Article Text

Statistics from Altmetric.com
BSG inflammatory bowel disease symposium
0-01 DIETARY DOCOSAHEXAENOIC ACID REDUCES THE RISK OF DEVELOPING ULCERATIVE COLITIS – A MULTI-CENTRE EUROPEAN PROSPECTIVE COHORT STUDY
A. R. Hart for The IBD in EPIC Study Investigators. School of Medicine, University of East Anglia, Norwich, UK
Introduction: Dietary docosahexaenoic acid (DHA), an n-3 polyunsaturated fatty acid obtained principally from fish, has anti-inflammatory effects on many cellular processes, and may prevent the development of ulcerative colitis. Currently, there are no prospective epidemiological data from multicentre studies investigating this hypothesis.
Aims and Methods: The aim was to examine the prospective relationship between the dietary intake of DHA and the development of ulcerative colitis in participants enrolled in a large European cohort study. The populations comprised 189 610 men and women, aged 30–74 years, participating in a cohort study (EPIC European Prospective Investigation Into Cancer & Nutrition). Participants were resident in either the UK, Sweden, Denmark or Germany. They provided information on diet at recruitment, by completing food frequency questionnaires, and were followed up for the diagnosis of ulcerative colitis. Each incident case was matched with four controls and the intake of DHA divided into quartiles. The analysis was performed using logistic regression adjusted for gender, age, total energy intake, smoking, centre and other fatty acids which affect DHA formation.
Results: A total of 118, initially healthy participants, developed ulcerative colitis (53 women, 65 men) after a median follow-up time of 4.0 years (range 1.7–11.3 years). The odds ratio for the highest versus the lowest quartile of intake of DHA acid was 0.24 (95% CI 0.06 to 0.99).
Conclusion: These results, together with plausible biological mechanisms, support the hypothesis that dietary DHA may reduce the risk of developing ulcerative colitis. Further epidemiological studies are needed to investigate this finding, which if confirmed, has implications for the prevention of ulcerative colitis. If the association is causal then increasing the population’s intake of DHA may prevent 30% of cases of ulcerative colitis.
0-02 AUTOLOGOUS STEM CELL TRANSPLANTATION FOR CROHN’S DISEASE (ASTIC) TRIAL: EARLY REPORT OF TOXICITY AND EFFICACY
C. J. Hawkey. Nottingham Digestive Diseases Centre and Biomedical Research Unit, Nottingham University Hospital, Nottingham, UK
Introduction: Some patients with Crohn’s disease are resistant to available treatments and these control but do not cure the disease. By resetting immune responses and by other mechanisms, autologous stem cell transplantation has the potential to cure Crohn’s disease. Case reports suggest this is the case for some but not all patients.
Aims and Methods: The ASTIC Trial randomises patients with poor quality of life despite 3 immunosuppressive agents to undergo stem cell mobilisation followed by ablation and transplantation immediately or after 1 year, and compares the number in drug free clinical and endoscopic remission at the end of 1 year.
Results: Eighteen patients have been considered by the Steering Committee. Eight have been approved unconditionally and five subject to specific improvements in health or management. Nine patients who have entered the study are shown in the table. Four patients did not proceed to trial entry because of spontaneous improvements. As at November 1 2008, 4 serious adverse events have been reported (3 infective, 3 serious, 1 SUSARs). Data on efficacy will be analysed on March 1 2009 and will be presented.
Conclusion: There are a significant number of patients with Crohn’s disease for whom stem cell transplantation is an appropriate course of action. The main risks are related to infection.
Pathology free papers
0-03 DOES THE ECTOPIC EXPRESSION OF CDX2 PROVOKE EXPRESSION OF INTESTINAL GENES IN OESOPHAGEAL CELLS?
1B. J. Colleypriest, 2J. M. Farrant, 1D. Tosh, 1J. M. W. Slack. 1Biology and Biochemistry, University of Bath, UK, 2Gastroenterology, Royal United Hospital, Bath, UK
Introduction: Oesophageal adenocarcinoma and its precursor lesion, Barrett’s metaplasia, are both exhibiting a rapidly increasing incidence. Whilst many of the molecular mechanisms in the progression from Barrett’s metaplasia to cancer are understood the initial step to intestinal metaplasia is not. The transcription factor caudal type homeobox transcription factors 2 (cdx2) has been implicated in the pathogenesis of Barrett’s. The expression of cdx2 is normally limited to the post pyloric epithelium of the gastrointestinal tract, but it is present in Barrett’s tissue. Transgenic studies have demonstrated that ectopic expression of cdx2 in the gastric mucosa results in ectopic intestinal tissue; this has not however been demonstrated in oesophageal tissue. We present a novel long term in vitro model of squamous mouse oesophagus which recapitulate the full repertoire of cell phenotypes found in the oesophagus. We have investigated the result of ectopic cdx2 expression within this model.
Aims and Methods: Explants of mouse oesophageal epithelium are cultured and characterised using immunofluorescent immunohistochemistry. Transgenes are expressed within the explant culture using recombinant adenovirus such as ad-cmv-GFP and ad-cmv-cdx2. Changes in gene expression, particularly the induction of intestinal genes, are assessed by PCR.
Results: The explant culture system is viable in culture for over 6 months. There is a connective tissue and epithelial components, as demonstrated by smooth muscle actin and e-cadherin expressing cells, within the culture. The epithelial cells within the model express markers of full stratification; cytokeratins 5, 14 and 4, involucrin and loricrin as well as the squamous transcription factor p63. Incubation with recombinant adenovirus, ad-cmv-cdx2 results in epithelial expression of cdx2 protein assessed by immunofluorescence. The ectopic expression of cdx2 within the epithelium of this model does not promote the transcription of any intestinal genes. Mucin 2, sucrose isomaltase, lactase phlorizin, alkaline phosphatase, trefoil factor 3, villin, chromogranin A and cryptdin 1 were all looked for using PCR.
Conclusion: The long-term in vitro model of squamous oesophagus recapitulates the full repertoire of oesophageal cells found in vivo. Ectopic gene expression, and the effects thereof, is possible using adenoviral vectors. Cdx2 expression within oesophageal squamous cells does not result in the expression of intestinal genes. These findings contrast with previous studies in gastric mucosa suggesting that other factors are necessary in the oesophageal cells.
0-04 HUMAN SMALL INTESTINAL CRYPTS ARE CLONAL, CONTAIN MULTIPLE STEM CELLS AND MUTATED CRYPTS DIVIDE BY FISSION
1L. Gutierrez-Gonzalez, 1M. Deheragoda, 1S. J. Leedham, 1G. Elia, 2A. Shankar, 2C. Imber, 3D. M. Turnbull, 4M. Novelli, 5J. A. Jankowski, 6N. W. Wright, 5S. A. C. McDonald. 1Histopathology Unit, Cancer Research UK, London, UK, 2Surgery, University College London Hospitals, London, UK, 3School of Neurology, Neurobiology and Psychiatry, University of Newcastle upon Tyne, Newcastle upon Tyne, UK, 4Histopathology, University College London Hospitals, UK, 5Centre for Gastroenterology, London, UK, 6Institute of Cell and Molecular Sciences, Barts and the London School of Medicine and Dentistry, London, UK
Introduction: Little is known about the clonal structure or stem cell architecture of human small intestinal crypts and how mutations spread through the small bowel. Data from our laboratory, using mitochondrial (mt)DNA mutations as a marker of clonal expansion of stem cell progeny has shown that normal colonic crypts are clonal with every cell type within a crypt containing the same mtDNA mutation. Furthermore we have shown that clonal patches can occur with multiple crypts each containing the same mutation.
Aims and Methods: Here we investigate the clonal makeup of the normal human small bowel crypt and determine how mutations spread. Enzyme histochemistry (for cytochrome c oxidase (CCO) and succinate dehydrogenase) was performed on 6 μm frozen sections of normal human duodenum. Laser-capture microdissection was used to isolate CCO-ve crypts, PCR was used to amplify the entire mt genome and mutations were identified by sequencing. Immunohistochemistry was performed for markers of all differentiated epithelial cells.
Results: CCO-ve small bowel crypts were observed within all sections. This suggests that crypts are clonal, and sequencing confirmed that all cells from a negative crypt contained the same mtDNA mutation. Immunohistochemistry revealed that all the major differentiated lineages were present in such crypts. Interestingly mixed crypts were also present (containing both CCO+ve and −ve cells) suggesting multiple stem cells are present in these crypts. Furthermore, we observed crypts whose Paneth cells were CCO+ve but the rest of the crypt was negative suggesting that Paneth cells have a specific progenitor or are long lived. Patches of CCO-ve crypts which all contain the same mtDNA mutation were also observed, suggesting that a founder crypt has expanded by fission.
Conclusion: These data suggest that small bowel crypts are clonal, contain multiple stem cells and that fission is a method by which mutations spread through the small bowel. Partially-mutated crypts revealed some interesting features of small bowel crypt stem cell biology where Paneth cells, in some cases remained CCO+ve in otherwise CCO−ve crypts. This suggests slow turnover of Paneth cells or a committed, specific long-lived progenitor was present. These results may have important implications for the development of small bowel tumours and demonstrate how mutations are fixed and spread in the small intestine.
0-05 METHODS FOR TRACING CRYPT STEM CELLS ANCESTRY AND CLONAL ARCHITECTURE USING CPG ISLAND METHYLATION AND MITOCHONDRIAL DNA MUTATIONS
T. A. Graham, A. Humphries, S. J. Leedham, S. A. McDonald, N. A. Wright. Histopathology Unit, Cancer Research UK, London Research Institute, London, UK
Introduction: We have been investigating the utility of methylation patterns to investigate the clonal expansion of human colonic crypts. Methylation of the CpG islands of some non-expressed genes has been shown to be a useful clonal marker to study cell turnover within crypts.1 2 However, doubt remains about the efficacy of methylation as a clonal marker to investigate expansion of the crypts themselves. However, despite this uncertainty, methylation patterns are used to study clonality throughout the gastrointestinal tract. Recently, we have shown that mitochondrial DNA (mtDNA) mutations provide an excellent method to investigate clonal expansion of colonic crypts.3 Patches of adjacent mutated crypts, deficient in the mitochondrially encoded enzyme cytochrome-c-oxidase, are frequently observed: these patches form through repeated rounds of fission of the original mutated crypt. Mutated crypts share the exact same mtDNA mutation, confirming their shared ancestry. Here, we have investigated whether methylation patterns can reveal the shared ancestry of crypts that have been shown to be related by mtDNA. We considered how the dynamics of stem cell division may cause the methylation patterns of two related crypts to diverge.
Aims and Methods: Serial sections of normal colonic mucosa were histochemically stained for cytochrome-c-oxidase activity. A second stain for succinate dehydrogenase activity was used to highlight cytochrome-c-oxidase deficiency. Crypt relatedness was confirmed by direct sequencing of the entire mtDNA genome. Mutated crypts, and nearby wild-type crypts, were then individually laser-capture micro-dissected. DNA was extracted, bisulphite treated, and the BGN and CSX loci were PCR amplified. Single cell resolution was achieved by TA-cloning of the PCR products. Individual clones were then sequenced. The methylation patterns were analysed using a mathematical model of stem cell division and crypt fission.
Results: Two crypts shown to be related by mtDNA mutation tended to have methylation patterns that were as dissimilar to one another, as the methylation patterns from two unrelated crypts. This result could be explained by a rapid turnover of stem cells within a crypt, asymmetric segregation of stem cells between daughter crypts during fission, or a divergence of methylation patterns in the long intervals between successive crypt fission events.
Conclusion: Methylation patterns do not confirm the shared ancestry of crypts that are clonal for the same mtDNA mutation. Methylation patterns are changeable over long time periods and reflect the dynamic processes of stem cell turnover within a crypt.
0-06 ANTIGEN RETRIEVAL AND PRIMARY ANTIBODY TYPE AFFECT SENSITIVITY BUT NOT SPECIFICITY OF CD117 IMMUNOHISTOCHEMISTRY
N. A. Wong, Z. Melegh. Department of Histopathology, Bristol Royal Infirmary, Bristol, UK
Introduction: CD117 (c-kit) immunohistochemistry plays important roles in the diagnosis of gastrointestinal stromal tumours (GISTs) and the assessment of whether a neoplasm may be suitable for tyrosine kinase inhibitor therapy. There is concern that using antigen retrieval with such immunohistochemistry will produce false positive results, and there are some data suggesting different CD117 antibodies stain different cell and neoplasm types. However, this concern has not been formally investigated, and the data derive from only a handful of studies looking at a few neoplasm types.
Aims and Methods: This study was designed to comprehensively investigate the effects of antigen retrieval and primary antibody selection on specificity and sensitivity of CD117 immunohistochemistry, using a wide range of neoplasm types including those previously described as suitable for tyrosine kinase inhibitor therapy. A survey and literature review were performed to determine the most commonly used CD117 antibodies. All the antibodies thus identified were tested with various immunohistochemical protocols to see whether optimal staining was achievable both with and without antigen retrieval. All the optimisable antibodies were used to immunostain (with and without antigen retrieval) 32 GISTs and 139 neoplasms (comprising 24 neoplasm types) that are differential diagnoses for GIST and/or have been reported to express CD117.
Results: Of the six most commonly used CD117 antibodies highlighted by the survey and literature review, three (Neomarkers polyclonal RB-1518, Novocastra monoclonal T595, and Santa Cruz polyclonal C19) were rejected as only suboptimal staining was achieved. With the three remaining antibodies (Cell Marque polyclonal CMC766, Dako polyclonal A4502 and Epitomics monoclonal YR145), antigen retrieval generally increased the sensitivity (amongst GIST and non-GIST neoplasms), but did not alter the specificity of immunostaining. The different antibodies showed variations in sensitivity but did not stain different spectrums of neoplasm type. A small number of neoplasms showed scattered nuclear staining (particularly seen without antigen retrieval), which was regarded to represent cross-reactivity.
Conclusion: Antigen retrieval and changing between the three antibodies tested affect sensitivity but not specificity of CD117 immunohistochemistry. Antigen retrieval does not produce false positive CD117 immunostaining.
0-07 CITED 1 IS A NOVEL COLORECTAL CANCER GENE WHOSE DEFICIENCY INHIBITS THE GROWTH OF COLORECTAL CANCER
1F. Song, 2T. Phesse, 1J. Jenkins, 2A. Clarke, 1A. J. M. Watson. 1School of Clinical Sciences, University of Liverpool, Liverpool, UK, 2School of Bioscience, University of Cardiff, Cardiff, UK
Introduction: APC gene mutation is one of the early genetic lesions in the pathogenesis of colorectal cancer. To investigate the primary consequences of APC loss in the intestine, a conditional knock-out mouse model has been developed. We have shown that most of the genes that are deregulated following deletion of APC in mouse intestinal epithelium are also deregulated in human colorectal cancer. We found that Cited1 (CBP/p300-interacting transactivators with glutamic acid [E]/aspartic acid [D]-rich carboxyl-terminal domain, 1) is over-expressed 2.74-fold (n = 40, p<0.00001) in human colorectal cancers compared to adjacent uninvolved colonic mucosa. Little is known about Cited1 but has been characterised as a non-DNA binding transcriptional co-factor. It has been implicated in embryogenesis and breast and thyroid carcinogenesis. These preliminary data suggested that Cited1 may be involved in colorectal carcinogenesis.
Aims and Methods: We investigated the effects of Cited1 deficiency on colorectal carcinogenesis both in vivo and in vitro. ApcMin/+Cited1+/+, ApcMin/+Cited1−/+and Apc Min/+Cited1−/Y mice were generated by crossing Cited1 null mice onto an ApcMin/+background. Semi-QPCR was performed to characterise recombined Cited1 expression in the adenomas taken from the three cohorts. siRNA was transfected into human colon cancer cell lines HT29 and HCT116 to reduce Cited1 expression (mRNA expression was detected by taqman QPCR). Cell survival and proliferation post transfection were measured by clonogenic and SRB assays.
Results: As Cited1 is X-linked, the homozygous null mice are all males. The median life span of ApcMin/+Cited1+/+(n = 17) was 250 days, which was significantly increased to 333 days on ApcMin/+Cited1−/+ (n = 20, p = 0.0008), and further to 378 days on ApcMin/+Cited1Y/− (n = 6, p = 0.0004). Cited1 expression was reduced by target siRNA by 80% in HT29 (n = 3, p = 0.018) and 95% in HCT116 cells (n = 4, p = 0.007). In clonogenic assay, both cell lines were less viable when treated with target Cited1 siRNA than when treated with non-target siRNA (n = 6, p<0.002), suggesting that loss of Cited1 increases cell death. Cell proliferation was most dramatically reduced 5 days post transfection in HT29 (44% reduction, n = 6, p<0.001) and 4 days in HCT116 cells (34% reduction, n = 6, p<0.001).
Conclusion: Cited1 is over-expressed in human colorectal cancer, which implies that Cited1 is involved in intestinal carcinogenesis. Our data demonstrates that deficiency of one or both Cited1 alleles leads to a stepwise increase in life span of MIN mice. In cultured human colon cancer cells, reduction in expression of Cited1 increases cell death and significantly reduces cell proliferation. We conclude that Cited1 is a previously unrecognised component of colorectal carcinogenesis.
Small bowel and nutrition free papers
0-08 RECENT EXPERIENCE OF ADULT SMALL INTESTINAL TRANSPLANTATION AND MULTIVISCERAL TRANSPLANTATION AT ADDENBROOKE’S HOSPITAL, CAMBRIDGE, UK
1A. Wiles, 2N. V. Jamieson, 1J. Woodward, 2C. Watson, 2A. Butler, 2P. Gibbs, 2R. Praseedom, 3S. Gabe, 1S. Duncan, 1S. J. Middleton. 1Gastroenterology, Cambridge University Hospital, Cambridge, uK, 2Surgery, Cambridge University Hospital, Cambridge, UK, 3Gastroenterology, St Mark’s Hospital, London, UK
Introduction: The first intestinal transplantation in the UK was undertaken in Cambridge in 1991. Despite comparatively good results, only 14 further adult patients underwent the procedure in the UK over the next 15 years. However, over the last 12 months 5 patients have received small intestinal grafts in Cambridge.
Aims and Methods: All candidates for transplantation are discussed at the national adult intestinal transplantation forum (NASIT) by a multidisciplinary team from the intestinal failure and transplantation centres before being listed for transplantation. Patients receive lymphocyte depleting induction therapy and single agent maintenance immunosuppression.
Results: In the last 12 months in Cambridge, 5 patients received intestinal grafts either isolated or part of a cluster with other organs. All patients survived and are independent of parenteral nutrition. A male (35 years) with visceral myopathy, loss of venous access, and intractable vomiting received a modified multivisceral graft (stomach, pancreas, small intestine, spleen). An episode of cutaneous graft versus host disease resolved with treatment. A female (24 years) with long segment Hirschsprung’s and loss of venous access received an isolated intestinal graft and had an uncomplicated post operative course. A male (34 years) with short bowel from Crohn’s disease and PN related cirrhosis received a multivisceral graft (liver, stomach, small intestine, pancreas), experienced a single episode of mild rejection and remains well. A female (36 years) with FAP, a large unresectable duodenal polyp, extensive intra-abdominal desmoid disease encasing mesenteric vessels and causing ureteric obstruction, received a multivisceral graft (stomach, small intestine, pancreas, liver) and made an uncomplicated recovery. A female (35 years) with FAP and desmoid disease has recently undergone a modified multivisceral procedure (stomach, intestine, pancreas, kidney); she remains well and is PN independent 2 weeks after surgery. The postoperative inpatient stay of completed episodes ranged from 41 to 84 days, with a mean of 45 days.
Conclusion: Our recent experience demonstrates that short term survival after intestinal transplantation is now excellent and grafts are fully functional restoring normal oral nutrition. Multivisceral grafting resolves problems with associated organ dysfunction or failure. It is imperative to refer patients before they develop co-morbidity that precludes transplantation. Clinicians are welcome to attend the NASIT Forum.
0-09 THE BRITISH INTESTINAL FAILURE SURVEY (BIFS) – A REGISTRY TO DETERMINE THE FREQUENCY AND OUTCOME OF CHILDHOOD INTESTINAL FAILURE
1H. S. M. Gowen, 2J. W. L. Puntis, 3C. Lloyd. 13rd Floor Registry Office, Institute of Child Health, Birmingham, UK, 2Room 142, B Floor, Clarendon Wing, The General Infirmary, Leeds, UK, 3Liver Unit, Birmingham Children’s Hospital, Birmingham, UK
Introduction: Intestinal failure (IF) is a complex, life threatening disorder requiring highly specialised treatment and with great variation in outcome. Most patients recover, many require continuing support on home parenteral nutrition and a proportion may progress to intestinal transplantation (ITx). The paucity of information in the UK about incidence, causes and outcome of IF has impeded planning of long term clinical services including transplantation.
Aims and Methods: The British Intestinal Failure Survey (BIFS) aim is to prospectively identify all cases of IF (defined as parenteral nutrition dependency for >28 days) in children throughout the UK. In an initial pilot study set up by the British Society of Paediatric Gastroenterology, Hepatology and Nutrition (BSPGHAN), children <19 years of age were enrolled; outcome data (PN dependency status; complications; transplantation; death) were solicited at 6 monthly intervals.
Results: Currently 22 centres have Trust R&D approval to participate in BIFS, 10 of which have so far registered patients; 3 more centres are currently seeking approval. Between July 2005 and September 2008, 162 infants and children (83 M, 79 F) were registered; the median age at commencement of PN was 11 days (range from birth to 17 years).
Conclusion: This pilot study has successfully collected national data on children with IF through a cooperative effort on the part of the BSPGHAN and BAPS (British Association of Paediatric Surgeons). Maintaining recruitment over time and obtaining follow up data will depend on continuing commitment fostered through close links between the BIFS Registry Manager and reporters in participating centres.
0-10 META-ANALYSIS: THE USEFULNESS OF ANTIBODIES TO DEAMIDATED GLIADIN PEPTIDES TO EXCLUDE OR DIAGNOSE COELIAC DISEASE
N. R. Lewis. Division of Epidemiology and Public Health, University of Nottingham, Nottingham, UK
Introduction: With the appreciation of the high prevalence of coeliac disease there is increasing use of serology in screening asymptomatic people and testing those with suggestive features. Both endomysial antibody and tissue transglutaminase antibody (tTG) have very high sensitivities (93% for both) and specificities (>99% and >98% respectively) for the diagnosis of typical coeliac disease with villous atrophy,1 though with a number of practical advantages tTG is the most commonly used test. Food-derived gliadin peptides are deamidated in the gut by tissue transglutaminase as part of the immune response to gluten in coeliac disease; quantitative detection of antibodies to these deamidated gliadin peptides has been proposed as a new and reliable tool for diagnosing coeliac disease.
Aims and Methods: To compare the sensitivities and specificities of the deamidated gliadin peptide (DGP) and tTG antibody tests. MEDLINE and EMBASE databases were searched up to October 2008 for relevant papers using the terms deamidated gliadin peptide and tissue transglutaminase antibody. Statistical heterogeneity across the studies was assessed using Cochran’s Q statistic. Random effects meta-analysis modelling was used to derive pooled estimates of sensitivity and specificity using Stata software.
Results: 10 relevant studies were identified containing 1414 controls and 774 (35%) people with untreated coeliac disease that compared DGP with tTG. Pooled sensitivity of IgA DGP antibody test was lower (90.0%, 95% CI 86.1 to 94.1) than that of IgA tTG (94.3%, 95% CI 91.5 to 97.1). Pooled specificity of IgA DGP (95.2%, 95% CI 93.4 to 97.1) was similar to that of IgA tTG (96.9%, 95% CI 95.1 to 98.7). The highest positive likelihood ratio (i.e. the most powerful at confirming a diagnosis of coeliac disease) was provided by IgA tTG (30.4) versus 18.8 by IgA DGP. The lowest negative likelihood ratio (i.e. most powerful at excluding coeliac disease) was provided by IgA tTG (0.06) versus 0.11 by IgA DGP.
Conclusion: IgA DGP has equivalent specificity to IgA tTG for the purposes of ruling out coeliac disease but somewhat lower sensitivity for making the diagnosis. When compared with DGP, IgA tTG remains the preferred test for screening asymptomatic people and for excluding coeliac disease in symptomatic individuals with a low pre-test probability.
0-11 LONG TERM FOLLOW UP OF PATIENTS WITH REFRACTORY COELIAC DISEASE: A SINGLE CENTRE EXPERIENCE
1S. S. Salunke, 1M. Priest, 2R. Jackson, 1A. J. Morris. 1Gastroenterology Unit, Glasgow Royal Infirmary, Glasgow, UK, 2Pathology, Glasgow Royal Infirmary, Glasgow, UK
Introduction: Coeliac disease (CD) is a common condition seen in people of North European/Celtic decent. A proportion of patients develop refractory coeliac disease (RCD) and subsequent complications like ulcerative jejunitis (UJ) and enteropathy associated T-cell lymphoma (EATL). A European study has suggested a very high risk of transformation from refractory coeliac to lymphoma.
Aims and Methods: We aimed to study our large single centre cohort of RCD patients to assess their long term outcome. We identified patients with RCD or abnormal immunophenotype of intraepithelial lymphocytes (IELs) from our Pathology database between 1995 and 2008. Each of the patients was analysed to find out the timing of onset of RCD, abnormal immunophenotype and development of UJ or EATL. We also studied the mean survival of the group.
Results: 35 patients with RCD or abnormal intraepithelial T-cell immunophenotype were identified. Of these 8 were excluded as they were not under follow up in our unit. Of the remaining 27, 16 (59%) were females. In 55% of patients there was documented evidence of adherence to gluten free diet. The tissue transglutaminase (TTG)/anti-Endomyseal antibody (anti-EMA Ab) status was negative in 11 of the patients at the time refractory status was confirmed. 22 patients (81%) expressed the high risk CD3+/CD8− IEL immunophenotype. In 5 patients, it was noted that they expressed CD8+ve IELs. 30% of patients had coexisting CD30+ve lymphocytes. 75% showed evidence of monoclonality to T-cell receptor gene rearrangement. Of these patients, 41% (11 of 27) showed evidence of UJ during the disease course. 5 patients (18%) (3 males) developed either EATL or extraintestinal lymphoma with the same clone as found in the small bowel. All 5 were CD8 negative, 4 were CD30+ve. 4 expressed a monoclonal T-cell gene rearrangement. 3 patients in the lymphoma group suffered from UJ. The average time from development of RCD to lymphoma in this group was 3.68 years. Median survival of patients with EATL was 2 years (range 0.1 to 13 years, mean 4.4 years).
Conclusion: In our experience of patients with RCD, 41% develop ulcerative jejunitis. Of our patients with RCD 18% percent develop enteropathy associated T-cell lymphoma (EATL).
0-12 CAUSES OF DEATH IN PEOPLE WITH COELIAC DISEASE: OBSERVATIONS MADE IN DERBY, UK, OVER A QUARTER OF A CENTURY
1J. West, 1M. J. Grainge, 1T. R. Card, 2G. K. T. Holmes. 1Epidemiology and Public Health, University of Nottingham, Nottingham, UK, 2Gastroenterology, Derby Royal Infirmary, Derby, UK
Introduction: Cause-specific mortality has been described infrequently in coeliac disease, primarily due to a lack of population based cohorts of adequate size and follow up. We therefore aimed to quantify the risks of major causes of death in a large, unselected cohort that has been followed for over a quarter of a century.
Aims and Methods: We used a prospective cohort study of people with coeliac disease who were identified in Derby, UK during 1978 to 2006 with follow up for death until 31 December 2006. We calculated Standardised Mortality Ratios (SMR) for all cause mortality and various cause-specific groups using population data from the Office of National Statistics for the period 2 years after diagnosis of coeliac disease.
Results: There were 1505 people with coeliac disease identified (the majority of which >90% were incident) in Derby during the study of whom 1224 had greater than 2 years of follow up. 47 deaths occurred within 2 years of diagnosis and 151 occurred in the post-diagnosis period during 10554 person years of follow up. The mean age at entry to the study was 45 years and the majority of individuals were female (69%). We found statistically significant increases in all cause mortality (SMR 1.4), deaths from cancer (SMR 1.5) and deaths from digestive diseases (SMR 2.3). Three of the deaths from digestive disease causes were due to coeliac disease itself.
Conclusion: Two years after diagnosis people with coeliac disease have a 40% increase in all cause mortality compared with the general population. This excess is mostly explained by deaths from cancer and respiratory disease. There was a 2-fold increased risk of dying from non-malignant digestive disease which was partly explained by deaths from coeliac disease. Coeliac disease confers only a small increase in mortality risk compared with the general population.
0-13 SELECTIVE USE OF METOCLOPRAMIDE IMPROVES THE COMPLETION RATE OF SMALL BOWEL CAPSULE ENDOSCOPY
R. Sidhu, K. Drew, R. Sood, D. S. Sanders, M. E. McAlindon. Gastroenterology, Royal Hallamshire Hospital, Sheffield, UK
Introduction: Capsule endoscopy is a first line investigative modality for the small bowel. However 15–20% of examinations terminate before the capsule reaches the caecum. The real time viewer (RTV) allows the clinician to view live transmitted images and determine whether or not the capsule has left the stomach.
Aims and Methods: To determine if the selective use of metoclopramide in patients with delayed gastric emptying of the capsule improves small bowel examination completion rate. Data collected included demographics, co-morbidity, medications (including opiates and tricyclic antidepressants), indication for procedure, gastric and small bowel emptying times and diagnostic yield. All patients underwent a 12 hour fast and had 2L polyethylene glycol electrolyte solution the day before the procedure. Data were compared (using SPSS) before and after the introduction of a protocol whereby trained nursing staff administered metoclopramide (10 mg iv) if the RTV showed gastric retention of the capsule at 30 mins.
Results: Data were collected on 245 consecutive patients (group 1 (n = 145): standard procedure; group 2 (n = 100): new protocol). The mean age in the entire cohort was 52 years (16–86 years). The prevalence of comorbidities or use of drugs affecting gastric emptying did not differ between the groups. Metoclopramide was administered in 14% of patients in group 2. There was no significant difference in the gastric emptying times (GET) between the two groups (mean±SE GET 76 min±15 and 64 min±24 (p = 0.67) for groups 1 and 2, respectively), although small bowel transit time was reduced in group 2 (329 min±24 compared to 411 min±27 in group 1 (p = 0.025, 95% CI 10.3 to 153)). Thus complete small bowel examination was significantly more likely in group 2 (90% compared to 77% in group 1 (p = 0.01)). On logistic regression, the presence of co-morbidity or medication did not affect completion of small bowel examinations. There was no significant difference in the diagnostic yields between the two groups (50% versus 43%, p = 0.3).
Conclusion: A protocol using the RTV to guide the selective use of metoclopramide reduces small bowel transit time and improves complete small bowel examinations without affecting diagnostic yield.
0-14 PANCREATIC INSUFFICIENCY IN ADULT COELIAC DISEASE: DO PATIENTS NEED PROLONGED ENZYME SUPPLEMENTATION?
1J. S. Leeds, 2S. M. Morley, 1D. S. Sanders. 1Gastroenterology and Liver Unit, Royal Hallamshire Hospital, Sheffield, UK, 2Clinical Chemistry, Royal Hallamshire Hospital, Sheffield, UK
Introduction: Coeliac disease (CD) is associated with exocrine pancreatic insufficiency which may lead to continued or recurrent gastrointestinal symptoms. We previously reported on a large cohort of patients with CD (n = 209) and found that 20/66 patients with current/persistent diarrhoea had exocrine insufficiency. In addition, 19/20 patients improved on pancreatic supplementation. There are, however, no data on long term need for treatment.
Aims and Methods: The 20 patients who had initially received therapy for exocrine pancreatic insufficiency were prospectively followed up for 4 years since the intervention with pancreatic supplementation. Current gastrointestinal symptoms were recorded along with coeliac antibody status and duration/dose of enzyme supplementation. Faecal elastase-1 was repeated to reassess exocrine pancreatic function.
Results: 19/20 patients were reviewed as 1 had died (mean age 59.7, 6 males). Mean duration of coeliac disease was 13.2 years. 11/19 were still taking enzyme supplementation at a mean dose of 45,000 units of lipase per day. Only 1/11 did not feel there was symptomatic benefit. 8/19 patients had discontinued supplementation as their diarrhoea had improved. When comparing those who were still on supplementation and those who had discontinued supplementation, there was no difference in median number of stools per day (p = 0.21), duration of CD (p = 0.86), mean age (p = 1.0), median tTG (p = 0.67) or mean faecal elastase-1 levels (p = 0.13), but there were significantly more males still taking supplementation (6/11 vs 0/8, p = 0.01). In the whole group there was a significant increase in faecal elastase-1 levels from diagnosis, at six months and currently with median values of 90, 212 and 365, respectively (p<0.0001).
Conclusion: Faecal elastase-1 is helpful in identifying CD patients with diarrhoea and exocrine pancreatic insufficiency. Our longitudinal data suggest that pancreatic enzyme supplementation could be discontinued in a substantial proportion of patients as symptoms improve. Females are more likely to discontinue supplements than males.
0-15 SMALL BOWEL BACTERIAL OVERGROWTH BREATH TESTING: COMPARISON OF GLYCOCHOLATE AND HYDROGEN BREATH TESTS
1S. C. Cooper, 1R. Kalaiselvan, 2P. Nightingale, 3W. Johns, 3J. Shaffer. 1Intestinal Failure Unit, Hope Hospital, Salford, UK, 2Wolfson Computer Laboratory, Queen Elizabeth Hospital, Birmingham, 3Nuclear Medicine Department, Hope Hospital, Salford, UK
Introduction: As jejunal aspiration and culture, the gold standard for diagnosing small bowel bacterial overgrowth (SBBO), is both invasive and impractical, hospitals employ breath testing, compromising practicality for reduced sensitivity and specificity. Hope Hospital performs both glycocholate and hydrogen breath testing, attempting to improve accuracy. We examined the agreement of breath tests, identifying causes for any disparity.
Aims and Methods: All breath test reports for SBBO at Hope Hospital, Salford 1992–2008 were examined. Kappa statistic identified degree of agreement. Patients with heterogeneous results had their electronic records examined, with comparison of variables including anatomy and primary diagnosis using Fisher’s exact test.
Results: 1903 patients underwent simultaneous glycocholate and hydrogen breath testing. Test agreement in 77% (1472/1903), kappa coefficient 0.45 (moderate agreement): 306 cases glycocholate +ve and hydrogen −ve (45 notes examined), and 95 cases glycocholate −ve and hydrogen +ve (27 examined). Presence of stoma, intact stomach or small bowel did not differ between groups. Crohn’s disease, and absence of an intact colon was more common in the glycocholate +ve, hydrogen −ve group (p = 0.019 and p = 0.023, respectively).
Conclusion: Agreement is only moderate between breath tests, with glychocholate testing positive more frequently than hydrogen, as a consequence of confounding from Crohn’s disease and the absence of an intact colon. Hydrogen breath testing may offer greater accuracy, but reports from breath testing need to be correlated with clinical findings and gastrointestinal anatomy, especially the presence of the colon. Combining two tests does not appear to clarify reports.
0-16 PREVALENCE AND CONSEQUENCE OF HYPERTRANSAMINASAEMIA IN INCIDENT COELIAC DISEASE: HOW COMMON IS IT AND DOES IT MATTER?
1N. R. Lewis, 2D. S. Sanders, 3K. Teahon, 1R. F. A. Logan, 1K. M. Fleming, 1J. West. 1Division of Epidemiology and Public Health, University of Nottingham, Nottingham, UK, 2Department of Gastroenterology, Royal Hallamshire Hospital, Sheffield, UK, 3Department of Gastroenterology, Nottingham City Hospital, Nottingham, UK
Introduction: Small-sized and historical case series report that elevated serum transaminases in the absence of autoimmune liver disorders is common in coeliac disease, affecting 40% of untreated coeliacs. Such reversible, gluten-related hepatic injury has been coined “coeliac hepatitis”.1 However, we have little idea of the true contemporary prevalence of hypertransaminasaemia in incident coeliac disease and what happens on treatment.
Aims and Methods: To quantify the prevalence of hypertransaminasaemia in a contemporary cohort of adults with incident coeliac disease and response to treatment with a gluten-free diet (GFD). 616 people newly diagnosed with coeliac disease between 2002–2006 at Nottingham University Hospital and Royal Hallamshire Hospital were studied. Alanine aminotransferase (ALT), alkaline phosphatase (ALP), albumin and platelet counts were measured at diagnosis and following a mean 12.3 months treatment with GFD. Abnormal tests were defined as above the upper limit of normal range (ULN) for the laboratory of each hospital.
Results: ALT was elevated in 60 of 572 patients (10.49%; 95% CI 8.24 to 13.27) at diagnosis of coeliac disease with ALT elevated within 2×ULN in 52 patients (9.09%; 95% CI 7.00 to 11.73). Only 1.40% (95% CI 0.70 to 2.74; n = 8) of the incident coeliac cohort had ALT value above 2×ULN. Abnormal ALT at diagnosis of coeliac disease was associated with those presenting with malabsorption (OR 2.89; 95% CI 1.88 to 7.01) or with a more severe histological abnormality (OR 2.00; 95% CI 1.09 to 3.69). ALP was elevated in 61 of 580 (10.52%; 95% CI 8.28 to 13.28) newly diagnosed coeliacs though only 1.90% (95% CI 1.06 to 3.37; n = 11) of the cohort had ALP above 2×ULN. Presence of osteomalacia was associated with 8-fold increased risk of having abnormal ALP at diagnosis of coeliac disease (OR 8.00; 95%CI 1.11, 57.78). Significant mean reductions in ALT (3.67 U/L; SD 25.69) and ALP (18.90 U/L SD 61.23) occurred on treatment with GFD.
Conclusion: Clinically important abnormalities of liver profile tests are uncommon in incident coeliac disease with only 9% of incident coeliacs having an elevated ALT. With proportion of hypertransaminasaemia similar to that expected in the general population2 and significant reduction in ALT occurring on treatment, our results suggest that a rigorous search for liver disease in people newly diagnosed with coeliac disease may not be warranted.
0-17 IDIOPATHIC BILE ACID MALABSORPTION IS AN IMPORTANT CAUSE OF SYMPTOMS FREQUENTLY MISDIAGNOSED AS DIARRHOEA-PREDOMINANT IRRITABLE BOWEL SYNDROME
1L. Wedlake, 2R. A’Hern, 3D. Russell, 4K. Thomas, 5J. R. F. Walters, 6J. Andreyev. 1Dept of Dietetics, Royal Marsden Hospital, London, UK, 2Statistics, Institute of Cancer Research, London, UK, 3Knowledge Resources, Royal Marsden Hospital, London and Sutton, UK, 4Statistics, Royal Marsden Hospital, London, UK, 5GI Unit, Hammersmith Hospital, London, UK, 6GI Unit, Royal Marsden Hospital, London, UK
Introduction: Chronic or recurrent, watery diarrhoea affects one third of patients diagnosed as having irritable bowel syndrome (IBS). In the last 30 years, repeated suggestions have been made that idiopathic bile acid malabsorption (I-BAM) may be the cause of this diarrhoea in patients whose clinicians have failed to consider this as a possibility, or have lacked access to appropriate diagnostic tools.
Aims and Methods: To determine the prevalence of idiopathic bile acid malabsorption as a cause for unexplained chronic diarrhoea in patients suffering from diarrhoea-predominant irritable bowel syndrome (IBS-D). A systematic search was performed of all publications reporting the proportion of patients presenting with diarrhoea-predominant irritable bowel type symptoms, who were subsequently confirmed as having I-BAM on the basis of a (SeHCAT) test. Data were combined to produce summary estimates of the prevalence of I-BAM amongst this patient group.
Results: 18 (English language) studies, 15 prospective, published between 1985 and 2007 comprising 1223 patients were identified in which patients diagnosed with IBS-D type were investigated for bile acid malabsorption. Pooled data from 5 studies (429 patients) indicated a 10% (CI: 7% to 13%) prevalence of I-BAM at 7 day (7d) SeHCAT cut-off <5%; at 7dSeHCAT cut-off <10%, 17 studies (1073 patients) indicated prevalence to be 32% (CI: 29% to 35%); 7 studies (618 patients) using a 7dSeHCAT cut-off <15% indicated prevalence of I-BAM to be 26% (CI: 23% to 30%). Pooled data from 15 studies showed a dose-response relationship according to severity of malabsorption to treatment with a bile acid binder: response to colestyramine occurred in 96% of patients with <5% retention, 80% at <10% retention and 70% at <15% retention.
Conclusion: Idiopathic adult-onset bile acid malabsorption is not rare. International guidelines for the management of IBS need to be revised so that clinicians become more aware of this possibility.
Endoscopy free papers
0-18 EFFICACY OF BISPECTRAL MONITORING AS AN ADJUNCT TO PROPOFOL DEEP SEDATION FOR ENDOSCOPIC RETROGRADE CHOLANGIOPANCREATOGRAPHY (ERCP): A RANDOMISED CONTROLLED TRIAL
1I. Chainaki, 2G. Tribonias, 2K. Konstantinidis, 1M. Parasiri, 1R. Rouchota, 3K. Psaras, 2A. Theodoropoulou, 2E. Vardas, 1M. Manolaraki, 2G. A. Paspatis. 1Anesthesiology, Benizelion, Heraklion, Greece, 2Gastroenterology, Benizelion, Heraklion, Greece, 3Radiology, Benizelion, Heraklion, Greece
Introduction: Bispectral (BIS) monitoring provides an objective measure of the level of consciousness in sedated patients. Occasionally, therapeutic endoscopic retrograde cholangiopancreatography (ERCP) lasts for an hour or even longer and so “proper” sedation is a reasonable request. In this study, we hypothesised that if we achieved the desired level of deep sedation with minimal doses of propofol by using BIS, then the risk of respiratory depression would be reduced. We sought to determine whether BIS is a useful adjunct to the administration of propofol titrated to deep sedation as measured by reductions of doses of propofol administered during ERCP. To the best of our knowledge, this is the only prospective, randomised, comparative study on this subject.
Aims and Methods: Sample size calculation showed that at least 41 patients on each group were needed in order to achieve a statistical power of 80% to detect a 0.05 mg/kg/min reduction in the amount of propofol given between the two groups at the 5% level of significance. Ninety consecutive patients undergoing ERCP were randomised to receive propofol titrated to deep sedation with BIS visible to anaesthesiologist (n = 46) versus BIS invisible to anaesthesiologist – control group (n = 44). In the BIS group, the anaesthesiologist was instructed to use BIS as the primary endpoint for titration of sedation, and to target BIS value ⩽60. In the control group, the anaesthesiologist was instructed to titrate propofol according to routine practice in the unit using the modified assessment of alertness/sedation (MOAA/S) scale. In both groups, propofol was administered by continuous infusion using a medical pump.
Results: The mean (SD) propofol dose (mg/min/kg) was 0.13 (0.02) and 0.19 (0.02) for BIS and controls, respectively (p<0.001). The mean (SD) total propofol dose was 477.46 (187.3) and 584.5 (182.7) for BIS and controls, respectively (p = 0.007). The mean (SD) BIS value throughout the procedure was 61.68 (7.5) and 56.93 (4.77) for BIS and controls, respectively (p = 0.01). During the maintenance phase of sedation (MOAA/S: 0 or 1), the mean (SD) BIS value was 53.73 (8.67) and 45.65 (4.39) for BIS and controls, respectively (p<0.001).
Conclusion: Our data suggest that BIS led to a reduction in the mean propofol dose when used as the primary target for sedation in ERCP procedures. These results need to be confirmed in larger studies.
0-19 PROPHYLACTIC PANCREATIC DUCT STENTS IN THE PREVENTION OF POST- ENDOSCOPIC RETROGRADE CHOLANGIOPANCREATOGRAPHY (ERCP) PANCREATITIS: AN ANALYSIS OF PRACTICE IN A SINGLE UK TERTIARY REFERRAL CENTRE
P. Kennedy, E. A. Russo, N. Kumar, N. Powell, D. Bansi, A. Thillainayagam, P. Vlavianos, D. Westaby. Gastroenterology, Hammersmith Hospital, London, UK
Introduction: Post-ERCP pancreatitis is associated with significant morbidity and mortality. In selected cases, temporary prophylactic pancreatic duct (PD) stent insertion reduces the incidence of post-ERCP pancreatitis. There are few data available regarding the utility of PD stent insertion in British ERCP clinical practice.
Aims and Methods: The aim of this study was to report “real-life” clinical data from a single UK tertiary referral pancreatobiliary centre, where prophylactic PD stent insertion is routine practice in selected high risk endoscopic retrograde cholangiopancreatography (ERCP) procedures. We report data including indications for PD stenting, rates and severity of pancreatitis and clinical outcome for each procedure. We also assessed a number of clinical and laboratory parameters in patients developing post-ERCP pancreatitis with and without prophylactic PD stent insertion.
Results: Data are reported from 1000 consecutive ERCPs performed in 688 patients (377 female) in our unit. Prophylactic PD stents were inserted in 5.8% of procedures. Indications for stent placement were difficult or prolonged cannulation (50%), sphincter of Oddi dysfunction (SOD) (31.1%), pre-cut sphincterotomy (15.5%) and pancreatic sphincterotomy (3.4%). The overall incidence of post-ERCP pancreatitis was 3.6%. Post-ERCP pancreatitis occurred in 22.4% of patients receiving prophylactic PD stents. However, amongst patients developing post-ERCP pancreatitis the frequency of moderate or severe pancreatitis was significantly lower in stented patients (31%) compared to pancreatitis in unstented patients (74%, p<0.002). Similarly, the mean peak serum CRP concentration was also significantly lower in stented patients developing pancreatitis (76.2 mg l−1) compared to unstented patients developing pancreatitis (152.9 mg l−1), p<0.03. The mean peak blood leukocytosis was significantly lower in stented pancreatitis (9.3×109 l−1) compared to stented pancreatitis (14.3×109 l−1) and the mean nadir in serum albumin was significantly higher stented pancreatitis (33.5 g l−1) compared to unstented pancreatitis (26.2 g l−1), p<0.003. In all instances prophylactic PD stents were removed electively without complication.
Conclusion: In our practice, prophylactic PD stents are a safe and effective preventive measure against the development of moderate and severe post-ERCP pancreatitis in selected patients.
0-20 ENDOSCOPIC BALLOON SPHINCTEROPLASTY AS A USEFUL ADJUNCT TO ENDOSCOPIC BILIARY SPHINCTEROTOMY FOR EXTRACTION OF LARGE BILE DUCT STONE – AN EXPERIENCE FROM PAKISTAN
1F. Tariq Berlas, 1S. S. G. Ghazanfar, 1S. S. Q. Qureshi, 2A. A. S. Siddiqui, 1S. S. N. Niaz, 1S. S. Q. Quraishy. 1Surgical Unit 4, Civil Hospital Karachi, Karachi, Pakistan, 2Dow University of Health Sciences, Karachi, Pakistan
Introduction: Endoscopic biliary sphincterotomy is used regularly in therapeutic endoscopic retrograde cholangiopancreatography (ERCP) during extraction of bile duct stones, but sometimes in cases of large bile duct stones it may not be as effective and endoscopic biliary sphincteroplasty may then be used in combination with sphincterotomy to facilitate stone removal.
Aim: Our study aims to evaluate the effectiveness of combined endoscopic biliary sphincterotomy and sphincteroplasty in removal of difficult common bile duct (CBD) stones.
Methods: From February 2007 to September 2008, 60 patients with large CBD stones who underwent combined sphincterotomy and sphincteroplasty were included in the study. Sphincteroplasty was only done when it was either felt that stone size made it unlikely for it to be removed by standard sphincterotomy or the standard attempts failed in removing the stone. Patient bio data, clinical and imaging details and procedural findings were recorded. Endoscopic sphincterotomy followed by endoscopic balloon dilatation using CRE balloon of diameter 15 to 18 mm was performed. Stone extraction and duct clearance were achieved by balloon sweep and using basket or mechanical lithotripter where needed. Immediate and short term complications arising within 1 week of procedure were recorded.
Results: Combined endoscopic sphincterotomy and sphincteroplasty was performed in 60 patients, 24 (40%) male and 36 (60%) female patients. Mean stone diameter was 18.1 mm (range 9 mm–30.2 mm). CRE balloon diameter used ranged from 15 to 18 mm. Complete stone removal was achieved in 57 (95%) patients; stone removal was achieved in single session in 56 (93.3%) patients while 4 (6.7%) patients required two sessions. Stone was removed by balloon sweep alone in 41 (68.3%) patients, basket was used in 14 (23.3%) and mechanical lithotripsy in 5 (8.3%) patients. 3 patients had minor intra procedural bleeding, in 1 patient it stopped spontaneously while in the other two it responded to adrenaline injection at bleeding site. There was no major immediate or short term complications such as perforation or severe pancreatitis. There were no procedure related deaths.
Conclusion: Endoscopic biliary sphincterotomy combined with sphincteroplasty is a relatively safe and effective means of stone removal in difficult and large CBD stone extraction
0-21 COLONOSCOPY – HEALTH GAINS BUT HEART STRAINS ?
1A. T. George, 1A. Rangaraj, 1C. Davis, 2M. C. Allison, 3A. Brian, 2C. Edwards, 2H. Khan, 2P. G. Campbell, 1V. L. Chamary, 1K. J. Swarnkar. 1General Surgery, The Royal Gwent Hospital, Newport, UK, 2General Medicine, The Royal Gwent Hospital, Newport, UK, 3Biochemistry, The Royal Gwent Hospital, Newport, UK
Introduction: Colonoscopy is classed by the American Heart Association as a low risk procedure. However, there have been no studies which have examined in detail, the cardiac effects of undergoing colonoscopy
Aims and Methods: To identify whether colonoscopy can provoke cardiac rhythm disturbances, myocardial ischaemia or cardiac injury as evidenced by troponin I elevation. Patients participating in this prospective cohort study were stratified into three groups according to their risk factors for cardiovascular disease. Group A included patients with any documented significant cardiac co-morbidities. Group B included patients with risk factors for but no proven heart disease. Group C included patients with no risk factors for heart disease. All patients underwent 12-lead Holter monitoring to record their ECGs during the colonoscopic procedure along with a pre and 24-hour post-procedure troponin I estimation. All results were blinded with the ECGs being evaluated independently, by 2 cardiologists.
Results: Two hundred patients participated in the study. There was one 15-day and one 30-day mortality in Group A, from myocardial infarction. Three patients – two in Group A and one in Group B – had high pre-procedure troponin I concentrations (0.12, 0.15 and 0.21 μg/L) with some rise post-procedure to 0.13, 0.16 and 0.23 μg/L respectively (normal troponin I value <0.08 μg/L). None of these three patients had underlying renal dysfunction. Of the 150 ECG analyses which have been completed to date, 3 patients (8%) in the high risk group had significant ST depression and 3 patients (8%) had bundle branch blocks during the procedure. Two patients (5%) developed significant pauses >2 seconds, bradycardia or heart block during the procedure. In Group B, 4 patients (4%) developed supraventricular tachycardias or ST segment depression during the procedure. No patient in Group C had any significant ECG changes during the procedure.
Conclusion: This study demonstrates that colonoscopy can provoke significant cardiac strain and rhythm disturbances. The high incidence of cardiac strain identified in both the high and medium risk group could indicate that non-invasive bowel imaging procedures may need to be discussed as an alternative diagnostic procedure. If confirmed by others, these findings could have implications for colonoscopy-based bowel screening programmes. This study also adds a new dimension in the informed consent of patients with known heart disease or at risk of heart disease, for colonoscopy.
0-22 DEVELOPMENT OF A NEW FREEHAND RADIAL 3D-EUS SYSTEM FOR THE EXAMINATION OF OESOPHAGUS
1S. Inglis, 1D. Christie, 2J. N. Plevris. 1Department of Medical Physics, The Royal Infirmary, Edinburgh, UK, 2Centre for Liver and Digestive Disorders, The Royal Infirmary, Edinburgh, UK
Introduction: Endoscopic ultrasound is an established technique for the examination of malignant and benign GI disorders. However, the procedure is complex and operator dependent, and it is possible to miss subtle changes during examination. The application of 3D-EUS could increase accuracy, provide accurate dimensional and volume measurements, and reduce the subjective nature of the examination.
Aims and Methods: To develop and evaluate a freehand radial three-dimensional EUS system that can be used in the upper GI tract. This technique consisted of image (Matrox Morphis card) and positional (Microscribe 3D digitising arm) capture devices, controlled by a custom program (IC3D), to simultaneously acquire image and position at 12.5 fps, as the scope is withdrawn. The arm tip was secured to the guiding hand of the endoscopist. The reconstruction, analysis and display package was written in Matlab and displayed the volume using different views and allowed distance and volume measurements to be performed. The 3D-EUS system was evaluated in-vitro in a custom EUS ultrasound phantom and in-vivo in different upper GI pathology.
Results: From in-vitro phantom measurements, the average Z dimensional error was <1% and volume errors were 1.2% (object volume = 48930 mm3) and 4.1% (object volume = 5100 mm3). This technique provided accurate dimensional and volume measurements. There is no direct interface with the patient or scope, and can be used with any radial EUS system. It was capable of detecting structures that were missed or not fully investigated by conventional EUS. It could detect an increased number of nodes and localise pathology relative to anatomical structures, to aid treatment planning. In a typical example of the 3D acquisition phase a 30 cm pullback, at an average speed of 0.5 cm/s and captured at a rate of 12.5 fps would last 48 seconds and result in the capture of 600 images, at a 400 μm interval. Examples of a malignant T3N1 tumour and benign cyst are shown in the figures.
Conclusion: 3D reconstruction of EUS images in the endoscopy room results in better characterisation of oesophageal structures, and accurate dimensional/volume measurements. It also enables the endoscopist to review “off-line” the EUS examination in case important information was missed during examination.


0-23 ENDOSCOPIC RESECTION OF LARGE COLONIC POLYPS: FEASIBILITY AND SAFETY
M. D. Duku, R. J. Mead, A. Muddu, A. Fitzjohn, P. Bhandari. Gastrornterology, Queen Alexandra Hospital, Portsmouth, UK
Introduction: Endoscopic resection of large and flat colonic polyps is associated with a high risk of perforation and bleeding. Historically, a significant number of these polyps were referred for surgical resection. However, with advances in therapeutic endoscopy, experienced endoscopists can now endoscopically resect most of these polyps safely. We established a colonic EMR service at Portsmouth towards the end of 2006. We have a dedicated colonic EMR list every week on which only 2 cases are booked. Our patients are all secondary referrals from other consultant colleagues or those referred to surgeons for surgical resection.
Aims and Methods: To assess the feasibility and safety of endoscopic resection of large and difficult colorectal polyps. Records of all patients who had resection of polyps measuring more than 2 cm were retrieved from our EMR service database. We analysed the data for polyp location, morphology, completion of resection, complications and histological staging.
Results: 112 polyps with a mean size of 43 mm (range 20–150 mm) were assessed for endoscopic resection. 23/112 (20.5%) appeared invasive and were referred for surgical resection. 79% of all polyps were left-sided and 75% were flat lesions (LST). In 92% of cases complete endoscopic resection was achieved in one session. EMR related complications were seen in 8/87 of cases. The complications were 1 micro-perforation (exposed muscle layer with no endoscopically visible defect) which was surgically treated, 2 delayed bleeds successfully treated endoscopically, and 5 post polypectomy syndromes treated conservatively. There was no EMR related mortality. Post EMR pathological staging revealed 5 (6.0%) cases, with a mean polyp size of 31 mm (range 20–50 mm), had submucosally invasive adenocarcinoma and underwent surgical resection. 3/5 had no residual tumour in the surgical resection specimen.
Conclusion: Our series demonstrate that endoscopic resection of large (20–150 mm) and flat colonic polyps is feasible and can be done safely, with minimal morbidity and no mortality by experienced advanced endoscopists. The low incidence of invasive cancer in our series highlights the importance of careful endoscopic assessment before resection. We also found that polyps with cancers were not necessarily the largest in size.
0-24 UTILITY OF KUDO PIT PATTERN FOR DISTINGUISHING ADENOMATOUS FROM NON-ADENOMATOUS COLONIC LESIONS IN VIVO: META-ANALYSIS OF DIFFERENT ENDOSCOPIC TECHNIQUES
V. Subramanian, J. Mannath, C. J. Hawkey, K. Ragunath. Nottingham Digestive Diseases Centre and Biomedical Research Unit, Nottingham University and Hospital, Nottingham, UK
Introduction: The pit pattern classification system proposed by Kudo is being increasingly utilised as a tool to predict histology of colorectal lesions with sensitivities of over 90% reported in expert hands. Chromoendoscopy, magnification endoscopy, narrow band imaging (NBI) and Fuji intelligent chromoendoscopy (FICE) are all techniques adopted to improve pit pattern determination. Accurate colonoscopic assessment in vivo has been advocated to avoid the need for histopathology and reduce costs.
Aims and Methods: To do a meta-analysis of the utility of Kudo pit pattern classification in distinguishing adenomatous and non-adenomatous colorectal lesions. We searched several electronic databases for studies which utilised Kudo pit pattern classification for characterisation of colorectal lesions compared with histology (gold standard). The endoscopic methods used to characterise the pit pattern were also recorded. A random effects meta-analysis with correction for over dispersion was done to pool data within the specified subgroups based on the endoscopic method used. Heterogeneity was evaluated using chi square and I2 test.
Results: A total of 26 studies involving 10907 patients and 11585 polyps were included. The pooled sensitivities, specificities, diagnostic odds ratios and AUROC (area under the receiver operating curve) are given in the table above.
Conclusion: The accuracy of Kudo pit pattern to distinguish adenomas depends on the endoscopic technique used. Sensitivities of over 90% can be achieved by magnification endoscopy (ME) with chromoendoscopy (CE). The diagnostic odds ratio for ME with CE seems significantly better than WLE, ME or CE alone. This was the same for small polyps under 10 mm as well. Using ME with CE more than 90% of adenomatous polyps can be identified in vivo.
0-25 RESULTS FROM THE NATIONAL NURSE ENDOSCOPY PROJECT: HANDS-ON TRAINING IMPROVES AND MAINTAINS POLYPECTOMY SKILLS IN THE LONG TERM
A. V. Haycock, M. Vance, S. Thomas-Gibson. Wolfson Unit for Endoscopy, St Mark’s Hospital, Imperial College London, London, UK
Introduction: Nurse endoscopists have become increasingly important for service delivery and to meet national targets. The National Nurse Endoscopy Project (NNEP) aims to standardise training and ensure competence. To utilise the workforce effectively, it is necessary for nurse endoscopists to be competent at basic polypectomy. A dedicated training day was designed involving knowledge-based teaching and hands-on training sessions in polypectomy. Quality assurance evaluation was inbuilt with formative and summative skills assessments, clinical audit and six-month follow-up.
Aims and Methods: Nine nurse endoscopists were trained in the first cohort. A questionnaire completed at their base hospitals was used for pre-assessment of clinical practice and a multiple choice questionnaire was used as a formative assessment of core knowledge underpinning safe polypectomy technique. A pre-course practical skills assessment was performed on ex-vivo animal models using validated assessment tools. Knowledge-based teaching consisted of structured clinical lectures and an interactive DVD training module on the theory and practice of diathermy and polypectomy. Structured practical hands-on skills training was delivered by expert instructors on ex-vivo animal models and computer simulations. A summative assessment was performed at the end of the course. All nurses completed a 6 month prospective clinical audit of practice at base hospitals. All were recalled for follow-up with a repeat of the knowledge assessment and skills assessment at 6 months.
Results: Following training, nurses improved their skills assessment scores from a median (IQR) of 22 (21–26) pre-course to 39 (36–41) post-course (p = 0.003). Assessment scores at six month follow-up showed skills were maintained with median scores of 39 (37–42) (p = 0.78 compared to end of course scores). Knowledge improved significantly with median MCQ scores of 63% pre-course to 77% at six-month follow-up (p = 0.034). The nurses’ continuous audit practice improved with 2/9 (22%) recording their polyp detection rates pre-course to 7/8 (87.5%) at follow-up. Audit of procedures done during the follow-up period was extremely variable, with some nurses having performed less than 5 polypectomies.
Conclusion: A structured hands-on model-based training day significantly improved nurses’ practical skills in polypectomy. At six-month follow-up, skills were maintained and knowledge was improved despite limited ongoing procedural exposure. Such quality assurance indicators confirm the clinical efficacy of this skills based training programme. The NNEP should aim to ensure nurses obtain regular exposure to polypectomy following the course to maximise the educational benefit from the training.
BSG trainee symposium
0-26 ACCEPTABILITY OF SIMULATOR TRAINING IN COLONOSCOPY: RESULTS FROM A MULTINATIONAL RANDOMISED BLINDED CONTROLLED TRIAL
1A. V. Haycock, 2A. D. Koch, 3P. Familiari, 4F. van Delft, 5J. S. Bladen, 4E. Dekker, 3L. Petruziello, 2J. Haringsma, 1S. Thomas-Gibson. 1Wolfson Unit for Endoscopy, Imperial College London, London, UK, 2Department of Gastroenterology and Hepatology, Erasmus Medical Centre, Rotterdam, The Netherlands, 3Digestive Endoscopy Unit, Catholic University-A.Gemelli University Hospital, Rome, Italy, 4Department of Gastroenterology and Hepatology, Academic Medical Center, Amsterdam, The Netherlands, 5JSB Medical Systems, Sheffield, UK
Introduction: Simulators are now recommended for use in endoscopic training. However, first generation colonoscopy simulators have suffered from the lack of accurately modelled colonic looping, and ratings of realism and usefulness diminish with increasing experience. The new second-generation Olympus colonoscopy simulator has been specifically designed to model colonic looping, and initial validation studies reported a high degree of usefulness as judged by experts. A multinational trial utilising the Olympus colonoscopy simulator randomised novices to 16 hours structured simulator training or patient-based training. A “like-with-like” comparison of acceptability was made between simulator training compared to real-life training in colonoscopy.
Aims and Methods: 37 novice trainees from four centres in the UK, Italy and the Netherlands were randomised to two days of simulator training with minimal supervision (N = 19) or hands-on patient training under expert guidance (N = 18). Participants completed an initial questionnaire regarding their expectations of training. Following their training, all participants were assessed on both simulator test cases and patient test cases, and completed feedback regarding the quality of their training.
Results: Initial expectations were high for both groups, with Visual Analogue Scores above 7 out of 10 for all measures. Post training scores were equivalent for quality, usefulness and enjoyment, and both groups felt their training met or exceeded their expectations for quality and usefulness. Both groups felt they were reasonably well prepared for their assessments with scores of 6.0 for simulator trainees and 7.0 for patient trainees respectively (p = 0.40), with similar anxiety levels.
Conclusion: Training using the second generation Olympus colonoscopy simulator was highly acceptable to novice trainees and rates as equivalent to hands-on training with expert instructors. As the simulator requires minimal instructor time and effort and no exposure to patient risk it should be considered as a valuable training tool for skill acquisition in colonoscopy.
0-27 GASTROENTEROLOGY TRAINING IN 2008: RESULTS FROM THE TIG/BSG NATIONAL TRAINING SURVEY
A. V. Haycock, P. Flanagan, A. Ignjatovic, S. Kendrick, R. Mead, P. Mizen, M. Mottershead, V. Patel, K. Pollock, T. Valliani, J. Williams. Trainees Committee, British Society of Gastroenterology, London, UK
Introduction: The 2004 national survey of gastroenterology trainees revealed wide variation in both the quality and quantity of training. Significant changes to postgraduate medical education have taken place since that time in the UK. Modernising Medical Careers and the European Working Time Directive (EWTD) have altered the structure, delivery, and evaluation of training in gastroenterology.
Aims and Methods: The aim of the 2008 survey was to investigate the impact of these changes and gather data on current standards of teaching, training, and supervision. A web-based questionnaire was developed with questions in eight domains: demographics, general gastroenterology, specialist training, general medicine, study leave, assessments, endoscopy and general questions. An invitation to complete the survey was emailed by the regional TiG representatives to all trainees in their region. Data were collected during October 2008.
Results: 249 out of 411 trainees from 20 different training regions completed the survey (response rate 60.6%). 217 (88.6%) were in general gastroenterology posts. 55/234 (23.4%) trainees thought they were unlikely to attain competence in at least one aspect of the basic curriculum, and 40.6% do not think that their training days systematically cover the curriculum. Only 18/217 (8.3%) were rarely or never able to discuss new outpatients with their consultant. Overall, only 21/235 (8.9%) were not very satisfied or very unsatisfied with their general gastroenterology training so far. 50.9% would consider moving permanently to another region to obtain better training in a sub-speciality. 97.9% of trainees are dual training with GIM, but less than half have separate periods of GIM training. Only 51.8% of trainees have a personal development plan (PDP) and 33% meet their educational supervisor every 6 months or less. Over 75% have completed a DOPS, mini-CEX and MSF assessments within the last year, and 134/211 (63.5%) found them easy or manageable to complete. 31.4% say their training has been greatly impaired by the EWTD, and 87.7% believe that their training can be improved.
Conclusion: The majority of trainees are satisfied with their current training, although many have concerns regarding aspects of its provision in their region. Educational supervision and personal development plans are not widely utilised. Specific areas for improvement identified will be fed-back to regional programme directors.
Inflammatory bowel disease free papers
0-28 A NOVEL TEST TO PREDICT EFFECTIVE TREATMENT REGIMENS FOR PATIENTS WITH ANTIBIOTIC RESISTANT POUCHITIS
1S. D. McLaughlin, 2S. K. Clark, 3L. Petrovska, 4P. P. Tekkis, 3P. J. Ciclitira, 4R. Nicholls. 1Gastroenterology, St Mark’s Hospital, London, UK, 2Surgery, St Mark’s Hospital, London, UK, 3Nutritional Sciences, King’s College, London, UK, 4Biosurgery and Surgical Technology, Imperial College, London, UK
Introduction: Empirical antibiotic therapy remains the mainstay of treatment for pouchitis. Combination regimens of ciprofloxacin (C) and metronidazole (M) can be effective for patients resistant to a single antibiotic agent but failure to enter remission and relapse on withdrawal or during maintenance treatment can occur. Faecal coliform antibiotic sensitivity testing was used to select optimal treatment for pouchitis resistant to standard therapy.
Aim: To develop a novel approach to treating patients with resistant pouchitis.
Method: Faecal samples from patients with active pouchitis (pouch disease activity index (PDAI) ⩾7) who failed standard antibiotic treatment were inoculated onto Iso-sensitest agar (Oxoid) using a sterile swab and rotary spreader. Antibiotic discs containing ciprofloxacin, trimethoprim, cefalexin, co-amoxiclav, nitrofurantoin, cefpodoxime, cefuroxime, and cefixime were added. The plates were incubated at 37°C for 24 hours and the sensitivity patterns recorded. Following 4 weeks treatment with an antibiotic selected on its sensitivity, the clinical component of the PDAI was remeasured.
Results: 15 patients with endoscopic and histologically proven chronic pouchitis were studied. 13 had failed to enter remission with CM, two had relapsed on maintenance ciprofloxacin. Antibiotic coliform sensitivity testing showed: ciprofloxacin resistance in all samples; co-amoxiclav resistance in four samples; trimethoprim resistance in 11 samples, cefixime resistance in eight samples. Four samples contained extended spectrum beta lactamase (ESBL) producing organisms. All 15 patients were treated with an antibiotic to which their faecal coliforms were sensitive. Twelve (80%) entered clinical remission with a PDAI symptom score of 0.
Conclusion: Targeted antibiotic therapy is effective in the majority of patients with antibiotic resistant pouchitis. Faecal coliform sensitivity testing and targeted antibiotic therapy should be used in all patients who fail to respond to empirical antibiotic treatment or relapse on long term antibiotic therapy.
0-29 FAECAL LACTOFERRIN – A NON-INVASIVE MARKER FOR THE DETECTION OF GASTROINTESTINAL INFLAMMATION: A COMPARATIVE STUDY OF PATIENTS WITH INFLAMMATORY BOWEL DISEASE, IRRITABLE BOWEL SYNDROME AND HEALTHY CONTROLS
1R. Sidhu, 2P. Wilson, 1C. Yau, 1F. D’Cruz, 2S. Morley, 1M. E. McAlindon, 1A. Wright, 2L. Foye, 1A. J. Lobo, 1D. S. Sanders. 1Gastroenterology, Royal Hallamshire Hospital, Sheffield, UK, 2Clinical Chemistry, Royal Hallamshire Hospital, Sheffield, UK
Introduction: The assessment of inflammatory activity in patients with inflammatory bowel disease (IBD) can be difficult. In addition, there may be an overlap between IBD and conditions such as irritable bowel syndrome (IBS) causing a delay to the diagnosis. Whilst patient reported activity indices can be unreliable, colonoscopy is the accepted gold standard but is invasive. Lactoferrin is a glycoprotein expressed by activated neutrophils which has been demonstrated in patients with IBD, coeliac disease and infective diarrhoea. It has been proposed as a tool to screen for the presence of inflammation; however, there is paucity of data on the use of faecal lactoferrin (FEL) in IBS in comparison to the IBD population.
Aims and Methods: To investigate the clinical utility of FEL as a marker of GI inflammation in patients with IBD, Rome II IBS and healthy controls. Disease activity in IBD patients were assessed using the modified Harvey-Bradshaw Activity Index (HBI). Stool samples were analysed using an ELISA assay (Techlab). A two-tailed t test was used to compare means between groups and Kendall–Tau correlation calculations were performed between lactoferrin concentrations and disease activity.
Results: 137 patients with IBS, 230 patients with IBD: 126 ulcerative colitis (UC) and 104 Crohn’s disease (CD) and 98 healthy volunteers were recruited. The mean±SE FEL concentration (μg/g faecal weight) was 1.39±0.29 for IBS patients, 69.5±14.9 for UC patients, 41.4±13.6 for CD patients, and 2.44±0.72 for healthy controls. FEL levels were significantly higher in IBD patients compared to IBS patients (p = 0.001) and healthy controls (p = 0.001). There was no significant difference in mean FEL concentration between UC and CD patients (p = 0.17) and between IBS and healthy controls (p = 0.18). However, the mean FEL concentrations were significantly higher in active UC patients compared to inactive UC patients (mean FEL: 130±32 vs 28±11, p = 0.003, 95% CI 36 to 169). This comparison was not significant for Crohn’s patients (p = 0.5). The correlation coefficient between disease activity and FEL concentrations was fair, 0.4 for UC patients (p = 0.0001) and 0.2 for CD patients (p = 0.004). The sensitivity, specificity, positive and negative predictive values of FEL in distinguishing active IBD from IBS/healthy controls was 68% and 95.7%, 87% and 86.8%, respectively. In the IBD group, analysis of disease activity based on the HBI >4 revealed a sensitivity and specificity of 77.6% and 70% for UC, and 58% and 80% for CD patients.
Conclusion: FEL is an inexpensive and non-invasive test that can provide the clinician with a marker to differentiate between IBD and IBS and to stratify patients who require endoscopic investigations. FEL can also be used as an adjunct to blood parameters and clinical symptoms to determine IBD patients who have ongoing inflammation.
0-30 ABNORMAL TLR4-MEDIATED INTERFERON RESPONSE IN ULCERATIVE COLITIS
1F. Z. Rahman, 1A. M. Smith, 1B. Hayee, 1G. Sewell, 1D. J. Marks, 2S. L. Bloom, 1A. W. Segal. 1Medicine, University College London, UK, 2Medicine, UCL Hospitals Foundation NHS Trust, London, UK
Introduction: Although the aetiology of ulcerative colitis (UC) remains an enigma, strong evidence implicates an exuberant response to microbial components in the pathogenesis. Recent studies provide evidence of a protracted acute inflammatory response to heat-killed E. coli (HkEc) in UC.1 The underlying pathogenic mechanisms remain unclear.
Aims and Methods: The acute inflammatory response to microbial stimulation was compared in UC and age/sex-matched healthy control (HC) subjects. UC patients were on either no medication or a 5-ASA alone (<2.4 g/day). Serum cytokine levels at baseline and 24, 48 and 72 hours following subcutaneous injection of 3×107 HkEc were quantified (13 UC, 6 HC). We then characterised the response of primary monocyte-derived macrophages to microbial stimulation (HkEc, LPS (TLR4), Pam3-CSK4 (TLR2) and Flagellin (TLR5)) by analysing TLR pathway-associated gene expression (8 UC, 8 HC) and cytokine secretion (15 UC, 9 HC).
Results: Serum IP-10 levels were significantly elevated at 48 (2.5-fold, p<0.01) and 72 (8.6-fold, p<0.05) hours after HkEc injection in UC, the time points when blood flow was raised in these patients.1 Analysis of TLR pathway-associated gene expression following HkEc stimulation showed that macrophages from patients with UC significantly over-express the interferon (IFN) family-related genes; IFN-\alpha, IFN-\beta (both 6-fold, p<0.02), CD80 (8-fold, p<0.01) and CD86 (4.5-fold, p<0.05) (T cell co-stimulatory molecules). After stimulation with HkEc (p<0.01) and LPS (p<0.001), but not Pam3-CSK4 and Flagellin, macrophage IP-10 secretion was significantly elevated in UC.
Conclusion: Increasing evidence highlights the importance of IP-10, a potent T cell chemoattractant, in the pathogenesis of UC. Raised levels have been reported locally2 and systemically3 in patients with active disease and its inhibition has been shown to ameliorate inflammation in mouse models of colitis.4 Here we demonstrate that abnormally elevated IP-10 levels in UC occur in response to bacterial stimulation. The underlying defect appears to lie at the level of the macrophage, and specifically relates to dysregulated TLR4 signalling. Over-expression of IFN family-related and T cell co-stimulatory genes during the acute inflammatory response may eventuate in the T cell-mediated chronic inflammation characteristic of UC. Work to define the precise molecular defects underlying dysregulated TLR4 signalling in UC is ongoing and may offer novel therapeutic targets in the future.
0-31 THE REGULATION OF COLONIC HUMAN BETA-DEFENSIN 2 (HBD2) PRODUCTION IN INFLAMMATORY BOWEL DISEASE
M. C. Aldhous, K. Soo, C. L. Noble, J. Satsangi. Gastrointestinal Unit, University of Edinburgh, Edinburgh, UK
Introduction: The beta-defensins are antimicrobial peptides expressed in the gastrointestinal tract. Low copy number and concomitant low mRNA expression of the human beta-defensin-2 (HBD2) gene have been implicated in susceptibility to colonic CD.1 In analysis of microarray expression data2 we found HBD2 mRNA to be differentially expressed in inflamed biopsies from Crohn’s disease (CD) and ulcerative colitis (UC): in CD mRNA was highest in proximal colon, whereas in UC expression was highest in sigmoid colon. This study aimed to extend these findings by further investigating the effects of environmental and genetic factors on HBD2 protein production using ex vivo organ culture.
Aims and Methods: Biopsies were obtained from the sigmoid colon of CD (n = 22), UC (n = 26) and control (n = 21) patients undergoing endoscopy. Biopsies were stimulated in ex vivo organ culture3 with bacterial lipopolysaccharide (LPS) and/or nicotine for 24 hours. HBD2 and IL8 production were measured in culture supernatants by ELISA. HBD2 copy number variation analysis was carried out by qPCR on paired DNA samples. Sequences similar to NF-kappaB consensus binding sequences were identified by TESS4 in the HBD2 gene promoter region and were sequenced.
Results: HBD2 production was increased in inflamed sigmoid colon biopsies from UC compared with CD or HC (2-way ANOVA: inflammation p = 0.0078). In UC patients, HBD2 protein levels significantly increased with degree of inflammation defined by histology, and also correlated with IL8 production (p<0.001) – this relationship was not seen in CD patients. HBD2 protein production was induced by LPS (p = 0.0246) and LPS + nicotine (p = 0.0463) in IBD but not controls. Induction by LPS was stronger in CD (p = 0.0375) than in UC (p = 0.2017). Induction of HBD2 protein was augmented by nicotine in UC (p = 0.0308) but not CD. Nicotine alone had no effect on HBD2 production. HBD2 production did not correlate with HBD2 gene copy number. Variations in the promoter sequences were found, but no polymorphism changed the site to the NF-kappaB binding consensus sequence, nor affected HBD2 production.
Conclusion: In colonic inflammatory bowel disease (IBD), HBD2 is induced by bacterial LPS – this response is differentially modified by nicotine in CD and UC. In UC, HBD2 production is increased by acute inflammation. HBD2 CNV does not influence protein production. These results provide insights into the environmental and genetic determinants of dysregulated innate immunity in IBD.
0-32 ARACHIDONIC ACID INCREASES THE RISK OF ULCERATIVE COLITIS – A PROSPECTIVE COHORT STUDY IN EPIC-DENMARK USING BIOMARKER DATA
1P. S. A. de Silva, 2A. Olsen, 2A. Tjonneland, 3K. Overvad, 4E. Berg Schmidt, 5A. R. Hart. 1Department of Gastroenterology, Norfolk and Norwich University Hospital, Norwich, UK, 2Institute of Cancer Epidemiology, Danish Cancer Society, Copenhagen, Denmark, 3Departments of Cardiology and Clinical Epidemiology, Aarhus University Hospital, Denmark, 4Department of Cardiology, Aalborg Hospital, Aalborg, Denmark, 5School of Medicine, University of East Anglia, Norwich, UK
Introduction: Arachidonic acid (AA), an n-6 polyunsaturated fatty acid (n-6 PUFA), is a component of the phospholipid bilayer of colonocyte membranes and can be metabolised to the pro-inflammatory eicosanoids PGE2 and LTB4. The latter are found in increased concentrations in the mucosa of patients with ulcerative colitis (UC).
Aims and Methods: The aim of this study was to measure, for the first time, in a prospective cohort investigation, if an increased AA concentration in adipose tissue biopsies, which reflect dietary intake, increases the risk of developing incident ulcerative colitis. A total of 57 053 men and women, aged 50-64 years, were recruited in the EPIC-Denmark Study (European Prospective Investigation In to Cancer) between 1993–97. Adipose tissue biopsies were taken from the gluteal region of participants at recruitment and AA fatty acid constituents measured. The cohort was monitored to up to June 2004 to identify individuals who developed UC. Each case was matched with 4 controls for age and gender, and levels of AA divided into quartiles. Unconditional logistic regression was used to calculate univariate odds ratios for the level of AA and an additional multivariate analysis performed adjusted for cigarette smoking and marine n-3 PUFAs in adipose tissue.
Results: During the follow-up, 34 subjects (15 women, 19 men) developed incident UC with the diagnoses confirmed by physicians. The median age at diagnosis was 58.8 years (range 53.3–71.1 years) with a median time between recruitment and diagnosis of 3.7 years (1.7–7.1 years). The highest adipose concentration of AA was associated with an odds ratio for UC of 12.3 (95% CI 2.6 to 57.8, p = 0.002) with a statistically significant trend across quartiles (OR for trend = 1.9, 95% CI 1.3 to 2.8, p = 0.001) in the univariate analysis. Adjustment for co-variates did not affect the magnitude of the findings.
Conclusion: Initially, well participants, who have higher adipose tissue concentrations of AA, which represent dietary intake, have a significantly higher risk of developing ulcerative colitis compared with those with lower levels. These findings support previous data from dietary questionnaire-based epidemiological studies showing n-6 PUFAs may be involved in the aetiology of this condition. Lowering the dietary intake of AA may prevent the development of UC.
0-33 METRONIDAZOLE 10% OINTMENT IMPROVES SYMPTOMS IN PERIANAL CROHN’S DISEASE WITH LOW SYSTEMIC EXPOSURE
1Y. Maeda, 2S. C. Ng, 3P. Durdey, 3C. Burt, 4J. Torkington, 4P. Dhruva-Rao, 5J. Mayberry, 5T. Moshkovska, 6C. Stone, 2C. J. Vaizey. 1Physiology Unit, St Marks Hospital, Harrow, UK, 2Physiology Unit, St Mark’s Hospital, Harrow, UK, 3Department of Surgery, Bristol Royal Infirmary, Bristol, UK, 4Department of Surgery, Llandough Hospital, Penarth, UK, 5Department of Gastroenterology, Leicester General Hospital, Leicester, UK, 6Department of Gastroenterology, Washington University in St Louis, Missouri, USA
Introduction: Pain and discharge cause significant morbidity in perianal Crohn’s disease. In a prospective, controlled study, we demonstrate here the potential for metronidazole (MET) 10% ointment to exert therapeutic benefit in perianal Crohn’s disease (CD) whilst minimising adverse effects seen with oral MET. Systemic exposure to MET was examined in a separate study.
Aims and Methods: Patients with perianal CD were prospectively randomised to MET 10% ointment (S.L.A. Pharma, Watford, UK) or placebo ointment (0.7 g applied perianally tds for 4 weeks). Perianal Crohn’s Disease Activity Index (PCDAI; 0–20; entry score ⩾5) was scored at baseline and at 4 weeks. Each PCDAI component (discharge; induration; pain; type of disease; restriction of sexual activity) was analysed individually. Perianal pain was assessed on a 10 cm VAS line. Patient Global Impression of Improvement (PGI-I) was scored on a 7-point Likert scale. Data were analysed by ANCOVA, Fisher’s exact or Wilcoxon tests as appropriate. In a separate study, blood samples taken from 12 healthy volunteers (HV) and 7 patients with perianal CD before a single application of MET 10% ointment and over 24 h after were analysed for metronidazole and hydroxymetronidazole. A single sample was taken on Day 7 after tds dosing for 6 days.
Results: 61 patients (27 MET; 34 placebo) with perianal CD were evaluated. At week 4, mean (±SEM) reduction in PCDAI was 3.2±0.5 (metronidazole) vs 2.1±0.5 (placebo) (p = 0.093). The discharge component of the PCDAI improved significantly in the MET group compared to the placebo group (p = 0.012). The VAS score for perianal pain fell 16.7 mm (MET) vs 5.7 mm (placebo; p = 0.059). There was a significant difference in favour of MET for the PGI-I (p = 0.015). No serious adverse events were reported with MET 10% ointment. Maximum plasma levels of MET and hydroxymetronidazole were somewhat higher and more variable in the CD subjects compared to HVs after a single application of ointment (CD 52.3±88.0 vs HV 12.4±6.2 ng/mL) and after repeat dosing (CD 46.2±26.1 vs HV 29.1±28.1 ng/mL). This compares with values of 13 ng/mL for single oral doses of 500 mg MET.
Conclusion: MET 10% ointment reduced perianal discharge and pain and was associated with better impressions of global improvement in subjects with perianal CD. MET 10% ointment was well tolerated, with minimal adverse effects, in keeping with observed blood levels <1% of those seen with standard oral doses, and has potential as adjunctive therapy for perianal CD.
0-34 CIGARETTE SMOKE DOWN REGULATES NOD2 EXPRESSION AND NF-KAPPAB ACTIVATION IN SW480 CELLS
1M. C. Aldhous, 1K. Soo, 1A. Ulanicka, 1J. E. Pearce, 2L. A. Stark, 2M. G. Dunlop, 1J. Satsangi. 1Gastrointestinal Unit, University of Edinburgh, Edinburgh, UK, 2Colon Cancer Genetics Group, University of Edinburgh, Edinburgh, UK
Introduction: The mechanisms whereby smoking influences susceptibility and phenotype in CD are unknown. Germline variations in the NOD2 gene predispose to fistulising/stenosing small bowel CD, the same phenotype associated with smoking. NOD2 signalling involves critical interactions with RIPK2 leading to activation of NF-kappaB, and associated effects on chemokine, cytokine and defensin production. We investigated whether cigarette smoke extract (CSE) or chemicals within cigarette smoke altered NOD2 expression and downstream effects in the SW480 intestinal epithelial cell line, which express wild-type NOD2.
Aims and Methods: CSE was made by bubbling cigarette smoke through PBS. SW480 cells were stimulated with TNF-alpha with and without 2% CSE for 4 hours. NOD2 mRNA expression was measured by qRT-PCR. To determine effects of specific components of cigarette smoke, cells were also stimulated with combinations of TNF-alpha and nicotine, acrolein, hydroxy-nonenal (HNE) or hydrogen peroxide (HP). In separate experiments, NF-kappaB activity was measured at 18 hours by luciferase reporter assays. Co-immunoprecipitation assays were used to determine the interaction between NOD2 and RIPK2 in cells stimulated with combinations of CSE, nicotine and TNF-alpha. CXCL8/IL8 and CCL20/MIP3-alpha were measured in culture supernatants of cells stimulated with combinations of CSE, nicotine and TNF-alpha after 24 hours by ELISA.
Results: TNF-alpha induced NOD2 expression, which was inhibited by CSE in a dose-dependent manner, when CSE was titrated out from 2 to 0.0625%. TNF-alpha-induced NOD2 expression was reduced by acrolein, HNE and HP but not affected by nicotine. NF-kappaB activity was significantly reduced by CSE (p<0.001) but not by nicotine, acrolein, HNE or HP. Basal and TNF-alpha-induced levels of CXCL8/IL8 and CCL20/MIP3-alpha were decreased by CSE but not nicotine. Preliminary co-immunoprecipitation experiments suggest that TNF-alpha increased RIPK2/NOD2 interactions and that these were reduced by CSE.
Conclusion: CSE down-regulated the increased NOD2 expression in response to TNF-alpha, as well as inducing effects on down-stream signalling consistent with reduced NOD2 function. These data suggest that smoking may reduce innate immune responses in intestinal cells, thereby identifying a novel gene-environmental interaction which may be critical in the pathogenesis of inflammatory bowel disease.
0-35 BACTERIAL CLEARANCE IS DELAYED IN PATIENTS WITH CROHN’S DISEASE
1B. Hayee, 1F. Z. Rahman, 1A. M. Smith, 1D. J. B. Marks, 1G. W. Sewell, 2T. J. Sweeting, 3S. L. Bloom, 1A. W. Segal. 1Molecular Medicine, University College London, UK, 2Statistical Science, University College London, UK, 3Gastroenterology, UCLH NHS Foundation Trust, London, UK
Introduction: Recent work provides evidence for a failure of acute inflammation in Crohn’s disease (CD), supporting the hypothesis that a defective innate immune response is a primary defect.1 The abnormalities observed suggested that bacteria or debris breaching the intestinal mucosal barrier would not be adequately cleared. Bacterial persistence would then provide the stimulus for chronic granulomatous inflammation.2
Aims and Methods: This study was conducted to determine whether bacterial clearance is abnormal in CD. Ethical permission was obtained from the Joint UCL/UCLH Committees on the Ethics of Human Research and the Administration of Radioactive Substances Advisory Committee (ARSAC). An antibiotic-sensitive clinical isolate of E. coli was labelled in culture with 32P then killed by UV-irradiation. Labelled bacteria (1 kBq activity) were mixed with identical, unlabelled UV-irradiated E. coli (3×107 bacteria per inoculum). The mixture was injected subcutaneously into both forearms of study subjects, and its clearance determined by measuring radioactivity at the injection sites over the subsequent 72 hours. Clearance kinetics were modelled using a nested mixed effects model with non-linear dynamics.
Results: 14 healthy controls (HC), 16 patients with quiescent CD and 3 patients with ulcerative colitis (UC) were studied. All subjects displayed two-phase clearance kinetics with an initial rapid phase. Clearance was significantly delayed in CD compared to HC (p<10−5) with a trend toward more rapid clearance in UC (p = 0.08). Extrapolating clearance curves to a point when 99% of injected bacteria should have been removed gave total clearance times of 10.2 days (95% CI: 8.3 to 13.0) for HC, 7.1 days (5.4 to 10.4) for UC, and 44.3 days (21.8 to inf.) in CD.
Conclusion: This is the first study to use radiolabelled bacteria in human subjects to examine their clearance kinetics. It clearly demonstrates a gross defect in bacterial clearance in CD, and that these organisms persist for an unusually long duration in their tissues. These are precisely the conditions known to elicit granulomatous chronic inflammation,3 and therefore likely to be of primary relevance to the pathogenesis of CD.
BHH and FZR contributed equally to this work.
0-36 METHOTREXATE FOR PAEDIATRIC INFLAMMATORY BOWEL DISEASE IN THE BIOLOGICAL ERA
1A. Tybulewicz, 1P. Rogers, 2D. Hoole, 3J. Satsangi, 1P. M. Gillett, 4D. C. Wilson. 1Paediatric Gastroenterology, Royal Hospital for Sick Children, Edinburgh, UK, 2Pharmacy, Royal Hospital for Sick Children, Edinburgh, UK, 3GI Unit, University of Edinburgh, Edinburgh, UK, 4Child Life and Health, University of Edinburgh, Edinburgh, UK
Introduction: There are limited data on the use of methotrexate (MTX) for induction and maintenance of remission in children with Crohn’s disease (CD), and many proceed to biological therapy if azathioprine (AZA) fails. We therefore aimed to review our patients treated with MTX, in terms of both induction and maintenance of remission.
Aims and Methods: A cohort study of all 244 patients diagnosed with early-onset (<18 years of age) IBD and managed in a UK regional centre over a 10 year period (1/8/97–31/12/07). Within this cohort were 165 patients with CD; we studied those resistant to or intolerant of AZA/6-MP who were treated with MTX (16 week induction course of s/c MTX (15 mg/m2) followed by the equivalent oral dose). Paediatric Crohn’s Disease Activity Index (PCDAI) was used to objectively measure disease activity during treatment; PCDAI ⩽10 indicated full remission, ⩽15 indicated partial remission and a score >30 indicated severe disease.
Results: 122 with CD were treated with AZA/6-MP; 53 children (52 with previous ADA, 1 who refused ADA) received a MTX induction course. These 53 patients had CD diagnosed at a median (range) age of 10.9 years (4.0–16.5) and received MTX at 14.0 years (6.8–17.9). The median PCDAI at start of treatment was 35 (IQR 20–37.5). 41 (78%) patients entered remission; median (range) time to partial/complete remission was 11 (3–16) weeks. 2 of 41 had recalcitrant OFG and were excluded from maintenance evaluation; the remaining 39 had luminal CD and a median (range) duration of follow-up of 85 (26–310) weeks. 20 (51%) maintained long-term remission with no relapse; 7 (18%) had only a single relapse of which 6 (15%) re-entered remission, and 12 (31%) had >1 relapses. The median (range) time to first relapse was 39 (20–181) weeks. Of the 19 relapsing, 14 proceeded to repeat s/c courses of MTX, 9 to infliximab, 6 to surgery and 4 to adalimumab. On MTX treatment, 24 (46%) had nausea/vomiting, 18 (34%) had raised ALT (1 subsequently undergoing liver biopsy, with treatment then continued), 1 had shingles and none had bone marrow toxicity.
Conclusion: MTX appears to be effective in inducing (78%) and maintaining (51%) remission in patients who have failed to remit on AZA, even if biological therapy is available. MTX also appears to be well tolerated and safe. Those who have had multiple relapses have all had complicated clinical courses and severe intractable disease. However, a stronger evidence base is needed from well-designed RCTs for both induction and maintenance of remission of early-onset CD by MTX.
0-37 WHICH ACTIVITY INDEX FOR ULCERATIVE COLITIS? EVALUATION OF INTER-OBSERVER VARIATION IN CLINICAL, ENDOSCOPIC AND COMPOSITE INDICES
1A. J. Walsh, 1A. O. S. Brain, 1S. Keshav, 1O. C. Buchel, 1S. Jacobovits, 1B. Merrin, 1M. Rolinski, 1S. Thomas, 1L. White, 2A. Von Herbay, 2B. F. Warren, 3D. G. Altman, 1S. P. L. Travis. 1Gastroenterology, The John Radcliffe Hospital, Oxford, UK, 2Cellular Pathology, The John Radcliffe Hospital, Oxford, UK, 3Biomedical Statistics, University of Oxford, Oxford, UK
Introduction: Clinical trials of ulcerative colitis (UC) use many different activity indices, making it difficult to compare data between trials. It is unclear which index is most reproducible and how inter-observer variation (IOV) impacts on trial inclusion and outcomes.
Aims and Methods: Our aims were to assess IOV in all commonly used indices and to determine the impact of this variability on inclusion criteria and outcomes in key published trials. 100 patients with UC were seen independently, each patient on the same day, in random order, by 4 gastroenterologists. Each physician completed a pro forma to calculate the following indices: Mayo Index (MAYO), UC Disease Activity Index (UCDAI), Simple Colitis Clinical Activity Index (SCCAI), Seo Index (SEO), Modified Truelove and Witts Severity Index (MTW), and Colitis Activity Index (CAI). A separate physician performed video-recorded sigmoidoscopy on the same day. The video record was later scored by the 4 assessing physicians, blinded to other results. To assess the impact of IOV in recruiting patients to, or meeting outcome criteria of clinical trials, pivotal papers were selected for each index. Quadratic weighted kappa statistics assessed agreement within and between indices, in which disagreements are weighted in relation to their magnitude (number of categories).
Results: Of 100 patients, 50% were male, median age 49 years (range 19–82), and median duration of disease 107 months (range 0–575). Maximum disease extent: proctitis 27%, left-sided colitis 39% and pancolitis 34%. 23% were in remission, 40% had mild, 32% moderate and 5% severe colitis. The mean inter-rater kappa for MAYO, UCDAI and SCCAI were 0.88, 0.90 and 0.88, respectively; the SEO (kappa = 0.95) scored highest and CAI lowest (kappa = 0.78) but this does not imply best or worst indices, as utility depends on several factors. The kappa for agreement of activity category between MAYO and UCDAI, and MAYO and SCCAI were 0.92 and 0.80, respectively. For endoscopic indices, kappa for agreement between Baron and Mayo, and Baron and modified Baron indices were 0.83 and 0.89, respectively. For trial inclusion, the median mismatch was 23% (complete concordance in 65–97%), with most agreement for severe UC by MTWSI and least for mild-moderate UC by UCDAI. For MAYO, there was disagreement by > = 1 observer estimating current stool frequency in 53% which changed the score by 1 in 22% and by 2 in 2%. Median mismatch for remission was 21% (complete concordance in 77–91%) with most agreement for SCCAI.
Conclusion: IOV in the assessment of UC is substantial and should be taken into account when calculating the power of clinical trials. With 4 independent specialists assessing the same patients in the context of this study, about 1 in 5 patients would have been affected by disagreement whether they met entry criteria or achieved remission for already published clinical trials.
Liver free papers
0-38 ALCOHOLIC LIVER DISEASE – THE SOUTH INDIAN DIMENSION
1C. Chong, 1E. Harazi, 1T. M. Tian, 2T. Darch, 2J. Wells, 1M. Y. Morgan. 1Centre for Hepatology, Department of Medicine, Royal Free Campus, University College London Medical School, London, UK, 2Institute of Child Heath, University College London Medical School, London, UK
Introduction: Alcohol produces a spectrum of liver injury but less than 20% of individuals who misuse alcohol will develop cirrhosis. Recently, it was reported that South Indian (non-Moslem) men are significantly over-represented in the cirrhotic population in Birmingham, UK (Douds et al, 2003); additionally 37% of the Asian men presented aged <40 years compared with only 17% of white men. Women develop cirrhosis at an earlier age and after ingestion of less alcohol than men because their total body water (TBW) is smaller. No information is available on alcohol pharmacokinetics and body composition in the Asian population.
Aims and Methods: The aim was to assess alcohol kinetics in healthy white and Asian volunteers in relation to body composition variables. Twenty-four Asian and 24 white volunteers (50% female; age: 20–34 years; BMI:17–28) drank 0.5 g/kg of 99% ethanol, as a 25% v/v solution in orange juice, 2 hours after a standard breakfast. Breath alcohol was measured every 5 min for 6 hours. Body composition was assessed using a 3-component model from direct measurements of body density (densitometry), TBW (deuterium dilution) and body weight. Pharmacokinetic parameters were calculated using a modified one compartment model with zero-order kinetics (Mumenthaler et al, 2000). Correlations between body composition and pharmacokinetic variables were assessed using Pearson’s r.
Results: The one compartment model did not describe the pharmacokinetics of alcohol as well in the Asians. No significant differences were observed in Cmax, AUC and elimination rates between the Asian and white populations, although significant differences were observed in both Tmax and the apparent volume of distribution (aVd). TBW was significantly higher in men than women and in Asians compared with whites. The calculated aVd showed a highly significant correlation with TBW in the whites (r = 0.96; p<0.0001), but not in the Asians (r = 0.30; p = 0.48). Differences in fat mass and fat free mass were observed between the two population groups but were insufficient to explain this discrepancy.
Conclusion: Significant differences were observed in alcohol pharmacokinetics in the Asian population which might explain their increased propensity to develop significant liver disease. These differences could only be explained, in part, by differences in body composition. No significant differences were observed in alcohol elimination rates suggesting that differences must, therefore, exist in the absorption, distribution or non-hepatic elimination of alcohol between these two populations. There is a clear need to establish a robust model for alcohol pharmacokinetics in the Asian population.
0-39 COMPARISON OF TRANSIENT ELASTOGRAPHY, APRI SCORE, AST/ALT RATIO, HYALURONIC ACID AND CLINICAL SIGNS FOR THE DIAGNOSIS OF COMPENSATED CIRRHOSIS
1R. Malik, 2M. Lai, 2I. Nasser, 2M. Curry, 2D. Schuppan, 2N. Afdhal. 1Hepatology, The Institute of Hepatology, UCL, London, UK, 2Medicine, Beth Israel Deaconess Medical Center/Harvard Medical School, Boston, USA
Introduction: Non-invasive diagnosis of compensated cirrhosis is important as liver biopsy has limitations.
Aims and Methods: We compared transient elastography, APRI score, AST/ALT ratio, hyaluronic acid (HA) and clinical signs to determine which modality performed best at identifying cirrhosis. Patients undergoing evaluation at a single academic centre in Boston, USA were recruited and had clinical evaluation, serological studies, endoscopy, radiological imaging, liver stiffness measurement and liver biopsy.
Results: 404 patients were stratified into two groups depending on whether cirrhosis was present. There were 124 patients in the cirrhotic group out of whom 54 were biopsy proven (Metavir stage 4) and 70 had a clinical diagnosis (radiology+endoscopy). There were 280 patients in the non-cirrhotic group all of whom had a liver biopsy (Metavir stage 0–3). The mean transient elastography measurement in the cirrhotic group (29.1±3 kPa) was significantly higher than the non-cirrhotic group (8.1±2.9 kPa, p<0.05). Transient elastography (AUC 0.9±0.04) was superior to HA (AUC 0.81±0.04, p<0.05), clinical signs (AUC 0.74±0.04, p<0.05), APRI score (AUC 0.71±0.03, p<0.05), and AST/ALT ratio (AUC 0.66±0.03, p<0.05) at identifying cirrhosis. In addition, using optimal cut offs for each modality, TE >12 kPa yielded a sensitivity and specificity of 89% and 87% respectively, which was significantly higher that HA >150 ng/ml (72%; 79%), positive clinical signs (69%; 81%), APRI >1 (73%; 54%), and AST/ALT >1 (64%; 59%) (p<0.05 for all). We performed further analysis to compare biopsy proven cirrhosis (stage 4) with the control group (all biopsy proven stage 0–3) to determine the performance at identifying histologically proven cirrhosis. Transient elastography yielded an AUC 0.88±0.03, which was significantly higher than the other four tests (p<0.05 for all). A high degree of diagnostic accuracy was seen for transient elastography on sub-group analysis in hepatitis C (AUC 0.899±0.02) and non-hepatitis C (AUC 0.928±0.03) groups, with elastography diagnostically superior to the other four tests (p<0.05 for all). We identified 38 Childs Pugh A patients with biopsy proven cirrhosis in whom a definitive diagnosis of cirrhosis was uncertain prior to liver biopsy. Transient elastography performed the best in this important cohort, yielding an AUC 0.87±0.04 compared to HA (AUC 0.77±0.05, p<0.05), APRI Score (AUC 0.64±0.03, p<0.05) and AST/ALT ratio (AUC 0.63±0.03, p<0.05).
Conclusion: Transient elastography accurately identified compensated cirrhosis using a liver stiffness cut off of 12 kPa. It performed better than hyaluronic acid, APRI, AST/ALT ratio and clinical signs as a non-invasive modality.
0-40 CRITICAL FLICKER FUSION FOR THE DIAGNOSIS OF HEPATIC ENCEPHALOPATHY
1H. R. Wilson, 2C. D. Jackson, 3R. W. Morris, 2B. D. Youl, 1M. Y. Morgan. 1Centre for Hepatology, Royal Free Campus, UCL Medical School, London, UK, 2Department of Neurophysiology, Royal Free Hospital, London, UK, 3Department of Primary Care and Population Studies, Royal Free Campus, UCL Medical School, London, UK
Introduction: The development of hepatic encephalopathy (HE) has a significant negative effect on survival in patients with cirrhosis. Nevertheless, there is still no “gold standard” for its diagnosis. Thus, unless floridly manifest, its presence is often missed, and, in consequence, patients are often suboptimally managed.
Aims and Methods: The aim of this study was to evaluate critical flicker fusion thresholds for the diagnosis of HE in patients with cirrhosis. The patient population comprised 76 individuals (48 men, 28 women) of mean (range) age 57 (32 to 81) years, with biopsy proven alcohol-related (n = 57) or non-alcohol related (n = 19) cirrhosis. Patients were classified using clinical, electroencephalographic and psychometric variables, as either neuropsychiatrically unimpaired (n = 43) or as having minimal (n = 19) or overt HE (n = 14). The reference population comprised 40 healthy volunteers (17 men, 23 women) of mean age 39.8 (21 to 70) years. Critical flicker fusion was assessed using a Lafayette model 12021. The threshold frequencies at which light pulses were perceived as fused (fusion frequency) or flickering (flicker frequency) were assessed and the mean calculated to provide the critical flicker fusion frequency (CFF).
Results: Fusion, flicker and CFF values were corrected for age and gender effects. The fusion frequency and CFF were significantly lower in the patients overall, and significantly distinguished the population subgroups, e.g. fusion frequency at 1 Hz/sec: controls (36.6 Hz) vs unimpaired patients (34.1 Hz) vs minimal HE (30.3 Hz) vs overt HE (25.9 Hz) (p<0.0001). A threshold of 33.4 Hz for fusion frequency, recorded at 1 Hz/sec, diagnosed HE with a sensitivity of 79% and a specificity of 63%. Separate thresholds were identified in patients with alcohol-related cirrhosis: 32.0 Hz (sensitivity 75%, specificity 78%) and non-alcohol related cirrhosis: 34.9 Hz (sensitivity 85%, specificity 83%). All fusion and CFF indices correlated significantly with the classification variables and the Pugh’s score. CFF values accurately mirrored changes in clinical status.
Conclusion: CFF is a simple, reliable measure which could be useful in the screening and monitoring of HE in patients with cirrhosis.
0-41 LONGITUDINAL ANALYSIS OF HEPATITIS C VIRUS SPECIFIC T CELL RESPONSES IN EXPOSED UNINFECTED INTRAVENOUS DRUG USERS
1P. Thurairajah, 1U. Warshow, 1A. Demaine, 2E. Kaminski, 1D. Hegazy, 3M. E. Cramp. 1Institute of Biomedical Sciences, Peninsula Medical School, Plymouth, UK, 2Department of Immunology, Derriford Hospital, Plymouth, UK, 3Department of Hepatology, Derriford Hospital, Plymouth, UK
Introduction: Hepatitis C virus (HCV) specific T lymphocyte responses of low magnitude have been demonstrated amongst high risk injection drug users (IDU) who test negative for HCV infection, suggesting viral exposure without infection.1 We have termed these cases as “Exposed Uninfected” (EU). We report a longitudinal study of HCV-specific T cell responses in EU cases and correlate this with likely ongoing HCV exposure through drug injecting patterns.
Aims and Methods: 21 high risk EU cases have been studied on 3 or more occasions. All tested negative for HCV antibodies and HCV RNA. Details of injecting behaviour were ascertained by structured questionnaire and cases were subdivided into 3 groups according to drug injecting patterns. Group 1: EU cases who stopped injecting during follow-up, Group 2: EU cases in prisons, Group 3: EU cases who continued to inject in the community. Lymphocytes were isolated from fresh blood and an enzyme linked immunospot assay (ELIPSOT) was used to measure interferon gamma (IFN-g) production in response to a panel of HCV proteins (Core, NS3-NS5). 7 healthy controls were studied at similar intervals.
Results: Only 2 control cases exhibited any ELISPOT response to HCV antigens, which were not reproducible on subsequent testing. In contrast, EU’s demonstrated more frequent, stronger and multispecific ELISPOT responses. On follow up, ELISPOT responses were frequently maintained in group 3, with all but two cases maintaining HCV specific responses over time. In contrast, most of groups 1 and 2 lost their HCV specific responses during follow up. Pooled IFN-g responses to all HCV antigens were significantly stronger in group 3 (continued IDU, p = 0.005) and in group 2 (prisoners, p = 0.035) than group 1 (stopped injecting).
Conclusion: Injection drug users can show HCV-specific T cell responses to a variety of HCV antigens in the absence of any evidence of HCV infection. Maintenance of these weak T cell responses over a period of several months appears to be dependent on continuing injection drug use and, presumably, ongoing HCV exposure. In those entering rehabilitation and stopping injecting, HCV-specific responses mostly waned rapidly. Whether these T cell responses merely indicate priming of the immune system by a sub-infectious inoculum of HCV or a response that is able to prevent infection becoming established remains to be clarified. Further study of the development of these responses early in the course of injection drug use would be of interest.
0-42 PLASMA PROTEOMIC PROFILING OF PATIENTS WITH CHOLANGIOCARCINOMA
1P. Nassim, 2R. J. Edwards, 3H. Wasan, 4I. Cox, 5M. B. Toledano, 1S. D. Taylor-Robinson, 1S. A. Khan. 1Hepatology and Gastroenterology, Imperial College London, London, UK, 2Experimental Medicine & Toxicology, Imperial College London, London, UK, 3Cancer Medicine, Imperial College London, London, UK, 4Imaging Sciences, Imperial College London, London, UK, 5Epidemiology & Public Health, Imperial College London, London, UK
Introduction: Cholangiocarcinoma (CC) incidence and mortality rates are steadily increasing. Overall prognosis is poor and there are currently no diagnostic biomarkers with good sensitivity and specificity. Proteomic profiling of plasma is a promising technique for new biomarker discovery to improve the early diagnosis of CC.
Aims and Methods: The aim of this study was to use surface enhanced laser desorption/ionisation time-of-flight mass spectroscopy (SELDI-TOF MS) Protein-Chips to compare the proteomic profiles in plasma of patients to identify any potential biomarkers that can differentiate malignant CC from benign biliary disease. Plasma samples from 19 patients were collected for analysis. Ten patients had a confirmed diagnosis of CC and the remaining nine were undergoing endoscopic retrograde cholangiopancreatography for benign biliary disease (choledocholelithiasis). All samples were analysed using hydrophobic (H50) and carboxymethyl (CM10) Protein-Chips via SELDI-TOF MS and biomarker models were developed.
Results: Univariate analysis of the SELDI-TOF MS spectra revealed 10 and 13 peaks that varied significantly between the CC and benign disease subjects on H50 and CM10 Protein-Chips, respectively (p<0.05, in each case, Mann-Whitney U test). One, with mass-to-charge (m/z) of 8403 had a sensitivity of 89% and specificity of 90% (p = 0.001, receiver operating characteristics (ROC) area under the curve (AUC) = 0.92). Several biomarker models were developed using multiple regression. This included one using two potential biomarkers with m/z 2701 and 3311 peaks that distinguished CC from non-malignant samples with 100% sensitivity and specificity (p = 0.0002, ROC AUC = 1.0). Several other models that performed similarly were also produced.
Conclusion: This preliminary study identified several potential plasma biomarkers of CC. The results highlight the potential role of proteomic profiling in biomarker discovery that may lead to new diagnostic tests to distinguish CC from non-malignant disease. Further studies in larger numbers of patients and other HBP cancers are warranted.
0-43 ROLE OF ENDOSCOPIC ULTRASOUND IN THE MANAGEMENT OF LIVER DISEASE PATIENTS WITH ECTOPIC OR GASTRIC VARICES
1J. N. Plevris, 2S. Inglis, 1A. M. Lennon, 1N. McAvoy, 1P. C. Hayes. 1Centre for Liver and Digestive Disorders, The Royal Infirmary, University of Edinburgh, Edinburgh, UK, 2Department of Medical Physics, The Royal Infirmary, University of Edinburgh, Edinburgh, UK
Introduction: The availability of new endoscopic ultrasound (EUS) scopes with Doppler ultrasound facilities has made it possible to assess the severity of portal hypertension and to control variceal bleeding under EUS guidance. In addition the varied endoscopic appearances of ectopic varices in the stomach or small bowel often present a diagnostic challenge as biopsy of these lesions can put patients at risk of severe bleeding.
Aims and Methods: To report our experience in the use of EUS to assist the management of patients with chronic liver disease and portal hypertension. 15 patients (13 male, 2 female) with known chronic liver disease and portal hypertension presented to our Unit as diagnostic or management challenge. All patients following standard diagnostic and/or therapeutic endoscopy, required further examination with an electronic radial or linear echoendoscope and/or EUS miniprobes for further management.
Results: In 10 patients polypoid looking lesions were seen in the fundus, body or gastric outlet not entirely typical of varices. In 8/10 cases these were varices under EUS while in 2 cases these were true polyps that were biopsied under EUS guidance. In 3/10 cases there were stigmata of recent bleeding and in all three cases thrombin was injected (250 iu/ml) with excellent effect and clot formation under EUS. Five patients with actively bleeding varices despite standard endoscopic therapy or TIPSS received thrombin injections under EUS guidance with a 22-gauge FNA needle or a standard injection needle. In 4/5 patients treatment was carried out in ITU/HDU and in one patient with chronic blood loss in the Endoscopy Unit. In 2 ITU patients (both ALD), 5–10 ml of thrombin was injected using a 22G FNA needle through an Olympus linear EUS scope until a clot was formed with real-time abolition of blood flow. One of the 2 patients had a variceal pseudo-aneurysm in the oesophagus directly communicating with the azygos vein and the second had bled from an ectopic duodenal varix directly communicating with the portal vein despite a successful TIPSS insertion. In 3 patients the Fujinon EUS miniprobes (12 MHz) were used through the biopsy channel of a standard endoscope before and after 5–10 ml of thrombin injection to assess clot formation. One of the 3 patients bled from gastric varices due to PV thrombosis, one from an oesophageal varix at 30 cm post-TIPSS and one had chronic bleeding due to ectopic duodenal varices secondary to SMV thrombosis and had been transfusion dependent. In all 5 cases haemostasis was achieved although one patient subsequently died in ITU due to liver failure.
Conclusion: (a) EUS with Doppler is a valuable technique to assist in the diagnosis and management of ectopic or gastric varices. (b) EUS-guided or assisted thrombin injection is a safe and effective way of achieving haemostasis in complex cases of bleeding varices where other therapies had failed.
0-44 PERSISTENT HISTOLOGICAL INFLAMMATION IN AUTOIMMUNE HEPATITIS DESPITE BIOCHEMICAL REMISSION: FREQUENCY AND PROGNOSTIC SIGNIFICANCE
1B. S. R. Höeroldt, 2A. K. Dube, 2J. C. E. Underwood, 3E. McFarlane, 1P. Basumani, 3D. Gleeson. 1Gastroenterology, Rotherham General Hospital, Rotherham, UK, 2Histopathology, Sheffield Teaching Hospitals, Sheffield, UK, 3Hepatology, Sheffield Teaching Hospitals, Sheffield, UK
Introduction: Most patients with autoimmune hepatitis (AIH) achieve clinical and biochemical remission following treatment with prednisolone ± azathioprine. Despite this, active inflammation persists on follow-up biopsy in some patients. There are limited data on the frequency and clinical significance of this phenomenon; follow-up biopsy is not routinely performed in patients with AIH in many centres.
Aims and Methods: Evaluation of the frequency and significance of persistent inflammation on follow-up biopsy in patients with AIH who have achieved clinical and biochemical remission. 81 patients with definite or probable AIH by International AIH Group criteria 1 who underwent repeat liver biopsy median (range) 25 (7–112) months after initial biopsy. All had achieved clinical and biochemical remission, defined as disappearance of symptoms and serum ALT<50 U/L. Biopsies were scored for inflammation and fibrosis using the Ishak Scoring system by one of two pathologists without reference to the clinical details.
Results: Ishak necro-inflammatory and fibrosis scores fell from (mean +SD) 11.4+4.7 and 3.6+1.7 respectively on initial biopsy to 3.1+2.9 and 2.5+0.5 on follow-up biopsy (p<0.01 by Wilcoxon paired test). However, 27 of the 81 patients had mild inflammation (necro-inflammatory score (NIS) 4–6) and 5 had moderate inflammation (NIS >6) on follow-up biopsy. Follow-up necro-inflammatory score (NIS) was positively associated with serum AST (p = 0.001) (but not serum ALT or globulin) at the time of biopsy and was negatively associated with time interval since initial biopsy (p = 0.008). In multiple regression analysis, follow-up NIS was independently associated with fibrosis stage (p = 0.005) on follow-up biopsy, with progression of fibrosis since initial biopsy (p = 0.047) and with disease relapse rate (p = 0.003). All-cause death or liver transplant rate was higher in patients with mild or moderate inflammation (NIS >3) than in those without (NIS 0–3): 14+9% vs 3+3% after 10 years and 57+14% vs 8+6% after 20 years. In Cox regression analysis, follow-up NIS was the strongest independent factor predictive of all-cause death or transplantation (p = 0.002). A similar association between follow-up NIS and liver-related death/transplantation was only significant in univariate.
Conclusion: Immunosuppressive treatment of AIH results in marked improvement in inflammation, and also improvement in fibrosis. However, almost 40% of patient with AIH who achieve biochemical remission have persistent histological activity on follow-up biopsy. This is predicted by a raised serum AST and is associated with disease relapse, fibrosis progression and increased mortality.
0-45 ALPHA1-ANTITRYPSIN HETEROZYGOSITY IS A SIGNIFICANT CO-FACTOR FOR PARENCHYMAL LIVER DISEASES
1W. Gelson, 2G. Maguire, 3S. Davies, 1W. Griffiths. 1Hepatology, Addenbrooke’s Hospital, Cambridge, UK, 2Biochemistry, Addenbrooke’s Hospital, Cambridge, UK, 3Histopathology, Addenbrooke’s Hospital, Cambridge, UK
Introduction: The degree to which heterozygous forms of alpha1-antitrypsin, principally MZ, cause liver disease is uncertain. Around 2% of the population carry the MZ phenotype. If heterozygosity is a relevant co-factor, over-representation in patients with end stage liver disease would be predicted.
Aims and Methods: The aim of this study was to evaluate a cohort of patients with severe liver disease for frequencies of abnormal alpha1-antitrypsin phenotype. We retrospectively analysed 278 consecutive patients with chronic liver disease assessed for liver transplantation in our unit between January 2005 and May 2007. Alpha1-antitrypsin heterozygotes were identified on the basis of agarose gel serum electrophoresis and/or histology demonstrating alpha1 globule deposition consistent with an abnormal phenotype (non serum-derived). Patients with PiZZ alpha1 anti-trypsin deficiency were excluded.
Results: 37 patients were identified as having an abnormal phenotype (35 MZ, 1 SZ, 1 MF). The prevalences of alpha1-antitrypsin heterozygosity according to main aetiological groups are shown in the table.
Conclusion: In our cohort, alpha1-antitrypsin heterozygosity was strongly over-represented in patients with advanced parenchymal liver disease, particularly NASH, alcohol and autoimmune-related. These figures are higher than those previously reported. The absence of alpha1 heterozygotes in patients with biliary disease further suggests that alpha1-antitrypsin deposition, in the heterozygote form, causes clinically-relevant hepatocyte damage. Alpha1-antitrypsin heterozygosity should be actively sought in patients with non-biliary liver disease and considered a significant risk factor for progression.
0-46 CIRCULATING CYFRA 21–1 IS A HIGHLY SPECIFIC DIAGNOSTIC AND PROGNOSTIC BIOMARKER IN BILIARY TRACT CANCER
1M. H. Chapman, 2N. Sandanayake, 2D. Dhar, 2F. Andreola, 3J. S. Dooley, 1S. P. Pereira. 1Institute of Hepatology, University College London and UCL Hospitals NHS Trust, London, UK, 2Institute of Hepatology, University College London, UK, 3Centre for Hepatology, UCL Medical School, London, UK
Introduction: Biliary tract cancer (BTC) has a poor prognosis, in part related to difficulties in diagnosis. The most commonly used biomarker, CA 19–9, has limited accuracy for diagnosis or for screening of high risk groups such as those with primary sclerosing cholangitis (PSC). Cytokeratin 19 (CK19) is a constituent of the intermediate filament proteins responsible for the structural integrity of epithelial cells. CK19 fragments (CYFRA 21–1) are rarely identified in the blood of healthy individuals, but have been recently reported to be associated with poor postoperative outcomes in Japanese patients with intrahepatic cholangiocarcinoma (CC).1 We assessed the utility of CYFRA 21–1 as a diagnostic and prognostic marker of BTC in a UK population.
Aims and Methods: Blood samples (n = 129) were collected prospectively from patients with benign biliary disease (n = 42), PSC (n = 20), PSC-related CC (n = 6) and BTC (n = 61; CC 57, gallbladder cancer 4). CYFRA 21–1 levels were measured in duplicate by ELISA (DRG Instruments, Marburg, Germany), either in serum (n = 81) or plasma (n = 48), after calculation of a correction factor using paired serum and plasma samples (n = 13).
Results: The sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) for CYFRA 21–1 and CA19–9, and both markers combined, are shown in the table. The area under the curve was 73% (95% CI 64% to 82%) for CYFRA 21–1 and 84% (76% to 91%) for CA19–9. Using the Kaplan-Meier method, neither the usual cut-off of 37 U/ml nor a higher cut-off of 129 U/ml for CA19–9 was a prognostic marker in BTC. However, CYFRA 21–1 (3.0 ng/ml) alone, or in combination with CA19–9, was a strong predictor of prognosis (median survival 4 months vs 10 months, p = <0.001). In PSC, the sensitivity and specificity for BTC were 82% and 87% using the combined lower cut-offs, and 57% and 94% for the higher cut-offs.
Conclusion: Elevated circulating CYFRA 21–1 is a highly specific diagnostic and prognostic marker in BTC. The combination of CYFRA 21–1 and CA19–9 further improves diagnostic accuracy. Multicentre validation studies of these biomarkers for the diagnosis of BTC in patients with and without PSC are planned.
0-47 ANTIMITOCHONDRIAL ANTIBODY POSITIVE WITH NORMAL LFTS – 20 YEARS ON: IS THIS PBC AS WE KNOW IT?
1R. E. Swann, 2M. Bassendine, 3O. James, 2D. E. Jones, 4H. Mitchison, 5M. Prince, 6J. Metcalf. 1Gastroenterology, Royal Victoria Infirmary, Newcastle Upon Tyne, UK, 2Department of Hepatology, School of Medicine, Newcastle University, Newcastle Upon Tyne, UK, 3School of Medicine, Newcastle University, Newcastle Upon Tyne, UK, 4Department of Gastroenterology, Sunderland Royal Infirmary, Sunderland, UK, 5Department of Gastroenterology, Manchester Royal Infirmary, Manchester, UK, 6Department of Gastroenterology, University Hospital of North Tees, Stockton on Tees, UK
Introduction: In 1986 we reported 29 antimitochondrial antibody (AMA) +ve (indirect immunofluorescence 1/40 or greater) patients, with normal lever function tests (LFTs). All had liver histology: 24 had histology compatible with PBC.1 By 1996, 20 had “definite PBC”, 9 “possible”. (Definite PBC was defined as cholestatic LFTs, AMA positivity and compatible biopsy. Probable PBC was defined as 2 out of 3 of the above). 21/29 were found to be PDC-E2 M2 ELISA +ve, 6−ve, 2NA.2
Aims and Methods: We aimed to determine outcomes of these patients compared with “classical” PBC patients after 20 years of follow up. We collected lab and clinical details from case records, and Death Certificates. The results were compared with those for our whole unselected cohort of 770 PBC patients3 and times to specific outcomes calculated using Kaplan-Meier plots. A smaller group of 48 matched controls were selected for comparison of mortality data.
