Article Text

Statistics from Altmetric.com
Polymorphisms in collagen type iii gene linked to gastro-oesophageal reflux and hiatus hernia
Twin studies suggest a strong genetic component to susceptibility to develop gastro-oesophageal reflux disease (GORD). This extensive genetics study used four separate patient groups. A whole genome linkage analysis performed in 237 patients with GORD from 36 families and 168 controls identified a 35 megabase pair region on chromosome 2. The authors then analysed gene expression in oesophageal biopsies and found three candidate genes. Using 364 patients with GORD and 728 controls from a trio collection of parents with children affected by GORD aged <17, the authors showed significant association of single nucleotide polymorphisms (SNPs) of the gene COL3A1 with GORD in males (see table). This same gene association was confirmed in a further cohort of 256 patients with GORD, 229 patients with hiatus hernia (HH) and 485 controls, although the SNP associated with HH was different from that associated with GORD. Finally, the authors showed that collagen type III was increased in GORD oesophageal biopsies. Mutations in COL3A1 cause the Ehlers–Danlos syndrome but plainly those linked to GORD cause much milder defects. The fact that different SNPs are linked to GORD and HH indicates different underlying mechanisms, which might include impaired wound healing as well as altered elasticity of connective tissue.
See pages 1063
Pathology of norovirus diarrhoea
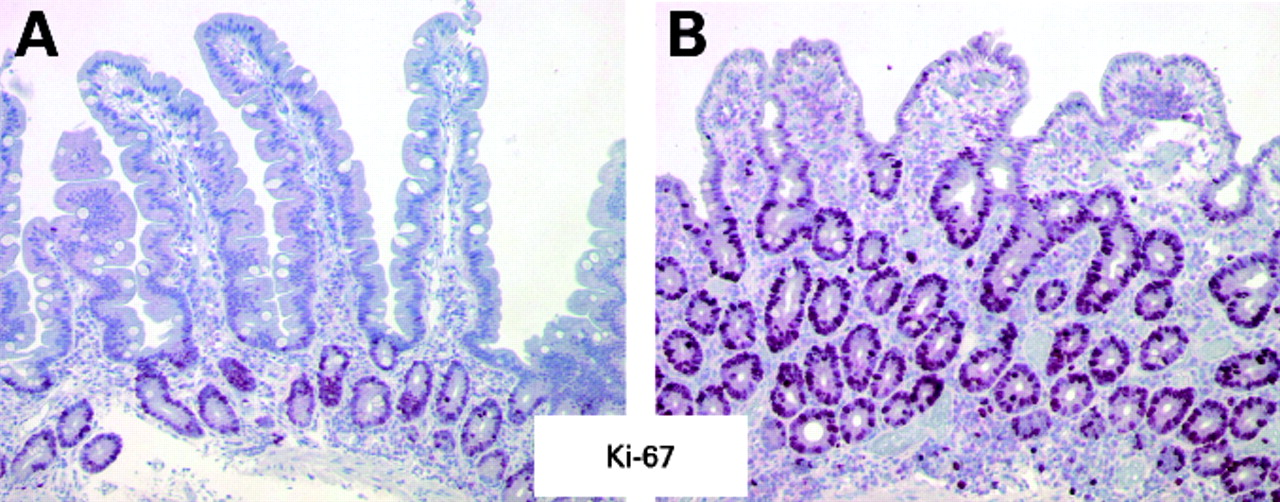
Although viral gastroenteritis is one of the commonest afflictions of man, detailed description of its human pathology is extremely limited, so this study of seven subjects with norovirus diarrhoea is of great interest. Endoscopic biopsies were used to assess epithelial resistance, secretion and permeability in an Ussing chamber, while immunohistochemistry was used to characterise the inflammatory response. Although the villi were apparently only slightly blunted, quantitative assessment showed that the surface area fell by nearly 50%. There was a marked infiltration with intraepithelial lymphocytes, which showed a cytotoxic phenotype with increased expression of perforin. Enterocyte proliferation was increased, as shown by a marked increase in Ki-67 (see fig). The functional effect of this was that epithelial resistance and permeability fell, while epithelial chloride secretion increased. The marked increase in markers of apoptosis suggests that the villous blunting may well be due to enterocyte apoptosis induced by the cytotoxic T cells, which probably also mediate the decrease in epithelial resistance.
See pages 1070

Duodenal biopsies in a control (A) and norovirus infected patient (B) showing a marked increase in the cell proliferation marker Ki-67.
