5 Africans (prevalence 3%). All 42 HBV positive women (8 eAg +ve, 34 eAg –ve (81%)) were referred to the hepatology clinic. 33 (79%) women attended clinic, their characteristics are as follows: 8 (24%) eAg +ve, 2 of whom were immunotolerant and 3 had ALT>40 IU/ml and viral load (VL) >20 000 IU/ml. There were 25 (76%) eAg -ve, only 4 had a VL >2000 IU/ml, 1 of whom had an ALT>40. 2/33 (4.8%) patients are on treatment with Lamivudine. 11/29 (38%) of the Asian HbSAg +ve patients were born in Pakistan.
Conclusion: This study suggests a lower prevalence of HBV in our Asian population presumably due to a mixture of first and second generation women and some of who may have been immunised against HBV. The prevalence of HBV in African women is high due to the fact that they are mostly a first generation population. The prevalence of HBV in the Caucasian population is low as expected. There is a high attrition rate to the hepatology clinic. This study gives an insight into the approximate prevalence and characteristics of HBV in the local population and may help other areas with a high ethnic minority plan HBV services.
BLOOD GLUCOSE AND GLYCOSYLATED HAEMOGLOBIN ARE INSENSITIVE DIAGNOSTIC INDICATORS OF GLUCOSE INTOLERANCE IN PATIENTS WITH CIRRHOSIS
K. J. Rhee1, K. A. Chandarana1, R. Ruparelia1, E. Woolman2, S. Kanagalingam1, M. Thomas2, M. Y. Morgan1. 1Centre for Hepatology, Department of Medicine, Royal Free Campus, Royal Free and University College Medical School, 2Department of Clinical Biochemistry, Royal Free Hospital, Royal Free Hampstead NHS Trust, London, UK
Introduction: The prevalence of impaired glucose tolerance and diabetes mellitus in patients with cirrhosis ranges from 43–80% and 10–29% respectively, although these data are based on relatively small series of patients.1 The presence of diabetes has a significantly negative effect on survival, particularly following orthotopic liver transplantation.2 Currently there are no guidelines for the diagnosis of impaired glucose metabolism in this patient population.
Aims & Methods: The aims of this study were to determine (1) the frequency of impaired glucose tolerance in patients with cirrhosis and (2) the sensitivity and specificity of random/fasting blood glucose concentrations and glycosylated haemoglobin (HbA1C) for the diagnosis of impaired glucose metabolism in this patient population. All patients with biopsy-proven cirrhosis attending a hepatology out-patient clinic over one three month period were recruited for the study; patients with diabetes mellitus were excluded. Fasting/random blood glucose and HbA1c levels were measured. An extended glucose tolerance test (GTT) was undertaken after consumption of a 75 g glucose load (394 ml original Lucozade); blood glucose concentrations were measured at baseline and at 30 minute intervals for 3 hours.
Results: The total population comprised 55 individuals; eight (15%) were known to have diabetes. The remaining 47 patients (28 women, 19 men; mean age 56 (range 39–80) years) were assessed per protocol. The majority of patients showed one or more abnormalities of glucose tolerance,3 viz: diabetes (10; 21%); impaired glucose tolerance (10; 21%); impaired fasting glucose (8; 17%; late hypoglycaemia (15; 32%). Only the minority (15; 32%) had normal glucose tolerance. Routinely used screening blood tests were not sufficiently sensitive for diagnostic purposes (table).
Conclusion: Patients with cirrhosis show significant abnormalities of glucose metabolism which can not be diagnosed reliably using conventional blood tests. These patients should undergo intermittent oral GTTs and a low threshold for treatment should be adopted.
SLOW-RELEASE CARBOHYDRATES: A RATIONAL, PATIENT-ACCEPTABLE APPROACH FOR THE NUTRITIONAL MANAGEMENT OF PATIENTS WITH CIRRHOSIS?
K. A. Chandarana1, S. J. Eaton2, M. Y. Morgan1. 1Centre for Hepatology, Department of Medicine, Royal Free Campus, Royal Free and University College Medical School, 2Unit of Paediatric Surgery, Institute of Child Health, Royal Free and University College Medical School, London, UK
Introduction: Patients with cirrhosis progress to a state of early, accelerated starvation even after short periods of fasting. The European Society for Parenteral and Enteral Nutrition (ESPEN) has, therefore, recommended that these individuals should consume small frequent meals throughout the day, together with a late-night snack.1 However, this frequent feeding requirement is disruptive and could result in the consumption of high fat, high carbohydrate snacks rather than a balanced redistribution of food portions. Therefore, other, more patient-acceptable approaches of modulating fuel use are required.
Aims & Methods: The aim of this study was to determine if use of corn-starch, a slow-release carbohydrate, might provide a more convenient and sustainable way of preventing early, accelerated starvation in patients with cirrhosis. Eight patients (6 men: 2 women; mean (range) age, 56 (46–64) years; mean BMI, 23.3 (17–27)) with biopsy-proven alcohol-related cirrhosis and normal random blood glucose and HbA1c levels were selected for study; none had consumed alcohol for at least 3 months. Seven healthy volunteers (all men; mean age 32 (21–57) years; mean BMI, 25.6 (21–31)), served as controls. Subjects were provided with 50 g of corn starch dissolved in 150 ml water to drink over 30 s. Blood glucose concentrations were measured immediately before, and at 30 min intervals for up to 7 h post corn starch ingestion. Corn starch use was assessed by measurement, at similarly timed intervals, of breath 13CO2 using isotopic ratio mass spectrometry.
Results: There were no significant differences between the patients and the healthy volunteers in the corn starch release pharmacokinetics. However, corn starch ingestion was associated with greater variability in blood glucose concentrations and in blood-glucose time profiles in the patients (table).
Conclusion: In patients with cirrhosis corn starch is used adequately but results in more sustained fluctuations in blood glucose levels than in healthy volunteers, even in the absence of obvious glucose intolerance. This may limit its usefulness, and that of other sustained release carbohydrates, as nutritional supplements in this patient population.
SYSTEMATIC REVIEW OF THE DIAGNOSTIC PERFORMANCE OF SERUM MARKERS OF LIVER FIBROSIS IN ALCOHOLIC LIVER DISEASE
J. Parkes1, I. Guha2, S. Harris1, W. M. C. Rosenberg3, P. J. Roderick1. 1Public Health Sciences and Medical Statistics, 2Department of Hepatology, University of Southampton, Southampton, 3Institute of Hepatology, University College London, London, UK
Introduction: Alcoholic liver disease (ALD) is an important consequence of hazardous drinking, and a significant cause of death and morbidity in many countries. Detection of liver fibrosis at an early stage could provide opportunities for more optimal management. Serum markers of liver fibrosis offer an attractive alternative to liver biopsy. Evidence of the diagnostic performance of such biomarkers of liver fibrosis in ALD is needed to assess the effectiveness of such tests. To provide such evidence, a systematic review of diagnostic studies of serum markers was conducted.
Aims & Methods: MEDLINE, EMBASE, and reference lists from retrieved articles were searched. Studies were included if they evaluated paired samples of liver biopsy and serum, included >30 participants, and presented data as sensitivity, specificity, or receiver operator characteristic curves.
Results: 12 studies were eligible for inclusion. There were 14 separate markers—5 evaluated as single markers and the rest as components of 6 panels of markers. Studies were heterogeneous, and were generally smaller and older than similar studies in other liver diseases. Serum markers were able to identify/exclude those people with severe fibrosis/cirrhosis with good diagnostic accuracy at the thresholds presented, performance was less good at detection of less severe levels. Both panels of markers and hyaluronic acid (the best single marker but in few studies) performed well to identify cirrhosis/severe fibrosis, although there was no consistency in threshold of HA reported by studies.
Conclusion: In ALD there are few small studies that have evaluated serum markers ability to identify fibrosis on biopsy. These showed that they are promising in the identification of cirrhosis/severe fibrosis. Due to the paucity of studies and lack of direct comparisons of single markers and panels it is not possible to recommend any one specifically. Markers have lower diagnostic accuracy at lesser stages of fibrosis where panels tended to perform better than single markers. More research needed into detecting early ALD.
HIGH FREQUENCY OF TISSUE TRANSGLUTAMINASE ANTIBODIES IN PATIENTS WITH ALCOHOLIC LIVER DISEASE
C. A. Salmon, J. S. Leeds, R. J. Atkinson, D. S. Sanders, D. C. Gleeson, M. A. Karajeh. Liver and Gastroenterology Unit, The Royal Hallamshire Hospital, Sheffield, UK
Introduction: It has been suggested that a link exists between chronic liver disease and coeliac disease. Earlier reports have shown high rates of false positive assays for antigliadin and tissue transglutaminase (tTG) antibodies in patients with chronic liver disease. Human anti tTG has been found to be more specific than guinea pig tTG, however there are few data specifically assessing the relationship between human tTG and severe alcoholic liver disease (ALD).
Aims & Methods: The aim was to assess the reliability of human tTG in patients with severe ALD. We also assessed for correlation between tTG and the severity of the liver disease as measured by albumin and bilirubin. We identified patients who had coeliac serology performed (for various clinical indications) from a database of patients with severe ALD defined as portal hypertension, previous decompensation or biopsy proven cirrhosis. Patients with inflammatory bowel disease (IBD) and irritable bowel syndrome (IBS) were age and sex matched to provide two control groups. All patients had coeliac serology with anti-tTG using human recombinant tTG linked gliadin specific peptides and IgA endomysial antibody (EmA). The patients with ALD also had bilirubin and albumin as a measure of their liver disease. Patients with positive tTG were offered duodenal biopsy.
Results: We identified 74 ALD patients (mean age 54.2 years, 47 males). These were age and sex matched to the same number of patients in the IBD and IBS groups. tTG was positive in 32/74 (43.2%) with ALD, 6/74 (8.1%) with IBD and 9/74 (12.2%) with IBS (p<0.0001). Median tTG (IQR) levels in those with ALD, IBD and IBS were 13 (17.25), 4 (6) and 3 (6) respectively (Kruskal-Wallis, p<0.0001). EmA was positive in 1/74 with ALD, 1/74 with IBD and 4/74 with IBS. Of the patients with a positive tTG, 27 of 33 (81.8%) ALD, 4 of 6 (66.7%) IBD and 8 of 9 (88.9%) IBS had duodenal biopsies. These revealed no cases of coeliac disease in the ALD group, whereas 2 patients in the IBD group and 4 patients in the IBS group had histological changes of coeliac disease. There was a positive correlation between tTG and bilirubin (Spearman’s rho 0.39, p = 0.001) and a negative correlation between tTG and albumin (Spearman’s rho, −0.38, p = 0.001).
Conclusion: In patients with severe ALD there is a high frequency of false positive tTG. This was not related to the presence of a positive EmA or coeliac disease on biopsy. This suggests that tTG in isolation is not a good screening tool for coeliac disease in patients with ALD. There does seem to be a correlation between the level of tTG and the severity of liver disease raising the possibility of an aetiopathological role which merits further exploration.
LONG-TERM FOLLOW-UP OF BONE MINERAL DENSITY FOLLOWING ORTHOTOPIC LIVER TRANSPLANTATION
D. A. Sheridan1, L. Smith1, R. M. Francis2, M. Hudson1. 1Liver and Transplant Unit, 2Musculosketetal Unit, Freeman Hospital, Newcastle upon Tyne, UK
Introduction: With increasing survival following orthotopic liver transplantation (OLT), data regarding the long-term impact on bone mineral density (BMD) are needed. We conducted an audit of 108 patients attending the liver transplant annual review clinic to determine assessment and treatment of reduced BMD up to 13 years following OLT.
Aims & Methods: A retrospective review of notes from the annual review clinic collected age at time of OLT, diagnosis, immunosuppression, body mass index and treatment with calcium/vitamin D3 and bisphosphonates. Results of total lumbar spine and total hip BMD by DEXA scanning at initial assessment and intervals up to 13 years following OLT were recorded. Comparison was made between those whose primary indication for OLT was cholestatic liver disease (PBC + PSC; n = 31) to those with hepatitic liver disease (alcoholic liver disease, hepatitis B/C and autoimmune hepatitis; n = 50). 27/108 patients had acute liver failure with no pre-transplant assessment of BMD.
Results: Overall those with cholestatic liver disease had significantly lower pre-transplant BMD of the total lumbar spine and total hip than the hepatitic group (p = 0.033). Steady recovery in bone density of the lumbar spine is then seen but a decline in bone density of the hip at 1 year post OLT in the cholestatic group. Subgroup analysis showed this decline to be attributable to those maintained on long-term steroids. There was no significant difference in long-term bone density between those on tacrolimus compared to cyclosporin A at the lumbar spine (0.977±0.191 and 0.972±0.158 g/cm2; p = 0.963) or at the hip (0.791±0.109 and 0.822±0.146 g/cm2; p = 0.649). Timing of DEXA scans post OLT and use of bone prophylaxis was variable.
Conclusion: Short-term fracture risk in patients coming to liver transplantation is greatest in the first year in those with cholestatic liver disease. Long-term fracture risk declines in the majority following liver transplantation as bone density of the lumbar spine recovers. However those on long-term steroids have a fall in total hip BMD which may increase long term hip fracture risk. This audit highlights that evidence based guidelines for the long-term assessment of bone density and bone prophylaxis following liver transplantation are needed and should be targeted to high risk individuals.
THE INFLUENCE OF CHRONIC HEPATITIS C INFECTION AND HOST APOLIPOPROTEIN E GENOTYPE ON SERUM LIPID PROFILES
D. A. Sheridan1, D. A. Price2, P. Donaldson1, G. Toms1, D. Neely3, M. Bassendine1. 1Liver Research Group, Medical School, 2Department of Medicine, 3Department of Clinical Biochemistry, Royal Victoria Infirmary, Newcastle upon Tyne, UK Kingdom
Introduction: Hepatitis C virus (HCV) utilises pathways of lipoprotein metabolism within the liver for viral replication and infectivity. Host ApoE genotype is a major determinant of serum LDL cholesterol levels and correlates with cardiovascular risk. ApoE genotype may influence outcome in acute HCV infection.1 It has also been suggested that LDL cholesterol level may influence response to anti viral therapy.2
Aims & Methods: In the present study we assessed the influence of HCV genotype and host ApoE genotype on serum total cholesterol, non HDL cholesterol, triglycerides and HDL in HCV infected patients. These parameters were compared in those achieving a sustained virological response (SVR) and non-responders. Paired pre and 24 weeks post treatment lipid profiles were retrospectively obtained in 100 patients who achieved a sustained virological response (SVR) and 66 non-responders (NR) to antiviral therapy. Each individual thereby acted as their own control for age, sex and BMI. ApoE genotype was compared in 72 SVRs and 57 non-responders and 288 healthy controls.
Results: Those with HCV genotype 3 had significantly lower pre treatment total cholesterol levels than HCV genotype 1 (3.97 mmol/l±0.14 and 4.63 mmol/l±0.12 respectively, p<0.001). This effect was reversible in the SVR group but persisted in the non responders post treatment. In both SVRs and non-responders, non-HDL cholesterol was also significantly lower in HCV genotype 3 (2.80 and 2.52 mmol/l) than genotype 1 (3.63 and 3.31 mmol/l; SVR and NR respectively; p<0.001). Triglyceride level significantly increased in those with HCV genotype 3 achieving a SVR but there was no difference in HDL between HCV genotypes, SVR’s or non responders. In the HCV infected patients, the Apo ∊2/∊3 genotype was found in only 3.5% of non-responders compared to 9.7% in SVR’s and 11.1% in a healthy control group. In those infected by HCV genotype 1, cholesterol levels correspond to expected levels for ApoE genotype. In contrast, in HCV genotype 3 infection, cholesterol levels were lower than expected in ∊3/∊3 and ∊3/∊4 genotypes.
Conclusion: The influence of host ApoE genotype should be considered in investigating the association of serum cholesterol levels and treatment outcome in HCV infection. We found that HCV genotype 3 lowers total and non-HDL cholesterol levels, and exerts a greater influence than HCV genotype 1 or host ApoE genotype.
BACTERIAL TRANSLOCATION AND INTESTINAL DYSFUNCTION IN CIRRHOSIS
U. Thalheimer1, F. De Iorio1, F. Capra1, M. Lleo2, V. Zuliani1, V. Ghidini2, M. Tafi2, G. Caburlotto2, M. Gennari2, I. Vantini1. 1Dipartimento di Scienze Biomediche e Chirurgiche, Policlinico GB Rossi, 2Dipartimento di Patologia, Sezione di Microbiologia, Universitá di Verona, Verona, Italy
Introduction: Bacterial infections are common in cirrhotic patients and seem to play an important role in the development of the complications of cirrhosis.1 Bacterial translocation seems to be the initial step preceding the occurrence of overt bacterial infection in the cirrhotic patient. The presence of bacterial DNA in blood and ascites has been reported to correlate well with the presence of bacterial translocation in rats. A recent study reported the presence of bacterial DNA in serum and ascites in patients with advanced cirrhosis without signs of infection.2
Aims & Methods: Our aim was to search for bacterial DNA in a range of cirrhotic patients both with and without ascites, and to study its correlation with any abnormality of intestinal motility or permeability and the presence of bacterial overgrowth. We studied 7 cirrhotic patients with or without ascites. Exclusion criteria were age less than 18 years, presence of the systemic inflammatory response syndrome (SIRS), overt infection or positive blood or ascitic fluid cultures, upper GI bleeding or antibiotics within the preceding 2 weeks, intestinal disorders including major abdominal surgery, use of any drug with an effect on small bowel motility such as beta blockers, lactulose or prokinetics, presence of HCC or portal vein thrombosis, acute alcoholic hepatitis, pregnancy and refusal of consent. Serum and ascites samples were obtained on day 1, and serum samples were taken twice daily for the following 3 days. Bacterial DNA was assayed by PCR using universal primers for rRNA 16s. Oro-caecal transit time and bacterial overgrowth were assessed with H2 breath testing. Intestinal permeability was assessed by determining urinary lactulose and mannitol excretion with HPLC.
Results: Six patients were male and 1 female, age range was 42–78 years, aetiology was alcohol in 4, HCV in 2, HBC in 1. Ascites was present in 4 and Child Pugh grade was A in 4 and B in 3. All patients had increased intestinal permeability, 6 had decreased transit time and 1 had bacterial overgrowth. In only one patient (with ascites), PCR was positive for bacterial DNA both in ascites and serum for all 4 days on which samples were taken.
Conclusion: Bacterial translocation as assessed by presence of bacterial DNA is less common in less severe cirrhosis and seems to be anticipated by changes in intestinal motility and permeability.
INCREASED MORTALITY AND LENGTH OF STAY RELATED TO ABNORMAL LIVER FUNCTION TESTS ON ADMISSION TO THE GENERAL INTENSIVE CARE UNIT: A 6 MONTH RETROSPECTIVE ANALYSIS
S. J. Thomson1, M. L. Cowan2, S. Musa3, P. Collinson4, M. Grounds5, T. M. Rahman3. 1Gastroenterology and Intensive Care, 2Gastroenterology, 3Gastroenterology and Intensive care, 4Chemical Pathology, 5Intensive Care, St George’s Hospital, London, UK
Introduction: Abnormalities of liver enzymes and albumin are common in the critically ill patient for a number of reasons. Liver function tests (LFT) are routinely analysed at the time of admission to the Intensive Care Unit (ICU) but the significance of abnormal results is not clear. We sought to define the incidence of abnormal LFT and effect on length of stay and 30 day mortality.
Aims & Methods: The results of LFT of patients undergoing first admission to the General ICU of a large teaching hospital in South London between 1 October 2006 and 31 March 2007 were obtained from Chemical Pathology. Mortality statistics were obtained from the hospital records.
Results: A total of 661 patients had a first admission to the ICU during the 6 months studied. The average age was 59.7 years (SD 18.1), 58% were male and the mean length of stay was 4.1 days (range 1–45). Mortality rate at 30 days was 22.2% (147/661). On the day of admission serum albumin was <35 g/dl in 614 patients (93%; median 22 g/dl). Excluding albumin, only 333 (50%) had entirely normal LFT. Average length of stay (LOS) was greater in those with an abnormal bilirubin, or albumin below 22 g/dl on admission. Abnormalities in each of ALT, AKP, GGT and Albumin below 22 g/dl on admission, were associated with greater 30 day mortality.
Conclusion: Abnormality of LFT is common in the critically ill patient admitted to the General ICU. Albumin is almost invariably below the normal range. Relatively minor elevations of liver enzymes are associated with increased LOS and 30 day mortality. Lower levels of albumin at the time of admission are likely to reflect chronic illness and therefore result in prolonged stay and mortality. The cause of these abnormalities is likely to be multifactorial and further prospective studies are needed to elucidate the cause.
REVIEW OF LIVER BIOPSIES IN A HEPATOLOGY CENTRE: HOW OFTEN AND WHY IS THE DIAGNOSIS CHANGED?
J. I. Wyatt. Histopathology Department, St James’s University Hospital, Leeds, UK
Introduction: 160 liver biopsies/year are sent to Leeds for review, at request of the local pathologist (PR, x/year) or because the patient is referred to Leeds and there are uncertainties about the original report (CR, y/year). To determine the proportion of medical biopsies where review had affected patient management, original and referral reports for 100 consecutive cases were reviewed.
Aims & Methods: Inclusion criteria: adult medical liver biopsies referred to Leeds were original pathology report was available for review. The original pathologist’s diagnosis was compared retrospectively with that in the centre histology report (JIW) which included a note of any CPC discussion. Original clinical information included in the referred report was noted, together with further information from correspondence and at CPC discussion. Cases were categorised as major change in diagnostic category (for example, chronic hepatitis to chronic biliary disease, possible on basis of original clinical information and histology slides alone), minor change in interpretation within category (for example, most likely aetiology, change in stage, second diagnosis, including information from CPC), or no change.
Results: Biopsy review and clinical discussion let to a major change in 21% and minor change in 27% diagnoses. Contributory factors included misleading clinical information (2) misinterpretation of special stains (2). Review most often resulted in a major change in chronic biliary disease (9/25), acute hepatitis (3/12), cholestases (2/6) and vascular outflow (2/5). Incorrect interpretation of the Shikata stain for copper associated protein contributed to 7/9 instances in chronic biliary disease. Minor changes were usually a result of insights from additional clinicopathological correlation, and showed less clustering in diagnostic categories. No more specific diagnoses was achieved in 8 cases originally reported as normal/non-specific.
Conclusion: Biopsy review led to revised diagnosis in 48% cases. A major diagnosis not recognised initially in 21%; 11/21 may have been avoided with correct clinical information and appreciation of special stains. A minor change in 27, more often due to specialist interpretation in the light of clinical pathological discussion. This audit has highlighted areas of liver histology CPD helpful to DGH pathologists.
AUDIT OF CHANGE IN NEEDLE BIOPSY GAUGE FOR ULTRASOUND GUIDED MEDICAL LIVER BIOPSIES: ROOM FOR FURTHER IMPROVEMENT
J. I. Wyatt, S. Karthik, D. Treanor. Histopathology Department St James’s University Hospital, Leeds, UK
Introduction: Histopathological diagnosis in hepatology depends on the features of diffuse liver disease being adequately represented in the biopsy specimen. Larger biopsies give more diagnostic information. Pragmatically biopsies with >6 portal tracts (PTs) are considered adequate1 although >10 portal tracts are necessary to avoid underscoring chronic hepatitis C.2 To reduce inadequate biopsies, we changed from 18 g to 16 g needles for routine ultrasound guided outpatient medical liver biopsies during summer 2006. This is a blinded retrospective audit of the size and diagnostic value of tissue sections obtained from liver biopsies during this transition period.
Aims & Methods: 40 consecutive patients biopsied during May–July 2006 and their needle gauge (18 g or 16 g) were identified from radiology records. Slides were retrieved and studied retrospectively, blinded to needle gauge. Objective analysis: Slides were scanned (imagescope) and the length, width and area of the best level were measured using virtual slide viewing software. Subjective analysis: Slides were reviewed by one pathologist (JIW) for: the number of PTs in the best level; assessment of biopsies as inadequate (no useful diagnosis possible), insufficient (for example, evidence of chronic biliary disease? ductopaenia; hepatitis C, insufficient for scoring), sufficient for full diagnosis.
Results: Two of 22 18 g cases were excluded because of multiple passes. 16 g needles (n = 18) produced significantly wider sections than 18 g needles (n = 20) (mean 0.96 and 0.85 mm respectively; p<0.037) but there was no difference in length (mean 11.16 vs 11.19 mm) or tissue area (mean .8.23 mm2 vs 7.86 mm2) Median PT counts were 9 (4–17) for 16 g and 7 (4–12)for 18 g (p = NS); on average there were 7.8PT/10 mm for 16 g biopsies and 5.5PT/10 mm for 18 g biopsies. Only one biopsy from each group was inadequate for any useful diagnosis. Biopsies assessed as sufficient for full diagnosis increased from 45% (18 g) to 67% (16 g) (p = 0.31).
Conclusion: Wider biopsy needles provide significantly wider specimens; these have more portal tracts, although the range is large and the difference did not reach significance. Subjectively, they are more often sufficient for full histological diagnosis. However with 16 g needle this is still only achieved in 67% biopsies, and a broader needle or second pass would be needed to improve the diagnostic value of medical liver biopsies further.
Nutrition posters
IGG ANTIBODIES TO FOODS ARE OF NO RELEVANCE TO IGE MEDIATED FOOD ALLERGY
I. Seerat1, N. M. Croft1, A. Hickey2, H. Longhurst2. 1Digestive Diseases Clinical Academic Unit, 2Immunopathology, Barts and the London, London, UK
Introduction: IgG food antibodies have been claimed to be important in both enhancement and suppression of IgE mediated food allergic reactions. They are often measured in commercial laboratories with little in the way of clinical evidence to justify this.
Aims & Methods: The aim of this study was to examine the serum concentrations of IgG antibodies to casein, egg and peanut in children with IgE mediated allergy to dairy, egg and peanut. Patients with food allergy and controls were recruited from the allergy and paediatric gastroenterology clinics. Controls were children having bloods taken in the paediatric gastroenterology clinic with no atopy or inflammatory bowel disease. Total serum IgE, and specific IgE and IgG antibodies to casein, egg and peanut using the Pharmacia Unicap system were measured. Medians were compared using the Mann-Whitney U test.
Results: A total of 94 children were recruited. 62 had food allergies requiring dietary avoidance (mean age 6 years), with raised RAST or SPT and/or acute onset within one hour of ingestion. 21 reacted to dairy products, 25 to egg and 27 allergic to peanut. There were 32 controls, with a median age of 11 years. As expected the allergic group had higher total IgE and RAST concentration to casein, egg and peanut than the controls. All three food antibody IgG levels were higher for the food allergy group as a whole than the controls (p<0.05). However in the food allergic patients there were no significant differences found in the food IgG to which they react (for example, casein IgG in dairy allergy) when compared to allergic children without that specific allergy.
Conclusion: Although food allergic children have higher levels of food specific IgG antibodies than controls, these data suggest that IgG food antibodies in serum are not related to the presence (or absence) of IgE mediated food allergic reactions. Any direct relevance to the pathogenic process remains unlikely.
MUSCLE CRAMPS ARE THE COMMONEST SIDE EFFECT OF HOME PARENTERAL NUTRITION
D. A. Elphick1, M. Baker2, J. P. Baxter3, J. Nightingale2, T. Bowling4, M. E. McAlindon1. 1Department of Gastroenterology, Royal Hallamshire Hospital, Sheffield, 2Nutrition Support Team, Leicester Royal Infirmary, Leicester, 3Nutrition Support Team, Ninewells Hospital, Dundee, 4Nutrition Unit, Queen’s Medical Centre, Nottingham, UK
Introduction: Quality of life is adversely affected by the need for home parenteral nutrition (HPN), partly because of complications of feed delivery. The major complications of catheter related sepsis, venous thrombosis and liver disease are well recognised but infrequent.
Aims & Methods: This study aimed to determine if there were other minor, but common complications that caused patient distress. All patients from four HPN centres were asked if they suffered any side effects of parenteral nutrition and whether these side effects related to the timings of the feed or required specific intervention.
Results: 45 patients (24 male, 21 female, median age 47 (23–75) years) were included in the study. The patients had been on HPN for median 2 (0.3–16) years, and administered feed on median 5 (2–7) days per week. Reported side effects from HPN were muscle cramps (n = 7), nausea (n = 3), headache (n = 2) hand/foot swelling (n = 1), palpitations (n = 1), weakness (n = 1), ache at Hickman line site (n = 1) and thirst (n = 1). Hot flushes/sweating were reported by four patients, but this is likely to be a physiological response due to thermogenesis. Of the seven patients reporting cramps as a side effect of their HPN, six had tried quinine and/or baclofen, and 2 had slowed the rate of administration of their feeds to reduce the symptoms. The underlying pathologies leading to HPN requirement in these 7 patients were Crohn’s disease (n = 2), refractory coeliac disease, sclerosing mesenteritis, small bowel intussusception, mesenteric ischaemia and intestinal dysmotility. When asked specifically whether they suffered muscle cramps in relation to their HPN, a further 5 patients (small bowel dysmotility (n = 4), mesenteric ischaemia (n = 1)) reported this to be the case; 3 of whom had tried baclofen or quinine to reduce symptoms but none had altered their feed administration. A further 11 patients suffered muscle cramps at times unrelated to parenteral nutrition administration. 22 did not suffer from muscle cramps. Serum electrolytes showed no consistent difference between those with cramps and those without.
Conclusion: Muscle cramps were the commonest minor side effect of HPN. Although not life-threatening, the cramps were of sufficient severity to warrant pharmacological intervention in 9 of 12 patients who had cramps in relation to feeds, and parenteral nutrition administration was slowed in 2 of the 12. Muscle cramps are therefore likely to affect the quality of life of these patients.
A NEW ERA IN ENTERAL NUTRITION PRACTICE?
S. Khair, S. Karanth, H. Lawrence, S. Galbraith, S. McClean, C. Hames, Q. Tuffnell, S. Cottee, J. Woodward. Gastroenterology and Clinical nutrition, Addenbrooke’s Hospital, Cambridge, UK
Introduction: Tube feeding into the stomach via nasogastric or percutaneous gastrostomy tubes revolutionised the practice of enteral alimentation in the latter half of the twentieth century. Paradoxically, greater use of gastrostomies resulted in higher mortality rates—with one month mortality rates as high as 20% reported by 2002. This study aimed to determine the effects on enteral nutrition practice of modern enteral feeding techniques and patient selection.
Aims & Methods: Retrospective review of records of all patients receiving gastrostomy tubes during the same period over the years 2000–1, 2003–4 and 2006–7 from one institution. Indications and outcomes were recorded. Nasal bridles were routinely placed from 2003 for patients who experienced frequent nasogastric tube displacement. A “feeding issues multidisciplinary team” (FIMDT) was established in 2006 to discuss all gastrostomy requests and other contentious nutrition issues.
Results: (1) Fewer gastrostomy tubes were placed in each time period—89 (2000), 80 (2003) and 69 (2006). (2) The proportion of gastrostomies placed for cerebrovascular disease declined—54 (61%), 30 (38%) and 9 (13%). (3) The proportion of gastrostomies placed for head and neck cancer increased—11 (12%), 8 (10%) and 26 (38%). (4) A dramatic reduction in 30-day mortality rates was observed: 15 (17%), 6 (8%) and 1 (1.4%). In 2000, 9/15 deaths within one month of gastrostomy insertion were in patients following stroke. (5) The use of nasal bridles to secure nasogastric tubes increased from 11 in 2003 to 63 in 2006. 22% of nasal bridles were used in stroke patients. Of 14 patients in 2006 requiring a bridled nasogastric tube, only one required a gastrostomy for long-term feeding.
Conclusion: The last five years have seen a remarkable change in the practice and outcome of enteral nutrition due to the improved delivery of nasogastric feeding and better patient selection for gastrostomy tube placement. In most reported series, stroke patients comprise the majority requiring gastrostomy placement. These patients are at high risk of dying within one month of the procedure. Careful selection of patients by discussion at the FIMDT and the use of nasal bridle fixation has resulted in a reduction of gastrostomy placements in these patients with resultant improvement in overall outcome.
ARE WE RECOGNISING AND APPROPRIATELY TREATING MALNUTRITION AMONG HOSPITAL IN-PATIENTS?
C. Lamb, J. Parr, M. Warren. Gastroenterology, North Tyneside General Hospital, Tyne and Wear, UK
Introduction: The UK National Institute for Health and Clinical Excellence (NICE) released guidance on “Nutrition support in adults” in February 2006, recommending that all in-patients be screened for malnutrition on admission to hospital. Appropriate and immediate referral to nutrition and dietetic services should then be undertaken.
Aims & Methods: The study was carried out on a single day in 2007 and based in a hospital serving a population of 350 000 in North East England. A screening tool was in use within the hospital. Local policy dictates its use on all patients at admission and referral to nutrition and dietetics services of those identified as suffering from malnutrition. Compliance with this policy was measured by prospective audit of both the screening tool use and whether those identified as malnourished were referred for nutritional support. Patients provided with nutritional support—for example, food supplements without appropriate referral were also recorded. The tool was then applied to all those not assessed on admission to accurately measure malnutrition on the day of study. All adult patients admitted for more than 24 h were included.
Results: All 328 (100%) patients meeting inclusion criteria were assessed (185 female, 143 male, mean age 71.1 years). Median length of admission was 8 days. In 226 (68.9%) cases, the screening tool had been completed and 74 patients (22.6%) were malnourished. Only 26 of these patients (35.1% of total identified) were appropriately referred to dietetic services. No action was taken in 37 (50%) patients identified as malnourished. 11 patients (14.9%) received dietary intervention without formal dietetic referral. Assessment of the remaining 102 “unscreened” patients revealed a prevalence of malnutrition across the whole cohort of 31.1% (102/328) thus 27.5% (28/102) of malnourished patients had gone unrecognised and untreated.
Conclusion: Using a “NICE-compliant” malnutrition screening tool the prevalence of malnutrition was 31.1% in our in-patient population. National guidance states that all patients should be screened for malnutrition on admission. In practice this occurred in only two thirds (68.9%) of patients thus over a quarter (27.5%) of the total malnourished cohort went unrecognised. Moreover only a third (35.1%) of the identified group were appropriately referred to dietetic services and a further 15.1% were provided nutritional support without appropriate referral. We conclude therefore that even with a locally developed screening tool and policy in place, current levels of recognition and treatment of malnutrition are low and opportunities for intervention are being missed. In the face of recent NICE guidance, hospitals must ensure that staff are properly trained and dietetics services equipped to meet the demand that will arise from the increased identification of malnourished patients.
UNDERSTANDING MORTALITY AFTER GASTROSTOMY TUBE INSERTION: USE OF A SURVIVAL MODEL BASED ON COMORBIDITY
G. R. Longcroft-Wheaton1, P. Marden2, B. Colleypriest3, D. Gavin3, G. Taylor4, M. Farrant5. 1Gastroenterology, St Richards Hospital, Chichester, 2Gastroenterology, Bristol Royal Infirmary, Bristol, 3Gastroenterology, 4Research and Development Support Unit, Royal United Hospital, 5Gastroenterology, Royal United Hospital, Bath, UK
Introduction: There has been considerable discussion concerning percutaneous gastrostomy tube (PEG) feeding and the high mortality seen after insertion. This study aims to improve our understanding of the causes of mortality of in-patients receiving a PEG by comparison with a survival curve predicted from a model proposed by Levine et al.1
Aims & Methods: A retrospective study of patients receiving a PEG over an 18-month period was performed. 55 cases were analysed. 44 were found to be eligible for inclusion. A Levine score was calculated for this cohort. A survival curve after PEG was produced and compared to the Kaplan-Meier curve predicted by the Levine model.
Results: The mortality at 1, 3, 6 and 12 months was 16%, 20%, 25% and 28% respectively. This matched the predicted death rate from the Levine model closely (Pearsons = 0.96). A χ2 was performed, which confirmed no statistically significant difference in survival between the 2 groups (p = 0.35).
Conclusion: We found that the mortality of patients receiving a PEG followed that predicted for a similar cohort of patients without PEGs in the Levine et al model. It would suggest that the deaths observed were due to underlying comorbidities. This can provide a baseline for mortality targets for PEG services and is useful information for patients regarding the risks and benefits of the procedure. It demonstrates that PEG does no harm. However, it also shows that most deaths occur within the first month of placement, and would support arguments for delaying placement until outcome from the underlying condition is more predictable.
TEN YEARS’ EXPERIENCE OF PEG-RELATED MORTALITY FROM A DISTRICT GENERAL HOSPITAL
J. Mannath, H. Hart, N. J. Trudgill, I. Mohammed. Gastroenterology, Sandwell General Hospital, West Bromwich, UK
Introduction: PEG tube placement is common practice, however the NCEPOD enquiry 2004 showed high 7-day mortality. A multidisciplinary approach and careful patient selection was recommended.
Aims & Methods: To review the PEG related mortality over a period from 1997–2006 and compare mortality and PEG insertion rates after implementing trust guidelines in 2001. Data on all PEG insertions at Sandwell Hospital were collected prospectively by specialist nurse and mortality obtained through Patient Administration System.
Results: A total of 387 PEGs were done, of which 57% were males and 43% females. Mean age was 70 (17–96). Median number of PEGs per year was 42. CVA (66%) and other neurological diseases (13%) were the commonest indications. Only 4% dementia patients received PEG. Since implementation of trust guidelines in 2001, there has been a reduction in the number of total PEG insertions due to a reduction of PEGs for CVA. The cumulative 7-day and 30-day mortality over the 10-year period was 7.5% and 23% respectively. There was an absolute reduction in 7-day as well as 30-day mortality over the past 5 years, although not statistically significant (p = 0.3). This was achieved by a combination of careful patient selection and education of other medical teams by our specialist nurse. Older patients (>75) had significantly higher 30-day mortality (70.5% vs 29.5%, p = 0.021).
Conclusion: Our long term PEG-related mortality compares favourably to the NCEPOD enquiry. There is a reduction in absolute mortality and number of PEG insertions over past 5 years due to careful patient selection after review by the specialist nurse and discussion in MDT. Elderly patients (>75) have a significantly higher mortality following PEG insertion.
RESPONSE TO 5 G OR LESS OF LACTOSE IN PATIENTS WITH LACTOSE INTOLERANCE
L. Harrington, J. F. Mayberry. Department of Digestive Diseases, University Hospitals of Leicester, Leicester, UK
Introduction: It is estimated that some 5–10 million people in the UK may have lactose intolerance, with many remaining undiagnosed although they experience symptoms. Researchers however disagree about the amount of lactose needed to cause symptoms in those who are lactose intolerant. The consensus is that at least 12 g of lactose is needed to cause mild symptoms, although some papers and case-studies suggest that less than 6 g, or even the amount included as a “filler” in medication, may be enough to provoke symptoms. At the same time, lactose is being used in greater quantities commercially during food preparation.
Aims & Methods: To investigate the effect of 5 g and less of lactose in lactose-intolerant patients to determine whether the quantities of lactose “hidden” in food and medication are sufficient to cause symptoms. Lactose-intolerant patients participated in a double-blind randomised controlled study. They were restricted to a lactose-free diet for four days and then took one of four doses of 5 g or less of lactose. Their response to the dose was recorded on a study-designed questionnaire that measured total system response. This process was repeated with a second dose of lactose.
Results: Of the doses that contained lactose, symptoms were recorded for 47.1% of these doses. All participants who recorded a response, including those with a low total symptom rating, indicated that they would avoid that dose in the future. It is estimated that 75% of patients with lactose-intolerance will react to approximately 4.3 g of lactose, but the amount of lactose contained in medication is not sufficient to cause symptoms of lactose intolerance.
Conclusion: Lactose-intolerant patients react to doses of lactose less than 5 g and, when asked, state this is not tolerable. They should be told that they may react to the amount of lactose found in less than half a glass of milk—lower amounts of lactose than acknowledged in current literature. When people are lactose intolerant they need clear, correct, information about foods and drinks that they should avoid. However, these patients should be informed that if their medications contain lactose, this is unlikely to cause problems. This may increase medication compliance.
10-YEAR AUDIT OF PARENTERAL NUTRITION SERVICE IN A DGH: IS COMPLIANCE WITH ALL NICE GUIDELINES ESSENTIAL TO PROVIDE A HIGH QUALITY SERVICE?
K. M. J. Robinson1, J. McKiernan1, G. Uprichard2, S. A. Kapadia3, B. C. McKaig3. 1Dietetics, 2Pharmacy, 3Gastroenterology, Royal Wolverhampton Hospitals NHS Trust, Wolverhampton, UK
Introduction: The nutrition support team (NST) at New Cross Hospital was established in 1997. Prospective data have been collected annually on all adult patients referred to the NST. BAPEN1 and NICE2 have published recommended guidelines for PN practice, a key recommendation being the need for a nutrition support nurse. We compare our 10-year data audit against standards from these guidelines.
Aims & Methods: Prospective audit data has been collected on 887 patients (>8500 PN days) referred to the adult NST from 1997–2007. Analysis of this data is compared to national guidelines and to previously published PN outcomes of established centres.
Results: Despite identifying a need for a support nurse, the NST has functioned with dietetic, medical and pharmacy input alone. Over the 10-year period, there has been a substantial reduction in the number of patients exposed to PN (126 in 1997 to 48 in 2007) and total PN days (1422 in 1997 to 400 in 2007). Our current figures are now comparable to national standards. The use of enteral tube feeding (ng/nj) has correspondingly increased. The number of patients receiving PN inappropriately has fallen from 64% to 10%. Following trust initiated infection prevention measures the number of infectious complications has fallen from 23% to 9% since 2001. This also coincides with the rationalisation of catheter usage, in particular the withdrawal of PIC lines. In our series, infection, inappropriate use of PN and interruption of PN was associated with patients in whom PN was administered via IC lines. Patient assessment and monitoring is compliant with NICE guidelines and to date we have had no metabolic complications from PN therapy.
Conclusion: A consistent approach to promoting enteral feeding can reduce the need for inappropriate PN. Basic infection prevention measures are effective in reducing infective complications of PN. Although nurse support is desirable, we have demonstrated that a safe, appropriate PN service can be provided by a dedicated team without specialist nurse support.
OSTEOPOROSIS IN PATIENTS OVER 50 FOLLOWING RESTORATIVE PROCTOCOLECTOMY FOR ULCERATIVE COLITIS, IS DEXA SCREENING WARRANTED?
S. D. McLaughlin1, Z. L. Perry-Woodford2, M. W. Johnson3, S. K. Clark2, P. P. Tekkis1, P. J. Ciclitira3, R. Nicholls1. 1Department of Biosurgery and Surgical Technology, Imperial College, 2Department of Surgery, St Mark’s Hospital, 3Department of Gastroenterology, Nutritional Sciences Research Division, King’s College, London, UK
Introduction: Ulcerative colitis (UC), corticosteroids and age are risk factors for osteopenia and osteoporosis. The current BSG guidelines1 recommend performing DEXA in high risk patient groups. There are no studies of bone density in patients over 50 following restorative proctocolectomy. We hypothesised that these patients would be at high risk since they are likely to have had worse disease and received higher doses of corticosteroids than an average population of UC patients. We sought to establish whether DEXA should be routinely performed in this group.
Aims & Methods: We sought to establish whether DEXA should be routinely performed in patients over 50 following restorative proctocolectomy for UC. All RPC patients over 50 seen in an outpatient clinic from August 2006 to August 2007 underwent a DEXA bone scan unless recently performed. The notes were reviewed.
Results: See table. Osteoporosis was found in 18% of patients.
Conclusion: Males are at increased risk; this is in keeping with studies in UC.2 RPC may increase bone density; those patients with reduced bone density had undergone RPC more recently than normals. Osteopenia was very common, this is important and clinicians should ensure RPC patients over 50 take adequate dietary calcium and vitamin D or consider supplementation to prevent osteoporosis. This study suggests that osteoporosis in RPC patients over 50 is no more common that in normal UC patients; routine DEXA is not warranted and the standard BSG guidelines should be followed.
RE-FEEDING SYNDROME AND RE-FEEDING-LIKE ABNORMALITIES IN PATIENTS WITH ALCOHOLIC LIVER DISEASE: ARE WE VIGILANT ENOUGH?
S. Menon, J. Dillon, A. Bohan, A. Brind. Gastroenterology, University Hospital of North Staffordshire, Stoke on Trent, UK
Introduction: Patients with alcoholic liver disease represent a group that are vulnerable to re-feeding syndrome (RS) when fed, due to pre-existing undernourishment and electrolyte abnormalities. Clinical signs of RS are often overlooked due to these factors.
Aims & Methods: To evaluate the incidence of RS and re-feeding-like abnormalities (RL) in patients with alcoholic liver disease admitted to an acute Hepatology ward. All patients with a diagnosis of alcoholic liver disease admitted over a period of 4 months (December 2006 to March 2007) were prospectively assessed for electrolyte abnormalities. Severe hypophosphataemia (SH) was defined as serum phosphate <0.5 mmol/l and mild to moderate hypophosphataemia (MH) was defined as serum phosphate 0.5–0.8 mmol/l. Hypomagnesemia and hypokalemia were defined as serum magnesium <0.75 mmol/l and serum potassium <3.5 mmol/l respectively. All patients with electrolyte abnormalities were treated.
Results: 36 patients were admitted over a 4-month period (22 male, 14 female: mean age 52 years, 16/44, 44% cirrhotics). All patients were commenced on oral nutritional supplements (mean 540 kcal/day) and 13 patients received supplemental nasogastric (NG) feeding. 11/36 (30%) patients developed MH and one patient developed SH (normal initial serum phosphate). Of these, 8/11 (73%) were on NG feeding (see table). 5/11 (45%) of patients with MH had concurrent hypokalemia and hypomagnesemia and of these, 4 were on NG feeding. 9/11 (81%) of patients developing MH had symptomatic liver disease. Two patients with MH died due to hepatorenal syndrome.
Conclusion: RS and RL are common in patients with alcoholic liver disease. Clinical signs are often subtle and a high index of clinical suspicion must be exercised to detect and aggressively treat these abnormalities in this vulnerable population.
A TESTING TIME . . . ARE PATIENTS AT RISK OF RE-FEEDING SYNDROME BEING ADEQUATELY MONITORED?
J. Parr, C. Lamb, M. Warren. Gastroenterology, North Tyneside General Hospital, North Tyneside, UK
Introduction: The UK National Institute of Health and Clinical Excellence (NICE) have recently published a guideline entitled “Nutrition support in adults”(February 2006) containing recommendations on the management of malnourished patients. It is known that a significant proportion of adult patients admitted to hospital are suffering from malnutrition and are therefore at risk of developing re-feeding syndrome when nutritional support is introduced.
Aims & Methods: Our study took place in a District General Hospital in the North East of England. All 328 adult inpatients were screened on a single day (01/05/2007) for malnutrition using MUST (Malnutrition Universal Screening Tool) scores. We aimed to determine whether those patients identified as being malnourished at the time of admission to hospital, as defined by MUST score of 2 or greater (and therefore at potential risk of the re-feeding syndrome) had received adequate biochemical and electrolyte monitoring as recommended by NICE. Data regarding blood results were obtained retrospectively from the computerised biochemistry results system.
Results: 100% of adult patients (n = 328) were screened. All adult speciality wards were included. 105(32%) were identified as being at risk of malnutrition using the MUST score. 35 males: 70 females. Average age 75 years (range 17–98). Average inpatient length of stay at the time of the study was 15.5 days (range 1–90). All high risk patients had potassium levels checked on admission. Only 24% (n = 25) had phosphate levels and 9.5% (n = 10) had magnesium levels checked within 24 h of admission. In only 30 patients of 105 overall (28%), were both phosphate and magnesium checked at some stage during their stay and in 52 patients (50%) neither phosphate nor magnesium had been checked at any stage. In those who had stayed 3 days or more both phosphate and magnesium levels had been checked in only 13 of 92 (14%) over the initial 3 day period.
Conclusion: Malnutrition is common among hospital in-patients and emphasis is being put on early recognition and treatment. Our study shows that full and early monitoring of the biochemical markers of the re-feeding syndrome is not currently being performed in high-risk patients. Early recognition, monitoring and appropriate treatment of those at risk are essential in order to reduce the potentially life-threatening complications and electrolyte imbalances associated with the condition.
SIGNIFICANT NUMBERS OF COELIAC PATIENTS ON A GLUTEN-FREE DIET DO NOT MEET RNI TARGETS FOR MICRONUTRIENTS
G. G. Robins, D. Wild, P. D. Howdle. Academic Unit of Medicine, University of Leeds, Leeds, UK
Introduction: A strict gluten-free diet (GFD) is the only recognised treatment for patients diagnosed with coeliac disease (CD). However, there is little information on the quality of the GFD, especially with regard to micronutrients. The main source of selenium in a typical diet is bread and cereals.
Aims & Methods: The aim of this study is to identify whether patients on a GFD are meeting the recommended nutrient intake (RNI) of a number of micronutrients. Over a 9-month period, all patients seen in a weekly, specialist gastroenterology clinic in a large UK teaching hospital, with histologically confirmed CD and on a strict GFD for at least 6 months were invited to complete prospectively a validated 5-day food diary. 65 patients were identified, of whom 46 returned completed usable diaries. Completed diaries were inputted into “Microdiet for Windows v2.52”, a computerised nutrient databank. Data for gluten-free foods not in the nutrient databank were obtained from direct communication with the manufacturers.
Results: Mean age of respondents was 54.0 years (range 21–79). 32 out of the 46 patients were female. Although self-reported, no food diary included in the analysis contained gluten. Results are shown in the table.
Conclusion: Significant numbers of CD patients on a GFD fail to meet RNI targets across a number of micronutrients. This is particularly true with regards to selenium, magnesium and calcium recommendations for patients with CD.
FEMALE COELIAC PATIENTS ON A GLUTEN-FREE DIET CONSUME A DISPROPORTIONATE AMOUNT OF NON-EXTRINSIC MILK SUGARS
G. G. Robins, D. Wild, P. D. Howdle. Academic Unit of Medicine, University of Leeds, Leeds, UK
Introduction: Previous local research1 has shown that female patients with coeliac disease (CD) on a gluten-free diet (GFD) consume significantly more calories, although percentage of energy obtained from the major food groups did not differ significantly from the representative population. Current guidelines recommend only 10% of all energy is derived from non-milk extrinsic sugars (NMES).
Aims & Methods: The aims are to confirm or refute the above findings in a larger group and to identify which subgroups of foods are responsible for the increase in calorie consumption. Over a 9-month period, all patients seen in a weekly, specialist gastroenterology clinic in a large UK teaching hospital, with histologically confirmed CD and on a strict GFD for at least 6 months were invited to complete prospectively a validated 5-day food diary. 65 patients were identified, of whom 46 returned completed usable diaries. Completed diaries were inputted into “Microdiet for Windows v2.52”, a computerised nutrient databank. Data for gluten-free foods not in the nutrient databank were obtained from direct communication with the manufacturers. Results obtained were compared against the “National Diet and Nutrition Survey of Adults 19–64” published in July 2003 by the Office for National Statisitics. Student’s unpaired t test was used to test for statistical significance.
Results: Mean age of respondents was 54.0 years (range 21–79). 32 out of the 46 patients were female. Mean BMI for females was 24.7 kg/m2 and for males 27.7 kg/m2. Overall, for women 36% of energy was obtained from fats, 48% from carbohydrates, (including 15% from NMES) and 15% from protein. This compares with 34% from fats, 49% from carbohydrates (including 12% from NMES) and 17% from protein in a female representative population from Northern England. Corresponding figures for males were 35%, 48%, 15% and 15% (vs 35%, 48%, 13% and 17%). These differences were not significant. Mean (SD) energy intake for the males was 2373 (588) kcal/day, vs 2259 (533) kcal/day) in the representative population and 1912 (366) kcal/day, vs 1618 (440) kcal/day for the females (p<0.001). For females on a GFD, mean carbohydrate intake was 244 (59) g per day vs 202 (58) g in a representative population. Increased fibre intake accounted for only 1 g of this, whereas non-milk extrinsic sugars accounted for 23 g (p<0.0001), equivalent to 29% of the extra calories ingested by these patients.
Conclusion: Female CD patients on a strict GFD do have a significantly higher energy intake, a large percentage of which is accounted for by simple sugars, reflecting the sugary nature of a lot of GFD foods. This implies less sugary snack foods should be more readily available for those on a GFD.
CALCIUM INTAKES AND OSTEOPOROSIS SCREENING IN PATIENTS WITH COELIAC DISEASE, CROHN’S DISEASE AND ULCERATIVE COLITIS
J. E. Dart1, M. Abraham2, V. Bara2, S. P. L. Travis3, D. P. Jewell3, K. Whelan2. 1Department of Nutrition, Alfred Hospital, Melbourne, Australia, 2Nutritional Sciences Division, King’s College London, London, 3Gastroenterology Unit, John Radcliffe Hospital, Oxford, UK
Introduction: The increased risk of osteoporosis in patients with coeliac disease, Crohn’s disease and ulcerative colitis (UC) is multifactorial and includes alterations in calcium absorption and metabolism as well as steroid treatment in Crohn’s and UC. While the recommended calcium intake for healthy adults is 700 mg/d (Department of Health), guidelines for these patients recommend intakes of 1000 mg/d (ECCO guidelines), 1000–1200 mg/d (2007 BSG guidelines) or 1500 mg/d (2000 BSG guidelines).
Aims & Methods: The aim of this study was to measure dietary and supplemental calcium intakes and osteoporosis screening in these patients and to investigate whether differences exist between disease groups. Ninety one patients with coeliac disease (n = 31), Crohn’s disease (n = 36) or UC (n = 24) were recruited from gastroenterology outpatient clinics at the John Radcliffe Hospital, Oxford, UK. Exclusion criteria were patients with osteoporosis or previous fractures. Dietary calcium intake was measured using a validated food-frequency questionnaire and supplemental calcium intake was measured using prescription data and patient reports. Details of DEXA scans were recorded from medical notes.
Results: Median dietary calcium intake was 1079 mg/d (min 285, max 3098) and median total calcium intake was 1150 mg/d (min 285, max 3598). Supplemental calcium was prescribed to 18 (58%) patients with coeliac disease, 8 (22%) patients with Crohn’s and only one (4%) patient with UC (p<0.001). Dietary (p = 0.042), supplemental (p = 0.002) and total (p = 0.001) calcium intakes differed significantly between patient groups. Of those patients who should have had a DEXA scan (2000 BSG guidelines), 28 out of 31 (90%) with coeliac disease, 8 out of 20 (40%) with Crohn’s and none out of 16 (0%) with UC actually had one performed (p<0.001, coeliac vs Crohn’s).
Conclusion: Dietary, supplemental and total calcium intakes in patients with coeliac disease, Crohn’s disease and UC are highly variable and differ between patient groups. Although patients with UC had the lowest dietary calcium intakes, they were least likely to be prescribed calcium supplements and undergo DEXA scan.
Endoscopy posters
IMPROVING VIEW QUALITY AND TRANSIT TIME IN CAPSULE ENDOSCOPY
L. Muntane1, V. Gummer2, J. O’Brien2, M. K. McStay2. 1Barts and the London Medical School, London, 2Gastroenterology, Southend University Hospital, Southend, UK
Introduction: Capsule endoscopy is a new diagnostic method allowing painless visualisation of the entire small bowel. Standard preparation consists of clear fluids from 12:00pm the day before the test, and then nil-by-mouth from midnight. However, the test may be limited by poor luminal views and by incomplete small bowel transit in up to 25% of cases. Current data on the use of bowel preparation and pro-kinetics in order to improve the quality and completeness of the examination are limited and inconsistent.
Aims & Methods: We assessed whether magnesium citrate (Citramag) and senna bowel preparation taken with oral metoclopramide as a pro-kinetic agent resulted in superior luminal views and completion rates compared to standard preparation or Citramag alone. Patients were prospectively allocated to one of the following groups: (1) standard preparation (N), (2) Citramag (2 sachets in 2 l water) taken on the afternoon/evening prior then nil-by-mouth from midnight (C), 3) Citramag and senna (1 sachet) taken as above +10 mg metoclopramide 15 minutes pre-procedure (CSM). All patients were given simethicone with water when the capsule was swallowed to reduce bubble artefact. The studies were reviewed by a single investigator blinded to the preparation given. The view quality was graded using a previously validated 5-point scale based on the degree of obscured mucosal views (0 = 0–20%, 1 = 20–40%, etc).1 The score was applied to 5-minute segments of video from entry into the duodenum and every 10% of the small bowel transit time thereafter (max score = 44). The gastric transit times (GTT), small bowel transit times (SBTT), completion rates, significant findings and adverse events were recorded.
Results: View quality was significant improved and SBTT significantly reduced in the CSM group compared to standard preparation (median score 34 vs 30, p = 0.04; median SBTT 180 vs 241 min, p = 0.008; n = 18). View quality was better and SBTT significantly reduced in the CSM group compared to the C group (median score 30, p>0.05; 180 vs 235 min, p = 0.03; n = 18). There was no difference in view quality or SBTT between N and C. Completion rates were equivalent in all three groups: 94%. There was no significant difference in GTT between the groups. There was no difference between groups in patient demographics or the number of findings seen. There were no adverse events.
Conclusion: Bowel preparation with Citramag and senna used together with metoclopramide pre-procedure results in significantly better small bowel visualisation and reduced small bowel transit times than standard preparation or Citramag alone.
MANAGEMENT OF EARLY PERI-AMPULLARY NEOPLASIA: SURGICAL VERSUS ENDOSCOPIC RESECTION
R. J. Mead1, M. D. Duku1, P. Goggin1, R. D. Ellis1, D. N. Poller1, D. Cowlishaw1, N. Pearce2, C. Johnson3, S. Sadek4, M. Walters4, P. Bhandari1. 1Gastroenterology, Portsmouth Hospitals Trust, Cosham, 2Upper GI Surgery, 3Upper GI Surgery, Southampton University Hospital, Southampton, 4Upper GI Surgery, Portsmouth Hospitals Trust, Cosham, UK
Introduction: Despite centralisation of surgical expertise, and dedicated meticulous surgical selection pancreaticoduodenectomy remains a procedure with considerable morbidity and mortality. In recent years we have used endoscopic papillectomy for further assessment and cure, in conjunction with more traditional surgery or palliation. We present our outcomes to date.
Aims & Methods: All patients with early neoplasia of the ampulla of vater were included in our study. These included T1 tumours, adenomas with dysplasia, and other benign lesions. All patients were either treated with Whipples, endoscopic papillectomy or best palliative care, on their own or in combination. Decisions were made on the basis of likely pathology, technical feasability, and medical comorbidity. Diagnostic workup consisted of chromendoscopy, CT scan, and EUS. Patients with endoscopic appearance at chromendoscopy or biopsy suggestive of invasive cancer were offered surgery. Patients with a benign appearance and biopsy, or who were unfit for surgery had a papillectomy. Patients unfit for either were palliated. We aim to compare the survival, morbidity, mortality, and hospital stay outcomes between surgical and endoscopic groups.
Results: We identified early neoplasia between 2005–7. 10 men and 14 women met the criteria. 7 were palliated. 1 patient underwent a papillectomy and subsequent Whipples.
Conclusion: Surgery is an ultimate curative option but is associated with significant morbidity and mortality. Endoscopic treatment is challenging, but safe and effective. All patients decisions require very careful assessment and expertise.
TECHNICAL FEASIBILITY AND SAFETY OF ENDOSCOPIC MUCOSAL RESECTION OF LARGE AND FLAT COLONIC POLYPS
A. K. Muddu1, R. Mead1, D. Poller2, D. Cowlishaw2, A. Parvaiz3, M. Thompson3, D. O’Leary3, T. Trebble1, A. Quine1, P. M. Goggin1, P. Bhandari1. 1Department of Gastroenterology, 2Department of Pathology, 3Department of Surgery, Queen Alexandra Hospital, Portsmouth, UK
Introduction: With the advent of bowel cancer screening an increasing number of asymptomatic individuals are being diagnosed with large and flat colonic polyps. Traditionally, these would be surgically resected due to concerns about the efficacy and safety of endoscopic resection and risks of underlying cancer. However, with improved experience and techniques in endoscopic mucosal resection (EMR), these may be endoscopically resected and we report our experience of EMR of large and flat colonic polyps.
Aims & Methods: The aim was to examine the technical feasibility and outcome of EMR of large colonic polyps (>25 mm). We reviewed the data of all patients who had colonic polyps resected by EMR and ESD (endoscopic submucosal dissection) using an IT+ needle knife since December 2006. Data were collected on polyp size and type, resectability, histology, complications and completion of excision.
Results: 55 colonic polyps above 25 mm (range 25 mm–70 mm) in diameter from 51 patients were considered for endoscopic mucosal resection with 9 Is (sessile polypoid type) Paris type polyps (mean diameter 33 mm) and 46 LST (laterally spreading tumours), (mean diameter 44 mm). 5/55 polyps were deemed unsuitable for endoscopic resection due to endoscopic suspicion (based on non lifting sign and type V pit pattern) of invasive carcinoma in four polyps and the lesion crossing the dentate line in one polyp. These polyps were then surgically resected with three found to have invasive cancer and two found to have high grade dysplasia. Out of the 50 polyps resected endoscopically 44/50 (88%) polyps had complete resection in one sitting. 6/50 (12%) polyps required two procedures to achieve complete resection. The average time taken for endoscopic resection was 45 min (30–120 min). Significant bleeding occurred in one patient at 48 h requiring further endoscopy and haemostatic treatment. No perforations occurred in our series and no one required emergency surgery or had EMR-related mortality.
Conclusion: This series shows that it is technically feasible to endoscopically resect and cure more than 96% of large and flat colonic polyps. It is safe to perform endoscopic resection of high risk lesions with no mortality and minimum morbidity. Accurate endoscopic assessment of the lesion prior to EMR is essential.
A COMPARISON OF SCOPEGUIDE WITH CONVENTIONAL COLONOSCOPY
P. J. Mullen. Department of Gastroenterology, The Princess Elizabeth Hospital, Guernsey, UK
Introduction: The movement of electromagnetic transmission coils, built into the insertion tube of the colonoscope, within the magnetic field of a receiving dish enables the Olympus ScopeGuide system to provide a real time 3D image of the position and configuration of the colonoscope inside the patient. This system has several potential advantages but is primarily designed to reduce the difficulty of colonoscopy by allowing for early identification and prevention/resolution of loop formation.
Aims & Methods: In order to evaluate these proposed advantages, the completion rate and insertion time of 390 colonoscopies performed with an Olympus CFQ260L colonoscope using the ScopeGuide technology were compared with the preceding 420 performed with a conventional, variable-stiffness colonoscope (Olympus CF240AL). One experienced operator undertook all the procedures and data were collected prospectively.
Results: The 2 groups were equivalent as regards age, gender, previous colon resection and use of electrocautery. There were 12 failures (8 non-operator dependent) in the ScopeGuide group, giving overall and adjusted completion rates of 378/390 (96.6%) and 378/382 (99.0%). These were significantly better (p<0.005) than the conventional group (381/420, 90.7% and 381/401, 95.5%). Contrary to expectation, insertion times were the same in each group, although there was a non-significant trend with ScopeGuide for there to be fewer prolonged procedures (⩾13 min), particularly in females. Only 1 of the 4 true failures in the ScopeGuide group was classified as being due to excessive patient discomfort, compared with 10 of 20 in the conventional group.
Conclusion: ScopeGuide can improve the completion rate of colonoscopy even for experienced operators. Insertion times in this study were not shortened but there was evidence of procedures being less painful.
THE EFFECT OF MUSIC ON ANXIETY LEVELS OF PATIENTS ATTENDING FOR ENDOSCOPY
H. El-Hassan, K. McKeown, A. F. Muller. Department of Gastroenterology, The Kent and Canterbury Hospital, Canterbury, UK
Introduction: Music has been recognised in some studies to have a calming effect and may relieve stress. Patients attending for gastrointestinal endoscopy are often anxious and worried. This study examined whether the provision of music before endoscopic procedures altered anxiety levels in these patients.
Aims & Methods: Prospective randomised controlled trial. Patients fulfilling the following five inclusion criteria were invited to participate: (a) first ever endoscopy; (b) aged ⩾18 years; (c) ability to read and comprehend the information sheet; (d) competent to give consent; (e) ability to listen to music. Patients were randomised into two groups—Control (C) and Music (M); anxiety levels were measured using the State-Trait Anxiety Inventory (STAI)1 on arrival in the Unit and immediately before the endoscopy procedure, after 15 minutes listening to self-selected music therapy (M) or no music for the same period (C). Group scores ranged from a minimum of 20 to a maximum of 80 points. The effect of age (⩽ or >51 years) and procedure (gastroscopy or flexible sigmoidoscopy/colonoscopy) on anxiety levels was also assessed. Ethical approval was obtained from the local research and ethics committee prior to commencement.
Results: 180 patients (M: F 81: 99) mean age (±SD) of C: 59.18±17.80 and M: 60.73±15.24 years. There was no difference in anxiety levels at baseline based on age (<51 years, n = 56: 42.21±9.18; >51 years, n = 124: 39.99±10.13 (p = 0.15) or procedure: Gastroscopy, n = 87: 39.43±9.9, flexible sigmoidoscopy/colonoscopy: n = 93: 41.86±9.75 (p = 0.98). There was no difference in anxiety scores for group C (n = 88) at baseline (38.92±9.87) and immediately pre-endoscopy (38.182±11.40, p = 0.243). There was a significant reduction in anxiety scores in group M (n = 92) from 42.37±9.62 to 26.45±6.82 (p<0.001).
Conclusion: Anxiety levels in patients attending for endoscopy are not influenced by age or procedure, but are significantly reduced by listening to music compared to controls. The availability of music within the endoscopy unit is a simple strategy that will improve the well being of patients.
A PROSPECTIVE SINGLE CENTRE STUDY OF THE CLINICAL SIGNIFICANCE OF ERYTHEMA ON COLONOSCOPY
S. C. Ng, M. Shariff, G. Holdstock, D. Datta. Gastroenterology, The Hillingdon Hospital, London, UK
Introduction: Erythema in the absence of other signs is a finding commonly visualised on colonoscopy but the significance of this non-specific feature is unclear. Whether mucosal biopsies reveal clinically important histological abnormalities has not been formally studied.
Aims & Methods: The aim of this study was to assess the clinical and histological significance of erythema as the only endoscopic finding in patients referred for colonoscopy of all indications. Consecutive patients referred for colonoscopy found to have erythema were prospectively included. Patients with other endoscopic variables including loss of vascular pattern, granular mucosa, friable mucosa, ulceration, erosions, pseudopolyps, visual dysplasia, strictures or cancers were excluded. Between two to four biopsies were taken from the site of erythema and approximately two further biopsies were obtained from normal looking mucosa. Procedures were performed by two experienced endoscopists (more than 400 colonoscopies per year) and one supervised trainee endoscopist.
Results: Forty patients (22 male, 18 female) with a mean age of 50 (range 18–85), were included. Subjects were prepared for colonoscopy with sodium picosulphate. Indications for colonoscopy were altered bowel habits (n = 12), rectal bleeding (n = 9) and diarrhoea (n = 19). Erythema was identified in the rectum in 20 cases, left colon in 14 cases and right colon in six cases. Of the targeted biopsies, abnormal histology was reported in 13 cases (33%). Clinically significant pathology was found in seven cases (20%). There were four cases of non-specific colitis, three cases of inflammatory bowel diseases (2 ulcerative colitis, 1 Crohn’s disease), four cases of melanosis coli and two cases of mucosal prolapse. Non-targeted samples were normal apart from one case of collagenase colitis. The remaining 27 patients (67%) had normal biopsies. Of the seven cases of colitis, five patients presented with diarrhoea and two had rectal bleeding.
Conclusion: Clinically important pathology can exist in significant number of cases in spite of non-specific colonoscopic finding like erythema. This suggests that erythema in the absence of other signs may represent an early stage in the evolution of chronic non specific inflammatory bowel disease and biopsies are important, especially when clinical suspicion is high.
ADENOMA DETECTION RATES ARE HIGHER THAN PREDICTED AND CORRELATE WITH COLONOSCOPIC WITHDRAWAL TIMES IN THE BOWEL CANCER SCREENING PROGRAMME
D. L. Nylander1, M. Rutter2, G. Clifford3, J. Singh3, L. Hurst2, J. Painter4, C. Rees5. 1South of Tyne Bowel Cancer Screening Centre, Sunderland Royal Hospital, Sunderland, 2Tees Bowel Cancer Screening Centre, North Tees Hospital, Stockton, 3South of Tyne Bowel Cancer Screening Centre, Queen Elizabeth Hospital, Gateshead, 4South of Tyne Bowel Cancer Screening Centre, Sunderland Royal Hospital, Sunderland, 5Tees Bowel Cancer Screening Centre, South Tyneside General Hospital, South Shields, UK
Introduction: One aim of the bowel cancer screening programme (BCSP) is to detect and remove adenomas by colonoscopy, hoping that this will reduce the incidence of future colorectal cancer (CRC). In planning the service, we estimated from the first phase screening pilot, that adenomas would be detected in 40% of individuals undergoing screening colonoscopy.
Aims & Methods: The South of Tyne and Tees BCS centres (total population 1.5 million) began screening colonoscopies in 3/2007. We analysed data collected during all procedures in the first 6 months (extracted from BCSP central database) to assess the following: (1) adenoma detection rate (ADR); (2) colonoscopy withdrawal times (CWT), to see if endoscopists complied with the suggested mean of 6 minutes or more1; (3) if CWT correlated with ADR; (4) if endoscopists with similar ADR in BCSP have similar ADR in “symptomatic” service. Procedures in which there were no polyps, neoplastic lesions or pathology needing biopsy were identified and used to calculate CWT for each endoscopist. We also obtained data from the symptomatic service of endoscopist numbers 1–3 performed over the same period.
Results: Five endoscopists performed total of 515 procedures. Adenomas were detected in 272 (53%), significantly more than the 40% predicted in the pilot study (p<0.0001). There was significant correlation between mean CWT and ADR (Spearman r = 0.9747; p = 0.0167). In their symptomatic service, endoscopists 1, 2 and 3 had ADRs of 10%, 10% and 18% respectively. There was no significant difference between these ADRs (p = 0.1 for endoscopist 3 vs 2; p = 0.1 for endoscopist 3 vs 1).
Conclusion: ADR was significantly higher in our centres than in the pilot study. This has impact on workload and is important for those planning to set up BCSP. All endoscopists had mean withdrawal time of 6 min or more, but one had an ADR lower than the rest. Despite all endoscopists being compliant with CWT 6 min or more, strong correlation exists between mean CWT and ADR, supporting importance of slow, methodical extubation. Endoscopists who have similar ADRs within the BCSP also have similar ADRs in their symptomatic service sugesting no difference in practice between these services.
Research submitted on behalf of the Northern Region Endoscopy Group (NREG).
USE OF THE SX-ELLA SELF-EXPANDING MESH METAL STENT IN THE MANAGEMENT OF VARICEAL HAEMORRHAGE: INITIAL EXPERIENCE IN EIGHT PATIENTS
M. Reynolds, A. K. Burroughs, D. W. Patch, J. P. O’Beirne. Sheila Sherlock Department of Hepatobiliary-pancreatic Medicine and Liver Transplantation, Royal Free Hospital, London, UK
Introduction: Patients with variceal bleeding that is refractory to endoscopic or pharmacotherapy often undergo salvage procedures such as Sengstaken-Blakemore (SBT) or transjugular intrahepatic stent shunt (TIPS) insertion. While highly effective these procedures have important limitations. SBT is a temporary therapy and often requires the patient to be intubated while TIPS is associated with a high mortality in patients with advanced liver disease. The recently described SX-Ella DANIS stent is a self expanding covered mesh metal stent that is deployed in the lower oesophagus achieving haemostasis by compressing oesophageal varices. The stent may be left in situ for up to 2 weeks and is removable.