Results: The average age of our cohort at first AMA+ve was 52 years (33–69), mean follow up was 21.5 years (6.1 to 30.5). By this time 22 had definite PBC, 4 probable PBC, 1 overlap syndrome and 1 was unlikely to have PBC (developing negative AMA and normal LFTs). The time to death from symptom or abnormal LFTs development was much greater in our 29 patients than would be expected from the classical PBC cohort data (see table), with a 10 year survival from symptom development of 89% (compared with 50% in the symptomatic classical PBC cohort). Mortality data from the group of matched PBC patients showed a trend towards longer survival in our AMA+ve/N LFTs group; however this did not reach significance over the follow up period (p 0.09). 6 patients developed clinical signs of cirrhosis, 2 of which died (7.8% liver deaths vs 41.7% in main cohort). All these patients were PDC-E2 ELISA+ve. Overall 16/29 died, mean age of death 77.8 years (range 66.7–90.6 years) with the mean age for liver death being 77.6 years.
Conclusion: After over 20 years of follow up it appears the vast majority of AMA positive patients who have normal LFTs do have PBC. However, we can confidently reassure them their illness is likely to take a benign course.
Service development free papers
0-48 A 12 MONTH STUDY OF JAUNDICE CLINIC OUTCOME IN THE MODERN NATIONAL HEALTH SERVICE
1R. Arulraj, 2J. Dowman, 3A. Simons, 4S. Roy-Choudhury, 3I. Chesner. 1Gastroenterology, Walsall Manor Hospital, Walsall, UK, 2Liver unit, Queen Elizabeth Hospital, Birmingham, UK, 3Gastroenterology, Birmingham Heartlands Hospital, Birmingham, UK, 4Radiology, Birmingham Heartlands Hospital, Birmingham, UK
Introduction: Jaundice clinic and hotline shortens time to diagnosis, length of stay in hospital and treatment. We run a twice weekly jaundice clinic with a 24/7 fax/phone referral service (maximum 4/week) from 2003.
Aims and Methods: We audited our jaundice clinic outcomes over a 12 month period with an aim to demonstrate jaundice clinic’s efficiency in keeping with modern NHS targets through outpatient based service. All referred patients (maximum 4/week) have ultrasound on arrival followed by a gastro registrar/consultant review. We reviewed the electronic records (vortal system) of all patients referred to the jaundice clinic over 12 months (October 06–October 07).
Results: 82 patients (M: F 47: 35) with a mean age of 64.5 years were referred. On the initial ultrasound 40 patients had dilated ducts and 16 had mass demonstrated. Common presenting symptoms were weight loss 50% (41/82) and abdominal pain 47% (39/82); common signs were jaundice 94% (77/82) and organomegaly 24% (20/82). The 3 most common diagnoses were pancreatic cancer 24% (20/82), common bile duct stones 21% (17/82), and cholangiocarcinoma 10% (8/82). 98% (80/82) of patients were seen within a week’s time of referral. 2 week rule was met in all cancers; 62 day treatment rule was met in 90% (26/29). In benign diseases 18 week treatment rule was met in 91% (48/53). The average waiting time for CT/MRI was 5.4 days (61%, 50/82) and ERCP/PTC was 7.6 days (59%, 48/82). Only 1 patient needed inpatient admission (cholangitis) via jaundice clinic; rest were managed as outpatients (9 were admitted post ERCP for failed stenting/complications). 6% of referrals (5/82) were inappropriate; 40% (79/186) of liver screen tests were inappropriate (done in patients with dilated ducts).
Conclusion: Most of our patients were managed as outpatients with ultra short waiting time for review/duct drainage/further management. A GI consultant/registrar led jaundice clinic is an effective way of meeting modern NHS targets in an outpatient setting without compromising patient care and workforce.
0-49 A YEAR IN THE LIFE OF AN INDEPENDENT SECTOR TREATMENT CENTRE (ISTC): THE ENDOSCOPY SERVICE AT ST MARY’S NHS TREATMENT CENTRE
1S. Caronia, 1A. Murkin, 2H. Ludford. 1Endoscopy Unit, St Mary’s NHS Treatment Centre, Portsmouth, UK, 2General Manager, St Mary’s NHS Treatment Centre, Portsmouth, UK
Introduction: Independent Sector Treatment Centres (ISTC) were controversially launched throughout the UK with concerns about their ability to deliver a high quality health service. This abstract illustrates 1 year of activity of the endoscopy Unit at St Mary’s NHS Treatment Centre in Portsmouth (SMTC).
Aims and Methods: Clinical quality and safety data from all consecutive endoscopic procedures performed at SMTC were collected and analysed as outlined by the Global Rating Scale (GRS) assessment of UK endoscopy units’ key quality and safety indicators. Patient satisfaction surveys were conducted by two different means: 1) continuous survey by an independent company, published on a monthly basis; 2) in-house survey administered every 3 months. Decontamination standards were monitored and audited on a regular basis. A multiple levels clinical governance structure was implemented. SMTC was entered as pilot ISTC for JAG accreditation.
Results: Between October 2007 and October 2008, 452 colonoscopies, 65 sigmoidoscopies and 1210 gastroscopies were performed at SMTC. “A” status was achieved for all the GRS key quality and safety indicators. Patient satisfaction was rated as 98% in both means of testing. Decontamination standards were met in all cases. In September 2008, SMTC received full JAG accreditation with “A” status at first visit. SMTC was commended by JAG for, its “patient centred services, excellent teamwork, strong governance structure, excellent environment and facilities, productivity tracking and reporting, strong training and competence culture, its quality focus, auditing and performance”.
Conclusion: The example of SMTC demonstrates that ISTCs can deliver a first class endoscopy service and should be regarded as a valuable addition to the UK health system.
0-50 STRAIGHT TO TEST FOR COLONOSCOPY CAN REDUCE TIME TO DIAGNOSIS FOR SUSPECTED COLORECTAL CANCER?
N. R. O’Shea, M. Walshe, V. Wong. Centre of Gastroenterology, Whittington Hospital NHS Trust, London, UK
Introduction: Colorectal cancer (CRC) is a common cause of mortality in the UK. Early diagnosis is crucial in determining prognosis. Patients with suspected CRC are being referred via Two Week Wait (2WW) to expedite diagnosis. We have previously piloted a Straight To Test (STT) for colonoscopy whereby patients could be triaged directly to colonoscopy without a prior gastroenterology clinic consultation and this showed encouraging results (BSG 2008). This study has been extended to include Type II diabetic patients and urgent referrals with alarm symptoms.
Aims and Methods: GP referrals for urgent and 2WW colonoscopies were faxed to endoscopy between Jan 07 and Oct 08 (21 months) and reviewed by a Gastroenterology Consultant. The Colorectal Nurse Specialist triaged the patients by telephone consultation, explained the procedure and bowel preparation. Data were collected using a standard proforma to assess an individual’s suitability. Patients had the choice to be seen in clinic first if they preferred. Exclusion criteria: Age >75, ASA score >2, on warfarin, unable to speak English or consent.
Results: 87 patients were eligible for STT (46 males, 41 females, aged 32–78). 89% (77/87) of patients were triaged and contacted by telephone within 6 days of GP referral. 88% (64/73) were colonoscoped within 14 days, 16% (14/87) did not attend (DNA). All patients referred via 2WW who did not proceed STT had a colonoscopy within 14 days of their hospital clinic appointment. 97% (71/73) of STT colonoscopies were successfully carried out to caecum. 49% (35/71) of the colonoscopies were normal to the caecum. Abnormal findings in 51% (36/71) were 1 colorectal cancer, 20 polyps (7 moderate dysplasia, 6 mild dysplasia, 4 hyperplastic, 1 inflammatory, 2 no histology), 5 colitis, 5 haemorrhoids, 4 diverticulosis, 1 melanosis coli, 1 angiodysplasia. No adverse events or patient dissatisfaction documented.
Conclusion: These findings suggest that it is possible to proceed STT for colonoscopy if patients are selected carefully using a simple exclusion criteria. Our experience suggests this method is acceptable to patients and potentially cost and time effective. It could be used as a strategy for reducing waiting times and decision making regarding management. Based on these findings we intend to expand our STT service and include patients referred for urgent and routine colonoscopies who fulfil a pre-determined criteria.
0-51 IMPLEMENTING AN UPPER GASTROINTESTINAL BLEEDING ROTA AT THE JAMES PAGET UNIVERSITY HOSPITAL
B. T. Brett, A. de Silva, G. Vautier, J. Dron, K. Muhdi, R. Guruswamy, M. Williams. Department of Gastroenterology, James Paget University Hospital, Great Yarmouth, UK
Introduction: Acute upper gastrointestinal bleeding (AUGIB) is a serious common and life threatening condition. Despite this many hospitals including our own did not or continue not to offer an out of hours service. The BSG has worked with partner organisations to encourage Trusts to develop such services either on their own or in collaboration with neighbouring Trusts.
Aims and Methods: The development of an out of hours AUGIB service required several different approaches: the Chief Executive, Executive Team and Trust Board had to be convinced of the need for such a service; a business case had to be developed and presented to the Trust Investment Group; negotiations with the Trusts’ general physicians had to take place and an agreement needed to be reached; negotiations and agreement also had to be reached with the endoscopy nursing staff and endoscopists.
Results: Financial approval for an AUGIB out of hours service was obtained from the Trust Investment Group after gaining backing from the Chief Executive, Executive Team and Trust Board. A new hybrid GI bleeding/General Medical rota was negotiated, with gastroenterologists remaining on the General Medical rota during the week and supporting the Emergency Assessment and Discharge Unit on weekend mornings whilst on for GI bleeding. The service was commenced in September 2008. Each week so far there has been between 1 and 4 out of hours referrals with AUGIB, virtually all of which were endoscoped within 24 hours (in 1 case it was not felt appropriate to offer further endoscopy). In every case management has been altered – ranging from early discharge to early referral for surgery. We continue to monitor the impact of this new service.
Conclusion: It is possible to establish a viable acute upper GI bleeding service in a hospital serving less than 250 000 population. Novel solutions such as hybrid GI bleeding/General Medical rotas may need to be explored in other similar Trusts. Early cases and data suggest that such a rota is likely to influence the management of the majority of patients. This fledgling service will need modifying in time to ensure it offers the maximal benefit to patients whilst remaining acceptable to hospital staff.
0-52 RESULTS FROM AN ENDOSCOPY WAITING LIST VALIDATION PROJECT
D. Chan, R. Shah, M. W. Johnson, D. H. Dewar. Gastroenterology, Surrey and Sussex Healthcare NHS Trust, Redhill, UK
Introduction: Our institution was identified as having increasing and unacceptable waiting times for endoscopic procedures, a situation which evolved in part due to merging of two hospitals and their waiting lists. In total 3627 patients were waiting for initial endoscopy or recall as part of their gastroenterology follow-up. An Endoscopy Validation Project was set up comprising an independent Clinical Lead, two locum Consultant Gastroenterologists, and three administrative staff. We wish to report the successful mechanisms and outcome of this project.
Aims and Methods: An algorithm was established for validating all active waiting list and recall patients. Waiting list patients were prioritised and a rapid decision was made whether to proceed to endoscopy. BSG guidelines were used to validate the indications for endoscopy with allowance made for clinical judgement where stated. All recall patients had their medical records, previous endoscopy reports and previous histology examined before a validation decision was made. Where insufficient information was available, further clarification was sought from patient, GP or referring Consultant. Patients were given the opportunity to be reviewed in clinic. Provision was made for additional endoscopy lists. The aims were clearance of the existing waiting list and attaining compliance with a target of a maximum 5 week wait at the end of a six month period.
Results: New referrals were matched with existing capacity to ensure 98% compliance with a maximum wait of 5 weeks from referral with an average waiting list of 230 patients (5 samples over 3 months). Out of 2684 patients on the initial existing waiting list, 1991 (74%) patients required their procedure and of these, 1732 (87%) underwent endoscopy (median wait 7.5 months). Sixty patients (3%) declined their procedures and 199 (10%) had moved out of the area. The recall list comprised 974 patients overdue at the mid-point of the project. After validation, 202 procedures (21%) were overdue by a median 6 months and underwent their procedure, 303 (31%) were postponed by a median of 23 months and 469 (48%) were deemed not required based on clinical indications or co-morbidity. Clerical or administrative error affected 17% of waiting list entries. Following additional information provided in 13 cases, colonoscopy was re-instated. We received 19 written complaints about the Endoscopy Validation Project, 17 from GPs and 2 from patients. Apart from clinical risk associated with delay in clinically indicated endoscopy, two adverse events were reported with no evidence of patient harm. No patients remained outstanding or unaccounted for after six months.
Conclusion: Our Endoscopy Validation Project was highly successful in eliminating a large waiting list and restoring a balance between demand and capacity in our endoscopy unit.
BSG information group symposium
0-53 UNDERSTANDING VARIATION IN HOSPITAL LENGTH OF STAY FOR GASTROINTESTINAL DISORDERS ADMITTED AS EMERGENCIES IN ENGLAND: CLINICALLY-DRIVEN ANALYSIS OF HOSPITAL EPISODE STATISTICS
1K. Bodger, 2C. Grant-Pearce, 2E. Thompson, 2D. Lowe, 2M. Pearson. 1Gastroenterology Division, School of Clinical Sciences, University of Liverpool, Liverpool, UK, 2Department of Clinical Evaluation, University of Liverpool, Liverpool, UK
Introduction: Efficient use of costly inpatient resources is a priority in all healthcare systems. Managerial focus on mean “length of stay” (mLOS) is inevitable but often LOS figures are presented for heterogeneous cohorts of patients (eg. by “hospital” or “ward”) making interpretation and action difficult. This study aimed to analyse national LOS data for gastroenterological emergencies in a statistically robust and clinically meaningful manner with a view to producing comparative local data.
Aims and Methods: HES data for 2006/7 (relating to 2.236 million emergency admissions to 151 acute Trusts in England) was analysed. A steering group comprising BSG representatives, physicians, surgeons, public health, patient groups and IT specialists guided the project. Coded episodes were converted to spells of care (“admissions”) and primary diagnosis fields were used to categorise patients into logical clinical baskets of disorders based on ICD-10 codes. The national data were used to construct a look-up table representing the expected LOS (eLOS) for patient age (in 5-year age bands) and diagnostic sub-groups. For each emergency admission, the difference between eLOS and actual LOS were calculated and averaged across each Trust.
Results: 286 316 emergency gastrointestinal (GI) admissions were coded (13% of acute medical workload in England). National mLOS was 8.4d with “prolonged” stay (21+d) in 9.9% and strong correlation between the two measures (r = 0.94). LOS rises by >1d/decade increment in age. Range of mLOS across trusts for GI emergencies was 5.5–12.5d compared to a predicted range of 6.9–9.9d, suggesting unexplained variation. Longer mLOS was associated with GI cancer (14.47d) and hepatology/pancreaticobiliary diagnoses (11.96d), whereas admissions coded with “Symptom/Sign” ICD-10 codes (eg. “Vomiting”) had shorter stays (5.15d). Tabulation of excess bed days by age- and diagnostic-group may identify areas for targeted action (eg. a trust with selective “excess” LOS for “benign luminal conditions” in younger patients may identify non-urgent inpatient endoscopy provision as a limiting factor). There was no trend for large city conurbations to be at one end of the spectrum nor a strong effect of deprivation variables.
Conclusion: Emergency care for GI disorders accounts for a significant proportion of acute workload in English hospitals (13%). mLOS varies widely between hospitals but a minority of “prolonged stay” patients are a major contributing factor to crude mLOS figures. Using national data to derive “expected” values by age and diagnostic group revealed unexplained variations between hospitals which may allow local teams to better target areas for potential action. The next phase of the project will deploy the data on a website for gastroenterologists in order to seek feedback, drive improvements in coding quality and encourage local use of the data. Analysis of additional co-morbidity variables is under evaluation. (Funding: NHS Information Centre)
0-54 INTEGRATION OF QUALITY AND SAFETY INDICATORS FOR ENDOSCOPY FROM THREE DATABASES ACROSS FOUR HOSPITAL SITES
R. M. Valori, J. L. Brown, K. Dowler. Gastroenterology, Gloucestershire Hospitals, Gloucester, UK
Introduction: For revalidation to be meaningful endoscopists will, in future, be required to submit performance data for all the procedures they perform. Endoscopists often work on different sites and there may be more than one database that captures essential quality and safety information. Thus there is a need to collect, collate and integrate data from different databases to provide meaningful performance data for revalidation.
Aims and Methods: The aim of this work was to provide a single performance record for individual endoscopists that contains quality, comfort and safety indicators, and productivity data. Data are entered into one of two endoscopy reporting systems (ERS) on four different hospital sites. The reporting systems are a local, custom-made ERS and a commercial system (Unisoft). Key quality indicators are extracted from these two reporting systems and downloaded into an endoscopist performance database. Immediate adverse outcomes, patient and nurse comfort assessments, and productivity data are collected on the patient administration system (PAS) and then extracted and downloaded into the performance database. Data from the different systems is matched using unique patient identifiers.
Results: Data from two endoscopy reporting systems, situated in four endoscopy units, was successfully combined with PAS data to produce a combined performance record for each endoscopist. This record includes endoscopy outcomes, patient and nurse assessed comfort, productivity data and immediate adverse events.
Conclusion: It is possible to combine key quality and safety performance data for individual endoscopists from different endoscopy reporting systems and PAS, on four discrete endoscopy sites. The methodology underpinning this work could be used to create a regional or national database of endoscopist performance.
BSG endoscopy videos and free papers
VC-55 ENDOSCOPIC RESECTION OF LARGE FLAT RIGHT-SIDED COLONIC POLYPS: PUSHING THE BOUNDARIES OF THERAPEUTIC ENDOSCOPY
M. D. Duku, R. J. Mead, P. Bhandari. Gastrornterology, Queen Alexandra Hospital, Portsmouth, UK
Introduction: Endoscopic resection of large flat polyps in the right colon is technically challenging. Amongst the most challenging are large flat polyps in the periappendicular region, on the ileocaecal valve and extending into the terminal ileum. Traditionally most of these polyps were referred for surgical resection; however, with advances in the endoscopic therapy most of these polyps can be safely resected endoscopically.
Aims and Methods: To illustrate, using three video clips, the principles of safe and effective resection of large flat polyps in the right colon and treatment of intraoperative bleeding. The polyps are located at:
The Ileocaecal valve extending into the terminal ileum.
The periappendicular region
The hepatic flexure
A gastroscope was used in both straight and retroflexed positions to assess and resect the polyps. The polyps were first assessed for the absence of invasive cancer features and their margins clearly defined using indigo carmine chromoendoscopy and/or FICE. This was followed by submucosal injection, and depending on size, the polyp is snared en bloc or piece meal. All resected specimens were retrieved for histological staging.
Results: In the last 24 months, we have resected 89 large (>2 cm) flat colonic polyps of which 12 were in the right colon. Complete endoscopic resection was achieved in all 12 cases in one session. There was one intraoperative bleeding, successfully controlled endoscopically, but no delayed bleeding, and no perforations. Histological assessment of the resected polyps showed only low-grade or high-grade dysplasia.
Conclusion: Endoscopic resection of large flat right colonic polyps is feasible and can be performed safely in experienced hands. They are best resected using a gastroscope after careful endoscopic assessment for the absence of features of invasive cancer.
VC-56 ENDOSCOPIC SUBMUCOSAL DISSECTION/ENDOSCOPIC MUCOSAL RESECTION (ESD/EMR) HYBRID: A NOVEL KNIFE ASSISTED EMR TECHNIQUE FOR RESECTING FLAT COLORECTAL LESION
M. D. Duku, R. J. Mead, P. Bhandari. Gastroenterology, Queen Alexandra Hospital, Portsmouth, UK
Introduction: Traditional piece meal endoscopic resection of flat polyps greater than 30 mm is associated with a high recurrence rate due to residual adenoma at the lateral resection margins. This led to the development of knife-assisted technique of endoscopic submucosal dissection (ESD), which allows en bloc resection with very low recurrence rate. In skilled (Japanese) hands ESD is a very good technique but even in Japanese hands this technique has a long learning curve, long procedure time (1–5 hours) and a significant risk of perforation and bleed. We have developed a novel technique which significantly reduces the procedure time, the complication rate and can still achieve the low recurrence rate as seen with ESD.
Aims and Methods: We aim to illustrate the principles of this new technique using five video clips resecting large flat colorectal polyps and submucosal tumours in the upper gastrointestinal (GI) tract. All lesions are carefully assessed using chromoendoscopy and/or FICE to assess for features of invasive cancer and to clearly define their margins. We have used a series of endoscopic knives including needle knife, IT knife-1 and 2, flush knife, hook knife and flex knife. The technique involves identification of margins, premarking (if necessary) peripheral submucosal injection, a knife assisted circumferential incision which isolates the neoplastic tissue from the non neoplastic tissue, further submucosal injection into the neoplasia, and finally snare resection of the lesion in one or multiple pieces.
Results: We have used this technique in more then 25 lesions of various sizes in upper and lower GI tract. We haven’t had any perforations or delayed bleeds. Intraoperative ooze is not uncommon but can be effectively controlled by endotherapy. Time of the procedure depends on the size of the lesion and in our experience it has been between 30–120 minutes.
Conclusion: We have shown the safety and feasibility of our novel technique. We believe that our technique is best suited for western endoscopists as it has a short learning curve and avoids the need for radical and unnecessary surgery or ESD.
VC-57 DIFFICULT, LARGE, AND FLAT ANORECTAL POLYPS – IS ENDOSCOPIC RESECTION FEASIBLE?
R. Mead, M. D. Duku, P. Bhandari. 1Gastroenterology, Queen Alexandra Hospital, Portsmouth, UK
Introduction: Advances in endoscopic techniques and pathological understanding (pit pattern) are allowing endoscopists to resect very large, flat, and challenging lesions in the recto-sigmoid region. Traditionally >3 cm lesions, or those touching the dentate line, have been treated with transanal resection of tumour/transanal endoscopic microsurgery (TART/TEMS), or anterior resection. We have developed an EMR service in Portsmouth Hospital where all these lesions are now treated endoscopically. We will illustrate the principles and techniques we use in their resection.
Aims and Methods: We use a wide range of ESD knives (flex, hook, IT, and flush, needle) and snares to achieve these resections. We will illustrate: endoscopic control of bleeding; pain control in dentate line lesions; use of the gastroscope and the J manoeuvre; stepwise techniques common to all endoscopic resections; new and established techniques for endoscopic resection.
Results: We have resected 35 rectal adenomas in the last 2 years, with a mean size of 5.6 cm (2.5–15 cm). These are all referral cases from colorectal surgeons or gastroenterologists. Two complications occurred in the first 7 days; 1 micro-perforation; and 1 delayed bleed controlled endoscopically.
Conclusion: We have demonstrated the feasibility of resecting large, flat and difficult recto-sigmoid polyps, showing novel and established endoscopic resection techniques. These patients would have otherwise required a surgical approach, including anterior resection.
VC-58 CONTROL OF BLEEDING DURING ENDOSCOPIC PIECEMEAL MUCOSAL RESECTION AND ENDOSCOPIC SUBMUCOSAL DISSECTION
N. Suzuki, B. P. Saunders. Wolfson Unit for Endoscopy, St Mark’s Hospital, Harrow, UK
Introduction: Endoscopic piecemeal mucosal resection (EPMR) and endoscopic submucosal dissection (ESD) are effective therapeutic modalities for removal of large colorectal neoplasms. Control of haemorrhage is crucial for successful endoscopic therapy.
Aims and Methods: This video demonstrates methods of haemostasis during EPMR and ESD.
Results: Case 1—Small oozing was encountered during mucosal incision. Accurate identification of a small bleeding vessel was achieved by irrigation of the visual field with the Flush knife® (Fujinon) and treatment with the tip of the knife using forced coagulation 35W (ICC 200, ERBE). Cases 2 and 3—Coagulation forceps are essential for control of more significant bleeding from larger vessels during ESD. Moderate bleeding shown in case 2 was managed with the Cograsper® (Olympus). The exact bleeding point is grasped with the forceps, resulting in cessation of blood flow from mechanical pressure prior to the application of soft coagulation 60W. In extreme cases as shown in case 3, spurting arterial bleeding is encountered during submucosal dissection. Several attempts may be required to coagulate the responsible vessels. The grasped vessel should be tented up during application of coagulation to avoid heat injury to the deeper bowel wall. Case 4—A combination use of haemostatic modalities may be required in some cases. The application of endoclips before the dissection/resection is complete is best avoided because early application of endoclips may obscure the view and obstruct the procedure. In case 4, piecemeal polypectomy was carried out without treating the bleeding vessel in order to provide a better field of view. Once space was created around the bleeding vessel it was initially treated with argon plasma coagulation and then forceps coagulation. This was ineffective therefore finally three endoclips were required.
Conclusion: With the introduction of bowel cancer screening programmes the need for advanced polypectomies may increase. Colonoscopists must be familiar with haemostatic techniques and be confident in managing complications to ensure patient safety and avoid unnecessary surgery.
VC-59 ENDOTHERAPY WITH BALLOON ENTEROSCOPES
S. John, M. L. Remedios, M. N. Appleyard. Gastroenterology, Royal Brisbane and Women’s Hospital, Brisbane, Australia
Introduction: Balloon enteroscopy allows endoscopic evaluation and therapeutic intervention in the small bowel. The commonest indication is obscure gastrointestinal bleeding. However, balloon enteroscopy is also performed in the context of an abnormal capsule study and less commonly for abnormal small bowel radiology.
Aims and Methods: Several therapeutic interventions are possible with a balloon enteroscope. These include treatment of bleeding lesions with endoclipping, argon plasma coagulation or injection of adrenaline or glue and also tattooing of lesions, performing balloon dilatation, polypectomy and endoscopic retrograde cholangiopancreatography (ERCP) in a surgically altered small bowel. The submitted video shows some of these.
Results: The video shows a case of endoclipping in the jejunum followed by injection of small bowel varices with glue, performing ERCP and balloon dilatation of a hepatico-jejunostomy and polypectomy and retrieval of specimen from the jejunum.
Conclusion: Balloon enteroscopy allows a variety of endotherapy anywhere in the small bowel. The availability of these has changed the way we manage small bowel pathology.
0-60 ENDOSCOPIC ULTRASOUND GUIDED ELASTOGRAPHY FOR LYMPH NODE ASSESSMENT IN UPPER GASTROINTESTINAL CANCER
S. Paterson, A. J. Stanley. Gastroenterology, Glasgow Royal Infirmary, Glasgow, UK
Introduction: Endoscopic ultrasound (EUS) is an integral investigation in the staging of oesophageal and selected gastric cancers as per national and international guidelines. Determination of lymph node disease in particular is of critical prognostic importance. There have been a limited number of studies assessing the accuracy of EUS elastography for nodal assessment in upper GI malignancy but no published UK data. Elastography relies on the stiffer consistency and reduced deformity of pathologically abnormal tissue compared with surrounding normal tissue. This difference can be detected during EUS as a strain ratio. This may provide complementary information to standard EUS nodal assessment and possibly avoid the need for fine needle aspiration biopsy (FNAB) of suspicious nodes.
Aims and Methods: The aim was to apply elastography at the time of EUS-FNAB for upper GI cancer staging to determine if discrimination between benign and malignant nodes is possible. Patients undergoing EUS-FNAB for staging of upper GI tract cancer during the period July 2007 to September 2008 had elastography of the node prior to sampling. The strain ratio was determined between the node and surrounding tissue. The mean of three strain ratio values was calculated. Lymph nodes were also characterised using standard EUS assessments of site, size, echogenicity, shape and the distinction of node boundary. FNAB was performed on 3 passes using a 22 gauge needle before cytological analysis.
Results: Elastography and FNAB were performed on 35 lymph nodes in 33 patients. Both interventions were successful in 34 nodes, with one technical failure in the elastography measurement. Cytological malignancy was found in 12, one was indeterminate, one was a GIST and 20 were negative for malignant disease. Excluding the indeterminate node and GIST and applying a strain ratio of >9 as a cut-off for malignant involvement gave a sensitivity of 100% (10/10), specificity of 91% (20/22), positive predictive value of 83% (10/12) and negative predictive value of 100% (20/20). Elastography was more sensitive and specific in determining malignant nodal disease than the standard EUS combined criteria of size, echogenicity, shape and clarity of boundary (p<0.05).
Conclusion: EUS elastography is a promising modality that may complement standard EUS in the differentiation of benign and malignant lymph nodes in upper GI tract cancer.
0-61THE LARGEST UK EXPERIENCE ON CAPSULE ENDOSCOPY
R. Sidhu, D. S. Sanders, K. Drew, M. E. McAlindon. Gastroenterology, Royal Hallamshire Hospital, Sheffield, UK
Introduction: Internationally small bowel capsule endoscopy (CE) is well established. However, there is a paucity of published data from the UK pertaining specifically to the clinical utility of CE and its impact on subsequent patient management.
Aims and Methods: To evaluate the diagnostic yield and effect of CE on patient management in routine clinical practice, in a tertiary setting. All patients who underwent CE since June 2002 were recruited. Data were collected prospectively including demographics, indication of CE, diagnosis and subsequent change in clinical outcome. Follow up data were obtained from the referring hospitals. The data were analysed using SPSS.
Results: 950 examinations were performed over 76 months. Females represented 58% with a mean age of 51 years. 50% of the referrals were from outside the North Trent region. Indications included obscure gastrointestinal bleeding (OGB): iron deficiency anaemia (IDA) (n = 373), overt bleeding (OB) (n = 125), Crohn’s disease (n = 260), coeliac disease (n = 73) and miscellaneous (n = 92); 27 examinations failed due to gastric retention or loss of transmission. The overall diagnostic yield was 40%; but was notably higher in patients with OGB: 50% when compared to other referral indications (p<0.001, OR 2.4, 95% CI 1.8 to 3.2). There was no significant difference in the diagnostic yield between patients who presented with IDA (48%) or OB (55%, p = 0.15). The commonest finding was angiodysplasia in 52% of patients with OGB whilst small bowel tumours accounted for 3% of the diagnoses. In 11.7% of patients with OGB, the pathology found on CE was located in the stomach (9.4%) or colon (2.3%). Patients who were diagnosed with active Crohn’s disease on CE had five or more ulcers and mucosal erythema ± additional erosions and mucosal oedema. In the Crohn’s subgroup, the diagnostic yield was 65% in the established Crohn’s disease and 23% in the suspected Crohn’s disease (p<0.001, OR 6.2, 95% CI 3.1 to 12.2). As a result of CE, management was altered in 27% of patients in the entire cohort. This was mainly in the form of endoscopic treatment of angiodysplasia (heater probe/argon plasma coagulation) or referral for surgery for small bowel tumours/strictures in patients with OGB (29%). Management was also altered in 79% of patients who were found to have Crohn’s disease on CE: step up of inflammatory bowel disease therapy/referral for surgery.
Conclusion: This is the largest series of CE from the UK. This study has shown that CE has both a high diagnostic yield and a positive impact on patient management. Our results support the role of CE in routine clinical practice in the UK.
Joint IBD and pathology symposium
0-62 A FUNCTIONAL STUDY OF THE EFFECT OF THE 14 BP INSERTION DELETION POLYMORPHISM OF THE HLA-G GENE ON RESPONSE TO IMMUNOMODULATORY THERAPY IN INFLAMMATORY BOWEL DISEASE
1B. Baburajan, 2N. Prescott, 1B. Hudspith, 1A. Ansari, 1M. Smith, 3M. Arenas-Hernandes, 2C. Mathew, 4L. Fairbanks, 2C. Lewis, 4A. Marinaki, 1J. Sanderson. 1Nutritional Sciences Division, Kings College London, UK, 2Department of Medical and Molecular Genetics, Kings College London, UK, 3Purine Research Laboratory, St Thomas Hospital, London, UK, 4Purine Research Laboratory, Kings College London, London, UK
Introduction: In inflammatory bowel disease (IBD), immunosuppression is standard therapy but success is limited by side effects and non-response. The effect of a 14bp ins/del polymorphism in the HLA-G gene on chromosome 6 on individual response to methotrexate (MTX) is recognised.
Aims and Methods: To study the influence of a 14bp ins/del polymorphism in the HLA-G gene on response to azathioprine (AZA) and to examine the functional effects of this polymorphism on the expression of soluble HLA-G and the closely related IL10 by stimulated peripheral blood mononuclear cells (PBMCs) when exposed to 6 mercaptopurine (6-MP) and MTX in vitro. Patients with IBD (n = 99) were prospectively studied for response to AZA in a dose of 2 mg/kg body weight. Drug response was correlated with genotype. PBMCs from 16 normal volunteers were stimulated with LPS and then cultured with 6 MP and MTX for 48 hours. sHLA-G and IL10 levels were then estimated.
Results: There is a strong influence of the 14bp del/del polymorphism on favourable clinical response to AZA (p = 0.001, OR = 5.469, 95% CI 1.869 to 15.9). Normal subjects with the 14bp del/del polymorphism expressed significantly higher levels of soluble HLA-G (sHLA-G) after incubation with 6-MP (p = 0.02) and MTX (p = 0.006) than carriers of the insertion allele. sHLA-G is thought to mediate the immuno-tolerant effects of HLA-G. No correlation was noted with IL10 expression.
Conclusion: This novel effect appears to be a strong marker of response to immunomodulatory therapy in patients with IBD and may identify a group of subjects with the potential for poor therapeutic response to standard treatment protocols and who could instead be treated with early anti-TNF strategies.
Pancreatic free papers
0-63 POSTERIOR MARGIN INVOLVEMENT ALONE DOES NOT INFLUENCE SURVIVAL IN RESECTED PANCREATIC CANCER
1N. B. Jamieson, 1P. Glen, 2K. A. Oien, 2J. J. Going, 2A. K. Foulis, 1E. Dickson, 1C. W. Imrie, 1C. J. McKay, 1R. Carter. 1West of Scotland Pancreatic Unit, Glasgow Royal Infirmary, Glasgow, UK, 2Department of Pathology, Glasgow Royal Infirmary, Glasgow, UK
Introduction: Pancreatio-duodenectomy for ductal adenocarcinoma of the pancreas results in resection margin involvement in around 75% of specimens. The significance of which margins are involved has not been previously studied. No lymphatics drain through into the posterior margin and it was felt that this margin was less likely to influence survival. The aim of the present study was to assess correlation of posterior margin involvement with survival.
Aims and Methods: Patient and tumour characteristics were extracted from a prospective database. Patients who died within 30 days were excluded from the analysis. Margin involvement was defined as positive if tumour was present within 1 mm of circumferential or transection margin. Margins were defined as anterior, posterior, medial and transection margin.1
Results: 126 consecutive patients undergoing pancreato-duodenectomy for pancrentic cancer were studied. 31 were defined as R0 and 95 (75%) as R1, with median survival 27.5 months and 13.6 months, respectively (p = 0.030). In 16 patients, posterior margin only was involved and survival in this group compared with R0 resections was not significantly different (p = 0.920). Survival was significantly better in R1 posterior only patients than any other R1 patients (p = 0.02). Modifying the R0 resection group (R0mod) to include patients with R1 involvement of the posterior margin allowed comparison with the R1mod. R0mod (n = 47) and R1mod (n = 79) had median survivals of 28.5 months and 13.3 months respectively (p = 0.001).
Conclusion: Involvement of the posterior margin alone in pancreatic ductal adenocarcinoma is not associated with a poor outcome in this cohort. Further work in a larger cohort of patients is required to corroborate these results; however our results suggest that an isolated positive posterior margin should not be considered to have had a R1 resection.
0-64 DIAGNOSIS OF PANCREATICOBILIARY MALIGNANCY BY DETECTION OF MINICHROMOSOME MAINTENANCE PROTEIN 5 IN BILIARY BRUSH CYTOLOGY SPECIMENS
1L. Ayaru, 2K. Stoeber, 3G. J. Webster, 3A. R. W. Hatfield, 2A. Wollenschlaeger, 2G. Williams, 1S. P. Pereira. 1Institute of Hepatology, University College London, UK, 2Wolfson Institute for Biomedical Research, University College London, UK, 3Department of Gastroenterology, University College London NHS Trust, London, UK
Introduction: Minichromosome maintenance proteins (Mcm 2–7) are DNA replication licensing factors which can be utilised as biomarkers to detect proliferating cells as well as cells with growth potential.1 Biliary brush cytology is a standard method of detecting malignancy in biliary strictures, but has a diagnostic yield of only 20–50%. We have recently shown that Mcm proteins are dysregulated in pancreaticobiliary malignancy and the detection of Mcm 5 in bile is a significantly more sensitive (66% vs 20%) and accurate (80% vs 60%) marker of malignancy than routine brush cytology.2 Since the cellularity of brush cytology is much greater than bile aspirates, we hypothesised that cells derived from brush cytology specimens may further improve the accuracy of the Mcm 5 test.
Aims and Methods: To determine if Mcm proteins detected in brush cytology specimens is a sensitive marker of malignancy. Brush cytology specimens were collected prospectively from 20 consecutive patients (mean age 63 years, range 46–87 years; M: F 1:1) with biliary strictures. Biliary Mcm5 levels were analysed in a blinded fashion using monoclonal anti-human Mcm5 antibodies in an automated immunofluorometric assay. A diagnosis of malignancy was made by positive cytology/biopsy, or evidence of disease progression on imaging. Benign disease was confirmed by negative pathology during a minimum of 12 months follow-up.
Results: Among the 20 patients, 13 (65%) had malignant disease: pancreatic cancer (n = 9), cholangiocarcinoma (n = 4). Benign strictures (n = 7) were attributed to gallstone disease (n = 2), primary sclerosing cholangitis (n = 2), or other conditions (n = 3). The level of Mcm 5 protein in brush cytology specimens from malignant strictures (median 10600 range 5040–25600) was significantly higher than that from benign strictures (median 3960 range 1930–8920), p<0.005. At a cut off point of >5000 the Mcm 5 test had a sensitivity of 100%, specificity of 75% and accuracy of 89% for the detection of malignancy.
Conclusion: These data suggest that the detection of Mcm5 in biliary brush cytology specimens may provide an exceptionally high sensitivity for the detection of malignancy. We aim to test this in a larger group of patients, including high risk groups such as chronic pancreatitis and primary sclerosing cholangitis, as part of a multicentre study.
Colorectal/anorectal free papers
0-65 ROLE OF PROTON PUMP INHIBITORS ON SEVERITY AND OUTCOME OF CLOSTRIDIUM DIFFICILE ASSOCIATED DISEASE
A. Aravinthan, M. Nikolić, Y. M. Lee. Gastroenterology, Addenbrooke’s Hospital, Cambridge University Hospitals NHS Foundation Trust, Cambridge, UK
Introduction: Role of gastric acid suppressant as a risk factor for Clostridium difficile is unclear. Few reports suggest that proton pump inhibitors (PPI) contribute to an apparent increase in C. difficile-associated disease (CDAD) rates. Nevertheless, the effect of PPI on the severity of CDAD has not been addressed in the literature.
Aims and Methods: The aim of the study was to determine if PPI therapy is associated with the severity or the outcome of the CDAD. We conducted a retrospective study of 305 patients diagnosed with CDAD in a tertiary hospital between 1 April 2007 and 31 March 2008. 10 patients who were treated with H2 receptor antagonists were excluded from this study. Severity scoring system was devised for this study based on the presence of white cell count >15 or <4×109/l, albumin <25 g/l, haemoglobin <10 g/dl, C-reactive protein >200 mg/dl, evidence of dilatation or perforation by X-ray or computed tomography. One point each was given for each parameter. Patients were classified into a mild to moderate disease group if the score was <4 or a severe disease group if the score was ⩾4. Outcome of these patients were assessed using duration of diarrhoea, requirement of treatment escalation (intensive care or high dependency unit management), immunoglobulin treatment, colectomy, CDAD-related deaths and recurrence.
Results: Among 295 patients, 164 patients received PPI therapy. Baseline demographic characteristics were similar in both groups. The majority of patients were females and the mean age was above 70 years. There were significantly greater number of patients with severe disease score in the PPI therapy group (p = 0.004). There were no significant differences between the two groups in the duration of diarrhoea, requirement of treatment escalation (intensive care or high dependency unit management), immunoglobulin treatment, colectomy, CDAD-related deaths, and recurrence (see table).
Conclusion: Our study results show a strong association between CDAD disease severity and the use of PPI. This supports the discontinuation of PPI during CDAD. Further prospective studies are required to validate the severity scoring system and the role of PPI therapy in the outcome of CDAD.
0-66 MORTALITY IN 3 COHORTS OF PATIENTS WITH CLOSTRIDIUM DIFFICILE – IMPLICATIONS FOR IMPROVING OUTCOME
1C. A. Lamb, 1E. I. M. Lamb, 2J. Sarma, 2G. Idle, 1M. Welfare. 1Gastroenterology, Northumbria Healthcare NHS Foundation Trust, North Shields, UK, 2Microbiology, Northumbria Healthcare NHS Foundation Trust, North Shields, UK
Introduction: Clostridium difficile associated diarrhoea (CDAD) is an important cause of morbidity and mortality in hospitalised patients, especially in elderly patients with co-morbid illness. Little data exist on absolute and attributable mortality following diagnosis of CDAD.
Aims and Methods: We explored the distribution of deaths following a diagnosis of CDAD in our community. An initial cohort of all patients diagnosed with CDAD in our NHS Trust from 1st October to 31st December 2006 were identified and followed up for one year. Time elapsed between diagnosis and death was the main end-point measured. We then went on to examine the mortality in another two cohorts to validate the findings in the first cohort.
Results: In the first cohort there were 105 patients, (44 male, 61 female), median age 83 years (range 67–104 years). The distribution of deaths is shown in the table. The second cohort contained all patients diagnosed with CDAD in our Trust from 1st January to 31st March 2007. There were 96 patients in total. Their mortality at 30 days was lower (25%) but the proportion of deaths that occurred before day 15 was similar to cohort 1. 15 of the 24 patients (62%) who died in the first month were dead by day 15. The third cohort contained all patients diagnosed with CDAD in our Trust from 1st June to 30th November 2007. There were 151 patients with an overall 30 day mortality of 37% ranging between 32% and 46% per calendar month (June 40%, July 46%, August 32%, September 32%, October 33%, November 39%).
Conclusion: Evidence from these three cohorts shows that CDAD is associated with high early mortality, varying between 25% and 42% at 30 days in each of the three cohorts that we examined with 60–70% of these deaths occurring before 15 days. After the first 30 days the mortality in the subsequent 11 months is low, suggesting that this cohort of patients have good prognosis if they survive the episode of CDAD. Our conclusion is that successful attempts to reduce mortality from CDAD will have to be introduced before day 14 in the acute illness.
0-67 INTRAVENOUS IMMUNOGLOBULIN FOR THE TREATMENT OF CLOSTRIDIUM DIFFICILE ASSOCIATED DIARRHOEA – EXPERIENCE AT A UK TEACHING HOSPITAL
1N. Prasad, 2J. Lilleker, 2M. Cullen, 1J. Ramesh. 1Gastroenterology, University Hospital of South Manchester, Manchester, UK, 2Microbiology, University Hospital of South Manchester, Manchester, UK
Introduction: Clostridium difficile associated diarrhoea (CDAD) is the most common cause of nosocomial diarrhoea worldwide. Recent epidemiology suggests increasing incidence in the UK with a 50-fold rise since 1990. Mortality has also risen due to the emergence of hypervirulent strains, particularly in the elderly. A poor IgG response to CD Toxin A has been shown to cause severe and recurrent CDAD. This led to the use of intravenous immunoglobulin (IVIG) for the treatment of CDAD but there is a relative paucity of evidence for its effectiveness in the literature.
Aims and Methods: We present our experience of using IVIG in the management of C. difficile associated diarrhoea. Twelve patients were treated with IVIG for CDAD between Jan 2007 and March 2008. Data were collected by retrospective review of medical notes. Patients were classified by disease pattern (recurrent, primary refractory and secondary refractory) as well as by a severity score based on age, WBC, albumin, temperature, creatinine rise, lactate and the presence of ileus.
Results: There were six (50%) male patients and the mean age was 78.4 years (range 55–89). All patients had recent exposure to antibiotics and at least one chronic medical condition. 64% were taking a proton pump inhibitor. 73% were identified to have severe disease (median score 4, range 1–7) and 64% had ileus with fulminant colitis. There were five patients (45%) in each of the recurrent and primary refractory CDAD groups, while one patient (10%) had secondary refractory disease. Patients were treated with standard therapy (metronidazole ± vancomycin) for a mean of 22.8 days (range 4–42) prior to receiving IVIG. 400 mg/kg of Vigam® was administered on three consecutive days to the entire cohort. Two patients received a second course of IVIG, one for partial response and the other for recurrent disease. Overall, 64% responded with complete resolution of diarrhoea after a mean of 7.3 days (range 2–18). In total, mortality was 42% at 30 days with deaths occurring after a mean of 12.5 days (range 1–27). There were three (60%) deaths in the recurrent CDAD group and one (20%) death in the primary refractory group. The single patient with secondary refractory CDAD died. Mortality was associated with a higher severity score (5.25 vs 2.89, p = 0.004). All patients who survived the initial period also survived to the limit of follow up (up to 13 months) with no further recurrences.
Conclusion: IVIG is effective in the treatment of severe CDAD. However, this is a very sick cohort of patents who have a high mortality and careful selection of patients is essential. We would advocate the use of IVIG for selected cases of CDAD when surgery is not possible and all other treatment options have been exhausted.
0-68 HIGH PREVALENCE OF SERRATED POLYPS IN PATIENTS UNDERGOING COLONOSCOPY: A PROSPECTIVE STUDY
1A. Buda, 1E. Zabeo, 2M. De Bona, 3R. Barbazza, 4P. Piselli, 2A. Bellumat, 2F. Valiante, 1G. Sturniolo, 5M. Pignatelli, 2M. De Boni. 1Surgical and Gastroenterological Sciences, University of Padova, Padova, Italy, 2Gastroenterology Unit, S. Maria del Prato Hospital, Feltre, Italy, 3Pathology Unit, S. Maria del Prato Hospital, Feltre, Italy, 4Epidemiology, IRCSS L. Spallanzani, Roma, Italy, 5Pathology, University of Bristol, Bristol, UK
Introduction: A growing body of evidence indicates that serrated polyps (SP) have a substantial risk for subsequent malignancy and the serrated pathway colorectal tumorigenesis is recognised as an alternative to the adenoma-carcinoma sequence. SP include sessile serrated adenomas (SSA) and traditional serrated adenomas (TSA). However, the overall impact of SA on colorectal cancer is uncertain because the true prevalence is unknown.
Aims and Methods: The aim of this study was to determine the prevalence, characteristics of SP in a prospective series of patients. A consecutive series of patients age >50 years undergoing colonoscopy over 18-month period was studied. Asymptomatic patients with positive FOBT+ or subjects at first colonoscopy for different clinical indications were included. Only patients without history of colorectal cancer (CRC) or adenomas, inflammatory bowel disease were enrolled. All colonoscopies were performed with white light conventional endoscopes, the mean withdrawal time was 11.4 min and the caecum was reached in 94% of cases. For purposes of the analysis, the junction of the splenic flexure and the descending colon, as determined by the endoscopist, defined the border between the proximal and the distal colon. All retrieved polyps were examined by 2 independent pathologists (RB, MP) and SP classified using the system described by Torlakovich et al.1
Results: Among 2036 patients included (48.9% M, mean age 59.3±6 years, and 51.1% F, mean age 60.1±4 years), 707 (34.7%) had polyps. Most were adenomas (68.6%), followed by SA (20.8%, SSA 18%, TSA 2.8%, respectively) and hyperplastic polyps (5.4%). SSA were less than 5 mm in 81.5% of cases (p<0.001) and mostly located in the distal colon (88%, p<0.001). TSA were more prevalent in distal colon (77.8%, p<0.001) and the size was less than 5 mm in 78.3% of cases. SP were significantly associated with adenomas (p<0.001). The presence of at least one SSA but not TSA was associated with malignant polyp (p<0.001) and colorectal cancer (p<0.010). The prevalence of SA was significantly higher in the FOBT+ group compared to symptomatic consecutive patients (11.8% vs 5.4%, p<0.0001).
Conclusion: In our series SP prevalence was higher than previously described, particularly in the asymptomatic screening subgroup with FOBT+ (11.8%) and associated with adenomas. SSA were flat, small (<5 mm) and significantly associated with malignant polyp burden and CRC. Because of their potential for malignant transformation, SSA should be identified and completely removed.
0-69 COMPARISON OF ANATOMICAL AND STAGE DISTRIBUTION IN SYMPTOMATIC AND SCREEN DETECTED COLORECTAL CANCERS
1I. Kostourou, 2G. Libby, 3F. A. Carey, 1R. J. C. Steele. 1Surgery and Molecular Oncology, Ninewells Hospital and Medical School, Dundee, UK, 2Scottish Bowel Screening Centre, 3Pathology, Ninewells Hospital and Medical School, Dundee, UK
Introduction:Although screening is known to improve Dukes stage at diagnosis in colorectal cancer, little is known about the effect on T stage, anatomical distribution or the interaction between stage and anatomical site.
Aims and Methods: The study comprised patients diagnosed with colorectal cancer (CRC) in Tayside, Scotland between March 2000 and September 2007. Data came from the CRC database held at Ninewells Hospital. Patients with FOBT screen detected cancers (SCR) were identified from the Scottish Bowel Screening Pilot Study and were then electronically linked to the cancer database by a unique patient identifier. Patients not identified as screen detected were deemed to be symptomatic (SYM). The age range of SYM patients was limited to that of subjects who had been invited for bowel screening (50–69 years).
Results: There were 437 (60.2% males) SYM and 187 (64.7% males) SCR patients. As expected, there was a significant difference in stage distribution with 83 (19.0%) of the SYM group compared with 77 (41.6%) of the SCR group diagnosed at Dukes A (p<0.0001). By the end of the study period 115 (26.3%) of the SYM group had died from CRC compared to 25 (13.4%) of the SCR group (P<0.0001). Within all three Dukes stages there were significant differences in the T stage distribution in the two groups with consistently more favourable distributions for the SCR group (all p<0.04). In Dukes A 40.9% were staged as T1 and 59% as T2 in the SYM group compared to 58.4% and 41.6% in SCR group. Within Dukes B 90.6% were stage T3 and 9.4% as T4 in the SCR group compared to 77.3% and 22.7% in the SYM group. Within Dukes C a similarly favourable shift in the T stage was seen in the SCR group. When anatomical site was examined there was a significant difference (p = 0.02) in the anatomical distribution of cancers in the two groups with a preponderance of left colon tumours in the SCR group at the expense of right colonic and rectal tumours. When the stage distribution in the different anatomical sites was scrutinised the proportion of Stage A cancers in the right colon, left colon and rectum was 6.6%, 20.6% and 26.6% respectively compared with 24.3%, 43.8% and 50% respectively for the SCR group.
Conclusion: In this cohort of patients defined by age and geographical location, it was found that Dukes staging may be misleading is assessing screen detected cancers as they had a more favourable T stage distribution within each Dukes stage. In addition, screening appeared to slightly underdiagnose right sided and rectal cancers, and although stage at presentation improved from the right colon to the rectum in the symptomatic cancers this was mirrored by significantly better stage distributions in all anatomical sites in the screen detected group.
0-70 CONSENTING FOR COLORECTAL CANCER SCREENING – DOES PROVISION OF NUMERICAL DATA AND PICTOGRAPHS ON BENEFIT AND RISK DIMINISH UPTAKE?
I. Patanwala, V. Brocklebank, P. N. Trewby. Gastroenterology, Memorial Hospital, Darlington, UK
Introduction: Information given to patients invited for bowel cancer screening in the UK is descriptive and gives little numerical information on individual benefit or risk.1 Although the screening figures are impressive in the context of population benefit, it is the individual, not the population, that decides whether to be screened. Graphical displays of information increase the effectiveness of risk communication, but understanding numerical information is difficult. To allow true informed consent, information must be tailored to the individual.
Aims and Methods: We aimed to clarify: if presenting numerical facts including absolute risks and benefits affected uptake of bowel cancer screening; if pictorial representation of data affected the uptake and understanding of the risks and benefits of colorectal cancer (CRC) screening; and, which of the many established facts concerning screening might incline individuals more towards accepting screening. We gave 239 subjects (Group 1) an enhanced information pack containing numerical information expressed pictorially, including numbers needed to screen to accrue benefit (862); cancers missed by screening (50%); effect on survival (none); numbers of CRC prevented by earlier polyp pick up (0.5% at 18 years). We asked, on the basis of information presented, whether subjects wished to be screened and the points most influencing their decision and compared responses to a matched group of 239 subjects (Group 2) sent the standard NHS pack. We asked if pictorial representation of data on risks and benefits had an impact on their decision to be screened or not and if patients found them useful in making an informed decision.
Results: 53% replied, of whom 85% in group 1 and 90% in group 2 wished to be screened. The use of pictographs with incorporated numerical data significantly informed decision making (p = 0.0127, two sided Fisher exact test). This significance persisted when data were shown numerically without the aid of a pictogram (p = 0.039, two sided Fisher exact test). Those wanting to be screened found the statement “bowel cancer is the second commonest cause of death” had the highest impact. For those in group 1 not wanting to be screened the statement “the programme will miss 50% of cancers” had the highest negative impact. 83% of the respondents in the intervention group found the numerical data helpful and 61% felt that the pictograms helped understand these data better.
Conclusion: Providing numerical information did not diminish overall uptake of screening in this hypothetical study but did help informed decision making. For this reason, and to allay future concerns about adequacy of informed consent, numerical data should be included in information packs. Pictograms may be useful adjuncts to help patients better understand numerical data explaining risk and benefit.
0-71 CIRCULATING GALACTOSIDE-BINDING GALECTINS ARE INCREASED IN COLORECTAL CANCER PATIENTS, PROMOTE CANCER CELL ADHESION TO HUVEC AND MAY HAVE AN IMPORTANT ROLE IN CANCER METASTASIS
H. Barrow, J. M. Rhodes, L. G. Yu. Gastroenterology Research Unit, University of Liverpool, Liverpool, UK
Introduction: Galectins are a family of 15 mammalian galactoside-binding proteins that are expressed in many cell types intracellularly, extracellularly and sometimes in the circulation. Circulating galectin-3 increases up to 5-fold in patients with colon cancer and increased circulating galectin-3 concentrations are closely correlated with metastasis. Recently we have demonstrated that recombinant galectin-3 at pathological concentrations increases colon cancer cell adhesion to endothelium,1 indicating a potential role of circulating galectin-3 in promoting haematogenous dissemination of cancer cells to remote sites.
Aims and Methods: To assess the circulation and role of other members of the galectin family as potential mediators of colorectal cancer metastasis. Galectin 1, -2, -3, -7 and -8 concentrations were analysed by ELISA in the sera of 20 colorectal cancer patients without known metastasis and 11 with liver metastasis and 31 healthy people. Recombinant galectins 1, 2, 3, 7 and 8 were then tested for their effect on colon cancer HT29-5F7 cell adhesion to human umbilical vein endothelial cell monolayers (HUVECs).
Results: The concentrations of galectin-1, -2, -3 and -8 were not significantly increased in patients without metastasis but significantly increased up to 3-fold (169.2–13834.1 ng/ml, p = 0.009), 2-fold (13.3–1155.8 ng/ml, p = 0.002), 31-fold (30.9–5106 ng/ml, p<0.001) and 6-fold (2.4–223.1 ng/ml, p = 0.0048), respectively, in patients with liver metastasis. Introduction of recombinant galectin-1, -2, -3, -7 and -8 at pathological concentrations (0.25–1.0 μg/ml) to HT29-5F7 colon cancer cells resulted in dose-dependent increases of the cell adhesion to HUVEC monolayer. An increase of 294±12% (mean±SE, p<0.0001,), 217±10% (p<0.0001), 236±14% (p<0.0001), 320±7% (p<0.0001), and 255±20% (p<0.0001) was induced by recombinant galectin-1, 2-, -3, -7 and -8 respectively, all at 1.0 μg/ml, and these effects were largely abolished by pre-incubation of the galectins with galectin-binding lactose (20 μm) or asialo-fetuin (20 μg/ml).
Conclusion: These results indicate that the increased circulation of members of the galectin family may play an important role in promoting metastasis by increasing cancer cell adhesion to blood vasal endothelium. And such galectin-cancer cell interaction in the blood circulation therefore represents a novel therapeutic target for metastasis prevention.
0-72 DOES THE LOCATION OF SCREEN DETECTED CANCERS DIFFER FROM THAT SEEN IN THE UNSCREENED POPULATION?
C. Harmston, J. Hunter, L. Wong. Surgery, University Hospital Coventry, Coventry, UK
Introduction: The UK bowel cancer screening pilots have recently ended. It is important that screening detects cancers regardless of their location within the colon. The aim of this study was to see if the location of cancers detected by the pilot screening program differed from that of unscreened cancers.
Aims and Methods: The colorectal cancer dataset of University Hospital Coventry was analysed retrospectively. A seven year period was used to include all three rounds of the pilot screening. Two groups of patients were selected, those with colorectal cancers detected by the pilot screening programme and those detected outside of screening. Tumour location was categorised and the two groups were compared for statistical significance using χ2 test.
Results: 1490 patients were included, 100 of which were in the screened population and 1390 were in the unscreened population. Location of cancers in both groups is outlined in the table. There was no significant difference in tumour location between the two groups with a p-value of 0.49.
Conclusion: This study has shown that screen detected cancers do not differ in their location from unscreened cancers and suggests that FOBt screening detects cancer irrespective of location within the colon.
0-73 OMEGA-3 POLYUNSATURATED FATTY ACID-DERIVED PROSTAGLANDIN E3 ANTAGONISES PROSTAGLANDIN E2-EP4 RECEPTOR SIGNALLING IN HUMAN COLORECTAL CANCER CELLS
G. Hawcroft, L. Bretsztajn, M. A. Hull. Section of Molecular Gastroenterology, Leeds Institute of Molecular Medicine, Leeds, UK
Introduction: One possible mechanism of the anti-colorectal cancer (CRC) activity of omega-3 polyunsaturated fatty acids (PUFAs) such as eicosapentaenoic acid (EPA) is reduced cyclooxygenase (COX)-dependent prostaglandin (PG) E2 production with a concomitant switch to synthesis of PGE3. However, it is currently not known whether PGE3 can act directly on human CRC cells. We have previously implicated the EP4 receptor in the pro-tumorigenic activity of PGE2 on human CRC cells (Oncogene 2007;26:3006–19). Therefore, we tested the hypothesis that PGE3 antagonises PGE2-EP4 receptor signalling in human CRC cells.
Aims and Methods: Stably transfected EP4 receptor-expressing HT-29 (termed HT-29-EP4) and EP4 receptor-positive LoVo human CRC cells were treated with exogenous PGE2 and PGE3, with or without the selective EP4 receptor antagonist ONO-AE3-208. Immunofluorescence for V5-tagged or untagged EP4 was used to determine ligand-induced EP4 receptor internalisation.
Results: PGE3 induced an EP4 receptor-dependent elevation of intracellular cAMP levels in both HT-29-EP4 and LoVo cells. However, PGE3-induced EP4 receptor activation was less efficient than for PGE2. PGE3 also induced EP4 receptor internalisation. Importantly, co-administration of an equimolar concentration of PGE3 antagonised EP4 activation by PGE2.
Conclusion: PGE3 is a partial agonist at the EP4 receptor in human CRC cells. Therefore, direct activity of PGE3 on human CRC cells may contribute to the anti-CRC activity of omega-3 PUFAs in combination with a reduction in COX-dependent PGE2 synthesis. Evidence from in vitro cell experiments and mouse models suggests that EPA administration leads to PGE3 synthesis. Our data should prompt clinical studies investigating whether intake of omega-3 PUFAs such as EPA lead to PGE3 synthesis in humans.
0-74 POSITIVE LYMPH NODE RETRIEVAL RATIO OPTIMISES PATIENT STAGING IN COLORECTAL CANCER
S. J. Moug, J. D. Saldanha, J. R. McGregor, M. Balsitis, R. H. Diament. Departments of General Surgery and Pathology, Crosshouse Hospital, Kilmarnock, UK
Introduction: TNM staging system is currently used in the UK to stage colorectal cancer. Other lymph node parameters have been proposed that may result in improved staging. This study aimed to compare one of these alternative parameters, positive lymph node ratio (pLNR),1 with conventional TNM staging in predicting long term survival in patients undergoing curative resection for colorectal cancer.
Aims and Methods: 295 consecutive patients (mean age 70 years; range 39–95; SD 10.4) who underwent curative resection for colorectal cancer in two centres between 2001–2004 were analysed (median follow up 4 years, range 0.1–6.9 years). The following variables were recorded: age, sex, site of primary tumour; TNM stage and neo/adjuvant chemotherapy and/or radiotherapy. Lymph node (LN) parameters analysed were: total number of LN and subsequently, adequate retrieval (⩾12) and inadequate (<12); total number of negative LN; total number of positive LN and the ratio of positive LN to total LN (pLNR). To determine the influence of LN retrieval on long term outcome, univariate and multivariate survival analysis was performed.
Results: The median number of LN retrieved was 10 (1–57) with adequate LN retrieval achieved in 110 cases (37.3%). For each T and N stage, inadequate LN retrieval did not adversely affect long term survival (p>0.05). On univariate analysis, age, site of primary, LN negative, LN positive, pLNR and TNM staging were all significant. On multivariate analysis, only age and pLNR were independent predictors of overall survival (HR 11.6, 95% CI 5.8 to 24.0; p<0.001). Application of pLNR subdivided patients into 4 prognostic groups.
Conclusion: Calculation of the pLNR improved patient stratification in colorectal cancer and has been found to be superior to the current TNM staging system.
Neurogastroenterology/motility free papers
0-75 PHARYNGEAL ELECTRICAL STIMULATION AS AN ADJUNCT TO REHABILITATION OF DYSPHAGIA FOLLOWING STROKE : A RANDOMISED CONTROL TRIAL
1V. Jayasekeran, 1E. Michou, 1S. Singh, 2J. Borrelli, 1S. Mistry, 1S. Jefferson, 1S. Hamdy. 1Gastrointestinal Sciences, University of Manchester, Salford, UK, 2Speech and Language, Leeds Metropolitan University, Leeds, UK
Introduction: Dysphagia in stroke is a common complication with serious consequences including aspiration pneumonia and death. However, current treatment options for dysphagic stroke often lack clinical efficacy. We have previously shown that plasticity in the brain regions controlling swallowing can be enhanced using short durations (10 minutes) of pharyngeal electrical stimulation (PES) in both health and in stroke.1 Furthermore, an observational dose response study identified the optimal parameters for PES in stroke patients.2 We now describe early results in the first placebo controlled randomised study of PES.
Aims and Methods: Stroke patients were recruited prospectively from 2 hospitals within 3 weeks from the onset of their stroke. Dysphagia was determined by videofluoroscopy (VFS) using the validated Penetration-Aspiration (PA) scale. Dysphagic patients were randomly allocated to either the PES or control. PES was delivered via an intraluminal pharyngeal catheter for 10 minutes at 5 Hertz for three consecutive days. The sham group had the catheter for the same duration without current. A follow up VFS was conducted 2 weeks later to determine changes in the PA scores, analysed by investigators blinded to the intervention.
Results: 27 patients out of 51 patients who underwent initial VFS were dysphagic. 20 of the dysphagic patients (average age 75±10 years) completed the protocol. 12 patients were randomised to the real treatment group, and 8 to the sham group. In the active PES group cumulative PA scores reduced by 28% whilst in sham group it increased by 15%. Compared to baseline, the reduction in penetration and aspiration was only significant in the PES group (p = 0.0384, paired t-test), being unchanged in the sham group (see figure). Patients who received PES also had significantly greater reductions in absolute numbers of unsafe swallows compared to sham (25% vs 4.16%).
Conclusion: Pharyngeal electrical stimulation in dysphagic stroke significantly reduces penetration-aspiration scores. This study provides further evidence that PES may be useful in expediting the recovery of dysphagia in acute stroke.
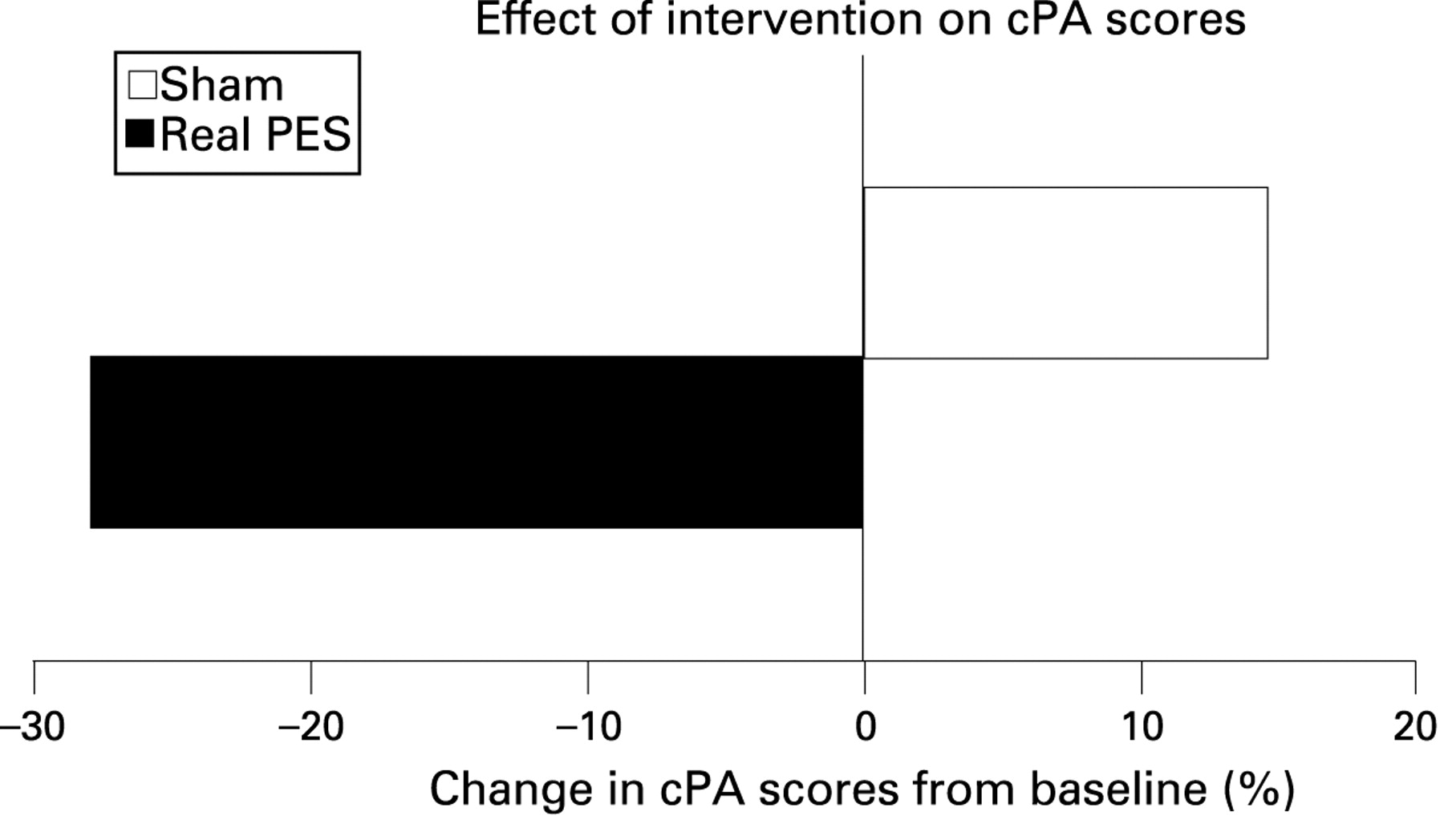
0-76 NEUROTICISM PREDICTS AUTONOMIC NERVOUS SYSTEM AND HYPOTHALAMIC PITUITARY ADRENAL AXIS RESPONSES TO SOMATIC AND VISCERAL PAIN
A. D. Farmer, M. Shwahdi, J. Kishor, M. Kano, S. J. Coen, Q. Aziz. Wingate Institute of Neurogastroenterology, Barts and the London, School of Medicine and Dentistry, London, UK
Introduction: Pain is a complex phenomenon involving sensory-discriminative, affective-motivational and cognitive-evaluative processes. Visceral pain is a characteristic feature of many of the functional gastrointestinal disorders (FGIDs) which are more common in neurotic individuals. Recently, a link between personality constructs, brain stem mediated autonomic nervous system (ANS) responses and the hypothalamic pituitary adrenal (HPA) axis has been suggested. Data collated from human and animal studies suggest that the parasympathetic nervous system (PNS) is predominantly anti-nociceptive.1 However, there is a paucity of data examining the link between personality traits, PNS and HPA axis responses to pain.
Aims and Methods: We aimed to investigate whether personality traits can predict ANS and HPA axis responses to pain. 50 healthy subjects (26 males, median age 32.2 years age range 22–53 years) had personality traits assessed using the validated Big-Five Inventory. Subjects had the validated PNS parameters of cardiac vagal tone (CVT) and cardiac sensitivity to the baroreflex (CSB) measured continuously throughout the study. Following baseline ANS recordings, subjects were intubated with a naso-oesophageal balloon catheter positioned in the mid oesophagus. Subjects were randomised to receive visceral followed by somatic pain, or vice versa, and asked to rate pain intensity and unpleasantness on a verbal rating scale. Seven painful visceral stimuli were administered, by oesophageal distension through inflation of the oesophageal balloon, to the subject’s pain tolerance with an inter-stimulus interval of 2-minutes. Seven painful somatic stimuli, using nail bed pressure with a 2-minute inter-stimulus interval, were administered to the subject’s pain tolerance. Cortisol was measured at baseline, 5 minutes post visceral and 5 minutes post somatic stimulation.
Results: Baseline CVT and CSB correlated negatively with neuroticism (r = −0.6, p = <0.0001 and r = −0.4, p = 0.01 respectively). Baseline CVT and CSB correlated with CVT (r = 0.86, p<0.0001 and r = 0.7, p<0.0001) and CSB (r = 0.8, p<0.0001 and r = 0.62, p<0.0001) response to somatic and visceral pain. Subjects rated visceral pain as more unpleasant (p<0.0001), but not more intense, than somatic pain. Neuroticism correlated with baseline cortisol levels and also to cortisol levels following somatic and visceral pain stimuli (r = 0.35, p = 0.01 and r = 0.37, p = 0.008 and r = 0.38, p = 0.006).
Conclusion: These results demonstrate that the personality construct of neuroticism can predict baseline PNS and HPA tone and responses to somatic and visceral pain. Neuroticism, cortisol levels and PNS measures may represent clinically applicable biomarkers for pain responsiveness in health. These findings warrant further assessment in a larger cohort of healthy volunteers and in those with FGIDs.
0-77 ELEVATED CHEMOKINE MRNA IN RECTAL MUCOSA IN IRRITABLE BOWEL SYNDROME; INCREASED BY GASTROINTESTINAL INFECTION BUT UNRELATED TO GUT PERMEABILITY
1R. C. Spiller, 1E. Campbell, 1M. Richards, 1K. Garsed, 1A. Zaitoun, 2M. Hastings, 1Y. Mahida, 3I. Hall, 1K. Neal, 4J. Cox, 4F. Kelly, 4J. Wilde, 4G. Dukes, 2P. Whorwell. 1Nottingham Digestive Diseases Centre BRU, University of Nottingham, Nottingham, UK, 2Department of Gastroenterology, University of South Manchester, Wythenshawe Hospital, Manchester, UK, 3Department of Therapeutics and Molecular Medicine, University of Nottingham, Nottingham, UK, 4Discovery Technology Group, Molecular Discovery Research, GSK, Harlow, UK
Introduction: Previous studies have suggested inflammatory changes in colonic mucosa peripheral blood mononuclear cells (PBMC) in irritable bowel syndrome (IBS) patients with diarrhoea (IBS-D). We have previously reported persistent IBS symptoms following C. jejuni enteritis. We hypothesised that genes upregulated by infection may also be upregulated in other subtypes of IBS.
Aims and Methods: 25 healthy volunteers (HV), 31 patients 6 months after C. jejuni infection, 37 IBS-D patients and 19 IBS with constipation (IBS-C) provided stool and blood samples and 24 hour urine collection for measuring gut permeability. Rectal mucosal biopsy mRNA was assessed using an Affymetrix genechip to identify genes whose expression was altered by C. jejuni infection or in IBS. Findings were confirmed using TaqMan RT-PCR and correlated with histology, PBMC cytokine production, gut permeability, bowel and psychological symptoms.
Results: Expression of the chemokines genes CCL11, CCL 13 and Calpain 8 were significantly increased in rectal biopsies 6 months after C. jejuni infection while NR1D1 was decreased (see table). The same changes were also seen in IBS-D and also IBS-C. Gut permeability, mucosal mast cells and PMBC production of TNF-alpha and IL6 were significantly elevated 6 months following C. jejuni infection. Individuals with persistent bowel dysfunction had higher mast cell numbers but otherwise showed no differences in mucosal mRNA nor PBMC cytokine production from those who recovered completely, though they were more likely to have rectal bleeding. PI-BD patients were also more likely to be female, younger and have significantly higher PHQ12, anxiety and depression scores than PI-non-IBS. Overall PBMC TNF, IL10 and IL1-beta production correlated closely (r = 0.8–0.90) but none correlated with gut permeability. TNF showed a weak correlation with days per week with loose stool, r = 0.24, p<0.05. Stool cytokines, plasma CRP and urine neopterin showed no group differences.
Conclusion: Mucosal expression of proinflammatory chemokines genes, mast cell numbers and PBMC cytokine production are elevated 6 months following C. jejuni infection. Similar increased chemokine mRNA and PCMC cytokine production are also seen in IBS patients regardless of subtype.
0-78 SOUP MEAL DELAYS GASTRIC EMPTYING, ENHANCES GALLBLADDER CONTRACTION AND INCREASES SMALL BOWEL WATER CONTENT AND SATIETY COMPARED TO EQUICALORIC MIXED SOLID/LIQUID MEAL
1L. Marciani, 1N. Hall, 2S. E. Pritchard, 3J. J. Totman, 2C. L. Hoad, 2P. A. Gowland, 1R. C. Spiller. 1Nottingham Digestive Diseases Centre Biomedical Research Unit, Nottingham University Hospitals, Nottingham, UK, 2Sir Peter Mansfield Magnetic Resonance Centre, Nottingham, UK, 3Brain and Body Centre, University of Nottingham, Nottingham, UK
Introduction: There is currently great interest in manipulating the physical form of food to enhance satiety. The stomach can “sieve” water from the solid component of a meal leading to faster gastric emptying. We hypothesised that if sieving was prevented by blending a solid/liquid meal to a soup: (a) gastric volumes would fall more slowly; (b) satiety would be enhanced; (c) the CCK duodenal response (as inferred from gallbladder contraction)1 would be enhanced; and (d) the small bowel secretion would be greater.
Aims and Methods: To investigate how blending a solid/liquid meal to a soup affects satiety, gastric emptying, gallbladder contraction and small bowel gastric content. Satiety study 1: 22 healthy volunteers attended in the morning, having fasted overnight and were fed either a roasted chicken and vegetables meal with a glass of water (241 kcal) or the same meal and water blended to a soup. The volunteers were asked to fill in satiety questionnaires fasting and at intervals for 3 hours postprandially. Mechanistic study 2: 18 healthy volunteers attended in the morning, having fasted overnight, and were scanned in a 1.5T MRI scanner. They were then fed the same meals as above and underwent scanning at intervals for 3 hours. Gastric contents and gallbladder contraction were measured from the abdominal volume scans. Small bowel water content was measured from magnetic resonance cholangiopancreatography (MRCP) scans, as previously described, and validated by intubation studies in which measured values were shown to closely parallel infused volumes.2 Two-way analysis of variance and paired comparisons were used.
Results: (mean±SEM) Study 1: The soup meal induced lower feelings of hunger (p<0.02). Study 2: Gastric volumes were greater after the soup than solid meal at 30 min (360±15 ml vs 265±8 ml respectively, p<0.0003) and 75 min (198±10 ml vs 256±22 ml, p = 0.02). The % gallbladder contraction was greater after the soup meal at 30 min (58±2% vs 48±2%, p = 0.0002) and 75 min (44±2% vs 32±2%, p<0.0001). Small bowel water content was initially higher for the solid meal (111±15 ml vs 70±8 ml immediately after feeding, p<0.02) whilst the soup meal induced greater secretion at later times (186±23 vs 124±16 ml at 165 min, p<0.007).
Conclusion: Blending the test meal to a soup abolished gastric “sieving” resulting in larger gastric volumes and enhanced gallbladder contraction, a marker of CCK release.1 The small bowel water content was higher for the soup meal at the later time points, implying that the latter induced greater secretory stimulation. These combined gastrointestinal factors induced an enhanced satiety after the soup meal. MRI provided exquisite insights into the functional gastrointestinal response to altered physical form of meals.
0-79 AN “INSIGHT” INTO DIABETIC GASTROENTEROPATHY USING CORNEAL CONFOCAL MICROSCOPY
1P. Begum, 2M. Tavakoli, 2R. A. Malik, 1J. McLaughlin. 1GI Sciences, University of Manchester, Salford, Manchester, UK, 2Cardiovascular & Endocrine Sciences, University of Manchester, Manchester, UK
Introduction: Diabetes causing autonomic dysfunction is associated with various gastrointestinal (GI) motility disorders such as gastroparesis and diabetic diarrhoea (diabetic gastroenteropathy, DGE). However, symptoms are often poorly predictive of motor abnormalities and vice-versa, despite underlying diabetic autonomic neuropathy (DAN). Accurate quantification of the severity of DAN remains time consuming and challenging, but corneal confocal microscopy (CCM) is a novel, non-invasive technique which quantifies small C-nerve fibre pathology.
Aims and Methods: This study aimed to determine whether corneal C-fibre status would mirror DAN in diabetic patients with gastrointestinal (GI) symptoms. Twenty diabetic subjects (14 Type 1, 6 Type 2) with symptoms of gastroparesis and/or diarrhoea, and 14 control subjects underwent cardiovascular autonomic profiling using the Composite Autonomic Scoring Scale (CASS). The severity of gastroparesis was evaluated using the Gastroparesis Cardinal Symptom Index (GCSI), whilst nuclear scintigraphy or the 13C-sodium acetate breath test determined gastric emptying. Corneal nerve morphology was quantified using CCM and corneal aesthesiometry assessed Corneal Sensitivity (CS). All data are expressed as mean ± SD.
Results: DAN was seen in 18/20 diabetic subjects. The severity by CASS was moderate-severe in 12 and mild in 6 patients (mean CASS 4.0±2.2). The severity of gastroparesis was also moderate (mean GCSI 2.3±1.0), yet gastric emptying studies confirmed delay in only 10/18 (56%) subjects (mean GCSI 2.4±1.1; CASS 4.6±1.8). Rapid emptying/dysmotility was seen in 3 subjects (GCSI 2.9±0.9; CASS 1.7±2.1), whilst 5 patients had normal emptying (GCSI 1.7±0.5; CASS 5.0±1.6). Correlation of CASS vs GCSI was poor (r = −0.3; p = 0.254). Corneal nerve fibre density (NFD, 17.8±13.3 vs 48.3±12.4), nerve branch density (NBD, 8.9±7.9 vs 30.1±5.3) and nerve fibre length (NFL, 3.6±3.1 vs 9.7±2.5) were all significantly reduced in diabetics vs controls (p<0.0001). CS was also reduced with significant elevation of corneal sensory thresholds (1.6±0.9 vs 0.7±0.2; p<0.0004). All abnormalities were reduced in proportion to the severity of DAN, with highly significant correlations (p<0.0001) between CASS and NFD (r = −0.713), NBD (r = −0.726), NFL (r = −0.786) and CS (r = 0.659).
Conclusion: In patients with DGE, DAN was common. GI symptoms were not necessarily reflective of motor dysfunction, nor representative of the severity of underlying neuropathy. Corneal nerve morphology was also abnormal in these patients compared with healthy controls and the severity of nerve damage was very strongly associated with the severity of autonomic neuropathy. This suggests that CCM may be a useful rapid, simple and non-invasive diagnostic marker of DAN or indeed DGE.
Supported by Diabetes UK/CORE
Oesophageal free papers
0-80 GENERATION AND VALIDATION OF A PROGNOSTIC GENE SIGNATURE FOR OESOPHAGEAL ADENOCARCINOMA
1C. J. Peters, 2J. R. E. Rees, 3J. S. Hardwick, 3C. Zhan, 4R. H. Hardwick, 1R. C. Fitzgerald. 1MRC Cancer Cell Unit, Hutchison-MRC Research Centre, Cambridge, UK, 2Department of Surgery, Bristol Royal Infirmary, Bristol, UK, 3Molecular Profiling, Merck Research Laboratories, North Wales, USA, 4Cambridge Oesophago-Gastric Centre, Addenbrookes Hospital, Cambridge, UK
Introduction: Oesophageal adenocarcinoma is an increasingly common cancer with a poor prognosis. The incidence has increased more than 6 fold in the last 3 decades and survival at five years remains less than 14%. Complex management decisions and the highly invasive nature of oesophageal surgery mean that patients and clinicians need better prognostic information.
Aims and Methods: This study aims to generate and validate a molecular prognostic signature for oesophageal adenocarcinoma. Snap frozen tumour samples were collected from 91 patients undergoing potentially curative surgery at Bristol Royal Infirmary for oesophageal and junctional adenocarcinoma. Median length of follow-up was 1.7 years for all patients and 7.0 years for patients alive at last follow up. RNA was extracted and hybridised to a 44K 60-mer oligo-microarray. The data were detrended and normalised and the resulting expression correlated with clinical features to derive a molecular prognostic signature. The prognostic signature is being validated at the protein level via immunohistochemistry both internally on the same samples and externally with tissue microarrays from a further 600 cases of adenocarcinoma.
Results: High quality data were obtained from 76 of the tumour samples. Lists of 119 genes associated with survival and 270 genes associated with the number of involved lymph nodes were created. Gene list filtering using statistical and biological criteria produced a short list of the 20 genes most predictive of survival. Combined this list of genes was highly prognostic. Patients with dysregulation of at least 4 of the 20 genes had a median survival of 11.4 months compared with 52.5 months for those with dysregulation of <4 genes (p<0.0001). This prognostic signature outperforms all the clinical indicators in predicting survival in multivariate analysis. To date two genes have been validated internally: PAPPS2- if not expressed median survival is 6.4 months compared with 27.2 months if expressed (p = 0.002); and HEF1- if not expressed median survival 7.8 months compared with 17.0 months if expressed (p = 0.027).
Conclusion: We have determined that a 20 gene expression signature may outperform clinical indicators in predicting outcome. Protein validation is underway with the aim that a combination of a smaller number of genes and the existing clinical staging could dramatically improve our ability to predict survival and allow better targeting of novel treatments.
0-81 PERSONALISING CHEMOTHERAPY TO IMPROVE OESOPHAGO-GASTRIC CANCER OUTCOMES
1A. L. Paterson, 2T. M. Gilmer, 3R. F. Wooster, 1R. C. Fitzgerald. 1MRC Cancer Cell Unit, Hutchison MRC Research Centre, Cambridge, UK, 2Translational Medicine, GlaxoSmithKline, North Carolina, USA, 3Translational Medicine, GlaxoSmithKline, Philadelphia, USA
Introduction: Oesophago-gastric cancers have been identified as a major public health concern due to their increasing incidence and 13% 5-year survival. On average neoadjuvant chemotherapy prior to surgery extends survival by only 4 months. In many tumours constitutively active receptor tyrosine kinases (RTKs) provide necessary growth and survival signals for disease progression. We hypothesise that personalising chemotherapy by profiling a tumour’s RTK proteome and adding targeted agents against key RTKs could dramatically improve patient survival.
Aims and Methods: The activity of 42 different RTKs was profiled using proteome arrays in a cell line panel and snap frozen tumour samples. Cell lines were treated with tyrosine kinase inhibitors (TKIs) targeting RTKs of interest; cell proliferation and apoptosis was quantified after 72 hours and 24 hours, respectively. A dynamic ex vivo assay was developed for tumour samples to predict the potential efficacy of these drugs in vivo.
Results: The constitutive activation of multiple RTKs was commonly seen. In general, one RTK was considerably more active than the others and was selected for inhibition. TKI treatment in cases with FGFR2, PDGFRa, ErbB2 and Met constitutive activity dramatically reduced proliferation and increased the activation of caspases 3 and 7 from 1.5 to 6 fold. TKI treatment of MKN1, which has no constitutively active RTKs, had little effect on proliferation. In OE33 both ErbB2 and Met were strongly active. It was insensitive to lapatinib (a dual EGFR/ErbB2 TKI, TykerbTM, GlaxoSmithKline) and Met TKIs when used separately but was highly sensitive to dual ErbB2 and Met inhibition. The profiling of snap frozen tumour samples demonstrated constitutively phosphorylated RTKs. Fresh tumour samples were then incubated with a TKI targeting RTKs shown to be active. Subsequent western blotting confirmed the ability of the TKI to suppress RTK constitutive phosphorylation; confirming the relevance of the in vitro findings for future patient therapy selection.
Conclusion: Receptor tyrosine kinase profiling reveals key proteomic changes which are valid therapeutic targets. TKI treatment can considerably reduce proliferation and cause substantial cell death. These observations support the concept of individualised therapy in oesophago-gastric carcinomas. RTK profiling of tumours at diagnosis may be one strategy to personalise chemotherapy regimens and increase their efficacy.
0-82 THE EDINBURGH DYSPHAGIA SCORE CORRECTLY IDENTIFIES PATIENTS WITH DYSPHAGIA AND HIGH RISK OF OESOPHAGEAL MALIGNANCY
1E. Rhatigan, 2I. Tyrmpas, 2C. Scott, 3G. Murray, 2J. N. Plevris. 1College of Medicine, University of Edinburgh, Edinburgh, UK, 2Centre for Liver and Digestive Disorders, The Royal Infirmary, University of Edinburgh, Edinburgh, UK, 3Centre for Public Health and Primary Care Research, University of Edinburgh, Edinburgh, UK
Introduction: Dysphagia is an alarm symptom, caused by both benign and malignant pathologies, requiring urgent investigation. We aimed to identify the parameters associated with oesophageal cancer and to develop a simple predictive scoring system that accurately determines which patients with dysphagia are at highest risk of oesophageal cancer; thereby stratifying dysphagia referrals into a higher risk cohort in need of urgent endoscopy and a lower risk cohort on whom endoscopy could be done with less urgency.
Aims and Methods: Clinical data from the complete referral forms of 394 dysphagia patients and the outcome of their subsequent endoscopy was recorded. Univariate analysis (χ2 test and t-test) and then multivariate analysis (Binary logistic regression analysis) were performed to identify parameters independently related with oesophageal cancer. These parameters were then included in the Edinburgh Dysphagia Score (EDS). Its ability to predict malignancy was evaluated and it was validated on a separate dataset of 154 patients.
Results: The EDS was developed from 6 parameters independently associated with oesophageal cancer: age, gender, weight loss, duration of symptoms (less than 6 months), localisation of dysphagia and the absence or presence of acid reflux (see equation below). The EDS stratified the development cohort in which 40 cases of cancer were found, into a high risk group (score > = 3.5), comprising 64.2% of the referrals, and a low risk group (point score = <3) comprising 35.8% (see table). It did this with a sensitivity of 97.5%, and a negative predictive value (NPV) of 99.3%. On validation the EDS divided the cohort into a high risk group (68.8% of referrals) and a lower risk group of 31.2% (see table). It correctly identified all 23 cancer cases as high risk, thereby stratifying the referrals with a sensitivity and NPV of 100%. EDS specificity was 39.5% in the development and 36.6% in the validation cohort.
Conclusion: In the 548 dysphagia referrals the EDS correctly identified 62/63 cancer cases as high risk. Moreover, 188 cases were correctly identified as lower risk and could therefore have been investigated less urgently. Thus, using variables recorded by GPs referring new dysphagia patients, we have developed a simple scoring system that can be used to sensitively select and prioritise dysphagia patients at high risk of malignancy. This will enable better use of endoscopy resources.
EDS calculation: Age group (0–11) + Female gender (Y = −1, N = 0) + Weight loss (Y = 2, N = 0) + Duration of symptoms ⩽6/12 (Y = 0, N = −1.5) + Localisation to neck (Y = −2, N = 0) + Acid reflux (Y = −1, N = 0)
Low risk = score of ⩽3
High risk = score of⩾3.5
0-83 MALE PREDOMINANCE OF UPPER GASTROINTESTINAL ADENOCARCINOMA CANNOT BE EXPLAINED BY DIFFERENCES IN TOBACCO SMOKING IN MEN VERSUS WOMEN
1N. Freedman, 2M. H. Derakhshan, 1C. C. Abnet, 1A. Schatzkin, 1A. R. Hollenbeck, 2K. E. L. McColl. 1Division of Cancer Prevention, National Cancer Institute, Bethesda, USA, 2Division of Medical Sciences, University of Glasgow, Glasgow, UK
Introduction: Adenocarcinomas of the upper gastrointestinal tract show remarkable male predominance that is evident in nearly all populations. Our recent studies demonstrated a 17 year delay in rise of age specific incidence rates of these tumours in women versus men. The aim of the current study is to investigate the role of tobacco smoking in the male predominance of upper gastrointestinal adenocarcinomas.
Aims and Methods: The study used the NIH-AARP Diet and Health Study. Participants (285 962 men and 194 132 women) lived in the USA and responded to a questionnaire about cigarette, pipe, and cigar smoking and other risk factors between 1995 and 1996. Over a median 7.5 years of follow-up, incident gastric and oesophageal cancers were identified by linkage to individual state cancer registries. We calculated age-standardised incidence rates for adenocarcinoma of the oesophagus, the gastric cardia and the gastric non-cardia in men and women separately. We also calculated incidence rates with standardisation for both age and tobacco smoking, number of cigarettes smoked per day and year of cessation for former smokers.
Results: After 2 013 142 person-years follow up, there were 338 new adenocarcinomas of the oesophagus, 261 of the gastric cardia, and 222 of the gastric non-cardia in men. After 1 351 958 person-years follow up, there were 23 new case of adenocarcinoma of the oesophagus, 36 of the gastric cardia, and 88 of the gastric non-cardia in women. The age standardised incidence rate of all adenocarcinoma sites was 40.5 (37.8–43.3) in men and 11.0 (9.2–12.8) in women, respectively. The corresponding male to female ratio was 3.68. Incidence rates of all upper GI adenocarcinomas after standardisation for age and all categories of tobacco smoking were 39.6 (95% CI 36.8 to 42.4) in men and 12.1 (95% CI 9.9 to 14.3) in women. The sex ratio for all upper gastrointestinal adenocarcinomas, after accounting for smoking status, changed only slightly (3.27 vs 3.68) (see table).
Conclusion: The male predominance of upper gastrointestinal adenocarcinomas is not explained by differences in tobacco smoking and may be related to endogenous rather than environmental factors.
0-84 96 HOUR BRAVO INCREASES YIELD IN PATIENTS WITH NEGATIVE 24 HOUR OESOPHAGEAL CATHETER PH TESTS RESULTS
R. R. Sweis, A. Anggiansah, R. Anggiansah, M. Fox, T. Wong. Department of Gastroenterology, St Thomas’ Hospital, London, UK
Introduction: 24 hour oesophageal pH monitoring (C-pH) is an important tool in evaluating patients with suspected gastro-oesophageal reflux disease (GORD). However, its clinical value has diminished due to limitations including tolerability, effect on patient daily activities and poor yield. Bravo is a novel wireless pH monitoring system which has the capability of measuring up to 96 hours. Prolonged measurement increases diagnostic reproducibility and sensitivity, especially in patients with intermittent symptoms. This study aimed to investigate whether Bravo has improved the diagnostic value in patients with ongoing symptoms suggestive of GORD but negative catheter pH results.
Aims and Methods: From November 2006 to August 2008 results of 18 consecutive patients referred for Bravo who had symptoms suggestive of reflux and negative C-pH were compared and analysed.
Results: The mean age was 46 (range 25–73); 3M:15F. Standard oesophageal acid parameters used were: total reflux (TR) (normal 0–5.3%), upright reflux (UR) (normal 0–8.15%), and supine reflux (SR) (normal 0–3.45%). All patients were negative for C-pH and diagnosed as normal. Average pH measurements at 48 and 96 hours that resulted in a change in diagnosis were as follows: TR increased to 5/18 (27.8%) and 7/18 (38.9%), UR increased to 5/18 (27.8%) and 6/18 (33.3%), and SR increased to 6/18 (33.3%) and 8/18 (44.4%), respectively; p<0.05 for all measurements at 96 hours. Worst day pH measurements at 48 and 96 hours that resulted in a change in diagnosis were as follows: TR increased to 6/18 (33%) and 12/18 (66.7%), UR increased to 5/18 (28%) and 9/18 (50%), and SR increased to 8/18 (44%) and 9/18 (50%), respectively; p<0.05 for all. Any positive reflux parameter would result in a diagnosis of GORD. Therefore, 7/18 (38.9%) and 9/18 (50%) using average pH measurements and 9/18 (50%) and 14/18 (77.8%) using single worst day measurements had a positive diagnosis at 48 and 96 hours respectively.
Conclusion: Individuals with negative results on 24 hour pH monitoring and ongoing symptoms are often considered to have “heightened sensitivity”, functional oesophageal symptoms or even psychological disease. This study shows the importance of prolonged pH monitoring to further investigate these patients. Prolonged pH measurement reduces the impact of day to day variability and increases the sensitivity and yield of the test. Had it not been for Bravo many patients with pathological pH exposure would not have received a definitive diagnosis of GORD.
Plenary session
0-85 OUTCOMES FOLLOWING EARLY RED BLOOD CELL TRANSFUSION IN ACUTE UPPER GASTROINTESTINAL BLEEDING
1S. A. Hearnshaw, 2T. Card, 2R. F. A. Logan, 3S. P. L. Travis, 4K. R. Palmer, 5M. F. Murphy. 1Gastroenterology, Royal Victoria Infirmary, Newcastle upon Tyne, UK, 2Epidemiology and Public Health, University of Nottingham, Nottingham, UK, 3Gastroenterology, John Radcliffe Hospital, Oxford, UK, 4Gastroenterology, Western General Hospital, Edinburgh, UK, 5NHS Blood and Transplant, John Radcliffe Hospital, Oxford, UK
Introduction: More than 60% of red blood cells (RBC) are now transfused to medical patients. Patients with acute upper gastrointestinal bleeding (AUGIB) are one of the leading medical patient groups using blood (∼14% of all transfusions).1 In massive exsanguinating upper gastrointestinal bleeding the value of RBC transfusion is self evident, but in less severe bleeding its value is less obvious with two trials failing to show that RBC transfusion was beneficial.2 3 This study uses data collected prospectively as part of the UK comparative audit of AUGIB to examine the relationship between RBC transfusion within 12 hours of presentation, re-bleeding and mortality.
Aims and Methods: Prospective data were collected electronically on patients presenting to all UK hospitals with AUGIB between 1st May and 30th June 2007. All patients included in this analysis underwent upper gastrointestinal endoscopy. A Rockall risk score4 was calculated for each patient and used with initial haemoglobin concentration in univariate and multivariate logistic regression models to examine the relationship between early RBC transfusion, re-bleeding and death.
Results: Data were received from 6750 patients from 208 UK hospitals treating patients with AUGIB. 4441 patients were included for analysis having had inpatient endoscopy for AUGIB and having complete data on early RBC transfusion. 44% of included patients received early RBCs. There was an association between early RBC transfusion and re-bleeding (OR 4.05, 95% CI 3.36 to 4.87) which remained after adjusting for both Rockall score and haemoglobin concentration (OR 2.26, 95% CI 1.76 to 2.90). Early RBC transfusion was also associated with a 28% increase in mortality (after risk adjustment) but this was not statistically significant (OR 1.28, 95% CI 0.94 to 1.74).
Conclusion: After adjusting for case mix and initial haemoglobin early RBC transfusion in AUGIB was associated with a two fold increase in risk of re-bleeding and a non-significant increase in mortality. A large randomised clinical trial is urgently required.
0-86 ALL-CAUSE MORTALITY FOLLOWING ENDOSCOPIC RETROGRADE CHOLANGIOPANCREATOGRAPHY IN ENGLAND: ANALYSIS OF HOSPITAL EPISODE STATISTICS LINKED TO DEATH REGISTRATION DATA
1K. Bodger, 2K. Bowering, 2S. Sarkar, 3C. Grant-Pearce, 3E. Thompson, 3M. Pearson. 1Gastroenterology Division, School of Clinical Sciences, University of Liverpool, Liverpool, UK, 2Digestive Diseases Centre, University Hospital Aintree, Aintree, UK, 3Department of Clinical Evaluation, University of Liverpool, Liverpool, UK
Introduction: The UK National Confidential Enquiry into Patient Outcome and Death report (NCEPOD, “Scoping our practice” 2004) and the UK Global Rating Scale encourage endoscopy units to audit 30-day post-procedure mortality. A UK study reported crude mortality rate of 2.7% at 30 days for first endoscopic retrograde cholangiopancreatography (ERCP) for a sample of UK hospitals.1 The true “national” figure is unknown. This study aimed to: (a) Determine feasibility of analysing all-cause post-ERCP mortality (at 7 and 30 days) using the national Hospital Episode Statistics (HES) dataset linked to Office of National Statistics (ONS) death certification data; and (b) Identify factors associated with crude mortality rates. This provided an opportunity to generate data for all English hospitals and provide local teams with pilot analyses for local verification.
Aims and Methods: HES data for 2006/7 was linked to ONS alive-dead status. Episodes of care (including day cases) containing OPCS-4 procedure codes for ERCP were identified during the first 11 months of the data year and deaths within 7 days and 30 days identified. For patients having >1 ERCP, the “last occurring” ERCP was analysed. Diagnostic fields containing ICD-10 codes were analysed for diagnosis. Factors associated with death were identified by univariate and multiple logistic analyses. Crude mortality rate at each hospital Trust were analysed versus ERCP number to explore “volume” effect.
Results: 34 817 ERCPs were coded (26 171 were “last” occurring; mean age: 66 years; emergency admission: 47.4%; cancer diagnosis coded: 16%). Deaths: n = 427 (7 days) and 1670 (30 days). Crude all cause mortality rate: 1.2% (7 days) and 4.8% (30 days). Univariate analyses confirmed age (>8 fold increased risk for >85 years vs <55 years), a coded cancer diagnosis (>8 fold risk vs non-cancer) and emergency admission (2.5 fold vs elective) as factors associated with death (p<0.001). At Trust level no significant correlation was observed between ERCP volume and mortality (Pearson r = −0.02, p = 0.8) and all units had mortality rates within appropriate confidence limits.
Conclusion: Linkage of HES-ONS data provides a tool for exploring crude mortality data and may provide local teams with audit data relevant to their endoscopy activity. Based on national data, 30 day mortality following ERCP is higher than previous reports1 but this reflects capture of all coded procedures nationally and mortality from any cause. Crude mortality is strongly associated with age and underlying disease (eg. acute illness requiring emergency admission or a malignant indication), consistent with the major role of disease progression and co-morbidity as predictors of short-term outcome. This is the largest-scale UK-based study available and provides a model for predicting outcome based on demographic and simple clinical variables. (Funding: NHS Information Centre)
Gastrointestinal physiology free papers
0-87 INCREASED SIGMOID COMPLIANCE MAY EXPLAIN GUT SYMPTOMS AND RESPONSE TO TREATMENT IN SUPRACONAL SPINAL CORD INJURY
1P. M. Trivedi, 1A. Bajwa, 2P. B. Boulos, 3M. C. Craggs, 1A. V. Emmanuel. 1Physiology Unit, University College Hospital, London, UK, 2Department of Surgery, University College, London, UK, 3Spinal Injuries Unit, Royal National Orthopaedic Hospital, Stanmore, UK
Introduction: Supraconal spinal cord injury (SCI) results in major gut dysfunction, most typically constipation and faecal incontinence. The underlying mechanisms are not well understood due to incomplete knowledge of colon physiology and the role of the enteric neural networks. Compliance is a measure of how distensible a hollow viscus is, and comparison of compliance between SCI and spinal intact (SI) controls may help define the pathophysiology of bowel dysfunction following SCI. The aim of this study was to prospectively investigate sigmoid and rectal compliance in SCI.
Aims and Methods: Fifteen (10 sigmoid compliance and 5 rectal compliance) SCI persons (7 male, mean age 42 years) were compared with 18 (10 sigmoid compliance and 8 rectal compliance) SI controls (7 male, mean age 50 years). The barostat catheter was placed into the sigmoid colon under direct vision using a flexible sigmoidoscope. Staircase distensions were performed (0–40 mmHg) in 4 mmHg increments. Anorectal manometry was performed using the station pull-through technique. Data are presented as mean ±standard deviation (SCI vs control).
Results: SCI persons had a significantly higher sigmoid compliance than controls (8.54±1.93 ml.mmHg−1 vs 5.24±1.68 ml.mmHg−1: p = 0.0021). There was no difference in rectal compliance (13.39±4.70 ml.mmHg−1 vs 11±1.29 ml.mmHg−1). In both SCI persons and SI controls, sigmoid compliance is significantly lower than rectal compliance (p = 0.0125 and p<0.0001 respectively). The amplitude of the recto-anal inhibitory reflex (RAIR) was significantly greater in SCI than SI (61.2%±20 vs 43.2%±13.3: p = 0.0064).
Conclusion: Sigmoid, but not rectal, compliance is significantly increased in supraconal SCI persons with constipation. This phenomenon may firstly explain why suppositories are often ineffective, whilst irrigation regimes clearing the left colon are helpful. It also suggests that the sigmoid colon is more dependent upon descending neuromodulation than is the rectum. An increased RAIR amplitude in SCI is coupled with an unchanged rectal compliance; this suggests there may be descending modulatory effects on this reflex. Finally, the difference between sigmoid and rectal compliance is preserved in SCI, suggesting that enteric nerve factors may be important in maintaining this differential. The physiological meaning of this differential, and the potential to exploit this therapeutically, will be determined in future studies.
0-88 LOWER MOTOR NEURONE SPINAL CORD INJURY REDUCES RECTAL COMPLIANCE WHILST PRESERVING SIGMOID COMPLIANCE
1P. M. Trivedi, 1N. Thoua, 2P. B. Boulos, 3M. C. Craggs, 1A. V. Emmanuel. 1Physiology Unit, University College Hospital, London, UK, 2Department of Surgery, University College, London, UK, 3Spinal Injuries Unit, Royal National Orthopaedic Hospital, Stanmore, UK
Introduction: The most common gut symptoms of lower motor neurone spinal cord injury (LMN-SCI) are constipation and faecal incontinence. The pathophysiology remains poorly understood. Compliance is a measure of how distensible a hollow viscus is, and comparison of compliance between LMN-SCI and spinal intact (SI) controls may help define the pathophysiology of bowel dysfunction following LMN-SCI. It may also further understanding of normal colorectal physiology. The aim of this study was to prospectively investigate sigmoid and rectal compliance in LMN-SCI.
Aims and Methods: Eleven (8 rectal compliance and 3 sigmoid compliance) LMN-SCI persons (4 male, mean age 40 years) were compared with 18 (8 rectal compliance and 10 sigmoid compliance) SI controls (7 male, mean age 50 years). The barostat catheter was placed into the sigmoid colon under direct vision using a flexible sigmoidoscope. Staircase distensions were performed (0–40 mmHg) in 4 mmHg increments. Standard anal manometry and rectal distension sensitivity testing were performed in all. Data are presented as mean±standard deviation (LMN-SCI vs control).
Results: LMN-SCI persons had a significantly lower rectal compliance than controls (6.77±1.45 ml.mmHg−1 vs 11±1.29 ml.mmHg−1: p = 0.0002). There was no difference in sigmoid compliance (6.56±2.03 ml.mmHg−1 vs 5.24±1.68 ml.mmHg−1). In SI controls, sigmoid compliance is significantly lower than rectal compliance (p<0.0001). However, this difference is not observed in LMN-SCI. Urge volume (p<0.05) and maximal tolerated volume (p<0.05) were significantly reduced in LMN-SCI. The amplitude of the recto-anal inhibitory reflex (RAIR) was significantly greater in LMN-SCI than controls (66%±21 vs 43%±13: p = 0.0033).
Conclusion: In LMN-SCI, rectal compliance is reduced, whereas sigmoid compliance remains unchanged. This may result from damage to the sympathetics, allowing unchecked parasympathetic discharge, hence reduced compliance. The physiological significance of a differential between sigmoid and rectal compliance, and why this is abolished in LMN-SCI, remains to be elucidated. The increased amplitude of the RAIR in LMN-SCI fits with the finding of reduced rectal wall compliance, as a stiffer rectal wall will relax more. Finally, this study suggests that the pathophysiology of faecal incontinence symptoms after LMN-SCI is related to rectal hypersensitivity and reduced rectal compliance overcoming the normal resting anal pressures which reduce to an exaggerated degree in response to rectal distension.
Gastroduodenal free papers
0-89 COULD MUCOSAL IRON MEDIATE THE HIGHER INCIDENCE OF GASTRIC CARCINOMA IN MALES?
1H. Watabe, 1J. P. Seenan, 1E. Combet, 2A. Duncan, 1V. Fyfe, 1D. Gillen, 3J. W. Winter, 1K. E. L. McColl. 1Medical Sciences, Western Infirmary, University of Glasgow, Glasgow, UK, 2Clinical Biochemistry, Glasgow Royal Infirmary, Glasgow, UK, 3Gastroenterology, Glasgow Royal Infirmary, Glasgow, UK
Introduction: The incidence of gastric carcinoma is higher in males than females. Male predominance is more apparent in the intestinal rather than the diffuse histological subtype. Epidemiological studies reveal a lag period of 17 years between the development of this cancer in males and females, with the peak difference occurring between the ages of 50 and 60 years and approximating the female menopause. In addition to the differences in sex hormone concentrations over this period there are differences in systemic iron levels between males and menstruating females. Iron is well recognised to induce free radicals which can produce DNA damage. However, little is known regarding the iron status of gastric mucosa in males or females.
Aims and Methods: To compare the mucosal iron status between males and females of reproductive years with and without Helicobacter pylori (Hp) infection. A total of 67 subjects (35 males, mean age 38.6) aged between 20 and 50 years were recruited. 24 tested positive for Hp infection (13 male). During endoscopy, 6 biopsy samples were obtained from the antrum of the stomach. A 15 ml blood sample was obtained for full blood count and serum ferritin. Mucosal iron concentration was measured using mass spectrometry. Mucosal ferritin and haemoglobin concentration were measured by enzyme-linked immunosorbent assay (ELISA). To eliminate the effect of blood contamination, iron concentration was corrected by mucosal haemoglobin concentration. Concentrations were calculated as per wet weight of each biopsy specimen.
Results: Blood haemoglobin (Hb) and serum ferritin (sFR) levels were higher in males than females; 15.1±0.2 g/dL vs 13.6±0.3g/dL (p = 0.0001) for Hb and 113.3±15.2 ng/dL vs 44.1±7.5 ng/dL (p<0.0001) for sFR. There was no significant difference in mucosal iron concentration between Hp negative males (13.3±1.6 μg/g) and Hp negative females (12.7±2.8 μg/g) or between Hp positive males (11.3±2.5 μg/g) and Hp positive females (11.7±0.6 μg/g). There was also no difference in mucosal ferritin level between Hp negative males (21.3±2.7 μg/g) and Hp negative females (15.3±1.6 μg/g) or between Hp positive males (53.5±8.9 μg/g) and Hp positive females (65.4±14.8 μg/g). However, mucosal ferritin level was increased in Hp positive versus Hp negative subjects irrespective of gender: 53.5±8.9 μg/g vs 21.3±2.7 μg/g in males (p = 0.0001) and 65.4±14.8 μg/g vs 15.3±1.6 μg/g in females (p = 0.0001).
Conclusion: Differences in mucosal iron are unlikely to contribute to the gender bias in gastric carcinoma. The increased mucosal ferritin concentration in the Hp positive subjects is consistent with its induction by inflammation.
0-90 IMPLICATIONS OF EOSINOPHILS IN DUODENAL BIOPSIES: AN ASSOCIATION WITH ATOPY, ALLERGY, MEDICATION AND EARLY SATIETY
1M. M. Walker, 1S. S. Salehian, 1C. E. Murray, 2J. M. Hoare, 2R. Negus, 2N. Powell, 3N. J. Talley. 1Histopathology, Imperial College, London, UK, 2Gastroenterology, Imperial College Healthcare NHS Trust St Mary’s Hospital, London, UK, 3Gastroenterology, Mayo Clinic College of Medicine, Jacksonville, USA
Introduction: Eosinophils are a normal constituent of the gastrointestinal (GI) mucosa. Emerging evidence suggests that they may preferentially accumulate in the small bowel mucosa of patients with specific upper gastrointestinal symptoms in functional dyspepsia.1 Patients with atopy and allergy have been reported to have an accumulation of eosinophils in the GI tract resembling the inflammatory reaction occurring in the airways.2 3
Aims and Methods: This study aimed to assess the prevalence of eosinophilia in duodenal biopsies of patients attending for routine endoscopy and audit associated clinical conditions and symptoms. Consecutive patients (n = 100, mean age 54 years, SD17.5, range 16–83 years, 38 males) attending for oesophogastroduodenoscopy between 2004 and 2007 with duodenal biopsies (reported normal by histology) were randomly selected for audit from the histopathology files. Eosinophil counts at microscopy in 5 high power fields (HPF) were assessed by two independent, blinded observers. Duodenal eosinophilia was defined by a sum eosinophil count of >22/5HPF.1 The clinical records of patients were analysed for symptoms, clinical diagnosis and medications.
Results: The prevalence of duodenal eosinophilia was 25% in this population. Inter-observer concordance (un-weighted kappa score, 0.81) showed almost perfect agreement. An association of eosinophilia was found with symptoms of early satiety (odds ratio (OR) 9.1, 95% CI 1.646 to 50.60; p = 0.01), a history of atopy (OR 3.7, 95% CI 1.43 to 9.58; p = 0.01) and medications including non-steroidal anti-inflammatory drugs (NSAIDs) (OR 9.96, CI 1.27 to 78.26, p = 0.01). There was no association for eosinophilia with body mass index, smoking, age, Helicobacter pylori infection, HIV, irritable bowel syndrome or with intraepithelial lymphocyte count.
Conclusion: Subtle duodenal eosinophilia may be relatively common in a healthcare seeking population but has been previously overlooked; it may indicate a hypersensitivity mechanism in some patients with symptoms of functional dyspepsia and is associated with allergy, atopy and medication.
0-91 INCREASED ASPIRIN USE AND UPPER GASTROINTESTINAL BLEEDING RATES IN SOCIALLY DEPRIVED PATIENTS
1Y. Vivogravada, 2M. Leighton, 1A. Avery, 2R. F. A. Logan, 1D. Kendrick, 2J. C. Atherton, A. Shonde J Hippisley-Cox, 2C. J. Hawkey. 1Primary Care, School of Community Health Sciences, University of Nottingham, Nottingham, UK, 2Nottingham Digestive Diseases Centre and Biomedical Research Unit, Nottingham University Hospital, Nottingham, UK
Introduction: Cardiovascular morbidity is associated with social deprivation but it is not clear whether this results in greater use of aspirin nor whether more aspirin associated gastro toxicity results. QRESEARCH is a new larger database that includes information on deprivation.
Aims and Methods: We used QRESEARCH to investigate aspirin use in relation to the Townsend Index of deprivation and to co-morbidity and whether this was associated with a higher incidence of gastrointestinal bleeding. All patients aged 45–100 years with continuous aspirin use (definition: new prescription ⩽8 weeks after previous) at any time during the period 1 April 2003–31 March 2007 were included.
Results: 459 practices met inclusion criteria to generate 4.87 million person years of observation. Over 99% of aspirin use was for ⩽300 mg per day. Aspirin use was higher at younger ages in men but similar between sexes by age 80. It increased from 9.9% in 2003 to 14% in 2007. Use was higher in deprived compared to affluent areas (11.8% in lowest quintile versus 8.6% in highest quintile in 2003, 15.9% and 12.5% in 2007). Of patients with coronary heart disease 55.2% were prescribed aspirin in 2003 and 59.1% in 2007, 50.8% and 54.2% for stroke, 33.7% and 44.1% for diabetes, 24.3% and 29.2% for hypertension. Coronary heart disease was more common in deprived than affluent areas (12.0% vs 8.8%). The incidence of upper gastrointestinal bleeding rose with age (from 44.3 per 100 000 at aged 60 to 325.2 per 100 000 at age 85 for women and 62.7 per 100 000 and 378.4 per 100 000 for men) but not over the four years of the study (80.1 per 100 000 in 2003/4, 72.3 per 100 000 in 2006/7); more men than women were affected and rates were higher in deprived than affluent areas (100.9 per 100 000 vs 58.3 per 100 000). Upper gastrointestinal bleeding was more common in patients with cardiovascular disease, diabetes or hypertension. Aspirin increased the risk of upper gastrointestinal bleeding, even after adjustment for age, sex, deprivation and co-morbidities (1.59, 1.47–1.73).
Conclusion: Patients in deprived areas are prescribed more aspirin than in affluent areas and have higher rates of upper gastrointestinal bleeding. Aspirin may contribute to this. However, upper gastrointestinal bleeding appears not to be increasing despite increased use of aspirin.
0-92 FAMOTIDINE FOR THE PREVENTION OF PEPTIC ULCERS IN USERS OF LOW-DOSE ASPIRIN: PLACEBO-CONTROLLED PROSPECTIVE TRIAL
1A. S. Taha, 1C. McCloskey, 1R. Prasad, 2V. Bezlyak. 1Gastroenterology, Crosshouse Hospital, Kilmarnock, UK, 2Robertson Centre for Biostatistics, University of Glasgow, Glasgow, UK
Introduction: The use of low-dose aspirin in a wide range of conditions has been increasingly associated with peptic ulcers and their complications, with limited preventative options.
Aims and Methods: We aimed at testing the efficacy of famotidine at standard dose of 20 mg twice daily, in the prevention of oesophagitis, gastric, and duodenal ulcers in patients taking low-dose aspirin (75 mg daily). Adult patients were recruited from the cardiovascular, neurovascular (strokes, transient ischaemic attacks, etc), or diabetes clinics if they took aspirin with or without clopidogrel or dipyridamole, and regardless of the level of comorbidity. Patients were endoscoped at baseline and 12 weeks after taking famotidine 20 mg twice daily or its placebo. At baseline, patients were still included if they had erosions or ulcer scars, and excluded if they had active ulcers, malignancy, or if they took warfarin or other anti-ulcer agents. Comorbidity was graded by the Charlson score and oesophagitis by the LA system.
Results: Of 14 515 patients screened for suitability to consider the study, 404 were randomised. The rest were either unsuitable (not taking aspirin, or having ulcers at initial endoscopy, etc), or refused to consider the trial. In the randomised group (n = 404), 277 (68.6%) were males, the median (range) age was 63 (36–86) years, 128 (31.8%) had Helicobacter pylori gastritis, and 354 (87.6%) had erosions or scars at baseline endoscopy. These characteristics were evenly distributed between the famotidine and placebo groups. After 12 weeks of treatment, the primary end-points are as shown in the table (intention-to-treat analysis). Also, haematemesis, melaena, cardiac events, or death were observed in 4 patients (1.96%) taking famotidine and 9 (4.5%) taking placebo (p = 0.17, not significant).
Conclusion: Famotidine is effective in the prevention of erosive oesophagitis, gastric and duodenal ulcers in patients taking low-dose aspirin. Also, famotidine is well tolerated in patients with cardiovascular or neurovascular diseases, or those with diabetes, who require low-dose aspirin.
0-93 DETERMINANTS OF HELICOBACTER PYLORI LOCALISATION AND IL8 EXPRESSION IN THE HUMAN GASTRIC MUCOSA
S. R. Patel, D. P. Letley, N. R. Hussein, K. Robinson, J. C. Atherton. Nottingham Digestive Diseases Centre BRU, Centre for Biomolecular Sciences, Nottingham, UK
Introduction: The density of Helicobacter pylori on the gastric mucosa may be influenced by a number of factors, including the host immune response and virulence determinants expressed by the colonising strain. The cag pathogenicity island is a major determinant of mucosal IL8 secretion and is associated with duodenal ulceration (DU) and gastric cancer. Duodenal ulcer promoting gene A (dupA) is associated with IL8 secretion and DU. Gastric cancer is associated with pan-gastritis, and DU with antral-predominant gastritis, but the determinants of distribution of inflammation in the stomach are unknown.
Aims and Methods: We aimed to investigate the effect of H. pylori virulence factor expression on the gastric cytokine response to infection, and determine the impact of these on bacterial localisation and colonisation density in humans. Twenty H. pylori-positive patients attending an upper gastrointestinal (GI) endoscopy donated gastric biopsy samples. Total DNA and RNA were extracted, and colonising bacterial strains were isolated. To assess the host immune response, IL8 mRNA expression was quantified by reverse transcriptase-polymerase chain reaction (RT-PCR). Virulence genotypes of colonising strains were determined by PCR for cagA and dupA. Bacterial colonisation density was assayed by real-time PCR to provide the numbers of bacteria/human cell.
Results: Colonisation with a dupA+ strain was associated with a 5-fold increase in IL8 expression compared to dupA- infections (median 120 vs 23 units, p = 0.027). In contrast, cagA+ strains were associated with similar IL8 expression levels as cagA- strains (median 42 units vs 32 units). A 6-fold increase in antral:corpus bacterial colonisation was observed with dupA+ (median 2.8 units) compared with dupA- infections (median 0.5 units, p = 0.025), suggesting that dupA+ strains have a tendency towards antral predominant colonisation. No such trend was seen with cagA. A negative association between IL8 expression and bacterial density was seen, in that very high expression of IL8 was observed only in biopsies with low bacterial loads, and very high colonisation densities were seen only in biopsies with low IL8 expression.
Conclusion: Infection with a dupA+ strain was associated with a more aggressive inflammatory response and antral-predominant colonisation, consistent with the increased risk of duodenal ulceration attributed to this virulence factor. Bacterial colonisation density appeared to follow a reciprocal association with inflammatory cytokine expression implying that inflammation may limit H. pylori growth in the human gastric mucosa.
Interactive case presentations
CC-94 UNSUSPECTED CAUSE OF HEPATOSPLENOMEGALY IN AN ADULT SRI LANKAN IMMIGRANT ON A BACKGROUND OF CHRONIC ALCOHOLISM AND VITILIGO LIKE SKIN LESIONS
R. L. Satarasinghe, A. A. A. Riyaaz, M. A. R. Jayawardana. Department of Medicine, Sri Jayewardenepura General Hospital and Postgraduate Training Center, Nugegoda, Sri Lanka
Introduction: Hepatosplenomegaly is a common clinical problem encountered in gastroenterological practice. Chronic alcoholism is one of the causes of hepatosplenomegaly which is of interest to the gastroenterologist and it is commonly attributed to the presence of portal hypertension with or without ascites, but at times needs consideration of other causes in the differential diagnoses as illustrated by the following case description.
Case History: A 40 year old Sri Lankan male who had lived in Italy for 5 years, spending 2 years as a gardener in the countryside, presented with 6 month history of progressive asthenia, anorexia and weight loss. He had been investigated for anaemia without a definitive diagnosis. He consumed alcohol above safe limits for more than 15 years. Examination revealed cachexia, pallor, generalised macular, depigmented skin rash resembling vitiligo, grade 2 finger clubbing, a non-tender smooth hepatomegaly of 3 cm and a firm splenomegaly of 10 cm below respective costal margins without ascitis.