Coeliac disease associated genetic risk variants in TNFAIP3 and REL implicate altered NF-κB signalling
A recent genome-wide association study (GWAS) identified several risk variants for coeliac disease. In the current study, the authors (who were part of the initial GWAS) studied 458 SNPs showing more modest association in the original GWAS, to identify additional risk variants for coeliac disease. They genotyped 1682 cases and 3258 controls from three populations (UK, Irish and Dutch) as well as an independent Italian cohort of 538 cases with coeliac disease and 593 controls for confirmation. Two novel coeliac disease risk regions were identified. The strongest association was seen on the long arm of chromosome 6 (6q23.3) in a block of linkage disequilibrium (LD) between the OLIG3 and TNFAIP3 genes. Of note is that SNPs in the same LD block have previously been associated with rheumatoid arthritis, systemic lupus erythematosus and type 1 diabetes. The TNFAIP3 gene plays a role in NF-κB signalling. The second locus was located on chromosome 2p16.1, harbouring the REL gene. REL is also a component of the NF-κB transcription complex, which plays a critical role in promoting immune and inflammatory responses. When adding these two novel loci to the loci already identified through the previous GWAS, the human leucocyte antigen (HLA) risk factors and the 10 established non-HLA risk factors explain 40% of the heritability of coeliac disease.
See pages 1078
A new animal model of postsurgical bowel inflammation and fibrosis shows importance of commensal microbiota
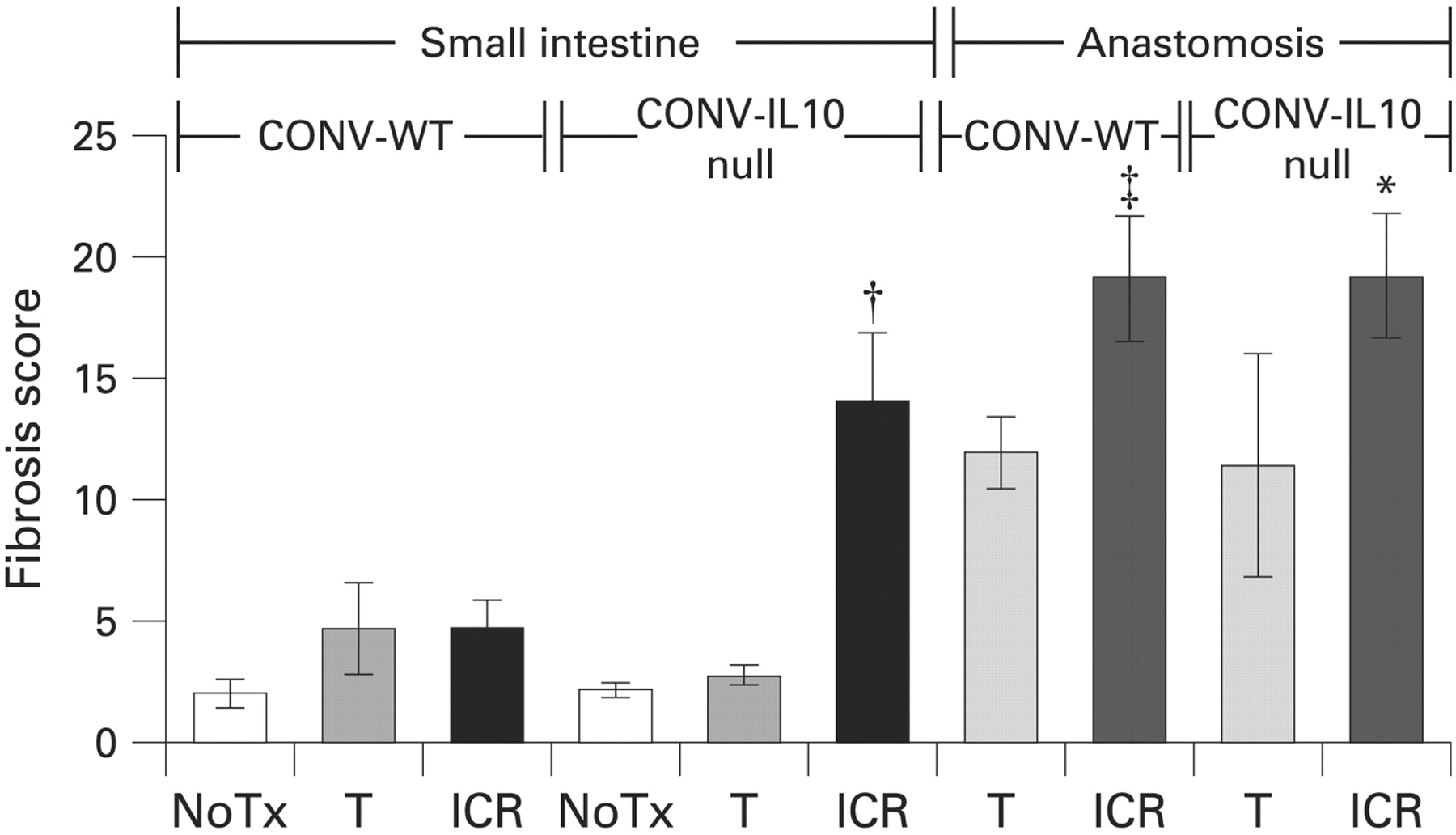
Crohn’s disease (CD) is characterised by transmural inflammation, leading to thickening of the muscularis layers, fibrosis and stenosis. Bowel obstruction is one of the main reasons why patients need ileocaecal resection (ICR) but ICR does not cure the disease and, often, disease recurs at the site of anastomosis and in the small bowel proximal to the anastomosis. The mechanism of recurrence is unknown but the microbiota is believed to play an important role. An animal model of postsurgical recurrence would offer a well-controlled experimental system to address mechanisms of postsurgical inflammation and fibrosis and to test treatments. Here, the authors chose the interleukin (IL) 10 null mouse to develop a model of postsurgical inflammation and fibrosis and tested whether the microbiotia promotes postsurgical inflammation or fibrosis. Germfree (GF)-IL10 null mice were