Aims & Methods: We evaluated the use of the SX-Ella stent in the management of patients with endoscopically proven or suspected variceal bleeding who were refractory to standard therapy and who had contraindications to TIPS or where SBT could not be inserted. Stents were deployed as per the manufacturers instructions. The delivery system was placed in the distal stomach either over an endoscopically placed guidewire or blindly. A balloon was then inflated to anchor the distal end of the stent at the cardia before deployment of the stent. The balloon was then deflated and the delivery system removed. Satisfactory stent deployment was confirmed by endoscopic examination and radiography.
Results: Eight patients (all Childs-Pugh Class C) underwent stent insertion. Indications for stent insertion were: contraindication to TIPS (n = 5), failed SBT insertion (n = 2) and oesophageal perforation due to SBT (n = 1). Stent insertion was successful in 7/8 (87.5%). In patients with successful stent deployment, haemostasis was achieved in 5/7 (71%). 3 patients survived the acute bleeding episode (37.5%) and had the stents removed endoscopically at 10 (4–14) days post insertion. Causes of death were exsanguination in 2 (proven subsequently to be bleeding from gastric varices), terminal HCC (n = 1) and progressive multiple organ failure (n = 2). There were no complications related to stent insertion or removal and no stent migration was observed.
Conclusion: In patients with oesophageal variceal haemorrhage, insertion of the SX-Ella DANIS stent offers an alternative to other methods of salvage therapy. Stent insertion is easy and appears safe. Haemostasis rates are good (71%) but mortality is affected primarily by severity of the underlying liver disease.
GASTROSCOPY AFTER COMMUNITY TESTING FOR H PYLORI: WHAT DO WE FIND?
J. Parr, A. Saeed. Gastroenterology, Queen Elizabeth Hospital, Gateshead, UK
Introduction: H pylori testing is a key part of dyspepsia investigation in the UK, as patients without alarm symptoms may receive eradication therapy before considering further investigation. The H pylori stool antigen test (HPSA) is used for all H pylori testing in our region. All results from the area are collected centrally. We examined gastroscopy (OGD) reports of patients who had an HPSA test within the previous year, to discover if significant pathology was detected.
Aims & Methods: We aimed to find out the proportion of patients who have HPSA tested and proceed to having an OGD within 1 year of follow-up. In addition, we obtained information regarding the mode of referral, age and prevalence of significant OGD findings in this group. We used the HPSA database to identify all patients having an HPSA test over a 13 month period. Temporary residents were excluded. We cross referenced this against our endoscopy database to identify patients in whom an OGD had been scheduled within 1 year from the date of HPSA testing.
Results: 2171 patients were included. There were 713 positive HPSA tests and 1458 negative. 139 patients(19.5%)who tested positive were scheduled for OGD within 1 year. 60% of these were in patients >55 years old. This compares to 278 (19%) of those testing negative(51% were >55 years old).The average time to OGD was 4.8 months in both groups. The findings at OGD were divided into normal/mild abnormalities(inflammation only) and more serious abnormalities (cancers, ulcers, strictures, Barrett’s). The results are shown in the table. In 4 cancers detected under the 2 week rule, time to OGD from intitial HPSA test was less than 6 weeks. The other cancers detected took longer in the HPSA positive group (3, 7, 10 months) than in the HPSA negative group (2, 2, 4, 7 months) to come to OGD. Only 1 out of 11 cancers occurred in a patient under the age of 55 years (oesophageal) and the OGD was performed less than 4 weeks after HPSA negative result, due to the presence of alarm symptoms. Cancer pick up rates in patients proceeding to OGD were 0.4% in the under 55 years age group compared to 4.4% in patients >55 years. This gives a cancer detection rate of 2.6% in patients referred for further investigation. Cancers were diagnosed endoscopically in 0.5% of all patients having an HPSA test.
Conclusion: A significant number of patients proceed to OGD in the year following HPSA testing (19%). In our study, cancer and other serious abnormalities were uncommon, regardless of methods used for referral. In patients under 55 with no alarm symptoms, endoscopy appears to add little to patient management over a test and treat policy.
PRECUT SPHINCTEROTOMY: IS IT WORTH THE RISK?
K. K. Peddi1, L. Wilbraham2, R. England2, D. F. Martin2. 1Gastroenterology, 2GI Radiology, South Manchester University Hospital NHS Trust, Wythenshawe, UK
Introduction: Precut Sphincterotomy by needle knife technique is a method of gaining deep biliary access when standard methods fail and its safety is widely debated. Expert endoscopists argue that it is a very effective way of gaining deep biliary access and the benefits outweigh the risks if carefully performed.
Aims & Methods: We analysed a large database of all needle knife papillotomies performed at our tertiary centre over a five year period (December 2000 to July 2006)to see whether it was worth the risk. They were performed by either of the two very experienced endoscopists in the centre. All the cases were analysed retrospectively using a proforma.
Results: A total of 2800 ERCPs were performed in this period and a precut sphincterotomy using needle knife was required in 312 patients (11.4%) with an intention to gain deep biliary access. 131 were males and 181 females. 155 of 312 were referred from other hospitals. Patients age ranged from 20 to 98 years (mean age 71.9). Sedation was with Midazolam (1–25 mg) along with either Pethidine (12.5–100 mg) or Fentanyl (10–150 μg). Flumazenil was required in 7 patients for reversal. 3 patients required general anaesthetic. Indications were jaundice (129), dilated ducts (40), abnormal LFTs (44), cholangitis (22), stones (118), acute pancreatitis (34), stent review (3), biliary leak (6), pseudocyst (2), pain (21), previously failed (52), tumour (15), PSC (1). Deep biliary cannulation was achieved in 209 patients at first (67%), 55 out of 65 patients (84.61%) at second and 2 patients at 3rd attempt, making overall successful cannulation in 266 out of 312 (85.25%). Each patient was assessed immediately after procedure, 24 hours later and then followed up at 30th day by a specialist nurse. Complications were defined and graded according to the consensus criteria.1 There were 52 “adverse events” reported during first attempt with needle knife papillotomy (14.4%) and 18 of these met the definition of “complication” (5.76%). One mild and one moderate bleeds reported (0.64%). There were 2 mild and 3 moderate pancreatitis (1.6%). Two mild and one moderate perforations occurred (0.96%). Seven cases of mild cholangitis reported (2.24%). One death occurred due to pancreatitis (0.3%). Other events include submucosal injection (10), abdominal pain (14), sore eye and rhinitis at 30 days.
Conclusion: Precut sphincterotomy using needle knife papillotomy can result in mild complications even in expert hands but severe/fatal complications are very rare. It is worth taking the risk in selected patients if performed carefully by expert endoscopists.
DO ALARM FEATURES CONFER AN INCREASED RISK OF UPPER GASTROINTESTINAL CANCER IN PATIENTS AGED UNDER 55 YEARS WITH DYSPEPSIA?
N. Powell, J. Mawdsley, J. Teare, H. Thomas, R. Negus, J. Hoare, T. Orchard. Gastroenterology, Imperial College Healthcare NHS Trust, London, UK
Introduction: To expedite the diagnosis of upper gastrointestinal (GI) cancers, the National Institute for Health and Clinical Excellence (NICE) and the British Society of Gastroenterology recommend urgent endoscopy for patients of all ages with dyspepsia, if alarm features such as weight loss coexist. However, upper GI cancers are predominantly diseases of the elderly and the merit of endoscopy in young patients, even those with alarm features, has not been well defined.
Aims & Methods: We identified all patients undergoing upper GI endoscopy for dyspepsia in our unit over a 23-year period. We also recorded the presence of 4 NICE defined alarm features (weight loss, anaemia, dysphagia and vomiting) concomitantly listed as indications for endoscopy. The prevalence of upper GI cancers diagnosed in patients aged <55 years undergoing endoscopy for dyspepsia in both the presence and absence of alarm features was calculated. For comparison we also included patients aged >55 years with dyspepsia and alarm signs.
Results: From our dyspepsia population we identified 1371 patients aged <55 years with alarm features, 11 672 aged <55 years with no alarm features and 1663 patients aged >55 years with alarm features. The cancer prevalence was significantly higher in patients aged <55 years in the presence of alarm features (2.1%) compared to those without (0.4%, OR 5.34 (95% CI 2.29 to 12.47), p<0.0001). The presence of 2 alarm features was associated with significantly more cancers (10.6%) than the presence of 1 alarm feature (1.7%, p<0.0001). The alarm feature most significantly associated with cancer was weight loss (OR 12.01, 95% CI 2.01 to 71.84, p<0.0001), followed by vomiting (OR 5.08, 95% CI 1.34 to 19.27, p<0.0001). In older patients (aged >55 years) with dyspepsia and alarm features the prevalence of cancer (7.2%) was significantly higher than in younger patients (<55 years) with (OR 3.62, 95% CI 2.44 to 5.36, p<0.0001) or without (OR 19.32, 95% CI 8.99 to 41.50, p<0.0001) alarm features. The number of endoscopies and cost (based on Department of Health tariffs) required to diagnose 1 cancer was 14.0 (£5558) in patients >55 years with alarm features, 47.3 (£18,778) in patients aged <55 years with alarm features and 259.4 (£102,982) in patients aged <55 years with no alarm features.
Conclusion: The presence of alarm features significantly increases the diagnostic yield of upper GI cancer in young patients with dyspepsia, but is still very low with cancers only present in 2.1% of patients. Consequently offering urgent endoscopy to this population is a high cost strategy. The presence of particular alarm features such as weight loss or vomiting, or the presence of two or more coexistent alarm signs might offer improved determination of which young patients should undergo urgent endoscopy.
VALIDATION OF BOWEL PREPARATION QUALITY SCALES
M. Rahman, N. Van Someren, K. Besherdas, R. D’Souza. Gastroenterology, Chase Farm, Enfield, Middlesex, UK
Introduction: It is vital that colonoscopy completion rates in the UK improve before a screening programme for colon cancer can be successfully implemented. A completion rate of 90% is considered acceptable and has been accepted by the UK Endoscopy community. The main reason for failure to complete colonoscopy in our unit were poor patient intolerance or bowel preparation or severe diverticular disease. Adequate preparation of the colon is essential for proper colonoscopic visualisation. At our unit a non-validated 3-point scoring system based on subjective items is used to evaluate colonic cleansing.
Aims & Methods: Several scoring systems for bowel preparation have been developed. In this study our objective was to compare the Aronchick and Ottawa scoring system with our current standard system. A total of 100 patients undergoing routine diagnostic colonoscopy were included in the study. This study was performed over a 5-month period from May to September 2007 and carried out at two hospitals: Edgeware Community Hospital and Chase Farm Hospital. Of these 100 patients 50 had Moviprep at one centre and 50 Picolax at the other centre. Patients response regarding quality of bowel preparation were assessed prior to the colonoscopy and compared with the endoscopists. We compared three different scoring system for colonoscopy preparation—that is, Standard, Aronchick and Ottawa scale.1, 2 Before performing the Ottawa scale we carried out a calibration exercise. Standard: (1) Good; (2) Satisfactory; (3) Poor.
Results: The inter-observer agreement was assessed statistically using Pearson’s correlation coefficient. Picolax was found to be superior in elderly patients compared to Moviprep; while there was no significant difference between Picolax and Moviprep in younger patients (<45 years of age). Younger patients had better score for the colonic cleansing compared to older patients (p<0.01). Patients were unreliable judges of the quality of bowel preparation leading to overestimation of the cleanliness of their colon. The Aronchick and Ottawa scoring systems were superior to the standardised scoring system (p<0.01). However no difference was found between these two colonic preparation scaling system (p = NS).
Conclusion: Picolax was superior to Moviprep in older patients. Younger age was a good predictor for adequate bowel preparation. Patients are unreliable judges of the quality of bowel preparation tending to over estimate the cleanliness of their colon. The Ottawa scale gives much more specific information about which area of bowel is poorly prepared, whereas Aronchick outlines the whole picture. Both the Aronchick and Ottawa quality scale are easy to perform and give much more information than the standard scoring system and should be implemented into current endoscopy practice.
A UK AUDIT INTO THE RADIATION SAFETY AWARENESS AND PRACTICE IN ERCP
N. Rajoriya, A. Mee. Gastroenterology, Royal Berkshire Hospital, Reading, UK
Introduction: Endoscopic retrograde cholangiopancreatography (ERCP) relies on the use of ionising radiation, however risks and awareness of the safety aspects of the procedure are often not appreciated by the ERCP’ist. Guidelines have been published (Ionising Radiation Regulations 1999) with recommended levels of annual exposure.
Aims & Methods: The aim of this audit was to assess the safety practices and awareness of the radiation aspect of ERCP by doctors in the UK carrying out the procedure. An electronic questionnaire was sent (via email) to physicians, surgeons and radiologists registered with the British Society of Gastroenterology (BSG). Professors, Consultants and trainees (Specialist Registrars (SPRs)) were included. Emails were also sent to doctors in the ERCP community (provided from list previously used in a national audit of ERCP). The audit questionnaire was returned electronically to a base website (www.surveymonkey.com) and the information collated thereafter.
Results: 172 responses (92.4% male) were collected over a 2-month period. 93.5% were consultants, 4.8% trainees, and 1.8% professors. 51.5% were between the ages of 45–65, 42.7% between 36–45 and the rest below 36 years of age. 85.5% were gastroenterologists, 9.3% surgeons and 5.2% radiologists. Most (48%) have been practicing ERCP for 11–20 years, 21.7% >20 years, and 30.4% <10 years. 73.4% do 1 session per week, 17% do 2 sessions, 1.2% do 3 sessions and 7.6% do on average less than 1 session on a weekly basis. In the last 12 months 2.4% have done >250 ERCPs, 7.6% between 200–250, 19.4% between 150–200, 37.6% between 100–150, and 32.9%<100 ERCPs. With regard to protection: 37.2% always wear a thyroid shield, 8.1% >75% of the time, 6.4% 50–75% of the time, 6.4% <50% of the time, and 41.9% never wear a thyroid shield. 95.3% do not wear protective lead eyewear (only 1.7% do 100% of the time). Of those who did wear protective eyewear, 60% (10% prescription lenses) were provided free by the NHS trust/hospital. With regards to radiation exposure badges, 32% did not wear one. The majority (42.7%) wear a badge on the trunk (under the lead apron), 18.1% on the pelvic area (under apron) and 3.5% on the trunk and pelvis (under the apron). 61.8% of doctors have never been informed on their annual radiation exposure and only 11.8% regularly informed on an annual basis. 92.1% were unsure of their last year’s exposure. Only 29.1% had been on an ERCP course (involving safety lectures) in the last 5 years with 53% of 157 consultants not been on a course since becoming an SPR.
Conclusion: This audit highlights a wide variation of practice and awareness of UK ERCP’ists regarding safety in ERCP. We recommend that radiation protection officers have more input, and assess ERCP’ists practice to ensure that UK ERCP’ists are exposed to the lowest doses of radiation as possible to carry out the service provided.
A STEP-WISE ASSESSMENT OF COLONOSCOPIC BOWEL PREP EFFECTIVENESS
E. Hall1, J. Lattaway1, J. Vasani2, M. D. Rutter3. 1Endoscopy, 2Gastroenterology, University Hospital of Hartlepool, Hartlepool, 3Gastroenterology, University Hospital of North Tees, Stockton-on-Tees, UK
Introduction: Effective and well-tolerated bowel preparation is essential for optimal colonoscopic imaging and adenoma detection. There are almost as many different regimens as there are endoscopy units, involving different types and timing of medication and differing diets and restrictions. Some are more effective than others, and our unit felt its bowel prep was suboptimal.
Aims & Methods: The aim was to assess the effect of incremental adjustments in the bowel prep regimen. Bowel prep effect is entered onto the hospital endoscopy reporting system at the time of the procedure, graded as good, satisfactory or poor. Although the categorisation is subjective, the hospital’s colonoscopist population remained unchanged during the study, reducing this potential bias. In April 2007, we changed our original bowel prep (low residue diet 3 days and fluids only 1 days before procedure; 4 senna tablets and 2 Picolax sachets taken the day before the procedure) by increasing the senna dose to 10 tablets (as used in our sister hospital). To minimise potential bias, we did not publicise the change widely to colonoscopists. Two-sided Fisher’s exact analysis was performed, comparing “good” prep versus “not good” (a combination of those recorded as satisfactory or poor). As no difference was noted, a further change was made to the regimen in September 2007, reverting to 4 tablets of senna but bringing the diet and Picolax timing in line with our sister hospital (low residue diet 2 days and fluids only 1 days before procedure; 4 senna tablets and 1 Picolax sachets taken the day before the procedure, second Picolax taken on day of procedure). Further statistical analysis was performed.
Results: See table.
Conclusion: Increasing senna dose from 4 to 10 tablets did not improve the quality of bowel prep. Adjusting the timing of Picolax and liquids only aspect of the diet resulted in a statistically significant improvement in bowel prep quality. This improvement was achieved despite a shorter duration of altered diet prior to the colonoscopy, thus impacting less on the quality of life of our patients.
A SURVEY OF RIGID SIGMOIDOSCOPY USE AMONG UK GASTROENTEROLOGY TRAINEES IN TWO DEANERIES
G. J. Sadler, P. Ellul, B. C. McKaig. Gastroenterology, New Cross Hospital, Wolverhampton, UK
Introduction: Studies have shown rigid sigmoidoscopy (RS) causes more patient discomfort, has a lower diagnostic yield and poorer ease of use for procedures such as biopsy and polypectomy when compared to flexible sigmoidoscopy (FS). Visualisation of the rectosigmoid junction and sigmoid colon at RS is successful in only 40–70% of examinations. In addition, disposable instruments may pose an infection risk by potentially harbouring organisms in the bellows or light head. For these reasons, and due to the increasing availability of FS in out-patient clinic settings, the utility of RS is being called into question. However, there is no doubt it remains an effective, cheap and widely available diagnostic tool.
Aims & Methods: We conducted a questionnaire survey of registrars in the West Midlands and North Western Deaneries about RS use in their current working practice.
Results: 47 trainees responded—70% male and 30% female. 15% had never used RS. Only 32% of those who had used RS had been trained to do so; 89% felt they had received insufficient training. More than two thirds of trainees do not use RS in clinical practice, for reasons including the lack of available facilities (47%), its use being actively discouraged (16%) and feeling incompetent to perform the procedure (19%). 38% cannot take biopsies during RS. Reasons a trainee thought it may be appropriate to consider RS were: rectal bleeding (57%), change in bowel habit (17%), colitis assessment (45%), tenesmus (30%), pruritus ani (9%), proctalgia (19%), and cancer/polyp follow-up and weight loss (0%). Only 57% thought RS was a skill all gastroenterologists should be competent in. When asked if they had rectal symptoms requiring investigation, 79% said they would rather defer RS for an elective FS.
Conclusion: For a variety of reasons, the vast majority of trainees across these two Deaneries do not use RS in clinical practice, and believe insufficient training is given in its use. Surprisingly few would even consider using it in patients with worrying rectal symptoms such as bleeding, tenesmus and proctalgia. This may simply reflect a preference to defer investigation to FS which is increasingly available in the out-patient clinic setting, and is also the investigation, given the choice of RS or FS, most trainees would prefer to undergo themselves. It therefore seems unlikely, especially considering just over half believe RS is a gastroenterological skill, that many of these trainees will use RS in future clinical practice or even become competent in its use—if the same is true across the rest of the UK, is the “passing of the rigid sigmoidoscope” something for us to be concerned about?
COMPARATIVE SHORT AND LONG-TERM OUTCOMES OF ENTERAL STENTING IN PALLIATING GASTRIC-DUODENAL OUTLET OBSTRUCTION IN ADVANCED GASTRIC AND NON-GASTRIC MALIGNANT DISEASE
S. Sagi, K. Bodger, S. Sarkar. Digestive Disease Centre, University Hospitals Aintree, Liverpool, UK
Introduction: Enteral stenting is recognised as an effective method of palliation in malignant gastric and duodenal outlet obstruction with success rates similar to surgical palliation. Most published data are from case series and there is a lack of comparative data in efficacy of palliative enteral stenting between gastric and non-gastric malignant disease.
Aims & Methods: To compare the outcomes of enteral stenting in palliating gastric-duodenal obstruction in gastric and non-gastric malignant disease. All patients who underwent endoscopic metal stent placement for symptomatic malignant obstruction between 10/98 and 12/05 were identified using the Endoscribe database. Patients with proximal (oesophageal, junctional or proximal gastric) lesions were excluded. Data were abstracted from case notes using a standard Proforma and, pre- and post-procedure oral intake was assessed using a simple scale (1 = None/Inadequate; 2 = Liquids/Thickened Only; 3 = Semisolids; 4 = Unmodified diet).
Results: 32 patients, underwent palliative enteral stenting for malignant gastric (n = 16) and non-gastric (n = 16) disease. Non-gastric diagnoses included; pancreatic primary (n = 9), duodenal primary (n = 3) and other malignancies (n = 4). 14 patients in the gastric and 15 in the Non-gastric groups had metastatic disease. Patients with gastric disease were older (age 75 vs 67 years; p = 0.048) but ASA scores were similar (3.8 vs 3.9: gastric and non-gastric respectively) and the doses of sedation used were identical (mean Midazolam 4.6 mg and Fentanyl 39 μg). Oral intake showed a mean improvement by 1.1 and 1.3 points for gastric and non-gastric disease respectively. Discharges: 72% were successfully discharged; which was slightly higher for those with gastric disease (81% vs 66% for gastric and non-gastric disease respectively). Mean survival in days (SD) were similar at 107 (163) and 93 (110) days (p = 0.8) for gastric and non-gastric disease respectively. 30-day mortality was high with a higher trend for non-gastric disease at 50% compared to 25% for gastric disease (p = 0.1). Complication rates were high in both groups at 50% for gastric and 62.5% for non-gastric disease as was the re-intervention rate at 44% for gastric and 37.5% for non-gastric disease. 25% in each group required either re-stenting or by-surgery.
Conclusion: Enteral stent offers reasonable palliation of symptoms with successful hospital discharge in the majority. However, complications, re-intervention and 30-day post-procedure mortality rates were high with a possible potential benefit towards gastric disease despite the older patient population. All these factors should be considered in an MDT setting before stenting these terminally ill patients.
DO ENDOSCOPY AUDIT TOOLS OVERESTIMATE POLYP DETECTION RATES?
N. Jawad1, T. Bhagat1, S. Murray1, F. Jawad2, R. J. Makins1, E. W. Seward1. 1Endoscopy Unit, Whipps Cross University Hospital, 2Final Year Student, Barts and the London Medical School, London, UK
Introduction: Adenoma detection is taken as a proxy marker of the quality of colonoscopy. The accepted benchmark varies, and many professional societies have judged that ten or even 20% is the expected level for practising colonoscopists. This has attained more importance due to the welcome focus on colonoscopy quality in the UK at present. The majority of commercially available endoscopy recording systems allow the endoscopist to audit their practice very easily by maintaining a database of procedures that can be regularly interrogated. However, unless they possess a means of being updated by access to histology reports, there is a real risk that the adenoma detection rate will represent an overestimate—as self-reported “adenomas” may actually represent alternative diagnoses such as hyperplastic polyps, inflammatory polyps and cancers. Updating the database is currently laborious and time-consuming.
Aims and Methods: We proposed to audit our actual adenoma detection rate (as determined by histology) against our polyp detection rate (as determined by our endoscopy database) to establish if there is a significant difference. Every colonoscopy performed at our institution between July-December 2006 was reviewed and if polyps were identified, the histology was obtained. Confirmatory histology was required to record it as an adenoma. Each independent endoscopist was assessed, significance measured by χ2 test. A significant value was taken to be p<0.05.
Results: Seven consultant and three trainee endoscopists performed a total of 1052 colonoscopies in the study period. Caecal intubation rate for respective colonoscopists varied between 88 and 96%. Breakdown of polyp and adenoma detection rate by colonoscopist is shown in the table. Four procedures were incompletely entered and had no endoscopist identified and were therefore excluded from analysis.
Conclusion: There is no significant fall in the adenoma detection rate as established by our endoscopy database with the addition of histology, thus the audit tool in our unit can be relied upon to produce an accurate assessment of the true adenoma detection rate. Some of our colonoscopists are below accepted standards for polyp detection and need to improve.
COLONIC WALL THICKENING ON CT SCANNING AS A SOLE INDICATION FOR ENDOSCOPIC INVESTIGATION HAS A LOW YIELD OF SERIOUS PATHOLOGY
M. J. Shale, S. Ghosh. Department of Gastroenterology, Imperial College London, Hammersmith Hospital, London, UK
Introduction: Thickening of the colonic or terminal ileal (TI) wall is a common finding on abdominal CT scanning, and generally leads to colonoscopic examination. Previous studies attempting to correlate CT and endoscopic findings have examined small numbers of patients, and produced conflicting results regarding the diagnostic yield of endoscopy performed for this indication. We aimed to investigate the yield of colonoscopy where the indication was investigation of colonic or TI wall thickening reported on CT in a large unselected cohort of patients.
Aims & Methods: 113 consecutive patients undergoing lower GI endoscopy for the assessment of reported colonic or TI abnormality on CT scanning between 2002–7 were identified from endoscopy unit records. 26 patients with CT reports of stricture or intra-luminal mass were excluded. 87 patients (42 male), mean age 65 years (range 17–95) with colonic or TI wall thickening were included in this study. Indications for CT scanning were abdominal pain (n = 44), weight loss (n = 17), both symptoms (n = 5), and incidental reasons, including raised CRP, fever or suspicion of abnormalities on clinical examination (n = 21).
Results: Wall thickening on CT scan was pancolonic in 11 patients, pancolonic+TI in 5, TI only in 11, right sided in 17, left sided in 16 and rectosigmoid in 27. Lower GI endoscopy was normal in 40 patients (46%). Colorectal cancer (CRC) was diagnosed in 10 patients (11.5%) and IBD in 7 (8%) patients (Crohn’s, n = 6; UC, n = 1). 11 (12.5%) patients had non-specific (including infectious) colitis. 7 (8%) patients had ischaemic colitis. Therefore, serious pathology was diagnosed in 24 patients (28%). In 12 patients, incidental findings which did not affect management were diverticular disease (n = 7), polyps (n = 3) and miscellaneous others (n = 2). 24/41 (59%) and 9/11 (82%) colonoscopies were normal when the sole indication for CT scan was abdominal pain or weight loss respectively. TI Crohn’s disease was diagnosed in 4/16 (25%) patients with TI thickening on CT. Left-sided or rectosigmoid thickening was associated with the highest yield (7/43) of CRC (16%). Compared with patients with normal endoscopic findings, patients with CRC had significantly lower Hb and albumin (median Hb 10.4 vs 12.0 g/dl, albumin 23 vs 31 g/l; both p<0.05) and ischaemic colitis patients had a significantly higher WCC (median 11.8 vs 8×109/l; p<0.05).
Conclusion: In this study, only 28% of lower GI endoscopies performed to investigate colonic or TI thickening on CT scanning demonstrated serious pathology directly affecting management. Abnormal haematological or biochemical indices may have provided a further clue to underlying GI pathology in these patients. Colonic thickening noted on CT scanning performed to investigate abdominal pain or weight loss alone has a low yield of serious pathology on subsequent endoscopy.
GASTRIC POLYPS: A RETROSPECTIVE STUDY OF 8890 UPPER GASTROINTESTINAL ENDOSCOPY PROCEDURES
U. A. Sheikh, R. Sultana, B. Javaid. Gastroenterology, West Cumberland Hospital, Whitehaven, UK
Introduction: Data on the frequency and incidence of various types of gastric polyps are inconsistent.
Aims & Methods: To analyse the incidence of various types of gastric polyps in a patient population over a period of three and half years with respect to gender, age, histopathological type, concomitant endoscopy findings, Helicobacter pylori (HP) status and proton pump inhibitor (PPI) usage.
Results: A total of 278 patients (3.1%) were found to have gastric polyps, However clinical records of only 197 cases were available and these were finally included in the study. A significant female predominance (1:1.70) was seen with 125 (63%) women and 72 (37%) men having been diagnosed with gastric polyps. 167 (85%) of the patients were aged 50 years or over. Mean age was 64 years (range 22–94). Dyspepsia was the most commonly reported symptom (n = 126, 64%). 23% (n = 46) of the polyps were 1–2 mm in size, 35% (n = 70) polyps were 3–10 mm, while 5.5% (n = 11) were >10 mm. In 43% (n = 85) patients multiple polyps were found, 13% (n = 25) cases had 2–3 polyps and 27% (n = 54) patients had a single polyp. Majority of the polyps were fundic gland (FG) type (68%, n = 134). The frequency of inflammatory, hyperplasic and adenomatous polyps was 12% (n = 23), 8% (n = 16) and 3% (n = 6) respectively. One (0.5%) of the polyp was reported to be xanthoma. One (0.5%) polyp was regenerative histologically. Sixteen (8.1%) consisted of normal gastric mucosa. In five cases no biopsy was taken. Two (1%) polyps showed dysplasia out of which one turned out to be carcinomatous. The most common endoscopic finding apart from polyps was gastritis (n = 80, 41% patients). Two patients (1%) were diagnosed with gastric cancers and 2 (1%) had oesophageal cancer. 95 patients (48%) patients were on a PPI and 62 (65%) of these patients had FG polyps. A total of 51 (26%) patients had evidence of (HP) infection and 35 (68%) of these patients had FG polyps.
Conclusion: Gastric polyps were more commonly seen in women and in patients aged 50 years or over. FG polyps were the most frequently encountered polyps as an incidental finding in patients undergoing OGD for a variety of indications with dyspepsia being the commonest. FG polyps were more common in patients on a PPI and those with evidence of HP infection as compared to other type of gastric polyps.
THERAPEUTIC ENDOSCOPY IN THE PALLIATION OF UPPER GASTROINTESTINAL CANCERS: CAN IT BE SAFELY DONE IN DISTRICT GENERAL HOSPITALS?
S. Siddique1, J. Deacon1, I. R. Sargeant2, D. L. Morris1. 1Department Of Gastroenterology, Queen Elizabeth II Hospital, Welwyn Garden City, 2Department Of Gastroenterology, Lister Hospital, Stevenage, UK
Introduction: Dysphagia in patients with inoperable oesophageal and gastric malignancies compromise nutrition and quality of life. Nearly two thirds of patients diagnosed with inoperable malignancy will need intervention to relieve dysphagia or stop upper GI bleeding. Therapeutic endoscopy often forms the mainstay in symptom palliation. With increasingly older patients and complexity of procedures, we assessed whether this was safe in the setting of district general hospitals.
Aims & Methods: All patients diagnosed with oesophageal or gastric cancer between 1 January 2004 and 31 December 2006 were included. Data were collected from two District General hospitals serving a total population of 500 000. All endoscopic modalities used were included and are listed below by frequency. All endoscopies were performed or supervised by consultant gastroenterologists.
Results: Over the 3-year study period, 232 patients were diagnosed with upper GI cancer (oesophageal 145, gastric 87). 58 patients were found to be suitable for surgery with curative intent (oesophageal 34, gastric 24). The rest were treated palliatively combining different modalities including chemotherapy, radiotherapy and endoscopic interventions as required. In total, 314 therapeutic upper GI endoscopies were done on 144 patients. 10 patients required a combination of different modalities. There were 5 perforations following dilatation (2 with balloon and 2 with bougie and 1 while trying to negotiate the lesion with the endoscope itself). Of these, 4 could be managed with stents while one required Celestin tube insertion. There were 3 significant GI bleeds requiring hospital admission (1 following laser and radiotherapy-died within 24 h and 2 following bougie dilatation).
Conclusion: 62% of all patients with upper GI cancers required therapeutic endoscopy over a 3-year period. Our unit has a favourable perforation rate of 2.9% for dilatation of malignancies compared with the NCEPOD data of 4.3%1 or the BSG data of 4–6%.2 Major complication rate was low at 2.5%. Most of our patients were able to eat or drink following the procedure during advanced stages of their disease. Our results are encouraging and support the safety and efficacy of therapeutic endoscopy in the palliation of symptoms for upper GI cancers in district general hospitals.
THE ROLE OF CAPSULE ENDOSCOPY IN OBSCURE GASTROINTESTINAL BLEEDING: THE LARGEST REPORTED SINGLE CENTRE SERIES
R. Sidhu1, D. S. Sanders1, J. S. Leeds1, K. Kapur2, M. E. McAlindon1. 1Department of Gastroenterology, Royal Hallamshire Hospital, Sheffield Teaching Hospitals NHS Trust, Sheffield, 2Department of Gastroenterology, Barnsley Hospital NHS Trust, Barnsley, UK
Introduction: Capsule endoscopy (CE) has revolutionised the investigation pathway of patients with suspected small bowel (SB) pathology. In patients with obscure gastrointestinal bleeding (OGB), overt bleeding (OB) or iron-deficiency anaemia (IDA), CE is the investigation of choice after negative conventional endoscopy. The diagnostic yield of CE in OGB has been reported to be between 45–80%, however there is paucity of data on which clinical factors predict the ability of CE to detect pathology.
Aims & Methods: To evaluate the diagnostic yield of CE in OGB, in routine clinical practice and the subsequent impact on patient management. We investigated which clinical factors help predict a higher diagnostic yield for CE in OGB. Patients with OGB referred for CE over 76 months were studied. Case notes were reviewed for type of OGB (overt/OB or iron deficiency anaemia/IDA), demographics, comorbidity, use of anticoagulants, non-steroidal anti-inflammatory drugs (NSAIDs), transfusion dependence, minimum haemoglobin, subsequent CE diagnosis and follow-up data. Multiple logistic regression was performed to identify factors that predicted a higher yield.
Results: There were 363 patients with a mean age of 58 years (range 17–92), 43% of referrals were from outside the region. 73% of patients had IDA and 11% of CE was performed as an inpatient (IP) setting. The overall diagnostic yield was 51% with a change in management in 34% of patients. The commonest finding was angiodysplasia in 27% of patients. In 4.7%, the capsule did not enter the colon at the end of battery life and in 3.6% SB examination failed due to either gastric retention of the capsule (n = 11) or failed transmission (n = 2). There was no significant difference in the diagnostic yield between the two groups (OB 58%, IDA 48%, p = 0.076). In 12 patients, a second CE was performed due to recurrence of symptoms: an additional yield of 33% was obtained in the second capsule group. On univariate analysis the presence of comorbidity (p = 0.002, OR 2, 95% CI 1.3 to 3.0) particularly cardiovascular (p = 0.003, OR 2.2, 95% CI 1.3 to 3.7) or liver (p = 0.003, OR 12.4, 95% CI 1.6 to 96.5), age >60 (p = 0.0001, OR 2.7, 95% CI 1.8 to 4.1), an IP setting (p = 0.001, OR 2.4, 95% CI 1.2 to 4.8) and patients who were transfusion dependent (p = 0.01, OR 2.8, 95% CI 1.3 to 6.3) were significant factors which predicted a higher yield with CE. On multiple logistic regression age >60 (p = 0.0001) and liver comorbidity (p = 0.001) remained significant although there was a positive trend towards transfusion dependence (p = 0.06).
Conclusion: This is the largest series of CE in OGB reported in the literature. Age and liver comorbidity are significant predictors of a positive diagnostic yield.
COLONOSCOPIC ULTRASOUND IS ASSOCIATED WITH A LEARNING PHENOMENON DESPITE PREVIOUS RIGID PROBE EXPERIENCE
P. N. Siriwardana1, J. Hewavisenthi2, K. I. Deen1. 1University Surgical Unit, North Colombo Teaching Hospital, 2Department of pathology, Faculty of Medicine, Ragama, Sri Lanka
Introduction: Rigid probe transrectal ultrasound (TRUS) is reliable in assessing rectal cancer. A CUS will enable total colonoscopic examination combined with wall staging in rectal cancer. Because CUS is relatively new, it is likely to be associated with a learning curve. The effect of previous experience with a rigid probe TRUS on the accuracy of CUS staging of rectal cancer is unknown.
Aims & Methods: The aims of this prospective study was to evaluate CUS predictability in preoperative staging of rectal cancer, select patients who would benefit from neo-adjuvant therapy and, to demonstrate the presence of a learning curve in the initial examinations, despite experience with a rigid probe ultrasound in examining rectal cancer. Forty four patients (21 male, 23 female; median age 64 years, range 32–88) with non-obstructing rectal cancer were assessed by colonoscopy and colonic ultrasound using a 7.5 mHz rotating transducer. Wall involvement by tumour and nodal involvement was predicted using standard criteria. Accuracy of ultrasound staging was compared with pathological staging.
Results: CUS staging versus pathology staging assessing depth of wall penetration is shown in the table. Ultrasound predicted appropriate treatment in 37 (84%) while in 7 (16%; 6 pT3 tumours and 1 pT4 tumour), it would have resulted in under-treatment. The overall unweighted kappa of CUS staging of rectal cancer was 0.18 (poor) compared to 0.94 (excellent) of TRUS. Accuracy of CUS increased from poor to good along the learning curve (fig). In 30 patients where nodes were visualized using ultrasound, the positive predictive value, negative predictive value, sensitivity and specificity were 59%, 82%, 85% and 53% respectively.
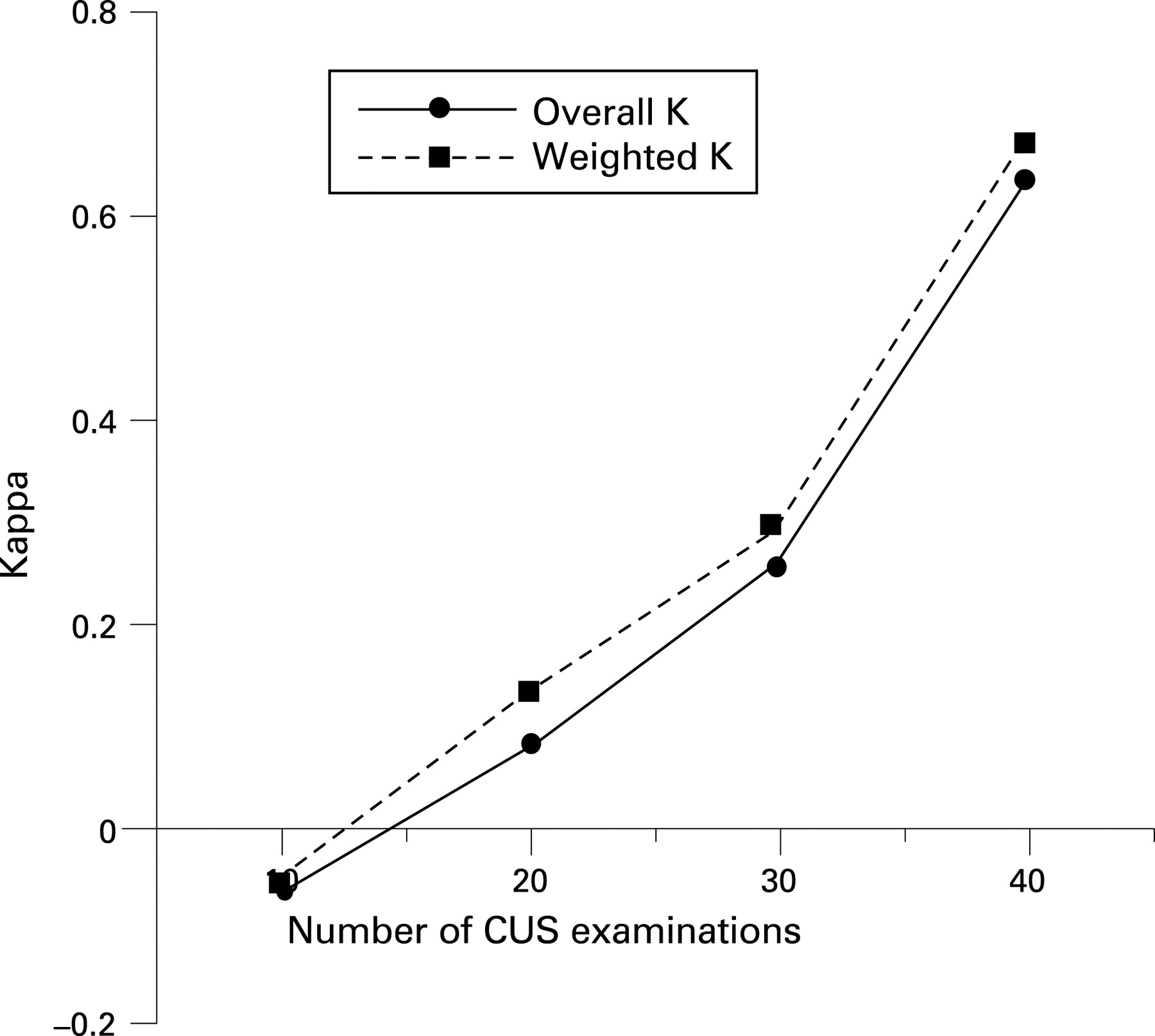
Conclusion: The predictive value in tumour staging of CUS is suboptimal in the learning phase, with a clearly demonstrated learning curve despite previous experience with TRUS.
PALLIATIVE STENTING IN MALIGNANT GASTRIC OUTLET OBSTRUCTION: A SINGLE OPERATOR EXPERIENCE
E. Matovu, H. L. Smart. Gastroenterology, Royal Liverpool University Hospital, Liverpool, UK
Introduction: Gastric outlet obstruction (GOO) occurs as a late complication of a variety of upper gastrointestinal and metastatic cancers. It is often associated with significant morbidity, coupled with severe reduction in oral intake and quality of life. This audit reports a single operator experience using self expanding metal stents (SEMS) to palliate GOO.
Aims & Methods: The endoscopy database (Unisoft Computers Limited) at the Royal Liverpool University Hospital was searched to identify patients who had undergone palliative stenting for GOO. Demographic data, procedural information and subsequent outcome were collected from a variety of sources, including review of case notes and MDT records.
Results: A total of 19 patients (mean age 75 years, 13 men) were identified as having undergone stenting for GOO between January 2006 and August 2007. The underlying diagnosis was pancreatic cancer 8, gastric cancer 5, duodenal cancer 4, cholangiocarcinoma 1 and metastatic cancer 1. In all patients the underlying disease was not amenable to curative surgery. The procedure was performed by a single operator (HLS) under conscious sedation using a therapeutic gastroscope (Olympus GIF 1T/2T 240) and radiological assistance, if needed. All patients were successfully stented using one or more SEMS (Wallstent or Wallflex Enteral, Boston Scientific; length 60–90 mm, diameter 18–22 mm) placed through the working channel of the gastroscope. There were no procedure related complications. All patients pre-procedure had varying symptoms of GOO; nausea, vomiting, and decreased oral intake. 18 patients (94.7%) showed symptomatic improvement after SEMS insertion, with return of oral intake. Subsequently during follow-up 2 patients (10.5%) required endoscopic re-intervention due to tumour in/over growth and stent blockage. The 30-day mortality after SEMS insertion was 10.5%; this was due to disease progression in all cases.
Conclusion: Palliative stenting of GOO with SEMS can be performed safely with a high technical and clinical success, allowing a return to oral intake. Re-intervention may be needed to maintain stent patency in those patients who have a more prolonged short-term survival.
ENDOSCOPIC RESECTION OF DUODENAL LESIONS
L. Smith, S. Enaganti, B. J. Rembacken. Gastroenterology, The General Infirmary at Leeds, Leeds, UK
Introduction: Endoscopic mucosal resection (EMRs) of lesions in the gastrointestinal tract is well described for oesophagus, stomach and colon. There is however, a lack of data published on EMR for lesions in the duodenum.
Aims & Methods: Retrospective data were collected on all EMRs for duodenal lesions within our centre. From 2000–6, we undertook 44 EMRs in 32 patients, including 8 patients (undergoing 19 EMRs) known to have inherited polyposis syndromes. The remaining (25/44) were sporadic lesions. All EMRs were performed by experienced endoscopists within our centre, using established “lift and cut” or the “strip biopsy” techniques.
Results: In total, 44 lesions were removed. Histology confirmed 35 adenomas, 2 intramucosal carcinomas (IMC), 2 neuroendocrine tumours and 3 non-neoplastic lesions, two polyps were not retrieved. There were two perforations (4.6%); one noted during EMR and managed endoscopically with the application of (14) metal clips. The patient made an uneventful recovery following conservative management including intravenous antibiotics. The second occurred in a patient who previously had undergone a surgical, open mucosectomy for a large duodenal adenoma and had local recurrence. This patient required emergency surgery but made a good recovery. There was one major haemorrhage (2.3%), 48 h post-EMR. Initial endoscopic therapy failed, necessitating blood transfusion and radiological embolisation. Subsequently the patient made a good recovery. Removal was regarded as endoscopically complete in 38/44 lesions (86%). The 6 lesions in which endoscopic removal was incomplete, 2 lesions failed to lift after submucosal injection due to scarring from previous EMRs, 2 lesions were too large for safe removal, 1 endoscopic resection was abandoned under conscious sedation due to restlessness and 1 procedure was abandoned after developing endoscopic evidence of perforation. It was impossible to confirm complete removal of the 19 duodenal adenomas in the 8 patients with inherited polyposis. These patients harbour many small lesions and it was impossible to distinguish local recurrence from new polyp development. In the sporadic lesions removed, 10 had no endoscopic recurrence on surveillance (ranging from 3 months to 6 years), 3 had local recurrence, 5 undergo surveillance at referring hospitals, 2 do not require surveillance, 2 were awaiting endoscopy and 3 are lost to follow-up.
Conclusion: EMR is increasingly used for the treatment of early malignancies and pre-malignant lesions. Its benefit and safety have been established within the colon, oesophagus and stomach although safety data are thin for removal of duodenal lesions. Within the experience at LGI, there were only 3 major complications but we would suggest that duodenal ER is performed within centres with on-call radiological and hepatobiliary support.
WHAT MAKES A GOOD COLONOSCOPIST?
L. Smith, B. J. Rembacken. Gastroenterology, The General Infirmary at Leeds, Leeds, UK
Introduction: Caecal intubation rate and duration of withdrawal have traditionally been regarded as the main quality benchmarks in colonoscopy. There is a wide range in the number of neoplastic lesions discovered by the colonoscopists in Leeds with the difference between the “best” and the “worst” being almost twofold. A similar wide range in polyp detection rate was noticed in 2004 during the UK Flexible sigmoidoscopy trial.1
Aims & Methods: We analysed 2913 unselected colonoscopies, carried out by 31 fully trained colonoscopists, to determine what aspects of a colonoscopy correlated with a better detection of neoplastic lesions. We constructed a ‘Polyp Detection Index’ by dividing the number of polyps detected by the number of colonoscopies performed by each endoscopist and correlated this with the individual’s unadjusted caecal intubation rate, duration of examination, average sedation doses used, number of digital images recorded, patient comfort levels, complication rate, bowel preparation and patient demographics.
Results: The polyp detection index was correlated to factors relating to the quality of the clinical examination. There was a positive correlation between polyp detection and caecal intubation rate (correlation rate 0.41), longer duration of the examination (0.38), number of weekly examinations carried out (0.45) and the average number of endoscopic images taken (0.49). We also examined the relationship of polyp detection with patient related factors. There was little or no correlation with age of the patient (0.16), ASA status (0.16), poor bowel preparation (0.15), complications (0.15) or average number of biopsies taken. There was a significant negative correlation with the average amount of sedation used (−0.59) but no association with opiate analgesia use (fentanyl (0.13) or pethidine (0.02)). There was a weak association with patient discomfort (0.27). Gastroenterologists found significantly more polyps than surgeons (614/1298 vs 158/618, χ2 test p<0.01).
Conclusion: The old quality measures of caecal intubation rates and withdrawal times do not tell the whole story when describing the characteristics of a good colonoscopist. The colonoscopists who found the most neoplastic lesions (0.43 lesions for the “best” examination vs 0.25 for the “worst”), were more likely to reach the caecum, with a longer withdrawal time, perform more colonoscopies each week, use less sedation and follow the ESGE guidelines on taking random colonic images.2
ENDOSCOPIC SUBMUCOSAL DISSECTION: EARLY EXPERIENCE IN A UK CENTRE
N. Suzuki1, B. P. Saunders1, T. Toyonaga2, T. Gunther3. 1Wolfson Unit for Endoscopy, St Mark’s Hospital, Harrow, 2Endoscopy, Kobe University Hospital, Kobe, Japan, 3Histopathology, St Mark’s Hospital, Harrow, UK
Introduction: Endoscopic submucosal dissection (ESD) is recognised in Japan as an effective therapeutic modality for the clearance of gastrointestinal neoplasms, providing an en bloc specimen to confirm lateral and deep resection margins and minimising the risk of recurrence. However, due to the technical complexity and risk of complications, few European centres have introduced this technique. This study assessed the feasibility and efficacy of ESD in a UK setting.
Aims & Methods: After gaining experience on an animal model (Erlanger), two endoscopists (NS/BPS) highly experienced in endoscopic mucosal resection performed the ESD procedures. The first 6 cases were directly supervised by a recognized expert from Japan (TT). Following submucosal injection with either hyaruolonate in the colon or saline in the stomach, incision and dissection was done with either a “Flush knife” (Fujinon) or a “Flex knife” (Olympus). Any bleeding during the procedure was treated with soft electrocautery, a “Coagrasper”(Olympus). The electrosurgical units used were ICC200 (ERBE) or VIO 200 (ERBE). The following factors; patient and lesion characteristics, sedation used, achievement of en bloc resection, histology, complications and follow-up data were recorded prospectively.
Results: Twelve colorectal and 2 gastric lesions were removed by ESD. The resected lesions were between 10 mm and 70 mm in diameter (median 30 mm) and included five “salvage” procedure where recurrence had occurred after previously attempted endosocpic snare resection. Two patients received propfol sedation and 12 patients received conscious sedation with midazolam (mean 2.52 mg) and pethidine (mean 50 mg). The mean procedure time was 112 min (20–300 min). En bloc resection was achieved in 10/14 patients. The only major complication was post polypectomy bleeding in one patient 14 days after the procedure which required a 2 unit blood transfusion but no endoscopic or surgical intervention. Twelve out of 14 patients had follow up examinations between 3–6 months after the initial procedure and 11/12 patients were free of recurrence.
Conclusion: ESD appears to be feasible and effective for the excision of selected colorectal and gastric lesions with an acceptable safety profile. However, the procedure is time-consuming and technically demanding and should only be attempted at specialist endoscopic centres.
PATIENT SATISFACTION AUDIT ON THE BOWEL CANCER SCREENING PROGRAMME ONE YEAR IN, BASED ON A SINGLE SCREENING CENTRE
A. Smith, U. Meagher, J. Cook, A. Cook, M. R. Tighe. Department of Gastroenterology, Norfolk and Norwich University Hospital, Norwich, UK
Introduction: The Norfolk and Norwich University Hospital was one of the first bowel cancer screening centres in the new programme, commencing in July 2006. In the first year, 584 patients with positive faecal occult blood tests have been referred for colonoscopic examination. We have conducted an extensive satisfaction audit to reflect on the programme from the public’s viewpoint to ascertain if we delivering what is intended.
Aims & Methods: 290 people responded to a questionnaire form 30 days after their colonoscopic examination. The form allows both for tick box and free text replies.
Results: Before attending the screening centre: 99% of people found the invitation letter and information leaflets easy to understand and useful. 47% contacted the hub for information on the freephone number, with 96% receiving a satisfactory answer. Before the colonoscopy: 100% of respondents found the pre-assessment meeting with the Specialist Screening practitioner useful. All felt they had adequate time to discuss the screening pathway and health issues, and 99% were happy with the response to their questions. 100% felt they had adequate information to make informed consent on whether to proceed to colonoscopy. The colonoscopy: 85% felt they had the right amount of sedation, while 14% felt they should have had additional sedation. From free text comments, patients who were concerned about their level of sedation related mainly to one colonoscopist, who tends to use lighter sedation—and this has been taken on board. 24% found the procedure more uncomfortable than expected, 33% as expected and 43% found the procedure less uncomfortable than expected. After the procedure: 87% felt they knew the outcome of the colonoscopy at the time of discharge and 97% were aware of follow-up arrangements prior to discharge and 89% reported that they were called the next working day to check all was well. 14% reported problems after their procedure when at home—largely discomfort from wind.
Conclusion: The bowel cancer screening programme has been very positively received in Norfolk with glowing feedback from users. The feedback emphasises the central role of the Screening practitioners in delivering the programme and as the primary point of interaction with the public. The pre-assessment visits to meet the Specialist Screening Practitioners are highly thought of by the public and worth the extra trip to the hospital. The only negative comment related to discomfort largely after the procedure, and we have now changed over to CO2 insufflation in response.
ENDOSCOPY FOR DYSPHAGIA IN YOUNG PATIENTS
T. A. Treibel, J. Mawdsley, R. Negus, J. M. Hoare, T. R. Orchard, H. J. Thomas, J. P. Teare, N. Powell. Gastroenterology, Imperial College Healthcare NHS Trust, London, UK
Introduction: Dysphagia is considered a sinister symptom that necessitates urgent referral for gastrointestinal endoscopy (GIE), chiefly to exclude oesophageal malignancy. However, GIE is costly, disliked by patients and has been associated with small, but finite risks of morbidity and mortality. There are few data available regarding GIE findings in young patients with dysphagia, in whom the risk of oesophageal malignancy is likely very small.
Aims & Methods: We conducted a retrospective, case-control study of all patients with dysphagia referred to our GIE unit over a 20-year period. We calculated the prevalence of important causes of dysphagia, including oesophageal cancer, oesophagitis and peptic strictures in young patients (aged ⩽40 years) and for comparison in elderly patients (aged ⩾65 years).
Results: We identified 455 patients aged ⩽40 years (median age 34 years, 304 males) and 1574 patients aged ⩾65 years (median age 76 years, 826 males) referred for GIE to evaluate dysphagia. The prevalence of oesophageal carcinoma was significantly lower in patients aged ⩽40 years (0%) compared to patients aged ⩾65 years (10.4%, p<0.0001). The prevalence of benign oesophageal lesions was also significantly increased in patients aged ⩾65 years compared to patients aged ⩽40 years, including peptic strictures (21.6% vs 8.8%, p<0.0001) and oesophagitis (27.4% vs 19.3%, p<0.0006). However, in patients aged ⩽40 years we did identify 5 cases of oesophageal Kaposi’s sarcoma. Four out of five cases were associated with candidiasis or oesophagitis, likely accounting for the dysphagia and were all associated with HIV infection. In patients aged ⩽40 years the prevalence of oesophageal candidiasis (5.9%) was also significantly greater than in patients aged ⩾65 years (1%, p<0.0001).
Conclusion: Malignant and benign oesophageal lesions are significantly less common in young patients (aged ⩽40 years) with dysphagia, compared to elderly patients. However, there was still an important yield of treatable lesions including peptic strictures (9%) and oesophagitis (19%). In our population of young patients, the prevalence of lesions associated with immunocompromise, including oesophageal Kaposi’s sarcoma (1%) and oesophageal candidiasis (6%) was significantly increased. These data suggest that upper GI endoscopy is still of value in the investigation of young people with dysphagia but does not need to be performed urgently (within two weeks).
THE PRODUCTIVITY TOOL
S. Varghese1, H. Avakian1, A. Ball2, R. Harvey2. 1Gastroenterology, 2Endoscopy, Bedford Hospital NHS Trust, Bedford, UK
Introduction: There has been a steady increase in demand for services from endoscopy units throughout the country. This demand has emphasized the need for proper use of capacity in endoscopy units. The National targets for March 2008 suggests that no patient should wait for more than 6 weeks for a diagnostic procedure. In order to meet these national targets and to comply with the GRS (Global Rating Score) recommendations (see http://www.grs.nhs.uk), it was essential to adopt new methods in the Endoscopy unit at Bedford Hospital NHS Trust. The “productivity tool” has the potential to improve productivity and has been used by our unit.
Aims & Methods: Data were entered retrospectively on a weekly basis on the GRS website. The data entered included the measures: capacity, activity (procedures), cancellations, waiting times, staff absences and utilisation of external staff. The aim of the tool is to provide the unit with outcomes that would identify areas for improvement.
Results: The productivity tool analysed the data provided and generated several outcomes including: Use of plant and human resource, total number of procedures and total activity points, percentage of activity done as service list, percentage of activity done as training list, effective utilisation of capacity, percentage of cancellations, shortest and longest wait periods, percentage of inpatients, percentage of staff absence due to sick or study leave and percentage of staff that are bank or agency. From the time of introduction of the productivity tool we saw a rapid rise in room use from 62% in week 1 to 100% by week 4. This level of use has been maintained in subsequent weeks. The level of activity points did not change over subsequent weeks thus suggesting adequate use of resources. There has also been a drop in the average waiting time for endoscopic procedures from a mean of 6.6 weeks (range 6.2–7.0) in July 2007 to a mean of 5.85 weeks (range 5.6–6.2) in October 2007.
Conclusion: Our experience with the productivity tool provided by the GRS has enabled us function better and provide an effective service as an Endoscopy unit. It enables us to utilise the finite resources more effectively while maintaining activity. It helps in planning and implementing additional lists with required staff to meet demands and targets thereby utilising capacity effectively. The tool is proving a valuable resource in discussions with management for additional resources. It helps visiting teams and assessors to understand the functioning and effectiveness of the unit.
FEASIBILITY OF CONFOCAL ENDOMICROSCOPY IN THE DIAGNOSIS OF PAEDIATRIC GASTROINTESTINAL DISORDERS: THE FIRST HUMAN STUDIES
K. Venkatesh1, D. P. Hurlstone2, M. Cohen3, C. Evans3, N. Tiffin4, P. Delaney5, S. Thomas5, C. Taylor1, A. Abou-Taleb1, R. Kiesslich6, M. Thomson7. 1Centre for Paediatric Gastroenterology, Sheffield Children’s Hospital, 2Department of Endoscopy, Royal Hallamshire Hospital, 3Department of Histopathology, Sheffield Children’s Hospital, 4Department of Histopathology, Royal Hallamshire Hospital, Sheffield, UK, 5Optiscan, Melbourne, Australia, 6Department of Gastroenterology, I. Med. Klink und Poliklinik, Mainz, Germany, 7Centre for Paediatric Gastroenterology, I. Med. Klink und Poliklinik, Mainz, Germany
Introduction: Confocal laser endomicroscopy is a recent development which enables surface and subsurface imaging of living cells in vivo at ×1000 magnification.
Aims & Methods: To evaluate the feasibility and utility of the confocal laser endomicroscope (CLE) in the description of normal gastrointestinal mucosa and in the diagnosis of gastrointestinal disorders in children in comparison to histology. Forty one patients (18 female) median age 10.9 years (range 0.7 to 16.6 years) with suspected or known GI pathology underwent oesophago-gastroduodenoscopy (OGD) (n = 31) and/or ileocolonoscopy (IC) (n = 29) with CLE using sodium fluorescein and acriflavine as contrast agents. Histological sections were compared with same site confocal images by 2 experienced paediatric and GI histopathologists and endoscopists respectively.
Results: Duodenum and ileum were intubated in all but one patient undergoing OGD and IC respectively. The median procedure time for OGD was 16.4 min (range 7–25 min) and for IC was 27.9 min (range 15–45 min). A total of 4368 confocal images were compared with 132 biopsies from the upper GI tract from 33 procedures and 4520 confocal images were compared with 184 biopsies from the ileo-colon from 30 procedures. Confocal images were comparable to conventional histology both in normal and in pathological conditions such as oesophagitis, H pylori gastritis, coeliac disease inflammatory bowel disease, colonic heterotopia and graft versus host disease.
Conclusion: Confocal laser endomicroscopy offers the prospect of targeting biopsies to abnormal mucosa thereby increasing diagnostic yield, with consequent reduction in number of biopsies taken, with the potential decreased burden on the histopathological services, and associated cost savings.
PRIORITIZATION OF GASTROSCOPY AND COLONOSCOPY IN PATIENTS WITH IRON DEFICIENCY: DEVELOPMENT OF A RISK ASSESSMENT TOOL
A. Ahmed1, D. Chowdhury1, D. Bowen1, D. Sheppard1, S. Paul2, K. Barbara3, R. John3, S. K. Vyas1. 1Gastroenterology, 2Research and Development Support Unit, Salisbury NHS Foundation Trust, Salisbury, 3Gastroenterology, North Hampshire NHS Foundation Trust, Basingstoke, UK
Introduction: Colonic carcinoma (5–10%) and gastro-oesophageal carcinoma (5%) may present with iron deficiency (ID). Despite the relatively high prevalence of cancer in ID patients, investigating all patients urgently with endoscopy would be challenging. A literature search failed to identify a validated strategy which could reliably identify this group of patients in need of urgent endoscopy.
Aims & Methods: This study evaluated the predictive value of 11 possible clinical variables in identifying those patients most likely to have a cancer using a logistic regression analysis. Data were collected prospectively for all new patients referred to the Gastroenterology services at Salisbury District Hospital and North Hampshire Hospital, Basingstoke. Patients had tissue transglutaminase and/or gastroscopy/colonoscopy with small bowel biopsies at the discretion of the investigating clinician.
Results: A total of 313 patients were included in the analysis. There were positive findings in 200 (64%) patients. There were 50 cancers (16%) of which 6 were gastro-oesophageal and 44 were colorectal. Logistic regression analysis revealed that age, weight loss, altered bowel habit and haemoglobin <10.5 g/dl were significant predictors of gastrointestinal cancer. The area under the associated receiver operating characteristic (ROC) curve was 0.85. A logistic probability threshold of ⩾0.09, identified from the ROC curve and jack-knifed cross-classification analysis, identified all 50 of the confirmed cancers, a threshold sensitivity of 100%. Of the remaining 263 non-cancers, 139 fell below the above threshold—that is, a specificity of 53%. In summary, the 0.09 rule identifies a subset of endoscopy referrals at significantly greater risk (about 30%) of gastrointestinal malignancy.
Conclusion: All patients with iron deficiency who are at high risk of malignancy need to be investigated urgently. This initial study suggests a simple rule for identifying such patients. The rule has 100% sensitivity with sufficient specificity to warrant further investigation of its role in management of patients with ID. The logistic risk assessment tool has been translated into a nomogram to facilitate direct and easy access to calculation of the risk of malignancy.
A MODEL OF TEACHING ENDOSCOPY
C. W. Wells, S. Corbett, M. R. Welfare, J. R. Barton. Research and Development, Northumbria Healthcare NHS Foundation Trust, North Shields, UK
Introduction: Endoscopy training in the UK has improved through the establishment of endoscopy training centres. Most training is still done at the trainee’s base hospital, where further improvements could be made.1 There is little research on how best to teach endoscopy. The production of a model of ideal endoscopy training will help guide trainers.
Aims & Methods: In depth, semi-structured interviews (n = 20) were conducted with members of four stakeholder groups in the UK endoscopic community: national experts, regional trainers, regional trainees and nurse endoscopists. They were asked to identify attributes of an ideal endoscopy trainer. The interview transcripts were analysed using the framework technique.
Results: A number of components in the endoscopic teaching process were identified. Central is the scaffolding of support by the trainer, with initial high input from the trainer which gradually fades away as the trainee progresses:
This support initially includes demonstration (occasionally taking over the scope) and direct instruction
As training progresses the volume of input from the trainer reduces and the quality of input changes (from instruction to prompting to questioning to reassuring) allowing the trainee to develop independent practice
The trainer is available throughout to deal with specific difficulties
The trainer physically withdraws as training progresses
Key skills for the trainer include:
Being proficient at performing endoscopy
Being able to closely analyse & understand the performance of the trainee to identify areas for improvement
The ability to provide specific constructive feedback in a supportive manner
The ability to adapt teaching to meet the needs of the trainee
Motivation needs to be maintained by providing a supportive, safe, constructive and relaxed learning atmosphere. This atmosphere is established by the trainer through:
Patience
Good communication
Enthusiasm
Empathy for the anxieties of trainee
Encouragement
Being non-judgemental
Confidence in his/her own teaching ability
Being present in endoscopy room
Concentrating on teaching
Preparation of lists to meet trainee’s needs (avoiding pressure on time)
Support
Respect for patient and nurses
Building a close relationship with trainee
Conclusion: Some of the identified concepts map onto existing models of teaching and learning.2–4 Others are more specific to the teaching of a complex psychomotor skill, an area which has been under-investigated in medicine. The findings of our study could be used to help endoscopic trainers evaluate and enhance their own teaching. This has the potential to lead to further improvements in endoscopic teaching within the UK.
RIGID, FLEXIBLE, OR THE WHOLE COLON?
D. Woolf, A. J. Kent, L. Sibthorpe, J. McCue, S. M. Greenfield. Gastroenterology, Queen Elizabeth II Hospital, Welwyn Garden City, UK
Introduction: Colorectal cancer (CRC) is the third most common cause of cancer deaths in the UK. A large percentage of referrals to secondary care are for the investigation of suspected CRC though most patients have minor pathology. It is therefore important to ensure investigations are used appropriately and are matched to the presenting symptom whilst considering the risk, cost and availability of the procedure.
Aims & Methods: We reviewed the presenting symptoms of CRC, and how symptoms influence choice between flexible sigmoidoscopy (FS) and colonoscopy. Furthermore, we evaluated whether we are using the investigatory tests for CRC in a safe and appropriate manner. We interrogated the endoscopic and CRC (“Infoflex”) databases, for patients diagnosed with CRC between April 2005 and March 2006 inclusive. Information was gathered which included symptomatology, primary investigation and site of cancer. We obtained hospital or GP records for any details not gathered from these databases.
Results: A total of 153 patients were diagnosed with CRC between April 2005 and March 2006. 36.6% (56) of these had rectal or anal cancer which theoretically should be seen on rigid sigmoidoscopy. Of this group 44.6% (25) were diagnosed with a rigid sigmoidoscope whereas the remainder were diagnosed by formal endoscopy (colonoscopy or FS). 22/153 patients (14.4%) presented solely with rectal bleeding. All of these had left-sided cancers but 14 (64%) had a colonoscopy as their first investigation. One patient (0.7%) had rectal bleeding with a right-sided cancer, but he also presented with anaemia and weight loss. 26/153 (17.6%) FS were performed although 50% of these did not have symptoms solely suggestive of left-sided disease but had anaemia/weight loss.
Conclusion: Investigations should be tailored to the presenting symptom. Patients who present with rectal bleeding as their sole symptom should have a FS. This will avoid an unnecessary colonoscopy for many patients who have minor pathology. If we assume our sample is representative of the average patient being investigated for rectal bleeding, then two thirds will have an inappropriate colonoscopy using up vital resources and increasing risk to the patient. Conversely patients with symptoms suggestive of right-sided lesions should have a colonoscopy rather than FS to avoid repeated investigation and the risk of missing a CRC. A consultant gastroenterologist now vets all requests for FS or colonoscopy to ensure the correct investigation is requested. Our data suggest that there might be an increasing role for rigid sigmoidoscopy, as a safe and speedy investigation in clinic.
ENDOSCOPIC ANTI-REFLUX THERAPY WITH THE ESOPHYX ENDOLUMINAL FUNDOPLICATION DEVICE: RESULTS OF THE FIRST UK STUDY
P. L. Youd1, A. Emmanuel2, E. Tripoli1, A. Roy2, J. Harris3, K. Koniezcko3, C. Fraser1. 1Wolfson Unit for Endoscopy, Imperial College London, 2Department of Physiology, University College Hospital, London, 3Department of Anaesthetics, Northwick Park Hospital, Harrow, UK
Introduction: The EsophyX anti-reflux device is a novel endoscopic technology for the treatment of patients with gastro-oesophageal reflux (GOR). Multiple full thickness fasteners are used circumferentially to create an endoluminal fundoplication with reconstruction of the gastro-oesophageal valve (GOV). St Mark’s Hospital is the first hospital in the UK to perform this procedure and we report our experience to date.
Aims & Methods: All patients had PPI-dependent GOR in the absence of Barrett’s oesophagus, hiatus hernia >3 cm or oesophageal dysmotility. Jobe length and Hill grade of the GOV and oesophageal physiology were measured pre- and post-procedure and the circumference of the new valve was recorded. Outcome measures included: (1) complications, (2) quality of life indicators (GORD-HRQL and Reflux-Qual), (3) medication use and (4) changes in oesophageal physiology.
Results: 15 patients (m = 13) were recruited. The mean number of fasteners deployed was 13 (5–19) to create a mean valve circumference of 237 degrees (160–290). Jobe length increased from mean 0.9 cm to 3.7 cm and median Hill grade improved from 2 to 1. 14 patients were discharged after overnight admission while one needed an extra day in hospital in view of transient pyrexia. One procedure was repeated due to fastener fall-out within the first week. Mean pain score at 24 h was mild to moderate. Patients returned to normal daily activities by mean 10.7 days (4–28) and resumed a normal diet by mean 13.8 days (10–21). There were no reports of pain, dysphagia or bloating >10 days post-procedure. 10 out of 15 patients (67%) remain completely off PPIs after a mean follow-up of 6 months. Of the 5 patients with >6 months’ follow-up data, 2 patients remain asymptomatic (A, B), 1 patient had symptom recurrence after 6 months (C), 1 patient proceeded to Nissen fundoplication (D) and in 1 patient the procedure failed due to a large hiatus hernia (E) (table).
Conclusion: While our experience of the EsophyX device continues to develop, our initial findings suggest it is possible to achieve a good outcome with respect to side effect profile, quality of life indicators and PPI requirements for some patients with GOR. Current follow-up physiology data remain inconclusive. Follow-up data on all 15 patients will be available within the next 5 months.
Gastroduodenal posters
OPPOSING TRENDS IN THE COMMUNITY PREVALENCE OF PEPTIC ULCER, GASTRO-OESOPHAGEAL REFLUX DISEASE AND BARRETT’S OESOPHAGUS IN ENGLAND AND WALES, 1996–2005
K. Alexandropoulou1, J. Van Vlymen2, A. Majeed3, A. Poullis1, J. Kang1. 1Gastroenterology, 2Biomedical Informatics, St George’s Hospital, 3Primary Care and Social Medicine, Imperial College, London, UK
Introduction: Few data are available regarding the burden of peptic ulcer disease (PUD), gastro-oesophageal reflux disease (GORD) and Barrett’s oesophagus (BO) with studies mainly focusing on hospital admissions and outcomes. Helicobacter pylori eradication and proton pump inhibitors (PPIs) introduced in the 1990s have had a significant impact on the management of these conditions. Furthermore, over the same time, an increasing incidence of oesophageal adenocarcinoma has focused attention on Barrett’s, a recognised complication of longstanding GORD. Most patients with these conditions are treated symptomatically in primary care. The period prevalence of peptic ulcer from 1994–8 was previously studied using the GPRD.1 Over this five-year period, the prevalence of peptic ulcer decreased by half. Our study aimed to extend the data on PUD and obtain also prevalence trends for GORD and Barrett’s over the study period, 1996–2005.
Aims & Methods: GPRD is the General Practice Research Database, where approved GP practices in England and Wales, following agreed guidelines, record clinical and prescribing data on all their patients, whose identity is anonymised. OXMIS and READ codes for the conditions of interest were used to identify patients with a diagnosis of peptic ulcer disease and gastro-oesophageal reflux (and oesophagitis) and Barrett’s oesophagus. Retrieved data were used to calculate annual sex- and age-specific prevalence rates for these conditions.
Results: There was an expected decline in the prevalence of peptic ulcer disease, from 2.4/1000 population in 1996 to 0.7/1000 population in 2005, a 70% decline. This was mainly due to a 75% reduction in duodenal ulcer prevalence from 1.4 to 0.34/1000 population and particularly among women aged <34 years. There was a more modest 40% drop in gastric ulcer prevalence from 0.5 to 0.3/1000 population The prevalence of GORD remained stable but that of BO increased markedly from 0.14 to 0.44/1000 population, a threefold increase over the study period.
Conclusion: We had previously shown a decline in the community prevalence of peptic ulcer disease between 1994–8, and this trend has continued on till 2005, especially among younger individuals, consistent with the effect of eradication of Helicobacter pylori in the community. The community prevalence of BO increased markedly but contrary to our expectations, that of GORD remained stable over the study period.