Results: Routine investigations revealed a pancytopenia with a haemoglobin of 5.4 g/dl, white cell count of 2300 k/microlitre and platelets of 64 k/microlitre, an ESR of 160 mm, a C-RP of 96 mg/dl, a polyclonal gammapathy, normal liver function tests except for a raised alkaline phosphatase of 580 u/l, a hypoalbuminaemia of 24 g/l, a normal clotting profile, a normoglycaemia, normal renal function tests, negative malarial antigen tests, hepatitis B serology, C serology and an HIV screening test. His blood picture confirmed pancytopenia with a relative neutrophilia, and an ultrasonography confirmed hepatosplenomegaly without any other abnormalities. A bone marrow aspiration and trephine biopsy showed intracytoplasmic inclusions and the histology of skin lesions too showed similar findings. Subsequent tissue culture confirmed the diagnosis. Hepatosplenomegaly and pancytopenia in this instance could have been attributed to chronic alcoholism and hypersplenism, and the true diagnosis could have been overlooked. Skin lesions could have been misdiagnosed as vitiligo. Nevertheless, globalisation of employment opportunities has made this a reality, thus adding uncommon flavours to the differential diagnosis.
Conclusion: This case history illustrates that with increasing travel abroad, rare acquired causes should be entertained in the differential diagnosis of a clinical problem which are otherwise non-existent in that geographical distribution.
CC-95 AN UNUSUAL CAUSE FOR ABDOMINAL PAIN AND OBSTRUCTIVE JAUNDICE IN A YOUNG MALE
1A. D. Dhanda, 2A. Selman, 2V. Wong. 1Department of Gastroenterology, North Bristol NHS Trust, Bristol, UK, 2Department of Gastroenterology, Whittington Hospital NHS Trust, London, UK
Introduction: A 37 year old male city worker presented with acute severe ulcerative colitis and was treated with intravenous steroids and ciclosporin. He was commenced on maintenance azathioprine 2 mg/kg and was discharged in remission. He presented 4 months later with severe upper abdominal pain radiating to the back with associated nausea and vomiting.
Aims and Methods: Not applicable.
Results: He had biochemical markers of an inflammatory process. Acute pancreatitis was excluded with a normal serum amylase and normal appearance of the pancreas on CT scan. This CT did not identify any abnormality within the abdomen. His abdominal pain worsened over the following 3 days, and he then developed jaundice. Liver biochemistry showed a cholestatic picture. A further CT scan of his abdomen now showed a dilated common bile duct and intrahepatic ducts with a dilated gallbladder, but no calculi seen. The pancreas looked bulky but did not appear to have any focal abnormalities. An ERCP showed a distal tight common bile duct stricture with proximal dilatation. There was also irregular narrowing of the pancreatic duct within the body of the pancreas. An autoimmune profile was normal but brushings taken at ERCP were weakly positive for IgG4. This man was treated with oral glucocorticoid therapy, and 3 months later a repeat ERCP showed complete resolution of the CBD stricture and the irregular narrowing of the pancreatic duct.
Conclusion: We describe the first case, to our knowledge, of an acute presentation of autoimmune pancreatitis which was successfully treated with oral glucocorticoid therapy and relief of the acute obstructive jaundice with a plastic stent inserted at ERCP.
CC-96 GASTROINTESTINAL BLEEDING—OCCULT AND ACUTE
1B. Lee, 1J. J. Hurley, 1J. Turner, 1K. Axe, 1S. Dolwani, 2J. Torkington, 1G. Swift, 1J. Green. 1Gastroenterology, 2Surgery, Llandough Hospital, Vale of Glamorgan, Wales, UK
Introduction: Gastrointestinal bleeding is extremely common. We present two rare and interesting causes of gastrointestinal bleeding presenting in the same patient.
Aims and Methods: A 66 year old man presented to the medical assessment unit with a 2 week history of breathlessness, vomiting and 1 stone weight loss following a holiday in Jamaica. He also had a 3 week history of melaena prior to admission. His initial investigations showed a microcytic anaemia (haemoglobin 8.7 g/dl MCV 77), thrombocytosis (platelet count 534×109), normal liver and renal function tests but a raised CRP at 142 mg/l. He had a swinging pyrexia but urine and urine cultures were negative. A chest x ray and echocardiogram were normal.
Results: The initial plan was to perform an upper GI endoscopy; however whilst awaiting this, a CT abdomen was performed to exclude an infective cause of his symptoms as he continued to spike high grade fevers. This was reported as showing bilateral large adrenal masses and a 6 cm mass in the mid small bowel wall. The urinary catecholamines and 24 hour urinary free cortisol were normal. However, there was evidence of adrenal insufficiency on the short synacthen test. The patient underwent a laparoscopy to obtain tissue diagnosis of the small bowel mass. The histology of this was reported as typical of a “starry sky pattern.” He was started on appropriate treatment which was complicated by a persistent pyrexia. The patient then had a large lower gastrointestinal bleed with clinical signs of peritonitis necessitating an emergency laparotomy. The findings at laparotomy were “tumour masses” in the caecum, sigmoid and proximal small bowel with a gangrenous area at the ileocaecal junction. The tumour was resected en masse. Surprisingly the histology of the resected mass did not show any malignancy but revealed a different aetiology for the lower gastrointestinal haemorrhage. This was treated but the patient died 2 months later due to aggressive recurrence of the initial pathology.
Conclusion: In the presence of a microcytic anaemia and a history of melaena, occult bleeding from the gastrointestinal tract should always be considered. The presence of his other symptoms suggested involvement of other systems and a search for a unifying diagnosis needed to be sought. The subsequent lower gastrointestinal bleed was a rather unexpected, but not unknown complication of treatment of the initial disease.
CC-97 DILEMMA WITH ABNORMAL LIVER FUNCTIONS
1C. Puli, 1M. Khattak, 1D. Joy, 1M. Patel, 2D. J. Mutimer. 1Gastroenterology, Prince Charles Hospital, Merthyr Tydfil, UK, 2Gastroenterology, Queen Elizabeth Hospital, Birmingham, UK
Introduction: Seronegative (also known as non-A, non-B or non-A, non-B, non-C or non-A–E) acute liver failure refers to an idiopathic hepatitis resulting in acute liver failure (ALF). Well recognised causes of ALF are excluded and serological markers for hepatitis A–E serology are negative. The development of liver failure in a patient with seronegative hepatitis is associated with a poor prognosis, and spontaneous recovery is unlikely in most cases.
Aims and Methods: We are reporting a 52 year old lady who was diagnosed with acute seronegative hepatitis and treated with oral prednisolone. The diagnosis was based on clinical features and results of biochemical markers like LFTs, viral hepatitis screen, autoimmune screen, ferritin, iron studies, serum immunoglobulins, anti-TTG, copper, caeruloplasmin, alpha-1-antitrypsin levels and imaging studies such as USS abdomen, CT Abdomen, MRCP.
Results: Prednisolone was commenced about 6 weeks after first presentation of symptoms. Improvement of serum transaminases level was noticed within a week of starting steroid and which continued over next 4 weeks.
Conclusion: Steroids should be considered in all patients with acute seronegative hepatitis prior to developing acute liver failure. The association of immune dysregulation and response to steroid treatment could be indicative for an autoimmune pathogenesis of the disease. Further large-scale controlled trials are required to validate the role of steroid and its duration of treatment in seronegative hepatitis.

CC-98 AN UNUSUAL CASE OF NOCTURNAL DIARRHOEA
1J. R. Neale, 2S. Bridger, 2C. Hovell. 1Gastroenterology, Southampton General Hospital, Southampton, UK, 2Gastroenterology, Dorset County Hospital, Dorchester, UK
Introduction: We present a case of chronic diarrhoea in a 65 year old gentleman with an unusual aetiology. We highlight the process of investigation and describe the pathophysiology behind his condition.
Aims and Methods: This 65 year old gentleman presented to the gastroenterology department with a 6 month history of frequent loose motions, including 2–3 times at night. He had previously undergone an outpatient colonoscopy and biopsies which had proved to be unhelpful. He had no other “red flag” symptoms, but his nocturnal bowel opening raised suspicions of a significant disease process.
Results: Further initial investigations also proved to be unhelpful. These included coeliac antibodies, gastroscopy and duodenal biopsies, carcinoid screening and faecal elastase. He subsequently presented to the acute ENT services with stridor and dyspnoea. After further investigation he was diagnosed with medullary cell carcinoma of his thyroid gland (MTC).
Conclusion: This is a rare cause for a common presenation to gastroenterology services. It is also an unusual way for these tumours to present. MTC can cause a secretory diarrhoea. They may be sporadic or genetic, in association with defects in p53 and ret oncogenes. There is also an association with multiple endocrine neoplasia syndromes. Genetic and family screening is therefore required. We use this case to report an unusual case and highlight the need for vigilance in the investigation of patients with symptoms such as nocturnal diarrhoea.
CC-99 CHRONIC ABDOMINAL PAIN IN A YOUNG SRI LANKAN LADY—A DIAGNOSTIC AND THERAPEUTIC DILEMMA IN THE TROPICS
M. A. R. Jayawardana, R. L. Satarasinghe, A. A. A. Riyaaz. Department of Medicine, Sri Jayewardenepura General Hospital and Postgraduate Training Center, Nugegoda, Sri Lanka
Introduction: The incidence of chronic bowel disorders and certain specific disorders have progressively increased globally over the last several decades. There is a close resemblance in pathogenic, clinical, radiological, endoscopic and histological features between certain specific bowel diseases, which makes the accurate diagnosis of the condition quite difficult in the odd instance, thus causing a therapeutic dilemma as illustrated by the following case presentation.
Case Report: A 21 year old Sri Lankan housewife, married with one child presented with a history of abdominal pain and loss of appetite of 3 months’ duration. Although she was suffering from non-specific abdominal pain for couple of years, she had no significant past medical or surgical condition necessitating treatment except for a bout of bleeding per rectum which was uninvestigated. Her family and social history was unremarkable. Clinical examination revealed a distressed lean lady with a BMI of 19, with mild pallor and some right iliac fossa tenderness. Routine laboratory tests revealed the following. A hypochromic microcytic anaemia with a Hb of 8.9 g/dl, ESR 48 mm in the first hour, serum ferritin 7.7 ng/ml (normal 12–237 ng/ml), C-RP of <6 mg/dl. The blood sugars, thyroid, renal, liver profiles, stool tests, CXR-PA, abdominal and pelvic ultrasound were all normal. The Mantoux test was equivocal with a value of 7 mm. A colonoscopy revealed nodules in the caecum with a normal CT scan of the abdomen and pelvis, done subsequently. The histology of the caecal nodules revealed non-caseating granuloma with no other specifications. Histology revealed characteristic granulomatous lesions which include a differential diagnosis out of which two conditions were most likely. PCR for a specific bacterial infection was not done as it was thought irrelevant at the time of biopsy of the colonic lesions. A quadruple therapy was initiated commonly administered as a single combined tablet with appropriate omission of the relevant drugs. Apparently a favourable response was shown and anaemia improved with haematinics, and she was discharged from the clinic at the end of 6 months, with a normal ESR. Twenty months later in 2005 she presented again with fever, abdominal pain and vomiting, and repeat colonoscopy revealed the same endoscopic appearance and histology. She was commenced on treatment which was most appropriate for the most likely diagnosis. Clinical implications are discussed in the text of the interactive session.
Conclusion: The differential diagnosis of the two conditions could be a difficult task in the tropics and the decision of initial therapeutic modality. It is always wiser to treat the most likely condition in this instance, as the treatment of less likely conditions could be detrimental. Certain bowel disorders could also run a very indolent course, as in this instance. Certain drugs with antibacterial properties could have immunomodulatory actions which could modify the natural history of disorders with an immunological aetiology.
CC100 A CASE OF DELAYED DIAGNOSIS IN A PATIENT WHO PRESENTED WITH RECURRENT DIARRHOEA
1T. Lim, 2B. H. L. Tan, 3R. Pepple, 1E. Mohamed, 1N. Radhakrishnan, 4S. Sabir, 3S. Afify, 1R. George. 1Gastroenterology and Medicine, Rochdale Infirmary, Rochdale, UK, 2Surgery, Edinburgh Royal Infirmary, Edinburgh, UK, 3Surgery, 4Radiology, Rochdale Infirmary, Rochdale, UK
Introduction: We report an unusual and complicated case of diarrhoea in an elderly lady.
Aims and Methods: As above.
Results: A 71 year old woman was referred to our hospital with abdominal pain, vomiting, diarrhoea and pyrexia. Full blood count was normal. C-reactive protein (CRP) was raised at 54 mg/l. Liver function tests were unremarkable apart from a raised serum alanine transaminase (ALT) of 70 U/l. Stool and blood cultures were negative. Clostridium difficile toxin (CDT) was not detected. A week later, she developed severe upper abdominal pain, rigors and pyrexia of 39°C and was readmitted to hospital. The abdominal ultrasound showed a thickened and inflamed gall bladder wall suggesting possible gall stones. However, she failed to respond to medical treatment, and further investigations with contrast CT abdomen revealed concurrent mesenteric ischaemia. An exploratory laparotomy was then performed and a 17 cm segment of the jejunum was found to be ischaemic and gangrenous. The affected section of small bowel was resected followed by an end to end anastomosis. She made an uneventful recovery.
Conclusion: Symptoms of mesenteric ischaemia can be vague and non-specific particularly in the elderly patients. Consider mesenteric ischaemia in patients presenting with unexplained abdominal pain and diarrhoea.
CC101 “PRIMUM NON NOCERE”
V. Jairath, E. Wood, A. Hall, C. Blanshard. Department of Gastroenterology, Homerton University Hospital, London, UK
Introduction: We report an interactive case of a patient with complex Crohn’s disease who presented with a life-threatening opportunistic infection secondary to a combination of immunosupressant medications. We hope to highlight the difficult clinical challenge facing all inflammatory bowel disease(IBD) physicians in deciding which concomitant medication to use, and which to discontinue in order to maximise clinical response whilst keeping the risk of adverse effects to a minimum.
Aims and Methods: A 24-year-old Asian man was diagnosed with Crohn’s colitis in 2002 based on a characteristic colonoscopy and biopsies demonstrating active granulomatous colitis. Over the next 12 months his disease flared requiring 2 prolonged courses of steroids and then surgery to lay open a peri-anal abscess and fistulo-in-ano. He was commenced on azathioprine in 2003 and steroids were successfully weaned. However, despite a maximum dose of azathioprine and trial of elemental feed his disease remained active and steroid dependent; therefore he was commenced on infliximab (5 mg/kg) in 2004. He achieved remission after 3 doses of infliximab after which he was maintained on azathioprine monotherapy throughout 2005. After further flares in 2006 he was switched from azathioprine to methotrexate which kept him in steroid free remission for 1 year. Following further relapses requiring steroids he was re-commenced on regular infliximab infusions in October 2007; however weaning steroids proved to be difficult. Thus his dose of infliximab was increased to 10 mg/kg in addition to his methotrexate (25 mg/week) and prednisolone 40 mg daily.
Results: 3 weeks later he presented with myalgia, fever and night sweats. On examination he was systemically unwell, tachycardic, hypotensive, pyrexial with neck stiffness and altered mental state. There were no focal neurological signs. Blood cultures confirmed Listeria monocytogenes in 6/6 bottles. CT brain was unremarkable with no signs of raised intracranial pressure; hence we proceeded to lumbar puncture. This contained >500 white cells (70% polymorphs, 30% lymphocytes), raised protein, low glucose and Gram-positive rods consistent with a diagnosis of Listeria meningitis.
Conclusion: Listeria is a facultative intracellular parasite with a primary habitat in soil and decaying vegetation. It is an important pathogen in neonates, the elderly, pregnant women, immunosupressed patients and occasionally in previously healthy individuals. The mortality of treated Listeria meningitis is 20–40%, and 100% if untreated. We discuss in detail the serious potential risks of combination immunosupressant medication in complex IBD. Furthermore we must not forget the important role of surgery in patients with chronic severe Crohn’s disease. As with any clinical decision, we must assess risks/benefits and remember to “First do no harm.”
Plenary posters
PP102 ANEUPLOIDY ASSOCIATED WITH HELICOBACTER PYLORI INFECTION IS COMMON IN EARLY STAGES OF GASTRIC CANCER
1A. Somasekar, 1J. Williams, 2L. Williams, 3J. Davies, 4P. Griffiths, 3G. Jenkins. 1Gastroenterology, Neath Port Talbot Hospital, Port Talbot, UK, 2Gastroenterology, Royal Glamorgan Hospital, Llantrisant, UK, 3Institute of Life Science, Swansea University, Swansea, UK, 4Pathology, ABM Trust Hospitals, Swansea, UK
Introduction: Losses and/or gains of whole chromosomes (aneuploidy) are extremely common in most cancers. Indeed aneuploidy is thought to occur early in carcinogenesis and the genetic instability induced is thought to provide a pool of selectable clones for tumour evolution. We have been interested in aneuploidy as a biomarker for cancer risk for some time. Here we aimed to determine how early aneuploidy occurred in the development of gastric cancer and if it could be related to infection with H pylori. We also concurrently assessed NF-kB activation (by examining up-regulation of IL-8 and presence of phosphorylated p65).
Aims and Methods: We collected 52 cytology brush samples of gastric mucosa during routine endoscopic examination. We examined aneuploidy levels in these exfoliated cells using fluorescent in situ hybridisation, specifically looking at copy numbers of chromosome 1. We assessed chromosome copy numbers in an average of 180 cells per patient. Concurrently, during endoscopy biopsy samples were obtained for histological assessment and for CLO testing for H pylori presence. Further biopsies were collected for IL-8 analysis by realtime PCR using extracted RNA and for p-p65 analysis by Western blotting of extracted proteins.
Results: Aneuploidy levels (percentage of cells with abnormal copy numbers) of 2.6% of cells were noted in the histologically normal gastric controls (n = 11). Interestingly, aneuploidy levels mirrored histological progression in the stomach with gastritis specimens (n = 22) having an average aneuploidy level of 3.8%, rising to 5.5% when H pylori infection was present (n = 7). In the small number of samples with atrophy or intestinal metaplasia (n = 3) the aneuploidy levels rose further to 6.2%. The increases in aneuploidy levels in patients with gastritis and H pylori +ve gastritis were significant (p<0.05), whilst the increase in aneuploidy in patients with atrophy/IM was highly significant (p<0.01). In terms of IL-8 expression analysis and p-p65 abundance, the highest levels were evident in the H pylori +ve gastritis specimens, tailing off in the atrophic gastritis/IM samples.
Conclusion: Aneuploidy levels mirror the histological progression in early stages of gastric neoplasia. Infection with H pylori significantly increases the level of aneuploidy in the gastric mucosa. Whilst H pylori also led to increased IL-8 expression and p-p65, this receded in atrophic gastritis/IM specimens. Hence NF-kB activation may represent a marker solely of inflammation. In contrast, the aneuploidy introduced early in gastric carcinogenesis persists and may contribute to neoplastic progression. Importantly, aneuploidy might be a suitable marker of cancer risk in pre-malignant diseases of the GI tract.
PP103 THE DOWNSTAGING OF COLORECTAL CANCERS BY THE UNITED KINGDOM NATIONAL BOWEL CANCER SCREENING PROGRAMME—DATA FROM THE FIRST SCREENING CENTRE
1P. Ellul, 1E. N. Fogden, 2B. Rowlands, 3C. Simpson, 3B. C. McKaig, 3E. T. Swarbrick, 3A. M. Veitch. 1Department of Gastroenterology, 2Department of Histopathology, 3Bowel Cancer Screening Centre, Royal Wolverhampton Hospital NHS Trust, Wolverhampton, UK
Introduction: A high proportion of patients with colorectal cancer (CRC) present late with an associated poor prognosis. Data from two randomised controlled trials of CRC screening in Nottingham and Funen demonstrated significant downstaging of the cancers diagnosed in the screened population with a reduction in CRC-associated mortality at 11–13 years’ follow-up respectively. Pilot data from the National Bowel Cancer Screening Programme (NBCSP) demonstrated predominantly early stage disease amongst the screened population. Wolverhampton was the first centre to start screening and has completed the prevalent round (2 years) of screening.
Aims and Methods: A case-control study was conducted to investigate whether downstaging occurred in the NBCSP at Wolverhampton. Patients aged 60–69 diagnosed with CRC at colonoscopy during NBCSP in the 2 years since screening started in July 2006 were included in the study group. Control data were obtained regarding patients aged 60–69 from the screening catchment area diagnosed with CRC prior to the introduction of the NBCSP (July 2004–June 2006).
Results: The total population in the screening area is 850 000. 87 876 FOB kits were sent out with 45 849 returned (52% uptake). 913 colonoscopies were performed with a 94.75% caecal intubation rate. There were 3 complications (3 haemorrhages and no perforations). The NBCSP in Wolverhampton identified 90 CRC in the first 2 years, and complete staging data are available for 85 to date. 67.8% were male. 256 CRC were identified in the control group (61.3% male). There was a highly significant shift towards earlier stage disease in the screened group (see table).
Conclusion: The 2 year data from the first centre to start bowel cancer screening demonstrate significant downstaging of cancer and are consistent with both the RCT and pilot data. This is likely to lead to a reduction in CRC-associated mortality in the screened population.
PP104 ADENOMA DETECTION RATE IN THE BOWEL CANCER SCREENING PROGRAMME AND IMPLICATIONS FOR RESOURCE ALLOCATION AND SERVICE PROVISION
N. Powell, J. Hoare, G. Smith, J. Martin. Gastroenterology, Imperial College NHS Trust, London, UK
Introduction: The NHS bowel cancer screening programme (BCSP) has been implemented to improve early diagnosis of colorectal cancer (CRC) and premalignant adenomas in a bid to increase survival. Pilot studies have been used to model the impact of the programme on resource and service provision, since additional colonoscopic surveillance is recommended following adenoma detection during the index colonoscopy. Accordingly, data from local screening centres regarding adenoma detection rates in local populations are needed to facilitate appropriate allocation of resources and service provision.
Aims and Methods: The frequency and profile of adenomas detected in our local BCSP experience were calculated and compared with expected frequencies based on data from the second bowel cancer screening pilot.1 Adenomas were categorised as low, intermediate or high risk based on the number and size of adenomas detected, which in turn was used to dictate the subsequent colonoscopic surveillance intervals required, in accordance with current BSG guidelines,2 which have been adopted by the BCSP. In this study adenomas with high grade dysplasia, or carcinoma in situ were regarded as high risk, irrespective of the number or size of adenomas present.
Results: Data from 265 consecutive BCSP colonoscopies are reported. We detected significantly more adenomas in our screening population (124 adenomas, prevalence 46.8%) compared with an expected frequency of 35%, expected from experience reported from the second pilot study (p<0.005). Unsuspected carcinomas were identified in an additional 7 endoscopically resected polyps. High risk adenomas accounted for 26.9% of adenomas in our cohort compared with only 15.7% in the second pilot study (p<0.025). Extrapolation of these data to a primary care population of 500 000 individuals, where 600 first round screening colonoscopies are anticipated (following the age extension to 74 years), would predict the requirement of 46 additional surveillance colonoscopies each year to provide appropriate follow-up for the high risk adenoma group alone. This translates to an additional cost of £22 448 (based on a payment by results tariff of £488 per colonoscopy) and an extra 9.2 colonoscopy lists per annum for each 500 000 head of population served by a screening centre.
Conclusion: The adenoma detection rate, particularly of high risk lesions, was significantly higher than anticipated in our population of BCSP subjects. These findings have important implications for local resource and service provision. Data from other local BCSP centres regarding adenoma detection rates are needed to determine whether this experience is replicated nationwide, and whether remodelling of costing and service provision structures are necessary.
PP105 LINEAR EUS AND EUS-FNA IN THE DIAGNOSIS OF PANCREATIC CYSTIC LESIONS IN A SINGLE TERTIARY REFERRAL CENTRE
1K. W. Oppong, 1K. Elamin, 1M. Nayar, 2V. Wadehra, 1P. Matthews, 1D. Manas, 1B. Jaques, 1S. White, 1R. Charnley. 1HPB Unit, Freeman Hospital, Newcastle, UK, 2Cytopathology, Royal Victoria Infirmary, Newcastle, UK
Introduction: As a consequence of the increased use of high quality cross-sectional imaging, pancreatic cysts are increasingly diagnosed. 10–30% of these will be cystic neoplasms. The accurate classification of pancreatic cysts into malignant/potentially malignant or benign would facilitate management decisions. Enoscopic ultrasound with FNA has the potential to provide high resolition imaging as well as aspirating fluid and tissue for analysis.
Aims and Methods: To assess EUS with EUS guided FNA in our high volume pancreatic unit in correctly classifying pancreatic cysts as malignant/malignant potential or benign. Inclusion of consecutive patients with suspected neoplastic pancreatic cysts between June 03 and December 06. Linear echoendoscope assessment of cyst appearance, fluid viscosity and FNA for cytology and fluid amylase, CEA and CA19-9 assays were done. Final diagnosis was positive cytology, histology or cyst resolution. Analysis was performed for the differentiation of malignant and potentially malignant from benign (see table).
Results: 173 EUS-FNA were performed in 149 patients. Average age was 64 (19–94). Female to male ratio was 1.6:1. 50 patients had surgery. A final diagnosis was reached in 80 patients (93 procedures); they formed the study group. 56 patients had malignant or premalignant lesions. 24 patients had benign lesions.
Conclusion: The global performance of EUS and EUS-FNA in our series compares favourably with previous studies. However, we have demonstrated an improved performance by combining the test results. Our data support decision-making based on results of linear EUS with EUS-FNA.
PP106 IS ANTIBIOTIC PROPHYLAXIS REQUIRED IN SUCCESSFUL ERCP?
P. G. Mayhead, M. Wilkinson, T. Wong. Gastroenterology, St Thomas’ Hospital, London, UK
Introduction: The UK ERCP audit revealed a 1.1% rate of post ERCP cholangitis.1 Guidelines recommend ciproxin, a cephalosporin or gentamicin.2 The most important predictor of post ERCP sepsis is incomplete bile duct drainage.3 We aimed to demonstrate that our antibiotic policy was safe and effective within a teaching hospital practice.
Aims and Methods: Ciproxin or cefuroxime 750 mg were given pre ERCP. Bile was aspirated from patients undergoing ERCP following wire cannulation of the bile duct before injection of contrast. Using electronic records, the clinical course for 30 days post ERCP was evaluated for evidence of post ERCP cholangitis.
Results: Bile was collected from 80 ERCPs. 59 were positive (74%). 7 had isolates resistant to either ciproxin or cefuroxime or both. 51 underwent first ERCP. 54% of these had positive cultures. All had definitive treatment for stone disease or had stents placed to establish biliary drainage. No post ERCP cholangitis was seen. Cholangitis was suspected prior to the procedure in 11 ERCPs. All had their biliary obstruction relieved. One with Primary Sclerosing Cholangitis (PSC) who had 2 ERCPs grew an isolate that was resistant to the ciproxin he had been given in both times. His stricture was stented, a stone removed and he recovered uneventfully from both ERCPs. All but one stented patient had a positive culture. Only one who had ERCP for a stent that had migrated distal to his hilar tumour required a percutaneous approach to drain the affected liver, but despite positive biliary cultures, cholangitis had not been suspected pre ERCP.
Conclusion: No deterioration in infection developed after successful ERCP in this small series. Cultures were similar to other published data.2 Infection can be avoided after ERCP without liberal use of antibiotics if biliary drainage is complete.4 Giving ciproxin pre ERCP when incomplete drainage was likely to occur resulted in only 26% of 4039 cases receiving antibiotics with a post ERCP cholangitis rate of 0.23%.4 Our antibiotic policy is safe and no antibiotic associated diarrhoea was seen post ERCP. Resistance, however, could be a problem. Whilst our practice conforms to current guidelines and the use of antibiotics in all patients reflects the therapeutic nature of the procedures undertaken, timely drainage of the bile duct is likely to allow limited use of antibiotics without increasing post ERCP cholangitis.
PP107 ENDOSCOPIC SPHINCTEROTOMY VERSUS CHOLECYSTECTOMY AS DEFINITIVE TREATMENT OF GALLSTONE PANCREATITIS
1R. U. Uwechue, 2G. David, 3M. Deakin, 1D. J. Corless, 1J. P. Slavin. 1General Surgery, Leighton Hospital, Crewe, UK, 2General Surgery, Macclesfield General Hospital, Macclesfield, UK, 3General Surgery, University Hospital of North Staffordshire, Stoke-on-Trent, UK
Introduction: Gallstone pancreatitis is a common condition, accounting for 30–40% of all cases of pancreatitis. British Society of Gastroenterology guidelines advocate definitive treatment, that is cholecystectomy or endoscopic sphincterotomy (ES) at the index admission or within 2 weeks. The evidence that ES is effective at preventing GSP is derived largely from small case series and one randomised study.
Aims and Methods: To investigate the rate of recurrent pancreatitis in a cohort of patients admitted with GSP and treated with either cholecystectomy or ES. Hospital Episode Statistics (HES) data from England from the years 2002–3 till 2005–6 were used. The index cohort included all patients admitted with GSP in 2002–3 who underwent ES, or cholecystectomy. This cohort was then followed until April 2006 to identify any patients admitted to English hospitals with a further bout of pancreatitis (see table).
Results: 3831 patients were admitted with GSP in 2002. 571 (15%) underwent ES as the sole treatment, and 1310 (34%) underwent cholecystectomy. Patients undergoing ES were older (median age 68) compared with patients undergoing cholecystectomy (median age 55). Recurrent pancreatitis was more common in patients who had undergone ES as compared with cholecystectomy in the first year; in subsequent years there was no difference.
Conclusion: Following an attack of GSP, ES is as effective as cholecystectomy at preventing further bouts of pancreatitis after the first year and is an appropriate treatment in elderly patients who are unfit for surgery.
PP108 COLONOSCOPY COMPLETION RATES IN THE ENGLISH BOWEL CANCER SCREENING PROGRAMME
1R. M. Valori, 2J. Patnick, 2C. Nickerson. 1Gastroenterology, Gloucestershire Hospitals, Gloucester, UK, 2NHS Cancer Screening Programmes, Fulwood House, Sheffield, UK
Introduction: The English Bowel Cancer Screening Programme (BCSP) began roll out in August 2006 using faecal occult blood test (FOBT) as the primary screening test. Colonoscopy is the principal investigation following a positive FOBT. Completeness of the procedure (or caecal intubation rate) is a key quality indicator of colonoscopy. This abstract describes the early results of caecal intubation rates within the programme.
Aims and Methods: A 90% unadjusted completion rate is the minimum standard for colonoscopy. Completion is defined by ileal intubation or visualisation of the ileo-caecal valve. Completion rates are not adjusted for obstruction or other reasons such as poor bowel prep. Completion rate data for all screening centres are recorded at the time of the procedure on a centralised database.
Results: Up to the end of October 2008, 15,495 colonoscopies had been performed in the BCSP by 128 colonoscopists. Because of the sequential nature of implementation there was wide variation in the number of colonoscopies performed (1–675). The completion rates are summarised in the table. The numbers in each column refer to the number of colonoscopists within each completion rate range. Each row illustrates data for colonoscopists that have performed fewer or more than 100 procedures in the programme. Four colonoscopists that have not yet reached 100 procedures in the programme have intubation rates below the standard. Colonoscopists that have performed more than 100 colonoscopies in the programme have intubation rates above the minimum standard of 90%.
Conclusion: The caecal intubation rate of each colonoscopist that has performed more than 100 colonoscopies in the English BCSP is above the standard. The majority of colonoscopists, regardless of how many procedures they have done in the programme, are achieving rates well above the standard.
PP109 CAGA/CAG PAI INDEPENDENT H PYLORI-INDUCED ERK ACTIVATION IN GASTRIC EPITHELIAL CELLS
1A. Ishiguro, 2C. Josenhans, 1K. Bransfield, 2N. Lotzing, 1P. A. Robinson, 1J. E. Crabtree. 1Leeds Institute of Molecular Medicine, St James’s University Hospital, Leeds, UK, 2Department of Medical Microbiology, Hannover Medical School, Hannover, Germany
Introduction: H pylori activates extracellular-signal related kinases 1 and 2 (ERK1/2) in gastric epithelial cells, in part, following EGFR transactivation. Epithelial cell hyperproliferation induced by H pylori may be a consequence of activation of this signalling cascade. Identification of bacterial virulence factors contributing to ERK1/2 activation will provide insight into the bacterial mechanisms involved in the increased risk of carcinogenesis following H pylori infection.
Aims and Methods: Isogenic mutants (Δcag PAI, ΔcagA, ΔcagC, ΔcagL and ΔHp525) were constructed in H pylori strains cag positive 7.13, 42GX, 48GX and 36.9. Wild-type strains and mutants were co-cultured with AGS gastric epithelial cells for 20–180 min and phosphorylation of ERK1/2 (pERK) quantified by “In Cell Western” assay.
Results: All four wild type strains induced significant ERK1/2 activation relative to unstimulated controls, but levels were markedly increased with strain 48GX compared with 7.13, 36.9 and 42GX. Mutant strain 7.13 Δcag PAI induced significantly reduced (p<0.05) pERK compared with 7.13 at 45 min, but there was no difference in stimulation at 90 min. ERK1/2 activation was also reduced at 45 min with 7.13 ΔcagA but not at later timer points. In contrast, 48GX ΔcagA stimulated pERK to the same extent as 48GX. Levels of pERK were also reduced (N.S) following culture with 42GX Δ525 than with 42GX at all time points. However 7.13 Δ525 induced significantly lower (p<0.05) ERK phosphorylation than 7.13 at 45 min and 90 min post-infection, but not at 180 min. ERK activation was significantly higher (p<0.05) following stimulation with 36.9 ΔcagC than with the wild type 36.9 strain at 20 and 45 min. ERK1/2 activation induced by 36.9 ΔcagL, however, did not differ from the wild type 36.9 strain.
Conclusion: In strain 7.13 the CagA protein and Hp0525 have a small role in increasing ERK1/2 phosphorylation in AGS gastric epithelial cells at early time points following stimulation with H pylori. However substantial levels of ERK phosphorylation are also induced by isogenic mutants lacking these virulence genes, and deletion of cagC increased ERK activation in strain 36.9. H pylori is thus stimulating ERK activation in a CagA/cag PAI independent manner. Strain-related differences in ERK activation are evident and the relation to gastric pathology requires further investigation.
PP110 HYDROCORTISONE AND NORADRENALINE DOWN-REGULATE THE EXPRESSION OF CONSTITUTIVELY EXPRESSED COLONIC EPITHELIAL ANTIBACTERIAL PEPTIDES
A. Javaid, J. Goodhand, D. S. Rampton. Centre for Gastroenterology, Barts and the London School of Medicine and Dentistry, London, UK
Introduction: Psychological stress worsens inflammation in inflammatory bowel disease (IBD). In experimental animals, stress increases intestinal mucosal ingress of bacteria1 and in the skin modulates the expression of antibacterial peptides (ABPs).2
Aims and Methods: To test the hypothesis that constitutively expressed ABPs are inhibited by stress and that this predisposes to relapse in patients with quiescent IBD, we have assessed the effects of three putative neurohumoral stress mediators, hydrocortisone, noradrenaline and histamine on colonic epithelial expression of human beta defensin-1 (hBD1) and lysozyme in vitro. Confluent cells from the human colon cancer-derived HT29 cell line were incubated with each of the mediators for 24 h. RNA was subsequently extracted, reverse-transcribed and gene expression of lysozyme and hBD1 determined using real-time RT-PCR. Gene expression was calculated by relative quantification against the housekeeping gene, GAPDH, and by calibrating the samples to untreated controls. For each mediator, ⩾5 samples were included in the analysis, and differences sought using the Mann–Whitney U test. Results are expressed as fold-reduction (FR) from the vehicle control-treated samples for each mediator.
Results: Hydrocortisone dose-dependently down-regulated expression of both hBD1 and lysozyme. Fold-reductions for hBD1 compared with untreated controls were FR 4.42 (mean)±0.01[SEM] for 10–9 M, and 32±7.9, p<0.01 for 10–6 M hydrocortisone; for lysozyme, the equivalent FRs were 1.19±0.53 for 10–9 M and 9.1±2.2, p<0.01 for 10–6 M hydrocortisone. Noradrenaline (10–6 M) also reduced hBD1 (FR 4.8±0.9, p<0.01) and lysozyme expression (FR 6.5±2.0). Histamine (10–6 M) had no effect on the expression of either gene.
Conclusion: These results suggest that psychological stress, by releasing hydrocortisone and noradrenaline, may down-regulate the expression of constitutive antibacterial peptides, potentially allowing bacterial ingress and precipitating inflammation in the lamina propria. The inhibitory effects on antibacterial peptide expression of hydrocortisone could underlie its tendency to cause sepsis when used therapeutically in IBD and other settings.
PP111 IN VITRO RESPONSES OF MACROPHAGES TO E COLI CHALLENGE IN CROHN’S DISEASE
1B. N. Hudspith, 1N. B. Rayment, 2N. J. Prescott, 2K. Dominy, 1G. C. Parkes, 1L. Petrovska, 1J. Brostoff, 2C. G. Mathew, 1J. D. Sanderson. 1Nutritional Sciences Division, King’s College London, London, UK, 2Medical & Molecular Genetics, King’s College London, London, UK
Introduction: The aetiology of Crohn’s disease (CD) remains unknown but a genetically determined dysregulated immune response to resident intestinal microflora is a favoured hypothesis. We and others have shown the consistent presence of viable E coli in lamina propria macrophages in patients with CD consistent with a failure in the process of bacterial clearance and an ineffective inflammatory response. The association of CD with polymorphism in genes controlling autophagy (ATG16L and IRGM) is also consistent with these findings. The cellular mechanisms involved are unclear.
Aims and Methods: To measure the response of CD peripheral blood monocytes and their derived macrophages to specific E coli strains isolated from patients. Cytokine release was measured 16 hours following challenge with E coli and a control laboratory strain (K12) in 32 CD patients and 10 health controls. This response was compared with the ability of bacteria to survive within the cells as measured by the gentamicin survival assay and with specific known genotypes (NOD2/CARD15, ATG16LI and IRMG).
Results: Four E coli isolates and the K12 strain, stimulated production of IL-8 and IL-10 with levels similar in controls and Crohn’s patients. However cells isolated from Crohn’s patients tended to release less IL-23 and TNFα than control cells. We found that the initial uptake of E coli was similar in CD and control. In control cells there was an initial growth phase cells but they were rapidly killed; however in the patient macrophages we saw a rapid replication of the bacteria (doubling time: control = 130 minutes versus CD = 54 minutes, p = 0.0034). In the majority of cases this was short lived with bacteria being undetected by 24 hours; we could isolate viable E coli up to 48 hours in 28% of the patients studied. Although we found no correlation between cytokine and survival we did note a correlation in patients homologous for the CD related polymorphism ATG16LI with a significantly lower TNFα production from monocytes compared with wild type (p = 0.01).
Conclusion: Peripheral blood myeloid cells have a reduced bactericidal capacity and TNFα production compared with those isolated from healthy subjects and this correlated with an ATG16LI polymorphism. These results appear to be at odds with the clinical situation given the effectiveness of anti-TNFα therapy in CD. However given the known compartmentalisation of the immune system these peripheral cells may reflect the early innate response whereas colonic macrophages are part of the late inflammatory stage of this disease.
PP112 AN INVESTIGATION OF MEDICATION ADHERENCE TO 5-AMINOSALICYLIC ACID THERAPY IN PATIENTS WITH ULCERATIVE COLITIS
1T. A. Moshkovska, 2M. A. Stone, 3R. Baker, 4R. M. Smith, 5J. Clatworthy, 5R. Horne, 1J. F. Mayberry. 1Digestive Disease Centre, Leicester General Hospital, Leicester, UK, 2Department of Health Sciences, University of Leicester, Leicester, UK, 3Department of Health Sciences, Leicester General Hospital, Leicester, UK, 4Department of Chemistry, Loughborough University, Loughborough, UK, 5Centre for Behavioural Medicine, University of London, London, UK
Introduction: Non-adherence to 5-aminosalicylic acid (5-ASA) therapy in patients with ulcerative colitis (UC) is an important factor in predicting disease relapse and there is some evidence that it is associated with an increased risk of developing colorectal cancer in the long term. There is a need to identify predictors of non-adherence so that these factors can be addressed.
Aims and Methods: We aimed to identify determinants and potential risk factors of non-adherence to 5-ASA therapy by patients with UC in a range of UK communities. Medication adherence was assessed using self-report questionnaires and urine sampling. Participants completed two validated questionnaires: the Beliefs about Medication Questionnaire (BMQ; Horne 1999) and the Satisfaction with Information about Medicines Scale (SIMS; Horne 2002), together with a further study-specific questionnaire. Urinary 5-aminosalicylic and N-acetyl-5-ASA were measured by high-performance liquid chromatography. Logistic regression was used to investigate predictors of self-reported non-adherence.
Results: One hundred and seventy patients from three UK sites were studied. Urine data were available for a sub-cohort of 151 cases. 34% of patients reported missing prescribed medication. Urine from 20 patients (13%) contained no detectable 5-ASA and N-acetyl-5-ASA, and 41 patients (27%) had levels well below those expected. Thirteen (14%) of the 93 people who self-reported high adherence and from whom urine data were collected had no detectable metabolites of 5-ASA in their urine. Logistic regression indicated that the independent predictors of self-reported non-adherence were South Asian (SA) ethnicity and younger age (<40 years) regardless of ethnicity (p<0.001, p<0.001 respectively). Questionnaire responses indicated that SA patients had significantly higher levels of concern about treatment than non-Asian patients (p<0.001).
Conclusion: Non-adherence with maintenance 5-ASA therapy is common in patients with UC, with younger age and SA ethnicity being predictors of non-adherence. Beliefs about medicine are potentially modifiable predictors of non-adherence.
PP113 CYCLOSPORINE ENEMA IN CONVENTIONAL±IMMUNOMODULATOR REFRACTORY DISTAL ULCERATIVE COLITIS: READY FOR PRIME TIME OR HYPE
1V. N. Mahesh, 2R. Campbell, 2N. K. Ahluwalia. 1Gastroenterology, The Royal Oldham Hospital, Manchester, UK, 2Gastroenterology, Stepping Hill Hospital, Stockport, UK
Introduction: A significant proportion of patients with distal Ulcerative Colitis (U.C) remain refractory to both steroids and immunomodulators. The role of both, intravenous and oral cyclosporine in refractory extensive U.C is well described, but there is a paucity of data on the role of cyclosporine enema in refractory distal U.C. Cyclosporine enema is considered to be safe with no systemic absorption, and hence no toxicity.
Aims and Methods: To review the role and efficacy of cyclosporine enema in refractory distal ulcerative colitis. A retrospective study. Cyclosporine enema 250 mg was specially formulated and prepared at Stepping Hill Hospital pharmacy (in the northwest of England). Patients who had failed to respond to oral and/or local 5 ASA preparations, corticosteroids and/or immunomodulators were offered cyclosporine enema. Data were collected for the periods of Jan 2000–June 2008. Composite clinical and endoscopic activity index (Mayo score-disease activity index) was calculated prior to and 4–12 weeks post cyclosporine enema administration.
Results: Altogether, 27 adults (15F: 12M); mean age 42 years (range 24 to 75 years) with refractory distal UC were offered cyclosporine enema. 8 patients had proctitis, 11 procto-sigmoidits and 8 were left-sided (up to splenic flexure) with median disease duration of 3.9 years (range 1 to 13 years). 16 (59%) patients were also on immunomodulator therapy (azathioprine 9, Mercaptopurine 3, Methotrexate 3, adalumimab 1) prior to initiation of cyclosporine enemas. All patients had endoscopic assessment prior to cyclosporine enema treatment but only 16 had post treatment endoscopy. Average Mayo scores were 8.1 (range 4 to 11) prior to initiation of therapy and 3.4 (range 0 to 6) post therapy. 21 (77.7%) patients achieved remission (defined as symptomatic improvement and endoscopic healing) on an average follow-up of 37 months. 6 (22%) patients did not respond to cyclosporine enema; 1 was re-classified as Crohn’s and treated with infliximab; the other 6 progressed to surgery. Average duration of use was 13.7 months. No major side effects were noted. 6 patients needed repeat cyclosporine enema therapy and 10 patients are being treated regularly (2–3 times/week) within the follow-up period. No patients had detectable blood levels whilst on therapy.
Conclusion: We have demonstrated a 78% response rate to cyclosporine enema in patients with refractory distal colitis. Cyclosporine enema is a safe and effective treatment in patients with refractory left-sided colitis.We recommend further large scale double-blind multi-centre randomised clinical trials before universal adoption of this otherwise safe, efficacious treatment.
PP114 HEPATITIS TREATMENT OUTCOMES OF INDIVIDUALS WITH A RECENT HISTORY OF INJECTING DRUG USE
J. M. Tait, D. Knight, J. F. Dillon. Department of Gastroenterology, Ninewells Hospital, Dundee, UK
Introduction: 80% to 90% of individuals diagnosed with Hepatitis C will be either current or former drug users. Drug users often experience multiple problems and often require support from drug services, psychiatric services and social services. Current guidelines do not restrict the use of this treatment to individuals with a recent history of substance misuse; however it is recognised that they may require more support to complete treatment.
Aims and Methods: The aim of this study was to evaluate the outcomes of Interferon and Ribavirin treatment on individuals who have injected drugs within the last 12 months. We carried out a prospective audit on all patients who had received treatment in our centre between 2004 and 2007. Exclusions included those who were co-infected with HIV or were an inmate in prison.
Results: 133 individuals received combination Interferon and Ribavirin therapy. 68.4% (91/133) had no intravenous (IV) drug use within the last 12 months, (Group 1). 31.5% (42/133) were currently under the care of Drug Problem Services and had used intravenous drugs within the last 12 months (Group 2). Genotype and sex of individuals were similar in both groups. 56% (51/91) of group 1 and 59.5% (25/42) of group 2 were Genotype 2/3. 70.3% (64//91) of group 1, and 73.8% (31/42) of group 2 were male. The mean age was slightly higher at 46.2 in group 1 as opposed to 39.1 in group 2. Overall 73.7% (98/133) completed treatment. The percentage of individuals who completed treatment was similar in both groups with 73.6% (67/91) in group 1 and 73.8% (31/42) in group 2 completing treatment. Overall sustained viral response (SVR) was 60.9%. 62.2% (57/91) in group 1 and 57.1% (24/42) of group 2 achieved a SVR and there was no statistical difference in these results. Relapses were 9.8% and 11.9% respectively.
Conclusion: Hepatitis C treatment has similar outcomes in individuals who have injected drugs within 12 months and are on opiate substation therapy compared with conventional treatment groups. Gold standard SVR rates can be achieved in HCV infected patients who have recently used IV drugs.
PP115 ALCOHOL INTAKE AND DEVELOPMENT OF GALLSTONES: AN INVERSE ASSOCIATION—A UK PROSPECTIVE COHORT STUDY
1P. J. R. Banim, 2R. Luben, 1H. Bulluck, 3N. Wareham, 3S. Sharp, 2K. Khaw, 4A. R. Hart. 1Gastroenterology, Norfolk and Norwich University Hospital, Norwich, UK, 2Institute of Public Health, 3MRC Epidemiology, University of Cambridge, Cambridge, UK, 4School of Medicine, University of East Anglia, Norwich, UK
Introduction: Alcohol may prevent gallstone formation by decreasing biliary cholesterol saturation. The magnitude of this effect has never been investigated in a cohort study using information on alcohol intake obtained from the most accurate form of dietary assessment, namely food diaries. The aim of this study was to estimate the risk reduction in a UK cohort study using food diaries and, for the first time, document the effect by units of alcohol consumed per week.
Aims and Methods: A total of 25 639 men and women, aged 45–74 years, participated in the EPIC-Norfolk Study (European Prospective Investigation into Cancer). Alcohol intake was estimated from seven-day food diaries, with detailed information on both the frequency and quantity of alcohol intake. The diaries were coded using a computer program with information on the alcohol content of 433 different drinks consisting of beers (183), wines (150), spirits (78) and liqueurs (22). The cohort was monitored for participants who developed symptomatic gallstones over a 10 year period. The analysis was performed using Cox regression to calculate a hazard ratio of developing gallstones between quartiles of alcohol intake (g/week), with the lowest quartile including both non-drinkers and those with the lowest intake. Secondly, a hazard ratio was calculated for every extra unit of alcohol/week, with all analyses being adjusted for age, gender and body mass index (BMI).
Results: During the follow-up period, 265 participants (68.3% women) developed symptomatic gallstones at a median age of 61.8 years (range 42.7 to 76.5 years). The highest quartile of alcohol intake was associated with a hazard ratio of developing gallstones of 0.68 (95% CI 0.47 to 1.0, p = 0.05). Each increase in unit of alcohol consumed per week decreased the risk of gallstones by 3% (95% CI 1% to 4%, hazard ratio = 0.97 (CI 0.96 to 0.99, p = 0.009)).
Conclusion: This study confirmed an apparent protective effect of alcohol against gallstone formation using an accurate dietary assessment method. For the first time, the precise quantitative effect for each unit of alcohol was estimated. Alcohol appears to have a protective role in preventing gallstone aetiology and should be measured accurately in epidemiological studies.
PP116 INCREASED GASTROINTESTINAL SYMPTOMS IN PATIENTS WITH ALLERGIC AIRWAYS DISEASE
1N. Powell, 1E. Ng, 1V. Loh, 2M. Walker, 1J. Hoare, 3N. J. Talley, 4O. Kon, 1T. Orchard. 1Gastroenterology, 2Histopathology, Imperial College NHS Trust, London, UK, 3Gastroenterology and Hepatology, Mayo Clinic, Jacksonville, USA, 4Respiratory Medicine, Imperial College NHS Trust, London, UK
Introduction: Patients with allergic diseases such as asthma and allergic rhinitis have been reported to have microscopic inflammatory changes in the gastrointestinal (GI) tract resembling the inflammatory reaction occurring in the airways, with accumulation of eosinophils, T-cells and pro-allergic cytokines.1 2 It is not certain whether these subtle microscopic changes of the GI tract might manifest with increased GI symptoms.
Aims and Methods: We conducted a prospective, case control study assessing GI symptoms in patients with atopic asthma and/or rhinitis compared with controls. Atopy was defined by a positive skin prick test (or RAST) and asthma was defined by reversibility of forced expiratory volume in 1 second of >15%. All patients completed a validated GI symptom questionnaire (GSRS questionnaire).3 The GSRS assesses 5 individual GI symptom complexes (reflux, indigestion, abdominal pain, constipation and diarrhoea) and yields a total GI symptoms score. We also evaluated whether GI symptoms correlated with the clinical severity of asthma, using the validated Aas score.4
Results: Data were available in 70 atopic patients and 69 controls. Our study groups were comparable with regard to age, gender, smoking history and alcohol consumption. The overall GSRS score was significantly higher in atopic patients (2.17) compared with controls (1.46), p<0.0001. For each symptom complex assessed, scores were also significantly higher in atopics compared with controls, including reflux (1.73 vs 1.34, p<0.02), indigestion (2.7 vs 1.9, p<0.0001), abdominal pain (2.4 vs 1.5, p<0.0001), diarrhoea (1.9 vs 1.3, p<0.0001) and constipation (2.0 vs 1.3, p<0.0001). The total GSRS score also significantly correlated with increasing asthma severity, r = 0.50, p<0.002.
Conclusion: Our data are consistent with the hypothesis that GI symptoms are increased in patients with atopic asthma and rhinitis. GI symptoms were also observed to escalate with increasing asthma severity. Whether these symptoms are attributable to activated eosinophils entering gut mucosal sites deserves additional research attention.
PP117 LYMPH NODE LOCATION IMPROVES THE PROGNOSTIC POWER OF OESOPHAGEAL ADENOCARCINOMA STAGING
1C. J. Peters, 2R. H. Hardwick, 3S. L. Vowler, 1R. C. Fitzgerald. 1MRC Cancer Cell Unit, Hutchison-MRC Research Centre, Cambridge, UK, 2Cambridge Oesophago-Gastric Centre, Addenbrookes Hospital, Cambridge, UK, 3Bioinformatics Core, Cancer Research UK Cambridge Research Institute, Cambridge, UK
Introduction: Despite now being the commonest oesophageal malignancy in the west, adenocarcinoma is still staged using a system developed for squamous cell carcinomas. This system does not take into account the number of involved lymph nodes and places undue prominence on the presence or absence of coeliac axis nodes, despite growing evidence they should not be considered metastatic for tumours around the gastro-oesophageal junction.
Aims and Methods: We aimed to determine if the location of involved lymph nodes in relation to the diaphragm was prognostic and then to incorporate this feature into a revised classification for oesophageal and junctional adenocarcinomas. 444 patients with oesophageal adenocarcinoma (Siewert type I and II) undergoing oesophagectomy with curative intent were randomly assigned to generation (313) and validation (131) data sets. In the generation dataset patients with involved lymph nodes on both sides of the diaphragm were compared with those with involved nodes on only one side of the diaphragm. The location of involved lymph nodes in relationship to the diaphragm and a revised classification based on number of involved lymph nodes were then combined and applied to the validation dataset to test their prognostic power.
Results: In the generation dataset lymph node positive patients with involved nodes both sides of the diaphragm have a median survival of 17 months compared with 30 months for node positive patients with involved nodes on only one side of the diaphragm (p = 0.008). This feature was combined with a revised classification incorporating the number of involved lymph nodes to produce a hybrid system: N0 = no involved lymph nodes; N1 = 1–5 involved lymph nodes on one side of the diaphragm; N2 = 6 or > involved lymph nodes OR involved lymph nodes on both sides of the diaphragm. In the validation dataset this revised system provided greater discrimination between node positive patients than the existing TNM system (p<0.001); in addition we demonstrated that patients with low nodal burden (1–5 involved lymph nodes) who were upstaged to N2 by having nodes both sides of the diaphragm had a significantly worse outcome than those who were not upstaged (p = 0.014).
Conclusion: Our revised N-stage based on number and location of involved lymph nodes provides improved prognostic power. Moreover this system incorporates features that it should be possible to assess before surgery, using clinically relevant imaging modalities.
PP118 CAN WE FIND THE MISSING HEPATITIS C PATIENTS?
J. M. Tait, S. McLeod, J. Dillon. Department of Gastroenterology, Ninewells Hospital, Dundee, UK
Introduction: The long-term consequences of the hepatitis c virus (HCV) are significant; however it is estimated that many individuals are not in contact with specialist care. In 2004 a Hepatitis C Managed Clinical Network (MCN) was formed in our region. The aim of the MCN was to improve patient centred care by introducing a new care pathway, which included open referrals and outreach clinics, and to establish a database that would establish accurate follow-up data on all HCV positive individuals in our region.
Aims and Methods: The aim of this study was to determine the number of individuals in our region who had accessed care. We carried out a retrospective cohort study on all hepatitis C antibody positive individuals tested in our region between September 1991 and 2008. We are unique in the fact that we can identify and trace individuals in the hospital and community, as they will have been allocated a Community Health Index (CHI) number.
Results: There were 1767 hepatitis C antibody individuals identified. 1331 (75.3%) were male. 23 (1.3%) had been tested as a neonate and 1292 (73.1%) tested were aged between 16 and 39. 447 (25.2%) of tests had been carried out in a GP practice, 364 (20.5%) in the Prison service, 328 (18.5%) in hospital. Follow-up HCV PCR was available on 1243 and 928 (74.6%) were positive. Transmission risk was known in 1304 and in 1122 (86%) cases this was injecting drug use. 892 (50.4%) individuals had not been referred to the specialist centre; 269 (30.1%) were dead, 164 (18.3%) were PCR negative, 118 (13.2%) had relocated from our area, 141 (15.8%) had moved Prison, 26 (2.9%) were being followed up by other units and 37 (3.6%) were unable to be traced. 137 (15.3%) are known to be in our region and had not been referred to our service. Of these, 67 (48.9%) are in contact with local drug services, 6 (4.3%) are currently in Prison and 6 (4.3%) are under the care of the Mental Health Team. 40 (29.1%) had attended their General Practitioner in the last 2 years, and 18 (13.1%) had no contact with Health Services within the last 2 years. 1021 individuals are currently within our region and 875 (85.7%) had been referred to the Specialist Service. 721 (82.4%) had attended the Specialist Clinic. 379 (52.5%) are receiving continued follow-up, 122 (16.9%) have been discharged, 44 (6.1%) are dead, 45 (6.2%) have moved from our locality, and 133 (18.4%) have been lost to follow-up.
Conclusion: Our data show that the creation of a MCN has resulted in 85.7% of individuals being referred to the clinic and 82% of referrals attending the specialist services. This demonstrates that simple service redesign within an MCN can have a radical effect at improving access to care in this traditionally hard to reach population.
PP119 A PROSPECTIVE SURVEY ON THERAPEUTIC ENDOSCOPY TRAINING FOR ENDOSCOPY NURSE ASSISTANTS
1R. Saravanan, 1C. King, 1T. Creed, 2P. Sylvester, 3A. Beale. 1Gastroenterology, 2General Surgery, University Hospitals Bristol NHS Foundation Trust, Bristol, UK, 3Gastroenterology, Royal Gwent Hospital, Newport, UK
Introduction: There are currently no mandatory formalised training courses for endoscopy nurse assistants despite the longstanding recognised need for such courses.1 The recent UK comparative audit of upper gastrointestinal bleeding emphasised the need for the appropriate skill mix for emergency therapeutic endoscopy.2 In addition, the high therapeutic burden associated with the introduction of bowel cancer screening has increased the need for highly skilled nurses.
Aims and Methods: A prospective survey on the impact of formal therapeutic endoscopy training for endoscopy nurse assistants who attended the Therapeutic Endoscopy Course for Nurse Assistants and Nurse Consultants (TECNA course). Forty eight endoscopy nurse assistants attended the Therapeutic Endoscopy Course for Nurse Assistants and Nurse Consultants (TECNA, Bristol Royal Infirmary) and were surveyed prospectively, responding to a pre (sent 2 weeks prior) and two post course questionnaires (on the day of the course and 3 months following the course).
Results:
48 delegates attended from 17 institutions.
43 (89%) delegates completed the questionnaires.
Median endoscopic experience was 3.5 years (range 0 to 15 years).
21/43 (49%) had previously attended some form of endoscopy training.
Prior to the course, 34% considered their therapeutic knowledge to be only basic.
After the course, just 5% considered their therapeutic knowledge to be only basic.
100% of the delegates felt that their practical skills had been improved by the course.
Confidence in assisting the endoscopist with therapeutic procedures increased from 21 (48%) to 38 (88%) of attendees after the course and this confidence was maintained at 3 months.
95% (41/43) of the attendees agreed that all endoscopy nurse assistants should undergo a mandatory training course within the first year of their post on joining an endoscopy unit.
Conclusion: Just over half of the endoscopy nursing staff attending had no formal training in endoscopy procedures, despite a median time working in an endoscopy unit of 3.5 years. The TECNA training course improved their confidence and ability, and this improvement was maintained for at least 3 months. Formal training for all endoscopy nurse assistants in therapeutic skills is desirable and ideally should be undertaken within the first year of joining an endoscopy unit. Funding of such courses remains the major barrier to wider uptake of such courses. Central funding for such courses should be considered.
PP120 INTESTINAL PROTECTIVE EFFECT OF A COMMERCIAL FISH PROTEIN HYDROLYSATE PREPARATION
1T. Marchbank, 2G. Elia, 1R. J. Playford. 1Gastroenterology, Barts and The London School of Medicine, Queen Mary University of London, London, UK, 2Histopathology Unit, Cancer Research UK-London Research Institute, London, UK
Introduction: A partially hydrolysed, dried, product of Pacific whiting fish is marketed as a health food supplement supporting “intestinal health” but scientific data supporting these claims are severely limited. We, therefore, examined if it influenced intestinal injury caused by the NSAID, indomethacin.
Aims and Methods: Effects of various concentrations of fish hydrolysate on proliferation ([3H]-thymidine incorporation) and indomethacin-induced apoptosis (active caspase-3 immunostaining) were determined using in vitro assays of HT29 cells. In vivo studies employed six groups of mice (n = 8/group). 4/6 groups had fish hydrolysate (25 or 50 mg/ml) supplemented to their drinking water for 7 days. All mice received a subcutaneous injection of indomethacin (85 mg/kg) or placebo, 12 h prior to killing. Small intestinal injury was assessed using morphometry and morphology and changes in proliferation and apoptosis determined using crypt BrdU labelling and active caspase-3 immunostaining.
Results: Fish hydrolysate stimulated proliferation of HT29 cells in a dose-dependent manner. Apoptosis was increased by about 3-fold following incubation with indomethacin. Co-presence of the fish hydrolysate given 2 h prior, or at the time of indomethacin administration, truncated this effect by about 40% (p<0.01). In mice, fish hydrolysate did not affect baseline morphology but reduced villus damaging effects of indomethacin by 60% (p<0.05). Indomethacin increased intestinal proliferation by 65%, irrespective of presence of hydrolysate. In contrast, intestinal caspase-3 activity increased by 83% in animals given indomethacin and placebo but this rise was truncated by 70% by co-presence of hydrolysate (p<0.01).
Conclusion: This natural bioactive product reduced apoptosis and the gut damaging effects of indomethacin.
PP121 FAECAL LACTOFERRIN, CAPSULE ENDOSCOPY AND SMALL BOWEL CROHN’S DISEASE—IS THERE A THREE WAY RELATIONSHIP? A PILOT STUDY
1R. Sidhu, 1D. S. Sanders, 2P. Wilson, 2S. Morley, 2L. Foye, 1M. E. McAlindon. 1Gastroenterology, 2Clinical Chemistry, Royal Hallamshire Hospital, Sheffield, UK
Introduction: There is a reported delay of 1–7 years in the diagnosis of Crohn’s disease particularly as conventional radiological methods are reported to have a poor yield. Capsule endoscopy (CE) has been shown to be useful in diagnosing Crohn’s disease with a reported yield of 40–70%. Parameters such as elevated inflammatory markers and family history have been suggested as factors which may help the diagnostic yield of CE. Faecal lactoferrin (FEL) has been shown to have a high sensitivity and specificity in discriminating between IBD and IBS. Based on this observation it could be suggested that FEL could be used as a marker to determine which patients should have further investigations. There have been no studies on the use of FEL in the setting of suspected Crohn’s disease using CE.
Aims and Methods: To investigate the clinical utility of faecal lactoferrin in patients with suspected Crohn’s disease using CE. Prospective data were collected on patients referred for CE with suspected Crohn’s disease. Patient symptoms (presence of abdominal pain, weight loss, diarrhoea, abdominal mass, extra-intestinal manifestations of IBD), family history and blood parameters (full blood count, albumin, elevated inflammatory markers) were noted. Patients were requested to return a stool sample, and quantitative and qualitative analysis using sandwich ELISA was performed for FEL. The expert CE reader, was blinded to the results of FEL. The data were analysed using SPSS, and sensitivity, specificity, PPV and NPV were calculated. Kendall–Tau correlation calculations were performed between lactoferrin concentrations and CE findings. Logistic regression was used to identify factors which helped to predict a positive yield with CE.
Results: Fifteen patients were recruited with 53.3% female, average age 45.7 years (range 25 to 73). All patients had more than one criterion for referral (symptoms/family history or elevated blood parameters).The diagnostic yield of CE was 40%. Sixty-seven percent of patients in this positive cohort group had an elevated FEL (correlation co-efficient 0.5, p = 0.03). The sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) of FEL using the quantitative analysis were 67%, 100%, 100% and 81% respectively. The corresponding values using the qualitative FEL (positive/negative) test were 33%, 78%, 50% and 64% respectively. On logistic regression, the presence of anaemia (p = 0.04) and an elevated FEL (p = 0.039) was helpful in predicting a positive yield with CE.
Conclusion: FEL has a high PPV and NPV for the diagnosis of small bowel Crohn’s disease, detected by CE. FEL is a useful marker (in conjunction with clinical parameters) to determine which patients should be referred for CE.
Cellular and molecular pathology posters
PM122 CHANGES IN GENE EXPRESSION IN HCT116 COLORECTAL CANCER CELLS FOLLOWING RETROVIRAL VECTOR GENE TRANSFER OF COX-2
1E. N. Fogden, 2M. Wilson, 1T. Hagen, 2C. Hodgman, 1C. J. Hawkey. 1Wolfson Digestive Diseases Centre, University of Nottingham, 2Multidisciplinary Centre for Integrative Biology, University of Nottingham, Nottingham, UK
Introduction: Increased expression of Cyclooxygenase-2 (COX-2) and the synthesis of Prostaglandin E2 (PGE2) plays a central role in the pathogenesis of colorectal cancer (CRC). The non-COX-2 expressing cell line HCT116 was used to create a pair of stably transfected cell lines with and without COX-2 expression for use in experiments to study aspirin’s effects on colorectal epithelium.
Aims and Methods: Microarray experiments were carried out to investigate the effects on gene expression from COX-2 transduction and the process of retroviral vector gene transfer. A pseudotyped lentiviral vector gene transfer technique was used to transduce murine COX-2 into HCT116 cells to create a pair of stably transfected HCT116 cell lines with and without COX-2 expression (VSV-G:COX-2 and VSV-G:Empty Vector respectively). 293GP packaging cells were transfected with Vesicular Stomatitis Virus-G envelope protein and either muCOX-2-FLAG-Puro-Marx or Puro-Marx-Empty Vector (EV) using GeneJuice (Novagen). After 72 h, fresh retroviral vector was applied to HCT116 cells with Polybrene 8 mu/ml. Neoresistant clones were picked after selection with puromycin (1 mu/ml). COX-2 expression was confirmed with Western Blotting and PGE2 synthesis demonstrated by ELISA. Cells were passaged for over 6 months prior to the gene expression experiments, and COX-2 expression was stable over this period. Total RNA was isolated from parent HCT116, VSV-G:EV and VSV-G:COX-2 HCT116 cells, labelled and hybridised to Ocimum 30 K Human arrays. Data were analysed using R software.
Results: Expression of TCF-4 and LEF-1 (transcription factors involved in the Wnt signalling pathway), c-myc (a proto-oncogene) and COX-2 was increased in COX-2 cells relative to EV. Expression of Bcl-2 (anti-apoptotic gene), 15-PGDH (the enzyme which catabolises PGE2) and the PGE2 receptor EP1 was significantly reduced in COX-2 cells compared with EV. Expression of COX-1, mPGES and EP2-4 showed no significant changes in COX-2 compared with EV. The process of retroviral vector gene transfer itself resulted in few significant changes in gene expression.
Conclusion: 15-PGDH is a tumour suppressor, and loss of expression has been shown in CRC. 15-PGDH-knockout mouse models have higher numbers of colonic tumours. These results suggest that the expression of 15-PGDH is dependent on COX-2. Several of the gene expression changes found in the VSV-G:COX-2 cell line are in genes linked to the Wnt signalling pathway, consistent with previous studies linking PGE2 to activation of the pathway. The process of retroviral vector gene transfer itself had little effect on gene expression. Retroviral vector gene transfer is a useful technique to create stably transfected cell line with long-term persistence of the gene of interest in the host cell genome.
PM123 PRIMARY PERITONEAL MESOTHELIOMA—DIAGNOSIS AND SURVIVAL IN THE 21ST CENTURY
H. Sharma, G. Bird. Gastroenterology, Maidstone General Hospital, Maidstone, UK
Introduction: Primary peritoneal mesothelioma is a rare, aggressive tumour with a median survival time of 6–12 months. Unlike pleural mesothelioma, the diagnosis and treatment are often delayed due to its non-specific clinical and radiological presentation. The main risk factor is asbestos exposure yet 50% of cases do not give a history of asbestos contact. Mesothelioma is increasing in incidence, and The British Thoracic Society predicts a peak from 2011 to 2015 with an estimated 1950–2450 deaths per year in the UK, of which about 8% will be peritoneal in origin. We present six cases of peritoneal mesothelioma, representing the largest British series.
Aims and Methods: All patients presenting over a three year period (2005–8) with primary peritoneal mesothelioma to a regional cancer centre (Kent Oncology Centre) are included. In all cases the diagnosis was made through investigation of abdominal symptoms with CT scanning and laparoscopic biopsy. Patients were offered chemotherapy if recommended by the MDT meeting after full assessment and discussion.
Results: All of the patients were aged 56–65, and all but one showed thrombocytosis (see table). All cases were classified as epithelioid subtype. Two of our cases are alive 2 years after the diagnosis despite underlying characteristics, including the histological features, tumour load and comorbidities, being similar to the other cases.
Conclusion: Diagnosis of these cases rested upon laparosopic biopsy in addition to imaging etc. Despite similarities in clinical, histological and radiological features, our patients exhibited a wide range of patterns of progression, indicating the difficulty in providing an accurate prognosis in this group. The overall prognosis of peritoneal mesothelioma is extremely poor but it is possible that survival is comparable with pleural mesothelioma (median of 8–14 months) and therefore better than stated in the BTS guidelines. A wide range of interventions have been suggested for peritoneal mesothelioma but its rarity and variability in prognosis indicate that evaluation of therapies with RCTs will be problematic.
PM124 DEGRADED RNA ISOLATED FROM BILE AND BILIARY BRUSHINGS IS SUITABLE FOR DOWNSTREAM APPLICATIONS SUCH AS QPCR
1M. H. Chapman, 2F. Andreola, 1N. Sandanayake, 2V. Cerec, 3J. Dooley, 1S. P. Pereira. 1Institute of Hepatology, University College London and UCL Hospitals NHS Trust, London, UK, 2Institute of Hepatology, University College London, London, UK, 3Centre for Hepatology, UCL Medical School (Royal Free Campus), London, UK
Introduction: RNA isolated from bile or biliary brushings taken at ERCP is highly degraded. Advances in molecular biology now permit degraded RNA to be used in downstream applications such as real time quantitative polymerase chain reaction (qPCR) and microarray analysis.
Aims and Methods: We aimed to assess whether: (i) RNA isolated from bile or biliary brushings is useful for qPCR; and (ii) bile or x ray contrast (Omnipaque) could be responsible for the RNA degradation observed in detached cells. Fresh bile and brushings taken at ERCP were snap frozen in liquid nitrogen. TFK-1 cells (a cholangiocarcinoma cell line) were cultured for 0 to 24 hours in filtered bile or Omnipaque solution (25% or 50%). RNA samples were isolated using TRI reagent and treated with DNase I followed by spin column purification. RNA was quantified by NanoDrop spectrophotometer and its quality assessed by both gel electrophoresis and Agilent 2100 Bioanalyzer. cDNA synthesis reactions were primed with random hexamers. qPCR was performed using SYBR Green dye. The expression of the housekeeping gene GAPDH was assessed using three sets of primers producing amplicons of variable length (87, 130 and 220 bp). Amplification of genes expressed by biliary epithelial cells (CK19 and EGFR), as well as CD45 (to exclude leucocytes as the major source of RNA in clinical samples), was also performed.
Results: RNA isolated from bile and biliary brushings was of variable quantity (100–1500 ng), relatively poor quality (RNA Integrity Number (RIN) <5) and highly degraded, as assessed by agarose gel electrophoresis and Agilent Bioanalyzer electropherogram. In contrast, RNA samples isolated from TFK-1 cells cultured for at least 6 hours in bile or Omnipaque solution were of excellent quality (RIN>8.5). In bile and biliary brushings, RNA fragments were estimated to be primarily 100 to 600 base pairs long. When assessing GAPDH mRNA expression in the clinical samples, the lowest Ct values (ie, greatest amplification) were consistently obtained using primers for the short 87 bp amplicon; however, due to the RNA degradation, Ct values rose significantly in a stepwise fashion when primers generating larger amplicons were used. In contrast, stable Ct values were observed when amplifying GAPDH from intact control RNA (TFK cells), regardless of the primer set used. When assessing other genes of interest, appropriate Ct values were obtained in both control and clinical samples using primers amplifying regions <100 bp.
Conclusion: Despite being highly degraded, RNA isolated from bile and biliary brushings is suitable for downstream applications such as qPCR using appropriately designed primers amplifying regions shorter than 100 bp. These data suggest that RNA isolated from bile and biliary brushings should also be useful for high throughput techniques such as gene expression arrays.
PM125 SUCCESSFUL AMPLIFICATION OF CYTOKINE RNA FROM CROHN’S DISEASE-DERIVED, E COLI-LADEN LAMINA PROPRIA MACROPHAGES ISOLATED BY LASER CAPTURE MICRODISSECTION (LCM)
N. B. Rayment, B. Hudspith, L. Petrovska, G. Parkes, J. Brostoff, J. Sanderson. Nutritional Sciences Research Division, King’s College London, London, UK
Introduction: Intestinal macrophages are important in the regulation of gut homeostasis. We and others have reported the persistence of strains of E coli in lamina propria macrophages in patients with Crohn’s disease (CD). These macrophages appear unable to complete the normal lysosomal process of bacterial killing and therefore viable (culturable) bacteria persist within these cells. Studies of CD associated E coli show only low grade pathogenicity in keeping with hypothesis that there is a primary macrophage defect enabling bacterial persistence rather than a property of the E coli themselves.
Aims and Methods: We have investigated the feasibility of applying laser capture micro-dissection (LCM) of intestinal macrophages to investigate differences in the cytokine profile of bacteria laden and bacteria free macrophages isolated from CD patients. Snap frozen mucosal biopsies were taken at routine colonoscopy from patients with CD and controls with normal colorectal mucosa. Using LCM combined with immuno-histochemistry (IHC), CD-68 positive macrophages containing clusters of E coli and those free of bacteria were identified, captured and total RNA extracted. The methodology was then optimised to obtain RNA of sufficient purity to permit successful qRT-PCR using specific primer pairs to amplify cytokine RNA.
Results: RNA could be successfully extracted from laser dissected macrophages which was of sufficient quality and quantity in order to perform qRT-PCR to amplify IL-1, TNFα, iNOS, COX-2 and GM-CSF RNA. Preliminary analysis shows down-regulated expression of the pro-inflammatory cytokine IL-1 in E coli containing macrophages compared with those free of bacteria and controls.
Conclusion: As a proof of concept, we have shown that LCM can be successfully applied to isolate E coli laden macrophages from the lamina propria in CD and specific cytokine RNA amplified. Altered expression of cytokines in E coli containing macrophages may support the hypothesis of an innate defect permitting bacterial persistence in CD.
PM126 B CELLS IN THE PATHOGENESIS OF THE OROFACIAL GRANULOMATOSIS/ORAL CROHN’S DISEASE SPECTRUM
1P. Patel, 2F. Barone, 2L. Boursier, 3C. Nunes, 4E. Odell, 5M. Escudier, 5S. Challacombe, 3J. Brostoff, 2J. Spencer, 3J. Sanderson. 1Nutritional Sciences Division, King’s College London, London, UK, 2Immunobiology, 3Nutritional Sciences Division, 4Oral Pathology, 5Oral Medicine, King’s College London, London, UK
Introduction: The oral mucosa is an immunologically responsive site associated with the generation of protective mucosal and systemic immune responses to vaccination and also hyper-responsiveness to allergens in some individuals. Classically, immune responses in oral mucosa are considered to be mediated by mucosa-associated lymphoid tissues (MALT), secondary lymphoid follicles that are intimately associated with epithelia. Orofacial granulomatosis (OFG), which includes oral Crohn’s disease, is a chronic inflammatory condition presenting characteristically with lip swelling but also affecting a number of other sites in the oral cavity. Although the cause remains unknown, dietary triggers and allergic phenomena are established features.
Aims and Methods: To investigate the B cell component of the inflammatory infiltrate in OFG.
Methods: Using immunohistochemistry and PCR on paraffin embedded (n = 44) and fresh frozen (n = 8) oral mucosal biopsies, we characterised in detail the B cell component of the inflammatory infiltrate in OFG (n = 14) and a variety of non-OFG inflammatory oral conditions (n = 38).
Results: CD20 staining revealed large, active, dendritic B cells in oral mucosa, closely associated with other cellular components of the immune response such as T cells and macrophages. They were not associated with any organised lymphoid tissues in the local subepithelial microenvironment. These B cells expressed Activation Induced cytidine Deaminase (AID), essential for immunoglobulin gene diversification by somatic hypermutation and class switch recombination. AID transcripts were also demonstrated in frozen oral biopsies by PCR. They were negative for naïve B cell markers and a proportion (10%) expressed the nuclear proliferation marker, Ki67. These dendritic B cells also expressed surface IgE and this expression was significantly greater in OFG compared with other oral conditions (mean % of B cells expressing surface IgE 6.5% vs 0.2%; p<0.0001). Epsilon transcripts, which provide further evidence for IgE production locally, were also demonstrated in the single frozen OFG biopsy by PCR.
Conclusion: Subepithelial dendritic B cells described here do not align with any other previously described B cell subset in secondary lymphoid tissues in terms of morphology, proliferative activity or phenotype. We propose that these cells contribute to the immune responsiveness of the oral mucosa including IgE mediated allergic responses, notably in OFG but also in other oral inflammatory disease.
Endoscopy posters
PM127 DOUBLE BALLOON ENTEROSCOPY—TOLERABILITY IN 119 CASES, WHO NEEDS PROPOFOL?
A. Deo, S. Hughes. Gastroenterology, North Bristol NHS Trust, Bristol, UK
Introduction: Double balloon enteroscopy (DBE) is a difficult, time-consuming and uncomfortable procedure. There is no consensus regarding sedation. Sedation with propofol, midazolam and pethidine as well as general anaesthesia have been used in different centres. We present our experience of 137 consecutive cases where patients were sedated with a combination of midazolam and pethidine.
Aims and Methods: 137 procedures were performed in our endoscopy unit as a day case. All procedures were performed under conscious intravenous sedation using a combination of midazolam and pethidine. Initial doses were midazolam 5 mg and pethidine 50 mg given intravenously. Additional midazolam was given in 1 mg boluses. Sedated patients were monitored in the standard way in accordance with local guidelines. Tolerability was assessed using a 3-point scale and assessed independently by the endoscopist and 2 nurses and agreed at the end of the procedure. Well tolerated was defined as patient being comfortable throughout the procedure. Moderately well tolerated was defined as patient being uncomfortable at times and the examination was not curtailed. Poorly tolerated was defined as patient uncomfortable most of the time and the procedure was curtailed.
Results: Tolerability data were calculated on 119 procedures (75 via the oral route and 44 via the rectal route). DBE was well tolerated in 94 patients (80%), moderately tolerated in 19 patients (15%) and poorly tolerated in 6 patients (5%). DBE via the oral route was well tolerated in 57 (76%) patients, moderately tolerated in 12 (16%) patients and poorly tolerated in 6 (8%) patients. DBE via the rectal route was well tolerated in 37 (84%) patients and moderately tolerated in 7 (16%) patients. There were no patients whose tolerance was poor via the rectal route. 135 patient’s data were used to calculate averages for age, time taken and drug doses. Data were incomplete in 2 procedures and therefore discarded. The average dose midazolam used was 9 mg for the oral route and 6 mg for the rectal route. The average dose of pethidine was 50 mg for both routes. Average time taken for the DBE was 50 and 62 minutes for oral and rectal routes respectively. One patient required reversal of sedation with Flumazenil. The average age of patients was 61 and 60 years for oral and rectal routes respectively. Seventy-four males and 61 females were included in the study; the average age of males was 60.09 years (32–84 years) and for females 60.61 years (41–89 years). There were no complications in this series of patients.
Conclusion: Double balloon enteroscopy is a safe and well tolerated procedure under conscious intravenous sedation using a combination of pethidine and midazolam. DBE via the oral route was shorter in duration and less well tolerated than DBE via the rectal route. There were no complications and the procedure can be safely performed as a day case.
PM128 EUS-GUIDED CYSTOGASTROSTOMY FOR PANCREATIC PSEUDOCYSTS; ANALYSIS OF A CASE SERIES USING MINIMAL ENDOSCOPIC PROCEDURES
1A. D. Farmer, 2S. Menon, 3S. Kapadia, 2N. C. Fisher. 1Wingate Institute of Neurogastroenterology, Barts and the London, Whitechapel, UK, 2Department of Gastroenterology, Russell’s Hall Hospital, Dudley, UK, 3Department of Gastroenterology, New Cross Hospital, Wolverhampton, UK
Introduction: EUS-guided cystogastrostomy is a valuable technique for drainage of persistent pancreatic pseudocysts. Practice varies in terms of the number of endoscopic procedures that are planned for a successful outcome. Herein we review our own experience of using a limited number of interventions.
Aims and Methods: The aim of this study was to evaluate the technical success and complication rates of EUS-guided cystogastrostomy at our institution. A retrospective case note review was done of all cases of attempted cystogastrostomy. The procedure was performed with a linear echoendoscope and using a cystotome cannula (Cook UK). One or two guidewires were inserted under fluoroscopic guidance to facilitate placement of 1 or 2 stents. For recent cases we have adopted routine usage of a nasocystic drain in place of 1 stent. Further endoscopic intervention was not routinely planned.
Results: Twenty-two procedures were performed on 20 patients including 2 cases of late cyst recurrence (median age 52, range 15–78 years). Median pseudocyst size was 10.1 cm×8.3 cm. Cyst puncture was successful in 21 out of 22 cases; of these, stent insertion was successful in 20 out of 21 patients (9 patients had a single stent, 9 patients had twin stents and 4 patients had single stent and nasocystic drain). One procedural complication occurred (pneumothorax, 1 patient). Seven cases required further intervention within 30 days (4 endoscopic, 2 radiological and 1 surgical intervention); all of these cases had sepsis due to incomplete cyst drainage and most (5/7) were early pseudocysts (<3 months after first presentation); in each case re-intervention was successful. Stents were removed after a median of 19 weeks.
Conclusion: EUS-guided cystogastrostomy with twin stents or stent/nasocystic drain was successful in most cases in this series. There is a small but important risk of complications requiring further intervention with this approach, especially if intervention is done early in the disease course.
PM129 COLONOSCOPY SKILLS TRANSFER FROM A SECOND-GENERATION VIRTUAL REALITY SIMULATOR TO PATIENTS: A MULTINATIONAL RANDOMISED BLINDED CONTROLLED TRIAL
1A. V. Haycock, 2A. D. Koch, 3P. Familiari, 4F. van Delft, 5J. S. Bladen, 4E. Dekker, 3L. Petruziello, 2J. Haringsma, 1S. Thomas-Gibson. 1Wolfson Unit for Endoscopy, Imperial College London, London, UK, 2Department of Gastroenterology and Hepatology, Erasmus Medical Centre, Rotterdam, The Netherlands, 3Digestive Endoscopy Unit, Catholic University—A.Gemelli University Hospital, Rome, Italy, 4Department of Gastroenterology and Hepatology, Academic Medical Center, Amsterdam, The Netherlands, 5JSB Medical Systems, Sheffield, UK
Introduction: Training on virtual reality simulators has been shown to improve skills for novice endoscopists compared with no training. To date simulators have not accurately modelled colonic looping and its management, which is a key factor in skills development. A second-generation colonoscopy simulator has been specifically designed to model colonic looping and has the potential to teach knowledge and skills as effectively as standard training with no risk to patients and minimal instructor input. The Olympus colonoscopy simulator was assessed for training in transferrable skills.
Aims and Methods: 37 novice trainees from four centres in the UK, Italy and The Netherlands were pre-assessed on the simulator using three previously validated test cases. They were randomised to receive 16 hours’ training on the simulator (subjects, N = 19) or on patients (controls, N = 18) in a standardised fashion. All participants were then re-assessed on the same three simulator test cases and on three patient test cases by blinded expert endoscopists using validated assessments.
Results: On simulator test cases, subjects achieved significantly better post-training results on previously validated metrics such as completion rate (95% vs 70%, p = 0.001), completion time (407 vs 743, p = 0.001) and loop resolution (p<0.001) than the controls. They also demonstrated superior technical skills on safety aspects such as excessive insertion with an embedded tip (35% vs 74%, p<0.001) and obscured lens (5% vs 41%, p<0.001), and on patient factors such as maximum patient pain scores (0.24 vs 0.45, p = 0.002). On the patient test cases, the subjects achieved equivalent success in terms of completion rates (11% vs 7%, p = 0.51), distance intubated (48 cm vs 52 cm, p = 0.35), Directly Observed Procedure Scores (16 vs 18, p = 0.92) and Global Scores (16 vs 17, p = 0.35). Much less instructor time (4 hours vs 16 hours), organisation and effort was required for training in the simulator group.
Conclusion: There is excellent skills transfer from the simulator to real colonoscopy. The simulator trained group demonstrated equivalent performance outcomes on real patients, suggesting initial training can effectively be employed utilising a simulator rather than real patients. This would reduce the burden both on patients and on instructors. The simulator should be considered as a valuable training and assessment tool in the development of colonoscopy skills.
PM130 ENDOSCOPY TRAINING IN 2008: RESULTS FROM THE TIG/BSG NATIONAL TRAINING SURVEY
A. V. Haycock, P. Flanagan, A. Ignjatovic, S. Kendrick, R. Mead, P. Mizen, M. Mottershead, V. Patel, K. Pollock, T. Valliani, J. Williams. Trainees Committee, British Society of Gastroenterology, London, UK
Introduction: The 2004 national survey of gastroenterology trainees revealed wide variation in both the quality and quantity of training in endoscopy. The level of supervision was of particular concern, with 55% of trainees saying they were not being supervised for over half their procedures. Since that time, the UK National Endoscopy Training Programme has aimed to standardise training and assessment. Central funding for 3 years provided JAG accredited courses free of charge to trainees. Training-the-trainers courses were implemented to improve the quality of training at base hospitals. Summative and formative assessments are now mandatory to document competency.
Aims and Methods: The aim of the 2008 survey was to investigate the impact of these changes and gather data on current standards of teaching, training and supervision in endoscopy. A web-based questionnaire was developed with questions in eight domains including endoscopy. An invitation to complete the survey was emailed by the regional TiG representatives to all trainees in their region. Data were collected during October 2008.
Results: 249 out of 411 trainees from 20 different training regions completed the survey (response rate 60.6%). 217 (88.6%) were in general gastroenterology posts. 115/220 (52.3%) attend the recommended minimum of 2 endoscopy sessions per week, although only 43% of these are dedicated training lists, and 37% of trainees say that training actually occurs less than half the time. Eighteen per cent of trainees say they have no dedicated training lists at all. 79% of trainees had been on at least one accredited training course. Only 95/223 (43%) routinely get formative DOPS filled in for their lists, and 52% have not yet had any kind of summative DOPS. 184/236 (78%) are fairly or very satisfied with their endoscopy training so far, with only 5/236 (2.1%) very unsatisfied. By far the most common complaint from trainees was lack of access to regular supervised training lists.
Conclusion: The majority of trainees are satisfied with their current training, although the provision of training lists does not seem to have changed substantially since 2004 and is the main cause of concern for trainees. Less than half of trainees routinely use DOPS forms during their training lists, which should be addressed by training leads, as it is now a requirement for annual RITA appraisal.
PM131 DEVELOPMENT AND IMPLEMENTATION OF A STANDARDISED, EVIDENCE-BASED COLONOSCOPIC TATTOOING PROTOCOL
1A. V. Haycock, 2R. H. Kennedy, 1S. Thomas-Gibson, 1B. P. Saunders. 1Wolfson Unit for Endoscopy, St Mark’s Hospital, Imperial College London, London, UK, 2Department of Surgery, St Mark’s Hospital, Imperial College London, London, UK
Introduction: Placing tattoos in the colon is now common practice in order to mark lesions prior to surgery or for endoscopic follow-up. A recent audit in our unit showed wide variation in the technique used as well as the number and placement of tattoos. Published studies confirm such variation in technique as well as subsequent variation in serosal visualisation at surgery.
Aims and Methods: The aim was to develop a standardised, evidence-based protocol for tattooing during colonoscopy and to review its use in practice in a single unit. A review of the literature was performed regarding all aspects of endoscopic tattoo placement. A standardised protocol was drawn up utilising the evidence base by experienced colonoscopists and colorectal surgeons. The procedure involves a “no-spill technique” with a saline lift to minimise leakage and resulting complications. To maximise visualisation at surgery (particularly at laparoscopy) three tattoos are placed at 120 degrees to each other 3 cm from the lesion. Site of placement (distal for right sided lesions, proximal for left sided lesions and distal for rectosigmoid lesions) facilitates surgical decision making regarding resection margins. The protocol was presented at an endoscopy user meeting, distributed by email to all endoscopists and displayed in all endoscopy rooms. A prospective database was kept of all tattoos placed.
Results: In 10 months, tattoos were placed during colonoscopy on 53 occasions; 29 (55%) for suspected malignancy and 24 (45%) for polyp follow-up. Overall compliance with all aspects of the protocol (documentation, number and location) was 45.3%. For cancers, documentation of the location and number of tattoos was 96.6% and 93.1% respectively, with location and number both compliant with the protocol on 65.5% of occasions. For polyp follow-ups, documentation of the location and number of tattoos was 83.3%, with only 20.8% compliant with the protocol.
Conclusion: Compliance with the protocol was more likely with suspected cancers compared with polyp follow-up. Re-education of endoscopists is needed before investigation of the efficacy of the prococol in terms of visualisation at surgery can be undertaken.
PM132 DO OUTLIERS FACE A GREATER RISK OF HARM? A COMPARISON OF PATIENTS TREATED FOR ACUTE UPPER GASTROINTESTINAL (UGI) BLEED ON A SPECIALIST OR OUTLYING WARD
A. Ireland, A. Baldwin, M. Renshaw. Digestive Diseases, Royal Sussex County Hospital, Brighton, UK
Introduction: The term outlier refers to hospital in-patients who occupy a different specialty bed to that of their admitting specialty. Outliers are assumed to face a greater risk of harm than patients treated on specialist wards, and evidence suggests outliers face a longer in-patient stay. This hypothesis was tested by comparing mortality rate, length of hospital stay and time to endoscopy of patients with acute UGI bleed treated on an outlying ward to patients treated on a specialist gastrointestinal ward.
Aims and Methods: Retrospective analysis of clinical information systems and case note review were undertaken to identify patients presenting from June 2006 to May 2007 with a confirmed diagnosis on admission of acute UGI bleed. Two criteria were used to categorise patients as ideal or outlier. Criterion 1 (C1) defined ideal patients solely by appropriate ward location, and Criterion 2 (C2) defined ideal patients by appropriate ward location and a time to endoscopy of less than 24 hours from admission. Any patient who did not fit either ideal criterion was classified as an outlier. Retrospective calculation of a patient’s Rockall Score allowed patients to be matched for severity of bleed.
Results: 171 patients were identified. Over two-thirds were classified as outliers (C1: 70.8%, 121/171; C2: 78.4%, 134/171). Overall mortality was 9.4%. Mortality for C1 was 12.0% (6/50) for ideal patients and 8.3% (10/121) for outliers (p = 0.563). For C2, mortality was 13.5% (5/37) for ideal patients and 8.2% (11/134) for outliers (p = 0.343). Of those undergoing endoscopy, 73.7% of ideal patients did so within 24 hours of admission (28/38) compared with 64.1% of outlying patients (50/78) (C1: p = 0.302). In-patient mortality was reduced significantly when endoscopy was performed within 24 hours (all patients), 1.28% vs 10.52%, p = 0.039, as was length of stay (all patients) (<24 hours 4.58 vs >24 hours 8.08 days, p = 0.002). C2 outlying patients had a significantly longer length of stay (Ideal 4.16 vs Outlier 5.93 days, p = 0.034) and fewer medical reviews per day (Ideal 2.74 vs Outlier 2.00 reviews/day, p = 0.034). There was no significant difference in length of stay between ideal and outlying patients by C1 (Ideal 4.88 vs Outlier 5.82 days, p = 0.264) or in the number of medical reviews per day (C1: Ideal 2.52 vs Outlier 2.01 reviews/day, p = 0.065).
Conclusion: There was no significant difference in mortality rate between outliers and ideal patients. There was however a significant reduction in mortality in patients undergoing endoscopy within 24 hours. Criteria 2 patients had a significantly shorter in-patient stay and a higher number of medical reviews. The classification of outliers however remains problematic.
PM133 INTENSIVE DAY CASE COLONOSCOPY FOR THE UNRELIABLE, FRAIL OR ELDERLY PATIENT
1A. Ghanbari, 1T. T. C. Cuming, 2A. A. B. Ballinger, 1H. H. P. Pardoe. 1Academic Gastroenterology, Homerton University Hospital, London, UK, 2Gastroenterology, Queen Elizabeth the Queen Mother Hospital, Margate, UK
Introduction: We observed that many patients admitted for an inpatient bowel preparation prior to colonoscopy were still badly prepared and commonly stayed more than scheduled overnight admission.
Aims and Methods: The objective of our study was to see if it is safe, feasible and acceptable for patients who are normally admitted as an inpatient for bowel preparation to undergo day stay full bowel cleansing using an oral polyethylene glycol (PEG) Klean-prep solution and same day colonoscopy without needing hospital admission. Patients who would fulfil the criteria in our institution for in patient bowel preparation prior to colonoscopy were admitted to the endoscopy unit and underwent bowel cleansing in the morning using an oral PEG solution followed by colonoscopy in the afternoon and discharge on the same day. The first 10 patients were interviewed at the end of the procedure to assess the procedure for patient acceptability. All colonoscopies using an intensive day case regime with PEG Klean Prep were assessed using GRS criteria for quality control.
Results: Patients who would fulfil the criteria in our institution for in patient bowel preparation prior to colonoscopy were admitted to the endoscopy unit and underwent bowel cleansing in the morning using an oral PEG solution followed by colonoscopy in the afternoon and discharge on the same day. The first 10 patients were interviewed at the end of the procedure to assess the procedure for patient acceptability. All colonoscopies using an intensive day case regime with PEG Klean Prep were assessed using GRS criteria for quality control.
Conclusion: 43 patients have now undergone intensive day case colonoscopy. The unadjusted completion was 90.2% and 91.5% for the Klean prep and inpatient bowel preparation groups respectively. The bowel preparation was classified as satisfactory or good in 76.7% of Klean prep cases and only 40% inpatient cases. Polyp detection for the Klean Prep group was 44.2% compared with 20% for the inpatients. The total bed occupancy rate for elective colonoscopy was reduced from 184 days to 0 over a 12 month period. Ninety per cent of patients interviewed found the process acceptable and preferred Klean-prep as their method of bowel cleansing.
PM134 OPTICAL BIOPSY AT COLONOSCOPY: ARE WE READY? DISCARD STUDY: EARLY RESULTS
1A. Ignjatovic, 1N. Suzuki, 1M. Vance, 2T. Guenther, 1N. Palmer, 1B. P. Saunders. 1Wolfson Unit for Endoscopy, St Mark’s Hospital, Harrow, UK, 2Department of Academic Pathology, St Mark’s Hospital, Harrow, UK
Introduction: 90% of polyps removed at colonoscopy are <10 mm in size, and only 50% of these are neoplastic. The number of neoplastic polyps is the key determinant of future surveillance intervals, and small adenomas, especially those less than 5 mm in size, rarely contain advanced pathology. Accurate characterisation of small polyps in vivo could reduce the number of unnecessary polypectomies, reduce the need for polyp retrieval and greatly reduce histopathology costs. Accurate characterisation of small polyps in vivo is feasible, with a number of studies reporting accuracy around 90% when using magnification, chromoendoscopy or narrow band imaging (NBI). However the ability to make clinical decisions based on optical biopsy has not been investigated.
Aims and Methods: This prospective study examined whether colonoscopists could accurately assess small polyps in vivo and determine appropriate surveillance intervals based on real time optical biopsy. Consecutive patients attending for colonoscopy (FOBT positive or adenoma surveillance) were included. Four endoscopists with varying experience of optical biopsy performed all the colonoscopies. Once a polyp <10 mm was encountered, the endoscopist predicted polyp histology using one or a combination of optical modalities (high-definition white light alone, NBI or indigocarmine chromoendoscopy). At the end of the procedure, future surveillance intervals based on optical biopsies were determined according to BSG guidelines. Optical diagnosis was compared with histopathology findings. The primary outcome measure was the accuracy of optical polyp characterisation and clinical decision making (ie, to resect or leave polyps in situ). A secondary outcome was any change in surveillance interval following histopathological assessment.
Results: 168 (out of 296 planned) polyps smaller than 10 mm (mean size 3.5 mm, range 1–9 mm SD 2.2) were found in 57 patients. Histology was available for 141 lesions—85 adenomas, 38 hyperplastic polyps, 1 inflammatory, 3 lymphoid follicles and 14 normal. 92% (78/85) of adenomas and 95% (36/38) of hyperplastic polyps were correctly diagnosed by optical biopsy. In 82/86 (95%) cases the decision to resect and discard the polyp could be considered correct. Two adenomas contained high-grade dysplasia—in both of these cases, the colonoscopist predicted the diagnosis of adenoma and elected to resect and discard but the subsequent colonoscopy surveillance interval was unaffected. Following BSG Guidelines for polyp surveillance, 0/57 patients had their predicted surveillance interval changed after formal histopathology.
Conclusion: Optical biopsy using HR WLE, with optional use of NBI and chromoendoscopy is feasible and safe, with accuracy comparable with conventional histopathology. These preliminary data suggest the potential for a fundamental change in colonoscopic practice with major benefits in terms of procedural efficiency.
PM135 EN-BLOC RESECTION OF MULTIPLE TYPE I GASTRIC CARCINOID TUMOURS BY ENDOSCOPIC MULTI-BAND MUCOSECTOMY
1A. D. Hopper, 1M. J. Bourke, 2L. F. Hourigan, 1K. Tran, 1M. P. Swan. 1Endoscopy, Westmead Hospital, Sydney, 2Endoscopy, Princess Alexandra Hospital, Brisbane, Australia
Introduction: Gastric carcinoid tumours are rare but increasing in incidence. Current recommendations suggest endoscopic resection for type I carcinoids found in the stomach; however reports of incomplete resection have led to difficulty planning future management.
Aims and Methods: Our purpose was to describe the application of the endoscopic multi-band mucosectomy (MBM) device to achieve en-bloc resection of multiple gastric carcinoid tumours. Over a 2-year period (June 06–August 08) 6 patients attending for endoscopic assessment of gastric carcinoid tumours were identified at two tertiary referral centres. Patients underwent endoscopic resection of the carcinoids with a MBM device. En-bloc specimens underwent histological evaluation for identification and tumour resection margins. Patients had a maximum of 6 carcinoids removed at one gastroscopy. After the initial treatment session, a repeat gastroscopy was performed at 3 monthly intervals to remove any remaining tumours and/or check the resection sites. If no further carcinoids were identified then patients were enlisted into surveillance endoscopy at 12 month intervals if type I carcinoid lesions were confirmed.
Results: A total of 29 gastric carcinoid tumours were removed from 6 patients. One patient (number 6: table) underwent 3 treatment sessions to remove all initial carcinoids. This same patient and another patient had further carcinoids resected at a yearly follow-up gastroscopy (table, patient 5 and 6). On histological analyses 5 out of 6 patients were diagnosed with type I tumours. In the remaining patient a single, sporadic (type III) gastric carcinoid was diagnosed. All specimens were shown to have clear deep and peripheral histological resection margins.
Conclusion: Complete “en-bloc” endoscopic resection of multiple “type I” gastric carcinoid tumours can be safely and easily performed with a MBM technique.
PM136 ENDOSCOPIC BILIARY MANOMETRY: THE END JUSTIFIES THE MEANS
A. Dias, N. Ali, C. C. Ainley. Department of Gastroenterology, Royal London Hospital, London, UK
Introduction: Sphincter of Oddi dysfunction (SOD) is a clinical syndrome of biliary or pancreatic obstruction related to mechanical or functional abnormalities of the sphincter of Oddi. Even though there are the Rome III guidelines1 for the investigation and management of SOD, patients may present with a variety of symptoms which may be biliary, pancreatic, mixed or atypical in nature, and this may make diagnosis difficult. Unless patients meet all these criteria, the recommendation is that they should not undergo invasive investigations. Endoscopic biliary manometry (EBM) is a technique for measuring the biliary and pancreatic pressures and can determine treatment which is usually endoscopic sphincterotomy or Botulinum toxin injection.
Aims and Methods: The Royal London Hospital is a tertiary referral centre for SOD, and this study was a retrospective audit of patients referred here for the investigation of SOD and who underwent EBM. The audit involved patients who had EBM from 1st January 2004 to 31st July 2008 and looked at the long-term outcomes and complication rates.
Results: 131 patients (104 females) underwent EBM during this period. 60 patients had biliary symptoms, 21 had pancreatic symptoms, 23 had mixed biliary and pancreatic symptoms and 27 had atypical abdominal symptoms. Overall 63% of patients had some improvement of symptoms, and long term no one had worsening of symptoms post EBM. The Rome III guidelines do not include atypical patients for the investigation of SOD. However in our study, 11 patients in the atypical group had elevated biliary or pancreatic duct pressures (>40 mm Hg) of which 6 underwent sphincterotomy and 9 patients had ampullary Botulinum toxin injection. Eleven of the atypical patients showed some improvement following EBM. Of the atypical group, two patients developed post-ERCP pancreatitis, and one patient suffered a fatal guide wire perforation. In total, 19 patients developed post-ERCP pancreatitis (12 following sphincterotomy and 5 post-Botulinum toxin injection), and 5 patients developed perforation.
Conclusion: Rome III guidelines for the diagnosis of SOD are unnecessarily restrictive and therefore may lead to the under-diagnosis and treatment of this condition. Many patients, who may not fit these criteria, including those with atypical symptoms, may potentially benefit from undergoing EBM.
PM137 CAECAL INTUBATION WITH A GASTROSCOPE FOLLOWING AN INCOMPLETE COLONOSCOPY—IS IT FEASIBLE?
B. Paranandi, N. Anglim, A. Sawyerr, E. Carty, E. Seward. Department of Gastroenterology and Hepatology, Whipps Cross University Hospital, London, UK
Introduction: It is common practice in the majority of endoscopy units in the UK to use shorter, more flexible endoscopes in order to complete a difficult colonoscopy. Current published data are very limited but suggest that this may achieve caecal intubation in up to 62% of cases.1
Aims and Methods: Between October 2005 and October 2008, the endoscopy reports of all patients undergoing colonoscopy at WXUH with a conventional gastroscope were audited. These patients were identified from our database using the departmental reporting tool. A broad range of variables were assessed including total number of procedures, indication for endoscopy, caecal/terminal ileum (TI) intubation rate, reasons for failing to complete an examination and sedation usage.
Results: During the audit period, there were 7495 colonoscopies undertaken, 94 of which were performed using gastroscopes (1.3%). Seven procedures were excluded from our results because they were performed on resected colons. The most common documented indication for switching from a colonoscope to a gastroscope was complex diverticular disease in 36/87 [41%]. Of the 87 procedures we audited, the caecal intubation rate was 69/87 [79%] and the TI intubation rate was 40/87 [46%]. Using conventional colonoscopes, the caecal and TI intubation rates of our unit are 91% and 62% respectively. In the 18 [21%] cases where there was failure to complete the colonoscopy even with a gastroscope, the main identifiable causes included diverticular disease [50%], looping [22%] and strictures [22%]. Sedation usage was less than or equal to 2 mg of midazolam per procedure in 72/87 [83%].
Conclusion: Gastroscopes can be useful when trying to complete a difficult colonoscopy. We have shown that this is especially the case in complex diveticular disease. The completion rate with gastroscopes in our unit exceeds that of other studies.
PM138 ISOLATED IRON DEFIENCY ANAEMIA: AT WHAT LEVEL OF HAEMOGLOBIN SHOULD WE INVESTIGATE?
1C. C. Henson, 2A. Saeed. 1Gastroenterology, Royal Preston Hospital, Preston, UK, 2Gastroenterology, Queen Elizabeth Hospital, Gateshead, UK
Introduction: Upper and lower GI endoscopy is the gold standard investigation for isolated iron deficiency anaemia. The National Institute for Clinical Excellence (NICE) guidelines1 advise investigation of isolated iron deficiency anaemia with upper and lower GI endoscopy at levels of <11 g/dL Hb for men of any age and <10 g/dL Hb for post-menopausal women in the absence of another obvious cause. The British Society of Gastroenterology (BSG)2 advises such investigation when haemoglobin levels fall below the lower limit of the normal range.
Aims and Methods: This retrospective study aims to determine the level of haemoglobin below which investigation of iron deficiency anaemia should occur to ensure the identification of significant GI pathology, that is colorectal carcinoma/significant polyps, yet avoid unnecessary invasive interventions.3 An Endosoft search was performed to identify all patients having colonoscopy for isolated iron deficiency anaemia in 2005. Patients with additional indications for colonoscopy were excluded, for example GI bleeding/change in bowel habit. Patients in which iron deficiency was not be confirmed by low MCV/ferritin in the 6 months prior to colonoscopy were also excluded. The results of colonoscopies were defined as positive, that is GI carcinoma/significant polyp (intermediate or high risk according to BSG guidelines), negative, that is no significant pathology, or excluded, that is colitis, angiodysplasia, etc. The lowest haemoglobin reading in the 6 months preceding the colonoscopy was recorded. Receiver operator characteristic (ROC) curve analysis was used to define the haemoglobin level under which significant colorectal pathology is likely to be identified.
Results: 385 patients were identified in the initial search. 196 patients were eligible for inclusion: 28 positive and 168 negative according to the defined criteria. Data were analysed using ROC curve analysis. The area under the ROC curve was 0.521 with a standard error of 0.0569. p = 0.3544. This suggests that haemoglobin levels alone in iron deficiency anaemia are a poor test to predict the presence of colorectal cancer or significant polyps. In fact 27.3% (3) of female and 30.8% (4) of male malignancies or significant polyps would not have been detected if NICE guidelines were followed.
Conclusion: All patients with proven iron deficiency anaemia of any severity should have a colonoscopy to examine for colorectal cancer or significant polyps in line with the current BSG Guidelines to avoid missing significant pathology.
PM139 IS GASTROINTESTINAL ENDOSCOPY A RISK FACTOR FOR CLOSTRIDIUM DIFFICILE ASSOCIATED DIARRHOEA?
C. P. Selinger, S. Greer. Department of Gastroenterology, Royal Albert Edward Infirmary, Wigan, UK
Introduction: Although endoscopy has been described as a risk factor for the development of Clostridium difficile associated diarrhoea (CDAD) in several review articles no conclusive evidence exists to support this claim.1
Aims and Methods: This retrospective Case-Control study aims to explore in a large patient cohort whether gastrointestinal (GI) endoscopy is an independent risk factor for CDAD. Cases were all patients who newly tested positive for Clostridium difficile Toxin A and/or B between March and December 2006. Age and sex matched controls were drawn from a cohort of patients with diarrhoea and negative Clostridium difficile Toxin A and B tests. Gastrointestinal endoscopy in the 30, 60 and 90 days prior to Clostridium difficile Toxin A and B testing in both groups was recorded and data analysed using exact McNemara’s significance probability test. The absolute risk of developing CDAD within 30, 60 and 90 days after GI endoscopy was calculated for all patients undergoing endoscopy between March and September 2006.
Results: The 287 case-control pairs had a mean age of 78 years, and 65% were female. The endoscopy exposure rate for cases was higher than for controls at all time points, but this apparent increase in endoscopy exposure was clearly not of statistical significance for the 90 (p = 0.18) day data although it was of borderline statistical significance for the 30 (p = 0.057) and 60 (p = 0.053) day data. Odds ratios vary between 1.55 (95% CI 0.83 to 2.98) at 90 days and 2.09 (95% CI 0.97 to 4.75) at 30 days. 25 of 4959 patients undergoing GI endoscopies between March and September 2006 developed CDAD. The absolute risk ranged between 0.32% at 30 days and 0.5% at 90 days.
Conclusion: This study suggests there may indeed be a modest (odds ratio of 2) temporary increase in CDAD risk in the first 60 days following endoscopy. The absolute risk of CDAD after endoscopy is however very low. Further studies by other centres are required to confirm our findings. CDAD prevention strategies should in our opinion focus on well established risk factors with higher odds ratios rather than on endoscopy until further evidence arises.
PM140 CAPABILITY INDEX: AN EFFECTIVE TOOL TO MEASURE CLINICAL PERFORMANCE IN COLONOSCOPY
C. P. Challand, E. Wu, K. B. Hosie. GI Directorate, Derriford Hospital, Plymouth, UK
Introduction: Clinical performance requires quality and competency being delivered in a cost-effective way. The defining characteristic of high performing teams is their willingness to measure performance and make continuous improvements accordingly.
Aims and Methods: Data from all endoscopy procedures performed within the main endoscopy unit at Derriford Hospital between January and December 2007 were analysed using the Endosoft™ database. Points were allocated as follows: two points per colonoscopy and one point for gastroscopy. A local health economic analysis revealed that ⩾8 points (or 4 colonoscopies) must be performed to meet costs.
Results: In total, 3884 colonoscopies were performed with mean crude Caecal Intubation Rate (CIR) 89.6% and 8.3 Points/List. “Clinical Performance” was compared by plotting a capability index of individual crude CIRs against Points/List (see fig). Only 6/20 endoscopists consistently achieved the JAG standard in a cost-effective way. Endoscopists’ polyp detection rate and sedation rate were not discriminatory. An annual colonoscopy rate ⩾150 cases was associated with higher points per list (p = 0.04). Endoscopists offering ⩾15% training cases had significantly higher crude CIRs and Points/List (p = 0.045; p = 0.022).
Conclusion: Clinical performance needs quality and competency being delivered in a cost-effective way. Our capability index is an effective and reproducible way of measuring clinical performance and potentially developing quality improvement programmes. Training was not associated with reduced volume and was more likely to be offered by the best performing colonoscopists.

Capability index plotting crude CIR against Points List for individual endoscopists
PM141 ENDOSCOPIC THERAPY FOR LARGE COMMON BILE DUCT STONES (CBDS) IN PATIENTS WITH PREVIOUS SPHINCTEROTOMY—CAN THIS BE MADE EASIER?
D. Nylander, H. Mitchison. Gastroenterology, City Hospitals Sunderland NHS Foundation Trusts, Sunderland, UK
Introduction: There are several concerns about performing endoscopic sphincterotomy (EST) in patients with CBDS who have had previous EST. These include some reports of increased risks of perforation and bleeding. Also, adequate repeat EST can be unsafe or difficult especially if CBDS are large or there is a periampullary diverticulum. These factors can cause reduced success at common bile duct (CBD) clearance. Ampullary balloon dilatation (ABD) immediately after small sphincterotomy has been shown to be effective in the treatment of large CBDS.1 There are minimal data on use of APB long after previous EST.
Aims and Methods: We report our preliminary experience in the use of ABD in patients who present with large CBDS a minimum of 6 weeks after previous EST. Olympus duodenoscopes were used and passed to the second part of the duodenum in a standard way. Cholangiogram was obtained using a balloon or standard catheter. If the stone size was 1 cm of more, balloon dilatation was performed of the previous sphincterotomy using a wire guided “CRE” dilating balloon (Boston Scientific). The diameter of the dilating balloon used depended on the endoscopist's judgement of the diameter of the longest stone.
Results: Details of procedures are shown in the table. Median procedure duration—25 minutes (range 18 to 32). Minor oozing settled spontaneously in all cases with no drop in haemoglobin. Lithotripsy was never required. All but one of these patients have been seen in the follow-up clinic around 6 weeks after ERCP.
Conclusion: APB can be used in patients with large CBDS recurring long after previous EST and in whom adequate repeat EST would be unsafe or risky. In our experience, CBD clearance rates are high and procedure times are short for these otherwise difficult cases. Short/medium term complications are insignificant.
Health service research & IT posters
PM142 AN ELECTRONIC ADVICE AND TRIAGE SERVICE FOR GASTROENTEROLOGY
1J. I. W. Jones, 2S. Riding, 3A. Elves, 4I. Crane. 1Gastroenterology, Royal Shrewsbury Hospital, Shrewsbury, UK, 2The Medical Centre, Easthope Road, Church Stretton, UK, 3Urology, 4IT, Royal Shrewsbury Hospital, Shrewsbury, UK
Introduction: Traditional secondary care referral has many limitations. It is a crude tool for obtaining specialist advice hampered by administrative delay and a very limited means for communicating advice. Many unnecessary outpatient appointments are created where simple advice or a direct-to-test approach would have been more appropriate. The work pattern of both GPs and consultants makes telephone communication difficult and can descend into farce with messages left with various administrative staff. Choose-and-book software has exacerbated the problem by further breaking the link between GPs and individual consultants. Although the choose-and-book software has an “advice” option the module is very limited with poor data recording and lack of clarity over accountability.
Aims and Methods: We aimed to design an in-house software package “GP Portal” that allowed rapid communication between GP and consultant to minimise unnecessary clinic appointments and journeys to hospital for a predominantly rural population. The database was based on the hospital intranet and accessed remotely from the GP practices within one rural practice based commissioning group. From September 2008 all GPs within a rural practice based commissioning group were asked to send all referrals/requests for advice via this portal. “Two-week” rule referrals were excluded from this.
Results: During the first 2 months of the service 43 referrals have been received via the GP portal. Average consultant response time was 1.3±1.3 days (mean±SD). Average time for GP to read response was 1.3±2.0 days. Of these referrals only 7 (16%) were advised to be seen directly in clinic. One patient (2.3%) was advised to have primary care tests and then to be referred. Of the rest 20 (47%) were diverted directly to endoscopy and 15 (35%) just given advice electronically.
Conclusion: The electronic GP portal provided rapid personalised advice to GPs with the majority of patients not having to be seen in clinic. The system has the flexibility to support patient preference such that we could proceed directly to investigations for many patients, give simple advice for others but maintain the ability to see patients in clinic where necessary or desired. We believe this communication process supports both GPs and their patients.
PM143 ANALYSIS OF THE IMPACT OF THE MES PROGRAMME BY THE ENIGMA STUDY USING SERVICE-RELATED ENDOSCOPY DATA
1K. Thorne, 1H. A. Hutchings, 2G. Elwyn, 1J. G. Williams. 1School of Medicine, Swansea University, Swansea, UK, 2Department of Primary Care and Public Health, Cardiff University, Cardiff, UK
Introduction: The Modernising Endoscopy Services (MES) programme was set up by the NHS Modernisation Agency (NHSMA) to facilitate modernisation in 26 NHS endoscopy units in England. The “Evaluating innovations in Gastroenterology by the NHSMA” (ENIGMA) study was set up to independently evaluate the MES programme by comparing 10 MES-funded sites (Intervention sites) with 10 Control sites who redesigned their services independently. The ENIGMA study was a mixed methods study using patient quality of life scores as a primary outcome measure and interviews with patients and health professionals, health economics, GP questionnaires and service-related data as secondary outcome measures.
Aims and Methods: One aspect of the ENIGMA study involved analysing service-related data collected from Intervention and Control sites for eight specific time points to (1) determine whether the services in both Intervention and Control sites had changed over time and (2) identify whether there were any significant differences between the Intervention and Control sites at specific points in time. All 20 study sites were asked to submit service-related data pertaining to Referral numbers, Number of patients waiting more than 3 months (Wait >3 m), Total number of patients waiting (Snapshot), Number of lost appointment slots (Lost slots) and Activity for eight time points between Jan 03 and Apr 06. These data were chosen as they closely reflected the data capture requirements of the MES Toolkit used by the Intervention sites. Where endoscopy units did not provide data, Trust data were obtained. Data were aggregated into years (2003, 2004, 2005/06) and by site type (Intervention and Control groups) for statistical analysis using a two-way ANOVA.
Results: Referral numbers, Wait >3 m, Snapshot, Lost slots or Activity did not change significantly over time within either the Intervention or the Control group. There was also no significant difference between Intervention and Control group data at any point in time for these data measures. These findings were also mirrored in all other aspects of the ENIGMA study.
Conclusion: Based on the data analysed in this study and by the ENIGMA study in its entirety, we conclude that the MES project had no significant impact on the services of participating endoscopy units as a whole, and had limited benefits when compared with the Control site endoscopy units. It appears that while the MES project may have been a focus for thinking about redesigning services for both Intervention and Control sites during the application phase, the project itself did not appear to significantly improve endoscopy services overall in the Intervention sites over and above what could have been achieved independently.
PM144 ACCESS TO CLINICAL INFORMATION AND THE LITERATURE: A SURVEY OF BSG MEMBERS
M. Gregory, H. Ellison, T. Smith, T. Heymann. Information Group, BSG, London, UK
Introduction: Muir Gray has observed that National Health Service (NHS) clinicians are overwhelmed with information but cannot find particular information when and where it is needed.1 The support to access such information appears to vary.2 Such differences create challenges in delivering uniform care nationally.
Aims and Methods: The Information Group of the British Society of Gastroenterology (BSG) aimed to quantify the challenge for gastroenterologists working in the UK by establishing what access is available, to whom and satisfaction levels with current arrangements. In August 2008 we developed, piloted then revised a questionnaire which we e mailed to 1500 gastroenterologists, consultants and trainees, all members of the BSG working in clinical practice in the UK. We asked for information by Strategic Health Authority or country, nature of institution (teaching hospital or district general (DGH)) and seniority. We asked about clinical information sources used, frequency and ease of access to each and user satisfaction with access arrangements. We sought free text comment
Results: We received 107 responses in 2 weeks. Respondents included ∼10% of trainees surveyed and 7% of consultants. The teaching hospital/DGH split was 51:56. Clinicians from all parts of the UK replied in broadly equal numbers. Those in Scotland approached “very satisfied” with their access to information, mean score 4.5/5. Elsewhere respondents were neither satisfied nor dissatisfied (mean scores from 2.8 to 3.7, Northern Ireland to South East Coast). Respondents made frequent use of online information resources, journals and guidelines, sometimes accessible only by costly personal subscription. Twelve per cent reported no use of such resources. Institutional firewalls were one reason given. Others were put off by a need for multiple usernames and passwords. Some use was also made of institutional intranets (80%), NHS websites (65%), commercial websites such as Uptodate.com (56%), National Library for Health (39%), Google and institutional libraries.
Conclusion: Gastroenterologists working in the NHS access a wide variety of information sources to help with their work. Only those in Scotland appear to be satisfied with current arrangements. Personal subscriptions to journals and commercial sites such as Uptodate.com are used by many. Some appear to have no ease of access to, or less plausibly use for, online information. For all, the issue of multiple user names and passwords remains, and for some with more limited institutional subscriptions the need to pay for access highlights a need for a revised approach if the NHS is to deliver uniform care nationally, based on best available information, a policy objective. Click-though full paper access in particular could be improved. The BSG could offer the member’s area of its web portal as a single, password-protected route of auditable access to pertinent online clinical information for NHS gastroenterologists were the funding available.
PM145 HOW ACCURATE ARE THE PERFORMANCE DATA COLLECTED BY THE BCSS?
1T. Brooklyn, 1S. Boyle, 1S. Brooklyn, 1M. Mulrenan, 1C. Quance, 2K. Dowler, 1J. Anderson. 1Gastroenterology, 2IT, Cheltenham General Hospital, Cheltenham, UK
Introduction: As part of quality assurance for the National Bowel Cancer Screening Programme (BCSP), data are prospectively collected by Specialist Screening Practitioners during each screening colonoscopy. These data are used to monitor the performance of each accredited colonoscopist and could potentially be used to revoke their accreditation if National Targets are not met. The data are entered onto the Bowel Cancer Screening System (BCSS), a web-based programme that is designed to manage the BCSP including the colonoscopy. Concerns have been raised about the accuracy of these data as the BCSS has experienced teething problems during the roll out of the BCSP.
Aims and Methods: Bowel Cancer Screening began in Gloucestershire in January 2007 and data from all the screening colonoscopies have been recorded simultaneously on the BCSS and the local electronic reporting systems (ERS) (Unisoft in Cheltenham and SQL Scope in Gloucester). The BCSS was interrogated to provide performance data on both screening colonoscopists from 22/01/2007 up to and including 08/10/2007. Information on total number of colonoscopies plus completion rates, polyp detection and polyp recovery were obtained. Colonoscopies performed on the BCSP lists were identified by interrogating the Patient Administration System and then performance data were extracted from these procedures.
Results: We demonstrated a discrepancy between the total number of cases performed with Colononscopist A (CA) having 185 procedures recorded on BCSS, but 203 recorded on the local ERS and colonoscopist B (CB) recording 216 on BCSS and 236 on the ERS. The completion rates, polyp detection and recovery rates were all similar for both colonoscopists. The table shows the comparative results.