conventionalised (CONV) and 3 weeks later randomised to ICR, transaction (T) or no treatment (NoTx). Age-matched CONV-wild-type (WT) and GF-IL10 null mice received the same procedures. Following ICR, CONV-IL10 null mice—but not the CONV-WT mice—developed significant inflammation and fibrosis in the small bowel and inflammation at the anastomosis compared with NoTx or T controls. In contrast, GF-IL10 null mice developed little or no inflammation or fibrosis after ICR. In conclusion, ICR in CONV-IL10 null mice provides a new animal model of postsurgical inflammation and fibrosis in the small bowel and anastomosis. The absence of inflammation and fibrosis in the CONV-WT and in the GF-IL10 null mice following ICR indicates that postsurgical small bowel disease occurs only in genetically susceptible (IL10 null mice) and is bacteria dependent (only after bacterial colonisation).
See pages 1104
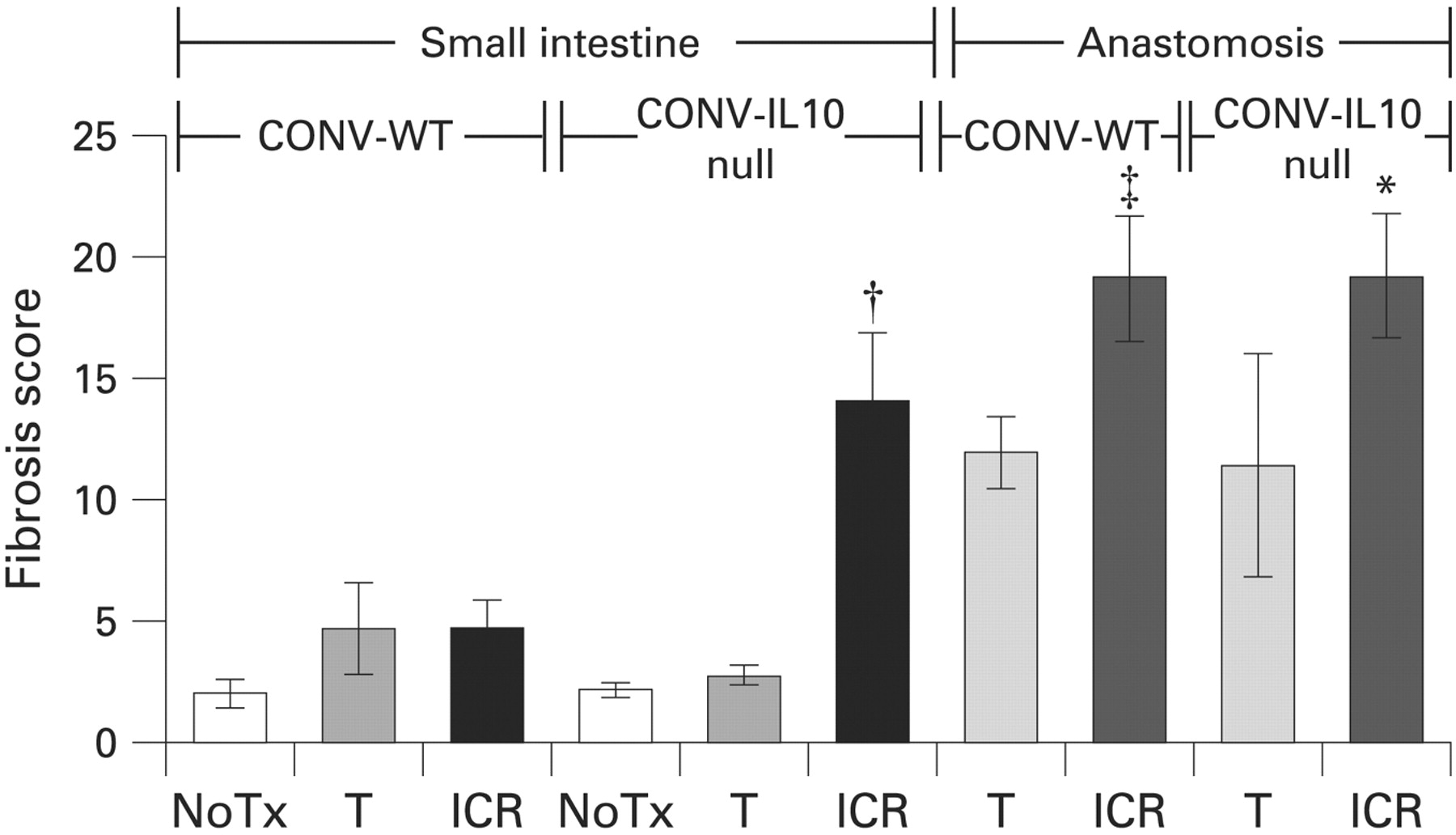
Fibrosis scores in small intestine and anastomosis of conventionally raised interleukin 10 (CONV-IL10) null and wild-type (WT) mice. Histograms show the mean fibrosis scores for both mice, 28 days after no treatment (NoTx), transection (T) or ileocaecal resection (ICR). In the small intestine, ICR caused significant fibrosis in IL10 null mice but not WT mice. Fibrosis at the anastomosis was not restricted to IL10 null mice, as WT mice also had significantly higher fibrosis scores than NoTx controls.
MRI for assessment of disease activity and severity in Crohn’s disease
An accurate assessment of the disease activity in patients with CD is crucial to guide management. Mostly, this is done using endoscopy. As endoscopy is invasive, brings discomfort and/or pain to the patient and carries a risk for bowel perforation, alternative techniques, preferably avoiding radiation, have been proposed. In this study, the authors investigated the accuracy of MRI for this purpose. A total of 50 patients with clinically active (n = 35) or inactive (n = 15) CD underwent ileocolonoscopy and MRI. Endoscopic activity was evaluated using the Crohn’s Disease Endoscopic Index of Severity (CDEIS). The key findings were that among the independent predictors for CDEIS were wall thickness (p = 0.007), relative contrast enhancement (p = 0.01), presence of oedema (p = 0.02) and presence of ulcers at MRI (p = 0.003). Using these parameters, the authors built a magnetic resonance index of activity (MRAI) and showed a very good correlation between the CDEIS of the segment and the MRAI (r = 0.82). The MRAI had a high accuracy for the detection of disease activity (area under the receiver operating characteristic (AUROC) curve = 0.891) and for the detection of ulcerative lesions (AUROC curve = 0.978). MRI may, therefore, become an non-invasive alternative to endoscopy in the evaluation of ileocolonic CD.