HELICOBACTER PYLORI-INDUCED GASTRIC EPITHELIAL SIGNALLING RESPONSES ARE MODIFIED BY EPSTEIN-BARR VIRUS LMP2A
K. Danjo1, C. Dawson2, K. Bransfield1, P. A. Robinson1, L. S. Young2, J. E. Crabtree1. 1Leeds Institute of Molecular Medicine, St James’s University Hospital, Leeds, 2Cancer Research UK Institute, University of Birmingham, Birmingham, UK
Introduction: Helicobacter pylori activates several signalling pathways in gastric epithelial cells of relevance to epithelial hyperproliferative responses and gastric carcinogenesis. H pylori-induced activation of extracellular-signal related kinase 1/2 (ERK1/2) is both via epithelial translocation of CagA, and in a cag pathogenicity island (PAI)-independent manner. ERK activation by H pylori is considered, in part, to be via tyrosine kinase receptors such as the epidermal growth factor receptor (EGFR). Epstein-Barr virus (EBV) has also been linked to the development of gastric cancer. The consequence of concomitant infection of EBV on H pylori-induced epithelial signalling responses has not been investigated.
Aims & Methods: The aim of this study was to examine H pylori induced ERK1/2 activation in AGS gastric epithelial cells containing (a) rEBV (b) LMP2A (EBV latent-membrane associated protein 2) (c) rEBV minus LMP2A and (d) AGS neo (control). Gastric epithelial cell lines were stimulated with H pylori cag PAI+ strain G27 and G27cagM- with a non-functional cag PAI, and phosphorylation of ERK1/2 was measured from 20–180 minutes post-stimulation using a quantitative In Cell Western assay (ICW).
Results: H pylori induced pERK1/2 in AGS rEBV cells was increased relative to AGS/AGS neo cells at early time points (20 and 45 min) following stimulation with G27cagM-, but not with the cag PAI+ G27 strain. In AGS+LMP2A cells pERK1/2 was significantly decreased compared to AGS/AGS neo cells following stimulation with both G27 and G27cagM- strains. EKB-569, an EGFR inhibitor, blocks H pylori-induced ERK1/2 activation in AGS cells by circa 30%. To determine whether the effect of LMP2A on H pylori-induced ERK1/2 activation in AGS + LMP2A cells was mediated by changes in function of the EGFR, AGS + LMP2A and AGS/AGS neo cells were incubated with EGF (1 ng–100 ng/ml) for 10 min, and the level of pERK determined by ICW assay. EGF induced similar levels of ERK1/2 activation in AGS and AGS neo cells. In contrast, in AGS+LMP2A a significant reduction (p<0.01) in the ERK1/2 phosphorylation was observed at all EGF concentrations.
Conclusion: These studies demonstrate that EBV infection of AGS cells alters H pylori induced activation of ERK1/2 in a strain dependent manner. The reduced responsiveness of AGS +LMP2A cells to EGF suggests the impaired H pylori activation of ERK1/2 in AGS + LMP2A cells is a consequence of impaired EGFR signalling.
PREDICTING BENIGN POLYPS AT GASTROSCOPY: DO ALL GASTRIC POLYPS NEED TO BE BIOPSIED?
C. J. Crooks, A. Stokes, A. F. Goddard. Department of Gastroenterology, Derby City General Hospital, Derby, UK
Introduction: Gastric polyps are a heterogeneous group of histological entities with differing malignant potential. For instance fundic gland polyps have low malignant potential and occur in normal mucosa. In contrast hyperplastic and adenomatous polyps have higher malignant potential and occur in inflamed and abnormal mucosa. Endoscopically identifying sporadic fundic gland polyps from other polyp types would allow more selective biopsies to be taken, saving time and money.
Aims & Methods: This study aimed to identify whether fundic gland polyps were similar to other polyp types in age, sex, site, size and number. We identified consecutive patients over 3 years at Derby hospitals who had gastric polyps identified at endoscopy by a single operator. The pathology reports were obtained for the histological diagnoses. Age and sex of patients along with site, size and number of polyps identified at gastroscopy were recorded.
Results: A total of 1518 gastroscopies (female 51%, mean 60 years) were performed over the 3 years by a single operator. Of these 139 patients (female 59%, mean 63 years) had gastric polyps identified. 131 patients were biopsied (see table). Metaplasia occurred in all locations within the stomach and occurred as frequently with a solitary polyp as with multiple polyps. The neuroendocrine carcinoma occurred as a solitary 4 mm polyp. Size, site and number of polyps did not differentiate between polyp types. All polyps excised in patients younger than 50 years were benign (20 patients out of 139 patients).
Conclusion: The proportions of polyp types identified in this study were similar to previously published series. In this study size, site and number of gastric polyps do not allow differentiation between fundic gland and other polyp types. Therefore we suggest all gastric polyps and their surrounding mucosa should be biopsied at gastroscopy to assess for metaplastic and dysplastic changes.
SMOKING AND GENDER INFLUENCE THE CELLULAR IMMUNE REACTION TO H PYLORI AND COULD CONTRIBUTE TO DISEASE RISK
N. R. Hussein, K. Robinson, J. C. Atherton. Wolfson Digestive Diseases Centre and Institute of Infection, Immunity and Inflammation, University of Nottingham, Nottingham, UK
Introduction: H pylori induces adaptive immunity, but the balance of the response varies between individuals. Since a more pro-inflammatory T-helper 1 (Th1) response is linked with the development of gastric adenocarcinoma, we investigated the expression of Th subset-associated cytokines and a regulatory T-cell gene in gastric biopsy samples from the UK and Iraq (where there is a low incidence of gastric cancer). Associations of smoking and gender with the cytokine responses were also investigated.
Aims & Methods: 44 (35 H pylori-infected) and 52 (39 H pylori-infected) gastric biopsies were collected from patients with different clinical outcomes, in Iraq and the UK respectively (infected: Iraq: peptic ulcer (PUD) = 15, non-ulcer = 29; UK: PUD = 14, non-ulcer = 25, all non-infected = non-ulcer). Real-time PCR was performed to quantify the levels of interferon-γ (IFNγ), interleukin-4 (IL-4) and FOXP3 mRNA, which are indicative of Th1, Th2 and Treg responses respectively. Serum IgG subsets were measured by ELISA.
Results: In both populations, the level of FOXP3, IL-4 and IFNγ mRNA was found to be elevated in samples from infected patients compared to those from H pylori-negative patients (p<0.01, p<0.0001, p<0.0006 respectively). No significant differences were found between the samples from Iraq and the UK. Interestingly, we found high IFNγ mRNA levels to be associated with smoking (mean±SEM, smoker 93±27, non-smoker 16±10 p<0.009), and elevated IL-4 mRNA levels with female gender (female 146±36, male 18±7 p<0.005). Next, to confirm our results, we studied serum IgG subsets response to H pylori. Our results showed that there was a significant difference in the IgG1 response (low level indicates Th1 response) between smokers and non-smokers (smokers 2797±657, non-smokers 6239±717, p<0.05). Additionally, we found an inverse relationship between the gastric IFNγ mRNA level and the IgG1 response in peripheral blood (p = 0.011).
Conclusion: As no differences were seen between samples from Iraq and the UK, differences in Th and Treg response appear unlikely to explain the differences in gastric cancer incidence between these countries. The association between high Th1 response and smoking suggests that smoking may promote a pro-inflammatory Th1 response: such a response is known to induce precancerous gastric atrophy and metaplasia. The association between female gender and a higher IL-4 (Th2) response may help to explain the lower gastric cancer incidence in women.
THE CHANGING PATTERN OF PEPTIC ULCER DISEASE IN LONDON
N. Powell, T. Treibel, J. Mawdsley, R. Negus, J. P. Teare, T. R. Orchard, H. J. Thomas, J. M. Hoare. Gastroenterology, Imperial College Healthcare NHS Trust, London, UK
Introduction: With the introduction of proton pump inhibitor (PPI) therapy in the late 1980s, improved diagnosis and treatment of Helicobacter pylori infection, and changes in non-steroidal anti-inflammatory drug (NSAID) prescribing, the epidemiology of peptic ulcer disease (PUD) is thought to be changing.
Aims & Methods: We retrospectively analysed data from more than 45 000 upper gastrointestinal (GI) endoscopies performed in our unit between 1985 and 2006 inclusive. We identified all benign gastric and duodenal ulcers of at least 5 mm diameter diagnosed at endoscopy. We excluded malignant ulcers, oesophageal ulcers (except at the gastrooesophageal junction) and ulcers observed in the same patient on repeat endoscopy if performed within 6 months of the index endoscopy. We also excluded incomplete endoscopies. Data were collected regarding ulcer prevalence and characteristics including size, depth and anatomical distribution.
Results: Peptic ulcers were present in 2513 (5.6%) of 45 192 upper GI endoscopies performed during the defined time period. The prevalence of PUD diagnosed at endoscopy has fallen from 8.9% in the 1980s to 6.2% in the 1990s and 4.1% in the 2000s (p<0.0001 for all comparisons). This pattern was also observed in peptic ulcers >10 mm in size (4.3% in 1980s, 2.4% in 1990s and 1.5% in 2000s, p<0.0001 for all comparisons). The proportion of ulcers >10 mm in size has also fallen significantly from 48.4% in the 1980s, to 38.6% in the 1990s (p<0.0007) and 36.0% in the 2000s (p<0.0001). Mean ulcer size in the 1980s (12.7 mm) was also significantly larger than in the 1990s (9.4 mm, p<0.0001) and 2000s (9.5 mm, p<0.0001). The proportion of ulcers described as “deep” rather than “superficial” was also significantly higher in the 1980s (52.3%) compared to 1990s (42.2%, p<0.0002) and 2000s (45.8%, p<0.03). However, the proportion of peptic ulcers located in the duodenum (rather than stomach) has not significantly changed over the study period (61.9% in the 1980s, 64.3% in the 1990s and 59.2% 2000s).
Conclusion: The prevalence of PUD has significantly fallen since 1985 in patients undergoing endoscopy. Peptic ulcers in the 1990s and 2000s are also significantly smaller and more superficial than ulcers in the 1980s. The anatomical distribution of peptic ulcers does not appear to be changing.
30 DAY MORTALITY AFTER PEPTIC ULCER PERFORATION AND THE USE OF LOW-DOSE ASPIRIN AND NON-STEROIDAL ANTI-INFLAMMATORY DRUGS
A. S. Taha1, W. J. Angerson2, R. Prasad1, C. McCloskey1, D. Gilmour1, C. G. Morran2. 1Gastroenterology, Crosshouse Hospital, Kilmarnock, 2Surgery, University of Glasgow, Glasgow, UK
Introduction: Low-dose aspirin has been increasingly used in cardiovascular and cerebrovascular prevention, while the use of non-steroidal anti-inflammatory drugs (NSAIDs) has been changing in recent years. Little is known about the outcome of peptic ulcer perforation in light of these changes.
Aims & Methods: We aimed to assess the 30 day mortality after peptic ulcer perforation in association with the use of low-dose aspirin (75 mg/day) and NSAIDs while considering the presence of other risk factors. Therefore, we studied all patients with first attack of peptic ulcer perforation who presented over a 10 year period to our institution. We recorded details of their demography, drug intake, coexisting conditions, management, and outcome including death. The mortality rate ratios were computed using Cox’s regression analysis with censoring at 30 days after perforation.
Results: In 270 patients hospitalised for peptic ulcer perforation, the unadjusted mortality rate ratios (MRR), using univariate analysis, were as shown in the table. Multivariate analysis showed only the following to be independently significant covariates: other drugs: adjusted MRR, 7.79 (95% CI, 1.06 to 57.47), p = 0.044; cerebro-vascular disease, 3.35 (1.62 to 6.94), p = 0.001; and other diseases, 2.20 (1.06 to 4.58), p = 0.034.
Conclusion: Low-dose aspirin, unlike NSAIDs, is associated with a twofold increase in early mortality after peptic ulcer perforation. However, mortality was more strongly and independently associated with other comorbid conditions.
LYMPHOCYTIC DUODENOSIS: CLINICAL PRESENTATION AND INVESTIGATION IN A RETROSPECTIVE STUDY OF 55 PATIENTS
M. Rahim1, J. Macnaughtan2, J. Hoare2, R. Negus2, M. M. Walker1. 1Histopathology, Imperial College London, 2Gastroenterology, St Mary’s Hospital, London, UK
Introduction: Lymphocytic duodenosis (LD) may represent the early manifestation of coeliac disease and is defined histologically as an intraepithelial lymphocyte count (IEL) of greater than 25 per 100 enterocytes in the context of normal villous architecture. However, this histological diagnosis is also associated with hypersensitivity to non-gluten proteins, infection, autoimmune disorders and drugs. Between October 2004–5, a histological diagnosis of LD was made in 91/920 duodenal biopsies taken in our unit (9.89%).
Aims & Methods: The aims of this study were to characterise the clinical features of patients with LD and to assess their subsequent investigation and management. 55 patients with LD were selected at random from the histopathology files. 40 patients with normal duodenal biopsies and 30 patients with villous atrophy (VA) were selected as a control group. Data were extracted from the records of these patients with regard to clinical presentation, investigations performed, subsequent management and follow-up.
Results: Common symptoms of patients with LD in this study were abdominal pain (62%), diarrhoea (40%), weight loss (24%), abdominal bloating (24%) and nausea (20%). These symptoms were also common in patients with normal duodenal biopsies. However, 14.5% of LD patients were found to have arthralgia (p = 0.023) and 22% a past medical history of autoimmune disease (p = 0.004). Non-steroidal anti-inflammatory use was similar amongst all the groups. 7.3% and 6.7% of the LD and VA patients were underweight at presentation. 24 of the 55 LD patients were found to have an anaemia of which 19 were iron deficient. Coeliac serology was found to be positive in 23% of the cases in which it was performed (p = 0.025). H pylori status was only determined in 35% of LD patients. Colonoscopy was performed in 30 LD subjects of which 17 had abnormal findings (IBD (1), colonic polyps (10), microscopic colitis (2), other (4)). 58% of LD cases did not have an identified aetiology.
Conclusion: LD occurred in 1/10 of routine duodenal biopsies. In this large series, the clinical presentation of patients with LD in our study overlaps with that of coeliac disease and concurs with previous data. Serological markers are the most important investigation to exclude the diagnosis of coeliac disease in patients with LD. If coeliac serology is negative these patients should be further investigated to identify other conditions which may be amenable to treatment.
Health service research and IT posters
MEASUREMENT OF PATIENT FOCUSED OUTCOME ROUTINELY IN CLINICAL PRACTICE: FEASIBILITY AND CLINICAL VALUE
F. Ali1, S. Gaze2, D. Russell3, I. Russell3, J. Williams2. 1Department of Gastroenterology, Neath Port Talbot Hospital, Port Talbot, 2School of Medicine, Swansea University, Swansea, 3Institute of Medicine & Social Care Research, Bangor University, Bangor, UK
Introduction: The need to involve patients more actively in decisions about their care is recognised in the NHS Plans for England and Wales. Central to this is the ability to measure a patient’s progress from their own perspective which can be assessed by patient completed health-related quality of life (HRQL) questionnaires.
Aims & Methods: To assess the feasibility of patients routinely completing electronic questionnaire about their health-related quality of life, in a busy gastroenterology out-patient department, and for doctors to use this information—does this intervention improve process of care and patient outcome? A pragmatic single centre randomised controlled study was carried out between August 2006–April 2007. The intervention used was the electronic GSRQ/EQ-VAS health-related quality of life questionnaire. Patients randomised into 3 groups. The intervention group completed electronic GSRQ in clinic and had HRQL information available to clinicians during the consultation. Repeat measurements used to follow-up patients over a 4-month period. The primary outcome measures were the SF36 and EQ5D scores. Secondary outcomes included patient satisfaction, clinic waiting times and consultation lengths. A qualitative study was also carried out through self completed questionnaires to explore the views and attitudes of the patients and staff.
Results: 505 patients recruited into the study. Mean age 54.3 years (range 16–91 years). 295 females:210 male. There was no difference in health outcome scores between the groups. Electronic questionnaire completion was very high at 97.6% (330/338) with mean completion time of 6 min 31 s. There was no difference in patient waiting times or consultation lengths. There was some impact on management decisions with significant difference in drug prescription (16% vs 8.7%, p<0.05) and the number of follow-ups (mean 1.6 vs 1.35, p 0.007) between intervention and control groups. Patient satisfaction was very high in all three groups. The qualitative study showed that most patients and clinicians found the process feasible. Completing the questionnaire helped patients to discuss their condition and acting as a “memory-jogger” or helping them “organise their thoughts”. Staff did not report any major issues regarding the process.
Conclusion: It is feasible to use the electronic GSRQ routinely in clinical practice to monitor patient related outcomes in patients with gastrointestinal disorder. Although health outcomes did not change patients do find the questionnaire helpful and it may help in the process of care.
DOES THE DETECTION OF HEPATITIS C MATCH THE DISTRIBUTION OF METHADONE PRESCRIPTIONS AND MULTIPLE DEPRIVATION IN SCOTLAND?
T. E. Astell-Burt1, R. T. Flowerdew1, P. J. Boyle1, J. F. Dillon2. 1School of Geography and Geosciences, University of St Andrews, St Andrews, 2Ninewells Hospital and Medical School, Ninewells Hospital, Dundee, UK
Introduction: By December 2006, approximately one in 260 of Scotland’s population had been diagnosed with Hepatitis C. It is estimated that the number of people infected with Hepatitis C remaining undiagnosed exceeds those known by a factor of 1.5. The lowest rates of referral of Hepatitis C patients are in more remote, rural locations. Some geographical factors that might explain this could be: poorer Hepatitis C screening practices; poorer access to treatment centres; and a lower exposure of rural populations to the major risk factors. Recent work in France suggests that geographic access to medical care may affect the diagnosis of Hepatitis C.1 Unfortunately, that research did not control for the substantial difference in the number of Hepatitis C diagnoses expected between urban and rural areas, due to injecting drug use.
Aims & Methods: This paper tests the spatial inequality of Hepatitis C detection and the likely distribution of injecting drug use in Scotland. Negative binomial regression methods are used to examine the detection of approximately 20 000 Hepatitis C anti-body positive tests and surrogate indicators of injecting drug use: (1) area deprivation; (2) methadone prescriptions.
Results: Positive relationships were found between Hepatitis C antibody positive tests, deprivation, and methadone prescriptions in increasingly urban areas.
Conclusion: Hepatitis C has been detected throughout Scotland, but is not evenly spatially distributed. People diagnosed with Hepatitis C are likely to live in urban areas characterised by high levels of deprivation and high numbers of methadone prescriptions. This information will be used in a follow-up study, building on and increasing the sophistication of previous research, which questions whether geographic access to healthcare influences the detection of Hepatitis C in Scotland.
ENGAGING CLINICIANS WITH THEIR NHS DATA: PILOT PHASE AND LAUNCH OF A NATIONAL PROJECT FOR GI PHYSICIANS
K. Bodger1, C. Grant-Pearce2, M. Pearson2. 1Department of Medicine, Clinical Science Centre, University Hospital Aintree, 2Clinical Evaluation, University of Liverpool, Liverpool, UK
Introduction: The NHS collects routine administrative data (Hospital Episode Statistics, HES) on inpatient care. Work by the RCP (iLab 2006) highlighted data limitations yet HES data inform Payment-by-Results. We report a national project seeking to engage GI specialists with their data to drive improvements in accuracy and promote clinically-driven, logical analysis.
Aims & Methods: (1)To develop analyses of HES data to generate valid “reports” (for example, speciality and general workload, casemix, selected “outcomes” such as length-of-stay, LOS) by engaging feedback with GI specialists. Phase I: Data for one unit (teaching hospital serving >330 000 patients) used to generate analysis of in-patient spells for GI and non-GI physicians and a classification scheme based on grouping primary diagnostic field (ICD-10 diagnosis) into logical “baskets”. Case volume and LOS was computed. Phase II: Entire UK HES dataset obtained and draft reports in progress for dissemination to pilot group prior to National roll-out.
Results: Phase I: Of 2521 admissions under GI physicians, 1923 (76%) had a GI diagnosis (enteric infections: 2%; benign upper gut disorders 21%; benign lower gut disorders 14%; benign pancreaticobiliary disease 7%; hepatology 15%; GI cancer 9%; anaemia 6%; non-GI alcohol-related 15%; miscellaneous 12%). The “top three” primary coded diagnoses at this Trust were: (1) mental and behavioural disorders due to use of alcohol (F10); (2) alcoholic liver disease (K70) and (3) other non-infective gastroenteritis and colitis (K52). Average LOS by ICD-10 code varied from 1.7–47.3 days for GI and 1–54 for non-GI diagnoses. Average LOS correlated closely with age.
Conclusion: For analysis of HES data to be of value to local teams and patient care, specialists need to engage with the data collected about their activity to ensure that coding errors and local anomalies are corrected and that the analyses are clinically logical. Crude statistics, such as LOS, have little meaning without correction for casemix and age profile.
FAST-TRACK SERVICES FOR UPPER GASTROINTESTINAL CANCER: PATIENT SCREENING TOOL TO DETECT DELAYED AND INAPPROPRIATE TWO-WEEK RULE REFERRALS AND SURVEY OF GENERAL PRACTITIONER PREFERENCES FOR SERVICE ORGANISATION
G. Pritchard1, N. Kapoor1, R. Sturgess1, K. Bodger2. 1Digestive Diseases Centre, 2Department of Medicine, Clinical Science Centre, University Hospital Aintree, Liverpool, UK
Introduction: The “Two-Week Rule” (TWR) aims to improve early diagnosis of cancer by fast-track referral to a specialist for patients with alarm symptoms. Various models of delivery have been applied (for example, direct-to-test versus fast-track clinic). Trusts are monitored to ensure TWR referrals are seen but there are no systems to assess timeliness of referral into the system from primary care (“delayed” referrals) nor whether some referrals fail to meet the TWR criteria (“inappropriate” referrals). General practitioner (GP) preferences for different models of service are not known. A patient and GP questionnaire were designed to address these questions.
Aims & Methods: Setting: a rapid access upper gastrointestinal cancer service (RAUGICS) based at a university hospital in North Liverpool, UK. The service has the highest volume of TWR referrals in the UK.1 Patient survey: self-administered patient questionnaire containing previously validated symptom scores for dyspeptic and “alarm” symptoms plus items about preceding consultations, investigations and treatment (The Aintree Rapid Gastroscopy Evaluation Tool, TARGET) was sent to all TWR referrals. Patient responses were compared to information provided by the GP in the referral proforma. Possible “inappropriate” referral was defined as absence of a TWR referral criterion in patient-elicited responses. GP survey: postal survey of all GP surgeries referring to RAUGICS (identified as mean referral volume >1 case per annum over 5 years; n = 92 practices). Non-respondents received a second mailing. Items asked about preferred model of initial evaluation and patient follow-up.
Results: Patient survey: data for first 474 respondents (mean age 63 years). Symptom duration >6 months in 35%; Time from first consultation to referral >6 months in 20%; 3 or more GP consultations before referral in 34%. Based on TARGET symptom data, “inappropriate” referral in 6.64% of cases overall (higher for dyspepsia with an alarm feature compared to dysphagia, 8.89% vs 1.32%, p<0.05). Primary care survey: Survey response rate 80% (74/92). Preferred model of TWR assessment: direct-to-test, 74% (single partner 65% vs multipartner 89%); gastroenterology clinic, 14.9%; surgical clinic, 0%; no preference, 12.2%. Preferred follow-up after gastroscopy: RAUGICS system (selective follow-up for serious pathology or ongoing symptoms on telephone review), 78.4%; hospital follow-up of all TWR referrals, 6.7%; no preference, 14.9%.
Conclusion: The TARGET questionnaire identified possible delays in consultation and referral for at least 1 in 5 patients with alarm symptoms referred under TWR but the rate of “inappropriate” referrals is low. The tool may improve case identification for TWR referral. GP survey indicated a preference for the RAUGICS model of direct-to-test followed by selective follow-up for suspected upper GI cancer. Improved patient and GP education are required to encourage earlier access into the system.
DEVELOPMENT OF A WEB-BASED E-LEARNING MODULE TO IMPROVE LESION RECOGNITION AT CAPSULE ENDOSCOPY
A. J. Postgate, A. V. Haycock, S. Thomas-Gibson, A. Fitzpatrick, S. Preston, C. H. Fraser. Wolfson Unit for Endoscopy, Imperial College London, London, UK
Introduction: The use of capsule endoscopy (CE) in the UK for investigating suspected small bowel disease is rapidly increasing and the service is now devolving from tertiary centres to local hospitals. However there are few training opportunities and there is no established accreditation process. Local units are unlikely to be exposed to sufficient volume to allow for adequate training. Unlike flexible endoscopy training, the lesion recognition skills required for CE are ideally suited to web-based e-learning. This would offer exposure to a wide range of pathology in an interactive learning environment which is independent of time and place. St Mark’s Hospital is a national training centre for flexible endoscopy and has the UK’s largest CE database with over 650 studies performed including many unusual and rare findings.
Aims & Methods: The aim was to develop a high-quality web-based e-learning module in lesion recognition at CE, aimed at gastroenterology consultants, trainees and nurses. Module design was planned using strong educational principles. An assessment tool was developed using 50 de-identified video clips and used as a formative assessment to allow identification of knowledge gaps and provide a stimulus for learning and reflection. A topic-based teaching module was designed using multimedia content on normal anatomy, anatomical variations/incidental findings, and pathological findings, incorporating written content, image stills and video clips. “Check your understanding” questions, literature references and hyperlinks are interspersed to stimulate active learning. Learners are then encouraged to perform a second knowledge assessment to consolidate understanding and identify remaining gaps.
Results: Initial development of the module was done in PowerPoint format and a pilot evaluation of the e-learning module and assessment tool was conducted on 3 experienced physician endoscopists and one nurse endoscopist, to ensure educational quality and to identify potential areas of improvement. Baseline performance on the assessment tool averaged 57.3%, with improvement to 68.3% after completing the learning module. The module was then translated into an interactive web-based format, which will be accessible at www.wolfsonendoscopy.org from mid-December 2007.
Conclusion: We report on development of the first e-learning tool for teaching and assessing lesion recognition skills at CE. It combines strong educational principles with a unique collection of images and expertise into a web-based resource that will allow dissemination to individuals wishing to develop CE skills. If successful, this approach could be expanded to incorporate a full on-line course in CE, and could form part of JAG accreditation in CE.
21ST CENTURY GASTROENTEROLOGY: UPDATING THE JOURNAL CLUB FOR WEB 2.0
A. V. Haycock1, M. Jacyna2. 1Wolfson Unit for Endoscopy, Imperial College London, London, 2Department of Gastroenterology, Northwick Park and St Mark’s Hospital, Harrow, UK
Introduction: Web 2.0 technology represents a revolutionary way of managing online information and enabling social software. New tools include social networking and syndication services (for example, RSS), file sharing and tagging, wikis, blogs and podcasts. They aim to provide easy generation, access and updating of web content with the intent of sharing ideas and promoting discussion within a community. This is ideally suited for the distribution of scientific information and can facilitate discussion and analysis. The Digital Atlas of Video Endoscopy (DAVE) project (www.daveproject.org) has been set up as a collection of teaching tools consisting of a gastrointestinal endoscopy video atlas, medical lectures and presentations. It is open-source software providing content that is free to view online or download as a Windows Media File or as a Podcast. All content is cross-referenced to the American College of Gastroenterology Curriculum.
Aims & Methods: The aim of this project was to update the gastroenterology journal club at St Mark’s Hospital, a weekly presentation and discussion of two recent journal articles relevant to current practice. These are presented as PowerPoint slides detailing the article and critiquing the methodology and results, followed by a wider debate about issues raised. Participants are encouraged to critique using established guidelines (CONSORT and STROBE recommendations). From June 2007, each presentation was recorded using a desk-top microphone and the “record narration” function within PowerPoint. They were then uploaded to the DAVE project website where they were included into the Journal Club section as the first international contributions. Each presentation is linked to the journal abstract and hyperlinked to a PubMed search of keywords providing other articles on the topic. An RSS feed is available for continuing updates on the topic.
Results: The contributions from our institution have had nearly 3000 hits in the last six months, with each individual able to retrieve their download statistics for their own records. The incentive of international peer review has appreciably raised the quality of the presentations. Participants have also reported using the website as a reference source for their own learning since their contribution has gone online.
Conclusion: The simple addition of recording a narration during a journal club presentation can be a powerful driver for change. It produces a high-quality web-based learning module that is widely accessible to an international audience and time and location independent. It can be linked to learner-centred tools, enabling multi-source evaluation and real-time updating of related online content via RSS feeds. Possible future developments include incorporation of other Web 2.0 technology such as feedback threads or blogs to promote wider discussion of important current publications.
THE TWO-WEEK RULE AND THE DIRECT TO TEST POLICY HAVE IMPROVED LOCAL GASTROINTESTINAL CANCER SERVICES
T. J. W. Lee, R. Swann, L. Clipsham, E. Carbro, D. Dwarakanath. Gastroenterology, University Hospital of North Tees, Stockton on Tees, UK
Introduction: The Two-Week Rule (2WR) was introduced by the Department of Health in 2000 to improve the care of patients presenting to their GP with symptoms suggestive of cancer. The Direct to Test (DtT) policy was introduced in North Tees and Hartlepool in 2005 to remove the delay of a patient seeing a hospital specialist prior to the diagnostic test. It was hoped that these strategies would streamline services and reduce waiting times. There has been concern that there would be a negative impact on routine clinical work and it has been suggested that the 2WR is failing because of a lack of genuine clinical gain or evidence of improved survival.1
Aims & Methods: We performed 2 retrospective audits of all 2WR referrals. The first audit was conducted shortly after the introduction of the DtT policy, the second audit was conducted 18 months later. Data on waiting times and cancer diagnosis rates were obtained from the trust’s clinical effectiveness department.
Results: A summary of the results is shown in the table. The number of referrals in the two periods were similar however there were a higher proportion of inappropriate 2WR referrals in the second period. Cancer pickup rates were similar but the proportion of GI cancers diagnosed via the 2WR as opposed to other pathways (for example, emergency admissions, routine referrals) increased significantly.
Conclusion: The 2WR and DtT policy have effectively streamlined local GI cancer services. We believe the 2WR has been successful in its aims. However, there is still room for refinement, in particular reducing the number of patients inappropriately referred via the 2WR pathway. The 2WR has not been shown to reduce the stage of colorectal cancer at presentation2 and there is no suggestion that it improves outcome or mortality. However, these outcomes were not the intended aims of the policy.
COMFORTABLE COLONOSCOPY? A SIMPLE AND RELIABLE METHOD FOR RECORDING PATIENT DISCOMFORT
A. Wahab1, J. Brown1, R. M. Valori1, K. Dowler2, P. Dunckley1, E. Nowell1, I. S. Shaw1. 1Department of Gastroenterology, 2Information Department, Gloucestershire Hospitals NHS Foundation Trust, Gloucester, UK
Introduction: Patient comfort during colonoscopy has been adopted by the Global Rating Scale and the Joint Advisory Group for Endoscopy as an important measure of procedure quality and endoscopist competence. However patient comfort can be difficult to assess objectively, as there is potential for bias to effect endoscopist reporting of patient comfort.
Aims & Methods: We set out to investigate the feasibility of incorporating a simple 5-point comfort scale into our standard endoscopy reporting system and to assess the correlation between scores recorded by the colonoscopist and by endoscopy nurses present in the room. Our endoscopy reporting software was modified to require the colonoscopist to record their assessment of patient comfort using a simple 5-point comfort scale, where 1–5 represented a comfort level of normal comfort, mild discomfort, moderate discomfort without distress, moderate discomfort with occasioanl distress and severe discomfort with frequent distress. The nurses’ “SwiftOp” procedure record was also redesigned to include an identical scale. Endoscopists were notified of the changes to the system by email, but recieved no specific training in the scale. The endoscopy nurses were given a demonstration of their system and invited to intend a short talk about the comfort score. Comfort scores were then recorded separately and prospectively by endoscopists and nurses during consecutive routine unselected colonoscopies.
Results: A total of 619 colonoscopic procedures were conducted by 15 operators between May to October 2007. The endoscopists reported the comfort score as 1 in 210 (33.9%), 2 in 238 (38.4%), 3 in 92 (14.9%), 4 in 66 (10.7%), and 5 in 13 (2.1%) of cases respectively. Frequency of comfort scores varied between operators; with recording of comfort score 1 ranging from 14 to 50%. Colonoscopist scores correlated well with nurse reported scores; with complete agreement in 260/619 (42.3%) of cases, disagreement by 1 in 273/619 (44.1%)and disagreement by more than 1 in only 13.9%. Endoscopists were more likely to record greater discomfort than the nurses, with the nurses rating the discomfort higher than the endoscopists in 130/619 (21.0%) of cases compared with 229/619 (37.0%) cases where the endoscopist recorded greater discomfort.
Conclusion: We have demonstrated that it is possible to incorporate a simple comfort score into the standard colonoscopy report. Furthermore we have shown that there is good correlation between scores recorded by endoscopy nurses and colonoscopists, suggesting that the scoring system is reliable and valid; although on average endoscopists tend to record higher levels of patient discomfort than endoscopy nurses.
EVALUATION OF THE TWO-WEEK RULE: A SYSTEMATIC LITERATURE REVIEW
K. Thorne1, H. A. Hutchings1, G. Elwyn2, J. G. Williams1. 1School of Medicine, Swansea University, Swansea, 2Department of Primary Care and Public Health, Cardiff University, Cardiff, UK
Introduction: The Two-Week Rule (TWR) was introduced to allow GPs to fast-track patients with suspected colorectal cancer (CRC) to shorten the length of time they waited for a diagnosis. GPs were given guidelines by the DoH in 20001 for the appropriate, timely referral of these patients so that endoscopy services were not overburdened to the detriment of other service users. It was hoped that these guidelines would increase the number of CRC patients being diagnosed at an earlier stage of their disease. Many hospitals in the UK have reported on the impact of the TWR on endoscopy services, although most of these never become peer-reviewed publications. This has resulted in a lack of high-quality evidence against which to assess the impact of the TWR for successfully identifying patients with suspected CRC.
Aims & Methods: The aim of this study was to provide this high quality evidence using a systematic literature review. The review was conducted using peer-reviewed studies published about the TWR for CRC patients in the endoscopy units of UK NHS Trusts from 2000 onwards. Letters and abstracts were excluded from the review.
Results: A total of 16 papers were eligible for inclusion. Meta-analysis was done to determine the overall TWR CRC pick-up rate and the overall proportion of CRC patients who had been diagnosed via the TWR compared with emergency and non-urgent routes. The analyses found that only 9.4% (4.4%–15.7%) of patients referred using the TWR were subsequently diagnosed with CRC. Only 32% (16.7%–50%) of all CRC patients diagnosed had been referred using the TWR route, higher than the 24% published in 2006 using the literature available at that time.2 This indicated that more recent studies had found a larger proportion of CRC patients diagnosed using the TWR than alternative routes. However, the CRC pick-up rate had also dropped from 10.3%.
Conclusion: This evidence suggests that the TWR guidelines are not sensitive enough to capture high numbers of symptomatic CRC patients. This is a major concern because the CRC patients are not being referred appropriately onto the TWR route and are found in high numbers in emergency and routine clinic appointments. It is also clear that since the preliminary review published in 2006, no major improvements in CRC pick-up rate have been achieved following the introduction of the 2005 NICE guidelines.3
ANALYSIS OF THE IMPACT OF THE MES PROJECT BY THE ENIGMA PROJECT USING SERVICE-RELATED ENDOSCOPY DATA
K. Thorne1, H. A. Hutchings1, G. Elwyn2, J. G. Williams1. 1School of Medicine, Swansea University, Swansea, 2Department of Primary Care and Public Health, Cardiff University, Cardiff, UK
Introduction: The Modernising Endoscopy Services (MES) project was set up by the NHS Modernisation Agency (NHSMA) to facilitate modernisation in 26 NHS endoscopy units in England. The “Evaluating Innovations in Gastroenterology by the NHSMA” (ENIGMA) study was set up to independently evaluate the MES project by comparing 10 MES-funded sites (intervention sites) with 10 control sites who had been forced to redesign independently.
Aims & Methods: One aspect of the ENIGMA study involved comparing service-related data collected from intervention and control sites for eight specific time points in order to (1) determine whether the services in both intervention and control sites had changed over time and (2) identify whether there were any significant differences between the intervention and control sites at specific points in time. All 20 study sites were asked to submit service-related data pertaining to referral numbers, number of patients waiting more than three months (wait >3 m), total number of patients waiting (snapshot), number of lost appointment slots (lost slots) and activity for eight time points: Jan, Jun and Dec 2003, Apr and Nov 2004, Apr and Oct 2005 and Apr 2006. Where endoscopy units did not provide data, Trust data were obtained. Data were aggregated into years (2003, 2004, 2005/6) and by site type (intervention and control groups) for statistical analysis using a two-way ANOVA.
Results: There were no significant differences in the data over time for referral numbers, wait >3 m, snapshot, lost slots or activity within either the intervention or the control group. There was also no significant difference between intervention and control group data at any point in time for referral numbers, wait >3 m or lost slots. However, there was a significant difference in the data from the intervention and control groups for (1) snapshot for 2004 and 2005/6 due to a decrease in the intervention group matched by an increase in the control group, and for (2) activity for 2003 due to significant differences in data at the start of the study for the intervention and control groups.
Conclusion: The MES project had no significant impact on the services of participating endoscopy units as a whole, and had limited benefits when compared to the control site endoscopy units. Only the waiting lists of the intervention sites benefited from the project, although that improvement that was sustained long after the project close. It appears that while the MES project may have been a focus for thinking about redesigning services for both intervention and control sites during the application phase in 2002, the project itself did not appear to significantly improve endoscopy services overall in the intervention sites over and above what could have been achieved independently.
DEATHS FROM DIGESTIVE DISEASES: A VIEW FROM THE 3RD MILLENNIUM
J. West, T. R. Card. Division of Epidemiology and Public Health, University of Nottingham, Nottingham, UK
Introduction: The Cooksey report found that non-malignant digestive disease accounts for about 6% of Disability Adjusted Life Years lost while attracting less than 3% of total health expenditure.1 It did not however break down the contribution between diseases nor tell us about trends over time. Using mortality which is a simpler and more readily accessible measure we have sought to describe the importance of digestive disease, and its trends over time from 2001–5.
Aims & Methods: We used data from the Office for National Statistics which included numbers of deaths and populations for the years 2001–5. We calculated European age-standardised mortality rates and rate ratios. We defined all deaths from digestive diseases as those coded within the follow groups for underlying cause of death in ICD-10: K00–K93, C15–C26, A00–A09 and B15–B19. Within this broad group we then subclassified digestive disease deaths by major subcauses.
Results: While all-cause mortality rates declined from 2001–5, deaths from digestive diseases remained stable and in 2005 accounted for 12.7% of all deaths. Subdividing this 12.7% malignant digestive diseases (which are marginally declining) accounted for 7.3% of all deaths in 2005, and non-malignant digestive diseases (which are increasing as a cause of death) for 5.4%. Rates of death from liver disease rose by 9% over the 5 years and in 2005 accounted for 10.6% of digestive disease deaths. Deaths from gastrointestinal haemorrhage declined while for ischaemic colitis they rose. The mortality rate for Clostridium difficile showed a nearly threefold increase. Over the 5 years there were only a total of 94 deaths attributed to coeliac disease, 1868 to inflammatory bowel diseases and 7 to irritable bowel syndrome.
Conclusion: Digestive diseases are an important and increasing (proportionately) cause of death. This is primarily due to a rise in non-malignant deaths and in particular deaths from liver diseases. While gastrointestinal bleeding is decreasing there has been an almost threefold increase in mortality from Clostridium difficile which caused more death in the study period than inflammatory bowel disease or gastrointestinal haemorrhage.
Inflammatory bowel disease posters
HOW DO PATIENTS WITH INFLAMMATORY BOWEL DISEASE WANT TO HAVE THEIR BIOLOGICAL AGENT ADMINISTERED?
P. B. Allen1, H. Lindsay2, T. C. K. Tham1. 1Division of Gastroenterology, 2Department of Quality and Effectiveness, Ulster Hospital, Belfast, UK
Introduction: Infliximab is administered by intravenous infusion initially with three separate infusions over 6 weeks and then if given for maintenance, every 2 months. In many centres, patients attend a hospital day case facility for their infusions. Adalimumab is a recently licensed biological agent for the treatment of Crohn’s disease. It is administered as a subcutaneous injection with a loading dose and then if given for maintenance, every 2 weeks. The advantage of adalimumab is that patients can self administer avoiding a visit to hospital. However no studies have evaluated patient preference for these two modes of administration in IBD patients.
Aims & Methods: The aim of our study was to evaluate patient preference for the route of administration of biologics if their management required their use. An anonymous questionnaire was devised and distributed to 125 patients with inflammatory bowel disease. These patients were identified from the Ulster Hospital inflammatory bowel disease database (Rotherham, Ferring Pharmaceuticals). Patients were given a choice of whether they would prefer in a hypothetical setting, to receive either infliximab (infusion) or adalimumab (self-administered subcutaneous injection) and the reasons for their choices.
Results: In total 78 patients responded (62%); of these 74% were in employment. Average age of respondents was 44 years. The diagnoses were: ulcerative colitis 51%; Crohn’s disease 36%; and indeterminate colitis 13%. The average duration of disease was 8 years. 23% had already undergone surgery, and of these 47% required greater than 3 procedures. Of those surveyed, 45 patients (58%) preferred infliximab. The commonest reasons stated were: “I do not like idea of self-injecting” (51%); “Prefer less frequent injections” (33%). 22 patients (28%) preferred adalimumab, the commonest reason stated was: “Convenience” (82%). 10 patients had previously received infliximab (13%). Of these, 7 (70%) patients stated that they would prefer to have infliximab to adalimumab. Of the 68 infliximab naïve patients (86%), 38 (57%) preferred infliximab, 19 patients (28%) preferred adalimumab, and 11 patients (16%) had no preference of biological agent.
Conclusion: More patients preferred the route of administration of infliximab to that of adalimumab if given the choice. The majority of patients who had infliximab preferred to continue therapy with infliximab, while over a half of those who have never had a biological agent preferred infliximab. Therefore if appropriate, patients should be allowed to make informed decisions regarding their choice of biologic therapy with respect to the mode of administration.
METHOTREXATES IN CROHN’S DISEASE: EIGHT-YEAR FOLLOW-UP, BETTER ON OR OFF?
A. Al-Rifai, A. J. Cairns, K. Kemp, S. S. Campbell, A. J. Makin. Gastroenterology, Manchester Royal Infirmary, Manchester, UK
Introduction: In steroid refractory Crohn’s disease (CD), Azathioprine (AZA) and 6-mercaptopurine (6MP) are the most commonly used Rx. Intolerance to these is reported in approx 30% of patients. Methotrexate (MTX) is often used in AZA/6MP intolerant pts. There is a lack of long-term data to support this and concerns remain on long-term side effects.
Aims & Methods: We retrospectively analysed our IBD database for patients between 1999–2007 who had received MTX Rx. Demographics, disease anatomy, duration of MTX (and total dose), side effects and time to 1st relapse were collected. Comparison between survival curves were performed using Log Rank Test. Relapse was defined by clinical, laboratory and radiological findings.
Results: 30 MTX patients were identified (12M:18F), Median age 43 years (23–76)). Median duration of MTX Rx was 335 days (30–1232) and median duration of follow-up after MTX was stopped 1250 days (650–2000). All but two had small bowel disease with or without large bowel involvement. Twelve (40%) patients were smokers. All patients had AZA prior to starting MTX. AZA was stopped in 22 (73%) patients due to intolerance and in 8(27%) failure to control the disease. Median duration of treatment with MTX was 11 months (1–44) Mean average total dose of 880 mg (12.5–2022 mg); there was no correlation between total MTX dose and number of relapses (p = NS). In 18 (60%) patients MTX had a steroid sparing effect. Nine (30%) patients managed to wean off steroids completely. MTX was stopped due to side effects in 9 (30%) patients. No patients had significant hepatopulmonary toxicity. In 8 (26%) cases MTX was stopped because of failure to control CD. Time to first relapse data were analysed for patients while taking MTX and during follow-up after MTX was stopped. On MTX, 40% of patients were in remission at 1 year and 25% at 3 years. Follow-up after MTX was stopped gave similar results with 40% in remission at 1 year and 25% in remission at 5 years (p = NS).
Conclusion: MTX is a well tolerated treatment in patients intolerant of AZA or when it is ineffective. Once remission is achieved with MTX these patients (n = 13) do well once MTX is discontinued. Total MTX did not correlate with increased side effects nor improved remission rates. Hepatopulmonary side effects were not reported in this long-term cohort. MTX has comparable long-term remission rates to other immunomodulators and should be considered in CD patients as a third line agent.
FUNCTIONAL VARIANTS IN THE MACROPHAGE STIMULATING 1 RECEPTOR GENE ARE ASSOCIATED WITH CROHN’S DISEASE
J. B. Beckly1, L. Hancock2, F. Cummings1, A. Geremia1, R. Cooney1, S. Pathan1, D. Jewell1. 1Gastroenterology, Radcliffe Infirmary, 2Colorectal Surgery, John Radcliffe, Oxford, UK
Introduction: Early genome-wide linkage studies identified chromosome 3p as a potentially important inflammatory bowel disease locus. Genome-wide association studies have supported this locus with the Wellcome Trust case control consortium1 demonstrating a 0.6 Mb region on 3p21 where the test statistic was above background.
Aims & Methods: The objectives of our study were to perform a two-stage candidate gene association study of the 3p locus and to identify linkage disequilibrium (LD) between significant SNPs and an Oxfordshire subset (n = 282) of the WTCCC. 197 SNPs in 53 genes from the 3p locus were genotyped on the Illumina platform in an initial screening cohort of 469 Crohn’s disease (CD) patients and 461 controls. Significant associations were then genotyped on the iPLEX platform in the original cohort as well as a second cohort of 139 CD patients, 670 ulcerative colitis patients and 1131 controls. All cases and controls were Caucasian and from the Oxfordshire region of the UK. All markers were in Hardy-Weinberg equilibrium in the control cohorts and genotyping rates were >95%. LD was sought between significant SNPs and the WTCCC study as well as HapMap SNPs using Haploview version 4.0.
Results: An association was seen for the minor allele of the intronic SNP rs1128535 in the Traf interacting protein (TRIP) gene and CD (p = 0.01) which was not significant after correction for multiple testing in the screening cohort but was significant in the validation (n = 139, p = 0.00007 (corrected p = 0.001), OR 0.58 (95% CI 0.45 to 0.76)) and combined cohorts (n = 608, p = 0.0004 (corrected p = 0.002), OR 0.77 (95% CI 0.67 to 0.89)). No association was seen for UC. Strong epistasis was seen with the presence of the common NOD2 mutations (p = 0.00003 (corrected p = 0.0006), OR 0.48 (95% CI 0.34 to 0.68)). Genetic heterogeneity was demonstrated with ATG16L1 (Ala197Thr) (p = 0.0002 (corrected p = 0.002) OR 0.47 (95% CI 0.32 to 0.70). No LD was demonstrated with the WTCCC SNPs in the 3p locus. However, using HapMap data strong LD was demonstrated with two non-synonymous SNPs in the MST1R gene which is in an adjacent LD block to the peak association seen in the WTCCC study.
Conclusion: These data suggest a separate association in a distinct LD block from the currently published genome-wide association studies. The strong LD with functional variants in the MST1R gene suggests a possible role for this gene and requires further study. In addition, important epistatic interactions have been identified with the established IBD gene NOD2.
CICLOSPORIN USE IN ACUTE ULCERATIVE COLITIS: THE OXFORD REGIONAL DISTRICT GENERAL HOSPITAL EXPERIENCE
N. Chandra1, N. Rajoriya2, D. A. Gorard3, A. S. McIntyre3, J. Simmons2, A. J. Ellis1. 1Gastroenterology, Horton Hospital, Banbury, 2Gastroenterology, Royal Berkshire Hospital, Reading, 3Gastroenterology, Wycombe Hospital, High Wycombe, UK
Introduction: Ciclosporin (CsA) rescue therapy has been shown to be effective in the management of steroid-refractory, acute ulcerative colitis (UC). The published literature has focused on the use of CsA in specialist centres. A paucity of data exists regarding usage in district general hospitals (DGH).
Aims & Methods: To assess the initial response and long-term outcome in patients treated with CsA in a DGH setting, and compare these results with our tertiary centre. A retrospective database was constructed of UC patients given CsA between 2003 and 2007 in 3 centres within the Oxford region. These data were compared with those from the John Radcliffe Hospital (JRH).1
Results: 24 patients (16 male, mean age 39 years) received CsA. Median disease duration prior to treatment was 0.83 years (1st presentation for 2 patients). Median CRP and stool frequency at day 3 was 47 mg/l and 8 per day respectively. Median duration of both IV steroids prior to CsA and that of combined therapy was 5 days. 17 patients (71%) achieved clinical remission and did not require colectomy during their admission. 7 patients (29%) underwent surgery on the same admission and all received oral CsA. 18 patients from Centres 1 and 2 received oral CsA (median duration 46.5 days, range 2–165) and of these, 61% responded and 39% proceeded to inpatient colectomy. 4 of 9 patients discharged on oral CsA received triple immunosuppressant therapy, while the remainder commenced azathioprine on discontinuation of CsA. All 6 patients from Centre 3 who were treated with IV CsA (median duration 10 days, range 9–12) responded. A dose of 4 mg/kg was used in 5 cases, and 2 mg/kg in the remaining patient. CsA was discontinued and azathioprine commenced at the time of discharge. One elderly patient developed a hospital-acquired pneumonia and died after receiving oral CsA for 33 days as an inpatient. 2 patients reported minor parasthaesia. Patients were followed-up for a median period of 1 (0.1–3.6) year. At 1 year, 36% had relapsed and at 3 years, 64% had relapsed. Colectomy rate at 1 year was 37.5%, 42% at 2 years and remained at 42% at 3 years.
Conclusion: CsA can be used effectively and safely in a DGH setting. Our data compare favourably with the JRH experience who reported an initial response and colectomy rate of 74% and 26% respectively, and a relapse rate of 65% and 90% at 1 and 3 years respectively. These data demonstrate a variation in practice between Gastroenterologists and their use of CsA. A national comparison between patients receiving oral and IV CsA is merited with standardisation of treatment guidelines.
THE RISK OF ORAL CONTRACEPTIVES IN THE AETIOLOGY OF INFLAMMATORY BOWEL DISEASE: A META-ANALYSIS
J. A. Cornish1, E. Tan2, C. Similis3, S. K. Clark4, J. P. Teare5, P. P. Tekkis2. 1Department of Biosurgery and Surgical Technology, Imperial College, St Mary’s Hospital, 2Department of Biosurgery and Surgical Technology, Imperial College, 3Department of Biosurgery and Surgical Technology, St Mary’s Hospital, 4Department of Surgery, St Mark’s Hospital, 5Department of Gastroenterology, St Mary’s Hospital, London, UK
Introduction: There have been several aetiological factors implicated in the development of Crohn’s disease (CD) and ulcerative colitis (UC) however the pathogenesis of inflammatory bowel disease (IBD) remains unknown. Although there is strong evidence for the role of smoking and genetics, there has been a lack of convincing evidence for the link between use of oral contraceptive agents (OCP) and the development of IBD.
Aims & Methods: The aim of this study is to provide a clear assessment of risk of oral contraceptive use in the aetiology of inflammatory bowel disease. A Medline, OVID and Cochrane database literature search was performed to identify studies reporting on the association of oral contraceptive use in the aetiology of IBD. Random-effect meta-analysis was used to compare outcomes between those patients with IBD and normal control patients.
Results: A total of 2134 IBD patients (CD 1251 (58.6%), UC 883 (41.3%)) and 32 756 controls were reported on in fourteen studies that satisfied the inclusion criteria. A meta-analysis was performed for CD and UC, adjusted and non-adjusted for smoking. The pooled relative risk (RR) for CD was 1.46 (95% CI 1.26 to 1.70; p<0.001) adjusted for smoking and RR 1.51 (95% CI 1.17 to 1.96; p = 0.002) non-adjusted. The relative risk for UC was 1.28 (95% CI 1.06 to 1.54; p = 0.011) adjusted for smoking and RR 1.53 (95% CI 1.21 to 1.94; p = 0.001) non-adjusted.
Conclusion: This study provides evidence of a statistical correlation between the use of oral contraceptive agents and development of IBD, in particular Crohn’s disease.
THE PATTERN AND OUTCOME OF ACUTE SEVERE ULCERATIVE COLITIS
L. Dinesen1, M. N. Protic1, A. Walsh1, F. Cummings1, T. Ahmad2, S. P. L. Travis1. 1Gastroenterology Department, John Radcliffe Hospital, Oxford, 2Gastroenterology Unit, Royal Devon and Exeter Hospital, Exeter, UK
Introduction: The initial outcome, likelihood of recurrence and long-term prognosis of acute severe ulcerative colitis (ASUC) are measures of the burden of disease and therefore influence therapeutic decisions. There are few data on the prevalence and characteristics of ASUC, although the UK National IBD Audit (2006) estimates that one patient is admitted to every UK hospital each month.
Aims & Methods: The aims of this study were to define these characteristics and determine if the outcome was related to the number of Truelove and Witts’ criteria (TWC) on admission. A systematic, retrospective study of all patients with UC diagnosed in Oxford from 1950–2007 was performed. Non-Oxford diagnosed patients were excluded from the analysis. ASUC as defined by TWC was the indication for admission for intensive therapy throughout this period. Demographic, clinical and biomedical characteristics on admission were recorded, with medical or surgical treatment and outcome.
Results: 747 patients with UC diagnosed in Oxford between 1950–2007 (median follow-up 129.0 months, range 0–647.6 months) were evaluated out of a total cohort of 1827 patients. Of these, 27.6% (206/747) had ASUC as defined by TWC. There were 317 admissions in 206 patients. Age at latest follow up in those with an episode of ASUC was significantly lower than those without an episode (49.6 vs 53.1 years, p = 0.007), but there was no significant difference in gender or duration of disease. 49.3% were admitted within 1 year of initial diagnosis (median time to admission 12.7 months, range 0–453.4 months). 67% had a single episode, 20% had two, and 13% three or more episodes. 87/227 (38.7%) of patients with one or more episodes of ASUC had a colectomy. The likelihood of colectomy on the first, second, third, fourth and fifth admissions was 19.9%, 29.0%, 36.6%, 38.2%, 39.8% respectively. Although half of all colectomies (36/75) occurred on the first admission the colectomy rate on the first admission (48/152, 31.5%) was lower than on the second or subsequent admissions (39/75, 52.0%; OR 2.35, 95% CI 1.33 to 4.14, p = 0.003). 18/147 patients who had a single TWC in addition to a bloody stool frequency 6/day required colectomy, while 61/170 patients who had ⩾2 additional TWC required colectomy (p = 1.2×10−6; OR 4.01, 95% CI 2.24 to 7.19) (+1 additional criterion = 18/147 (12.2%); +2 = 30/99 (31.3%); +3 = 27/59 (45.8%); +4 = 4/12 (33.3%).
Conclusion: This is the largest single centre cohort study on the natural history of ASUC. A quarter of all UC patients experience at least one episode of ASUC. A third come to colectomy on the first admission, but half of those who have two or more admissions come to colectomy. When there are two or more TWC in addition to a bloody stool frequency >6/day, the risk of colectomy is fourfold higher than when there is only one additional TW criterion on admission.
THE GENETICS OF NOD-LIKE RECEPTOR PROTEINS IN CROHN’S DISEASE
F. Cummings1, R. Cooney1, G. Clarke2, J. Beckly1, A. Geremia1, L. Hancock1, S. Pathan1, L. R. Cardon2, D. P. Jewell3. 1IBD Genetics Group, 2Bioinformatics and Statistical Genetics, Wellcome Trust Centre for Human Genetics, 3Gastroenterology Unit, Radcliffe Infirmary, Oxford, UK
Introduction: The Nod-like receptor proteins NLRP1, NLRP2 and NLRP3 have been shown to form the central scaffold of the caspase-1 activating complex, the inflammasome, which is crucial for the processing and maturation of the proinflammatory cytokines IL-1_eta; and IL-18. One cluster of NLRP genes is located under a peak of linkage in Crohn’s disease (CD) on chromosome 19 when data are stratified on the non-carriage of CARD15 disease susceptibility alleles. The remaining genes are found on chromosomes 1, 11 and 17. NLRP1 has been associated with vitiligo and other common autoimmune diseases whilst NLRP3 has been associated with a number of uncommon autoimmune diseases.
Aims & Methods: We aimed to study the role of NLRs in the genetic susceptibility to CD using 547 rigorously sub-phenotyped CD patients and 483 controls. Haplotype tagging SNPs were selected for each NLRP gene using the HapMap data and Haploview (v3.32) while non-synonymous SNPs (nsSNPs) from each gene were identified using the SNPper website. The Illumina and iPLEX genotyping platforms were used. 402 SNPs were genotyped in total. Analysis was carried out using PLINK. Results are presented as allelic p value (OR, 95% CI). Data were stratified by CARD15 and IBD5 risk haplotype carriage. Markers within all the NLRP genes were extracted from the WTCCC study data (with Oxford patients removed) and used as a replication cohort.
Results: 119 SNPs were excluded by the quality control process. Four SNPs found within NLRP3 which are in tight LD with each other (r2>0.9) were associated with overall disease susceptibility with the strongest association being for rs10925019 (p = 6.5×10−4, (1.65, 1.24 to 2.19)). Within NLRP1, 5 SNPs were weakly associated with susceptibility to CD, the strongest being rs8079727 (p = 0.02, 1.25, 1.01 to 1.54). No association was seen with NLRP11. On stratification of data by CARD15 carriage rs1539019 within NLRP3 became significant (p = 0.0006, 0.74, 0.60 to 0.92). None of the markers within the 19q NLRP cluster were significant on stratification. Six SNPs in NLRP1 were associated with inflammatory disease behaviour (p = 0.04–0.0001), with 3 of them also being associated with pure colonic disease (p = 0.03–0.004). A further 4 SNPs were associated with skin extraintestinal manifestations. Four SNPs in NLRP14 (rs10839708, rs1979669, rs17280682 and rs7131269) which are in tight LD were found to be protective against the inflammatory disease behaviour subphenotype (p = 0.0001–0.0009, OR 0.61–0.70). None of the associations were replicated in the WTCCC data although the density of markers within the NLRP genes was relatively low. Therefore this may not be a true negative replication.
Conclusion: We have presented preliminary evidence of association for markers within NLRP1 and NLRP3 with CD susceptibility and subpehontype. Replication in an accurately sub-phenotyped independent cohort is now required.
CLINICAL PROFILE OF CROHN’S DISEASE FROM A TUBERCULOSIS ENDEMIC REGION
K. Das1, K. Das2, G. K. Dhali1. 1Division of Gastroenterology, 2Division of Hepatology, School of Digestive and Liver Diseases, IPGMER, Kolkata, India
Introduction: Despite Crohn’s disease (CD) being reported from India since the 1960s, doubts persisted whether these were true CD in view of the widespread endemicity of tuberculosis in India. To define the clinical profile and disease behaviour of Indian patients with CD, we undertook a retrospective analysis of these patients who are being followed-up in an IBD clinic in Eastern India (Kolkata, West Bengal).
Aims & Methods: The data regarding all patients being followed from August 2000 until 30 September 2007 or last follow-up were retrieved. The diagnosis, disease severity and extent were based on European Crohn’s and Colitis Organisation (ECCO) consensus guidelines. Disease profile was classified according to the Montreal classification. At their last follow-up, the patients were classified to have a disabling disease if they had any one of the following: >2 steroid courses and/or dependence; further hospitalisation after diagnosis for flare/complication; disabling chronic symptoms present for >12 months; need for immunosuppressive Rx; intestinal resection or surgery for perianal fistulae.
Results: 81 patients were analysed. Mean age at onset of symptoms was 34.7±1.5 years with no bimodal peak. M:F::2.4:1 with an urban preponderance (urban:rural::1.4:1). 26% were current or ex-smokers. 4 (5%) had previous appendicectomy. Abdominal pain with or without partial intestinal obstruction (SAIO), bloody diarrhoea and anaemia were the most common presenting symptoms. Mean duration of symptoms pre-diagnosis was 4.6±0.6 years (0.1–28 years) with 80% having moderate-to-severe disease at diagnosis. 35% (n = 28) had received a course of anti-tubercular therapy (ATT) prior to their diagnosis. Diagnosis was established by histology (n = 29; 36%), clinico-radiological criteria (n = 37; 46%) or after non-response to a trial of ATT in combination with either of above (n = 15; 18%). Histology was available in 58 (72%) with granulomas in 12 (23%). 64 (79%) had definite and 17(21%) had probable CD, respectively. The Montreal classification was A1:A2:A3::6%:63%:31%; L1:L2:L3:L4::46%:31%:15%:8% and B1:B2:B3::41%:36%:23% with perianal- and UGI-modifier in 10% each, respectively. 45 (56%) had localised and 36 (44%) had extensive disease. Remission induction was by surgery (n = 34; 43%), steroids with or without immunosuppression in 22 (28%) and aminosalycilates (ASA) in 22 (27%). 4 patients received ATT also as initial therapy. Maintenance therapy was ASA alone (n = 51; 72%), azathioprine + ASA in 17 (24%). Follow-up was available in 63 patients(78%; mean±SEM 23.9+2.9 months) with a follow-up of >12 months in 40 (64%) of them. In the latter, disabling disease was present at last follow-up in 22 (55%). One patient, with fulminant colitis, died immediately after colectomy due to postoperative sepsis.
Conclusion: Our CD cohort is characterised by male preponderance, absence of an older peak, predominant ileal or UGI disease, delayed diagnosis and more severe disease at presentation requiring surgery or immunosuppression for initial control.
EMPIRICAL ANTI-TUBERCULAR THERAPY DELAYS DIAGNOSIS AND WORSENS CROHN’S DISEASE FROM A TUBERCULOSIS-ENDEMIC REGION
K. Das1, K. Das2, G. K. Dhali1. 1Division of Gastroenterology, 2Division of Hepatology, School of Digestive and Liver Diseases, IPGMER, Kolkata, India
Introduction: Differentiating Crohn’s disease (CD) from intestinal tuberculosis is extremely challenging and often therapeutic trial of antitubercular therapy (ATT) is used in cases of confusion. A retrospective analysis of patients with CD who are being followed-up in an IBD clinic in Eastern India (Kolkata, West Bengal), a place where tuberculosis is endemic, was undertaken to look at the role of factors that contribute to delayed disease diagnosis or disabling disease on follow-up.
Aims & Methods: 81 patients of CD being followed from August 2000 to 30 September 2007 were analysed. The diagnosis, disease severity and extent were based on the European Crohn’s and Colitis Organisation (ECCO) consensus guidelines. At their last follow-up, the patients were classified to have a disabling disease if they had any one of the following present: >2 steroid courses and/or dependence; further hospitalisation after diagnosis for flare/complication; disabling chronic symptoms present for >12 months; need for immunosuppressive Rx; intestinal resection or surgery for perianal fistulae. Statistical analysis was done with SPSS 13.0 for Windows (SPSS Inc, USA). Pearson’s χ2, Fischer’s exact test, Mann-Whitney U test, Kruskal-Wallis H and Spearman’s rho were calculated. Cox’s proportional hazard’s (forward stepwise conditional) was used for multivariate analysis.
Results: The mean duration of symptoms prior to diagnosis was 4.6±0.6 years (0.1–28 years). 30% (n = 24) had previously received >1 courses of anti-tubercular therapy (ATT). 13 had an initial symptomatic response while 11 did not. These 13 patients were diagnosed to have CD after a median (±SD) of 6.0 (4.82) years after receiving ATT. Longer duration of symptoms prior to diagnosis of CD correlated with history of ATT (r = 0.42; p<0.001), urban residence (r = 0.32; p<0.01), younger age of onset (r = 0.31; p<0.01), presentation with partial intestinal obstruction (r = 0.31; p<0.01) and disease behaviour (r = 0.27; p = 0.02). Follow-up of >1 year in 40 (50%). In them, disabling disease at last follow-up was in 22 (55%). On univariate analysis, the risk of having a disabling disease was associated with presence of moderate-severe disease at diagnosis (p<0.01), history of ATT (p<0.01), history of appendicectomy (p = 0.04), disease extent (p<0.05), disease behaviour (p<0.01) and presence of granulomas on histology (p = 0.02). On multivariate analysis using Cox’s proportional hazards model after stratifying for those with follow-up for >12 months, history of ATT (OR 4.0 (90% CI 1.3 to 12.8); p = 0.045), extensive disease (OR 10.0 (90% CI 2.3 to 42.6); p<0.01) and presence of granulomas (OR 4.4 (90% CI 1.4 to 13.9); p = 0.035) were associated with the hazard of having disabling disease.
Conclusion: In a tuberculosis-endemic region difficulty in adequately differentiating CD from intestinal tuberculosis delays diagnosis and is one of the risk factors for having disabling disease on follow-up.
LACTOSE INTOLERANCE AND INFLAMMATORY BOWEL DISEASE
P. Eadala1, J. P. Waud2, S. B. Matthews2, J. T. Green1, A. K. Campbell3. 1Department of Gastroenterology, 2Department of Biochemistry, Llandough Hospital, 3Department of Medical Biochemistry & Immunology, Cardiff University, Cardiff, UK
Introduction: Lactose intolerance (LI) is caused by the inability to digest and absorb the sugar lactose. LI has been associated with abdominal symptoms and more recently systemic features have been reported. The prevalence of LI is mainly determined by ethnicity with 60–90% in Asians but only about 10% in Northern Europeans. The clinical significance of secondary LI in patients with established gastrointestinal (GI) diseases is not known. Doctors differ widely in the advice they give their patients; some advocate avoidance of milk products when the diagnosis is made whereas others discount the possible influence of these foods on conditions like inflammatory bowel disease (IBD).
Aims & Methods: Patients attending the GI clinics in Llandough Hospital, Cardiff, UK, with established IBD in remission aged 18 or more of Caucasian origin were recruited. Patients with known LI, pregnant or concurrent life threatening illness were excluded. Healthy volunteers (HV) without evidence of GI disease were included. The Lactose hydrogen breath test was performed using 50 g of lactose after an overnight fast and expired air samples are collected before and at 30-min intervals for 4 h to assess hydrogen and methane concentrations. A rise in breath hydrogen concentration more than 20 parts per million (ppm) or rise in methane concentration more than 5 ppm over the baseline after lactose ingestion along with symptoms suggests lactase deficiency. The study was approved by the Local Research Ethics Committee. Statistical analysis was performed using χ2 test.
Results: A total of 114 patients, 44 Crohn’s disease (CD) and 50 ulcerative colitis (UC) and 20 HV were included. The prevalence of LI is 43% in CD, 26% in UC and 15% in HV. The prevalence of LI based on disease extent in CD affecting small bowel, small and large bowel and large bowel was 82%, 53% and 11% respectively and in UC affecting whole colon, left colon and rectum was 32%, 24% and 17% respectively. There is a statistically greater number of LI in patients with CD affecting small bowel (p<0.001) and CD affecting large and small bowel (p<0.04) when compared to HV.
Conclusion: The prevalence of LI is significantly greater in patients with CD involving the small bowel than it is in patients with CD involving the colon, UC or HV. LI may be influenced by factors like bacterial overgrowth or small bowel transit. The effects of a reduced lactose diet in these patients should be examined in a formal clinical trial.
A STUDY IN MAN TO INVESTIGATE THE COLON TARGETING PERFORMANCE OF A NOVEL ENTERIC AND POLYSACCHARIDE BASED DRUG DELIVERY SYSTEM: POTENTIAL APPROACH FOR IMPROVING TREATMENT OF INFLAMMATORY BOWEL DISEASES
V. C. Ibekwe1, H. M. Fadda1, M. K. Khela2, D. F. Evans2, A. W. Basit1. 1Pharmaceurtics, The School of Pharmacy, University of London, 2The Wingate Institute, Queen Mary College, University of London, London, UK
Introduction: Extensive evidence exists in the literature demonstrating large intra- and inter-individual variability in disintegration times and site of release of enteric coated products for treating inflammatory bowel diseases (for example, Eudragit S coated mesalazine preparations).1–3 Here we have designed a novel delivery system which comprises an enteric polymer and a naturally occurring polysaccharide. The latter component is resistant to digestion in the upper gastrointestinal tract however constitutes a substrate for the numerous enzymes of the resident colonic bacteria. We therefore utilise a double mechanism for drug release.
Aims & Methods: The coating formulation comprised a mixture of an enteric polymer with a dissolution pH threshold of 7 (Eudragit S) with a high amylose starch (Eurylon VII). Tablet cores were coated with this mixture and radio-labelled with Indium-111. These were administered to eight healthy male volunteers in a three-way crossover study. In two arms of the study, volunteers were fasting on tablet administration and food was administered either after 30 min (pre-feed) or 4 hours (fasted). In the third arm of the study tablets were given after breakfast (fed state). The transit and disintegration site of the tablets in the gastrointestinal tract was followed using a gamma camera.
Results: The results show excellent colonic targeting; with four tablets disintegrating in the ileo-caecal junction, 16 disintegrating in the ascending colon and the remaining four tablets administered disintegrating in the transverse colon. Tablet disintegration time and site do not appear to be affected by the feed status of the individual. Tablets successfully disintegrated in all volunteers; this is in contrast with a previous study with Eudragit S only coated tablets whereby disintegration failed in three out of eight volunteers.4 These results illustrate the success of a double release mechanism whereby if the pH trigger fails the bacterial enzyme trigger exists as a back-up. For instance, in one quarter of healthy individuals a pH of 7 is not reached in the small or large intestine,5 and in a similar proportion of ulcerative colitis patients, a luminal pH>7 was only maintained for less than 30 min.6
Conclusion: A combined enteric/polysaccharide drug delivery system displayed excellent colonic targeting in humans. Inclusion of starch provides an additional substrate and therefore a fail-safe mechanism which guarantees drug release.
IMPACT OF ADALIMUMAB MAINTENANCE THERAPY ON PATIENT-REPORTED OUTCOMES AMONG PATIENTS WITH FISTULISING CROHN’S DISEASE IN THE CHARM TRIAL
J. F. Colombel1, E. V. Loftus2, B. G. Feagan3, D. A. Schwartz4, E. Q. Wu5, A. Yu5, P. F. Pollack6, J. Chao7, P. Mulani7. 1Hepatogastroenterology, CHU Lille, Lille, France, 2Gastroenterology, Mayo Clinic, Rochester, MN, USA, 3Robarts Research Institute, London, ON, Canada, 4Gastroenterology, Vanderbilt University Medical Center, Nashville, TN, 5Analysis Group Inc, Boston, MA, 6Immunology Development, Abbott, Parsippany, NJ, 7HEOR, Abbott, Abbott Park, IL, USA
Introduction: Fistulas occur in 17%–43% of patients with Crohn’s disease (CD)1 and are associated with poor quality of life. Complete and sustained fistula closure has been observed with adalimumab (ADA) therapy in CHARM, a Phase III, randomized, double-blind, placebo-controlled trial assessing the maintenance of clinical remission with ADA therapy in patients with CD.2
Aims & Methods: To assess the impact of ADA maintenance therapy on CD-specific health-related quality of life among randomised patients with draining fistulas at screening visits and baseline of the CHARM trial, Inflammatory Bowel Disease Questionnaire (IBDQ) evaluations were conducted at baseline and at weeks 4, 12, 26, and 56 of CHARM. IBDQ scores over time were compared between groups receiving ADA 40 mg every other week (eow), ADA 40 mg weekly, or placebo using analysis of covariance. Chi-square tests were used to compare the percentage of patients achieving ⩾16-point improvement in Total IBDQ from baseline, the minimum clinically meaningful improvement.