Conclusion: There are discrepancies between the two sets of data, but these seem to relate to the number of cases only, and there are two factors that may account for this. This may reflect that screening began in Gloucestershire before the investigation data set on BCSS was live and colonoscopy data were recorded manually. These data have not all been added to BCSS. Another factor is that early in the programme, non-BCSP patients were scoped on the BCSP lists to ensure that they were full. The completion rates, polyp detection rates and polyp recovery rates are all reassuringly similar and suggest that the BCSS is collecting these data accurately.
Inflammatory bowel disease posters
PM146 METHOTREXATE IN CROHN’S DISEASE; A USEFUL ALTERNATIVE?
A. J. Cairns, A. Al-Rifai, A. Robinson, J. Shaffer. Department of Gastroenterology, Salford Royal NHS Foundation Trust, Manchester, UK
Introduction: The use of methotrexate in refractory Crohn’s disease remains limited despite a positive Cochrane review.1 We examined our use of methotrexate over the last 7 years with the aim of establishing clinicians’ reasons for initiating methotrexate treatment, side effects and tolerance of treatment and the benefits of methotrexate.
Aims and Methods: We examined case records of all patients who started Methotrexate between 2001 and 2008 in a tertiary Gastroenterology department. A record was made of the distribution and phenotype of Crohn’s disease, the reasons for treatment, the length of treatment and its outcome. A relapse was defined as an increase of steroid greater than 10 mg, an increase in methotrexate or the addition of immunomodulators.
Results: 34 methotrexate treatment episodes were recorded in 33 patients between 2001 and 2008. Fourteen patients had stricturing disease, 8 inflammatory and 7 penetrating. Eleven patients were smokers. 21 Patients were started on 25 mg im weekly for 16 weeks then 15 mg weekly. The remaining 13 patients had a starting dose between 7.5 mg and 15 mg, with the dose increased as tolerated (either im or oral). The median length of treatment was 511 days (range 31–2162 days), and median total dose 1212 mg (100–3440 mg). 22 of the 34 patients were still on Methotrexate at the time of data collection. The indications for methotrexate were azathioprine failure (n = 14), azathioprine side effects (n = 16) and physician decision (4). 22 of 35 patients reported no side effects. Nausea (4) and lethargy (4) were the most common problems. No serious complications occurred. There was no significant difference in incidence of side effects with 25 mg of methotrexate compared with 15 mg or less (7/21 vs 5/13). At 6 months 25/32 (78%) patients remained relapse free, and at 1 year 18/28 (64%) patients were relapse free. 21 patients were on steroids at the time of starting MTX; of these 20 (95%) experienced a steroid sparing effect.
Conclusion: In this cohort of patients Methotrexate has been a well tolerated, effective treatment for steroid dependent or difficult Crohn’s Disease. The majority of patients (95%) experience a steroid sparing effect and more than half (64%) the patients were free of relapses at 1 year. There were no serious side effects of treatment, and there was no increased risk of side effects with the recommended higher starting dose (1) of 25 mg a week. We believe that methotrexate is a useful alternative if azathioprine fails or is not tolerated. Concerns about potential side effects should not limit the starting dose or the use of methotrexate.
PM147 DETAILED HAPLOTYPE-TAGGING STUDY OF GERMLINE VARIATION OF MUC19 IN INFLAMMATORY BOWEL DISEASE
A. M. Phillips, J. van Limbergen, E. R. Nimmo, H. Drummond, L. Smith, J. Satsangi. GI Unit, University of Edinburgh, Edinburgh, UK
Introduction: A recent meta-analysis of three genome wide association studies (GWAS) has identified novel loci associated with the genetic susceptibility to Crohn’s disease (CD).1 The genome-wide significant rs11175593 allele has implicated the Chromosome 12q12-locus which contains the autophagy gene, LRRK2 (leucine-rich repeat kinase 2) as well as the MUC19 gene, one of a family of genes encoding mucin monomers which are involved in the maintenance of epithelial barrier integrity. Alteration of the mucin-layer composition through dysregulated autophagy has recently been demonstrated in CD.2 In order to further narrow the association signal on this locus, we performed a haplotype-tagging study of germline variation of the MUC19 gene.
Aims and Methods: 437 CD patients, 451 ulcerative colitis (UC) patients and 428 population controls were genotyped for 3 MUC19 alleles. The alleles were chosen using solid spine of linkage disequilibrium (LD), to tag haplotypic variation of the MUC19 gene including the extended 5′ and 3′ regions (haplotype freq>5%). Given the association of rs11175593 with CD with a case-control Odds Ratio (OR) of 1.54, our study had more than 95% power to detect an association with CD for each of the 3 tagging variants. All IBD cases were phenotyped using the Montreal classification.3
Results: Single marker and haplotype susceptibility analysis did not show an association with any of the MUC19 haplotype-tagging variants, in IBD overall, CD and UC. Allelic frequencies in cases and controls are shown in the table. Genotype–phenotype analysis, assessing disease location and behaviour in CD and UC, was also negative. Detailed analysis of available HapMap data showed a complete lack of LD between rs11175593 and the 3 MUC19 tagging variants (r2 = 0).
Conclusion: We have demonstrated that the genome-wide significant association of the 12q12 locus with CD is not due to germline variation of the MUC19 gene. Our findings support the detailed investigation of other genes on this locus, notably the autophagy-gene, LRRK2.
PM148 MMX™ MESALAZINE THERAPY INDUCES MUCOSAL HEALING IN PATIENTS WITH MILD-TO-MODERATELY ACTIVE ULCERATIVE COLITIS REGARDLESS OF ESTABLISHED OR NEWLY DIAGNOSED DISEASE
1G. R. Lichtenstein, 2W. Sandborn, 3M. A. Kamm, 4D. Solomon, 4R. Karlstadt, 5K. Barrett, 5B. Abhyankar, 4R. E. Joseph. 1Division of Gastroenterology, University of Pennsylvania, Philadelphia, USA, 2IBD Clinic, Mayo Clinic, Rochester, USA, 3St Vincent’s Hospital, Melbourne, Australia, 4Shire Pharmaceuticals Inc., Wayne, USA, 5Shire Pharmaceuticals Inc., Basingstoke, UK
Introduction: MMX mesalazine (Mezavant XL™; Shire Pharmaceuticals, Wayne, Philadelphia, USA) is a once-daily (QD), oral 5-aminosalicylic acid (5-ASA) therapy for the induction and maintenance of remission of mild-to-moderate ulcerative colitis (UC). This formulation utilises MMX Multi Matrix System (Cosmo, Milan, Italy) technology to delay and extend delivery of mesalazine (1.2 g/tablet) throughout the colon. Following two phase III induction-of-remission trials, we evaluated the ability of MMX mesalazine to induce mucosal healing in patients with recently diagnosed UC, compared with patients who had a longer duration of disease and a history of clinical relapse.
Aims and Methods: We pooled data from two 8-week, randomised, double-blind, placebo-controlled, phase III studies (SPD476 3011 and −3022), with the same entry criteria and endpoints. Patients with mild-to-moderate UC (modified UC Disease Activity Index [UC-DAI] score: 4–10) received MMX mesalazine 2.4 g/d (QD or twice daily [BID]), 4.8 g QD, or placebo. The following subgroups were explored, patients with <1 year disease duration, and patients with ⩾1 year disease duration with ⩾3 relapses in the last 2 years prior to study entry. The primary endpoint was mucosal healing; defined as a modified UC-DAI sigmoidoscopy score of ⩽1 (patients with mucosal friability were assigned a score of ⩾2).
Results: Overall, 340 patients met the criteria for one of the subgroups. In both subgroups, a greater proportion of patients who received MMX mesalazine achieved mucosal healing compared with placebo (table).
Conclusion: MMX mesalazine 2.4 or 4.8 g/d therapy is effective for mucosal healing in mild-to-moderate UC regardless of disease history. Particular benefit was seen for patients with longer disease duration and a history of clinical relapse. MMX mesalazine 4.8 g/d appears to be highly effective for inducing mucosal healing in patients with recently diagnosed disease.
PM149 5-AMINOSALICYLIC ACID (5-ASA) FOR THE TREATMENT OF ULCERATIVE COLITIS: EXPLORING THE LINK BETWEEN PHARMACOKINETICS, COLONIC CONCENTRATIONS AND CLINICAL OUTCOMES
1G. R. Lichtenstein, 2D. Solomon, 3B. Abhyankar, 2S. Pampati. 1Div. Gastroenterol, Uni of Pennsylvania, Philadelphia, USA, 2Shire Pharmaceuticals Inc., Wayne, USA, 3Shire Pharmaceuticals Inc., Basingstoke, UK
Introduction: We reviewed published data to evaluate the relationship between pharmacokinetic (PK) analysis and mucosal concentrations (MC) of mesalazine. Specifically, we asked (1) do increasing serum concentrations of 5-ASA correlate with increasing concentrations at the colonic mucosa and (2) is MC linked to clinical efficacy?
Aims and Methods: Medline and Embase were searched for clinical trials in humans (1980–present) that included the terms mesalazine and sulfasalazine. The search was further refined to studies relating to MC and PK.
Results: The PK analysis found higher plasma 5-ASA with increasing doses. In a study by Hussain et al1 an increase in mucosal 5-ASA concentration correlated with increasing plasma concentration with a dose increase from 1.2 g to 2.4 g. However, patients treated with mesalazine have been reported to have higher steady-state plasma 5-ASA than patients treated with balsalazide, suggesting PK may be affected by differences in precolonic absorption2. Further, D’Inca et al3 have shown that the formulation of 5-ASA can affect the MC. Indeed, in a search of recent conference abstracts, a higher colonic MC was seen with balsalazide than mesalazine, yet this did not correlate with clinical improvement in patients with UC.4 In contrast, a number of other studies have reported clinical/sigmoidoscopic/endoscopic/histological improvements in UC with a high mucosal mesalazine concentrations.5–7 High rectal mesalazine concentrations have been recorded in patients receiving oral mesalazine who were given additional rectal mesalazine; however, topical treatment was associated with high inter-subject variability suggesting that uptake of 5-ASA by mucosal cells may be influenced by inconsistencies between patients.8 Indeed, in patients receiving both oral and rectal mesalazine, a high concentration of mesalazine in the rectal mucosa was capable of maintaining some patients in complete remission for 2 years, but unable to prevent mild exacerbations in others.6 MC also varies with the severity of mucosal inflammation, with higher MC seen in patients with slight endoscopic and histological lesions compared with those with moderate endoscopic signs of disease.9
Conclusion: The utility of PK measurements for assessing topical therapies in patients with UC is limited. In contrast, MC of 5-ASA may be important in determining therapeutic effect, but further studies are needed to determine this relationship.
PM150 POST OPERATIVE CROHN’S DISEASE—THE ROLE OF FAECAL CALPROTECTIN AND LACTOFERRIN IN ASSESSING DISEASE RECURRENCE FOLLOWING ILEAL RESECTION
1M. K. Mohiuddin, 2C. A. Lamb, 3J. Gicquel, 3D. Neely, 1F. G. Bergin, 1J. M. Hanson, 2J. C. Mansfield. 1Colorectal Surgery, 2Gastroenterology, 3Biochemistry, Newcastle upon Tyne Hospitals NHS Foundation Trust, Newcastle upon Tyne, UK
Introduction: Optimal treatment of post operative Crohn’s disease depends on assessment of gut inflammation. Patients with recurrent symptoms and high inflammatory activity may require immunosuppression, while patients with low levels of inflammation may find symptomatic improvement with loperamide and cholestyramine. Quantitative measurement of faecal markers may offer a valuable, non-invasive method of assessing the symptomatic post operative patient.
Aims and Methods: We aimed to determine if faecal calprotectin (FC) and lactoferrin (FL) measurement may identify gut inflammation in symptomatic post operative Crohn’s disease. Patients who underwent ileal resection for Crohn’s disease from January 1999 to August 2007 were recruited. A single stool sample for FC (normal<50 mcg/g) and FL (normal<7.25 mcg/g) measurement was collected from each patient, and using a value of twice the upper limit of normal (2×ULN) patients were separated into groups with high or low levels of gut inflammation. The Harvey Bradshaw Index (HBI) was applied to each patient to determine their symptom profile and clinical disease activity (score 3 or less inactive disease, 4–5 mild/moderately active disease, 6 or more severely active disease).
Results: 104 patients were recruited; male to female ratio 43:61; median age 45 years; mean duration of disease 13 years; mean duration from last resection to time of study 5 years. FC and FL correlated significantly with disease activity measured by the HBI (r = 0.532; p<0.001 and r = 0.687; p<0.001 respectively). The table presents the HBI, and mean faecal marker levels in active versus inactive disease as defined by a FC or FL value more or less than 2×ULN. Of particular note in those patients with HBI 4–5, FC and FL allowed identification of two groups with similar clinical severity indices but with very different biomarker levels of gut inflammation.
Conclusion: This study has shown that not only do FC and FL correlate with post operative disease activity, but they also provide an additional useful method of identifying high inflammatory activity in those with mild to moderate symptoms who may benefit from further immunosuppressive treatment. Often this is the hardest group of patients to assess in everyday clinical practice. FC and FL are safe, non-invasive and reliable tests which should now be routinely applied to the clinical problem of symptom recurrence in post operative Crohn’s disease.
PM151 LONGITUDINAL STUDY OF FAECAL MARKERS FOLLOWING ILEAL RESECTION IN CROHN’S DISEASE—DO CALPROTECTIN AND LACTOFERRIN NORMALISE POST OPERATIVELY?
1C. A. Lamb, 2M. K. Mohiuddin, 3J. Gicquel, 3D. Neely, 2F. G. Bergin, 2J. M. Hanson, 1J. C. Mansfield. 1Gastroenterology, 2Colorectal Surgery, 3Biochemistry, Newcastle upon Tyne Hospitals NHS Foundation Trust, Newcastle upon Tyne, UK
Introduction: Crohn’s disease is characterised by inflammatory cell migration to the diseased bowel mucosa. Faecal concentrations of granulocyte degradation products can therefore be used as a non-invasive quantitative method of monitoring disease activity. Research has shown that elevated levels of faecal calprotectin and lactoferrin are strongly associated with mucosal inflammation. No previous studies have investigated how quickly and indeed if faecal markers normalise post ileal resection.
Aims and Methods: We aimed to monitor the trend of post operative faecal calprotectin and lactoferrin concentrations. Thirteen patients who were to undergo ileal resection for symptomatic Crohn’s disease were identified and faecal markers were measured pre operatively and at intervals post operatively for 1 year. Patients were closely monitored for disease recurrence. A control group was not required as normal ranges of both markers are well defined (calprotectin <50 mcg/g, lactoferrin <7.25 mcg/g).
Results: Five patients had a complicated 12 month post operative follow-up period. The table shows the mean faecal marker results with standard errors for the remaining 8 patients without evidence of complication. In each case a raised preoperative FC and FL normalised within 1 month. Of the 5 patients with a complicated post operative recovery, 3 had evidence of disease recurrence and 2 developed post operative intra abdominal collections. In each case both FC and FL increased at the time of complication and all normalised again within 4 weeks following commencement of therapy, be that collection drainage and antibiotics or commencement of azathioprine or infliximab.
Conclusion: This novel research clearly demonstrates that following ileal resection, faecal calprotectin and lactoferrin levels do not remain elevated and begin to fall within a week. Normalisation of both markers is reached by 1 month post operatively and maintained in non relapsing patients. New onset diarrhoea post ileal resection may be due to bile salt malabsorption or altered gut motility, but invasive tests such as colonoscopy or radiological investigation are often required to exclude disease recurrence. Our data suggest that faecal calprotectin and lactoferrin have the potential to non-invasively test for disease recurrence post operatively, monitor response to therapy following relapse, and therefore avoid invasive investigation.
PM152 PERIANAL CROHN’S DISEASE—THE EFFICACY OF COMBINED SURGICAL AND INFLIXIMAB THERAPY
1C. Johnston, 2A. Watson, 1S. Campbell. 1Gastroenterology, Manchester Royal Infirmary, Manchester, UK, 2General Surgery
Introduction: Perianal Disease affects up to 30% of patients diagnosed with Crohn’s Disease. Infliximab is a monoclonal antibody therapy which is well established in the therapy of intestinal Crohn’s disease. The efficacy of treatment of infliximab for perianal Crohn’s disease is controversial. This study assessed the outcome of a cohort of patients with perianal Crohn’s who were treated with infliximab solely for their peri-anal disease.
Aims and Methods: We used a prospective database of 106 patients treated with Infliximab within a single institution between 2000 and 2008. Data collected included demographics, disease anatomy/type (Vienna Classification), clinical findings, adverse events, time to loss of response, concomitant immunosuppressive therapy, smoking status, examination under anaesthetic, large and small bowel resection numbers and results of those proceeding to definitive surgery for perianal Crohn’s disease (ie, defunctioning stomas and completion colectomies/proctectomies with end ileostomies). The Perianal Crohn’s Disease Activity Index was used to score the patients disease before starting infliximab infusion and at 8 weeks after the third loading dose (standard regime of loading of 0, 2 and 6 weeks).
Results: 27 patients underwent inflixiamb therapy for primary perianal Crohn’s disease (17F:10M, median age 38.5 years (range 19–71 years)). Of these, 11 patients (41%) had colonic involvement, 15 patients (56%) had ileocolonic involvement and one patient (4%) had terminal ileal involvement. Nine patients (33%) were non-smokers, seven patients (26%) were classified as ex-smokers and 11 patients were currently smoking (41%). 25 patients had undergone an examination under anaesthesia prior to infliximab infusion with 21 (84%) requiring one or more surgeries for drainage of abscess or insertion of one or more setons. Fifteen patients underwent magnetic resonance imaging to delineate complex perianal fistulae and clinically occult collections. Perianal Crohn’s disease activity index improved after infliximab infusion (preinfusion: median, 14, range 4–19; postinfusion: median, 7.5 range 4–18). Five patients (18.5%) had a severe reaction/complication of infliximab treatment. At median follow-up of 24 months, 7 patients (26%) had gone on to require defunctioning or proctectomy. Only 3 patients (11%) had achieved sustained fistula healing (defined as cessation of discharge and proctalgia).
Conclusion: Infliximab therapy in combination with examination under anaesthesia/seton drainage is a safe and effective short term treatment for perianal Crohn’s disease. Long term healing rates for severe perinal disease are low.
PM153 INCREASED EFFICACY OF MODIFIED-RELEASE MESALAZINE 4.8 G/D (800 MG TABLET) COMPARED TO 2.4 G/D (400 MG TABLET) FOR TREATMENT OF MODERATELY ACTIVE ULCERATIVE COLITIS IN PATIENTS WITH A HISTORY OF MORE DIFFICULT TO TREAT DISEASE
1S. B. Hanauer, 2D. Ramsey, 3W. J. Sandborn. 1Section of Gastroenterology and Nutrition, University of Chicago, Chicago, USA, 2Biostatistics, Procter and Gamble Pharmaceuticals, Cincinnati, USA, 3Division of Gastroenterology, Hepatology and Internal Medicine, Mayo Clinic, Rochester, USA
Introduction: To determine the efficacy of and identify patients more likely to respond to higher dose (4.8 g/d using an 800 mg tablet) mesalazine for the treatment of moderately active ulcerative colitis (UC) according to prior medical therapies.
Aims and Methods: Data from 3 Phase III, multi-centre, randomised, double-blind, 6-week active-controlled studies of similar design (ASCEND I, II, and III) were combined and analysed. Efficacy of modified-release mesalazine 4.8 g/d (800 mg tablet) was compared with 2.4 g/d (400 mg tablet) in patients with moderately active UC (Physician’s Global Assessment [PGA] = 2). The primary endpoint was treatment success defined as improvement from baseline in PGA (based on clinical assessments of rectal bleeding (RB), stool frequency (SF) and sigmoidoscopy) with no worsening in any individual clinical assessment. [Note that patient functional assessment was also considered in ASCEND I and II and that sigmoidoscopy results were assessed differently in ASCEND III as compared with ASCEND I and II]. Hallmark symptoms of UC, RB and SF, were evaluated identically in all three studies. Improvement in RB and SF was defined as a decrease from baseline of at least 1 point based on a 4 point scale (0–3). Clinical remission was defined as resolution of both RB and SF.
Results: A total of 1220 patients with moderately active UC were randomised and dosed. At 6 weeks, treatment success occurred in 69% and 62% of patients receiving 4.8 g/d vs 2.4 g/d, respectively, p = 0.006. Similarly, at 6 weeks, more patients receiving 4.8 g/d vs 2.4 g/d had RB improvement (83% vs 79%, p = 0.04), SF improvement (78% vs 73%, p = 0.07) and clinical remission (43% vs 37%, p = 0.06). A therapeutic advantage of 4.8 g/d was seen in patients with previous use of UC medications as evidenced in the table.
Conclusion: Modified-release mesalazine at 4.8 g/d (800 mg tablet) demonstrated efficacy for the treatment of moderately active UC, with evidence of a therapeutic advantage in patients with a history of more difficult to treat disease (eg, previous use of oral 5-ASAs, rectal therapies, steroids, or multiple medications).
PM154 INFLAMMATORY BOWEL DISEASE IN CAUCASIAN AND UK SOUTH ASIAN PATIENTS: DIFFERENCE IN CLINICAL PHENOTYPE
1D. G. Walker, 1H. R. T. Williams, 2S. Padaruth, 1A. N. Milestone, 2J. Arnold, 3S. Kane, 1H. J. W. Thomas, 1J. P. Teare, 1A. Hart, 4D. P. Jewell, 1T. R. Orchard. 1Gastroenterology, Imperial College London, UK, 2Gastroenterology, Ealing Hospital, London, UK, 3Gastroenterology, West Middlesex University Hospital, London, UK, 4Gastroenterology, University of Oxford, Oxford, UK
Introduction: Inflammatory bowel disease (IBD) was traditionally considered rare outside Europe and North America. However, recent studies have shown that the incidence of IBD is increasing throughout Asia.1 Since the 1950s there has been substantial migration from South Asia to the UK and currently 2.33 million South Asians live in the UK and 0.86 million live in London. There have been few studies examining the characteristics of IBD in this population.
Aims and Methods: The aim of the study was to define the clinical phenotype of South Asian IBD patients living in West London and compare the findings with a White IBD cohort. A retrospective case note review was performed on South Asian patients (patients originating from India, Pakistan, Bangladesh or Sri Lanka) under active follow-up at IBD clinics in five West London hospitals. Diagnosis and disease extent were confirmed by standard criteria and classified according to the Montreal classification. Any history of extraintestinal manifestations (EIMs) was also noted. The results were compared with a well phenotyped UK White IBD cohort from the John Radcliffe Hospital in Oxford using the Chi-squared test.
Results: 242 South Asian patients with IBD were identified (174 UC, 62 CD, 6 IBD unclassified) and compared with 976 White UC patients and 483 CD patients. Within the South Asian UC population there was a male predominance (1.5:1), median age at diagnosis was 30 years (range 9–69). 65% of South Asian patients had extensive colitis compared with 30% of the White cohort (p<0.001). Left sided disease was similar in each group (27% and 38%) but limited rectal disease was rare in the South Asian UC patients (8% vs 32% in Whites; p<0.001). Of the 62 South Asian CD patients, 39 were male (median age at diagnosis: 33 [12–83]). Disease phenotype was predominantly colonic (L2 = 45%) and ileocolonic (L3 = 40%). Ileal disease was less common compared with the White population (L1 = 15% vs 40%; p<0.001). There was a statistically higher number of White CD patients with at least one EIM compared with the South Asian CD cohort (30% vs 13%; p = 0.003). There was no statistical difference in EIMs between the UC cohorts (8.6% vs 13% of White patients).
Conclusion: UC is more common than CD in the West London South Asian IBD population. Disease location differed significantly from White patients: the majority of South Asian UC patients had extensive colitis, and colonic involvement was the most common CD phenotype. These phenotypic variations between different ethnic groups offer interesting data that will likely reflect genetic, environmental and behavioural factors.
PM155 URINARY METABOLIC PROFILING IN CROHN’S DISEASE: IS THERE A DIFFERENCE BETWEEN ETHNIC GROUPS?
1D. G. Walker, 1H. R. T. Williams, 2I. J. Cox, 1T. R. Orchard. 1Gastroenterology, 2Imaging Sciences, Imperial College London, London, UK
Introduction: The pathogenesis of Crohn’s disease (CD) relates to the interaction of genetically predisposed individuals with environmental stimuli; the key environmental triggers being derived from host intestinal microbiota. Nuclear magnetic resonance spectroscopy (NMRS) is a potential technique that can be used to study the intestinal microflora. It allows quantification of specific metabolites resulting from luminal bacterial metabolism. Distinct metabolic profiles for CD have been demonstrated in the White population.1 In particular, levels of hippurate (a specific metabolite arising from the shared metabolism of the host and gut microflora) were significantly lower in CD patients compared with healthy controls. It is not known whether the metabolic differences observed in White CD patients are the same for patients of different ethnicities.
Aims and Methods: The primary aim was to determine if there were significant differences in the urinary metabolites that are dependent on gut bacterial metabolism (hippurate, formate, trimethylamine-N-oxide [TMAO] and dimethylamine [DMA]) between South Asian CD patients and healthy South Asian controls. The 500 MHz 1H NMR spectra of 14 South Asian CD patients were analysed and compared with 31 South Asian controls. A White CD cohort (n = 14) matched for diagnosis, age, sex and diet were also compared with the South Asian CD patients to confirm any differences. Patients with co-morbidities including diabetes were excluded from the study.
Results: Hippurate levels were significantly lower in South Asian CD patients when compared with South Asian controls (p<0.001, Mann–Whitney U test). No differences were found for formate, TMAO or DMA. Hippurate levels did not differ significantly between the South Asian and White CD cohorts.
Conclusion: South Asian CD patients are characterised by the same significant differences in hippurate, a host-bacterial co-metabolite, as seen in White CD cohorts. The results suggest that the metabolic differences in CD, attributable to an altered intestinal microflora, are independent of ethnicity and characteristic of CD.
PM156 ARE ACCELERATED INFLIXIMAB INFUSIONS SAFE IN PATIENTS WITH INFLAMMATORY BOWEL DISEASE?
D. Sharma, S. Bhat, P. Doherty, T. C. K. Tham, G. R. Caddy. Gastroenterology, Ulster Hospital Dundonald, Belfast, UK
Introduction: Infliximab is a monoclonal antibody used in the treatment of inflammatory bowel disease.1 Manufacturer recommended administration is over 2 hours followed by 2 hours of patient observation. Small previous studies have found that an accelerated protocol for infusion is not associated with an increase in adverse outcomes.2
Aims and Methods: Our unit utilises an accelerated protocol for infliximab infusion in selected patients with inflammatory bowel disease (those with no reaction in their first 4 standard infusions). Our aim was to assess if the accelerated infusion protocol (1 hour/30 minute infusion with1 hour/0 hour monitoring) was associated with any increase in adverse outcomes. Data were collected retrospectively on protocol used and adverse outcomes for all infliximab infusions between October 2005 and June 2008.
Results: Out of 69 patients, 27 received the accelerated protocol (130 infusions). All patients received a total of 306 infusions on the standard protocol. No adverse reactions were reported in the accelerated protocol patients. In patients on the standard protocol, 16 adverse reactions were observed: 7 were acute (occurring during infusion); 9 were delayed (occurring within 1–7 days following infusion). No patient required intramuscular adrenaline or hospitalisation.
Conclusion: Our findings suggest that an accelerated protocol for infliximab infusion is well tolerated in selected patients. The monitoring period following infusion may not be necessary as all acute reactions occurred within an hour of initiating infusion and did not warrant hospitalisation. The accelerated infusion may allow more efficient utilisation of hospital resources and reduce patient inconvenience.
PM157 A YEAST TWO-HYBRID SCREEN USING CARD15/NOD2 IMPLICATES NOVEL PATHWAYS IN IBD SUSCEPTIBILITY
1E. R. Nimmo, 1A. J. Smith, 1M. C. Aldhous, 1M. Quail, 1K. Soo, 1H. Drummond, 2J. van Limbergen, 3R. K. Russell, 1C. L. Noble, 4D. C. Wilson, 1J. Satsangi. 1Gastrointestinal Unit, 2Clinical Lecturer in Child Life and Health, University of Edinburgh, Edinburgh, UK, 3Department of Paediatric Gastroenterology, Yorkhill Hospital, Glasgow, UK, 4Paediatric Gastroenterology and Nutrition Department, University of Edinburgh, Edinburgh, UK
Introduction: NOD2 was first identified as a Crohn’s disease susceptibility gene in 2001. Since then more than 30 susceptibility genes have been identified by large-scale association studies, but it is estimated that these genes still account for less than 30% of those involved. In order to identify other genes and pathways involved in the development of IBD we have performed a yeast two hybrid screen to identify NOD2 interacting proteins and thereby candidate genes for association studies.
Aims and Methods: Full length NOD2 cDNA was used as the bait in a yeast two-hybrid screen to identify interacting proteins using a cDNA library from the intestinal epithelial cell line, SW480. Interacting proteins were confirmed by co-immunoprecipitation. Genotyping was performed on the Illumina Goldengate platform and analysis performed using Haploview 4.1.
Results: 700 bacterial colonies generated by the yeast two-hybrid screen were analysed and from these 16 interacting proteins were identified. These include proteins in pathways involved in regulation of transcription (TLE1, EGR1); NFkB regulation (MAP3K11, TLE1); Wnt signalling (TIP60, TLE1); apoptosis (TIP60, PA2G4, BPY2IP1, TTC11, VIMENTIN); androgen receptor (TIP60, FKBP4, PA2G4) and in epigenetic control of expression (TLE1, EGR1, TIP60, PA2G4). Interaction with NOD2 in SW480 cells was confirmed for TIP60, vimentin, PPP2R5E, TLE1, GALNT2, PA2G4, TTC11 and EGR1 by co-immunoprecipitation in SW480 cells. No interaction with Erbin or Grim-19 was detected. Genotyping data will be presented.
Conclusion: These interactions broaden our understanding of NOD2 function and implicate NOD2 signalling in regulation of a number of molecular pathways. As well as NFkB regulation and apoptosis, we identify for the first time a potential role for NOD2 in Wnt signalling and epigenetic regulation in intestinal epithelial cells.
PM158 LOSS OF HUMAN GAMMA DELTA T-CELLS IN CROHN’S DISEASE AND ULCERATIVE COLITIS
1E. R. Mann, 1N. E. McCarthy, 1A. N. Milestone, 2S. A. Cochrane, 3A. J. Stagg, 1A. L. Hart, 1S. C. Knight. 1Antigen Presentation Research Group, Imperial College London, St Mark’s Hospital, Harrow, UK, 2SEAC, Unilever Colworth, Bedford, UK, 3Centre for Infectious Disease, Barts and the London School of Medicine and Dentistry, London, UK
Introduction: γδ T-cells are innate lymphocytes that are increased in number in the gut of patients with inflammatory bowel disease (IBD). Some mouse models of IBD suggest that γδ T-cells are immuno-protective in the mucosa, while others indicate a role in exacerbation of disease. The role of γδ T-cells in gut immunity and IBD is far from clear.
Aims and Methods: Human peripheral blood was obtained from patients (n = 10) with Crohn’s disease or ulcerative colitis on minimal treatment (5-aminosalicylic acid or azathioprine) or from healthy volunteers (n = 11). Mononuclear cells were isolated on Ficoll gradients and labelled with monoclonal antibodies for analysis by flow cytometry. γδ T-cells were analysed for expression of tissue-homing molecules such as β7 integrin, a molecule associated with leucocyte homing to the gut.
Results: In healthy control subjects, the majority of γδ T-cells were CD3hi and expressed β7 and memory cell marker, CD45RO. The co-stimulatory receptor CD28 was expressed on 20–30% of γδ T-cells. Expression of skin homing markers was minimal. There was a significant decrease in both the number and proportion of γδ T-cells in the blood of IBD patients compared with healthy controls. The proportion of γδ T-cells exhibiting the memory cell phenotype was also significantly reduced in IBD, while preliminary data indicated that expression of the lymph node homing marker, CCR7, was increased on γδ T-cells in IBD.
Conclusion: Taken with reports that γδ T-cells are increased in the gut of IBD patients, it seems likely that the reduced numbers of γδ T-cells in the circulation are a result of γδ T-cell migration to gut. The reduced proportion of blood γδ T-cells expressing CD45RO in IBD, and possible increases in expression of CCR7, may indicate a loss of effector memory phenotype in IBD.
PM159 EXPERIENCE ON THE USE OF ADALIMUMAB AS MAINTENANCE THERAPY IN CROHN’S DISEASE IN ENGLAND AND IRELAND
1E. A. Russo, 2J. Lindsay, 3S. Campbell, 4A. L. Hart, 5P. J. Hamlin, 6T. R. Orchard, 4N. Arebi, 4J. Nightingale, 4M. R. Jacyna, 4M. O’Connor, 7A. W. Harris, 8C. A. O’Morain, 1S. Gosh. 1Gastroenterology, Hammersmith Hospital, London, UK, 2Gastroenterology, Barts and the London NHS Trust, London, UK, 3Gastroenterology, Manchester Royal Infirmary, Manchester, UK, 4Gastroenterology, St Mark’s Hospital, London, UK, 5Gastroenterology, Leeds General Infirmary, Leeds, UK, 6Gastroenterology, St Mary’s Hospital, London, UK, 7Gastroenterology, Kent & Sussex Hospital, Tunbridge Wells, UK, 8Gastroenterology, Adelaide and Meath Hospital, Dublin, Ireland
Introduction: Adalimumab (ADA) has been shown to be effective in inducing and maintaining response/remission in patients with Crohn’s Disease (CD) both naive to biological therapies and following secondary failure of infliximab (IFX). Recent data from Scotland suggested that 13 of 22 patients (59%) required dose escalation to 40 mg every week. We present the first “real-life” data from England and Ireland on the use of ADA in induction and maintenance of response/remission in patients with moderate to severe CD.
Aims and Methods: We carried out secure web-based data collection from 8 hospitals on the use of ADA in CD. We collected data on disease distribution and duration, and previous/current use of 5-aminosalicylic acid, steroids, thiopurines, methotrexate and IFX. We report on response rates (change in CDAI >70, or HBI ⩾3 or as per Physician Global Assessment (PGA)), remission rates (CDAI<150, or HBI ⩽4 or as per PGA) and the side-effect profile of ADA.
Results: We report on 61 patients (35 female) with a mean age of 35 years (17–71). The mean follow-up period was 8 months. 46% had ileo-colonic, 21% had ileal and 25% colonic disease. Rectal involvement was observed in 54%, perianal disease in 46% and 41% had fistulising disease. All patients had previously required corticosteroids. Four patients were biologic-naive (6.6%); of the remainder, IFX was discontinued due to intolerance (41%), lack of response (5%), loss of response (44%) or both (3.3%). 46% were induced with 160 mg and 80 mg of ADA on weeks 0 and 2, respectively, and 54% with 80–40 mg. 100% received 40 mg every other week (EOW) as initial maintenance dose, of which 13% were escalated to 40 mg weekly and 3% to 80 mg weekly. 83.6% of patients achieved response on maintenance ADA, of which 96% had steroid-free response, 67% remained off an immunomodulator and 59% were on ADA monotherapy. 57% of patients were in complete remission from their CD, of which 94% had steroid-free remission, 57% remained off an immunomodulator and 51% were on ADA monotherapy. An additional 8.2% of participants had a secondary loss of response to ADA, at an average of 8.4 months (range 2–17) from onset. Fourteen of 61 patients (23%) had adverse effects (local pain 4, infection 5, headaches 2, leucopenia (on Azathioprine) 1, painful rash 1, serum-sickness type reaction 1, the latter 2 of which led to discontinuation of therapy.
Conclusion: Results from an English/Irish cohort show satisfactory response/remission and safety profile of ADA in the treatment of CD. In contrast to previous data from Scotland, dose escalation was only seen in 16% of patients.
PM160 THE USE OF EMAIL AND TEXT MESSAGING TO REMIND PATIENTS TO HAVE BLOOD MONITORING WHILST ON IMMUNOSUPPRESSANTS
H. Ludlow, J. Hurley, S. Dolwani. Gastroenterology, University Hospital Llandough, Penarth, UK
Introduction: Patients on long term Azathioprine or 6-Mercaptopurine for Inflammatory Bowel Disease (IBD) require frequent blood tests and may often forget to have these taken resulting in delays and subsequent safety concerns. Email and text messaging have been shown to improve concordance for other health issues, including smoking cessation, asthma and diabetes management. Increased access to the internet and mobile phone ownership make this an ideal method of communication with this group of patients.
Aims and Methods: We aimed to determine whether the use of email and text messaging could improve delays in blood monitoring compared with standard telephone call reminders and to compare this with delays prior to the IBD nurse being in post. Between September 2007 and August 2008 patients on established treatment for >1 year were invited to participate in the study and also those newly commenced once maintenance dose reached. Test delays during the study were compared with previous delays, when only telephone calls were used. The table shows the delays pre-IBD nurse post and then pre- and post-study delays and reminders required.
Results: 115 patients were included in the study—63 had been on treatment for at least 1 year and 52 new starters (63 UC, 49 CD, 3 indeterminate). The median ages of those who chose contact by email was 41 years (n = 44), text messaging 40 years (n = 42) and telephone contact or did not reply (control) 61 years (n = 39). Reasons for not wishing contact by email or text were: no computer or mobile telephone (n = 19, median age 68.5), too intrusive (n = 1), prefers telephone (n = 1) and no reason given (n = 5).
Conclusion: Following the introduction of the IBD nurse the delay in blood tests fell dramatically from a maximum of 307 days to 34 days. There are many issues/causes surrounding delays including holidays and restricted GP phlebotomy clinics. The text group showed further reduction in delay whereas the control group without intervention actually increased. Multiple call attempts and answer machine messages are avoided (reducing issues regarding confidentiality), thus reducing time involved. Texts and emails are cost-effective in relation to frequent calls to mobile numbers. Any form of intervention by the nurse reduces delays although email and text messaging are convenient and preferred by both patients and the nurse.
PM161 USE OF TARGETED ANTIBIOTICS TO TREAT ULCERATIVE COLITIS
1T. Nakayama, 1K. L. Blackett, 1H. Steed, 1S. Macfarlane, 2N. Reynolds, 1J. H. Cummings, 1G. T. Macfarlane. 1Pathology and Neuroscience, University of Dundee, UK, 2Gastroenterology, NHS Tayside, Dundee, UK
Introduction: The cause of ulcerative colitis (UC) is unclear, but bacteria colonising the colonic mucosa are thought to play a key role in disease aetiology. Despite this, antibiotics have been unsuccessful in managing acute UC, and have had only limited benefit in long-term treatment. The failure of antibiotics might be because the target organisms are unknown, or that the organisms are protected in mucosal biofilms.
Aims and Methods: To identify putative pathogens on mucosal surfaces in the large bowel in active UC patients, and to determine their antibiotic sensitivities, with the aim of designing therapies for their suppression. 33 patients with active UC were enrolled in the trial. Clinical status was scored using the simple clinical colitis activity index (SCCAI), and rectal biopsies were taken for analysis of biofilm community structure and antibiotic sensitivity tests. Patients received two antibiotics (coamoxiclav, ciprofloxacin, clarithromycin, doxycycline, rifaximin) for 4 weeks, and clinical assessments were repeated. Patients were included if they had stable drug therapies for 3 months or were non-responders to oral steroids. Twenty-four patients completed the study.
Results: E coli, enterobacteria, peptostreptococci, staphylococci and streptococci were the predominant pathogenic species present in rectal biopsies. After 1 month of treatment with combination antibiotic therapy, there was a significant reduction in the total number of bacteria present in rectal biopsies (p<0.0001) and a significant reduction in the number of eubacteria (p = 0.0051) from 5.01×102 to 0.65×101. There was no significant change in the numbers of lactobacilli or bifidobacteria, which are potentially beneficial bacteria. There was a significant improvement in SCCAI from 7.1 to 4.8 (p = 0.005) and a significant improvement in patients IBDQ from 139 to 157 (p = 0.002). There was no significant improvement in the Baron’s score (p = 0.07), but there was a significant improvement in the histological score from 11.04 to 8.91 (p = 0.029). Analysis of bacteria in patients with no improvement, or a worsening of their SCCAI showed that there was a significant reduction in the number of prevotella from 1.4×105 to complete eradication (p = 0.002), and a reduction in the number of bacteroides from 2.4×104 to complete eradication (p = 0.022). In the group with improved clinical scores, there was a significant increase in bacteroides (p = 0.049) (2.3×103 to 2.4×105) and enterobacteria (2.3×101 to 9.6×102) and a significant reduction in eubacteria (1.9×102 to 2.6×101).
Conclusion: Targeting specific mucosal populations on the rectal mucosa demonstrated that antibiotics were unsuccessful in selectively eradicating immunogenic bacterial species in UC biofilms. However, targeted antibiotic treatment did facilitate the re-establishment of benefical populations in the mucosal microbiota, which was associated with improved clinical and histological status.
PM162 VOLATILE ORGANIC COMPOUNDS AS DIAGNOSTIC FAECAL BIOMARKERS IN INFLAMMATORY BOWEL DISEASE—METHOD DEVELOPMENT
I. Ahmed, S. Smith, C. S. Probert. Gastroenterology, Bristol Royal Infirmary, Bristol, UK
Introduction: Despite better understanding in recent years, the diagnosis of inflammatory bowel disease requires invasive and expensive procedures. Current studies are focusing on non-invasive markers which could assist in diagnosis and monitoring the disease, and also in early prediction of relapses and complications. Among the other non-invasive modalities, faecal biomarkers such as Calprotectin, Lactoferrin, etc have appeared recently in the diagnostic armamentarium. The diagnostic role of volatile organic compounds (VOCs) emitted in faeces of patients with IBD remains to be explored further. As little is known about VOCs in human faeces, a convenient analytical method to quantify them has not been addressed. This work presents a facile and rapid methodology to quantify faecal VOCs by using solid phase micro extraction (SPME) combined with gas chromatography mass spectrometry (GC/MS) by identifying suitable variables for sample preparation and analysis.
Aims and Methods: 10 healthy volunteers produced 70 samples for experiments. Headspace SPME was used as a sample pre concentration technique prior to the determination of VOCs by GC-MS. Samples were collected in a standard 50 ml faecal sample bottle and aliquoted to a 10 ml Supelco phial. Samples were placed in thermostatted water at 60°C for 1 hour to equilibrate prior to SPME extraction and fibre was then transferred to the injection port of the GC/MS for analysis. The VOCs were identified using NIST library followed by manual visual inspection and retention time matching of selected standards. The VOCs obtained by these experiments were compared in order to ascertain the most efficient methodology. The effects of extraction variables, such as the type of fibre, extraction time (10 min vs 20 min), sample quantity (1 gm/2 gm/4 gm), and effect of time at room temperature and freezing on −20°C, on the amount of extracted VOCs were studied.
Results: Results showed that use of PDMS/Car fibre identified maximum numbers of VOCs as compared with DVB fibre. More VOCs were detected in 2 gm of sample in comparison with 1 gm and 4 gm quantities. There was no meaningful difference in VOCs quantification by 10 min extraction by SPME fibre in comparison with 20 min. Samples left over a 24 hour period at room temperature were found to produce lower numbers of VOCs compared with samples analysed within 6 hours of production. Samples which were analysed following freezing within 6 hours of production showed only minimal reductions in total VOCs.
Conclusion: The optimum conditions for precise VOC quantification in faecal samples are: 2 gm quantity of faecal sample analysed within 6 hours of sample production with a use of PDMS/CAR type of SPME fibre injected in headspace above sample for 10 min extraction. If samples have to keep for longer then they should be frozen at −20°C to preserve VOCs.
PM163 THE STRESS MEDIATORS ADENOSINE AND HYDROCORTISONE IMPAIR COLONIC EPITHELIAL WOUND HEALING IN VITRO
J. Goodhand, M. Wahed, D. S. Rampton. Centre for Gastroenterology, Barts and the London School of Medicine and Dentistry, London, UK
Introduction: Psychological stress worsens gut inflammation in inflammatory bowel disease (IBD). In some models, stress delays mucosal ulcer healing.1 This process is initiated by restitution, the ingress of motile epithelial cells into the wound. The pro-inflammatory chemokine, interleukin (IL)-8, accelerates epithelial cell restitution.2
Aims and Methods: To determine the effects of four putative neurohumoral mediators of the stress response on colonic epithelial cell restitution and IL8 production in vitro. Cell restitution velocity was measured over 24 h in linear wounds made in confluent monolayers of human colon cancer-derived HT-29 cells. Cells were incubated with noradrenaline, adenosine, histamine and hydrocortisone in the presence and absence of fetal calf serum (FCS) (positive and negative control, respectively) and photomicrographs at 24 h analysed with Digimizer software. For the IL8 studies, HT-29 cells were pre-incubated with each stress mediator for 1 h, then stimulated with IL1β (1 ng/ml). IL8 in supernatants collected at 6 h was assayed by ELISA. In each case n⩾4, and ANOVA was used to compare differences; restitution results for FCS are shown.
Results: Restitution velocity was dose-dependently inhibited by adenosine (10–6 M: 3.3 (mean) ±0.42 (SD), p<0.01; 10–3 M: 2.4±0.31, p<0.01, compared with relevant controls 4.9±0.21) and by hydrocortisone (10–9 M: 4.8±0.75, p<0.05; 10–6 M: 4.4±0.66, p<0.01 vs controls 6.0±0.73). Adenosine (10–6 M: 327 pg/ml ±27, p<0.01; 10–3 M: 127±17, p<0.01) and hydrocortisone (10–9 M: 325±25, p<0.01; 10–6 M: 294±16, p<0.01) each reduced IL8 production compared with controls (449±30). At 10–9 and 10–6 M, neither noradrenaline nor histamine altered wound healing or IL8 production.
Conclusion: These results suggest that psychological stress, by causing release of adenosine and hydrocortisone with subsequent reduction of epithelial IL8 production, could impair mucosal healing in IBD and perhaps other inflammatory diseases such as peptic ulcer. The adverse effects of hydrocortisone on epithelial restitution in vitro could also contribute to its failure to induce mucosal healing in Crohn’s disease.
PM164 INFLIXIMAB USE IN ADOLESCENTS WITH INFLAMMATORY BOWEL DISEASE
1J. Goodhand, 2J. Tang, 1S. Naik, 1N. M. Croft, 1J. O. Lindsay. 1Centre for Gastroenterology, Barts and the London School of Medicine and Dentistry, London, UK, 2Department of Medicine, University of Toronto, Toronto, Canada
Introduction: The incidence of inflammatory bowel disease in adolescence is increasing.1 Compared with adults, the proportion of adolescents with Crohn’s disease is greater, disease is more extensive, and patients more frequently require treatment with immunosuppressants and surgery.2
Aims and Methods: To compare the clinical use and response to infliximab in adolescents versus adults at a tertiary IBD centre with a specialist transitional adolescent clinic. We performed a retrospective study of infliximab use at Barts and the London NHS trust, in adults and adolescents with Crohn’s disease (CD), ulcerative colitis (UC) and indeterminate colitis (IC). Demographic details, disease extent and course were recorded as well as response to induction and maintenance therapy. Differences between categorical data were detected with chi-squared analysis and for continuous data with unpaired t-tests.
Results: Between 2000 and 2008, 28 adolescents (age<25, in 2008) [26CD:1UC:1IC] and 40 adults [33CD:5UC:2IC] were treated with infliximab. Adolescents (YA) received infliximab earlier in their disease course than adults (AD) [YA 5 years vs AD 11.4 years, p<0.001 (95% CI = 2.79 to 10.5)]. Primary non-response to infliximab was not observed in the adolescent group compared with 7 out of 40 in the adult group (p<0.05). However, there was no difference between the proportion of patients losing response [YA 31% vs AD 37%, p = 1] or time to loss of response [YA 16.8 months vs AD 15.4 months, p = 0.87] during maintenance therapy; likewise the frequency of infusion reactions was comparable in the two groups. Patients who lost response to infliximab had dose escalation, increase in infusion frequency or switch to adalimumab with no difference in strategy between groups.
Conclusion: In keeping with their more severe disease phenotype, adolescents receive infliximab earlier in the natural course of their disease. Induction therapy in adolescents is more successful than adults. Prolonged response during maintenance therapy in adolescence is similar to randomised control clinical trial data.3
PM165 EPIDEMIOLOGICAL RISK FACTORS FOR CHILDHOOD ONSET INFLAMMATORY BOWEL DISEASE IN SCOTLAND: A CASE-CONTROL STUDY
1J. E. Van Limbergen, 1H. Spiers, 1R. Farhadi, 2M. L. Wilson, 3R. K. Russell, 4G. Mahdi, 5J. Satsangi, 2D. C. Wilson. 1Paediatric Gastroenterology and Nutrition, Royal Hospital for Sick Children, Edinburgh, UK, 2Child Life and Health, University of Edinburgh, Edinburgh, UK, 3Paediatric Gastroenterology, Yorkhill Hospital, Glasgow, UK, 4Paediatric Gastroenterology, Royal Aberdeen Children’s Hospital, Aberdeen, UK, 5Gastrointestinal Unit, University of Edinburgh, Edinburgh, UK
Introduction: The incidence of inflammatory bowel disease (IBD) is increasing among children in Scotland and is among the highest worldwide, yet the aetiology of IBD remains largely unknown. Genetic and environmental risk factors have been implicated. We have shown that the phenotype of childhood-onset IBD is more extensive than adult-onset IBD in Scotland, but also that the carriage of variants of genes implicated in IBD susceptibility (NOD2, IBD5, DLG5 and IL23R) does not differ between these Scottish IBD populations.1 2
Aims and Methods: We aimed to investigate the influence of a range of potential environmental factors in the development of paediatric IBD. 126 paediatric IBD cases (diagnosed <17 years of age; median age at diagnosis 9.8 years (Q1–Q3: 7.5 to 11.7)) were each matched with one control subject by age, sex and geographical location (to match for socio-economic status). Children with IBD and their parents were interviewed face-to-face to obtain data on breastfeeding, immunisation history, surgical and medical history and family history (FH). Control data were obtained via a postal questionnaire. Unifactorial analyses using the Chi-squared test and multifactorial analysis using binary logistic regression were performed.
Results: FH of IBD was associated with IBD (OR3.34; 95% (1.70 to 6.56) p = 0.0003). History of asthma, eczema and food allergy (OR 2.48 (1.28 to 4.78) p = 0.005, OR 2.83 (1.50 to 5.36) p = 0.001 and OR 2.98 (1.04 to 8.54) p = 0.03, respectively) show a significant association with paediatric IBD and CD. There were no significant differences between cases and controls regarding breastfeeding (52% vs 55%, p = 0.71). On multivariate analysis the significant factors were FH of IBD, bowel cancer and history of asthma and eczema (p<0.001, 0.033, 0.045 and 0.015, respectively). In contrast with findings on unifactorial analysis, no association of IBD with parental smoking during pregnancy, at birth and currently, was found in the multifactorial analysis, irrespective of FH of IBD.
Conclusion: We have shown an association between atopy and paediatric IBD but none with breastfeeding practices. Family history of IBD or bowel cancer is associated with IBD. Our epidemiological data are especially noteworthy in the context of the increasing number of genetic associations related to common inflammatory pathways identified in IBD and cancer.
PM166 2 YEAR FOLLOW-UP OF ADALIMUMAB THERAPY IN PATIENTS WITH CROHN’S DISEASE
1K. Kemp, 2M. Dibb, 2A. J. Makin, 2S. S. Campbell. 1Department of Gastroenterology and School of Nursing, Manchester Royal Infirmary and University of Manchester, Manchester, UK, 2Department of Gastroenterology, Manchester Royal Infirmary, Manchester, UK
Introduction: Adalimumab (Ad), a fully humanised, anti-TNF antibody, has demonstrated ability to induce and maintain remission in Crohn’s Disease (CD). There remains relatively little data on long-term safety data as well as long-term remission maintenance in CD.
Aims and Methods: A database of pts who received Ad over a 27 mth period (June 2006–September 2008) was created. Demographic data, SAEs, durability, time to loss of response, previous exposure to infliximab (IFx), concomitant immunosuppressive therapy and smoking status were evaluated. Loss of response to IFx was defined as the first occasion a reduction in dosing interval or increase in dose was required. Remission/relapses were based upon standard clinical, radiological and endoscopic criteria. Kaplan–Meier survival analysis was used to compare durability of response.
Results: A total of 25 pts (16F:9M), median age 44 years (17–73 years), were included. Twenty-one pts received an induction regime of 80/40 mg, 4 pts 160/80 mg followed by 40 mg EOW maintenance. Median follow-up was 6 months (2–27 months). Disease anatomy included colonic disease 4 (16%); ileocolonic 20 (80%); duodenal disease 1 (4%). Twenty-three (92%) pts received IFx prior to Ad with a median duration of IFx of 17.5 months (4–58 months). Patients were grouped into 3 categories: primary non-responders, 3 (12%), defined as failure to improve after 0, 2 infusions; loss of response 9 (36%) defined as an interval time of <5 weekly; and discontinuation of IFx due to side effects 11 (44%). Eight pts smoked and 12 pts were on concomitant immunosuppressive therapy. Median Rx with Ad was 6 months (2–27 months). Dose escalation of Ad (40 mg EOW to 40 WKLY) occurred in 5 (20%) pts with a median time to dose escalation of 10 months (range 2–12 months). The 5 pts received a loading dose of 80/40 mg with 1 pt on concomitant immunosupression therapy at time of dose escalation. SAEs were recorded, 1 cellulitis, 1 pneumonia and 1 viral meningitis. The SAEs resulted in the discontinuation of Ad in 2 pts (pneumonia and phial meningitis). No malignancy was detected. Comparisons were made between smoker and non-smoker as well as primary IFx non-responders vs secondary IFx non-responders. Time to dose escalation for both comparison groups was not significant. The 3 primary non responders to IFx are in remission with Ad. Sixteen (64%) of the 25 pts are in remission with Ad.
Conclusion: Concurring with Edinburgh, Ad is efficacious in the treatment of patients with CD who have lost response to, or suffered a reaction to IFx. The number of pts that required dose escalation is lower in our cohort. This may be due to a number of factors including shorter median follow-up (6 mths vs 12 mths) and differences in concomitant immunosuppressive therapy (48% vs 68%) raise the possibility that our pts had less severe disease. This study adds to the growing body of evidence and safety profile of Ad in every day clinical practice.
PM167 THE PROFILE OF INFLAMMATORY BOWEL DISEASE (IBD) IN THE UK. LESSONS LEARNED FROM THE IBD DATABASE (DB)
1K. D. Bardhan, 2A. Dhar, 1C. Royston, 3N. Simmonds, 4C. M. Edwards. 1Department of General Medicine, Rotherham NHS Foundation Trust, Rotherham, UK, 2Department of Gastroenterology, County Durham & Darlington NHS Foundation Trust, Bishop Auckland, UK, 3Department of Gastroenterology, Luton & Dunstable NHS Foundation Trust, Luton, UK, 4Department of Gastroenterology, South Devon Healthcare NHS Trust, Torbay, UK
Introduction: Safe clinical management of the IBD patient requires ready access to complete information, particularly for those with complex disease, often difficult using paper based case notes. The Rotherham IBD database, created to meet local needs, was developed for wider use for both individual patient management and collating information across centres. Results from 2 pilot centres were presented here previously 1. On behalf of the IBD-DB User Group we now present our results from across the UK.
Aims and Methods: Access® based, with a minimum dataset. Data were censored to the end of October 2006 and anonymised for analysis.
Results: See table. 11 432 patients from 21 centres across England and Northern Ireland were included. The demographic profile was broadly similar across centres.
Conclusion: We have learned that data need to be simple, well defined, validated and continuously updated. Although self-evident, these “simple needs” are not always achieved, particularly when information changes (eg, smoking), hence the need for updating data at every patient contact. A little data collected systematically from each patient and updated at every visit is more helpful than detailed data collected from few.
Observations: This large cohort shows the profile of IBD across the UK is similar to other large series. Each centre practices independently yet achieved reassuringly similar results suggesting we all strive towards “best practice.” Despite time and effort invested, gaps have emerged in our data, the result of variable interpretation of definition; thus there is room for improvement in the process of multi-centre data collection and handling. Our observations have bearing on the intended development of a National IBD-DB and give insight into the real effort required to sustain electronic patient records.
Database Facilities: “At a glance” summary, automated production of clinic letters, monitoring and audit. In conclusion, we have learned as much from the process of developing the IBD-DB as from the data generated.
PM168 WHO LOOKS AFTER PATIENTS WHEN THEY ARE HOSPITALISED AS AN EMERGENCY: NATIONAL-LEVEL ANALYSIS OF A SPECIALIST GASTROENTEROLOGICAL CONDITION
1K. Bodger, 2C. Grant-Pearce, 2E. Thompson, 2D. Lowe, 2M. Pearson. 1Gastroenterology Division, School of Clinical Sciences, 2Department of Clinical Evaluation, University of Liverpool, Liverpool, UK
Introduction: Crohn’s disease (CD) and Ulcerative colitis (UC) are treatable chronic disorders but decisions about when to use more complex drugs or opt for surgery are likely to require specialist care. Most patients expect to be cared for by a specialist but in the past, emergencies would be under the care of a physician on-call regardless of specialty. We examined Hospital Episode Statistics for England and assessed the proportion of patients with defined conditions discharged from the care of a known GI specialist (GI-Sp).
Aims and Methods: HES data for 2006/7 contain information on 2.236 million emergency admissions to 151 acute Trusts in England. A steering group of BSG representatives, physicians, surgeons, public health, patient groups and IT specialists guided the project. We identified all medical admissions with a gastroenterological diagnosis (13%) and defined Inflammatory Bowel Disease (IBD) as being the predominant reason for admission both when coded in the first diagnosis field and when ICD-10 codes for UC/CD were in the second or third fields but with diagnostic/symptom codes in the first field likely to be IBD-related (adding 25% to number of cases identified). There is no nationally complete list of GI-Sp, so lists were created with the help of the BSG, the national electronic staff record, augmented by telephone contacts to hospitals.
Results: There were 286 316 emergency medical GI admissions (13% of acute medical workload in England). 45.9% were with Benign Luminal Conditions, of which just 30.9% (IQR for Trusts: 26–37%) were coded at discharge under a “known” GI-Sp. There were 10 476 (3.6%) IBD admissions (5739 CD, 4737 UC) across 151 hospitals—a median of 34 (IQR 22 to 49) CD and 27 (IQR 19 to 40) UC patients per Trust. 62% of IBD patients were discharged under a known GI-Sp (IQR 53–72%; range 15–95% across trusts). 80% of IBD patients were aged <65 years so there was little overall effect from age-related admission policies. A plot of % under a GI-Sp vs total numbers of admissions showed a typical funnel plot with greater range in smaller hospitals but with no trends related to hospital size.
Conclusion: These data suggest that most patients admitted with GI problems will not be under the care of a GI-Sp at discharge. Local coding quality issues are a correctable source of error, the list of GI-Sp may be incomplete and obviously patients will be seen by GI-Sp as “ward consults” but remain under the care of a non-GI physician. Nevertheless, although twice as many patients with IBD seem to reach a GI-Sp at the time of discharge, there remains an apparently wide range between hospitals that is unrelated to size. Significant numbers may be managed by non-specialists. This probably reflects internal organisation/triage of hospitals but a shortfall in GI-Sp beds relative to the casemix of the emergency take may be a factor in some centres. [This project was funded by the NHS Information Centre]
PM169 EXPRESSION OF WNT FAMILY OF GENES IN PRIMARY HUMAN INTESTINAL MYOFIBROBLASTS
K. R. Hughes, Y. R. Mahida. Institute of Infection, Immunity and Inflammation, University of Nottingham, Nottingham, UK
Introduction: The Wnt family of secreted glycoproteins are important signalling molecules that regulate functions of intestinal epithelial stem cells and their progeny. Wnt signals are transduced after binding Frizzled (Fz) receptors and low-density lipoprotein-receptor-related protein (LRP) 5 and 6. Members of secreted Frizzled-related proteins (SFRPs) and Dickkopf families are inhibitors of Wnt signalling. In their location immediately subjacent to the basal surface of overlying epithelial cells, intestinal myofibroblasts are believed to be in a key position to regulate epithelial function.
Aims and Methods: Aim: To investigate the expression of Wnt family and related genes in cultures of primary human intestinal myofibroblasts. Pure cultures of normal colonic (NC), normal ileal (NI), ulcerative colitis (UC), and ileal Crohn’s disease (ICD) primary intestinal myofibroblasts were established following their migration via basement membrane pores present in intestinal mucosal samples denuded of the epithelium. Expression of the Wnt family of genes was studied by an RT-PCR array system. Transcripts were deemed to be strongly expressed if the cycle threshold (CT) value was <32, weakly expressed if the CT value was 32.1–35 (similar to the low expression housekeeper, hypoxanthine phosphoribosyltransferase), and not expressed if CT >35.
Results: In the RT-PCR array using cells isolated from NC (n = 3), NI (n = 2), UC (n = 3) and ICD (n = 3) mucosa, all the myofibroblast cultures expressed transcripts for Wnt 5A, Wnt 5B, Fzd 1, Fzd 2, LRP 6 and SFRP1. The majority (>70%) of the isolated myofibroblasts also either strongly (Fz 7, Fz 8) or weakly (Dickkopf 1, Fz 4, Fz 6, Wnt 2) expressed Wnt glycoprotein/receptors/inhibitor. Conventional PCR confirmed weak expression of Wnt 2. By contrast, transcripts of Fz 3, Fz 5, Wnt 1, Wnt 3A, Wnt 6, Wnt 7A, Wnt 7B, Wnt 8A, Wnt 10A, Wnt 11 and Wnt 16 were deemed not to be expressed by any of the myofibroblast cultures studied. Array analysis also demonstrated reduced expression of SFRP1 in UC myofibroblasts, which was confirmed by real-time RT-PCR using myofibroblasts isolated from UC (n = 7) and NC (n = 8) mucosal samples (3.34-fold reduction, p = 0.005).
Conclusion: In myofibroblasts isolated from normal and chronically inflamed intestinal mucosal samples, there is consistency in the expression of specific members of the Wnt family of genes. Compared with myofibroblasts isolated from normal colonic mucosa, those from ulcerative colitis samples showed significantly reduced expression of SFRP1. Since reduced SFRP1 expression has been associated with malignancy, low myofibroblast expression of this inhibitor of Wnt signalling may be implicated in increased risk of cancer in ulcerative colitis.
PM170 SULFASALAZINE, BUT NOT SULFAPYRIDINE OR 5-AMINOSALICYLIC ACID, INDUCES APOPTOSIS IN HUMAN INTESTINAL MYOFIBROBLASTS
K. R. Hughes, A. Robins, Y. R. Mahida. Institute of Infection, Immunity and Inflammation, University of Nottingham, Nottingham, UK
Introduction: Human intestinal myofibroblasts are prominent below the surface epithelium and are believed to play an important role in the pathogenesis of inflammatory bowel disease. Alterations in myofibroblast function may involve changes in proliferative capacity and/or susceptibility to cell death. In the presence of impaired epithelial barrier function and ulceration, the myofibroblasts become exposed to luminal constituents. These include orally administered drugs such as sulfasalazine (SUSZ), which may also be cleaved by luminal bacteria to sulfapyridine (SUPY) and 5-aminosalicylic acid (5ASA).
Aims and Methods: Aim: To investigate basal proliferation rate and susceptibility to cell death in myofibroblasts isolated from normal intestinal mucosal samples and those affected by ulcerative colitis (UC). Epithelial cells were removed, using EDTA, from normal colonic (NC) and ileal (NI) mucosal samples and those affected by UC. Myofibroblasts were subsequently established in culture, following their migration out of the lamina propria, and studied at passage 3–6. Propidium iodide-stained cells were studied by flow cytometry to assess those undergoing DNA synthesis (events in S phase of the cell cycle) and apoptosis (events in the hypodiploid/sub-G1 region). To assess proliferation, the myofibroblasts were cultured for 24 h in 0.1% fetal calf serum (FCS). Effects of SUSZ, SUPY and 5ASA were studied in myofibroblasts cultured (for 24 h) in the presence of 10% FCS. Data are expressed as mean (SEM).
Results: Compared with those isolated from NC (n = 11), greater proportion of myofibroblasts isolated from UC samples (n = 9) were in S phase [6.2(0.8)% vs 10.0(1.2)%; p = 0.01]. There was no significant difference in the basal rate of apoptosis in these cells [0.7(0.1)% vs 1.1(0.2)%]. Exposure to SUSZ resulted in a dose-dependent increase in the number of events in the sub-G1 region in myofibroblasts isolated from NC (n = 5), NI (n = 3) and UC (n = 3) samples (table). Apoptosis was confirmed by Hoechst staining. By contrast, there were no significant differences in the sub-G1 regions of myofibroblasts exposed to similar concentrations of SUPY [10 mM: 1.16 (0.21)%] or 5ASA [10 mM: 1.10 (0.20)%], compared with control medium [0.71 (0.22)%].
Conclusion: Compared with NC, myofibroblasts isolated from UC mucosa proliferate more rapidly. In vivo, this may lead to disruption of mucosal function in UC. In contrast to SUPY or 5 ASA, SUSZ induces apoptosis in intestinal myofibroblasts. Thus, compared with 5ASA, SUSZ may possess additional biological activities in vivo.
PM171 AUDIT OF NUTRITIONAL TREATMENT OF ACTIVE CROHN’S DISEASE IN ADULTS
L. M. McGeeney. Department of Nutrition and Dietetics, Box 119, Addenbrooke’s Hospital, Cambridge, UK
Introduction: Elemental diets (EDs) induce remission in Crohn’s Disease (CD) but doubt exists over the optimal subsequent nutritional management. Food reintroduction may be by a number of protocols, including the LOw Fat, Fibre Limited EXclusion (LOFFLEX) diet. This retrospective audit assessed the success of this treatment in everyday practice in matching standards achieved in previous carefully supervised research studies as regards the appropriateness of the referrals, remission rates on elemental diet and maintenance of remission at 2 years with the LOFFLEX diet.
Aims and Methods: Treatment success in 2003 was assessed by reference to patients’ dietetic and medical notes. Relapse was defined as the return of symptoms necessitating further medical treatment.
Results: Twenty-four patients started an ED on 29 occasions. Fifteen were female and 9 were male, aged 16–51. All referrals were for active CD and therefore deemed appropriate. Fourteen patients continued on medications at the start of ED. During 8 (28%) episodes patients did not complete the recommended 2 weeks of ED. On intention to treat analysis 20 (69%) of episodes on the ED achieved remission and 8 (28%) maintained remission with the LOFFLEX diet over 2 years. Per protocol analysis for those who followed the diets as recommended was 95% and 62% respectively. Two patients reported nausea and vomiting while on ED, but there were no significant long term side-effects. Overall results are shown in the table. The 2-year remission rate for compliant patients on medication was 75%, and 56% for those not on medication. All three audit standards were met.
Conclusion: ED followed by LOFFLEX has been shown to be an effective treatment in everyday practice for adults with active CD who are able to follow the diets. Supporting patients to aid adherence is essential to success and may be improved by increased specialist dietetic input. Concomitant medication is not essential to achieve remission.
Liver posters
PM172 POLYCHLORINATED BIPHENYLS IN BILE OF PATIENTS WITH BILIARY TRACT CANCER
1A. Adenugba, 2S. A. Khan, 2S. D. Taylor-Robinson, 3I. Cox, 4M. B. Toledano, 2A. V. Thillainayagam, 2D. S. Bansi, 1R. W. Gibson, 2H. C. Thomas, 1A. J. Beck. 1Faculty of Natural Sciences, 2Hepatology and Gastroenterology, 3Imaging Sciences, 4Epidemiology & Public Health, Imperial College London, London, UK
Introduction: Polychlorinated biphenyls (PCBs) are anthropogenic, organic compounds. Although banned in the 1970s, PCBs are poorly biodegradable and hence ubiquitous in the environment. They accumulate in adipose tissue and are implicated in various malignancies, including breast and pancreatic cancer. The hepatobiliary system is the main excretory route for such xenobiotic toxins. Incidence rates of intrahepatic biliary tract cancer are increasing worldwide. Measurement and comparison of PCB levels in bile from human patients with benign and malignant bile duct disease have not previously been done.
Aims and Methods: The aims were to compare PCB concentrations in bile from patients with malignant (n = 8) and non-malignant (n = 7) biliary disease. Fifteen human bile samples, collected endoscopically, were analysed using gas chromatography mass spectrometry for seven target PCB congeners (28, 52, 101, 118, 153, 138 and 180), known to occur in the environment and food.
Results: Amongst males, total PCB concentrations in bile ranged from 6 ng/ml (aged 73 years) to 49 ng/ml (aged 90 years), and in females from 8 ng/ml (aged 33 years) to 43 ng/ml (aged 67 years) bile. Although there was no overall difference in mean PCB levels between non-cancer and cancer patients, levels of congener 28 were significantly higher in patients with biliary tract cancer (p<0.05).
Conclusion: Despite the banning of PCBs over 30 years ago, these xenobiotics are present in the bile of patients with biliary disease. PCB levels tend to increase with age, suggesting chronic bioaccumulation. Further research is necessary to investigate the relevance of increased levels of congener 28 in bile in biliary tract cancer.
PM173 UPDATE OF INCIDENCE AND MORTALITY RATES AND REVIEW OF DIAGNOSTIC TRENDS FOR INTRAHEPATIC CHOLANGIOCARCINOMA AND SELECTED HEPATOBILIARY TUMOURS IN ENGLAND AND WALES
1M. B. Toledano, 2A. Mehtan, 1P. Elliott, 2S. D. Taylor-Robinson, 2H. C. Thomas, 2S. A. Khan. 1Epidemiology & Public Health, 2Hepatology and Gastroenterology, Imperial College London, London, UK
Introduction: The increasing mortality from primary liver cancer in England and Wales has largely resulted from a marked rise in age-standardised incidence and mortality rates (ASIR and ASMR) of intrahepatic bile duct (IHBD) malignancy.
Aims and Methods: The primary aim was to update age- and sex-specific trends in mortality and incidence rates of pancreatico-hepatobiliary malignancy in England and Wales. The secondary aim was to analyse trends in histology and the basis of diagnosis, using cancer registry data. Incidence and mortality data for England and Wales were obtained from the Small Area Health Statistics Unit. Directly age-standardised rates (based on the European standard population) and age-specific rates for selected tumour sites in males and females were calculated up to 2004 for incidence and 2005 for mortality. For selected sites, the annual percentage of cases was determined according to major morphological subtypes and modalities employed in diagnosis.
Results: ASIR and ASMR for primary liver tumours (PLT, predominantly representing hepatocellular carcinoma) have risen to their highest levels. The rate of increase has accelerated considerably in the over-65 age group since 2001. ASMR and ASIR have continued to rise for IHBD malignancy, whereas for EHBD malignancy they have continued to fall. Rates for gallbladder carcinoma have remained stable. Trends in morphological coding and basis of diagnosis suggest a possible influence of improvement in case ascertainment on the epidemiological trends of hepatobiliary tumours.
Conclusion: Although PLT rates have increased, IHBD malignancy remains the most common cause of death from a liver tumour in England and Wales. Trends in PLT are likely to represent the delayed manifestation of progression to hepatocellular carcinoma in HCV-related cirrhosis. Further research is required in order to elucidate the reason for the divergent trends in IHBD and EHBD malignancy, which cannot be entirely attributed to artefact. Continued monitoring of incidence and mortality trends in hepatobiliary tumours is recommended.
PM174 LONG TERM OUTCOME IN AUTOIMMUNE HEPATITIS (AIH): RELATIONSHIP TO AZATHIOPRINE TREATMENT
1B. S. R. Höeroldt, 2E. McFarlane, 1P. Basumani, 2D. Gleeson. 1Gastroenterology, Rotherham General Hospital, Rotherham, UK, 2Hepatology, Sheffield Teaching Hospital, Sheffield, UK
Introduction: Standard therapy of AIH consists of Prednisolone plus Azathioprine (AZA) 1 mg/kg BW/day to induce remission. Subsequently, AZA maintenance therapy 1–2 mg/kg BW/day is commonly employed in an attempt to prevent disease relapse. However, the long-term effects of AZA treatment on disease progression are not established.
Aims and Methods: Aim: Retrospective analysis of the relationship between AZA treatment and long-term outcome in AIH. Methods: Kaplan–Meier life table analysis, log rank test, Cox multiple regression analysis.
Results: 248 patients with definite (n = 160) or probable AIH by International AIH Group criteria1 presenting to a single centre between 1971 and 2007 were included. 208 patients received AZA for median (range) 5 (0.1 to 30) years, comprising a median of 85% of the total period of follow-up for per patient (range 0–100%). Median AZA dose throughout the period of treatment was 83 mg/d (1.3 mg/BW). 231 patients achieved initial clinical and biochemical remission (serum ALT<50) within 12 months. Liver related death or transplant rate was 13+3% and 33+5% after 10 and 20 years respectively and: (a) as previously reported2 it was significantly correlated with decompensation at presentation, failure of serum ALT to normalise and relapse rate; (b) it was higher in patient not given AZA (n = 40) than in those receiving AZA (n = 208); however in patients (n = 240) followed up for >6 months, rates were identical; (c) it was inversely related to length of AZA treatment (as expected because this was closely correlated with total follow-up period); (d) however it was not significantly related to % of total follow-up period on AZA; (e) it was not significantly related to length of AZA treatment (categorised as 0, 0.1–2, 2–5, 5–10 and >10 years) in patients (n = 116) already followed up for 10 years or more; (f) in patients given AZA, it was not significantly related to mean dose or dose/kg BW over the treatment period. Results were essentially the same if all-cause death or liver transplantation was considered and also after excluding patients (n = 43) who also received other immunosuppressive agents apart from Prednisolone.
Conclusion: In this large retrospective analysis, we were unable to detect a relationship between long-term AZA treatment of AIH and outcome. The efficacy of long-term AZA maintenance treatment in AIH requires formal prospective evaluation.
PM175 PATIENTS WITH M2 ANTIBODIES—WHAT DIAGNOSIS AND FOLLOW-UP ARE THEY GIVEN?
1E. A. L. Byrne, 1R. Katbamna, 2C. Scott, 1S. W. Coppack, 1G. R. Foster. 1Hepatology, 2Immunology, ICMS, Barts and The London School of Medicine, London, UK
Introduction: The M2 substrate of antimitochondrial antibody (AMA) is over 95% sensitive and specific for the diagnosis of Primary Biliary Cirrhosis (PBC) or its future development.1–3 The American Association for the Study of Liver Disease recommends a diagnosis of PBC can be made with a positive AMA and cholestatic liver biochemistry (biopsy can be used to confirm) and that patients who are AMA positive only should be followed up with annual liver biochemistry.1
Aims and Methods: Our aim was to evaluate whether the AASLD guidelines were followed in patients testing positive for M2 antibody between January 2004 and July 2008. The records of these patients were reviewed to address this issue.
Results: See figure. Of the 39 patients who were M2 positive but without a diagnosis of PBC, 15 have had liver biochemistry within the last year. Five of the 39 patients have had no liver tests at all. 32 of the 39 patients have been seen in clinic since the test, in 7 cases clinic letters mention the positive M2 but do not discuss its relevance, 3 mention the positive M2 but say it is irrelevant, 2 mention the positive M2 and give the correct advice but this was not subsequently followed up, and in 20 cases the positive M2 is not commented on at all.
Conclusion: Early PBC is being underdiagnosed and underinvestigated. Less than 50% (35/74) of patients testing positive for M2 antibodies were followed up appropriately. Of the patients with positive M2 antibody who were not diagnosed with early PBC, 61.5% (24/39) were not receiving the advised annual follow-up; this figure could be higher as we are yet to see whether patients testing positive in 2008 (n = 5) are appropriately followed up. 28% (11/39) of the patients not diagnosed with PBC had a raised Alk Phos at the time of the test, this should have led to a diagnosis of probable PBC. Many patients with a positive M2 antibody test are being seen in clinic yet are not receiving the appropriate diagnosis and follow-up, suggesting a need for better education.

PM176 APOPTOSIS AND ITS REGULATORY PROTEINS FAS AND BAX IN EXPERIMENTAL SCHISTOSOMIASIS: RELATIONSHIP TO HEPATIC FIBROSIS
1H. A. El Aggan, 1E. H. El Kashef, 2N. M. Baddour, 3M. M. Essa. 1Department of Medicine, 2Department of Pathology, 3Department of Parasitology, Faculty of Medicine, University of Alexandria, Alexnadria, Egypt
Introduction: Apoptosis plays an important role in the pathogenesis of different liver diseases. Schistosomiasis leads to granuloma formation and fibrosis in the liver. Therefore, the present study was designed to evaluate the role of apoptosis and its regulatory pro-apoptotic proteins, Fas and Bax, in the progression of liver disease in experimental schistosomiasis.
Aims and Methods: Ninety Swiss Albino mice were infected with 150 Schistosoma mansoni cercaria. Every 10 infected mice were sequentially sacrificed at 3, 5, 7, 8, 9, 10, 13, 15 and 20 weeks post-infection and 10 non-infected mice were used as controls. The livers of sacrificed mice were examined using the in situ end labelling (ISEL) method for detection of apoptosis and by immunohistochemical staining for identification of the pro-apoptotic proteins, Fas and Bax and for the assessment of the proliferating cell nuclear antigen labelling index (PCNA-LI) as a marker of cell proliferation. Hepatic fibrosis was evaluated by a semi-quantitative scoring system using Masson trichrome stain.
Results: The liver of infected mice showed significant increases in the apoptosis rate, Fas and Bax expression and fibrosis score compared with normal liver tissues (p<0.05). During the course of infection, apoptosis and Bax and Fas proteins in the liver were detected in the early stages of the disease starting from in the 8th week post-infection and continued to increase progressively with the advance of infection in parallel with the progressive increases in periportal fibrosis (p<0.05). The apoptosis rate/PCNA-LI ratio was significantly higher in the livers of infected mice than in the control livers during all stages of the disease particularly at the 13th week (p<0.05). The apoptosis rate and Fas and Bax expression were positively correlated with the fibrosis score in the liver (p<0.05).
Conclusion: It can be concluded that the increase in apoptosis rate in the liver with overexpression of the pro-apoptotic proteins, Fas and bax may play a role in the development and progression of hepatic fibrosis in schistosomiasis. Meanwhile, the increase in the absolute proliferating capacity of the liver cells cannot compensate for the enhancement of apoptosis in this disease.
PM177 BACTERIAL OVERGROWTH AND TRANSLOCATION IN CIRRHOTIC LIVER DISEASE USING 16S RNA TECHNIQUES
H. Steed, K. L. Blackett, S. Macfarlane, M. Miller, G. T. Macfarlane, J. F. Dillon. Pathology and Neuroscience, University of Dundee, Dundee, UK
Introduction: A third of deaths in cirrhotic patients are attributable to sepsis. Most of these infections are due to Gram-negative bacteria, predominantly E coli. In animals, the gut has been shown to be the principal source of these organisms, which invade through a process known as bacterial translocation. The primary mechanism of translocation has been assumed to be bacterial overgrowth of the small bowel. Examinations of jejunal aspirates in chronic alcoholics show a higher incidence of anaerobic bacteria, while patients with severe chronic hepatitis have lower numbers of faecal bifidobacteria and bacteroides, and increased yeasts and enterobacteria. These changes are associated with raised levels of serum TNF-α.
Aims and Methods: To identify, quantitate and visualise specific bacterial species colonising small bowel mucosae in patients with chronic liver disease, and compare these with subjects without liver disease. Thirty-three consecutive patients were recruited into the study, 10 without cirrhosis and 23 with cirrhotic liver disease (18 Child’s A, 5 Child’s B, 14 with alcoholic liver disease with the remainder being a mixture of other aetiologies). Patients were excluded if they had received antibiotics in the last 3 months, used probiotics or H2 antagonists. Six distal duodenal biopsies were obtained and snap frozen for RNA and DNA extraction, or frozen for fluorescence in situ hybridisation. Peripheral venous blood samples were obtained from 30 patients, 8 controls, 4 NAFLD, 1 post liver transplant and 17 chronic liver disease patients (10 Child’s A, 5 Child’s B, 2 Child’s C). Tayside tissue bank provided 5 samples of liver tissue from hepatocellular carcinoma patients. Bacterial DNA and RNA were extracted and analysed by real-time PCR, using group, genus and species-specific primers to assess total bacteria, bifidobacteria, bacteroides, enterobacteria, staphylococci, streptococci, lactobacilli, enterococci, Helicobacter pylori and moraxella, as well as TNF-α, IL8 and IL-18.
Results: Bacteria were present in low numbers in the small bowel at 101–102 biopsy. Based on 16S rRNA gene copy numbers per 1000 GAPDH molecules, there was no evidence of bacterial overgrowth of total bacteria or any of the individual bacterial groups, with the exception of enterococci, which were present in significantly higher numbers in the cirrhotic group. There were no statistically significant differences between the patient groups in any of the cytokines investigated. There was no difference in the level of E coli found in any of the blood samples compared with the control group and the liver tissue group.
Conclusion: This investigation found no evidence of bacterial overgrowth or translocation in cirrhotic patients. Acknowledgments: Foundation of Liver Research, Tayside Tissue Bank.
PM178 WITHDRAWN
PM179 PREVALENCE OF CLOSTRIDIUM DIFFICILE ASSOCIATED DIARRHOEA AFTER LIVER TRANSPLANTATION AND RISK FACTORS FOR ITS DEVELOPMENT: A UK-BASED SINGLE CENTRE CASE CONTROL STUDY
I. C. Coltart, N. Stoesser, A. Gera, A. Verma, E. Sizer, G. Auzinger, W. Bernal, J. Wendon. Institute of Liver Studies, King’s College Hospital, London, UK
Introduction: Clostridium difficile associated diarrhoea (CDAD) is the leading cause of nosocomial diarrhoea, and its incidence is increasing in hospitals worldwide. Liver transplant recipients are high risk candidates for CDAD. Rates of CDAD after liver transplantation are quoted between 3.5% and 8%; however, there are no recent studies in a UK transplant unit.
Aims and Methods: We retrospectively identified all cases of CDAD in patients who received a liver transplant at King’s College Hospital between January 2006 and April 2007. A diagnosis of CDAD was made on the basis of clinical symptoms (abdominal pain and diarrhoea) and a positive Clostridium difficile toxin stool assay. We reviewed data for all patients who developed CDAD in the first 90 days post-operatively. Detailed demographic, physiological, laboratory and microbiological data were collected using hospital notes, prescription charts and clinical databases. Additionally we reviewed donor characteristics, and transplant operation details. These data were compared with a cohort of 31 patients, transplanted between 2005 and 2007, matched for age, sex and aetiology of liver disease.
Results: 191 adult patients underwent liver transplantation during the study period and 16% (31/191) developed CDAD. Ninety per cent (28/31) developed CDAD in the first 90 days post-transplant. Median age was 50.2 years (IQR = 40.8 to 56.7), and 17 (59%) were female. Most were transplanted for chronic liver disease; however 6 (21%) had acute liver failure. Median MELD score prior to transplant was 16.8 (IQR 14.2 to 30.0). Median number of days post transplant until diagnosis of CDAD was 15.5 days (IQR 7.3 to 31.0). Risk factors for the development of CDAD included longer length of stay prior to transplantation: (4.0 days vs 0.0 days p = 0.017), longer total length of stay in hospital (60.0 days vs 23.0 days p<0.001), steatotic graft (50% vs 23% p = 0.028) and high donor body mass index (26.8 kg/m2 vs 24.7 kg/m2 p = 0.005). Those patients with CDAD also had a higher rate of colonisation with Acinetobacter (14% vs 0% p = 0.045). There was no statistical difference in number of courses of antibiotics post transplantion, type of immunosuppression, use of proton pump inhibitors or rate of complications (bleeding, bile leak, episode of acute cellular rejection). Additionally, there was no difference in the rates of patients with organ failure following transplantation, or pre-transplant MELD score. No patient had clinical evidence of megacolon, required surgery or died as a direct consequence of their CDAD.
Conclusion: CDAD is common after liver transplantation. Risk factors for its development in the first 90 days relate to time in hospital and graft steatosis.
PM180 IDENTIFICATION AND INTERVENTIONS IN ALCOHOL MISUSE RELATED ACUTE HOSPITAL ADMISSIONS
J. J. Hurley, B. Lee, J. Turner, K. Axe, G. L. Swift. Gastroenterology, Univeristy Hospital Llandough, Penarth, UK
Introduction: Fifteen per cent of acute hospital admissions can be directly attributed to the misuse of alcohol, taking up 30 000 bed days a year and costing in excess of £85 million a year to the Welsh NHS.1 Up to 20% of patients admitted to hospital for non-alcohol related conditions are found to be consuming hazardous levels of alcohol defined as alcohol intake exceeding the recommended limit and likely to cause harm.2 Hazardous drinkers who are not alcohol dependent have been found to benefit from “brief interventions” which include discussions raising the awareness of potentially harmful drinking. This can be carried out by doctors or trained nurses, and have been shown to cut alcohol intake by up to 20% in those patients not directly seeking treatment for alcohol dependence.3
Aims and Methods: A case note review of all inpatients admitted to University Hospital Llandough was carried out over a 48 hour period in May 2008. The reason for admission, documentation of alcohol history, and crude biochemical markers such as the mean corpuscular volume (MCV), and gamma GT (GGT) were recorded in order to identify patients admitted as a direct result of alcohol or likely to be at risk of alcohol-related complications. Any utilisation of alcohol intervention was also recorded.
Results: 335 patients (148 male and 187 female) were included in the study. 37 (11%) patients were admitted as a direct result of alcohol, including decompensated liver disease and acute intoxication. 32 (9.5%) patients (14 males, 18 females) were identified as drinking over the recommended limit. Only 8 of these patients received any form of brief intervention, 3 were offered alcohol liaison services, and 5 were given verbal advice. 158 (47%) patients (65 males and 93 females) had no documentation of alcohol intake. 33% of patients with no documentation of alcohol intake had elevated liver function tests and 9% had raised MCV (no other aetiology identified). GGT was rarely performed. Two patients admitted for reasons unrelated to alcohol and without a documented alcohol history developed features of alcohol withdrawal syndrome on the ward.
Conclusion: Failure to identify alcohol misuse amongst acute inpatients may result in missed opportunities to intervene before hazardous drinking becomes harmful as well as leading to episodes of alcohol withdrawal during the admission. The psycho-social care of hazardous and harmful drinkers requires improvement, with low numbers of patients appearing to have had any form of brief intervention and uptake of alcohol liaison services underutilised. A combined approach, considering clues in the medical history and examination, self-reported consumption, biochemical markers and a high score on standardised screening questionnaires needs to be undertaken to identify those who consume alcohol above the recommended levels.
PM181 EARLY EXPERIENCE OF GRANULOCYTAPHERESIS (ADACOLUMN) IN SEVERE ALCOHOLIC HEPATITIS
1J. M. Morris, 1M. Neilson, 1S. Dickson, 2P. Hodgins, 1E. H. Forrest. 1Gastroenterology, Glasgow Royal Infirmary, Glasgow, UK, 2Otsuka Pharmaceuticals (UK), London, UK
Introduction: Controversy continues regarding the management of alcoholic hepatitis (AH). Reports from Japan have suggested Granulocytapheresis (GCAP) as a possible treatment for severe AH.1 2 This treatment has also been advocated for other TNFα driven diseases such as rheumatoid arthritis and Crohn’s disease.
Aims and Methods: We aimed to assess the tolerability of GCAP therapy in a group of patients with severe AH. Patients with severe AH were identified with a Glasgow Alcoholic Hepatitis Score greater than or equal to 9. Patients underwent an initial GCAP treatment with another planned for 1 week later if possible. Clinical and laboratory responses to this treatment were noted.
Results: Six patients were identified and received GCAP therapy. All patients had received prednisolone treatment (40 mg/day), but 4 were non-responders (<25% fall in bilirubin after 1 week) at the time of GCAP and had been converted to pentoxifylline treatment (400 mg tds). All but two patients received only one GCAP treatment. All patients tolerated GCAP without haemodynamic compromise. Patient characteristics at the time of GCAP and subsequent outcome are shown in the table. The mean fall in bilirubin 48 h after treatment was 12±16% (p = 0.2). Cause of death was variceal haemorrhage in one patient, pneumonia in one patient and multi-organ failure in the remaining 3 patients. The surviving patient was a steroid-responder.
Conclusion: GCAP was tolerated by this group of patients with severe AH. There was a trend towards a reduction in serum bilirubin in the 48 hours after treatment. However this small study failed to identify any improvement in outcome with GCAP.
PM182 AUTONOMIC DYSFUNCTION MEASURED BY BAROREFLEX SENSITIVITY IS MARKEDLY ABNORMAL IN STABLE CIRRHOSIS DESPITE MINIMAL SYSTEMIC HAEMODYNAMIC CHANGES
K. A. Rye, G. Mortimore, A. Austin, J. Freeman. Liver Unit, Digestive Diseases Centre, Derby City General Hospital, Derby, UK
Introduction: Baroreceptor sensitivity (BRS) is well recognised as a composite marker of the overall integrity of the autonomic nervous system, maintaining cardiovascular status both at rest and during physiological stress. Autonomic dysfunction occurs in 43–80% of cases of cirrhosis, affecting both sympathetic and parasympathetic branches. BRS impairment occurs independently of aetiology and correlates with disease severity and the hyperdynamic circulation. BRS has been studied extensively in advanced disease, especially pre-transplantation but less so in more compensated disease. Impaired BRS is associated with a 5-fold increase in mortality, independent of cirrhosis stage, yet can be improved by drugs and liver transplantation.
Aims and Methods: The aim of this study was to determine the prevalence of BRS abnormalities in a stable population of cirrhotics. We studied 16 cirrhotic patients with stable disease for >6 months. Systemic haemodynamics and BRS were assessed non-invasively in the supine position on two different days using the Finometer® (TNO instruments, Amsterdam). Data were downloaded to a PC-based analysis program (Beatscope®). Spontaneous BRS was assessed using software studying the relationship between inter-beat variability and beat-to-beat changes in systolic blood pressure. Portal pressure was assessed by measurement of the hepatic venous pressure gradient (HVPG).
Results: Median age 47 (30 to 67) years, 63% male, median Child–Pugh (CP) score 6 and MELD 11. 94% alcoholic aetiology, 69% abstinent. 9/16 (56%) concomitant spironolactone. Median haemodynamic data as follows: systolic BP 147 (115 to 169) mm Hg, diastolic BP 82 (65 to 103) mm Hg, MAP 104 (87 to 131) mm Hg, HR 89 (54 to 117) bpm, SV 89 (36 to 164) ml, CO 7.0 (3.5 to 12.0) lpm, PVR 0.98 (0.45 to 2.14) MU, HVPG 18 (7 to 25) mm Hg. 12/16 (75%) had abnormal BRS (normal 8 to 10 ms/mm Hg) with median BRS 3.38 (1.14 to 11.19) ms/mm Hg. Sequential BRS readings were not significantly different (3.38 vs 3.98 ms/mm Hg, p = 0.87). Systemic haemodynamics were not significantly different in patients with impaired BRS compared with those with normal BRS. BRS did not correlate with disease severity (CP A 2.96 vs CP B 3.80 ms/mm Hg, p = 1.0), systemic haemodynamics, serum sodium or variceal size. There was a significant negative correlation between BRS and HVPG (r = −0.523, p = 0.045).
Conclusion: Autonomic function as assessed by BRS is frequently abnormal in stable cirrhotic patients. Abnormalities of BRS are not associated with marked haemodynamic changes, suggesting that it is predominantly the vagal aspect that is impaired in stable disease. Abnormalities of BRS are associated with HVPG which may suggest that portal pressure itself plays a pivotal role in its causation. The significance of impaired BRS in this stable group needs to be determined by assessing long-term outcome.
PM183 TISSUE ADVANCED GLYCATION ENDPRODUCTS IN TWO POPULATIONS ASSOCIATED WITH INCREASED OXIDATIVE STRESS: NORMAL IN CIRRHOSIS BUT ELEVATED IN HAEMODIALYSIS PATIENTS
1K. A. Rye, 1G. Mortimore, 2S. John, 2H. Jefferies, 2S. Korsheed, 2P. Owen, 2R. Fluck, 3C. McIntyre, 1A. Austin, 1J. Freeman. 1Liver Unit, Digestive Diseases Centre, 2Department of Renal Medicine, Derby City General Hospital, Derby, UK, 3School of Graduate Entry Medicine and Health, University of Nottingham, Derby, UK
Introduction: Advanced glycation endproducts (AGE) result from non-enzymatic glycation between reducing sugars and proteins and are a measure of cumulative metabolic stress. Tissue and serum AGE are known to predict cardiovascular mortality in end stage renal disease. Serum AGE levels are elevated in euglycaemic cirrhotics and correlate with disease severity yet cirrhosis appears to be protective against coronary atherosclerosis. Tissue AGE has not been assessed in cirrhosis.
Aims and Methods: We aimed to assess tissue AGE in two populations with increased oxidative stress: cirrhosis and haemodialysis (HD) and determine whether skin AF is a non-invasive marker of liver disease severity. We studied 56 patients (28 cirrhotics, 28 age and sex matched HD patients) and compared with a normal control database (NC). Tissue AGE was measured using UV autofluorescence (AF) (AGE Reader, DiagnOptics, The Netherlands). Three sequential readings were taken from the palmar aspect of the forearm, approximately 10 cm below the elbow, avoiding pigmentation or vascular structures. History of diabetes mellitus (DM) and ischaemic heart disease (IHD) was noted and Child–Pugh (CP) and Model for End Stage Liver Disease (MELD) scores calculated.
Results: Mean age 56±15 years, 64% male. 71% alcoholic cirrhosis, median CP score 8, MELD 12. DM and IHD prevalence was similar in both groups; no cirrhotic patient had renal impairment. Compared with NC, mean AF was significantly higher in both HD (3.264 vs 2.218, CI 0.691 to 1.402, p = <0.0001) and cirrhosis (2.632 vs 2.218, CI 0.082 to 0.746, p = 0.016). When cirrhotic patients with DM and IHD were excluded, this became insignificant (2.352 vs 2.157, CI to 0.116 to 0.506, p = 0.209). Mean AF was significantly higher in HD compared with cirrhosis (3.264 vs 2.632, CI 0.180 to 1.084, p = 0.007).
Conclusion: Despite high levels of cumulative metabolic stress in both HD and cirrhosis, tissue AGE is only increased in HD. Both conditions are associated with elevated serum AGE levels but the mechanism underlying the differential tissue deposition is unknown. One hypothesis that may explain the reduced cardiovascular risk in cirrhosis is that soluble RAGE acts as a decoy receptor preventing AGE-RAGE interaction and the resulting endothelial dysfunction. Skin AF measurement is unhelpful as a non-invasive tool to detect cirrhosis.
PM184 MORTALITY RATES IN CIRRHOTIC PATIENTS ADMITTED TO ICU: THE VALUE OF PROGNOSTIC SCORES ON ADMISSION
1L. A. Possamai, 2A. Gordon, 2M. Gribbon. 1Hepatology, 2Intensive Care, Imperial College, London, UK
Introduction: Patients with cirrhosis who require admission to intensive care experience poor outcomes. Accurate identification of the minority who will survive to discharge from hospital would be of great clinical value when making the difficult decision to offer or withhold ICU level care. Disease-specific and ICU prognostic scores are widely used in clinical practice. It has yet to be established which prognostic score best predicts ICU-associated mortality in this patient population.
Aims and Methods: Charing Cross Hospital ICU database was searched for patients admitted from January 2004 to August 2008 with a diagnosis of cirrhosis. The electronic notes of 117 patients were reviewed. Patients were included if there was an established diagnosis of chronic liver disease and either imaging or biopsy evidence of cirrhosis or clinical evidence of portal hypertension. Prognostic scores were calculated from admission data.
Results: 62 separate admissions fulfilled the inclusion criteria. The overall unit mortality was 50% and hospital mortality 76% with 12 patients surviving to discharge. The mortality associated with values above and below the median for the different prognostic scores is shown in the figure. Receiver–operator characteristics showed the MELD, MELDNa, SOFA, APACHE II and Bilirubin to have similar value at predicting hospital mortality with AUC values of 0.756 (+/−0.07standard error) 0.740 (+/−0.07) 0.754 (+/−0.08) 0.64 (+/−0.08) and 0.746 (+/−0.06) respectively. The serum sodium level had no predictive value with a AUC of 0.48 (+/−0.08)
Conclusion: Hospital mortality for cirrhotic patients admitted to a general ICU over the last 44 months was 76%. The MELDNa score was no better at predicting mortality than the MELD score. Serum sodium had no relationship to mortality. Serum bilirubin alone was as accurate a predictor of hospital mortality as the MELD, MELDNa, APACHE II and SOFA scores.
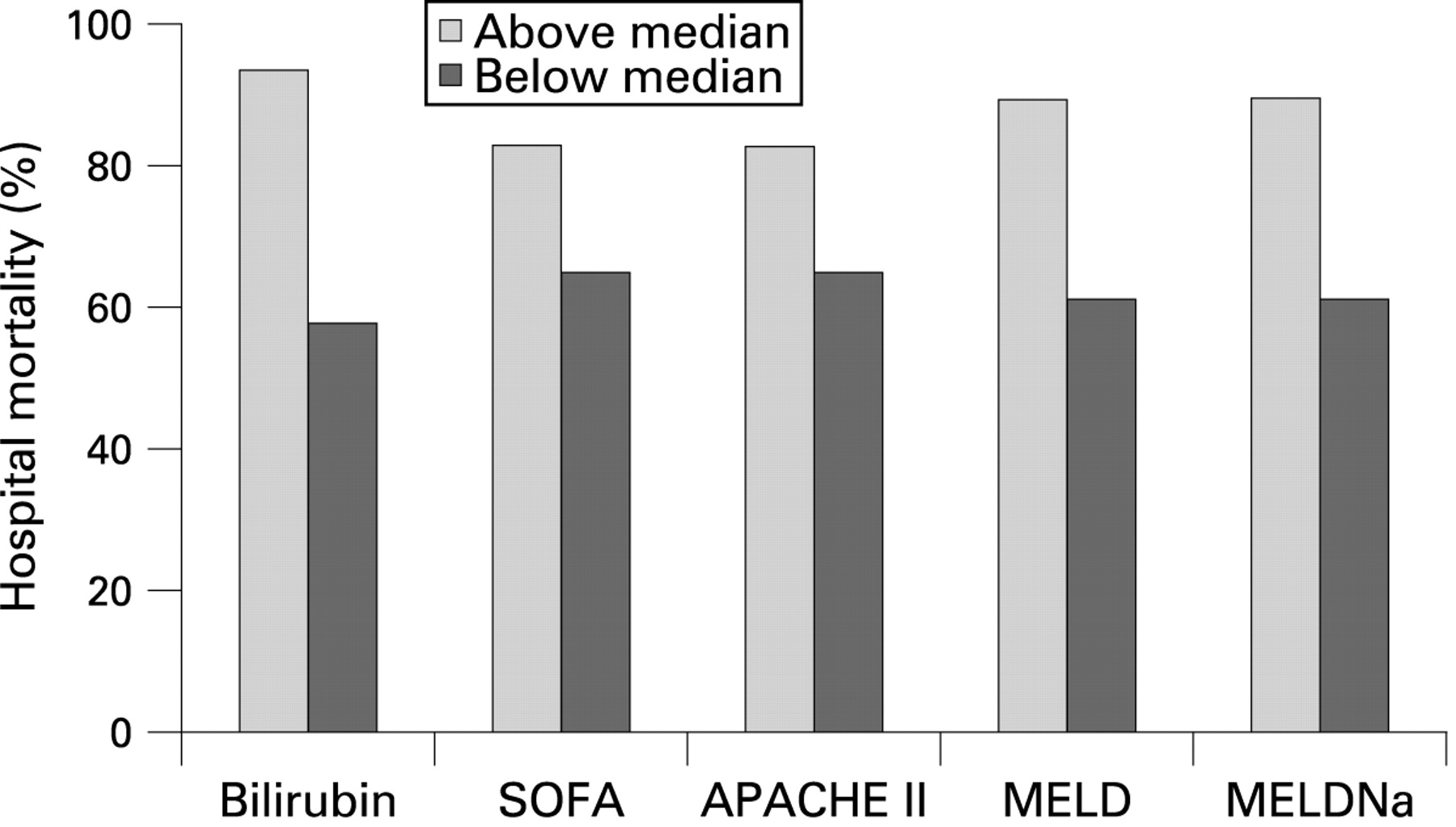
PM185ANAEMIA IN THE POST LIVER TRANSPLANT POPULATION—AN UNDER-INVESTIGATED PROBLEM
I. Corless, C. Preston, C. Millson. Hepatology—Ward 71, St James University Hospital, Leeds, UK
Introduction: Anaemia is common in the transplant population but the prevalence in liver recipients is unknown. In this complex group, anaemia is often multifactorial, particularly in the longer term (>6 months) when post surgical complications are less likely. It is important to identify and investigate anaemia since it can be a cause of significant morbidity and may be an indicator of undiagnosed pathology. Despite this, there is little published advice available on optimal management of this group.
Aims and Methods: The initial audit was performed to ascertain the prevalence of anaemia in our post transplant population and to assess whether these patients were identified and managed appropriately. Following the development of a guideline, we re-audited to investigate whether its introduction had affected our practice. Anaemia was defined as haemoglobin <12 g/dl in males and <11 g/dl in females. All anaemic patients at least 6 months post transplantation were included and a case note review undertaken to ascertain both the actual and documented prevalence. We identified whether a relevant history had been taken and whether appropriate investigations had been performed. A guideline was subsequently developed as a recommended management pathway for anaemic patients. Six months later, a subset of the population was re-audited to see if improvements had occurred following introduction of the guideline.
Results: The initial audit demonstrated a prevalence of anaemia of 11.7%. This was documented by medical staff in 51% of cases. Haematinics were checked in 61%. No cause was found for anaemia in 30.6% of the identified patients. Medication was identified as the cause of anaemia in 11% of people and this resulted in a change of drug in one patient. In the second audit, the prevalence was similar at 13.7%. Anaemia was documented in a greater proportion of the group (69.4%) and haematinics were checked in 80%. 64% of the identified group had a documented cause for the anaemia and a further 32% were undergoing investigation. There was no documented cause and no plan for investigation in 4%. A significant proportion of the patients with anaemia had not been identified by medical staff. Across the whole group, 19% of those with anaemia had not been investigated in accordance with the guideline.
Conclusion: Following introduction of the guideline, we found a greater number of anaemic patients were identified. The majority of these were appropriately investigated to rule out significant pathology. However, despite the improvements, a sizeable proportion of the group were still not being identified. The initial audit cycle has demonstrated a need to increase staff awareness of anaemia in the post transplant population and to repeat the audit process in future.
PM186 SHORT T-LYMPHOCYTE TELOMERE LENGTH COMPROMISES SUSTAINED VIROLOGICAL RESPONSE WITH PEGYLATED INTERFERON-ALPHA AND RIBAVIRIN IN CHRONIC HEPATITIS C VIRUS (HCV) INFECTION
1M. Hoare, 1W. T. H. Gelson, 2S. E. Davies, 3M. D. Curran, 4S. L. Vowler, 5A. N. Akbar, 1G. J. M. Alexander. 1Department of Medicine, 2Department of Pathology, University of Cambridge, Cambridge, UK, 3Clinical Microbiology and Public Health Laboratory, Health Protection Agency, 4Centre for Applied Medical Statistics, Department of Public Health and Primary Care, University of Cambridge, Cambridge, UK, 5Department of Immunology and Molecular Pathology, Royal Free and University College Medical School, London, UK
Introduction: Ageing is associated with impaired immunity and features of immune senescence, including shortened lymphocyte telomeres. In patients with chronic HCV, increasing age is associated with higher fibrosis stage and a failure to respond to antiviral therapy. We have shown strong correlations between measures of clinical outcome and lymphocyte telomere length in chronic HCV infection, suggesting accelerated immune senescence in chronic HCV infection and in this study assessed whether immune senescence was also related to the response to antiviral therapy.
Aims and Methods: Telomere length was measured through antiviral therapy for HCV infection in peripheral CD8+ and CD4+T-cells from 85 patients (75% male, 45% genotype 1, mean Ishak fibrosis stage 3.6) by Flow-FISH. Patients were followed to SVR. Results were analysed by multiple logistic regression (LR); age, sex, Ishak fibrosis stage, viral genotype, viral load, BMI, CD8+CD45RO+ and CD4+CD45RO+ telomere length were input variables.
Results: Baseline median (IQR) CD8+CD45RO+(128.1 (113.4 to 142.3) and CD4+CD45RO+(119.0 (107.8 to 126.8) telomere lengths were longer in the 38 patients (44.7%) who achieved SVR than those who did not: 112.5 (104.5 to 118.2) (p = 0.0006) and 105.5 (99.4 to 114.2) (p = 0.0003) respectively. CD8+CD45RO+ and CD4+CD45RO+ telomere lengths were unaffected by therapy. By univariate LR viral load (p = 0.02) and CD8+CD45RO+ telomere length (p = 0.01) were associated with SVR; in this model age (p = 0.19), male sex (p = 0.51), severe fibrosis (p = 0.11), genotype (p = 0.18) and BMI (p = 0.94) were not associated with SVR. Utilising “backwards stepwise regression” to remove non-significant variables age (p = 0.048), viral load (p = 0.02) and CD8+CD45RO+ telomere length (p = 0.007) were associated independently with SVR. Each single point increase in CD8+CD45RO+ telomere length was associated with an OR of achieving SVR of 1.05 (1.01 to 1.08). CD4+CD45RO+ lymphocyte telomere length (p = 0.006) and viral load (p = 0.02) were also associated with SVR; in this model age (p = 0.37), male sex (p = 0.48), presence of severe fibrosis (p = 0.07) genotype (p = 0.19) and BMI (p = 0.89) were not associated with SVR. Utilising “backwards stepwise regression” viral load (p = 0.02) and CD4+CD45RO+ telomere length (p = 0.001) were associated independently with SVR. Each single point increase in CD4+CD45RO+ telomere length was associated with an OR of achieving SVR of 1.08 (1.03 to 1.13).
Conclusion: Immune senescence, measured as shortened CD8+CD45RO+ and CD4+CD45RO+ T-lymphocyte telomeres, predicted a failure to respond to antiviral therapy for HCV infection, independent of other known factors.
PM187 DIAGNOSIS OF SIGNIFICANT LIVER FIBROSIS SECONDARY TO CHRONIC HEPATITIS C VIRUS INFECTION WITH SERUM PROTEOMIC PROFILING
1M. L. Cowan, 2S. J. Thomson, 3P. Rice, 2D. M. Forton, 2T. M. Rahman, 1S. Krishna. 1Division of Cellular and Molecular Medicine, St George’s, University of London, London, UK, 2Department of Gastroenterology and Hepatology, 3Department of Virology, St George’s Hospital, London, UK
Introduction: Chronic infection with hepatitis C virus (HCV) causes hepatic fibrosis that may progress to cirrhosis. Staging of liver fibrosis requires liver biopsy, an expensive invasive procedure whose accuracy is compromised in small biopsy specimens. Previous studies of non-invasive fibrosis markers have been criticised for inclusion of suboptimal liver biopsies. Serum profiling with surface enhanced laser desorption ionisation time-of-flight mass spectrometry (SELDI ToF MS) offers an opportunity for high throughput screening for potential biomarkers.
Aims and Methods: Serum samples from 103 subjects with parenchymal liver biopsies for assessment of hepatic fibrosis secondary to chronic HCV were identified in the long term storage facility of the Department of Virology. Only patients with biopsy specimens longer than 20 mm or containing more than 11 portal tracts were considered. Proteomic spectra were obtained in triplicate with a ProteinChip System 4000 SELDI ToF MS. Potential biomarkers were identified with ProteinChip Data Manager software.
Results: 165 protein clusters were detected on CM10 weak cation exchange arrays and 184 on Q10 anion exchange arrays. Thirty-seven protein peaks were differentially expressed in patients with significant fibrosis (Ishak stage>1). The median value of 10 differentially expressed peaks (p<0.01) increased with increasing fibrosis group (Ishak stages 0/1, 2–4, 5/6). The median value of 7 peaks decreased across the three groups. The ability of any individual peak to diagnose fibrosis was modest with an area under receiver operator curve (AUROC) of 0.63 to 0.71. A logistic regression analysis model with the two most significant peaks classified 73% of subjects correctly, with an AUROC of 0.83.
Conclusion: This study of HCV fibrosis biomarkers has been limited to patients with “gold standard” staging liver biopsies. SELDI ToF MS identified potential biomarkers of liver fibrosis secondary to chronic HCV. A significant proportion of these protein peaks correlate with fibrosis stage. Accurate diagnosis of significant fibrosis was possible in 73% of subjects with a composite model. These proteins merit identification and validation in future studies.
PM188 HEPATITIS C TRANSMISSION IN HIV+ MEN WHO HAVE SEX WITH MEN (MSM)
P. G. Mayhead, J. Tibble, L. McKie. Department of Gastroenterology, Royal Sussex County Hospital, Brighton, UK
Introduction: The main mode of hepatitis C (HCV) transmission in the UK is injecting drug use, but the reason for a third of cases is unknown.1 The incidence of acute HCV in HIV+ MSM attending clinic in Brighton has been rising in recent years from 0.39/100 in 2001 to 3.26/100 in 20062 This raises implications for screening of Hepatitis C and identifying risk factors for transmission of HCV. Having multiple sexual partners, a history of sexually transmitted infections (STI), and certain sexual practices have been associated with HCV infection. An increasing prevalence of HCV acute infection has been found in HIV+ MSM with greater incidence of risky behaviour (unprotected anal intercourse).3 4
Aims and Methods: We undertook a retrospective study comparing co-infected men (HIV-HCV) with HIV+ men with STIs (HIV-STI) and HIV- MSM. Data were collected on sexual practices, partners in the last 3 months and HIV viral load at the time of HCV diagnosis.
Results: There were 92 cases (42 MSM, 24 HIV-STI and 26 HIV-HCV). All had similar numbers of partners (p = 0.741). Twice as many men were practising safe sex (condom use) in the MSM group (23%) compared with the HIV-HCV group (11.5%). 21% in the HIV-STI group practised safe sex. The chance of having safe sex in the HIV-HCV group was 8:1 against (or less than half (0.430) (95% CI 0.107 to 1.738)) the chance of having safe sex in the MSM group (3:1 against). Viral load was similar in the HIV+ groups (p = 0.268).
Conclusion: There is more unsafe sex in the HIV-HCV group. Due to the small sample sizes, it is not statistically significant, but in keeping with other published data on high risk sexual practice.5 Viral load is similar in the HIV+ groups. This implies sexual practice rather than immune suppression that contributes to HCV transmission in HIV+ men. The information is gathered from men attending clinic for all reasons suggesting that it is applicable to this particular population. Treating HCV acutely can allow a clearance rate of up to 80% in HIV+ patients irrespective of the viral load6 and could therefore reduce the burden of chronic HCV infection within the HIV+ community.
PM189 HEV IGG SEROPREVALENCE IN PATIENTS WITH CHRONIC LIVER DISEASE
R. J. Ali, L. Farrington, V. Ellis, R. P. Bendall, G. Courtauld, H. Hussaini, H. R. Dalton. Gastrointestinal Unit, Royal Cornwall Hospital, Truro, UK
Introduction: Autochthonous (locally acquired) hepatitis E is an emerging infection in developed countries such as the UK, and is thought to be a porcine zoonosis. It seems to have a predilection for older men and carries a significant morbidity and mortality. The outcome in patients with pre-existing chronic liver disease is poor with a mortality rate of approximately 70%.1 It is likely that most infections with HEV are subclinical/unrecognised, as we have previously shown that the seroprevalence of HEV IgG is 16% in UK blood donors.2 Few data are available regarding HEV IgG seroprevalence in patients with chronic liver disease.
Aims and Methods: The aim of this study was to document the seroprevalence of HEV in patients with compensated chronic liver disease of differing aetiologies. 136 patients with compensated chronic liver disease were studied from the hepatology clinic at the Royal Cornwall Hospital. Patients were tested for HEV IgG using the Wantai HEV IgG assay (Beijing, China).
Results: The HEV IgG seropositivity results were as follows: autoimmune hepatitis/PBC/PSC 7/34 (20.5%), chronic HBV/HCV 4/25 (16%), NASH 5/29 (17.2%), miscellaneous 1/9 (11%), and 0/39 (0%) in alcoholic liver disease. Patients with compensated chronic alcoholic liver disease were significantly less likely to be HEV IgG positive compared with patients with compensated non-alcoholic chronic liver disease (χ2 test with Yates correction, p<0.05).
Conclusion: The reason for the above findings is uncertain and the absence of HEV IgG in patients with alcoholic liver disease could have a number of explanations. Firstly, it could be that alcoholics for some reason are less exposed to HEV. Secondly, alcoholics may have impaired humoral responses and might not mount a detectable/sustained IgG response. Finally, the absence of HEV IgG in alcoholics may represent a “culled” population, that is for some reason alcoholic patients when infected with HEV have a higher mortality than patients with other forms of chronic liver disease.
PM190 IS THERE ANY DIFFERENCE IN RAPID (RVR) AND EARLY (EVR) VIRAL RESPONSE RATES BETWEEN CIRRHOTIC AND NON-CIRRHOTIC HCV PATIENTS ON COMBINATION ANTIVIRAL TREATMENT?
1M. Ganesh, 2R. N. Ganapathy, 1S. Halder. 1Gastroenterology, Salford University Hospital, HOPE, Salford, UK, 2Gastroenterology, Manchester Royal Infirmary, Manchester, UK
Introduction: Chronic hepatitis C patients with cirrhosis have a higher risk of developing complications and are in particular need of treatment. Rapid and early viral response rates with combination treatment were reported to be lower in cirrhotics compared with non-cirrhotics.1
Aims and Methods: To compare Rapid and Early viral response rates between cirrhotic and noncirrotic HCV patients undergoing combination antiviral treatment. All HCV infected (genotype 1, 2 and 3) patients proven by PCR underwent antiviral treatment between August 2006 and August 2007. Co-infection with HBV or HIV, decompensated cirrhosis, usage of less than 80% of the recommended drug dose, current alcohol and recreational drug abuse were the exclusion criteria. Pegylated Interferon and Ribavirin were used at the recommended dosage for treatment. A 2 log drop in viral load from baseline at 4 weeks and at 12 weeks was considered a rapid and early viral response respectively. The sample size was 85. Chi-squared test was used to assess statistical significance between comparing groups. Age, gender, race and genotype presence of cirrhosis were taken into univariate and multivariate analysis as predictors of RVR and EVR.
Results: Out of the total study population 79% had RVR and 94% had EVR. There was no significant difference demonstrated between cirrhotic (83%) and non-cirrhotic groups (72.73%) in RVR and EVR rates (p = 0.273) and (p = 0.956), respectively (see table). Statistically, distributions of viral genotypes among the two groups were not different. In the non-cirrhotic group with genotype 2 or 3, no significant difference in rapid viral response (RVR) was seen between Asians and Whites (p = 0.541). In a multivariate analysis increasing age (odds ratio 1.11) and genotype 1 (odds ratio 2.8) stood as independent predictors for poor RVR and EVR rates.
Conclusion: In our study there was statistically no significant difference in rapid and early viral response rates between cirrhotics and non-cirrhotics. 69% of patients in the study group had genotype 2 or 3 and all patients received >80% dose of combination treatment. This could explain the good RVR and EVR achieved in our study.
PM191 PROSPECTIVE COMPARISON OF SEVERITY SCORES IN ALCOHOLIC HEPATITIS
1R. Parker, 1C. A. McCune, 1F. H. Gordon, 2A. di Mambro, 3H. Taylor, 1P. L. Collins. 1Department of Hepatology, Bristol Royal Infirmary, Bristol, UK, 2Department of Medicine, University of Bristol, Bristol, UK, 3R&D, Bristol Royal Infirmary, Bristol, UK
Introduction: Alcoholic hepatitis is the most florid manifestation of alcoholic liver disease and is associated with a poor prognosis. Several scoring systems have been used to predict prognosis in patients with alcoholic hepatitis since Maddrey described the Discriminant Function in 1979,1 but it is often unclear which is the most useful in routine clinical practise.
Aims and Methods: This study aimed to determine which of five clinical scoring systems is most useful in predicting outcome in an unselected cohort of patients with alcoholic hepatitis presenting to a busy UK teaching hospital. 56 consecutive patients diagnosed with alcoholic hepatitis had scores calculated for: modified Discriminant Function (mDF), Glasgow Alcoholic Hepatitis Score (GAHS), MELD, Child–Pugh and the Lille model. The primary outcome measure was survival to 6 months, assessed by logistical regression analysis. As a secondary outcome, length of hospital stay was analysed by fitting Cox proportional hazard models to each score.
Results: GAHS and the Lille Model were significantly associated with survival at 6 months (p = 0.01 and p = 0.017 respectively). Other scores did not achieve significance. An increase of 1 in the Glasgow score was associated with an OR of dying within 6 months of 1.72 [95% CI 1.14 to 2.60]. An increase of 0.1 in the log Lille Score was associated with an OR of dying within 6 months of 1.28 [95% CI 1.07 to 1.52]. GAHS, Lille Model and Child–Pugh score were significantly associated with length of stay (p = 0.021, p = 0.018, p = 0.006 respectively).
Conclusion: The Glasgow Alcoholic Hepatitis Score accurately predicts survival in alcoholic hepatitis in this unselected alcoholic hepatitis cohort. This score has the added advantage of being simply calculated when patients are admitted to hospital. The modified Discriminant Function, widely used to guide practice, is not significantly associated with survival in this dataset. We suggest that the Glasgow Alcoholic Hepatitis Score is of the most value in clinical practice, but further data should be collected to demonstrate this.
PM192 DOSE REDUCTIONS IN THROMBOCYTOPAENIC PATIENTS IN THE TREATMENT OF HEPATITIS C WITH PEGYLATED INTERFERON
R. L. Shenderey, M. Aldersley, R. Jones. Leeds Liver Unit, St James University Hospital, Leeds, UK
Introduction: Sustained Virological Response (SVR) rates to treatment of Hepatitis C vary greatly depending on a large number of factors including genotype, stage of disease, comorbidity and importantly compliance with therapy. The two licensed pegylated interferon products in the UK are Pegylated alpha2a (Pegasys®, Roche) and Pegylated alpha2b (Viraferonpeg®, Schering Plough). The product licences state the platelet count must be above 100×109/l for Pegylated interferon alpha2b and 90×109/l for Pegylated Interferon alpha2a in order to commence treatment and that the dose must be reduced if the platelet count drops below 50×109/l and treatment stopped if less than 25×109/l. It is known that dose reduction will reduce the ability to achieve an SVR.
Aims and Methods: This department has aimed to avoid dose reduction and has not followed the product licenses with respect to thrombocytopaenia. We reviewed the database of all our patients treated for Hepatitis C during the period January 2004–July 2007 to determine the number of patients with thrombocytopenia, those who underwent Peginterferon dose reduction and the overall SVR.
Results: 178 patients were treated during this 3.5 year period. 27 patients were commenced on full dose treatment with platelet counts less than 100 (range 50 to 97). Records could be traced for 23/27 patients. Treatment was given for the complete course in 9 patients of which 5 achieved SVR. Only two patients had a dose reduction in their Peginterferon, and neither of these achieved SVR. Reasons for not completing treatment included: 2 failed to attend for follow-up, 3 had treatment discontinued for non-response as per NICE guidelines, 2 had decompensation of their liver disease, 3 found side-effects of treatment intolerable, 1 developed colitis, 1 sepsis, 1 cancer and only 1 for haematological reasons. None of these patients achieved SVR. No patients died during treatment. 17 patients developed platelet counts less than 50 during treatment. 16 of these started with platelet counts under 100×109/l. Two patients had a dose reduction and failed to achieve SVR. Two patients achieved an SVR and neither had a dose reduction. There were no clinically significant bleeding episodes in any of these patients.
Conclusion: Most patients with thrombocytopenia can be treated safely with careful monitoring of platelet count in order to try to maximise SVR rate in the treatment of Hepatitis C.