See pages 1113

(A) T1 image after intravenous contrast administration of the descending colon and splenic flexure, showing discontinuous lesions with segmental thickening of the colon wall and deep ulcers (arrowheads) alternating with a segment without inflammatory changes (arrow). (B) colonoscopy of the same segment shows the presence of deep ulcers in the mucosa.
Increased yield from screening colonoscopy in patients infected with HIV compared with uninfected controls
As highly active anti-retroviral therapy (HAART) is more widely used, the incidence of AIDS-defining malignancies—such as Kaposi’s sarcoma and non-Hodgkins lymphoma—has fallen and life expectancy for patients infected with HIV has increased. However, their risk of developing other cancers appears increased. This study examined the yield of screening colonoscopy in 136 asymptomatic patients infected with HIV aged >50 years compared with 272 controls matched for age, sex and family history of colorectal cancer (CRC). Patients infected with HIV were more likely to be from ethnic/racial minorities, more likely to smoke and less likely to take aspirin. Most had been diagnosed with HIV >10 years before. After adjusting for age, sex and race, patients infected with HIV were significantly more likely to have a neoplastic lesion (Odd’s ratio 2.38; 95% confidence interval 1.56 to 3.63). The yield for all neoplastic lesions was increased (62.5% vs 41.2% ) and patients infected with HIV were significantly more likely to have polyps 6–9mm in diameter. Other neoplasms were commoner but this did not reach statistical significance (see fig). Patients infected with HIV also had more proximal lesions (37.5% vs 24.3%). Predictors of having a neoplastic lesion were a positive family history and not taking HAART. Further studies are needed to determine how HAART protects from CRC.
See pages 1129

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Incidence of neoplastic lesion in patients infected with HIV (solid bar) versus uninfected controls (open bar)
Linked Articles
- Oesophagus
- Small intestine
- Small intestine
- Inflammatory bowel disease
- Inflammatory bowel disease
- Colon