Results: Baseline CDAI and IBDQ were similar for patients with or without fistulas (mean CDAI: 314 vs 311, respectively; IBDQ: 123 for both groups). Of 117 patients with fistulising CD who entered the study, 75 had IBDQ measurements after week 4 and were followed through week 56. Statistically significant and clinically meaningful improvements in IBDQ scores were achieved and sustained through week 56 with ADA maintenance therapy (table).
Conclusion: In patients with fistulising CD, ADA maintenance therapy is associated with sustained and clinically meaningful improvement in CD-specific quality of life as measured by the IBDQ.
IMPACT OF ADALIMUMAB THERAPY ON PATIENT-REPORTED OUTCOMES
E. V. Loftus1, B. G. Feagan2, J. F. Colombel3, E. Q. Wu4, A. Yu4, P. F. Pollack5, J. Chao6, P. Mulani6. 1Gastroenterology, Mayo Clinic, Rochester, MN, USA, 2Robarts Research Institute, London, ON, Canada, 3Hepatogastroenterology, CHU Lille, Lille, France, 4Analysis Group, Inc., Boston, MA, 5Immunology Development, Abbott, Parsippany, NJ, 6HEOR, Abbott, Abbott Park, IL, USA
Introduction: Adalimumab (ADA) is approved in the EU for the treatment of adults with severe Crohn’s disease (CD). Limited data are available regarding the impact of anti-TNF therapy on depressive (D) and fatigue (F) symptoms in patients with CD.
Aims & Methods: To assess the effect of ADA maintenance on F and D symptoms and traditional patient-reported outcomes (PROs) in randomised responders (RRs) (patients with a decrease ⩾70 points from baseline (week 0) CDAI score at week 4) in CHARM.1 All patients received an induction regimen of open-label (OL) ADA 80 mg at week 0 and 40 mg ADA at week 2. At week 4, patients were stratified by response and randomized to a maintenance regimen of 40 mg ADA every other week or weekly, or placebo. PROs (SF-36, IBDQ, FACIT-Fatigue (F), and Zung Depression scale (ZD)) collected at weeks 0, 4, 12, 26 and 56 were compared for RRs receiving ADA induction only (IO) and ADA maintenance (IM) therapy. Fatigue was measured by FACIT-F (scale range 0–52); a 3–4 point change was considered clinically meaningful. Depressive symptoms were measured by ZD (scale range 20–80, with >50 = D state).
Results: At week 4, 499 responders were randomised (IO, n = 170; IM, n = 329). PROs suggested an impaired health-related quality of life (HRQOL) at week 0. The mean FACIT-F score at week 0 (23) was similar to cancer patients with anemia. The mean ZD score at week 0 (IO = 55, IM = 56) indicated depressed states among CD patients. During the IO phase, patients improved across all 4 PROs (week 4 vs week 0). Patients in the IM group showed a significantly improved quality of life according to PRO measures from weeks 12–56 compared to patients in the IO group. In the IM group, FACIT-F scores showed reduced F symptoms (p<0.01 vs IO). Improvements in D symptoms, as seen in statistically significant reductions in ZD scores, were observed in the IM group (p<0.01 vs IO). At weeks 26 and 56, SF-36 Physical Component (PCS) and Mental Component (MCS) Summary PROs were greater for the IM group (all p⩽0.05 vs IO). Disease-specific IBDQ scores showed highly significant and sustained improvements for the IM group (p<0.01 vs IO) throughout the study.
Conclusion: Substantial and sustained improvements in F and D outcomes were observed in patients receiving ADA IM therapy for CD. Significant and sustained improvements in CD-specific (IBDQ) and general (SF-36 PCS and MCS) HRQOL measurements were also achieved with ADA IM therapy, compared to IO therapy.
COMPARISON OF A SIMPLE GLOBAL RATING WITH ESTABLISHED SCORING SYSTEMS FOR INFLAMMATORY BOWEL DISEASE
M. Abdullahi, I. Ordas Jimenez, C. Pavlidis, P. Siakouli, A. Forbes. Gastroenterology and Clinical Nutrition, University College London Hospitals, London, UK
Introduction: Treatment of inflammatory bowel disease (IBD) is designed to enable affected patients to live normally without symptoms or complications of their disease. Quality of life measures provide one means of determining the extent to which these objectives are met. The “0–100” visual analogue scale that forms part of the EuroQoL tool (EQ-VAS) is simple and reflects the subjective evaluation of health state. The Harvey Bradshaw (HBI) and Birmingham Royal Free (BRFI) indices are symptom-based indices developed for assessing disease activity, respectively in Crohn’s disease and ulcerative colitis (UC). Although both were designed to be simple and quick to use it is clear that neither are sufficiently so as to be widely used in clinical practice.
Aims & Methods: The aim of the study was to determine whether a single value from the EQ-VAS provided comparable and reproducible information to that of the two IBD-specific scoring systems, and whether this information was sufficiently robust to inform clinical practice. In total 352 IBD patients were assessed by HBI, BRFI and EQ-VAS. The EQ-VAS was elicited verbally, with a written version used only for patients having difficulty in understanding the concept. Data were initially recorded from 238 patients, and in 114 cases (analysed separately) there were paired assessments at an interval of at least 3 months. Reader operating characteristic curves (ROC) were generated in an attempt to determine thresholds for the recognition of active disease.
Results: Eliciting the EQ-VAS very rarely took more than 30 seconds (median of 21 seconds amongst 40 timed cases). A written version was needed only twice. There was a statistically significant negative correlation between the EQ-VAS score and the relevant disease activity index in both main forms of IBD: −0.61 (p<0.001) for the HBI in Crohn’s (n = 127); and −0.68 (p<0.001) for the BRFI in UC (n = 115). Among the paired assessments there was a similar negative correlation, which showed a weak trend towards closer linkage at the second assessment in Crohn’s patients (−0.561 and 0.693 respectively; p = 0.23; n = 62), and which remained high in UC (−0.721 and −0.752; NS; n = 52). ROC analysis provided putative thresholds for the designation of active disease when the EQ-VAS falls below 62 in UC (sensitivity 75%; specificity 92%); and below 70 in Crohn’s (sensitivity 87%; specificity 92.5%).
Conclusion: The EQ-VAS value provides clinically meaningful and reproducible information in the individual patient, and more so still in comparisons between patient groups. It is very easily adopted into everyday practice and is recommended for wider use.
ORAL CICLOSPORIN FOR CHRONICALLY ACTIVE STEROID-DEPENDENT ULCERATIVE COLITIS
A. Haycock1, J. Hoare1, J. Patel1, S. Ralphs1, A. Forbes2. 1Gastroenterology, St Mark’s Hospital, Harrow, 2Gastroenterology and Clinical Nutrition, University College London Hospitals, London, UK
Introduction: Ulcerative colitis (UC) is frequently managed adequately with aminosalicylates, adding steroids for acute exacerbations, and thiopurines for more chronically active disease. When these fail, but in the absence of indications for surgery, other immunomodulatory therapy may be considered. Intravenous ciclosporin has proved a valuable agent in acute severe UC, continuing into an oral maintenance phase in some patients. The value of oral ciclosporin for resistant, chronically active disease has not previously been assessed.
Aims & Methods: The aim was to evaluate use of ciclosporin in chronically active UC. Out-patients with steroid-dependent UC which had not responded to azathioprine/6-mercaptopurine (failure after at least 3 months’ therapy or drug intolerance) and for which surgery was not felt warranted or was declined by the patient were recruited prospectively into the protocol under the direct supervision of a single consultant. An initial daily dose of 5 mg/kg was prescribed and adjusted according to blood levels. Those in whom ciclosporin had been started (orally or intravenously) at the time of severe active disease were excluded. Retrospective analysis was performed.
Results: Full records were obtained for 28 patients (20 male) of median age 43 years (range 20–80). The disease was extensive in 17 cases, left-sided in 6 and distal in 5. The median initial Birmingham disease activity index was 6 (range 2–11) (>3 considered to indicate active disease). Patients improved on therapy in 17 cases. The median Birmingham score was 3 at 4 weeks, and (excluding 3 operated patients) 2 at 12 weeks. In 14 patients there had been complete weaning from steroids without surgery at 12 weeks. Ciclosporin therapy was clearly unsuccessful in 9 patients (failure of response in 4; failure of response with some identified toxicity in 5) who proceeded to colectomy. One further patient underwent colectomy having accepted a long-term need for surgery despite resolution of the majority of his symptoms on ciclosporin. Adverse events occurred in a total of 13 patients; in all cases these were mild examples of toxicities well-recognised for ciclosporin—namely: paraesthesiae in 6; transient increases in creatinine in 3; muscle aching and weakness in 3; headaches in 3; skin or gum changes in 2; mild hypertension in 1; increased liver enzymes in 1; and mild hirsutism in 1. For the potentially more serious adverse events the dose was reduced and in the 1 patient with renal impairment (creatinine 150) in whom the drug was withdrawn the patient pleaded for its reintroduction as it had given such good control of the colitis.
Conclusion: In conclusion, in this particularly difficult group of patients there is a case for the more formal evaluation of oral initiation of ciclosporin. The alternatives available have not been well studied in chronically active steroid dependent disease, and comparative studies are clearly legitimate.
DIETARY LINOLEIC ACID AND THE AETIOLOGY OF ULCERATIVE COLITIS: A EUROPEAN MULTICENTRE PROSPECTIVE COHORT STUDY
A. R. Hart for The IBD in EPIC Study Investigators. School of Medicine, Health Policy & Practice, University of East Anglia, Norwich, UK
Introduction: Dietary linoleic acid, an n-6 polyunsaturated fatty acid, is metabolised to arachidonic acid, a component of cell membranes. Metabolites of arachidonic acid have marked proinflammatory properties and are found in increased concentrations in the mucosa of patients with ulcerative colitis. Currently there are no epidemiological data investigating whether a high dietary intake of linoleic acid increases the risk of ulcerative colitis.
Aims & Methods: To examine the relationship between the dietary intake of linoleic acid and the development of ulcerative colitis in participants enrolled in a large European cohort study. Dietary data from food frequency questionnaires were available for 203 193 men and women aged 30–74 years and resident in the UK, Sweden, Denmark, Germany or Italy, participating in a prospective cohort study (EPIC - European Prospective Investigation into Cancer and Nutrition). Participants were followed up for the diagnosis of ulcerative colitis. Each incident case was matched on age, gender and follow-up time with four controls. An analysis of disease risk by quartile of intake of linoleic acid was performed using logistic regression adjusting for gender, age, smoking and energy intake.
Results: 126 participants developed ulcerative colitis (59 women, 67 men) after a median follow-up of 4.0 years (range 1.7–11.3 years). The highest quartile of intake of linoleic acid was associated with an increased risk of ulcerative colitis (OR 2.22, 95% CI 1.14 to 4.30, p = 0.02). A significant trend across quartiles was observed for an increasing linoleic acid intake (OR for trend 1.26, 95% CI 1.02 to 1.56, p = 0.04).
Conclusion: These data, together with a plausible biological mechanism, support a role for dietary linoleic acid in the aetiology of ulcerative colitis. Further epidemiological studies are needed to confirm the finding in other populations.
THE PREVALENCE OF UNDIAGNOSED DISORDERS OF NEUTROPHIL FUNCTION MIMICKING CROHN’S DISEASE
B. Hayee1, F. Z. Rahman1, J. Tempero1, D. J. B. Marks1, A. M. Smith1, S. L. Bloom2, A. W. Segal1. 1Medicine, University College London, 2Gastroenterology, UCLH NHS Trust, London, UK
Introduction: Inherited disorders of neutrophil function, such as chronic granulomatous disease (CGD), are associated with gastrointestinal inflammation indistinguishable from Crohn’s disease (CD) in up to 50% of cases.1 2 Normal neutrophil microbicidal activity requires the NADPH oxidase enzyme complex to mount a “respiratory burst”—leading to the generation of superoxide (O2−) to optimise the action of digestive enzymes. This process is defective in a number of neutrophil disorders with disparate aetiologies,1–3 making its integrity a potentially useful “screening” test. The existence of defects in innate immunity in CD is of increasing interest, and it is possible that a proportion of patients with CD possess an underlying disorder of neutrophil function.
Aims & Methods: To determine the frequency of such defects, neutrophils were isolated from 50 healthy control subjects and 100 consecutive, unselected patients with quiescent CD attending a tertiary inflammatory bowel disease (IBD) clinic. O2− production was calculated in a spectrophotometric assay based on the reduction of cytochrome-c by neutrophils after stimulation with phorbol-myristyl-acetate. Patients demonstrating a defect were investigated further.
Results: Mean O2− production in healthy controls (27M; mean age 31.7±7.2 years) was 10.96±1.9 nmolO2/106cells/min. O2− production in three unrelated patients (table) in the CD group was abnormally low (<35% healthy control mean2). Common characteristics were: diagnosis of CD at a young age; granulomatous inflammation in colonic biopsies; a history of recurrent systemic bacterial infections. Subsequent analysis diagnosed p47-deficient CGD (CGD-p47) in one patient, glycogen-storage disease type-1b (GSD-1b) in another, while the third has an as yet uncharacterised defect.
Conclusion: In this group of patients with CD, 3% were found to have neutrophil dysfunction. A high index of suspicion for such disorders is prudent, particularly for patients with CD presenting at a young age, with complex disease or with a history of recurrent systemic bacterial infections. It is important to identify these patients to improve their prognosis by altering or augmenting the conventional treatment regimens employed for idiopathic CD.
BH and FZR contributed equally to this abstract.
FACTORS THAT LIMIT RECRUITMENT TO CLINICAL TRIALS IN CROHN’S DISEASE
C. R. H. Hedin1, A. Koutsoumpas1, A. Forbes2, J. Sanderson3, A. J. Stagg4, S. C. Knight4, K. Whelan1, J. O. Lindsay5. 1Diet and Gastrointestinal Health, Nutritional Sciences Division, Kings College London, 2Department of Gastroenterology, University College London Hospitals NHS Foundation Trust, 3Department of Gastroenterology, Guys and St Thomas Hospitals NHS Foundation Trust, 4Antigen Presentation Research Group, Imperial College London, Northwick Park and St Marks Campus, 5Gastroenterology Clinical Academic Unit, Barts and the London NHS Trust, London, UK
Introduction: The 2006 UK IBD audit identified that fewer than 1% of Crohn’s disease (CD) patients were participating in clinical trials.
Aims & Methods: To determine the factors that limit recruitment of patients with active CD to clinical trials. We prospectively documented the recruitment process for a clinical trial (with standard inclusion and exclusion criteria) by reviewing case notes of consecutive CD patients attending outpatient clinics at three London teaching hospitals.
Results: Of the total 1258 patients, 1204 (95.7%) were ineligible due to the factors shown in the table. This includes 22 (1.7%) patients with clinically active disease who were excluded due to either a normal CRP/ESR (13, 1.0%) or a Crohn’s disease activity index (CDAI) of <220 (9, 0.7%). Of the 54 patients who met the inclusion criteria, 18 (33.3%) declined participation. Only 25 (46.3%) were recruited to our study and 11 (20.4%) to other studies within our unit, representing just 2.9% of the 1258 patients screened.
Conclusion: Few patients attending outpatient clinics are eligible for clinical trials in active CD which use standard entry criteria. Disease remission accounts for a large proportion. Increased availability and use of biological treatments is likely to reduce the number of eligible patients further. The population of patients excluded on the basis of CDAI and standard laboratory inflammatory markers includes some patients with evidence of inflammation on other (endoscopic/radiological) investigations, who require conventional therapy. Disease-defining criteria based on other (or several combined) features may increase recruitment whilst maintaining specificity. These data provide a rationale for the low involvement of CD patients in clinical trials and will enable researchers to estimate the potential recruitment of patients from similar patient populations.
ELEVATED FAECAL CALPROTECTIN LEVELS ARE ASSOCIATED WITH NEED FOR COLECTOMY IN ACUTE SEVERE ULCERATIVE COLITIS
G. Ho1, H. Lee1, G. Brydon1, N. Hare1, T. Ting1, H. Drummond1, A. Shand1, I. Penman1, D. Bartolo2, G. Wilson2, M. Dunlop2, I. Arnott1, K. Palmer1, J. Satsangi1. 1Gastrointestinal Unit, 2Department of Surgery, Western General Hospital, Edinburgh, UK
Introduction: Consistent data show that 30–40% of patients with acute severe ulcerative colitis (UC) will fail to respond to medical therapy and require emergency colectomy. Calprotectin, a granulocyte neutrophil-predominant cytosolic protein, is elevated in intestinal inflammation.
Aims & Methods: To investigate the role of faecal calprotectin as a non-invasive biomarker in predicting the clinical course of acute severe UC. In 94 consecutive patients (January 2005-September 2007), we investigated the discriminant ability of faecal calprotectin on admission to predict colectomy, corticosteroid and infliximab non-response.
Results: Overall, 33 (35.1%) required urgent colectomy, 22 (23.9%) patients were treated with infliximab (5 mg/kg) and 8 (36.4%) patients did not respond to infliximab. 64 (68.1%) patients had specific faecal calprotectin levels on admission for analysis. Overall, faecal calprotectin was high (1020.0 μg/g IQR: 601.5–1617.8); and was significantly associated with the need for urgent colectomy (1200.0 vs 887.2 μg/g, p = 0.04 in colectomy vs no colectomy respectively). There were strong trends to significance when comparing corticosteroid (1100.0 vs 863.5 μg/g, p = 0.08) and infliximab non-responders/responders (1795.0 vs 920.5 μg/g, p = 0.06) respectively. Using receiver-operator characteristic analysis, an area under curve of 0.65 (p = 0.04) was achieved in predicting need for colectomy. A cut-off value of 1922 μg/g yielded a maximum likelihood ratio of 9.23, specificity 97.6%, sensitivity 24.1%. Kaplan Meier analysis, showed significant association to subsequent need for colectomy (log-rank p = 0.02, median 0.90 years follow-up, IQR 0.49–1.39). There were no correlation with albumin (p = 0.33) and CRP (p = 0.23) in the acute setting.
Conclusion: This is the first dataset in acute severe UC to demonstrate that faecal calprotectin levels are dramatically elevated in severe UC. Furthermore, these analyses raise the possibility that this biomarker may predict response to first or second-line medical therapy in this setting.
THE ROLE OF MACROPHAGES AND LYMPHOCYTES IN ACUTE POUCHITIS
M. W. Johnson1, N. Gonzalez-Cinca2, J. R. Ellis2, A. Forbes3, P. J. Ciclitira2, R. Nicholls4. 1Gastroenterology, St Mark’s Hospital, Middlesex, 2Gastroenterology, St Thomas’s Hospital, 3Gastroenterology, University College London, 4Surgery, St Mark’s Hospital, London, UK
Introduction: Pouchitis is an acute inflammatory condition that can occur in patients post-restorative procto-colectomy, characterised by neutrophilic infiltration and ulceration of the mucosa. Neutrophils are clearly important in the pathogenesis of pouchitis, however, little is known about the role of macrophages and lymphocytes. Using immunohistochemical staining techniques we aimed to address this issue.
Aims & Methods: The pouchitis status of 27 ulcerative colitis patients was assessed using both the objective pouchitis score (OPS) and the pouchitis disease activity index (PDAI). Cut sections were prepared from pouch biopsies and incubated with stains using FITC conjugated monoclonal mouse anti-human primary antibody to CD3 (clone UCHT1, F0818, Lot 075, DAKO) and to CD68 (clone KP1, F7135, Lot 098, DAKO). A monoclonal mouse anti-human primary antibody to IL15 was also used following the manufacturers instructions (MAB647 clone 34505, lot AZX0, R&D systems). Stained sections were analysed using an LSM 510 laser scanning confocal microscope at 40× magnification. Three representative fields were captured per slide and stored in a jpeg format. Staining intensity was then assessed using Adobe Photoshop software. Statistical analysis was performed using Spearman rank (r) or Pearson’s (p) test (for Gaussian data).
Results: On average 9 luminosity results were collected for each of the 27 patients and their means were calculated as arbitrary units. Using the OPS, 11 patients had pouchitis and 16 had healthy ileal pouches. There was a statistically significant correlation between the intensity of the CD68 staining and the neutrophil score (r = 0.0184), acute histological score (r = 0.0028), endoscopy score (r = 0.025), and OPS (r = 0.04). No correlation was seen with the subjective PDAI (r = 0.061). Significant differences in CD 68 staining were noted between healthy and inflamed pouches (p = 0.019) using an unpaired t test. IL 15 staining correlated with that of the CD 68 (p = 0.0404). The CD3 staining correlated with the lymphocyte count (p = 0.04) but not with either of the disease activity scores (OPS p = 0.99, PDAI p = 0.85).
Conclusion: Lymphocytes do not appear to play a key role in the acute inflammatory process of pouchitis. The presence and degree of macrophage infiltration is, however, clearly related to the inflammation seen at both histological and endoscopic examination. It is likely that the macrophages play a vital role in both the innate and adaptive inflammatory processes. Interestingly, IL 15, typically produced by macrophages during innate immune response to environmental stimuli and infectious agents, closely correlated with the CD68 macrophage staining.
PREDICTORS OF 5-ASA PRESCRIPTION PERSISTENCE DURING THE CHRONIC PHASE IN PATIENTS WITH ULCERATIVE COLITIS
S. Kane1, S. Magowan2, N. Accortt3, D. Brixner4. 1Section of Gastroenterology and Nutrition, University of Chicago, Chicago, 2Medical and Technical Affairs, Procter and Gamble Pharmaceuticals, Cincinnati, 3Biostatistics, Procter and Gamble Pharmaceuticals, Cincinnati, 4Department of Pharmacotherapy, University of Utah, Salt Lake City, USA
Introduction: To identify predictive factors for 5-ASA non-persistence in patients with UC (defined as no repeat 5-ASA prescription at 12 months).
Aims & Methods: This retrospective cohort study used records of health service use from the Thomson Medstat MarketScan research database. Treatment initiation (index date) was defined as 5-ASA use between Oct 2002 and Sept 2004 with no 5-ASA use in the prior 6 months. Study subjects were patients ⩾18 years of age with a diagnosis of UC (ICD-9:556) in the period of interest and had repeated their prescription at 3 months post index date. Subsequent 5-ASA repeat prescription activity was captured at 12 months; chronic keepers were defined as individuals who repeated their 5-ASA prescription at 12 months (+/−30 days) whereas quitters did not repeat their prescription at 12 months (+/−30 days). Parameters of interest were captured from the 3 month time point until the 12 month time point and compared between keepers and quitters. Logistic regression modelling was used to identify independent predictors of non-repeat persistence.
Results: 2044 UC patients with 5-ASA prescriptions were identified; 920 patients (45%) did not repeat their 5-ASA prescription at 12 months. GI hospitalisation, comorbid illness, mail order, and younger age were among the parameters significantly associated with non-persistence. Factors not found to be significantly associated with persistence were gender, endoscopy, psychiatric history, steroid or immunomodulator use, number of GI office visits, and non-UC concomitant medications.
Conclusion: Persistence of maintenance therapy among UC patients taking 5-ASAs is multifactorial, though the factors related to persistence during the chronic disease phase differ somewhat from those of the acute phase, particularly sex and psychiatric history. Clinical knowledge of these factors can help with patient management.
PREVIOUS HISTORY OF STEROID USE DOES NOT PRECLUDE TREATMENT WITH MESALAZINE IN ULCERATIVE COLITIS
S. Katz1, B. R. Yacyshyn2, D. L. Ramsey3, G. R. Lichtenstein4. 1School of Medicine, New York University, New York, 2Medical and Technical Affairs, 3Biostatistics, Procter and Gamble Pharmaceuticals, Cincinnati, 4Department of Gastroenterology, Hospital of the University of Pennsylvania, Philadelphia, USA
Introduction: To determine the effect of high dose modified-release oral mesalazine (4.8 g/d) in patients with moderately active ulcerative colitis (UC) previously treated with oral or IV steroids.
Aims & Methods: Data from two multicentre, randomised, double-blind, active-controlled studies of similar design (ASCEND I and II) were combined and analysed. Efficacy and safety of modified-release mesalazine 4.8 g/d (800 mg tab) was compared with 2.4 g/d (Asacol, US marketed 400 mg tab) for treatment of mildly and moderately active UC. The primary efficacy variable in the combined analysis was treatment success in patients with moderately active UC (defined as baseline Physician’s Global Assessment (PGA) score = 2). Treatment success was defined as improvement from baseline at week 6 in PGA accompanied by improvement in at least one clinical assessment (stool frequency, rectal bleeding, patient functional assessment (PFA), or sigmoidoscopy findings) and no worsening in any of the remaining clinical assessments. Improvement was defined as a decrease from baseline of at least 1 point based on a 4-point scale (0–3). Improvement in the individual clinical assessments was also assessed.
Results: A total of 423 analysable patients with moderate UC were randomised in the two studies, of which 137 patients had received previous oral or IV steroid therapy. The incremental benefit of 4.8 g/d over 2.4 g/d was apparent in patients previously treated with steroids (p<0.01 stratified by protocol using CMH test). Improvement in the individual clinical assessments (rectal bleeding, stool frequency and sigmoidoscopy) further support the response of 4.8 g/d in patients previously treated with steroids compared to 2.4 g/day (p<0.05 stratified by protocol using CMH test). The 4.8 g/d dose of mesalazine was well tolerated, with adverse events comparable to 2.4 g/d.
Conclusion: A previous history of steroid use does not preclude treatment with mesalazine. There is a role for mesalazine in moderate UC patients previously treated with steroids. UC patients with moderately active disease previously treated with oral or IV steroids respond better to higher initial doses (4.8 g/d) of mesalazine.
USE OF FAECAL CALPROTECTIN TEST IN UK
V. Mahesh, D. Kejariwal, A. Aravinthan. Gastroenterology, Ipswich Hospital NHS Trust, Ipswich, UK
Introduction: Laboratory markers have an important role in inflammatory bowel disease (IBD) firstly, to gain an objective measurement of disease activity and secondly, to avoid unnecessary invasive procedures. Various serum markers in current use lack specificity as they may be increased by various conditions other than gut inflammation and therefore faecal markers would have a higher specificity for IBD. Faecal calprotectin (FC) is a well-validated objective faecal marker of intestinal inflammation in IBD and has been shown to be very useful in the diagnosis, differential diagnosis, monitoring of disease activity and prediction of relapse in IBD.1 2 Calprotectin is a cytosolic protein in granulocytes and hence FC is directly proportional to neutrophil migration to the intestines. Despite the evidence, FC has been less extensively employed in UK as a measure of disease activity compared to other laboratory markers.
Aims & Methods: This study’s purpose was to examine the use and awareness of faecal calprotectin as a biomarker among gastroenterologists in UK. A survey was emailed to 1154 non-trainee members of the British Society of Gastroenterology. Only 995 emails could be delivered. Respondents were asked to describe their awareness of the test as well as their clinical experience in its use.
Results: 135 (13.5%) members responded. Only 37% of the respondents used FC in their clinical practice. Interestingly 62% of the respondents who have not used FC would recommend its use in IBD. More than 75% respondents felt FC was a good test to distinguish IBD from irritable bowel syndrome as well as distinguishing inflammatory from non-inflammatory causes of relapse in IBD. Fifty five per cent of the respondents felt FC would be useful in predicting relapse in IBD.
Conclusion: We conclude that a substantial number of gastroenterologists under use faecal calprotectin as a biomarker in IBD. The comments received suggested lack of funding and awareness besides patients’ reluctance to perform stool tests as the barriers to its under use. FC is cheap and simple to perform which requires only 5g of spot stool sample and needs no dietary restrictions. Use of FC along with other serum markers in IBD may help us in making better therapeutic decisions and optimising the use of invasive procedures.
INFLAMMATORY BOWEL DISEASE IN HIV SEROPOSITIVE INDIVIDUALS: ANALYSIS OF A LARGE COHORT
J. Landy, M. Harbord, B. G. Gazzard. Gastroenterology, Chelsea and Westminster, London, UK
Introduction: It is not known whether HIV infection influences the pathogenesis of IBD. We examined the prevalence of IBD between 1999 and 2006 in a very large cohort of HIV seropositive patients and assessed the relevance of CD4 count to IBD onset.
Aims & Methods: HIV clinic and pharmacy databases at the Chelsea and Westminster Hospital were searched. A diagnosis of IBD was confirmed by review of endoscopy and histology records. Infectious colitis was excluded by review of microbiology records. Patients referred for a specialist “tertiary” opinion were excluded.
Results: 23 patients were identified with a diagnosis of both HIV and IBD. All 23 patients were male. Median age was 45 years (IQR 12). 6 patients were diagnosed with IBD before HIV. Of the 17 patients subsequently diagnosed with IBD, 4 had left sided/extensive ulcerative colitis, 5 proctitis, 1 Crohn’s disease and 7 indeterminate colitis. Median CD4 count at the time of IBD diagnosis was 355 cells/mm3 (IQR 180 cells/mm3). There was no significant change in CD4 count 6 months before or after IBD was diagnosed (median +18 cells/mm3, IQR +58). The mean annual incidence of UC and CD was 1.9/10 000 and 0.2/10 000 respectively.
Conclusion: Our cohort is the largest reported with a combined diagnosis of HIV and IBD. The incidence of UC is about double that expected in a normal population, although less than that published previously.1 There is no clear association with CD4 count and the time of diagnosis of IBD.
CERVICAL DYSPLASIA AND IBD: NO EFFECT OF DISEASE STATUS OR IMMUNOSUPPRESSANTS ON ANALYSIS OF 2055 SMEAR RECORDS
C. W. Lees1, J. Critchley1, N. Chee1, R. E. Gailer1, A. R. W. Williams2, A. G. Shand1, I. D. R. Arnott1, J. Satsangi1. 1Gastrointestinal Unit, Western General Hospital, 2Department of Pathology, Royal Infirmary of Edinburgh, Edinburgh, UK
Introduction: It has been variously reported that there is an increase in cervical dysplasia and neoplasia in women with inflammatory bowel disease (IBD) taking immunosuppressive therapy. However, this has not been studied in sufficient detail for meaningful clinical interpretation.
Aims & Methods: We aimed to assess in a large, case-controlled population whether women with IBD had increased rates of abnormal cervical smears and whether there was any effect of immunosuppressive therapy or disease phenotype. Women diagnosed with IBD prior to the age of 60 were identified from the pre-existing IBD database in Edinburgh. Full cervical smear histories were available on 411 women (204 Crohn’s disease, 207 ulcerative colitis, median age at diagnosis 28 years, median current age 45 years). Disease phenotyping, including detailed drug and smoking data, was collected by case-note review. Fertility, pregnancy and menstrual history was available on 49.9% of women. All the cases were matched 4:1 to healthy controls (n = 1644) from the same geographical location (Lothian, Scotland). Cervical pathology was classified as negative, low-grade (borderline smear and CINI) and high-grade (CINII-III and cervical cancer), reflecting clinical relevance.
Results: There was no difference in rates of abnormal smears between patients with IBD (80.5% negative, 10.5% low-grade and 9.0% high-grade) and controls (82.2%, 10.2% and 7.5%, p = 0.60). 2/411 (0.5%) cases (1 CD, 1 UC) had cervical cancer; neither had immunosuppressive therapy, but both were current smokers. The use of immunosuppressants (azathioprine, mercaptopurine and methotrexate) and anti-TNF therapy had no impact on rates of cervical dyplasia or neoplasia. Furthermore, there was no effect of disease location or behaviour on cervical pathology. However, there were significantly more abnormal cervical smears in IBD patients who were current smokers compared with those who had never smoked (36.5% vs 15.9%, p = 0.0002, OR 3.04, CI 1.72 to 5.35). Pregnancy and use of the oral contraceptive pill did not affect incidence of cervical dysplasia.
Conclusion: The rates of cervical dysplasia and neoplasia are the same in patients with IBD as in the background population, and this is not affected by the use of immunosuppressants. However, young women with IBD who smoke are at increased risk of cervical dysplasia. These data suggest that young women with IBD should be managed as per the background population, attending for regular smear testing and undergoing vaccination against cervical cancer when available.
EXPRESSION ANALYSIS OF ALL GENES IMPLICATED IN SUSCEPTIBILITY TO CROHN’S DISEASE ON GENOME-WIDE ASSOCIATION STUDIES
C. W. Lees1, C. L. Noble1, L. Diehl2, J. Satsangi1. 1Gastrointestinal Unit, Western General Hospital, Edinburgh, UK, 2Department of Pathology, Genentech Inc, San Francisco, USA
Introduction: Genome-wide association studies in the UK, Belgium, Germany and North America in the past 12 months have identified several new genes directly implicated in the pathogenesis of Crohn’s disease (CD). These include IL-23R, ATG16L1, IRGM, NKX2.3 and PTPN2. Ongoing meta-analysis of UK, Belgium and American datasets and subsequent replication studies promise to yield another several CD genes that did not meet genome-wide significance (p<10−7) on the individual scans. However, little is known of the direct functional relevance of many of these genes in CD and indeed UC.
Aims & Methods: We aimed to analyse the expression profiles of all CD susceptibility genes from our existing genome-wide microarray dataset. Microarray expression data (Agilent platform) were available on colonoscopic biopsies from 53 CD and 67 UC patients and 33 healthy controls (HC). The major findings from this dataset have previously been presented (Noble et al, BSG 2007 and submitted). The Agilent probes for each gene were identified from existing databases. In addition to IL-23R, expression of IL-23A (p19), IL-23B/IL-12B (p40) and IL-12A (p35) were analysed. No microarray expression data were available for IRGM. For regions of extensive linkage disequilibrium, all genes in the area of association were analysed. The expression profiles for each gene were compared in CD vs HC and UC vs HC and then further analysed by the inflammatory status of the disease biopsies.
Results: The expression of the autophagy gene ATG16L1 was significantly lower in CD vs HC biopsies regardless of inflammatory status (p = 0.0017), but there was no difference between UC and HC. NKX2.3, a homeobox gene critical to normal intestinal development, was expressed at higher levels in inflamed and non-inflamed CD vs HC (p<0.001) and inflamed UC vs HC (p<0.0001), but not in non-inflamed UC biopsies. There was no difference in expression profiles of IL-23R in inflamed or non-inflamed CD or UC samples and HC. However, IL-23A (p19) was increased in inflamed CD and UC compared with controls (p<0.0001). There were no significant differences in expression profiles of IL-12B (p40) or IL-12A (p35). PTPN2 did not show any consistent expression differences between CD, UC and HC. Data on all confirmed and replicated genes/regions from the ongoing international meta-analysis will be presented.
Conclusion: These expression data provide the first insights into the potential functional relevance of a series of exciting new discoveries in CD genetics based on genome-wide association scanning. Key expression differences are noted for ATG16L1 in CD, NKX2.3 in CD and UC and the IL-23 pathway in intestinal inflammation.
11 YEAR AUDIT OF THE MANAGEMENT OF SEVERE ULCERATIVE COLITIS IN A DISTRICT GENERAL HOSPITAL
A. G. Lim1, H. Sharma1, C. Jefnes2. 1Department of Gastroenterology, Epsom General Hospital, Epsom, UK, 2Audit department, Epsom General Hospital, Epsom, UK
Introduction: In 2000 we reported a 6-year audit into the outcome of patients treated with severe ulcerative colitis (UC) in our hospital. We found an unexpectedly high mortality, 6 deaths in 32 cases (19%). Factors associated with this high mortality included care by non gastroenterologists and delays to surgery. Changes in practice were implemented. Furthermore, intravenous cyclosporin was introduced as an option for patients who failed to respond to intravenous steroids.
Aims & Methods: We now report on a re-audit of the next 5 years (2000–5). All in-patients coded as having UC were identified, the notes reviewed and data collected on a proforma. Patients were considered to have severe UC as defined by Truelove and Witt’s criteria. 88% (352/400) of the identified notes were reviewed. There were 32 episodes of severe colitis in 30 patients (median 42.25, range 18–80). In these patient episodes, 96% of patients had stool cultures and abdominal x rays on admission. All patients not known to have colitis were treated with antibiotics. All patients received IV steroids within 72 hours and all patients had subcutaneous heparin. The table shows outcome data from 1994–9 compared with 2000–5.
Results: In the current audit, at day 10 there were 17 cases who failed to achieve complete response to steroids, 5 went directly to colectomy and 12 received intravenous cyclosporin. Of these patients, only 3 responded to cyclosporin but 09 went on to colectomy. At final outcome, 18 patients left hospital without surgery, 14 had colectomy but there were no deaths.
Conclusion: Following the first audit, changes introduced included the care of all in-patient UC by gastroenterologists with formal shared care with colorectal surgeons. This has led to early identification of patients not responding to medical therapy and expedited surgery. This has resulted in improved mortality outcome. The use of intravenous cyclosporin as salvage therapy was disappointing as a means of avoiding surgery in our cohort.
A STUDY OF PATIENTS’ UNDERSTANDING OF THE ROLE OF CHEMOPROPHYLAXIS AND DRUG COMPLIANCE IN CROHN’S AND ULCERATIVE COLITIS
A. E. Low1, M. Love1, B. Gannon2, K. Kane1, R. Walt1, R. Eksteen3, C. May3, J. Goh1. 1Department of Gastroenterology, 2Liver Unit, 3Department of Liver Medicine, University Hospital Birmingham NHS Trust, Birmingham, UK
Introduction: Inflammatory bowel disease (IBD) is a known risk factor for colorectal cancer.1 Surveillance techniques are far from perfect. Therefore gastroenterologists focus more on chemoprophylaxis, in particular with mesalazine (5-ASA), and ursodeoxycholic acid (UDCA) for colitis Primary sclerosing cholangitis (PSC). Evidence for a chemopreventative effect of these medications is accumulating,2 yet little is known about patients’ understanding of this relatively novel therapeutic role, which may influence drug compliance.
Aims & Methods: To assess patients’ compliance and understanding of 5-ASA or UDCA treatment. We conducted a questionnaire based study which comprised self assessment of compliance and perception of reasons for being on the drugs using a 5 point opinion scale. Questionnaires were sent to a representative sample of 74 patients with PSC/IBD (post-liver transplant) and 192 patients with colitis only.
Results: Response rates were 42/74 (56%) and 114/192 (59%). In total, 98/151 (64%) claimed full compliance; 78% for the PSC/IBD group, and 60% in the IBD only group. 84% patients considered daily compliance with 5-ASAs and UDCA during remission to be very important. 62% of patients had had a flare of their symptoms in the past year. This group had higher compliance rates than those who were stable. Overall, 114/151 (75%) stated they understood the reasons for taking the drugs. 76/151 (50%) patients however, were unaware of any link of their condition to bowel cancer (14/37 PSC/IBD and 62/114 IBD), or that 5-ASA or UDCA may potentially reduce cancer risks. Among the IBD only group, 91/114 (79%) patients felt their compliance would be improved if they were informed of the chemoprophylactic potential of the medication. Patients were asked to give their own recommendations of how we could improve their compliance. Suggestions included providing printed information and updates on research in the area. Most wanted more information on the links between their condition and bowel cancer. 94% of patients felt that evidence showing reduced risk of bowel cancer with 5-ASA would improve their compliance.
Conclusion: Despite good self-reported compliance, half of the patients are unaware of an association between colitis and bowel cancer. Explaining the potential chemoprophylactic benefits, in addition to helping maintain remission, may enhance patients’ compliance and improve the doctor patient relationship.
ORAL CALCIUM AND VITAMIN D SUPPLEMENTATION HELPS MAINTAIN BONE MASS IN INFLAMMATORY BOWEL DISEASE. A RANDOMISED, DOUBLE BLIND, PLACEBO CONTROLLED TRIAL
P. F. Marden1, D. Robertson1, G. Taylor2, A. Bhalla3, A. Holdoway4, W. Fickling1. 1Gastroenterology, Royal United Hospital, 2Statistics, Bath University, 3Rheumatology, RNHRD, 4Dietetics, Royal United Hospital, Bath, UK Kingdom
Introduction: The aims of this randomised control trial were to see whether, in patients with inflammatory bowel disease, calcium and Vitamin D supplements: (1) improved bone density compared with placebo over 24 months; (2) bone turnover markers would predict a response to such supplementation; (3) dietary calcium intake predicted a response to supplementation.
Aims & Methods: Patients with IBD were randomised to 1000 mg of calcium and 800 units of cholecalciferol or placebo. Bone mineral density (BMD) was measured at 0, 6, 12 and 24 months. Bone turnover markers were recorded at 0 and 12 months. 56 patients also had results analysed based on their baseline dietary intake of greater or less than 700 mg calcium per day.
Results: 46 patients were randomised to receive placebo and 49 to calcium and Vit D. A statistically significant different percentage change from baseline in all BMD measurements over 24 months was seen in the Lumbar BMD 0.8914±0.42445 p = 0.040, trochanter 1.3581±0.47662 p = 0.006 and Total BMD 1.2948±0.50962 p = 0.014. No statistically significant positive changes were seen in the placebo group only the calcium and Vit D. At 6 months the percentage change in BMD was statistically different between the two groups at the trochanter, with a total trochanteric BMD percentage change of 0.13±0.34850 in the placebo group and 1.4386±0.53163 in the active group (p = 0.044). At 12 months a statistically significant difference was seen in the total T (p = 0.046), Intertrochanteric Z (p = 0.048), lumbar Z (p = 0.046) and Total BMD (p = 0.045) measurements. At 24 months only the Total T and Total Z BMD score with p = 0.049 and 0.04 respectively were significantly different between groups. No statistically significant changes in percentage and absolute change in bone turnover markers are seen when the Vit D and placebo groups are compared. Ten patients were found to have a calcium intake of <700 mg/day and in this group statistically significant differences between the two treatment arms percentage change in BMD were seen in the Total BMD (placebo −2.5% vs Ca Vit D 2.56% p = 0.033) and intertrochanteric BMD (placebo −3.7845% vs Ca and Vit D 1.54516% p = 0.05). No difference was seen in the >700 mg group.
Conclusion: This trial shows treatment with calcium and Vit D improves and maintains bone mineral density measurements in patients with inflammatory bowel disease and the use of bone turnover markers to assess such treatment is not helpful. When dietary intake at baseline is taken into account the patients with poor dietary calcium intake have a greater benefit than those with normal calcium intakes.
COLORECTAL CANCER PREVENTION IN ULCERATIVE COLITIS: THE PRESCRIBING HABITS OF BRITISH GASTROENTEROLOGISTS
H. F. Mayberry, T. Moshkovska, J. F. Mayberry. Department of Digestive Diseases, University Hospitals of Leicester, Leicester, UK
Introduction: It is now generally accepted that 5-ASA compounds can reduce the risk of colorectal cancer amongst patients with extensive or pancolitis. This phenomenon does not seem to be directly related to control of disease flare-ups as it is not seen with azathioprine of 6 mercaptopurine. As a result gastroenterologists are faced with the dilemma of needing to decide whether to co-prescribe 5-ASA compounds with immune-modulators.
Aims & Methods: The purpose of this study was to identify the current practice of senior British gastroenterologists in relationship to the chemoprevention of colorectal cancer in ulcerative colitis through their prescription of 5ASA compounds, immune modulators and folic acid. The email addresses of 254 senior gastroenterologists were identified from the Handbook of the British Society of Gastroenterology. They were each sent a questionnaire about colorectal cancer prevention for patients with ulcerative colitis. The questionnaire dealt with use of 5-ASA compounds and immune modulators and the duration of treatment, as well as the prescription of folic acid. Details were collected on the occurrence of neutropaenia as a side effect. Completed questionnaires were returned to a central email address for analysis. The group of gastroenterologists were polled and re-polled until no further responses were returned to the central address.
Results: Ninety seven completed questionnaires were received. Of these senior clinicians 91 recommended lifelong therapy with 5-ASA compounds for patients with extensive or pan-colitis. In 90 cases they prescribed the medication on a daily basis. Seventy two clinicians, who prescribed azathioprine or 6 mercaptopurine for patients with colitis of this extent, also co-prescribed 5-ASA compounds. Again in all but one case they recommended that this treatment should be given on a daily basis. The median percentage of patients reported by these clinicians as being on both drugs was 20% (interquartile range 10–50%). Neutropaenia was seen in a median percentage of 3.5% of patients (interquartile range 1–5%). Only 3 clinicians prescribed daily folic acid in an attempt to reduce colorectal cancer risk amongst patients with extensive or pan-colitis.
Conclusion: 72 of 97 senior clinicians in the British Isles co-prescribe 5-ASA compounds for patients whose colitis is controlled by immune-modulators with a median of 20% of patients on such therapy on a life long basis. This practice is followed although there are no long term trials to support it.1 Although concerns have been expressed over the possibility of neutropaenia being more frequent amongst such patients this does not appear to be borne out in practice.
COMBINATION ANTIBIOTIC THERAPY IS EFFECTIVE IN THE TREATMENT OF PRE-POUCH ILEITIS FOLLOWING RESTORATIVE PROCTOCOLECTOMY
S. D. McLaughlin1, A. J. Bell2, S. K. Clark3, P. P. Tekkis1, P. J. Ciclitira4, R. J. Nicholls1. 1Department of Biosurgery and Surgical Technology, Imperial College, London, 2Department of Gastroenterology, Weston-Super-Mare General Hospital, Somerset, 3Department of Surgery, St Mark’s Hospital, 4Department of Gastroenterology, King’s College London, London, UK
Introduction: Pre-pouch ileitis (PI) is a recently described condition1 which may occur following restorative proctocolectomy. There are no published data on effective treatment and its aetiology is unknown. We report a series of 11 patients treated and followed up with repeat pouchoscopy.
Aims & Methods: 12 consecutive patients with symptomatic PI were treated with 28 days of ciprofloxacin 500 mg bd and metronidazole 400 mg bd. Symptomatic, endoscopic and histological assessment was performed before and following treatment using the pouchitis disease activity index (PDAI) with a score of 7 or more indicative of pouchitis. All had concurrent pouchitis. The Wilcoxon rank-sign test was used to analyse the differences.
Results: See table. 9 patients (82%) entered symptomatic remission. 6 patients (67%) patients had either resolution of PI or a reduction in length of PI. The reduction in stool frequency was significant; p = 0.008. The reduction in length of PI was significant; p = 0.028.
Conclusion: Our results suggest that combination antibiotic therapy is effective in reducing the length of PI, furthermore it induces symptomatic remission in most patients even where there is no change in the degree of PI. These results suggest the aetiology of PI and pouchitis are similar and a bacterial dysbiosis may be causative. Affected patients should be treated with combination antibiotic therapy.
EVIDENCE FOR A BACTERIAL DYSBIOSIS IN POUCHITIS AFTER RESTORATIVE PROCTOCOLECTOMY USING 16 S RRNA SEQUENCING: PRELIMINARY REPORT OF AN ONGOING STUDY
S. D. McLaughlin1, L. Petrovska2, A. Walker3, S. K. Clark4, M. W. Johnson5, P. P. Tekkis6, J. Parkhill3, G. Dougan3, P. J. Ciclitira5, R. Nicholls6. 1Department of Biosurgery and Surgical Technology, Imperial College, London, 2Nutritional Sciences Research Division, King’s College, 3The Wellcome Trust Sanger Institute, Cambridge University, Cambridge, 4Department of Surgery, St Mark’s Hospital, 5Nutritional Sciences Research Division, King’s College, 6Department of Biosurgery and Surgical Technology, Imperial College, London, UK
Introduction: Restorative proctocolectomy (RPC) is the operation of choice for ulcerative colitis (UC) and some with familial adenomatous polyposis (FAP). Pouchitis is the most common complication following RPC. A bacterial dysbiosis has been proposed as the cause of this inflammatory process. Bacterial phyla in the ileal pouch mucosa were identified using the highly sensitive 16s rRNA PCR sequencing technique.
Aims & Methods: Ileal pouch biopsies were taken from pouch patients as follows: ulcerative colitis (UC) non-inflamed 4, UC pouchitis 7, familial adenomatous polyposis (FAP) non-inflamed 6, FAP pouchitis 2. PCR was performed using universal 16s rRNA primers on the DNA extracted from the biopsies. Clone libraries were sequenced using high-throughput DNA sequencing. The Ribosomal database project1 was used to identify bacterial phyla from the sequences. Chi-squared was used to analyse the differences between the groups.
Results: See table. Bacteria from the phyla Actinobacteria, Bacteroidetes, Firmicutes and Proteobacteria phyla were identified in all samples. A small number of sequences were found in some patients from Deinococcus-thermus, Verrucomicrobia, Fusobacteria and Cyanobacteria phyla. UC pouchitis patients had a significantly higher proportion of Proteobacteria and significantly lower proportion of Bacteroidetes compared with the other groups. UC pouch controls had a significantly higher proportion of proteobacteria and significantly lower proportion of firmicutes compared with FAP pouch controls (p<0.0005).
Conclusion: This is the first study giving data on bacterial taxonomy to suggest that a bacterial dysbiosis may occur in pouchitis. Furthermore this study suggests that there is a significant difference in the composition of microflora within FAP and UC pouches. Further work is in progress to identify individual bacterial species in a larger patient group.
Oesophagus posters
BACTERIAL COLONISATION OF MUCOSAL SURFACES IN BARRETT’S OESOPHAGUS
K. L. Blackett, G. T. Macfarlane, S. Macfarlane, J. F. Dillon. Dundee University Gut Group, Ninewells Hospital and Medical School, Dundee, UK
Introduction: Barrett’s oesophagus (BO) is a consequence of chronic gastro-oesophageal reflux disease. Barret’s patients have an increased risk of oesophageal dysplasia and adenocarcinoma (AD), which is now the seventh most common cause of cancer death in the UK. All adenocarcinomas are thought to arise in Barrett’s, and over the last two decades there has been an increase in both BO and AD. The reasons for this are unclear, however, it is possible that there may be a microbial aetiology. The objectives of this investigation were to characterise microbial communities in oesophageal aspirates, and on distal oesophageal mucosae of BO patients.
Aims & Methods: Biopsies and aspirates were taken at endoscopy from 11 patients with BO, and nine controls with no oesophageal disease. Samples were cultured under aerobic, anaerobic and microaerophilic conditions for bacteria and yeasts. The isolates were identified by 16S rRNA gene sequencing, and analysis of cellular fatty acid methyl ester profiles. FISH in conjunction with confocal laser scanning microscopy (CLSM) was also used to determine the spatial localisation of these organisms in mucosal biofilms.
Results: Significant microbial colonisation of the oesophagus was observed in both BO patients and controls. Overall, 54 bacterial species belonging to 24 genera were identified, with only 10 species being common to both subject groups. Aspirates and tissues from BO patients contained complex populations of micro-organisms. Unusually, high levels of Camplylobacter concisus and C rectus, which are associated with tumour formation and enteritis in animals, as well as periodontal infections in humans, were found in 5/11 (45%) of BO patients, but not in any of the controls. CLSM demonstrated that micro-organisms in mucosal biofilms frequently occurred in microcolonies.
Conclusion: The presence of atypical nitrate-reducing campylobacters in BO patients indicates that there could be a link in either the promotion or exacerbation of disease processes leading to AD.
A LONG-TERM IN VITRO MODEL OF ADULT OESOPHAGUS FOR INVESTIGATING THE PATHOGENESIS OF BARRETT’S OESOPHAGUS
B. J. Colleypriest, D. Tosh, J. M. Farrant, J. M. W. Slack. Biology and Biochemistry, University of Bath, Bath, UK
Introduction: Investigating the pathogenesis of Barrett’s metaplasia requires a long term in-vitro model of normal oesophagus. Three culture techniques are possible, explant, primary cell and immortalised cell lines, to attempt this. Explant culture offers the advantages of a mixed cell population, allowing epithelial mesenchymal interactions, and uses more physiologically normal non-immortalised cells.
Aims & Methods: The aim was to achieve a long-term explant culture model of adult oesophagus that was representative of adult oesophagus. Epithelium was seeded onto plastic coverslips and cultured in supplemented Basal Medium Eagle. The morphology of the cells in culture was assessed with immunohistochemistry.

Results: Explants remain viable in culture for at least 35 days. An outgrowth of cells, containing a mixed population of epithelial and connective tissue cells, surrounds the original tissue and continues to increase in size and cell number. The epithelial component of the outgrowth differentiates similarly to the in vivo oesophagus with the presence of cells expressing cytokeratin 14, involucrin and loricrin representing spectrum of cell types. p63, a gene essential to squamous differentiation, is demonstrated in the epithelium.
Conclusion: Long-term culture of adult oesophagus has proven difficult in the past. The technique described allows for a long term culture which faithfully represents the cell types found in vivo. Furthermore the explant culture results in a mixed population of connective tissue and epithelial cells without using immortalised or cancerous cells. The model offers the unique ability to test exogenous compounds on all types of oesophageal cells and the possibility of ectopic gene expression.
EFFECT OF SELENIUM STATUS AND ACID EXPOSURE ON CELLULAR PROLIFERATION IN A BARRETT’S OESOPHAGUS-DERIVED OESOPHAGEAL ADENOCARCINOMA CELL LINE
A. H. Goh1, K. Park2, I. Broom1, G. Bermano1. 1Centre for Obesity Research and Epidemiology, The Robert Gordon University, 2Department of Surgery, Aberdeen Royal Infirmary, Aberdeen, UK
Introduction: The incidence of oesophageal adenocarcinoma (OA) in the Western world has risen sharply over the last three decades. The UK has the highest incidence rate in Europe. The cause of this rising trend remains unknown. Symptomatic gastro-oesophageal reflux disease (GORD) and associated oxidative stress have been suggested to be involved in the development of OA. Selenium (Se) is a trace element that plays an important role in the fight against oxidative stress in human tissues. High serum Se has been associated with a lower incidence of oesophageal and gastric cancer.
Aims & Methods: The aim of this study is to investigate the effect of acid pulse and Se status on proliferation and apoptosis in a BO-derived OA cell line. FLO-1, a BO-derived OA cell line, was cultured under Se deficient, Se adequate (40 nM Sodium Selenite) and Se supplemented (100 nM Sodium Selenite) conditions. Cells were exposed to an acid pulse (pH 5.0) for 1 h to simulate acid reflux disease in the oesophagus and then harvested 1, 3 or 24 h after treatment. Control cells were cultured at pH 7.0. Cell proliferation was assessed by measuring Proliferating Cell Nuclear Antigen (PCNA) expression by Western blotting and by MTT assay. Expression of total Caspase 3 was measured by Western blotting as an index of cell apoptosis.
Results: PCNA production was increased by 47%, 3 and 24 h after the acid pulse in Se adequate cells compared to the control cells cultured at pH 7.0. On the contrary, PCNA production was decreased (∼10%) in Se deficient cells at 3 and 24 h after acid pulse. Production of total Caspase 3 was increased by 66%, 1 h after acid pulse in Se adequate cells compared to Se adequate cells cultured at pH 7.0. The acid pulse did not affect total Caspase 3 expression in Se deficient cells. Supplementation of cells with Se (100 nM) abolished the increase in proliferation observed in Se adequate cells after acid exposure, as measured by MTT assay.
Conclusion: These preliminary data suggest that Se supplementation may protect cells from acid-induced stress, abolishing the adverse effects on proliferation and apoptosis observed in Se adequate cells exposed to the acid pulse. They provide preliminary evidence for a role of Se supplementation in the prevention of OA.
DEOXYCHOLIC ACID HAS A THRESHOLDED DOSE RESPONSE FOR DNA DAMAGE
G. J. S. Jenkins, J. Cronin, Z. Eltahir, P. Griffiths, T. Thomas, J. Baxter. School of Medicine, Institute of Life Science, Swansea, UK
Introduction: Bile acids are implicated in oesophageal adenocarcinoma development. Deoxycholic acid (DCA), a secondary bile acid, is associated with histological progression in Barrett’s oesophagus1 and is known to induce DNA damage and initiate oncogenic signalling.2 3 The amount of DCA in oesophageal aspirates has been shown to range widely from 0 μM to 280 μM.1 It is possible that the actual level of bile acids (like DCA) reaching the oesophagus is an important determinant in neoplastic development.
Aims & Methods: We aimed to assess the dose dependency of DCA in causing DNA damage. We have used the micronucleus method to measure chromosome damage (the appearance of fragments of chromosomes or micronuclei) in DCA treated OE33 cells. We have studied large numbers of cells post treatment across a previously defined dose range to assess the shape of the dose response. We have also assessed the dose response of DCA to the induction of oncogenic signalling (by real-time PCR of NF-κB regulated genes).
Results: We have shown that DCA displays a thresholded dose response for DNA damage. That is, there is a non-linear dose relationship, with low doses of DCA causing no increase in chromosome damage above the background level. At a dose of 125 μM, there is a point of inflection in the curve, with subsequent increases in chromosome damage. This effect was similar for DCA’s ability to induce oncogenic NF-κB signalling.
Conclusion: Low doses of DCA exposure to oesophageal cells do not induce chromosome damage nor oncogenic signalling. However, doses of 125 μM or more are effective at inducing these events. This threshold effect is presumably due to the indirect manner in which DCA causes chromosome damage (and oncogenic signalling). We have previously shown that DCA induces chromosome damage via the generation of ROS.3 Hence antioxidant defences are probably responsible for the initial protection against DCA at low doses. At higher doses, this protection is lost as DCA overcomes the antioxidant protection. Therefore, in refluxing patients, neoplastic risk may be associated with the amount (and subtype) of bile reflux. This may suggest that the amount of DCA (or other bioactive bile acid) in patient refluxate may be a useful biomarker of cancer risk.
IDENTIFICATION AND VALIDATION OF BIOMARKERS FOR USE IN BARRETT’S OESOPHAGUS SCREENING
P. Lao-Sirieix1, A. Boussioutas2, L. Harihar1, R. C. Fitzgerald1. 1Cancer Cell Unit, Hutchison-MRC Research Centre, Cambridge, UK, 2Peter MacCallum Cancer Centre, Melbourne, Australia
Introduction: The majority of patients with Barrett’s oesophagus (BO) are undiagnosed and therefore screening has been advocated to facilitate early detection of oesophageal adenocarcinoma. We have previously demonstrated that non-endoscopic screening is feasible using a sampling device called a capsule sponge. The swallowed capsule expands to a spherical sponge within the stomach and is pulled out using a string. Since the device collects cells continuously from gastric cardia (GC) to the oro-pharynx, it is essential to identify biomarkers specific for BO and absent in the adjacent tissues (normal oesophagus (NE) and GC).
Aims & Methods: The aims of this study were to identify novel biomarkers which will discriminate between cellular subtypes and to validate them for BO screening. Three publically available datasets from spotted cDNA arrays were used to identify putative biomarkers. Analysis 1: Dataset 1 (15 NE and 14 BO) was analysed, using a one-tailed t test with a Bonferroni correction, to identify genes whose expression was significantly upregulated in BO (log2 ratio >2) compared to NE (<1), (p<0.0001). This list was then used to interrogate dataset 2 (57 gastric samples (G)) for genes that were under-expressed in G (<1). Analysis 2: Dataset 3 (39 NE and 26 BE) was analysed in a similar fashion to dataset 1 to produce a set of genes with BE>2, NE<1 and then this list was compared to dataset 3 to identify genes with a low expression in G (<1), (p<0.0001). Genes common to both analyses were considered for further validation by real-time PCR in endoscopic biopsies of NE, BO and GC (n = 10 for each). Expression was further determined by immunohistochemistry on 11 NE, 32 BO with IM, 20 G and 17 duodenum (D2). Trefoil factor 3 (TFF3) immunostaining was scored as 0, 1+, 2+ or 3+ compared to positive control D2.
Results: 24 genes were identified from analysis 1 and 93 from analysis 2. 14 genes overlapped between the two analyses: AGR2, ATP7B, DAPK1, DDC, FBP1, FM05, FOXA3, FUT4, GOLPH2, LYZ, PLCL2, RNASE A, TFF1 and TFF3. By RT-PCR only the mRNA expression of dopa-decarboxylase (DDC) and Trefoil Factor 3 (TFF3) were confirmed to be upregulated in BE compared to NE (p<0.001 for both) and GC (p<0.01 and p<0.05 respectively). Immunohistochemical analysis confirmed that DDC was only expressed in biopsy specimens from BE but was confined to <1% of the cells within the crypt compartment. This would preclude its use in an immunocytological test which samples the epithelial surface. In contrast, TFF3 protein was expressed to high levels in BE (median 3+) compared to NE (median 0) and GA (median 0) at the luminal surface of the tissue. Only 1/20 gastric sample had expression of TFF3 at the luminal surface.
Conclusion: TFF3 is a very promising screening marker since it is expressed at the luminal surface of BE but not in adjacent tissue types such as normal oesophagus and stomach. We are currently testing the antibody in specimens collected from the capsule sponge.
DIFFERENTIAL EFFECTS OF TNF-α ON OESOPHAGEAL CELL LINES ALONG THE METAPLASIA-DYSPLASIA-ADENOCARCINOMA SEQUENCE
A. M. Nicholson, R. Arscott, A. Milicic, J. J. A. Jankowski. Clinical Pharmacology, University of Oxford, Oxford, UK
Introduction: Inflammatory response is known to have a role in the early stages of Barrett’s metaplasia. Oesophageal tissue levels of TNF-α in particular increase along the metaplasia-dysplasia-adenocarcinoma sequence. However, much less is known about how inflammatory signalling could differentially affect the clonal expansion of Barrett’s lesion that leads to increased malignancy.
Aims & Methods: Expression levels of TNF-α and TNFR1 in squamous (EPC), Barrett’s (Qh-TERT), high-grade dysplasia (Gilh-TERT), squamous carcinoma (OE21) and adenocarcinoma cell lines (OE33, SEG1 and TE7) and tissue biopsies were assessed using ELISA and Western blotting. Biopsy explants of squamous epithelium, Barrett’s epithelium and stomach fundus taken from 5 patients were treated with TNF-α (50 ng/ml) and immunostained for Ki67 and active caspase 3. In vitro, the effect of TNF-α was investigated using assays for cell proliferation, cell cycle, apoptosis and migration. TNF-\alpha inhibitor Infliximab was used in all assays at 10 μM to test for specificity of the observed TNF-α effect.
Results: There was <1 pg of TNF-α per μg total protein, in both the biopsies and the cell lines analysed. We noted a significantly higher level of TNF-α in the squamous compared to the fundus tissue (p<0.05). Within the explants we observed considerable heterogeneity in cell proliferation and apoptosis in response to TNF-α stimulation. To investigate the role of TNF-α further we exploited a variety of oesophageal cell lines. The EPC cell line produced highest endogenous level of TNF-α but had low levels of TNFR1 and was less responsive to TNF-α stimulation. Effects of TNF-α on the cell cycle after 24 h/48 h differed among the cell lines, causing apoptosis in OE21 (p<0.01) and SEG1 (p<0.01) and having no significant effect on OE33 and TE-7 lines. No effect of TNF-α on the cell cycle of cell lines derived from normal squamous, Barrett’s and dysplastic tissue was observed. Only the TE-7 and QhTERT lines responded to TNF-α by migration (p<0.01), which was inhibited by Infliximab. These results are summarised in the table.
Conclusion: This study confirms the pleiotropic nature of TNF-α. The different responses of the oesophageal cell lines suggest that the role of TNF-α in the MDA sequence might be focused in the stage of early cancer development, especially by promoting migration of some cell clones in the ulcerated mucosa and possibly inducing apoptosis in other competing clones.
EXPRESSION OF HYPOXIA INDUCIBLE FACTOR 1α (HIF-1α) IN THE PROGRESSION TO OESOPHAGEAL ADENOCARCINOMA: A KEY TARGET FOR THERAPY
N. Teratani, A. M. Nicholson, P. Atherfold, A. Milicic, J. J. A. Jankowski. Clinical Pharmacology, University of Oxford, Oxford, UK
Introduction: Hypoxia inducible factor-1α is recognised as a key mediator in the development of several tumours. A recent report has showed increased expression of HIF-1α in oesophageal cancer. Here we investigate the pattern of HIF-1α expression along the esophageal metaplasia to adenocarcinoma sequence using cell lines and resected tissue samples.
Aims & Methods: We studied HIF-1α protein expression by Western blotting in cell lines subjected to hypoxia treatment over a time course. Cell lines used were derived from normal squamous epithelium (EPC), Barrett’s metaplasia (Qh-TERT), high grade dysplasia (Gil-TERT) and oesophageal cancer (adenocarcinoma and squamous cell carcinoma). We also examined the HIF-1α protein expression in normal esophageal mucosa, Barrett’s metaplasia, high grade dysplasia and esophageal adenocarcinoma (resected samples and biopsies) by immunohistochemistry.
Results: The expression of HIF-1α protein in esophageal cancer cell lines was first observed after 2 h of hypoxia treatment and peaked at 4 h or 8 h, depending on the cell line. After 24 h of hypoxic treatment, the level of expression of HIF-1α protein was significantly reduced. Cell lines derived from normal epithelium, Barrett’s metaplasia and high grade dysplasia demonstrated a similar pattern of expression of HIF-1α during hypoxia treatment to the cancer cell lines. In tissue biopsies and resected samples, the expression of HIF-1α protein was higher in adenocarcinoma than normal mucosa and Barrett’s metaplasia. Importantly, Barrett’s metaplasia appears to express higher levels of HIF-1α than the normal oesophagus, contrary to the previous report.
Conclusion: Our results suggest that HIF-1α may play an important role in Barrett’s metaplasia to adenocarcinoma progression and is inducible in response to environmental hypoxia. These findings open up the possibility of developing new therapies for oesophageal adenocarcinogenesis based on suppression of the HIF-1α protein.
INCIDENCE OF EOSINOPHILIC OESOPHAGITIS IN DYSPHAGIA AND FOOD BOLUS OBSTRUCTION
T. Dadge1, K. Mackey1, H. Fellows2, J. Mathew3, L. Jackson2, I. A. Murray2. 1Medical student, Peninsula medical school, Universities of Exeter & Plymouth, 2Gastroenterology, 3Histopathology, Royal Cornwall Hospital, Truro, UK
Introduction: Eosinophilic oesophagitis (EO) is increasingly being recognised as a frequent cause of dysphagia and food bolus obstruction in adults. The annual incidence in the UK is reported as 1 in 10 000 in paediatric and adult populations. EO is a histological diagnosis: marked eosinophilic infiltration (>20 per high power field) in the proximal-mid oesophagus and is associated with normal endoscopic appearances or concentric rings. We proposed that all patients with no identifiable cause for dysphagia or food bolus obstruction should have EO excluded.
Aims & Methods: We requested endoscopists to take two mid- and lower-oesophageal biopsies in all patients with dysphagia without identifiable cause presenting from March 2006 to May 2007. Repeat procedures were excluded. Patient demographics, endoscopic findings and biopsy results were recorded to determine which patients were most likely to have EO and whether we could target a specific patient population.
Results: 430 patients (219 male: 49.3%) had a first endoscopy for dysphagia or food bolus obstruction. 5 (1.2% of the total) patients were diagnosed with EO in this time. 153/430 (35.6%) had no pathology visible at endoscopy to explain their symptoms, of whom 54 were biopsied. Of these 5/153 (3.2% of the total without visible pathology to explain their symptoms) were diagnosed with EO (9.2% of those biopsied). Of those biopsied 25/53 (47.17%) were male and 28/53 (52.83%) were female. All patients diagnosed with EO were male (p = 0.01: χ2). Those diagnosed with EO had a lower mean age (mean age 42.6+4.6 years: range 28–52) then other patients without endoscopically recognisable pathology who were biopsied (mean 65.6+2.2 years: p<0.005, t test). 2 of those with EO described food bolus obstruction one also with intermittent dysphagia. Of those with EO with dysphagia (n = 4) median duration was 15 months, dysphagia was intermittent, not progressive in all and was at pharyngeal or mid-sternal level or both in all. One patient had marked concentric rings at endoscopy, the others being normal or with small hiatus hernia. One had history of atopy (asthma).
Conclusion: EO has an incidence of at least 3.2% and possibly up to 9.2% in patients presenting with dysphagia and/or food bolus obstruction without visible pathology. We suggest that all such patients are biopsied to exclude EO, particularly young and middle aged males with pharyngeal or mid sternal level dysphagia or food bolus obstruction.
OESTRADIOL INHIBITS PROLIFERATION OF BARRETT’S OESOPHAGUS AND OESOPHAGEAL ADENOCARCINOMA CELLS IN VITRO
O. O. Ogunwobi1, I. L. P. Beales2. 1School of Medicine, Health Policy and Practice, University of East Anglia, 2Gastroenterology Department, Norfolk and Norwich University Hospital, Norwich, UK
Introduction: The incidences of Barrett’s oesophagus (BO) and oesophageal adenocarcinoma (OAC) are rapidly increasing. Epidemiological studies suggest that women are less predisposed to OAC than men. The specific biological reasons for this are currently not understood. Women generally have higher oestrogen levels than men. It is currently unknown whether the higher oestrogen levels in women may account for the decreased risk of OAC in them.
Aims & Methods: The aim of this study was to determine whether oestradiol has any effect on BO and OAC cells in vitro. The OE33, OE19, BIC-1, FLO-1 and SEG-1 OAC cells and Go, Gi, C and Q HTERT Barrett’s cells were used as models. Expression of alpha- and beta-oestradiol receptors was assessed using reverse-transcriptase polymerase chain reaction (RT-PCR). The effect of 0.001 nM to 100 nM oestradiol on cell viability was assessed using the 3-[4, 5-dimethylthiazol-2-y-l]-2, 5-diphenyltetrazolium bromide (MTT) assay.
Results: OE33, BIC-1 and SEG-1 OAC cells expressed both alpha- and beta-oestradiol receptors. OE19 and FLO-1 OAC cells expressed only alpha-oestradiol receptors. Go HTERT Barrett’s cells expressed only beta-oestradiol receptors. Oestradiol receptor expression was not detected in the Gi, C and Q HTERT Barrett’s cell lines. Oestradiol inhibited proliferation of OE33 and SEG-1 OAC cells as well as Q HTERT Barrett’s cells in a dose-dependent manner. Maximum effect below untreated control was 12.0±2.8% in OE33 cells, 12.7±3.5% in SEG-1 cells and 9.8±1.5% in Q HTERT Barrett’s cells observed at 100 nM concentration.
Conclusion: Oestradiol inhibits proliferation of BO and OAC cells. This may provide a biological explanation for the decreased risk of OAC observed in women. Further studies are required to confirm this.
ISOTHIOCYANATES INHIBIT PROLIFERATION OF BARRETT’S OESOPHAGUS AND OESOPHAGEAL ADENOCARCINOMA CELLS
O. O. Ogunwobi1, G. Mutungi1, I. L. P. Beales2. 1School of Medicine, Health Policy and Practice, University of East Anglia, 2Gastroenterology Department, Norfolk and Norwich University Hospital, Norwich, UK
Introduction: Oesophageal adenocarcinoma (OAC) is a very devastating disease. The outcome is still dismal in spite of current treatment strategies. Isothiocyanates (ITCs) are dietary constituents that have been suggested to have anti-cancer actions. It is, however, currently unknown whether they may have any effects on Barrett’s oesophagus (BO) and oesophageal adenocarcinoma (OAC) cells and whether they may have a role in chemoprevention of OAC.
Aims & Methods: The aim of this study was to assess the effect of a variety of common ITCs on the proliferation of BO and OAC cells.The OE33 and SEG-1 OAC cells as well as the Q HTERT Barrett’s cells were used as models. The effect of 0.1\muM to 10 mM of allyl isothiocyanate (AITC) from cabbage, benzyl isothiocyanate (BITC) from garden cress and phenethyl isothiocyanate (PEITC) from water cress on cell viability was assessed using the 3-[4, 5-dimethylthiazol-2-y-l]-2, 5-diphenyltetrazolium bromide (MTT) assay.
Results: All concentrations of all ITCs tested significantly inhibited the proliferation and cell viability of all cell lines tested. The overall effects observed were dose-dependent. In OE33 cells: 1 μM of AITC reduced cell viability by 39.5±18.5% as compared to untreated control, 1 μM of BITC reduced cell viability by 69.5±11.5% as compared to untreated control and 1 μM of PEITC reduced cell viability by 62% as compared to untreated control. In SEG-1 cells: 1 μM of AITC reduced cell viability by 72% as compared to untreated control, 1 μM of BITC reduced cell viability by 61% as compared to untreated control and 1 μM of PEITC reduced cell viability by 41% as compared to untreated control. These effects were also apparent in the non-transformed Q HTERT Barrett’s cells: 1 μM of AITC reduced cell viability by 24% as compared to untreated control, 1 μM of BITC reduced cell viability by 37% as compared to untreated control and 1 μM of PEITC reduced cell viability by 21% as compared to untreated control.