PM193 HOW ARE ABNORMAL RESULTS FOR LIVER FUNCTION TESTS DEALT WITH IN SECONDARY CARE?
R. I. Fearn, N. Van Someren, R. D’Souza, K. Besherdas. Gastroenterology, Barnet and Chase Farm NHS Trust, Enfield, UK
Introduction: Liver function tests (LFTs) are commonly requested to identify severe, but potentially treatable conditions. In primary care abnormal LFTs are often not adequately investigated. Of 873 patients who had one or more abnormal liver function test 157 (18%) were inadequately followed up, and over half of these were later found to have undetected major liver disease.1 This has never been investigated in secondary care. The AGA guidelines state that abnormal LFTs should either be followed until normal or investigated in a stepwise approach until a cause is found.2
Aims and Methods: This study aimed to determine whether patients found to have deranged LFTs during a hospital presentation are followed up adequately. We identified all patients who had an alanine aminotransferase (ALT) result greater than twice the upper limit of normal on tests performed in Chase Farm Hospital, Enfield, UK (a district general hospital) in September and October 2007 (n = 99). After 6 months we used the computer database to identify whether the result had been followed up to normal. Those with persistently abnormal results had the database queried to find what investigations had been performed and then GPs were contacted to assess follow-up.
Results: 99 patients with ALT greater than twice the upper limit of normal were identified. Eighty were admitted to wards and 19 were discharged from Accident and Emergency (A&E). 39 resolved on repeat testing and 16 patients died during admission. Of the remaining 44 patients, at 6 months 33 patients (33%) were either lost to follow-up (18 patients) or known to their GP but no further tests or follow-up had been organised (15 patients). Of these 15, 8 had been admitted under hospital consultants and 7 had been assessed and discharged from A&E. The remaining 11 patients (11%) were being investigated by their GP or consultant.
Conclusion: This study shows that 33% of patients found to have raised ALT did not receive adequate investigation or follow-up when discharged from secondary care. It can be concluded that the AGA guidelines of following deranged LFTs up to resolution or until an underlying cause is found are not being implemented.2 Early diagnosis and treatment in chronic liver disease can improve prognosis,3 but our findings suggest that important cases may be missed. Thorough discharge summaries for all patients who have abnormal results in hospital along with concise advice for GPs may improve implementation of the AGA guidance.
PM194 DEVELOPMENT OF HEPATOCELLULAR CARCINOMA AND OF PORTAL VEIN THROMBOSIS IN PATIENTS WITH DECOMPENSATED ALCOHOLIC LIVER DISEASE
S. J. Bonner, C. Barclay, E. Mcfarlane, K. Shafique, J. Jones, D. Gleeson. Liver Unit, Royal Hallamshire Hospital, Sheffield, UK
Introduction: Hepatocellular carcinoma (HCC) may develop in cirrhosis from any cause, but may be commoner in some forms than in others. There are few recent data on incidence of HCC in alcoholic liver disease (ALD). We have previously reported (Mcfarlane Gut 2006 Abst) on outcome in 249 patients (162 men, median age 49 years) with first episode of decompensated ALD (Childs Grade B or C), presenting consecutively between 1998 and 2005.
Aims and Methods: Aim: To assess the subsequent incidence of HCC and also of Portal Vein Thrombosis (PVT) in this cohort. Available ultrasound and laboratory reports up to October 2008 were viewed. Patients were not formally screened for HCC unless absent from alcohol, but ultrasound scans (USS) were usually performed in the event of hospital readmission. Follow-up was defined as time between initial presentation with decompensated ALD and the most recent ultrasound scan. HCC was defined as a compatible focal liver space-occupying lesion on ultrasound plus a raised serum alfa feta protein.
Results: Liver histology was available in 67 patients and suggested cirrhosis in 52 (78%). Of the remaining 182 patients, 128 (71%) were presumed to have cirrhosis based on presence of varices and/or ascites. Follow-up was (median (range)) 15 (0 to 112) months and was 43 (6 to 112) months in the 149 patients followed up for >6 months. Four men, all with cirrhosis, were diagnosed with HCC: one at presentation, the others after 35–106 months. Serum AFP levels were elevated (1163–17 800 units/l) in all four. All four subsequently died of HCC (average survival = 54 days). 153 other patients have died, none apparently of HCC, although circumstances of death are still unknown in 20. Incidence of HCC was 0.7/100 patient-year follow-up. Actuarial incidence of HCC after 1, 2 and 5 years was 1+/−0.1%, 1.4+/−0.1% and 3.6+/−0.2% respectively in the cohort as a whole and was 1+/−0.1%, 2+/−0.1% and 5+/−0.2% in the 180 patients with confirmed or presumed cirrhosis. Three females and two males (2.0%) developed PVT. One patient had both HCC and PVT.
Conclusion: Although under-diagnosis is possible, the incidence of HCC in this cohort of patients with decompensated ALD, most of whom had cirrhosis, appears to be lower than that in some reports of cirrhosis due to HBV and HCV.
PM195 ANTI-HBC AND HBSAG SCREENING AMONG NIGERIAN HEALTH CARE WORKERS
1111, 2434212S. O. Ola, 1J. A. Otegbayo, 2O. D. Olaleye, 3W. A. Shokunbi, 4C. B. Summerton. 1Department of Medicine, 2Virology, 3Haematology, University College Hospital, Ibadan, Nigeria, 4Gastroenterology, Trafford General Hospital, Manchester, UK
Introduction: HBV infection is common among Nigerian health care workers,1 2 and as such efforts should be made to determine the status of the workers prior vaccination against the infection.
Aims and Methods: In order to determine anti-HBsAg and anti-HBc status among Nigerian health care workers at UCH, Ibadan, Nigeria, blood specimens of 804 volunteered subjects were screened for the presence of Hepatitis B surface antigen (HBsAg) and antibody to Hepatitis B-core antigen(anti-HBc) using Enzyme Linked Immuno-sorbent Assay. Statistical analysis was carried out using Student t at p<0.05.
Results: The subjects were in a male:female ratio of 1:2 and aged 21–65 years. The detection rates of HbsAg and anti-HBc were 6.1% and 59.1% (p<0.05) in all the subjects respectively. Lone HBsAg (1.9%) and anti-HBc (54.8%) were present among the subjects while the combination of the two markers was present in only 4.3%. HBsAg and anti-HBc were detected in 6.2% and 69% of males respectively and in 6% and 54.3% respectively of females. Using both markers, HBV infection was detected in 60.9% of the subjects (table). Among the dental and medical personnel, the infection was commonest among the Gynaecologist and Obstreticians (93.3%) and lowest among the Paediatricians (52.6%). There was no difference in the rates of the infection among the different risk groups for the infection among the workers and only 39% of them were sero-negative for both markers of the HBV infection.
Conclusion: Both HBsAg and anti-HBc should be tested among Nigerian heath care workers in detection of their status for HBV infection prior vaccination. The infection is very common among the workers regardless of their professional and risk groups.
Keywords: health care workers; HbsAg; Anti-HBc; Nigerian.
PM196 PLASMA CORTISOL PROFILES IN PATIENTS WITH CIRRHOSIS: BEWARE THE TIME OF SAMPLING
1S. Montagnese, 2B. Middleton, 1A. R. Mani, 2D. J. Skene, 1M. Y. Morgan. 1Centre for Hepatology, Royal Free and University College Medical School, London, UK, 2Centre for Chronobiology, Faculty of Health and Medical Sciences, University of Surrey, Guildford, UK
Introduction: The prevalence of relative adrenal insufficiency is reported to be high in patients with end-stage liver disease; the term hepato-adrenal syndrome has been proposed to describe this condition.1 In addition, liver transplant recipients are prone to functional adrenal gland atrophy, secondary to prolonged corticosteroid treatment.2 The diagnosis of adrenal insufficiency is based, in the first instances, on measurement of the cortisol concentration at 08:00, although cortisol release stimulating tests are used for confirmation. Limited information is available on the features of the 24-hour cortisol profile in patients with cirrhosis.
Aims and Methods: The aim of this study was to determine whether the 08:00 cortisol concentration provides an accurate “snap-shot” of adrenal function in patients with cirrhosis. The study population comprised 20 patients with cirrhosis [mean (range) age 59 (39 to 77) years; Child A:14, B:4, C:2] and nine healthy volunteers [age 60 (38 to 84) years]. Hourly blood samples for measurement of plasma cortisol were obtained, under light and posture-controlled conditions, over 24 hours; plasma cortisol concentrations were measured by RIA and the 24-hour profiles were evaluated by cosinor analysis; standard circadian indices were obtained.
Results: There were no significant differences in the average 24-hour plasma cortisol concentration or in the amplitude of the 24-hour rhythm between patients and healthy volunteers. However, both the timing of the cortisol rhythm onset and that of its peak were considerably delayed in the patients compared with the healthy volunteers (05:24±02:06 vs 03:54±01:00, p = 0.02; 10:18±02:54 vs 08:54±01:24, p = 0.06). No significant differences were observed in the rhythm offset but the duration of the peak was significantly shorter in the 13 patients compared with the seven healthy volunteers in whom this parameter was available (7.0±3.8 vs 10.6±2.3 hours, p = 0.03). A significant correlation was observed between the plasma cortisol peak time and the Pugh score (R = 0.49, p<0.05).
Conclusion: Significant abnormalities were observed in plasma cortisol profiles in patients with cirrhosis, most likely due to dysfunction in central circadian control.3 The observed delays in the cortisol 24-hour rhythm in cirrhotic patients might result in erroneously low estimates of plasma cortisol if performed at 08:00 and, consequently, in unnecessary cortisol release stimulating tests.
PM197 INCIDENCE OF PARACETAMOL THERAPEUTIC MISADVENTURE AS A CAUSE OF MASSIVELY RAISED AST: RESULTS OF A RETROSPECTIVE ANALYSIS
S. T. Barclay, E. H. Forrest. Gastroenterology, Glasgow Royal Infirmary, Glasgow, UK
Introduction: Hepatotoxicity resulting from deliberate overdose of paracetamol is a well recognised clinical entity. Outwith deliberate overdose paracetamol hepatotoxicity has been dubbed “paracetamol misadventure.” Toxicity due to inadvertent excess of paracetamol is accepted; however the concept of a “paracetamol therapeutic misadventure” (PTM) resulting from ingestion of ⩽4 g/day of paracetamol remains controversial.
Aims and Methods: We aimed to establish the incidence of PTM amongst acute admissions with massively elevated transaminases. Using Glasgow Royal Infirmary biochemistry computer records we identified samples originating from our medical and surgical admissions units between January 1st 2005 and December 31st 2006 with an AST of >1000 IU/ml. Patients with a raised troponin I or amylase were excluded from further evaluation. Case notes for the remaining patients were examined to establish the investigations undertaken and the cause attributed to the raised AST. Probable PTM was diagnosed on the basis of clinical history together with the absence of a hypotensive/hypoxic insult to the liver, and ideally exclusion of viral, autoimmune and metabolic causes of acute hepatitis.
Results: Of 181 admissions identified with an AST >1000 IU/ml, case notes were available for 142. Of these 29 were felt to have an AST rise of non-hepatic origin (19 seizure or rhabdomyolysis, 10 MI). Causes of raised AST, together with mortality rates are illustrated in the table. PTM incidence was equal to that of paracetamol overdose, and associated with significant mortality. Amongst those with a diagnosis of PTM one case related to enzyme induction by phenytoin, the remaining 17 to excessive alcohol consumption (range 60 to 450 u/week, median 196 u/week). Patients with PTM tended to have a higher AST to ALT ratio at presentation (median 2.7, range 0.7 to 8.1) compared with deliberate paracetamol overdose (median 1.3, range 0.4 to 5.4 p = 0.02).
Conclusion: PTM is a frequent cause of significantly raised AST, often associated with alcohol excess. PTM should be considered in patients with otherwise unexplained transaminitis, particularly if there is a history of alcohol excess or the use of enzyme-inducing medication. A high AST to ALT ratio may be helpful in identifying such patients.
PM198 THE CHANGING FACE OF HEPATITIS B IN GREATER GLASGOW: EPIDEMIOLOGICAL TRENDS 1993–2007
1S. T. Barclay, 2S. Cameron, 3P. R. Mills, 3M. Priest, 3F. Ross, 4R. Fox, 5C. Goulding, 1E. H. Forrest, 1A. J. Morris, 1M. Neilson, 1A. J. Stanley. 1Gastroenterology, Glasgow Royal Infirmary, Glasgow, UK, 2West of Scotland Regional Virus Laboratory, 3Gartnavel General Hospital, 4Brownlee Centre for Infectious Diseases, G.G.H, 5Victoria Infirmary, Glasgow, UK
Introduction: Chronic hepatitis B (HBV) is uncommon in the West of Scotland, being largely confined to patients born overseas and those who develop chronic HBV infection following sexual or intravenous transmission. We sought to establish whether the incidence of acute and chronic HBV has changed in Greater Glasgow over a 15 year period. We also assessed the number of patients initiated on HBV therapy during recent years.
Aims and Methods: The West of Scotland Regional Virus laboratory database was interrogated to obtain all hepatitis B surface antigen (HBsAg)+ve samples from 1st January 1993 to 31st December 2007. Analysis was restricted to named adult samples from hospitals in Greater Glasgow Health Board (GGHB). For each patient the date of first positive testing was identified. Patients were classified as “acute” if IgM anti-HBc+ve and chronic if IgM anti-HBc–ve at initial test or two positive HBsAg samples were received >6 months apart. Patients were classified as indeterminate if IgM anti-HBc was not tested. Numbers of patients initiated on anti-viral therapy for HBV during “06 & “07 were obtained from the GGHB viral hepatitis treatment centres.
Results: Whilst the annual incidence of new diagnoses of HBV has remained stable over the 15 year period, the incidence of acute HBV has fallen from a peak in the year 2000 (see figure). In contrast, the incidence of chronic HBV has trebled since 2000, with 195 new chronic HBV patients diagnosed in 2006–7. Data obtained from the four GGHB treatment centres showed that only 15 patients were initiated on antiviral therapy for HBV during those 2 years.
Conclusion: The incidence of acute HBV is falling in Greater Glasgow, whilst that of chronic HBV is rising. This will require increased resources to allow patient assessment and monitoring. Despite increasing therapeutic strategies, few patients with chronic HBV are currently initiated on treatment.

PM199 INPATIENT MORTALITY AND RATES OF ICU REFERRAL AMONGST INPATIENTS WITH LIVER DISEASE: RESULTS FROM A PROSPECTIVE AUDIT
S. T. Barclay, E. H. Forrest, A. J. Morris, J. Winter, R. Gillespie, D. Gaya, A. Stanley. Gastroenterology, Glasgow Royal Infirmary, Glasgow, UK
Introduction: As the incidence of liver disease rises, the burden on inpatient medical services increases. Patients with liver disease are often thought as being poor candidates for intensive care and there is a risk that they may be denied access to appropriate higher level medical care. Our aim was to prospectively audit mortality and rates of ICU referral and admission amongst patients admitted to our hospital with liver disease.
Aims and Methods: Patients with jaundice, encephalopathy, ascites, variceal haemorrhage or known cirrhosis were identified on admission to the acute medical unit, the gastroenterology wards or by referral to the on-call gastroenterology page from other hospital units. Patients with jaundice relating to extra hepatic biliary obstruction or paracetamol poisoning were excluded. Between 01.05.08 and 01.08.08 data were prospectively collected on presentation, diagnoses made, clinical and laboratory data relevant to disease severity, inpatient survival and consideration and/or acceptance for ICU care.
Results: 102 admissions in 79 patients were identified meeting the above criteria. Median age was 51 years (95% CI 45 to 51). 11/79 of patients (14%) took irregular discharge during the audit period, 10 of whom were readmitted. Mean UKELD score on admission was 55.0 (95% CI 53.7 to 56.2) with 46% of cirrhotic patients having Child’s C disease. 75% of patients were admitted with jaundice, 31% with worsening ascites, 8% with variceal haemorrhage and 7% with encephalopathy. The mean length of admission was 11 days (95% CI 12 to 20 days). Alcohol was the most common aetiology (49/79, 62%), followed by alcohol with hepatitis C (15/79, 19%) and NAFLD (4/79, 5%). Amongst those with alcohol aetiology, 63/84 had recent alcohol excess (mean 202 units/week, 95% CI 160 to 245). 5/79 (6%) and 10/79 (13%) of patients were active and former intravenous drug users respectively. 10/79 (13%) were receiving methadone. 16/79 (20%) patients died during admission. Of these, 11 were not considered appropriate for ICU care by their consultant (mean UKELD = 59.4 95% CI 53.0 to 65.7), whilst 4 were referred and accepted into ICU (mean UKELD = 56.6, 95% CI 54.0 to 59.1) but subsequently died. Reasons for non-referral included malignancy, multi-organ failure and premorbid functional state. One patient was referred but died just prior to ICU assessment. No patients were referred but not accepted. One patient was referred (UKELD = 55.5), accepted and survived to discharge.
Conclusion: Liver disease is associated with a lengthy inpatient stay and a high mortality amongst a relatively young patient population. All patients who died had been considered for ICU, although most were deemed not suitable for referral. All patients refferred were accepted. Further work is underway to asess the optimal timing of ICU referral.
PM200 QUANTITATION OF STEATOSIS BY MAGNETIC RESONANCE IMAGING (MRI) AND SPECTROSCOPY (MRS) IN LIVER DISEASE: EFFECT OF HEPATIC FIBROSIS AND IRON
1S. McPherson, 2G. Cowin, 3P. O’Rourke, 4A. Volp, 1L. Horsfall, 1L. Burke, 5J. R. Jonsson, 1A. Clouston, 1J. Fawcett, 2G. Galloway, 6M. Benson, 1E. Powell. 1Gastroenterology and Hepatology, Princess Alexandra Hospital, 2Centre for Magnetic Resonance, University of Queensland, Australia, 3Cancer and Population Studies Group, Queensland Institute of Medical Research, Brisbane, Australia, 4Radiology, Princess Alexandra Hospital, Brisbane, Australia, 5Medicine, University of Queensland, Australia, 6Radiology, Princess Alexandra Hospital, Brisbane, Australia
Introduction: Hepatic steatosis is present in 30% of the population and a proportion of these subjects have steatohepatitis that may lead to cirrhosis. Currently the diagnosis and severity of steatosis can only be established accurately by liver biopsy. Previous small studies found that steatosis measured by MRS and MRI closely correlated with histological assessment of liver fat. However, the effect of fibrosis on the accuracy of MRS/MRI for the quantitation of steatosis has not been addressed.
Aims and Methods: Our aim was to determine discriminative values for grading steatosis by MRS and MRI in patients with chronic liver disease and to determine the effect of fibrosis and iron. Sequential patients who underwent percutaneous liver biopsy or liver resection at the Princess Alexandra Hospital between January 2007 and March 2008 had MRS and MRI (In phase/Out phase [IP/OP] and with/without fat saturation [±FS] images) to determine liver fat content. Histology was used as the reference standard.
Results: 66 patients had MRI, of whom 53 also had MRS. 26 patients had HCV, 15 had fatty liver and 25 had other liver diseases. 38 patients had steatosis on biopsy and of these 17 patients had >33% steatosis. Close relationships were observed between the percentage of steatosis estimated by histology and MRS (rs = 0.91 p<0.001), IP/OP (rs = 0.82 p<0.001) and ±FS (rs = 0.78 p<0.001). Linear regression showed that the percentage of steatosis was underestimated by MRS, IP/OP and ±FS in patients with advanced fibrosis compared with those with no/mild fibrosis. Aberrant results were obtained for the extent of steatosis measured with IP/OP and MRS in subjects with grade 4 hepatic iron but ±FS gave consistent results for all patients. Consistent results for steatosis were obtained with IP/OP, MRS and ±FS for subjects with grade 1–3 liver iron. MRS, IP/OP and ±FS had good diagnostic accuracy for >5% steatosis (area under receiver operating characteristic curve [AUROC] 0.96, 0.91, 0.89 respectively) and >33% steatosis (AUROC 0.96, 0.91 0.96 respectively) for all patients. When patients with advanced fibrosis (Metavir stage 3 and 4) were excluded, the diagnostic performance for >33% steatosis improved for MRS, IP/OP and ±FS (AUROC 0.99, 0.99 and 0.99 respectively).
Conclusion: MRS and MRI had good accuracy for the diagnosis and quantitation of steatosis in subjects with chronic liver disease. However, MR may underestimate the percentage of steatosis in subjects with advanced fibrosis.
PM201 HEPATITIS B STATUS AND FLARE IN ASIAN PATIENTS WITH INFLAMMATORY BOWEL DISEASE RECEIVING IMMUNOSUPPRESSION THERAPY—ARE WE TESTING AND DO WE NEED TO?
V. Appleby, P. B. Southern, J. Healey, D. Patterson, O. Bebb, S. Moreea. Digestive Diseases Centre, Bradford Teaching Hospitals NHS Foundation Trust, Bradford, UK
Introduction: Bradford has a significant ethnic minority population originating from South Asia (estimated 26% by 2011) where the prevalence of Hepatitis B (HBV) may be 3–4%. It is recognised that HBV can flare during immunosuppressive therapy but data in patients with inflammatory bowel disease (IBD) are sparse. Groups such as the European Crohn’s and Colitis organization (ECCO) are due to release guidelines which will clarify the status of pre-treatment testing for HBV.
Aims and Methods: To establish the incidence of HBV flare in our Asian IBD patients treated with immunomodulators. Secondary outcomes are analysis of characteristics of our Asian patients with IBD, HBV prevalence and outcome of HBV flare. Our IBD database and the hospital’s computerised results service were analysed to obtain the following data: demographics, ethnicity, immunosuppression treatment, ALT levels and hepatitis B serology/virology for our IBD patients. Immunosuppression therapy consisted of azathioprine, methotrexate, 6 mercaptopurine (6MP) and infliximab with or without steroids. Patients receiving steroids alone were excluded.
Results: There were 1243 patients (675 ulcerative colitis, 490 Crohn’s disease and 78 indeterminate colitis) on the IBD database: 603 (48.5%) males (M)—mean age 50 years and 639 (51.5%) females (F)—mean age 48 years. 290 patients (23%) were of Asian origin—167M (57.5% of Asians) mean age 41 years, 123F (42.5% of Asians) mean age 42 years. 35 (22F,13M) Asians (12%) had an HBsAg test, and 2 patients (2M, 0F) were HBV positive, prevalence rate 5.7%. Most female patients (20/22) were tested for HBV during pregnancy and males tested if they had an abnormal ALT rather than at the start of treatment. One patient was found to be HBV immune. There were 58 Asians on immunosuppression therapy (53 on azathioprine, 5 6MP)—this represented 20% of all Asians and 4.7% of the total population. 26/58 (50%) had an ALT flare—17M, 9F. Six of the 23 patients (23%, 4M,2F) were tested for HBV and 1 male patient was found to have HBV (3.8% of patients with an ALT rise). This patient was eAg negative with viral breakthrough and was treated successfully with Lamivudine.
Conclusion: The prevalence of IBD in Asians (23%) reflects the ethnic mix of the region.1 Asian patients with IBD are younger (mean age of Asians 41.4, non-Asians 50.2 (p 0.03)) and there is a preponderance of males in our Asian cohort (57.6%) compared with our non-Asian group (45.9%), p<0.001. Our figures suggest a HBV prevalence rate of 5.7% in the local Asian population with IBD, which is higher than in our previous study. This work lends further weight to the calls to screen patients for viral hepatitis prior to initiation of immunomodulator therapy, particularly ethnic groups with high prevalence.
PM202 IMMUNE SENESCENCE CHARACTERISES LIVER TRANSPLANT RECIPIENTS WITH ESTABLISHED GRAFTS
1W. Gelson, 1M. Hoare, 1A. Shankar, 2A. Akbar, 1G. Alexander. 1Hepatology, Addenbrooke’s Hospital, Cambridge, UK, 2Immunology, University College, London, UK
Introduction: Immune senescence is the normal process whereby the human immune system ages, becoming less effective. Lymphocyte immune senescence is characterised by progressive telomere shortening, reduced expression of CD27 and CD28 and increased expression of membrane proteins including CD45RO, KLRG1 and CD57. Immune senescence is accelerated by persistent viral infections such as CMV, EBV and HIV, as well as by smoking and obesity.
Aims and Methods: (1) To evaluate whether liver transplantation is associated with premature immune senescence and (2) to determine which clinical and demographic characteristics of liver graft recipients are related to immune senescence. Lymphocytes from 97 liver transplant recipients with established grafts and 41 age and sex-matched controls were subjected to an 8-colour flow cytometry assay to measure lymphocyte expression of KLRG1, CD127, CD45RO, CD27, CD28, CD4, CD8 and CD57. Lymphocyte telomere length was assessed in cells positive for CD4 and CD45RO or CD8 and CD57 by flow-FISH. For each marker of immune senescence, cases were compared with controls using a Mann–Whitney Test. For liver transplant recipients, simple linear regression assessed for associations between each marker of immune senescence and clinical or demographic characteristics: age, sex, paediatric or adult recipient, transplant number, disease aetiology, HCC at transplantation, CMV status, normal liver biochemistry, type of immune suppression, and number of infective episodes, acute rejection episodes, malignancies and pre-cancerous lesions. Significant associations (p<0.1) were carried through to multiple linear regressions to assess for independent associations (p<0.05).
Results: There was significantly greater expression of all markers of lymphocyte immaturity on lymphocytes in controls compared with liver transplant recipients and significantly greater expression of all markers of lymphocyte maturity (except KLRG1) on lymphocytes in liver transplant recipients compared with controls. Lymphocyte telomeres were shorter in liver transplant recipients than controls, with significant and pronounced differences in the subsets: CD4+, CD8+, CD4+CD45RO- and CD8+CD57-. Age and previous CMV were associated independently and positively with most cell surface markers of maturity but independently and negatively with most markers of immaturity. Age, HCC at transplantation and skin malignancy developing after transplantation were associated independently and negatively with telomere length in most lymphocyte subsets.
Conclusion: Lymphocytes from liver transplant recipients are “biologically” older than lymphocytes from age and sex-matched controls. HCC at transplantation, skin malignancy and CMV status are associated independently with lymphocyte senescence in liver transplant recipients.
Nutrition posters
PM203 CAN NUTRITIONAL STATE ON ADMISSION BE USED TO PREDICT 30-DAY MORTALITY IN PATIENTS PRESENTING WITH ALCOHOLIC LIVER DISEASE?
A. Claridge, T. Smith. Gastroenterology, Royal Bournemouth Hospital, Bournemouth, UK
Introduction: Alcoholic liver disease (ALD) is a common presenting problem, with 92% of gastroenterologists reporting a rise in the amount they see.1 A number of prognostic tools already exist to help guide the management of ALD: the Childs–Pugh score, Glasgow alcoholic hepatitis score, Mayo end-stage liver disease score (MELD) and the discriminant function. These, however, often require complex equations and the results of biochemical tests. Measurements of nutritional state, including the malnutrition universal screening tool (MUST), are easy to calculate at the bedside and have previously been shown to be useful predictors of mortality in a variety of patient groups.2
Aims and Methods: This study set out to find if the commonly used markers of nutrition, weight, height, body mass index, MUST score and mid-arm circumference are useful prognostic markers of survival in patients with ALD. Data were prospectively collected on all patients with a diagnosis of ALD admitted to the gastrointestinal ward at Royal Bournemouth Hospital for a 6-month period from 1 March to 31 August 2008 inclusive. The diagnosis of ALD was made on clinical history with other appropriate investigations performed to rule out an alternative aetiology. All patients were followed up for a minimum of 30 days.
Results: 55 consecutive patients were included, 69% (38/55) were men; median age 54 years. 22% of patients (12/55) died within 30 days of admission. Body mass index, weight and mid-arm circumference were not useful in helping to predict survival. However, 90% of patients with a MUST score of 0 on admission survived more than 30 days compared with only 56% of patients with a MUST score of 2 or more. A MUST score of 2 or more gives a relative risk of surviving less than 30 days of 4.4. 18 patients had a Childs–Pugh score of C, of which 61% (11/18) survived more than 30 days (see table).
Conclusion: This study suggests that the MUST score is at least equally as effective at predicting 30-day survival as traditional methods. The simplicity of the MUST tool makes it an excellent bedside prognostic tool in patients with ALD.
PM204 SURVEY OF UK GASTROENTEROLOGISTS’ PRACTICE REGARDING DIETARY ADVICE AND FOOD EXCLUSION IN IRRITABLE BOWEL SYNDROME AND INFLAMMATORY BOWEL DISEASE
S. J. Inns, S. L. Bloom, A. V. Emmanuel. Department of Gastroenterology, University College Hospital, London, UK
Introduction: Patients with irritable bowel syndrome (IBS) and inflammatory bowel disease (IBD) frequently express the perception that they are intolerant to certain foodstuffs. Many undertake dietary restriction secondary to this and medical staff have a variable opinion of the available evidence.
Aims and Methods: The aim of this study was to assess the dietary advice practice of UK gastroenterologists regarding IBD and IBS. A questionnaire that investigated aspects of dietary advice practice in patients with IBD and IBS was e-mailed and mailed to all consultant gastroenterologists in the UK registered as members of the British Society of Gastroenterologists (n = 983).
Results: 363 questionnaires were returned (response rate 37%). Respondents more often gave specific dietary advice to more than 25% of patients with IBS than IBD (84% vs 27%, p = 0.001) and gave advice about dietary exclusions to more than 25% of patients more commonly in IBS than IBD (61% vs 13%, p<0.001). The foods most commonly advised to avoid were fibre, dairy and wheat. The vast majority of respondents (97% in IBD and 89% in IBS) did not use allergy testing. Respondents were most likely to provide dietary advice to patients with small bowel Crohn’s disease, difficult to control IBD, diarrhoea-predominant IBS and “difficult-to-control” IBS. The majority of respondents agreed strongly or a little that dietary exclusion was effective in the treatment of IBS, compared with the minority in IBD (71% vs 39%, p<0.05).
Conclusion: UK gastroenterologists give dietary advice, including advice regarding dietary exclusion, more commonly to IBS than IBD patients. The majority of UK gastroenterologists have some confidence in the use of dietary exclusion in IBS, the converse is true in IBD. However, the advice given is largely empiric and mostly comprises the exclusion of fibre, dairy and wheat. Utilisation of allergy testing was low.
PM205 WITHDRAWN
PM206 THE INTRODUCTION OF “PROTECTED MEALTIMES” INCREASES NUTRITIONAL INTAKE IN ACUTE MEDICAL PATIENTS
C. M. Stuckey, G. O’Malley, S. Matthias, A. Hawkins, S. Geldart, S. A. Weaver, T. R. Smith. Nutrition and Gastroenterology, Royal Bournemouth Hospital, Bournemouth, UK
Introduction: Malnutrition, both a cause and consequence of disease, affects up to 40% of patients admitted to hospital. Nutritional status often deteriorates during admission due to poor nutritional intake and underlying disease. “Protected mealtimes”, one of the 10 key characteristics of good nutritional care in hospital, aims to stop all non-urgent clinical activity during mealtimes. This aims to promote an environment conducive to eating and allowing ward staff to support those patients who require assistance to eat their meals. We investigated the impact of implementing “protected mealtimes” on the number of non-urgent interruptions and nutritional intake during mealtimes on an acute medical ward.
Aims and Methods: The number of non-urgent interruptions and nutritional intake of all patients (excluding those nil by mouth or on clear fluids) was assessed during five separate mealtimes over a 5-week period both before and following the introduction of “protected mealtimes”. The menu choices of each patient and amount consumed were observed and recorded. The energy content of the meal consumed was estimated by an experienced dietitian.
Results: 94 meals were observed before the introduction of “protected mealtimes”. 50% of patients experienced one or more non-urgent interruptions during their meal (total of 74 interruptions over 94 meals). Drug rounds and routine observations accounted for 48% and 19% of interruptions, respectively. The mean energy intake per meal was 346 kcal, with only 40% of patients managing 400 kcal or more. 78 meals were observed following the introduction of “protected mealtimes”. 18% of patients experienced one or more non-urgent interruptions (total of 14 interruptions during 78 meals). Drug rounds accounted for 29% of interruptions, with none due to routine observations. The majority of interruptions (64%) were due to the activities of non-clinical staff that were not routinely based on the ward. The mean energy intake per meal increased to 432 kcal, with 56% of patients managing 400 kcal or more.
Conclusion: The introduction of “protected mealtimes” on an acute medical ward was feasible and reduced the number of non-urgent interruptions while also increasing energy intake during mealtimes. Future research should examine the effect of “protected mealtimes” on nutritional status and clinical outcome during hospital admission.
PM207EFFECT OF A FISH INTERVENTION ON MARKERS OF COLORECTAL CARCINOGENESIS: THE FISHGASTRO STUDY
1G. K. Pot, 2G. Majsak-Newman, 1A. Geelen, 2L. J. Harvey, 2K. Przybylska, 3A. Hart, 4M. P. Williams, 2J. Dainty, 1P. van t’Veer, 1G. Schaafsma, 5F. M. Nagenast, 6B. J. Witteman, 7P. C. van de Meeberg, 8R. Timmer, 1E. Kampman, 2E. K. Lund. 1Division of Human Nutrition, Wageningen University, Wageningen, The Netherlands, 2Institute of Food Research, Norwich, UK, 3Gastroenterology, NNUH, Norwich, UK, 4Gastroenterology, James Paget Hospital, Great Yarmouth, UK, 5UMC, St Radboud, Nijmegen, The Netherlands, 6Gastroenterology, Gelderse Vallei Hospital, Ede, The Netherlands, 7Gastroenterology, Slingeland Hospital, Doetinchem, The Netherlands, 8Gastroenterology, St Antonius Hospital, Nieuwegein, The Netherlands
Introduction: Diet is considered to be a major factor in relation to the development of colorectal cancer. High fish consumption has been linked to a decreased colorectal cancer risk but it is unclear if this is limited to oil-rich fish such as salmon. Therefore, we have assessed whether a 6-month intervention with salmon or cod can modify apoptosis and mitosis within the colonic crypt.
Aims and Methods: A multicentre, randomised, controlled, parallel intervention trial was performed at eight clinical centres in The Netherlands and the UK between November 2004 and December 2007. Participants (n = 242) received dietary advice plus either 300 g salmon/week, 300 g cod/week, or only dietary advice. Colonic biopsies were collected before the intervention by colonoscopy and after by sigmoidoscopy. Crypts were stained with Feulgen’s stain, microdissected and the numbers of mitotic and apoptotic cells per crypt were counted. Serum fatty acids were also measured. Results were analysed by analysis of covariance.
Results: Salmon consumption significantly increased circulating n-3 fatty acids. Overall, there was no significant benefit of consuming either salmon or cod in relation to mitosis and apoptosis. After the intervention, the number of mitotic cells per crypt was not significantly different in the salmon or cod group compared with the dietary advice group. Similarly, neither apoptosis rates not crypt length were significantly different between the three intervention groups (see table). The cause of the observed change over time cannot be determined but could be due to the dietary advice or difference in bowel preparation.
Conclusion: This novel intervention trial does not support the hypothesis that eating fish for 6 months modifies the colorectal cancer risk as assessed by measuring apoptosis, mitosis, or crypt length.
PM208 VITAMIN D LEVELS IN 70% OF PATIENTS ATTENDING FOR COLONOSCOPY IN THE UK AND THE NETHERLANDS ARE SUBOPTIMAL BUT CONSUMPTION OF SALMON DOES NOT PROVIDE ANY SIGNIFICANT IMPROVEMENT
1G. Majsak-Newman, 2G. K. Pot, 1E. Maxwell, 2A. Geelen, 1L. J. Harvey, 3F. M. Nagengast, 4B. J. Witteman, 5P. C. van de Meeberg, 6R. Timmer, 7A. C. I. T. Tan, 8P. J. Wahab, 9A. Hart, 10M. P. Williams, 2E. Kampman, 1E. K. Lund. 1Gastrointestinal Biology and Health, Institute of Food Research, Norwich, UK, 2Division of Human Nutrition, Wagenigen University, Wageningen, The Netherlands, 3UMC, St Radboud, Nijmengen, The Netherlands, 4Gastroenterology, Gelderse Vallei Hospital, Ede, The Netherlands, 5Gastroenterology, Slingeland Hospital, Doetinchem, The Netherlands, 6Gastroenterology, St Antonius Hospital, Nieuwegein, The Netherlands, 7Gastroenterology, Canisius Wilhelmina Hospital, Nijmegen, The Netherlands, 8Gastroenterology, Rijnstate Hospital, Arnhem, The Netherlands, 9Gastroenterology, Norfolk and Norwich University Hospital, Norwich, UK, 10Gastroenterology, James Paget Hospital, Great Yarmouth, UK
Introduction: Low vitamin D status is increasingly recognised as a major risk factor for a number of cancers including colorectal cancer. Vitamin D deficiency (<50 mmol/l) is common in the UK and The Netherlands where access to sufficient sunlight may be limited due to a range of lifestyle factors. It is often recommended that the consumption of oil-rich fish can to some extent counteract this problem.
Aims and Methods: The aim of this study was to assess levels of 25OH-vitamin D in serum samples from patients attending gastrointestinal clinics before and after participation in a larger fish intervention trial (FISHGASTRO NCT00145015). Participants (201) with colorectal polyps, ulcerative colitis in remission, or “normal” colonic mucosa were recruited throughout the year from colonoscopy clinics at two hospitals in the UK and six in The Netherlands. They were given either salmon (300 g/week; n = 71), cod (300 g/week; n = 62), or generic dietary advice to eat healthily (n = 64) for 6 months. 25OH-vitamin D was measured by enzyme immunoassay (IDS Ltd, UK) in serum samples before and after dietary interventions.
Results: At baseline, 32% of patients were vitamin D deficient and 71% had suboptimal levels, higher than previously reported for a UK middle-aged population. As expected, deficiency was greatest in January (69%), with 94% having suboptimal levels (<80 nmol/l). Even in the summer months approximately 10% of patients were deficient and 50% had suboptimal levels. Patients gained no significant benefit in terms of their vitamin D levels from consuming salmon for 6 months.
Conclusion: Patients attending gastrointestinal clinics are very likely to have suboptimal levels of vitamin D. They should be strongly encouraged to have a sensible outdoor lifestyle in order to rectify this problem. Any nutritional advice should be more targeted towards cod-liver oil and herring or fortified foods as better sources of vitamin D than salmon.
Funding: This work was funded under EU FP6 SEAFOODplus project 506359, the UK Food Standards Agency and BBSRC.
PM209 THE NASAL BRIDLE EFFECTIVELY SECURES NASOGASTRIC FEEDING TUBES AND AVOIDS UNNECESSARY INVASIVE ENTERAL AND PARENTERAL NUTRITION
1J. A. Bennell, 1S. Black, 1C. D. Murray, 2K. Moore. 1Gastroenterology, Royal Free Hospital, London, UK, 2Hepatology, Royal Free Hospital, London, UK
Introduction: Nasogastric feeding tubes are used in patients who are unable to manage an oral diet and who have a functioning gastrointestinal tract. However, many patients (17–67%) repeatedly dislodge their feeding tubes1 leading to potential malnutrition, patient discomfort and increased nursing time. Alternative nutrition delivery such as a feeding gastrostomy tube or parenteral nutrition each have inherent risks. Bridles, in which the nasogastric tube is secured round the nasal septum, have been used for many years, and lead to improved patient outcomes.2 3
Aims and Methods: All patients referred to the nutrition nurse over 12 months were included in the audit. Referral criteria included patient dependent on enteral feeding, with dislodgement of the nasogastric tube at least three times in one week resulting in missed feeds, or feeding tubes requiring endoscopic or radiological guidance and which had been dislodged once. All nasogastric tubes and bridles were placed by one clinical nutrition nurse specialist.
Results: Sixty bridle placements were requested (median age 75 years, range 28–100). Of the 60 requested, 51 requests were judged to be appropriate, and successful bridle placement was carried out in 45 of these 51 patients. Five patients were seen to pull their bridles, were restless or wore mittens. No nasal trauma was seen in any of the patients. Five stayed in for less than 24 h. Fifteen of 45 bridles stayed in place for 1–5 days. Fifteen patients kept the bridles in situ for 6–20 days and eight for more than 20 days (two unknown because patient transferred to another hospital). Sixteen of 45 bridles were unplanned removals by the patient, of which six continued with a form of tube feeding, four progressed to oral nutrition and six died. Of the remaining 29 patients who kept their bridles in, 12 patients progressed to oral feeding, seven to gastrostomy feeding, five had a second nasogastric tube and bridle placed, three coped with a nasogastric tube alone, two patients transferred to another hospital, eight patients had their treatment withdrawn and bridles removed and eight patients died with bridles in situ.
Conclusion: Bridles were safe, well tolerated and effective in this group of patients in delivering enteral nutrition. Bridles facilitate nutrition delivery until the patient recovers sufficiently to manage an oral intake. It avoids unnecessary escalation to percutaneous endoscopic gastrostomy feeding or intravenous nutrition.
PM210 USE OF NASAL BRIDLES TO SECURE NASOGASTRIC TUBES IMPROVES DELIVERY OF ENTERAL NUTRITION IN AT-RISK PATIENTS
1K. T. Cheung, 1E. Donaldson, 1T. Earley, 2P. Coulthurst, 1T. Shaw, 1P. L. Shields. 1Gastroenterology, Royal Preston Hospital, Preston, UK, 2Dietetics, Royal Preston Hospital, Preston, UK
Introduction: One of the major limitations of nasogastric feeding tubes is their frequent displacement, contributing to suboptimal delivery of nutrition. The repeated insertion of nasogastric tubes can be uncomfortable and is associated with risks including interruptions in the delivery of feed and repeated chest x rays. The use of nasal bridles allows for the securing of nasogastric tubes, avoiding the need for repeated nasogastric tube reinsertion, and theoretically this should result in less disruption to the delivery of prescribed feed. We have incorporated the use of nasal bridles into routine practice since 2005.1
Aims and Methods: The aim of the study was to determine if nasal bridles were effectively improving delivery of nutrition by preventing nasogastric tube displacement. A retrospective review of records was performed of patients who had a nasal bridle placed between March 2007 and February 2008. The indication for nasal bridle insertion was established. The previous number of repeated nasogastric tube insertions was determined. Delivered nasogastric feed was assessed for a 7-day period before nasal bridle insertion and a maximum of 30 days post-nasal bridle insertion. Reasons for inadequate feed delivery were determined.
Results: 134 patients were referred for nasal bridle insertion over the 12-month period. Notes were retrieved and feed delivery was assessed in 69 patients. 48 patients were referred for nasal bridle placement due to repeated nasogastric tube displacement (mean of 2.3 nasogastric tubes per patient). There were no significant complications associated with bridle insertion. Pre-bridle insertion, feed delivery was less than 50% prescribed in 67.3% (298/443) of total patient days. Post-nasal bridle insertion, days of feed delivery less than 50% fell to 13.4% (168/1256) (p<0.0001). 33% of patients required more than one nasal bridle (mean 1.4 reinsertions) during the follow-up period. This was mainly due to intentional removal by patients (n = 23) but nasogastric tube blockage (n = 3) also occurred.
Conclusion: Our experience shows that the use of nasal bridles is a safe and effective means of improving the delivery of enteral nutrition in malnourished patients. They also reduce nasogastric tube displacement. Nasal bridles can still be removed intentionally by patients and do not prevent feed disruption secondary to other causes. Nonetheless, in patients who continuously displace their nasogastric tubes, a nasal bridle should be used to limit disruption to feed delivery and the risks associated with repeated reinsertion.
PM211 DEFINING THE NON-SURGICAL CARE PATHWAY FOR PATIENTS WITH ENCAPSULATING PERITONEAL SCLEROSIS
1N. Abdul Satar, 1M. McGregor, 2C. Bebb, 2C. Byrne, 2M. Devonald, 2G. Mchaffie, 2S. Roe, 1K. Teahon. 1Gastroenterology, Nottingham City University Hospital, Nottingham, UK, 2Renal, Nottingham City University Hospital, Nottingham, UK
Introduction: Encapsulating peritoneal sclerosis (EPS) is a rare but recognised complication seen in patients who have had peritoneal dialysis.1 It is an inflammatory process that transforms the peritoneum into calcified, fibrous tissue enveloping the bowel into a “cocoon” formation. Because of its gastrointestinal manifestations, these patients are likely to present to gastroenterologists. However, their diagnosis and presentation are poorly defined, making management challenging.
Aims and Methods: Retrospective review of patients diagnosed with EPS in the past 5 years in Nottingham city hospital. Data were collected on: symptoms, investigations, management and complications.
Results: We identified nine patients (six men). The average age was 41 years (range 29–58). Risk factors are shown in the table. Of the nine, seven had had renal transplants. Four transplants had failed and of these, three had had two failed transplants. EPS presented with recurrent symptoms of ascites (33%), peritonitis (44%), small bowel obstruction (33%), vomiting (22%) and bloody ascites (11%). Other dominant symptoms were nausea and weight loss. The diagnosis was made on clinical suspicion confirmed with computed tomography (89%) and histology (66%) taken at laparotomy. Significant co-morbidities included diabetes, Goodpasture’s disease, anti-phospholipid syndrome and cystinosis. Complications included small bowel perforation, intra-abdominal sepsis and multi-organ failure. The medical management included converting peritoneal to haemodialysis (if not already done), tamoxifen to limit progression, ascitic drainage and nutritional support (often parenterally because enteral intake was limited by obstruction). 89% had at least one episode of total parenteral nutrition. There was one death secondary to intra-abdominal sepsis. Four have been considered for surgery.
Conclusion: Key issues in the non-surgical management of EPS are: (1) High clinical suspicion in patients who have been on peritoneal dialysis (>5 years’ duration) or who develop gastrointestinal symptoms, especially weight loss. (2) Early nutritional intervention to maximise oral intake and early consideration for parenteral nutrition. (3) Joint care with surgical team. (4) To help plan care we suggest documentation of: confirmation of diagnosis (computed tomography, laparotomy with or without histology), possible aetiology, nutritional state and monitoring plan, psychological health and support. (5) In defining the disease, the following subgroups are suggested: ascites predominant (serous, bloody or chyle); dilated gut predominant (present without overt obstruction but with nausea and weight loss); recurrent obstruction; recurrent infection.
PM212 A REVIEW OF OUTCOMES IN PATIENTS ON HOME PARENTERAL NUTRITION MEETING CRITERIA FOR INTESTINAL TRANSPLANT: PRELIMINARY RESULTS FROM A SINGLE CENTRE LONGITUDINAL STUDY
1P. Paskaran, 1A. U. Murugananthan, 1T. C. Shepherd, 1D. A. J. Lloyd, 2S. J. Middleton, 1J. M. D. Nightingale, 1S. M. Gabe. 1Lennard–Jones Intestinal Failure Unit, St Mark’s Hospital, Harrow, UK, 2Gastroenterology, Addenbrooke’s Hospital, Cambridge, UK
Introduction: Survival following intestinal transplantation (ITx) is improving, but despite this referral rates in the UK remain low. Current survival at 5 years post-ITx ranges between 37% and 50% compared with 73% 5-year survival for patients on home parenteral nutrition (HPN).1 2 We have previously shown that 37% of all patients on HPN at our institution meet the criteria for referral for ITx.3 Despite this only 16% were referred for consideration of ITx.
Aims and Methods: Our aims were to assess: (1) the number of patients receiving HPN at St Mark’s Hospital meeting the criteria for ITx; (2) the number of patients referred for ITx and (3) differences in survival rates between the two groups. All patients receiving HPN on 1 January 2005 were assessed at yearly intervals for 3 years according to the Medicare ITx criteria.1 Eligibility for referral was based on the fulfillment of one or more of the following criteria over each 12-month period: advanced parenteral nutrition-associated liver disease; thrombosis of two or more major veins; frequent central venous catheter sepsis (two or more episodes in the previous 12 months, fungaemia or septic shock); frequent severe dehydration and patient request/quality of life.
Results: 123 patients were reviewed in 2005, 122 in 2006 and 118 in 2007, the fall representing either discontinuation of HPN or death. Underlying aetiologies resulting in intestinal failure for these patients were Crohn’s disease (31%), vascular (27%), pseudo-obstruction (16%), surgical complications (13%) and others (13%). The percentage of patients meeting ITx criteria was fairly stable over the 3 years as was the percentage of patients referred. All patients with parenteral nutrition-associated liver disease were referred, but only 21% of patients with venous thrombosis and 6.5% of patients with central venous catheter sepsis were referred. There was no significant difference in mortality between the two subgroups, with a 6.1% mortality rate in patients meeting the criteria and 6.5% in those who did not.
Conclusion: The referral rate for consideration of ITx was considerably lower than the number of patients meeting the criteria. Our results show similar mortality rates in patients meeting ITx criteria as opposed to those not meeting the criteria, suggesting that the ITx criteria are not selecting patients with a poor prognosis.
PM213 GASTRIC HYPOCHLORHYDRIA AND INTESTINAL BARRIER DYSFUNCTION IN HIV INFECTION IS NOT DEPENDENT ON NUTRITION: A RANDOMISED CONTROLLED TRIAL OF SUPPLEMENTATION
1P. Kelly, 2T. Shawa, 1I. Sanderson. 1Institute of Cell and Molecular Science, Barts and The London School of Medicine, London, UK, 2TROPGAN, University of Zambia School of Medicine, Lusaka, Zambia
Introduction: Although there is evidence that supplementation with some micronutrients reduces morbidity and mortality caused by diarrhoeal disease, host defence against intestinal infection and bacterial translocation is poorly understood. We took the opportunity of a randomised controlled trial of micronutrient supplementation in Zambian adults to test the hypothesis that micronutrient supplementation can enhance barrier function of the gut.
Aims and Methods: To assess determinants of barrier function in a nutrition trial in Zambian adults. All consenting adults (18 years or older) living in a carefully defined sector of Misisi, Lusaka, Zambia, were included in a randomised, double-blind placebo-controlled trial with a mid-point crossover. There were no exclusion criteria. Participants were randomly assigned to receive a daily tablet containing 15 micronutrients at just above the recommended nutrient intake, or placebo. Primary endpoints were gastric pH, mucosal permeability, mucosal monosaccharide absorption, lipopolysaccharide and anti-lipopolysaccharide antibodies in peripheral blood and tumour necrosis factor activation.
Results: Hypochlorhydria (fasting gastric pH >4.0) was present in 75 (37%) samples from 203 participants. HIV infection (odds ratio (OR) 4.1; 95% CI 2.2 to 7.8; p<0.001) was associated with hypochlorhydria, but taking highly active antiretroviral therapy (OR 0.16; 95% CI 0.04 to 0.67; p = 0.01) and allocation to micronutrient supplementation (OR 0.53; 95% CI 0.28 to 0.99; p<0.05) were protective. Hypochlorhydria was associated with an increased risk of salmonellosis. Intestinal permeability, lipopolysaccharide concentrations in serum, anti-lipopolysaccharide IgG and IgM, and serum tumour necrosis factor receptor p55 concentrations were measured in 87 participants, but did not differ significantly between micronutrient and placebo groups. No correlations of any of these measures of barrier function with nutritional status were detected.
Conclusion: Apart from an effect on hypochlorhydria, which was only revealed after adjustment for HIV status, micronutrient supplementation did not impact on these measures of barrier function at the doses used. Important effects of HIV and highly active antiretroviral therapy on gastric pH may explain some of the increased susceptibility of HIV-infected adults to intestinal infection.
PM214 HEALTHCARE PROFESSIONALS’ KNOWLEDGE ABOUT PERCUTANEOUS GASTROSTOMY FEEDING: HOW WELL ARE WE DOING?
1S. Thomas, 2F. C. Leslie. 1School of Medicine, University of Keele, Keele, UK, 2Department of Gastroenterology, University Hospital of North Staffordshire, Stoke-on-Trent, UK
Introduction: There is a reasonable body of evidence to support the use of percutaneous gastrostomy (PEG) feeding for stroke patients, but no evidence to support this practice in advanced dementia. A previous study showed that 34% of UK consultants would refer a patient with dementia for a PEG.1 In the light of the new Mental Capacity Act it is vital that healthcare professionals are able to make evidence-based decisons and advise patients and families appropriately.
Aims and Methods: We were keen to explore healthcare professionals’ knowledege about PEG feeding. We were also keen to identify whether teaching had any influence on knowledge. A simple questionnaire was given to a range of healthcare professionals in four hospitals across the midlands and to an expert group (Midlands Gastroenterogy Group). Participants were asked about two scenarios of dysphagic stroke and advanced dementia. They were also asked if they had received any teaching and how much relevant experience they had.
Results: 556 of 714 questionnaires were collected (78%) from hospital doctors of all levels and general practitioners (GPs), medical students, nurses and dieticians. More respondents answered questions about dysphagic stroke correctly compared with dementia. Only 10% of hospital consultants would refer the dementia patient for a PEG compared with 31% of GPs, 37% of F1/F2 doctors, 36% of medical students and 45% of nurses. Only 29% of all respondents felt that PEG would prevent aspiration pneumonia in the dementia patient (although nurses’ opinion was split 45% vs 45%). 20% of respondents felt PEG would improve life expectancy. Dieticians as a group were most likely to answer questions correctly. 64% of respondents had experience with similar patients including 77% of GPs and 69% of foundation doctors. Teaching significantly influenced answers for the dementia scenario (p = 0.001). Only 29% had received teaching and only 4% of GPs had attended relevant teaching. Experts were more likely to answer correctly (p = 0.004).
Conclusion: Despite improvements in consultants’ knowledge compared with previous studies, there are still significant gaps in knowledge. Training improves knowledge and this study suggests more teaching should be planned, particularly aimed at nurses, medical students, junior doctors and GPs.
PM215 GLUTEN LEVELS IN COMMERCIAL QUINOA PRODUCTS
1V. F. Zevallos, 1H. J. Ellis, 2L. I. Herencia, 1P. J. Ciclitira. 1Gastroenterology, St Thomas’s Hospital, London, UK, 2Producción Vegetal, Universidad Politécnica de Madrid, Madrid, Spain
Introduction: The only effective treatment for patients affected by coeliac disease is to follow a gluten-free diet (GFD). Permanent exclusion of gluten from the diet is essential to maintain normal villous architecture and to reduce the risk of other complications. A GFD includes naturally occurring gluten-free cereals such as rice, millet and maize. Quinoa can be an alternative for the diet of coeliac disease patients1 but its incorporation as a food ingredient could be accompanied by the risk of contamination. Therefore, we have assessed the safety of various gluten-free quinoa products in the UK.
Aims and Methods: We used dot immunobinding assays and four murine monoclonal antibodies to known coeliac-toxic gluten proteins and peptides. Furthermore, we used ELISA2 to quantify toxic peptides. Prolamins were extracted from quinoa products and commercially obtained wheat starches of known gluten content using an in-house extraction buffer with a reducing agent. All samples were spotted onto a nitrocellulose membrane and exposed separately to the antibodies, enzyme-linked anti-mouse secondary antibody and chromogen. The ELISA was performed using a monoclonal antibody to a toxic A-gliadin peptide.
Results: The wheat starches had strong, moderate and negative reactions in the dot assays. Most quinoa products were negative, a few borderline and one positive to one or both of the antigliadin antibodies. ELISA indicated that products with borderline results had no detectable gliadin, as measured by PN3 (anti-A-gliadin 31–49) but one product had a gluten content of 76 mg/kg.
Conclusion: Quinoa products may be a safe alternative for coeliac disease patients, the majority of gluten-free products containing quinoa have levels of gluten below 20 mg/kg, which is in agreement with the current recommendations.3 However, one product may need to be relabelled as it contains more than 20 mg/kg but less than 100 mg/kg. New legislation to regulate the labelling of gluten-free products is expected to come in the near future. Therefore, further tests will be undertaken to assess the safety of new and existing gluten-free products.
Colorectal/anorectal posters
PT216 PREDICTION OF SEVERE 5-FLUOROURACIL TOXICITY IN GASTROINTESTINAL CANCER CHEMOTHERAPY: ROLE OF DIHYDROPYRIMIDINE DEHYDROGENASE DEFICIENCY
1A. Loganayagam, 2L. Fairbanks, 2M. Arenas-Hernandez, 3P. Ross, 2T. Marinaki, 1J. D. Sanderson. 1Gastroenterology, Guys and St Thomas NHS Trust, London, UK, 2Purine Research, Guys and St Thomas NHS Trust, London, UK, 3Oncology, Guys and St Thomas NHS Trust, London, UK
Introduction: 5-Fluorouracil (5-FU) and its analogues remain a key component of chemotherapeutic regimens for the adjunctive treatment of gastrointestinal cancer. Up to 20% of patients experience severe (grades 3 and 4) toxicity, particularly severe mucositis, limiting effective therapy and resulting in significant morbidity, healthcare costs and, occasionally, fatality. 5-FU toxicity has been reported in association with polymorphic variation dihydropyrimidine dehydrogenase (DPD) activity but such polymorphism has previously been considered absent in UK populations. The DPYD IVS14+1G>A mutation has a reported frequency of 1.8% in European populations
Aims and Methods: To assess the contribution of DPYD polymorphism to 5-FU toxicity among UK patients treated for gastrointestinal cancer. Sequencing of the coding region of the DPYD gene was undertaken in 47 patients (27 women, mean age 61 years), mainly with colorectal cancer, experiencing grade 3 or 4 toxicity on 5-FU according to common terminology criteria for adverse events.
Results: Myelotoxicity (38%) and diarrhoea (38%) were the most frequent toxicities, followed by mucositis (18%), hand–foot syndrome (4%) and neurotoxicity (2%). Four of 47 (8.5%) patients carried the DPYD IVS14+1G>A mutation. All four cases were women and three of the four had severe diarrhoea. A further six cases carried other DPYD mutations (D949V n = 4, I560S n = 1, V7321 n = 1). In total, 10 (21%) patients carried DPYD mutations.
Conclusion: Contrary to previous estimates for a UK population, genetic DPD deficiency may account for approximately 20% of cases of severe 5-FU toxicity. Higher frequencies of 25–30% have been reported in non-UK European series, also with a gender bias. The metabolic influence of DPD deficiency is such that toxicity should be avoidable by previous testing and an appropriate 5-FU dose or regimen alteration.
PT217 20 MHZ HIGH-FREQUENCY MINIPROBE ULTRASOUND AS AN AIDE TO TRANSANAL ENDOSCOPIC MICROSURGERY: COMPARISON WITH MAGNETIC RESONANCE IMAGING
1A. K. Haji, 2S. Ryan, 3I. Bjarnason, 1S. Papagrigoriadis. 1Colorectal Surgery, Kings College Hospital, London, UK, 2Radiology, Kings College Hospital, London, UK, 3Gastroenterology, Kings College Hospital, London, UK
Introduction: Transanal endoscopic microsurgery (TEMS) is a technique for the resection of rectal tubulovillous adenomas and early cancer. Accurate local staging of these lesions is of paramount importance to guide management before TEMS resection. This study compares the local staging of magnetic resonance imaging (MRI) and 20 MHz miniprobe ultrasound of consecutive patients deemed suitable for the TEMS procedure.
Aims and Methods: Inclusion criteria included all rectal tumours below the peritoneal reflection and benign histology on endoscopic biopsy. Informed consent was obtained in all cases. All patients had MRI of the anorectum and pelvis (unless contraindicated), colonoscopy and 20 MHz miniprobe ultrasound (Olympus Keymed UM-3R, Japan). Depth of invasion (T stage) of the lesion by MRI and 20 MHz ultrasound were compared with final histology. Statistical differences were analysed using χ2 and Fisher’s exact t tests with Graphpad Prism 5 (version 5.1, 2007).
Results: 19 patients were studied, mean age 69.5 years (range 27–89). Mean distance of the tumour from the anal verge was 10 ±3 cm (SE 0.7, range 5–15 cm). The tumours occupied 10–50% of the rectal circumference, with a mean of 30 ± 15% (SE 3.4). Histological assessment revealed 11 benign lesions with dysplasia (five high grade, six low grade) and eight adenocarcinomas (seven T1 with three mucosal and four submucosal cancers, one T3). 16/19 (84%) patients had clear histological resection margins. MRI did not discriminate between mucosal and submucosal lesions and these were grouped together for analysis. Therefore, 18 patients had lesions superficial to the muscularis propria (11 benign and seven malignant). Four patients did not have preoperative MRI including the patient with histological T3 stage. For lesions superficial to the muscularis propria (T0/T1), MRI correctly staged five of 15 lesions (33%), overstaging 10 patients (67%): six as T2 lesions and four as T3. 20 MHz ultrasound was superior to MRI for lesions superficial to the muscularis propria (p = 0.002). The accuracy of 20 MHz ultrasound for assessing the depth of lesion was 95% (18/19 correctly identified). In addition, 20 MHz ultrasound was able to differentiate between mucosal and submucosal lesions with a sensitivity of 93% and specificity of 75%, giving a positive predictive value of 93% and a likelihood ratio of 3.7.
Conclusion: 20 MHz miniprobe ultrasonography is superior to the conventionally used MRI for the assessment of T1 lesions with high sensitivity in differentiation between mucosal and submucosal lesions. This may become an essential adjunct for the assessment of patients undergoing TEMS.
PT218 DIFFERENTIAL EXPRESSION PROTEOMICS IN APCMIN/+ MICE COLON FOLLOWING TREATMENT WITH PEROXISOME PROLIFERATOR-ACTIVATED RECEPTORS ALPHA LIGAND, FENOFIBRATE
1A. Shonde, 1V. Subramanian, 2A. Bennett, 1C. Hawkey. 1Wolfson Digestive Diseases Centre, Nottingham University Hospital, Nottingham, UK, 2Biological Sciences, University of Nottingham, Nottingham, UK
Introduction: Peroxisome proliferator-activated receptors (PPAR) are ligand-activated nuclear receptors that were discovered in 1990. PPARα is expressed at low levels in human colorectal cancers. APCMin/+ mice fed with fenofibrate (a PPARα ligand) have significantly less tumour burden in the small intestine and colon compared with controls. Our group has looked at PPARα gene expression changes, but RNA expression does not predict the synthesis of a corresponding protein.
Aims and Methods: 25–50 mg flash-frozen fragmented colonic tissue from three APCMin/+ mice treated with fenofibrate 100 mg/kg per day and three APCMin/+ mice treated with vehicle were used for this experiment. The cytosolic protein fraction was extracted using ProteoExtract (Merck, Nottingham, UK) subcellular proteome extraction kit. Samples were fractionated using reversed-phase solid phase extraction followed by sodium dodecylsulphate polyacrylamide gel electrophoresis of the fractions. Differentially expressed proteins were subjected to in-gel tripsinolysis. The peptides were then analysed by matrix-assisted laser desorption ionisation time of flight mass spectrometry. Proteins of interest were then identified by interrogating the Mascot database. The identity of the proteins was reconfirmed by standard Western blotting.
Results: We identified four proteins with significantly altered expression in colonic tissue of APCMin/+ mice colon tissue treated with fenofibrate compared with controls. Two of these proteins, superoxide dismutase 2 (SOD2) gene (increased expression by fenofibrate) and alpha-enolase 1 (decreased expression by fenofibrate) expressions were confirmed by using Western blot analysis. The others were carbonic anhydrase II and transgelin, both of which showed reduced expression in treated colonic tissue. SOD2 has been implicated as a candidate tumour suppressor gene for human malignant melanoma and SOD2 mutations have also been found in 60% of colon cancer cell lines examined.1 Transgelin and alpha-enolase 1 protein expression has been shown to be decreased in colitis-associated colon cancer. In addition, transgelin expression has been shown to be significantly reduced in human colon tumours compared with adjacent non-tumorous tissues.2 Interestingly, the expression of carbonic anhydrase I has been shown to be correlated with the biological aggressiveness of colorectal cancer.3
Conclusion: In APCMin/+ mice, fenofibrate treatment results in the differential expression of proteins that could mediate the PPARα activation-related suppression of colon tumour formation.
PT219 WHAT ARE THE CHARACTERISICS OF POLYPS DETECTED BY THE NHS BOWEL CANCER SCREENING PROGRAMME
C. Harmston, J. Hunter, L. Wong. Surgery, University Hospital Coventry, Coventry, UK
Introduction: The NHS bowel cancer screening programme is currently being introduced following three rounds of pilot screening. This study outlines the important characteristics of polyps detected by pilot screening.
Aims and Methods: The first 100 patients with screen-detected polyps at University Hospital Coventry and Warwickshire were identified from the colorectal cancer screening database. Polyp charactersitics were drawn from the hospital’s computerised endoscopy reporting system and cross-referenced with the pathology reporting system for further information. Polyp location was compared with the location of symptomatic cancers detected in the University Hospital Coventry and Warwickshire symptomatic cancer database.
Results: 100 patients were selected for investigation. 179 polyps were detected. The average age of patients with polyps was 61 years. 35% of patients were under the age of 60 years. There were 68% men and 32% women. The average size of the largest polyp per patient was 13.8 mm. 85% of polyps were excised. Histology was available on 162 polyps: tubulovillous 43%, tubular adenoma 33%, metaplastic polyp 9.3%, hyperplastic polyp 8%, villous adenoma 4%. 90% showed low-grade dysplasia, 10% high grade. The location of screen-detected polyps is outlined in the table. The location of screen-detected polyps was significantly different from that of the location of symptomatic cancers detected in our database (p<0.01). There was a higher proportion of sigmoid polyps and a lower proportion of caecal polyps when compared with symptomatic cancers.
Conclusion: This study outlines the important characteristics of screen-detected polyps. The significant difference in location of polyps from cancer suggests a variation in the malignant potential of polyps, dependent on location.
PT220 INCIDENCE OF COMPLICATIONS IN BOWEL CANCER SCREENING COLONOSCOPY IS LOW DESPITE INCREASED NEED FOR THERAPY
1D. Nylander, 2M. Ritchie, 1J. Painter, 3M. Rutter, 3L. Hurst, 2J. Singh, 4C. Rees. 1Gastroenterology, South of Tyne Screening Centre, Sunderland Royal Hospital, Sunderland, UK, 2South of Tyne Screening Centre, QE Hospital, Gateshead, UK, 3Teesside Screening Centre, North Tees, UK, 4South of Tyne Screening Centre, South Tyneside Hospital, South Shields, UK
Introduction: Many publications have estimated the complications of colonoscopy (summarised by Bowes et al).1 These are used to help inform patients undergoing colonoscopy. The estimates are also used in NHS publications given to patients attending for bowel cancer screening colonoscopy (BCSC). However, these data are mainly from colonoscopies in symptomatic patients. The incidence of polyps, hence the need for therapy in BCSC (approximately 48%) is significantly higher than in “symptomatic” colonoscopy services. The BCSC patient leaflet quotes the risk of “heavy” bleeding from polypectomy as one in 150; the risk of perforation from colonoscopy is one in 1500.
Aims and Methods: We aimed to assess our 30-day complications to see if we have been giving accurate information to patients. BCSC has been carried out at the South of Tyne Screening Centre and the Teesside Screening Centre since March 2007 as part of the first wave. Data from colonoscopies performed between 1 March 2007 and 30 September 2008 were extracted from the national screening database and checked against our local record of “adverse” incidents.
Results: 1386 colonoscopies were performed in the study period. The caecal intubation rate on an intention to treat basis was 98.3%. Adenomas were found and endoscopic therapy was performed in 622 patients. A further 36 patients had polyp cancers resected. Recorded adverse events were as follows: bleeding—three patients after polypectomy, two immediate (one had been on warfarin; international normalised ratio 1.4 before the procedure), each needed two units blood transfusion and one at day 4 settled spontaneously; perforation—one patient, 24 h after resection of 4 cm polyp, had right hemicolectomy as histology was malignant; death—one patient died at day 25 post-polypectomy, post-mortem identified left main coronary occlusion as cause of death, unrelated to colonoscopy; other—one patient had persistent clinical obstruction after polypectomy within tight sigmoid diverticular stricture, histology—malignant with complete extraction, sigmoid colectomy confirmed stricture with no complications of polypectomy; one patient had chest pain on day 10 post-polypectomy, felt to be unrelated.
Conclusion: The incidence of bleeding from polypectomy was one in 219. This incidence would be lower if it was quoted per polypectomy, as several patients had more than one polyp and also several had metaplastic polyps removed. Despite there being more therapeutic procedures than in the symptomatic service the complication rates are well within internationally quoted ranges.
Submitted on behalf of the Northern Regional Endoscopy Group.
PT221 REDUCED PREDICTED MORTALITY FOR COLORECTAL CANCER IN ASYMPTOMATIC PATIENTS DETECTED BY MASS SCREENING WITH IMMUNOCHEMICAL FAECAL OCCULT BLOOD TEST IN ITALY
1F. Parente, 1B. Marino, 1A. Anderloni, 2P. Tricomi, 3G. Ucci, 3M. Gilardoni, 4P. Carzaniga, 4M. Costa, 5N. Devecchi, 5F. Tortorella, 6M. Pirona, 5R. Moretti. 1Gastrointestinal Unit, A Manzoni Hospital, Lecco, Italy, 2Pathology Service, A Manzoni Hospital, Lecco, Italy, 3Oncology Department, A Manzoni Hospital, Lecco, Italy, 4Surgical Department, A Manzoni Hospital, Lecco, Italy, 5Screening Unit, Local Health Care Centre, Lecco, Italy, 6Screening Unit, Regional Reference Centre, Milan, Italy
Introduction: The major aim of population-based colorectal cancer (CRC) screening programmes is to reduce disease-related mortality by the detection of cancers at an earlier stage and by removal of its precursors (adenomatous polyps). However, measuring a reduction of mortality takes many years after screening implementation. In the mean time there is a need for intermediate outcome measures in order to estimate the improvement of prognosis and, therefore, the efficiency of the programme.
Aims and Methods: We aimed to compare tumour stages at diagnosis and predicted mortality of asymptomatic CRC detected by immunochemical faecal occult blood test (FOBT) during the first round of a mass-screening programme of Lecco province (characterised by a FOBT uptake of 50% and colonoscopy compliance of 92%) with those of CRC detected in the same population during the screening period (January 2006–8). Tumour–node–metastasis (TNM) classification and tumour stages were assessed in 95 screened CRC (4.6% of FOBT-positive individuals undergoing colonoscopy) and in 100 out of 285 non-screening cancers belonging to the same age strata (50–69 years). According to data from the regional registry of cancer, the 5-year mortality of the two cohorts of patients was estimated by TNM stage and analysed with a two proportion test. We also compared the anatomical distribution of cancers and the presence of synchronous lesions along the colon in the two populations.
Results: Predicted 5-year-specific mortality was significantly higher in non-screening CRC patients compared with asymptomatic cancers detected by FOBT (43% vs 18%, p<0.0001). Treatment could be confined to colonoscopy and polypectomy/mucosectomy alone in 34% of screen-detected cancers compared with only 5% (p>0.0001) of non-screening CRC, whereas chemotherapy/radiotherapy was necessary in 35% and 92% of patients of the two groups, respectively (p>0.0001). No significant difference in the anatomical distribution of cancers nor in the presence of synchronous lesions along the colon was found between symptomatic and asymptomatic patients.
Conclusion: CRC are detected at earlier stages in asymptomatic individuals with positive immunochemical FOBT compared with symptomatic patients not participating in the screening programme. Therefore, the predicted 5-year disease-related mortality rate is significantly reduced already by the first round of screening with immunochemical FOBT. In as many as 34% of asymptomatic screen-detected CRC, treatment could be confined to colonoscopy and polypectomy/mucosectomy alone, thus saving significant economic resources.
PT222 POST-POLYPECTOMY COLONOSCOPY SURVEILLANCE: ADENOMA RECURRENCE AND RISK AT FOLLOW-UP
G. J. Sadler, J. Fallaha, B. C. McKaig. Gastroenterology, New Cross Hospital, Wolverhampton, UK
Introduction: Patients who have adenomas removed at colonoscopy are at increased risk of developing colorectal cancer (CRC) in the future. Current British Society of Gastroenterology guidelines stratify adenomas at baseline as low risk (1–2 small; <1 cm), intermediate risk (3–4 small or at least one >1 cm) or high risk (>5 adenomas or >3 adenomas at least one of which is >1 cm). Sessile lesions are classified separately. Risk is refined at each subsequent colonoscopy and determines surveillance after adenoma removal.1
Aims and Methods: We audited our database to determine colonoscopy findings at follow-up for patients undergoing polyp surveillance and compared these with the findings at the most recent previous colonoscopy.
Results: Data from 180 colonoscopies performed for the purpose of “polyp follow-up” are presented. 84% of patients whose most recent previous examination was negative and 63% of those patients with low-risk adenomas at the most recent previous colonoscopy were found to have adenomas at the next follow-up. Of those with intermediate-risk, high-risk and sessile adenomas at the most recent previous colonoscopy, 69%, 63% and 77%, respectively, were found to have intermediate, high-risk or sessile adenomas at the next follow-up. CRC was found in 6.6% of the total population undergoing surveillance—91% of cases occurred in patients in whom the adenoma risk at the most recent previous colonoscopy was classed as intermediate, high or sessile. No significant relationships were found between adenoma risk at previous and follow-up colonoscopy, other than for sessile polyps, which occurred significantly more frequently in those with a previous history of sessile polyps (p<0.05).
Conclusion: With the exclusion of sessile lesions, polyp risk at the most recent previous colonoscopy does not appear to predict polyp risk at the follow-up examination. Although CRC tended to occur in patients with a previous polyp risk of intermediate grade or greater, which supports the shorter screening interval proposed for higher-risk lesions, it is clear that adenomas are found at subsequent colonoscopy in the vast majority of patients with a history of polyps, even in those whose most recent examination was negative. Given these findings, should we consider discharging patients with a history of adenomatous polyps from follow-up at all?
PT223 CLINICAL SIGNIFICANCE OF FLUORINE-18 FLUORODEOXYGLUCOSE POSITRON EMISSION TOMOGRAPHY FOR RECURRENT COLORECTAL CANCER
H. Ishikawa, A. Watanabe, T. Ohyama, T. Mukogawa, T. Inoue, S. Kinoshita, N. Kawai, K. Nakagawa, K. Emoto, S. Ogawa. Department of Surgery, Nara Prefectural Hospital, Nara, Japan
Introduction: Fluorine-18 fluorodeoxyglucose positron emission tomography (FDG-PET) has been accepted as an effective tool of diagnosis and staging for patients with known or suspected recurrent colorectal cancer.
Aims and Methods: This study is to analyse the clinical significance of FDG-PET on the diagnosis and indication for surgical intervention for recurrent colorectal cancer. 31 consecutive patients, with known or suspected recurrence of colorectal cancer based on the elevation of tumour markers or abnormal findings on the follow-up computed tomography (CT) image, underwent FDG-PET 49 times between December 2003 and August 2007. Patients were aged between 35 and 79 years (median 61), 18 were men, 10 were Duke’s A or B stage and 17 had a history of colon cancer. The average of recurrence was two times (range 1–6). The average period between operation and first FDG-PET was 28 months (range 1–89). Of 31 cases, 30 had elevated serum carcinoembryonic antigen or CA19-9 (96.7%). For each case the diagnosis of FDG-PET image was compared with that of CT image and the final diagnosis.
Results: 31 patients were divided into three groups according to the purposes of FDG-PET: to identify recurrent colorectal cancer by FDG-PET (identification group, n = 4); to determine malignancy and disease spread (disease spreading group, n = 23); and to evaluate the possibility of surgical intervention in recurrence-confirmed cases (follow-up group, n = 4). In the identification group, FDG-PET alone could identify recurrence and indicate operation for three cases (six times). One of three cases showed diease-free survival for 18 months after a common iliac replacement operation. In the disease-spreading group, 11 cases with localised disease spread by FDG-PET findings were indicated for operation, nine cases with diffuse disease spread were judged as contraindicated for operation. The average survival period of the operation series was longer than that of the contraindicated series (24 vs 12 months). In the follow-up group, no case was indicated for salvage operation because FDG-PET could detect lesions of the whole body at one study. FDG-PET was shown to be false positive in one case and false negative in one case. The sensitivity of FDG-PET was 93.8% and its accuracy was 91.8%, whereas those of CT were 83.3% and 81.6%, respectively.
Conclusion: FDG-PET could visualise malignant lesions and was an effective modality to evaluate not only disease spread but distant metastasis for the recurrence of colorectal cancer. FDG-PET is very useful in detecting recurrence at an earlier stage and in decision-making for surgical intervention.
PT224 THE USE AND EFFICACY OF STERCULIA FOR PATIENTS WITH DEFAECATORY DISORDERS
1U. Khalid, 2K. Thomas, 1A. Lalji, 1J. Andreyev. 1Gastrointestinal Unit, Royal Marsden Hospital, London, UK, 2Computing, Royal Marsden Hospital, London, UK
Introduction: Normacol is a bulk-forming laxative that consists of 62% sterculia granules, a vegetable gum extract from the karaya tree. Sterculia absorbs water and can swell to more than 60 times its original volume, allowing it to bulk stool and stimulate peristalsis. It is poorly fermented and thus does not significantly increase flatulence. There is very little research-based evidence to support its use.
Aims and Methods: The aim of this study was to evaluate the use of normacol and its efficacy in patients with bowel symptoms related to previous cancer treatments. A retrospective audit was conducted for all patients who were prescribed normacol between January 2005 and August 2008 and who had returned for follow-up evaluation.
Results: 76 men and 47 women, median age 68 years, were identified. In 84% previous pelvic radiotherapy was the likely cause of their symptoms. 62% of patients were prescribed normacol for faecal loading/constipation, 83% for urgency/loose stool, 70% for frequency, 52% for faecal incontinence, 28% for tenesmus and 26% for wind. Follow-up was available for a median 63 days (range 8–1085) after the first date of prescription. 57% of the constipated group, 68% of the urgency group, 35% of those with frequency, 39% of those with incontinence, 44% of those with tenesmus and 41% of those with wind reported significant benefit from the use of this bulking agent. No serious adverse effects were seen. 66% of patients were fully compliant, 15% partly compliant and 10% non-compliant with their prescription of normacol. Of those who were partly or non-compliant, 52% found it ineffective and 22% were unable to tolerate it (due to taste and aggravated symptoms). At least 50% of patients continued to use this bulking agent long term.
Conclusion: This audit suggests that normacol can be an effective treatment in many patients with a range of defaecatory disorders, especially following pelvic radiotherapy. Further prospective evaluation of the efficacy of normacol is warranted.
PT225 THE IMPACT OF CHRONIC CONSTIPATION ON QUALITY OF LIFE IN ADULTS AND CHILDREN: A SYSTEMATIC REVIEW
1J. Belsey, 2S. Greenfield, 3D. Candy, 4M. Geraint. 1JB Medical Ltd, Sudbury, UK, 2QE2 Hospital, Welwyn Garden City, UK, 3Royal West Sussex Trust, Chichester, UK, 4Norgine Pharmaceuticals Ltd, Harefield, UK
Introduction: The objective was to identify published quality of life assessments in patients with constipation and to place the impact of constipation within the context of other chronic conditions.
Aims and Methods: A systematic review was carried out using MEDLINE, EMBASE, Cochrane Library and Google Scholar, supplemented by hand searching of journals. Studies that assessed health-related quality of life (HRQoL) in patients of any age with chronic functional constipation were identified. The results were then limited to those studies that used a generic, rather than gastrointestinal-specific assessment tool.
Results: The search identified 14 studies that fulfilled the inclusion criteria. Eight adult studies used the short form 36 (SF-36) questionnaire, one the short form 12 (SF-12) and two the psychological general well being index. Two studies in children used the PedsQL questionnaire and one the CHQ-PF50. All studies showed reduced HRQoL in patients with constipation compared with population norms. Pooled and normalised results from studies using the SF-36 and SF-12 showed quality of life impairment compared with control populations on both the mental composite score (MCS; 45.8 vs 48.8) and the physical composite score (PCS; 47.5 vs 51.3). Although scores were reduced across all domains, the main reductions contributing to this difference were in the domains: general health, mental health and social functioning. The table compares the results for MCS and PCS in constipation with values obtained for other common chronic conditions.1 These findings were consistent with the results from studies using other HRQoL tools and were noted equally in adult and elderly populations. The paediatric studies yielded similar qualitative results.
Conclusion: The impairment in HRQoL observed in chronic functional constipation is comparable with that seen in conditions that might be regarded as more “serious”, such as osteoarthritis, rheumatoid arthritis and diabetes. Unlike in these conditions, constipation is amenable to alleviation using a range of well-established, safe and low-cost treatments. Given that the population prevalence of constipation is approximately 15%, the adoption of strategies to improve management may be expected to yield significant gains in quality of life in a cost-effective fashion.
PT226 MEDIUM-TERM OUTCOME WITH TRANSANAL IRRIGATION FOR NEUROGENIC BOWEL DYSFUNCTION IS RELATED TO RECTAL COMPLIANCE
J. B. Storrie, S. Harding, A. J. Raeburn, P. M. Trivedi, G. Preziosi, A. V. Emmanuel. Gastrointestinal Physiology, University College Hospital, London, UK
Introduction: Management of neurogenic bowel dysfunction (NBD) is empirical and often of limited success, leaving bowel symptoms as a major source of physical and psychological distress in patients with neurological disease. Transanal irrigation (Peristeen) has been shown in the short-term to improve constipation, faecal incontinence and symptom-related quality of life in these patients. However, longer-term data are not available and it is not clear whether response can be predicted by baseline physiology parameters. We hypothesised that rectal compliance, a measure of distensibility, would predict response to such an irrigation regime.
Aims and Methods: Ten patients (seven women, median age 47.5 years) were enrolled. Three had multiple sclerosis, three supraconal spinal injury, two cauda equina lesions and two spina bifida (median disease duration 10.5 years). Compliance was assessed (at baseline and at the end of treatment) using a barostat catheter placed into the rectum, with staircase distensions performed (0–40 mm Hg) in 4 mm Hg increments. The validated NBD score was assessed before training in the irrigation system and again after at least 4 months (median 6 months) of treatment.
Results: The median baseline NBD score was 17.5 (severe >14), with eight of 10 patients having scores greater than 14. At a median of 6 months of transanal irrigation, the median NBD score was significantly reduced (p = 0.0003) to 9.5 (minor 7–9), with one of 10 patients having a score greater than 14. Compliance did not change with treatment (median 12.7 ± 5.7 ml/mm Hg vs 12.4 ± 4.8 ml/mm Hg). However, baseline compliance was significantly negatively associated with a reduction in the NBD score, implying that reduced rectal compliance was predictive of good response to transanal irrigation.
Conclusion: Transanal irrigation provides medium-term benefit in patients with neurogenic bowel dysfunction secondary to a range of neurological disorders. Reduced rectal compliance predicts good outcome. This may represent a phenomenon that patients with a greater resistance to rectal overdistension are the most likely to respond to an irrigation regime.
PT227 COLORECTAL CANCER DETECTION: TIME TO ABANDON BARIUM ENEMA?
1K. Sheikh, 1M. K. Shariff, 2N. Carroll, 3D. Greenberg, 3K. Wright, 1E. A. Cameron, 1M. Parkes. 1Department of Gastroenterology, Addenbrooke’s Hospital, Cambridge, UK, 2Department of Radiology, Addenbrooke’s Hospital, Cambridge, UK, 3Eastern Cancer Registration and Information Centre, Cambridge, UK
Introduction: The sensitivity of double contrast barium enema (DCBE) for colorectal cancer (CRC) has been reported as 85–95%, but many hospitals in the UK still rely on DCBE to investigate a substantial proportion of symptomatic patients—mainly as a demand management strategy. Given its low sensitivity for serious pathology, we wanted to address the question of whether, in the era of colorectal cancer (CRC) screening, this strategy is still valid.
Aims and Methods: Our aim was to identify what proportion of patients diagnosed with CRC in Cambridge had undergone DCBE within 2 years of diagnosis without CRC having been identified. We have previously presented data from 2000–3 and partial data for 2004. Here we update this with complete data from 2004 to end-2006. All CRC cases were identified retrospectively from the Eastern Cancer Registration and Information Centre (ECRIC). For each case we identified whether they had undergone DCBE within 2 years of diagnosis and whether this was reported to show the CRC, to be technically inadequate or to be clear of CRC. In addition, we interrogated the Department of Health (DoH) website http://www.performance.doh.gov.uk/diagnostics/provider.html to ascertain the approximate proportion of patients in the UK having DCBE versus colonoscopy.
Results: 1310 CRC were recorded during the study period. DCBE had been undertaken in 215 of these patients (16%) within 2 years of diagnosis. CRC or large polyps were not identified in 53 (24%) cases, 32 in 2000–4 and 21 in 2004–6. After excluding DCBE reported as technically inadequate, 40/215 patients with CRC had undergone barium enema within 2 years reported as normal—providing an overall sensitivity of just 81.3% for the diagnosis of CRC. From our web search it is evident that 34% of symptomatic patients in the UK are still undergoing DCBE rather than colonoscopy.
Conclusion: A negative result might reflect a true negative (cancer developed between DCBE and diagnosis) or a false negative (cancer present but not visible on DCBE or visible but missed). Setting a 2-year window makes a large number of the former unlikely. The low “prior probability” of CRC might have adversely impacted sensitivity: over 8000 DCBE were done in Cambridge in the 7-year study window and patients strongly suspected of CRC were streamed for colonoscopy. A large proportion of CRC are not detected on DCBE. In the era of CRC screening, patients with established colonic symptoms should be investigated using the more sensitive modalities of colonoscopy or computed tomography colonography. Adequate capacity needs to be developed to allow this.
PT228 AN ASSOCIATION STUDY OF A MITOCHONDRIAL TUMOUR SUPPRESSOR 1 COPY NUMBER POLYMORPHISM AND COLORECTAL CANCER
1K. J. Monahan, 2S. Spain, 1H. J. W. Thomas, 2I. P. Tomlinson. 1Family Cancer Clinic, Cancer Research UK, Imperial College, London, UK, 2Molecular and Population Genetics Laboratory, Cancer Research UK, London, UK
Introduction: Mitochondrial tumour suppressor 1 (MTUS1) lies in a region of chromosome 8p deleted in approximately 50–60% of colorectal cancer. A common 162 bp insertion/deletion polymorphism includes exon 4 of this gene, and a significant association of the deletion variant with a decreased risk of both familial and high-risk familial breast cancer has been demonstrated in a recent study. This is the first case–control study of this copy number polymorphism (CNP) in colorectal cancer.
Aims and Methods: Agarose gel electrophoresis was used to differentiate genotypes among 993 colorectal cancer cases (enriched for family history) and 919 controls from the Colorectal Gene Identification (CORGI) study, with subsequent 100% confirmation of approximately 5% of genotypes by direct sequencing. Associations of genotypes with the following clinicopathological features were tested: sex; site of tumour; Duke’s stage; age of onset; presence of adenomas. Using genotype data obtained from the Hap550 platform by colleagues1 plus the genotypes at the insertion/deletion, we reconstructed haplotype blocks around the MTUS1 gene in the controls using 85 tagging single-nucleotide polymorphisms.
Results: There is no significant association of the MTUS1 deletion polymorphism with colorectal neoplasia (allelic p = 0.177, χ2; odds ratio 1.26, 95% CI 0.9 to 1.78) or with any clinicopathological variable. Two large r2 linkage disequilibrium blocks (∼77 kb and ∼105 kb) lie on either side of this copy number polymorphism, which lies at a recombination hotspot, and notably none of the Hap550 markers are in linkage disequilibrium with the CNP (r2 = 0).
Conclusion: Despite being proposed as an important tumour suppressor gene in colorectal cancer, there is no evidence of an association of a common CNP within MTUS1 and colorectal neoplasia in this study. However, similar CNP are likely to yield much interesting data in future case–control studies.
PT229 INITIAL FINDINGS OF A FIRST WAVE BOWEL CANCER SCREENING CENTRE: PROSPECTIVE AUDIT OF FIRST 18 MONTHS EXPERIENCE
M. A. P. Hughes, G. S. Duthie. Humber and Yorkshire Coast Bowel Cancer Screen Centre, Hull and East Yorkshire Hospitals NHS Trust, Cottingham, UK
Introduction: The Humber and Yorkshire Coast Bowel Cancer Screening Centre became “live” from February 2007. Participants with postive faecal occult blood tests (FOBT) were referred to the screening centre by the screening hub. We report our first 18 months findings as our participants journey through the screening programme.
Aims and Methods: To report initial findings of screening partipants who were referred to the screening centre following positive FOBT. Participants referred to the screening centre between February 2007 and August 2008 were offered an appointment within community screening clinics to discuss their FOBT finding with a bowel screening nurse specialist. During this discussion, the participant discussed and received further information with regard to the significance of the FOBT result and was offered colonoscopy to see if any significant pathology within the colon and rectum (polyps or cancer) were present. For those who were unfit for colonoscopy but fit for bowel preparation alternative tests (combined flexible sigmoidoscopy and barium enema or computed tomography (CT) colonography) were offered. Gender, age, colonoscopy findings, histology, screen episode outcomes were collected prospectively and entered into the screen centre’s database.
Results: 407 screening particpants were referred to the screening centre following a positive FOBT. 65% (265) were men and 35% (142) were women, 99% attended (n = 404). 404 were seen within the clinic and 85% (n = 337) of these wished to proceed to colonoscopy. Those who did not proceed to colonoscopy were either paused within their screening episode or could not proceed (eg, declined colonoscopy but wished recall in 2 years, under surveillance, etc). Of those who chose to proceed to colonoscopy (n = 337), 19 are currently waiting, one was undertaken within the private sector and one within the symptomatic service. 316 colonoscopies were carried out by two accredited screening colonoscopists (94% completion rate). 24% were normal, 15% had diverticular disease, 48% had polyps, 12% had cancer and 1% had irritable bowel disease. Of the 152 individuals who were found to have polyps, 17 were hyperplastic, 129 were adenomatous and six contained cancer. Of the alternative tests (flexible sigmoidoscopy and barium enema, n = 14; CT colonography, n = 11; plain CT, n = 2) 15 were normal, five had diverticular disease, four had polyps and three had cancers. One cancer was an incidental renal carcinoma picked up at CT colonography. A further four flexible sigmoidoscopies either to remove polyps or check if polyps were present were undertaken. Three large adenomas were removed and no polyp was found in the other.
Conclusion: Significant pathology (polyps and cancers) in 60% of individuals were detected within individuals who continued with the screening programme. Although still in the “prevalent” round of screening, approximately one in two individuals will have a significant finding.
PT230 IS BOWEL CANCER SCREENING ACCEPTABLE TO PATIENTS? A REVIEW OF THE 30-DAY PATIENT SATISFACTION QUESTIONNAIRE AT 18 MONTHS
1M. C. Ritchie, 1G. M. Clifford, 1N. J. Dempsey, 1B. A. Tingle, 1J. Singh, 2D. L. Nylander, 2J. E. Painter, 3C. J. Rees. 1South of Tyne Bowel Cancer Screening Centre, Queen Elizabeth Hospital, Gateshead, UK, 2South of Tyne Bowel Cancer Screening Centre, Sunderland Royal Hospital, Sunderland, UK, 3South of Tyne Bowel Cancer Screening Centre, South Tyneside District Hospital, South Shields, UK
Introduction: Participation of eligible men and women is vital to the success of the National Health Service (NHS) bowel cancer screening programme (BCSP). Patient satisfaction surveys are an effective strategy to evaluate care given and monitor patients’ perceptions. In addition they are a useful tool in identifying potential barriers to attendance.
Aims and Methods: To evaluate the experience of faecal occult blood (FOB) positive patients attending the bowel cancer screening service at the South of Tyne screening centre. A comprehensive multiple choice patient satisfaction survey is automatically generated 30 days after each completed patient episode. This excludes repeat examinations, patients diagnosed with cancer and surveillance patients discharged from screening due to age. Patients evaluate each stage of their screening experience from invitation to screening to post-colonoscopy with regard to communication and information given; privacy and dignity and comfort/sedation level when applicable.
Results: A total population of 680 000 is served and 1.6% of patients undertaking FOB tests were positive. 634 patients were assessed regarding fitness for colonoscopy. 654 procedures were performed between March 2007 and September 2008. 482 patients were sent questionnaires and 413 (86%) were returned. 99% of patients considered the invitation and pre-clinic information very/quite useful and easy to understand. All respondents were happy with the pre-assessment service and all patients were happy with the process of consent. 28% of patients reported no discomfort during the colonoscopy; 28% reported less discomfort than expected; 31% reported discomfort at a level they had expected; 12% reported more discomfort than expected and 1% did not comment. 91% of patients reported being discharged knowing the outcome of their test and only 9% of patients reported post-procedure discomfort. No patients reported being treated without privacy or dignity.
Conclusion: Examination of the 30-day patient satisfaction questionnaire demonstrates that most patients have a positive experience of bowel cancer screening. Patients are well informed regarding the procedure. The overwhelming majority of patients experienced discomfort at a level they expected or less than expected.
Abstract submitted on behalf of the Northern Region Endoscopy Group.
PT231 CAN COLONOSCOPISTS SIZE COLONIC POLYPS ACCURATELY AND DOES IT MATTER?
N. S. Anglim, E. W. Seward, A. M. Sawyerr, E. Carty. Gastroenterology, Whipps Cross University Hospital, London, UK
Introduction: Colonic polyp follow-up guidelines depend on polyp size. It is not clear from published guidelines whether follow-up should be based on estimated polyp size at the time of colonoscopy or histological assessment with the risk of polyp shrinkage during processing. Moreover, the sensitivity of computed tomography (CT) colonography for colonic polyp detection uses colonoscopy as the gold standard. We have previously reported that polyp detection mirrors adenoma detection. In our unit most polyp surveillance colonoscopy requests are made at the time of the index colonoscopy and before histological examination. We were concerned that colonoscopists may overestimate polyp size and thus request inappropriate colonoscopic follow-up.
Aims and Methods: Patients were identified using the endoscopy reporting tool. Polyps excised piecemeal or not intact at the time of histological assessment were excluded. The size of 100 colonic polyps recorded by the colonoscopists was compared with the size of the polyp recorded at histological assessment. Mann–Whitney U tests were used to compare the two sets of size data.
Results: 100 polyps from 82 colonoscopies in 79 patients were compared. For the total group of polyps, although a trend to overestimating size was seen there was no significant difference between the size assessment of the polyps by the colonoscopist and the size at histological assessment (p = 0.09, n = 100). For polyps less than 10 mm, however, colonoscopists overestimated the size of the polyps (p = 0.009, n = 82). For polyps 10 mm or larger colonoscopists and histological sizing were not significantly different (p = 0.85, n = 18). For non-bowel cancer screening (BCS) programme-trained colonoscopists there was a significant overestimating of polyp size for polyps less than 10 mm (p<0.0001, n = 56), whereas BCS programme-trained colonoscopists were more accurate assessors of size for polyps less than 10 mm (p = 0.18, n = 29).
Conclusion: Colonoscopists overestimate the size of small (<10 mm) colonic polyps. However, this may not be clinically relevant as the cut-off for the current British Society of Gastroenterology recommendations for follow-up procedures is for polyps 10 mm and larger. BCS-trained colonoscopists in our unit size small polyps more accurately than other colonoscopists. This disparity suggests that histological processing does not shrink polyp size. Using colonoscopy sizing of polyps as a gold standard for comparisons with CT colonography may not be fair unless histological measurements are used.
PT232 CACO-2 INTESTINAL EPITHELIAL CELLS ARE MORE SENSITIVE TO CLOSTRIDIUM DIFFICILE TOXIN A-INDUCED CELL DEATH THAN HT29 CELLS
N. Mullan, Y. R. Mahida. Institute of Infection, Immunity and Inflammation, University of Nottingham, Nottingham, UK
Introduction: Clostridium difficile infection is a common clinical problem in which colonic inflammation and disease is mediated by secreted toxins A and B. Intestinal epithelial cells are believed to be the first host cells that interact with luminal bacterial toxins and there is little information regarding differences between epithelial cell types in their responses to C difficile toxins.
Aims and Methods: To compare responses to C difficile toxin A by Caco-2 and HT29 human intestinal epithelial cells. Toxin A was purified by the application of supernatant samples to a thyroglobulin affinity chromatography column, followed by two sequential anion exchange chromatographic steps. Caco-2 and HT29 cells were exposed to control medium or toxin A (0.1–1000 ng/ml) for 48 h and 72 h. Mitochondrial dehydrogenase activity (MTT assay) was used to assess cell cytotoxicity in response to toxin A (expressed as optical density 570 nm). After incubation of the cells with 5000 ng/ml fluorescently labelled toxin A (followed by washing), toxin internalisation was quantified by flow cytometry and expressed as median fluorescence intensity (MFI). Data are expressed as mean (SEM).
Results: Exposure to toxin A led to concentration-dependent cell rounding in both cell types. MTT assays showed that, in contrast to HT29 cells, a significant loss of mitochondrial dehydrogenase activity occurred in Caco-2 cells exposed to 100 and 1000 ng/ml toxin A over 48 h and 72 h (see table). Studies using trypan blue confirmed loss of cell viability in toxin A-exposed Caco-2 cells, but not HT29 cells. Analysis of propidium iodide-labelled cells by flow cytometry showed an increase in events in the hypodiploid/sub-G1 region of the cell cycle in toxin A-exposed Caco-2 cells, confirming cell death by apoptosis. After exposure to fluorescently labelled toxin A, there was a time-dependent increase in cell-associated fluorescence in Caco-2 and HT29 cells. However, there were no significant differences between Caco-2 and HT29 cells in cell-associated fluorescence after 5 h incubation (MFI 75.0 (21.0) vs 71.3 (6.7)) or 24 h incubation (MFI 259.0 (6.9) vs 332.7 (30.4)) with the fluorescently labelled toxin A.
Conclusion: In contrast to Caco-2 cells, HT29 epithelial cells are resistant to toxin A-induced cell death. Both Caco-2 and HT29 cells have similar capacity to internalise toxin A, implying that the difference between the two cell types in susceptibility to cell death is due to disparity in intracellular effects of the toxin.
PT233 FAECAL INCONTINENCE IN SYSTEMIC SCLEROSIS IS RELATED TO SPHINCTER ATROPHY AND REFLEX DYSFUNCTION
1N. M. Thoua, 1M. Abdel-Halim, 2C. Denton, 1A. V. Emmanuel. 1Gastrointestinal Physiology Unit, University College Hospital, London, UK, 2Rheumatology Department, Royal Free Hospital, London, UK
Introduction: Systemic sclerosis (SSc) is a chronic multisystem autoimmune disorder with the gastrointestinal tract being affected in up to 90% of patients. The pathogenesis of gastrointestinal abnormalities may be both myogenic and neurogenic. Anorectal involvement occurs in up to 50% of patients, but to date studies have not shown correlation between manometric findings and clinical symptoms.
Aims and Methods: 21 consecutive SSc patients with faecal incontinence referred to a tertiary referral centre (18 women, mean age 58 years, mean disease duration 13 years) and 21 incontinent controls (IC; 19 women, mean age 56 years), matched for sex, age and parity, were assessed. They underwent anorectal manometry, endoanal ultrasound, rectal compliance (barostat) and rectoanal inhibitory reflex assessment.
Results: (Mean and 95% CI). Manometry: Resting anal pressure was not significantly different between the two groups (SSc 52 (40 to 63) vs IC 37 (28 to 47) cmH2O, p = NS), but maximal squeeze pressure was greater in the SSc group (SSc 120 (97 to 143) vs IC 58 (38 to 78) cmH2O, p<0.001). Endoanal ultrasound: 15 of the SSc patients had internal anal sphincter (IAS) atrophy (six severe, nine mild), compared with one of the controls. There was external anal sphincter atrophy in seven (one severe, six mild) SSc patients and two controls (both mild). In contrast, five incontinent controls but none of the SSc patients had external anal sphincter (EAS) and IAS defects. Rectal compliance was lower in the SSc patients (SSc 10.5 (8.4 to 12.6) vs IC 14.3 (11.9 to 16.7), p<0.03). Sensation: Threshold, urge and maximal tolerated volumes to balloon distension were all significantly lower in the SSc patients. Anal and rectal sensory thresholds to electrical stimulation were not significantly different. Rectoanal inhibitory reflex (RAIR): seven SSc patients, five with IAS atrophy, had an absent RAIR compared with only one of the controls. Latency and duration components of the RAIR were prolonged in SSc (see table).
Conclusion: There is both IAS and EAS atrophy in some SSc incontinent patients, which influences reflex anal function more than just pressures. This reflex dysfunction is contributed to by sensory dysfunction and reduced rectal compliance as a result of rectal infiltration. Future studies investigating SSc patients without anorectal symptoms may identify early changes.
PT234 HELMINTHS: A SIGNIFICANT BURDEN OF UNDIAGNOSED DISEASE AMONG MIGRANTS IN A GASTROENTEROLOGY CLINIC?
1P. J. Smith, 1B. Theis, 1S. McCartney, 2M. Brown. 1Department of Gastroenterology, University College Hospital, London, UK, 2Department of Infectious Diseases, Hospital for Tropical Diseases, London, UK
Introduction: Helminths are a common cause of gastrointestinal pathology and may be fatal if undiagnosed. Some infections persist for decades after migration from endemic countries and may present to secondary care with a range of non-specific gastrointestinal manifestations. Preliminary data from our clinic revealed that peripheral, rather than tissue, eosinophilia was a predictor of helminthiasis. Studies suggest that more than 50% of migrants with peripheral eosinophilia harbour helminths. We performed a complete audit of eosinophilia, ethnicity and parasitological investigations in a general gastroenterology clinic.
Aims and Methods: Initially a retrospective audit explored the relevance of eosinophilia as a marker of helminthiasis. Data on ethnicity, eosinophil count and parasitological investigations were recorded for all new attenders over a 12-month period. Ethnicity was used as the best available proxy for migrant status. With the results of this audit, clinic staff were trained in appropriate diagnosis and an evidence-based diagnostic protocol was instituted. We prospectively audited parasitological investigation among migrants with eosinophilia attending general and irritable bowel disease clinics over the following 4 months. Patients missing relevant investigations were invited to re-attend.
Results: Eosinophilia was identified in 34/426 patients (8.8%). 10 (37%) patients with eosinophilia were African or Asian, whereas only 19% of patients overall were from these ethnic groups. No patients were appropriately investigated for helminths. Following the introduction of a diagnostic protocol, 38 patients of Afro-Caribbean or Asian ethnicity, with eosinophilia, attended in the subsequent 4 months. 11 had inflammatory bowel disease and 27 patients had a variety of gastrointestinal symptoms. Patients came from various ethnic backgrounds, most commonly African (29%), Bangladeshi (29%) and Indian (18%). Parasitological tests were performed in 11 (29%) patients, in whom helminths were diagnosed in over 50% (three with strongyloides, two with schistosomiasis and one with trichuris). Appropriate screening per protocol was performed in less than 10%. We expect to diagnose additional infections after the re-attendance of patients recalled for investigations not requested at their clinic visits.
Conclusion: Raised eosinophil counts are found infrequently in the gastrointestinal clinic but are overrepresented among patients from countries where helminth infections are endemic. Investigations to exclude important infections, eg, strongyloides and schistosomiasis, which are common in these patients and may explain their presenting symptoms, were rarely performed in our clinic. A prospective audit of an evidence-based protocol for appropriate investigation demonstrated a high prevalence of clinically important gastrointestinal helminth infections.
PT235 EARLY EXPERIENCE OF COLON CAPSULE ENDOSCOPY IN ROUTINE CLINICAL PRACTICE
R. Sidhu, K. Drew, D. S. Sanders, M. E. McAlindon. Gastroenterology, Royal Hallamshire Hospital, Sheffield, UK
Introduction: The diagnostic capabilities of colon capsule endoscopy potentially adds to existing endoscopic and radiological modalities although comparative clinical trial data are sparse. Effective bowel preparation is essential as cleansing cannot take place during the procedure, although its remote, non-invasive nature makes it attractive to both patients and physicians.
Aims and Methods: This study evaluates colon capsule endoscopy in routine clinical practice and the bowel preparation regimen used. Alternative imaging modalities were discussed with all patients. Patients took clear liquids only on the day before the procedure. They drank 1.5 l moviprep (Norgine) on the evening before and 0.5 l on the morning of the procedure (09:00 hours), followed by 20 mg domperidone (10:45 hours) before swallowing the capsule (11:00 hours). The patient had 45 ml Fleet phospho-soda (DeWitt) at 13:00 hours and 30 ml (each time with 1 l water) at 17:00 hours, a light snack at 18:00 hours, a 10 mg bisacodyl suppository at 19:30 hours and was allowed home at 21:00 hours. A bowel cleanliness score was assigned during video reading (1, excellent; 2, good; 3, fair; 4, poor). Findings were arbitrarily categorised as to whether they changed management, helped in guiding management or were not helpful.
Results: Patients had either refused (n = 3) or undergone unsuccessful (n = 6) colonoscopy. Eight patients were women, aged 43 years (±6), the capsule spent 90 minutes (±30) in the small bowel and 248 minutes (±62) in the colon. Ileum was seen in all and complete colon examination was achieved in seven (78%) patients. Cleanliness scores were 2 (n = 6), 3 (n = 2) and 4 (n = 1). Indications included: symptoms plus abnormal blood parameters or histology (n = 3); symptoms alone (n = 2); symptoms plus Crohn’s disease family history (n = 1); assessment of known Crohn’s disease (n = 1); symptoms plus previous colonic polyps (n = 1) and asymptomatic polyp surveillance (n = 1). Findings included: polyps (n = 3); diverticulosis (n = 3); non-steroidal anti-inflammatory drug colopathy (n = 1); Crohn’s disease (n = 1); minor extracolonic findings (n = 2); no (n = 2) and more than one pathology (n = 3). The patient with active Crohn’s disease was treated with adalimumab; findings in six patients were considered helpful and one patient had no clear benefit.
Conclusion: Colon capsule endoscopy may be helpful in patients who refuse or undergo unsuccessful colonoscopy, although comparative trials with other modalities are needed. If so, further optimisation of bowel preparation regimens is needed as a third of patients using this protocol had fair or poor results. Over two-thirds (n = 7) of this small cohort underwent the examination primarily to exclude active Crohn’s disease; as the ileum and right ascending colon was viewed in all cases, this might prove a valuable role for this modality in the future.
PT236 INVESTIGATION OF INTESTINAL EPITHELIAL STEM CELL FUNCTION UNDER BASAL CONDITIONS AND FOLLOWING IRRADIATION
R. Gândara, C. Potten, Y. R. Mahida. Institute of Infection, Immunity and Inflammation, University of Nottingham, Nottingham, UK
Introduction: Epithelial stem cells located in small and large intestinal crypts divide continuously to give rise to progeny that differentiate to perform specific functions in the gut. The stem cells are highly sensitive to radiation-induced cell death and during recovery post-irradiation generation of new stem cells and their proliferative function can be investigated using a synthetic analogue of thymidine (bromodeoxyuridine; BrdU) that is incorporated in newly synthesised DNA.
Aims and Methods: To investigate epithelial stem cell proliferation in the small and large intestine of control and irradiated mice. Crypt size and epithelial cell proliferation in unirradiated and irradiated BDF1 mice was studied 40 minutes after parenteral BrdU. Following 12 Gy gamma-irradiation, samples (from the ileum, ascending colon (AC), mid-colon (MC) and descending colon (DC)) were collected after 6 h and 2, 4, 8 and 12 days. Nuclear uptake of BrdU was assessed in tissue sections by immunohistochemistry. Apoptotic cells were identified by morphology. Using the Score and Wincrypts program, cells were assigned a cell position (cp) along the crypt-villus (ileum) and crypt-surface (colon) axis (cell number increasing sequentially from cp 1 at the centre of crypt base). At least 50 good longitudinally sectioned half crypts were scored per mouse. The percentage of BrdU-labelled (or apoptotic) cells at a particular cell position is expressed as the labelling index (LI). Area under the curve (AUC) from LI graph was used to reflect the total number of proliferating cells.
Results: Basal conditions: compared with MC (mean 23.9 (SEM 4.7) cells) and DC (26.9 (8.2)), crypt size was smallest in AC (13.4 (2.4); p<0.04). The total number of proliferating cells was significantly (p<0.003; n = 7) lower in AC, compared with other regions (see table). At crypt base (cp 1–3), which is the putative stem cell position, LI in AC was significantly lower than in MC (p = 0.009) and DC (p = 0.041). After irradiation, apoptosis was most prominent in cp 1–6 in the ileum and AC and in cp 1 in MC and DC. In all regions post-irradiation, total epithelial proliferation was 1.5–4-fold higher than controls at days 4–12, when an increase in crypt size was also prominent.
Conclusion: Basal cell proliferation is significantly lower in AC, compared with other regions of the colon. Distribution profiles of proliferating cells and apoptotic cells (post-irradiation) in AC show some similarities to those in the ileum. Post-irradiation, the dynamic pattern of cell proliferation and change in crypt size is similar in all regions.
PT237 HOW ALERT ARE WE IN DETECTING MICROSCOPIC COLITIS?
S. K. Butt, H. Defoe, N. van Someren, K. Besherdas. Gastroenterology, Chase Farm Hospital, Middlesex, UK
Introduction: Microscopic colitis is diagnosed when a patient with chronic watery non-bloody diarrhoea has an endoscopically or radiographically normal colon but colonic biopsies show unique inflammatory changes. As the mucosa is not ulcerated or otherwise disrupted, the diarrhoea generally does not contain blood or pus. The true incidence is not known, although the disease has been increasingly diagnosed over the past 20 years. The incidence of microscopic colitis has increased significantly from 1.1 per 100 000 persons in the late 1980s to 19.6 per 100 000 persons by the end of 2001. The key in detecting microscopic colitis is obtaining biopsies from a macroscopically normal colon. It is recommended that biopsies should be taken from the rectosigmoid and from the right side of the colon. But how good are we at detecting microscopic colitis in clinical practice?
Aims and Methods: To assess the frequency of colonic biopsy obtained in patients with non-bloody diarrhoea who have a normal macroscopic appearance at colonoscopy. This was a single centre, retrospective analysis of patients with diarrhoea attending for lower gastrointestinal endoscopy. Patient details were obtained from the Unisoft endoscopy database. Patients who had a normal colonoscopy were assessed to see if colonic biopsies were obtained.
Results: A total of 398 colonoscopies was undertaken for the indication of chronic non-bloody diarrhoea between October 2005 and October 2008 by both medical and surgical endoscopists. 208 (52%) colonoscopies were deemed to be normal macroscopically. Of these normal colonoscopies, 137 (66%) were biopsied by the endoscopist for further investigation, 130 (95%) were biopsied by a gastroenterologist, the remainder being done by a surgeon. A total of 71 (34%) patients was not biopsied, of which 32 (45%) were endoscopies completed by surgeons and 39 (55%) were completed by physicians.
Conclusion: This study demonstrates that in a third of patients with diarrhoea (who have a macroscopically normal colon) biopsies are not obtained to look for microscopic colitis. When biopsies are obtained, it tends to be the physician endoscopist rather than the surgical endoscopist who performs them. The diagnosis of microscopic colitis may be more prevalent in clinical practice and should be investigated. All clinicians should have a higher index of suspicion for this and therefore colonic biopsies should be obtained in all patients with diarrhoea who have a macroscopically normal colonoscopy.
PT238 HOW ACCURATE IS AN ENDOSCOPIST’S HUNCH FOR CANCER? CORRELATION WITH HISTOLOGY
1S. K. Butt, 1K. Jaggs, 2S. Warren, 2D. Francis, 2M. Ward, 2M. Klein, 1N. van Someren, 1K. Besherdas. 1Gastroenterology, Chase Farm Hospital, Middlesex, UK, 2Surgery, Chase Farm Hospital, Middlesex, UK
Introduction: The cancer plan in the UK states that the government believes the ultimate goal in the treatment of cancer should be to “offer patients a maximum one month wait from an urgent referral for suspected cancer to the beginning of treatment”. When patients are required to wait longer, this should be because of the needs of the diagnostic process or their personal choice and not because of any inbuilt delay in the system of care. Any reduction in the time taken between obtaining a diagnosis and staging of colorectal cancer is helpful. One such step is the interval between endoscopy and histological confirmation before arranging further imaging (ie, staging computed tomography (CT)/magnetic resonance imaging (MRI)). If endoscopic diagnosis has a strong correlation with histology in the diagnosis of cancer then arranging CT/MRI scans in the staging process in cancer management could narrow the time from diagnosis to treatment.
Aims and Methods: To assess the accuracy of the endoscopist’s impression of a malignant lesion in the colon and rectum with histology. A retrospective single centre study looking at consecutive patients from July 2005 to April 2008 with an endoscopic report of “colorectal cancer” was undertaken. Patients with a potential cancer diagnosis at endoscopy were identified from the Unisoft endoscopy reporting software. The histology of these patients was obtained from the “Powerchart” hospital database of histology and from the colorectal cancer multidisciplinary meeting records. The percentage of patients with histologically confirmed cancer in comparison with endoscopic findings was evaluated.
Results: Records show that 166 patients were diagnosed with a malignant-looking colonic lesion at the time of colonoscopy. In 141 of these, histology was obtained. Following from this, 131 (93%) histologies confirmed malignancy (130 with adenocarcinoma of the colon, one with metastatic carcinoma). In the 10 patients with malignant-looking lesions but negative histology, three had severe dysplasia, one had moderate dysplasia, one had a normal biopsy with liver metastases, four had inflammatory polyps and one was normal.
Conclusion: The majority (93%) of patients thought to have a malignant lesion at endoscopy was confirmed to be so histologically. Arrangements to stage colorectal lesions thought to be malignant at endoscopy should therefore be made following endoscopy rather than waiting until histology is available. This would save valuable time in the diagnosis to treatment pathway in patients suspected of having colorectal cancer.
PT239 CONSTIPATION AND EXPOSURE TO STRESSFUL LIFE EVENTS IN 10–16 YEAR OLDS: A SRI LANKAN EXPERIENCE
1S. Rajindrajith, 2N. M. Devanarayana. 1Paediatrics, Faculty of Medicine, University of Kelaniya, Ragama, Sri Lanka, 2Physiology, Faculty of Medicine, University of Kelaniya, Ragama, Sri Lanka
Introduction: Constipation is a common paediatric problem, but little is known regarding its aetiology. The majority have functional constipation. Emotional stress is considered to be associated with functional gastrointestinal diseases including constipation.
Aims and Methods: The aim of this study was to assess the association between constipation and exposure to stressful life events in Sri Lankan school children and adolescents. A validated, self-administered questionnaire was distributed to randomly selected children, aged 10–16 years, in five randomly selected schools, in three geographically and socioeconomically different provinces in Sri Lanka. Constipation was defined using Rome III criteria.
Results: A total of 2770 questionnaires was distributed and 2699 (97.4%) were included in the analysis (1368 (50.6%) males, mean age 13.17 years, SD 1.72 years). According to Rome III criteria 416 (15.4%) had constipation and they were compared with 2278 children without defaecation disorders (eg, constipation, diarrhoea, functional faecal retention, non-retentive faecal soiling, etc). The prevalence of constipation was higher in those who were exposed to at least one stressful life event during the previous 3 months (odds ratio (OR) 0.38, p<0.0001). During univariate analysis the stressful life events associated with constipation were change in school or address, corporal punishment in school, separation from their best friend, preparation for government exams, exam failure, being bullied at school, sibling birth, severe illness or death in a family member, loss of job by a parent, separation or divorce of parents, parent remarriage to a step-parent, hospitalisation of the child himself/herself for other illness, frequent punishment by parents, father’s alcoholism, domestic fights and living in an area affected by ongoing separatist war (p<0.005). During multiple logistic regression analysis, separation from the best friend (adjusted OR 0.737, p = 0.016), severe illness in a family member (adjusted OR 0.588, p = 0.001), loss of job by a parent (adjusted OR 0.55, p = 0.017), frequent punishment by parents (adjusted OR 0.581, p = 0.005) and living in a war-affected area (adjusted OR 0.666, p = 0.0001) remained to be significantly associated with constipation.
Conclusion: Childhood constipation was significantly higher in those exposed to stressful life events. Modulation of gut motility through the brain–gut axis probably delays colonic transit causing constipation.
PT240 MAINTENANCE ANTIBIOTIC THERAPY FOR CHRONIC POUCHITIS, COMPLICATIONS AND CLINICAL OUTCOME
1S. D. McLaughlin, 2S. K. Clark, 3S. Shafi, 4P. P. Tekkis, 5P. J. Ciclitira, 4R. Nicholls. 1Gastroenterology, St Mark’s Hospital, London, UK, 2Surgery, St Mark’s Hospital, London, UK, 3Microbiology, St Mark’s Hospital, London, UK, 4Biosurgery and Surgical Technology, Imperial College, London, UK, 5Nutritional Sciences, King’s College, London, UK
Introduction: Approximately 5% of restorative proctocolectomy patients have chronic pouchitis. British Society of Gastroenterology guidelines recommend maintenance therapy with antibiotics or the probiotic VSL#3.1 Many patients do not achieve endoscopic remission after antibiotics. VSL#3 has been shown to be effective in those who achieve clinical and endoscopic remission after antibiotic treatment but further experience has been disappointing, with less than 20% of patients able to maintain remission.2 Therefore, many patients with chronic pouchitis require antibiotic maintenance therapy.
Aims and Methods: We report our experience with maintenance antibiotic treatment. Patients treated with antibiotic maintenance therapy were identified from the hospital pouch database. Data including stool testing, functional outcome, side effects and Cleveland global quality of life score (CGQoL) were analysed.
Results: 24 patients (16 (67%) men) treated for a mean of 15.7 months were identified. Seven (29%) had previously failed treatment with VSL#3 and 11 (46%) did not enter endoscopic remission and therefore were ineligible for this treatment. At follow-up the mean 24-h stool frequency was seven (range 4–11), the mean clinical pouchitis disease activity index was 0 (range 0–1) and CQGoL score was 0.7 (range 0.5–1.0). Side effects included vaginal thrush (n = 1) and occasional nausea (n = 1). All patients reported improved quality of life after starting maintenance treatment. Six (25%) patients developed antibiotic resistance during follow-up but treatment with rotating antibiotics was successful in all cases. No patient developed Clostridium difficile infection.
Conclusion: Antibiotic maintenance therapy is safe, well tolerated and efficacious even in those who fail or are eligible for VSL#3. It results in improved quality of life and function. Antibiotic resistance can be managed with rotating antibiotics.
PT241 QUALITY OF LIFE AND FUNCTIONAL OUTCOME IN PATIENTS USING A MEDINA CATHETER FOLLOWING RESTORATIVE PROCTOCOLECTOMY
1S. D. McLaughlin, 2S. K. Clark, 2Z. L. Perry-Woodford, 3P. P. Tekkis, 4P. J. Ciclitira, 3R. Nicholls. 1Gastroenterology, St Mark’s Hospital, London, UK, 2Surgery, St Mark’s Hospital, London, UK, 3Biosurgery and Surgical Technology, Imperial College, London, UK, 4Nutritional Sciences, King’s College, London, UK
Introduction: Intubation of the pouch is required by some patients with failure of spontaneous defaecation after restorative proctocolectomy (RPC). We assessed function, social, work and dietary restrictions, and quality of life (QoL) in patients who were using a Medina catheter to evacuate. The Cleveland global quality of life score (CGQoL) has been reported to be 0.8 in the global RPC population.1
Aims and Methods: 31 RPC patients prescribed a Medina catheter were identified from the pouch database and were sent a questionnaire by post. CGQoL and data on function, social, work and dietary restrictions were recorded.
Results: 23 (74%) of 31 patients (median age 56 years; 15 men (68%)) returned the questionnaire. Pouch configurations were: J:8, W:10, S:5. The median duration of catheter usage was 9 (0.5–30) years. 22 (71%) patients reported improved QoL after starting regular intubation. Median 24-h bowel frequency was 4 (range 2–14). 16 (48%) patients used the catheter for every defaecation, eight (26%) experienced social or work-life restriction, seven (22%) reported catheter blockage and 12 (52%) reported dietary restriction. The median CGQoL score was 0.72.
Conclusion: Medina catheter usage is tolerated in the long term and is associated with satisfactory quality of life of RPC patients with outflow obstruction. Frequency of defaecation and CGQoL scores are comparable with the global RPC population.