Conclusion: ITCs inhibit the proliferation of BO and OAC cells in vitro by reducing cell viability. Consequently, they may be safe chemopreventative agents for use in OAC. Further studies are warranted to confirm this potentially beneficial effect and elucidate the underlying mechanisms.
EGFR AND ERBB2 PHOSPHORYLATION STATUS: IMPLICATIONS FOR ERBB TARGETED THERAPIES
A. L. Paterson1, H. Z. Shi2, L. Liu2, T. M. Gilmer3, R. F. Wooster2, R. C. Fitzgerald1. 1MRC Cancer Cell Unit, Hutchison MRC Research Centre, Cambridge, UK, 2Translational Medicine, Glaxosmithkline, Philadelphia, 3Translational Medicine, Glaxosmithkline, North Carolina, USA
Introduction: The incidence of oesophageal adenocarcinoma (AC) has increased fourfold in the last 30 years and the 5-year survival is 15%. Preliminary studies show ErbB2 over-expression in 15–20% AC making it a potentially valuable therapeutic target. ErbB2 targeted therapy (trastuzumab) has revolutionised breast cancer treatment, however only a subset of patients with ErbB2 over-expression respond. The next generation of agents target multiple ErbB family members. More insight into factors predictive of response is required.
Aims & Methods: (1) To use AC as a model to characterise factors affecting the function of and interactions between ErbB family members. (2) Determine the implications of ErbB interactions on sensitivity to EGFR and ErbB2 tyrosine kinase inhibition. (3) Determine the potential role of the next generation of ErbB inhibitors in the treatment of AC. The EGFR and ErbB2 status was comprehensively characterised (copy number, mRNA expression, protein expression and receptor activation) in a total of ten oesophageal carcinoma and high grade dysplasia cell lines. Sensitivity to the dual EGFR and ErbB2 inhibitor lapatinib (Tykerb, GlaxoSmithKline) was determined in cell lines shown to have ErbB2 or EGFR amplification.
Results: In the AC cell lines OE-19 and OE-33, ErbB2 genomic amplification resulted in protein over-expression, constitutive phosphorylation of both EGFR and ErbB2 and the continuous presence of EGFR-ErbB2 heterodimers. These features were exclusive to ErbB2 amplified lines (2/5 adenocarcinoma lines studied). In OE-19, lapatinib suppressed EGFR and ErbB2 continuous activity, resulting in reduced proliferation (IC50 0.046 μM; 95% CI 0.035 to 0.059 μM), and increased apoptosis measured by caspases 3 and 7 activation and cell death ELISA. EGFR genomic amplification, observed in the squamous carcinoma line OE-21, correlated with protein over-expression but not constitutive phosphorylation of EGFR or ErbB2; these cells were moderately sensitive to lapatinib which inhibited proliferation (IC50 0.43 μM; 95% CI 0.31 to 0.6 μM) and activated caspases 3 and 7 within 24 h. Lapatinib induced cytostatic and cytotoxic effects in both OE-19 and OE-21 lines at drug concentrations below 3 μM, a clinically attainable plasma concentration. However, lapatinib failed to suppress constitutive ErbB2 and EGFR phosphorylation in OE-33 and this was associated with drug resistance (IC50 7.3 μM; 95% CI 3.4 to 15.5 μM).
Conclusion: Lapatinib exhibits cytostatic and cytotoxic effects in cell lines with EGFR or ErbB2 over-expression. In ErbB2 amplified lines, suppression of EGFR and ErbB2 constitutive phosphorylation was predictive of sensitivity.
ALGINATES INHIBIT THE EFFECTS OF IRON IN AN IN VITRO MODEL OF OESOPHAGEAL ADENOCARCINOMA
K. Roberts1, R. Spychal2, M. Brookes1, V. Strugala3, P. W. Dettmar3, L. M. Johnstone4, I. G. Jolliffe4, C. Tselepis1. 1Cancer studies, CRUK, 2Surgery, City Hospital, Birmingham, 3Technostic Ltd, The Deep Business Centre, 4R and D, Reckitt Benckiser Healthcare, Hull, UK
Introduction: There is an emerging body of evidence that iron is important in oesophageal carcinogenesis. In particular, we have recently shown that the proteins implicated in cellular iron import are over-expressed in oesophageal adenocarcinoma.1 This culminates in elevated intracellular iron which mediates cellular proliferation. The aim of this study was to determine if alginate, which can be defined as a dietary fibre and is an active ingredient in the over-the-counter medicine Gaviscon Advance, could inhibit these iron mediated effects in an oesophageal model.
Aims & Methods: Oesophageal adenocarcinoma derived cell lines OE33 and SEG-1 were exposed to iron (100 μM) in the presence or absence of Gaviscon Advance (0.1%) or alginate (1 mg/ml). Following exposure cellular proliferation, migration and anchorage independent growth were determined using standard assays.
Results: As previously demonstrated exposing cell lines OE33 and SEG-1 with iron resulted in a significant increase in proliferation (1.54-fold and 3.26-fold respectively). This effect was partially inhibited by co-culture with alginate (21% and 20% reduction respectively; p<0.05) and completely inhibited by co-culture with Gaviscon Advance (73% and 75% reduction respectively; p<0.001). Cell migration was significantly elevated in both lines following culture with iron. However, co-culture with either the alginate or Gaviscon Advance resulted in a significant (p<0.001) repression in migration. Similarly iron mediated anchorage independent growth could be suppressed with the use of Gaviscon Advance.
Conclusion: Alginate and Gaviscon Advance can inhibit both iron mediated cellular proliferation, migration and transformation. This may provide a platform of therapeutic intervention in the treatment and prevention of oesophageal adenocarcinoma development.
A POTENTIAL ROLE FOR PERIOSTIN IN BARRETT’S CARCINOGENESIS
A. Saadi1, M. Das1, N. Clemons1, C. Zhang2, G. Tokiwa3, K. Serikawa3, M. Ferguson4, J. S. Hardwick5, H. Dai2, R. C. Fitzgerald1. 1MRC Cancer Cell Unit, Hutchison MRC Research Centre, Cambridge, UK, 2Custom analysis, 3Gene expression, Rosetta Inpharmatics, Seattle, WC, 4Management, 5Molecular profiling, Merck Laboratories, West point, PA, USA
Introduction: Periostin is a secreted extracellular matrix protein which is important in embryonic development and wound repair, with a potential role in cancer progression. Periostin mRNA over-expression was recently reported in Barrett’s and oesophageal adenocarcinoma (OAC) tissues.1
Aims & Methods: (1) Use gene expression data to determine whether periostin is over-expressed during Barrett’s carcinogenesis. (2) Validate array data in independent samples. (3) Investigate the capacity of periostin to promote invasion in vitro. Genome-wide RNA expression was determined in human samples using Agilent microarrays (normal squamous-oesophagus (NE) n = 6; intestinal metaplasia (IM) n = 21; low-grade-dysplasia (LGD) n = 17; high-grade-dysplasia (HGD) n = 13; OAC n = 8). Immunohistochemistry for periostin was performed on an independent dataset (n = 21). Oesophageal stromal fibroblasts were isolated from normal (NAFs), Barrett’s (BAFs), and cancer-associated tissues (CAFs). Periostin expression was determined by Western blotting and QPCR in primary fibroblasts, OAC (SEG, FLO, OE33, BIC) and dysplastic epithelial cell lines (GohTert, ChTert, GihTert). Effects of recombinant periostin (100–400 ng/ml) and addition of fibroblasts on FLO invasiveness and motility were investigated using matrigel and wound healing assays.
Results: Periostin was significantly over-expressed in OAC compared to each of: NE (4.36-fold, p = 0.0035), IM (2.76-fold, p = 0.0275), LGD (3.61-fold, p = 0.0027) and HGD (14-fold, p = 8.83×10−8). IHC showed that Periostin protein expression was restricted to the stroma of BE and cancer tissues. Primary fibroblasts and epithelial cell lines were used to characterise the cell specific expression of periostin. Apart from SEG cells, dysplastic and OAC epithelial lines expressed lower levels of periostin mRNA compared to fibroblasts derived from patients with dysplasia or cancer (twofold, p<10-4). Recombinant Periostin (100 ng/ml) promoted invasion of FLO cells in vitro (1.7-fold, p = 0.0092), but had no significant effect on cell motility. 2/3 CAFs increased invasiveness of co-cultured FLO cells compared to corresponding NAFs (p = NS), but this was not directly attributable to periostin.
Conclusion: Overexpression of periostin in fibroblasts and in cancer tissue stroma, combined with periostin-induced promotion of invasion in vitro, suggests a role for fibroblast-derived periostin in cancer. The isolation of stage-specific fibroblasts offers a valuable tool for further functional studies of stromal-epithelial interactions in Barrett’s carcinogenesis.
OUTCOMES AFTER OESOPHAGECTOMY FOR PT1 ADENOCARCINOMA
A. K. Saha, C. Sutton, H. M. Sue-Ling, S. P. L. Dexter, A. I. Sarela. Academic Division of Surgery, The General Infirmary at Leeds, Leeds, UK
Introduction: We examined the prevalence of lymph node metastasis and patterns of disease recurrence for patients with pT1 oesophageal adenocarcinoma.
Aims & Methods: From January 2000 to December 2006, 44 patients had pT1 oesophageal adenocarcinoma with pre-operative staging (spiral, CT scanning of the neck, thorax and abdomen and endoscopic ultrasound (EUS)) of HGD or T1/T2 and N0. No patients had neo-adjuvant treatment. 24 patients had an Ivor Lewis operation, 4 had an open transhiatal and 16 had a laparoscopic transhiatal operation.
Results: There were 37 men. Median age was 64 years (range 35–80). 36 patients (82%) were on Barrett’s surveillance. Median lymph node yield was 19 (3–51). There was no R1 resection. Four patients (9%) had poorly-differentiated tumours. Two patients had N1 disease; one patient had 1 metastatic node (no adjuvant treatment) and one patient had 3 metastatic nodes (adjuvant chemotherapy). Estimated survival (Kaplan-Meier) at 1 year and 3 years was 94% and 88%, respectively. Alive patients had median follow-up of 36 months (5–87). Two patients (8%) with N0 disease and 1 patient with N1 disease developed recurrence. The second patient with N1 disease is alive and well at 14 months. Three of the 4 patients with poorly-differentiated disease developed recurrence; the 1 remaining patient is disease-free at 16 months. All patients with recurrence received systemic 5FU and cisplatin.
Conclusion: pT1 oesophageal adenocarcinoma was associated with 5% prevalence of N1 disease. 7% of patients died of recurrent disease within 2 years. 8% of patients with N0 disease developed recurrence. Poorly-differentiated pT1 disease appeared to be at high risk for recurrence.
TYLOSIS WITH OESOPHAGEAL CANCER: CHARACTERISING THE ENDOSCOPIC APPEARANCE WITH MAGNIFICATION AND NARROW-BAND IMAGING
H. L. Smart, S. Subramanian, S. Khalid, A. Ellis. Gastroenterology, Royal Liverpool University Hospital, Liverpool, UK
Introduction: Tylosis (focal non-epidermolytic palmoplantar keratoderma) is an autosomal dominant skin disorder strongly associated with squamous cell oesophageal cancer (Tylosis with oesophageal cancer, TOC). In this condition the estimated risk of developing oesophageal cancer by the age of 65 years exceeds 90%. There are no reports of the endoscopic findings in Tylosis. This abstract presents a single operator experience of using endoscopy with magnification and narrow-band imaging to characterise the oesophageal appearances in Tylosis.
Aims & Methods: Patients with Tylosis attending the Royal Liverpool University Hospital for surveillance endoscopy were studied. Endoscopy was undertaken by a single experienced operator (HLS) under conscious sedation. An Olympus XGIF-240FZ endoscope with an Olympus Evis Lucera processor (XCV 260HP) and light source (XCLV 260HP) was used to perform each procedure. White light (WLI) and narrow-band imaging (NBI) were undertaken, magnification being performed as necessary. Video and hard copies were obtained. Multiple mucosal biopsies were taken for histological assessment at 3 levels and from focal lesions.
Results: 18 consecutive patients (mean age 48, range 23–71 years, 9 men) were examined between December 2006 and September 2007. WLI revealed mild, patchy hyperkeratosis in 10 patients, more confluent hyperkeratotic plaques and fissuring in 6 (moderate change), with 2 patients having focal abnormalities (mild stricture formation 1, focal erythematous patch 1), classified as severe change. 6 patients had associated endoscopic findings including hiatal hernia 3, reflux oesophagitis 3, Barrett’s oesophagus 2 and inlet patch 1. NBI enhanced the mucosal changes in all subjects but was not necessary for detecting those with severe change. Adding magnification (up to 115×) to NBI revealed changes to the normal appearance of intrapapillary capillary loops (IPCLs). Hyperkeratotic plaques frequently obscured these structures; in some patients changes of IPCLs dilatation were observed. In the 2 patients with severe change marked disruption of the normal IPCLs pattern was seen, both patients had dysplasia on targeted biopsy, which was not present in those with either mild or moderate change.
Conclusion: This report is the first to characterise the endoscopic appearance in Tylosis. WLI can define changes to the oesophageal mucosa of variable hyperkeratosis (mild to moderate change) and identify focal, more significant abnormalities (severe change), as seen in 2 of 18 cases. Associated findings are frequent. NBI enhances visualisation of the mucosal changes in Tylosis but is not necessary to define severe disease. When used with magnification, NBI can demonstrate changes to the IPCLs and reveal altered vascularity compatible with dysplasia, prompting detailed further assessment and consideration of surgery.
PREDICTING PROGRESSION OF INDEFINITE FOR DYSPLASIA IN BARRETT’S OESOPHAGUS WITH AMACR (ALPHA-METHYLACYL-COA-RACEMASE) IMMUNOSTAINING
S. A. Sonwalkar1, O. Rotimi2, N. Scott3, E. Thomas2, M. Dixon2, A. Axon1, S. Everett1. 1Gastroenterology, 2Pathology, The General Infirmary at Leeds, 3Pathology, St James University Hospital, Leeds, UK
Introduction: Biomarkers have the potential for earlier identification of those patients at risk for progression to cancer. AMACR has shown increased sensitivity and specificity for its expression in foci of dysplasia in BO.
Aims & Methods: To evaluate the expression of AMACR as a predictive marker for identification of progression in patients with BO with a special emphasis on Indefinite for dysplasia (IND). 41 cases of IND and 15 controls, each with a diagnosis of BO, low grade dysplasia (LGD), high grade dysplasia (HGD) and oesophageal adenocarcinoma (OA) were identified over a 21-year period and slides retrieved. Three GI histopathologists reassessed the slides independently based on the revised Vienna classification. Data were collected for outcome (progression). After immunohistochemical staining with AMACR by monoclonal antibody the slides were evaluated in a blinded fashion for the presence, extent and location of AMACR expression by two pathologists according to the following protocol: 0<1% cells positive; 1+, 1% to 10% cells positive; 2+, 10% to 50% cells positive; or 3+, >50% cells positive.
Results: 21/41 cases (50%) were reclassified as IND by at-least one of the three histopathologists. 41 cases were followed up for a median of 38.7 months (range 6–122 months). 31 cases (73%) did not progress to more severe grades of dysplasia but 10 (27%) did. AMACR staining was carried out in slides from 87/101 patients. Overall, the IND, LGD, HGD and OA foci were positive for AMACR in 9/37 (27%), 2/11 (18%), 6/10 (60%) and 10/15 (67%) cases respectively. All the BO cases were negative. Extent of AMACR staining increased significantly in the HGD and the OA group with 20% and 32% foci showing 2+ and 3+ staining as compared to 0% and 4% in the BO and IND group (95% CI 0.111 to 0.460, p = 0.0006) respectively (table). The sensitivity of AMACR for the detection of dysplasia was 27% for IND, 18% for LGD, 60% for HGD and 67% for OA. The specificity was 100% in all. Of the 10 patients with an initial diagnosis of IND that progressed (including the 2 with coexistent dysplasia and 2 with progressive dysplasia within 3 months), 6 were positive for AMACR staining and of the 31 IND cases that did not progress, 4 were positive. Of these 4, 1 regressed to BO while 3 stayed IND at last surveillance.
Conclusion: AMACR shows promise as a marker to indicate those patients in need of more intensive surveillance. Prospective, multicentre studies with larger case numbers are required to help identify high-risk cases that might progress.
AN ALGINATE RAFT FORMING SUSPENSION IS ABLE TO INHIBIT PEPSIN ACTIVITY
V. Strugala1, J. Avis1, L. M. Johnstone2, I. G. Jolliffe3, P. W. Dettmar1. 1Technostics, Technostics Ltd, 2Professional Relations, 3Research and Development, Reckitt Benckiser Healthcare (UK) Ltd, Hull, UK
Introduction: Pepsin is the major damaging component of the gastro-oesophageal refluxate. Animal models have shown that pepsin causes erosive damage to the oesophagus when acid alone does not.1 Gaviscon Advance (GA) is an alginate-containing raft forming suspension that acts as a barrier to reflux by forming an aerated buoyant gel upon contact with stomach acid. Alginate has been shown to inhibit pepsin activity2 and here we evaluate if GA, in which alginate is the active, can do the same.
Aims & Methods: Pepsin activity was measured using two distinct in vitro assays against different substrates. The Azocoll assay3 measured digestion of an insoluble dye-labelled collagen substrate at pH2 in which the azo-dye was released and solubilised on cleavage. The N-terminal assay2 4measured the digestion of a protein substrate (succinyl albumin) at pH2.2 by trinitrophenylation of newly formed amino groups after cleavage of peptide bonds. GA comprises 1000 mg alginate in a 10 ml dose (100 mg/ml) and the effect of dilutions of GA were assessed (1 mg/ml–20 mg/ml alginate). In all cases the change in pH (due to acid neutralisation by excipients) was strictly controlled for. A positive control (pepstatin) was used in all experiments and complete pepsin inhibition was consistently observed. Mean percentage inhibition of pepsin activity of each GA dilution was calculated (n = 10 Azocoll, n = 18 N-terminal).
Results: Using the Azocoll assay complete inhibition of pepsin was observed and there was a clear dose response curve seen until no inhibition was seen at 3.3 mg/ml and below. Using the N-terminal assay the maximal percent inhibition of pepsin was 78% (10 mg/ml alginate) since no higher concentration of GA could be evaluated in this assay. There was a dose dependant decrease in pepsin inhibition but even at 1 mg/ml inhibition was observed.
Conclusion: Using two established in vitro assay methods GA was shown to substantially inhibit pepsin activity at acidic pH. Complete pepsin inhibition was clearly observed and dose dependency seen with some enzyme inhibition even when GA was highly diluted. These data demonstrate that the alginate-containing raft forming suspension (GA) has a novel mode of action for the treatment of gastro-oesophageal reflux disease by inhibiting potentially one of the most damaging components of the refluxate.
RETENTION OF THE BILE ACIDS IN THE GASTRIC REFLUXATE BY AN ALGINATE RAFT FORMING PRODUCT
V. Strugala1, J. Avis1, L. M. Johnstone2, I. G. Jolliffe3, P. W. Dettmar1. 1Technostics, Technostics Ltd, 2Professional Relations, 3Research and Development, Reckitt Benckiser Healthcare (UK) Ltd, Hull, UK Kingdom
Introduction: The gastric refluxate contains a range of bile acids (BA)1 and they have been implicated in the aetiology of gastro-oesophageal reflux disease (GORD) and in the development of Barrett’s oesophagus and oesophageal adenocarcinoma.2 BAs at pH4 were shown to induce the oncogene c-myc in oesophageal cell lines3 and alginate was able to abrogate this detrimental effect.4 Gaviscon Advance (GA) is an alginate-containing reflux treatment that works by forming a buoyant alginate raft on top of the gastric contents to prevent refluxate entering into the oesophagus. We postulate that GA may have a role to play in the protection of the oesophagus from BAs and here we investigate if GA can prevent BAs in the refluxate entering the oesophagus.
Aims & Methods: A GA raft was formed by adding a 10 ml dose (containing 1000 mg alginate) to 0.1 M HCl at 37°C. An in vitro reflux model was established and a simulated gastric refluxate (SGR) was forced through the GA raft. The SGR contained 1 mM of BA (taurocholic acid (TCA); deoxycholic acid (DCA); glycocholic acid (GCA); cholic acid (CA)) in HCl of a specified pH. BA remaining in the SGR was assessed by UV spectrometry (203 nM) and quantified using a standard curve after controlling for background released from the GA raft. Mean (SD) %BA retained by the GA raft of n = 6 was calculated (>100% is due to calculation only).
Results: The ability of a GA raft to retain BAs from a 5 ml SGR was evaluated. Essentially all the BA was removed by the GA raft (table). BA retention by the GA raft was related to the volume of the SGR with only 40% retained when 50 ml SGR was applied. The ability of a GA raft to retain BAs from multiple reflux events was investigated by evaluating 10×5 ml SGRs. Essentially all BA was retained from the first SGR (93 (3)%)but with each successive SGR there was a small drop in the capacity to retain BA with 67 (3)% after 5 SGRs but even after 10 SGRs 51 (5)% of BA was still removed from the SGR.
Conclusion: The in vitro study clearly showed that a GA raft was capable of removing BAs from a SGR of a volume that was realistically representative of GORD (5 ml). This was the case no matter which BA was used or the pH of the refluxate. A GA raft has considerable capacity to accommodate BAs from multiple reflux events as would occur in the clinical situation. GA has a role to play in the protection of the oesophagus from damage caused by BAs in patients with GORD.
ANDROGEN RECEPTOR EXPRESSION IN THE STROMA OF OESOPHAGEAL CARCINOMA
N. Waraich1, P. Clarke2, A. Meckenzie2, A. Grabowska2, S. Iftikhar1, S. Watson2. 1General Surgery, Derby Hospitals NHS foundation Trust, Derby, 2Pre Clinical Oncology, University of Nottingham, Nottingham, UK
Introduction: The role of androgens and stroma-epithelial cell interactions is well-established in prostate cancer. This study examined the expression of Androgen Receptors in oesophageal adenocarcinoma (EAC), in which tumour incidence in males is also higher.
Aims & Methods: Fibroblasts were isolated from human oesophageal carcinoma (n = 7) and mouse oesophageal cancer n = 1 (SW 19). LnCap, 46BriGs and 3T3 cell-lines were used as controls. Immunofluorescence, florescence activated cell study (FACS) and PCR were performed for Androgen Receptor (AR) expression in cancer-associated fibroblasts.
Results: AR protein expression by immunoflorescence was significantly higher among human fibroblasts cells (p<0.0001) treated with androgens as compared to LnCap and 46BriGs cells. Similarly AR expression by immunoflorescence was also significantly higher among mouse fibroblasts cells (SW19 cells p<0.0001) treated with androgens as compared to mouse 3T3 cells. Gene expression was also noted to be significantly higher (p<0.001) among the tumour-derived primary human fibroblast as compared to controls (LnCap Cells and 46Brigs). Gene expression in tumour-derived mouse fibroblast was significantly higher (p<0.001) as compared to established mouse 3T3 cell line. FACS studies on all the fibroblasts has confirmed the IF results.
Conclusion: Our results confirm the expression of androgen receptors among the stroma of oesophageal carcinoma. This highlights the concept of androgen-induced effects in oesophageal cancer.
Radiology posters
COLONIC THICKENING ON ABDOMINAL COMPUTERISED TOMOGRAPHY, HOW OFTEN ARE THE RADIOLOGISTS RIGHT?
G. C. Parkes1, S. Natas2, D. Borrow3, J. D. Sanderson1. 1Gastroenterology, 2Radiology, 3Endoscopy, Guy’s and St Thomas’ Foundation Trust, London, UK
Introduction: The increasing use of abdominal computerized tomography (CT) has meant a corresponding rise in finding incidental colonic wall thickening (CWT). This in turn has led to a rise in referrals for lower gastrointestinal endoscopy (LGIE). Few studies have attempted to assess the significance of radiological CWT.
Aims & Methods: To assess the diagnostic yield of incidental CWT found on CT and to ascertain whether there are specific clinical and radiological factors which correlate with a positive yield. We performed a retrospective study of endoscopy requests in a large London teaching hospital over one year. Reports in which colonic thickening, as defined by abdominal or pelvic CT, was mentioned, were included. Patients were aged 18 and above. Patients had to have had an endoscopic examination of the colon that included the region of the bowel showing thickening on CT. Patients were excluded if: the thickening was focal as to suggest a mass, there was a clear radiological diagnosis of diverticular disease or were known to already have, colorectal cancer or inflammatory bowel disease. A positive yield was defined as either a endoscopic or histological diagnosis of inflammation or neoplasia. Incidental polyps were not included as a positive finding.
Results: In a one-year period approx 3400 abdominal CTs were performed in the hospital. We identified 38 patients who had subsequent LGIE because of CWT on CT. Of these 18 (47%) had positive findings as detailed in the table. We correlated the reason for referral with the incidence of positive findings either on initial LGIE or if later performed surgery. In patients who had additional change in bowel habit or PR blood loss, at the time of LGIE, the yield was significantly greater 58% vs 14% (p<0.03) than in those with either abdominal pain or no GI symptoms. In those who had pain only as the reason for the CT referral, 0/5 had positive findings on LGIE. There was no correlation between maximal colonic thickness radiologically and positive findings (p<0.3). Neither age or sex predicted positive yield on LGIE endoscopy.
Conclusion: Incidental colonic wall thickening represents significant pathology in 47% of our series of which 15% were cancers. Change in bowel habit or per rectum blood loss were strong predictors of significant findings, however in patients with CWT and abdominal pain only there was no significant pathology. There was no correlation between the diameter of the colonic wall and positive findings although it could be that our numbers were too small.
EVALUATION OF “PREPLESS” CT COLONOGRAPHY FOR INVESTIGATION OF IRON DEFICIENCY ANAEMIA IN PATIENTS OVER THE AGE OF 60
P. Sakellariou1, K. Kapur1, P. McAndrew2, A. Soliman1, S. A. Riley3, M. Karajeh1. 1Gastroenterology, 2Radiology, Barnsley Hospital NHS Foundation Trust, Barnsley, 3Gastroenterology, Northern General Hospital, Sheffield, UK
Introduction: Iron deficiency anaemia (IDA) is a common presentation in elderly patients for which total colonic examination is indicated, either a colonoscopy or a double contrast barium enema. However, both require full bowel preparation which can be a daunting aspect for the elderly or frail patient. “Prepless” CT colonography (CTC) using oral contrast for faecal tagging, has been shown to be feasible with encouraging initial results. The role of CTC for the investigation of IDA has not been evaluated previously.
Aims & Methods: To compare “prepless” CTC to conventional colonoscopy (CC) for the investigation of IDA in patients above the age of 60 years. We carried out a prospective, evaluator blinded, study of patients with IDA seen in the gastroenterology clinic. Informed consent was obtained from all patients participating in the study. Faecal tagging was achieved using dilute barium sulphate (2.1% barium sulphate weight/volume) ingested with the main meals starting 36 hours before CTC, but no bowel cleansing agents were given. CTC was performed using a Philips 4 detector row MX-8000 scanner, with slice collimation of 2 mm, using the prone and supine acquisitions. Images were analysed on a dedicated workstation (EZEM Innerview) using 2D images cross-referenced to the 3D fly-through by a single radiologist. All patients underwent CC within 3 weeks of CTC by experienced endoscopists who were blinded to the results of the CTC. Prior to the CC patients received standard bowel preparation (4 sachets of Kleanprep). The extent of colonic examination, pathological findings (tumours, polyps over 9 mm, diverticular disease) on CTC and CC and extraluminal findings for CTC were recorded. Analysis according to polyps and cancer was performed and the sensitivity of CTC for their detection was calculated using CC as the gold standard.
Results: Forty six patients completed the study (median age 74 years, 28 males). The median Hb was 9.9 g/dl (6–11.9). The colonoscopic examinations were completed to: the terminal ileum or the caecum in 40 patients (87%), ascending in 4 (9%) and transverse in 2 (4%) only due to looping (3 cases), an obstructing tumour (2 cases) and severe diverticular disease (1 case). CTC was non-diagnostic in one patient due to faecal residue. There were 9 colonic cancers and 10 polyps >9 mm detected on CC. CTC detected 8/9 (89%) cancers and 3/10 (30%) polyps.
Conclusion: Our study suggests that “prepless” CTC can be used as a tool in elderly and frail patients with IDA to exclude tumours but has low sensitivity for polyp detection.
NOVEL IMAGE ANALYSIS METHODS FOR THE NON-INVASIVE DIAGNOSIS OF INTRA-ABDOMINAL ADHESIONS
B. P. Wright1, J. W. Fenner1, R. Gillott2, P. V. Lawford1, P. Spencer2, K. D. Bardhan3. 1Academic Unit of Medical Physics, The University of Sheffield, Sheffield, 2Clinical Radiology, 3Gastroenterolgy, Rotherham General Hospital, Rotherham, UK
Introduction: Abdominal pain due to suspected adhesions remains a common reason for hospital admission and investigation, and diagnosis is difficult without laparoscopy or laparotomy. Magnetic resonance imaging (MRI) studies in healthy volunteers have shown smooth movement of the intra-abdominal contents over each breathing cycle. In contrast, patients with Crohn’s disease who had previously undergone gut resection and were known to have adhesions showed subtle disruptions to the pattern of movement. It is hypothesised that adhesions may be detectable by their disrupting influence. This approach does not identify adhesions as a structure but instead infers their presence from distortions in movement.
Aims & Methods: Standard dynamic non-contrast MR images were obtained from volunteers and from patients with Crohn’s disease (described as above). Novel image processing and registration methods enabled semi-automated analysis, highlighting disturbances to smooth movement. Vector fields denoting image movement were computed, from which maps of movement were constructed. Movement maps were then displayed and interpreted using mathematical operators.
Results: Sagittal MRI sections (fig A) were examined from volunteers and patients. Application of the registration algorithms illustrates vector and contour plots (fig B) that represent organ movement.

Conclusion: (1) Encouragingly the pilot data captures and quantifies the complexity of abdominal movement. (2) Sophisticated mathematical vector operators seem better than traditional image inspection for identifying areas of potential abnormality. These observations are also borne out with in vitro models. (3) This study demonstrates the feasibility of imaging augmented by mathematical analysis as a means of characterising abdominal movement and offering non-invasive detection of adhesions.
Colorectal/anorectal posters
THE ROBOTS 1 STUDY: A RANDOMISED CONTROLLED TRIAL OF TREATMENT FOR NEW ONSET FAECAL INCONTINENCE AFTER PELVIC RADIOTHERAPY
J. Andreyev1, C. Hackett1, A. Lalji1, A. R. Norman2. 1Medicine, 2Computing, Royal Marsden Hospital, London, UK
Introduction: Approximately 2500 patients develop chronic faecal incontinence after pelvic radiotherapy for prostate, gynaecological, bladder, rectal or anal cancer per year in the UK. It is rare for patients to be referred for specialist help. There are no previous prospective studies of any non-surgical treatment for faecal incontinence developing after radiotherapy.
Aims & Methods: Patients were eligible for inclusion in this randomised controlled trial if they completed pelvic radiotherapy at least 3 months ago, had not previously had faecal incontinence and were now faecally incontinence more than once a month. Patients were randomised to toileting exercises or toileting exercises+sterculia. Patients in the toileting arm could be crossed over to sterculia after 32 weeks. Other medication was prescribed for uncontrolled symptoms if required at subsequent follow-up visits. The primary end point was change in the Vaizey incontinence score at 6 weeks (0 = perfect continence, 24 = appalling). Secondary end points included quality of life and bowel function at 6 and 12 months assessed using a modified Inflammatory Bowel Disease Questionnaire (IBDQ) (224 = perfect, 32 = appalling). Anorectal physiological assessments and endoanal ultrasound were performed at baseline, 32 and 52 weeks in the first 20 patients randomised.
Results: 24 female patients (15 cervix, 4 endometrium, 3 vagina, 2 bladder) median age 52 (range 30–76) and 18 male (15 prostate, 2 anal, 1 testicular) median age 66 (44–82) were randomised a median of 1.5 years (0.4–32.3) after the end of radiotherapy. The mean baseline Vaizey score for women was 16.7 and men 13.8 (p = 0.038). Maximal benefit (defined as improvement in Vaizey score) was seen at or after 32 weeks (women mean 2 point improvement from baseline, men 5.8). Improvement in quality of life and overall bowel function (IBDQ) improved in women (baseline mean 128, best 154) but to a greater degree in men (baseline 162, best 205). Improvements in continence were sustained during follow-up. The trial was underpowered to determine whether the addition of sterculia to toileting exercises conveyed additional benefits, though a consistent non-significant improvement in the sterculia arm was seen in some physiological parameters.
Conclusion: This is the first prospective intervention of any non-surgical treatment for faecal incontinence developing after radiotherapy. It demonstrated that simple interventions can lead to significant sustained benefit in men and modest benefits in women. These data will help power future studies which probably should be further stratified according to the amount of bowel which is included in the radiation field.
A PILOT STUDY OF GENE SPECIFIC METHYLATION IN DIVERTICULAR DISEASE: A NOVEL FINDING
R. P. Arasaradnam1, D. M. Commane1, J. Mathers1, M. Bradburn2. 1Human Nutrition Research Centre, School of Clinical Medical Sciences, Newcastle University, 2Department of Surgery, Northumbria Healthcare NHS Trust, Newcastle, UK
Introduction: We have previously shown evidence of global DNA hypomethylation in patients with diverticular disease (DD) possibly as a consequence of low grade mucosal inflammation.1 DD is an age related colonic disease with recent renewed debate as to possible common molecular disruptions in both DD and colorectal cancer to the collagen matrix micro-environment (CRC).2 Epigenetic modifications such as gene specific methylation occur early in the multi-step pathway of colorectal carcinogenesis. We hypothesise that certain genes such as ESR-1 and N-33 (both putative tumour suppressor genes and methylated with ageing and CRC3) are also hypermethylated in DD subjects. There are no studies to date on gene specific methylation in DD.
Aims & Methods: To assess gene specific methylation of ESR-1 (oestrogen receptor -1) and N-33 (tumour suppressor candidate-3) in macroscopically non-inflamed DD subjects. 28 patients were recruited (10 DD and 18 age- and sex-matched controls). Colorectal mucosal biopsies were obtained and DNA extracted. Gene specific methylation was quantified using the COBRA method described by Xiong et al.4
Results: Percentage methylation of both ESR-1 and N-33 were significantly (p = 0.003 and p = 0.01 respectively) higher in DD subjects compared with age- and sex-matched controls.
Conclusion: In this pilot study, we have shown novel findings of hypermethylation of both ESR-1 and N-33 (putative age related tumour suppressor genes) in DD subjects. On going work is being undertaken to determine if lifestyle factors such as smoking and diet influence gene specific methylation.
This study is funded by the Food Standards Agency (N12015)
DUSP1/MKP-1, DUSP2/HPAC1 AND DUSP8/VH5 EXPRESSION IN COLORECTAL CANCER
A. Conlin1, R. J. C. Steele2, C. R. Wolf1. 1Biomedical Research Centre, 2Surgery and Molecular Oncology, Ninewells Hospital, Dundee, UK
Introduction: The mitogen-activated protein kinase (MAPK) signalling pathway is negatively regulated by the dual-specificity mitogen-activated protein kinase phosphatases (DUSPs). Malignant transformation has long been associated with activation of MAPK pathways and blockade of these pathways have been shown to suppress tumour growth.1 2 DUSP expression has been shown to be differentially regulated in cancer and we have now examined mRNA expression of DUSP1/MKP-1, DUSP2/hPAC1 and DUSP8/VH5 in colorectal cancer.3
Aims & Methods: Colorectal carcinomas and matched normal colorectal tissue from 95 patients were used in this study. TaqMan technology was used for real time PCR mRNA quantitation and data analysed using the ABI Prism sequence detection system. The comparative CT method was used to generate fold differences in gene expression between tumour and matched normal controls. Fisher’s exact test and Wilcoxon signed rank test were used to analyse the data.
Results: 84% of 90 tumours demonstrated down-regulation of DUSP1/MKP-1. In total 61% of these tumours showed ⩾2-fold down-regulation compared to matched normal tissue. This difference was considered extremely significant (p<0.0001). DUSP2/PAC1 was over-expressed in 73% of a cohort of 70 colorectal cancers compared to matched normal tissue. Twofold or greater over-expression was seen in 60% of the panel. This differential expression was statistically significant (p<0.0001). DUSP8/VH5 was down-regulated in a total of 64% of 95 tumours with ⩾twofold under-expression in 35% of cases. The difference between tumour and normal expression was not quite statistically significant (p = 0.0506).
Conclusion: While the exact mechanism of DUSP1/MKP-1 differential regulation remains unclear it seems that DUSP1/MKP-1 may have an inhibitory effect on cellular motility and growth and that loss may promote tumorigenesis. DUSP2/PAC1 was shown to be over-expressed and may function as an oncogene. It could be a potential marker for disease recurrence or progression or may even serve as a target for colon cancer therapy. Further research in this field is essential and should involve the development of reliable methods for the detection of MAP kinase and DUSP proteins in colorectal cancer tissue. Specifically, determining the expression pattern of stress-activated protein kinases may help explain the mechanisms of differential expression of DUSP1/MKP-1 and DUSP2/PAC1 in colon cancer.
DUSP6/MKP-3 EXPRESSION AND K-RAS MUTATION IN COLORECTAL CANCER
A. Conlin1, G. Smith1, R. J. C. Steele2, C. R. Wolf1. 1Biomedical Research Centre, 2Surgery and Molecular Oncology, Ninewells Hospital, Dundee, UK
Introduction: We have previously found that mutations in K-ras infer poor prognosis in colorectal cancer.1 K-ras is involved in activation of the mitogen-activated protein kinase pathway through ERK1 and ERK2. Recent studies have suggested a link between mutated Ras in cancer and differential expression of DUSP6/MKP-3, a downstream regulator of ERK1 and ERK2.2 We have investigated this possible link in colorectal cancer in an attempt to further understand the prognostic effect of mutated K-ras.
Aims & Methods: Colorectal carcinomas and matched normal colorectal tissue from 104 patients were used in this study. K-ras mutation detection was carried out using PCR and direct bi-directional DNA sequencing. TaqMan technology was used for real time PCR mRNA quantitation and data analysed using the ABI Prism sequence detection system. The comparative CT method was used to generate fold differences in gene expression between tumour and matched normal controls. Fisher’s exact test and Wilcoxon signed rank test were used to analyse the data.
Results: DUSP6/MKP-3, ERK1 and ERK2 expression in human colon was confirmed by analysing mRNA expression in a human total RNA panel. 28 of 104 tumours (27%) were then found to harbour K-ras mutations. 9 cases were excluded from analyses as extracted mRNA was poor quality and/or very low concentration. Relative expression of ERK1, ERK2 and DUSP6/MKP-3 was, therefore, calculated for 95 cases. Tumour DUSP6/MKP-3 mRNA expression was shown to differ significantly from matched normal tissue (p = 0.0031). Specifically, 56 of the 95 cases (59%) demonstrated tumour over-expression of DUSP6/MKP-3. ERK1 and ERK2 expression did not differ significantly between tumour and normal samples (p = 0.5613 and p = 0.0858 respectively). DUSP6/MKP-3 mRNA expression was not significantly associated with K-ras mutations in this panel of colorectal cancers (p = 0.6274).
Conclusion: Our results suggest that DUSP6/MKP-3 is over-expressed in a significant proportion of colorectal cancers and may act as a tumour suppressor. Mutations in K-ras were not, however, associated with DUSP6/MKP-3 or ERK expression suggesting that this pathway is unlikely to be a mechanism of tumorigenesis in this disease. The prognostic effect associated with K-ras mutations in colorectal cancer is not associated with DUSP6/MKP-3 and alternative downstream pathways of K-ras such as the phosphoinositide-3-kinase pathways require further evaluation in this context.
TISSUE MICROARRAY TECHNOLOGY DNA DAMAGE RESPONSE PROTEINS IN SPORADIC COLORECTAL CANCER
S. Din1, E. Gibson1, D. Faratian2, D. Harrison2, S. Guichard1, D. Jodrell1. 1CRUK Pharmacology and Drug Development Group, 2Department of Pathology, University of Edinburgh, Edinburgh, UK
Introduction: Colorectal cancer (CRC) is a multistep process, progressing from adenoma to a carcinoma by accumulation of defects in genes that regulate cell survival and apoptosis. Two types of genetic aberrations dominate in colorectal cancer; chromosomal instability commonest in sporadic cancers and microsatellite instability (MSI) that accounts for over 90% of hereditary non-polyposis colon cancer (HNPCC). Increasing evidence suggests that the efficacy of conventional chemotherapy and radiotherapy for the treatment of cancer is related in the ability to induce DNA damage. Indeed, both subsets of CRC have demonstrated altered expression of the proteins involved in the DNA damage response (DDR) pathway. Furthermore, several studies have correlated the MSI phenotype of HNPCC with altered protein levels for ATM, Mre11 and Rad50; but no data is available in sporadic cancers.
Aims & Methods: The aim of the study was to determine the expression of DDR proteins in a cohort of sporadic colorectal cancer samples according to their MSI status. A tissue micro-array (TMA) was created from 186 colorectal cancers; 83% were MSI negative and 17% (27) were MSI positive. Three ×0.6 mm cores of each colorectal cancer were represented on the TMA. Core loss was 2–5 cores (1–3%) in MSI negative cancers and 0–1 cores (0–3%) in the MSI positive cancers. Immunohistochemical staining has been undertaken for ATM, Chk2, p53 and p21 proteins. A nuclear histoscore was calculated and each core was given low staining (0–100), moderate staining (101–200) or high staining (201–300) grading.
Results: Sixty one per cent of MSI negative cancers had low staining for ATM compared to 74% of MSI positive cancers. Forty eight per cent of MSI negative and 45% of MSI positive cancers had low ATM-low Chk2 staining. High Chk2 staining was demonstrated in 29% of MSI negative cancers and MSI positive cancers. Common Chk2 mutations result in a more unstable protein compared with the wildtype; therefore the high staining may reflect wildtype protein. In the MSI negative cancers 46% had low staining for p53 and 53% had moderate to high staining; in contrast the majority of MSI positive cancers (74%) had low staining for p53. Both MSI positive and MSI negative cancers had approximately 85% low grade staining for p21.
Conclusion: These results demonstrate a positive association between low ATM-Chk2 expression in all cancers and confirm the differential p53 staining between MSI negative and MSI positive cancers. Immunohistochemistry is underway to investigate other proteins of the DDR pathway and to establish whether activated (phosphorylated) proteins can be reliably detected using TMA technology. These data may give insights into the differential response between the subsets of CRC to current treatment regimens.
CREATION OF A STABLE CELL LINE USING PSEUDOTYPED RETROVIRAL VECTOR GENE TRANSFER OF COX-2 INTO HCT116 CELLS: CHARACTERISATION OF A MODEL SYSTEM FOR THE STUDY OF ASPIRIN’S EFFECTS ON THE PATHOGENESIS OF COLORECTAL CANCER
E. N. Fogden, T. Hagen, C. J. Hawkey. Wolfson Digestive Diseases Centre, University of Nottingham, Nottingham, UK
Introduction: The use of aspirin or non-steroidal anti-inflammatory drugs (NSAIDs) is associated with a reduced risk of colorectal cancer and polyps. Cyclooxygenase (COX)-2 expression is progressively increased in colorectal adenomas and cancer and is thought to play a central role in tumorigenesis. How aspirin affects this process is uncertain.
Aims & Methods: In order to study the effects of aspirin on colorectal carcinogenesis, we used a pseudotyped lentiviral vector for gene transduction of murine COX-2 into HCT116 cells (deficient in COX-2) to create a pair of HCT116 cell lines with and without COX-2 expression. 293GP packaging cells were transfected with Vesicular Stomatitis Virus-G envelope protein and either muCOX-2-FLAG-Puro-Marx or Puro-Marx-Empty Vector using GeneJuice (Novagen.) After 72 h, fresh retroviral vector was applied to HCT116 cells with Polybrene 8 mug/ml. Neoresistant clones were picked after selection with puromycin (1 mug/ml). COX-1 and COX-2 expression was determined by western blotting and immunocytochemistry. EV and COX-2 cell lines were characterised in terms of PGE2 synthesis (PGE2 ELISA), apoptosis (Annexin V/Propidium Iodide Flow Cytometry) and proliferation (Bromodeoxyuridine incorporation) following treatment with aspirin, DFU (COX-2 selective inhibitor) and SC-560 (COX-1 selective inhibitor).
Results: COX-2 expression was demonstrated in the VSV-G:COX-2 infected cells on western blotting and was localised to the cytoplasm and peri-nuclear membrane on immunocytochemistry. Neither uninfected nor VSV-G: Empty Vector HCT116 cells expressed COX-2. Similar levels of COX-1 expression were seen in all three cell lines. Transfection with COX-2 increased PGE2 levels after six hours from 0.95 ng/well in unstimulated VSV-G: Empty Vector cells to 32.45 ng/well in unstimulated VSV-G:COX-2 cells; stimulation with 2.5 μM A23187 (calcium ionophore) increased this further to 103.2 ng/well. The COX-2 selective inhibitor DFU inhibited PGE2 synthesis with COX-2 IC50s of 10−6 M (stimulated) and 10−7 M (unstimulated); the COX-2 IC50s for aspirin were 10−6 M and 5×10−5 M respectively. However, 10−4 M aspirin and 10−5 M DFU caused limited effects on apoptosis and proliferation; aspirin 10−4 M causes a significant reduction in cell viability at 48 hours in VSV-G: COX-2 but not in VSV-G: Empty Vector cells.
Conclusion: 10−4 M Aspirin has limited effects on apoptosis and proliferation in VSV-G:COX-2 HCT116 cells despite effective inhibition of PGE2 synthesis.
VSL3 PROBIOTIC CAN IMPROVE QUALITY OF LIFE IN PATIENTS WITH CHRONIC POUCHITIS
S. J. Gonsalves, P. Mackley, K. Smith, D. A. Burke, P. M. Sagar, P. J. Finan. Colorectal Surgery, The General Infirmary at Leeds, Leeds, UK
Introduction: Chronic pouchitis is a long-term complication after ileal pouch-anal anastomosis (IPAA). Recent studies have suggested that dysbiosis within the pouch may be a contributing factor.1 The McMaster Inflammatory Bowel Disease Questionnaire2 assesses the quality of life (QoL) of patients with inflammatory bowel disease and comprises of 32 questions which are divided into four subscales (bowel, social, systemic and emotional). We aimed to quantify the incidence of chronic pouchitis in our IPAA patients and assess the impact of oral administration of the probiotic VSL3 on quality of life.
Aims & Methods: From 1991 to 2006, 171 patients received an IPAA at our institution of whom 12 patients (7%) were identified with chronic pouchitis. These patients were given a continuous course of oral VSL3. The McMaster questionnaire was sent to patients to record their symptoms before and after commencement of VSL3. The QoL scores before and after VSL3 were compared using a paired Wilcoxon’s test.
Results: Six patients (50%) had pouchitis that was unresponsive to antibiotic therapy. Nine patients (75%) had six or more episodes of pouchitis prior to commencement of VSL3. The median length of time to commencement of VSL3 was 54 (range 11–183) months and the median length of time on VSL3 was 3 (range 1–17) months. Seven patients (58%) returned their questionnaires. Median quality of life scores in all four subscales significantly improved with VSL3 treatment (table).
Conclusion: VSL3 significantly improved the quality of life in a group of our patients with chronic pouchitis. Further studies to determine the changes in histology and endoscopic appearances of the pouch after VSL3 may be useful to explain this improved quality of life.
THE OUTCOME OF POUCH SURGERY IN OLDER PATIENTS
M. W. Johnson1, P. Das2, C. Rippingale3, A. Forbes4, P. J. Ciclitira5, R. Nicholls6. 1Gastroenterology, St Mark’s Hospital, 2Surgery, St Mark’s Hospital, Middlesex, 3Geriatrics, Royal Surrey Hospital, Surrey, 4Gastroenterology, University College London, 5Gastroenterology, St Thomas’s Hospital, 6Surgery, St Mark’s Hospital, London, UK
Introduction: Restorative procto-colectomy (RPC) with ileal pouch anal anastomosis (IPAA) has become the most common elective surgical procedure for patients with ulcerative colitis (UC) and is becoming popular in those with familial adenomatous polyposis (FAP) coli. The medical literature is limited in its assessment of the outcome of RPC and IPAA in those over 60 years of age. The procedure, however, tends to be avoided due to the perceived increased risk of postoperative complications, such as leakage and incontinence.
Aims & Methods: We aimed to assess the true risk and benefits of this type of surgery in older patients. A retrospective study was performed reviewing the St Mark’s RPC database and 22 patients over the age of 60 had undergone the procedure. The notes of 21 of these patients were acquired and data were collected and reviewed.
Results: Of the 21 older patients 15 were male and 6 were female with an average age of 65 years. One had Crohn’s disease, 3 had FAP and 17 had UC. Two procedures were done secondary to perforation, 13 were performed for medically refractory UC, 3 had cancer or severe dysplasia and 3 were done as part of FAP cancer prophylaxis. In total 17 J, 3 W and 1 S pouches were performed, 10 of which were stapled and 11 were hand sutured. Pre-operatively the average stool frequency was 6 with 12 complaining of urgency and 7 suffering from incontinence. Of those who underwent ano-rectal physiology assessment prior to surgery the average maximum resting anal pressure was slightly low at 49 cm/H2O (60–160), with a reduced average anal length of 3.33 cm (3.5–5). All the other markers were within normal ranges. Despite this only 6 postoperatively complained of any leakage and 4 suffered incontinence. Six (29%) developed mild IPAA strictures, 1 (5%) had an intra-abdominal haemorrhage, 2 (10%) suffered wound infection and 2 (10%) developed abscesses. At follow-up 1 suffered chronic recurrent antibiotic sensitive pouchitis whilst 3 had episodic pouchitis. Sixteen (76%) claimed their quality of life had improved, 4 (19%) remained stable, and 1 worsened. No obvious vitamin deficiencies were noted at follow-up.
Conclusion: Age alone should not be used as an exclusion criterion for RPC. Each patient should be assessed individually with open discussions about the risks and benefits. Post operative complications are more frequent but on average the QOL is significantly improved.
CLOSTRIDIUM DIFFICILE-ASSOCIATED DIARRHOEA: LOCAL SOLUTIONS TO A NATIONAL PROBLEM
R. J. Makins1, V. Longstaff2, J. Holland1, A. Mifsud2. 1Gastroenterology, 2Infection Control, Whipps Cross University Hospital, London, UK
Introduction: Clostridium difficile-associated diarrhoea (CDAD) represents an increasing public health concern, particularly with the emergence of virulent strains such as 027. In response to a worrying rise in the number of CDAD cases at Whipps Cross University Hospital (WXUH) the infection control department initiated a number of measures to combat this trend. As well as ongoing staff education and awareness this involved actions such as daily chlorine based cleaning in all adult in patient areas, a trigger system for deep cleaning, establishment of a dedicated working group including input from the gastroenterology department, a CDAD patient care pathway and a highly restrictive antibiotic prescribing policy.
Aims & Methods: To compare the number of cases of CDAD identified at WXUH in 2006/7 following the introduction of these measures compared to the previous 12 months (2005/6) prior to any significant change in management policy. We retrospectively identified patients diagnosed with CDAD from our hospital database.
Results: The changes in hospital practice in relation to CDAD and chronology of introduction were as follows; dedicated isolation August 2006, increased number of isolation rooms September 2006, use of chlorine based cleaning October 2006, deep cleaning trigger system (2 patients with CDAD on same ward) January 2007, establishment of care pathways and formation of working group February 2007, 7 day stool specimen testing for C diff toxin March 2007, piloting of restrictive antibiotic policy March 2007, finalised in June and ongoing education and staff awareness campaign. The table shows the monthly reported, hospital acquired, rates of CDAD. In the 8 months since March 2007 the total number of CDAD cases was signficantly less at 100 (12.5/month) compared to 209 (mean 26.125) in the same period in 2006; p = 0.003. The trend suggests rates continue to fall.
Conclusion: By introducing wide-ranging, step wise, trust wide policies to combat CDAD we have successfully seen a significant reduction in the rates of CDAD at WXUH. The most efficacious interventions have been the formation of a working group, 7-day stool testing for c diff toxin and a highly restrictive antibiotic policy, in particular the cessation of cephalosporin and quinolone use unless absolutely clinically indicated. From an unenviable position of 5th worst rate in London for CDAD for 2006 we now have the 6th best rate among London acute hospitals, as calculated from data submitted to the Health Protection Agency. We have shown that simple measures can be used to address the current critical nationwide situation with c diff to enhance patient safety and ensure the delivery of a health system fit for the 21st century.
AN AGGRESSIVE TREATMENT STRATEGY REDUCES THE MORTALITY ASSOCIATED WITH CLOSTRIDIUM DIFFICILE INFECTION
R. M. P. Mathew1, P. Rastall1, J. Banner2, V. Whately2, D. Hunt3, H. E. Jones4, D. K. Dobie4, I. Perry1, M. A. Cooper4. 1Department of Gastroenterology, 2Infection Prevention Board, New Cross Hospital, Wolverhampton, 3Regional Epidemiologist, Health Protection Agency, West Midlands, 4Department of Microbiology, New Cross Hospital, Wolverhampton, UK
Introduction: The management of Clostridium difficile (C difficile) infection has been hampered by a lack of evidence and a limited appreciation of the significance of the problem. In 2006 we developed a treatment algorithm, drawing on the available evidence, to standardise the treatment of C difficile. This involved an initial patient assessment based on abdominal distension, FBC, CRP and AXR. Severe cases were all assessed by a colorectal surgeon, started on high dose vancomycin and metronidazole and careful attention paid to fluid balance. Recurrences were managed in a standardised manner, including the use of 6 weeks tapering vancomycin and immunoglobulin infusions. This algorithm was launched with an extensive Trust-wide education package supported by readily available advice from gastroenterologists and microbiologists.
Aims & Methods: All cases of C difficile infection were identified by the infection control team and the 28 day mortality was recorded (n = 382 patients).
Results: The table illustrates the mortality patterns in the two periods studied. There is a significant reduction in the mortality associated with C difficile infection (41% reduced to 28%) following the introduction of the treatment algorithm (χ2 test, relative risk of death 0.69 following the introduction of the algorithm, p = 0.023). Limited ribotyping confirmed the presence of the 027 strain in both time periods.
Conclusion: We have demonstrated a significant reduction in the mortality associated with C difficile infection which followed the introduction of an aggressive treatment algorithm.
CLINICAL EXPERIENCE WITH VSL#3 IN PATIENTS WITH CHRONIC POUCHITIS
S. D. McLaughlin1, M. W. Johnson2, S. K. Clark3, P. P. Tekkis1, P. J. Ciclitira2, R. Nicholls1. 1Department of Biosurgery and Surgical Technology, Imperial College, 2Nutritional Sciences Research Division, King’s College, 3Department of Surgery, St Mark’s Hospital, London, UK
Introduction: Pouchitis is common following restorative proctocolectomy for ulcerative colitis. The probiotic VSL#3 is now available in UK pharmacies and has been reported to be effective in maintaining remission in 85% of patients with chronic relapsing pouchitis (CRP) who achieved symptomatic and endoscopic remission following antibiotics (pouch disease activity index (PDAI) ⩽3).1 2 Results in clinical practice have been disappointing.3 The trial dose given was 6 g of 300 billion bacteria (BB) per gram (1800 BB), however because VSL#3 available commercially is 450 BB per gram in 3 g sachets (1 sachet = 1350 BB) the trial dose cannot be given. Excess VSL#3 is known to cause diarrhoea which may be important in clinical practice. We report our clinical experience.
Aims & Methods: Patients with symptomatic CRP without prior history of NSAID use had a flexible pouchoscopy before and following 4 weeks treatment with ciprofloxacin and metronidazole. The (PDAI) was calculated. Those with a clinical PDAI ⩽3 were treated with VSL#3. n = 7 received VSL#3 1350 BB (3 g) per day and n = 8 received VSL#3 2700 BB. n = 3 received both doses.
Results: n = 25 were studied. 12 (48%) had a reduction of PDAI ⩽3 following antibiotic treatment. 13 of 25 (60%) entered symptomatic remission but had a PDAI >3 (no mucosal healing) following antibiotic treatment. 2 subjects (13%) maintained remission with VSL#3 2700 BB at 3 months following antibiotic treatment.
Conclusion: VSL#3 has only been shown in previous work to be effective in patients who achieve endoscopic and clinical remission (clinical PDAI ⩽3) with antibiotics. In this study all achieved clinical remission following antibiotics however, only 12 (48%) had concurrent endoscopic remission and were thus suitable for treatment with VSL#3. Of these, 2 maintained remission at 3 months, both were treated with VSL#3 2700 BB (6 g). The remainder all relapsed at ⩽2 months. Given the low rate of mucosal healing following antibiotics we recommend pouchoscopy should be performed in all patients before considering treatment with VSL#3. Our results and the experience of others(3) suggest that VSL#3 when used in clinical practice may be less effective than originally reported, but should be given at a dose of 6 g VSL#3 (2700 billion bacteria) per day.
MISSED CROHN’S DISEASE IS UNLIKELY AS A CAUSE OF UNEXPLAINED IRON DEFICIENCY IN POUCH PATIENTS: EVIDENCE FROM VIDEO CAPSULE ENDOSCOPY
S. D. McLaughlin1, A. J. Bell2, A. J. Postgate3, S. K. Clark4, P. P. Tekkis1, P. J. Ciclitira5, R. J. Nicholls6. 1Department of Biosurgery and Surgical Technology, Imperial College, London, 2Department of Gastroenterology, Weston-Super-Mare General Hospital, Somerset, 3Department of Gastroenterology, 4Department of Surgery, St Mark’s Hospital, 5Department of Gastroenterology, King’s College London, 6Department of Surgery, Imperial College, London, UK
Introduction: Iron deficiency anaemia (IDA) is common following restorative proctolectomy (RPC). Causes include pouchitis, pre-pouch ileitis and missed Crohn’s disease (CD). Video capsule endoscopy (VCE) is commonly used to investigate unexplained IDA and exclude small bowel CD, however there are significant cost implications and no studies of its use following RPC.
Aims & Methods: We aimed to establish whether IDA following RPC is associated with significant pre-pouch small bowel inflammation. 10 patients who had VCE for IDA were identified from the St Mark’s database, notes were reviewed. All had pouch and/or pre-pouch ileal inflammation at pouchoscopy. 6 had chronic refractory pouchitis and 1 antibiotic resistant pouchitis. Coeliac disease, inadequate diet and NSAID use had been excluded as a cause of IDA.
Results: See table. At follow-up (mean 24 months); no patient has been reclassified as CD.
Conclusion: In contrast to a recent Italian study of VCE in which all 15 patients with chronic refractory pouchitis (CRP) were found to have diffuse small bowel lesions,1 in our study. only one of ten had signs of inflammation proximal to the pre-pouch ileum. Numbers are small but our findings suggest that in IDA following RPC investigations need go no further than endoscopy of the pouch and pre-pouch ileum if these are inflamed. Re-classification to CD is inappropriate without re-assessment of the colectomy specimen and classical findings away from the pre-pouch ileum.2 3
WHAT IS THE INCIDENCE OF COLORECTAL CANCER FOR GIVEN COLONOSCOPIC INDICATIONS AND PATIENT AGES?
V. Mitra, V. Mitra, S. Whitehouse, M. Rutter. Gastroenterology, University Hospital of North Tees, Stockton, UK
Introduction: Colorectal cancer (CRC) is the third most common cancer in the U.K. and the second most common cause of cancer death with more than 16 000 deaths each year. Colonoscopy is the gold standard investigation for CRC. Knowing the incidence of CRC for a given indication and patient age permits a more meaningful discussion with patients.
Aims & Methods: We aimed to determine the colonoscopic incidence of CRC for different presenting symptoms and age cohorts. We carried out a retrospective audit of all colonoscopies performed in our trust between February 2007 and September 2007. Cases were identified using our endoscopy reporting software (Unisoft). Demographic details, indications for the procedure and colonoscopic diagnosis were recorded, and colonoscopic incidence of CRC calculated.
Results: The table shows the percentage of patients in each age cohort (total number of patients in each age cohort) diagnosed with CRC referred with various indications for colonoscopy.
Conclusion: Our study shows that most colorectal cancers are detected over the age of 60, the incidence rising each decade thereafter. For patients diagnosed with CRC, iron deficiency anaemia (IDA) was the commonest indication, accounting for 41.5% of all CRC detected. A high proportion of patients over 60 years of age referred with IDA (including 22% of those aged 80 or over) had CRC on colonoscopy, reiterating the importance of investigating these patients urgently. These data also allow a more meaningful discussion with patients prior to investigation, and help both the patient and clinician to make an informed decision on whether colonoscopic investigation is appropriate.
IDENTIFICATION OF GENETIC VARIATION IN DUT, A POTENTIAL COLORECTAL TUMOUR SUPPRESSOR GENE
K. J. Monahan1, L. Carvajal-Carmona2, C. Thirlwell2, H. J. W. Thomas1, I. P. Tomlinson2. 1Family Cancer Clinic, St Mark’s Hospital, Imperial College, 2Molecular and Population Genetics Lab, Cancer Research UK, London, UK
Introduction: Gene expression arrays have been used for almost a decade to further our understanding of carcinogenesis. Recently the technology has led to the discovery of a new cancer predisposition gene for the first time.
Aims & Methods: The aim of this project was to identify potential tumour suppressor genes by studying gene expression profiles of patients with a predisposition to colorectal neoplasia. Affymetrix U133 Plus 2.0 GeneChip oligonucleotide arrays were used to generate expression profiles for 12 multiple polyp patient, 6 young cancer patient and 6 control cell lines. Three differentially expressed genes were screened in 94 cases using Lightscanner technology and direct sequencing.
Results: Sixty three transcripts representing 58 genes were expressed with a more than threefold difference in multiple polyp patients compared to controls (p<0.01). Sixty three transcripts representing 61 genes were identified in young cancer patients with the same significance level. Two genes with potential tumour suppressor function DUT, POLE2 (both DNA repair genes) and CXCR4 (a proto-oncogene with a proven role in colorectal neoplasia) were screened for germline mutations. An amino acid changing variant DUT V154G was identified in 5/47 multiple polyp patients, and 0/47 controls (p = 0.028, Fisher’s exact).
Conclusion: A novel variant has been identified in a DNA repair gene DUT in multiple polyp patients using germline expression profiling to identify candidate genes. Further work is necessary to characterise the functional importance of this variation.
A CASE CONTROL STUDY OF TP53 ARG72PRO IN COLORECTAL CANCER AND A META-ANALYSIS OF THE ROLE OF THIS POLYMORPHISM IN CANCER
K. J. Monahan1, A. Walther2, H. J. W. Thomas1, I. P. Tomlinson2. 1Family Cancer Clinic, St Mark’s Hospital, 2Molecular and Population Genetics Lab, Cancer Research UK, London, UK
Introduction: Loss of TP53 function is likely to be a critical event in tumorigenesis and approximately 70% of colorectal cancers show this alteration. An amino acid altering polymorphism Arg72Pro has been studied as a potential low penetrance allele for colorectal cancer in over 12 studies with equivocal results.
Aims & Methods: The Idaho technology Lightscanner was used to differentiate genotypes among 1873 colorectal cancer cases and 1299 controls, with subsequent 100% confirmation of about 5% of genotypes by direct sequencing. Associations of genotypes with the following clinicopathological features were tested: sex; site of tumour; Dukes stage; age of onset; presence of adenomas; and three-year overall and disease-free survival. A meta-analysis of this polymorphism in colorectal and other cancer was also performed. 177 studies were included, which consisted of a total of 55 274 controls and 39 869 patients.
Results: No significant association was found between TP53 Arg72Pro and colorectal neoplasia. A meta-analysis of 13 studies showed no association with colorectal neoplasia (OR 0.99, 95% CI 0.86 to 1.15; fig). In studies examining the association in all cancer types a positive association was identified only among Chinese subjects (OR 1.22, 95% CI 1.08 to 1.38).

Conclusion: No association of the Arg72Pro polymorphism was identified with colorectal neoplasia overall or for any clinicopathological characteristics. A meta-analysis confirmed this lack of association in all groups except for a subgroup analysis of Chinese cancer patients.
CHARACTERISATION OF PROGENITOR CELLS IN COLORECTAL CANCER AND THE ADULT HUMAN COLON
J. Murphy, S. Khalaf, R. E. Hands, K. A. Gill, S. M. Scott, N. S. Williams, S. A. Bustin. Bowel and Cancer Research Laboratory, Centre for Academic Surgery, London, UK
Introduction: Prominin-1 gene encodes the CD133 cell surface antigen which has been proposed as a colorectal “cancer stem cell” marker. However, CD133 has also been suggested to play a role in the cellular organisation of non-malignant cells.
Aims & Methods: The purpose of this study was to clarify CD133 expression patterns in the human gut. Twenty normal small bowel, colon/rectal samples, and twenty colorectal cancer samples were obtained following ethics committee approval and informed consent. Samples were analysed for prominin-1 mRNA/CD133 epitope expression using RT-qPCR, immunohistochemistry, western blotting, as well as for co-localisation of CD133 with specific lineage markers (gastrointestinal, CDX-1/2; haematopoietic, CD13/CD34; monocyte, CD68; endothelial, CD144).
Results: Prominin-1 mRNA was detected in all samples, with no difference found between normal tissue and cancer (p = NS). Two patterns of CD133 expression were found: small bowel displayed baso-lateral and apical epithelial cell membrane expression, while colon and rectum expressed CD133 on epithelial and subepithelial myofibroblast cell membranes. CD133 co-localised with CDX1/2 and CD34, but not with CD68/144, in normal tissue. CD133 was expressed unevenly in colorectal cancer epithelial cells.
Conclusion: CD133 expression in a subpopulation of cancer cells may represent epithelial/myofibroblast lineage, rather than identifying “cancer stem cells”. CD133 co-localised with CD34, thus supporting the hypotheses that either a proportion of epithelial cells derive from haematopoietic progenitors homing to the intestinal niche, or that epithelial progenitors express markers of haematopoietic lineage, suggesting continued multipotency. Further studies are necessary to assess these hypotheses.
STRAIGHT-TO-TEST COLONOSCOPY FOR TWO-WEEK TARGET SUSPECTED COLORECTAL CANCER REFERRAL: IS IT BETTER?
A. Nikolopoulos1, M. Walshe1, C. Ingham-Clark2, V. Wong1. 1Gastroenterology, 2Surgery, the Whittington hospital NHS trust, London, UK
Introduction: Colorectal cancer (CRC) remains the second commonest cause of cancer death in UK. Early diagnosis is crucial in determining the prognosis of the disease. Currently the patient’s pathway from a GP’s two-week target (2WT) referral for suspected CRC usually involves an out-patient clinic consultation prior to appropriate test including colonoscopy.
Aims & Methods: The aim of this pilot study was to assess prospectively whether straight-to-test (STT) after an initial triage via a telephone assessment by a nurse would be a safe and acceptable pathway of investigating 2WT CRC referrals. 50 consecutive 2WT CRC referrals between January to September 2007 were included. Patients were assessed by using a standard proforma via telephone. Exclusion criteria were age >75, diabetes, ASA score >2 (patients with severe systemic disease) or inability to speak English.
Results: Of the 50 patients, 33 patients were eligible for analysis (17 patients excluded because they were either not contactable or spoke no English). There were 21 males and 12 females aged 33–77 years. In most cases it took up to 6 days from the referral to triage (47/50 patients). Out of the 33 patients another 7 did not proceed to having a direct colonoscopy because of exclusion criteria. The colonoscopy results for the 26 patients (17 male) were normal for 15, 5 showed a colonic polyp (2 adenomatous, 2 hyperplastic and 1 inflammatory), 3 ulcerative colitis, 2 diverticulosis and 1 angiodysplasia. There were no serious adverse events documented.
Conclusion: Our preliminary results suggest that after careful selection of patients with appropriate exclusion criteria it is possible to proceed STT colonoscopy without a pre-procedure clinic appointment. STT colonoscopy seems to be a safe way of reducing waiting time and potentially costs for suspected CRC. This pilot project is in progress and we plan to include other patients referred with alarm symptoms as well as assessing patient satisfaction.
DETECTION OF EARLY CANCERS BY COLORECTAL CANCER SCREENING AND ANALYSIS OF THE PRESENCE OF UNDERLYING SYMPTOMS
C. J. Rees1, M. Ritchie1, D. Nylander2, J. Painter2, J. Singh3, G. Waddup4, L. Hurst4, T. Pugh4, M. Rutter4. 1South of Tyne Bowel Cancer Screening Centre, South Tyneside General Hospital, South Shields, 2South of Tyne Bowel Cancer Screening Centre, Sunderland Royal Infirmary, Sunderland, 3South of Tyne Bowel Cancer Screening Centre, Queen Elizabeth Hospital, Gateshead, 4Tees Bowel Cancer Screening Centre, University Hospital of North Tees, Stockton, UK
Introduction: Few colorectal cancers present at an early stage (46% Dukes stage A or B). The national Bowel Cancer Screening Programme (BCSP) aims to identify cancers at an early stage and reduce mortality from colorectal cancer. Symptomatic patients should be referred urgently for specialist opinion.
Aims & Methods: Data from the South of Tyne and Tees screening centres were collected from March to October 2007. These centres serve a population of 1.5 million. Analysis of the data identified the % of positive FOBs, the number of colonoscopies undertaken and the pathology diagnosed. Pathology was categorised per BCSP criteria as cancer (including polyp cancers) high risk polyps; intermediate risk polyps; low risk polyps; abnormal but not polyp or normal. Where cancer was diagnosed data on stage were collected where sufficient time since diagnosis allowed. Patients were questioned as to whether they had underlying symptoms and whether they had sought medical advice.
Results: 1.6% of FOBs performed in the screening populations were positive. 521 colonoscopies were undertaken in 2 centres by 5 colonoscopists. 53 (10%) patients had colorectal cancer diagnosed; 49 (9%) patients had high risk polyps; 101 (19%) had intermediate risk polyps; 103 (20%) had low risk polyps; 96 (18%) were abnormal but not polyps (these included mostly patients with inflammatory bowel disease, diverticulosis, angiodysplasia or haemorrhoids); 119 (23%) colonoscopies were recorded as normal. Of the 521 colonoscopies, in 284 (55%) instances the patients had lower GI symptoms. Of 53 cancers diagnosed, 38 (72%) of these patients were symptomatic. Cancer patients were more likely to be symptomatic when compared to patients with a normal colonoscopy (48/119 (40%)) (p = 0.0002). 9 (17%) cancer patients had consulted their general practitioner but had not been referred for investigation. 41 cancer patients were fully staged at the time of submission and 31/41 (75%) of these patients had Dukes A or B disease. The table demonstrates the Dukes stage of the diagnosed cancers.
Conclusion: Bowel cancer screening detects early cancers and many polyps. Many patients attending for colonoscopy had lower GI symptoms including 72% of patients diagnosed with cancer. While screening identifies significant pathology more must also be done to get patients with lower GI symptoms to attend for investigation.
Research submitted on behalf of the Northern Region Endoscopy Group.
THE INCIDENCE AND MANAGEMENT OF POLYP CANCERS IN THE BOWEL CANCER SCREENING PROGRAMME
T. Pugh1, W. Copping1, G. Waddup1, L. Wells1, M. Ritchie2, L. Hurst1, J. Singh2, J. Painter3, D. Nylander3, C. Rees4, M. D. Rutter1. 1Tees Bowel Cancer Screening Centre, University Hospital of North Tees, Stockton-on-Tees, 2South of Tyne Bowel Cancer Screening Centre, Queen Elizabeth Hospital, Gateshead, 3South of Tyne Bowel Cancer Screening Centre, Sunderland Royal Hospital, Sunderland, 4South of Tyne Bowel Cancer Screening Centre, South Tyneside District Hospital, South Shields, UK
Introduction: Polyp cancers are relatively rare, but are being detected regularly within the bowel cancer screening programme (BCSP). We report the incidence and management decisions from two screening centres.
Aims & Methods: A comprehensive prospective dataset is collected as part of the BSCP. We analysed these data to assess the incidence and management of polyp cancers detected during the first 6 months practice of the South of Tyne and the Tees Screening Centres (combined population 1.5 million people).
Results: Index screening colonoscopies were performed on 521 people. 48 cancers were detected, of which 9 were polyp cancers (incidence at colonoscopy 1.7%; representing 18.75% of cancers detected). Seven patients were male and two female. As this was a screening population, all patients were aged 60 to 70 years. In the pre-colonoscopy nurse clinic, 4/9 patients had described overt bowel symptoms (3 rectal bleeding and 1 altered bowel habit; none had presented to their GP with these symptoms). Only 1/9 patient had a strongly positive initial FOB test –8/9 were referred for colonoscopy after an ongoing weak positive result on retesting. 2 cancers were in the rectum, 5 in the sigmoid and one each in the caecum and descending colon. There were no synchronous cancers. 7/9 were pedunculated and 2/9 sessile. All were felt to have been completely excised endoscopically. 3/9 were classified as Haggitt stage 1; 2 as Haggitt stage 2; 3 as Haggitt stage 3 and one was not classifiable owing to fragmented histological specimen. All underwent staging cross-sectional imaging by CT/MRI according to site of lesion—no evidence of invasive disease was detected. No patient had evidence of residual local disease on re-scoping. All patients were discussed at colorectal multidisciplinary team (MDT) meetings. Six patients are being managed without surgery, 1 was offered but declined right hemicolectomy (caecal Haggitt stage 1), one patient is awaiting surgery for a Haggitt stage 3 lesion in the sigmoid colon and 1 other patient is awaiting MDT decision.
Conclusion: Polyp cancers are common within the screening programme. 8/9 were only referred after FOB re-testing of an initial weakly positive result. Standardised guidance on polyp cancer management would be worthwhile. Ongoing monitoring of this particular cohort will provide valuable additional prognostic information.
Submitted on behalf of the northern region endoscopy group (NREG).
PEROXISOME PROLIFERATOR ACTIVATED RECEPTOR-α LIGAND, METHYCLOPHENAPATE, SUPPRESSION OF COLONIC TUMOURS APCMIN/+ MICE IS PPAR-α DEPENDENT
A. Shonde1, D. Bell2, A. Bennett3, C. Hawkey1. 1WDDC, University Hospital Nottingham, 2Biology, 3Biological Sciences, University of Nottingham, Nottingham, UK
Introduction: Peroxisome proliferator-activated receptor-α (PPAR-α) is expressed at low levels in human colorectal cancers. The significance of this receptor in colorectal carcinogenesis is unknown. APCMin/+ mice fed with methylclofenapate (a PPAR-α ligand) have significantly less tumour burden in the small intestine and colon compared to control.1 It is not certain that this response is PPAR-α dependent. We hypothesise that PPAR-α activation in the colon can prevent colon cancer. We studied the effect of pharmacological PPAR-α ligand, methyclofenapate on colon carcinogenesis in APCMin/+ PPAR-α−/− mice.
Aims & Methods: We aimed to establish whether the tumour suppressive function of methylclofenapate in APCMin/+ mice is PPAR-α dependent. Once weaned, male and female APCMin/+ (n = 20) and APCMin/+ PPAR-α−/− mice (n = 20) were randomised to recieve methylclofenapate 25 mg/kg/day (suspended in safflower oil) or safflower oil alone. The drug was administered daily by oral gavage. These mice were monitored for signs of distress and white paw. Mice were sacrificed if they show signs of distress, had rectal prolapse or if they lost >20% body weight. The colons were laid open and tumour number assessed.
Results: APCMin/+ PPAR-α−/− mice treated with MCP did not have significantly different tumour numbers to mice administered safflower oil alone. The mean number of tumours in the colon was 2.35 (SE 0.38) in APCMin/+ PPAR-α−/− mice treated with MCP and 2.30 (0.46) in mice treated with safflower oil (p>0.05). However the mean number of tumours in APCMin/+ treated with safflower oil was 2.26 (0.37) compared to 1.05 (0.25) in mice treated with MCP (p<0.020). 70% of tumours were located in the distal third of the colon in both groups.
Conclusion: The failure of MCP to reduce tumour number in APCMin/+ PPAR-α−/− mice suggest that the reduction of tumour burden in APC Min/+ mice colon by MCP was due to activation of PPAR-α. Greater understanding PPAR-α dependant genes may enable the pathogenesis of colon cancer to be further understood.
LOSS OF NUCLEAR STAT-1 AND ATM ARE AN INDEPENDENT MARKER OF BAD PROGNOSIS IN COLORECTAL CANCER
J. A. Simpson1, N. N. F. S. Watson1, J. J. H. Scholefield1, M. Ilyas2, L. L. G. Durrant3. 1Academic Department of Surgery, 2Department of Pathology, Queens Medical Centre Campus, Nottingham University Hospital, 3Academic Department of Clinical Oncology, Institute of Immunology, Infections and Immunity, University of Nottingham, City Hospital, Nottingham, UK
Introduction: STAT-1 (Signal Transducer and Activator of Transcription 1) is activated by stress and type-1 interferons and has an important role in controlling cell cycle progression and apoptosis. Considered a tumour suppressor, STAT-1 activation is associated with phosphorylation of Chk2, p53 and ATM, leading to growth arrest and/or apoptosis following DNA damage.1
Aims & Methods: Our aim was to determine whether the presence of STAT-1 and ATM confers a survival advantage in colorectal cancer. Using tissue microarrays, we analysed interferon gamma receptor 1 (IFNGR1), STAT-1 and ATM expression in over 400 colorectal tumours, correlating expression with clinicopathological factors and disease-specific survival.
Results: On survival analysis, nuclear STAT-1 +ve tumours were associated with a longer disease specific survival of 77 months (95% CI 66 to 87) vs 62 months (95% CI 56 to 68) than nuclear STAT-1 -ve tumours (p = 0.0113). In contrast lack of nuclear ATM staining was not associated with survival. Of particular interest was that survival of nuclear STAT-1 +ve tumours was not affected by the expression or loss of ATM, survival of 78 months (95% CI 64 to 93) and 76 months (95% CI 62 to 91) respectively. However in the tumours lacking nuclear STAT-1 loss of ATM conferred a significantly (p = 0.018) worse survival of 56 months (95% CI 47 to 64) compared to STAT-1-ve ATM +ve tumours with survival of 67 months (95% CI 56 to 75). On multivariate analysis, tumour (TNM) stage, extramural vascular invasion and lack of nuclear STAT-1 (p = 0.04) and ATM expression (p = 0.01) were identified as independent prognostic factors.
Conclusion: These results show that lack of STAT-1 and ATM leads to lack of DNA repair and growth delay and/or apoptosis leading to an aggressive tumour phenotype.
DEFECTS IN GAMMA INTERFERON SIGNALLING CAN ALTER THE PROGNOSIS OF COLORECTAL CANCER
J. A. Simpson1, N. N. F. S. Watson1, J. J. H. Scholefield1, M. M. Ilyas2, L. L. G. Durrant3. 1Academic Department of Surgery, 2Department of Pathology, Queens Medical Centre Campus, Nottingham University Hospital, 3Academic Department of Clinical Oncology, Institute of Immunology, Infections and Immunity, University of Nottingham, City Hospital, Nottingham, UK
Introduction: Stat1 (Signal Transducer and Activator of Transcription 1) is activated by type-I interferons and has an important role in controlling cell-cycle progression and apoptosis. Considered a tumour suppressor, Stat1 activation is associated with growth arrest. It has been suggested that defective Stat1 signalling favours tumour development by compromising immune surveillance.
Aims & Methods: Using immunohistochemical staining we have screened 10/80 colorectal cancer cell lines for their ability to phosphorylate STAT-1 and up-regulate MHC class I in response to gamma interferon (IFNγ).
Results: Two cell lines failed to express any MHC, one cell line failed to respond to IFNγ and was shown to lack expression of the receptor and a fourth cell line constitutively phosphorylated STAT-1 and showed no further response to IFNγ and no up regulation of MHC.
Conclusion: These results suggest that defects in this pathway are common and that they can occur at several places in the pathway. Using tissue microarrays, we have previously shown that reduced expression of MHC class I is an independent marker of poor prognosis.1 We have now analysed interferon gamma receptor 1 (IFNGR1) and Stat1 expression in over 400 colorectal tumours, correlating expression with clinicopathological factors and survival. Latent (cytoplasmic) Stat1 was detected in 85% of the tumours examined, with activated (nuclear) Stat1 in 18%. Nuclear Stat1 expression was associated with tumour de-differentiation. On survival analysis, nuclear Stat1 +ve tumors were associated with a longer disease specific survival of 77 months (95% CI 66 to 87) vs 62 months (95% CI 56 to 68) in nuclear Stat1 -ve tumours (p = 0.0113). On multivariate analysis, tumour (TNM) stage, extramural vascular invasion and nuclear Stat1 expression were identified as independent prognostic factors. These results show that IFN-γ signalling is associated with less aggressive colorectal tumours and suggests a role for immune surveillance in this group of tumours.
THE UK NATIONAL BOWEL CANCER SCREENING PROGRAMME: EXPERIENCE OVER THE FIRST SIX MONTHS FROM THE NORTHEAST OF ENGLAND
J. N. Singh1, N. Dempsey1, M. Ritchie1, W. Copping2, L. Wells2, M. Rutter2, C. Rees3, D. Nylander4, J. Painter4. 1South of Tyne Bowel Cancer Screening Centre, Queen Elizabeth Hospital, Gateshead, 2Tees Bowel Cancer Screening Centre, North Tees General Hospital, Stockton, 3South of Tyne Bowel Cancer Screening Centre, South Tyneside General Hospital, South Shields, 4South of Tyne Bowel Cancer Screening Centre, Sunderland Royal Hospital, Sunderland, UK
Introduction: The UK National Bowel Cancer Screening Programme (BCSP) uses faecal occult blood tests to screen 60–69-year-olds. UK pilot studies have demonstrated a pick up rate of 8.6 to 10.18% for cancers and 45.9 to 46.9% for adenomas in this age group.
Aims & Methods: A prospective dataset is collected as part of the BSCP. Presented is combined data from the first 6 months’ practice of the South of Tyne and the Tees screening programmes.
Results: Initial colonoscopies were performed on 472 people between 23/3/07 and 22/9/07. Of these 24 had 1 further colonoscopy, 1 had 2 follow-up colonoscopies, 11 had 1 follow-up flexible sigmoidoscopy (Flexi-sig), 1 had 2 flexi-sigs, 4 had both a 2nd colonoscopy then flexi-sig; and 2 had a barium enema. Repeat procedures: initial poor bowel prep (3); tortuous bowel (4); patient discomfort (1); inconclusive histology or to confirm complete excision (18); and at the discretion of the screening colonoscopists following polypectomy (but outside of the BSG polyp surveillance recommendations) (16). Bowel preparation was excellent or adequate in all but 8 procedures. Colonoscopy completion rate was 96.4% (malignant stricture (6); poor prep (1); looping (2); intended “limited” repeat colonoscopy (6), patient discomfort (2), bradycardia (1)). Median procedure time was 21 min (range 5–95). Median withdrawal time was 10 min (range 2–75). Out of 537 GI scopes: 41 normal; 308 had polyps (median 2; range 1–16 in those with polyps) of which 272 had adenomas (detection rate 50.7%); 48 cancers (10.2%); 37 had other abnormalities (diverticular diseases (27); angiodysplasia (4); proctitis (1); ileitis (1); radiation colitis (1); haemorrhoids (3)). 84 patients (15.6%) had intermediate risk polyps according to BSG Polyp Surveillance Guidelines requiring repeat colonoscopy in 3 years. 41 (7.6%) had high-risk polyps requiring colonoscopy at 1 year. No sedation used (n = 112). Sedation used: Midazolam 1 mg (n = 1), 2 mg (258), 3 mg (55), 4 mg (67), 5 mg (1); Pethidine 25 mg (48), 50 mg (12); Buscopan 10 mg (63), 20 mg (109). Comfort levels: no or minimal pain 66.3%; mild 19.7%; moderate 12.8% and severe 1.2%. Sedation levels: awake 73.6%; drowsy 25.2% and asleep but responding to name 1.2%. Complications: prolonged pain (2); haemorrhage (2); bradycardia (1). None required surgery.
Conclusion: Our cancer and adenoma detection is in keeping with expectations from the pilot studies. Nearly 1 in 4 screened will require subsequent polyp surveillance within the screening programme.
Presented on behalf of the Northern Region Endoscopy Group (NREG).
BOWEL CANCER SCREENING: ARE WE SCREENING AN ASYMPTOMATIC POPULATION?
G. J. Sadler1, A. Giles2, C. L. Simpson2, E. T. Swarbrick1, A. M. Veitch1. 1Gastroenterology, New Cross Hospital, Wolverhampton, 2Bowel Cancer Screening, Wolverhampton, UK
Introduction: Population bowel cancer screening with faecal occult blood test (FOBT) and colonoscopy has been shown to reduce colorectal cancer mortality. The UK National Bowel Cancer Screening Programme commenced in July 2006 in Wolverhampton (screening population 850 000). 60–69-year-olds are offered FOBT, then colonoscopy if FOBT-positive. We aimed to determine whether we are screening an asymptomatic population, or whether there are pre-existing symptoms.
Aims & Methods: FOBT-positive patients attending nurse clinics were questioned prospectively regarding symptoms. Data were analysed to determine the prevalence of symptoms, pathology detected and whether symptoms predicted pathology.
Results: Data from the first 15 months of the bowel cancer screening programme in Wolverhampton were analysed. Some patients had more than one symptom. There was no statistically significant association between the presence of individual or collective symptoms and pathology detected.
Conclusion: The majority of patients in the screening programme report recent gastrointestinal symptoms. Only approximately 1 in 3 patients overall, and 1 in 4 patients with cancer, were asymptomatic. This phenomenon of a high proportion of symptomatic patients is common in the first round of screening programmes, and can be attributed in part to raised awareness of the importance of pre-existing symptoms. Symptoms, individually or collectively, do not predict pathology in this bowel cancer screening population.
Inflammatory bowel disease posters
SUPERINFECTION IN INFLAMMATORY BOWEL DISEASE: DOES IT REALLY MATTER?
G. W. Moran1, S. Cherian1, S. DeSilva1, G. Roberts1, M. Gill2, P. Taniere3, R. Boulton1, J. Goh1. 1Department of Gastroenterology, 2Department of Microbiology, 3Department of Histopathology, University Hospital Birmingham, Birmingham, UK
Introduction: Hospital acquired infections, most notably Clostridium difficile (C diff) are increasing. At risk patients include the elderly, immunocompromised and those receiving antibiotics. This therefore encompasses inflammatory bowel disease (IBD) patients. Does superinfection effect the outcome of IBD?
Aims & Methods: Retrospective case series analysis of superinfection in an IBD cohort in a tertiary referral centre. Patients were identified from IBD, pathology and microbiology database and case note review.
Results: We identified 60 infective episodes in 55 patients. Mean age was 42.9 years. 35 female:20 male, 33 ulcerative colitis: 22 Crohn’s disease. Mean IBD duration was 82 months. The commonest pathogen was C diff with 45 cases (table) followed by campylobacter with 11 cases (table). Other infections of note were CMV colitis (n = 4), Salmonella ssp (n = 2), Giardia and strongyloides infection (n = 1 each). 42 episodes (70%) needed admission (79% C diff) for a mean stay of 17.9 days (5–53 days). No mortality was recorded. 3 patients had post-op complications.
Conclusion: Clostridium difficile was the commonest superinfection, and associated with immunosuppression, high admission rate, long hospital stay, and 11% risk of laparotomy but no increase in mortality. We have developed a C diff regression model with a specificity of 96% that identified patients failing medical therapy. Campylobacter was unexpectedly common in our patients. All were treated with antibiotics and only 1 case required surgery. CMV was generally diagnosed in patients with active colitis that failed to respond to immunosuppression. It responded to reducing immunosuppression and gancyclovir. One patient later required colectomy for UC. A further study comparing outcomes in a matched IBD cohort is underway.
NEUTRALISING ANTIBODIES TO CERTOLIZUMAB PEGOL DO NOT APPEAR TO IMPACT ON EFFICACY OR SAFETY IN PATIENTS WITH CROHN’S DISEASE
A. M. Nesbitt1, S. Stephens2, R. Bloomfield3. 1Antibody Biology Division, 2Clinical Assay Department, 3Biometrics, UCB Celltech, Slough, UK Kingdom
Introduction: Treatment of Crohn’s disease (CD) patients with anti-TNF therapeutic molecules has been shown to be efficacious; however, development of neutralising antibodies can potentially reduce the clinical response rate.1 Certolizumab pegol, a PEGylated Fab’ antibody fragment with high potency for human TNFα, was evaluated in two recently completed pivotal Phase III trials in CD (PRECiSE 1 and 2).
Aims & Methods: The aim of this study was to examine the effect of neutralising antibodies on efficacy and safety in PRECiSE 1 and 2. Patients received certolizumab pegol 400 mg at weeks 0, 2, 4, and then every 4 weeks up to week 24. Blood samples were considered antibody-positive (Ab+) if they reversed the ability of certolizumab pegol to block IL-6 production in response to TNFα in HeLa cells. Patients designated Ab+ had at least one blood sample positive for neutralising antibodies. Clinical response was defined as a decrease in CD Activity Index (CDAI) score of 3100 points at weeks 6 and 26. The influence of antibody status on the incidence of adverse events (AEs) was also examined.
Results: The numbers of patients who received continuous treatment with certolizumab pegol and had a clinical response were categorised according to the presence or absence of neutralising antibodies (table). There was no reduction in the proportion of responders in the Ab+ cohort vs the Ab- cohort in either trial. The incidence of most AEs was similar regardless of neutralising antibody status. AEs that occurred more frequently in patients after development of antibodies were viral gastroenteritis (3% (Ab+) vs 1% (Ab-)) and anaemia (5% vs 3%). AEs occurring more frequently in Ab- patients were nausea (9% (Ab-) vs 2% (Ab+)), pyrexia (8% vs 4%) and headache (17% vs 5%). No hypersensitivity signals (for example, injection-site reactions, injection-site pain, influenza-like illness or rash) were associated with the presence of antibodies.
Conclusion: The presence of neutralising antibodies to certolizumab pegol does not appear to have a marked effect on clinical response rates in patients with CD. The frequency of AEs was similar in Ab- and Ab+ patients. There was no indication of hypersensitivity reactions in patients.
OPTIMISATION OF PATIENTS WITH CROHN’S DISEASE PRIOR TO ILEOCOLIC RESECTION TOGETHER WITH MULTI-MODAL POSTOPERATIVE REHABILITATION MAY SHORTEN LENGTH OF STAY
R. Newbury1, S. Hultin1, K. Fazal1, V. Patel2, M. Ellwood2, E. Carapeti2, A. Ansari1, A. Williams2. 1Gastroenterology, 2Surgery, St Thomas’ Hospital, London, UK
Introduction: STH introduced an enhanced recovery programme (ERP) in October 2006 for lower GI surgery. Measures included high calorific drinks prior to surgery and early feeding post surgery, fluids PO until 2 hours before, Doppler-guided fluid replacement and early mobilisation. These have previously been associated with shorter length of stay after colorectal cancer surgery and one previous Danish study in Crohn’s ileocolic resections.1
Aims & Methods: To compare all patients with Crohn’s disease who underwent right ileocolic resection at STH in the 2 years prior to the introduction of the ERP to those performed with optimisation. Case notes and electronic records were reviewed retrospectively (2004–5) for patients during the 2 years prior to the ERP. For those patients within the ERP, data had been collected prospectively. Variables recorded included steroids, immunosuppressives, mesalazine and opiates prior to surgery, demographics, BMI, extent and type of surgery.
Results: 18 pre-ERP and 11 ERP patients were identified. Within both the ERP group and the pre-ERP group 3 had laprascopic or laprascopic assisted operations. A primary anastamosis without stoma was formed in 4 of the 11 pre-ERP patients as compared to 8 of the 10 ERP patients. Perforation, abscess and wound infections were similar in both groups. As were steroids and narcotics use prior to surgery use in each group. The chart compares length of stay in each group.

Conclusion: There was a significant decrease in length of stay, no confounding factors identified that would account for differences between the 2 groups. These data are comparable to a previous study for patients who underwent ileocolic resection for Crohn’s and CRC surgery.
A NOVEL POPULATION OF CD56+ HLA-DR+ COLONIC LAMINA PROPRIA CELLS IS ASSOCIATED WITH INFLAMMATION IN ULCERATIVE COLITIS
S. C. Ng1, S. Plamondon1, H. O. Al-Hassi1, N. English1, N. Gellatly1, M. A. Kamm2, S. C. Knight1, A. J. Stagg1. 1Antigen Presentation Research Group, 2Gastroenterology, St Mark’s Hospital, London, UK
Introduction: The immunopathology of ulcerative colitis (UC) relates to an inappropriate mucosal immune response to constituents of the intestinal microbiota in genetically susceptible individuals. HLA-DR+ lin-/dim (lin = anti-CD3, 14, 16, 19, 34) cells extracted from human intestinal tissue contain CD11c+ myeloid dendritic cells (DC) that contribute to the immunoregulatory events that normally limit inflammatory responses to commensal bacteria. Also present within the HLA-DR+ lin-/dim population are hitherto poorly characterised CD11c- cells. We hypothesised that this population in the gut may also contribute to intestinal inflammation in active UC.
Aims & Methods: HLA-DR+ lin-/dim cells were identified in freshly isolated lamina propria mononuclear cells by multicolour flow cytometry, from patients with UC (n = 48) and controls (n = 22). The proportion and number of CD11c+ and CD11c- cells within this population were determined. Surface expression of the activation/maturation markers CD40, CD86, Toll-like receptors (TLR), TLR-2, TLR-4, and the natural killer cell marker, CD56 was assessed on each cell population. Morphology was assessed by electron microscopy and T cell stimulatory capacity measured in allogenic mixed leukocyte reactions (MLR).
Results: Lamina propria colonic HLA-DR+ lin-/dim cells, of the CD11c-, but not the CD11c+ subset, were significantly increased in inflamed tissue of patients with UC compared with control tissue (UC 447±94 vs Control 104±17 per mg; p<0.001). Numbers of CD11c- HLA-DR+ lin-/dim cells decreased after resolution of macroscopic inflammation. Nonetheless, CD11c- HLA-DR+ lin-/dim cells were significantly increased in non-inflamed tissue of UC patients compared with colonic tissue from healthy subjects (p<0.05). In UC, these CD11c- cells expressed CD40, CD86, TLR-2 and TLR-4 at lower levels than on their CD11c+ counterparts and were weakly stimulatory in an MLR. Few CD11c- HLA-DR+ lin-/dim colonic cells expressed markers associated with blood CD11c- HLA-DR+ lin-/dim plasmacytoid DC (BDCA2, BDCA4 and high levels of CD123) but a major subset expressed high levels of the Natural Killer (NK) marker CD56.
Conclusion: Intestinal inflammation in UC is associated with the presence of a population of cells that share phenotypic features of both antigen presenting cells and NK cells. This novel population of human colonic cells may function in immune regulation or tissue repair. In addition, their increased presence in quiescent UC may be a marker of subclinical inflammatory activity.
INTESTINAL DENDRITIC CELLS IN ULCERATIVE COLITIS HAVE ALTERED CD103 (α-E) EXPRESSION: IN SUPPORT OF DYSREGULATION IN GUT-HOMING
S. C. Ng1, S. Plamondon1, M. A. Kamm2, S. C. Knight1, A. J. Stagg1. 1Antigen Presentation Research Group, 2Gastroenterology, St Mark’s Hospital, London, UK
Introduction: Attraction of T lymphocytes to sites of inflammation is central to the inflammatory process, and appears to be heavily influenced by specialised gut dendritic cells (DC). Intestinal DC induce expression of gut homing molecules on T cells that they activate. In the mouse, the ability to imprint gut homing is found in a population of intestinal DC that expresses the integrin chain CD103 (α-E).1 Colonic DC from ulcerative colitis (UC) induce higher levels of gut-homing β7 integrin on T cells than do DC from healthy tissue.2 Characterising the expression of CD103 by human intestinal disease in health and inflammatory bowel disease (IBD) is likely to increase our ability to alter inflammatory cell recruitment.
Aims & Methods: Using multicolour flow cytometry, CD103 expression was assessed on lamina propria mononuclear cell populations extracted from colonic tissue in UC patients (n = 13) and controls (n = 17). The proportion and number of CD103+ cells were determined. Level of CD103 expression was measured as an intensity ratio (IR) with reference to isotype-matched control labelling. CD103 expression was compared on myeloid DC (CD11c+ HLA-DR+ lineage-/dim), CD11c- HLA-DR+ lineage-/dim cells and lymphocytes identified.
Results: In controls, lamina propria CD103+ cells comprised a major fraction of myeloid DC population (mean±SEM 37±3%), but were infrequent among the CD11c- HLA-DR+ lineage-/dim (6±3%; p<0.05) and lymphocyte (8±1%) populations. Level of expression of CD103 by myeloid DC (IR = 7.3±1.2) and by lymphocytes (IR = 6.7±2%), was significantly higher than that of CD11c- cells (IR = 3.5±0.7; p<0.05). There was no significant difference in the proportion of DC expressing CD103 in paired samples from the ileum and colon. In UC, proportion of lamina propria myeloid DC and CD11c- HLA-DR+ lineage-/dim cells expressing CD103 (myeloid DC: 22±5%; CD11c- cells: 0±3%) was significantly lower than for equivalent populations from control subjects (p<0.05). The absolute number of colonic CD103+ myeloid DC was significantly lower for UC patients than controls. (UC 22±9 per mg tissue versus control 49±9 per mg tissue; p<0.05). In addition, colonic myeloid DC and CD11c- HLA-DR+ lineage-/dim cells from UC tissue expressed lower levels of CD103 than equivalent cells from control tissue (IR: 4±0.8 vs 7±1.3 myeloid DC, p<0.05; IR: 1±0.2 vs 3.0±0.7 CD11c- HLA-DR+ lineage-/dim cells, p<0.05).
Conclusion: CD103+ myeloid DC are present in the human colon and small intestine. Loss of CD103+ colonic DC in UC may result from effects on recruitment of precursors, local differentiation and/or migration from the tissues. These findings support a role for dysregulated control of gut-homing by DC in IBD.
CROSS-SECTIONAL STUDY ON THE CORRELATION BETWEEN PREOPERATIVE AZATHIOPRINE AND MYENTERIC PLEXITIS IN THE PROXIMAL RESECTION MARGINS AND AFFECTED CROHN’S DISEASE SEGMENT
S. C. Ng1, G. Arslan-Leid1, F. Sandu2, M. A. Kamm1, T. Guenther2, N. Arebi1. 1Gastroenterology, 2Histopathology, St Mark’s Hospital, London, UK
Introduction: Postoperative Crohn’s disease (CD) recurrence rate after ileo-colonic resection is high. Myenteric plexitis (inflamed ganglia and nerve bundles) in the proximal margins of ileo-colonic Crohn’s resection specimens is a potential predictor of early endoscopic recurrence. Whether preoperative immunosuppressive agents reduce the development and severity of myenteric plexitis in CD has not been established.
Aims & Methods: Retrospective single centre study to assess whether preoperative azathioprine (AZA) treatment alter the grade of myenteric plexitis in the proximal resection margins and affected segments of CD. Ileo-colonic resection specimens from 99 patients with CD were histologically scored for the grade of myenteric plexitis (Grade 0 (G0): no inflammatory cells; G1: <4 inflammatory cells; G2: 4 to 9 cells; G3: >10 cells) by two expert histopathologists blinded to the patients’ clinical history. The presence and grade of myenteric plexitis were correlated with AZA therapy for CD at least three months preceding surgery.
Results: Myenteric plexitis was present in 43% (40/94) of patients in the proximal resection margin and 85% (67/79) of patients in the affected segments of CD, in the absence of transmural inflammation. Twelve of 40 patients (30%) with plexitis and 16 of 54 patients (30%; NS) without plexitis in the proximal resection margin were receiving AZA prior to resection. Twenty of 67 patients (30%) with plexitis and 4 of 12 patients (33%; NS) without plexitis in the affected Crohn’s segment were on AZA before resection. There were no significant differences in the severity of myenteric plexitis in the proximal resection margins between the AZA (G1: 58%, G2: 33%, G3: 9%) and non-AZA group (G1: 71%, G2:25%, G3:4%).The severity of plexitis in the affected Crohn’s segment showed no differences between the AZA and non-AZA therapy group. There was also no correlation between the presence of plexitis and smoking history or the number of previous resections.
Conclusion: These preliminary data suggest that AZA before ileo-colonic resection for CD does not alter the presence or severity of myenteric plexitis in the proximal resection margin and affected segments of CD.
PRODUCTION OF IL-10 BY COLONIC DENDRITIC CELLS IS ASSOCIATED WITH HIGHER CONCENTRATIONS OF FAECAL MICROBIOTA IN PATIENTS WITH ACTIVE CROHN’S DISEASE
S. C. Ng1, A. Koutsoumpas2, C. R. Hedin2, N. E. McCarthy1, S. Plamondon1, M. A. Kamm3, S. C. Knight1, A. Forbes4, J. O. Lindsay5, K. Whelan2, A. J. Stagg1. 1Antigen Presentation Research Group, St Mark’s Hospital, 2Nutritional Science Division, King’s College London, 3Gastroenterology, St Mark’s Hospital, 4Centre for Gastroenterology and Nutrition, University College London, 5Clinical Academic Unit of Gastroenterology, Barts and the London NHS Trust, London, UK
Introduction: Intestinal dendritic cells (DC) sample luminal bacteria using pattern recognition receptors (PRR), linking innate and adaptive immune responses to commensal microbiota. In Crohn’s disease, more DC express PRR and produce pathologically relevant cytokines. Exogenously administered bifidobacteria are potent inducers of anti-inflammatory IL-10 production by DC in vitro. However it is unknown whether resident microbiota varies in its immunological effects.
Aims & Methods: We explored the relation between intestinal microbiota and ex vivo DC cytokine production in active Crohn’s disease patients(CDAI 220–450). Ongoing DC cytokine production was analysed by intracellular staining and multi-colour flow cytometry of cells extracted from non-inflamed rectal tissue of CD patients. Myeloid DC were identified as CD11c+ HLA-DR+ lin-/dim cells (lin = anti-CD3, CD14, CD16, CD19, CD34) and staining of permeabilised DC for IL-10,12p40 and IL-6 quantified using WinList software. Intestinal microbiota were analysed by fluorescent in situ hybridisation using oligonucleotide probes targeting 16S rRNA of total bacteria (EUB), bifidobacteria (Bif164), bacteroides (Bac303) and Clostridium coccoides-Eubacterium rectale (EREC482) of fresh faecal samples.
Results: IL-10 positive DC were detected in 7 of 13 patients with Crohn’s disease. Faecal concentrations of total bacteria (10.6±0.2 vs 10.2±0.4 log10/g, p = 0.049), in particular bifidobacteria (10.3±0.2 vs 9.8±0.5 log10/g, p = 0.039) and bacteroides (10.2±0.3 vs 9.6±0.5 log10/g, p = 0.025), were significantly higher in patients with IL-10 positive colonic DC than in those with no detectable IL-10 producing DC, respectively. However, concentrations of C coccoides-E rectale did not differ significantly between patients with and without IL-10 producing DC. There were also no significant differences in concentrations of bacterial strains when comparing IL-6 or IL-12p40 positive DC, with IL-6 and IL-12p40 negative DC, although numbers of patients whose DC were negative for these cytokines was small (2 and 4, respectively).
Conclusion: Increased concentrations of faecal microbiota, in particular bifidobacteria, were associated with the ex vivo production of anti-inflammatory IL-10 by colonic DC, an observation consistent with effects of bifidobacteria on DC in vitro. Although further work is required before a causal link can be established, these data suggest the potential of commensal microbiota to modulate the function of intestinal DC.
CAN BOWEL ULTRASOUND DETERMINE DISEASE ACTIVITY AND EXTENSION IN PATIENTS WITH ULCERATIVE COLITIS SUFFERING FROM RECURRENCE OF INTESTINAL SYMPTOMS? AN ENDOSCOPIC-CONTROLLED STUDY
F. R. Parente1, S. Greco2, S. Ardizzone2, B. Marino1, G. Bianchi Porro2, R. Moretti3. 1Gastrointestinal Unit, A.Manzoni Hospital, Lecco, 2Gastrointestinal Unit, L Sacco University Hospital, Milan, 3Section of Epidemiology, Community Health Care Centre, Lecco, Italy
Introduction: Whether or not patients with already known ulcerative coliti (UC) whenever suffer from recurrence of intestinal symptoms should necessarily undergo control colonoscopy is still a matter of debate.
Aims & Methods: Aim of this study was to evaluate the usefulness of bowel ultrasound (US) as surrogate of colonoscopy in evaluating disease activity and extension of colonic involvement in a consecutive series of UC patients with relapse of intestinal symptoms by comparing clinical, endoscopic and US parameters. 86 consecutive patients with already known UC admitted to our Centres for recurrence of intestinal symptoms were recruited. All patients underwent baseline colonoscopy and bowel US before starting any new therapy. Endoscopic severity of UC was graded 0–3 according to Baron score for the various colonic segments (rectum, sigmoid, descending, transverse and ascending colon); US severity was graded according to the maximum colonic wall thickening of the same various colonic tracts; clinical activity was graded 0–3 according to Truelove score. Accuracy, sensitivity, specificity, positive and negative predictive value of bowel US in determining severity of UC were calculated according to segment-by-segment analysis considering endoscopy as the reference test. Receiver operating characteristic (ROC) curve was also constructed taking into account colonic wall thickness for selecting UC patients with moderate to severe endoscopic relapse (Baron grade 2–3) from those with slight or no activity at colonoscopy (Baron grade 0–1).
Results: Considering endoscopy as the reference test for UC activity, segment-by-segment analysis revealed an high accuracy of bowel US in determining disease relapse: 93%, 90%, 93%, 89% accuracy for the sigmoid, descending, transverse and ascending colon, respectively. By contrast, accuracy of US was very low for the detection of rectal recurrence (41.8%) due to the well known difficulty of US in exploring the deep pelvis. ROC curve identified a colonic wall thickness >5 mm as directly associated with the risk of having moderate to severe endoscopic UC flare-up (hazard ratio 9.05; CI 95% 8.16 to 39.1). This colonic wall thickness threshold was also significantly correlated with the clinical activity (χ2 26.7, p<0.001).
Conclusion: In expert hands, bowel US is an highly accurate tool in diagnosing UC relapse as well as in determining the extension of colonic involvement; it may be therefore proposed as a non-invasive alternative to colonoscopy in order to evaluate objectively disease activity in UC patients whenever they refer recrudescence of intestinal symptoms.
NEUTROPHIL EXTRACELLULAR TRAP FORMATION APPEARS RELATED TO INOS BUT NOT MAST CELL ACTIVATION IN INFLAMMATORY BOWEL DISEASE
G. C. Parkes1, N. B. Rayment1, B. N. Hudspith1, J. Brostoff1, K. Whelan1, J. D. Sanderson1, L. Petrovska1. 1Nutritional Sciences Division, King’s College London, London, UK
Introduction: Neutrophils play a key role in killing bacteria at the early stages of infection. Recently it has been shown that contact with microbes activates neutrophils and induces formation of neutrophil extracellular traps (NETs) which are involved in entrapment of bacteria and prevention of bacterial spread, and neutralisation of the virulence factors. We have previously demonstrated the presence of NETs in the lumen and lamina propria of a Citrobacter rodentium murine model of colitis and in patients with active inflammatory bowel disease (IBD).
Aims & Methods: To establish whether NET formation correlated to markers of neutrophil activation in human subjects with normal and inflamed colonic mucosa. To establish whether mucosa-associated bacteria were associated with luminal NET formation. Colonic and ileal biopsies were taken from 10 healthy controls and 20 inflamed and 10 uninflamed regions in patients with ulcerative colitis (UC) and Crohn’s disease (CD) and snap frozen in liquid nitrogen. 6 μm sections were cut and fixed in acetone. NETs were identified using immunofluorescence staining for myeloperoxidase and DAPI. In addition, in several samples we used fluorescent in situ hybridisation (FISH) for Eubacteria to co-localise bacteria with the NETs. Separate sections were stained for tryptase and inducible nitric oxide synthase (iNOS) using an indirect peroxidase technique. Mast cells were counted in 5 consecutive high powered fields and iNOS activity was scored between 0–4 (no activity-high activity).
Results: Inflammation was associated with the formation of NETs which were present in 95% of actively inflamed sites and interestingly 60% of ‘uninflamed’ CD but not in uninflamed UC and in only one control. The presence of NETs strongly correlated with the increased iNOS staining (2.29 vs 1.49 p<0.005). However there was no correlation between the presence of NETs and numbers of mast cells (17.1 vs 16.5 cells per high powered field p<0.77). Using FISH mucosa-associated bacteria were co-localised with NETs.
Conclusion: In our study colonic NET formation correlates with mucosal iNOS production, a known activator of neutrophils. We have also co-localised mucosa-associated bacteria with NETs. Given recent studies suggesting impairment in the innate immune system in CD, further studies are required to examine initiation and function of NETs in CD.
THE COST EFFECTIVENESS OF SCHEDULED MAINTENANCE TREATMENT WITH INFLIXIMAB AMONG PATIENTS WITH CROHN’S DISEASE
J. Lindsay1, Y. Punekar2, B. Abhyankar3, G. Chung-Faye4. 1Gastroenterology Clinical Academic Unit, The Royal London Hospital, London, 2Health Technology Assessment, 3Medical Affairs, Schering-Plough Ltd, Welwyn Garden City, 4Gastroenterology, King’s College Hospital, London, UK
Introduction: The introduction of biological therapies such as infliximab has revolutionised Crohn’s disease (CD) management by inducing remission in previously therapy refractory patients and potentially reducing the need for surgery and hospitalisation. The objective of this study was to estimate the cost effectiveness of scheduled maintenance treatment with infliximab among adult patients suffering from moderate to severe active CD.
Aims & Methods: A Markov model was constructed to simulate the progression of a hypothetical cohort of CD patients through predefined health states on scheduled maintenance treatment with infliximab (5 mg/kg) based on results from the Targan and ACCENT I trials. The health states used in the model were remission, therapy (infliximab) responsive active disease, non-responsive active disease, surgery, post-surgery remission and post surgery complications. Standard care, comprising immunomodulators and/or corticosteroids was used as a comparator. The primary outcome was quality adjusted life years (QALYs) estimated using EQ-5D from a European CD population. An average patient weight of 60 kg was used to estimate the dose of infliximab. The costs and the outcomes were discounted at 3.5% over a period of 5 years. Stochastic sensitivity analyses were performed by varying the infliximab efficacy estimates, costs and utilities.
Results: The incremental cost effectiveness ratio (ICER) for scheduled maintenance treatment with infliximab was £25,903 in severe active CD patients. The one-way sensitivity analyses revealed patient weight and hence the total dose of infliximab to be the most influential parameter with ICERs ranging from £24,588–£38,623.
Conclusion: Scheduled maintenance treatment with infliximab (5 mg/kg) is a cost effective treatment option for adult patients suffering from severe active CD under an 8-week scheduled maintenance programme.
ATTENUATED TNF-α RELEASE FOLLOWING TLR STIMULATION OF MACROPHAGES IN CROHN’S DISEASE
F. Z. Rahman1, A. Smith1, S. L. Bloom2, A. W. Segal1. 1Department of Medicine, University College London, 2Department of Gastroenterology, UCL Hospitals Foundation NHS Trust, London, UK
Introduction: Although the aetiology of Crohn’s disease (CD) remains an enigma, strong evidence suggests that microbial components are involved in the pathogenesis. Recent work provides compelling evidence of a failure of acute inflammation in CD and suggests that the primary defect operates at the level of the macrophage.1 Macrophages play a major role in the induction of inflammatory responses to microbes via Toll-like receptors (TLRs), producing a variety of pro-inflammatory chemokines and cytokines. Tumour necrosis factor-α (TNF) is a pivotal pro-inflammatory cytokine and a major target of biologic therapy. Elevated TNF levels have been well described during the chronic inflammatory phase of CD, but little is known about levels during the preceding acute inflammatory response in these patients.
Aims & Methods: To assess whether the TLR2/4 response is defective in CD, TNF release by peripheral blood-derived macrophages was measured following challenge with the bacterial ligands Pam3Cys (TLR2) and LPS (TLR4). The macrophage response of 100 patients with quiescent CD, 57 healthy controls (HC) and 51 patients with quiescent ulcerative colitis (UC) were compared. Patients were on either no medication or a 5-ASA alone.
Results: TNF release by CD macrophages was significantly reduced following TLR2/4 stimulation and varied depending on disease location, being most attenuated in CD patients with colonic involvement. This phenomenon was independent of age, gender, smoking status, treatment and CARD15 genotype, and was not observed in UC.
Conclusion: TNF release following TLR2/4 stimulation of macrophages is significantly attenuated in CD. While colonic involvement in CD is strongly associated with a diminished TLR2/4 response, this defect is not apparent in UC. This finding seems counterintuitive given the success of anti-TNF therapy in CD, but supports the evolving theory that a defective acute inflammatory response precedes the granuloma formation and T cell-driven chronic inflammation characteristic of CD. Defining the precise molecular defects responsible for a lethargic acute inflammatory response in CD may thus offer novel therapeutic targets in the future.
CYTOKINE PROFILES FROM E COLI LADEN MACROPHAGES IN INFLAMMATORY BOWEL DISEASE
N. B. Rayment, A. Chairakaki, B. Hudspith, L. Petrovska, G. C. Parkes, J. Brostoff, J. Sanderson. Nutritional Sciences Division, Kings College London, London, UK
Introduction: Colonic macrophages are important contributors to the maintenance of gut homeostasis. We and others have previously reported the presence of E coli, but not other commensal bacteria, in the lamina propria of patients with active IBD. Further studies have shown that these E coli are co-localised to lamina propria macrophages however the significance of these findings remains uncertain.
Aims & Methods: To investigate the cytokine profile of macrophages laden with E coli compared to those free of bacteria. Snap frozen rectal biopsies were taken at routine colonoscopy from patients with ulcerative colitis (UC, n = 35), Crohn’s (CD, n = 6), and controls with normal colorectal mucosa (n = 25). Using a specific 16s rDNA probe, fluorescent in situ hybridisation (FISH) was used to identify intracellular E coli within CD 68+ve macrophages of cryosectioned material. Co-expression of both pro- and anti-inflammatory cytokines, chemokines and activation markers were then investigated histochemically in the E coli+ve as well as the E coli−ve macrophage populations of the different patient groups.
Results: An overall up-regulation of both chemokine and proinflammatory cytokines was observed in those macrophages positive for E coli. Enhanced TNFα, IL-15, IL-23, IL-8 and MCP-3 appeared to correlate well with FISH +ve macrophages although the expression of IL-6 in these cells was less well defined. Macrophages seen to be E coli−ve in the IBD cohort as well as those from the control group showed minimal expression of these cytokines.
Conclusion: Enhanced expression of pro-inflammatory cytokines in bacteria laden macrophages suggest that these cells are contributing to chronic inflammation in IBD. It remains uncertain whether the survival of E coli within macrophages in IBD is a property of the E coli, a defect in innate immunity or both.
MARKED AND CONTRASTING EFFECTS OF DIETARY SOLUBLE FIBRES AND PERMITTED FOOD EMULSIFIER ON TRANSLOCATION OF CROHN’S DISEASE E COLI ISOLATES ACROSS INTESTINAL M CELLS AND CACO-2 MONOLAYERS
C. L. Roberts, B. J. Campbell, J. M. Rhodes. Division of Gastroenterology, University of Liverpool, Liverpool, UK
Introduction: Crohn’s disease (CD) is common in westernised countries where low levels of soluble fibre are eaten and where the use of emulsifiers in food is common. The primary lesions in CD are thought to occur particularly at Peyer’s patches and colonic lymphoid follicles where bacterial invasion through specialised M cells occurs.1 We have examined the translocation across both M cells and Caco-2 monolayers of a variety of CD E coli isolates in the presence of varying concentrations of four soluble fibre (non-starch polysaccharide) preparations: plantain, leek, apple and broccoli. Plantain fibre has previously shown to inhibit adherence of CD E coli isolates to intestinal epithelial cells.2 In addition, we have investigated E coli translocation across M cells in the presence of varying concentrations of the permitted food emulsifier, Polysorbate 80.
Aims & Methods: M-like cells were generated in vitro by co-culture on Transwell filters of colon epithelial Caco-2 cells (grown on the apical aspect) with Raji B cells (on the basolateral aspect). M cell transformation was confirmed by electron microscopy. E coli translocation across cell monolayers in the presence of soluble fibre or emulsifiers was assessed by overnight culture on agar. TER (ohm/cm2) was monitored throughout to assess monolayer integrity.
Results: M cells showed 21-fold increase in CD E coli translocation compared to Caco-2 monocultures (P<0.01 ANOVA). Soluble plantain fibre markedly reduced E coli HM605 translocation across M cells in a dose-dependent manner, at 5 mg/ml (82.7±7.2% reduction, n = 5; p<0.05) and 50 mg/ml (86.2±12.9%, n = 6; p<0.005), as did incubation with soluble broccoli fibre at 0.5 mg/ml (49.4±13.5%, n = 6; p<0.005), 5 mg/ml (62.5±7.3%, n = 6; p = 0.0002) and 50 mg/ml (68.7±5.7%, n = 6; p<0.0001); data was comparable for all CD E coli investigated (HM615, HM605, HM580, LF82). Apple and leek fibre had little effect upon bacterial translocation. EM confirmed E coli within M cells. Polysorbate-80, at low concentration (0.01% vol/vol), equivalent to 1% persistence into the distal ileum of ingested polsorbate, caused 54-fold increased E coli translocation through Caco-2 monolayers (n = 3; p<0.01), but not M-cells, with no reduction in TER.
Conclusion: Both soluble plantain and broccoli fibre inhibit E coli translocation through both M cells and colonic epithelial cells. The permitted food emulsifier, Polysorbate 80, increases translocation across colonic epithelial cells, but not M cells. Effects occur at low concentrations likely to be relevant in vivo and may contribute to the impact of dietary changes on Crohn’s disease pathogenesis.
THE IMPACT OF ULCERATIVE COLITIS ON PATIENTS’ LIVES COMPARED WITH OTHER CHRONIC DISEASES: A SURVEY OF PATIENTS’ OPINIONS
D. T. Rubin1, M. C. Dubinsky2, R. Panaccione3, C. A. Siegel4, D. G. Binion5, S. V. Kane6, E. V. Loftus6, J. Hopper7, R. Karlstadt8. 1Section of Gastroenterology, Department of Medicine, University of Chicago Medical Center, Chicago, 2Pediatric IBD Center, Cedars-Sinai Medical Center, Los Angeles, USA, 3Division of Gastroenterology, University of Calgary, Calgary, Canada, 4Section of Gastroenterology and Hepatology, Dartmouth-Hitchcock Medical Center, Lebanon, 5Division of Gastroenterology and Hepatology, Medical College of Wisconsin, Milwaukee, 6IBD Clinic, Mayo Clinic, Rochester, 7Richard Day Research, Evanston, 8Shire Phamaceuticals Inc, Wayne, USA
Introduction: This study, conducted in the USA, was designed to gain an understanding of how patients with ulcerative colitis (UC) perceive that their disease affects their lives, and to directly compare this with other chronic diseases.
Aims & Methods: This internet-based survey was conducted in patients with UC, rheumatoid arthritis (RA), asthma or migraine. Differences in response rates between patient populations were considered significant if p<0.05.
Results: In total, 451 patients with UC (23% mild, 60% moderate, 16% severe (patient self-assessment)), 309 with RA, 305 with asthma and 305 with migraine responded to the survey. On average, patients with UC experienced eight (self-defined) flare-ups in the previous 12 months. The majority of patients with UC (81%) believed the number of flare-ups they experienced was “normal”, significantly more than patients with migraine (64%) or asthma (75%). Almost three quarters of patients with UC considered that not feeling well had become normal (73%) and almost two thirds found that it was difficult to lead a normal life (62%). Significantly fewer patients with asthma (43 and 33%) or migraine (64 and 59%, respectively) reported these feelings. Significantly more patients with UC felt that their condition was controlling their lives (53%) than patients with RA (44%), asthma (19%) or migraine (37%). Patients with UC were also significantly more likely to: feel anxious about the long term effects of their condition (84%); consider that it was making life more stressful (82%); and feel depressed (62%) and embarrassed (70%) than patients with the other chronic conditions.
Conclusion: These data demonstrate that, in the USA, UC has a substantial negative effect upon the lives of sufferers. Indeed, the impact of UC is often more severe and causes more limitation than other chronic diseases. In particular, patients with UC experience a much higher psychological burden of their disease than patients with the other chronic conditions.
COMPARABLE PHARMACOKINETICS OF TWO MODIFIED RELEASE FORMULATIONS OF ORAL MESALAZINE
W. J. Sandborn1, G. Balan2, B. Kuzmak3, S. B. Hanauer4. 1Division of Gastroenterology, Hepatology and Internal Medicine, Mayo Clinic, Rochester, 2Pharmacokinetics, 3Biostatistics, Procter and Gamble Pharmaceuticals, Cincinnati, 4Section of Gastroenterology and Nutrition, University of Chicago, Chicago, USA
Introduction: Both Asacol and Mezavant are modified release mesalazine preparations for topical action in the colon with a pH dependent coating that controls mesalazine release at pH⩾7. Mezavant also contains lipophilic and hydrophilic excipients. Asacol is licensed for divided dosing in the UK, historically 3 × day (TDS), and Mezavant is licensed for once daily (OD) for mildly to moderately active UC. The purpose of this study is to evaluate the pharmacokinetic (PK) parameters from 2.4 g/d of oral mesalazine administered as Mezavant OD, Asacol OD, and Asacol TDS.
Aims & Methods: 37 healthy volunteers completed a randomised, open-label, parallel group, steady state PK study. All doses were taken within 30 min of a meal/snack and subjects were dosed for 7 consecutive days. Plasma samples were obtained once daily up to day 7 and for 48 h after the first dose on day 7. Urine was collected over 8 h intervals for 24 h after the first dose on day 7. Plasma and urine samples were analysed for 5-ASA and N-Ac-5-ASA using a validated LC/MS assay. PK parameters were calculated using non-compartmental methods.
Results: 5-ASA plasma PK parameters and profile of all 3 treatment arms are shown in the table and figure. The plasma PK parameters for 5-ASA and N-Ac-5-ASA were comparable across all treatment arms. The total (5-ASA and N-Ac-5-ASA) urinary excretion was 18%, 17.7% and 15.2% for Mezavant OD, Asacol OD, and Asacol TDS, respectively.

Conclusion: Overall, Asacol and Mezavant dosed OD exhibited a similar PK profile in healthy volunteers. These results suggest no apparent differences in the release profile of Mezavant or Asacol given OD. In addition, although not statistically significant, the Asacol TDS arm shows less fluctuation relative to the Mezavant OD arm (p = 0.56). The clinical significance is unknown.
PREDICTING OUTCOME IN FIRST PRESENTATION OF FULMINANT INFLAMMATORY COLITIS
A. M. Sawyer, H. Lewis. Department of Gastroenterology, Whipps Cross University Hospital, London, UK
Introduction: Previous studies have provided excellent evidence to aid clinical decision making in patients with severe relapse of ulcerative colitis whose response to intravenous steroid therapy is poor and where other medical therapy or colectomy is required. Such evidence is less well developed for the first presentation of severe colitis. The clinical management of these patients presents additional challenges.
Aims & Methods: The aim of this study was to determine which initial factors best predict failure of intravenous steroid therapy in patients presenting with inflammatory colitis for the first time, with disease so severe that first contact with medical services was emergency admission to hospital. Records of 23 patients presenting to this institution as emergency admissions with first episodes of inflammatory colitis (ulcerative colitis or Crohn’s disease) between 1997 and 2007 were assessed retrospectively. All cases satisfied criteria for fulminant colitis. Cases of all forms of infective colitis were excluded.
Results: Of the 23 patients, 19 were female. Eight patients had colonic dilatation. Eighteen patients had ulcerative colitis and 5 had Crohn’s colitis. All had pan-colitis or extensive colitis. Two patients died. All patients with UC where initial medical therapy failed and who did not have toxic megacolon, chose colectomy rather than further medical treatment. Twelve of the 23 (52%) patients had colectomy during the first admission. A further 3 patients required colectomy during subsequent admission. CRP on admission was significantly higher in those failing initial medical treatment. All patients with an initial CRP >200 mg/l had colectomy. None of the other selected factors was predictive of outcome.
Conclusion: CRP level on admission helps predict outcome of initial steroid therapy and may aid clinical decision making in these patients with a first presentation of fulminant inflammatory colitis.
THE IMPACT OF INTRODUCING THIOGUANINE NUCLEOTIDE MONITORING INTO CLINICAL PRACTICE
M. A. Smith1, T. Marinaki2, M. Arenas2, E. Escuredo2, J. Sanderson1. 1Gastroenterology, 2Purine Research Laboratory, Guy’s and St Thomas’ NHS Foundation Trust, London, UK
Introduction: Azathioprine (AZA) and 6-mercaptopurine (6MP) are the immunomodulators of choice for inflammatory bowel disease (IBD). There are two main problems with these therapies: lack of response and toxicity. These problems conflict, making dosage decisions difficult, especially as the complex metabolism of thiopurines is subject to inter-individual variation such that even patients on the recommended dose are at risk of either non-response or toxicity. Therapeutic monitoring with thioguanine nucleotides (TGNs), the active metabolic end-product of AZA and 6MP, predicts both response to treatment and toxicity. TGN levels can be used to detect non-adherence, under- and over-dosing, as well as treatment resistance. However their true benefit in clinical practice remains unproven.
Aims & Methods: To assess the impact of a new TGN service at Guy’s and St Thomas’ Hospitals on clinical practice. All IBD patients on AZA or 6MP who had TGNs measured were identified and their clinical records and laboratory results reviewed. In particular we were interested in finding incidences where the TGN result had resulted in a change in management.
Results: 50 patients have had their TGN levels measured to date. 6 (12%) were non-adherent, of whom only 1 was in remission. A further 10 (20%) were potentially under-dosed with an opportunity for dose escalation, particularly 3 non-responders. Two patients had extremely high TGN levels (>1000 pmol/8x108RBC). One admitted to doubling her own dose, the other had a low, decreasing WBC which had not been addressed. 7 patients with high TGNs were lymphopaenic and 3 were leucopaenic. In 25% of those with therapeutic TGN and 20% with high TGN MCV and lymphocyte count remained normal. TGN measurement led to a documented change in treatment in 13 patients (26%) (6 non-adherent, 3 under-dosed non-responders, 3 high TGN low WBC, 1 dose-doubler). At £30 per test this equates to £120 per treatment change.
Conclusion: TGNs appear useful in clinical practice, identifying non-adherence and under-dosing and probably preventing toxicity. MCV, WBC and lymphocyte count do not reflect TGN level in all patients. This preliminary analysis suggests that TGNs are good value for money. A more formal economic analysis is warranted.
SEEKING PHARMACOGENETIC LOCI WHICH EXPLAIN NON-THIOPURINE METHYLTRANSFERASE RELATED SIDE EFFECTS IN PATIENTS TAKING AZATHIOPRINE FOR INFLAMMATORY BOWEL DISEASE
M. A. Smith1, T. Marinaki2, A. Ansari1, J. Sanderson1. 1Gastroenterology, 2Purine Research Laboratory, Guy’s and St Thomas’ NHS Foundation Trust, London, UK
Introduction: The thiopurine drugs azathioprine (AZA) and 6-mercaptopurine (6MP) remain the immunosuppressants of choice for inflammatory bowel disease (IBD). Both are pro-drugs which are enzymatically converted to active metabolites (thioguanine nucleotides, TGNs). This production process competes with two enzymes which inactivate thiopurines: firstly, thiopurine methyltransferase (TPMT) which is a well-established predictor of side effects and inefficacy with thiopurine therapies and secondly, xanthine oxidase/dehydrogenase (XDH) which breaks down thiopurines to uric acid. Whilst total deficiency of XDH is rare, variation in activity between individuals is considerable and co-administration of an XDH-inhibitor (allopurinol) causes high TGN levels and toxicity. While there are numerous reported SNPs in the XDH gene, assessment of their clinical impact is lacking. Molybdenum cofactor is required for the activity of XDH. This cofactor is activated by the enzyme molybdenum cofactor sulfurase (MOCOS) which is also subject to genetic polymorphism the functional impact of which is unknown.
Aims & Methods: To search for an association between documented genetic polymorphism in XDH and MOCOS and outcome on thiopurine therapy. A cohort of 182 prospectively recruited patients starting 2 mg/kg azathioprine for IBD was divided into responders, non-responders and those discontinuing treatment due to side effects. The cohort was genotyped for six non-synonymous coding SNPs for XDH and five for MOCOS using real-time PCR Taqman genotyping assays. Contingency tables and χ2 statistics were used to compare the frequency of these genes in the different outcome groups.
Results: 58% of patients recruited had Crohn’s, (mean age 40.3 years, 54% female). 74 (41%) withdrew due to side effects, 66 (36%) completely responded, 42 (23%) had partial or no response. One XDH SNP (837C>T, allele frequency 0.02) protects against side effects on thiopurine treatment as a dominant effect (p = 0.046). One MOCOS SNP (2107A>C, allele frequency 0.34) also appeared to be protective but this just fails to reach significance (p = 0.078), again this was a dominant effect. Patients with both of these SNPs (n = 7) did not experience any side effects (p = 0.039). There was no relationship seen between any of the SNPs tested and clinical response.
Conclusion: This study supports the premise that pharmacogenetic targets other than TPMT impact on thiopurine metabolism, although the effects are small by comparison. The XDH SNP 837C>T warrants further evaluation. At present it is not known whether this SNP is associated with decreased XDH activity, but if it does, our findings suggest that thiopurine metabolites produced by XDH may be toxic.
EFFICACY AND SAFETY OF INFLIXIMAB THERAPY IN A LARGE SINGLE CENTRE UK POPULATION: THE LEEDS IMMUNE MEDIATED INFLAMMATORY DISEASE CENTRE EXPERIENCE
M. Sprakes, C. Donnellan, L. Warren, D. Greer, J. Hamlin. Gastroenterology, Leeds General Infirmary, Leeds, UK
Introduction: The efficacy for infliximab (IFX) for the treatment of Crohn’s disease has been well documented.1 However, despite evidence that scheduled (8 weekly) therapy is superior to episodic infusions2 this mode of therapy is currently not recommended by NICE. In 2005 Leeds Immune Mediated Inflammatory Disease (IMID) centre was established for the delivery of biological therapies for patients with IBD or TNF mediated rheumatological diseases.
Aims & Methods: To retrospectively (pre-2005) and prospectively (post 2005) study the use of IFX therapy for IBD in our centre. In 2005 retrospective case note reviews were performed on our cohort treated with IFX. As a result a prospective database was established recording patient demographics, disease type, pre and post therapy HBI (at each visit), concomitant use of steroids and immunomodulators, body weight, adverse events and reasons for discontinuation of therapy.
Results: 143 patients (88f/55m), mean age 37, (range 17–90 years) received a total number of 1202 infusions, mean 8.4/patient (range 1–35). Mean treatment duration was 29 months (range 1–84). 94 patients had 3 dose induction therapy, 49 had single dose induction then episodic therapy with 43 moved to 8 weekly scheduled therapy to improve response. Ultimately 112 received 8 weekly scheduled treatments and 6 remained episodic. Others had 6 weekly due to losing response or 12 weekly infusions. 9 patients had primary non-response (defined as discontinuing therapy for treatment failure after 1–3 doses). The remaining 134 patients had a subjective clinical response. Where pre- and post-IFX HBI data were available (65 patients) the mean HBI prior to therapy was 9 indicating severe disease. Of these, 29 (45%) achieved remission (HBI<5) 14 patients had ileostomy. Steroid sparing was achieved in 34 patients (72%) of which 30 (64%) completely discontinued them. Average weight gain was 2 kg (range −9 kg−16 kg). 20 patients had infusion reactions but only 7 (5% of total cohort) required discontinuation of therapy. A total of 39 (27%) patients discontinued therapy for the following reasons: loss of response 12 (31%), primary non-response 9 (23%), infusion reaction 7, patient choice 6, bridge to azathioprine 1, moved Trust 1. Of those failing therapy 11 (28%) had surgery, 2 received alternative anti TNF therapy and 1 leucocytapheresis.
Conclusion: IFX therapy is a safe, well tolerated and effective treatment for IBD as monitored in a large single centre UK population. Response and remission rates are in keeping with those reported in clinical trials.
SERUM PROTEIN FINGERPRINTS CAN ACCURATELY DISTINGUISH PATIENTS WITH INFLAMMATORY BOWEL DISEASE FROM PATIENTS WITH CLINICALLY RELEVANT DIFFERENTIAL DIAGNOSIS
V. Subramanian1, D. Subramanian2, S. Krishna3, M. Farthing4, R. Pollok1. 1Department of Gastroenterology, St George’s Hospital, London, UK, 2Department of Computer Science, Rice University, Houston, USA, 3Cellular and Molecular Medicine, 4Department of Gastroenterology, St George’s University, London, London, UK
Introduction: Inflammatory bowel disease (IBD) is an idiopathic chronic disease of the gastrointestinal tract with many significant debilitating sequelae some of which be life threatening. Invasive tests are necessary to confirm or rule out a diagnosis of IBD. Non-invasive serological testing using ASCA and p-ANCA are currently not sufficiently specific or sensitive for routine diagnostic use.
Aims & Methods: To develop serum protein fingerprints using SELDI-ToF mass spectrometry to distinguish patients with IBD from clinically relevant controls. Serum samples were collected from patients with IBD, Colorectal cancer (CRC), diverticular disease (DD), irritable bowel syndrome (IBS) and Clostridium difficile associated diarrhoea and stored at −80°C. Samples were applied to CM10 (a weak cation-exchange) protein chip arrays and mass spectra generated using a PBS-II mass spectrometer. The mass spectrometry data were extracted and preprocessed prior to analysis, which included spectral calibration, signal interpolation to impose a common time scale across spectra; spectral denoising, baseline correction and normalisation; peak detection; and peak quantification. These spectra were analysed using support vector machine (SVM) analysis utilising recursive feature elimination techniques with radial basis function and fivefold cross validation.
Results: 248 serum samples were processed of which 110 had IBD (Crohn’s disease 48 and ulcerative colitis 62). The classifier developed based on 15 peaks selected by soft-margin SVM (C = 10) using recursive feature elimination and radial basis kernel function (kernel width = 0.001) provided an overall accuracy of 79%, sensitivity of 79%, specificity of 79% and area under the receiver operative curve of 0.81. The top 15 peaks had a mass over charge ratio (m/z) of 3165, 3198, 3378, 3450, 3823, 4161, 4604, 4654, 5465, 7780, 9203, 9302, 9361, 9413 and 13776. The peak with an m/z of 3165 was identified by immunodepletion to be a fragment of inter alpha trypsin inhibitor 4, m/z of 7780 as platelet factor 4 and m/z of 13776 as transthyretin.
Conclusion: Protein fingerprints using SELDI-ToF mass spectrometry can distinguish patients with IBD from patients with clinically relevant differential diagnosis with reasonable accuracy. Further characterisation of these markers will lead to more efficient ways to diagnose and screen for IBD.
PRESENCE OF ANTI-SACCHAROMYCES CEREVISIAE ANTIBODY IN CLOSTRIDIUM DIFFICILE-ASSOCIATED DIARRHOEA IS SIMILAR TO THAT IN CROHN’S DISEASE
V. Subramanian, R. Pollok. Department of Gastroenterology, St George’s Hospital, London, UK
Introduction: Anti-saccharomyces cerevisiae antibodies (ASCA) are developed against baker’s yeast S cerevisiae. ASCA is found in 50 to 70% of patients with CD and only 6 to 14% of patients with ulcerative colitis. ASCA is thought to be highly specific for CD because it is rarely expressed by individuals who do not have IBD except for first-degree relatives of patients with CD. ASCA has been advocated as a diagnostic or a screening test for CD.
Aims & Methods: Serum was prospectively collected from 72 patients with CD and 74 controls (17 with Clostridium difficile-associated diarrhoea (CDAD), 24 with colorectal cancer and 33 with irritable bowel syndrome) and stored at −80°C. Sera were analysed for ASCA expression in a blinded manner using a fixed IgG and IgA ELISA assay, Aeskulisa (Aesku Lab, Wendelsheim, Germany) in an automated multitest, multibatch immunoassay analyzer-Triturus (Grifols, UK).
Results: There was no difference in ASCA seropositivity between CDAD and CD for either IgA or IgG antibody being positive (p = 0.8), but CD patients were significantly more likely (p = 0.05) to have both IgA and IgG antibodies positive.
Conclusion: ASCA is not suitable to distinguish patients with CDAD from CD unless both IgA and IgG ASCA are positive, which considerably reduces the sensitivity of this test. This may reflect a non-specific antibody response to altered intestinal barrier function. ASCA needs to be checked in other infectious and non-infectious inflammatory bowel pathologies before it can be advocated as a diagnostic or screening test for CD.
INFLIXIMAB AS A TREATMENT FOR ULCERATIVE COLITIS: 3½ YEARS’ EXPERIENCE IN A DISTRICT GENERAL HOSPITAL
K. M. Taylor, A. W. Harris. Gastroenterology, Kent and Sussex Hospital, Tunbridge Wells, UK
Introduction: Ulcerative colitis (UC) is a chronic relapsing and remitting inflammatory disease characterised by colonic mucosal ulceration. Current medical therapy involves mesalazines, thiopurine analogues and steroids. Infliximab (IFX), a chimeric monoclonal antibody against tumour necrosis factor α, is an established treatment for Crohn’s disease but its efficacy in UC is less clear. We report our experience with IFX in patients with moderate and acute severe UC since May 2005.
Aims & Methods: Retrospective analysis of case notes of all patients treated with IFX for biopsy-proven UC according to the ACT protocol.1 Patient details: All patients treated with infliximab had moderate (14) or acute severe (2) UC. Prior treatment with thiopurines, mesalazines and steroids (and in 2 cases, iv ciclosporin) had failed to induce remission, or was stopped because of adverse reactions or intolerable side effects. All patients underwent a flexible sigmoidoscopy following induction treatment to assess mucosal healing before starting maintenance therapy.
Results: 16 patients received IFX (8M; age 18–69 years). 15 patients completed induction phase (1 went for emergency colectomy after second dose of IFX). 3 patients failed to respond to induction treatment (persisting symptoms and active disease at endoscopy; underwent surgery). Of the remaining 12 patients, 11 remain in clinical and endoscopic remission and receive 8 weekly infusions of IFX (duration of treatment 6–40 months). All 5 patients who failed treatment (1 patient after 40 months treatment) underwent colectomy. Two patients required an increase in dose of IFX to 10 mg/kg after clinical relapse before returning to standard maintenance therapy; 1 of these relapsed again and had colectomy. None of the patients stopped treatment due to side effects or adverse events.
Conclusion: Our findings support the use of IFX in selected patients with moderate or acute severe UC in a DGH with 12 of 16 patients demonstrating clinical and endoscopic response for up to 40 months.
CHANGES IN THE MUCOSALLY ADHERENT MICROBIAL COMMUNITY IN ULCERATIVE COLITIS
J. M. Thomson1, P. Louis2, G. L. Hold1, N. G. Mowat1, H. J. Flint2, E. M. El-Omar1. 1Gastroenterology Group, Institute of Medical Sciences, Univeristy of Aberdeen, 2Microbial Ecology Group, Rowett Research Institute, Aberdeen, UK
Introduction: Ulcerative colitis (UC) is a common disorder that can be complex and challenging to manage. Several non-mutually exclusive pathogenic mechanisms have been proposed, and the prominent role of the colonic microbiota is well established in animal models. However the role of the mucosally adherent microbial community in the human colon remains elusive.
Aims & Methods: Six patients with an acute flare up of left sided ulcerative colitis and three “normal controls” were recruited into the study. Each of the colitis patients had mucosal pinch biopsies taken from inflamed and non-inflamed mucosa at colonoscopy, and three had repeat samples taken from the same sites after a period of 6–9 months when their symptoms had resolved and the mucosa appeared macroscopically and microscopically normal. The three “normal controls” were asymptomatic with macroscopic and microscopically normal colons and had mucosal pinch biopsies taken from the left colon. The microbial diversity of the 18 samples was assessed using culture independent molecular techniques to identify the microbial community via sequencing of the hyper-variable region of the 16S rRNA gene present in all bacteria. Sequence analysis used the Bio-Linux software.
Results: As expected there was wide inter-individual variation between the subjects. The microbial communities in all the colitis samples, were very different from the “normal control” subjects (p<0.001). Overall, there was a reduction in the dominance of Bacteroides species in the colitis samples compared to the controls (44% vs 63%, p<0.001) regardless of mucosal state or disease activity. There was no significant difference in the proportion of Bacteroides species on the basis of mucosal site or disease severity. The proportion of clostridial cluster IV species was increased during active disease in both the inflamed (23.8%) and non-inflamed (26.8%) mucosa. This proportion significantly reduced to 13.6% when the inflammation resolved (p<0.001) but was still significantly greater (p<0.01) than in the normal control subjects (6.4%). The opposite changes were seen in clostridial cluster XIVa species with a decreased proportion during active disease in both the inflamed (12.5%) and non-inflamed (13.0%) mucosa, which increased to 15.8% with resolution of the inflammation.
Conclusion: The microbial community at the mucosal surface is significantly different in patients with UC, during both active inflammation and following resolution of the inflammation. This suggests that a targeted manipulation of these underlying changes in the microbial community could present an opportunity to restore the microbiota towards “normal” and thereby prevent clinical relapse.
ASSOCIATION OF NON-CODING IL12B VARIANTS WITH INFLAMMATORY BOWEL DISEASE CONFIRMS IMPORTANCE OF IL23–IL17 SIGNALLING PATHWAY IN DISEASE PATHOGENESIS
M. Tremelling, D. C. Massey, C. Berzuini, F. Bredin, M. Parkes. Department of Gastroenterology, Cambridge University Department of Medicine, Cambridge, UK
Introduction: Confirmed association between inflammatory bowel disease (IBD) and IL23R has been demonstrated by genome-wide association scanning.1 2 The WTCCC scan further demonstrated association between Crohns disease (CD) and a marker 65 kb from the IL12b gene in an adjacent haplotype block.2 With no other candidates nearby key questions are whether the signal encompasses the IL12b gene, whether variation within IL12b is causal and whether ulcerative colitis (UC) is associated with this locus. IL12b encodes a shared subunit of inflammatory cytokines IL12 and IL23; genetic association localised to this locus would highlight the importance of variation in the IL23 signalling pathway to IBD pathogenesis.
Aims & Methods: Our aim was to ascertain evidence for association between IL12b variants and CD/UC susceptibility. 792UC, 669CD and 1077 healthy controls were genotyped using Taqman. This panel gives 94.6% power to identify an odds ratio of 1.26 at p = 0.01. Nine markers were selected using the Tagger algorithm which capture all IL12b variants (SNPs) with allele frequency >1% at r2>0.8. Additionally we genotyped all three amino acid changing SNPs identified in Ensembl.