PT242 HAS THE INTRODUCTION OF THE BOWEL CANCER SCREENING PROGRAMME LED TO AN EARLY CHANGE IN THE STAGE OF COLORECTAL CANCER AT DIAGNOSIS?
1T. J. W. Lee, 2C. Zwart, 2C. Rees, 1M. Rutter. 1Gastroenterology, University Hospital of North Tees, Stockton upon Tees, UK, 2Gastroenterology, South Tyneside General Hospital, South Tyneside, UK
Introduction: Colorectal cancer usually presents once the patient is symptomatic, as a result it tends to present at an advanced stage (Duke’s stage at diagnosis: A or B 46%, C or D 54%).1 Pilot studies of the bowel cancer screening programme (BCSP) showed a reduction in the stage of cancer at diagnosis in the screening population (Duke’s stage at diagnosis: A or B 71.8%, C or D 28.2%).2 The BCSP was rolled out in our region in February 2007.
Aims and Methods: This abstract examines whether the introduction of the BCSP has had an immediate impact on the stage of colorectal cancer at diagnosis in screening and non-screening populations. Data relating to BCSP patients were obtained from the Tees BCSP database. Data on non-BCSP patients was obtained from local cancer network databases. Two one-year periods were examined: April 2006 to March 2007 and April 2007 to March 2008, the second period being after the introduction of the BCSP across the region.
Results: The table shows the number of cancers and their characteristics for each time period.
Conclusion: A higher proportion of Duke’s A or B cancers are diagnosed in the BCSP population. Our results are in keeping with previously published data from a bowel cancer screening pilot study.2 Seven of the 22 cancers diagnosed in the BCSP group were polyp cancers. These have been included in the Duke’s A group. The median age at the start of treatment is lower in the second non-BCSP group. It is possible that this reflects earlier presentation due to increased public awareness of the symptoms of colorectal cancer as a result of the publicity generated by the BCSP. No other trends in the characteristics of bowel cancers diagnosed outside the BCSP are observed at this point. We plan to repeat this study annually to see if any trends emerge.
Abstract submitted on behalf of the Northern Region Endoscopy Group.
Inflammatory bowel disease posters
PT243 SCREENING OF ASYMPTOMATIC COLITIC PATIENTS
L. Clark. Gastroenterology, Stobhill Hospital, Glasgow, UK
Introduction: Patients with colitis are more likely to develop colonic malignancy than the general population.1 This risk increases by 0.5–1% yearly, 8–10 years after disease onset.2 Other risk factors include development of the disease at a young age, extensive colitis and worse inflammation.2 The presence of concurrent primary sclerosing cholangitis (PSC) further raises this risk.3
Aims and Methods: This audit was performed in the Southern General Hospital from September 2004 to August 2007 and audited if the current British Society of Gastroenterology (BSG) guidelines for the screening of patients with inflammatory bowel disease (IBD) were being followed. 764 patients with IBD were identified by clinical coding. Every sixth patient was selected, resulting in 127 patients, 24 were excluded (12 had full colectomies before the audit period, four did not have IBD, two were lost to follow-up and six were deceased), resulting in 103 patients being included. Their medical records were reviewed to see if they had colonoscopies and biopsies performed in line with BSG guidelines.
Results: Of the 103 patients audited, 34 did not require surveillance colonoscopy during the audit period, leaving 69 patients. This audit found that only 27 of the 69 patients (39%) had colonoscopies and biopsies performed to the standard recommended by the guidelines. 39 of the 69 patients (57%) had appropriately timed colonoscopies performed; however, biopsies were not taken as recommended. Dysplasia or malignancy was identified in four patients, (1597 patient-years); however, one patient was outwith protocol and adenocarcinoma was identified at colonoscopy when he became symptomatic. According to guidelines he should have had yearly colonoscopies; however, his last scope was 4 years before. These findings about the prevalence of dysplasia and colonic cancer among colitics support the published data, that it has a higher incidence in those with more extensive colitis, who have had the disease for longer and a higher incidence in those with concurrent PSC. (Low-grade dysplasia found in two patients with pancolitis, one of which had adenocarcinoma at operation, and high-grade dysplasia and adenocarcinoma found in two patients with IBD and PSC.)
Conclusion: Only 27 of the 69 patients (39%) were following the recommendations of the BSG for the screening of colitics. Therefore we need to make sure that the clinicians treating these patients follow the guidelines, to improve the early detection of cancer.
PT244 REPLICATION AND META-ANALYSIS OF THE IL23R AND ATG16L1 VARIANTS IN CROHN’S DISEASE
1L. Cotterill, 2D. Payne, 3S. Levinson, 3J. McLaughlin, 4E. Wesley, 4M. Feeney, 4H. Durbin, 5S. Lal, 6A. Makin, 6S. Campbell, 7S. A. Roberts, 3C. O’Neill, 4C. Edwards, 1W. G. Newman. 1Department of Medical Genetics, St Mary’s Hospital, University of Manchester, Manchester, UK, 2Centre for Integrated Genomic Medical Research (CIGMR), Manchester, UK, 3Department of Gastrointestinal Sciences, University of Manchester, Manchester, UK, 4Gastroenterology Unit, Torbay Hospital, Torbay, UK, 5Gastroenterology Unit, University Hospital Aintree, Liverpool, UK, 6Department of Gastroenterology, Manchester Royal Infirmary, Manchester, UK, 7Health Research Methodology Group, University of Manchester, Manchester, UK
Introduction: An increased risk of Crohn’s disease (CD) has been associated with variants in the IL23R and the autophagy-related 16-like 1 (ATG16L1) genes. An independent case–control association study was used to replicate this finding and a comprehensive meta-analysis was carried out to determine the true effect size of these variants with CD.
Aims and Methods: 500 inflammatory bowel disease (IBD) cases and 877 ethnically matched controls for the disease were genotyped for the known CD variants in the IL23R and ATG16L1 variants (rs11209026 and rs2241880, respectively). A comprehensive meta-analysis was performed on over 10 000 cases and 13 500 controls for each of the IL23R and ATG16L1 variants with CD. All studies used were independent published data.
Results: Both susceptibility variants showed highly significant associations in our white British cohort, including IL23R (rs11209026, p = 0.0006) and ATG16L1 (rs2241880, p = 0.0017). An association was found between ATG16L1 and CD in CARD15+ individuals (p = 0.0008), and an IL23R association with CD was identified with CARD15− individuals (p = 0.0009). The random effects model used in the meta-analysis showed similar combined effects for rs11209026 (odds ratio (OR) 0.42, 95% CI 0.37 to 0.47) and rs2241880 (OR 1.34, 95% CI 1.29 to 1.40) to that found in our cohort.
Conclusion: There is strong evidence in our case–control study and meta-analysis that both IL23R and ATG16L1 polymorphisms (and the CARD15 variants) are involved in CD susceptibility.
PT245 INFLIXIMAB IN CROHN’S DISEASE: LONG-TERM DURABILITY EXPERIENCE
1M. J. Dibb, 1K. Kemp, 2C. Johnson, 2A. Watson, 1A. Makin, 1S. Campbell. 1Gastroenterology, Manchester Royal Infirmary, Manchester, UK, 2General Surgery, Manchester Royal Infirmary, Manchester, UK
Introduction: Infliximab, a chimeric monoclonal antibody, has demonstrated its efficacy to induce and maintain remission in Crohn’s disease (CD) (ACCENT I/II). Long-term durability data beyond 54 weeks is needed with the use of infliximab in clinical practice, to help refine therapy further and obtain optimal long-term response.
Aims and Methods: We created a database of 106 CD patients treated with infliximab between October 1999 and October 2008 (9 years). Data collected included demographics, adverse events, time to loss of response, concomitant immunosuppressive therapy, smoking status, disease anatomy/type. Remission was defined by standard clinical parameters. Loss of response to infliximab was defined as the need for a reduction in the dose interval or increased dosage required to recapture a response. Kaplan–Meier survival analysis was used to compare time to loss of response of infliximab. Subgroups were compared using the log rank test. Statistical analysis was performed using XLStat with significance taken at p⩽0.05.
Results: A total of 106 patients (60 women and 46 men, median age 39 years (17–79)) was included. Disease anatomy: 40 (37.7%) patients ileum, 26 (24.5%) colonic, 33 (31.3%) ileocolonic and seven (6.6%) upper gastrointestinal tract. 51 (48.1%) patients had perianal involvement. Patients received induction infliximab at 0, 2 and 6 weeks. 20 (18.9%) patients stopped infliximab at induction due to side effects, lack of response or surgery. 14 patients (13.2%) were treated on an episodic basis, whereas the remainder received scheduled infliximab. The mean duration of infliximab was 19.7 months (2–93). 51 patients received 8-weekly doses, whereas 21 patients were maintained on 12-weekly doses. There was no difference in loss of response between 8 or 12-week maintenance (p = NS). 16% of initial responders to infliximab were in remission at 8 years follow-up. 18% of perianal patients were in remission at 5 years versus 44% of patients without perianal disease (p = 0.056). Non-smokers had a response of 58.7% at 5 years versus 31.6% of smokers. Ex-smokers performed poorly, with no responders beyond 5 years. This was significant (p = 0.007). There were no significant differences in durability between disease distribution and age groups. 10 (9.4%) patients had an allergic reaction to infliximab. Four (3.7%) patients developed infections (pneumonia, Epstein–Barr virus, cellulitis and tuberculosis) that required infliximab cessation. Two patients developed dyspnoea, which led to infliximab withdrawal. Treatment was stopped due to the onset of depression in one patient. Two patients in the study have died of causes unrelated to infliximab treatment.
Conclusion: These data confirm published short/medium-term durability data and suggest that only 16% of patients remain in remission at 8 years following infliximab. Patients with perianal disease and smokers have worse long-term outcomes to infliximab maintenance treatment. Episodic treatment does not appear to be inferior to scheduled therapy. As the majority of patients were on concomitant immunomodulators, the effects of this on durability could not be assessed.
PT246 A PHARMACOGENETIC INDEX TO PREDICT NON-RESPONSE TO THIOPURINES IN INFLAMMATORY BOWEL DISEASE
1J. D. Sanderson, 1M. Smith, 2B. Baburajan, 3A. Ansari, 4C. Lewis, 5T. Marinaki, 5M. Arenas-Hernandez. 1Gastroenterology, Guys and St Thomas NHS Trust, London, UK, 2Nutritional Sciences Research, Kings College London, UK, 3Gastroenterology, Chelsea and Westminster Hospital, London, UK, 4Molecular Genetics, Kings College London, London, UK, 5Puriune Research, Guys and St Thomas NHS Trust, London, UK
Introduction: Azathioprine and 6-mercaptopurine (6MP) remain the immunosuppressants of choice for inflammatory bowel disease (IBD). Despite their usefulness, however, therapeutic failure occurs in 30–45%, with as much as half of this due to lack of clinical response. Identification of those resistant to thiopurines before treatment should permit the earlier use of more effective therapy. High thiopurine methyltransferase (TPMT) activity is known to be associated with biochemical resistance to thiopurines. We analysed this, together with two other newly reported markers of non-response to azathioprine to establish what proportion of non-response could now be accounted for by a combination of pharmacogenetic markers.
Aims and Methods: A cohort of 182 prospectively recruited patients starting 2 mg/kg azathioprine for IBD was divided into responders (66), non-responders (44) and those discontinuing treatment due to side effects (72). TPMT activity was measured using mass spectroscopy. The whole cohort was genotyped for the presence of the coding single-nucleotide polymorphism AOX3404A>G using a real-time PCR Taqman drug metabolism genotyping assay and confirmed in a subset by traditional sequencing. The presence of the 14 bp insertion/deletion in the HLA-G exon 8 3′-untranslated region was established using traditional gel-based PCR. Analysis of responders versus non-responders used χ2 and trend tests.
Results: All genetic markers were in Hardy–Weinburg equilibrium. Each factor was independently associated with non-response (AOX3404A>G p = 0.025; TPMT activity >35 p = 0.0005, HLA-G p = 0.002). The additive effect on clinical response of having multiple adverse predictors was highly significant: p = 1.7 × 10−6. Those with no adverse predictors had a 95% chance of responding to azathioprine, compared with 14% in those with all adverse predictors (see fig).
Conclusion: This is the first description of a pharmacogenetic index that might permit more effective individualised prescribing of thiopurines. Replication of these influences is needed in other prospective cohorts. Individuals carrying all three markers appear very unlikely to respond to conventional thiopurine prescribing strategies and have most to gain by the earlier use of alternative regimes.

Figure PT-246 Response to azathioprine
PT247 INFLIXIMAB THERAPY SIGNIFICANTLY REDUCES SUBSEQUENT INFLAMMATORY BOWEL DISEASE-RELATED COSTS IN CROHN’S DISEASE PATIENTS: A 2-YEAR FOLLOW-UP STUDY
1M. B. Sprakes, 2A. C. Ford, 1L. Warren, 1D. Greer, 1J. S. R. Jennings, 1C. F. Donnellan, 1S. M. Everett, 1J. Hamlin. 1Gastroenterology, Leeds General Infirmary, Leeds, UK, 2Gastroenterology, St James’s University Hospital, Leeds, UK
Introduction: The efficacy of infliximab for the treatment of Crohn’s disease (CD) has been well documented in placebo-controlled trials. However, despite strong evidence that scheduled (8-weekly) maintenance therapy is superior to episodic infusions in terms of disease remission, this approach was recently not endorsed by the National Institure for Health and Clinical Excellence (NICE; October 2008). There are few published data examining inflammatory bowel disease-related costs in CD patients before and after commencement of infliximab therapy.
Aims and Methods: Our sample included 59 patients with CD. We collected data on the number of outpatient visits, number of inpatient days, medication use, number and type of surgical operations (from case notes), blood tests, radiological investigations, upper and lower gastrointestinal endoscopies (from computerised records) for the 12 months before and 12 months after the commencement of infliximab. We applied NHS reference costs for 2006–7 to these data to derive a total inflammatory bowel disease-related cost per patient for these two time periods and compared these using a paired samples t test.
Results: The mean inflammatory bowel disease-related cost per patient in the 12 months before infliximab was £4848, compared with £1836 in the 12 months following the commencement of infliximab. This represents a mean cost saving per patient of £3011 (p<0.001). Highly statistically significant cost savings were made following the introduction of infliximab therapy in all areas, with the exception of subsequent surgical operations and blood tests (see table). The greatest cost savings occurred due to less time spent as a hospital inpatient. The mean cost of infliximab therapy per patient over the 12 months of follow-up was £8962 (range £1748 to £36 708).
Conclusion: Treating CD patients with infliximab leads to a £3000 reduction in inflammatory bowel disease-related costs in the first 12 months following the commencement of therapy. Savings were made in all areas of patient care, but the majority of savings accrued as a result of less time spent as an inpatient in hospital, which may also lead to an improvement in the overall quality of life for patients.
PT248 SAFETY OF MODIFIED-RELEASE ORAL MESALAZINE 4.8 G/DAY (800 MG TABLET) COMPARED WITH 2.4 G/DAY (400 MG TABLET) FOR TREATMENT OF ACTIVE ULCERATIVE COLITIS: COMBINED ANALYSIS FROM THREE RANDOMISED, DOUBLE-BLIND, ACTIVE-CONTROLLED TRIALS
1W. J. Sandborn, 2M. Spravka, 2M. Hosterman. 1Division of Gastroenterology, Hepatology and Internal Medicine, Mayo Clinic, Rochester, New York, USA, 2Pharmacovigilance, Procter and Gamble Pharmaceuticals, Cincinnati, Ohio, USA
Introduction: To evaluate the safety of a modified-release oral tablet formulation (800 mg tablet) of mesalazine dosed at 4.8 g/day, compared with that of a currently marketed 400 mg modified-release oral mesalazine tablet dosed at 2.4 g/day for the treatment of mildly to moderately active ulcerative colitis.
Aims and Methods: Data from 1459 patients from three randomised, double-blind, 6-week studies (ASCEND I, II and III) were combined to compare the safety of a new 800 mg tablet formulation of modified-release mesalazine, dosed at 4.8 g/day, to that of the marketed Asacol 400 mg tablet (US formulation), dosed at 2.4 g/day, in patients with mildly to moderately active ulcerative colitis. Safety assessments evaluated across all three studies included adverse events and baseline and exit serum creatinine.
Results: There were no clinically meaningful differences in adverse event rates between the two treatment groups. The most frequent adverse events reported were headache, nausea, nasopharyngitis, abdominal pain, exacerbation of ulcerative colitis, diarrhoea and dyspepsia. The adverse event experience was similar across the subgroups examined, including age, sex, race and baseline disease state (mildly active versus moderately active ulcerative colitis). The majority of adverse events were assessed by investigators as mild or moderate in severity and doubtfully related to the study drug. Serious adverse events were reported in six patients in the 4.8 g/day group and 13 in the 2.4 g/day group and primarily involved gastrointestinal disorders. The greater number of serious adverse events in the 2.4 g/day dosing group (22) versus the 4.8 g/day dosing group (eight) was driven largely by a greater number of patients experiencing serious exacerbation of ulcerative colitis and ulcerative colitis symptoms. The distribution of types of adverse events resulting in study withdrawal (primarily gastrointestinal symptoms associated with ulcerative colitis) was similar between treatment groups. The percentage change of serum creatinine from baseline to exit was similar for both dosing groups with no evidence of a dose-related increase (see table).
Conclusion: Overall, the adverse events with modified-release oral mesalazine 4.8 g/day (800 mg tablet) in these clinical studies were comparable to 2.4 g/day (400 mg tablet) and consistent with the post-marketing experience of the currently marketed 400 mg tablet.
PT249 IDENTIFICATION OF BIOMARKERS PREDICTING STEROID RESPONSE IN ACUTE SEVERE ULCERATIVE COLITIS USING SURFACE-ENHANCED LASER DESORPTION/IONISATION–TIME OF FLIGHT MASS SPECTROMETRY
1N. C. Hare, 2M. Imrie, 1A. J. Smith, 1K. Soo, 1L. Smith, 2R. Gray, 1G. Ho, 1I. D. Arnott, 1J. Satsangi. 1Gastrointestinal Unit, Western General Hospital, Edinburgh, UK, 2Molecular Medicine Centre, Western General Hospital, Edinburgh, UK
Introduction: During an acute severe exacerbation of ulcerative colitis (UC), approximately two-thirds of patients will respond to intravenous corticosteroid therapy, the accepted first-line therapy. Clinical scoring systems such as the Edinburgh risk assessment and the Travis criteria incorporate standard serological tests to help predict which patients will fail to respond to corticosteroid therapy and ultimately require second-line medical therapy or surgery.
Aims and Methods: To determine novel serum and faecal biomarkers that will help to predict the outcome in acute severe UC using surface-enhanced laser desorption/ionisation–time of flight (SELDI–TOF) mass spectrometry and identify markers that may ultimately provide insight into the pathogenesis of steroid resistance. Blood and faecal samples were collected from 26 patients presenting with acute severe UC (satisfying Truelove and Witts criteria) within 24 h of starting intravenous steroid therapy. Blood samples were allowed to clot for 45 minutes before sera separation. All samples were stored at −80°C, sera were denatured using 9 mol urea, 2% CHAPS, 50 mmol TrisHCl pH 9; faecal samples were preprocessed using PhiCal extraction buffer. Samples were applied to CM10 ProteinChips (cationic exchange arrays) and mass spectra were generated using a PBS-IIc mass spectrometer at laser intensity settings of 165, 185 and 210. Spectra were calibrated and preprocessed with baseline subtraction, noise adjustment and normalisation. Peak identification was performed using ProteinChip software version 3.2.1. Peaks with a p value of less than 0.05 were considered significant discriminators between steroid-responsive and unresponsive patients.
Results: 15/26 (57.7%) patients responded to steroids, 11 underwent colectomy. Five serum biomarkers that discriminated between the two patient groups were identified. All of these markers are upregulated in steroid-responsive disease. The discriminant proteins have a mass over charge ratio (m/z) of 7565 (p = 0.004), 7927 (p = 0.003), 15 115 (p = 0.027), 15 855 (p = 0.046) and 28 007 (p = 0.040), respectively. None of the biomarkers identified in faecal samples showed a significant difference between steroid-responsive and unresponsive disease.
Conclusion: This is the first study, in the setting of acute severe UC, to look for predictive biomarkers of steroid response in serum or faecal samples using SELDI–TOF mass spectrometry. We have identified five serum biomarkers that discriminate between steroid-responsive and unresponsive individuals. Further work is being undertaken to identify these proteins and, using support vector machine analysis, to establish a model to determine the significance of protein fingerprints in predicting steroid response in acute severe UC.
PT250 EFFICACY OF ENTERAL FEEDING WITH MODULEN IN ADULTS WITH CROHN’S DISEASE: A RETROSPECTIVE STUDY
N. Y. Z. Chiang, T. Haslinger, E. Richman, J. M. Rhodes, K. Leiper. Gastroenterology, Royal Liverpool University Hospital, Liverpool, UK
Introduction: Previous studies have shown that some enteral feeds are as effective as corticosteroids in inducing remission in Crohn’s disease (CD). Modulen IBD has been shown to be effective in children and adolescents with CD. However, although it is widely used in adults, there are few clinical data on remission rates and duration of response.
Aims and Methods: The aim of this study was retrospectively to study the efficacy of 3 weeks of Modulen IBD enteral feed in adults with active CD. Enteral feeding in all cases was with Modulen, flavoured with Nesquick and taken orally as the sole nutrition for 3 weeks, with subsequent weaning over 3 months to a low-fat, low-fibre diet. Inclusion criteria: case note review of consecutive CD patients with a Harvey–Bradshaw index (HBI) greater than 4 and with stable concomitant medication treated with Modulen as their sole therapeutic intervention. Data collected on baseline characteristics, duration and site of disease, weight, C-reactive protein (CRP), albumin, HBI and adherence to exclusive Modulen diet. Remission was defined as HBI of 4 or less.
Results: 33 patients fulfilled the entry criteria. The mean age was 37 years (SD 15), the median duration of disease was 5 years (range 0–49) and 30% had previous surgery. At entry, 21% were receiving corticosteroids, 60% immunosuppressives, 27% antibiotics and 52% 5-ASA. The median HBI was 7 (range 5–17). At week 3 64% (21/33) achieved remission on an intention-to-treat analysis, with a median fall in HBI of 4 (p<0.001). Seventy per cent had a CRP of 10 mg/l or greater at baseline (median 30, range 10–242), 63% of these had a CRP of less than 10 at week 3. CRP fell from a median of 30 mg/l (range 10–242) to less than 5 mg/l (range <5–73), a median fall of 11 (range −29–173; p = 0.003). There were no significant changes in weight or serum albumin. Median (range) albumin 39 g/l (23–55) week 0 and 40.5 g/l (31–49) at week 3. Median (range) weight was 61 kg (40–103) week 0 and 63 kg (41–104) week 3. Self-reported adherence rate to Modulen as a sole feed for 3 weeks was 82% at week 3. The median duration of remission was 21 weeks. However, most patients gradually weaned from 100% Modulen towards a low-fat low-fibre diet over approximately 3 months. There were no significant side effects.
Conclusion: In this open-label study, oral Modulen as the sole feed was shown to be well tolerated in adults with CD and induced remission in 64% within 3 weeks with no reported side effects other than inconvenience. Randomised studies are required to compare its efficacy and safety profile with other therapies.
PT251 NINE-YEAR EXPERIENCE OF ORAL CYCLOSPORIN (NEORAL) IN THE TREATMENT OF STEROID-REFRACTORY SEVERE ULCERATIVE COLITIS
N. R. O’Shea, O. Epstein, K. Greveson, C. Murray, C. Toumpanakis, M. Hamilton. Centre for Gastroenterology, Royal Free Hospital, London, UK
Introduction: Initial publications suggest that the use of oral cyclosporin A (CyA) to induce remission in acute ulcerative colitis (UC) is both effective and safe. It has been reported that therapeutic levels can be achieved rapidly without toxicity and problems associated with intravenous CyA. Based on these findings our unit has treated acute colitics requiring CyA with oral Neoral over a 9-year period. We present a retrospective audit of response and side effects in these patients.
Aims and Methods: The notes of patients who were treated with oral CyA for an acute exacerbation of UC requiring hospital admission were reviewed. All patients had failed to respond to intravenous hydrocortisone. Patients were commenced on 5 mg/kg in two divided doses of oral CyA; trough levels were measured. The dose was adjusted according to levels, therapeutic range 100–300 ng/ml. Response to treatment (defined as a significant reduction in C-reactive protein, bowel frequency and discontinuation of intravenous steroids), side effects and colectomy rate were reviewed.
Results: 15 patients (nine women, six men, aged 21–68 years) received oral CyA as rescue therapy for acute UC, following 2–9 days of intravenous steroids. The majority of these patients had been treated with Neoral in the past 5 years, 71% (11/15). A thiopurine was commenced before or soon after discharge, CyA was continued for no more than 3 months. Response was achieved in 87% (13/15) after 2–11 days of oral CyA therapy, one had a delayed response due to subtherapeutic levels. 13% (2/15) proceeded to surgery on initial admission. 40% (6/15) experienced minor side effects: headache, flushing, tremor, hypertension, retrosternal pain, nausea, parasthesia and hirsuitism. In all but one case the symptoms responded to dose reduction; this patient was taking ciprofloxacin, an enzyme inhibitor. There were no major side effects. The 1-year colectomy rate was 27% (4/15); one patient received only 6 days of CyA due to minor side effects. In the 9-year follow-up period 67% (10/15) avoided surgery. Two patients were restarted on CyA following a flare of symptoms more than 6 months after discharge; remission was achieved in both.
Conclusion: Our experience reflects earlier studies that suggest that oral administration is a safe and effective way of administering CyA to induce remission in acute non-steroid-responsive colitis. Neoral is well tolerated, acceptable to patients and easy to administer. Oral administration is cost effective, less time consuming and non-invasive. None of our patients developed neurotoxicity, nephrotoxicity or anaphylaxis. Given the reduced risks and ease of administration of Neoral perhaps more patients could be considered for this treatment.
PT252 IMPROVEMENT IN SHORT INFLAMMATORY BOWEL DISEASE QUESTIONNAIRE SCORES IN ADALIMUMAB-TREATED CROHN’S DISEASE PATIENTS WHO FAILED INFLIXIMAB (CHOICE TRIAL)
1S. Lichtiger, 2D. H. Present, 3E. Wu, 3N. Beaulieu, 4J. D. Kent, 5K. G. Lomax, 4J. Chao, 4P. Mulani. 1Gastroenterology, Mount Sinai Medical Center, New York, New York, USA, 2Internal Medicine, Mount Sinai Medical Center, New York, New York, USA, 3Analysis Group, Boston, Massachusetts, USA, 4Global Health Economics and Outcomes Research, Abbott Laboratories, Abbott Park, Illinois, USA, 5Global Pharmaceutical Research and Development, Abbott Laboratories, Parsippany, New Jersey, USA
Introduction: Adalimumab, a fully human monoclonal antibody targeting tumour necrosis factor, is approved in the European Union for the treatment of severe active Crohn’s disease (CD) in adults. The short inflammatory bowel disease questionnaire (SIBDQ) is a simple, validated, 10-item instrument that assesses health-related quality of life (HRQoL) in inflammatory bowel disease patients. This analysis of CHOICE assessed the impact of adalimumab on HRQoL using the SIBDQ in CD patients who had failed infliximab therapy.
Aims and Methods: CHOICE was a US-based, multicentre, open-label trial of 673 patients with moderately or severely active CD who were primary non-responders to infliximab or who had initially responded and then either lost response or became intolerant. Planned study duration was at least 8 weeks. After a minimum 8-week washout period after the last infliximab dose, patients received adalimumab induction therapy of 160/80 mg at weeks 0/2, followed by 40 mg every other week maintenance dosing. At/after 8 weeks, patients could be switched to adalimumab 40 mg a week for failure/non-response. SIBDQ scores (10–70, with higher scores indicating better HRQoL, and a 9-point change correlated with a 100-point change in the CD activity index)1 were recorded at baseline and at weeks 4, 8, 12 and 24. Paired t tests assessed changes from baseline in total SIBDQ scores.
Results: The mean age was 40.8 years, 59% were women and 91% were white. The mean baseline SIBDQ score was 37.4 points, which reflected poor HRQoL. The table displays average changes in the SIBDQ score from baseline. There was a significant improvement in scores at all scheduled visits, with greatest impact at week 24 (11.9-point mean change for all patients, p<0.001). At week 24, the mean SIBDQ score change for all patients was clinically meaningful. Two sensitivity analyses were performed, one using a subset of patients (n = 277) with complete SIBDQ data at all scheduled visits and the other with imputation for missing data. Similar results were obtained.
Conclusion: Sustained HRQoL improvements were achieved by patients with CD receiving adalimumab among both infliximab primary non-responders and intolerant/initial responders.
PT253 MYENTERIC PLEXITIS DOES NOT PREDICT ENDOSCOPIC CROHN’S DISEASE RECURRENCE 12 MONTHS FOLLOWING ILEOCOLONIC RESECTION IN DISTRICT GENERAL HOSPITAL PRACTICE
1P. A. Blaker, 1B. Nedjat-Shokouhi, 2D. M. Thomas, 1A. W. Harris. 1Department of Gastroenterology, Kent and Sussex Hospital, Kent, UK, 2Department of Histopathology, Kent and Sussex Hospital, Kent, UK
Introduction: The recurrence of Crohn’s disease (CD) after an ileal or colonic resection is extremely common. Unfortunately, there are no reliable histological markers that predict future mucosal inflammation. Recent studies from tertiary referral centres have suggested that myenteric plexitis (inflamed ganglia and nerve bundles) in the proximal resection margin of ileocolonic resection specimens may indicate ongoing pathology and thereby predict the recurrence of CD.1 2 However, the value of looking for myenteric plexitis in a district general hospital (DGH) setting is unclear.
Aims and Methods: This study has investigated the hypothesis that myenteric plexitis may predict the recurrence of CD at 12 months following an ileocolonic resection in a DGH. Ileocolonic resection specimens from 15 patients with CD (26–65 years; six men, nine women) were scored by a single observer (MDT) for the presence of inflamed ganglia and nerve bundles in the proximal resection margins. At 12 months after surgery, endoscopic recurrence of CD was determined by a single observer (AWH) in all patients using the Rutgeert’s score.3 MDT and AWH were unaware of each others’ findings.
Results: Myenteric plexitis was observed in the proximal resection margins of seven (47%) patients with CD. There was no significant difference in the endoscopic recurrence of CD (Rutgeert’s score ⩾i2) at one year (50% vs 50%; odds ratio 0.5, 95% CI 0.0352 to 7.1043; p = 0.5538) between those patients with or without myenteric plexitis.
Conclusion: In our DGH the presence of myenteric plexitis in the proximal margins of ileocolonic resection specimens was not predictive of early endoscopic CD recurrence. There are three possible reasons to account for the difference in results between our study and that of the tertiary centres: first, there may be a difference in the phenotypes of patients with CD in secondary and tertiary care; second, there was a small number of patients with a low Rutgeerts score (i0–i1, n = 3) in our study, and finally, the relatively low postoperative recurrence of CD may reflect our practice of prescribing metronidazole for 3 months and continuing treatment with thiopurines or infliximab following surgery.4
PT254 RADIATION EXPOSURE AND CANCER RISK IN PATIENTS WITH CROHN’S DISEASE
P. J. Allan, E. Langdon, L. Kent, E. Culver, A. S. McIntyre. Gastroenterology, Wycombe General Hospital, High Wycombe, UK
Introduction: Exposure to low levels of ionising radiation may increase the risk of developing cancer. The use of computed tomography pulmonary angiogram for pulmonary emboli in women may add an additional 100 breast cancers per 100 000 patients exposed. Should we be concerned for Crohn’s disease (CD) patients who often need multiple x ray investigations to diagnose and assess disease at relatively young ages?
Aims and Methods: A retrospective study of 122 CD patients under the care of one gastroenterologist studied x ray exposure over the lifetime of their disease to estimate radiation exposure. A comparison was made with a similar patient group with ulcerative colitis (UC) and national population norms. Published national average radiation exposures were used for each procedure in milliSieverts (mSv) abdominal x rays (AXR, 0.7 mSv), small bowel enemas (SBE, 3), barium enemas (BaE, 7.2), computed tomography abdomen pelvis without (CTAP, 10) and with contrast (CTAP+C, 10). Total exposure (mSv) for each patient was used to estimate the excess risk of developing cancer.
Results: The 122 CD cohort (62.3% women) had a mean diagnosis age of 32.0 years (+2.7, 95% CI) compared with the 122 UC cohort (42.0% women), 42.0 years (+2.8). Mean disease duration was CD 18.0 years (+1.9) and UC 19.0 years (+1.9). CD disease distribution was 22.5% ileal, 45.8% ileocolonic, 30.0% colonic, 1.7% perianal only and 8.3% perianal plus other site. The number of inflammatory bowel diseases diagnosed per decade: 1950s four (50% CD), 1960s 11 (46% CD), 1970s 29 (48% CD), 1980s 54 (50% CD), 1990s 99 (49% CD), 2000–4 46 (57% CD). Total investigations performed, expressed as mSv: AXR 237.3 mSv (mean effective dose per CD vs UC patient 1.14 vs 0.80; p = ns); SBE 576 mSv (4.30 vs 0.42; p<0.01); BaE 1252.8 mSv (6.08 vs 4.19; p = 0.03); CTAP 450 mSv (2.95 vs 0.74; p<0.01); CTAP+C 550 mSv (3.28 vs 1.23; p = 0.04) and the mean number of 18 magnetic resonance imaging scans performed (0.07 vs 0.07; p = ns) and 238 ultrasound abdomen (1.53 vs 0.42; p<0.01). The mean total individual radiation dose (mSv) was CD 17.75 (+3.22, 95% CI) vs UC 7.38 (+1.60) p<0.01. Mean population norm exposures are 2.2 mSv/year (range 1.5–7.5), ie, 39.6 mSv over 18 years. Increased exposure for patients with CD is thus 57.35 mSv over 18 years, an increase of 44.8% over population norms, and for UC over 19 years is 49.18 mSv, a 17.7% increase; CD has a 23.1% increase over UC. CD and UC each occurs in 60 × 103 patients in the UK and radiation exposure (10 mSv 1 : 1000–10 000 risk) related to disease management might result in 10.6–106 extra cancers in CD and 4.4–44 in UC patients.
Conclusion: CD patients are exposed to substantially more radiation than either population norms or similar UC patients. We estimate this risk to be a 23.1% increase over UC patients and 44.8% above population norms. Given practices in previous decades this may underrepresent the radiation risk. Radiation exposure should be considered and minimised when investigating CD patients.
PT255 THE ALLERGIC BASIS OF THE OROFACIAL GRANULOMATOSIS/ORAL CROHN’S DISEASE SPECTRUM
1P. Patel, 2F. Barone, 2L. Boursier, 1C. Nunes, 3E. Odell, 4M. Escudier, 5S. Challacombe, 1J. Brostoff, 2J. Spencer, 1J. Sanderson. 1Nutritional Sciences Division, King’s College London, London, UK, 2Immunobiology, King’s College London, London, UK, 3Oral Pathology, Guy’s and St Thomas’ NHS Trust, London, UK, 4Oral Medicine, Guy’s and St Thomas’ NHS Trust, London, UK, 5Oral Medicine, King’s College London, London, UK
Introduction: Orofacial granulomatosis (OFG), which includes oral Crohn’s disease, is a chronic inflammatory condition presenting characteristically with lip swelling but also affecting the gingivae, buccal mucosa, floor of the mouth and a number of other sites in the oral cavity. Although the cause remains unknown, acute bouts of swelling and frequently reported atopy suggest an allergic component. There is evidence for the involvement of dietary triggers, with objective improvement on a cinnamon and benzoate-free diet.
Aims and Methods: To investigate the role of allergy in OFG/oral Crohn’s disease.
Methods: Using immunohistochemistry and PCR on paraffin embedded (n = 44) and fresh frozen (n = 8) oral mucosal biopsies, we looked for evidence of IgE-mediated hypersensitivity in patients with OFG and compared this with non-OFG oral inflammation. We also determined the incidence of atopy in a cohort of patients with OFG and performed skin prick tests to common allergens (n = 58).
Results: Large, active, dendritic B cells in the oral mucosa were present in the inflammatory infiltrate in OFG and these were independent of follicular structures. They expressed nuclear activation-induced cytidine deaminase, an enzyme that is essential for the process of class switch recombination to IgE. These dendritic B cells also expressed surface IgE, and this expression was significantly greater in OFG compared with other oral conditions. Epsilon transcripts, which provide further evidence for IgE production locally, were also demonstrated in OFG by PCR. Clinical allergy data from history and skin prick tests revealed an incidence of allergy of 83% in the oral OFG cohort compared with a reported incidence of between 4% and 20% in the general population. The incidence of the oral allergy syndrome was 30%, significantly higher than population estimates. OFG patients aged below 30 years had a significantly higher incidence of atopy and oral allergy syndrome than patients over 30 years (93% vs 74% and 41% vs 19%, respectively).
Conclusion: Patients with oral OFG have a high incidence of atopy. In addition, we provide evidence for local class switching to IgE in the oral mucosa in OFG in the absence of follicular structures and significantly greater IgE expression on dendritic B cells in OFG than non-OFG controls. It is already known that removing certain dietary components will improve oral inflammation in OFG. These subepithelial dendritic B cells may be cellular mediators of local hypersensitivity in OFG.
PT256 AUDIT OF ANTI-TUMOUR NECROSIS FACTOR THERAPY IN CROHN’S DISEASE: BETTER RESULTS IN PATIENTS WITH NO PREVIOUS SURGERY
R. N. Patel, B. Gregg, A. Kneebone, K. P. Leiper, A. Ellis, A. J. Watson, J. M. Rhodes. Gastroenterology, Royal Liverpool and Broadgreen University Hospital Trust, Liverpool, UK
Introduction: The UK inflammatory bowel disease (IBD) audit has shown considerable variations in access to and use of infliximab in Crohn’s disease. Maintenance versus episodic treatment is also contentious.
Aims and Methods: The aim of this audit was to assess the usage and results of anti-tumour necrosis factor (TNF) therapy in Crohn’s disease in routine clinical practice in a large university hospital. The hospital currently has 460 active patients with Crohn’s disease on its register. 102 of these have received infliximab since 2002, of whom 77 have received treatment for at least 12 months and are the subject of this audit. All 77 case notes were audited.
Results: Harvey–Bradshaw (HB) scores on initiation of therapy were 8, 2–40 (median, range), and 49 (64%) patients had a score of 8 or more, ie, treated within National Institute for Health and Clinical Excellence guidance. 36 patients had ileocolonic disease, 31 colon only and 10 ileal only. 28 had enterocutaneous fistulae, of which 22 were perineal. 53% had had previous surgery, 84% were receiving concomitant immunosuppression and 32% were receiving concomitant corticosteroids. 100% had had recent chest x ray. The overall remission rates (HB ⩽4) were 48%, 39% and 43% at 3, 6 and 12 months, respectively. 47% received “maintenance” treatments, defined as six or more infusions in the first 12 months and 53% episodic (median three infusions/12 months, range one to five). Two patients developed a systemic lupus erythematosis-like syndrome. There were no drug-associated fatalities. 55% of patients who failed on infliximab went on to receive alternative anti-TNF antibody therapy. Multivariate analysis for effect on remission at 12 months of previous surgery, concomitant immunosuppression, concomitant steroids and episodic versus maintenance, confirmed previous surgery as the only significant variable (p = 0.002, odds ratio for remission 0.23 (0.09 to 0.61)) (see table).
Conclusion: Remission rates with infliximab seem substantially better in routine clinical practice than previously reported in controlled trials, possibly reflecting more rigorous patient selection. Maintenance therapy shows a non-significant trend towards better remission. Results of infliximab therapy are considerably better in patients who have not had previous surgery (61% at 12 months) compared with those with previous surgery (27% at 12 months).
PT257 TELOMERE ATTRITION IN NON-DYSPLASTIC COLORECTAL MUCOSA OF PATIENTS WITH ULCERATIVE COLITIS
1R. P. Arasaradnam, 2K. K. T. Khoo, 3D. M. Commane, 2S. Kelly, 2M. Bradburn, 3J. Mathers. 1Gastroenterology and Medical School, UHCW and University of Warwick, Coventry, UK, 2Surgery, NHCT, Northumberland, UK, 3Human Nutrition Research Centre, Newcastle University, Newcastle, UK
Introduction: Telomeres are tandem repeated DNA sequences located at the ends of chromosomes. Shortening of telomeres has been reported to occur in ageing as well as in cancer.1 Previous reports have suggested shorter telomeric lengths in patients with ulcerative colitis (UC), particularly in those with active inflammation and dysplasia.2 We hypothesise that disease duration may affect telomere length in non-dysplastic tissue, and in addition demonstrate a relationship between promoter gene methylation of ESR1 and N33. We have previously described a possible alternative pathway for colorectal carcinogenesis in UC, ie, inactivation through methylation of putative tumour suppressor genes (ESR1 and N33).3
Aims and Methods: To assess telomere length in the macro and microscopically normal mucosa of UC patients. 63 subjects were recruited (22 UC patients and 41 age and sex-matched controls). Colorectal mucosal biopsies were obtained and DNA extracted. Telomere length was determined by quantitative real-time PCR and measurements were made in quadruplicate as described by Martin-Ruiz et al.4
Results: The mean duration of UC was 9 years with on average one flare-up per year and the mean simple clinical colitis activity index score was 2. Telomere lengths were significantly (p = 0.01) shorter in UC subjects compared with controls. There was no relationship between promoter gene-specific methylation of ESR1 and N33 or disease duration with telomere length in UC subjects (see table).
Conclusion: These findings suggest that telomere length may act as an index of cumulative chronic mucosal inflammation even in non-dysplastic tissue. Telomere shortening can reach a critical length whereupon resultant chromosomal instability leads to progression to colitis-associated neoplasia. Our data suggest that this is unlikely to occur through promoter silencing of tumour suppressor genes. Ongoing work is being undertaken to determine if lifestyle factors such as smoking and diet influence telomere lengths.
Funding: This study is funded by the Food Standards Agency (N12015) and National Ileostomy Association.
PT258 A UK-WIDE AUDIT OF THE EFFECTIVENESS AND SAFETY OF ADALIMUMAB IN CHILDREN AND YOUNG PEOPLE WITH CROHN’S DISEASE
1R. K. Russell, 2M. L. Wilson, 3N. Shah, 3G. Mahdi, 3W. Hyer, 3C. Spray, 3C. Daman, 3R. Heuschkel, 3N. A. Afzal, 3M. Elawad, 3F. Torrente, 3N. Ayub, 3J. M. E. Fell, 3G. Ho, 3S. Naik, 2D. C. Wilson. 1Department of Paediatric Gastroenterology, Yorkhill Hospital, Glasgow, UK, 2Child Life and Health, University of Edinburgh, Edinburgh, UK, 3British Society of Paediatric Gastroenterology Hepatology and Nutrition, Adalimumab Study Group, UK
Introduction: Adalimumab (Humira, Abbott, UK) is a humanised anti-tumour necrosis factor (TNF) therapy that has been shown to be efficacious for the induction and maintenance of disease remission for adults with Crohn’s disease (CD). Experience in children is extremely limited. We aimed to summarise the UK paediatric experience.
Aims and Methods: British Society of Paediatric Gastroenterology Hepatology and Nutrition (BSPGHAN) members were invited into the study via e-mail. Inclusion criteria were CD patients younger than 18 years when commencing adalimumab and with at least 4 weeks of follow-up. Patient details collected included previous infliximab therapy and surgery. Adalimumab dosing schedule, dose escalation and side effects were collected. Adalimumab effect was assessed using either the paediatric Crohn’s disease activity index or the physicians global assessment. Response to adalimumab was recorded at 1, 6 and 12 months.
Results: 26 patients from 13 centres received adalimumab at a median age of 14.5 years (range 3.3–17.8) and for a median of 0.7 years (0.1–7.2); 18 (69%) were male. The median age at CD diagnosis was 10.5 years (2.1–13.7), and 10 (38%) and 24 (92%) had required surgery and infliximab treatment, respectively, before adalimumab use. For induction 15 (58%) had an induction dose of 80/40 mg, two (8%) had 160/80 mg, three (12%) had 24 mg/m2 and six (23%) had a combination of other doses. By 4 weeks, eight (31%) entered remission, nine (35%) had a response and nine (35%) had no response. 25 (96%) proceeded to maintenance therapy, of which 80% commenced on 40 mg fortnightly, one (4%) had 80 mg, three (12%) had 24 mg/m2 and one (4%) had other. Seven (28%) required escalation of therapy (shortening of frequency or increase in dosage). 18 were followed up to 6 months and 12 to 12 months of maintenance therapy; of these, 14 (78%) and 10 (83%) were in remission at 6 and 12 months, respectively, although some patients needed adjuvant treatment to achieve this. 17 (65%) reported pain at the injection site and six (23%) reported serious side effects. Of these, there was one report each of serious bacterial infection, serious viral infection, transient visual loss, severe nausea and pain, transient leucopenia and a stomal bleed requiring surgical revision.
Conclusion: In UK paediatric practice, adalimumab is useful in treatment in refractory patients with overall remission rates of 31%, 78% and 83% at 1, 6 and 12 months, respectively. At present, however, there is a paucity of long-term safety data in this patient group.
PT259 THE BURDEN OF IONISING RADIATION FROM DIAGNOSTIC TESTS IN IMMUNOSUPPRESSED PATIENTS WITH INFLAMMATORY BOWEL DISEASE: A RETROSPECTIVE AUDIT
R. Basuroy, J. Bebb, R. Singh, A. Cole. Derby Digestive Diseases Centre, Derby Hospitals NHS Foundation Trust, Derby, UK
Introduction: Malignancy, and in particular hepatosplenic T-cell lymphoma, is a recognised complication of immunosuppressive therapy in inflammatory bowel disease (IBD). Radiation exposure of greater than 50 milli-Sieverts (mSv), seen in atomic bomb survivors and nuclear industry workers, is also known to increase the risk of malignancy. Radiological investigations are often used in the initial diagnosis of IBD, with computed tomography increasingly used to investigate for abdominal complications. We were interested to find out if our immunosuppressed patients with IBD were being exposed to significant levels of radiation, particularly when alternatives such as magnetic resonance imaging (MRI) are becoming increasingly available.
Aims and Methods: This study aims to quantify the total exposure to ionising radiation in IBD patients who require immunosuppressive treatment. Sequential patients from the adult IBD database were analysed, with three groups identified depending on disease (Crohn’s disease or ulcerative colitis) and on the type of immunosuppressive therapy; two groups consisting of ulcerative colitis and Crohn’s disease patients receiving non-biological agents and a group of Crohn’s disease patients receiving biological therapy. The radiology reporting system was used to calculate exposure for each radiological modality with effective dose data drawn from published standardised tables (National Radiological Protection Board).
Results: The results table outlines demographic data and ionising radiation exposure (mSv) in the three patient groups identified. Median values are quoted with ranges expressed within parenthesis.
Conclusion: Patients with Crohn’s disease treated with biological agents appear to be more likely to be exposed to harmful levels of ionising radiation. Almost 20% of these patients have been exposed to the 50 mSv effective dose associated with a significant increase in the risk of cancer. The use of these diagnostic radiological investigations should be minimised and alternative investigations, such MRI and capsule endoscopy, considered instead.
PT260 HOW MUCH AGREEMENT IS THERE BETWEEN HISTOLOGICAL, ENDOSCOPIC AND CLINICAL ASSESSMENTS OF REMISSION IN ULCERATIVE COLITIS?
1S. J. Thomas, 1A. Walsh, 2A. Von Herbay, 1O. Burchell, 1O. Brain, 1S. Keshav, 2B. Warren, 1S. Travis. 1Gastroenterology Unit, John Radcliffe Hospital, Oxford, UK, 2Department of Cellular Pathology, John Radcliffe Hospital, Oxford, UK
Introduction: Remission is the goal of therapy in ulcerative colitis (UC) and a primary endpoint of clinical trials recommended by the European Medicines’ Evaluation Agency (EMEA). Disparity between clinical, endoscopic and histological assessments of disease activity was reported as early as 1956.1 As the definition of remission now affects both clinical and regulatory decisions, this disparity needs to be re-evaluated.
Aims and Methods: The aim was to quantify disparities between clinical, endoscopic and histological assessments of remission in patients with an established diagnosis of UC. Clinical activity was defined by the simple clinical colitis activity index (SCCAI),2 endoscopic activity by the Baron score3 and microscopic activity by the Truelove and Richards’ score1 (remission scores <2, <1 and “no significant inflammation”, respectively). Consecutive patients requesting an early appointment were assessed by four specialist gastroenterologists, before video sigmoidoscopy and mucosal biopsy. Each scored clinical and endoscopic activity independently. Histological activity was scored by two specialist pathologists. Fleiss’ kappa was used to evaluate interobserver variation and the χ2 test to compare proportions of patients in remission, or with mild, moderate or severe activity.
Results: 91 patients were recruited; 37 (41%) were in clinical remission, 30/37 (81%) were also in histological remission, 30/37 (81%) were in endoscopic remission and 20/37 (76%) (20/91 = 22%) were in remission by all three measures. 56 (61%) were in endoscopic remission; of these, 26/56 (46%) had clinical activity and 10/26 (38%) had moderate or greater clinical activity (SCCAI 6–8). 47 (52%) were in histological remission; of these, 42/47 (81%) were in clinical remission and 30/47 (64%) were in endoscopic remission. Agreement between histological and endoscopic assessment (κ = 0.58, moderate agreement) was better than between clinical and endoscopic (κ = 0.27), or clinical and histological (κ = 0.47), or between all three methods (κ = 0.44).
Conclusion: Modest agreement between clinical and endoscopic or histological activity emphasises the differences between the measures, all of which may have prognostic value. Clinical assessment systematically overestimates disease activity (and therefore underestimates remission) when compared with endoscopic or histological assessment.
PT261 WITHDRAWAL OF GLUCOCORTICOIDS IN INFLAMMATORY BOWEL DISEASE PATIENTS WITH A MEDIAN DEPENDENCY PERIOD OF 14 YEARS: A PROPOSED WITHDRAWAL METHOD
1S. J. Murphy, 2L. Wang, 3L. A. Anderson, 2A. Steinlauf, 2D. H. Present, 4J. I. Mechanick. 1Medicine, Daisy Hill Hospital, Newry, UK, 2Gastroenterology, Mount Sinai Medical Center, New York, USA, 3Centre for Public Health, Queens University Belfast, Belfast, UK, 4Endocrinology, Diabetes and Bone Diseases, Mount Sinai Medical Center, New York, USA
Introduction: Glucocorticoid dependency causes much suffering among patients with inflammatory bowel disease (IBD). Methods of withdrawal of glucocorticoids in such patients are not well described.
Aims and Methods: To evaluate a method of glucocorticoid withdrawal adopted at a major IBD referral centre. Consecutive IBD patients who could not be weaned using traditional methods were transitioned from their current glucocorticoid to an equivalent dose of dexamethasone given orally twice a day and were educated about symptoms of the glucocorticoid withdrawal syndrome. A slow withdrawal was attempted under careful clinical supervision for signs of active IBD and/or adrenal withdrawal. Low-dose (1 μg) cosyntropin (synthetic adrenocorticotrophic hormone) stimulation testing was performed to detect subtle neuroendocrine recovery to help guide the pace of subsequent tapering and/or stopping of glucocorticoids. Conventional dose (250 μg) cosyntropin testing was performed 1–3 months following complete discontinuation of glucocorticoid. Multivariate analysis was performed to assess predictors of a slow weaning process.
Results: Twelve patients (10 men, two women), average age 54 years (range 29–75) were eligible for inclusion in the study during the period 1998–2006. Six had ulcerative colitis, six had Crohn’s disease and the median disease duration was 21 years (range 3–45). The median glucocorticoid dependency period was 14 years (range 2–45), with a median daily prednisone dose of 12.5 mg over this period. Ten patients (83%) were successfully weaned; two required re-treatment with glucocorticoids (duration 3 months in one patient and 2 years in the other) but have remained off glucocorticoids after follow-up periods of 48 and 31 months, respectively. The duration of follow-up from the final glucocorticoid wean was a median of 38 months (range 3–73). Two patients required treatment for active IBD during the withdrawal process; both were subsequently successfully weaned. Two patients were not weaned; one was lost to follow-up, the other developed an unknown autoimmune disease, which necessitated glucocorticoid treatment. The median weaning time in successful patients was 15 months (range 4–49) and the median number of hospital visits was 8.5 (range 3–37). Multivariate analysis did not show any significant predictive factors for a slow wean, including the average daily dose of glucocorticoid (p = 0.985). However, a longer duration of glucocorticoid use was associated with a slower wean, although the results failed to reach significance (p = 0.056).
Conclusion: Glucocorticoid withdrawal was slow and labour intensive but the success rate was high and the response durable. We recommend this approach because of the morbidity associated with chronic glucocorticoid use in IBD patients.
PT262 REDUCING TIME TO SYMPTOM IMPROVEMENT AND RESOLUTION FOR MODERATELY ACTIVE ULCERATIVE COLITIS
1T. R. Orchard, 2D. Ramsey, 3S. V. D. Geest, 4S. P. L. Travis. 1Department of Gastroenterology, St Mary’s Hospital, London, UK, 2Biostatistics, P&G Pharmaceuticals, Mason, Ohio, USA, 3M&TA, P&G Pharmaceuticals, Geneva, Switzerland, 4Department of Gastroenterology, John Radcliffe Hospital, Oxford, UK
Introduction: The purpose of this analysis was to investigate the time to symptom improvement and resolution of rectal bleeding, stool frequency or both rectal bleeding and stool frequency in patients with moderately active ulcerative colitis (UC) receiving 4.8 g/day or 2.4 g/day mesalazine.
Aims and Methods: Two randomised, double-blind, 6-week, parallel-group studies (ASCEND I and II) in patients with moderate UC were combined and analysed. The efficacy of modified-release mesalazine 4.8 g/day (800 mg tablets) was compared with 2.4 g/day (400 mg tablets). The median time to symptom improvement and resolution and the percentage of moderate UC patients who experienced symptom improvement/resolution by relevant time points were calculated. Time to symptom improvement/resolution was defined as the number of days between the first day of dosing and the first day of symptom improvement/resolution. Symptom improvement was defined as a decrease from a baseline of 1 point or more. Symptom resolution was defined as a score of 0.
Results: 423 analysable patients had moderate UC. Kaplan–Meier results for time to symptom improvement/resolution for 4.8 g/day and 2.4 g/day are shown. The median time to symptom resolution of both rectal bleeing and stool frequency was 19 days versus 29 days for 4.8 g/day versus 2.4 g/day (p = 0.02). By day 14, rectal bleeding resolution was achieved in 64% versus 49%, stool frequency resolution in 58% versus 50% and both rectal bleeding and stool frequency resolution in 43% versus 30% for 4.8 g/day and 2.4 g/day, respectively.
Conclusion: Mesalazine 4.8 g/day for patients with moderate UC results in faster symptom improvement/resolution than 2.4 g/day. 14 days is a nodal point for deciding whether to escalate therapy; mesalazine 4.8 g/day from the start of a flare could avoid the need for steroids in some patients.

PT-262 Figure Time to symptom improvement/resolution of both rectal bleeding and stool frequency. Imp, improvement; Res, resolution.
PT263 PREOPERATIVE INFLIXIMAB AND RISK OF POSTOPERATIVE COMPLICATIONS IN PATIENTS WITH INFLAMMATORY BOWEL DISEASE: META-ANALYSIS OF OBSERVATIONAL STUDIES
V. Subramanian, C. J. Hawkey. Nottingham Digestive Diseases Centre and Biomedical Research Unit, Nottingham University and Hospital, Nottingham, UK
Introduction: Abdominal surgery for inflammatory bowel disease (IBD) is not without risks. Inflximab has been approved for use in both Crohn’s disease (CD) and ulcerative colitis (UC) by the US Food and Drug Administration. The use of high-dose steroids has been shown in a previous meta-analysis to increase the risk of postoperative complications in patients with IBD.1 There is still debate whether the use of infliximab would also increase postoperative complications in this population.
Aims and Methods: To estimate the risk of postoperative complications following abdominal surgery in patients with IBD who received infliximab preoperatively, a meta-analysis of observational studies was conducted. We searched electronic databases for full journal articles published after 1990 reporting on postoperative complications in patients with IBD provided they compared patients on infliximab with those not on infliximab. We hand searched the reference lists of all retrieved articles. We carried out random effects meta-analysis and checked for bias using Egger’s method. We also calculated Cochran’s Q and the I2 statistic to assess for heterogeneity.
Results: A total of eight observational studies involving 1795 patients with IBD met the inclusion criteria for infectious complications and six studies involving 1306 patients met the criteria for total complications. Pooled analysis showed that the risk of total complications was significantly increased (odds ratio (OR) 1.38, 95% CI 1.01 to 1.90) and the risk of infectious complications was raised with the confidence intervals almost reaching significance (OR 1.69, 95% CI 0.96 to 2.97). Analysis on studies involving UC patients showed an increase in both infectious (OR 3.36, 95% CI 1.59 to 7.07) and total complications (OR 1.86, 95% CI 1.15 to 3.00). Subgroup analysis on studies involving only patients with CD showed no increase in pooled odds ratios of both infectious (OR 1.49, 95% CI 0.89 to 2.51) and total complications (OR 1.11, 95% CI 0.62 to 2.02). Heterogeneity among studies was higher when analysing all studies with IBD and was low for analysing studies involving patients with CD and UC separately.
Conclusion: There is an increased risk of both infectious and total postoperative complications among patients with UC exposed to infliximab but not for patients with CD exposed to infliximab. When the entire cohort of IBD patients was assessed the risk was higher for total complications and almost reached significance for infectious complications but there was a lot of heterogeneity when combining these studies.
PT264 MUCOSAL BARRIER BREAKDOWN IN ULCERATIVE COLITIS: THE CASE OF NITROSOTHIOLS IMPAIRING COLONOCYTES
1W. E. Roediger, 2A. Cummins, 1P. Cowled. 1Surgery, University of Adelaide and The Queen Elizabeth Hospital, Woodville, Australia, 2Gastroenterology, University of Adelaide and The Queen Elizabeth Hospital, Woodville, Australia
Introduction: The regional breakdown of the mucosal barrier in ulcerative colitis (UC) lacks clear explanation. A combination of nitric oxide derived from bacterial denitrification and sulphide derived from bacterial fermentation reliably reproduce the metabolic lesions of colonocytes in UC.1 Nitric oxide and sulphide may produce cellular nitrosothiols inactivating the cysteine groups of enzymes, proteins and coenzyme A.
Aims and Methods: To measure nitrosothiol levels in active UC and controls. Fresh rectal biopsies obtained at colonoscopies of cases with acute colitis, newly diagnosed or after recurrent attacks were analysed. Exposure to glutaraldehyde/formaldehyde was avoided and samples were stored in the dark at −70°C. After mechanical homogenisation nitrosothiols were measured with the Saville–Griess reaction with and without exposure to mercuric chloride. The reaction with sulfanilamide was measured at 540 nm after azo dye coupling. By calibration curves with S-nitrosoglutathione and tissue protein measurement (Bradford reaction) results were expressed as nmoles/mg protein.
Results: Nitrosothiols were not measured in tissues exposed to formaldehyde. Nitrosothiol levels were 129.3 ± 25.6 (n = 6) in acute UC compared with healthy controls of 53.8 ± 13.8 (n = 6) (p<0.02). Spectrometrically, nitrosothiols were produced from purified coenzyme A in the presence of nitric oxide at pH 2.0 and to a lesser degree at pH 6.9.
Conclusion: Elevated nitrosothiol formation (of which S-nitroso coenzyme A is an example) could explain older observations that free coenzyme A is depleted in experimental2 and human3 UC. Depletion of free coenzyme A diminishes lipid synthesis and beta oxidation that could initiate barrier breakdown in UC. Our preliminary results need to be confirmed by more extensive studies and related to the degree of nitric oxide production by bacterial denitrification.
PT265 BONE MARROW CELL CONTRIBUTIONS IN MURINE EXPERIMENTAL COLITIS: A COMBINED IMMUNOHISTOCHEMICAL AND IN SITU HYBRIDISATION STUDY
1C. Y. Lee, 1R. Jeffery, 2G. Hutchinson, 1R. Poulsom, 1N. A. Wright, 1W. R. Otto. 1Histopathology Laboratory, Cancer Research UK, London, UK, 2Biological Services, Cancer Research UK, London, UK
Introduction: We wished to improve upon the ability to score bone marrow (BM)-derived cells to epithelial tissues in the inflamed gut. Occasional reports have shown only individual cells engrafting within crypts, but the scoring of their BM derivation has been based on one parameter per cell, commonly the Y-chromosome in gender-mismatched BM transplants.
Aims and Methods: We have undertaken gender mismatched BM transplants from male Swiss Webster mice to B and T-cell-deficient female Rag-2 mice, which, 5 weeks later, were given 3% dextran sodium sulphate in the drinking water to induce colitis. A further BM-treated group of animals with a graft versus host-like disease was studied. We developed a new method to combine triple brightfield or fluorescent lectin or immunohistochemistry with fluorescent in situ hybridisation for the Y and X chromosomes to enable us unequivocally to analyse BM-derived male cells that presented as different cell types in the gastrointestinal tract.
Results: Entire intestinal preparations were scanned at several tissue levels. All Y chromosome-positive cells within crypt epithelia were also CD45 positive. We saw no evidence of cell fusion (XXXY). Levels of CD45-positive stromal and lymphoid cells and pericryptal myofibroblasts (positive for α-smooth muscle actin) increased with time up to a plateau, in parallel with untreated controls.
Conclusion: We conclude that BM-transplanted cells are unlikely to contribute to intestinal epithelial lineages in this model, even after ulceration. This method can usefully assist in the critical analyses of cell phenotypes following BM transplant.
PT266 ADACOLUMN APHERESIS THERAPY IN REFRACTORY ULCERATIVE COLITIS
Y. Siaw, M. O’Connor, A. Hart. Department of Gastroenterology, St Mark’s Hospital, Harrow, UK
Introduction: Activated granulocytes and monocytes play a pivotal role in the pathogenesis of inflammatory bowel disease (IBD).1
Aims and Methods: This study aimed to evaluate the safety and efficacy of leucocytapheresis in the treatment of patients with ulcerative colitis (UC) refractory to conventional therapy, including azathioprine, 6-mercaptopurine, ciclosporin, tacrolimus, methotrexate and infliximab. This was a retrospective review of all patients with UC treated with the adacolumn apheresis system (Otsuka Pharmaceuticals Europe Ltd, Uxbridge, UK). Each course of treatment consisted of five sessions of adacolumn apheresis over 5 weeks. Disease activity was evaluated by the Truelove–Witts index.2 Patients were monitored for benefits and side effects at each weekly apheresis session and approximately every 2 weeks to 3 months after adacolumn treatment. Clinical remission was defined as an inactive score on the Truelove–Witts index. Clinical response was defined as an improvement of the activity score on the Truelove–Witts index and/or a reduction in concurrent therapy.
Results: 14 patients underwent 17 courses of adacolum apheresis (three patients underwent two courses each). No patients achieved clinical remission. Six of 14 patients (42.9%) experienced a clinical response. Three of these six patients had an improvement of their Truelove–Witts activity scores only and the responses were maintained for 4 weeks, 3 months and one year, respectively. Three patients were able to stop steroids completely and had an improvement of their Truelove–Witts activity scores. The steroid-free period was one year in one patient and 2 years in two patients. Eight patients (57.1%) had no response to their adacolumn therapy, seven of whom had surgery. Time to surgery from adacolumn was 6 months (N = 5), one year (N = 1) and 2 years (N = 1). 84 of 85 adacolumn sessions were completed, one session was discontinued due to poor access. Three cases of side effects were reported including bruising, nausea and fainting.
Conclusion: Adacolumn apheresis is well tolerated and appears to play a role in the treatment of UC refractory to conventional therapies. Further controlled evaluation in this patient group is warranted.
Neurogastroenterology/motility posters
PT267 SOMATISATION PREDICTS SYMPTOM SEVERITY AND CONSULTING BEHAVIOUR IN IRRITABLE BOWEL SYNDROME PATIENTS AND THOSE WITH SYMPTOMATIC DIVERTICULAR DISEASE
1R. Spiller, 1D. Humes, 1M. Richards, 2M. Hastings, 1K. Neal, 2P. Whorwell. 1Nottingham Digestive Diseases Centre BRU, University of Nottingham, Nottingham, UK, 2Division of Gastroenterology, University of South Manchester, Wythenshawe Hospital, Manchester, UK
Introduction: When assessing patients with abdominal pain and disturbed bowel habit associated with normal physical findings it is useful also to assess psychological variables to aid management. However, although standard measures of anxiety and depression are often abnormal in irritable bowel syndrome (IBS) these fail to distinguish IBS reliably from organic disease. Non-gastrointestinal symptoms are also often prominent but their diagnostic value has not been formally assessed.
Aims and Methods: To assess the value of a modified version of the personal health questionnaire 15 (PHQ15),1 which excludes gastrointestinal symptoms, here called the PHQ12, in differentiating various subtypes of IBS from healthy volunteers and a disease control group with diverticulosis. 151 healthy volunteers were age and sex matched to 319 IBS patients (39 postinfective, 148 with diarrhoea and 132 with constipation) and compared with 91 subjects who had had campylobacter enteritis 6 months previously and 296 patients with diverticular disease (DD) (113 asymptomatic, 173 with symptoms, of whom 70 had a past history of diverticulitis and 103 had no such history, symptomatic DD).
Results: PHQ12 scores for all IBS groups were significantly higher than healthy volunteers and the diverticulosis patients except for the past history of diverticulitis group. Receiver operator curves showed that a cut-off of 6 gave the best combination of sensitivity 66.4% and specificity 94.7%. An elevated anxiety score (>7) gave a similar sensitivity of 74.4% but lower specificity at 74.8%, whereas a depression score greater than 7 gave sensitivity of 30.1% and specificity of 95.4%. Restricting analysis just to IBS patients showed that PHQ12 correlated more strongly with the IBS severity scale than anxiety or depression (r = 0.41 vs 0.29 and 0.34, all p<0.00, n = 845). PHQ12 was a significant predictor of general practitioner (GP) visits in IBS and DD. Visits were related to neither anxiety nor depression. The PHQ12 score is surprisingly unaffected by age and is only partly explained by associated anxiety and depression. Those with a past history of diverticulitis also scored highly on PHQ12, with 58% abnormal, whereas 40% were abnormally anxious and 51% were depressed.
Conclusion: The PHQ12 questionnaire is a simple useful clinical tool because it predicts IBS severity and GP visits. Elevated values after acute diverticulitis are unexplained but suggest that gut inflammation could contribute to somatisation.
PT268 A NEW APPROACH TO STUDYING PAIN IN IRRITABLE BOWEL SYNDROME USING FUNCTIONAL MAGNETIC RESONANCE IMAGING: ARTERIAL SPIN LABELLING
1E. A. Johns, 2B. J. MacIntosh, 2I. M. C. Tracey. 1Department of Gastroenterology, John Radcliffe Hospital, Oxford, UK, 2FMRIB Centre, John Radcliffe Hospital, Oxford, UK
Introduction: Functional magnetic resonance imaging (fMRI) has been used to study the neural correlates of acute experimentally induced pain in irritable bowel syndrome (IBS). Research into the neural correlates of spontaneous tonic pain that patients experience in IBS has been limited, because of technical considerations surrounding blood oxygen level-dependent-based fMRI methods, which require a changing stimulus input. Arterial spin labelling (ASL) is a non-invasive fMRI technique, which can be used to calculate cerebral blood flow (CBF) in absolute units (ml/100 g per minute) and potentially, to study the neural correlates of tonic pain. In this experiment, we aim to compare CBF values at baseline and during a sustained noxious stimulus in order to compare blood flow to brain regions of interest between the two conditions. We aim to confirm that ASL can detect and quantify changes induced by tonic pain in healthy volunteers before using it in patients with IBS.
Aims and Methods: 14 healthy volunteers gave informed consent. The study was approved by a local ethics committee. Psychophysics: topical 1% capsaicin cream was applied to the midline of the lower abdomen in order to generate a noxious stimulus. Subjects rated pain every minute using a visual analogue scale in which 0 equals no pain and 10 equals extremely painful until a rating greater than 5 was achieved for a period of at least 10 minutes (predicted length of ASL perfusion scan). Imaging: whole brain ASL sequences were performed on a 3 Tesla Siemans Trio scanner under two conditions, 10 minutes while pain free and 10 minutes of tonic pain. A non-parametric permutation-based statistical analysis was used to test for voxel-wise differences between baseline and pain conditions.
Results: Psychophysics: all 14 subjects (four men, mean age 29 years) experienced sustained pain for a minimum period of 10 minutes. This was repeated during the imaging session. Imaging: group analysis revealed significantly increased blood flow (p<0.05) in the left dorsolateral prefrontal cortex, the left anterior cingulate cortex, the left angular gyrus and the insula, caudate, putamen and globus pallidus bilaterally. Blood flow decreased significantly (p<0.05) in the right thalamus, the left angular gyrus, the left supplementary motor area, the precuneus and the hippocampus and parahippocampus bilaterally.
Conclusion: Significant differences in blood flow between baseline and the tonic pain condition were found in a number of brain regions known to be involved in the perception of pain. ASL can detect and quantify tonic experimental pain in healthy volunteers. This technique could allow us to determine the neural correlates of spontaneous tonic pain that patients experience in IBS.
PT269 SUBGROUPS OF IRRITABLE BOWEL SYNDROME HAVE A DISTINCT COLONIC MUCOSA-ASSOCIATED MICROBIOTA
G. C. Parkes, N. B. Rayment, B. N. Hudspith, L. Petrovska, M. Lomer, J. Brostoff, K. Whelan, J. D. Sanderson. Nutritional Sciences Division, Kings College London, London, UK
Introduction: Several studies have indicated a role for the gastrointestinal microbiota in irritable bowel syndrome (IBS). Studies have shown an altered gastrointestinal microbiota in IBS, although most focus on faecal microbiota. Given the increasing evidence of an inflammatory component to IBS and the proximity of the mucosa-associated microbiota to the colonic epithelium, we hypothesise that the mucosa-associated microbiota play a key role in the pathogenesis of IBS. In addition, differing subgroups of IBS based on bowel habit are likely to have distinct microbial populations.
Aims and Methods: To compare the mucosa-associated microbiota between patients with diarrhoea-predominant IBS (IBS-D), constipation-predominant IBS (IBS-C) and controls using fluorescent in-situ hybridisation. Patients with IBS-D were identified using Rome III criteria, whereas all controls had a normal bowel habit. Rectal biopsies were snap frozen in liquid nitrogen and 6\mum sections cut, fixed in 4% paraformaldehyde and permeabilised in 0.2% Triton/phosphate-buffered saline. Sections were hybridised overnight with oligonucleotide probes specific for total bacteria (EUB), bacteroides (Bac303), Clostridium coccoides–Eubacterium rectale (EREC482), bifidobacteria (Bif164), lactobacillus (Lab154) and Escherichia coli. Hybridised mucosa-associated microbiota were viewed under a confocal microscope and were quantified by counting five randomly selected high power fields.
Results: Results are summarised in the table. The mean (95% CI) age of IBS-D patients was 36.2 years (32.1 to 40.3), IBS-C patients 32.4 years (28.1 to 36.7) and controls 46.1 years (41.4 to 51.1). All bacteria were found in a mucinous layer adjacent but not adherent to the epithelium, with no invasive bacteria seen. There were significantly greater numbers of bacteroides and clostridia in the IBS subgroups than controls. Bifidobacteria were found in the highest numbers in IBS-C and the lowest in IBS-D. There was a non-significant trend towards increased numbers of total bacteria in the IBS subgroups.
Conclusion: This study demonstrates clear differences in the rectal mucosa-associated microbial populations of IBS-D, IBS-C and controls, although it is not clear from these data whether the changes are primary or secondary. Both IBS subgroups had higher levels of pro-inflammatory bacteroides and clostridia than controls. The numbers of bifidobacteria, which are known to be anti-inflammatory, were lowest in IBS-D and highest in IBS-C, which may reflect differences in the aetiology of these two subgroups of IBS. The data here support a role for the colonic microbiota in the aetiology and treatment of IBS.
PT270 DECREASED LACTOBACILLI IN THE ILEAL MUCOSA-ASSOCIATED MICROBIOTA IN DIARRHOEA-PREDOMINANT IRRITABLE BOWEL SYNDROME
G. C. Parkes, L. Petrovska, I. J. Woodman, N. B. Rayment, B. N. Hudpsith, M. Lomer, J. Brostoff, K. Whelan, J. D. Sanderson. Nutritional Sciences Division, Kings College London, London, UK
Introduction: There is increasing evidence for a role for the gastrointestinal microbiota in the aetiology of irritable bowel syndrome (IBS). The majority of studies to date have used faecal/colonic samples. However, recent studies demonstrating upregulation of the gastrointestinal mucosal immune system in the small intestine and the possible role of small intestinal bacterial overgrowth suggest that the microbiota of the small intestine may play a role in the aetiology of IBS. As a result of difficulty in obtaining samples, few studies have attempted to examine the ileal microbiota in patients with IBS. Previous studies have used culture techniques now known to underestimate the gastrointestinal microbiota grossly.
Aims and Methods: To compare the ileal mucosa-associated microbiota in patients with diarrhoea-predominant IBS (IBS-D) and controls using quantitative PCR. Patients with IBS-D were identified using Rome III criteria, whereas all controls had a normal bowel habit. Each patient underwent a colonoscopy at which ileal biopsies were snap frozen in liquid nitrogen. Total DNA was extracted using a commercial kit. PCR was performed using SYBR green, water, reference dye, target DNA and specific primers. Primers were specific to the following bacterial groups: total bacteria, Clostridium coccoides–Eubacterium rectale, bifidobacteria, lactobacilli, Escherichia coli, Bacteroides vulgatus and the bacteroides–prevotella group. Standard curves were created using extracted DNA from type strains of bacteria specific to each primer set. A primer specific to human DNA was used to quantify the size of each biopsy and adjust the results accordingly.
Results: In total, 28 ileal biopsies from patients with IBS-D and 22 from controls were obtained. The mean age of IBS-D patients was 36.5 years (32.8–40.2) and controls 42.6 years (37.6–47.6) and there were significantly fewer female controls (63% vs 27%, p<0.03). The table shows the results following analysis by ABI software. There was a significant reduction in the number of ileal mucosa-associated lactobacilli in patients with IBS-D.
Conclusion: This is the first study to examine in depth the ileal microbiota in patients with IBS. The use of quantitative PCR allows accurate culture-independent analysis of the gastrointestinal microbiota. Lactobacilli are known to have profound anti-inflammatory effects. In addition, there have now been a number of therapeutic trials of probiotic lactobacilli in IBS with some encouraging results. These findings support a hypothesis that the gastrointestinal microbiota may play a role in both the aetiology and treatment of IBS.
PT271 REACTIVITY TO IMAGERY IN HEALTH AND IRRITABLE BOWEL SYNDROME
1H. R. Carruthers, 2N. Tarrier, 1P. J. Whorwell. 1Medicine, Wythenshawe Hospital, Manchester, UK, 2Clinical Psychology, University of Manchester, Manchester, UK
Introduction: Irritable bowel syndrome (IBS) patients frequently exhibit rectal hypersensitivity and are also hypersensitive to sound. We have been using a medical artist to record the imagery of IBS and have hypothesised that the reaction to such images might differ in health and IBS.
Aims and Methods: Part 1. The four most evocative images of IBS were determined by showing 70 patients 12 paintings of the condition and scoring their responses. Part 2. The spontaneous response to these four images along with four “non-IBS painful” paintings and four neutral paintings was then assessed in a further 100 IBS patients and 100 controls. In addition, the prompted reaction in terms of whether an image evoked the notion of pain, discomfort or bloating and to what degree, was recorded.
Results: Part 1. Four images depicting bloating and pain rather than bowel dysfunction scored highest irrespective of symptom severity score. Part 2. These four IBS images prompted a significantly different spontaneous response in patients than controls (see table) and similarly a greater reactivity was observed in terms of their prompted reactions. Even “non-IBS painful” and neutral images resulted in an exaggerated and frequently significantly different response in patients than controls. Images of bloating induced the greatest differences between the two groups.
Conclusion: IBS patients appear to exhibit visual hypersensitivity. It is also possible that assessing the response to a particular image might give insights into which symptom most troubles a patient as well as enabling the selection of more homogenous populations for research purposes.
PT272 ALTERATIONS OVER TIME IN THE PREVALENCE OF IRRITABLE BOWEL SYNDROME AND ITS EFFECT UPON QUALITY OF LIFE
J. S. Leeds, R. Chiang, M. Bonney, W. Li, D. S. Sanders. Gastroenterology and Liver Unit, Royal Hallamshire Hospital, Sheffield, UK
Introduction: Irritable bowel syndrome (IBS) is a common reason for attendance in primary care and referral to secondary care. The prevalence of IBS in primary care may be up to 15%. There is a paucity of data pertaining to the prevalence of IBS within a community. We aimed to assess whether there has been a change in the prevalence of IBS over time. In addition, we assessed the quality of life in these individuals.
Aims and Methods: Two cohorts were recruited into the study from the community: 601 individuals from 2001 and 604 individuals from 2007. All were asked to complete a validated gastrointestinal symptom questionnaire, which also assessed IBS symptomatology using the Rome II criteria. In the 2007 cohort a short-form 36 (version 2) quality of life assessment tool was also completed. Thereafter, individuals with IBS were age and sex matched to non-IBS controls and quality of life scores were compared.
Results: The prevalence of IBS in 2001 was 68/601 (11.3%, 95% CI 9.0 to 14.1) and in 2007 it was 48/604 (7.9%, 95% CI 6.0 to 10.5) odds ratio (OR) 0.71, p = 0.04. There was no difference in the rate of tiredness all the time (OR 1.1, p = 0.66) or thyroid disease (OR 1.3, p = 0.44). There was an increase in those diagnosed with malabsorption (OR 4.0, 95% CI 1.3 to 12.0, p = 0.007), B12 deficiency (OR 6.9, 95% CI 0.9 to 56.8, p = 0.03) and a family history of coeliac disease (OR 3.6, 95% CI 1.0 to 13.1, p = 0.03). Analysis of the 48 individuals with IBS in the 2007 cohort (compared with controls) revealed no differences in rates of thyroid disease (OR 1.5), diabetes (OR 1.0) or anaemia (OR 1.3). However, there were significant differences in rates of abnormal bowel habit (OR 12.5), flatulence (OR 2.8), bloating (OR 2.8), floating stools (OR 3.7), abdominal pain (OR 3.3) and tiredness (OR 5.7). Comparison of short-form 36 (version 2) scores revealed a significant reduction in physical functioning (p = 0.003), role limitations due to physical health (p = 0.023), bodily pain (p = 0.001), general health perceptions (p = 0.001), social functioning domains (p = 0.048) and physical composite score (p<0.001).
Conclusion: In our region there has been a significant reduction in IBS symptoms in the community; however, this has been coupled with an increase in the diagnosis of malabsorption. Individuals with IBS symptoms have significantly reduced quality of life scores particularly in the physical domains by comparison with non-IBS controls.
PT273 AUTONOMIC REACTIVITY TO PSYCHOLOGICAL AND PHYSICAL STRESSORS DIFFERENTIALLY CORRELATES WITH MEASURES OF ANXIETY AND DEPRESSION IN PATIENTS WITH IRRITABLE BOWEL SYNDROME
1N. M. Thoua, 2A. Hobson, 2G. Dukes, 2D. Kelleher, 2K. Hicks, 2R. Boardley, 1A. Raeburn, 1A. Emmanuel. 1Gastrointestinal Physiology Unit, University College Hospital, London, UK, 2Gastrointestinal Discovery Medicine, GSK R&D Ltd, London, UK
Introduction: Psychological co-morbidity is prevalent in patients with irritable bowel syndrome (IBS) and stress-induced exacerbation of IBS symptoms is also commonly reported. The relationship between stress responsiveness and psychological phenotype in IBS is unknown. We investigated whether two key psychological domains, anxiety and depression, correlate with stress-induced changes in rectal autonomic tone and sensitivity in IBS patients.
Aims and Methods: Nine Rome II compliant IBS patients (eight women) were enrolled into the study. At the beginning of the study all patients completed the hospital anxiety and depression (HAD) questionnaire. Baseline measures of rectal electrosensitivity and rectal mucosal blood flow (RMBF) were established and then reassessed during 10-minute periods of psychological stress (dichotomous listening), physical stress (cold-pressor) and during a 10-minute recovery period. Data are reported as mean change from baseline with 95% CI.
Results: Confirming our previous findings,1 both periods of stress reduced RMBF (physical: −75.4 (−109 to −41.8); psychological: −59.5 (−93.1 to −25.9); p<0.01). Anxiety scores correlated significantly with the magnitude of change in RMBF during physical stress (r = −0.471, p = 0.0175). In contrast, during psychological stress, depression scores correlated significantly with the magnitude of change in RMBF (r = −0.442, p = 0.0271). Stress periods also reduced rectal sensory threshold (RST) (physical: −5.33 mA (−8.01 to −2.66); psychological: −4.56 mA (−7.23 to −1.88); p<0.02) and pain threshold (RPT) (physical: −8.61 mA (−12.56 to −4.66); psychological: −7.11 mA (−11.06 to −3.16); p<0.01). Although depression scores correlated positively with absolute pain thresholds (r = 0.432, p = 0.031), there was no correlation between HAD scores and the magnitude of change of RST and RPT.
Conclusion: We have shown that anxiety and depression correlate with the magnitude of the gut autonomic response (as measured by RMBF) elicited by experimental stress, but do so in a selective manner. Anxiety, which is commonly associated with hypersensitivity, correlated with physical stress, whereas depression, commonly associated with negative mood, correlated with psychological stress. The ability to assess the complex interplay between psychological profile and stress responsiveness objectively may help further differentiate clinical phenotypes in the IBS population.
PT274 THE EFFECT OF CENTRAL ADIPOSITY ON OESOPHAGEAL ACID EXPOSURE AND SYMPTOMS OF GASTRO-OESOPHAGEAL REFLUX DISEASE
R. Anggiansah, R. R. Sweis, A. Anggiansah, T. Wong, M. Fox. Department of Gastroenterology, St Thomas’ Hospital, London, UK
Introduction: Epidemiological evidence suggests a link between gastro-oesophageal reflux disease (GORD) and obesity.1 2 Mechanistic studies suggest that this relationship is due to the effects of central adiposity on intragastric pressure with disruption of the gastro-oesophageal junction (GOJ) reflux barrier;3 however, the clinical relevance of these findings has not been proved.
Aims and Methods: From August 2005 to December 2006, patients referred to a tertiary referral centre for oesophageal investigation of suspected GORD were studied. Height, weight and waist circumference (WC) were measured. Stationary manometry and 24-h ambulatory pH studies off acid-suppressant medications were performed and symptom severity was assessed by a validated questionnaire. Linear regression models were used to analyse associations between various covariates of interest and Pearson’s correlation coefficient (PC) was used for continuous variables.
Results: 582/676 (86%) consecutive patients (age 48 years (range 14–89), 56% women) had complete data for analysis. The prevalence of obesity defined by a body mass index (BMI) of 30 kg/m2 or greater in men and women was 16% and 23% (p = ns), respectively. More men had WC of 99 cm or greater (men 41%, women 28%; p<0.001). The percentage of time with pH less than 4 (%time pH<4) at 5 cm above the lower oesophageal sphincter (LOS) increased with obesity (PC 0.255 and 0.240 for BMI and WC, respectively; both p<0.001) and age (PC 0.162; p<0.001) and was higher in men than women (p = 0.014). An increase in the %time pH<4 was associated with a reduction in LOS pressure and abdominal LOS length (PC −0.327, −0.344, respectively; p<0.001). There was a weak negative association of BMI with LOS pressure (PC −0.140; p = 0.005) but no link with abdominal LOS length. In contrast, there was a significant negative association of WC with LOS pressure (PC −0.225; p<0.001) and abdominal LOS length (PC −0.213; p<0.001). Symptom severity increased with %time pH<4 (PC 0.209; p<0.001); however, there was no change in symptom severity with BMI (PC 0.056; p = 0.17) and the effect of WC on symptom severity was weak and of borderline significance (PC 0.083; p<0.05).
Conclusion: In this large cohort of clinical patients referred for investigation of reflux symptoms, gastro-oesophageal reflux (%time pH<4) increased with obesity (BMI and WC) and was most prevalent in elderly men with central adiposity. WC but not BMI was associated with both reduced LOS pressure and abdominal length. These findings confirm the mechanistic link between increasing WC and the risk of reflux via raised intragastric pressure and disruption of the GOJ. In contrast, there was little change in symptom severity as assessed by questionnaire. The relative insensitivity to acid reflux may explain the increased prevalence of severe and complicated reflux in the obese population.1 2
PT275 NORMAL VALUES FOR HIGH RESOLUTION MANOMETRY ASSESSMENT OF LIQUID, SOLID AND MULTIPLE REPEATED SWALLOWS IN THE UPRIGHT AND SUPINE POSITIONS
R. R. Sweis, T. Wong, A. Anggiansah, M. Fox. Department of Gastroenterology, St Thomas’ Hospital, London, UK
Introduction: High resolution manometry (HRM) is an advance in oesophageal measurement.1 2 Functionally relevant HRM measurements acquired by HRM include: peristaltic coordination between proximal and mid-distal contractions (transition zone width), intrabolus pressure (IBP) and oesophagogastric pressure gradient (OGPG). Normal HRM values for peristaltic and oesophagogastric junction (OGJ) function have been published for 5 ml water swallows in the supine position. This is of technical value; however, it does not reflect normal swallowing behaviour or clinical practice in many centres.
Aims and Methods: This study presents reference HRM results for water and solid bolus swallows in the physiological upright and supine positions. In addition, the normal results of multiple repeated swallows in both positions were collected.
Methods: 12 healthy volunteers (male : female ratio 7 : 5, age 21–46 years) underwent HRM with a 36-channel solid state assembly (Sierra Scientific Instruments, USA). 10 liquid swallows of 5 ml water, three solid swallows of 1 cc bread, 200 ml water by multiple repeated swallows (MRS). Measurements were performed in the upright and supine position on the same study day.
Results: 12 volunteers were studied. Median and interquartile range (IQR) for various parameters of oesophageal and lower oesophageal sphincter (LOS) function were measured and divided into upright and supine for liquid and solid swallows. These measurements are presented in the table. Then 200 ml MRS was measured. Average IBP 0–1 cm above LOS was 9.3 mm Hg (IQR 4.5–12) in the upright position and 8.8 mm Hg (IQR 6.7–10.9) supine. MRS maximum pressure was 17 mm Hg (IQR 11.7–23.8) in the upright position and 17.3 mm Hg (IQR 12.9–28).
Conclusion: Differences in swallow positions and bolus viscosity provide a physiological challenge that highlights the oesophageal response to increased workload. In order to improve diagnostic yield and accuracy, normal values are required for point comparison. This study provides such baseline measurements, which can be used when these manoeuvres are used in the clinical setting.
PT276 THE PREVALENCE OF ELEVATED SERUM CHROMOGRANIN A IN IRRITABLE BOWEL SYNDROME AND INFLAMMATORY BOWEL DISEASE COMPARED WITH HEALTHY CONTROLS
R. Sidhu, K. Drew, M. E. McAlindon, A. J. Lobo, D. S. Sanders. Gastroenterology, Royal Hallamshire Hospital, Sheffield, UK
Introduction: Elevated serum chromogranin A (CgA) is commonly found in patients with neuroendocrine tumours but may be falsely elevated in patients with impaired renal function or those on proton pump inhibitor (PPI) therapy. Elevated CgA levels have been reported incidentally in a small group of irritable bowel syndrome (IBS) patients (n = 19) used as controls in a study of neuroendocrine tumours. Elevated CgA levels may reflect enterochromaffin cell hyperplasia, which has been demonstrated in rectal biopsies of post-infectious IBS patients. There is, however, a paucity of data on the prevalence of elevated CgA in patients with diarrhoea-predominant IBS stratified according to Rome II criteria (D-IBS) and other gastrointestinal disorders such as inflammatory bowel disease (IBD).
Aims and Methods: To investigate the prevalence of elevated CgA levels in patients with D-IBS and IBD compared with healthy controls. Patients with Rome II D-IBS and IBD were recruited prospectively from the outpatient setting. Patients were investigated and treated for their diagnosis as per British Society of Gastroenterology guidelines. In addition, serial levels of CgA were measured using the new competitive radioimmunoassay, which uses antibodies against human CgA (Euro-Diagnostica, normal values <4 nmol/l). Healthy volunteers were screened with a questionnaire to exclude the presence of disease. Patients with elevated CgA levels were requested to have repeated levels done in addition to fasting gut hormones and urinary 5-hydroxyindole acetic acid.
Results: 87 patients with D-IBS (67.8% women), 39 patients with IBD and 50 healthy volunteers were recruited, mean age 43 years (range 20–60 years). The mean CgA levels in the IBS, IBD and healthy volunteer groups were 7.2 nmol/l, 6.4 nmol/l and 4 nmol/l, respectively. CgA levels were elevated in 50.6% (n = 44) of patients with D-IBS compared with 30.8% (n = 12) of patients with IBD (p = 0.04) and 30% (n = 15) of healthy controls (p = 0.02). In the D-IBS group, CgA levels were normal on repeated testing in 19 patients (22%) and were less than 10 nmol/l in 15 patients (17%) but with normal fasting gut hormones and urinary 5-hydroxyindole acetic acid. In a further 10 patients with levels greater than 10 nmol/l (11%), subsequent investigations failed to reveal alternative pathology/carcinoid but 70% of them were on PPI therapy. Within the IBD group with elevated CgA (n = 12), levels returned to normal in two patients on repeated testing, whereas they remained elevated but less than 10 μ/l in eight patients (20.5%). Five of these patients were on PPI therapy. One patient was investigated with a normal octreoscan and computed tomography scan, whereas the other patient declined repeat levels. In the 15 healthy volunteers with elevated CgA (4–10 nmol/l), nine returned to normal (16%), whereas six patients declined further tests.
Conclusion: CgA levels using the new radioimmunoassay appear to be non-specifically elevated in patients with IBS, IBD and in healthy volunteers. PPI therapy also appears to be a common reason for an elevated CgA level. A higher reference range may be more useful for the utility of this new assay.
PT277 WITHDRAWN
PT278 PSYCHOPHYSIOLOGICAL DETERMINANTS THAT MODULATE THE NUTRIENT-MEDIATED SENSATIONS DURING EXPERIMENTALLY INDUCED ANXIETY IN HEALTHY HUMAN INDIVIDUALS
U. Marreddy, K. S. Ng, K. Kamal, Q. Aziz. Neurogastroenterology, Barts and The London Medical School, London, UK
Introduction: It has been shown in healthy individuals that meal-induced sensations are heightened during experimentally induced anxiety. Furthermore, it is suggested that in patients with functional dyspepsia psychological factors modulate satiation signals and are partly responsible for the symptom burden experienced. However, assessment of meal-induced sensations in response to psychological stressors is subjective and it is not known if activation of the stress response such as the autonomic nervous system (ANS) also occurs and whether this ANS activation can act as an objective biomarker of the effect of stress on meal-induced symptoms. In this study we explored the interaction between psychological factors and autonomic reactivity patterns in the perception of meal sensations during experimentally induced anxiety in healthy individuals.
Aims and Methods: 25 healthy volunteers (aged 28 ± 9 years, 14 men and 11 women) received standardised nutrient challenge (Fortisip; Nutricia, 50 ml/minute) and were exposed to neutral and anxiogenic stimuli (shock threat). Anxiety ratings were assessed. Sympathetic and parasympathetic activity was measured (eg, heart rate, mean arterial blood pressure and cardiac vagal tone using NeuroScope. We assessed the personality traits and perceived stress and anxiety.
Results: 25 healthy volunteers with a mean age of 28 ± 9 years completed both the stress and neutral experiments. Anxiety visual analogue scale (VAS) scores and Spielberger trait anxiety index (STAI) anxiety scores confirmed anxiety induction during the stress experiment (anxiety VAS neutral 6.5 ± 1.9 vs anxiety 2.6 ± 1.2; p<0.02), (STAI scores, neutral 34.0 ± 1.8 vs anxiety 42.2 ± 2.4; p = 0.01). The intensity of epigastric symptom ratings scores to nutrient challenge for discomfort (1.4 ± 0.4 vs 2.9 ± 0.4; p = 0.01), fullness (5.1 ± 0.6 vs 6.0 ± 0.5; p = 0.01) and belching (1.5 ± 0.3 vs 2.6 ± 0.5; p = 0.01) were significantly higher during the anxious state. Autonomic reactivity patterns revealed increased sympathetic activity (coping strategies index baseline 1.6 ± 0.2 vs stress 2.3 ± 0.2; p = 0.03) and decreased parasympathetic tone (baseline 12.9 ± 1.8 vs 6.7 ± 0.8; p = 0.01) during the anxiety induction in most subjects. No significant correlation between psychological factors and symptom scores was seen, neither was any correlation found between symptom scores and ANS measures.
Conclusion: In our study we have found that experimental anxiety enhances the meal sensations and increases the intensity of perceived epigastric symptoms when compared with a neutral condition. A typical autonomic reactivity pattern was observed during anxiety induction, ie, increased sympathetic activity and withdrawal of parasympathetic activity. This ANS reactivity during anxiety, especially the lowering of vagal activity, might be responsible for the heightened perception of symptoms and requires further study in a larger cohort of healthy subjects and patients with functional dyspepsia.
PT279 PREVALENCE AND SYMPTOM PROFILING OF OROPHARYNGEAL DYSPHAGIA IN A COMMUNITY-DWELLING ELDERLY POPULATION: A SELF-REPORTING QUESTIONNAIRE SURVEY
1G. Holland, 1V. Jayasekeran, 2N. Pendleton, 2M. Horan, 2M. Jones, 1S. Hamdy. 1Gastrointestinal Sciences, School of Translational Medicine, University of Manchester, Manchester, UK, 2Age and Cognitive Performance Research Centre (ACPRC), School of Translational Medicine, University of Manchester, Manchester, UK
Introduction: Although the prevalence and clinical consequences of oropharyngeal dysphagia in diseases such as neuromuscular disorders and cancer are well established, virtually nothing is known about the prevalence of dysphagia in the healthy older population. Furthermore, the symptomatic basis for oropharyngeal dysphagia remains unclear. Here, we describe a detailed questionnaire-based survey of swallowing dysfunction in a large otherwise healthy community-dwelling older population in the UK.
Aims and Methods: A postal survey of the Sydney oropharyngeal dysphagia questionnaire1 was sent to 800 residences in the north of England that formed part of the University of Manchester Age and Cognitive Performance Longitudinal Study.2 This cohort comprises older (mean age 81 years, range 69–97) individuals who are otherwise healthy on entry, with no history of previous neurological disease. The postal questionnaire was a validated self-report inventory to measure the symptomatic severity of oral-pharyngeal dysphagia, which assessed a total of 17 domains of swallowing function. The maximal score obtainable is 1700, with a score of over 200 indicating significant swallowing difficulty. For the purposes of this study, domain questions were also subcategorised into obstructive or functional type symptoms. All data were analysed using SPSS.
Results: Of the 800 questionnaires sent out, 627 were returned, giving a response rate of 78%. 24 were later discarded as incomplete, giving a completed response rate of 76%. There was a female preponderance at 76.3% of the total respondents. 13.6% of the population indicated that they had significant dysphagia. Unsurprisingly, the levels of dysphagia severity were directly correlated with the subjects’ age (r = 0.12, p = 0.009). When subcategorised, 71% of the dysphagic subjects gave symptoms suggestive of functional dysphagia producing airway compromise, with 68% indicating symptoms more of an obstructive nature. The three commonest symptoms included a feeling of food sticking in the throat, a sensation of choking or coughing on swallowing and difficulty swallowing hard foods.
Conclusion: This is the first study carefully to quantify oropharyngeal dysphagia in the healthy old and shows that dysphagia is prevalent in older people, affecting nearly one in six people who are deemed otherwise healthy and living independently in the community. Clinicians should therefore be vigilant to the possibility of swallowing problems even in the seemingly well older population, which may require further evaluation.
Oesophagus posters
PT280 OESOPHAGEAL CONTRAST STUDIES BEFORE GASTROSCOPY IN THE INVESTIGATION OF HIGH DYSPHAGIA
1A. Mawas, 1E. Cameron, 1S. Middleton, 2N. Carroll, 1I. Nasr. 1Gastroenterology, Addenbrooke’s Hospital, Cambridge, UK, 2Radiology, Addenbrooke’s Hospital, Cambridge, UK
Introduction: It is contentious whether radiological investigation should precede endoscopy in patients with high dysphagia. Radiology may identify patients with pathology in whom it is potentially hazardous to perform flexible endoscopy (eg, those with pharyngeal pouches), although some suggest that endoscopy is necessary in almost all cases and careful intubation is safe. It has been our practice for some time to perform a water-soluble swallow in all patients with dysphagia above the manubrium before endoscopy. We have retrospectively reviewed all cases from 2005 until 2007 to establish the rate of significant high pathology and also to identify potential factors associated with significant proximal pathology.
Aims and Methods: All contrast oesophageal studies requested by the dyspepsia service to investigate high dysphagia between 2005 and 2007 were identified from the radiology database. Data were retrospectively collected regarding patient demographics and the results of contrast oesophageal studies.
Results: 376 patients underwent water-soluble swallow. 156 (41.5%) were men and the mean age was 64 years (SD 17). Pharyngeal pouches were identified in five of 376 (1.3%) patients. Four of 166 (2.4%) were older than 70 years and one was 54 years old, giving an incidence of oesophageal pouch of one in 211 (0.47%) in patients younger than 70 years. Cricopharyngeal web was found in four of 376 (1%), with an incidence of three in 166 (1.8%) in patients 70 years and older and one of 211 (0.47%) in patients younger than 70 years (one patient aged 69 years).
Conclusion: 1.3% of unselected patients referred with dysphagia above the manubrium will have a pharyngeal pouch. Almost all of these are over 70 years. These data suggest that, if pre-endoscopic oesophageal imaging for high dysphagia is limited to this patient group, the incidence of important findings will be seven in 166 (4.2%) and oesophageal contrast studies could be avoided with very little risk in 55% of all referrals.
PT281 A POPULATION-BASED STUDY OF POLYMORPHISMS OF THE INSULIN-LIKE GROWTH FACTOR AXIS AND THE OESOPHAGEAL INFLAMMATION, METAPLASIA, ADENOCARCINOMA SEQUENCE
1A. R. McElholm, 2A. J. McKnight, 2S. Heggarty, 1C. Patterson, 1B. T. Johnston, 3L. Hardie, 1L. Murray. 1Cancer Epidemiology and Prevention Research Group, Centre for Clinical and Population Sciences, Queens University of Belfast, Belfast, UK, 2Genomics Core Facility, Queens University of Belfast, Belfast City Hospital, Belfast, UK, 3Molecular Epidemiology Group, Leeds University, Leeds, UK
Introduction: The insulin-like growth factor (IGF) axis plays a key role in cell development, proliferation and survival and has been implicated in the aetiology of many cancers, including obesity-related cancers. To date, no studies have examined the relationship between this axis and oesophageal adenocarcinoma (OAC) or its precursors.
Aims and Methods: We investigated the association of common polymorphisms of the IGF axis with all stages of the oesophageal inflammation, metaplasia, adenocarcinoma sequence. The genes examined were IGF-1 and IGF-2, IGF-1 receptor (IGF-1R), IGF binding protein 3 (IGFBP3), the growth hormones (GH-1 and GH-2) and GH receptor (GHR). The Factors Influencing the Barrett’s Adenocarcinoma Relationship (FINBAR) study is an all-Ireland population-based, case–control study of OAC and its precursors. We analysed DNA from subjects with reflux oesophagitis (RO, n = 230), Barrett’s oesophagus (BO, ⩾3 cm BO at endoscopy with specialised intestinal metaplasia on biopsy, n = 189), OAC (n = 207) and normal controls (n = 223). Using a gene-based approach common single-nucleotide polymorphisms (SNP) were identified for each gene using a variety of publicly available online resources. Genotyping was performed using the Sequenom MassARRAY genotyping system and Taqman assay. Results were analysed using Haploview, a software package that provides computation of linkage disequilibrium statistics (including permutation testing) and population haplotype patterns from primary genotype data. 90 IGF axis SNP (tagging 299 alleles) met the inclusion criteria and were analysed. Three polymorphisms were associated with disease status.
Results: The IGF-1 SNP rs6214 was associated with BO (p = 0.005), even after multiple testing (10 000 permutations; p = 0.0389). Using AA genotype as a reference, the odds ratio (OR) for GG (“wild-type”) and BO was 2.40 (95% CI 1.31 to 4.41). The GHR SNP rs6898743 was associated with OAC, p = 0.0012 (10 000 permutations; p = 0.0112). With GG as the reference, the OR for CC (“wild-type”) genotype and OAC was 0.42 (95% CI 0.23 to 0.76). The IGF-1 (CA)19 “185” repeat was associated with “189” as a reference, the OR for “185” and RO was 7.67 (95% CI 1.73 to 69.92)
Conclusion: We systematically examined genetic variations of the IGF axis in a population-based case–control study of OAC, BO and RO. A microsatellite repeat and two SNP were statistically significantly associated with disease states: IGF-1 (CA)19 “185” repeat with RO, rs6214 (IGF-1) with BO and rs6898743 (GHR) with OAC. These SNP could potentially be used as a marker for disease risk, but independent validation of our findings is required. These results also suggest that the IGF pathway may be involved in the development of OAC and its precursors.
PT282 LONG-TERM OUTCOME OF BARRETT’S OESOPHAGUS-ASSOCIATED CANCERS IN SURVEYED AND NON-SURVEYED PATIENTS
1A. K. Muddu, 1J. Fallowfield, 2M. Lesn, 3N. Davies, 1P. Winwood. 1Department of Gastroenterology, Royal Bournemouth Hospital, Bournemouth, UK, 2Department of Histopathology, Royal Bournemouth Hospital, Bournemouth, UK, 3Department of Surgery, Royal Bournemouth Hospital, Bournemouth, UK
Introduction: Barrett’s oesophagus (BO) is a precursor of oesophageal adenocarcinoma. Endoscopic surveillance programmes aim to detect BO-associated adenocarcinomas at an earlier stage when intervention is likely to result in better survival. Other studies have demonstrated that surveillance-detected cancers have a better outcome than de novo cancers, but lead time bias may account for some or all of the survival benefit.
Aims and Methods: Our aim was to determine the long-term outcome of patients diagnosed with BO-associated adenocarcinoma between 1998 and 2002. The patients had originally been identified by review of the pathology computer databases and were divided into surveillance and de novo cancers and further subdivided into patients who had undergone resection and those who received palliative therapy. Information about survival was obtained through review of the notes and hospital administration systems.
Results: 54 BO-associated adenocarcinomas were identified between 1998 and 2002. Eight were detected in patients undergoing surveillance and all patients underwent oesophagectomy or endoscopic mucosal resection. Six patients (75%) had a survival greater than 5 years. 46 patients presented with “de novo” cancers and only 15 patients were suitable for resection. Of these, nine (64%) were alive at 5 years. 31 patients were only suitable for palliative therapy, three patients were lost to follow-up and of the remaining 28, one patient (4%) was alive at 5 years. In total, 5-year survival of the de novo group was 28% compared with 75% of surveillance cancers.
Conclusion: These data suggest that patients who have cancers detected during BO surveillance have an increased probability of being offered potentially curative resection with improved long-term survival compared with de novo cancers. Although lead time bias cannot be totally excluded, the sustained survival suggests that this is likely to be minimal and continued surveillance is justified.
PT283 ERBB2 EXPRESSION IN OESOPHAGEAL ADENOCARCINOMA AND BARRETT’S OESOPHAGUS: DEMONSTRATING THE POTENTIAL FOR A PRE-EMPTIVE STRIKE
1A. L. Paterson, 2E. Provenzano, 2M. O’Donovan, 2S. E. Davies, 3M. R. Novelli, 4L. B. Lovat, 1R. C. Fitzgerald. 1MRC Cancer Cell Unit, Hutchison MRC Research Centre, Cambridge, UK, 2Department of Pathology, Addenbrooke’s Hospital, Cambridge, UK, 3Department of Pathology, University College Hospital, London, UK, 4Department of Gastroenterology, University College Hospital, London, UK
Introduction: The incidence of oesophageal adenocarcinoma (OAC) has increased fourfold in the west in 30 years and has been highlighted as a major public health concern. It has a dismal 15% 5-year survival due to its late presentation and the limited benefit of current chemotherapy regimens. Targeted therapies have the potential to revolutionise chemotherapy as shown in ErbB2-overexpressing breast tumours, which account for 25% of cases. The role of the ErbB family in Barrett’s oesophagus and OAC development and progression remains to be fully explored.
Aims and Methods: The timing and frequency of ErbB2 overexpression in OAC and Barrett’s oesophagus was determined using tissue microarrays representing 136 tumours and a cohort of 73 Barrett’s oesophagus patients with high-grade dysplasia (HGD). Low-grade dysplasia (LGD) or non-dysplastic intestinal metaplasia biopsies were also available from these patients in 43 and 53 cases, respectively. The ErbB2 amplified OAC cell lines, OE19 and OE33, were used to explore the molecular consequences of ErbB2 overexpression, which were confirmed using Chinese hamster ovary (CHO) cells transfected with ErbB2 and/or epidermal growth factor receptor (EGFR) constructs and OAC resection specimens.
Results: Nine of 136 (7%) OAC had ErbB2 overexpression and amplification. Six of 73 (8%) patients had overexpression and amplification of ErbB2 in HGD areas; the overall frequency in LGD was two in 43 (5%), in one of these cases ErbB2 overexpression was also present in the adjacent HGD. No ErbB2 amplification was observed in intestinal metaplasia without dysplasia. In cell lines ErbB2 overexpression was associated with constitutive phosphorylation of EGFR and ErbB2 in the absence of exogenous ligand. Constitutive EGFR-ErbB2 heterodimers were demonstrated by immunoprecipitation with continuous activation of the downstream mitogen-activated protein kinase and Akt pathways. CHO cells transfected with EGFR and/or ErbB2 constructs confirmed that ErbB2 overexpression and low levels of EGFR resulted in ErbB2 and EGFR constitutive phosphorylation. The clinical relevance of these observations was demonstrated in seven consecutive OAC resection specimens in which both cases with ErbB2 overexpression also had EGFR and ErbB2 constitutive activation.
Conclusion: ErbB2 overexpression and amplification occurs before invasion with a similar frequency in HGD and OAC. The presence of EGFR and ErbB2 constitutive activation, ErbB2-EGFR heterodimers and downstream pathway activation provides molecular evidence for a key role of ErbB2 in these cases. ErbB-targeted therapies, with their limited toxicity, may play a role in OAC chemoprevention in patients with ErbB2-overexpressing Barrett’s oesophagus.
PT284 A PROSPECTIVE RANDOMISED CONTROLLED TRIAL OF ETHANOL-INDUCED TUMOUR NECROSIS WITH OR WITHOUT ADJUVANT EXTERNAL BEAM RADIOTHERAPY IN THE PALLIATION OF MALIGNANT DYSPHAGIA
1A. Shah, 1C. Grimley, 2I. Brown, 2R. Grieve, 1C. U. Nwokolo, 1D. E. Loft. 1Gastroenterology, University Hospital Walsgrave, Coventry, UK, 2Radiotherapy, University Hospital Walsgrave, Coventry, UK
Introduction: Ethanol-induced tumour necrosis (ETN) has been shown successfully to palliate malignant dysphagia. Its use is limited by the need for repeated procedures.
Aims and Methods: To assess the effects of combining ETN with radiotherapy, compared with ETN alone. 28 patients with unresectable cancer of the oesophagus were randomly assigned to ETN only (n = 14) or ETN plus radiotherapy, single-dose external beam 10 Gy (n = 14). Randomisation was performed independently by the clinical trials unit, Birmingham. Dysphagia was graded on a scale of 0 (normal swallowing) to 4 (total dysphagia).
Results: The median pretreatment dysphagia grade for both groups was 3. The best dysphagia grade achieved was 2 (ETN) and 1 (ETN plus radiotherapy), p<0.05. The median number of days between subsequent procedures was 19 (ETN) and 56 (ETN plus radiotherapy), p<0.01. The median number of days from first treatment to stent insertion was 51 (ETN) and 191 (ETN plus radiotherapy), p<0.05. Cumulative survival (see fig) was improved in the ETN plus radiotherapy group.
Conclusion: Compared with ETN alone, ETN plus radiotherapy was dramatically beneficial in terms of survival, time between treatments, time before stent requirement and best dysphagia grade.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
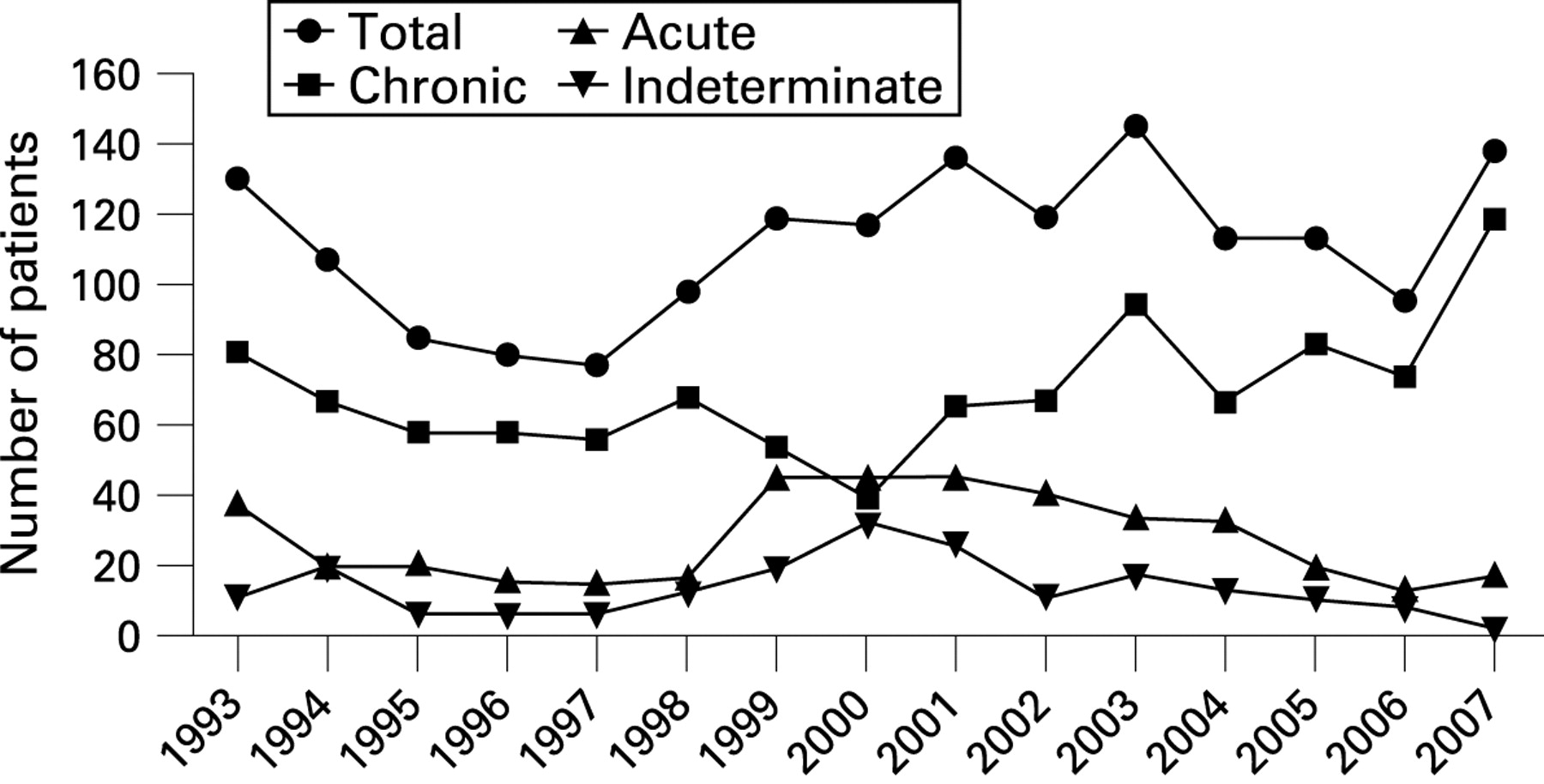{kind=link}
{kind=link}
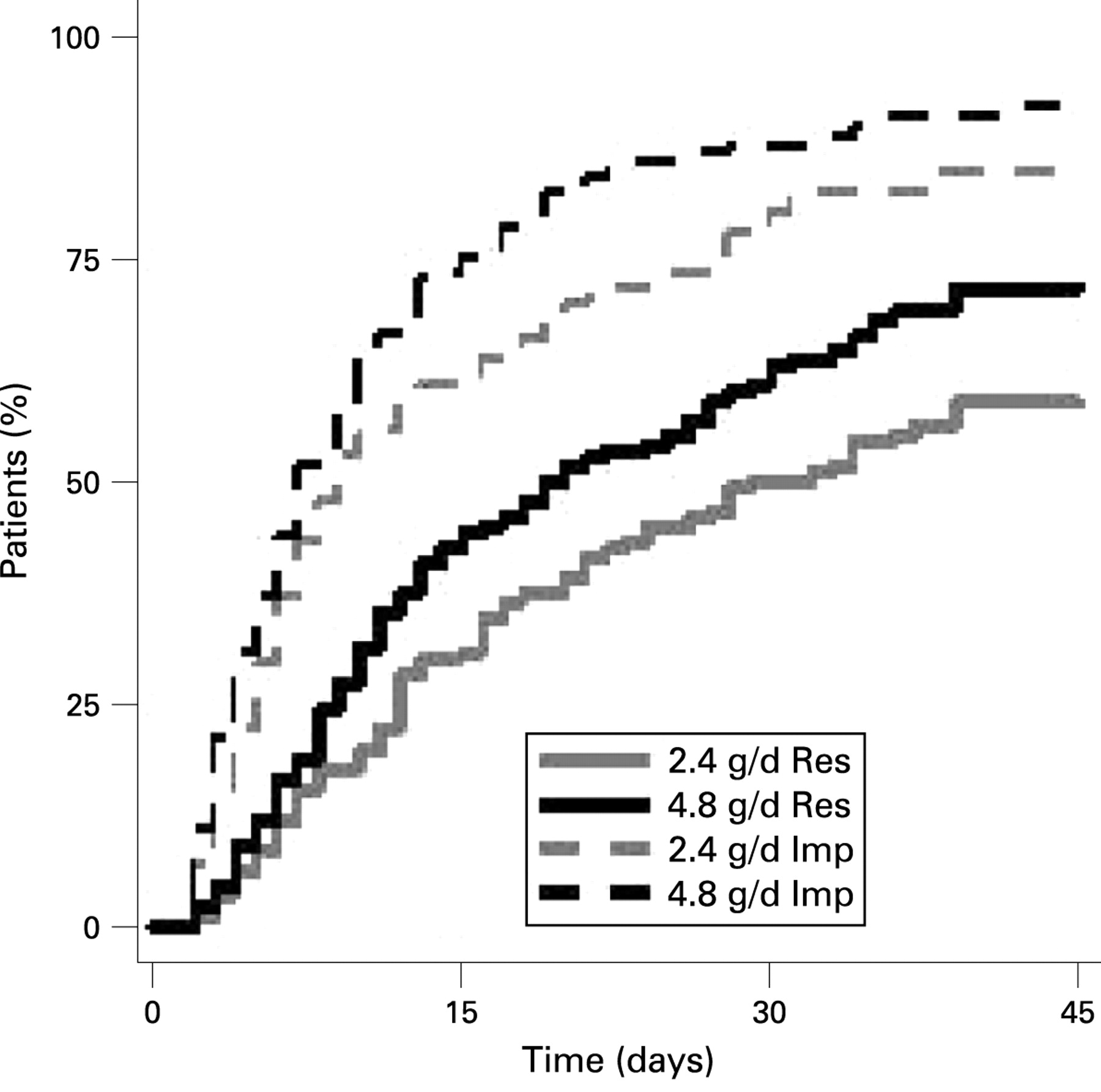{kind=link}
{kind=link}
Survival curve. DXT, radiotherapy; ETN, ethanol-induced tumour necrosis.
PT285 DNA PLOIDY AS A PROGNOSTIC BIOMARKER AFTER AMINOLEVULINIC ACID PHOTODYNAMIC THERAPY FOR HIGH-GRADE DYSPLASIA IN BARRETT’S OESOPHAGUS
1J. M. Dunn, 1G. D. Mackenzie, 2D. Oukrif, 1C. A. Mosse, 2S. Green, 2Y. Chew, 1S. Thorpe, 2M. Novelli, 1S. G. Bown, 3L. B. Lovat. 1National Medical Laser Centre, London, UK, 2Department of Histopathology, University College London, London, UK, 3Department of Gastroenterology, University College Hospital, London, UK
Introduction: Photodynamic therapy (PDT) is an approved minimally invasive treatment for high-grade dysplasia (HGD) in Barrett’s oesophagus. Complete reversal of HGD at one year post-therapy occurs in up to 90% of patients, but late relapse has been documented in 20%. DNA ploidy (aneuploidy/tetraploidy), as analysed by flow cytometry, is a strong predictor of future cancer risk in untreated Barrett’s oesophagus, independent of histology grade. Image cytometry is a simpler method that allows accurate evaluation of nuclear morphology on paraffin-embedded samples.
Aims and Methods: The aim of this study was to determine whether residual aneuploidy after successful treatment with aminolevulinic acid (ALA)-PDT predicts late relapse to HGD or cancer. 28 patients (82% men, mean age 66 years; range 45–86) treated with ALA-PDT for HGD in Barrett’s oesophagus between 1998 and 2006 were included in the analysis. HGD before treatment was confirmed on two separate occasions by two specialist gastrointestinal pathologists. Four quadrant biopsies were taken every 2 cm from the treated segment at 2, 4, 12, 18 and 24 months after PDT, then annually. All patients were clear of dysplasia at one year follow-up. DNA ploidy was analysed by image cytometry of monolayer preparations stained with Feulgen. 405 samples were analysed; 148 before PDT; 131 at 4 months post-PDT; 104 at one year post-PDT.
Results: 24 patients had aneuploidy before treatment. 11 of those remained aneuploid at one year post-PDT and nine of 11 have subsequently relapsed; five to invasive cancer and four to HGD. The median time to relapse was 30 months (range 14–64). 13 patients reverted to diploid at 4 months follow-up and remained diploid at one year. None have relapsed after a median 45-month follow-up (range 32–60 months; Fisher’s exact p<0.001). Four patients were diploid before treatment and two of four patients have relapsed, one to cancer (diploid throughout) and one to HGD (aneuploidy at one year). There was no significant difference in rates of aneuploidy within this small subset of patients.
Conclusion: Following successful PDT for HGD in Barrett’s oesophagus, patients who remain aneuploid are significantly more likely to develop HGD or cancer than those who become diploid. This may allow change in surveillance patterns to be tailored to the patient, with persistent aneuploidy one year post-PDT necessitating closer follow-up. Moreover, patients who have reverted to diploid after one year may return to 2-yearly follow-up and be reassured that the risk of cancer after 3 years is very low. These data demonstrate the utility of DNA ploidy as a prognostic biomarker following ablative therapy.