Results: Two tag markers in IL12b rs2853696 and rs2546893 showed modest but significant association with IBD by logistic regression (p = 0.03 at both loci. See table 1.) rs2546893 was independently associated with UC but not CD (p = 0.047 and p = 0.12.) Additionally multilocus haplotypes within IL12b were identified which were associated with UC, CD and IBD (p = 0.04, 0.02 and 0.03 respectively.) None of the coding variants was associated with disease.
Conclusion: Our data suggest that the previously identified association signal does include the IL12b gene, with non-coding variation associated with both UC and CD susceptibility. Further work must replicate this result, define the boundaries of the association signal and identify causal variants. The latter may affect expression and activity of IL23 and IL12, which are increasingly implicated as playing a central role in IBD pathogenesis.
A DETAILED INVESTIGATION INTO EPIDEMIOLOGICAL RISK FACTORS FOR CHILDHOOD ONSET INFLAMMATORY BOWEL DISEASE IN SCOTLAND
E. A. Hobbs1, J. E. Van Limbergen2, R. K. Russell1, E. R. Nimmo2, H. E. Drummond2, L. Smith2, N. H. Anderson3, G. Davies2, P. M. Gillett1, P. McGrogan1, L. T. Weaver1, M. W. Bisset1, G. Mahdi1, J. Satsangi2, D. C. Wilson1. 1Scottish Paediatric Gastroenterology Hepatology and Nutrition Group, 2Gastrointestinal Unit, 3Public Health Sciences, University of Edinburgh, Edinburgh, UK
Introduction: The incidence of inflammatory bowel disease (IBD) is increasing among children in Scotland and is now among the highest worldwide. Both environmental and genetic risk factors are implicated in the aetiology of IBD.
Aims & Methods: We aimed to investigate the association of asthma, vaccinations and breastfeeding with paediatric IBD in Scotland. 439 children diagnosed with IBD <17 years (274 CD, 101 UC, 54 IBDU; median age 11.2 years (Q1–Q3:8.7–13.1) were compared with more than 25 000 population-matched controls. Children with IBD and their parents were interviewed face-to-face to obtain data on breastfeeding, immunisation history (MMR, diphtheria, tetanus, pertussis, HIB3) and medical history. Control data were provided by the Information Services Division of NHS Scotland: information on breastfeeding for children born in 1996 was collected at the health visitor’s first review visit (around 10 days old) and were available for Lothian and Greater Glasgow; immunisation history was recorded at 24 months for children born in 1993 in Lothian, Greater Glasgow and Grampian. Doctor-diagnosed asthma prevalence data in Scottish children aged 2–15 were provided by the Scottish Health Survey 2003. Unifactorial analyses were performed and corrections for multiple comparisons were made. Breastfeeding data were stratified for geographical region and affluence (using the Carstairs Deprivation Score - DepCat).
Results: History of asthma was associated with IBD and CD (115/439 (26%) and 74/274 (27%) vs 521/2965 (17%) in controls: p<0.0001, OR 1.67 (1.32 to 2.10) and p = 0.0002, OR 1.74 (1.31 to 2.30)). Analysis of controls showed marked differences in breastfeeding rates (>1 week) between Lothian and Greater Glasgow (4368/8196 (53%) vs 2270/6775 (33%) p<10-4 OR 2.26 (2.12 to 2.42)). After stratification for geographical region, there was no significant difference of breast-feeding rates between IBD cases vs controls (p>0.05). Breastfeeding rate in IBD cases (stratified by DepCat (1–2, 3–5, 6–7)) was not statistically different from controls (p>0.05). Breastfeeding rates in IBD cases were significantly different between DepCat 1–2 and DepCat 6–7 (53/79 (67%) vs 17/67 (25%), p<10-4 OR 6.00 (2.91 to 12.36)). This difference was also present in controls (4226/6648 (63%) vs 1768/7750 (23%) p<10-4 OR 5.90 (5.49 to 6.35)). There was no significant association between immunisation history and IBD (p>0.05).
Conclusion: In the high incidence Scottish population, we have shown the novel association of childhood onset IBD and CD with asthma. We did not observe any association between paediatric IBD and either immunisation history or breastfeeding after stratification for geographical region and affluence.
A DETAILED HAPLOTYPE TAGGING INVESTIGATION OF THE IL23R GENE CONFIRMS GENE-WIDE ASSOCIATION WITH CHILDHOOD ONSET INFLAMMATORY BOWEL DISEASE AND CROHN’S DISEASE
J. E. Van Limbergen1, R. K. Russell2, E. R. Nimmo1, H. E. Drummond1, L. Smith1, N. H. Anderson3, G. Davies1, P. M. Gillett2, P. McGrogan2, L. T. Weaver2, M. W. Bisset2, G. Mahdi2, D. C. Wilson2, J. Satsangi1. 1Gastrointestinal Unit, University of Edinburgh, Edinburgh, 2Scottish Paediatric Gastroenterology Hepatology and Nutrition Group, 3Public Health Sciences, University of Edinburgh, Edinburgh, UK
Introduction: The association of CD with the IL23R (interleukin 23-receptor) Arg381Gln variant has been widely replicated, both in children and in adults. Multiple additional association signals throughout IL23R have been identified.
Aims & Methods: To assess the gene-wide contribution of germline variation of IL23R to childhood IBD susceptibility and phenotype and to investigate any interaction with NOD2/CARD15, by means of a detailed haplotype tagging investigation. 709 subjects consisting of 357 childhood IBD patients (233 CD, 86 UC, 38 IBDU) and 352 population-matched controls were genotyped for 8 IL23R haplotype tagging single nucleotide polymorphisms (SNPs) (rs3762318, rs4655679, rs12041056, rs6656929, rs10889668, rs10489630, rs1004819, rs790631). These SNPs were identified using HapMap data (minor allelic freq >10%, haplotype freq >5%, based on solid spine of Linkage Disequilibrium). Genotype/haplotype case-control, log-likelihood and genotype-phenotype analysis (Montreal classification) were performed. The IL23R Arg381Gln variant and the three common NOD2/CARD15 variants were previously genotyped. Subjects were stratified NOD2/CARD15 variant status.
Results: We observed significant associations of four of the tagging SNPs (rs3762318, rs6656929, rs10889668, rs1004819) with IBD/CD on analysis of allelic/genotype frequency. These associations were confirmed on log-likelihood analysis in IBD and CD ((1000 permutations) p = 0.01 and p = 0.002). Haplotype analysis demonstrated a protective effect of the 11221211 haplotype on IBD (2.1% vs 4.4% in healthy controls, p = 0.02 OR 0.49 (0.26 to 0.92)) and CD (2.0%, p = 0.02 OR 0.46 (0.22 to 0.97)). By extending the haplotype analysis to include the previously genotyped Arg381Gln variant, we were able to demonstrate that the protective effect the 11221211 haplotype was independent of the Arg381Gln variant (r2 with tagging SNPs ⩽0.05; IBD: p = 0.02 OR 0.50 (0.27 to 0.93); CD: p = 0.02 OR 0.46 (0.22 to 0.96)). When assessing the association signal for each haplotype block (based on solid spine of LD), we observed association with both 5′- and 3′-end haplotype blocks. After correction for multiple comparisons, no significant genotype-phenotype associations were seen. In wildtype NOD2/CARD15 patients and controls, we observed association with a new risk haplotype (21121212, 4.7% vs 0.9% p = 0.002 OR 5.17 (1.49 to 17.90).
Conclusion: We have demonstrated using a gene-wide haplotype tagging strategy that the multiple association signals of the IL23R locus are independent of the Arg381Gln variant in childhood onset IBD and CD. In our high-incidence population characterised by low NOD2/CARD15 variant carriage, we have observed interaction of the IL23R locus with NOD2/CARD15 through the identification of a novel IL23R risk haplotype.
THE CONTRIBUTION OF GERMLINE VARIATION IN THE AUTOPHAGY GENES ATG16L1 AND IRGM TO CHILDHOOD INFLAMMATORY BOWEL DISEASE
J. E. Van Limbergen1, R. K. Russell2, E. R. Nimmo1, H. E. Drummond1, L. Smith1, N. H. Anderson3, G. Davies1, P. M. Gillett2, P. McGrogan2, L. T. Weaver2, M. W. Bisset2, G. Mahdi2, I. D. R. Arnott1, D. C. Wilson2, J. Satsangi1. 1Gastrointestinal Unit, University of Edinburgh, Edinburgh, 2Scottish Paediatric Gastroenterology Hepatology and Nutrition Group, 3Public Health Sciences, University of Edinburgh, Edinburgh, UK
Introduction: The high incidence Scottish childhood CD population is characterised by a distinct phenotype of extensive intestinal involvement. The contribution of NOD2/CARD15 variants to CD susceptibility in Scotland is low. Recent genome-wide association studies in CD implicate the autophagy genes ATG16L1 (Autophagy-related 16-like 1) and IRGM (a member of the p47 immunity-related GTPase family).
Aims & Methods: Our aims were to assess the influence of germline variation of ATG16L1 and IRGM on childhood IBD susceptibility and phenotype in Scotland. 2418 subjects consisting of 392 childhood IBD (262 CD, 96 UC, 34 IBDU), 685 parents, 979 adult IBD (442 CD/537 UC) and 362 population-matched controls were genotyped for rs2241880 (ATG16L1) and 3 IRGM variants (rs10065172, rs13361189, rs4958847). In addition, 1958 British Birth Cohort control data were used for the analysis (n = 2937). Detailed sequencing of all 5 IRGM exons and exon-intron boundaries was performed. Our childhood onset CD study had 80% power to detect an effect with OR>1.3 for ATG16L1 and >1.4 for IRGM. Case-control analysis, transmission disequilbrium testing (TDT), haplotype analysis, log-likelihood analysis and genotype-phenotype analysis (Montreal) were performed.
Results: The ATG16L1 rs2241880G allele was not associated with childhood CD (54.1% vs controls 52.2%, p = 0.39) in contrast with adult CD (60.7%, p<10-4 OR 1.42 (1.21 to 1.66)). TDT analysis was negative. Genotype-phenotype analysis demonstrated an association of pure ileal disease with the rs2241880G allele (p = 0.02 OR 1.34 (1.03 to 1.74)). We confirmed the effect of rs2241880 genotype on ileal disease vs colonic disease using regression analysis (p = 0.03 OR 2.43 (1.05 to 5.65)). The IRGM rs13361189C allele was not associated with childhood CD (6.8% vs 6.8%, p = 0.97) in contrast with adult CD (9.2%, p = 0.01 OR 1.39 (1.06 to 1.82)). The allelic frequencies of the other IRGM variants did not differ significantly different between cases and controls (p>0.05). TDT analysis was negative. Sequencing analysis identified 7 informative IRGM alleles (D′ 1, paired r2>0.82 except with rs4958847). Haplotypic variation in this block was tagged by rs10065172 and rs4958847. Haplotype CD susceptibility analysis (10 000 permutations) was negative (p>0.40). Log-likelihood analysis in Scottish CD vs controls was negative (p>0.30). Detailed genotype-phenotype analysis for the 3 WTCCC SNPs showed no association with disease location/behaviour in childhood or adult CD.
Conclusion: In Scottish children, the effect of germline variation of ATG16L1 and IRGM on CD susceptibility is small (OR<1.4), and appears less than in adult disease. Other determinants need to be identified in this at-risk paediatric population.
EFFICACY OF METHOTREXATE IN CROHN’S DISEASE PATIENTS PREVIOUSLY ON THIOPURINE THERAPY
M. Wahed1, J. R. Louis-Auguste1, L. M. Baxter2, J. K. Limdi1, J. O. Lindsay2, S. A. McCartney1, S. L. Bloom1. 1Department of Gastroenterology, University College London Hospitals NHS Trust, 2Clinical Academic Unit of Gastroenterology, Barts and The London NHS Trust, London, UK
Introduction: Although thiopurine therapy is widely used in the management of steroid refractory Crohn’s disease, approximately 20% of patients cannot tolerate the drugs and 30% do not respond. In these patients management remains a challenge. Methotrexate has shown efficacy for the induction and maintenance of remission in thiopurine naïve patients, however, its benefit in patients who have failed thiopurine therapy is not clear.
Aims & Methods: We aimed to compare the efficacy of MTX in patients who fail to respond to thiopurine therapy to those who are intolerant. A retrospective review of CD patients treated with MTX at the IBD clinics of University College London Hospital and Barts and the London NHS Trust Hospitals was performed. Patients were identified using the units’ databases and their case notes reviewed. Clinical response (defined as steroid withdrawal, normalisation of previously raised C reactive protein (CRP), or physician’s clinical assessment of improvement) was assessed at 6 months.
Results: Between 2000 and 2007, 75 patients with CD were treated with MTX. The median (range) duration of disease prior to methotrexate was 82.5 (4–480) months. All 75 patients had previously been on a thiopurine for a median of 52 (1–864) weeks, discontinued due to lack of response in 24 (32%) and intolerance in 51 (68%). In the thiopurine non-responders group, the median induction dose of methotrexate used was 25 mg/week followed by a maintenance dose of 15 mg/week for a median duration of 70 weeks (7–208). In the thiopurine intolerant group these figures were 17 mg/week and 15 mg/week for 68 weeks (4–288). There was no significant difference in the MTX used between groups or duration of therapy (p = NS Mann Whitney). Clinical response assessed at 6 months occurred in 13/24 (54.2%) of the thiopurine refractory group and 28/51 (54.9%) of the intolerant group (p = 1.0; two-tailed Fisher exact). Complete steroid withdrawal was possible in 6 out of 6 patients in the refractory group and 7 out of 18 patients in the intolerant group (p = 0.14), although 15 managed a dose reduction. A normalisation of previously raised CRP was seen in 3 out of 12 patients in the refractory patients and 3 out of 18 in the intolerant group (p = 0.67). In the thiopurine non-responders 3/24 (12.5%) went onto receive infliximab and 8/51 (15.7%) in the intolerant group. In the entire study population side effects (bone marrow suppression, abnormal liver function tests, respiratory, nausea, hair loss) occurred in 14 (18.7%), but discontinuation in 7 (9.3%).
Conclusion: Methotrexate appears effective in patients who either fail to respond or are intolerant to thiopurine therapy with no difference between the groups.
EFFICACY OF METHOTREXATE IN ULCERATIVE COLITIS
M. Wahed1, J. R. Louis-Auguste2, L. M. Baxter1, J. K. Limdi2, S. A. McCartney2, S. L. Bloom2, J. O. Lindsay1. 1Clinical Academic Unit of Gastroenterology, Barts and The London NHS Trust, 2Department of Gastroenterology, University College London Hospitals NHS Trust, London, UK
Introduction: The use of thiopurine therapy in the management of ulcerative colitis (UC) is widespread. In those patients who fail to respond or are intolerant of thiopurines, management remains a challenge. Data on the use of methotrexate in ulcerative colitis are limited to a negative inappropriately dosed, randomised controlled trial1 and small case series.
Aims & Methods: The aim of this study was to investigate the efficacy and safety profile of methotrexate in UC. Patients at the IBD clinics of University College London Hospital and Barts and the London NHS trust were identified using the units’ databases. Retrospective data were obtained by case note review. Clinical response (defined as steroid withdrawal, normalisation of previously raised C reactive protein (CRP), or physician’s clinical assessment of improvement) was assessed at 6 months.
Results: Between 2001 and September 2007, 26 patients (mean (SD) age 47(18) with UC were treated with methotrexate. The duration of disease prior to methotrexate was 72 (12–468) months. All had previously been on a thiopurine for a median duration of 24 (2–290) weeks. These were discontinued due to lack of response in 7 (27%) and intolerance in 19 (73%). The median (range) induction dose of methotrexate (combination of oral and parenteral) used was 15 (10–25) mg/week followed by a maintenance dose of 15 (10–25) mg/week. Methotrexate was continued for 66 (2–290) weeks. Clinical response assessed at 6 months was achieved in 17/26 (65%), this included 5/7 (71%) in the thiopurine refractory group and 12/19 (63%) in the intolerant group. Steroid withdrawal was possible in 7 out of 16 patients on steroids at baseline, and a normalisation of previously raised C reactive protein (CRP) in 2 out of the 13 patients. Side effects: bone marrow suppression; abnormal liver function tests (LFTs); nausea and vomiting; and hair loss occurred in 5 (19%), but only warranted discontinuation in 3 (8%) (abnormal LFTs (n = 1), nausea and vomiting (1), hair loss (1)).
Conclusion: Methotrexate appears effective in ulcerative colitis in patients who either fail to respond or are intolerant to a thiopurines. It is also well tolerated in the majority of patients.
SMOKERS WITH ACTIVE CROHN’S DISEASE HAVE DIFFERENCES IN THE CONCENTRATION AND PROPORTION OF KEY BACTERIAL GROUPS OF THE FAECAL MICROBIOTA
A. Koutsoumpas1, C. R. H. Hedin1, S. C. Ng2, M. A. Kamm2, J. D. Sanderson1, S. C. Knight2, A. J. Stagg2, A. Forbes3, J. O. Lindsay4, K. Whelan1. 1Nutritional Sciences Division, King’s College London, 2Antigen Presentation Research Group, St Mark’s Hospital, Imperial College, 3Centre for Gastroenterology and Nutrition, University College London, 4Clinical Academic Unit of Gastroenterology, Barts and the London NHS Trust, London, UK
Introduction: The intestinal inflammation associated with Crohn’s disease results from an inappropriate T-cell response to the luminal microbiota in genetically susceptible individuals. Differences in faecal microbiota occur in patients with active Crohn’s disease, including lower concentrations of bifidobacteria, which are known to promote immunoregulatory dendritic cell responses, and higher concentrations of bacteroides. Smoking increases the risk of developing Crohn’s disease, diminishes the response to therapy and increases the risk of relapse after surgically induced remission. However, the interaction between smoking and the composition of the luminal microbiota is unknown.
Aims & Methods: The aim of this investigation was to investigate the composition of the faecal microbiota in non-smoking and smoking patients with active Crohn’s disease. Thirty six patients (23 non-smokers, 13 smokers) with mild to moderately active Crohn’s disease (CDAI 220–450) were recruited from specialist IBD clinics and baseline clinical and demographic data were collected. Faecal samples were analysed by fluorescent in situ hybridisation using oligonucleotide probes targeting the 16S rRNA of total bacteria (EUB), bifidobacteria (Bif164), bacteroides (Bac303) and Clostridium coccoides-Eubacterium rectale (EREC482).
Results: There were significantly lower concentrations of C coccoides-E rectale (9.6±0.6 vs 9.9±0.3 log10 cells/g, p = 0.05) and significantly higher proportions of bacteroides (47.3±14.8 vs 36.5±14.9%, p = 0.043) in smokers than in non-smokers. In addition, the ratio of bacteroides to bifidobacteria (ratio bac/bif) was significantly higher in smokers (1.1±0.4) compared with non-smokers (0.9±0.3, p = 0.019). There were no significant differences in any of the faecal microbiota between patients prescribed or not prescribed azathioprine or between patients with or without colonic disease. Nor were there significant correlations between any of the faecal microbiota and CDAI, disease duration or age.
Conclusion: There are significant differences in the faecal microbiota between smokers and non-smokers with active Crohn’s disease. As this was an observational study, further research is required to elucidate whether alterations in the luminal microbiota are a mechanism for the impact of smoking on Crohn’s disease.
A URINARY METABOLIC PROFILE ASSOCIATED WITH CROHN’S DISEASE
H. R. T. Williams1, I. Cox2, B. V. North3, V. M. Patel1, S. E. Marshall4, D. P. Jewell5, S. Ghosh1, H. J. W. Thomas1, J. P. Teare1, S. Jakobovits5, S. Zeki1, K. I. Welsh6, S. D. Taylor-Robinson1, T. R. Orchard1. 1Gastroenterology, 2Imaging Sciences, 3Statistics, Imperial College London, London, 4Immunology, University of Dundee, Dundee, 5Gastroenterology, University of Oxford, Oxford, 6Clinical Genomics, Imperial College London, London, UK
Introduction: The pathogenesis of Crohn’s disease (CD) is thought to involve a genetically-determined, abnormal host response to an environmental stimulus, likely to be bacterial, and differences have been demonstrated between the intestinal flora of CD patients and healthy controls. High resolution nuclear magnetic resonance (NMR) spectroscopy generates metabolic profiles from biofluids such as urine. Such urinary profiles are influenced by differences in the intestinal flora since gut bacterial metabolism generates specific metabolic products quantifiable in the spectra. We have previously shown that the levels of one such metabolite, hippurate, are significantly lower in CD patients. It was hypothesised that, in an enlarged cohort of CD patients and healthy controls, sophisticated multivariate statistical analysis would be able to distinguish the CD patients from the controls. This is the largest reported study to use urinary metabonomics in the investigation of any disease.
Aims & Methods: NMR spectra were acquired from the urine samples of 70 Caucasian CD patients (40 male, median (range) age 32 (16–63) years and 30 female, median age 34 (18–66) years) and 46 healthy controls (24 male, median age 31 (21–58) years and 22 female, median age 31 (21–60) years). Multivariate factor analyses were performed using principal components analysis (PCA) and partial least squares discriminant analysis (PLSDA). PCA provided an overview of the complex data, highlighting outliers and clustering. PLSDA related the metabolite data to class membership, elucidating separation between the groups. Validation of the discriminatory power of each model was carried out using an established cross validation technique.
Results: Hippurate levels were again significantly lower in CD patients compared to controls (p<0.0001, Mann-Whitney U test). These differences were independent of medication and diet. After the removal of outliers, PCA revealed clustering of the groups, due to hippurate and trimethylamine-N-oxide resonances. A PLSDA model was then constructed which was able to discriminate the CD patients from the healthy controls with 83.3% sensitivity and 80.4% specificity. Again, this was independent of medication and diet. With narrowing of the spectral range to include only the aromatic region, the CD and control cohorts were distinguished with 100% accuracy.
Conclusion: The novel technique of urinary metabolic profiling with multivariate pattern recognition analysis was able to distinguish the CD patients from the controls.
THE RELATION BETWEEN DISEASE ACTIVITY, QUALITY OF LIFE AND HEALTH UTILITY IN PATIENTS WITH ULCERATIVE COLITIS
A. Woehl1, A. B. Hawthorne2, P. McEwan1. 1CRC Ltd, 2Department of Medicine, University Hospital of Wales, Cardiff, UK
Introduction: Ulcerative colitis (UC) is a chronic that can be cured only by colectomy. It is associated with reduced quality of life (QoL). The objective of the study was to determine QoL and health utility in different disease states.
Aims & Methods: The survey research was conducted in Cardiff, UK. Patients with an active hospital profile and diagnosed with UC were included in the study. The survey covered QoL, measured by SIBDQ,1 demographics, surgery status, disease activity, medical treatment and resource use. To assess the health utility for patients related to different UC disease stages/severity, the SCAI2 was used. Health utility was measured by EQ5D. Statistical analyses included descriptive statistics, tests for group differences and regression analyses.
Results: A total of 329 patients could be identified and surveys were sent out. Of these 188 surveys were returned, 180 fulfilled the inclusion criteria. The average age was 55.0 (SD 14.2) and the average age at diagnosis 34.1 (SD 14.6). Overall, the mean EQ5D was 0.73 (SD 0.29). This was similar to Crohn’s disease in a parallel study (EQ5D 0.74 (SD 0.26)). Comparing severity group versus patients with IPAA and ileostomy these values were 0.87 (SD 0.15) for remission, 0.76 (SD 0.18) for mild disease, 0.41 (SD 0.34) for moderate/severe disease; patients who have undergone IPAA had health utility of 0.71 (SD 0.29), patients with an ileostomy had a health utility of 0.72 (SD 0.35), resulting in health utility for these surgery states slightly below a mild disease severity. The difference between these five groups was statistically significant difference (p<0.001). Patients with suffering from an active disease related condition (arthritis, uveitis, erythema nodosum or pyoderma gangrenosum) had a statistically significant (p<0.001) worse EQ5D of 0.55 (SD 0.36) than patients without (EQ5D 0.83 (SD 0.20)). There was a strong correlation (r = 0.72, p<0.001) between the SIBDQ score and EQ5D. The strongest correlation (r = 0.67, p<0.001) occurred in the social SIBDQ dimension. Disease severity was related with productivity loss and impairment of daily activity. Patients with moderate/severe disease were particularly affected in daily activity, while productivity loss was comparable to patients with a mild disease, but higher than patients in remission.
Conclusion: UC is associated with a reduced QoL and impairments in daily activity. The level of impairment strongly depends on disease severity and extraintestinal manifestations that reflect disease activity.
THE RELATION BETWEEN DISEASE ACTIVITY, QUALITY OF LIFE AND HEALTH UTILITY IN PATIENTS WITH CROHN’S DISEASE
A. Woehl1, A. B. Hawthorne2, P. McEwan1. 1CRC Ltd, 2Department of Medicine, University Hospital of Wales, Cardiff, UK
Introduction: Crohn’s disease (CD) is associated with reduced quality of life (QoL). The objective of the study was to determine QoL and health utility in different disease states.
Aims & Methods: The survey research was conducted in Cardiff, UK. Patients with an active hospital profile and diagnosed with CD were included in the study. The survey covered QoL, measured by SIBDQ,1 demographics, surgery status, disease activity, medical treatment and resource use. To assess CD disease severity the CDAI2 was used. The CDAI was derived applying the Crohn’s Index for Survey Research.3 Health utility was measured by EQ5D. Statistical analyses included descriptive statistics, tests for group differences and regression analyses.
Results: A total of 372 patients were identified and surveys were sent out. 199 surveys returned, of these 194 fulfilled the inclusion criteria. The average age was 47.3 (SD 17.6) and the average age at diagnosis 32.8 (SD 17.1). Overall, the mean EQ5D was 0.74 (SD 0.26). Compared to other chronic conditions e.g. diabetes (EQ5D 0.57 (SD 0.33)) and COPD (EQ5D 0.49 (SD 0.33))4 utility was high, but similar to Ulcerative colitis in a parallel study (EQ5D 0.73 (SD 0.29)). By severity group these values were 0.90 (SD 0.12) for remission, 0.64 (SD 0.23) for active disease, 0.31 (SD 0.31) for extremely severe disease. Patients who have undergone bowel resection had a health utility of 0.72 (SD 0.26), patients without surgery had a health utility of 0.75 (SD 0.25), but the difference was not significant (p = 0.295). Patients with peri-anal involvement had a statistically significant (p = 0.025) worse EQ5D of 0.69 (SD 0.28) than patients without (EQ5D 0.77 (SD 0.22)). There was a strong correlation (r = 0.75, p<0.001) between the SIBDQ score and EQ5D. The strongest correlation (r = 0.75, p<0.001) occurred in the social SIBDQ dimension. Disease severity was related with productivity loss and impairment of daily activity. Patients with extremely severe disease are relatively more affected than patients in other groups.
Conclusion: CD is associated with a reduced QoL and impairments in daily activity. The level of impairment strongly depends on disease severity, but is not dependent on surgery status.
Neurogastroenterology/motility posters
CLINICAL PHENOTYPING OF IRRITABLE BOWEL SYNDROME IN A PROSPECTIVE CONTROLLED TRIAL USING PSYCHOLOGICAL PROFILING AND CORTICAL EVOKED ACTION POTENTIALS
D. C. Bullas1, A. R. Hobson2, A. Khan1, K. J. Hicks2, G. E. Dukes2, M. A. Kamm1, N. Arebi1. 1St. Mark’s Hospital Campus, Imperial College, Harrow, 2Immuno-Inflammation CEDD, GlaxoSmithKline Medicines Research Centre, Stevenage, UK
Introduction: Irritable bowel syndrome (IBS) patients present with unexplained gastrointestinal symptoms including abdominal pain. Recto-sigmoid distension studies commonly purport to detect rectal hypersensitivity, the aetiology of which is uncertain. Pain sensitivity is determined by several factors including afferent nerve sensitivity and psychological profile. Dissecting the relative contribution of each component to disease expression in a clinically relevant manner would be valuable to target therapy.
Aims & Methods: To combine an objective measure of rectal central afferent sensitivity (cortical evoked potentials (CEPs)) in conjunction with detailed psychological profiling. IBS patients (Rome 2) and controls were recruited. CEPs were elicited by electrical rectal stimulation using validated methods. Primary endpoints: sensory (ST) and pain (PT) thresholds, CEP amplitude/latency and psychological questionnaire scores. Questionnaires: Spielberger State-Trait Anxiety Inventory (SSTAI), Hospital Anxiety and Depression Scale (HAD), Eysenck Personality Questionnaire-Revised (EPQ-R), Visceral Sensitivity Index (VSI), Patient Health Questionnaire (PHQ-15), Visual Descriptor Visual Analogue Scale (VDVAS) and Whiteley Index (WI). Statistical analysis utilised a 1-way Anova, presented as mean differences ±95% CI.
Results: Data for 13 IBS patients (age range 20–60; 10-females) and 16 controls (age range 21–39; 10- females;) were analysed. IBS patients scored higher on measures of anxiety (SSTAI-Trait: 6.96 (1.07 to 12.86); HAD: 3.66 (0.95 to 6.37)), depression (HAD: 3.46 (1.77 to 5.15) although within normal range), neuroticism (EPQ-R: n = 6.49 (2.48 to 10.49)), somatisation (PHQ-15: 6.24 (3.29 to 9.18)), hypochondriasis (WI: 12.05 (5.66 to 18.44)) and visceral specific symptoms (VDVAS-Urge: 8.46 (5.79 to 11.13), VDVAS-Intensity: 10.76 (7.85 to 13.68); VSI: 34.14 (24.58 to 43.69)). There were no differences in rectal sensitivity (ST: 1.70 (−7.40 to 10.80); PT: −14.32 (−32.10 to 3.46)) or CEP latency (Peak 1 latency: 15.63 (−1.02 to 32.27). CEP amplitudes were lower in the IBS group (Peak 1 amplitude: −3.98 (−7.05 to −0.91)). In IBS, many of the questionnaire scores were positively correlated.
Conclusion: Preliminary data reveal that few IBS patients had objective evidence of rectal afferent nerve hypersensitivity. At the group level, despite using equivalent stimulus intensities, mean CEP amplitude in IBS was significantly reduced. Increased scores seen across a variety of psychological domains (anxiety, depression, neuroticism, somatisation and hypochondriasis) highlight the important role of psychological comorbidity. Future studies in larger subject cohorts will determine the prevalence and stability of these clinical phenotypes over time.
IMAGES OF DISEASE: A STUDY IN IRRITABLE BOWEL SYNDROME AND THE EFFECT OF TREATMENT
H. R. Carruthers1, V. Miller1, N. Tarrier2, P. J. Whorwell1. 1Medicine, Wythenshawe, 2Psychology, University of Manchester, Manchester, UK
Introduction: Visual imagery is frequently utilised by a variety of non-pharmacological approaches to treatment and is especially useful in hypnotherapy (HT) for irritable bowel syndrome (IBS). Imagery assessment also forms an integral part of many hypnotisability scales. We have speculated that more specific imagery relating to the patients disorder, that is if they have a mental picture of their IBS, may have useful clinical applications such as predicting response to treatment.
Aims & Methods: 109 patients were asked if they had an image of their IBS pre- and post-HT by a medical artist (HRC) who then made watercolour paintings of any images described. Results were related to symptom severity, anxiety, depression, absorption (hypnotisability) and outcome.
Results: 49% of patients had an image of their IBS before treatment with a wide variety of images being described and examples of these will be shown at presentation. 57.8% of responders compared with 35.5% of non-responders to treatment had an image of their disease (p = 0.04) suggesting imagery has predictive value. Imagery did not relate to symptom severity or depression but was significantly associated with gender (p = 0.04), anxiety (p = 0.02) and absorption (p = 0.001). An image in colour was associated with a better outcome than a black and white image (p = 0.05). All images changed in responders, often becoming more abstract in nature.
Conclusion: Imagery of IBS, particularly when it is in colour, helps to predict response to HT and may also be useful in helping to understand the way patients think about their illness.
IS DIABETIC GASTROENTEROPATHY ASSOCIATED WITH AUTONOMIC DYSFUNCTION?
R. Doyle, J. McLaughlin, P. Begum. GI Sciences, CSB, Hope Hospital, Salford, UK
Introduction: Gastrointestinal (GI) symptoms are common in diabetes mellitus (DM), but robust evidence regarding prevalence is surprisingly limited. It is generally believed that GI dysmotility in DM is due to autonomic neuropathy (AN), but the prevalence of related autonomic symptoms in diabetics with GI symptoms is not well described.
Aims & Methods: To determine the prevalence of GI and non-GI autonomic symptoms in unselected DM patients, and to assess the association between gender, duration and glycaemic control and GI symptoms. Consecutive patients attending diabetes outpatient clinics over 2 months were asked to complete a validated autonomic symptom questionnaire, detailing autonomic symptoms in 9 different domains. The GI domain comprised questions regarding upper GI symptoms, diarrhoea and constipation during the previous year. A Composite Autonomic Symptom Scale (COMPASS) was derived.1 Duration of DM and glycaemic control (HbA1C) were recorded. The Mann-Whitney test and linear regression analysis were used.
Results: There was an 81.1% response rate. Of the 202 participants, 67.3% experienced GI symptoms while 60.4% reported wider symptoms suggestive of autonomic dysfunction. The mean COMPASS score was 30.0±23.3; range −8 to 106. This exceeded the upper limit of normal (18.8) in 60.4%.1 Of those reporting GI symptoms, upper GI symptoms, diarrhoea and constipation were experienced by 65.4%, 62.5% and 57.4% respectively. Type 2 DM participants experienced more GI symptoms than those with type 1 (p = 0.007). No gender differences existed (p = 0.28). Contrary to previous reports, there was no correlation between GI symptoms and HbA1c for type 1 (r = 0.003) or type 2 DM (r = 0.136). Also differing from earlier reports, there was no correlation between GI symptoms and the duration of diabetes (type 1 r = 0.066; type 2, r = 0.051). Other autonomic symptoms had a high prevalence in the study population and correlated with the GI score. This was most clear for orthostatic intolerance, reported in 69.3% (r = 0.444, p<0.0001), and secretomotor symptoms, reported in 67.3% (r = 0.355, p<0.0001).
Conclusion: In this diabetic population, the prevalence of GI symptoms was high. Contrary to previous studies we found no significant association between genders, duration of diabetes or glycaemic control in the participants reporting GI symptoms. However, there was a strong correlation between GI symptoms and the broader symptom domains suggestive of AN, particularly orthostatic intolerance and secretomotor dysfunction. These data strongly support the concept that a dysautonomic element underpins GI symptoms in DM, but suggest that their pattern of evolution may be distinct from other complications of chronic diabetes. This work was supported by a CORE/Diabetes UK Fellowship.
CORRELATION BETWEEN MUCOSAL LYMPHOCYTES, MAST CELL ACTIVATION AND SEROTONIN TRANSPORTER IN DUODENAL BIOPSIES AND PLATELETS OF PATIENTS WITH IRRITABLE BOWEL SYNDROME AND DIARRHOEA COMPARED WITH COELIAC DISEASE
S. J. Foley1, G. Singh2, L. C. Lau3, A. F. Walls3, G. Holmes4, A. Bennett2, C. Marsden2, R. C. Spiller1. 1Wolfson Digestive Disease Centre, 2Biomedical Sciences, University of Nottingham, Nottingham, 3Immunopharmacology Group, University of Southampton, Southampton, 4Gastroenterology, Derbyshire Royal Infirmary, Derby, UK
Introduction: We have previously shown increased postprandial plasma serotonin (5HT) in patients with post infective irritable bowel syndrome (IBS) and coeliac disease (CD). While coeliacs have obvious mucosal inflammation and depressed mucosal SERT mRNA, IBS patients have subtle inflammation, but the effect on SERT is unknown. There are reports in IBS of increased mucosal mast cells (MC) and lymphocytes and circulating cytokines, which both cell and animal studies show to depress SERT. We therefore assayed mucosal and platelet SERT together with 5HT and MC tryptase release (MCT) from duodenal biopsies which were also stained for inflammatory cells including intraepithelial lymphocytes (IEL) and 5HT-containing enterochromaffin cells (EC).
Aims & Methods: 28 healthy volunteers, 20 patients with IBS-D and 20 with untreated coeliac disease (CD) completed bowel symptom questionnaires and underwent duodenal biopsy. Secretion was assayed after 6 hour incubation. Immuno-histochemistry was performed to identify IELs and ECs. SERT mRNA expression measured by Taqman quantitive RT-PCR (normalised to cytokeratin20 (CK20) mRNA in arbitrary units). Platelet SERT function was assayed by 3H-5HT uptake and SERT binding sites in platelet membranes by 3Hparoxetine binding.
Results: Tryptase secretion was increased fourfold in IBS-D compared to HV. IBS-D also showed significant elevation in IELs but normal EC cell counts. As expected IEL and EC cell counts in CD were markedly increased. SERT mRNA in enterocytes was significantly depressed in IBS-D and platelet SERT function (5HT uptake) impaired in IBS-D and to a lesser extent in CD. Platelet paroxetine binding was significantly increased in IBS-D. Mucosal IELs correlated negatively with SERT mRNA, r = 0.37, p<0.01, and positively with EC cell counts, r = 0.39, p = 0.006, n = 46. Both IELs and EC counts correlated negatively with platelet 5HT uptake, r = 0.53 and 0.44 respectively, both p<0.01. Platelet 5HT uptake in HV and IBS-D correlated negatively with Paroxetine binding, r = 0.35, p = 0.007, n = 50.
Conclusion: IBS-D patients mucosa showed enhanced mast cell secretion and increased IELs which correlated negatively with mucosal SERT and platelet uptake which were both depressed, changes which may be driven by inflammatory mediators. The associated increased circulating plasma 5HT levels may lead to a compensatory increase in platelet paroxetine binding.
GHRELIN INHIBITS LIPID-INDUCED GASTRIC EMPTYING DELAY IN MAN
D. J. Lassman1, G. J. Dockray2, D. G. Thompson1. 1GI Sciences, University of Manchester, Salford, 2Physiological Laborotory, University of Liverpool, Liverpool, UK
Introduction: Ingested lipid in the form of fatty acids of carbon chain length 12 or more limits food intake by delaying gastric emptying through cholecystokinin-dependent pathways. The gastric regulatory peptide ghrelin stimulates feeding but it is unknown if it modulates the effects of lipid-induced CCK signalling in man.
Aims & Methods: The aim of this study was to explore the interactions between exogenous ghrelin and gastric emptying delay induced by a CCK-releasing lipid in man. Five healthy volunteers were studied on 4 separate occasions after an overnight fast in a double-blind randomised manner. Each received a 250 ml intra-gastric infusion of either a CCK-releasing lipid (0.05 M dodeconoic acid) or vehicle solution whilst also receiving an intravenous infusion of either 1.25 pmol/kg/min of ghrelin or 0.9% saline. The intra-gastric infusion was labelled with 100 mg 13C acetate and breath samples were taken every 5 minutes after the infusion for 45 min. Changes in the ratio of exhaled 13CO2:12CO2 were measured by infrared spectro-photometry and gastric emptying rate was determined as the cumulative change in the ratio over 45 min.
Results: Intra-gastric infusion of lipid significantly delayed gastric emptying compared to vehicle. The effect of lipid on gastric emptying delay was blocked by intravenous ghrelin infusion whereas ghrelin alone had no effect on gastric emptying with vehicle (multiple comparisons ANOVA, p<0.001).
Conclusion: These data show that ghrelin specifically reverses the effect of a CCK-releasing lipid on gastric emptying which suggests that in the postprandial period gastric emptying might be determined by an interplay between rising CCK concentrations and falling ghrelin concentrations.
PATIENTS WITH PRIMARY (IDIOPATHIC) ACHALASIA HAVE CIRCULATING PERIPHERAL BLOOD MONONUCLEAR IMMUNE CELLS THAT ARE HYPER-REACTIVE TO THE HERPES SIMPLEX 1 VIRUS
K. W. Lau1, C. McCaughey2, P. V. Coyle2, L. J. Murray3, B. T. Johnston1. 1Gastroenterology, 2Virology, Royal Victoria Hospital, 3Epidemiology & Public Health, Queens University of Belfast, Belfast, UK
Introduction: Primary achalasia is the best characterised oesophageal motor disorder but the aetiology is unknown. The pathology seen in this condition consists of a decrease in nitric oxide- producing neurones and the presence of an activated T-cell inflammatory infiltrate in the myenteric plexus.1 Certain Human Leucocyte Antigen (HLA) class II alleles are also more prevalent in patients with primary achalasia.1 These factors suggest that an autoimmune mechanism may be involved in the pathogenesis of primary achalasia. The stimulus initiating this is unknown but could involve the Herpes simplex 1 virus (HSV-1). A previous study has demonstrated the existence of oesophageal mononuclear immune cells reactive to HSV-1 antigens in an in vitro setting.2
Aims & Methods: The aim of this study is to test the hypothesis that circulating peripheral blood mononuclear cells in patients with primary achalasia may be reactive to HSV-1. Whole blood culture experiments were conducted with heparinised peripheral venous blood obtained from 151 patients with primary achalasia and 118 healthy controls. Whole blood was cultured in the presence of ultraviolet inactivated HSV–1 (multiplicity of infection of 1 TCID50/lymphocyte) or conditioned cell culture media. Reactivity of mononuclear cells to viral antigens was quantified by measuring expression of the cytokine gene interferon-γ using Taqman real-time polymerase chain reaction. Data are expressed as cytokine fold change corresponding to ratio of interferon-γ messenger RNA copies produced in antigen stimulated versus unstimulated cells. Interferon-gamma fold change was compared between cases and controls using the unpaired Student’s t test after log transformation and expressed as median (interquartile range).
Results: The interferon-γ fold change was higher in cases 61.33 (20.54 to 217.00) than controls 49.67 (10.05 to 157.05). Mean fold change difference between cases and controls was 1.66 times (95% CI interval 1.17–2.34, p = 0.004).
Conclusion: The results indicate that mononuclear immune cells hyper-reactive to HSV-1 are present in the peripheral blood of patients with primary achalasia and may contribute to the pathological changes observed in the myenteric plexus.
A PROSPECTIVE STUDY OF THE PREVALENCE OF GASTROINTESTINAL SYMPTOMS IN PATIENTS WITH TYPE 1 DIABETES MELLITUS AND CORRELATION WITH DIABETES CONTROL AND QUALITY OF LIFE
J. S. Leeds1, A. D. Hopper1, S. Tesfaye2, D. S. Sanders1. 1Gastroenterology, 2Diabetes, Royal Hallamshire Hospital, Sheffield, UK
Introduction: The relation between diabetes mellitus and the gastrointestinal tract has been described however symptoms are often missed during consultations in the diabetes clinics and their impact is therefore unknown. The effect of diabetes on the gastrointestinal tract and perception of symptoms has not been investigated. There has never been a large prevalence study determining the impact and relevance of gastrointestinal symptoms on diabetes control or quality of life in patients with Type 1 diabetes mellitus.
Aims & Methods: Patients with Type 1 diabetes mellitus were recruited from the Diabetes Centre and were asked to complete a previously validated gastrointestinal symptom questionnaire and Short Form 36 version 2 quality of life questionnaire. Blood was taken at the same time to measure Hba1c levels as a marker of diabetes control. 603 non-diabetic controls were questioned in the same manner to provide controls for age and sex.
Results: 364 patients with Type 1 diabetes mellitus (mean age 42.2 years) took part in the study of which 201 were males. Gastrointestinal symptoms were significantly more frequent in diabetics as compared to controls (OR 2.2, 95% CI 1.5 to 3.2, p<0.0001). In particular, excessive tiredness (OR 3.0), constipation (OR 2.6), weight loss (OR 2.5), floating stools (OR 2.3), diarrhoea (OR 2.3), alternating bowel habit (OR 2.1) and abdominal pain (OR 1.8) were significantly more frequent in diabetics compared to controls respectively (all p<0.01). Bloating (OR 1.3) and flatulence (OR 1.3) were not. A past history of pancreatitis was more frequent in diabetics (OR 5.5) but IBS, IBD, diverticular disease and bowel cancer were not. Glycaemic control was worse in those with diarrhoea 9.3% vs 8.0% (p = 0.008) or abdominal pain 8.8% vs 7.9% (p = 0.009) as compared to age, sex-matched controls in the diabetes cohort. Quality of life scores were lower in those with diabetes and diarrhoea compared to controls with diarrhoea (p<0.0001 for all domains) and those with diabetes and abdominal pain compared to controls with abdominal pain (p<0.01 for all domains).
Conclusion: Gastrointestinal symptoms are twice as frequent in patients with Type 1 diabetes mellitus as compared to age, sex-matched controls in the general population. Diarrhoea and/or abdominal pain are associated with poor diabetes control and quality of life scores. Whether patients with diabetes perceive gastrointestinal symptoms differently or poor glycaemic control is a product of underlying gastrointestinal disease is unknown as deserves further evaluation.
DEVELOPING INTERVENTIONAL PAIRED ASSOCIATIVE STIMULATION AS A TREATMENT FOR DYSPHAGIA AFTER STROKE: WHAT ARE THE BEST PARAMETERS?
E. Michou, S. Mistry, S. Singh, S. Jefferson, S. Hamdy. Gastrointestinal Sciences, The University of Manchester, Hope Hospital, Salford, UK
Introduction: Paired electrical pharyngeal and cortical stimulation (interventional paired associative stimulation (IPAS)) for 30 minutes has been shown to increase cortical excitability of pharyngeal motor cortex in healthy subjects, when the two stimuli are separated by 100 ms.1 The effects of shorter durations of IPAS on corticobulbar excitability remain unknown, yet are of relevance in developing this novel neurostimulation technique therapeutically.
Aims & Methods: We therefore investigated whether changing the duration of IPAS acts as a parameter for inducing brain excitation. In 12 healthy subjects, pharyngeal electromyographic (EMG) responses were recorded using an intraluminal catheter after the application of transcranial magnetic stimulation (TMS) over pharyngeal motor cortex, as a measure of cortico-bulbar excitability. IPAS was applied for 10, 20 and 30 minutes using paired stimuli every 20 s with an electrical pharyngeal stimulus (via the catheter) followed by a cortical stimulus to the pharyngeal motor cortex (via TMS) after 100 ms. Cortical excitability was reassessed immediately, 30, 60 and 90 minutes post-intervention. The three IPAS durations were randomly tested on separate visits.

{kind=link}
{kind=link}
{kind=link}
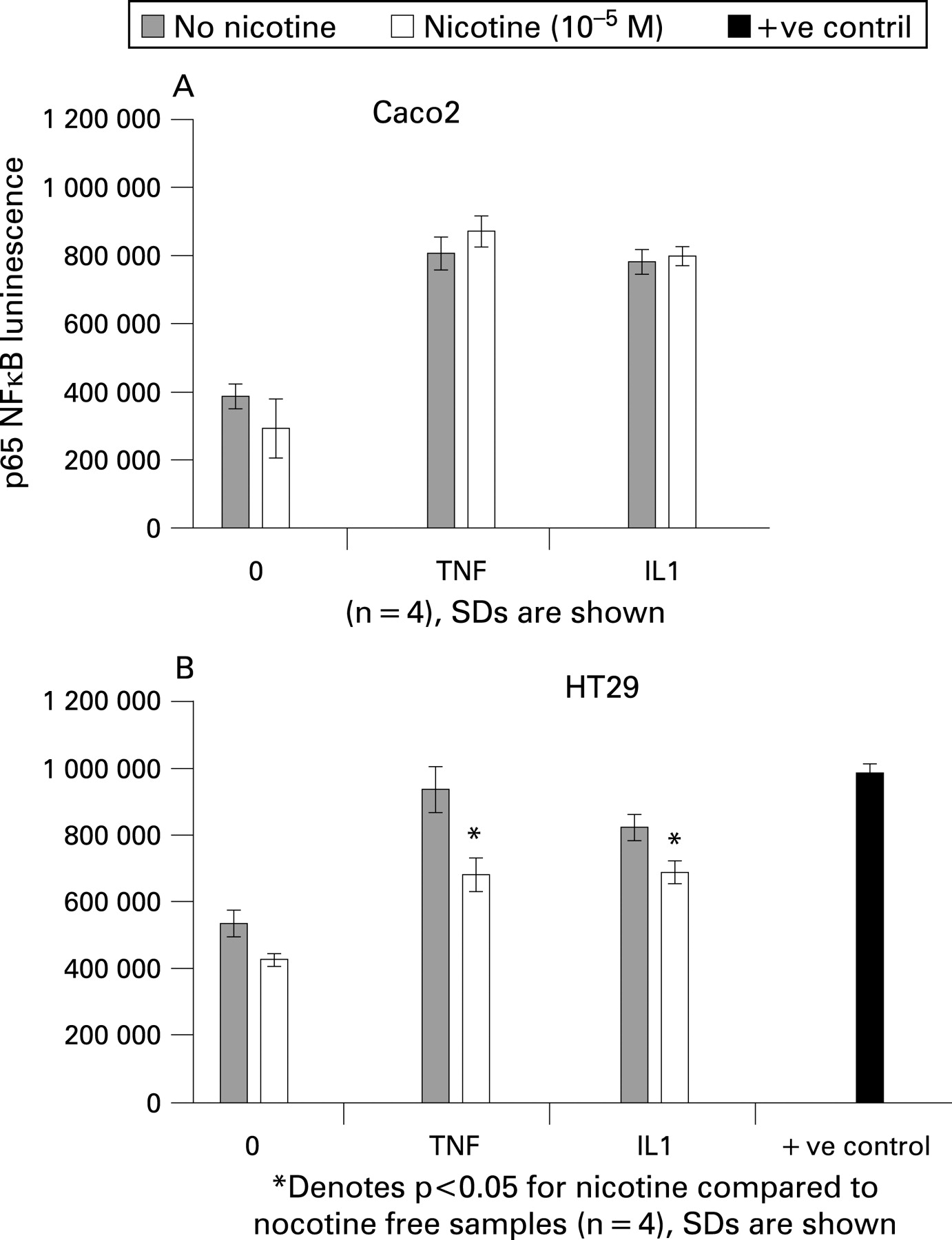{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Results: Compared to baseline, IPAS for 20 minutes induced the greatest increase in cortical excitability immediately, and after 60 and 90 min. ANCOVA confirmed a strong trend for IPAS 20 min increasing cortical excitability to a maximum of 53% at 90 min (p = 0.058), with only modest effects for 10 and 30 minutes (fig).
Conclusion: IPAS induced increases in pharyngeal motor cortex excitability are dependent on the duration of the stimulation, and may have a future role as a therapeutic intervention for dysphagia following stroke.
DYSBIOSIS IN DIARRHOEA PREDOMINANT IRRITABLE BOWEL SYNDROME: SIGNIFICANT INCREASE IN MUCOSA-ASSOCIATED BACTEROIDES
G. C. Parkes, N. B. Rayment, B. N. Hudspith, L. Petrovska, M. C. Lomer, J. Brostoff, K. Whelan, J. D. Sanderson. Nutritional Sciences Division, Kings College London, London, UK
Introduction: A number of studies indicate a role for the gastrointestinal microbiota in irritable bowel syndrome (IBS). Studies have shown that patients with IBS have altered gastrointestinal microbiota, although most of these focus solely on the faecal microbiota. Given the increasing evidence of an inflammatory component to IBS and the proximity of the mucosa-associated microbiota to the colonic epithelium we hypothesise that the mucosa-associated microbiota play a key role in the pathogenesis of IBS.
Aims & Methods: To compare the mucosa-associated microbiota between patients with diarrhoea predominant IBS (IBS-D) and controls using fluorescent in situ hybridisation. Patients with IBS-D were identified using Rome III criteria, while controls with a normal bowel habit and without abdominal pain, rectal bleeding or bloating were recruited from colorectal cancer screening and polyp surveillance. Rectal biopsies were snap frozen in liquid nitrogen and 6 μm sections cut, fixed in 4% paraformaldehyde and permeabilised in 0.2% Triton/PBS. Sections were hybridised overnight with oligonucleotide probes specific for total bacteria (EUB), bacteroides (Bac303), Clostridium coccoides-Eubacterium rectale (EREC482), bifidobacteria (Bif164), Lactobacillus (Lab154) and Escherichia coli. Hybridised mucosa-associated microbiota were viewed under a confocal microscope and were quantified by counting five randomly selected high power fields.
Results: Samples were collected from 27 patients with IBS-D and 26 controls. The mean (SD) age of IBS-D patients was 36.2 (10.1) and controls was 46.1 (11.7). All bacteria were found in a mucinous layer adjacent but not adherent to the epithelium and there were no invasive bacteria seen. There were significantly greater numbers of total mucosa-associated bacteria, highly significant greater numbers of bacteroides and a trend towards greater numbers of clostridia in patients with IBS-D.
Conclusion: This study demonstrates a clear dysbiosis in the mucosa-associated microbiota in diarrhoea predominant IBS. Bacteroides and some species of clostridia are proinflammatory. Studies in patients with inflammatory bowel disease have shown significantly higher numbers of bacteroides in the mucosa of patients compared with controls. Although we do not know whether this is a primary or secondary phenomenon, it does suggest that the gastrointestinal microbiota may be important in the aetiology of IBS and that modulation of the gut microbiota may be of benefit.
EFFECT OF A NOVEL TRANS-GALACTOOLIGOSACCHARIDE PREBIOTIC ON FAECAL MICROBIOTA AND SYMPTOMS IN PATIENTS WITH IRRITABLE BOWEL SYNDROME
A. Davis1, J. Vulevic2, G. Tzortzis3, G. R. Gibson4, D. B. SILK5. 1Dietetics, Central Middlesex Hospital, London, 2Food Microbial Sciences Unit, University of Reading, Reading, 3Academic Surgery, Clasado Ltd, Milton Keynes, 4Food Microbial Science Unit, University of Reading, Reading, 5Academic Surgery, Imperial College Healthcare NHS Trust, London, UK
Introduction: Gut flora-mucosal interactions may be involved in the pathogenesis of irritable bowel syndrome (IBS), and the probiotic bifidobacterium infantis 35624 has been shown to alleviate symptoms in IBS patients.1 Prebiotics are non digestible food supplements that are fermented by host bacteria thereby altering the microbiota of the host often by stimulating healthy bacteria.2 We have synthesised a novel trans-galactooligosaccharide bifidobacteria enhancing prebiotic and report here the first ever study undertaken to investigate the efficacy of prebiotic therapy in IBS.
Aims & Methods: 44 patients with Rome II positive IBS completed a 12 week single centre parallel cross over controlled clinical trial. (2 weeks baseline, 4 weeks placebo (PL), 2 weeks washout, 4 weeks prebiotic (PB). Patients were randomised to receive either 3.5 g/d PL, PB, 7 g/d PL PB or PL PL. IBS symptoms (abdominal pain/discomfort, bloating/distension, bowel movement difficulty) were monitored weekly and scored according to a 6 point Likert scale. Stool frequency and form (Bristol stool scale) SGA, anxiety and depression and QOL scores were also monitored.
Results: PB but not PL significantly enhanced the bifidobacterium proportion of faecal microflora (3.5 g/d p<0.005; 7 g/d p<0.001). PL PL was without effect on any of the clinical parameters monitored PB 3.5 g/d significantly improved stool consistency (p<0.05), flatulence (p<0.05) composite score of symptoms (p<0.005) and SGA (p<0.001). PB 7 g/d significantly improved SGA (p<0.05) and anxiety scores (p<0.05).
Conclusion: The galactooligosaccharide prebiotic is significantly bifido bacterium enhancing in IBS patients and is effective in alleviating symptoms. These findings suggest that the prebiotic has potential as a therapeutic agent in IBS and should prompt the undertaking of a large randomized controlled trials of suitably formulated prebiotics in IBS patients.
HIGH RESOLUTION MANOMETRY WITH LARGE VOLUME MULTIPLE REPEATED SWALLOWS AIDS THE DETECTION OF OESOPHAGEAL PATHOLOGY
R. R. Sweis, M. Fox, T. Wong, R. Anggiansah, A. Anggiansah. Oesophageal Lab, St Thomas’ Hospital, London, UK
Introduction: Conventional manometry does not provide a diagnosis in many patients referred with oesophageal symptoms because, in part, it fails to predict effective bolus transport.1 2 High resolution manometry (HRM) measures contractile activity and the intra-bolus pressure (IBP) gradient that drives fluid movement.3 In the pharynx, the position of maximum IBP gradient following 10–20 ml swallows identifies pathology causing significant resistance to flow.4 A similar approach with larger volumes has not been tested in the relatively wide lumen of the distal oesophagus.
Aims & Methods: This study assessed whether HRM during free drinking by multiple rapid swallows (MRS) can localise and quantify functional and structural pathology of the oesophageal body and lower oesophageal sphincter (LOS). A prospective study of 160 consecutive patients undergoing HRM for investigation of oesophageal symptoms was performed. HRM measurements for 10 water (5 ml) and five bread swallows were obtained in the upright position. Peristaltic pressure, baseline and nadir LOS pressure, IBP, and IBP gradient were recorded. Patients then drank 200 ml water by MRS. Contractile activity, IBP and IBP gradient were measured. Symptom events were recorded. The results of liquid, solid and 200 ml MRS were compared in patients with different diagnoses.
Results: 151 studies were technically successful and 125 provided complete data for analysis (78%). Failed swallows (p<0.001) and spasm (p<0.01) were more frequent and less reproducible for solids than 5 ml liquid swallows or MRS. Contractile pressure, IBP and IBP gradient were higher for solids (all p<0.001); LOS function was not affected. During 200 ml MRS contractile activity was suppressed (less in DOS). MRS produced more complete LOS relaxation than 5 ml swallows (97% vs 83%, p<0.01), also in achalasia (60% vs 34%, p<0.01). Overall IBP and IBP gradient decreased more during 200 ml MRS than 5 ml swallows (p<0.001); however both increased in achalasia (p<0.001) and in patients with structural LOS pathology. Average IBP gradient during MRS increased progressively from reflux, normal, hypertensive peristalsis, DOS and achalasia (1, 4, 10, 18, 35 mmHg respectively). Dysphagia and supra-gastric belching were more likely during 200 ml MRS than 5 ml swallows (p<0.001), especially when IBP >20 mmHg (p<0.01 vs lower values).
Conclusion: HRM with 200 ml MRS helps to localise and quantify the severity of oesophageal pathology by increasing IBP above and IBP gradient across the lesion compared to standard 5 ml swallows. Functional and structural diseases were identified by this technique. In addition, raised IBP during MRS was associated with the occurrance of typical, clinically relevant symptoms.
DUODENAL MASTOCYTOSIS IN IRRITABLE BOWEL SYNDROME: AN ADULT ENDOSCOPIC POPULATION-BASED CASE-CONTROL STUDY (KALIXANDA)
M. M. Walker1, N. J. Talley2, M. Prabhakar1, C. Pennaneac’h3, P. Aro4, J. Ronkainen4, T. Storskrubb4, A. R. Zinsmeister5, W. S. Harmsen5, L. Agreus4. 1Histopathology, Imperial College London, London, UK, 2Department of Internal Medicine, Mayo Clinic College of Medicine, Jacksonville, USA, 3Histopathology, St Mary’s Hospital, London, UK, 4Center for Family and Community Medicine, Karolinska Institute, Stockholm, Sweden, 5Division of Biostatistics, Mayo Clinic College of Medicine, Rochester, USA
Introduction: Irritable bowel syndrome (IBS) is a common functional gastrointestinal disorder with symptoms of abdominal pain and altered bowel habit. Recent studies show that IBS may have an organic component as demonstrated by mast cell hyperplasia in the jejunum and colon. Mast cells in the gut lie in close proximity to enteric nerve terminals and release potent mediators which alter enteric nerve and smooth muscle function.
Aims & Methods: The aim of this study was examine the mast cell population in duodenal biopsies of subjects with IBS to ascertain if the upper small bowel is involved in this syndrome. A random sample of an adult Swedish population (n = 1000; mean age 54 years; 51% female) underwent upper endoscopy and biopsy. Subjects with IBS (n = 34; 16 IBS constipation (IBS-C), 18 IBS diarrhoea, (IBS-D) and randomly selected healthy controls (n = 18) were identified in the population. Irritable bowel syndrome was defined as troublesome abdominal pain at any site plus concomitant bowel habit disturbance. Immunocytochemistry was performed for mast cells (CD117). Two blinded independent observers assessed duodenal mast cell counts, quantified by counting the number per 5 high power fields (HPFs) in the duodenal bulb (D1), and the second part of the duodenum (D2). Duodenal and pathology and the presence of H pylori in gastric mucosa were also assessed.
Results: Cases and controls showed similar demographics for gender and H pylori infection. The mast cell counts/5HPF were, in D1 controls, median 132 (range 87–259), IBS, median, 194 (range 148–236) and in D2, controls, median, 145 (range 66–206), IBS, median, 255 (range 124–443). Mast cell counts were significantly raised in the duodenal bulb (D1) and descending duodenum (D2) biopsies in both IBS-C and IBS-D subjects in comparison to controls, overall IBS, D1 p = 0.0085, D2 p = 0.0007. There was no significant difference between mast cells counts in IBS-C and IBS-D subjects (p = 0.30). No other duodenal pathology was noted.
Conclusion: Mast cell hyperplasia in the duodenum is linked to IBS. The intestinal mast cell alone, or as a participant in a more complex physiological-psychological pathway, may be fundamental to the pathogenesis of IBS. A duodenal biopsy may have a diagnostic role in IBS and mast cell suppression therapy could be explored as a novel treatment.
Pancreas posters
THE CONTRIBUTION OF BONE MARROW-DERIVED MYOFIBROBLASTS TO PANCREATIC FIBROSIS
O. Inatomi1, W. R. Lin2, Y. Kallis3, C. Y. Lee1, R. Jeffery1, M. Brittan2, M. R. Alison2, N. A. Wright1. 1Histopathology Unit, London Research Institute, Cancer Research UK, 2Centre for Diabetes and Metabolic Medicine, Queen Mary’s School of Medicine, 3Department of Hepatology, Imperial College, London, UK
Introduction: Pancreatic stellate cells and myofibroblasts are known to play a central role in pancreatic fibrosis. Bone marrow (BM)-derived cells have not only been credited with the ability to generate a range of other cell types, but also proven to functionally contribute to the mesenchymal cells in the intestine and liver after tissue injury.1 2 However, the role of BM-derived cells in pancreatic fibrosis still remains unclear.
Aims & Methods: Female C57Bl6 mice (6 weeks old) were lethally irradiated and rescued by a BM transplant from donor male mice. After 6 weeks, experimental pancreatitis was induced by repeated intraperitoneal injections of cerulein (100 u/kg×10 weeks), a cholecystokinin analogue. In situ hybridisation (ISH) for Y chromosome detection was combined with immunohistochemistry (IHC) for SMA, GFAP and CD45 to determine the phenotype of BM-derived cells. Their functional activities were analysed by combining ISH (for Y) with IHC (αSMA) and autoradiography (procollagen mRNA).
Results: Myofibroblasts (αSMA-expressing) were only found in the fibrotic areas and the number of them increased significantly in proportion to the severity of fibrosis. Approximately 15% of them were donor-derived whereas other types of cells were not. Moreover these cells expressed TGF-β, collagen type1 and fibronectin, suggesting a functional contribution.
Conclusion: Our results show BM contributed specifically to pancreatic myofibroblasts in fibrosis. This suggests BM-derived myofibroblasts play an important role in the development of fibrosis in the pancreas and they might be the target of antifibrosis therapy using genetically modified adult stem cells.
INCREASED IMMUNOGLOBULIN G LEVELS IN PATIENTS WITH EXOCRINE PANCREATIC INSUFFICIENCY: IS AUTOIMMUNE PANCREATITIS A PLAUSIBLE AETIOLOGY?
J. S. Leeds1, R. Sidhu1, S. R. Morley2, D. S. Sanders1. 1Gastroenterology, 2Clinical Chemistry, Royal Hallamshire Hospital, Sheffield, UK
Introduction: Autoimmune pancreatitis (AIP) has been shown to account for chronic pancreatitis in around 5% of cases and can lead to exocrine pancreatic insufficiency (EPI). We have described associations between EPI and both coeliac disease and diarrhoea predominant irritable bowel syndrome (D-IBS). However, we have not previously assessed what the pathogenesis for EPI may be in these groups of patients. We therefore undertook a case-control analysis of immunoglobulin G (IgG) as a possible marker for AIP in patients with EPI.
Aims & Methods: Patients with coeliac disease (CD) and EPI (defined by serial low faecal elastase levels) were identified as were age and sex-matched controls (CD patients without EPI) (Group 1). We also used the same methodology for D-IBS patients along with age and sex-matched controls (Group 2). All patients had blood taken for total IgG level radiological imaging of the pancreas performed. Demographic details, the presence of autoantibodies and known autoimmune conditions were recorded.
Results: 74 patients were included in the study; 40 patients from group 1 mean age 54.7, 7 males (20 with EPI and 20 controls) and 34 patients from group 2 mean age 60.5, 7 males (17 with EPI and 17 controls). Total IgG level in all patients with EPI (n = 37, both CD with EPI and D-IBS with EPI) was 11.5 g/l vs 9.8 in controls (p = 0.002). In group 1 total IgG level was 11.5 in those with EPI and 9.9 in controls (p = 0.039) and in group 2 total IgG level was 11.6 in those with EPI vs 9.7 in controls (p = 0.018). There were also significantly more individuals with additional autoimmune diseases in those patients with EPI compared to controls (14 vs 3, Fisher’s exact test p = 0.004). 5/37 (13.5%) patients with EPI had abnormalities on cross sectional imaging (1 in group 1 and 4 in group 2) compared to 0/37 (0%) in the control group (p = 0.054).
Conclusion: These data suggest that patients with a EPI are more likely to have a higher IgG level and an increased number of autoimmune diseases by comparison to controls. Although these data do not confirm that the underlying pathophysiology for these individuals EPI is autoimmune in origin—this is a biologically plausible hypothesis which may deserve further evaluation. Prospective measurement of the IgG4 fraction or anti-carbonic anhydrase or lactoferrin antibodies would be of value in future studies.
CAFFEINE PROTECTS PANCREATIC ACINAR CELLS FROM BILE SALTS THROUGH PREVENTION OF MITOCHONDRIAL CA2+ OVERLOAD
J. Murphy1, E. W. McLaughlin1, D. Criddle2, J. P. Neoptolemos1, O. V. Gerasimenko2, A. V. Tepikin2, O. H. Petersen2, R. Sutton1. 1Surgery and Oncology, Royal Liverpool University Hospital, 2Physiology, University of Liverpool, Liverpool, UK
Introduction: Bile salts induce prolonged, global elevations of the free cytosolic ionised Ca2+ concentration ([Ca2+]C) that are toxic to pancreatic acinar cells, but the mechanism of injury has remained unclear.
Aims & Methods: We sought to determine the contribution of mitochondrial Ca2+ overload to pancreatic acinar cell injury from the bile salt taurolithocholic-3-sulphate (TLCS) and to discover whether caffeine, an inhibitor of inositol-trisphosphate-elicited Ca2+ release, is protective. Isolated mouse pancreatic acinar cells were examined by confocal microscopy to measure changes in [Ca2+]C (Fluo4-AM), mitochondrial function (NADH autofluorescence), ATP concentration (Mg Green) and cell fate (propidium iodide, PI). TLCS (200 μM) was perfused externally while whole-cell recordings of Ca2+ -dependent Cl- currents were made. All experiments were repeated at least six times, and in some experiments, supplementary ATP was added to the internal pipette solution.
Results: Neither pipette application nor an absence of supplementary ATP (0 mM) in the internal pipette solution induced necrosis. TLCS induced prolonged (>30 s), global [Ca2+]C elevations accompanied by NADH and ATP depletion, producing necrosis. Supplementary ATP (4 mM) in the internal pipette solution reduced the period of globalisation associated with each [Ca2+]C elevation and prevented necrosis, as did removal of Ca2+ from the external medium. Caffeine (20 mM) inhibited [Ca2+]C elevations and significantly reduced the frequency of necrosis.
Conclusion: Bile salts induce pancreatic acinar cell injury through Ca2+ overload from excessive inositol-trisphosphate receptor Ca2+ channel release, which causes mitochondrial inhibition. Bile salt toxicity is significantly reduced by caffeine.
CCK-8 DIRECTLY EVOKES EXOCYTOSIS IN HUMAN PANCREATIC ACINAR CELLS
E. W. McLaughlin1, J. A. Murphy1, D. Criddle2, M. Sherwood2, M. Chvanov2, J. Gerasimenko2, O. Gerasimenko2, M. Raraty1, P. Ghaneh1, J. P. Neoptolemos1, A. V. Tepikin2, O. H. Petersen2, R. Sutton1. 1Surgery and Oncology, Royal Liverpool University Hospital, 2Physiology, University of Liverpool, Liverpool, UK
Introduction: CCK and its analogues are used extensively in experimental models of pancreatitis in rodents, both in isolated cells and in vivo work. There is debate as to whether CCK acts only indirectly on human pancreatic acinar cells, via vagal nerve stimulation, or by direct CCK receptor activation, which could limit the applicability of rodent studies.
Aims & Methods: We have investigated whether CCK-8 directly elicits exocytosis in isolated human pancreatic acinar cells, as occurs in isolated murine pancreatic acinar cells. Freshly isolated, perfused human or murine pancreatic acinar cells were loaded with fluorescent dyes including quinacrine, an acidophilic dye preferentially taken up by secretory granules, that has been widely used to detect and quantify exocytosis from a variety of isolated cell types, including pancreatic acinar cells. Confocal microscopy was employed to measure spatiotemporal changes in quinacrine fluorescence, when perfused with physiological (2 pM, 10 pM) and hyperstimulatory (10 nM) concentrations of CCK-8.
Results: A prompt drop in quinacrine fluorescence was seen when murine pancreatic acinar cells were perfused with physiological concentrations of CCK-8 2 pM (n = 13) and 10 pM (n = 9). Similar decreases in quinacrine fluorescence were seen in isolated human pancreatic acinar cells, with a similar time course, in response to similar concentrations of CCK-8. These responses were accompanied by similar calcium signaling patterns. The responses occurred in the presence of atropine (to prevent possible stimulation via cholinergic nerve endings) and tetrodotoxin (to prevent non-cholinergic nerve stimulation). In both cell types responses to hyperstimulation with 10 nM CCK-8 were less pronounced than at physiological concentrations, in keeping with the reduction of secretion seen in rodent pancreatic acinar cells following hyperstimulation with secretagogues.
Conclusion: Our results show that when CCK-8 is applied to human and murine pancreatic acinar cells at physiological concentrations, both cell types display similar calcium signaling and subsequent prompt secretion of secretory granules. At supramaximal concentrations, however, secretion is reduced. These data underline the relevance of rodent models for human pancreatic disease.
INHIBITION OF THE MITOCHONDRIAL MEMBRANE PERMEABILITY TRANSITION PORE AFFECTS MURINE PANCREATIC ACINAR CELL RESPONSES TO BILE ACIDS
R. Mukherjee1, D. Criddle2, O. Petersen2, R. Sutton1. 1Division of Surgery and Oncology, Royal Liverpool University Hospital, 2MRC Secretory Physiology Group, University of Liverpool, Liverpool, UK
Introduction: Increasing evidence implicates mitochondrial inhibition from calcium overload as an important early component of pancreatitis. Toxins or hypoxia cause the inner mitochondrial membrane to become permeable to solutes <1500 Da through the mitochondrial permeability transition pore (MPTP), which may be important in pancreatic acinar cell necrosis.
Aims & Methods: We have investigated the role of the MPTP in pancreatic acinar cell responses to bile acids known to cause pancreatitis. Confocal fluorescence microscopy of freshly isolated, perfused murine pancreatic acinar cells was undertaken to measure changes of cytosolic calcium ([Ca2+]c: Fluo-4), NAD(P)H (autofluorescence, a measure of mitochondrial ATP production) and mitochondrial membrane potential (ΔΨm: TMRM). Cells were exposed to the bile acid taurolitholcholic acid 3-sulphate (TLC-S) with or without pre-treatment using 50 μM bongkrekic acid, known to inhibit the MPTP.
Results: 500 μM TLC-S induced a partial fall in ΔΨm (n = 14) that was further fully depolarised with 10 μM carbonyl cyanide m-chlorophenylhydrazone (CCCP), a protonophore that uncouples mitochondria. NADH levels initially increased on 500 μM TLC-S exposure but then underwent a sustained fall (n = 8). [Ca2+]c rapidly increased to a sustained elevation throughout the period of exposure to TLC-S, with a further subsequent rise on the addition of CCCP (n = 13). Bongkrekic acid pre-treatment of cells exposed to 500 μM TLC-S (1) greatly reduced the partial fall in ΔΨm in response to TLC-S (n = 17); (2) maintained NADH levels (n = 11); and (3) markedly reduced the magnitude of the rise in [Ca2+]c (n = 13); no further rise in [Ca2+]c was seen on the addition of 10 μM CCCP.
Conclusion: The effects of bongkrekic acid on the maintenance of pancreatic acinar mitochondrial function and cellular calcium handling implicate the MPTP as a contributor to mitochondrial injury from toxins known to cause pancreatitis, and suggest that the MPTP could be a potential therapeutic target.
FAECAL ELASTASE TESTING IN SECONDARY CARE: CLINICAL EVALUATION IN ADULT PATIENTS
E. J. Nowell1, W. Woltersdorf2, J. E. Smithson1. 1Department of Gastroenterology, 2Department of Clinical Chemistry, Bristol Royal Infirmary, Bristol, UK
Introduction: Faecal elastase (FE) testing is a simple indirect measure of pancreatic exocrine function. To date there have been few studies to assess its clinical use in unselected hospital patients.
Aims & Methods: The aim of this study was to define the clinical characteristics of adult patients with abnormal FE results in a secondary care setting. A retrospective case note analysis was undertaken of all patients tested over a 12-month period in a University hospital.
Results: 114 adults were tested of whom 25% (16 men and 12 women, mean age 63) had an abnormal faecal elastase result (<200 μg/g stool). Of these, all had diarrhoea, most described weight loss or were malnourished (76%), but fewer had suspected steatorrhoea (35%), typical pancreatic pain (33%) or a history of alcohol excess (15%). The prevalence of Types 1 and 2 diabetes was 26%. The only frequent abnormal marker of malabsorption was isolated hypoalbuminaemia (present in 48% of cases). In 30% of patients, idiopathic pancreatic insufficiency was considered to be the primary cause of their symptoms. Of the patients who were treated with enzyme supplementation, 10/12 responded with weight gain and/or improvement in diarrhoea.
Conclusion: Faecal elastase testing yields a high positive rate in secondary care and identifies individuals who respond well to enzyme supplementation. The clinical characteristics of patients with abnormal results differ from those which are classically associated with chronic pancreatitis. This may suggest that significant pancreatic insufficiency is underdiagnosed in hospital patients and should be considered in cases of unexplained diarrhoea.
DIAGNOSIS, MANAGEMENT AND SURVIVAL OF PANCREATIC ENDOCRINE TUMOURS
R. Srirajaskanthan1, L. Marelli1, N. Mendes1, A. Krepska1, A. Davidson1, C. Toumpanakis1, T. Meyer2, A. Mayer2, M. Caplin1. 1Gastroenterology, 2Oncology, Royal Free Hospital, London, UK
Introduction: Pancreatic neuroendocrine tumours (NETs) are uncommon tumours, with a reported incidence of 1 in 100 000 in the general population. They are subclassified as functional (hormonal syndrome) or non-functional (no hormonal syndrome). We describe the diagnosis and management in a case series of 121 patients with pancreatic NETs.
Aims & Methods: To define the optimal management pathway for pancreatic NET patients. This is a retrospective study of 121 patients (57 male: 47 female) mean age 44 years (range 16–79) with histologically proven pancreatic NET. Data were assessed using SPSS stats package.
Results: The majority were non-functioning (69%). The functional tumours include gastrinomas 12%, insulinomas 5%, VIPomas 4%, PTHrp secreting tumours 2%, somatostatinoma 2%, carcinoid tumour of the pancreas 1% and 1 case of a glucagonoma. The histology assessed thus far (n = 100), shows 48% well differentiated tumours; 39% moderately differentiated tumours and 13% are poorly differentiated tumours. The Ki67 proliferation index was available in 77 cases, of which 62% were <10% (lower grade); the remaining 38% of cases being >10% (high grade). Of the 108 patients that underwent octreotide scans, 84% (91 cases) showed positive uptake for known disease and 16% (18) showed no uptake. Sensitivity of octreotide scan was 84%, specificity of 100%. MIBG scans were performed in 18 patients of which only 8 (44%) were positive, sensitivity of MIBG scan was 44%. Chromogranin A results was available in 109 patients, raised in 56 patients with known disease and normal in 53 cases of whom only 5 has no evidence of disease. Sensitivity of CgA 50% and specificity was 91%. 47 patients underwent surgery, of which 36 were curative surgery and 11 were palliative procedures. Chemotherapy was first line therapy in 53 cases, most common regimen was FCiSt (5-flurouracil, cisplatin and streptozosin). 9 cases were treated with somatostatin analogues alone as first line therapy. In addition patients with functional tumours were commenced on somatostatin analogues for symptomatic control. Overall 1 and 5 year survival was 90% and 72% respectively. There was significantly worse survival between high grade (Ki67>20%) vs low grade (Ki67<10%) (p = 0.05). Patients treated with surgery as initial therapy had a significantly better survival than those given chemotherapy (p = 0.029).
Conclusion: The majority of pancreatic NETs are well or moderately differentiated tumours. Chromogranin A is not a sensitive marker of disease in pancreatic NET. Surgery remains the treatment of choice; however, a number of other palliative treatments are available. The 5-year survival in pancreatic NETs is much higher than in other types of pancreatic cancer.
Service development posters
IS ROUTINE SCREENING FOR COELIAC DISEASE OF VALUE IN PEOPLE WITH TYPE 1 DIABETES?
K. A. Adamson1, A. E. White2, J. Geddes3, B. M. Frier3, C. J. R. Goddard1, H. R. Gillett1, M. W. J. Strachan2. 1Medical Unit, St John’s Hospital, Livingston, 2Metabolic Unit, Western General Hospital, 3Department of Diabetes, Royal Infirmary of Edinburgh, Edinburgh, UK
Introduction: A screening programme to identify the presence of coeliac disease in patients with type 1 diabetes has recently been put in place in our area.
Aims & Methods: We aimed to assess patients views on screening through administration of a questionnaire. In addition a review of patients notes was performed to assess the impact of coeliac disease on clinical indices in these relatively asymptomatic patients.
Results: Out of a population of 2752 individuals with type 1 diabetes, 53 patients were identified with a positive screen for coeliac disease (minimum prevalence 1.9%). Thirty-five patients subsequently had a positive biopsy for coeliac disease. In 11 patients (20.8%), serum ferritin and in four patients (7.5%) serum folate, was below the normal range. Forty two per cent of those with histological confirmation of coeliac disease had a DEXA scan. Three patients (20% of those undergoing DEXA) were osteoporotic at one or more sites and six (40%) were osteopenic. A gluten-free diet (GFD) was followed by 58.5% of all antibody positive patients. Serum ferritin levels showed a significant improvement with a GFD (p<0.05). Prior to screening, 32% of patients were asymptomatic. Only a fifth of patients found no improvement in well-being with a GFD and in those who followed a strict GFD the improvement in well-being was greater (p = 0.034). Screening was felt to be beneficial by 73%. Response did not relate to GFD adherence but did relate to symptom improvement (p = 0.037).
Conclusion: These data show that patients report an improvement in well-being with treatment and feel that screening for coeliac disease is beneficial.
IMPROVING OUTCOME IN HEPATITIS C MANAGEMENT: A NEED FOR DEDICATED SERVICE FOR COMPLIANCE WITH NICE GUIDELINES
I. Ahmed, A. A. Naqvi. Gastroentrology, Diana Princess Of Wales Hospital, Grimsby, UK
Introduction: Hepatitis C virus is a major health-related problem worldwide with around 170 million people chronically infected. The combination of pegylated interferon and ribaverin has improved outcome in recent years. Poor compliance with treatment has been a major problem that results in significant dropout rates. A dedicated service and compliance with NICE guidelines might improve the success rate in treatment.
Aims & Methods: We restructured our regional hepatitis services in 2002 with a dedicated team which included hepatitis specialist nurse and a formal psychological support service to improve compliance with NICE guidelines. The aim of this audit was to asses the success rate of hepatitis C treatment pre- and post-NICE guidelines in our centre. The case notes of all patients who were referred to our regional hepatitis clinic with a diagnosis of hepatitis C between 1995 and 2006 were studied retrospectively. We divided them into two groups, Group A before 2002 (pre-NICE guidelines) and Group B after 2002 (post-guidelines).
Results: 80 patients were enrolled for treatment, 56 patients in group A and 23 patients in Group B. The median age in Group A was 40 (range 27–60) and 39 (range 20–72) in Group B respectively. 6 patients were excluded from study in group A simply because they did not attend the clinic at all. There was a significant dropout rate in patients treated pre-NICE guidelines and about 29 patients lost to follow-up, refused treatment at some point or DNA from clinic, while all patients in Group B completed the full course of treatment without any dropout. Of those who completed the treatment, only one patient failed treatment. The sustained virological response was 82% (19/23) in those treated after 2002 while in 3 patients no viral load was checked at 24 weeks post-treatment and they were lost to follow-up. In the pre-NICE group, only 20 out of 50 patients managed to complete the treatment and documented SVR was only 52% (11/20).
Conclusion: We conclude from this audit that a well-structured and dedicated service and compliance with NICE guidelines improve the success rate in hepatitis C management.
ARE OUR IN-PATIENTS READY FOR US?
V. J. Gokani, S. Clark, D. James, M. Stalker, A. B. Ballinger. Endoscopy Unit, Homerton University Hospital NHS Foundation Trust, London, UK
Introduction: Consent for endoscopy is a continuous process, which begins with the written information that a patient receives prior to their appointment, and continues on their admission when questions or concerns can be addressed. As a result of this process, patients should fully understand the indications for, and possible complications of endoscopy. We would expect out-patients to be fully informed at the time of their procedure as a result of one or more of: clinic visits, postal consent with information leaflet, dedicated telephone service for questions and answers, and adequate time between booking and procedure for these various measures. However, the consent process for in-patients may be very different in that endoscopy is often urgent, and booked and/or requested by a variety of medical teams.
Aims & Methods: The aim of this study was to determine if in-patients are adequately prepared for endoscopy and compare with out-patients. Consecutive in- and out-patients who attended for an upper or lower GI endoscopy were asked to complete a simple questionnaire after the procedure and after recovery from sedation. The questionnaire was designed to assess their experience of the consent process.
Results: The results are summarised in the table as a percentage of the patients in each group who answered “yes” to the questions, or in the case of awareness and risks of the procedure were able to describe these based on information contained in our standard patient information leaflets. Significant differences (p<0.05) existed in all categories between in-patients and out-patients.
Conclusion: Our study indicates that in-patients, who are often the sickest and most susceptible to the complications of endoscopy, are poorly prepared for the procedure. A random survey of five other London hospitals indicates that they also do not have a firm policy in place for the provision of information and consent process of in-patients. Since the survey we have instituted a endoscopy nurse liaison service to see each in-patient on the ward who is booked for endoscopy and enable them to understand the procedure by discussion and provision of written information.
ENTONOX: AN ALTERNATIVE ANALGESIC IN LOWER GI ENDOSCOPIES
B. Ahmed, J. Blackburn, A. Green, C. Grimley. Endoscopy Unit, Burnley General Hospital, Burnley, UK
Introduction: Intravenous sedation in lower GI endoscopy is associated with risks. Moreover patients need to be escorted home, cannot drive and need a presence of a responsible adult for 24 hours after the procedure. Randomised controlled trials show entonox to be a superior analgesic to intravenous sedation,1 with the added benefit of early return to daily activities. We conducted a prospective, nurse-led study on the efficacy of entonox as an analgesic on patients undergoing lower GI endoscopy.
Aims & Methods: Team members underwent training in the use of entonox. All patients undergoing lower GI endoscopy during a period of 5 months (Sep 2006–Jan 2007) were offered a choice between sedation and entonox and those opting for the latter were included. The variables collected were patient demographics, reasons for referrals, final diagnosis, procedure and recovery times, caecal intubation rate, patient satisfaction and overnight stay. Visual analogue scores (VAS) before, during and after the procedure were used to record the severity of pain. The data were collected and analysed on Microsoft Excel.
Results: 301 patients were included, 52% (157) of whom were males. The mean age was 60 years (15–101 years). 63 flexible sigmoidoscopy (FOS) were carried out all of which were done with entonox. 238 colonoscopy were done of which 215 (90%) were carried out using entonox. 23 (10%) required addition of sedation. Mean procedure times for FOS and COL were 14.1 min and 34.2 min while mean recovery times were 33.2 min and 39.4 min respectively. Caecal intubation rate was 92% (220). VAS revealed four pain categories. In category 1, pain remained controlled throughout the procedure. In category 2, a rise in pain was fully controlled by entonox. In category 3, a rise in pain was not fully controlled and in category 4, pain was not controlled at all. Successful pain control was achieved in 176 (82%) COL and 58 (92%) FOS (category 1 and 2). Ineffective pain control was seen in 39 (18%) COL and 5 (8%) FOS (category 3 and 4). Nausea was the only side effect (11%). 290 (96%) procedures were done as day case. Overnight stay was prevented in 16 (5%). 92% of the patients were satisfied.
Conclusion: Entonox is a safe and effective analgesic, achieving high patient satisfaction. It allowed early return of patients to their daily activities and maximised trust resources by preventing unnecessary hospital stay. Training of the staff and patient information played a vital role. A local trust policy is implemented that will allow the patients to have a choice of analgesia during endoscopy.
NACC INFLAMMATORY BOWEL DISEASE PATIENT PANELS
P. H. Canham, R. Driscoll. National Association for Colitis and Crohn’s Disease, 4 Beaumont House, St Albans, UK
Introduction: The current government believes that with the involvement of Patients and the Public the NHS will be able to deliver a more enhanced, patient centred service. To achieve this aim the UK Department of Health has produced guidance and performance targets (monitored by the Health Commission’s Annual Health Check). In 2005 NACC decided to test these opportunities to see what improvements (if any) could be introduced to local gastroenterological services through organised and structured IBD patient feedback.
Aims & Methods: The model NACC chose was that of a Patient “Forum” or “Panel”. These have a membership of patients with colitis or Crohn’s disease, all of whom attend the same hospital for their ongoing care. The patients offer both their experience and their aspirations on their local IBD service to their NHS professionals. This initiative came under the auspices of NACC’s IBD Health Service Committee. Six pilot sites were identified. NACC appointed a Patient Panel coordinator. After 12 months the Panels achievements were assessed using qualitative data: through the completion of a self evaluation questionnaire; through an assessment by NACC’s IBD Health Service Committee; through an audit conducted by the Patient Panel coordinator.
Results: Four out of 6 Patient Panels completed the self evaluation questionnaire. All 3 methodologies concluded that from a patient perspective, Panels could bring about improvements in IBD services. They also concluded that the NHS was generally receptive to Patient feedback. Examples of achievements included: the reopening of the Paediatric Gastroenterology Department to new patients at Nottingham University Hospital; the appointment of a part time IBD dietician at North Cumbria Acute Hospitals Trust; the reorganisation of IBD out patient clinics at Bradford; the introduction of fridges (so that IBD patients with can keep food which meets their individual dietary needs) on the Gastroenterology ward at Brighton’s Royal Sussex Hospital.
Conclusion: NACC Patient Panels proved themselves to be a powerful agent for change. Their achievements showed that by working in partnership with local health professionals, small numbers of committed patients can make a difference to the service offered to all. The improvements or changes brought about do not have to be great or expensive in order to make an impact on a patients’ personal experience of their local IBD service. The patient/professional dialogue raised the understanding of patients’ needs. Each panel’s strength lies in its uniqueness, their diversity enables them to influence their own particular local IBD service. NACC plans to develop more patient panels and has made them part of NACC’s core activities. The number of Patient Panels has doubled and there is a growing interest in their potential for developing the dialogue between Patient and Professional.
NEW FORMAT CLINIC FOR COELIAC DISEASE
G. R. Davies1, J. Ridpath1, J. Gale2. 1Gastroenterology, 2Dietetics, Harrogate District Hospital, Harrogate, UK
Introduction: BSG guidelines recommend long-term specialist follow-up for patients with coeliac disease (CD). Unlike most gastroenterology (GE) out-patients, those with CD usually feel well, are not ill, and are expert in the practical management of their condition. We felt there was a need to develop an alternative format clinic dedicated to CD management.
Aims & Methods: In 2004 we searched the GE department database to identify patients with CD, and invited them to transfer to the new style clinics. Subsequently we used additional case finding techniques (endoscopy and histopathology databases; direct requests to consultants, GPs and local branch of coeliac UK; local radio; public lectures). Quarterly evening clinics are run by the 2 GE consultants, GE SpR, and our CD specialist dietician. The evening setting allows us to commandeer a large area of out- patients so national and local specialist gluten-free (GF) product manufacturers and our local branch of Coeliac UK can attend This creates an informal and educational atmosphere where patients find it easy to network. Secretarial staff send out blood request forms in advance, including regular screening for associated conditions such as diabetes and liver disease. A proforma checklist is used to promote systematic review of key management points (for example, follow-up histology; bone density; coeliac UK membership; risks for family members; use of prepayment prescriptions for GF products).
Results: The two initial departmental survey identified 125 cases: by Oct 2007 we had recruited 219 (hospital catchment is 150 000). Of the initial 125: 25% had been lost to regular follow-up, most commonly unintentional/administrative errors: most have returned to regular review; 11% had no record of follow-up biopsy after establishing a GF diet: unintentional in around half, explained by patient refusal/diagnosis made at another hospital in the others; baseline bone density (BMD) was missing in 15%: of the cases who had a baseline and warranted follow-up it had been omitted in 9%; key management/knowledge gaps (for example, use of pre payment certificates for GF products) were identified in every patient; a patient survey after 1 year confirmed a strong preference for the new style clinics.
Conclusion: A surprisingly high percentage of CD patients had been lost to follow-up. Based on BSG guidelines, 10% had major, and 100% more minor omissions in management, all of which were easily improved using our proforma-based approach in the context of a specialised multidisciplinary clinic. This format is unique as far as we are aware, and offers a more appropriate service for this patient group than conventional GE out-patients. This model is easy to set up without additional staffing and budget resources.
VALIDATING THE ENDOSCOPIC INVESTIGATION OF IRON-DEFICIENCY ANAEMIA: SERVICE PROVISION IN AN ERA OF PAYMENT BY RESULTS
B. Hayee, S. Patel, J. O’Donohue, D. Reffitt. Gastroenterology, University Hospital Lewisham, London, UK
Introduction: British Society of Gastroenterology guidelines for the investigation of iron-deficiency anaemia (IDA) recommend an upper gastrointestinal (GI) endoscopy and either colonoscopy or barium enema unless malignancy or coeliac disease is found. In attempting to provide an efficient and cost-effective endoscopy service in light of these guidelines, “cut-off” criteria may be useful to reduce the number of inappropriate investigations.
Aims & Methods: To determine whether patients with IDA are appropriately referred and investigated and whether referral patterns could be improved, an audit was undertaken. Case notes were analysed for consecutive patients referred for endoscopic investigation of anaemia from February to April 2006. To determine the potential lost revenue from uninvestigated patients, those fulfilling study criteria were also identified from a Haematology database and case notes examined. Cost implications were identified. IDA was defined as a haemoglobin (Hb) level of <12.5 g/dl for men and <11.5 g/dl for women with either mean cell volume <76 fl or ferritin <15 μg/l (or <50 if ESR raised). Patients with low Hb not fulfilling the criteria were termed “non-IDA”. A series of measures including referral form design were enacted and data re-audited prospectively from April to June 2007.
Results: In period 1, 118 patients (52F) were referred and investigated; 66 (56.9%) had non-IDA. The estimated annual cost of these inappropriate referrals is £155,787. 37 patients (30 F) were identified from the haematology database with undoubted IDA but not referred with potential lost annual revenue of £231,478. In period 2, 103 (67F) patients were referred, with inappropriate referrals significantly reduced (43 patients; 41.7%, p<0.05). In terms of avoiding inappropriate investigations, this represents an estimated annual cost saving of £54,290.
Conclusion: Many patients with anaemia are unnecessarily referred for investigation, but it is possible to improve this referral pattern using simple measures with significant financial implications. The application of specific criteria to determine which patients should be investigated appears useful in this regard.
BH and SP contributed equally to this work.
OPEN-ACCESS DYSPHAGIA SERVICE
P. Kant, P. Sahay. Gastroenterology, Pontefract General Infirmary, Pontefract, UK
Introduction: Dysphagia is a symptom requiring urgent investigation to exclude malignancy. This has led to a large volume of referrals for endoscopy (OGD), clinic appointments and long waiting lists. While OGD is the definitive test for detecting endoluminal oesophageal lesions it is invasive and widely accepted that barium swallow (BS) could precede it. It is known to be superior in demonstrating motility disorders and a normal double contrast BS virtually excludes the presence of oesophageal neoplasia.1 2
Aims & Methods: We evaluated our current practice by conducting two pilot studies with the aim of creating an open access dysphagia service. In the initial study, GP referrals for dysphagia were sent directly for a BS. Patients with abnormal or equivocal results were sent for urgent OGD. In the second study all GP referrals over a 15 month period were sent for both BS followed by OGD.
Results: In the first study, 120 patients had BS. 104 (87%) were clinically insignificant (negative). 16 (13%) had abnormal reports needing OGD. Of these, 8 had suspected malignancy, of which 2 were confirmed by OGD. None of the negative BS patients developed cancer. In the second study of 35 patients; after BS 30 (86%) patients were normal; 5 (14%) patients had clinically suspicious lesions. Of these, endoscopy confirmed 2 to be malignant. After OGD the other 33 were clinically insignificant. Mean time from referral to BS was 34 days, and from BS to OGD 32 days, giving an overall mean time from referral to OGD of 65 days. Our studies show that a drastic reduction in waiting times can be achieved by GPs referring directly for BS as our pilot studies highlighted the exclusion value of a negative BS. In the first study, the 104 patients reported as normal utilised approximately 13 clinics. If these patients were not seen, it would equate to a reduction in clinic waiting time of 3 months alone (8 new patients per clinic). In our second study, both malignant lesions were seen on BS and were confirmed on histology as squamous cell carcinoma. Importantly, no significant lesions seen at OGD were missed after BS and hence 86% of OGDs could be avoided.
Conclusion: Our studies show that only a small proportion of referrals for dysphagia lead to a diagnosis of cancer. GPs can safely investigate dysphagia by open-access BS. This would involve urgent referral for BS whereupon suspicious reports would be fast tracked and urgent OGD organised within 2 weeks. This would greatly reduce management waiting times for dysphagia, avoiding many inappropriate OGDs, and reduce clinic waiting times.
IS THERE A DIFFERENCE IN TIME TAKEN FOR IN-PATIENT AND OUT-PATIENT ENDOSCOPY?
C. S. Kothari, A. Ramdass, R. D. Souza, N. van Someren, K. Besherdas. Gastroenterology, Chase Farm Hospital, Enfield, UK
Introduction: Planning of endoscopy lists are important in order to ensure waiting times are achieved. This will become more important in delivering the 18 week waiting time target. The time allocated for endoscopic procedures between in-patients and out-patients is not differentiated in the document by Royal College of Physicians of London Consultant Physicians Working for Patients, third edition (January 2005; Section on Gastroenterology). Current hospital allocation times for in-patients and out-patients for endoscopy is the same. As in-patients are generally more unwell and may have multiple pathologies, endoscopy in them may be likely to take longer to perform. To date this has not been documented. Allocation of time for procedures is also important for endoscopy units in the “timeliness” arm of the Global Rating Score, as in-patients may require to be allotted a longer time slot.
Aims & Methods: To analyse the difference in time taken to perform in-patient against out-patient endoscopies. A retrospective analysis from a single centre (associate teaching hospital) of 1000 endoscopies was taken. The data of time to perform procedure (inclusive of consent and bring patient into the room, performing the procedure, and thereafter all documentation including the report and histology forms) were obtained from the procedure logbook. The findings at procedure were obtained from the endoscopy reporting software programme, Unisoft.
Results: There were 547 female and 453 males: mean age 44.4 (range 18–97). Please refer to the table for details. Also, an abnormality at endoscopy was detected in 150 in-patients (49.50%), versus 290 out-patients (41.60%). Moreover, endoscopic therapy was given to 80 in-patients out of total 303 endoscopies (26.40%), versus 96 endoscopic therapies given to out-patients, total out-patients being 697 (13.77%).
Conclusion: In this study inpatient endoscopies overall take longer to perform than out-patient endoscopies. To perform an in-patient gastroscopy, an average of 10 more minutes are required than an out-patient gastroscopy. To perform an in-patient colonoscopy, an average of 10 more minutes are required than an out-patient colonoscopy. We recommend that a longer time be allocated for in-patients on the endoscopy template. In addition this study demonstrates that there is a greater likelihood for inpatients in having pathology and therapeutic intervention at endoscopy than those attending for out-patient endoscopy.
ANOTHER NAIL IN THE COFFIN FOR BARIUM ENEMA?
G. W. Moran, S. Nizam, C. Angit, J. R. B. Green. Department of Gastroenterology, University Hospital North Staffordshire, Stoke-on-Trent, UK
Introduction: Colonoscopy is the gold standard in diagnosing colorectal cancer. Considerable variation still exists in this diagnostic pathway.
Aims & Methods: Analysis of the quality of our diagnostic services was carried out. A retrospective analysis of all colorectal cancer diagnosed from January 2005 to February 2007 was carried out. All colonic examinations during the 2 years prior to diagnosis were analysed.
Results: Of 293 cases of colorectal cancer diagnosed during the study period, 9 patients (3.1%) had a falsely negative colonic examination up to 2 years prior to diagnosis, 6 of these examinations within 12 months of subsequent diagnosis. Average age was 73.55 years. The table shows the relevant details. No patient had had a falsely negative colonoscopy. Barium enema and flexible sigmoidoscopy had a similar percentage of false negativity. This created a diagnostic time lag of 9.6 months (1–17) in the patients concerned before the correct diagnosis was made in these 9 patients. 67% of the undetected pathology was left sided including all the cancers undetected by sigmoidoscopy (all performed by consultants). For barium enema, pathology was distributed equally. 44.4% of the patients died and 75% of them within 2 months of diagnosis.
Conclusion: Is a negative Barium enema still reassuring in a patient referred with symptoms suggestive of colonic malignancy in the light of these findings? Certainly these findings suggest not. The patient morbidity and mortality incurred by such misdiagnoses is alarming. More gastroenterology departments across the country should assume colonoscopy as their primary investigation in such presentations.
WIRELESS CAPSULE ENDOSCOPY: IS IT TIME BSG CHANGED ITS GUIDELINES?
S. V. Murugesan, J. Preston, S. Campbell. Gastroenterology, Manchester Royal Infirmary, Manchester, UK
Introduction: Wireless capsule endoscopy (WCE) has been well established as a method of investigating the small bowel. Its current role in the investigation of iron deficiency anaemia is in patients who have had negative gastroscopy and colonoscopy and are transfusion dependant (BSG Guidelines).1 Small bowel radiology (SBR) has been described as the current standard for investigating the small bowel in patients with suspected small bowel Crohn’s disease,2 although several studies have shown that WCE is more sensitive in investigating the small bowel. NICE recommends using WCE for obscure GI bleeding.
Aims & Methods: There are no current up-to-date guidelines for the use of WCE either locally or nationally. We reviewed all WCE performed at our hospital with a view to establishing a local protocol for the appropriate use of this service. Retrospective analysis of all WCE performed from the commencement of this service (March–October 2007). We aimed to review clinical indications, complication rates, diagnostic yield and altered management as a result of WCE and hence to refine a protocol to increase this yield.
Results: A total of 44 WCEs were performed. Indications included Group I (25): obscure GI bleeding (44%), iron deficiency anaemia (56%); 8 had coagulation disorders; Group II (17): suspected small bowel Crohn’s (56%) and Group III (2): Crohn’s disease assessment (5%). In ∼92% of patients, bowel prep was deemed adequate for WCE and in only 2 patients was the caecum not identified. Of the 25 patients investigated for either IDA or obscure GI bleeding (GP I) a cause was found in 10 (40%). Among the 7 patients with coagulation disorders, a cause was found in 5 (83.3%). In GP II only one patient had a positive finding on WCE. WCE changed immediate management of 10 patients (23%). No complications were recorded.
Conclusion: WCE is a safe procedure. Our audit confirms that diagnostic yield is good but also (and more importantly) it changes management in approximately up to a third of patients. In select patients (especially those with coagulopathy, prion disease), WCE may have a place much earlier in the investigation algorithm than is currently in the BSG guidelines. Patient selection is essential when using WCE for the investigation of suspected small bowel Crohn’s. We have therefore introduced a protocol to streamline the service and will be shortly reviewed to complete this audit cycle. Results will be available by the BSG meeting.
CAN ROUTINELY COLLECTED HOSPITAL STATISTICS PREDICT MORTALITY IN PATIENTS WITH ACUTE UPPER GASTROINTESTINAL HAEMORRHAGE?
P. Sakellariou1, R. Sidhu1, D. S. Sanders1, G. Fothergill2, A. J. Lobo1. 1Gastroenterology Unit, 2Clinical Operations, Royal Hallamshire Hospital, Sheffield, UK
Introduction: Clinical outcome data are increasingly used to measure clinical performance of organisations and individuals. The Rockall score is a validated assessment of risk of death in patients with acute upper gastrointestinal haemorrhage (AUGIH). However, its routine collection requires appropriate processes. All hospitals routinely collect statistics on in-patient activity. The “Dr Foster” TM database is an organisational tool currently used by a large number (50%) of acute hospital trusts and PCTs. Using data from the Department of Health Hospital Episode Statistics (HES) database, information on selected outcomes (mortality, readmission, length of stay) is provided and compared with national data.
Aims & Methods: To compare in patients with AUGIH admitted to a gastrointestinal haemorrhage unit the predicted mortality, calculated by Rockall score, with the estimated risk of mortality from routinely collected hospital data. 255 consecutive admissions with AUGIH to the gastrointestinal haemorrhage unit at a single university teaching hospital were studied from January 2005 to December 2006. The median age (range) was 61.5 years (17 to 90) and 148 (58%) patients were male. Initial (pre-) and final (post-endoscopy) Rockall scores and Charlson comorbidity index were calculated from the notes. Corresponding risk of death and comorbidity scores were identified on the routine hospital statistic database (Dr Foster TM, Real Time Monitoring (RTM)). The RTM mortality risk is standardised according to age, sex, deprivation, primary diagnosis, primary procedure, comorbidities and method of admission. Rockall estimated risk of death and RTM mortality risk from routine data were compared (Spearman rho (SPSS v12)), as was investigator calculated and hospital recorded Charlson Index.
Results: Only 164 (64.5%) of admissions were identifiable on RTM, the median age (61.5 and 61), Rockall scores (3 and 3) and investigator-calculated comorbidity (1 and 1) were comparable between this group and the whole cohort. Both initial and complete Rockall scores correlated poorly with the RTM mortality risk (r = 0.31, p<0.001 and r = 0.28, p<0.001 respectively). Calculated and RTM comorbidity correlated poorly (r = 0.32, p<0.001). In the subgroup with the same calculated and the RTM comorbidity, correlation between Rockall estimated risk and RTM mortality risk improved (r = 0.56), but remained poor, indicating that the initial poor correlation was not just due to recording of comorbidity.
Conclusion: Nationally used routine hospital data may not be as reliable a measure of case-mix adjusted mortality in AUGIH as validated, specific scoring systems, and should be interpreted with caution as a measure of clinical performance.
PRELIMINARY RESULTS FROM A “VIRTUAL” GASTROENTEROLOGY OUT-PATIENT CLINIC
O. R. Saraj1, V. Talwar2, R. Robinson1. 1Digestive Disease Centre, University Hospitals of Leicester, Leicester General Hospital, Leicester, 2Gastroenterology, Peterborough District Hospital, Peterborough, UK
Introduction: Government initiatives are putting increasing pressure on secondary care to improve out-patient (OPD) efficiency. Many specialists routinely offer their new patients a follow-up OPD appointment where results can be reviewed. This system ensures that no results are overlooked. However, “paper”clinics in which investigations are reviewed without the patient attending have been used successfully in other specialities,1 reducing the need for unnecessary follow-up. The aim of this study was to evaluate whether such a clinic was practical in gastroenterology.
Aims & Methods: All patients attending gastroenterology OPD were eligible after discussion with the consultant. Investigations were requested, a comprehensive letter dictated and a “virtual” clinic proforma completed detailing the tests requested. A review date was given to the patient. The “virtual” clinics are consultant-led and held twice monthly. All investigations are reviewed with the original clinic annotation; a letter detailing the final diagnosis and outcome is then sent to both patient and GP. Patients can be discharged, further investigations arranged, out-patient review requested or referred to another speciality.
Results: During the last 7 months, 100 patients (59 new referrals) have been reviewed in 14 “virtual” clinics. Presenting symptoms included: dyspepsia/upper GI symptoms (19), IBS/diarrhoea/constipation (36), anaemia (13), abdominal pain (9), malabsorption/weight loss (9), IBD (4), deranged liver function tests (5), misc (5). Eighty six of these patients (54 (92%) of new referrals) were discharged from the “virtual” clinic, 3 were referred to another specialist, 9 required further follow-up in outpatients, 2 required further investigations and were offered further “virtual” clinic review.
Conclusion: Initial results suggest that many GI patients are suitable for “virtual” clinic review and it is likely that such a clinic can be used to increase the efficiency of gastroenterology outpatients by reducing the number of follow-up consultations. The “virtual” clinic ensures that results are not overlooked. Long-term follow-up is required and patients’ satisfaction with the service should be sought.
MOVIPREP IS AS EFFECTIVE AS AN INTENSIFIED PICOLAX REGIME (3 SACHETS) IN BOWEL PREPARATION AND YIELDS A 90% COMPLETION RATE FOR IN-PATIENTS UNDERGOING COLONOSCOPY
J. Shome, W. Azim, K. Bodger, S. Sarkar. Digestive Disease Centre, University Hospitals Aintree, Liverpool, UK
Introduction: Optimal bowel preparation is critical for good quality colonoscopy. Previous audits in our unit have highlighted that in-patient (elective and non-elective) bowel preparation was particularly poor and consequently, unit protocol changed in the use of Picolax (Sodium picosulphate) as bowel cleaning agent from the recommended 2 sachets to a more intensified 3 sachets regimen. Moviprep (PEG 3350+ ascorbic acid), is a newly licensed bowel cleansing agent with potential advantages of better tolerability and an improvement in the overall patient experience of colonoscopy.
Aims & Methods: To compare the effectiveness of Moviprep with the intensified regime of Picolax (3 sachets) with as an in-patient bowel cleaning agent for colonoscopy. 60 in-patients (elective and non-elective) given either Moviprep (n = 30) or an intensified Picolax regime (n = 30) as a bowel cleaning agent for colonoscopy was prospectively audited using a standardised proforma complete by reviewing the case notes and the Unisoft endoscopy reports. In addition, 10 patients from each group were given standardised questionnaires about their overall experience.
Results: Colonoscopy completion rate was 90% for the Moviprep group and 83% for Picolax group (p = 0.4). The sedation doses used were similar in both groups (Midazolam Dose 2.4 vs 2.0 mg, Fentanyl 54 vs 57 μg for Moviprep vs Picolax respectively). The quality of bowel preparation rated by the endoscopists was similar with verbal ratings of “Satisfactory” or “Good” of 70% in both groups, although there was a greater proportion rated as “Good” in the Moviprep group. Patient tolerability was similar in both groups, although the Moviprep group experienced less nausea but more flatulence and thirst. The colonoscopy experience rated by patients was good in both groups with scores of 4.1 and 4.0 (on a 5 point scale; 0; awful to 5; excellent) for the experience and 3.9 for each group for whether patients would have repeat procedure (0; never to 5; definitely) for Moviprep and Picolax respectively. The only complication recorded was failure of completion and there was 0% post-procedure 30-day mortality.
Conclusion: Moviprep was equivalent to the intense Picolax regime (3 sachets) as an in-patient bowel cleaning agent with a 90% examination completion rate. Consequently, our unit is now reviewing the cost implications of considering Moviprep as the bowel cleansing agent of chose for in-patient (elective and non-elective) colonoscopy.
THE IMPACT OF CROSS SPECIALITY IN-PATIENT SUPPORT SERVICES ON GASTROENTEROLOGY
K. Teahon, S. Gamble, L. Clark, W. Roome, T. Hill, P. Hagan, T. Buchannon. Digestive Diseases and Thoracic, Nottingham University Hospital, Nottingham, UK
Introduction: Every year since 1997 all NHS organisations report to the Department of Health on the cost of care for their Healthcare Resource Groups. The data are then used to determine the National tariff for the Payment by Result (PbR) programme. As the NHS moves from local prices to national tariffs, those in-patient specialties which provide cross-specialty support or procedures are at risk of financial instability unless such work can be identified, costed and monies directed into the correct internal financial streams. Gastroenterology, in its provision of consultation, procedure and nurse specialist services, is one such at-risk specialty. Nottingham City Hospital provides a tertiary referral and a DGH function. Ten years ago, we introduced an in-house electronic system for cross-specialty orders of all consultations, endoscopies and nurse specialist services. We now report on the extent of clinical activity involved in this type of service.
Aims & Methods: Data collection is “live” and all service requests are made using the in house electronic system (HISS and NotIS). All requests contain the patient demographics and request type is identified by unique codes: Consultations, Clinical Nurse Specialist Services (Alcohol liaison, Diarrhoea, IBD, Nutrition), OGD, ERCP, Colonoscopy and Sigmoidoscopy. Each unique code has a number of subcodes (Urgency, Reason for referral, Referring consultant and service). The data generated can then by interrogated by an Oracle based programme (QUIZ). Activity and trend charts are generated for any data item or group of items selected.
Results: In the 10-year period there have been 7700 non-endoscopy service requests. Analysis of the consultation service is presented and there were between 400 and 650 referrals for in-patient consultations each year. The commonest reasons for referral are Nutrition, Diarrhoea, GI bleed and Jaundice. Referrals for diarrhoeal illness and nutrition have doubled since 2001. General medicine and surgery are the commonest sources of referrals but an increasing number have come from the subspecialties (cardiac, renal and oncology). This activity equates to the number of new patients seen in a year by one consultant doing 3 clinics each week. Once activity from in-patient endoscopy is included then the cross-specialty support service for this Trust equates to 0.5 wte gastroenterologist. In addition the cross-specialty workload of the clinical nurse specialists in our service currently equates to 1.5 wte senior nurse. As PbR is currently structured it is not clear how the funding for these services will be identified.
Conclusion: In-patient cross specialty support services are a significant financial burden for gastroenterology. To ensure financial stability these activities and the funding streams need to be identified.
LONG-TERM FOLLOW-UP OF INFLAMMATORY BOWEL DISEASE: WHAT DO PATIENTS WANT?
J. R. Thiagarajah, P. Neild, R. Pollock, J. Y. Kang, A. Poullis. Department of Gastroenterology, St George’s Hospital, London, UK
Introduction: Current NHS policy on the management of chronic diseases has begun to shift the provision of care away from hospital-based services toward community-based services. This is based on research suggesting that poor management of chronic diseases leads to wasteful and costly use of high intensity resources, which may be prevented by suitable strengthening of community-based care. Currently inflammatory bowel disease (IBD) patients are mainly managed in specialist hospital-based out-patients clinics. Patient wishes clearly should be taken into consideration in deciding follow-up. A questionnaire-based study was undertaken to find out patient views on where and how IBD patients would like their condition to be managed.
Aims & Methods: 91 patients were recruited in IBD out-patients clinic at St George’s Hospital and completed a 37-item self-administered survey.
Results: 96% of patients did not want to be discharged back to primary care. Increasing time since diagnosis seemed to move choice away from specialist care toward community management (of those with disease duration <5 years 48% wanted secondary care management only, this dropped to 27% in those with disease duration >10 years). Hospital specialists remained the choice for symptomatic periods (89%). Patients also were generally happier with the care received in secondary care versus the primary (93% satisfied vs 59%). When surveyed on possibilities for the future there was interest particularly in hospital specialists in the GP surgery and telephone clinics and helplines.
Conclusion: Overall, patients expressed a general preference for hospital specialist based care particularly among those with newer disease and more hospital appointments. However, there was also considerable interest in specialist services (both doctor and nurse run) in the community.
AUDITING THE PROVISION OF HEPATOCELLULAR CARCINOMA SURVEILLANCE IN PATIENTS WITH LIVER CIRRHOSIS AT BRISTOL ROYAL INFIRMARY
L. M. Walker, M. Callaway, H. Roach, F. Gordon, A. McCune, P. Collins. Department of Digestive Diseases, Bristol Royal Infirmary, Bristol, UK
Introduction: The incidence of hepatocellular carcinoma (HCC) is increasing worldwide. Most cases occur in the context of cirrhosis and it is becoming widespread practice to screen these patients, following guidelines produced by British Society of Gastroenterology (BSG), the American and European Liver Associations. Screening is non-invasive, relatively cheap and has a high sensitivity/specificity. The most cost-effective method comprises of six-monthly ultrasound scans with measurement of alpha-feto protein (AFP). HCC screening at BRI has been undertaken on an ad hoc basis and never formalised, so it was unclear whether patients had been receiving adequate surveillance.
Aims & Methods: To conduct a retrospective audit of provision of HCC screening according to BSG guidelines and assess the impact on local radiological services of more stringent adherence to these guidelines in the future. A random sample of cirrhotic patients’ case notes were selected from the Hepatology department’s patient database in May 2007. The notes were scrutinised to assess diagnoses, age, gender, presence of HCC, date of last AFP and last ultrasound. The total number of screening ultrasounds and AFP measurements 6 months prior to May 2007 was recorded also for the sample group. BSG guidelines were used to assess suitability of the screening. As the BRI acts as the local GI cancer MDT centre, HCC patients referred from other centres were excluded to prevent bias.
Results: 120 patients with cirrhosis were selected with mean age 57 years (range 25–84). Most patients were male (64%). Alcoholic liver disease predominated (63%), and of these patients only 34% were recorded to be abstinent when reviewed. In total 53 patients (44%) were eligible for screening using BSG guidelines, of whom 7 (13%) were not adequately screened. In the preceding 6-month period, 62 ultrasound scans were performed and 70 AFP measurements were taken. In this cohort, 14 patients had a diagnosis of HCC, of which 6 were discovered by screening.
Conclusion: The lack of a formal screening infrastructure, resulted in unnecessary use of radiology and biochemistry services (9 extra scans and 17 blood tests) in patients ineligible for screening. By contrast, applying the audit’s findings to our unit’s cirrhosis cohort of 250 patients predicts a 77% increase in annual investigations (220 scans and blood tests). Despite our population being considered relatively low risk for the development of HCC (predominantly alcohol rather than viral hepatitis) even non-systematic screening led to a diagnosis of HCC in 6 patients (estimated annual incidence 5%). The incidence of the disease in our audit suggest that a formalised screening programme would be of benefit in our urban population—but this will require significant extra resources.
A RETROSPECTIVE AUDIT OF THE APPROPRIATENESS OF COLONOSCOPY AS FIRST LINE INVESTIGATION IN THE ELDERLY
M. A. Zubir, A. Ansari, J. D. Sanderson, M. Mccarthy. Department of Gastroenterology, Guy’s and St Thomas’ Hospital NHS Foundation Trust, London, UK
Introduction: Our two objectives were firstly to examine the safety, rates of caecal intubation and diagnostic yield of pathology in those over the age of 70 years undergoing colonoscopy. Secondly to determine what percentage of diagnoses would have been reached by alternative investigations such as CT pneumocolon alone, thereby avoiding unnecessary colonoscopy.
Aims & Methods: This was a retrospective study of 252 consecutive colonoscopies performed in elderly patients older than 70 years over a 3-month period (between July–September 2006) in a single unit. The data obtained were analysed for primary indication for colonoscopy, sedation doses, caecal intubation rates, pathology encountered and any complications during the procedures.
Results: The number of patients undergoing colonoscopy was n = 252 (males 126, females 126) with a mean age of 77 years (70–93 years). The mean dose of Midazolam used was 2.6 mg (1–5 mg), mean dose for pethidine was 42.4 mg (25–50 mg) and mean dose for Fentanyl was 64 μg (25–50 μg). Antispasmodics were used in 12 patients only. The primary indications for colonoscopy were altered bowel habit n = 74 (29.3%), anaemia n = 59 (23.4%), rectal bleeding n = 43(17.1%), colitis surveillance n = 21 (8.3%), polyps surveillance n = 21 (8.3%) and abdominal pain and weight loss n = 33 (13.6%). Carcinoma were identified in n = 23 patients (9%), polyps in n = 50 (20%), angiodysplasia in n = 8 (3%), colitis in n = 14 (6%) and n = 55 (22%) had diverticular disease. Overall 40% were normal colonoscopies. There were 36 polypectomy, 9 hot biopsies and 4 APC performed. Bowel preparation was described as good in 96 (38%) patients and poor in 59 (23.4%) patients. The rest were described as satisfactory. Caecal intubation rate was 80%. There were no immediate complications related to the procedures. The reason for incomplete colonoscopy were because of poor bowel preparation in n = 14 (28%), looping and bowel redundancy n = 12 (24%), diverticular disease n = 10 (20%), pathology encountered n = 10 (20%) and patient discomfort n = 4 (8%). 62% of patients whom caecal intubation failed secondary to poor bowel preparation were in-patients. In patients with incomplete colonoscopy, (n = 50) two further colonic carcinomas were picked up at later radiological investigation (4% pick up rate of significant pathology not found on colonoscopy).
Conclusion: While our results indicate satisfactory levels of safety and diagnostic yield of pathology (60% detected significant pathology), these results also show poorer caecal intubation rates than expected due mainly to poor bowel prep in the inpatient population. It also reflects that a considerable number of colonoscopies n = 157 (62%) could have been avoided by doing CT pneumocolon as first line investigation for the majority of indications.
Small bowel posters
HOW ROBUST ARE THE 2007 BSG GUIDELINES FOR OSTEOPOROSIS IN COELIAC DIEASE?
I. Amin1, K. L. Hicklin2, J. D. McNally2, A. Mee1, S. Ghataura3. 1Gastroenterology, 2Rheumatology, 3Histopathology, Royal Berkshire Hospital NHS Trust, Reading, UK
Introduction: Coeliac disease is well recognised as being associated with osteoporosis. There is a definite but modest increased risk of fracture in coeliac disease. Screening and treatment for osteoporosis aims to reduce fracture risk. New guidelines have recently been issued by the BSG for measuring bone density in patients with newly diagnosed coeliac disease. Rather than measuring BMD in all newly diagnosed coeliac patients a more targeted approach is recommended advising DXA in patients with 2 or more risk factors thought to be associated with a high risk of osteoporosis. These include BMI<20 kg/m2, weight loss of >10%, age >70 and persistent symptoms or poor adherence to GFD.
Aims & Methods: To examine impact of the new BSG guidance on the identification of osteoporosis in newly diagnosed adult coeliac disease and to look at clinical and demographic factors that may provide improved identification of high-risk patients. 100 consecutive patients with a new diagnosis of Coeliac disease who had been referred for BMD examination were identified on the NHS DXA database with a median time from diagnosis to DXA of 3 months (range 1–11 m). Scan data provided T-scores and Z-scores at the neck of femur and lumbar spine and also confirmed BMI. Retrospective review of hospital notes provided symptoms at presentation, endoscopy findings and date of diagnosis. Histology was reviewed and graded by a single observer. The effect on BMD of sex, age, BMI, presentation and degree of villous atrophy was assessed.
Results: 100 patients were identified (73% were female and 27% male)with a mean patient age of 47 (range 21–79). The median BMI of those studied was 24 (range 15.8–42.9 kg/m2) with 12% of all patients having BMI <20. Osteoporosis was diagnosed in 9% of all patients (3% hip and 7% spine). 6.8% of women with coeliac disease had osteoporosis at presentation compared to 14.8% in men. Male patients had strikingly lower BMD at all ages. 33% of patients with BMI <20 and only 5% with BMI >20 were diagnosed with osteoporosis. By following new BSG guidance only 7 out of 100 patients would have been offered BMD measurement at initial diagnosis. In our study population 75% of males diagnosed with osteoporosis were under 70, all of whom had a BMI >20 (mean 22.17), suggesting that 75% male patients would be missed if current guidelines were applied. No further patients with osteoporosis would be identified if only 1 criterion allowed for BMD measurement.
Conclusion: Using the BSG 2007 criteria for DEXA scanning we may miss patients who would benefit from treatment or reinforcement of lifestyle advice before further monitoring of their response to diet. The age cut-off of 70 used in the current BSG guideline may not be applicable for male coeliac population.
PATIENTS OF SOUTH EAST ASIAN ORIGIN WITH COELIAC DISEASE: A RETROSPECTIVE CASE-CONTROL STUDY OF ATTENDANCE AND OUTCOMES COMPARED WITH CAUCASIANS
N. Chandra, N. Imrit, D. A. Gorard, A. S. McIntyre. Gastroenterology, Wycombe Hospital, High Wycombe, UK
Introduction: For patients with coeliac disease, the gluten-free diet (GFD) is challenging and failure to comply results in persistence of symptoms and a greater risk of complications. We have observed an increase in patients of South East Asian origin with the diagnosis and speculated that their response to management may differ from our classical Caucasian population.
Aims & Methods: To compare clinical outcomes and attendance rates of Asian with Caucasian coeliacs. We conducted a retrospective case-control (matched for age, sex, age at diagnosis) study. Demographic details and symptom profile were recorded at presentation. Symptomatic response (0-no, 1-partial, 2-complete improvement) and clinical response (using a score from weight gain-1, lack of anaemia-1, serological or histological improvement-1, compliance-1, possible range 0–4) were assessed at 24 (±6) months. Attendance at dietician-led (score 0-no, 1-partial, 2-full attendance) and GI (% of appointments attended) clinic were also recorded. Data were compared using paired t tests.
Results: Twenty Asian patients (11 females, mean age 39 years) were identified and compared with 20 Caucasian patients (11 female, mean age 40 years). There was a non-significant trend for Asians to present with anaemia (30 vs 10%) and weight loss (35 vs 20%). Presentation with diarrhoea (40 vs 45%) and abdominal pain (55 vs 50%) were similar in both groups. By 24 months, the Asian cohort was less likely to report an improvement in their symptom profile (score 1.5 vs 1.95, p<0.05). Clinical response was significantly lower in Asians than Caucasians (score 2.05 vs 3.9, p<0.001). Twelve (60%) Asian patients failed to demonstrate either a serological or histological improvement after 2 years of advice on a GFD. Eight (40%) Asian patients were anaemic and 6 (30%) continued to lose weight after 2 years. Dietician-led clinics were less well attended by Asian coeliacs (1.3 vs 1.85, p<0.05). There was no difference in the attendance rates at the GI clinic (Asians 88% vs 93%, p = NS).
Conclusion: Coeliac patients of South East Asian origin appear to be less compliant than Caucasians with a strict GFD. They are also less likely to demonstrate a symptomatic or clinical response. While doctor-led clinics are well attended, this is not the case for dietician-led clinics. Numerous cultural, social and communication-based factors are likely to account for these differences. Once these are better understood and addressed the outcomes for Asians diagnosed with coeliac disease should improve.
CHANGING PATTERNS OF COELIAC SEROLOGY REQUESTS
K. E. Evans, A. R. Malloy, D. A. Gorard. Gastroenterology Department, Wycombe Hospital, High Wycombe, UK
Introduction: The availability of accurate serological tests has revolutionised the diagnosis of coeliac disease. We examined requests for coeliac serology at our hospital laboratory over a period of 10 years, to quantify the volume of requests, identify where requests are originating from, and assess positivity rates and subsequent biopsy rates.
Aims & Methods: Details of all patients in whom coeliac serology was requested over a period from 1997 to 2006 were obtained from laboratory databases. From 1997 standard coeliac serology at our hospital was endomysial antibody, and from 2002 tissue transglutaminase antibody was the serological test used. Requests for coeliac serology were categorised as originating from gastroenterology (GI) clinics, general practice (GP), paediatric department (paeds) or from other adult specialities. In the calculation of positive serology rates, duplicated tests in the same individual were excluded.
Results: A total of 9976 coeliac serological tests were requested. The annual number of tests increased each year from 302 in 1997, to 1826 in 2006. The mean age was 39.9 years. In every year females had more serological tests, with 66% of all requests being in females. Over the decade there was a progressive increase in the proportion of requests for coeliac serology from GPs. In 1997, 3.3% of coeliac serology requests originated in primary care. By 2006, 52% of requests were from primary care. Correspondingly, although the absolute number of GI clinic requests for serology increased over the decade, the proportion of the total from GI clinics fell from 60% in 1997 to 24% in 2006. Tests requested in patients <16 yrs old fluctuated between 14% and 25% of the total each year. The proportion of positive serological results fell from 5.7% in 1997 to 2.6% in 2006. In earlier years ∼90% of positive serology patients underwent duodenal biopsy. In contrast there was no record of duodenal biopsy in 30% patients with positive serology in 2006. The majority of these non-biopsied positive serology patients had serology requested by GPs. When duodenal biopsies were done for positive serology, 92% were confirmed as coeliac disease.
Conclusion: Increasingly, coeliac serological testing is more likely to be arranged by GPs. Twice as many females are tested. The increasing number of tests, coupled with the diminishing proportion of positive results indicates testing is requested at a lower symptom threshold or for non-specific symptoms. There is evidence that positive serological results received by GPs are not being followed up by duodenal biopsy.
IS TISSUE TRANSGLUTAMINASE ANTIBODY AN ACCURATE PREDICTOR OF MARSH GRADE IN BOTH NEWLY DIAGNOSED AND TREATED PATIENTS WITH COELIAC DISEASE?
A. D. Hopper, T. S. Chew, G. Wild, D. S. Sanders. Gastroenterology, Royal Hallamshire Hospital, Sheffield, UK
Introduction: The quantitative result obtained with IgA-tissue transglutaminase antibody (TTG) has been shown to be an accurate serological marker for detecting coeliac disease (CD). Once a diagnosis has been made, there is no single method which allows assessment of compliance.
Aims & Methods: The aim of our study was to assess if TTG was an accurate predictor for the Marsh grade severity in patients both newly diagnosed and treated CD.Adult patients undergoing gastroscopy that were found to have villous atrophy (Marsh 3a–c: new CD) or raised intraepithelial lymphocytes on their duodenal biopsy (Marsh 1 and 2: potential CD) were prospectively recruited over a 2-year period (group1). During the same period, patients with a known diagnosis of CD, referred for duodenal biopsy for assessment of histological remission were also recruited (group 2). These patients had been on a GFD for greater than 1 year. All patients had 4 duodenal biopsies taken and a blood sample taken for serological analysis of antibodies to human IgA-TTG and IgA-EMA. Duodenal biopsies were graded according to the modified Marsh criteria.
Results: We identified 155 patients in group 1 (mean age: 47.3, 69.2% female). 48 patients were identified in group 2 (mean age: 52.7, 68.8% female). The table shows the Marsh grade of the biopsies obtained for each group and the number of patients with a positive TTG or EMA is listed (including the average TTG titre) for each grade. In group 1: patients with Marsh 1 or 2 lesions had a significantly lower average TTG titre than patients with Marsh 3 lesions (p<0.05). Between Marsh grade 3a and 3c, there was a significant increase in the proportion of patients with a positive TTG and EMA (sensitivity) (p<0.02 and p<0.01 respectively). There was a significant relationship between marsh grade (1–3c) and average TTG titre r = 0.94 (p<0.02). Group 2: the number of patients with a positive TTG and EMA were significantly higher in patients with villous atrophy than in those without (EMA p<0.02; TTG p<0.05). In the 16 patients with villous atrophy, 7 (44%) had a normal TTG level. In patients on a GFD the ability of TTG to test for persisting villous atrophy had a sensitivity, specificity, positive predictive value and negative predictive value of 56.2%, 90.6%, 70%, 76.3% respectively.
Conclusion: The sensitivity of TTG decreases with lesser degrees of villous atrophy. Also, like EMA, a normal TTG level does not accurately predict the recovery of villous atrophy in patients with CD on a GFD, and we would suggest that a duodenal biopsy should always be considered if patients are still symptomatic.
DIETARY FODMAPS INCREASE DELIVERY OF WATER AND FERMENTABLE SUBSTRATES TO THE PROXIMAL COLON
J. S. Barrett, P. M. Irving, R. B. Gearry, J. G. Muir, M. L. Haines, P. R. Gibson. Gastroenterology, Box Hill Hospital, Melbourne, Australia
Introduction: Luminal distension of the distal small bowel and proximal colon may be a stimulus for the genesis of symptoms in patients with functional gut disorders. The high osmotic activity and rapid fermentability of poorly absorbed, short-chain carbohydrates (FODMAPs, for example, fructans, fructose, sorbitol) suggests they play a role in symptom induction. Observational and placebo-controlled, rechallenge studies demonstrate that reducing dietary FODMAPs leads to improvement in IBS symptoms. However, the validity of the simple principles upon which the hypothesis is based is untested.
Aims & Methods: To define the effect of dietary FODMAPs on the volume and nature of the ileal effluent and perception of output in patients with an ileostomy. Patients with ileostomies but no clinical evidence of small intestinal disease undertook two 4-day periods of dietary intervention, comprising diets differing only in FODMAP content (high vs low), with at least 14 days washout between (single blinded, cross-over design). All food was provided. Ileal effluent was collected 2 hourly during the day (14 h) and overnight as required, on day 4 of each diet. Patients rated effluent volume and consistency in addition to abdominal symptoms on a 10 cm visual analogue scale (VAS). The FODMAP content of the diet and effluent FODMAPs were measured by enzymatic and HPLC methods.
Results: 12 patients (aged 31–78 y, 6 men, 60% previous ulcerative colitis) completed the study. Compared with the low FODMAP diet, daytime ileal output was 19% greater with the high FODMAP diet (504±51 (mean ± SEM) vs 409±65, p = 0.01). High osmotic activity of FODMAPs was demonstrated with a 17% greater water volume (p = 0.01). Poor absorption of FODMAPs was proven with considerable FODMAP content in the high FODMAP diet effluent (for example, fructans 8.5± vs 0.9±; sorbitol 0.9± vs 0, oligosaccharides ± vs ±, all p<0.05), which also significantly increased dry weight (p = 0.03). Presence of this fermentable substrate was evident with reduction of pH in the overnight samples of the high FODMAP diet (ph data, p = 0.04). Patients perceived reduced output (VAS score 5.6±0.5 to 4.2±0.6 cm, p = 0.06) and significantly improved effluent consistency (4.8±0.6 to 2.3±0.6 cm, p = 0.01) with the low FODMAP diet.
Conclusion: Data support the hypothetical model regarding mechanism of action with dietary FODMAPs increasing delivery of water and fermentable substrates to the proximal colon. Patients’ perceive an improved effluent quality with a low FODMAP diet. The data suggest that a low FODMAP diet should be considered where ileostomy output is high.
PREVALENCE OF FRUCTOSE AND LACTOSE MALABSORPTION IN PATIENTS WITH GASTROINTESTINAL DISORDERS
J. S. Barrett, P. M. Irving, S. J. Shepherd, J. G. Muir, P. R. Gibson. Gastroenterology, Box Hill Hospital, Melbourne, Australia
Introduction: Fructose (FM) and lactose malabsorption (LM) may trigger functional gastrointestinal symptoms in disorders such as functional gut disorders (FGD), inflammatory bowel disease (IBD) and coeliac disease. When poorly absorbed, they distend the intestinal lumen via rapid fermentation and high osmotic activity, and induce symptoms such as bloating, diarrhoea, abdominal pain and flatulence. Hydrogen breath testing identifies subjects with FM or LM by detecting expired hydrogen produced when malabsorbed sugars are fermented by luminal bacteria.
Aims & Methods: To compare the prevalence of FM and LM in patients with IBD, functional gut disorders, coeliac disease and healthy controls. A secondary aim was to identify differences in responses to lactulose breath testing between the groups. Results for breath tests completed on consecutive patients with IBD and coeliac disease were obtained from the hospital database and disease information was collated. Patients with FGD were assessed prospectively and categorised by Rome III criteria. Healthy controls had no history of gastrointestinal disorders. Reports were analysed for presence of FM, LM and early rise in breath hydrogen after lactulose (ERBHAL), a surrogate marker for small intestinal bacterial overgrowth. Non-hydrogen producers and those at high ethnic risk of LM were excluded from analysis.
Results: There was a higher prevalence of FM in patients with Crohn’s disease compared to healthy controls (p<0.01), IBS (p<0.02), and both treated (p<0.02) and untreated coeliac disease (p<0.01). There was no significant difference in the prevalence of LM between groups. ERBHAL was more prevalent in healthy controls than in Crohn’s disease (p<0.01), IBS (p<0.03) and treated coeliac disease (p<0.01). Crohn’s disease phenotype sub-analysis demonstrated that ileal Crohn’s was associated with a higher prevalence of FM (82%) and LM (58%) than colonic Crohn’s disease (p<0.05). No differences were observed across FGD subtypes.
Conclusion: FM, LM and ERBHAL are normal phenomena. It is likely that that symptom induction depends on the response of the intestine to subsequent luminal distension. Thus, their presence in patients with functional gut symptoms provides an opportunity for therapy (for example, dietary change or antibiotics) to remove potential triggers for such symptoms.
21ST CENTURY COELIAC DISEASE: PRESENTING FEATURES AND CHANGES IN BIOCHEMICAL PROFILE WITH TREATMENT
N. R. Lewis1, D. S. Sanders2, R. B. Hubbard1, R. F. A. Logan1, J. West1. 1Division of Epidemiology and Public Health, University of Nottingham, Nottingham, UK, 2Gastroenterology and Liver Unit, Royal Hallamshire Hospital, Sheffield
Introduction: Although we now accept that the minority of coeliac disease presents in the classical manner, there has not been a large, prospective cohort study of contemporary patients’ presenting features or their biochemical response to a gluten-free diet.
Aims & Methods: Presenting features and physiological measures was prospectively collected on incident cases (n = 130) of coeliac disease at the Royal Hallamshire Hospital, at diagnosis and at 12 months post-exposure to a gluten-free diet from October 2004. We compared measures at diagnosis and 12 months after using paired t tests.
Results: The mean age at diagnosis was 47.9 years (SD 14.9) with no difference between men and women (p = 0.43). Iron deficiency anaemia was the most common presenting feature affecting 42.3% (n = 55) of the cohort but was more common in women than in men (53.4% vs 19.0%, p = 0.003). 31.0% (n = 40) had partial villous atrophy, 34.1% (n = 44) had subtotal villous atrophy and 20.8% (n = 27) had total villous atrophy. The median tTG at diagnosis was 215 IU (range 5–300) and 98.3% (n = 117) were EMA positive. The mean value of Hb, MCV, WCC, and folate significantly increased with exposure to a gluten-free diet (table). These changes did not vary by gender or by age. However, on stratifying according to severity of disease as measured by tTG titre and Marsh grading, physiological changes only significantly occurred in those people with more severe coeliac disease (subtotal and total villous atrophy). Mean CRP and ESR was 3.8 mg/l (SD 2.9) and 12.4 mm/Hr (SD 12.4) at diagnosis; these values did not significantly change with exposure to a gluten-free diet (p = 0.56).
Conclusion: Though there may be an improvement in symptoms, patients with lower levels of TTG and partial villous atrophy at the time of diagnosis may have fewer physiologically improvements on a gluten-free diet after 12 months. It may be that low levels of systemic inflammation persist in coeliac disease despite treatment with a gluten-free diet.
INTESTINAL TISSUE ENGINEERING USING COLON-DERIVED COLLAGEN SCAFFOLDS
D. A. J. Lloyd1, T. I. Ansari2, P. D. Sibbons2, S. M. Gabe1. 1Lennard-Jones Intestinal Failure Unit, St Mark’s Hospital, 2Northwick Park Institute for Medical Research, Northwick Park Hospital, Harrow, UK
Introduction: Tissue engineering offers the possibility of intestinal replacement in patients with short bowel syndrome. Current animal models employ either intestinal lengthening techniques using biologically derived scaffolds, or transplantation of partially digested neonatal small intestinal tissue, termed intestinal organoids, onto artificial scaffold materials.
Aims & Methods: The aim of this study was to develop a biologically derived tubular structure for use in both intestinal lengthening procedures and to support intestinal organoids. Lengths of colon were harvested from adult rats, decellularised and stabilised by collagen crosslinking. 1 cm lengths of were then interposed between defunctioned segments of healthy jejunum in a rat model. Animals were sacrificed at 4 and 8 weeks. In separate experiments 1 cm lengths of scaffold were loaded with intestinal organoids, and subcutaneously implanted into rodents. Scaffolds were harvested at 2, 4 and 6 weeks. Harvested tissue underwent routine H&E, PAS and Grimelius staining to identify epithelial cell lines, and immunohistochemistry to identify replicating cells.
Results: Decellularised scaffolds were successfully generated from colonic tissue. Assessment of interposed scaffolds revealed heavy infiltration with fibroblasts and inflammatory cells, and scaffold vascularisation. At both 4 weeks and 8 weeks after implantation there was evidence of in-growth of mucosa onto the luminal surface of the scaffold from the adjacent jejunal mucosa. Both columnar enterocytes and goblet cells could be seen in this neomucosal layer. Neomucosa appeared most developed at 8 weeks with evidence of crypt-villus architecture. In the subcutaneously implanted intestinal organoid-loaded scaffolds, neomucosa could be seen from 2 weeks onwards. By 6 weeks the neomucosal layer was relatively advanced with evidence of rudimentary crypts and villi and morphological architecture similar to normal intestinal mucosa. Histological assessment confirmed the presence of columnar epithelial cells, goblet cells, Paneth cells and enteroendocrine cells. Actively replicating cells were distributed predominantly towards the bases of the crypts. Multiple blood vessels and lymphatic vessels were visible in the submucosa along with layers of elongated and flattened smooth muscle-like cells.
Conclusion: Colon-derived collagen scaffolds can be employed to support the development of intestinal neomucosa generated both by interposition of scaffolds and by seeding with intestinal organoids. Neither the use of biologically derived tissue as a scaffold for intestinal organoid development, nor the use of the same scaffold material for both techniques of intestinal tissue engineering has been documented previously.
BSG GUIDELINES FOR DETECTING OSTEOPOROSIS IN COELIAC DISEASE: TOO RESTRICTIVE?
J. Burgess1, H. M. Gilbert1, E. Cotton2, A. Woolf2, H. R. Dalton3, D. F. Levine4, I. A. Murray3. 1Medical student, Peninsula medical school, Universities of Exeter & Plymouth, 2Rheumatology, 3Gastroenterology, Royal Cornwall Hospital, Truro, 4Gastroenterology, West Cornwall Hospital, Penzance, UK
Introduction: The 2000 BSG Guidelines for osteoporosis in coeliac disease1 (CD) suggested all CD patients should have their bone mineral density (BMD) assessed at diagnosis. An update this year2 restricted BMD measurement to those with additional risk factors eg over 70 years old or BMI<20; (overall relative risk of osteoporotic fracture in CD of 1.4). We studied whether present guidelines are too restrictive by reviewing the BMD results of CD patients in our Trust.
Aims & Methods: We have seen 357 CD patients (237 female: age range 16–90 years, median 59) over the past 6 years. Of these 262 (73.4%) have had dual-energy x ray absorptiometry (DEXA) scans of the hip and lumbar spines to measure BMD. Results were correlated with the risk factors that influence BMD as outlined in the 2007 guidelines.
Results: Of those scanned, 62 (23.7%) had osteoporosis, 106 (40.4%) were osteopenic and 62 (35.9%) had normal BMD. 22 (8.4%) were osteoporotic in the hip, 55 in the spine (21.0%). Median z scores were not significantly reduced however (−0.29 in hip: –0.22 in spine). BMD did relate to age with osteoporosis in 17.3% in under 70 years olds, 43.8% over this age. Less than 5% of those <55 years old had osteoporosis. BMD did not correlate with smoking, steroids, gender or associated diseases including hypothyroidism. One patient over 70 had not had a DEXA scan whilst 119 had had a DEXA scan unnecessarily—that is, under 70 years old without additional risk factors. Of these 24 (20.2%) were osteoporotic and 48 (40.3%) had osteopenia.
Conclusion: In this large cohort of predominantly treated CD patients, osteoporosis was almost 50% more common than has been reported recently (14% in spine, 7% in hip3). Although following current guidelines will reduce DEXA requests and costs we have shown that it will also miss many osteoporotic CD patients. We had limited numbers of patients with additional risk factors—for example, current smokers <10% but found no evidence to support guidelines that such risk factors increased the likelihood of osteoporosis in this population.
THE FIRST PROSPECTIVE DOUBLE BALLOON ENTEROSCOPY STUDY ON PATIENT TOLERABILITY: EXPERIENCE FROM THE UK
R. Sidhu1, M. E. McAlindon1, M. Thomson2, D. P. Hurlstone1, S. Hardcastle1, I. C. Cameron3, D. S. Sanders1. 1Department of Gastroenterology, Royal Hallamshire Hospital, Sheffield Teaching Hospitals NHS Trust, 2Department of Gastroenterology, Sheffield Children’s Hospital, 3Department of Surgery, Royal Hallamshire Hospital, Sheffield Teaching Hospitals NHS Trust, Sheffield, UK
Introduction: Double balloon enteroscopy (DBE) is a novel technique permitting pan small bowel (SB) endoscopy. International DBE studies report using benzodiazepines (with combination of opiates), propofol or a general anaesthetic (GA). In the UK, endoscopic procedures are generally done under conscious sedation with benzodiazepines alone or with a combination of an opiate. The use of a GA for endoscopy is rare and propofol is unlicensed without the presence of an anaesthetist. The optimal type of sedation/anaesthesia for DBE is currently unknown and there is no published literature on patient tolerability/preference.
Aims & Methods: To assess patient tolerability for DBE, using conscious sedation, in a tertiary setting in the UK. Data were collected prospectively: DBE route, procedure length and amount of sedation were noted. We used a previously validated (and published) sedation scoring system. The endoscopists were asked to subjectively evaluate the quality of sedation according to their perception of patient tolerability (1 = excellent, 2 = good, 3 = fair and 4 = poor). The patient evaluated the procedure the following day by telephone (1 = no discomfort/unable to remember, 2 = slightly uncomfortable, 3 = extremely uncomfortable, 4 = unacceptable). Patients were subsequently asked if they would have preferred to have DBE under GA.
Results: 21 patients underwent 30 DBE procedures (16 oral/14 anal route) between July 06–October 07. The mean procedure time was 70 min (range 2–120) with the mean doses of midazolam and fentanyl used of 8.6 mg (range 2.5–36) and 52 μg (25–75) respectively. There were no complications but DBE failed in 4 patients due to poor tolerance. 57% of patients found the procedure extremely uncomfortable, whilst 37% rated their procedure as slightly uncomfortable and 6.7% found it unacceptable. The endoscopists rated the sedation as excellent in 3.3%, good in 53.3%, fair in 20% and poor in 23.3%. There was no significant difference between patient and endoscopist scores (p = 0.57) and between patient scores and the route of DBE (oral/anal) (p = 0.71). There was also no correlation between tolerability and either duration of procedure or degree of sedation. Paradoxically, 63% of patients would have DBE repeated if clinically necessary. However, 77% would choose a general anaesthetic if offered.
Conclusion: DBE procedure time is lengthy compared to other forms of endoscopy with a high proportion of patients tolerating DBE suboptimally. Our pilot data suggest that the combination of midazolam and fentanyl may be inadequate for this procedure.