PT286 RADIOFREQUENCY ABLATION OF HIGH-GRADE DYSPLASIA IN BARRETT’S OESOPHAGUS AFTER FAILED PHOTODYNAMIC THERAPY: FIRST RESULTS OF THE UK HALO RADIOFREQUENCY ABLATION REGISTRY
1J. M. Dunn, 2G. Fullarton, 1S. Thorpe, 3M. Novelli, 1S. G. Bown, 4L. B. Lovat. 1National Medical Laser Centre, University College London, London, UK, 2Department of Surgery, Glasgow Royal Infirmary, Glasgow, UK, 3Department of Histopathology, University College London, London, UK, 4Department of Gastroenterology, University College Hospital, London, UK
Introduction: Photodynamic therapy (PDT) is an approved minimally invasive treatment for high-grade dysplasia (HGD) in Barrett’s oesophagus in the UK, but has a failure rate of between 15% and 50%. Radiofrequency ablation (RFA) is a new treatment for the eradication of non-dysplastic and dysplastic Barrett’s oesophagus. There are no studies of its use to eradicate residual HGD after failed PDT.
Aims and Methods: The aim of this prospective multicentre study was to assess the safety and efficacy of RFA for Barrett’s oesophagus with residual HGD following PDT. Ethical approval was obtained and all patients consented to be treated in the UK HALO Registry. 15 patients with residual HGD in Barrett’s oesophagus post-PDT (nine aminolevulinic acid (ALA), six Photofrin) were treated with RFA between April 2007 and October 2008. The presence of HGD was confirmed by two independent specialist gastrointestinal pathologists. All patients had endoscopic ultrasonography and endoscopic resection of any visible nodules before ablation. Patients received either circumferential balloon-based ablation (CA) or focal ablation (FA) every 3 months until there was no visible evidence of Barrett’s oesophagus or after three consecutive ablations. Four quadrant biopsies of the treated area were then taken.
Results: 30 ablations (18 CA, 12 FA) were carried out at two centres. The mean age was 66 years (range 50–83 years) and 80% were men. Median endoscopic Barrett’s oesophagus length post-PDT but pre-RFA was 5 cm (range 1–10 cm). Eight of 15 patients have completed treatment and are included in the analysis. Initial reversal of HGD was achieved in 88% (seven out of eight) with a median of two ablations (range one to five). The patient who failed had unifocal HGD in a nodule 2 months post-CA, which was completely excised by endoscopic resection. Complete reversal of intestinal metaplasia (IM) was achieved in 38%. Mean total follow-up is 10 months (range 2–14). Three patients with residual IM had recurrent low-grade dysplasia at the second follow-up endoscopy. This has been re-eradicated in one and the others are being retreated. Subsquamous IM was identified in one of eight patients (one of 141 follow-up biopsies). All patients were treated as day cases under conscious sedation. There was one overnight admission for minor bleeding from a hypopharyngeal abrasion, not requiring transfusion. One patient (failed ALA-PDT) developed a stricture post-RFA that was successfully dilated in one session.
Conclusion: This is the first report of the use of RFA for Barrett’s oesophagus in the UK. Preliminary data suggest that RFA is both safe and effective for the eradication of HGD in patients who have failed current standard minimally invasive therapy.
Finance: This work is supported by the CRUK Experimental Cancer Medicine Centre at UCL and the NIHR Comprehensive Biomedical Research Centre at University College Hospital, London.
PT287 ENDOSCOPIC MUCOSAL RESECTION FOR BARRETT’S HIGH-GRADE DYSPLASIA AND INTRAMUCOSAL CANCER: A TERTIARY CENTRE EXPERIENCE
J. Mannath, V. Subramanian, T. Thomas, P. V. Kaye, K. Ragunath. Nottingham Digestive Diseases Centre and Biomedical Research Unit, Queens Medical Centre, Nottingham University Hospital NHS Trust, Nottingham, UK
Introduction: Barrett’s oesophagus is a well-recognised precursor of oesophageal adenocarcinoma. Once high-grade dysplasia (HGD) or intramucosal cancer (IMC) is identified during surveillance, oesophagectomy has been the standard practice. In recent years endoscopic therapy with resection or ablation has become a viable alternative.
Aims and Methods: To determine the outcome of endoscopic mucosal resection (EMR) in terms of the eradication of dysplasia and complications. Electronic case records and endoscopy reports of all patients who underwent EMR since 2004 were analysed.
Results: 25 patients (56% men, mean age 67 years) with pretreatment diagnosis of HGD (21/25) or IMC (4/25) underwent EMR. Average length of Barrett’s segment; Prague criteria C 3 cm (0–13 cm) and M 4.7 cm (1–13 cm). 14 (56%) patients had short segment Barrett’s oesophagus (⩽3 cm). All patients had Paris type 0–II lesions with 17 having flat lesions (type 0–II B), seven with raised lesions (type 0–II A) and one with a depressed lesion (type 0–II C). High-resolution endoscopy supplemented with autofluorescence and narrow band imaging was used to identify the area and assist EMR resection. A multiband mucosectomy device (Duette, Wilson–Cook) was used in 17 (68%) cases and EMR-cap (Olympus) in the rest. Post-resection specimens showed IMC in 11 of 25 patients, confirmed HGD in nine of 25 patients, intestinal metaplasia only in three of 25 cases and submucosal invasive disease in two of 25. EMR upstaged the pretreatment diagnosis in 11 patients (44%) and downstaged it in three (12%). Two patients with submucosal invasive disease underwent oesophagectomy. Excluding the three patients with only intestinal metaplasia in the resection specimens, deep resection margins were clear in 20 (90%), involved with disease in two (1%) and uncertain in one (0.5%). Six patients (24%) underwent a second EMR for visible mucosal lesions (post-EMR histology IMC one, HGD two, low-grade dysplasia two). During a median follow up of 15 months (interquartile range 9–34) with a mean number of two (range none to four) endoscopies, none of the patients developed oesophageal cancer and complete remission was achieved in 21 of 23 patients (91%). Two patients had flat HGD on follow-up and are undergoing radio frequency ablation. Minor bleeding occurred during the procedure in five cases (20%), controlled by endoclips and argon plasma coagulation. No delayed complications were observed in any of the patients.
Conclusion: EMR is safe and effective in treating early neoplasia associated with Barrett’s oesophagus and helps in accurate local staging. It should be considered as an alternative to oesophagectomy. This series also highlights the importance of surveillance in short-segment Barrett’s oesophagus.
PT288 HIGH-RESOLUTION PH AND MANOMETRY CONFIRMS DISTAL OPENING OF THE LOWER OESOPHAGEAL SPHINCTER AFTER MEALS
J. P. Seenan, A. A. Wirz, A. T. Clarke, A. W. Kelman, K. E. L. McColl. Division of Medical Sciences, University of Glasgow, Glasgow, UK
Introduction: 30–50% of upper gastrointestinal tract adenocarcinomas occur at the gastro-oesophageal junction (GOJ) or gastric cardia. Unlike oesophageal adenocarcinoma, the association with reflux symptoms is weak. In studies using pull-through pH and manometry, we have observed loss of the distal lower oesophageal sphincter (LOS) with the pH step-up point moving closer to or even across the squamocolumnar junction (SCJ). This distal opening may explain the high incidence of GOJ pathology in asymptomatic individuals.
Aims and Methods: To investigate, using static high-resolution pH manometry, anatomical and physiological changes at the GOJ in normal individuals following a meal. 20 healthy volunteers (11 men) were studied. Each underwent endoscopy with clipping of a radio-opaque endoclip to the SCJ. On a separate day, high-resolution 12-sensor pH and 36-sensor manometry was performed during 15 minutes fasting and for 90 minutes following a standardised meal. A 10-s analysis period of stable sphincter tone (outwith sphincter relaxations) was selected during fasting and for the six consecutive 15-minute periods after the meal. The position of the proximal border of the high-pressure zone (HPZ; PHPZ), respiratory inversion point (RIP), pH step-up and distal border of the HPZ (DHPZ) was calculated for each time point. Videofluoroscopy was performed fasted and after the meal in 13 subjects. The location of the SCJ was determined using image analysis software and the measured distance of a pH sensor (1 cm) was used as a scale. Results are given as medians and ranges.
Results: Following the meal, there was no change in the position of the PHPZ relative to the nares; however, there was significant proximal movement of the DHPZ, a maximum 2.14 cm (−1.37–4.23, p<0.001). Sphincter length was reduced, a maximum 2.08 cm (−0.48–5.59, p<0.001). There was proximal movement of the RIP relative to the PHPZ, a maximum 1.09 cm (0–1.43, p<0.001). In addition, there was proximal movement of the pH step-up point relative to the PHPZ, a maximum 1.61 cm (−1.49–5.15, p<0.001). From the screening data, the DHPZ moved 1.72 cm (−0.37–2.93, p = 0.004) closer to the SCJ but there was no significant change in the position of the SCJ relative to the pH step-up point.
Conclusion: Distal opening of the LOS and proximal migration of the pH step-up point occurs after a meal. This may partly be mediated by proximal movement of the diaphragm. This mechanism may be important in the pathogenesis of disease at the GOJ.
PT289 STRONG CORRELATION BETWEEN SQUAMOCOLUMNAR JUNCTION POSITION AND AGE IN HEALTHY VOLUNTEERS
J. P. Seenan, A. A. Wirz, A. T. Clarke, A. W. Kelman, K. E. L. McColl. Division of Medical Sciences, University of Glasgow, Glasgow, UK
Introduction: The gastric cardia is an important site of pathology with a high incidence of inflammation, metaplasia and neoplasia. However, this complex area is poorly understood and it has been proposed that the cardia mucosa itself may be pathological, arising from columnar metaplasia of the distal oesophageal squamous mucosa. Previous autopsy studies show a near absence of cardia epithelium in neonates and an increase in length with age.
Aims and Methods: To determine if the position of the squamocolumnar junction (SCJ) within the lower oesophageal high-pressure zone (HPZ) changes with age in healthy individuals. 15 Helicobacter pylori-negative individuals (nine men) were studied. Each underwent upper gastrointestinal endoscopy with clipping of a radio-opaque endoclip at the SCJ. On a separate study day, synchronised 36 sensor high-resolution manometry and videofluoroscopy was performed with subjects fasted and in a semi-recumbent position. A 10-s analysis period of stable sphincter tone (outwith sphincter relaxations) was selected. The proximal HPZ was identified from manometry data as a step-down in pressure to the intrathoracic pressure. The location of the SCJ was determined using image analysis software with the measured distance of a pH sensor (known to be 1 cm) used as a scale. The distance between the position of the SCJ and the proximal HPZ was calculated for each individual.
Results: The median age of the subjects was 25 years (range 20–59). The median distance between the SCJ position and the proximal HPZ position for the group was 3.59 cm (range 0.31–4.46). There was a strong negative correlation between age and distance between the SCJ and proximal HPZ (r = −0.831, p<0.001) with the SCJ closer to the proximal HPZ with increasing age. The correlation was even stronger in men alone (r = −0.961, p<0.001). In multiple regression analysis the combination of both increasing age and body mass index was significantly associated with movement of the SCJ closer to the proximal HPZ (R2 = 73.6%, p<0.001) with a strong trend towards significance for both individual variables (p = 0.053 and p = 0.088, respectively).
Conclusion: The position of the SCJ relative to the proximal HPZ is strongly correlated to age in healthy subjects. This is consistent with proximal migration of the SCJ due to columnar metaplasia of the distal oesophageal squamous mucosa.
PT290 EOSINOPHILIC OESOPHAGITIS: GASTRO-OESOPHAGEAL REFLUX DISEASE INTERFACE
1K. Alexandropoulou, 2R. Ramakrishnan, 2H. Chong, 2C. Finlayson, 2N. Al Nasiri, 1A. Poullis, 1J. Kang. 1Gastroenterology, St George’s Hospital, London, UK, 2Pathology, St George’s Hospital, London, UK
Introduction: Eosinophilic oesophagitis (EOE) in adults presents with recurrent food bolus obstruction (FBO) and/or intermittent dysphagia. Eosinophil counts in oesophageal biopsies are much higher than normally found in reflux oesophagitis. Current guidelines require that gastro-oesophageal reflux disease (GORD) be excluded by normal pH monitoring of the distal oesophagus or lack of response to high-dose proton pump inhibitor (PPI) treatment.1 However, recent literature suggests that the two conditions can co-exist.2 We have therefore studied the prevalence of GORD in a series of patients with clinicopathological features of EOE.
Aims and Methods: Since 2005, patients presenting with FBO and/or dysphagia in St George’s Hospital, who had more than 20 eosinophils per high-power field (eo/HPF) in their oesophageal biopsies were offered oesophageal manometry and pH studies, off antisecretory treatment.
Results: Of 21 patients (19 men, three women) with EOE on histological criteria, 12 presented with FBO and nine with dysphagia. Four patients with dysphagia and one with FBO also had heartburn and another odynophagia. The median age at presentation was 38 years (range 18–55). Eosinophil counts ranged from 20 to 240 eo/HPF (median 40). 13 patients (11 men, two women) underwent oesophageal manometry and pH studies (five FBO, seven dysphagia). Manometry was abnormal in three patients (23%): low-amplitude lower oesophageal peristaltic waves in one case; diffuse oesophageal spasm in the second and poorly propagated low-amplitude waves in the third. Pathological acid reflux, defined as total oesophageal acid exposure (AET) to pH less than 4 for more than 4% of the time, was present in 10 patients (77%). Three patients had severe reflux (AET >11%), relatively low eosinophilic counts of less than 25 eo/HPF and endoscopic appearance of oesophagitis. Mild reflux (AET 4–11%) was present in seven other patients (median 62 eo/HPF). Only three patients had a normal pH study with AET less than 4% (one FBO, two dysphagia, median 40 eo/HPF). Eosinophil count, mode of presentation, presence of atopy or age at presentation could not predict the presence or severity of reflux. Five patients confirmed to have pathological reflux did not improve with standard-dose PPI treatment, but eight of nine patients, including one without reflux, improved markedly with high-dose PPI.
Conclusion: Ten of 13 patients (77%) presenting with FBO and/or dysphagia and who satisfied the histological criteria for the diagnosis of EOE had pathological gastro-oesophageal reflux. Patients with minimal or no reflux tended to have higher eosinophil counts compared with those with severe reflux. GORD may have an additive effect with EOE in causing FBO and dysphagia in susceptible patients.
Pancreas posters
PT291 BETA3-INTEGRIN DEFICIENCY IN BONE MARROW ENHANCES ANGIOGENESIS IN A MOUSE MODEL OF PANCREATIC CANCER
1A. R. Watson, 1S. Schier, 1N. A. Wright, 2K. M. Hodivala-Dilke. 1Histopathology Unit, Cancer Research, London, UK, 2Tumour Biology Laboratory, Queen Mary University of London, London, UK
Introduction: Angiogenesis—the development of new blood vessels—is vital for tumour growth and progression. Bone marrow-derived cells contribute to areas of tissue damage and repair and also to tumour stroma and blood vessels. Mice globally deficient in the cell adhesion molecule β3-integrin show increased tumour growth and increased pathological angiogenesis. Transplantation of bone marrow from β3-integrin null mice into mice that spontaneously develop pancreatic tumours enables the role of bone marrow β3-integrin deficiency in pancreatic cancer to be studied.
Aims and Methods: We aimed to study tumour frequency, size, vessel density and patency and to correlate this to survival. Recipient mice transgenic for the rat insulin promoter II gene linked to the large-T antigen of SV40 (RIPTag) develop solid β-cell tumours of the pancreas. Six to 8-week-old female RIPTag mice were irradiated to ablate the bone marrow and rescued with bone marrow from male, β3-integrin null, GFP+ donors. Control mice received transplants of male, β3-integrin wild type (WT), GFP+ bone marrow. Mice were killed and tumours harvested at 16 weeks of age or when ill. Pancreata were measured, weighed and examined for signs of macroscopic tumours, then fixed, embedded and sectioned. Tumour number, size and appearance was noted and blood vessel density, functionality and morphology was studied.
Results: Survival in β3-null-transplanted and WT transplanted groups was not affected; all mice survived to 16 weeks of age. Pancreatic weight was unaffected and was similar between groups. Very few macroscopic tumours were noted. Although there were similar numbers of microscopic tumours seen in each group, size-matched groups of tumours showed significantly increased blood vessel density in mice that had received β3-integrin null bone marrow transplantation (n = 15–22 tumours, p⩽0.05).
Conclusion: The absence of β3-integrin in bone marrow confers a pro-angiogenic phenotype in the RIPTag model of murine pancreatic cancer. Bone marrow β3-integrin status does not affect the number or size of tumours and does not affect survival. These results mirror our recent findings in subcutaneous xenograft models of tumour growth in β3-null bone marrow-transplanted mice. The likely mechanism is differential adhesion to, and mobilisation of, progenitor cells from the bone marrow niche. Ongoing work examines the contribution of bone marrow β3-integrin to the degree and distribution of engraftment of bone marrow-derived cells in RIPTag tumours.
PT292 RISK STRATIFICATION IN FAMILIAL PANCREATIC CANCER KINDREDS USING A MATHEMATICAL MODEL
1C. J. Grocock, 2A. Taktak, 2A. Eleuteri, 2F. Tortora, 1M. Harcus, 1L. Vitone, 1J. Butler, 1R. Sutton, 1M. Raraty, 1J. Neoptolemos, 1W. Greenhalf. 1School of Cancer Studies, The University of Liverpool, Liverpool, UK, 2Department of Clinical Engineering, Royal Liverpool University Hospital, Liverpool, UK
Introduction: Screening for pancreatic cancer is being trialled in high-risk groups. Improved risk stratification will increase the positive predictive value, minimise harm and reduce financial costs.
Aims and Methods: The aim was to create a mathematical model that would predict pancreatic cancer in high-risk individuals from familial pancreatic cancer (FPC) kindreds. Training and test sets were created from 1251 individuals (total affected 297) from 85 families with three or more pancreatic cancers. A hazard model was created and validated that estimated the likelihood of an individual belonging to a high-risk family, being a gene carrier and developing cancer within fixed periods. Results were tested with Hosmer–Lemeshow statistics and Harrell’s C index (modified receiver operator characteristic; ROC). An internet-compatible interface was developed and used to enter data for 138 individuals from high-risk families, as if it were the year 2000, to see if the model could detect a difference between those who subsequently developed pancreatic cancer.
Results: The model was accurate in terms of both discrimination (area under the curve 0.72; 95% CI 0.68 to 0.76) and calibration (no significant difference between estimated and observed events, eg, at 60–64 years p = 0.935, (ideal p = 1.0), goodness of fit: χ2 = 0.83). Discrimination points from ROC analysis would have allowed screening to be avoided in 23 of 138 individuals. All 27 pseudoprospective cancers would have fallen within the screened group, with none missed.
Conclusion: This is the most in-depth work on risk stratification in FPC so far. The model gives an individual probability of developing cancer within a set period and the online user interface permits registered clinicians to enter patient data and perform the probability calculation during a consultation. It has roles in both patient counselling and the selection of high-risk individuals for secondary screening. As secondary screening progresses, it will be possible to calculate values at which screening is clinically justifiable and cost effective.
PT293 CEREBRAL INVOLVEMENT IN AUTOIMMUNE PANCREATITIS/IGG4 SYSTEMIC DISEASE
1G. J. Webster, 2R. Jager, 3S. Hurel, 3S. Damodharan, 1S. Pereira, 4A. Winstanley, 4M. Deheregoda, 2N. Losseff. 1Gastroenterology, University College Hospital, London, UK, 2Neurology, National Hospital Queen Square, London, UK, 3Endocrinology, University College Hospital, London, UK, 4Histopathology, University College Hospital, London, UK
Introduction: Autoimmune pancreatitis (AIP) is a chronic inflammatory disease, characterised by raised serum IgG4 levels and pancreatic features that may mimick malignancy. Extrapancreatic involvement may occur in more than 50% of cases, especially biliary disease, with an IgG4+ lymphoplasmacytic infiltrate in affected organs. Several individual cases of cerebral/pituitary disease in AIP have been reported in the world literature.1 2 We investigated the presence of cerebral disease in our patient group.
Aims and Methods: All patients referred from 2004 to 2008 to our unit, in whom a diagnosis of AIP was made (according to established criteria), were followed prospectively. Oral steroid therapy was given for active disease. Neurological investigations were performed in those patients with overt symptoms or clinical problems suggestive of possible cerebral involvement.
Results: A new diagnosis of AIP was made in 34 patients over the study period. All were treated with a course of steroids. Clinical cerebral disease was identified in two of 34 (6%) patients. Case 1: 67-year-old man who had undergone biliary bypass for presumed pancreatic cancer, with subsequent sclerosing cholangitis, raised serum IgG4, and IgG4+ plasma cell infiltrate on liver biopsy (which showed cirrhosis). Excellent response to steroids (with control of hepatic, pancreatic and biliary disease), but on withdrawal developed profound fatigue and hypotension, with hormone profile confirming panhypopituitarism. Computed tomography (CT) and magnetic resonance imaging (MRI) showed pituitary mass. Resolution of mass, hormone imbalance and symptoms with further immunosuppression and hormone replacement. Patient remains well on maintenance prednisolone and azathioprine. Case 2: 56-year-old man with diffuse pancreatic enlargement, sclerosing cholangitis, raised serum IgG4 and IgG4+ plasma cell infiltrate in salivary gland. Excellent response to steroids. Confusion and precoma developed on low-dose steroid, with CT, gadolinium MRI, EEG and neurological assessment consistent with “autoimmune encephalopathy”.
Conclusion: Data show that cerebral disease may occur as an extrapancreatic feature of AIP and can occur independent of activity of pancreaticobiliary disease. A skewed referral population make interpretation of frequency of cerebral disease in AIP unreliable. Findings reinforce the multisystem nature of the disease, the need for a better term than autoimmune pancreatitis (eg, IgG4 systemic disease) and the importance of maintaining clinical awareness of its myriad clinical manifestations.
PT294 VITAMIN D STATUS IN CHRONIC PANCREATITIS
1N. Prasad, 2P. L. Selby, 1A. J. Makin. 1Gastroenterology, Manchester Royal Infirmary, Manchester, UK, 2Medicine, Manchester Royal Infirmary, Manchester, UK
Introduction: Chronic pancreatitis (CP) is associated with exocrine deficiency and malabsorption of fats and proteins. This may lead to deficiency of fat-soluble vitamins such as vitamin D, which has effects on bone and calcium metabolism. The extent of this is well documented in cystic fibrosis patients but there remains a relative paucity of information on CP in the literature.
Aims and Methods: Our objective was to assess the extent and severity of vitamin D deficiency in our cohort of patients with CP. We included 111 CP patients attending the gastroenterology clinic. Retrospective data were gathered on demographics, aetiology, disease classification, presence of endocrine deficiency, vitamin D studies, serum calcium and parathyroid hormone (PTH) assay. Pancreatic exocrine function was evaluated using the PABA test to obtain a pancreatic excretion index (PEI: normal >0.7) and by faecal elastase-1 (FE1: normal >200 μg/g).
Results: 85 patients were men (76.6%) with a median age of 49 years (range 14–79). Alcohol was the most common aetiology, being the cause in 54 patients (49%). Idiopathic pancreatitis had been diagnosed in 13 patients (12%) but a further 27% did not have a specific cause documented and were also likely to be idiopathic. The remaining 12% were due to obstructive, metabolic, genetic and autoimmune causes. 89 (80%) patients had chronic calcific, six (6%) had non-calcific and seven (6%) had recurrent acute pancreatitis. Nine (8%) patients were not classified. PEI was abnormal in 97 (88.2%) patients and, when available, FE1 was low in 44 of 49 patients (89.8%). All patients had normal serum calcium but PTH was elevated in 20.0%. 25-hydroxy-vitamin-D3 (25OHD) levels were graded as deficient (<10 ng/ml), insufficient (10–20 ng/ml), suboptimal (20–30 ng/ml) and normal (>30 ng/ml), with 49.5%, 32.4%, 11.7% and 5.4% in these groups, respectively. 25OHD was not linked to the 1,25-(hydroxy)2-vitamin-D level. Male patients had significantly lower mean 25OHD levels than women (11.5 vs 15.9, p = 0.05). Alcohol aetiology was associated with a lower mean 25OHD compared with other causes (10.6 vs 16.8, p = 0.01). There was no difference in 25OHD levels between patients with calcific, non-calcific and recurrent acute disease. The presence of endocrine deficiency was not related to lower 25OHD (p = 0.45). There was a poor correlation of 25OHD with age (r = ∧0.01), PEI (r = 0.19) and FE1 (r = 0.01) but there was a weak correlation with PTH levels (r = −0.40, p = 0.02).
Conclusion: Disturbance of vitamin D status in CP is very common. In our cohort, 94.6% had abnormal 25OHD levels and almost half had severe deficiency. Alcohol aetiology and male sex were significant risk factors, but the 25OHD level was not linked to the classification of CP, PEI, FE1 or the presence of diabetes. There is a weak negative association of 25OHD and PTH, which may reflect disordered calcium and bone metabolism. Further studies are required to evaluate the effects of vitamin D deficiency on bone mineral density and the long-term fracture risk among CP patients.
PT295 IDIOPATHIC PANCREATITIS: IS IT A CONSEQUENCE OF AN ALTERING SPECTRUM OF BILE NUCLEATION TIME?
1V. Abeysuriya, 2K. I. Deen, 3N. M. M. Navaratne, 2S. K. Kumarage. 1Clinical Anatomy, Faculty of Medicine, Ragama, Sri Lanka, 2Surgery, Faculty of Medicine, Ragama, Sri Lanka, 3Gastroenterology, National Hospital of Sri lanka, Colombo, Sri Lanka
Introduction: The pathogenesis of idiopathic pancreatitis (IP) remains poorly understood. Our hypothesis is that IP is a sequel of the microcrystallisation of hepatic bile.
Aims and Methods: A prospective case–control study compared 55 patients (symptomatic cholelithiasis, 30: 14 men, 16 women, median age 36 years, body mass index (BMI) 25.1 ± 0.33 kg/m2; gallstone pancreatitis, nine: six women, three men, median age 35 years, BMI 24.86 ± 0.23 kg/m2; and idiopathic pancreatitis, 16: seven women, nine men, median age 34 years, BMI 23.34 ± 0.2 kg/m2) with 30 controls (15 men, 15 women, median age 38 years, BMI 24.5 ± 0.23 kg/m2, undergoing laparotomy and who had normal gallbladder and no demonstrable stones on ultrasonography). Ultrafiltered bile from the common hepatic duct in patients and controls was anaerobically incubated and examined by polarised light microscopy, for nucleation time (NT). Ethical approval was obtained.
Results: Patients were similar to controls. Mean NT in all groups of patients was significantly shorter than controls (established gallstones cumulative mean NT, 1.73 ± 0.2 vs controls, 12.74 ± 0.4 days vs, p = 0.001, t test and IP patients mean NT, 3.1 ± 0.24 days vs controls, 12.74 ± 0.4 days, p = 0.001, t test). However, NT in those with IP was significantly longer compared with those with established gallstones (mean NT in IP, 3.1 ± 0.24 SEM days, vs cumulative mean in patients with established symptomatic gallstones, 1.73 ± 0.2 days, p = 0.002, t test).
Conclusion: NT in bile in patients with IP is abnormal and is intermediate in NT of lithogenic and non-lithogenic bile.
Small bowel posters
PT296 SMALL BOWEL STRICTURE DILATATION BY DOUBLE BALLOON ENTEROSCOPY: EXPANDING THE EXPERIENCE
1E. J. Despott, 1E. Tripoli, 1A. Polecina, 2K. Konieczko, 1C. Fraser. 1The Wolfson Unit for Endoscopy, St Mark’s Hospital, Imperial College, London, UK, 2Department of Anaesthesia, St Mark’s Hospital, Imperial College, London, UK
Introduction: Double balloon enteroscopy (DBE) facilitates the endotherapy of deep small bowel pathology. Our preliminary prospective proof of concept analysis on DBE dilatation of Crohn’s disease (CD) small bowel strictures was presented to the British Society of Gastroenterology Annual Meeting in 2008. We now report further on our prospective data of DBE stricture dilatation in an expanding cohort of patients with CD and non-steroidal anti-inflammatory drug (NSAID)-induced small bowel strictures.
Aims and Methods: Since the introduction of DBE to our unit in 2005, data on cases of DBE small bowel stricture dilatation were prospectively collected for outcome, the need for repeat dilatation and surgery. The DBE were performed using the EN-450T5 scope (Fujinon, Saitama, Japan). Balloon dilatation was performed using controlled radial expansion balloon dilators (Boston Scientific, Massachusetts, USA). A standardised 10 cm visual analogue scale (VAS) characterised symptoms and dietary restriction before DBE stricture dilatation and at follow-up.
Results: A total of 14 DBE were done in 12 consecutive cases (mean age 46.4 ± 7.8 years). In all but two cases, the strictures were characterised radiologically before DBE. In 11 of the cases, the small bowel strictures were CD related, in one case they were NSAID induced. Twenty-six small bowel stricture dilatations were performed in 10 of 12 patients. The patient with NSAID-related strictures had successful dilatation of eight strictures in one session. In another case of CD small bowel strictures, a retained video capsule was retrieved after dilatation of the culprit strictures. Mean stricture dilatation diameter was 14.5 mm (range 12–20 mm). In the two cases in which stricture dilatation was not performed, DBE hindrance by adhesions made reaching the strictures impossible. These two cases were then managed surgically. One case of complex CD stricture dilatation was complicated by a delayed perforation. This case required a temporary jejunostomy, which has since been reversed. In the other 10 cases small bowel stricture dilatation by DBE was a success; the symptom and dietary restriction scores improved dramatically and to date (mean follow-up 19.4 months, range 1–40) none of these cases has required surgery for small bowel strictures. During follow-up, two patients required a repeat straightforward DBE dilatation (at 6.5 and 13 months, respectively) due to the recurrence of some of their symptoms. Although the numbers in this series are small, the clinical improvements in pre and post-DBE VAS scores were large enough (means of 9.2 vs 1.7, respectively; p<0.001).
Conclusion: This series adds to the small body of evidence that DBE small bowel stricture dilatation can be very effective, with the potential to help avoid the risks of surgery, small bowel resection and the associated risks of short bowel syndrome.
PT297 SMALL BOWEL POLYPECTOMY BY DOUBLE BALLOON ENTEROSCOPY: ADVANCING ENDOSCOPIC THERAPY FOR PATIENTS WITH PEUTZ–JEGHER’S SYNDROME
1E. J. Despott, 2R. Phillips, 2S. Clark, 1A. Postgate, 1A. Fitzpatrick, 1E. Tripoli, 3K. Konieczko, 1C. Fraser. 1The Wolfson Unit for Endoscopy, London, UK, 2National Polyposis Registry, London, UK, 3Department of Anaesthesia, St Mark’s Hospital, Imperial College, London, UK
Introduction: Small bowel obstruction and gastrointestinal bleeding due to polyps are major causes of morbidity in patients with Peutz–Jegher’s syndrome (PJS). Before double balloon enteroscopy (DBE), a technique that allows complete enteroscopy, the main therapeutic option available for PJS patients was laparotomy with intra-operative enteroscopy (IOE). We report our experience of the endoscopic management by DBE of small bowel polyps in the largest cohort of PJS patients from the UK.
Aims and Methods: Data on PJS cases managed by DBE at St Mark’s since 2005 were prospectively collected. Patients deemed to have significant small bowel polyps (>15 mm), at capsule endoscopy or magnetic resonance enterography or both, were referred for elective DBE polypectomy. DBE procedures were performed under general anaesthetic. In one case, an emergency DBE was performed in the setting of small bowel obstruction due to polyp-induced intussusception. All patients remain under follow-up and surveillance.
Results: Nine patients (mean age 34 years, range 16–45) underwent 13 DBE procedures (three patients had two DBE). Although all patients had previous laparotomies (some multiple), adhesions did not cause significant hindrance to DBE. On average three polyps were removed per patient (mean size 18 mm, range 8–37). Polyp stalks were injected with lifting solution (dilute adrenaline and methylene blue) with additional endolooping on occasion before snaring to reduce bleeding risk. Sessile polyps were elevated with lifting solution to minimise perforation risk. One patient required three DBE procedures, one of which was laparoscopically assisted for a sessile distal duodenal polyp; one patient had a small post-polypectomy bleed that settled spontaneously and one patient, in whom an emergency DBE was attempted, polypectomy of a sessile 30 mm polyp led to perforation with conversion to IOE through the defect.
Conclusion: We highlight the role of DBE as an emerging therapeutic option for small bowel polyps in PJS that avoids the need for laparotomy and prolonged recovery; however, experienced surgical cover should always be available for this complex group of patients in view of the risk of potential complications.
PT298 TROUBLED TRABECULAE: OSTEOPOROSIS AND OSTEOPENIA IN COELIAC DISEASE AT OXFORD
1J. B. Canavan, 1P. Trivedi, 1A. A. Bailey, 2M. K. Javaid, 1S. Keshav, 1S. P. L. Travis. 1Gastroenterology Unit, John Radcliffe Hospital, Oxford, UK, 2Botnar Research Centre, University of Oxford, Oxford, UK
Introduction: Coeliac disease is a well-recognised risk factor for osteopenia and osteoporosis, but factors influencing changes in bone mineral density (BMD) following diagnosis are little understood.
Aims and Methods: The aim of this retrospective study was to identify factors associated with change in BMD over time in coeliac disease. Patients with biopsy-confirmed gluten-sensitive enteropathy and two or more subsequent dual-energy x ray absorptiometry (DEXA) scans were included. Data were acquired from a review of medical notes and laboratory records. Dietary adherence was assessed from dietetic records and/or negative endomysial antibody (EMA) serology. Positive EMA serology was categorised as poor compliance. We defined osteopaenia and osteoporosis according to World Health Organization definitions. Logistic regression analysis was performed and continuous variables were presented as median (interquartile range).
Results: 121 patients were included, 100 (83%) women, reflecting the number of DEXA scans in women with a perceived risk of osteoporosis. The median age at diagnosis was 44 years (34–57), with median symptom duration before presentation of 1.25 years (0.5–5) and median follow-up 10.9 years (6.9–16.9). The most frequent modes of presentation were anaemia (56%), diarrhoea (52%) and weight loss (21%). A positive family history of coeliac disease was present in 21%; 13% with a first-degree relative. 48 (40%) had osteopenia and 21 (17%) had osteoporosis at first DEXA scan. The median interval between the first and last DEXA scans was 5.4 years (3.9–6.5). 66% had more than one and 34% more than two risk factors for fracture related to low BMD. Age at scanning was an independent risk factor for reduced BMD at first DEXA (p = 0.002), whereas increasing body mass index was protective (p = 0.03). 92 (76%) had good dietary adherence during follow-up. Good dietary adherence (p = 0.006) and bisphosphonate prescription after first DEXA (p = 0.03) were independently associated with an improvement in BMD. Indeed, good dietary adherence was the strongest predictor of an increase in BMD of greater than 1% per annum, or above the 75th centile; odds ratio 11.5 (95% CI 1.4 to 94.2) p = 0.03. By the end of follow-up, 91% with osteopenia were appropriately taking calcium/vitamin D supplements and 86% with osteoporosis were on bisphosphonates.
Conclusion: Good adherence to a gluten-free diet and appropriate prescribing of bone-protecting medicines may not only maintain, but also improve, BMD in patients with coeliac disease.
PT299 CAPSULE ENDOSCOPY FOR OBSCURE GASTROINTESTINAL BLEEDING: THE LEEDS EXPERIENCE
J. S. R. Jennings, S. M. Everett. Gastroenterology, Leeds Teaching Hospital NHS Trust, Leeds, UK
Introduction: Capsule endoscopy (CE) plays an established role in the investigation of obscure gastrointestinal bleeding (OGB), small bowel Crohn’s disease, coeliac disease and the surveillance of familial polyposis syndromes. A meta-analysis identified a diagnostic yield of 63% for CE in patients with OGB.1 CE has been shown to be superior to push enteroscopy, barium follow through and computed tomography (CT) enteroclysis in OGB. The rate of rebleeding in patients with a negative CE is much lower than in those with a diagnostic CE.2 British Society of Gastroenterology (BSG) guidelines support the use of CE in patients with OGB after a negative gastroscopy and colonoscopy.3
Aims and Methods: We examined what effect the new BSG guidelines would have on our diagnostic service for OGB. A prospective database of patients undergoing CE has been kept at the Leeds General Infirmary since October 2003. The CE system was purchased from Given Imaging Ltd and images were analysed using Rapid 5 software. We looked at the characteristics of patients with OGB, the drug history, previous investigations and pathology detection rates.
Results: A total of 194 procedures was performed with 43% in men and a mean age of 50 years. 131 (67.5%) cases were for recurrent anaemia with OGB. In suspected OGB, eight (6.1%) described a single visible bleed, 39 (29.8%) recurrent bleeding episodes, 11 (8.4%) were iron dependent and 20 (15.3%) transfusion dependent. The following drug histories were obtained: warfarin 15 (11.5%); anti-platelet agents 18 (13.7%); non-steroidal anti-inflammatory drugs 10 (7.6%). Before CE the following negative diagnostic tests had been performed: colonoscopy 128 (97.7%); gastroscopy 128 (97.7%); barium follow through 90 (68.7%); push enteroscopy 28 (21.4%); Meckle’s scan 19 (14.5%); mesenteric angiogram 10 (7.6%); red blood cell scan 2 (1.5%); double balloon enteroscopy 1 (0.8%); laparoscopy 1 (0.8%); CT/magnetic resonance imaging 7 (5.3%). Overall for OGB, CE was normal in 37 (28.2%), it demonstrated a vascular abnormality in 55 (42.0%) and mucosal disease in 20 (15.3%).
Conclusion: The detection rate for CE in our OGB series was 71.8%. If the new BSG guidelines had been available then a considerable number of invasive procedures could have been avoided. This has clear implications for cost, time to diagnosis and safety.
PT300 A 4-YEAR EXPERIENCE WITH COLESEVELAM HYDROCHLORIDE: A NEW TREATMENT FOR BILE ACID MALABSORPTION?
1L. Wedlake, 2K. Thomas, 3A. Lalji, 4C. Anagnostopoulos, 3J. Andreyev. 1Dietetics, Royal Marsden Hospital, London, UK, 2Statistics, Royal Marsden Hospital, London, UK, 3Gastrointestinal Unit, Royal Marsden Hospital, London, UK, 4Nuclear Medicine, Chelsea and Westminster Hospital, London, UK
Introduction: Currently available bile acid sequestrants are frequently poorly tolerated by patients.
Aims and Methods: To describe the 4-year experience of using colesevelam hydrochloride, a newly available bile binder, in patients with bile acid malabsorption intolerant of, unresponsive to, or unsuitable for, treatment with colestyramine and in whom other causes of symptoms had been defined. Review of hospital notes and data obtained from a questionnaire sent to surviving patients were used to assess outcomes.
Results: Eight men, 38 women, median age 58 years (range 20–89) with bile acid malabsorption treated with colesevelam were identified. 67% had previously not responded to colestyramine. Symptom improvement following colesevelam treatment included diarrhoea (86% (notes)/80% (patient assessment)), frequency of defaecation (77%/83%), urgency of defaecation (76%/80%), steatorrhoea (76%/80%), faecal incontinence (69%/74%) and abdominal pain (74%/58%). Six patients stopped taking colesevelam because it was ineffective, three for side effects, seven for other reasons. 65% of patients have continued long-term colesevelam.
Conclusion: In this retrospective study, colesevelam appears to be a very useful new therapy for bile acid malabsorption and was often effective in patients who had failed treatment with colestyramine. Prospective studies are warranted.
PT301 CLINICOPATHOLOGICAL CORRELATION OF CLASSIC GASTROINTESTINAL AND ATYPICAL NON-GASTROINTESTINAL PRESENTATIONS OF COELIAC DISEASE
1J. H. Topping, 1V. Verma, 2C. Bloxham, 3M. R. Novelli, 1A. Dhar. 1Gastroenterology, Bishop Auckland General Hospital, Bishop Auckland, UK, 2Pathology, County Durham and Darlington NHS Foundation Trust, Durham, UK, 3Histopathology, University College London Hospitals NHS Foundation Trust, London, UK
Introduction: The epidemiological presentation of coeliac disease is changing, and we have previously presented to this society the changing epidemiology with the predominance of atypical non-gastrointestinal manifestations of coeliac disease (Gut 2006). The histological appearances of atypical/non-gastrointestinal coeliac disease are presumed to be milder than classic gastrointestinal coeliac disease but there is little literature about the Marsh grading of these presentations.
Aims and Methods: The aim of this study was to correlate the histological Marsh grading of coeliac disease in South Durham presenting with typical gastrointestinal and non-gastrointestinal symptoms. This was aimed to test the hypothesis that non-gastrointestinal coeliac disease has a milder histology and the typical subtotal or total villous atrophy patterns of classic coeliac disease may not be seen. The South of Durham coeliac database was used to carry out a retrospective case note study of patients between 2001 and 2004. Histology slides of these patients were retrieved and coded for a blinded review by two experienced gastrointestinal pathologists. Biopsies were graded according to the modified Marsh grading. Any discordance in grading between pathologists was resolved in favour of the higher grade. The clinical presentation was then correlated to the Marsh grade.
Results: 87 patients with a final diagnosis of coeliac disease were studied. The mean age at diagnosis was 51 years, with 69% of patients being women. Endomysial antibody (EmA) positivity was 80%, 15% patients were EmA negative and 5% had no serology. Common atypical manifestations were iron deficiency anaemia, osteoporosis, menstrual irregularities, infertility, recurrent miscarriage, anxiety and depression. The commonest Marsh grade overall was IIIb (37%). 23% of EmA-negative patients had Marsh grade I. In patients presenting with gastrointestinal symptoms alone, no patients had either Marsh grade I or II histology, whereas almost a third of patients presenting with non-gastrointestinal/atypical symptoms alone showed Marsh grade I (7%) or II (21%) histology, p = 0.02 by χ2.
Conclusion: We conclude that patients with atypical non-gastrointestinal manifestations of coeliac disease have a milder Marsh grade on duodenal histology. Diagnosis may therefore be difficult and requires specialist pathologist expertise. Patients who had predominantly gastrointestinal symptoms had a more severe Marsh grade on histology (the mildest grading in this group being IIIa) and are easier to diagnose.
PT302 WHAT ARE THE IMPLICATIONS OF NEWLY IDENTIFIED COELIAC DISEASE IN ADULT PATIENTS WITH TYPE 1 DIABETES MELLITUS? EFFECT UPON GLYCAEMIC CONTROL, QUALITY OF LIFE, CARDIAC RISK FACTORS, ALBUMINURIA AND PERIPHERAL NERVE FUNCTION
1J. S. Leeds, 1A. D. Hopper, 2M. Hadjivassiliou, 3S. Tesfaye, 1D. S. Sanders. 1Gastroenterology and Liver Unit, Royal Hallamshire Hospital, Sheffield, UK, 2Neurology, Royal Hallamshire Hospital, Sheffield, UK, 3Diabetes, Royal Hallamshire Hospital, Sheffield, UK
Introduction: The effect of undetected coeliac disease (CD) on adults with type 1 diabetes (DM) is unknown. Our previous study (n = 1000) diagnosed 12 new cases of CD (CDDM). We prospectively assessed glycaemic control, quality of life, cardiac risk factors, renal function and peripheral neural function on these individuals and made comparisons against age and sex-matched controls with type 1 diabetes. All participants were re-assessed at 12 months and the impact of a gluten-free diet (GFD) on the CDDM patients was determined.
Aims and Methods: The CDDM patients (n = 12) were matched with patients having type 1 diabetes alone (controls from the initial 1000 cohort). Haemoglobin A1c (HbA1c), short-form 36 (version 2) (SF-36v2), urinary albumin/creatinine ratio, lipid profile and peripheral nerve function were assessed at baseline and one year following a GFD.
Results: At baseline, median HbA1c was 8.5% in CDDM patients versus 7.3% in controls (p<0.001) and median albumin/creatinine ratios were 1.8 in CDDM patients versus 0.4 in controls (p = 0.027). There were no significant differences in quality of life or lipid profile at baseline but radial and common peroneal nerve conduction velocities were significantly reduced in those with CDDM compared with controls (p = 0.007 and p = 0.0001, respectively). In those with CDDM following one year on a GFD, median HbA1c changed from 8.2% to 8.6% (p = 0.45) and SF-36v2 scores did not differ significantly. There were no significant changes in total cholesterol or triglycerides but the cholesterol/high-density lipoprotein (HDL) ratio decreased from 3.7 to 3.2 (p = 0.033). The median albumin/creatinine ratio reduced from 1.8 to 1.2 (p = 0.11). Peripheral nerve function is still being reassessed.
Conclusion: Undetected CD has an adverse effect on glycaemic control, renal protein loss and peripheral nerve function but not quality of life or lipid profile. Following treatment with a GFD, glycaemic control, quality of life and renal protein loss are unaltered but HDL cholesterol improves. Longer follow-up is required in this group of patients.
PT303 ARE THYROID PEROXIDASE ANTIBODIES HELPFUL IN PREDICTING THYROID DISEASE IN PATIENTS WITH ADULT COELIAC DISEASE? THE LARGEST PROSPECTIVE LONGITUDINAL STUDY
J. S. Leeds, A. J. Ball, R. C. Bunn, D. S. Sanders. Gastroenterology and Liver Unit, Royal Hallamshire Hospital, Sheffield, UK
Introduction: The association between coeliac disease (CD) and autoimmune thyroid disease is described. Screening using thyroid peroxidase antibodies (TPO) has not been established in CD. We assessed the value of TPO and its predictive value for thyroid disease in CD patients.
Aims and Methods: Patients were recruited from the specialist coeliac clinic. Demographic details, current thyroid status (including TPO level), duration of both CD and thyroid disease were recorded. Compliance was measured using tissue-transglutaminase antibodies. Non-CD controls were also recruited.
Results: 414 CD patients (mean age 53.3 years, 110 men, median duration 6 years) and 41 controls (mean age 54.4 years, 12 men) were included. 95 of 414 (22.9%) CD patients were TPO positive compared with three of 41 (7.3%) controls (odds ratio (OR) 3.9, p = 0.01); however, 73 of 414 (17.6%) CD patients had thyroid disease compared with four of 41 (9.8%) controls (OR 1.9, p = 0.27). Of the 73 patients, 52 had thyroid disease (34 TPO positive) at diagnosis of CD, whereas 21 developed thyroid disease (nine TPO positive) during follow-up. TPO positivity was associated with an increased risk of having thyroid disease overall (OR 7.9, 95% CI 4.6 to 13.8, p<0.0001) and developing thyroid disease during follow-up (OR 4.2, 95% CI 1.7 to 10.4, p = 0.003). Women were more likely to be TPO positive (OR 1.7, 95% CI 0.9 to 3.1, p = 0.055). The tissue-transglutaminase titre was not associated with TPO positivity or thyroid disease. There was no difference in duration of CD in patients who developed thyroid disease during follow-up compared with euthyroid patients. On multivariable analysis only TPO was an independent predictor of thyroid disease (OR 2.8, 95% CI 2.3 to 3.7, p<0.001).
Conclusion: TPO positivity is more frequent in CD patients than controls. TPO positivity is associated with an increased risk of thyroid disease at diagnosis and during follow-up. Measurement of TPO in CD would identify those at higher risk of thyroid disease.
PT304 EXPRESSION OF SMALL INTESTINAL ANTIMICROBIAL GENES IN ZAMBIAN ADULTS: A RANDOMISED CONTROLLED TRIAL OF MICRONUTRIENT SUPPLEMENTATION
1P. Kelly, 1W. Dhaliwal, 2T. Shawa, 1I. Sanderson. 1Institute of Cell and Molecular Science, Barts and The London School of Medicine, London, UK, 2TROPGAN, University of Zambia School of Medicine, Lusaka, Zambia
Introduction: Diarrhoeal disease remains a major contributor to morbidity and mortality in Africa, and evidence suggests that micronutrient supplementation confers protection. In order to test the hypothesis that one mechanism of an effect could be on innate immunity in the gut, we carried out a randomised controlled trial of multiple micronutrient supplementation in adults living in a population in which there is evidence of borderline micronutrient deficiency.
Aims and Methods: All consenting adults living in a carefully defined residential area in Lusaka, Zambia, were included. There were no exclusion criteria. Participants were cluster-randomly assigned to a supplement containing 15 micronutrients at around the recommended nutrient intake in the form of a daily tablet, or placebo. Treatment allocation was crossed over at the mid-point. Small intestinal biopsies were taken at approximately annual intervals and messenger RNA of the intestinal Paneth cell defensins HD5 and HD6, epithelial human beta defensins 1 and 2 (hBD1, hBD2) and the cathelicidin LL-37 were quantified by real-time reverse transcriptase PCR. In addition, mRNA was compared during diarrhoea episodes and after convalescence.
Results: mRNA was quantified in 511 biopsies from 287 participants. There was no difference in mRNA transcripts for any of the five genes between micronutrient supplementation and placebo groups. However, in malnourished adults (body mass index <18.5 kg/m2), HD5 mRNA was increased from 3.0 log transcripts/μg total RNA in placebo recipients to 3.8 log transcripts (p = 0.007) and hBD1 was increased in HIV-negative participants only (p = 0.01). During diarrhoea, HD5 expression was reduced by 0.8 log transcripts/μg total RNA in placebo recipients (p = 0.02), but this effect was not seen in supplement recipients, nor was it seen after the cross-over. In further exploratory analysis, sex-specific correlations between HD5 and nutritional status were found that included serum leptin.
Conclusion: Although the trial showed no benefit overall, micronutrient supplementation was associated with the upregulation solely of HD5 in malnourished adults. We also found sex-dependent interactions between antimicrobial gene expression and nutritional status, which could be of wider interest in understanding innate immunity in the gut, especially as leptin has recently been identified as a Paneth cell product upregulated by the Crohn’s disease mutation in the gene ATG16L1.
PT305 PROGNOSTIC FACTORS IN GASTROENTEROPANCREATIC NEUROENDOCRINE TUMOURS
R. Srirajaskanthan, C. Toumpanakis, B. Warner, S. Sundaram, K. Desai, M. Caplin. Centre of Gastroenterology, Royal Free Hospital, London, UK
Introduction: Gastroenteropancreatic neuroendocrine tumours (NET) are relatively uncommon tumours, with a reported incidence of 2.5–5 per 100 000 population. There are limited data available on long-term clinical outcome and useful prognostic markers.
Aims and Methods: To perform a retrospective analysis to identify prognostic factors in patients who were referred to our unit from 1996 to 2008 who have subsequently died. Data were collected from 132 patient records (63 men, 69 women) median age 58.5 years (range 26–84) and a database, incorporating clinical findings, histopathological features, as well as anti-tumour therapies was created. Statistical analysis was performed using GraphPad software. Detailed survival analyses of multiple parameters were performed using the Kaplan–Meier method.
Results: In the studied cohort primary tumours arose from the fore, mid and hindgut in 49 (37.1%), 62 (47.0%), six (4.5%), respectively, and 15 (11.4%) patients with unknown primary sites. Distant metastases were seen in 114 (86.4%) of cases, the most frequent metastatic sites were liver in 107 (93.2%) cases, bones in 22 (19.3%) cases and lungs in 14 (12.2%) cases. The overall 5 and 10-year survival rates were 76.1% and 95.4% at 10 years. Time to progression was significantly shorter for pancreatic compared with midgut NET (p<0.05). Survival analysis showed a better clinical outcome for low-grade compared with high-grade tumours. No difference in survival was identified between low and intermediate-grade tumours. Survival was better in patients without metastatic disease at presentation than those with metastatic disease (p<0.001). There was improved survival for patients who underwent surgery at the time of diagnosis compared with those who did not.
Conclusion: This study has demonstrated a number of prognostic markers, including site of the primary tumour, histological grade, metastatic disease at presentation, which are important prognostic factors that should be considered in the management of NET.
PT306 MESENTERIC FIBROSIS IN PATIENTS WITH SMALL BOWEL CARCINOID TUMOURS: IMPACT ON QUALITY OF LIFE AND SURVIVAL
1R. Srirajaskanthan, 1C. Toumpanakis, 1A. Sogbodjor, 1K. Desai, 1A. Krepska, 1L. Marelli, 2M. Winslett, 2G. Ogunbyi, 1M. Caplin. 1Centre of Gastroenterology, Royal Free Hospital, London, UK, 2Academic Department of Surgery, Royal Free Hospital, London, UK
Introduction: Small bowel carcinoid tumours are generally indolent, slowly progressive malignancies. The development of mesenteric fibrosis is a well-documented feature in these tumours; it is probably associated with biogenic amine secretion and can result in the development of a plethora of complications.
Aims and Methods: To perform a retrospective analysis of 62 patients with small bowel carcinoids, who all had radiological evidence of mesenteric fibrosis to identify systemic complications, management and impact on morbidity and mortality. 62 out of 216 patients with small bowel carcinoid tumours had radiological evidence of mesenteric fibrosis and were included in the study. The tumours were classified into low-grade, intermediate-grade and high-grade neuroendocrine tumours. The cohort was divided into two groups dependent on the presence of signs or symptoms related to mesenteric fibrosis; these comprised small bowel obstruction and/or post-prandial abdominal pain. The groups were compared for surgical intervention, the presence of carcinoid heart disease and survival.
Results: 45 patients had clinical features related to mesenteric fibrosis, whereas the remaining 17 patients were asymptomatic. The Pearson χ2 test comparing the symptomatic group with the asymptomatic group showed no difference in terms of histological grade of tumour, sex and carcinoid heart disease. The average duration of follow-up for all patients was 59.7 months. Surgical intervention had been performed in 30 of the 45 symptomatic patients. The indication for surgery was related to small bowel obstruction in 26 cases and hydronephrosis in four cases. Seven of 17 patients (41.4%) in the asymptomatic group have died, whereas 24 of 45 patients (53.3%) in the symptomatic group died. The overall survival for both asymptomatic and symptomatic patients was the same. However, Kaplan–Meier analysis showed improved survival for patients who underwent surgery for complications related to mesenteric fibrosis compared with those who had no surgical intervention at any point of their treatment (p<0.001). Kaplan–Meier analysis showed that tumour grade was also a prognostic marker, with low-grade tumours having a significantly better outcome than intermediate or high-grade tumours (p<0.001).
Conclusion: In symptomatic patients, complications from mesenteric fibrosis are a major cause of mortality and morbidity. The primary cause of death is related to complications from mesenteric fibrosis rather than the progression of disease. In asymptomatic patients with midgut tumours, the cause of death is often related to tumour load. This study showed that surgical intervention for bowel obstruction improved outcome when compared with those without surgical intervention. These data imply that surgical intervention, when possible in patients with small bowel obstruction due to mesenteric fibrosis, can improve survival.
PT307 INTESTINAL FAILURE AND SMALL BOWEL BACTERIAL OVERGROWTH: ASSOCIATED RISK FACTORS
1S. C. Cooper, 2P. Nightingale, 3W. Johns, 1J. Shaffer. 1Intestinal Failure Unit, Hope Hospital, Salford, UK, 2Wolfson Computer Laboratory, Queen Elizabeth Hospital, Birmingham, UK, 3Nuclear Medicine Department, Hope Hospital, Salford, UK
Introduction: Intestinal failure (IF), with altered gastrointestinal physiology and/or anatomy, can promote small bowel bacterial overgrowth (SBBO).
Aims and Methods: We sought to identify features of IF associated with SBBO at a tertiary IF unit, Hope Hospital, where both glycocholate and hydrogen breath tests are employed. All IF patients undergoing breath testing from 2003 to 2008 were identified, and available notes examined. The kappa coefficient identified the degree of agreement between breath tests in IF and all patients tested. Kendall’s τ-b identified associations between potential risk factors for SBBO and breath test results.
Results: 92 IF patients underwent breath testing in 2003–8 (763 in total). The kappa coefficient for IF patients was 0.58 (37 both positive, 35 both negative and 18 heterogenous results) compared with 0.41 for all tested (both moderate agreement). Examination of 47 IF patients revealed that an intact colon and a blind loop were associated with a positive breath test result (p<0.0001 and p = 0.002, respectively), whereas the presence of a stoma, especially a high-output stoma, was associated with negative tests (both p<0.0001). Response to treatment was associated with a positive breath test (p = 0.024). No association was identified with intact stomach, jejunum or length of remaining small bowel. SBBO was not associated with a particular cause of IF (malabsorption, short gut or enteritis).
Conclusion: Breath tests in IF have a better agreement than non-IF patients. Combined with a response to treatment, this suggests a greater incidence of SBBO, associated with an intact colon and blind loop. The presence of a stoma, especially a high-output stoma, was unlikely to be associated with a positive result.
Endoscopy posters
PW308 MIDAZOLAM AND COMFORT DURING COLONOSCOPY: IS IT TIME TO QUESTION ITS BENEFITS?
1G. R. Longcroft-Wheaton, 1J. Fox, 1D. Sheppard, 1P. Goggin, 2N. Cripps, 2J. Simson, 1P. Bhandari. 1Department of Gastroenterology, Portsmouth Hospitals NHS Trust, Portsmouth, UK, 2Colorectal Surgery, St. Richard’s Hospital, Chichester, UK
Introduction: A combination of midazolam and pethidine during colonoscopy is standard UK practice. However, the role of midazolam in improving patient comfort and the quality of the procedure is unclear. It is widely accepted that excessive sedation increases risk during endoscopy. The bowel cancer screening programme targets individuals above the age of 60 years and a significant proportion of these individuals have co-morbidities. National colonoscopy audit clearly revealed sedation related complications. This study examined whether performing colonoscopy without any midazolam had any affect on patient comfort scores, time taken to complete the procedure or polyp detection rate.
Aims and Methods: The results from colonoscopies performed on the bowel cancer screening programme across Portsmouth Hospitals NHS Trust and St. Richard’s hospital were examined. 59 colonoscopies performed by a clinician who did not use midazolam (group A) were compared to 80 colonoscopies within the programme performed by clinicians who routinely administered midazolam (group B). The mean quantity of pethidine used was recorded, along with total procedure time, withdrawal time, mean number of polyps detected, level of sedation achieved and comfort scores during the procedure. Level of sedation was quantified as: 3 = awake, 2 = drowsy, 1 = asleep but responds to voice. Comfort was quantified as: 0 = no discomfort, 1 = mild discomfort, 2 = moderate discomfort, 3 = severe discomfort. Complications were recorded, as were caecal intubation rates.
Results: The caecal intubation rate for group A was 95%. Caecal intubation in group B was 94%. There was 1 complication encountered in each group, both minor bleeds which settled spontaneously. More pethidine was used in group A, but failed to reach statistical significance (P = 0.091). Retroversion of the endoscope was performed 90% of the time in group A, 92% in group B. 11.9% of the cases had cancers in Group A compared with 6.3% group B. The polyp detection rate was 57.6% in group A and 67.5% group B, with no statistically significant difference in the mean number of polyps detected. No other differences were observed. See table. The level of sedation was limited in both groups.
Conclusion: Midazolam does not affect the comfort of colonoscopy and has no affect on completion time, polyp detection rate, complications encountered or completion rates. In both groups the level of sedation achieved was low. As a whole colonoscopy was not found to be an uncomfortable procedure. It is possible that good technique, rather than sedation, is the key factor in comfort. Bowel cancer screening examinations are all performed by experienced clinicians, and this may have been a factor in the low pain scores seen.
PW309 ULTRAFINE TRANSNASAL ENDOSCOPY: AN AUDIT OF INITIAL EXPERIENCE IN A DISTRICT GENERAL HOSPITAL
G. R. Longcroft-Wheaton, A. Fitzjohn, T. Trebble, P. Bhandari. Department of Gastroenterology, Portsmouth Hospitals NHS Trust, Portsmouth, UK
Introduction: The use of an ultrafine endoscope for examination of the upper gastrointestinal tract transnasally (TN) may offer benefits in terms of patient experience and reduced requirement for sedation. However, its effectiveness in the secondary care clinical setting in the UK has been poorly described. We undertook an initial audit of this practice in a busy endoscopy unit in a DGH.
Aims and Methods: A consultant gastroenterologist and nurse endoscopist undertook training in nasal intubation in an ENT department. Unselected patients referred for gastroscopy were offered TN endoscopy in place of routine oro-gastric endoscopy. Patients receiving anticoagulation medication, a history of nose bleeds or altered nasal anatomy were excluded. Informed consent was obtained. Patients were assessed by a trained endoscopy nurse. Lidocaine 5% with phenylephrine 0.5% spray was applied to the nasal cavities, xylocaine spray was applied to the oro-pharynx, and an 18 Fr dilator was inserted 2–3 minutes prior to the procedure. TN endoscopy was performed with a Fujinon EG-530N transnasal gastroscope (5.9 mm diameter with 2.0 mm biopsy channel). Patients underwent the procedure in an upright position with the endoscopist to their right. Where nasal intubation was not possible, oral intubation was undertaken with the TG endoscope in the standard left lateral position. An audit was undertaken regarding completion rate, complications and histological reporting.
Results: Thirty six patients agreed to the procedure. 29 (80.5%) underwent successful nasal intubation. In 3 patients nasal intubation was not possible due to nasal anatomy, all of whom underwent oral intubation with the ultra thin nasal endoscope (two requiring sedation). Among 10 patients who had experienced a previous oro-gastric endoscope, 80% stated that they preferred the transnasal approach (three had previously required sedation). The endoscopists reported acceptable views in all procedures, other than a single case where dye spray was required for Barrett’s surveillance. There were no difficulties reported with obtaining biopsies or on the quality of the specimens taken for histological examination. Patients undergoing TN endoscopy required only a single endoscopy nurse during the procedure and were able to stand and walk immediately without the need for a recovery area. No additional problems were encountered by either endoscopist, however, the induction of nasal anaesthesia increased the preparation time, and the procedure was thought to take slightly longer.
Conclusion: We feel these data demonstrate both feasibility and safety of transnasal endoscopy in a district general hospital setting. Where nasal intubation is possible, there is an 88% non-sedated completion rate including patients who had previously required sedated oral endoscopy. We would expect this to improve as clinicians become more experienced in the technique. Further work is required to assess the cost-effectiveness of the procedure regarding reduced sedation and staff costs.
PW310 COMPARISON OF STANDARD VERSUS HIGH DEFINITION COLONOSCOPY FOR POLYP DETECTION: A RANDOMISED CONTROLLED TRIAL
1G. Tribonias, 1K. Konstantinidis, 1A. Theodoropoulou, 1E. Vardas, 1K. Karmiris, 2G. Chlouverakis, 1G. A. Paspatis. 1Gastroenterology, Benizelion, 2Social Medicine, University of Crete, Heraklion, Greece
Introduction: Colonoscopy is the most commonly performed gastrointestinal procedure due to its utility in colorectal cancer screening. Detection of polyps is an important goal of colonoscopy; therefore it’s of great interest to find out endoscopic techniques associated with the highest polyps’ detection rate. In the present study, we sought to compare the performance of colonoscopy using a high definition, wide-angle colonoscope versus a standard colonoscope for the detection of polyps. The literature data regarding this issue is limited.1 2
Aims and Methods: A total of 390 patients, aged 50 years or older with intact colons, submitted to routine colonoscopy, were prospectively randomised between high definition colonoscopy (HD group, n = 193) and standard colonoscopy (SC group, n = 197). Times required to reach and withdraw from the caecum were measured. All the examinations were performed by a single experienced endoscopist with a known high polyps’ detection rate.3 Sample size calculation showed that at least 182 patients on each group were needed in order to achieve a statistical power of 80% to detect a 15% increase in the number of detected polyps between the two groups at the 5% level of significance.
Results: The per-patient basis analyses demonstrated that there were no significant differences between the 2 groups, as far as the overall detection rate of polyps (SC, 1.31±1.90; HD, 1.68±2.31; P = 0.085), of large polyps (size⩾10 mm; SC, 0.39±0.89; HD, 0.48±0.80; P = 0.29) and of medium polyps (10 mm>size⩾5 mm; SC, 0.60±1.46; HD, 0.58±1.25; P = 0.83). In contrast, a significant difference was observed in the detection rates of small polyps (size<5 mm; SC, 0.32±0.86; HD, 0.71±1.65; P = 0.004). Moreover, no significant differences between the 2 groups were observed, in the overall detection rates of adenomas, large adenomas, medium adenomas, large hyperplastic polyps and medium hyperplastic polyps. On the other hand, the detection rates of small hyperplastic polyps (SC, 0.11±0.38; HD, 0.27±0.63; P = 0.003) and small adenomas (SC, 0.21±0.63; HD, 0.44±1.17; P = 0.018), as well as the overall detection rate of hyperplastic polyps (SC, 0.20±0.48; HD, 0.35±0.69; P = 0.011) were significantly increased with high definition colonoscopes.
Conclusion: High definition colonoscopy led to a significant increase in the detection of small polyps including adenomas and hyperplastic polyps.
PW311 COLONIC POLYPS ARE DIFFERENT IN THE SCREENING POPULATION AS COMPARED TO THE SYMPTOMATIC POPULATION: RESULTS FROM THE NORTH EAST ENDOSCOPY GROUP AND BOWEL CANCER SCREENING PROGRAMME, UK
1G. Pascall, 2T. Wood, 1C. Westwood, 2K. Gunning, 3M. Ritchie, 3B. Tingle, 3C. Rees, 1P. M. Moncur, 4A. Dhar. 1Bowel Cancer Screening Programme, County Durham & Darlington NHS Foundation Trust, Bishop Auckland, UK, 2Colorectal Surgery, Darlington Memorial Hospital, Darlington, UK, 3Bowel Cancer Screening Programme, South of Tyne Bowel Cancer Screening Programme & Gateshead Foundation Trust, South Tyneside, UK, 4Gastroenterology, Bishop Auckland General Hospital, Bishop Auckland, UK
Introduction: The clinico-pathological profile of colonic polyps found in the symptomatic population in Durham has recently been compared with those found in the first cohort of County Durham Bowel Cancer Screening Programme (BCSP) (Gut, October 2008). The BCSP continues to report larger and greater number of adenomatous polyps than the symptomatic population.
Aims and Methods: This study was aimed at comparing the clinico-pathological characteristics of colonic polyps between the symptomatic and the screening population in the North East of England. 160 symptomatic patients who underwent colonoscopy for evaluation of their bowel symptoms and were found to have colonic polyps were compared with 160 asymptomatic BCSP patients with colonic polyps (101 from County Durham Screening Programme, 59 from South of Tyne Screening Centre).
Results: 213 polyps were found in 160 symptomatic patients (1.33 polyps per patient) while 360 polyps were found in 160 BCSP patients (2.25 polyps per patient), p<0.001. Multiple (>3) polyps were significantly more common in the asymptomatic BCSP cohort (31%) as compared with symptomatic population (7%). Polyps in the BCSP cohort were more frequently adenomatous (84%) compared with the symptomatic population (55%), p<0.0001. Polyps in the BCSP cohort were also twice as likely to be larger than 10 mm (28%) when compared with the symptomatic patients (14%), p = 0.0018. The prevalence of flat polyps and high grade dysplasia was comparable. Histological completeness of excision was reported in 38% of BCSP group compared to only 20% of the symptomatic population.
Conclusion: As compared to the symptomatic population undergoing colonoscopy, the Bowel Cancer Screening Programme has consistently detected a greater number of adenomatous polyps per patient, and larger polyp sizes. This epidemiological observation needs to be co-related to polyp genetics to determine if the biological behaviour of BCSP patients is different. The data also suggest that the BCSP is likely to be effective in decreasing colon cancer in the UK.
PW312 LEAKS AFTER LAPAROSCOPIC CHOLECYSTECTOMY AND SALVAGE BY ENDOSCOPIC RETROGRADE CHOLANGIOPANCREATOGRAPHY
H. Sharma, G. Bird. Gastroenterology, Maidstone Hospital, Maidstone, UK
Introduction: Laparoscopic cholecystectomy (LC) has become the preferred operation for gallstones but is associated with an increased risk of bile duct injury compared with open cholecystectomy. Regardless of the nature of the injury, the majority are not recognised at the time of surgery and it is common for an endoscopic retrograde cholangiopancreatography (ERCP) to be requested in cases of suspected injury to identify a bile leak and if necessary to decompress the biliary system.
Aims and Methods: The aim of the study was to evaluate the nature of bile duct injuries and the success of ERCP in their identification and management over a long term period in a district general hospital setting. Data were collected prospectively in patients referred with suspected biliary leaks post LC from October 1994 to August 2008. All cases underwent ultrasound and/or CT imaging before ERCP showing features compatible with a biliary leak. ERCP was carried out by a single operator (GB) under sedation or general anaesthetic using standard techniques and procedures.
Results: 46 patients were referred during the study period and ERCP was carried out with IV sedation in 44 and general anaesthesia in 2. A satisfactory cholangiogram was obtained in 45 (98%). Of these, 32 (71%) had cystic duct stump leaks, 3 (6%) had common hepatic duct leaks, 2 (4%) had common bile duct (CBD) leaks, 3 (6%) had strictures in the CBD and 1 (2%) had a complete transection of the CBD. Of the 5 (12%) patients with a T tube left in situ at the time of surgery, stones were also present in the CBD (although in one patient no leak was present).
Patients with confirmed leaks and strictures on cholangiography were stented with 7 Fr or 10 Fr plastic stents which were removed after 2–6 weeks (with stone extraction if indicated) after apparent resolution of their symptoms. There was one case of mild pancreatitis but no other complications. All 3 cases with CBD strictures subsequently underwent hepaticojejunostomy and the patient with a transected CBD underwent reconstructive surgery.
Conclusion: Patients referred for ERCP with a suspected biliary leak after LC most commonly have a leaking cystic duct stump which responds well to a temporary stent placement. ERCP is valuable in detecting and treating these straightforward cases although a range of more serious biliary tree injuries can be expected.
PW313 COMFORT DURING COLONOSCOPY: DO NURSES TELL US MORE?
J. Falvey, C. King, A. Dixit, P. Marden, T. Creed. Department of Gastroenterology, Bristol Royal Infirmary, Bristol, UK
Introduction: Comfort during colonoscopy has been recommended as an auditable quality indicator within the Global Rating Scale. Comfort scores are largely reported by endoscopists, but JAG have suggested that for endoscopists failing to reach national standard further training might include comfort assessment by the nurses assisting the endoscopist and comparison of these scores against peers in the same institution.1 A previous study has shown that colonoscopist and endoscopy nurse estimates of patient discomfort correlate significantly with patients own reporting, although nurses were more accurate.2 We set out to test the “real life” relationship between colonoscopist and nurse recording of patient comfort by dual reporting comfort during colonoscopy without the knowledge of the endoscopist.
Aims and Methods: Data were collected from 210 colonoscopies prospectively. The endoscopist routinely completed a comfort score as part of an electronic reporting system (5-no pain, 4-little pain, 3-quite a lot of pain, 2-very bad pain, 1-as much pain as a patient can tolerate). Unknown to the endoscopist, the endoscopy nurses present (at least 2) also recorded patient comfort using the same score and without conferring. The duration of each nurses’ experience in endoscopy was noted.
Results: 13 colonoscopists performed a mean of 16 procedures (range 3–39). 28 endoscopy nurses took part in the study. Patients were sedated with a combination of midazolam plus either pethidine or fentanyl (mean dose 3 mg, 42 mg and 62 μg, respectively). The overall caecal intubation rate was 91%. While there was a significant correlation between comfort scores recorded by colonoscopists and endoscopy nurses (Spearman r = 0.5832; p<0.0001) and a high level of internurse agreement (Spearman r = 0.5824; p<0.0001), nurses recorded significantly more discomfort than colonoscopists (3.847 vs 4.162: p = 0.012; Mann Whitney). When individual endoscopists were considered, the majority, 11, recorded scores that were not significantly different to those of the nursing staff. Two endoscopists were found to have significantly under-recorded discomfort when compared with nurse data (and yet had among the highest throughput and completion rates). The amount of experience a nurse had in endoscopy did not affect perception of patient discomfort.
Conclusion: There is a highly significant correlation between endoscopist and endoscopy nurse scoring of patient comfort during colonoscopy. Nurse scoring of comfort enabled outlying endoscopists to be identified. The addition of comparative comfort scoring to standard outcome measures such as completion rate would be valuable to quality assurance.
PW314 ENDOSCOPIC RETROGRADE CHOLANGIOPANCREATOGRAPHY IN A DISTRICT GENERAL HOSPITAL: A REVIEW OF 1550 PROCEDURES OVER 9 YEARS
1J. Penston, 1P. B. Southern, 2V. K. Penston, 1J. Daws. 1Gastroenterology, Scunthorpe General Hospital, Scunthorpe, UK, 2Medical School, University Of Liverpool, Liverpool, UK
Introduction: With the introduction of alternative methods for the investigation of the biliary tract and pancreas, as well an increased awareness of the complications of invasive procedures, the number of endoscopic retrograde cholangiopancreatographies (ERCPs) has declined in recent years. This trend has raised questions about the ERCP service in the UK and the training of specialist registrars in this technically difficult procedure.
Aims and Methods: Data relating to demographic characteristics, technical success rates and complications were collected prospectively over a period of 9 years in a district general hospital serving a population of 160 000 in northern England. Analysis was performed on a strict intention-to-treat basis.
Results: Between 1997 and 2006, a total of 1550 ERCPs were performed. Technical success rates for cannulation of the common bile duct (CBD), sphincterotomy, pre-cut incision, stent insertion and stone removal were high. Cannulation of the CBD was achieved in 95% of all ERCPs, increasing to 98% between 2001–2006. The rate of complications was low: acute pancreatitis 3%, perforation 0.3% and haemorrhage 0.4%; the overall procedure-related mortality was 0.2%. Over time, the indications changed, resulting in a fall in the number of ERCPs and a reduction in the proportion of normal cholangiograms, together with an increase in therapeutic procedures; these trends were accompanied by increases in the success rates of diagnostic and therapeutic procedures, and a decrease in the rate of complications. During the period 2001–2006, 96% of patients were assessed beforehand by the endoscopist performing the ERCP who also reviewed 100% of patients within 6–8 hours after the procedure.
Conclusion: This study documents important trends in the practice of ERCP in the UK over the past decade and emphasises the benefits of patient selection and consultant-based care before, during and after the procedure. It also confirms that ERCP may be performed to a high level of expertise and with a low risk of complications in district general hospitals. However, the changes in practice have unwelcome implications for the training of specialist registrars.
PW315 SURFACE VISUALISATION AT CT COLONOGRAPHY SIMULATED COLONOSCOPE WITHDRAWAL: EFFECT OF HYOSCINE BUTYLBROMIDE AS ANTISPASMODIC
1J. E. East, 1B. P. Saunders, 2D. Burling, 2E. Tam, 3D. Boone, 3S. Halligan, 3S. A. Taylor. 1Wolfson Unit for Endoscopy, UK, 2Intestinal Imaging Centre, St. Marks Hospital, UK, 3Department of Specialist Radiology, University College Hospital, London, UK
Introduction: Antispasmodics have been recommended by some experts to improve mucosal visualisation during colonoscope withdrawal, potentially improving polyp and adenoma detection by reducing smooth muscle tone and flattening haustral folds; however, routine use of such agents is uncommon, only 20% of colonoscopists in a large UK audit,1 and their effectiveness unclear.
Aims and Methods: To assess the impact of hyoscine butylbromide on surface visualisation at CT colonography (CTC) simulated colonoscope withdrawal. Datasets for 86 patients suspected of having colorectal neoplasia from a previous CTC study examining the effect of antispasmodic were re-analysed with customised CTC software, adjusted to give a 140 degree field of view, equivalent to a standard colonoscope. Patients received intravenous hyoscine butylbromide 20 mg, 40 mg or no antispasmodic. A unidirectional 3D endoluminal flythrough facing the caecum simulated the view at colonoscope withdrawal.2 The software automatically calculates the percentage colonic surface visualisation, numbers and sizes of unseen areas, and colonic length.
Results: Use of antispasmodic was associated with a significant absolute increase in percentage surface visualisation of 2.3–3.4% (prone-supine), equivalent to an approximate 20% relative decrease in unseen area, compared to no antispasmodic. Total numbers of missed areas and intermediate sized (300–1000 mm2) missed areas were significantly decreased, by approximately 20%. There was no difference between 20 mg and 40 mg doses. Results for prone and supine datasets were similar. Mean colonic length was unchanged by the use of antispasmodic. More than 6% of patients had a colonic length >200 cm.
Conclusion: Hyoscine butylbromide 20 mg IV, a low cost intervention, at CTC simulated colonoscope withdrawal was associated with modest but significant improvements in surface visualisation, and significantly decreased numbers of clinically important sized missed areas. These data support the use of antispasmodics to potentially maximise polyp detection during colonoscopy.
PW316 ROLE OF ENDOSCOPIC ULTRASOUND AND ENDOSCOPIC MUCOSAL RESECTION IN THE EVALUATION OF PATIENTS WITH EARLY BARRETT’S NEOPLASIA
T. Thomas, J. Mannath, P. V. Kaye, G. P. Aithal, K. Ragunath. Nottingham Digestive Diseases Centre and Biomedical Research Unit, Queens Medical Centre, Nottingham University Hospital, Nottingham, UK
Introduction: The role of endoscopic ultrasound (EUS) in the pre-operative evaluation of Barrett’s early neoplasia remains contentious. Its diagnostic accuracy is dependent on the endoscopist’s experience, location of dysplasia and lesion morphology. Endoscopic mucosal resection (EMR) is now increasingly used to stage and treat Barrett’s early neoplasia.
Aims and Methods: Determine the role of EUS and EMR in managing patients with early Barrett’s neoplasia and evaluate its sensitivity to detect submucosal invasion. Patients with histological confirmation of early Barrett’s cancer from March 2003–March 2008 were initially evaluated with high-resolution endoscopy (Olympus Lucera video endoscope system, GIF H260 or Q240FZ) and visible lesions classified based on the Paris classification. Lesions were then staged by conventional radial scanning echoendoscope (7.5–20MH GF-UM 2000, Olympus) followed by EMR (only if mucosal disease suspected) or went direct for surgical resection.
Results: EUS was performed in 35 patients (21 males) with a median age of 69 years (IQR: 60–79) and a median Barrett’s length of 4 cm (IQR: 2–8). The Paris classification of lesions were as follows, type 0-IIa: 11, 0-IIb: 19, 0-IIa+c: 3, 0-IIc: 2. Mucosal biopsies showed high grade dysplasia in 28/35 (77.8%) and adenocarcinoma in the remainder. EMR in 27/35 (77%) patients showed adenocarcinoma in 13/27 (48%), HGIN in 12 (45%) and Barrett’s metaplasia in 2 (7%). Submucosal invasion or beyond was detected by EUS in 5/35 (14%) confirmed on oesophagectomy in 4 patients (one patient with T2N1 staging on chemotherapy), thereby impacting management strategy. In 3/35 (8%) cases submucosal invasion seen on EMR was not detected on EUS (false negatives).Two additional patients with submucosal invasion on EUS had T2 lesion or above on oesophagectomy. Therefore EUS understaged lesions in 5/35 (14%) cases but did not overstage lesions. Overall the sensitivity, specificity, negative predictive value and diagnostic accuracy of EUS to detect submucosal invasion was 57%, 100%, 90% and 91% respectively. Of the 22/25 (86%) of patients with intensive endoscopic follow up 19/22 (86%) were free of dysplasia or cancer at a median follow up duration of 13 months.
Conclusion: EUS prior to EMR changed management in 14% of patients with early Barrett’s neoplasia. The sensitivity of EUS to detect submucosal invasion remains poor at 57% and it understaged lesions in 14% of cases. Hence adding EMR to the algorithm following EUS can improve the accuracy of local staging and select patients suitable for curative endoscopic therapy.
PW317 ADEQUATE UPTAKE? A SURVEY OF THE USE OF CHROMOENDOSCOPY FOR COLITIS SURVEILLANCE IN ENGLISH ENDOSCOPY UNITS
J. Parr, M. Rutter. Gastroenterology, University Hospital North Tees, Stockton on Tees, UK
Introduction: In 2002 the BSG issued guidelines on colitis surveillance. These guidelines recommended taking quadrantic biopsies at 10 cm intervals throughout the colon looking for evidence of dysplasia. Since the publication of the guidelines, evidence from 4 prospective controlled trials has demonstrated that chromoendoscopy (dye-spraying) with targeted biopsies of abnormal mucosa significantly increases the dysplasia yield. Little is known about the current use of chromoendoscopy as the primary modality for colitis surveillance within endoscopy units in England.
Aims and Methods: A short questionnaire was constructed, aimed at gathering data on the use of, and opinions of, chromoendoscopy for colitis surveillance within English endoscopy units. This questionnaire contained a mix of yes/no answers and also allowed room for free text. The survey was distributed electronically to endoscopy leads in England.
Results: Responses were obtained from 47% (94/199). Of those who responded, 82% of units had a policy in place for colitis surveillance. Chromoendoscopy was a formal part of this policy in only 13%. Only 65% of units had at least one endoscopist with the ability to carry out chromoendoscopy procedures. In those who did offer the service, there were no units who reported using it in every case of colitis surveillance. In units where chromoendoscopy was being used, only 36% of respondents reported allocating extra time to procedures involving dye spray. 94% of units performed surveillance colonoscopies on a general list. Where chromoendoscopy was not the favoured technique for colitis surveillance, the most commonly cited reason was a lack of experience (71%), with 55% of respondents feeling the use of dye spray techniques to be unnecessary. When considering experience of colonoscopists in the use of chromoendoscopy techniques, 46% of units had no endoscopists with experience in this field. Where experience had been gained, the most common method was through watching videos (70%), followed by reading relevant literature (65%). Only 37% had attended a hands on course. Of those who replied, 74% thought a formal course teaching chromoendoscopy techniques would be useful.
Conclusion: Despite evidence favouring the use of chromoendoscopy in colitis surveillance, English endoscopy units have been slow to adopt the technique, with only 13% of units using chromoendoscopy as a formal part of their surveillance protocol. Cited reasons for the low uptake include the lack of familiarity with the technique and its evidence base. The majority of units felt that a formal training course would be beneficial.
(Submitted on behalf of NREG – Northern Region Endoscopy Group).
PW318 COMPARISON OF THE SHEFFIELD GASTROSTOMY SCORE WITH AN ARTIFICIAL NEURAL NETWORK ANALYSIS
1J. S. Leeds, 2S. R. Morley, 1H. E. Robson, 1J. Grant, 3J. Hensman, 3K. Worden, 1M. E. McAlindon, 1D. S. Sanders. 1Gastroenterology and Liver Unit, Royal Hallamshire Hospital, Sheffield, UK, 2Department of Clinical Chemistry, Royal Hallamshire Hospital, Sheffield, UK, 3Department of Mechanical Engineering, University of Sheffield, Sheffield, UK
Introduction: Despite gastrostomy insertion being a well accepted method for medium and long term feeding, there is still a substantial morbidity and mortality rate. We have previously reported on a simple clinical scoring system that provides estimated mortality rates at 7, 30 and 90 days. This scoring system provides a mortality range and not an absolute risk of death. Other investigators have tested the accuracy of clinical scoring systems with an artificial neural network (ANN). Our aim was to determine whether an artificial neural network performs with a higher accuracy than the clinical scoring system.
Aims and Methods: The original cohort (n = 403) of patients used to derive the scoring system was entered into the ANN. Each individual comprised of 12 clinical variables. The classifier in this case was a multi-layer perceptron which can attempt to determine if a given patient survives N days, given the measured features from the data. The multi-layer perceptron is simply a collection of connected processing elements called nodes or neurons, arranged together in layers. Signals pass into the input layer nodes, progress forward through the networks hidden layers and finally emerge from the output layer. Simple statistical analysis plus receiver operator curves (ROC) were calculated and compared.
Results: The cohort examined consisted of 403 new gastrostomy insertions (median age 64, 268 males) with an overall 30 day mortality rate of 51/403 (12.7%). Risk factor analysis using multiple logistic regression identified that age and albumin were independent predictors of mortality. Modelling of these risk factors and attribution of scores (age scoring 0 or 1 and albumin scoring 0, 1 or 2) provided composite scores from 0 to 3. Scores of 0, 1, 2 and 3 gave 30 day mortalities (95% confidence interval (CI)) of 0% (0 to 2.1), 7% (2.9 to 13.9), 21.3% (13.5 to 30.9) and 37.3% (24.1 to 51.9), respectively. Analysis using the ANN gave sensitivities of 66.7%, 60.9%, 70.6% and 63.2% and specificities of 62.1%, 66.1%, 73.8% and 71.8% at 7, 30, 60 and 90 days, respectively. ROC curves for the Sheffield gastrostomy score gave an area under the curve of 0.75 (95% CI 0.68 to 0.82, p<0.001) and the ANN analysis gave an area under the curve of 0.72 (95% CI 0.62 to 0.82, p<0.001).
Conclusion: The Sheffield gastrostomy score and ANN both perform well when predicting mortality rates following percutaneous endoscopic gastrostomy (PEG) insertion. The accuracy of these systems may be improved by conducting larger multicentre studies.
PW319 PATIENT SELECTION FOR PERCUTANEOUS ENDOSCOPIC GASTROSTOMY: IS CLINICAL ACUMEN SUFFICIENT?
J. S. Leeds, J. Grant, H. E. Robson, M. E. McAlindon, D. S. Sanders. Gastroenterology and Liver Unit, Royal Hallamshire Hospital, Sheffield, UK
Introduction: Percutaneous endoscopic gastrostomy (PEG) insertion is the method of choice for medium/long term enteral nutrition. There have been a number of studies examining outcomes in patients undergoing PEG insertion but little is known about those patients who are deferred on clinical grounds. The aim of this study was to prospectively examine outcomes in this specific cohort of patients and to make comparisons against those patients in whom a PEG was inserted.
Aims and Methods: All patients referred for PEG insertion in our institute are reviewed by the PEG nurse specialist (± a gastroenterologist and/or MDT) and are prospectively included in a database. Demographic, biochemical and outcome data are also included. PEG referrals from February 2004 to February 2007 were analysed.
Results: During the study period 556 patients had a PEG inserted and 144 (20.6%) were deferred. 62 patients were clinically deemed to be too unfit for PEG, or died prior to PEG insertion; 28 patients had an improvement in swallowing; 16 patients refused PEG insertion; 11 patients were deferred to re-assessment at 7 days; in 6 patients PEG failed and 21 patients were not placed for miscellaneous reasons. Median age was 64 years in those receiving a PEG vs 77.5 years in those without a PEG (p<0.001), but there were no differences in gender distribution. 30 day mortality rate was 75/556 (13.4%) in those who received a PEG and 66/144 (45.8%) in those without a PEG (OR 5.4, 95% CI 3.6 to 8.2, p<0.001). Median survival was 298 days in those receiving a PEG compared to 38 days in those without a PEG (p<0.001). Patients undergoing PEG insertion had lower serum creatinine (76.9 vs 93.6, p = 0.01) and a higher serum albumin (29.4 vs 25.6, p<0.001) compared to those not undergoing PEG insertion. Within the deferred PEG group predictors of survival for more than 30 days were age (younger: 63.8 years vs 79.3 years, p<0.001) and a higher serum albumin (27.8 vs 22.9, p<0.001). Multivariable analysis revealed that independent predictors of surviving more than 30 days without a PEG were age >60 (adjusted OR 2.8, 95% CI 1.9 to 5.9, p<0.001) and albumin >25 g/L (adjusted OR 6.2, 95% CI 3.0 to 25, p = 0.05).
Conclusion: In our institute 20.6% of PEG referrals were deferred. Predictors of mortality were age, renal impairment and a low serum albumin. It would appear that clinical acumen enhances appropriate patient selection.
PW320 “JUST IN TIME” COLONOSCOPY: A CHANGE IN THE PARADIGM FOR COLONIC IMAGING IN SYMPTOMATIC PATIENTS
1L. Marelli, 1L. Jackson, 1M. Bose, 2J. Bell, 2O. Epstein. 1Centre for Gastroenterology, Royal Free Hospital, London, UK, 2Department of Radiology, Royal Free Hospital, London, UK
Introduction: Primary 3D virtual reality colonoscopy (V3D – Viatronix) has similar sensitivity to optical colonoscopy (OC) in both screening and investigation of patients with colorectal symptoms.1 2 V3D is minimally invasive, does not require sedation and carries no risk of severe complications such as perforation.
Aims and Methods: We have assessed the potential impact of V3D as a primary colonic imaging modality in symptomatic patients followed by interventional OC for patients with polyps and/or tumours. A total of 163 patients (63M, 100F; mean age 63 years) underwent V3D. Patients with abnormal V3D were then considered for OC. All patients undergoing V3D were prepared with polyethylene glycol (PEG) and diluted stool tagging; this preparation is suitable for immediate follow-on OC. V3D was performed under CO2 insufflation.
Results: V3D was successful in 159 of 163 patients (98% – 1 unable to retain air and 3 technical failures). Indications for V3D were change in bowel habits (39%), abdominal pain (18%), anaemia (14%), rectal bleeding (6%), family history (8%), previous polyps or colon cancer (7%) and others (8%). V3D revealed a normal colon in 76 patients (48%), diverticular disease in 50 (31%), “possible polyps or faeces” >6 mm in 30 (19%) and cancer in 3 (2%). Polyp size was 6–10 mm in 25 of 30 patients (83%) and more than 1 cm in 5. The polyps were located in the right colon in 3 patients (10%), in the transverse colon in 2 (7%) and in the left colon in 25 (83%). Thirty-three of 159 patients (21%) required further investigation with OC. Of these, 27 (82%) required only left sided OC. OC confirmed cancer in 3 patients. In 5 patients with V3D showing “possible polyps” >6 mm of the right or transverse colon, OC confirmed the presence of polyps in 2 patients and was normal in 3. Of 25 patients with left colon “possible polyps” >6 mm at V3D, flexible sigmoidoscopy confirmed the presence of polyps in 12 patients and was normal in 13.
Conclusion: The use of V3D to image the colon in patients with colorectal symptoms allows identification of patients requiring optical intervention; this can be done the same day with the same bowel preparation. Using this strategy only 21% of patients in this study would have been directed to same day “just in time” OC; moreover, 82% of them, having only left sided lesions, would have required only unsedated flexible sigmoidoscopy. With the emergence of high quality V3D imaging, a new paradigm for imaging symptomatic patients might be V3D followed by immediate “just in time” OC or flexible sigmoidoscopy.
PW321 NEEDLE KNIFE FISTULOTOMY IN DIFFICULT AMPULLARY CANNULATION INCREASES THE RATE OF BILIARY CANNULATION: 10 YEAR EXPERIENCE IN A DISTRICT GENERAL HOSPITAL
1M. Aljabiri, 2 N. Joshi, 2 N. van Someren, 2 K. Besherdas. 1Gastroenterology, Barnet And Chase Farm Hospitals NHS Trust, London, UK, 2 Gastroenterology, Chase Farm Hospital, Enfield, Middlesex, UK
Introduction: Biliary cannulation is the first step in therapeutic endoscopic retrograde cholangiopancreatography (ERCP). Bile duct cannulation failure rate is estimated around 5–10% more often than not due to anatomical and physiological factors such as luminal folds in common cholangiopancreatic duct, duodenal diverticulum, small ampullary orifice and inversion or eversion of the ampulla. We retrospectively assessed our use of needle-knife fistulotomy (KNF) techniques in our district general hospital (DGH) in patients with difficult biliary cannulation.
Aims and Methods: To assess the success rate of early NKF in patients with difficult standard biliary cannulation in our DGH. We retrospectively assessed 2520 ERCPs performed over a period of 8 years. Two operators attempted standard biliary cannulation; if 4–5 ampullary attempts and 2 pancreatic duct cannulation were unsuccessful a NKF was performed. Standard biliary cannulation was attempted with a sphincterotome and a guide-wire. If this failed within 10 minutes or if there were more than 2 pancreatic cannulations, fistulotomy with sparing of the ampullary sphincter was performed. If access to the biliary tract was still unsuccessful the procedure was abandoned and rescheduled in 48 hours.
Results: The initial failure rate for cannulation with a sphincterotome was 214/2520 (8.4%), cannulation success rate pre KNF 2010/2520 (∼80%). 510 KNF were performed out of 2520 therapeutic ERCPs (∼20%), successful cannulation post KNF in 411/510 (80.5%), raising the overall success rate of biliary cannulation post KNF 2421 (96%). 451/510 (88.4%) had no complications in our KNF, the rest had complications ranging from ooze of blood to minor bleeding in 51 patients (1 significant bleed died after 36 hours post KNF), pancreatitis 7/510 (1.3%) (mild pancreatitis in 5 patients, 1 worsening pancreatitis, 1 died 5 days later from sever pancreatitis); there were no perforations in our experience post KNF.
Conclusion: In an experienced hand, the early pre-cutting technique for biliary cannulation is safe and effective as standard technique. This ultimately leads to an increased success rate of biliary cannulation and shortening the time for biliary cannulation, and avoids oedema of the papilla that can increase the risk of perforation. We recommended early KNF should be performed and should be standard technique for difficult biliary cannulation.
PW322 ENDOSCOPIC ULTRASOUND: A LARGE SINGLE CENTRE EXPERIENCE AT UK DISTRICT GENERAL HOSPITAL (TERTIARY REFERRAL UNIT)
M. Bhalme, M. Ng, V. Kaushik. Department of Gastroenterology, Royal Blackburn Hospital, Blackburn, UK
Introduction: Prospective data on experience of endoscopic ultrasound (EUS) is sparse from the UK. This study aimed to review the high volume diagnostic and interventional service at a centre in UK.
Aims and Methods: Data on all consecutive EUS at the Royal Blackburn Hospital was collected prospectively from March 2004 to February 2007. Patient demographics, indications, findings and fine-needle aspiration (FNA) were extracted from the database. Subset of 86 patients was studied retrospectively to assess the staging accuracy from post-operative and FNA histology.
Results: 532 patients had 561 procedures. Men comprised 46% (n = 243). Mean age was 60 years (range, 17–90 years). Mean duration for diagnostics was 28 minutes (range, 5–60 minutes) and for intervention was 45 minutes (range, 10–95 minutes). Indications were: (1) Luminal 35.2% (197), of which were oesophageal 19.3% (108), gastric 12.5% (70), duodenal 3.4% (19); (2) Pancreatico-biliary (PB) 63.3% (355); and (3) Mediastinal and lung 1.6% (9). The overall accuracy for oesophageal cancer staging was 50% (6/12) in first and 75% (9/12) in second half, indicating an improvement with more experience. This relative low accuracy was attributed to the mean interval between EUS and surgery which was 10 weeks (range, 2–20 weeks) allowing some tumours to progress. Two patients in the second half who were understaged had their surgery in over 2 months. The T-staging accuracy for PB cancers was 60% (12/20). This low accuracy was due to no FNA being performed (some patients had chronic pancreatitis) and confusion about the site of tumour, whether peri-ampullary, lower cholangiocarcinoma or pancreatic tumour. The mean interval between EUS and surgery in this group was 4 weeks (range, 1–9 weeks). EUS-FNA was carried out in 6.7% (37/561) procedures, with accuracy for pancreatic (both solid and cystic) and submucosal lesions of 70.8% (17/24) and 60% (6/10) respectively. Lymph node FNA accuracy was 87.5% (7/8). In total 6 patients had EUS guided drainage of pancreatic pseudocyst with 100% success rate and requiring only one stent insertion. There was one major complication, bleeding from an area of severe duodenitis which settled with adrenaline injection.
Conclusion: This is the largest reported UK experience of EUS to date. Overall, EUS was accurate and safe with no associated mortality. With newly improved non-invasive diagnostic imaging, the role of EUS is moving more towards therapeutic interventions.
PW323 SAFETY OF ENDOSCOPIC BALLOON DILATATION OF THE PAPILLA OF VATER FOR COMMON BILE DUCT STONES
M. S. H. Smith, M. R. Andrew. Department of Gastroenterology, Royal Shrewsbury Hospital, Shrewsbury, UK
Introduction: Recently published British Society of Gastroenterology guidelines on the management of common bile duct (CBD) stones advise against balloon dilatation of the Papilla of Vater on the grounds of a higher risk of severe pancreatitis when compared with sphincterotomy.1 However, balloon dilatation following sphincterotomy has been suggested as an option for large (>15 mm) or multiple CBD stones.2 We have performed balloon dilatation following sphincterotomy for these indications since 2006 and report our own experience.
Aims and Methods: The procedure reports of all patients undergoing endoscopic retrograde cholangiopancreatography (ERCP) since 2006 in our institution were screened in order to identify cases in which balloon dilatation of the Papilla of Vater was performed. The medical records for these patients were reviewed and the success of the procedure, complications, length of stay, emergency surgery within 8 days and 30 day mortality were recorded.
Results: 18 patients, mean age 74 years, underwent ERCP, sphincterotomy and balloon dilatation of the Papilla of Vater with a 15 mm or 18 mm balloon for multiple or large gallstones. The CBD was completely cleared of stones in each procedure. The mean length of stay was 2 days. There were no complications. No patient required emergency surgery and all patients survived beyond 30 days.
Conclusion: Our preliminary experience of balloon dilatation of the Papilla of Vater following endoscopic sphincterotomy for multiple or large CBD stones suggests that it is a safe and effective alternative to other modalities such as mechanical lithotripsy and allows complete clearance of the CBD at a single session.
PW324 IS INTRAVENOUS CANNULATION NECESSARY IN COLONOSCOPY?
M. Kurien, J. M. Hebden, M. Smith, M. T. Donnelly. Department of Gastroenterology, Sheffield Teaching Hospitals NHS Trust, Sheffield, UK
Introduction: Colonoscopy is established as the gold standard investigation for colonic symptoms as well as being the modality of choice for the Bowel Cancer Screening Programme (BCSP). Most colonoscopists feel it is mandatory to establish secure intravenous (iv) access before commencing the procedure. Indeed this is one of the criteria for passing the BCSP accreditation assessment. The rationale would appear to be able to quickly resuscitate the patient should complications occur, as well as allowing the easy administration of additional medication including antidotes. At the same time, the amount of non-sedated colonoscopy performed (or using inhaled nitrous oxide alone) is increasing. In such cases, an intravenous cannula is still inserted, in contrast to gastroscopy performed without sedation. With the increased emphasis on cannula related sepsis, including MRSA, we wanted to examine the necessity of cannula insertion in patients undergoing unsedated colonoscopy.
Aims and Methods: We interrogated our endoscopy records system and analysed the records of patients undergoing colonoscopy over a 6 month period. Patient demographics, iv sedation, inhaled analgesia used and complications, including flumazenil use, were recorded.
Results: 3117 patients were examined (M:F = 1444:1673) with a median age of 64 years, all of whom had an iv cannula inserted. 1077 / 3117 (34.6%) patients received iv midazolam (mean dose = 2.3 mg). 422 (39.2%) patients in this group also used iv buscopan. 389 (12.5%) patients had buscopan alone. 610/1077 (56.6%) patients also used inhaled nitrous oxide, and a further 39 (3.6%) had iv fentanyl. Intravenous access was required in 3 patients for prophylactic antibiotics. Therefore 1648 (52.8%) patients had no intravenous medication. In this group, there were no reported complications during or immediately after the procedure (including desaturation, brady- or tachy-arrhythmia, or hypotension).
Conclusion: We have previously shown that unsedated colonoscopy is safe and well tolerated in a large number of patients offered this option.1 We believe this study demonstrates that in such patients, iv cannulation is an unnecessary expense with previously well defined risks. In patients undergoing unsedated colonoscopy, iv cannulation should not be considered mandatory.
PW325 THE MANAGEMENT OF SUB-CENTIMETRE COLONIC POLYPS: STILL A HOT TOPIC?
M. J. Shale, J. Martin, D. Bansi, P. Vlavianos, G. Smith, D. Westaby. Gastroenterology, Imperial College Healthcare NHS Trust, London, UK
Introduction: Colonoscopic polypectomy can prevent colorectal cancer but is not without potential complications. Multiple polypectomy techniques exist including the use of biopsy forceps or snares, each with or without electric current. While the removal of polyps >10 mm generally mandates snare polypectomy, the possibilities for removal of smaller polyps are more varied. Technique related differences in the efficacy and safety of polyp removal have been reported, and vary by polyp size and location. Information regarding the management of small polyps in routine practice in the UK is limited.
Aims and Methods: A retrospective analysis of colonoscopies undertaken within two teaching hospital endoscopy units in the period 2003–07 was performed. Polypectomy procedures were identified from electronic records, and details of the polyp and excision method extracted. Reports not including an estimated polyp size, location or method of removal were excluded, as were those where polyp size was reported >10 mm.
Results: 1508 polyps were removed at 972 colonoscopy procedures (range 1–10 polyps per procedure). 762 (50%) polypectomies were performed by consultant gastroenterologists (n = 12), 699 (47%) by trainee gastroenterologists (n = 34), and the remainder by surgical endoscopists (n = 8). Mean polypectomies per operator 28, range 1–166. 947 (63%) polyps were left sided. Estimated polyp size was <3 mm in 49% (n = 744); 4–6 mm in 36% (n = 538) and 7–10 mm in 15% (n = 226). Polypectomy technique according to polyp size for the overall period is shown in the table. Hot snaring was consistently the predominant method of removal of polyps 7–10 mm, however significant inter-operator variation was seen in the management of polyps <7 mm. Within the period of study, there was a significant trend away from hot biopsy, noted in all operator groups and for all polyp sizes (2003: 62% overall, 2007: 8%; p<0.01). In contrast, in the same period the use of cold forceps and cold snares increased (2003: 3% and 0.3% respectively; 2007: 25% and 7%; each p<0.05). The use of snaring techniques for polyps <7 mm increased during the period of study (polyps <3 mm: 7.6% to 35.2%; 4–6 mm 50.8% to 74.2%). Similarly, the use of submucosal injection increased from 0.5–6% overall. In 2007 it was used in removing 3% of <3 mm polyps, 8% of 4–6 mm and 12% of 7–10 mm.
Conclusion: Polypectomy technique for small polyps is highly variable. Significant changes in practice have occurred in the last 5 years, with cold techniques largely replacing hot biopsy. The use of submucosal injection to facilitate removal of small polyps is growing. Better definition of optimal polypectomy strategies should be addressed in clinical trials.
PW326 A NOVEL SCORING SYSTEM TO PREDICT POOR BOWEL PREPARATION AT COLONOSCOPY
N. Prasad, P. D. Mullins. Gastroenterology, Royal Blackburn Hospital, Blackburn, UK
Introduction: Poor bowel preparation at colonoscopy is associated with lower completion rates, missed lesions, increased patient discomfort, longer procedure time and higher risk of complications. Inadequate or incomplete examinations may result in the need for repeat procedures or alternative investigations. This has an impact on cost and resources. Good bowel preparation is, therefore, essential for high quality colonoscopy.
Aims and Methods: The aim of this study was to analyse the characteristics of patients referred for colonoscopy and to devise a risk score to predict inadequate bowel preparation. This score could be used to identify those patients who require additional measures to ensure good bowel preparation. Data were gathered retrospectively using endoscopy reports, medical notes and nursing records. All patients had received the same bowel preparation (Citramag and Senna). The endoscopist’s judgement of the quality of bowel preparation (good, satisfactory and poor) was obtained from the colonoscopy report. Two groups were formed for analysis: adequate (those with good bowel preparation) and inadequate (those with satisfactory and poor bowel preparation). A total of 44 demographic and clinical parameters were analysed in order to devise the risk score using univariate statistical techniques and multivariate logistic regression.
Results: Data from 127 patient procedures was analysed (56.7% female, median age 62 years, range 21–88). 115 (90.6%) procedures were performed on out-patients. 52 (40.9%) had adequate and 75 (59.1%) had inadequate bowel preparation. Of the inadequate preparation group, 40.2% had satisfactory and 18.9% had poor mucosal views on colonoscopy. Univariate analysis identified 7 possible predictive factors which were significantly associated with inadequate bowel preparation: advancing age (p = 0.045), residence in a nursing home (p = 0.006), lack of capacity to consent (p = 0.049), male gender (p = 0.002), restricted mobility (p = 0.007), procedure not on Monday (p = 0.039) and procedure on a morning list (p = 0.001). Following multivariate analysis, only the latter four factors reached statistical significance as independent risk factors for inadequate bowel preparation. Each of these four factors was assigned 1 point on a scoring system. Using this score, 80.3% of patients with a score of ⩾2 and all patients with a score of ⩾3 had inadequate bowel preparation in this cohort.
Conclusion: This study has identified risk factors for inadequate bowel preparation. Using these factors a predictive four point risk score has been devised. A score of ⩾3 was highly predictive of inadequate bowel preparation. A further study is planned to validate the scoring system prospectively.
PW327 EFFICACY, ACCEPTABILITY AND SAFETY OF MOVIPREP VS CITRAMAG VS KLEANPREP IN PATIENTS UNDERGOING COLONOSCOPY
N. M. Kelly, C. Rodgers, N. Patterson, G. Jacob, I. Mainie. Gastroenterology, Whiteabbey Hospital, Belfast, UK
Introduction: Colonoscopy is considered to be the gold standard for investigation of the large bowel. Several proprietary preparations are available for bowel cleansing and KleanPrep (Macrogol 3350; Norgine Pharmaceuticals) is most commonly used in our unit. Patients frequently report that its large volume and bad taste make it difficult to take.
Aims and Methods: To compare tolerability and efficacy of KleanPrep, MoviPrep (PEG 3350; Norgine Pharmaceuticals Ltd) and Citramag (MgCO3; Sanochemia UK Ltd) for elective colonoscopy. A single-blinded study was carried out from October 2007–February 2008. Patients attending the nurse led pre-assessment clinic were allocated to one of the three treatment groups. Patients with Grade III–IV NYHA heart failure or significant renal impairment (eGFR<30) were excluded from the study. Patients completed a questionnaire reporting acceptability of the agent used. A blinded colonoscopist, using a standardised rating scale, scored the colon cleansing for each procedure.
Results: 259 patients recruited (86 MoviPrep, 92 KleanPrep, 81 Citramag). 45.65% of patients rated KleanPrep as tasting unpleasant (vs 10.47% MoviPrep p = 0.008; vs 9.88% Citramag p<0.0001). 19.6% of patients prescribed KleanPrep were unable to take the complete dose (vs 1.16% MoviPrep p<0.0001; vs 1.23% Citramag p<0.0001). Cleansing scores rated as “pass” in 3 groups (KleanPrep, MoviPrep and Citramag, respectively) were 73.9%, 74.5% and 86.5% (p<0.05 for Citramag vs KleanPrep). No adverse events were recorded.
Conclusion: Patients frequently reported that KleanPrep tastes unpleasant and a significant proportion of patients did not take the prescribed dose. Low volume cleansing agents were better tolerated and cleaned the colon equally effectively as KleanPrep. In clinical practice these advantages may lead to improved colonoscopy completion rates and enhanced diagnostic accuracy.
PW328 DO “HANDS ON” TRAINING COURSES IN ENDOSCOPIC RETROGRADE CHOLANGIOPANCREATOGRAPHY AFFECT SUCCESS RATES OF PROCEDURES?
N. S. Stern, R. Kuruvilla, H. L. Smart. Gastroenterology, Royal Liverpool University Hospital, Liverpool, UK
Introduction: Endoscopic retrograde cholangiopancreatography (ERCP) is a highly technical procedure requiring skilled operators for successful outcomes. Based at the Mersey School of Endoscopy we run “hands on” training courses for basic skills in ERCP to improve standards. Concerns have been raised about the outcomes of procedures performed as part of training courses.
Aims and Methods: Our aim was to compare ERCP success rates between those performed on a training course and those undertaken as part of normal departmental activity. A retrospective audit was performed using departmental records and computer system to access demographic data, indications and outcome. Endoscopy unit adverse event records were used to look for complications of ERCP. All patients having procedures as part of ERCP training courses (n = 12) from October 2003 to June 2008 were included. A control group of procedures, performed over 1 week, 2 weeks before the training course, was used as a comparator.
Results: 144 patients attended on courses with 134 controls. Age, gender and indications were similar in both groups (see table) except for tertiary pancreatic work only being done outside of courses. There was no significant difference in identification of the papilla (98.5 vs 94.8%, p = 0.078) or cannulation of the common bile duct (CBD) (92.1 vs 94.2%, p = 0.512). More pre-cut papillotomies were performed outside of courses (4.2 vs 11.2%, p = 0.032). Most cases were grade 1 ERCPs (77.8 vs 79.9%, p = 0.975) with similar numbers of grade 2 cases (18.8 vs 16.4%, p = 0.536). Known grade 3 cases were done outside of courses (0.7 vs 3.7%, p = 0.088). Complete stone extraction was successful in similar numbers of patients (<1 cm, 100 vs 95.5%, p = 0.117; >1 cm, 66.7 vs 70%, p = 0.856). Stent insertion was successful in all patients in both groups, whether low stents or hilar. Recorded complications were infrequent and did not differ between the two groups.
Conclusion: Endoscopy training courses are important in promoting high quality and safe procedures. In terms of ERCP “hands on” basic skills training, our data confirm that patients are as likely to have a successful procedure as part of the course with no increase in reported adverse events, when compared to those performed as part of normal clinical practice.
PW329 ACCURACY OF COLORECTAL CANCER LOCATION BY COLONOSCOPISTS
N. Chandra, S. D. Sharma, G. Davies, A. S. McIntyre. Gastroenterology, Wycombe Hospital, High Wycombe, UK
Introduction: The National Bowel Cancer Screening Programme (NBCSP) has set a standard that >95% of colorectal cancers (CRC) should be identified in the correct segment of colon at the time of colonoscopy.1 A previous UK study reported that localisation by colonoscopists was poor with only 61% of tumours correctly identified.2
Aims and Methods: The aim of this study was to determine the accuracy of colonoscopists in identifying the location of CRC. A retrospective analysis was performed for all endoscopically diagnosed CRCs at our institution between January 2005 and June 2008. For each patient, data including tumour location according to bowel segment was extracted from the colonoscopy report. Tumour location was compared with the CRC site as stated on the histopathology report once the patient had undergone surgical resection. A discrepancy of more than one segment deemed the colonoscopist to be inaccurate in their identification of tumour position.
Results: 174 patients were found to have histologically confirmed tumours. 3 patients had colorectal cancer in two locations giving a total of 177 cases of CRC cancer. 90 patients were male and 84 were female. 60% of all tumours were located within the rectosigmoid area, and 62% of patients were aged between 60–79 years at the time of diagnosis. Endoscopists identified tumour location in the correct segment of the colon in 153 (86.4%) cases, while location within one bowel segment was found in 174 (98.3%) cases (Spearman’s Rank correlation coefficient = 0.994, p<0.001). Consultants were significantly better at localising CRC at colonoscopy compared with Specialist Registrars (92% vs 69%, χ2 = 13.3, p<0.001). Correct identification of tumour position was comparable between surgeons and gastroenterologists (89% vs 84%, χ2 = 0.840, p = ns). Two out of 12 colonoscopies performed by general practitioners were incorrectly localised. Correct localisation of CRC within the rectosigmoid area was not significantly better than localisation of lesions within the proximal colon (86% vs 87%, χ2 = 0.048, p = ns). The reasons given for the 3 CRCs with >1 segment discrepancy included inadequate bowel preparation and pathology encountered.
Conclusion: This study demonstrates the highest accuracy of colonoscopists in correctly identifying CRC position to date.2 3 Despite this, the standard set by the NBCSP has still not been achieved. This highlights the need for the widespread use of adjunctive localising techniques such as endoscopic tattooing and use of scope guides. Given these results, a region-wide audit of endoscopic localisation is currently underway.
PW330 CURRENT PRACTICES FOR ASSESSING COLONOSCOPY BOWEL PREPARATION IN THE UK AND THE EVALUATION OF A NOVEL STANDARDISED CLASSIFICATION
1P. Marden, 1T. Creed, 2B. Colleypriest, 2D. Gavin, 2D. Robertson. 1Gastroenterology, Bristol Royal Infirmary, Bristol, UK, 2Gastroenterology, Royal United Hospitals Bath, Bath, UK
Introduction: Interpreting studies assessing efficacy of bowel preparations is difficult due to the lack of a universal classification. We assessed how UK endoscopists currently reported bowel preparation and to what extent a novel standardised classification method was usable and reliable in clinical practice.
Aims and Methods: Colonoscopists were surveyed by written questionnaire. Methods of recording bowel preparation, yearly endoscopic activity and attitudes to a novel classification—the Marden Bowel Preparation Classification (MBPC*)—were recorded. To assess usability and reproducibility, colonoscopists completed a questionnaire grading bowel preparation for 10 colonoscopy pictures showing procedural luminal views using the MBPC. Pictorial data were analysed using the proportion of overall agreement method, and non-parametric bootstrap to calculate confidence intervals. Subsequently the MBPC was validated in 50 consecutive colonoscopies by two independent endoscopists to assess its inter-user reproducibility in clinical practice. Colonoscopy inter-observer reliability was assessed using Pearson’s correlation coefficient and linear regression modelling.
Results: 128 endoscopists completed both questionnaires. Ten separate methods of assessing bowel preparation were described. 54% of respondents used 2–4 subjective descriptive categories such as poor, adequate, good and excellent. 19% wrote findings in the free text of reports and 11% used the Endoscribe reporting tool. 10% never commented on bowel preparation. 75% agreed a standardised grading scale for assessing the quality of bowel preparation was desirable. For the pictorial questionnaire, the proportions of overall agreement were 0.645 with a 95% confidence interval (0.602 to 0.707) for endoscopists who performed <100 colonoscopies/year (n = 90) and 0.683 with a 95% confidence interval (0.660 to 0.712) for endoscopists who performed >100 colonoscopies/year (n = 38). During colonoscopy the Pearson’s correlation coefficient (r) for bowel preparation classifications by independent endoscopists was 0.9672 (p<0.0001) and using linear regression the y intercept was 0.0023 and the slope 0.986. This shows a high level of correlation and score reproducibility between two endoscopic assessors.
Conclusion: Reporting of bowel preparation findings is currently disparate and highly subjective. The MBPC is a validated classification which standardises bowel preparation reporting with good levels of prospective reproducibility.
*MBPC. Grade 1 = >90% mucosa assessable—suction/moving patient allowed. Grade 2 = >90% mucosa assessable needed washing. Grade 3 = <90% mucosa assessable despite washing. Grade 4 = Stool obstructing lumen or preventing safe advancement of colonoscope. Each segment is assessed upon withdrawal (caecum, ascending, transverse, descending, sigmoid and rectum).
PW331 STUDY OF THE ILEOCAECAL VALVE CUSP MOVEMENTS IN LIVE NORMAL ADULTS USING VIDEO RECORDINGS DURING COLONOSCOPY
1P. S. Fernando, 1S. S. Salgadu, 2K. I. Deen. 1Anatomy, Faculty of Medicine, Ragama, Sri Lanka, 2Surgery, Faculty of Medicine, Ragama, Sri Lanka
Introduction: Direct visualisation is the best method to observe the morpho-functional features of a biological structure that changes its shape according to its functional needs. Currently available investigative tools cannot be used for prolonged observation of the ileocaecal valve. Colonoscopy may be useful to observe this valve, the function of which is still poorly understood.
Aims and Methods: Patients undergoing colonoscopy were selected to visualise the ileocaecal valve after obtaining informed written consent. 13 healthy individuals undergoing screening were studied through 121 minutes of continuous video recording. All individuals had had similar bowel preparation.
Colonoscopic views were recorded on magnetic tape. Ileocaecal videography was used to analyse the morphology and function of the ileocaecal valve. The following features were observed; shape of the valve orifice at resting position, appearance and size of the valve cusps, contractions of the valve cusps per minute, ejection of effluent per minute and active movements of the caecum per minute.
Results: The valve orifice was observed to be at rest alternating with periods of contraction. Contractions of the valve cusps seemed to change the shape of its orifice. In 11 subjects, during the resting period of the valve, the orifice was semilunar and either closed or partially closed. These subjects had a longer and more curved superior cusp. The valve cusps were thickened in 6 subjects, while 7 had narrow valve cusps. In all, 60 (mean – 5 per subject) active movements were observed in the ileocaecal valve cusps and 14 active caecal contractions were observed. The frequency of active movements of the valve was 0.5 movements per minute. Ejection of effluent was observed on 49 occasions (mean – 4 ejections per subject). Chime was ejected in 15 instances and air in 34. The ejection of effluent was always associated with active movements of the valve cusps. By contrast, some cusp movements were observed to be independent of the onward flow of effluent.
Conclusion: Videographic assessment suggests the presence of a valve mechanism in the majority. Valve movements were not always associated with propulsion of chime into the caecum, a phenomenon that may be associated with “housekeeping” activity of the terminal ileum. Thus, the ileocaecal valve demonstrated features of a flap valve.
PW332 VIDEO CAPSULE ENDOSCOPY: WHAT NEXT?
P. T. Rajasekhar, C. Davison, S. J. Panter. Gastroenterology, South Tyneside District Hospital, South Shields, UK
Introduction: Diagnostic video capsule endoscopy (VCE) is useful but if histology or therapeutics are required a further endoscopic modality must be chosen. We reviewed our data to evaluate how many needed further procedures, including repeat VCE, and by which modality.
Aims and Methods: All VCEs at South Tyneside District Hospital (June 2004–February 2008) were reviewed. We recorded the indication and, in relevant cases, the position of the lesions. Times of duodenal and colonic entry were noted and small bowel transit time (SBT) calculated. We used lesion time to determine which subsequent modality to choose. Where more than one lesion was present, the single modality that allowed access to all was chosen. Where the examination was incomplete but lesions amenable to treatment or biopsy were noted, results were included in the relevant endoscopic modality and repeat VCE groups. The modalities were chosen as follows: push enteroscopy (PE) 1, lesion within 60 minutes of duodenal entry, PE 2 within 10% of SBT, double balloon enteroscopy (DBE) oral within 75% of SBT, DBE anal beyond 75% SBT and ileocolonoscopy if the lesion was at the terminal ileum, ileocaecal valve or colon.
Results: 219 VCE studies were performed. 14 were repeat VCE due to initial incomplete examinations/poor views. 8 required endoscopic duodenal placement. 71 had positive findings (explaining symptoms) of which 67 potentially required further procedures, 30 for therapeutics and 37 for histology (see table). 74 had normal or insignificant findings and 72 were inconclusive, 45 due to an incomplete examination of the small bowel or poor views and 27 due to findings not explaining symptoms. 2 capsules failed.
Conclusion: Video capsule endoscopy is a simple and well tolerated method of small bowel examination but without histology is simply descriptive. From our data a significant proportion (21.9%) of patients require PE or DBE to provide diagnostic histology or perform therapeutics. With the increasing use of VCE, we suggest the demand for DBE will also rise requiring investment in service provision and training.
PW333 VIDEO CAPSULE RETENTION: A GOOD THING?
P. T. Rajasekhar, C. Davison, S. J. Panter. Gastroenterology, South Tyneside District Hospital, South Shields, UK
Introduction: Video capsule endoscopy (VCE) is increasingly used to visualise the small bowel. The principal indications include the investigation of obscure gastrointestinal bleeding and the diagnosis and assessment of Crohn’s disease. The most serious complication is capsule retention. It has been shown that the use of a patency capsule can successfully predict those in whom this is most likely.
Aims and Methods: We reviewed the results of patients who underwent video capsule endoscopy preceded by a patency capsule at South Tyneside District Hospital between June 2004 and February 2008. A radiofrequency scanner was used to detect the presence of the patency capsule at 24 to 30 hours after ingestion. Patients who scanned positive went on to have a plain abdominal x-ray (AXR) and subsequently a limited CT scan if localisation was difficult.
Results: 219 patients underwent VCE of which 61 (28%) had a preceding patency capsule. Of those, 10 scanned positive with the radiofrequency scanner. All went on to have a plain abdominal x-ray and this identified the patency capsule in the colon in 6 cases. Where there was doubt (n = 4) a limited CT scan the same day was performed. The CT scan identified the patency capsule to be still within the small bowel in 2, the remainder being in the colon. All patients in whom the scan was negative or in whom the patency capsule was shown to have reached the colon had an uncomplicated VCE study. The 2 patients in whom the patency capsule was noted to be in the ileum elected to go ahead with the VCE, accepting the extremely high risk of retention. Predictably this complication occurred requiring a laparotomy which diagnosed small bowel strictures. The presence of the VCE aided localisation of the pathology at surgery.
Conclusion: The use of a patency capsule prior to VCE in high risk patients does provide accurate information as to the risk of VCE retention. In the majority of cases the position of retained patency capsule can be accurately identified using plain abdominal radiology. A limited CT is occasionally required in cases where doubt remains. We would certainly recommend the use of patency capsule prior to VCE in those patients where small bowel narrowing is suspected. Subsequent predictable VCE retention is not always a negative outcome and can be useful in localising pathology when surgical intervention is required.
PW334 AUDIT OF CLINICAL INDICATION FOR RECALL ENDOSCOPY IN 974 PATIENTS
R. Shah, D. Chan, D. H. Dewar. Gastroenterology, Surrey and Sussex Healthcare NHS Trust, Redhill, UK
Introduction: Our institution comprises 13 Gastrointestinal Consultants or Associate Specialists across three separate hospitals, although all endoscopy is carried out in a single unit. As part of a major overhaul of endoscopy governance, we wished to establish audit standards for patients awaiting recall endoscopy in our institution.
Aims and Methods: In line with JAG standards, we wished to validate all patients on our unified endoscopy database who were scheduled for recall procedures. The aim was to audit recall patients against BSG standards and rationalise our recall list appropriately.
Results: In total 974 patients were overdue for recall endoscopy, comprising 720 colonoscopies (74%) and 254 gastroscopies. After validation only 202/974 procedures (21%) were considered overdue (43 gastroscopies, 159 colonoscopies). Overall 469 (48%) patients were deemed not to require their procedure (92 gastroscopies, 377 colonoscopies). The clinical indications in 299 patients were outside of BSG standards and a further 98 patients were no longer suitable on grounds of age or co-morbidity. 303 (31%) patients had their endoscopy recall date postponed by a median of 23 months (26 gastroscopies, 277 colonoscopies). Overall 772 (79%) patients were incorrectly appointed for recall (118 gastroscopies, 654 colonoscopies). Of these 88/118 gastroscopies (75%) concerned Barrett’s oesophagus with advanced age and co-existing comorbidity being the commonest reason for adjusting recall. Out of 654 adjusted colonoscopies, 401 (61%) concerned polyp follow-up, 75 (11%) concerned colorectal cancer follow-up, 104 (16%) related to family history of colorectal cancer and 70 (11%) to inflammatory bowel disease surveillance. In review of the 401 adjusted colonoscopies for polyp follow-up, the commonest reason for alteration was continued follow-up after an appropriate number of negative colonoscopies (45%). In review of the 104 cases of family history screening, the predominant reason for adjustment was incorrect interpretation of low risk family history as moderate or high risk in 85% of cases.
Conclusion: Using BSG guidelines to retrospectively audit our endoscopy recall requests, 48% of cases were not clinically indicated and a further 31% could be postponed by a median of 23 months. This significantly contributed to reducing endoscopy demand and assisting in attaining our 18 week target.
PW335 DOES THE BLIND SLIM ENDOSCOPIC ULTRASOUND SCOPE USED IN STRICTURING OESOPHAGEAL MALIGNANCY STAGING, INCREASE COMPLICATION RATE AND NEED FOR EXTRA SEDATION?
1M. Ganesh, 2R. Kalaiselvan, 2J. Vickers. 1Gastroenterology, Salford University Hospital, HOPE, UK, 2Surgical Gastroenterology, HOPE, Manchester, UK
Introduction: Endoscopic ultrasound (EUS) has revolutionised the staging of oesophageal malignancies. The use of EUS for staging oesophageal tumour is on the rise. Slim EUS scope is mainly used to stage stricturing oesophageal tumours where forward viewing large EUS scopes could not pass through. The slim scope is blind, without any forward viewing facility, theoretically increasing the risk of perforations. The scope is introduced blindly into the oesophagus through a wire guided system, traversing the stricture. Endoscopic ultrasound scanning is performed over the wire guided system.
Aims and Methods: This study is aimed to compare any difference in complication rate and the need for extra sedation used between the slim and large radial EUS scope. A retrospective analysis was performed on 171 patients who underwent EUS procedures between May 2006 and August 2008 in a tertiary care hospital.
Results: 75 (43.9%) patients underwent slim EUS scope examination for staging stricturing oesophageal tumours. Majority of the patients had lower oesophageal stricture 55 (73.3%), 14 mid oesophageal and 5 upper oesophageal stricturing tumour. None of them needed dilation of the strictures. 96 (56.1%) patients did not have strictures and underwent large EUS probe examination. All patients received a combination of midazolam and pethidine for sedation along with xylocaine throat spray. Out of 171 patients 150 (87.7%) received IV midazolam 5 mg and 162 (94.7%) received IV pethidine 50 mg as a baseline sedation. 21 patients received <5 mg midazolam dose. 9 patients who had <5 mg midazolam also had lesser dose of pethidine (25 mg). 7 patients had COPD, only 2 of them needed <5 mg midazolam, and none of them had any complications reported. There were no reported complications including perforation or aspiration pneumonia in both groups. 1 patient in the large probe group dropped oxygen saturation to 90% needing flumazenil for reversal. 15 (8.8%) out of 171 patients needed extra added sedation from the baseline 5 mg. 9 (60%) patients were from the large EUS scope group and 6 (40%) from the slim scope group. None of them received extra pethidine on the top of the base line dose. There was no statistically significant difference (p<0.59) between extra amount of sedation used in slim and large EUS scope groups.
Conclusion: There were no complications reported with the use of blind slim EUS scope in our study population. There is no difference in extra amount of sedation used between slim and large EUS scope group. Our study shows that blind slim EUS scope is as safe as the large forward viewing radial EUS scopes.
PW336 ENDOSCOPIC APPLICABILITY OF LOW COST VARICEAL BANDING LIGATION KITS TURNED OUT FROM URINARY CATHETERS: A BREAKTHROUGH INNOVATION FOR THE SOCIO-ECONOMICALLY DEPRIVED
R. L. Satarasinghe, M. A. R. Jayawardana, U. D. U. K. Wickramasingha, A. A. A. Riyaaz, R. Wijesinghe. Department of Medicine, Sri Jayewardenepura General Hospital and Postgraduate Training Center, Nugegoda, Sri Lanka
Introduction: To invent an alternative, low cost, safe, effective and reproducible kit for banding ligation of oesophageal varices suitable for developing countries, and to study the immediate and long term outcome of the results of such therapy as banding ligation of significant oesophageal varices has become the safest cornerstone treatment to save life in variceal bleeding.
Aims and Methods: The alcoholic and non-alcoholic patients who were endoscopically diagnosed to have Grade III–IV oesophageal varices admitted to the principal author’s unit from 1 November 2003 to 30 April 2008 were offered banding ligation, with bands turned out by slicing of 1 mm bands from a 14 G urinary catheter which was meticulously molded on to a ligating unit, using a string mechanism. The ligating unit was fitted onto a standard gastroscope. The bands were freed using a release mechanism following sucking of the varix into the ligating unit. The kit was disinfected using biodegradable PERAsafe® 10 minute medical device sterilant, prior to usage, similar to the endoscope disinfection. The patients were explained about the procedure and were given the option to select either the commercially available banding kit (cost $160 USD) and the locally made kit (cost $30 USD). Written consent was obtained prior to the procedure.
Results: The total population selected to buy the low cost banding kit. The total study population comprised 165 males and 25 females, with the characteristics shown in the table. Both groups were followed up to 1–5 years. Both groups who underwent secondary banding ligation, had effective control of variceal banding, without recurrences until the next session of banding, and had no complications during the follow up period.
Conclusion: The low cost banding set produced from the urinary catheters are very safe and effective in arresting variceal bleeding like the costly imported commercially available bands, which is an ideal alternative for developing countries.
We are extremely grateful to our endoscopic assistant, Mr AAA Perera, who was the inventor of the low cost bands.
PW337 COLONOSCOPIC PHOTOGRAPHY: IS IT ENOUGH TO PROVE COMPLETION OF COLONOSCOPY?
R. M. P. Mathew, M. M. Ahmed, C. H. Lim. Gastroenterology, Good Hope Hospital, Birmingham, UK
Introduction: Ileocaecal intubation is considered the gold standard at colonoscopy. Permanent documentation of completion can be achieved by photographing the caecum/ terminal ileum (TI) or by taking biopsies of the TI. The latter practice is discouraged in view of fears concerning transmission of prion disease.
Aims and Methods: To assess if photography is adequate in documenting completion of colonoscopy. Between 27 March 2006 and 11 September 2006, two consultant gastroenterologists performed 144 consecutive colonoscopies. In all cases the caecum was reached and the terminal ileum was intubated and biopsied to confirm completion. In each case, at least three “good” photographs were taken showing the TI, caecum and elsewhere in the colon. Photographs were digitalised and presented in a random order to raters (medical and surgical colonoscopists and endoscopy nurses). Raters were asked to determine if the photograph was of TI, caecum or elsewhere. Individual accuracies were determined and inter-observer agreement was calculated using kappa statistics (Stata v 8).
Results: 144 colonoscopies were performed (63 male; 81 female; median age 55.5 years, range 19–87 y). Median times to reach caecum, TI and completion were 13 minutes, 15 minutes and 28 minutes, respectively. A total of 569 photographs were taken (TI: 163, caecum: 240, other: 166). The 11 raters comprised 6 consultants (5 physicians, 1 surgeon; all colonoscopists), 3 SpRs (2 physicians, 1 surgeon) and 2 experienced endoscopy nurses. Individual accuracy in correctly assessing the site of the photograph ranged from 43.4% to 73.6%. The kappa between any two assessors ranged from 0.19 to 0.83. The kappa among consultants, SpRs and nurses were 0.38, 0.43 and 0.83, respectively. Agreement according to site was as follows: TI (kappa 0.54), caecum (kappa 0.43), other (kappa 0.33), combined (kappa 0.42). The two original colonoscopists were asked to rate the photographs 1 year later and the individual accuracies were 80.5% and 81.7% with a kappa agreement of 0.75.
Conclusion: Even when assessed by experienced colonoscopists, photographs alone do not “prove” completion of colonoscopy and inter-observer agreement is far from perfect. This may have medico-legal ramifications. In our view, a biopsy of the terminal ileum remains the gold standard to document completion.
PW338 CAN MICROSCOPIC COLITIS BE DIAGNOSED FROM LEFT SIDED COLONIC BIOPSIES ALONE?
1R. M. Palmer, 1F. M. Thompson, 2M. McCole, 1A. S. Mee. 1Gastroenterology, Royal Berkshire Hospital, Reading, UK, 2Histopathology, Royal Berkshire Hospital, Reading, UK
Introduction: Microscopic colitis (MC) is an important and easily overlooked cause of chronic diarrhoea1 characterised by watery, non-bloody stools.2 Colonoscopy reveals macroscopically normal mucosa but biopsies show characteristic histological features3 traditionally said to be most prominent in the right colon, although these data are based on small studies.4 5
Aims and Methods: If MC could be diagnosed from left sided biopsies, this would both minimise patient discomfort and risk by avoiding the need for colonoscopy, and reduce demand on endoscopy resources. Our aim was to elucidate whether left sided colonic biopsies might be sufficient for a diagnosis of MC. We identified 123 patients with histologically proven MC from biopsies taken at rigid or flexible sigmoidoscopy and colonoscopy over a 5 year period (Feb 03–Feb 08). 12 were excluded as no left sided biopsies were taken, or site of biopsy was not recorded.
Results: In total there were 111 cases of MC. Of these, 72 (65%) were female; 51 cases were lymphocytic colitis, 53 collagenous colitis, and 7 cases showed mixed features or were not otherwise specified. 105/111 (95%) had left sided biopsies that were diagnostic of MC. 43 patients had undergone colonoscopy, of whom 37 had left sided biopsies confirming a histological diagnosis of MC. In this cohort, 11 of 17 rectal biopsies and 29 of 34 sigmoid biopsies were diagnostic, while all (13/13) descending colon biopsies were diagnostic.
Conclusion: In the series of patients who underwent full colonoscopy we demonstrated a diagnostic yield of 65% for rectal biopsies, 85% for sigmoid biopsies, and 100% for descending colon biopsies. In total, 86% of the cases of MC diagnosed at colonoscopy had diagnostic changes on biopsies from the left colon. Interestingly, of the 14% of cases requiring right sided biopsies for diagnosis, none had descending colon biopsies taken. This raises the intriguing possibility that a left sided diagnosis could have been made if the descending colon had been examined. Our study indicates that flexible sigmoidoscopy with descending colon biopsies is adequate to diagnose the vast majority of cases of MC. Therefore we propose that flexible sigmoidoscopy is the investigation of choice in patients with suspected MC with no other worrying features indicating the need for full colonoscopic assessment. This practice would help minimise the risk and discomfort to the patient and reduce demand on endoscopy resources.
PW339 DOUBLE BALLOON ENTEROSCOPY EXPERIENCE FROM A TERTIARY CENTRE IN THE UK
R. Sidhu, M. E. McAlindon, S. Hardcastle, D. S. Sanders. Gastroenterology, Royal Hallamshire Hospital, Sheffield, UK
Introduction: Double balloon enteroscopy (DBE) is a novel technique that has the potential to allow pan-endoscopic visualisation of the SB, with the ability to perform therapeutic intervention. Despite this, there are few centres in the UK which offer this modality of investigation.
Aims and Methods: To assess the diagnostic yield of DBE and impact on patient management in a UK tertiary setting. Data were collected prospectively on all patients referred for DBE over 26 months. Case notes were reviewed for patient demographics and referral indications. All patients had capsule endoscopy (CE) prior to DBE and the route for DBE was directed by the location of abnormality on CE. DBE findings, therapeutic intervention performed and subsequent change in management were noted.
Results: 58 DBE procedures were performed in 41 patients between July 2006 and September 2008. 66.7% of the referrals originated from outside the region. 25 patients had DBE via the oral route and 33 patients had DBE via the anal route. 63% were female with a mean age of 53 years (range 20–77 years). The indications were obscure gastrointestinal bleeding–overt bleeding (n = 6) and iron deficiency anaemia (n = 22), suspected Crohn’s disease (n = 11), malabsorption (n = 1) and assessment of polyps (n = 1). Five patients were transfusion dependent while 12% had significant cardiovascular co-morbidity. The mean procedure time was 70 minutes (range 2–120) with no reported complications. The overall diagnostic yield was 44%. The diagnoses were angiodysplasia (n = 5 /12%), ulcers (n = 10 /24%), tumour (n = 1 /2.4%) and lymphangiectasia (n = 1/2.4%). DBE was normal in 56% and unsuccessful in 4 patients (3 anal route, 1 oral route) due to poor patient tolerance. Intervention was performed in 15% of patients, in the form of argon plasma coagulation in 83.3% and application of clips in 16.7%. Management was altered in 32% of patients. This included intervention to bleeding points at DBE (n = 6), inflammatory bowel disease (IBD) directed therapy (n = 4), referral for surgery (n = 1), helicobacter eradication (n = 1) and cessation of non-steroidal anti-inflammatory drugs (NSAIDs, n = 1). The diagnostic yield was not significantly different when comparing referral indications (p = 1) or whether referred from outside the region (p = 0.4).
Conclusion: Our experience from a tertiary centre in the UK has shown that DBE is a useful modality for diagnostic and therapeutic intervention in patients with suspected small bowel pathology. BE has a high diagnostic yield, low complication rate and a positive impact on patient management. Larger studies are required particularly in high risk patient groups before advocating its use in routine clinical practice.
PW340 IS CONSCIOUS SEDATION ADEQUATE FOR DOUBLE BALLOON ENTEROSCOPY? A STUDY ON PATIENT TOLERABILITY WITH CONTROLS
R. Sidhu, M. E. McAlindon, S. Hardcastle, D. S. Sanders. Gastroenterology, Royal Hallamshire Hospital, Sheffield, UK
Introduction: Double balloon enteroscopy (DBE) is a novel endoscopic technique but the optimal type of sedation/anaesthesia for it is currently unknown. International DBE studies report using conscious sedation, propofol or a general anaesthetic. In the UK, endoscopic procedures are generally done under conscious sedation with benzodiazepines ± an opiate. The use of a general anaesthetic for endoscopy is rare and propofol is unlicensed without an anaesthetist.
Aims and Methods: To assess patient tolerability for DBE in the UK, using conscious sedation. Data were collected prospectively on all patients referred for DBE over 26 months including DBE route, procedure length and amount of sedation. A previously validated sedation scoring system was used. The quality of sedation and tolerability was evaluated by the endoscopists (1 = excellent, 2 = good, 3 = fair and 4 = poor) and the patient (1 = no discomfort/ unable to remember, 2 = slightly uncomfortable, 3 = extremely uncomfortable, 4 = unacceptable). Patients were asked to compare their DBE experience to conventional endoscopy (colonoscopy and gastroscopy) and if they would prefer DBE under a general anaesthetic. Patients undergoing colonoscopy and gastroscopy under sedation by a single endoscopist were used as controls. Multiple logistic regression was used to investigate the relationship between procedural parameters and patients’ tolerability. The agreement of tolerability between the endoscopist and the patients was assessed using kappa statistics.
Results: 33 patients underwent 48 DBE procedures (22 anterograde and 26 retrograde) over 25 months, 62% females, mean age 55 years (range 20–77 years). The median doses of midazolam and fentanyl used was 6 mg (range 1.5–36 mg) and 50 μg (25–75) respectively (median dose midazolam for oral DBE: 8 mg and anal DBE: 5 mg (p = 0.6)).The agreement between the patient and the endoscopist on tolerability of the procedure was fair (kappa = 0.27). There was no significant difference between patient scores and gender (p = 0.39) and the route of DBE (oral/anal) (p = 0.64).There was also no correlation between tolerability and either duration of procedure (p = 0.4) or degree of sedation (p = 0.9). Although 62.5% of patients found DBE extremely uncomfortable or unacceptable, 67% would have DBE repeated if clinically necessary. However, 65% would choose a general anaesthetic if offered. Patients undergoing routine gastroscopy (n = 35) and colonoscopy (57) under sedation ± entonox were used as a comparative group to DBE patients, mean age 56.5 years (range 20–81 years). The mean dose of midazolam used in the control group was 2.5 mg (range 0–5 mg). In comparison to oral DBE, patients tolerated gastroscopy significantly better (p = 0.045). Similarly, patients tolerated colonoscopy better than anal DBE (p<0.001).
Conclusion: A significant proportion of patients tolerate DBE sub-optimally compared to conventional endoscopic procedures. Our data suggest that the combination of midazolam and fentanyl may be inadequate for this procedure.
PW341 THE USE OF FAECAL LACTOFERRIN AS A NON-INVASIVE MARKER IN THE DIAGNOSIS OF COLORECTAL DISEASES: PILOT DATA
1R. Sidhu, 2P. Wilson, 2L. Foye, 1M. E. McAlindon, 2S. Morley, 1A. J. Lobo, 1D. S. Sanders. 1Gastroenterology, Royal Hallamshire Hospital, Sheffield, UK, 2Clinical Chemistry, Royal Hallamshire Hospital, Sheffield, UK
Introduction: Lower gastrointestinal (GI) symptoms are a common presentation for referral to the gastroenterology service. Alarm features such as weight loss, a change in bowel habit and increasing age are factors which help predict a higher diagnostic yield with colonoscopy. However, the majority of routine colonoscopies are normal. Faecal lactoferrin (FEL) is a useful non-invasive marker for detecting the presence of inflammation in the GI tract. It has also been found to be positive in patients with inflammatory bowel disease (IBD) and infective diarrhoea. There is a paucity of data on the use of FEL in the detection of other gastrointestinal diseases.
Aims and Methods: To investigate the clinical utility of FEL in the detection of organic disease in the colon in routine clinical practice. To assess its suitability as a screening tool for referral to secondary care. Patients undergoing colonoscopy (routine/urgent/cancer pathway) were recruited from the outpatient clinic and via the post, pre-procedure. Patients were requested to return a stool sample in the specimen container provided. Data were collected prospectively including demographics, clinical presentation and indication for colonoscopy. Quantitative analysis using sandwich ELISA was performed for faecal lactoferrin. The data were analysed using SPSS and sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) were calculated.
Results: 88 patients were recruited from May to Sept 2008. Patients were subdivided into >50 years (n = 78) and <50 (n = 10). In the >50 group, the mean age was 62 years with 54% male. The mean FEL (μg/g) ± SE was 6.26±2.2 in patients > 50 and 0.12±0.12 in patients <50 (p = 0.004, 95% CI 2 to 10). Pathology was found in 43% of colonoscopies. The diagnoses included rectal cancer (n = 1), IBD (n = 5), diverticular disease (n = 12), polyps (n = 20) and miscellaneous (n = 4). FEL was normal in all patients <50 years, while colonoscopy was normal in all bar one patient with diverticular disease in this group. The sensitivity and specificity of FEL for detecting inflammatory colorectal pathology (IBD/cancer) was 100% and 93% respectively while the positive and negative predictive values were 50% and 100%. FEL was poor for the detection of hyperplastic (n = 0/10) and adenomatous polyps (n = 1/10) and diverticulosis (n = 2/11).
Conclusion: FEL has a high sensitivity in the detection of IBD and cancer in patients >50 years. In patients <50 years, FEL has a high specificity and is useful to exclude the presence of significant colorectal disease. The use of FEL in this latter group could act as a non-invasive screening tool for primary care physicians to determine patients who should be referred for lower GI investigations in secondary care.
PW342 HIGH QUALITY ENDOSCOPY: FIELD OF VISION AND DISCRIMINATORY CAPACITY IN MODERN ENDOSCOPES
R. Mead, M. D. Duku, P. Bhandari. Gastroenterology, Queen Alexandra Hospital, Portsmouth, UK
Introduction: Current endoscopes describe visual abilities by “angle of view” which is standard at 140 degrees for gastroscopes (except transnasal gastroscope) and colonoscopes made by all manufacturers. However, In our practice we noticed inter- and intra-manufacturer differences. There are no data on the field of vision and clarity of images obtained by the various endoscopes from different manufacturers.
Aims and Methods: We aimed to measure and compare the field of vision and visual clarity of zoom and non-zoom gastroscopes and colonoscopes made by Fujinon and Olympus. 11 different endoscopes were assessed. We designed a visual field measuring device in which the scope could be placed at a fixed distance of 6 mm from a 1 mm graph paper and then took a picture of the graph paper. This process was repeated five times. “Visual field” was measured by counting all visible squares. In an attempt to measure the endoscopes ability to discriminate v. small lesions, we developed the idea of a discriminant field. Squares were counted for the “discriminant field” when all four sides could be clearly seen.
Results: Gastroscopes—no significant differences between zoom and non-zoom gastroscopes were observed from the same manufacturer, but significant differences (p = 0.002) were seen between the two manufacturers. Colonoscopes—significant differences were observed between zoom and non-zoom colonoscopes for Fujinon (p = 0.0001), unlike Olympus scopes. However, significant differences (p = 0.0001) were seen between the two manufacturers. The transnasal gastroscope (designed to improve patient comfort) had a significantly lower (p = 0.003) field of view compared to the other gastroscopes from the same manufacturer.
Conclusion: Currently, all manufacturers claim to have the same angle of view (140 degrees) for all gastroscopes and colonoscopes, but we have clearly demonstrated the differences between various scopes from the same and different manufacturers. This highlights the difficulties with the current information provided by the manufacturers and demands new standards to compare and understand the weaknesses and strengths of various endoscopes.
PW343 GASTROINTESTINAL CANCER: AN OPPORTUNITY MISSED
S. Murray, M. Nizamuddin, A. Raj, E. Seward. Gastroenterology, Whipps Cross University Hospital, London, UK
Introduction: Gastrointestinal cancer is one of the commonest causes of cancer death. Effective treatment is dependent on early diagnosis; however the disease classically presents late. It is thought that non-specific symptoms can precede presentation, in some cases by a number of years. With the increasing availability of endoscopy, these patients may have been investigated prior to their diagnosis. Endoscopy has a known miss rate, perhaps 10% in colonoscopy, and hence an opportunity to diagnose cancer early may have been missed.
Aims and Methods: We proposed to retrospectively audit all patients diagnosed at our centre with gastrointestinal cancer (oesophageal, gastric, colorectal) in the last 3 years to establish a “missed early cancer rate”, i.e. the number of patients who had been investigated with endoscopy prior to their diagnosis and found to have normal or benign findings. Every patient diagnosed with gastrointestinal cancer at our hospital between 2006 and 2008 was identified from a database of diagnosed cancers. Using our endoscopy audit tool we noted the date of the endoscopy at which the diagnosis was made. Any endoscopies 3 years prior to this date were reviewed. We noted the indications for investigation, endoscopy findings, available histology and planned follow up. An endoscopic miss was one in which the examination was complete with no relevant pathology identified, with a subsequent cancer occurring up to three years later. The patient’s records were thoroughly reviewed to clarify why the cancer had been missed.
Results: Between 2006 and 2008, 269 patients were diagnosed with gastrointestinal cancer at our centre. This was made up of 136 male and 133 female patients with an average age at diagnosis of 72. Of these, there were 52 gastric cancers, 64 oesophageal and 153 patients had colorectal cancer. The overall missed early cancer rate was 2.60% (3/116 upper, 4/153 lower).
Conclusion: The study was a retrospective case note audit so our calculated missed early cancer rate is likely to be an underestimate. However, despite this it is encouraging to see such a low miss rate compared to previously published data. New endoscopic technology such as narrow band imaging and novel practices such as emphasising longer withdrawal times could reduce this further.
PW344 “SPIRAL LOOPING” OF THE SIGMOID IS COMMONLY SEEN ON SCOPEGUIDE ENABLED COLONOSCOPY
S. Gupta, S. Thomas-Gibson, C. B. Williams. Wolfson Endoscopy Unit, St Mark’s Hospital, Imperial College, London, UK
Introduction: Use of the magnetic endoscope imager (Scopeguide®, Olympus Corporation, Tokyo, Japan) has revolutionised understanding of loop formation during colonoscopy. The classic spiral or “alpha” loop has been described as occurring in only around 10% of colonoscopies but anecdotally when it occurs, it facilitates colonoscope insertion to the splenic flexure. To date there have been few data on the impact of Scopeguide® on routine colonoscopy training and practice.
Aims and Methods: To establish the frequency and type of sigmoid loops formed during colonoscopy. For one calendar year a single experienced colonoscopist using Scopeguide® variable-stiffness colonoscope (Olympus CF-240DL) routinely documented a description of the endoscope configuration when passing the sigmoid colon.
Results: 969 consecutive colonoscopy reports were available, of which 838 were suitable for analysis. 131 reports were excluded (61 due to insufficient information, 67 patients had previous colon resection, and 3 were incomplete examinations). Spiral looping, as seen on Scopeguide® split-screen with simultaneous frontal and lateral views, was observed in 387(46%) of all patients, representing 67% of all loops. Only 3 patients showed typical “N” looping on frontal view, without any spiral element on lateral view. Complex atypical looping occurred in 168 (20%), which included substantial “S-shaped” looping in 3 patients. In 276 patients (32.8%) there was no significant sigmoid looping. Women were more likely than men to develop sigmoid looping during colonoscopy (267/334 (80%) compared to 295/504 (58%)).
Conclusion: Scopeguide® in split-screen mode (both frontal and lateral views simultaneously) demonstrates that spiral looping of the colonoscope is much commoner than previously reported. Scopeguide® facilitates a better understanding of sigmoid loop configuration during colonoscopy. Further prospective analysis may demonstrate how it can rationalise insertion through the sigmoid which is potentially the most difficult stage of colonoscopy both in training and in practice.
PW345 WHEN SHOULD WE PERFORM ILEOSCOPY DURING COLONOSCOPY? EVIDENCE FROM A UK TERTIARY CENTRE
1S. S. Sami, 2S. Sebastian. 1Gastroenterology, Scunthorpe General Hospital, Scunthorpe, UK, 2Gastroenterology, Hull Royal Infirmary, Kingston-upon-Hull, UK
Introduction: While the diagnostic yield of ileoscopy has been reported in few studies, there have been virtually no studies specifying in which clinical presentation can ileoscopy lead to a change in patient diagnosis, disease classification and/or management decisions (in terms of treatment options, further tests and follow up planning). Such information will guide endoscopists in their decision as to whether or not a terminal ileum intubation is worthwhile.
Aims and Methods: We aimed to assess the outcome of ileoscopy according to the clinical indication for colonoscopy. We reviewed 400 colonoscopies that were performed by one consultant gastroenterologist in our endoscopy unit from January 2006 to May 2007. Patients’ demographics, indications for colonoscopy, macroscopic and histological findings were recorded. We reviewed the notes for patients who had positive findings on ileoscopy and identified whether it lead to a significant yield as defined by a change in patient diagnosis, disease classification and/or management decisions.
Results: A total of 400 patients underwent colonoscopy; the mean age was 54 years and female to male ratio was 1.4: 1. The terminal ileum was intubated in 243 (60%) patients in whom macroscopic and significant histopathological abnormalities were present in 67 (28%) and 24 (10%) cases, respectively. A significant yield occurred in 26 (11%) patients who were either diagnosed with Crohn’s or possible early Crohn’s and assigned for regular follow up and/or further tests. Normal colon and isolated ileal Crohn’s was noted in 9 (4%) patients (5 diarrhoea, 2 RIF pain and 2 anaemia).
Conclusion: Ileoscopy has a significant yield in patients presenting with RIF pain (OR 3.76, 95% CI 1.08 to 13.00) or diarrhoea (OR 5.5, 95% CI 2.27 to 13.30) when compared with other presentations (OR <1.0 for all other presentations), therefore we recommend that ileoscopy should be a standard practice in these patients. Ileoscopy is also worthwhile in patients with anaemia who have a normal colonoscopy and upper GI endoscopy.
PW346 AUDIT OF ENDOSCOPIC ULTRASOUND GUIDED FINE NEEDLE ASPIRATION OF SOLID PANCREATIC LESIONS
1S. Rajkumar, 2K. Harris, 3M. Aldersley. 1Gastroenterology, Leeds General Infirmary, Leeds, UK, 2Radiology, Leeds General Infirmary, Leeds, UK, 3Hepatology, Leeds General Infirmary, Leeds, UK
Introduction: Endoscopic ultrasound (EUS) guided fine needle aspiration (FNA) is probably the best method of obtaining cytological specimens from pancreatic lesions. The diagnostic accuracy of EUS-FNA improves with participation of on-site cytopathologist1 and performing 5 × passes into pancreatic solid masses.2 Suction improves cellularity but not diagnostic yield due to blood contamination.3
Aims and Methods: We reviewed all EUS-FNAs of solid pancreatic masses performed in our tertiary referral hospital from January 2004 to December 2007, comparing the diagnostic yield of cytology from FNA with final diagnosis based on histology and clinical/radiology follow-up. The reference standard for overall diagnostic accuracy of EUS-FNA was 71% based on multicentre studies.4
Results: FNA was performed using the Wilson-Cook 22 gauge FNA needle and Olympus Curvilinear Echoendoscope without/with suction based on specimen quantity on visual examination. The FNA samples were sent in CytoRich Red fluid to cytopathology department for analysis. 86 EUS-FNAs (n = 86) were performed on 85 patients, mean age 63.4 years (range 19–89 years), male 58.8% (n = 50), female 41.2% (n = 35). The site of FNAs were head/neck 74.4% (n = 64), body/tail 25.6% (n = 22). The cytology was reported as malignant cells in 27.9% (n = 24), suspicious of malignancy 10.5% (n = 9), no malignant cells 55.8% (n = 48) and insufficient specimen 5.8% (n = 5). 69.4% (59/85) of patients had final diagnosis of cancer, confirmed by cytology from EUS-FNA 40% (n = 24), histology by other methods 33.3% (n = 20) and radiological/clinical follow-up in the rest. The yearly sensitivity of EUS-FNA was 37.5% (2004), 30% (2005), 33.3% (2006), 53.3% (2007). All samples reported as suspicious of malignancy and 80% (4/5) of insufficient specimens were malignant on follow-up.
Conclusion: The recommendations to improve sensitivity of EUS-FNA:
1: 5 × passes with the FNA needle per pancreatic lesion
2: FNA without suction if feasible
3: FNA with 25 gauge vs 22 gauge FNA needle5
4: Immediate cytological evaluation of FNA material.
PW347 THE USE OF COMBINED ENDOSCOPIC SPHINCTEROTOMY AND LARGE BALLOON DILATATION FOR MANAGEMENT OF COMPLEX COMMON BILE DUCT STONES
1S. K. Putta, 1A. P. Holt, 1D. A. Freshwater, 1G. H. Haydon, 2S. Pathmakanthan. 1Liver Medicine, Queen Elizabeth Hospital, Birmingham, UK, 2Gastroenterology, Queen Elizabeth Hospital, Birmingham, UK
Introduction: It is recommended that symptomatic bile duct stones are removed whenever possible. Sometimes large stones are difficult to extract despite endoscopic sphincterotomy (ESP) and mechanical lithotripsy due to technical limitations or anatomical constraints. Sphincterotomy in combination with large balloon dilation (LBD) across the ampulla and distal bile duct has recently been reported as a safe and effective alternative to intra-ductal lithotripsy.
Aims and Methods: To report our early experience of combined ESP and LBD to facilitate removal of complex bile duct stones. University Hospital Birmingham is a tertiary referral centre for hepatobiliary disease. We report our experience of using ESP and LBD in 13 patients referred with complex biliary stone disease between March and September 2008. All patients had failed conventional endoscopic management including lithotripsy. Primary sphincterotomy or extension of a pre-existing sphincterotomy was performed using a short-wire sphincterotome (Fusion™, Cooke). A Jagwire® (Boston Scientific) was inserted into the bile duct and LBD performed using a wireguided 15 mm CRE™ balloon (Boston Scientific) positioned across the ampulla and distal bile duct via the sphincterotomy. The CRE balloon was inflated to 8 ATM for 30 seconds before the duct was cleared with an extraction balloon (Fusion™, Cooke). Electronic admission records were reviewed and patients were followed up via telephone enquiry or clinic review after discharge.
Results: Thirteen patients underwent combined ESP and LBD between March 2008 and October 2008. Median age was 65 years (21–84). Four patients had previously undergone a failed ERCP as their stones could not be extracted. Ten patients had multiple CBD stones. Stone size (the largest stone measured) was recorded in 11 patients. Median stone size was 13.8 mm (quartiles). Mean doses of sedation required to permit LBD were as follows: fentanyl 92 mg (50–100 mg) and midazolam 5.1 mg (3–8.5 mg). LBD of the biliary sphincterotomy allowed complete stone removal in 11/13 (88%) patients. In all 11 patients the duct was cleared at the index endoscopy. None of the patients developed any of the recognised complications of ERCP such as early or delayed bleeding, cholangitis, perforation or pancreatitis. The 2 patients in whom ERCP failed underwent open duct clearance at surgery. There were no deaths.
Conclusion: ESP and LBD is a safe and effective means of extracting complex bile duct stones in patients with multiple or large stones for whom conventional endoscopic techniques are unsuccessful.
PW348 ROLE OF SELF EXPANDING METALLIC STENTS IN THE MANAGEMENT OF MALIGNANT OBSTRUCTION OF PROXIMAL COLON
1S. Ramamurthy, 2S. S. Dronamraju, 3M. Hayat. 1Gastroenterology, Royal Victoria Infirmary, Newcastle Upon Tyne, UK, 2Colorectal Surgery, North Tyneside General Hospital, North Shields, UK, 3Gastroenterology, North Tyneside General Hospital, Newcastle Upon Tyne, UK
Introduction: Expandable metal stents have shown to be effective in the management of malignant large bowel obstruction both as a bridge to definitive surgery and for palliation.1 However, right colonic lesions account for less than 5% of all reported cases of colonic stenting.2
Aims and Methods: The aim of this study was to determine the outcomes following stenting for malignant obstruction of proximal colon (obstructing lesion proximal to splenic flexure). Hospital records of patients undergoing colonic stenting for large bowel obstruction at a district general hospital in north England during the period 2001–2007 were retrospectively reviewed. Data were analysed (SPSS version 15) to identify patient characteristics, site of obstructing lesion, intent for stenting and the outcomes measured included relief of obstruction, hospital stay and post procedure complications.
Results: Stenting was attempted in 90 patients (median age 73 years, 52 male) with large bowel obstruction. Of these 14 (15.5%) patients had lesions in proximal colon including 8 patients with lesions in ascending colon and 6 patients with lesions in transverse colon. SEMS was successful in relieving obstruction in 12 (85.7%) patients with proximal colonic lesions. Stenting was attempted as a bridge to definitive surgery in 5 patients and for palliation in 9 patients. One patient had post-stent bleeding which was managed conservatively and there were no perforation or stent dislodgement. The mean post procedure hospital stay was 1.6 days.
Conclusion: SEMS are safe and effective in the management of malignant large bowel obstruction in proximal colon. The technical success rates and post procedural complications are comparable to those for distal colonic lesions.
PW349 SINGLE BALLOON ENTEROSCOPY IN SMALL BOWEL PATHOLOGY: A PROSPECTIVE OUTCOME STUDY
S. John, M. Remedios, M. Appleyard. Gastroenterology, Royal Brisbane and Women’s Hospital, Brisbane, Australia
Introduction: Single balloon enteroscopy (SBE) allows endoscopic evaluation and intervention in the small bowel. Its role and performance are expected to be similar to double balloon enteroscopy but data regarding this are limited.
Aims and Methods: The aim of our study is to prospectively assess the use of single balloon enteroscopy in small bowel pathology. Consecutive patients referred to the Royal Brisbane & Women’s Hospital for balloon enteroscopy between April and October 2008 were invited to participate in the study. Informed consent was obtained. The initial enteroscopy approach was determined by capsule endoscopy findings. Oral (antegrade) examination was performed in those with capsule findings in the proximal two thirds of the bowel and rectal (retrograde) examinations if the abnormality was expected to be in the distal third. An Olympus 180 series single balloon enteroscope with overtube was used. All procedures were performed by endoscopists competent in double balloon enteroscopy. Data were collected on indications, capsule findings, transfusion requirements and haemoglobin pre-procedure as well as pathology detected, therapeutic interventions and any complications. The cohort was followed up at 3 months and data were collected prospectively about further bleeding, transfusion requirements, haemoglobin and any further intervention.
Results: 32 procedures were performed in 28 patients between April and October 2008.The commonest indication was obscure GI bleeding with 12 occult and 10 overt bleeding. Capsule endoscopy was done in 26 patients pre-enteroscopy and 25 had small bowel abnormality detected. Based on these, 26 procedures were performed by the antegrade or oral route and 6 by the rectal approach. SBE detected pathology in 22 procedures (68%). The commonest pathology detected was small bowel angioectasia (n = 14). Four polypoidal lesions were detected (1 lymphoma, 1 hamartoma, 2 adenomas). Endotherapy was performed in 19 cases (59%). This included 13 argon plasma coagulation, 1 gold probe application, 2 endoclips and 3 polypectomy. SBE detected pathology was seen on capsule in 19 of 25 patients (76%). There were no major complications. At 3 months follow up (n = 18), 4 patients had further bleeding requiring endoscopic intervention. Surgery with small bowel resection was performed for 2 of these patients. 72% of patients had no further bleeding or symptoms. There was a statistically significant improvement in haemoglobin post-enteroscopy in those patients with obscure bleeding (p = 0.013).
Conclusion: This is an ongoing study. Our early experience suggests that the diagnostic yield and therapeutic capability of the single balloon enteroscope in small bowel pathology is similar to double balloon enteroscopy.
PW350 ENDOSCOPIC VARICEAL GRADING IN PREGNANCY: DOES IT REFLECT THE TRUE COLOUR?
S. Suganya Devi, S. Nandhini, P. Rajesh. Gastroenterology, Govt. Theni Medical College, Theni, India
Introduction: Liver disease complicating pregnancy contributes significantly to the maternal and fetal morbidity and mortality. Hence it is mandatory to identify the factors which contribute to the major complications like variceal bleed. The role of endoscopic variceal screening and risk assessment in pregnancy needs validation.
Aims and Methods: To study the efficacy of endoscopy in assessing the variceal grades before and after delivery in pregnancy with decompensated chronic liver disease. 20 pregnant women with cirrhosis and portal hypertension due to varied aetiology, who were non-bleeders with endoscopic early variceal grade (Grade I to III), were included. Portal hypertension due to other causes like extrahepatic portal vein obstruction, non-cirrhotic portal hypertension, with endoscopic advanced grade of varices (Grade IV), and past bleeders were excluded. All were subjected to endoscopic variceal assessment once before delivery (in II trimester) and within six months after delivery. Patients with grade III varices were treated with prophylactic propranolol 20 to 40 mg daily, with adequate maternal and fetal heart rate monitoring. The variceal grades before and after delivery were compared.
Results: Mean age was 26.3 ± 7.34 years. 11 (61.1%) were primigravida. Among the 20 cases, 2 were excluded as they had variceal bleeding and required endoscopic band ligation. Out of the 18 cases, 7 (39%) were hepatitis B related, 2 (11.1%) hepatitis C related, 1 (5.6%) Wilson’s related, and the rest (44.4%) were cryptogenic. Before delivery, 3 (16.7%), 7 (39%) and 8 (44.4%) patients had grade I, II and III varices, respectively. After delivery, the variceal grade were I, II, and III in 7 (39%), 7 (39%), and 4 (22.2%), respectively. Among the 7 who had grade II before delivery, on endoscopic reassessment after delivery, 3 had grade I, and the rest had grade II. Among the 8 who had grade III before delivery, 1 had grade I, 3 had grade II and the remaining had grade III. Statistically significant downgrading of varices was documented after delivery in 50% of cases reported as grade III before delivery.
Conclusion: Endoscopic grading of varices in pregnancy is influenced by others factors like haemodynamic changes and extrinsic compression of major vessels by the gravid uterus and may not reflect the true colour.
PW351 ONE YEAR FOLLOW-UP COLONOSCOPIES WITHIN THE BOWEL CANCER SCREENING PROGRAMME: DATA FROM THE NORTHERN REGION ENDOSCOPY GROUP
1T. J. W. Lee, 1L. Hurst, 2D. Nylander, 2J. Painter, 3J. Singh, 4C. Rees, 4M. Rutter. 1Gastroenterology, University Hospital of North Tees, Stockton upon Tees, UK, 2Gastroenterology, Sunderland Royal Hospital, Sunderland, UK, 3Gastroenterology, Queen Elizabeth Hospital, Gateshead, UK, 4Gastroenterology, South Tyneside General Hospital, South Tyneside, UK
Introduction: 542 patients underwent colonoscopy as part of the Bowel Cancer Screening Programme (BCSP) in the Tees and South of Tyne area of England between February and September 2007. 41 (7.5%) of these had at least 5 small adenomas or at least 3 small adenomas with 1 >1 cm in size. This group of patients is defined as being at high risk of developing advanced adenomas and cancer.1 Current guidelines state that these patients should undergo a follow up colonoscopy one year after their index procedure.2
Aims and Methods: Data were obtained from the BCSP databases for the Tees and South of Tyne areas. Histological data were obtained from the local pathology departments.
Results: 41 patients underwent 1 year follow up colonoscopy. Median age 68 years. 32 were male, 9 were female. At index colonoscopy, a total of 197 adenomas were discovered (mean 4.8 per patient). The characteristics of the adenomas were as follows: 22% >1 cm (range 1–30 mm). 87% were tubular adenomas, 12.5% villous or tubulovillous. 95% displayed low grade dysplasia, 5% high grade dysplasia. 5 patients (12%) had at least 5 small adenomas, 26 (64%) had at least 3 with 1 >1 cm, 10 patients (24%) fulfilled both criteria. At follow up colonoscopy 56 adenomas and 2 adenocarcinomas were found in 26 of 41 patients (mean 0.8 adenomas per patient). 5 patients had lesions displaying advanced neoplasia (villous, severe dysplasia, size ⩾10 mm, carcinoma in situ or adenocarcinoma). All of these patients had at least one adenoma >10 mm found at their original colonoscopy. 2 cancers were discovered at 1 year follow up colonoscopy. One was a 9 mm sigmoid cancer, the second was a 45 mm ascending colon polyp.
Conclusion: Uptake of 12 month follow up colonoscopy within the BCSP is high (100% in our area). 5 of 41 (12%) patients had significant neoplasia at follow up endoscopy including 2 adenocarcinomas. It is likely that these lesions were missed at index colonoscopy rather than representing new neoplasia. All of these patients had at least one adenoma >10 mm found at their original colonoscopy. No patients with 5 or more small adenomas had advanced neoplasia at 1 year follow up. These data confirm that follow up colonoscopy at 1 year for patients with high risk adenomas is essential. Patients with 3 or more adenomas, of which one is >1 cm, may benefit from follow up colonoscopy sooner than 1 year given the high rate of significant pathology detected at follow up.
Abstract submitted on behalf of the Northern Region Endoscopy Group (NREG)
PW352 IS COLONOSCOPY QUALITY AND OPERATOR EXPERTISE IMPORTANT FOR PATIENT SATISFACTION? A COMPARISON OF ACCREDITED AND NON-ACCREDITED BOWEL CANCER SCREENING CONSULTANTS AND TRAINEE COLONOSCOPISTS
V. Athwal, D. Scerri, N. Prasad, C. Ormerod, N. Polavarapu, T. Gledhill, P. Kelly, V. Theis, M. Sephton, S. Sarkar. Digestive Diseases Centre, University Hospitals Aintree, Liverpool, UK
Introduction: Since the poor results of the BSG colonoscopy audit,1 there has been a large investment in improving training and standards in the UK, which has partly been driven by the introduction of the national bowel cancer screening (BCS) programme. However, it is unclear whether these improvements have positively impacted upon patient satisfaction.
Aims and Methods: To determine whether quality and operator expertise in colonoscopy contributes to patient satisfaction. Within a BCS unit, 251 colonoscopies were audited from 15 May 2008 to 15 September 2008 using a standard proforma. Information was attained using the endoscopy database, the hospital IT system and a follow-up patient telephone review. The data were analysed in 3 operator expertise groups: (1) BCS accredited consultants (BCS-Cons) (endoscopists n = 5, procedures n = 80); (2) Non-accredited BCS Consultants (Cons-Other) (endoscopists n = 7; procedures n = 68); and (3) Trainees (endoscopists n = 7, procedures n = 103).
Results: Patients age, ASA score, and procedural time were similar in all groups. The BCS-Cons group had more males than the Trainees group, and more diagnostic procedures (p<0.05 for all) than the others. Caecal intubation was higher in the BCS-Cons (p = 0.004) and Cons-Other (p = 0.01) compared to Trainees at 96.2%, 95.7% and 82.5%, respectively. While the fentanyl doses were similar, the midazolam doses (mean (SD)) were significantly different between all groups (p<0.05 for all) with lowest in BCS-Cons (0.96 mg (0.8)), followed by the Cons-Other (1.6 mg (1.1)) and then Trainees (2.6 mg (1.2)).
Conclusion: Overall patient satisfaction was high regardless of operator expertise. Despite superior caecal intubation rates and lower sedation doses in both Consultant groups compared to Trainees, satisfaction scores were similar for pain, comfort and expectation. The better patient experience with BCS-Cons compared to Trainees may reflect the gender and diagnostic to therapeutic differences. The increased willingness to have a repeat procedure in the BCS-Cons compared to Cons-Other group, but not Trainees group, may be explained by the higher pain score trend in the Cons-Other group.
PW353 TO PEG OR NOT TO PEG: WHAT IS THE OUTCOME OF PATIENTS REFERRED FOR PERCUTANEOUS ENDOSCOPIC GASTROSTOMY (PEG) INSERTION IN WHOM THE PROCEDURE IS NOT PERFORMED?
V. Lekharaju, A. Young, H. L. Smart. Gastroenterology, Royal Liverpool University Hospital, Liverpool, UK
Introduction: Percutaneous endoscopic gastrostomy (PEG) insertion is well established as an effective method to provide enteral nutrition in a variety of situations where patients cannot maintain adequate nutrition by oral intake. The simplicity of the technique has led to some concern about its use when there is little or no clinical benefit. This situation prevailed in early reports of PEG use with poor outcome in terms of 30 day mortality, which was often in excess of 25%. Improved patient selection has produced a dramatic improvement in this outcome measure, with 30 day mortality now <10%, but at what expense?
Aims and Methods: The aim of this study was to examine the effect of patient selection for PEG insertion, focusing on the outcome in patients in whom the procedure was not performed. All referrals for PEG insertion at the Royal Liverpool University Hospital are reviewed by a nurse consultant or nurse specialist in nutrition to ensure strict criteria are met prior to the procedure being performed. We examined all electronic referrals made to the service over a 1 year period from 1 January to 31 December 2006. Patients were documented as either undergoing or not undergoing PEG insertion, with the reason behind the latter being recorded. Referral details, nutrition team records and patient case notes were reviewed to ascertain patient demographics and outcome.
Results: Over the 12 month period there were a total of 221 referrals for PEG insertion. 128 patients (58%) had a successful PEG procedure; in 93 patients (42%) a PEG was not inserted. The main reasons for non-insertion were either that PEG was not indicated (33%) or it was considered inappropriate (59%) due to patient’s condition. In the remainder, PEG insertion was considered to be indicated but 2 patients refused the procedure, in 2 it was considered unsafe to proceed to insertion due to coagulopathy, and in 3 abnormal anatomy prevented successful placement. Outcome in terms of mortality is shown in the table. The highest 7 day mortality was in patients in whom PEG insertion was felt to be unsafe or who refused the procedure, with the lowest being in those patients in whom PEG was felt not to be indicated. The mortality in this group rose progressively over the 12 month period. In patients considered inappropriate for PEG insertion there was a progressive increase in mortality, with only 20% surviving 30 days and 5% 12 months. For comparison, 30 day mortality in patients who had a successful PEG insertion was 7%.
Conclusion: The ethics of PEG placement and feeding in patients with a perceived poor short-term survival is a difficult question. This study has shown that in patients in whom PEG insertion is deemed inappropriate there is significant 30 day mortality. This appears to validate the rigorous patient selection process which is undertaken in our unit.
PW354 UTILITY OF AN AUTO-FLUORESCENCE INDEX TO DETECT EARLY NEOPLASIA IN PATIENTS WITH BARRETT’S OESOPHAGUS
1V. Subramanian, 2L. Alvarez-Herrero, 1J. Mannath, 2W. L. Curvers, 2J. J. Bergman, 1K. Ragunath. 1Nottingham Digestive Diseases Centre and Biomedical Research Unit, Nottingham University and Hospital, Nottingham, UK, 2Department of Gastroenterology and Hepatology, Academic Medical Centre, Amsterdam, The Netherlands
Introduction: Auto-fluorescence imaging (AFI) endoscopy is a novel imaging technique that can identify neoplastic tissue by highlighting differences in tissue fluorescence properties and detect early neoplasia not detectable by conventional white light endoscopy. Normal areas appear “green” and abnormal areas are highlighted as “red” when using AFI endoscopy. Although it has a high sensitivity, it is associated with a high false positive rate up to 80%.1
Aims and Methods: To determine if auto-fluorescence index, defined as the ratio of the intensity of red and green tone between normal and abnormal AFI areas in patients with Barrett’s oesophagus (BO), can improve the specificity and accuracy of AFI endoscopy. Images of patients with both AFI true and false positive areas of BO were selected from a prospectively collected dataset using the Olympus Lucera-Hyperpro prototype video endoscopy system and GIF Q240FZ gastroscope. Biopsies from these areas had been confirmed by at least 2 specialist GI histopathologists to have no dysplasia or high grade dysplasia/carcinoma. Lesions with indefinite or low grade dysplasia were not included. The intensity of the red and green tone at the abnormal and 2 separate normal areas were read blinded using the NIS Elements AR 2.30 imaging software (Nikon instruments, Japan). Statistical analysis was done using SPSS version 15 (SPSS Inc, USA).
Results: There were 82 images of AFI abnormalities. Of these 19 had high grade dysplasia (HGD), 18 had carcinoma (Ca), 38 had intestinal metaplasia (IM) and 7 were from areas of gastric mucosa. The area under the receiver operating curve (AUROC) for the auto-fluorescence index ratio (AFI ratio) was 0.881 (0.81–0.95) and 0.91 (0.84–0.97) when utilising the two different normal AFI areas respectively for calculating the index. The two separate readings made were highly correlated (Spearman’s rho 0.82). Using an AFI ratio cut off of 1.32, the sensitivities for reading 1 and 2 were 92% (82–99) and 95% (85–99) respectively, specificities were 76% (67–80) and 62% (54–65), and likelihood ratio of a positive test was 3.8 (2.5–4.6) and 2.5 (1.9–2.8). None of the cancers and only 3 and 2 HGDs respectively were misclassified by the AFI ratio.
Conclusion: The AFI ratio shows promise as a tool to improve the diagnostic capabilities of AFI endoscopy. Further prospective studies with real time determination of the ratio during video AFI endoscopy will serve to confirm its utility in clinical practice.
PW355 A COST COMPARISON OF THE “BROWNE NINHYDRIN PROTEIN DETECTION KIT” WITH IN-HOUSE SURVEILLANCE CULTURES TO ASSESS THE QUALITY OF ENDOSCOPE CLEANING
1V. P. Jackson, 2R. P. D. Cooke, 2S. Sundeep, 1R. Sturgess. 1Endoscopy, Aintree Hospitals NHS Foundation Trust, Liverpool, UK, 2Medical Microbiology, Aintree Hospitals NHS Foundation Trust, Liverpool, UK
Introduction: Both HTM 2030 (UK) and EN ISO 15883-1: 2006 (EU) recommend that the cleaning efficacy of endoscope washer-disinfectors (WDs) should be tested weekly by the detection of protein residues within endoscope lumens. However, a review of endoscope practices in Scotland found that this was undertaken in only 8% of reprocessing units.1 With the recent introduction into the UK of an easy to use “Browne Ninhydrin Protein Detection Kit” (Steris Corporation), we have compared its use and cost-effectiveness with standard endoluminal surveillance cultures to monitor the quality of endoscope reprocessing.2
Aims and Methods: Study was undertaken in a busy teaching hospital endoscopy unit reprocessing approximately 18 000 endoscopes per year. Staff training and WD endoscope maintenance were fully compliant with national guidelines.3 Following endoscope disinfection (Sterilox) and final rinsing, all endoscopes underwent antegrade and retrograde flushing using a standard technique.3 All endoluminal flush and final rinse samples were then cultured by routine laboratory methods. In addition, all endoscopes were tested for protein residues following training and in accordance with the manufacturer’s instructions. An economic appraisal was undertaken of the two systems based on the weekly consumable and staff costs for ninhydrin testing and endoluminal surveillance cultures (assuming 55 endoscopes tested weekly).
Results: 55 endoscopes were studied. All endoluminal flush samples, final rinse waters and ninhydrin protein detection tests were negative. An analysis of annual costs for endoluminal sampling and ninhydrin testing is presented in the table. Consumable costs were 3.4 greater for ninhydrin tests while staff costs were 2-fold greater for surveillance cultures. Overall, weekly endoluminal surveillance cultures were approximately £1000 cheaper per annum.
Conclusion: Endoluminal surveillance cultures are a cost-effective alternative to weekly testing for protein residues within endoscopes. Though slightly cheaper, endoscope surveillance cultures are labour-intensive and therefore best suited to endoscopy units with dedicated reprocessing staff.
Gastroduodenal posters
PW356 PROTON PUMP INHIBITORS: ARE WE WASTING MONEY AND IGNORING THE RISK?
A. J. Kent, B. Graf, M. Harbord. Gastroenterology, Chelsea and Westminster Hospital, London, UK
Introduction: The National Health Service spends £300 million annually on proton pump inhibitors (PPIs). The National Institute for Health and Clinical Excellence (NICE) advise that patients with dyspepsia/gastro-oesophageal reflux disease (GORD) should receive a PPI for 1–2 months and if symptoms recur it should be prescribed at the lowest dose. £50 million could be saved annually if their guidelines were followed more strictly. There is growing concern regarding complications associated with PPI use, including increased risk of enteric infections (specifically Clostridium difficile infection1), community-acquired pneumonia, hip fractures and disturbed calcium homeostasis.
Aims and Methods: We aimed to assess the degree of inappropriate PPI prescription and assess potential associated complications. We prospectively reviewed prescriptions of medical patients admitted through Chelsea and Westminster Hospital. Information gathered included: patient demographics, comorbidities, body mass index (BMI), smoking/ETOH history, medications, indication for PPI and current symptoms. We contacted general practitioners for information not available from the patient or hospital records.
Results: Demographics—254 patients were assessed, of whom 129 were prescribed a PPI. Mean age was 72 years and 48% of patients were male. There was no statistical difference between patient demographics, alcohol or smoking history between the PPI and control groups. PPI—PPI used included omeprazole (67%), lansoprazole (32%) and esomeprazole (1%). Indications were dyspepsia (13%), peptic ulcer disease (13%) and prophylaxis (47%). The indication was unknown by patient, GP or hospital records in 27%. Over 77% patients had been taking PPI for greater than 1 year, despite only 25% having documentation stating long term PPI was required. Only 2 patients had undergone a trial without PPI. Complications—C difficile-associated diarrhoea (CDAD) occurred significantly more in patients on PPI (16% vs 5%, p<0.004). 2 patients from the PPI group died from CDAD, compared to none in the control group. Chest infections were more common in patients on PPI (25% vs 17%), but the PPI group had a higher incidence of underlying lung disease, so significance was impossible to determine. Osteoporosis was significantly more common in the PPI group (26% vs 10%, p 0.003) and subsequently bisphosphonate use was also higher (22% vs 9%, p<0.005).
Conclusion: Over-prescription of PPI is evident, with an increased incidence of potentially associated complications. We would advise doctors to review prescriptions in all patients, in an attempt to reduce cost and complications of unnecessary PPI use.
PW357 DIAGNOSTIC PRECISION OF PRIMARY CARE ELECTRONIC DATABASE FOR STUDY OF GASTROINTESTINAL BLEEDING AND ITS ABILITY TO DETECT THE INFLUENCE OF ASPIRIN
1M. Leighton, 2Y. Vivogravada, 2A. Shonde, 1J. C. Atherton, 3R. F. A. Logan, 2A. Avery, 2D. Kendrick, 2J. Hippisley-Cox, 1C. J. Hawkey. 1Nottingham Digestive Diseases Centre and Biomedical Research Unit, Nottingham University Hospital, Nottingham, UK, 2Primary Care, Nottingham University Hospital, Nottingham, UK, 3Epidemiology & Public Health, Nottingham University Hospital, Nottingham, UK
Introduction: Large primary care electronic databases offer good opportunities for systematic epidemiological research. However, general practitioners do not necessarily code events in the same way as Hospital Events Statistics do. We therefore investigated the extent to which coding influences recorded gastrointestinal (GI) bleeding event rates using QRESEARCH, a new larger electronic database.
Aims and Methods: Patients were included in the analysis if they were aged 45–100 years and had at least 12 months of electronic health records and were registered with a participating practice at any time between 1 April 2003 and 31 March 2007. All codes with mention of gastrointestinal bleeding were extracted and summarised to produce eight categories, as shown in the table.
Results: 459 practices met inclusion criteria to generate 4.87 million person years of observation. Over 99% of aspirin use was for ⩽300 mg per day. As shown in the table, high rates were recorded for upper gastrointestinal bleeding and rectal bleeding/melena, while specific ulcer bleeding was under recorded. Nevertheless, the study was able to detect a 1.58 (1.45–1.71) fold hazard ratio for upper gastrointestinal bleeding and a 1.47 (1.42–1.52) hazard ratio for rectal bleeding/melena, related to aspirin use.
Conclusion: Coding imprecision limits the exactitude of conclusions but is not enough to obscure the impact of aspirin on event rates. The impact of aspirin is likely to be higher when coding and exposure imprecisions are allowed for.
PW358 FEASIBILITY OF REDUCING ASPIRIN-ASSOCIATED ULCER BLEEDING BY HELICOBACTER PYLORI ERADICATION
1C. J. Hawkey, 2J. C. Atherton, 3R. F. A. Logan, 4A. Avery, 2A. Shonde, 2M. Leighton, 4D. Kendrick. 1Nottingham Digestive Diseases Centre and Biomedical Research Unit, Nottingham University Hospital, Nottingham, UK, 2Nottingham Research Centre and Biomedical Research Unit, Nottingham University Hospital, Nottingham, UK, 3Epidemiology & Public Health, Nottingham University Hospital, Nottingham, UK, 4Division of Primary Care, Nottingham University Hospital, Nottingham, UK
Introduction: In contrast to non-steroidal anti-inflammatory drugs, ulcers and ulcer complications on aspirin occur selectively in Helicobacter pylori positive individuals. The main effect of aspirin may be to provoke bleeding rather than cause ulceration. If so, H pylori eradication should reduce aspirin-associated ulcer bleeding and enlarge the population for which aspirin results in net benefit.
Aims and Methods: In preparation for a proposed 9000 patient outcomes study, with ulcer bleeding as an end point, we investigated the prevalence of H pylori (by breath testing), the willingness to participate and the rate of eradication in patients taking aspirin ⩽100 mg daily in 9 general practices in the North East, Midlands and South West of England.
Results: Of 2525 patients approached, 1199 replied (47.5%) and 945 (37.4%, range 32.6–48.8%). Of these, 84 (3.3%) were ineligible leaving 34.1% suitable for participation. Among these patients, 24.1% had a positive H pylori breath test (range 13.3–44.0%, IQR 21.4–25.9%). These patients underwent eradication treatment, with an eradication rate so far of 89.1%. In response to a questionnaire, 71.7% of patients in this non-randomised study said they would participate in a study with randomisation to immediate or delayed eradication treatment. A survey of 97 practices participating in the GP Primary Care Comprehensive Research Network found that 71.1% thought a controlled trial study was important and said they would definitely or very probably participate in.
Conclusion: Overall, 8.2% of patients taking aspirin are both H pylori +ve and willing to participate in a trial of eradication treatment. To enrol enough patients for an outcomes study, approximately 110 000 patients would need to be approached. Our study shows this is easy to achieve and the study would be suitable to be conducted through the comprehensive research network.
PW359 GASTRIC HELICOBACTER INFECTION INDUCES IRON DEFICIENCY IN THE INS-GAS MOUSE
1S. A. Boxall, 2D. M. Pritchard, 2A. Abuderman, 3T. C. Wang, 2A. Varro, 4J. E. Crabtree. 1Leeds Institute of Molecular Medicine, St Jame’s University Hospital, Leeds, UK, 2Division of Gastroenterology, University of Liverpool, Liverpool, UK, 3Columbia University Medical Centre, Columbia University, New York, USA, 4Leeds Institute of Molecular Medicine, St James’s University Hospital, Leeds, UK
Introduction: Iron deficiency is the most common nutritional disorder in the world. There is increasing evidence from clinical and population studies for a role of Helicobacter pylori infection in the aetiology of iron deficiency anaemia. Hypochlorhydria associated with initial infection, and gastric atrophy in late stages of infection, may be relevant to iron deficiency. The aims of this study were to determine the effects of gastric Helicobacter infection in INS-GAS mice on iron deficiency and the relation to parietal cell number.
Aims and Methods: Male transgenic hypergastrinaemic INS-GAS mice were inoculated with Helicobacter felis by oral gavage. Infected mice and uninfected controls were sacrificed 3, 6 and 9 months post-inoculation. Blood was collected and serum iron, total iron binding capacity (TIBC) and plasma amidated gastrin levels were measured. Gastric parietal cells were immunolabelled with H+K+ATPase and quantified.
Results: In uninfected controls there was no significant change in serum iron levels at 3, 6 or 9 months. In contrast, at 6 months, iron levels in H felis infected mice were significantly lower (p<0.002) than in 3 month H felis infected mice, and also significantly reduced (p<0.05) relative to 6 month uninfected controls. No further reduction in iron levels was evident at 9 months in H felis infected mice. At 3 months TIBC levels in H felis infected mice were significantly increased (p<0.05) compared to controls. TIBC levels in infected mice were further increased (p<0.02) at 9 months compared to 6 month infected mice. The decrease in iron levels at 6 months in H felis infected mice was associated with a concomitant decrease in parietal cell numbers relative to controls (p<0.05), which was also evident at 9 months (p<0.03). The percentage of transferrin saturation was also decreased in infected mice, becoming significantly reduced (p<0.03) by 9 months post-infection compared to control mice. Although in these hypergastrinaemic mice H felis infection was associated with significantly increased (p<0.001) gastrin concentrations at 9 months, there was no significant correlation between iron levels and plasma gastrin concentrations.
Conclusion: In INS-GAS mice H felis infection is associated with decreased serum iron, increased TIBC and decreased transferrin saturation. Changes in iron levels evident at 6 months are associated with decreased parietal cell number. Further studies are required to elucidate the exact mechanisms involved in Helicobacter-induced iron deficiency in the INS-GAS model.
PW360 HELICOBACTER PYLORI SEROPREVALENCE IN A HOSPITAL COHORT BETWEEN 2001–2007
1K. Alexandropoulou, 2H. Al-Ghusein, 3R. Holliman, 1A. Poullis, 1J. Kang. 1Gastroenterology, St George’s Hospital, London, UK, 2IT Department, St George’s Hospital, London, UK, 3Microbiology, St George’s Hospital, London, UK
Introduction: Over the last century, Helicobacter pylori (HP) prevalence decreased in developed countries in the context of improved living conditions. Widespread adoption of the “test and treat” strategy for dyspepsia may have further decreased the prevalence of HP infection in recent years. Although serology may remain positive after successful eradication of HP infection, it is possible that large-scale use of eradication treatment could have affected the sero-epidemiology of HP. We have studied the prevalence rate of positive serology to HP in an ethnically diverse area in London over a 7 year period.
Aims and Methods: Records of HP serology results from St George’s Hospital, London, between 2001 and 2007 were retrieved. Data were analysed to determine prevalence trends over this time period (χ2 test for trend). The effect of age, gender and race was also assessed.
Results: A total of 12307 patients were tested between 2001 and 2007. There was a statistically significant reduction in the proportion of positive HP tests over the study period from 42% to 37% (p<0.005). Two thirds (77%) of patients tested were under the age of 50. Mean HP prevalence was 39% but varied among the age groups, being lowest in <25 group at 30%, 38% for 26–50, 48% for 50–75 and 49% for >75 age group. There were comparable rates of decline in HP prevalence in the <50 and >50 age groups. More men than women tested positive for HP serology consistently over the 7 year period although the difference did not achieve statistical significance (p = 0.07).
Conclusion: HP prevalence in our population cohort is decreasing, even over a short period of seven years. While HP infection was more prevalent in older patients, a significant proportion of younger patients tested positive in this ethnically diverse population and the rate of decline was unaffected by age.
PW361 INCREASED PLASMA GHRELIN IN ALCOHOLIC CIRRHOSIS: EFFECT OF AN ORAL GLUCOSE CHALLENGE ON POST-PRANDIAL MECHANISMS
1S. J. Goodyear, 1M. Mottershead, 1E. Z. H. Sung, 2L. Wong, 3P. McTernan, 3S. Kumar, 1C. U. Nwokolo. 1Gastroenterology, University Hospital of Coventry, Coventry, UK, 2Surgery, University Hospital of Coventry, Coventry, UK, 3Endocrinology and Metabolism, University Hospital of Coventry, Coventry, UK
Introduction: Ghrelin abnormalities have been reported in chronic liver disease. This study assessed the response of anabolic peptides like ghrelin, growth hormone (GH) and insulin-like growth factor 1 (IGF-1) in alcoholic cirrhotics and healthy subjects to oral glucose. In a previous study using a similar oral glucose challenge we identified loss of ghrelin regulation in non-alcoholic steato-hepatitis.
Aims and Methods: 14 patients with alcoholic cirrhosis were compared with 11 healthy subjects. The cirrhotics were studied after period of hospital admission minimising the effect of fluid shifts, infection and persisting blood alcohol. After an overnight fast they ingested 100 g glucose in 250 ml of water. Blood was sampled before and every 20 min for 120 min. Plasma acylated and des acyl ghrelin, GH, IGF-1 and insulin were assayed by ELISA.
Results: Expressed as median 95% CI. 120 min integrated acylated ghrelin increased from 26 (19–66) in controls to 170 (129–252) pg/ml.hr in cirrhotics; p<0.001, Mann Whitney U Test. Both groups exhibited a normal post-glucose plasma ghrelin profile. Among cirrhotics (compared to controls) growth hormone was increased 15-fold and IGF-1 decreased 4-fold. Acylated ghrelin correlated with GH (Spearman r = 0.69, p = 0.0015) in controls but not in cirrhotics.
Conclusion: Acylated ghrelin is markedly increased in alcoholic cirrhosis with preservation of normal post prandial mechanisms of gastric ghrelin secretion. GH is also increased but regulation by acylated ghrelin confirmed in healthy subjects is lost. Despite increased ghrelin and GH alcoholic cirrhotics remain anorexic and catabolic, pointing to tissue resistance to these anabolic peptides.
GI physiology posters
PW362 SYMPTOMS, ENDOSCOPY AND PHYSIOLOGY: DO THEY CORRELATE?
A. J. Kent, B. Graf, M. R. Banks. Gastroenterology, Chelsea and Westminster Hospital, London, UK
Introduction: Oesophageal manometry and pH studies are well-established tools in the assessment of oesophageal symptoms, but are only available in tertiary referral centres in the UK. Criteria have been proposed to define diagnoses, but the overall benefit of manometric diagnoses that do not correlate with symptoms is unknown.
Aims and Methods: Our aim was to assess the correlation between symptoms, upper GI endoscopy findings and physiological findings. 200 consecutive patients undergoing oesophageal physiology investigations had details entered into a database designed for the study. Information gathered included patient demographics, past medical history, previous investigations, medications, symptoms and manometric findings.
Results: Symptoms—Dysphagia resulted in the following manometric diagnoses: normal 47%, achalasia 39%, ineffective oesophageal motility (IOM) 8%, diffuse oesophageal spasm (DOS) 6%. All patients with achalasia suffered with dysphagia. Patients with chest pain were diagnosed with achalasia 34%, DOS 8% and normal manometry 58%. Conversely patients with a manometric diagnosis of DOS suffered with chest pain 11%, dysphagia 22% and epigastric pain or reflux 67%. 78% of patients with IOM had acid reflux, and accounted for a total of 11% of all patients referred for pH studies to investigate persistent acid reflux. Furthermore 56% of patients with IOM had a hypotensive lower oesophageal sphincter, which may have contributed to their reflux events. Endoscopy—The majority of patients undergoing physiology testing had previously normal OGDs. All gastroscopies with findings suspicious for achalasia led to manometry that confirmed the diagnosis. However, only 50% of patients with achalasia had OGDs which suggested this diagnosis. Unsurprisingly, oesophagitis was significantly associated with evidence of acid reflux compared to normal endoscopies. However, 54% of endoscopically diagnosed oesophagitis had normal pH studies, despite all studies being performed off acid suppression. Furthermore, only 50% of patients with Barrett’s oesophagus had pathological acid reflux.
Conclusion: Oesophageal symptoms have a poor predictive value for clinical diagnoses. Patients with dysphagia should always undergo manometry testing to exclude achalasia, if endoscopy is non-diagnostic. Given the variety of symptoms for motility disorders, and lack of “classic” symptoms for conditions such as DOS, manometric testing should be used more prevalently in patients with oesophageal symptoms.
PW363 OBJECTIVE ASSESSMENT OF RECTAL AFFERENT SENSITIVITY AND PRIMARY CORTICAL PROCESSING IN PATIENTS WITH IRRITABLE BOWEL SYNDROME
1D. C. Bullas, 2A. R. Hobson, 1S. Gurmany, 2K. J. Hicks, 2G. E. Dukes, 1M. A. Kamm, 1W. S. Atkin, 1N. Arebi. 1St Mark’s Hospital Campus, Imperial College, Harrow, UK, 2Immuno-Inflammation CEDD, GlaxoSmithKline Medicines Research Centre, Stevenage, UK
Introduction: Abnormalities in endogenous pain modulation and sensitisation of afferent nerve pathways may contribute to the development and maintenance of symptoms in irritable bowel syndrome (IBS). Differentiating these distinct pathophysiological mechanisms in IBS is limited using conventional physiological assessments. Cortical evoked potentials (CEPs) allow a dynamic and objective assessment of visceral sensory function and could provide novel insight into IBS aetiology.
Aims and Methods: To measure primary rectal hypersensitivity by applying CEPs in IBS. Rome 2-positive patients and controls were recruited in a prospective study for 3 days of testing. Sensory and pain thresholds (ST, PT) were calculated, and CEPs were captured at a stimulus intensity of 75% PT. CEP morphology includes P1, P2, P3, P4, and P5 components, distinguished by latency (ms) and amplitude (microV). Anxiety scores were provided by Spielberger State Trait Anxiety Index (SSTAI). Data were analysed using 1-way ANOVA, presented as mean differences ± 95% CI.
Results: 33 IBS patients (27 females, mean age 40.1) and 15 controls (9 females, mean age 28.6) enrolled. IBS subjects had increased P1 and P3 latencies on day 1 (20.89 (6.20 to 35.59)) and day 3 (30.64 (2.82 to 5.46)) respectively. IBS subjects had decreased P2 amplitudes: (day 1: −6.96 (−13.89 to −0.03)); (day 2: −8.62 (−16.11 to −1.12)). IBS subjects had decreased P3 amplitudes: (day 1: −8.46 (−14.21 to −2.71)); (day 2: −3.36 (−5.66 to −1.06)); (day 3: −10.65 (−16.13 to −5.18)). IBS subjects had decreased P4 amplitudes on day 1 (−3.36 (−5.66 to −1.06)). ST and PT did not differ between groups on day 1. PT was decreased on day 3 (−15.63 (−29.24 to −2.03) in IBS. SSTAI-State scores (day 1: 5.92 (0.43 to 11.40)); (day 2: 8.87 (2.58 to 15.17)) and SSTAI-Trait scores (day 1: 9.55 (3.45 to 15.65)); (day 2: 8.84 (2.35 to 15.32)); (day 3: 11.88 (5.02 to 18.74)) were increased in IBS.
Conclusion: Analysis of cortical evoked potentials allows neurophysiological differentiation between IBS and controls at a group level. Primary rectal afferent hypersensitivity was not commonly seen in the IBS group. Pain thresholds showed a negative trend in IBS patients compared to controls on days 1 and 2 that reached statistical significance on day 3. This was a result of an increase in the pain thresholds of the controls rather than a relative decrease in IBS patients. In the context of persistent anxiety levels, this suggests that IBS patients maintain a level of visceral hypervigilance not shared by controls, who become acclimatised to the test protocol by day 3. The inability to inhibit central pain amplification, in a process of habituation to repetitive noxious stimuli, may be important factor in the maintenance of IBS symptomatology.
PW364 PROTON PUMP INHIBITORS, STATINS AND ACUTE CORONARY SYNDROME
M. A. Butt, J. W. L. Yong, N. C. Pegge. Cardiology, Worthing Hospital, Worthing, UK
Introduction: Proton pump inhibitors (PPI) are one of the most frequently prescribed medications in the UK as they combine a high level of efficacy with low toxicity. Patients with acute coronary syndrome (ACS) often receive PPIs to counteract the risk of gastrointestinal haemorrhage secondary to dual anti-platelet therapy. Both PPIs and statins interact with cytochrome p450 pathways. This interaction may reduce the effectiveness of statins.
Aims and Methods: We therefore conducted a retrospective analysis of patients treated for ACS. Two groups were selected; those treated with PPIs in addition to routine ACS treatment and matched controls. Data on age, sex, type of statin and PPI prescribed, admission serum cholesterol and triglyceride, and serum cholesterol and triglyceride 3 months post discharge were collected.
Results: 69 patients' notes were reviewed. There were 36 patients treated with PPIs in addition to ACS medication and 33 controls. 61% of patients were male, mean age 69 years. For those prescribed PPI medication, 78% received omeprazole, 19% lansoprazole and 3% rabeprazole. Documented indications for PPI prescription included dyspepsia (28%), previous gastric ulcer (17%), gastro-oesophageal reflux (8%), gastrointestinal haemorrhage (3%) and alendronate (3%). The majority of patients received simvastatin (90%) by the time of discharge. The following mean scores were observed; admission cholesterol in the PPI group (5.3±1.8) vs control (5.1±0.9), admission triglyceride in the PPI group (2.6±3) vs control (2.1±1.7), 3 month post-discharge cholesterol in the PPI group (4.7±1.2) vs control (3.7±0.6) and 3 month post-discharge triglyceride in the PPI group (1.5±0.7) vs control (1.3±0.2). To ascertain whether PPI therapy influenced the effectiveness of statin treatment, we used the Students one tailed t-test to compare if the percentage reduction in cholesterol and triglyceride between the PPI and control groups was significant. The following P values were obtained; for cholesterol reduction p = 0.15, for triglyceride reduction p = 0.08.
Conclusion: Our study demonstrates that the percentage reduction in cholesterol and triglycerides with statins at 3 months was lower in patients treated with PPIs, than matched controls. Although this difference did not reach significance, this was likely due to the small sample size in our study. Future prospective studies with narrower criteria, looking at patients treated with PPIs and statins of one type and at specific doses, may confirm a significant interaction.
Oesophagus posters
PW365 IS BARRETT’S OESOPHAGUS UNDERDIAGNOSED IN PATIENTS WITH EROSIVE OESOPHAGITIS?
K. K. V. Kosuri, J. de Caestecker, J. Jankowski. Gastroenterology, University Hospitals of Leicester, Leicester, UK
Introduction: Barrett’s oesophagus (BE) could be underdiagnosed in oesophagitis patients either because the ulcerative oesophagitis itself obscures BE or because BE could develop after healing.
Aims and Methods: Our aim is to evaluate the frequency of Barrett’s oesophagus on follow up upper GI endoscopy (oesophagogastroduodenoscopy, OGD) for reflux oesophagitis (RE). Retrospective observational study on patients undergoing repeat upper GI endoscopy following diagnosis of RE. All patients diagnosed with RE graded with Los Angeles (LA) or Savary-Miller criteria between 1997–2008 (LA grading not used till after 2001) were identified from the endoscopy database. Patients who did not have repeat OGD, diagnoses other than RE were excluded from the study. Along with demographics (age and sex), data collected included date of initial and repeat OGD, interval between OGDs, LA grade or Savary-Miller grade, presence of oesophageal strictures, whether oesophageal biopsies performed on initial and repeat endoscopies and the presence of Barrett mucosa. Results were analysed using Microsoft Excel 2007 and SPPS v13.0 software.
Results: Of the total 114 patients identified by the software as follow up of oesophagitis, 24 patients were excluded as they either had other oesophageal diagnoses or were not oesophagitis follow ups. Of the 90 patients with follow up endoscopies, 60 (65%) were males and 30 (35%) were females with a median age of 68 years. Mean number of follow up OGDs performed were 2.7 (range 2–10). Mean interval between the index OGD and repeat OGD was 75 days. Overall 40 patients had BE detected on follow up endoscopy. Of the 90 patients, 79 had biopsies performed on initial OGD and 64 patients had biopsies performed on follow up endoscopy. Though only 10 had Barrett’s segment detected along with RE on initial OGD, 40 patients had Barrett’s oesophagus detected on follow up endoscopy; mean length of BE was 3.8 cm (range 1–11). Further, when the RE was grouped as Mild oesophagitis (LA grade A & B; Savary Miller 1 & 2) and Severe oesophagitis (LA grade C & D or Savary Miller 3 and 4), BE is seen to occur in 50% of patients with severe oesophagitis (see table).
Conclusion: BE occurs with all grades of RE but most frequently with severe oesophagitis (LA grade C & D or Savary Miller 3 and 4) on initial endoscopy. Follow up endoscopy is recommended in this subgroup of patients to detect BE. It is not clear whether BE develops as RE heals or whether it is obscured by initial RE.
PW366 CDX2-DEPENDENT HOX GENE REGULATION IN BARRETT’S OESOPHAGUS
M. di Pietro, R. C. Fitzgerald. Cancer Cell Unit, MRC, Cambridge, UK
Introduction: Intestinal metaplasia (IM) of the oesophagus, commonly referred to as Barrett’s oesophagus, is a predisposing condition to oesophageal adenocarcinoma (OAC). The caudal-related homeobox gene CDX2 has been showed to be up-regulated in Barrett’s where it may act a master transcriptional regulator. Homeobox genes represent a large family comprising clustered (HOXs) and non-clustered genes and have been shown to transcriptionally regulate each other. HOX genes have been implicated in the antero-posterior body patterning and their mutation can be a cause of a homeotic shift, where specific body segments resemble others located more rostrally or caudally.
Aims and Methods: Oesophageal IM can be considered as a homeotic shift, therefore we set out to determine if HOX genes have a role in Barrett’s development and to establish a correlation with CDX2 transcriptional activity. To test this hypothesis we evaluated the expression of HOX genes in oesophageal tissue samples and in an in vitro model of gastro-oesophageal reflux induced cellular damage. Quantitative real time PCR and immunohistochemistry were used to assess HOX gene expression in an independent set of oesophageal normal mucosa and Barrett’s endoscopic samples. The OAC cell lines OE33 and OE19 (CDX2 positive) were exposed to acid (pH 4.5) and/or a mixture of bile salts. CDX2-negative HET1A cells were transfected with a CDX2 expression vector and/or siRNA targeting CDX2. CDX2 and HOX gene expression were quantified by real time PCR and western blotting.
Results: A number of HOX genes including HOXD3, HOXB5, HOXB6 and HOXC10 were significantly up-regulated in tissue samples of Barrett’s compared to normal squamous mucosa. OE33 and OE19, when co-treated with acid + bile salts, showed an up-regulation of HOXD3. In HET1A transfection with the CDX2 expression vector brought about up-regulation of HOXD3 and HOXB5, which was reverted by co-transfection with siRNA targeting CDX2.
Conclusion: Barrett’s oesophagus is characterised by derangement of specific HOX genes. In an in vitro model of gastro-oesophageal reflux induced cellular damage, HOXD3 expression was activated by exposure to bile salts and pH acid. The co-transfection of HET1A with CDX2 expression vector and siRNA targeting CDX2 showed that HOX genes are transcriptionally regulated by CDX2.
PW367 ALARM SIGNS IN PATIENTS WITH GASTRO-OESOPHAGEAL REFLUX DISEASE?
N. Powell, E. Russo, G. Mansfield, J. Teare, R. Negus, H. Thomas, T. Orchard, J. Hoare. Gastroenterology, Imperial College NHS Trust, London, UK
Introduction: Guidance from the National Institute for Health and Clinical Excellence (NICE) indicates that patients with dyspepsia and “alarm signs” should be offered urgent oesophagogastroduodenoscopy (OGD), as they are perceived to be at increased risk of cancer. However, there are few data regarding the predictive value of alarm signs in patients with symptomatic gastro-oesophageal reflux disease (GORD).
Aims and Methods: We analysed results from a database of 49 177 oesophagogastroduodenoscopies (OGD) performed at our institution over a 23 year period. Data including patient demographics, indications for endoscopy and endoscopic findings were recorded for each procedure performed. We identified all patients undergoing OGD for reflux/heartburn symptoms and correlated endoscopic findings (upper gastrointestinal (GI) cancers, erosive oesophagitis and Barrett’s epithelium) with the presence or absence of NICE defined alarm signs, including dysphagia, weight loss, vomiting and GI bleeding (anaemia, haematemesis or melaena). We also compared the prevalence and distribution of cancers in patients with reflux/heartburn and alarm signs compared to patients with dyspepsia and alarm signs.
Results: 5358 patients with reflux/heartburn symptoms were identified, comprising 10.9% of all endoscopies performed. Alarm signs were present in 14.3% of patients with GORD symptoms. Upper GI cancer was significantly more common in GORD patients with alarm signs (4.4%) compared to those without alarm signs (0.5%, P<0.0001). Similarly, erosive oesophagitis was significantly more common in patients with alarm signs (44.7%) compared to those without (31.9%, P<0.0001). However, the prevalence of Barrett’s epithelium was not significantly different in patients with alarm signs (3.8%) compared to those without (4.1%). Although the prevalence of upper GI cancer was similar in patients with GORD symptoms and alarm signs (4.4%) and patients with dyspepsia and alarm signs (4.9%), the distribution of cancers was significantly different. In patients with GORD symptoms, cancers of the oesophagus or gastric cardia predominated (76.3% of cancers), whereas these cancers only comprised 34.5% of cancers in patients with dyspepsia, P<0.0001.
Conclusion: In patients with GORD symptoms, the presence of alarm signs confers a significantly increased risk of upper GI cancer and erosive disease of the oesophagus. In contrast to patients with dyspepsia, the majority of cancers observed in patients with GORD are located in the oesophagus or gastric cardia.
PW368 THE EVOLVING EPIDEMIOLOGY OF GASTRO-OESOPHAGEAL REFLUX DISEASE: AN ENDOSCOPIC PERSPECTIVE
N. Powell, E. Russo, G. Mansfield, D. Adjogatse, K. O’Callaghan, J. Naguib, H. Thomas, J. Teare, R. Negus, J. Hoare, T. Orchard. Gastroenterology, Imperial College NHS Trust, London, UK
Introduction: A number of competing factors are potentially changing the epidemiology of gastro-oesophageal reflux disease (GORD). On the one hand, better acid suppressing therapies such as proton pump inhibitors are likely to improve symptom control and reduce the development of erosive disease and other reflux complications. However, risk factor profiles are also changing such as increasing obesity. From the perspective of the endoscopist, identifying meaningful changes in GORD epidemiology is yet further complicated by changes in guidance regarding which patients should undergo oesophagogastroduodenoscopy (OGD).
Aims and Methods: We analysed data from all OGDs performed in patients referred with GORD symptoms (heartburn/reflux) between 1984 and 2006 inclusive. We excluded incomplete examinations and patients diagnosed with malignancy during OGD. Endoscopic findings were defined, including the prevalence of erosive disease and oesophageal stricture, a well recognised complication of GORD. Temporal change in these variables was analysed.
Results: Data from over 45 000 OGDs were analysed. We identified 5294 patients referred for OGD to investigate GORD symptoms. Endoscopic findings in this cohort included macroscopic oesophagitis (33.1%), hiatus hernia (30.5%) and oesophageal stricture (2.3%). The prevalence of macroscopic oesophagitis in our GORD population fell significantly from 38% in the 1980s to 29% in the 1990s (P<0.0001). However, compared to the 1990s, macroscopic oesophagitis has subsequently significantly increased to 36% in the 2000s (P<0.0001). The severity of erosive disease has significantly decreased over time. In patients with erosive disease the proportion with severe oesophagitis has fallen from 30% in the 1980s to 23% in the 1990s and 15% in the 2000s, P<0.0001 for all comparisons. Over the same time period the prevalence of oesophageal strictures has also significantly fallen (4.2% in the 1980s, 2.7% in the 1990s and 1.6% in 2000s, P<0.005). Regarding referral practices, although there has been a statistically significant increase in the proportion of OGDs performed for reflux symptoms over time, these changes were small (9.6% in the 1980s, 10.8% in the 1990s and 12.5% in the 2000s, P<0.0001).
Conclusion: The epidemiology of GORD has likely changed over the last 23 years, at least from an endoscopic perspective. Although the prevalence of erosive disease in patients with GORD symptoms fell between the 1980s and 1990s, it appears that this benefit has been lost over the last decade. However, the prevalence of severe oesophagitis and oesophageal stricture formation has consistently fallen over time.
PW369 COMPARISON OF STAGING ACCURACY OF CONVENTIONAL AND THREE DIMENSIONAL ENDOSCOPIC ULTRASOUND IN SURGICALLY TREATED PATIENTS WITH STAGE III OESOPHAGEAL CANCER
1S. Inglis, 2D. Patel, 3S. Paterson-Brown, 4J. N. Plevris. 1Department of Medical Physics, The Royal Infirmary, University of Edinburgh, Edinburgh, UK, 2Department of Radiology, The Royal Infirmary, University of Edinburgh, Edinburgh, UK, 3Department of Surgery, The Royal Infirmary, University of Edinburgh, Edinburgh, UK, 4Centre for Liver and Digestive Disorders, The Royal Infirmary, University of Edinburgh, Edinburgh, UK
Introduction: Accurate staging of oesophageal cancer is important to rationalise treatment because survival is closely correlated with tumour, nodal involvement and the presence of metastases (TNM stage). To improve survival of more advanced cancers of the oesophagus, it is often necessary to consider additional treatment to surgery alone (for example, neo-adjuvant chemotherapy (NAC)).
Aims and Methods: To investigate the accuracy of conventional and three dimensional endoscopic ultrasound (3D-EUS) as a means to provide detailed and accurate information in the staging of advanced (T3 N1) cancers of the oesophagus when compared with the gold standard of surgically resected tissue histology. 24 patients (7 females and 17 males with mean ages of 69.9±8.2 and 60.8±10.7 years, respectively) had as part of their staging received a CT of thorax/abdomen and EUS with subsequent 3D reconstruction (3D-EUS). A reconstruction of the oesophagus was generated from images acquired during a free pullback of the echo-endoscope at a constant speed and at a rate of 12.5 fps. All patients subsequently had a surgical resection and were confirmed on histology to have T3N1 oesophageal cancer.
Results: In all cases EUS visualised the disease. Conventional EUS obtained correct staging in 75% (18) for T and 79.2% (19) for N staging. Three-dimensional EUS obtained correct staging in 91.2% (22) for T and 87.5% (21) for N staging. In addition to standard EUS, 3D–EUS provided more information and accurately determined tumour dimensions, layer involvement and in particular length relative to reference anatomical structures such as the aortic arch, sub-carinal area or the OGJ, as well as nodal burden. 18/24 patients received NAC. From the 6 patients who did not receive NAC, 4 were staged T3N1 by conventional EUS and 2 were staged T2N0 and T3N0 respectively. All 6 cases were staged as T3N1 by 3D-EUS.
Conclusion: 3D-EUS increased the accuracy of EUS staging and provided additional detailed information regarding tumour dimensions and layer involvement and number/size of nodes. Such information is important in treatment planning, in particular in cases where additional treatment to surgery alone is required.
PW370 THE EFFECT OF SMOKING, ALCOHOL, BODY MASS INDEX, AND WAIST CIRCUMFERENCE IN THE DEVELOPMENT OF OESOPHAGEAL ADENOCARCINOMA: RESULTS FROM MOSES (MIDLANDS OESOPHAGEAL ADENOCARCINOMA EPIDEMIOLOGY STUDY)
1S. C. Cooper, 1S. Prew, 1L. Podmore, 2P. Nightingale, 1N. J. Trudgill. 1Department of Gastroenterology, Sandwell Hospital, West Bromwich, UK, 2Wolfson Computer Laboratory, Queen Elizabeth Hospital, Birmingham, UK
Introduction: The UK has the highest incidence of oesophageal adenocarcinoma (OAC) in the world. We have undertaken the largest case-control study to date, to identify risk factors associated with the development of OAC.
Aims and Methods: Incident cases of OAC were recruited from 12 hospitals in the Midlands and age-, gender-, ethnically- and geographically-matched community control subjects were recruited from primary care. Logistic regression generated odds ratios (OR), corrected for age and gender, for potential aetiological factors 1 and 10 years prior to diagnosis.
Results: 191 OAC (163 men, median (range) age 68 (38–88) years) and 253 community subjects (216 men, age 67 (38–92) years) were recruited. Ever having smoked (OR (95% CI) 2.7 (1.72 to 4.26)), duration of smoking (1.02 (1.01 to 1.03) p<0.0001), and quantity smoked 1 year (1.05 (1.02 to 1.09) p = 0.002) and 10 years prior to diagnosis (1.02 (1.00 to 1.05) p = 0.025) were associated with OAC. OAC patients had a greater body mass index (BMI) 1 year before diagnosis than control subjects (27.8 (19.7 to 54.2) vs 26.6 (17.5 to 50.3), OR 1.07 (1.02 to 1.11) p = 0.004). Waist circumference was also greater among OAC patients 1 year before diagnosis (38 (24 to 60) inches vs 36 (30 to 46) inches, 1.07 (1.02 to 1.13) p = 0.009).
Conclusion: Smoking is strongly associated with the development of OAC with clear evidence of a dose-response relationship. Obesity, as defined by BMI, is also associated with OAC. Moreover, since increasing waist circumference was also associated with OAC, this suggests that male-pattern obesity in particular is associated with the development of OAC.
PW371 THE INFLUENCE OF SYMPTOMS OF GASTRO-OESOPHAGEAL REFLUX IN THE DEVELOPMENT OF OESOPHAGEAL ADENOCARCINOMA: RESULTS FROM MOSES (MIDLANDS OESOPHAGEAL ADENOCARCINOMA EPIDEMIOLOGY STUDY)
1S. C. Cooper, 1S. Prew, 1L. Podmore, 2P. Nightingale, 1N. J. Trudgill. 1Department of Gastroenterology, Sandwell Hospital, West Bromwich, UK, 2Wolfson Computer Laboratory, Queen Elizabeth Hospital, Birmingham, UK
Introduction: Barrett’s oesophagus is the result of chronic gastro-oesophageal reflux disease (GORD) and is associated with the development of oesophageal adenocarcinoma (OAC). We have undertaken the largest case-control study to date to examine the relationship between GORD symptoms and the development of OAC.
Aims and Methods: Incident cases of OAC were recruited from 12 hospitals in the Midlands and age-, gender-, ethnically- and geographically-matched community control subjects were recruited from primary care. Logistic regression generated odds ratios (OR), correcting for age and gender, for duration, frequency and nocturnal symptoms of heartburn and acid regurgitation 1 and 10 years prior to diagnosis of OAC.
Results: 191 OAC (163 men, median (range) age 68 (38–88) years) and 253 community subjects (216 men, age 67 (38–92) years) were recruited. The presence of heartburn and acid regurgitation symptoms, but not duration, were associated with OAC: OR (95% CI) 2.92 (1.96 to 4.35) and 2.07 (1.42 to 3.04) respectively, both p<0.0001. Increasing frequency of symptoms was also associated with OAC: daily heartburn 4.65 (2.18 to 9.9) p<0.0001, daily acid regurgitation 13.51 (3.04 to 60.09) p = 0.001, 1 year prior to diagnosis; daily heartburn 4.98 (2.45 to 10.12) p<0.0001, daily acid regurgitation 4.3 (1.33 to 13.87) p = 0.015, 10 years prior to diagnosis. Finally, nocturnal GORD symptoms were associated with OAC: 1 year prior to diagnosis acid regurgitation 2.54 (1.43 to 4.52) p = 0.002; 10 years prior to diagnosis heartburn 1.89 (1.11 to 3.24) p = 0.02 and acid regurgitation 2.42 (1.32 to 4.44) p = 0.004.
Conclusion: Subjects with GORD symptoms are at increased risk of developing OAC. Duration of GORD symptoms is not associated with OAC. The increased risk of developing OAC is most marked in those whose symptoms occur daily and when symptoms wake individuals from sleep.
PW372 PROTON PUMP INHIBITOR RELATED ACUTE INTERSTITIAL NEPHRITIS
1S. Ray, 2M. Delaney, 1A. F. Muller. 1Dept of Gastroenterology, The Kent and Canterbury Hospital, Canterbury, UK, 2Dept of Nephrology, The Kent and Canterbury Hospital, Canterbury, UK
Introduction: An increasing number of case reports have identified acute kidney injury (AKI) secondary to acute interstitial nephritis (AIN) provoked by proton pump inhibitor (PPI) therapy.1 The present collaborative study identifies experience from a major UK renal unit.
Aims and Methods: All cases of biopsy-proven AIN between Jan 1st 2007 and October 1st 2008 presenting to the regional renal centre (serving a population of 1.1 million), were identified. The notes of all patients (pts) with a diagnosis of AIN and a history of PPI were analysed. Pre-PPI treatment, diagnosis and most recent plasma creatinine concentrations and estimated glomerular filtration rate (eGFR) were obtained. Pts were considered likely to have PPI-associated AKI if a deterioration in kidney function was identified after starting PPI therapy in the absence of a history of any other medications associated with AIN and other renal or systemic causes.
Results: Of the 210 kidney biopsy reports analysed, 6 cases of AIN were found to be strongly associated with PPI therapy and PPIs were the most common drug class associated with AIN. Male : Female 1 : 5. The median age at diagnosis was 66 years (range 60–86). All pts presented with non-specific malaise and tiredness. 5 cases were due to omeprazole and 1 pt esomeprazole. Mean ± SD duration of PPI therapy was 7.7±5.6 months, (range 5–18). Mean ± SD pre-PPI creatinine was 73±30 μmol/L (range 45–103); eGFR 69±23 ml/min/1.73 m2 (range 45–90). At diagnosis, mean ± SD creatinine was 269±217 mumol/L (range 141–697) and eGFR 24±16 ml/min/1.73 m2 (range 5–52), representing a mean decline in eGFR of 65%. The PPI was immediately stopped in all pts. 1 pt required temporary renal replacement therapy. 5 pts were treated with steroids. The mean ± SD most recent creatinine post diagnosis was 129.5±36.5 μmol/L (range 94–196) and eGFR 41±11 ml/min/1.73 m2 (range = 23–52). Although kidney function improved following cessation of PPI and/or treatment with steroids, there was a net decline in kidney function from pre-PPI exposure levels.
Conclusion: PPI related AIN is an important iatrogenic cause of potentially reversible AKI and is likely to be significantly underestimated. Kidney function should be assessed in patients receiving PPI therapy presenting with non-specific malaise or tiredness. AIN should be considered in patients with deteriorating kidney function when receiving PPI therapy. Prompt identification of PPI induced AIN is important as our study suggests (in line with the established literature2) that cessation of therapy can at least partially reverse decline in renal function in most patients.
PW373 SEVERE OESOPHAGITIS AND ITS COMPLICATIONS ARE MORE COMMON IN WOMEN AFTER THE MENOPAUSE
1S. Menon, 2P. Nightingale, 3J. Butterworth, 1N. Trudgill. 1Department of Gastroenterology, Sandwell General Hospital, West Bromwich, UK, 2Wolfson Computer Laboratories, Queen Elizabeth Hospital, Birmingham, UK, 3Department of Gastroenterology, Royal Shrewsbury Hospital, Shrewsbury, UK
Introduction: Barrett’s oesophagus (BO) and oesophageal adenocarcinoma are more common in men. Symptoms of gastro-oesophageal reflux disease (GORD) are equally common in both genders. There are limited data on the effects of gender on the incidence of reflux oesophagitis (RO).
Aims and Methods: To identify the prevalence of reflux oesophagitis (RO) in pre and post menopausal women. Anonymised patient data were extracted from 3 endoscopy databases (Telford, Shrewsbury and City hospital) over an 8 year period (2000–2008). All patients with an endoscopic diagnosis of RO, peptic stricture and BO were identified, including the indication for endoscopy. The total numbers of gastroscopies performed during the corresponding period were also identified. Nominal data were assessed using χ2 test and association between variables was tested using logistic regression analysis.
Results: Of 64 908 gastroscopies performed during the study period, 9770 RO cases (5581 male, 4179 female, mean age 59 (SD 17) years), were identified (15.1%). Overall, RO was commoner in men (χ2 804.6, p<0.001). The incidence of severe RO increased with age (adjusted odds ratio 1.04 (95% CI 1.03 to 1.05), p<0.001) and this increase was more marked in women with increasing age (1.022 (1.014 to 1.030), p<0.001). BO was more common in men (1.39 (1.15 to 1.69), p<0.001) and was associated with increasing age (1.03 (1.035 to 1.043), p<0.001). Among women, the incidence of both BO (1.05 (1.02 to 1.09), p = 0.001) and peptic stricture (1.05 (1.05 to 1.065), p<0.001) increased more rapidly with age than in men. When the indication for endoscopy was reflux symptoms, (n = 8656), identical associations were noted.
Conclusion: Severe RO and its complications, BO and stricture are more common after the menopause in women. There are a number of potential explanations for this observation including hormonal factors, obesity, smoking and drug factors
PW374 A PILOT FEASIBILITY STUDY OF SCREENING FOR BARRETT’S OESOPHAGUS WITH A NOVEL NON-ENDOSCOPIC CAPSULE SPONGE DEVICE IN A PRIMARY CARE SETTING
1S. R. Kadri, 1I. Debiram, 1P. Lao-Sirieix, 1M. O’Donovan, 2J. M. Blazeby, 3A. Males, 4H. Morris, 5F. Walter, 6J. Emery, 1R. C. Fitzgerald. 1Cancer Cell Unit, Hutchison-MRC Research Centre, Cambridge, UK, 2Dept of Surgery and Dept of Social Medicine, University of Bristol, Bristol, UK, 3Cancer Cell Unit, York Street Medical Practice, UK, 4General Practice and Primary Care Research Unit, Cambridge, UK, 5Cancer Cell Unit, General Practice and Primary Care Research Unit, Cambridge, UK, 6Cancer Cell Unit, University of Western Australia, Perth, Australia
Introduction: Screening for Barrett’s oesophagus (BE) may be key to improving survival of oesophageal adenocarcinoma. We have therefore developed a non-endoscopic screening test suitable for primary care whereby the oesophagus is sampled using a sponge contained within a gelatine capsule and stained for immunohistochemical markers.
Aims and Methods: The current study aims to extend our previous experience (Lao-Sirieix Gut 2007) to the primary care setting. A GP prescribing database was searched to identify patients 50–70 years old who had acid suppressant therapy (>3 months in the last 5 years) but did not undergo recent endoscopy. Acceptability of the capsule sponge was measured using a 10 point visual analogue scale (0 is unpleasant and 10 is enjoyable) at day 0 and 7. Patients completed questionnaires at day 0, 7 and 90 to assess the impact of screening on anxiety. The samples retrieved were processed to a paraffin block and slides were stained for a panel of biomarkers validated in known BE (n = 26) and healthy volunteers (n = 25; see table).
Results: 39/211 (18.5%) patients participated (54 accepted but 15 did not attend or were excluded) in the study with a 1:1 male:female ratio and a mean age of 59.6 years. The mean BMI was 31.2 (range 20–48) with a waist to hip ratio of 0.92 (moderate risk) for males and 0.87 for females (high risk). 36/39 (92%) had ongoing reflux which in 21 (55%) occurred >1 per week. 18 (47%) had uncontrolled symptoms despite being on medication. There were no adverse events. The acceptability rating on day 0 was 5.1 (range 2–10) and 4.7 (range 2–8) on day 7. Patients’ general anxiety levels were not increased by undergoing screening but their anxiety related to a diagnosis of BE increased significantly at day 7 (p<0.0001) and reverted back to baseline at day 90. The prevalence of BE was 2/39 patients (5.1%). The best combination of biomarkers, Alcian blue and M1 yielded a sensitivity of 76% and a specificity of 92% (see table).
Conclusion: 20% of contacted patients were willing to participate in this screening study. The capsule sponge is safe and was well tolerated and did not induce unnecessary anxiety. These pilot data are encouraging for the ongoing study which aims to recruit 500 individuals.
PW375 ENDOTHERAPY FOR HIGH GRADE DYSPLASIA AND EARLY OESOPHAGEAL NEOPLASIA IN BARRETT’S OESOPHAGUS: A SINGLE CENTRE RETROSPECTIVE AUDIT
U. Duffy, K. Gowland, A. I. Morris, H. L. Smart. Gastroenterology, Royal Liverpool University Hospital, Liverpool, UK
Introduction: High grade dysplasia (HGD) develops in approximately 5% of patients with Barrett’s oesophagus and has typically been managed surgically. In recent years there has been much interest in the endoscopic treatment of HGD and that of early oesophageal neoplasia (EON), usually by endoscopic mucosal resection (EMR), argon plasma coagulation (APC) or photodynamic therapy (PDT).
Aims and Methods: The aim of this audit was to define the outcomes of endotherapy for HGD or EON in patients with Barrett’s oesophagus attending our gastroenterology unit. Patients who had undergone any form of endoscopic treatment for either HGD or EON were identified from a dedicated upper GI cancer database. Demographic information, diagnosis, procedural details and follow up data were extracted and placed in an Excel spreadsheet for analysis.
Results: A total of 22 patients were identified as having undergone endotherapy between July 2003 and July 2008. The mean age of the group was 71 (range 46–86) years; there were 18 men and 4 women. The underlying diagnosis was HGD in 19 and EON in 3, with all patients being either unfit or initially declining surgery. The primary treatment modality was EMR in 12 and APC in 10 patients. There were 4 procedure related complications: 3 bleeds in the EMR group (2 immediate, treated endoscopically, 1 delayed resulting in hospitalisation and transfusion) with 1 patient in the APC group developing an oesophageal stricture requiring dilatation. There was no procedure related mortality. Over a median follow up period of 33 (range 1–80) months 6 patients (27%) developed a recurrence of their condition, defined as the reappearance of HGD or EON after 1 or more negative biopsies. 2 patients had initially received EMR and 4 APC. The median time to recurrence was 10 months. All patients were subsequently re-treated endoscopically with EMR, APC or both. Over the follow up period there was 1 death. This occurred in a patient with HGD initially treated by EMR who subsequently agreed to undergo oesophagectomy and died in the postoperative period.
Conclusion: This audit has shown that endotherapy for HGD and EON in our unit was performed in mainly elderly patients unfit for surgery. Using EMR or APC, the technique appears safe with minimum morbidity and no procedure related mortality. Recurrence does occur in a significant minority but can be effectively managed by repeated endotherapy. We intend to develop local guidelines for the endoscopic treatment of HGD and EON, expanding the technique to a broader group through patient choice.
PW376 PILOT EVALUATION OF A STOPWATCH METHOD TO ASSESS TIME TO ONSET OF THE SOOTHING AND COOLING EFFECT OF HEARTBURN TREATMENTS
1V. Strugala, 1P. W. Dettmar, 2P. M. Dewland, 3K. Sarratt, 3J. Sykes, 3E. Thomas, 3P. Berry. 1Technostics Ltd, The Deep Business Centre, Hull, UK, 2Simbec Research Ltd, Merthyr Tydfil, UK, 3Benckiser Healthcare (UK) Ltd, Hull, UK
Introduction: A stopwatch method to evaluate the onset of action of drug treatments has previously been successfully used in subjective conditions of postoperative dental pain and migraine. The aim of this pilot study was to establish if the stopwatch methodology was appropriate in the condition of gastro-oesophageal reflux. A dual stopwatch technique was used to assess the time of onset of consumer-perceived feelings of soothing and cooling in response to treatments for the relief of heartburn (HB).
Aims and Methods: Single-centred, randomised, crossover pilot study. 20 subjects who experienced post-prandial HB (moderate severity), confirmed in a screening visit after a standardised refluxogenic meal, were recruited. 4 treatment visits (2–7 days apart) in which each subject evaluated 4 blinded treatments, Gaviscon Liquid® (GavLiq), Gaviscon Advance® (GavAdv), Gaviscon Double Action Liquid® (GavDALiq), and Control (a sublingual tablet) in a randomised order. The subject received a standardised refluxogenic meal and remained supine until moderately severe HB was experienced and then changed to a sitting position and dosed the allocated treatment. At the point of dosing, 2 stopwatches were started and the subject was asked to stop one when they perceived a “soothing effect” and the second when they perceived a “cooling effect” in the oesophagus/throat. If no perceived sensation was felt within 30 min the result was reported as censored at 30 min (>30).
Results: The dual stopwatch method was successfully used by all subjects to record the perceived sensations of cooling and soothing and also to distinguish between them. All of the subjects perceived a soothing effect within 30 min for the Gaviscon® products compared to only 20% for Control. Median time (min) to the first perception of soothing was 1.37, 1.34, 1.17 and >30 for GavLiq, GavAdv, GavDALiq and Control, respectively. Perception of a cooling effect within 30 min was seen by 100%, 85%, 95% and 15% of subjects for GavLiq, GavAdv, GavDALiq and Control, respectively. Median time (min) to first perception of cooling was 0.57, 1.03, 0.45 and >30 for GavLiq, GavAdv, GavDALiq and Control, respectively.
Conclusion: The dual stopwatch method was shown to be suitable for use in assessing relief from HB by timing onset of the subjective sensorial effects of soothing and cooling. The three Gaviscon® products evaluated displayed fast onset (<1.5 min) of soothing and cooling effects on the oesophagus during an episode of post-prandial HB induced by a standardised refluxogenic meal. In conclusion, this pilot study has shown that the dual stopwatch method is suitable for evaluation of the onset of action of Gaviscon® products in terms of providing a soothing and cooling effect.
Radiology posters
PW377 PROSPECTIVE COMPARISON OF HIGH FREQUENCY MINI PROBE ULTRASOUND AND CONVENTIONAL COMPUTED TOMOGRAPHY IN THE LOCAL STAGING OF COLONIC CANCERS
1A. K. Haji, 2S. Ryan, 3I. Bjarnason, 1S. Papagrigoriadis. 1Colorectal Surgery, Kings College Hospital, London, UK, 2Radiology, Kings College Hospital, London, UK, 3Gastroenterology, Kings College Hospital, London, UK
Introduction: The introduction of the colorectal cancer screening programme may see an increase in mucosal lesions and early cancers amenable to advanced colonoscopic and laparoscopic techniques. In addition, locally advanced colonic cancers are being subject to neo-adjuvant chemotherapy. Therefore, accurate pre-operative local staging of colonic cancers is becoming of paramount importance.
Aims and Methods: We prospectively compared the performance of endoscopic high frequency mini probe ultrasound (HFUS) and conventional computed tomography (CT) in the local staging of colonic cancers. 25 consecutive patients with colonic cancer were recruited after informed consent. Pre-operative investigations included colonoscopy and multi-slice CT with multiplanar reconstruction read by an experienced colorectal radiologist pre-operatively. All patients underwent both 12.5 MHz and 20 MHz US (Olympus Keymed UM-3R, Japan) either during the primary colonoscopy or on table prior to colonic resection. The images were read by 2 authors who were blind to the results of the CT. The local staging by both modalities were compared to the histological stage of the resected specimen. Statistical differences were analysed using χ2 and Fisher’s exact t tests with Graphpad Prism 5 (Version 5.1, 2007).
Results: The distribution of colonic cancers were: sigmoid (n = 8), caecum (n = 7), descending (n = 4), recto-sigmoid (n = 4), hepatic (n = 1) and splenic flexure (n = 1). Histological assessment of the resected specimens revealed 5 T1, 2 T2 and 18 T3 cancers. Conventional CT overstaged all T1 tumours, 4 as T2 and 1 as T3. For T3 tumours, the sensitivity and specificity of CT was 72% and 71%, respectively. This was significantly different to both 12 and 20 MHz US which accurately staged all T1 and T3 cancers offering 100% sensitivity and specificity (p = <0.005). All imaging modalities correctly staged only 1 out of 2 T2 tumours, overstaging to T3. Overall, accuracy of T staging by CT was 56% compared to 96% by both 12 and 20 MHz US (p = <0.005). Histologically 9/25 (36%) patients were positive for nodal disease. Both CT and 12 MHz US were significantly better than 20 MHz US for detection of nodal disease (p = <0.005), with no significant difference between CT and 12 MHz US (p = 0.30). The sensitivity and specificity for detection of nodal disease by conventional CT was 89% and 38%, respectively, with a positive predictive value (PPV) of 44% and negative predictive value (NPV) of 86%. In comparison, staging by 12 MHz US had a sensitivity of 100% and a specificity of 75%, significantly better than that offered by 20 MHz US at 25% sensitivity and 86% specificity (p = <0.005).
Conclusion: Colonic ultrasound with miniprobes is significantly more accurate than CT staging of colorectal cancers. The technique has potential application as a routine procedure during colonoscopy.
PW378 A CATHETER-MOUNTED MAGNETIC RESONANCE DETECTOR COIL FOR BILIARY IMAGING: FIRST IN VITRO BILIARY IMAGES
1C. A. Wadsworth, 2R. R. A. Syms, 1S. A. Khan, 3R. J. Dickinson, 4W. M. W. Gedroyc, 1M. R. Thursz, 2M. M. Ahmad, 3S. A. Awan, 4W. Caspersz, 1S. D. Taylor-Robinson, 2I. R. Young. 1Department of Hepatology and Gastroenterology, Imperial College London, London, UK, 2Department of Electrical and Electronic Engineering, Imperial College London, London, UK, 3Department of Bioengineering, Imperial College London, London, UK, 4IMR Unit, Imperial College London, London, UK
Introduction: The incidence of cholangiocarcinoma (CC) is rising globally. CC has increased to become the commonest cause of death from a primary liver cancer in the UK. Despite advances in CT and MR technology, the correct classification of biliary strictures as benign or malignant remains difficult. This is particularly so in patients with primary sclerosing cholangitis, the commonest known predisposing factor for CC. Even endoscopic retrograde cholangiopancreatography (ERCP) with brush cytology has a low sensitivity for neoplasm detection. Traditional axial MR systems have an external detector radio-coil built into the scanner gantry. An MR system in which the detection radio coil is closely apposed to the tissue of interest could improve the resolution of the images obtained. Our group has developed a prototype version of such a coil, designed such that it could be passed into the biliary tree via an endoscope to improve tissue conspicuity.
Aims and Methods: We aimed to confirm the utility of a prototype coil in obtaining MR images, collect quantitative resolution data and prove that the probe could function in wet conditions. Images were acquired using a 1.5T GE SignaTM scanner, using the main body coil for excitation and a wrap-around microcoil probe for detection. The microcoil is a 35 mm long 2-turn thin film device, tuned and matched at 63.8 MHz, with discrete SMD capacitors; and is attached to an 8F biliary catheter. Overall, the probe is 2.7 mm in diameter and is fully MR compatible. Range and resolution were established first, by placing the coil between a standard spherical water phantom and cuvettes containing microfabricated resolution test samples. The micro-coil was located at the magnet isocentre and arranged parallel to the magnet bore. 3D GRE sequences containing 28 slices, each 1.2 mm thick, were used (TR = 33 ms, TE = 15 ms, 256×256 image points, 8 cm field of view). Imaging was then carried out using meat models with the coil inserted into the biliary tree and liver parenchyma.
Results: Scanning microfabricated test samples produced images showing entire cuvettes (1 cm deep) with 1 mm resolution test bars clearly visible, together with a similar depth of water phantom. Imaging of porcine biliary tree revealed anatomical detail to a depth of more than 1.5 cm, 360 degrees around the coil, along 3.2 cm of its length. Branching bile ducts and blood vessels can be visualised clearly in the images presented.
Conclusion: The MR probe developed by our group can reliably produce images of a resolution of at least 1 mm and demonstrate anatomical detail in meat models. Further work is required to increase the useful length of the probe and improve the images obtained. Work is underway on a clinical trial of this device.
PW379 USE OF MOLECULAR IMAGING TO DIFFERENTIATE LIVER METASTASES ORIGINATING FROM TWO DIFFERENT PRIMARY NEOPLASMS IN THE SAME PATIENT
1K. K. Desai, 1A. Jayratnam, 1V. M. Robinson, 1E. Carras, 2A. Quigley, 2J. Buscombe, 1C. Toumpanakis, 1M. Caplin. 1Neuroendocrine Tumour Unit, Royal Free Hospital, London, UK, 2Nuclear Medicine Department, Royal Free Hospital, London, UK
Introduction: Synchronous malignant neoplasms in a single patient are well documented in the literature. At least 10% of patients with neuroendocrine tumour may develop another cancer, not infrequently colonic adenocarcinoma. FDG PET is recognised as “standard” imaging for staging metastatic disease in colorectal cancer and recently Gallium-68 DOTA Octreotate PET has been developed as molecular imaging for neuroendocrine tumour staging.
Aims and Methods: To assess molecular imaging utilising (18F) FDG PET scan and Gallium 68 DOTATATE PET scan for differentiating liver metastases arising from colorectal cancer or neuroendocrine tumour in an individual patient. We studied a patient who had recently undergone left hemicolectomy (Duke’s B adenocarcinoma) of the sigmoid colon, and was found to have multiple liver metastases and a pancreatic tail mass compatible with neuroendocrine tumour. The patient underwent (18F) FDG PET scan and (68Ga) DOTATATE PET scan. He also underwent ultrasound guided liver biopsy.
Results: The two types of PET scan showed differential uptake in the liver. Some metastases had avid uptake only on the FDG PET and the others only on the Gallium 68 PET, the latter also identifying the pancreatic NET primary. Ultrasound guided liver biopsy specimen confirmed the two types of metastases: moderately differentiated colonic adenocarcinoma and well differentiated neuroendocrine tumour with low grade proliferation index Ki67 <2%.
Conclusion: Uptake of specific peptides by tumours is dependent on the biology of the tumour. (18F) FDG PET is very sensitive in detecting metastasis arising from colon cancer in keeping with the fact that FDG PET targets the glucose transporter in these actively multiplying cells. However, neuroendocrine tumours are more indolent, and studies have shown that sensitivity of FDG PET in detecting metastasis in these tumours is much lower. NETs express somatostatin receptors, predominantly subtype-2, which has led to the development of new radio peptides such as (68) Gallium DOTATATE PET, which is much more sensitive and specific in defining distant metastasis related to NETs. We therefore demonstrate the utility of different PET agents for identifying different cancers in an individual patient.
PW380 AUDIT OF ULTRASOUND GUIDED PERCUTANEOUS LIVER BIOPSY: ARE WE DOING ENOUGH?
1S. S. Webster, 2M. Sriharan, 1M. Anderson, 2N. Khan. 1Gastroenterology, Chelsea and Westminster Hospital, London, UK, 2Radiology, Chelsea and Westminster Hospital, London, UK
Introduction: Liver biopsy is an important investigative tool in the management of a wide range of hepatic disease. Ultrasound guided percutaneous liver biopsy (UG-PLB) is an invasive but relatively safe procedure. To avoid sampling error and histological inaccuracy, it is important that technique maximises sample size. Recent evidence suggests that especially in chronic viral hepatitis (CVH) larger sample sizes give more accurate histological stage and grade of disease activity.
Aims and Methods: We aimed to retrospectively assess demographics, indications, operator experience, needle type, sample size, complications and overall helpfulness of PLBs at our centre over a 12 month period against standards suggested recently for CVH,1 to national audit data,2 to BSG guidelines3 and to our own previous audit (unpublished).
Results: 101 patients had UG-PLB during the 12 months analysed. 67% of patients were male, mean age 50.9 (range 16–85). 35% of patients had CVH (HBV or HCV). All PLBs were image guided and all were performed by radiologists. 56% of procedures were performed by radiology registrars. 66% were performed using a 16Fr Tru-Cut needle. 91% of procedures involved 1 or 2 passes. 98% of samples were suitable for histological analysis. 92% of samples exceeded aggregate length of 10 mm. 31% of samples had an aggregate length ⩾2 cm and portal tracts ⩾11. The histology was clinically helpful in 81%. The complication rate was 8%. One patient died within 30 days of the procedure.
Conclusion: The number of USG-PLB performed in our hospital (100/yr) is comparable between 2005 and 2007. The indications were consistent with BSG guidelines (2004). Documentation of procedure was generally good. 100% PLB were performed using ultrasound guidance compared to 38% nationally in 1991. All USG-PLB were performed by radiologists in contrast to 1991 national data (1/3 general physicians, 1/3 gastroenterologists, 1/3 radiologists). Complication rates were comparable with national data (8% vs 5%). One death within 30 days was not procedure related. Sample adequacy and usefulness was satisfactory. However, bigger sample sizes may be needed for CVH patients. To try and improve sample adequacy and histological accuracy our local policy has changed to advise 2 16Fr passes. This can be done safely without significantly affecting the complication rate.3 We are currently re-auditing our data with a larger subset of patients with CVH to assess whether sample adequacy has improved without compromising our complication rate.
PW381 DILATED COMMON BILE DUCT WITHOUT AN OBVIOUS CAUSE ON MAGNETIC RESONANCE CHOLANGIO-PANCREATOGRAM: A 5 YEAR RETROSPECTIVE STUDY
1Z. Ibrahim, 2C. Jones, 3M. Warren, 3S. Chatterjee. 1Medicine, North Tyneside General Hospital, North Shields, UK, 2Medicine, Wansbeck General Hospital, Ashington, UK, 3Gastroenterology, North Tyneside General Hospital, North Shields, UK
Introduction: Magnetic resonance cholangio-pancreatogram (MRCP) is now widely available as a modality for imaging the biliary tree. We aimed to define the profile of patients who had a dilated common bile duct (CBD) on MRCP, but without an obvious cause being demonstrated.
Aims and Methods: We reviewed the MRCP reports of all patients at North Tyneside Hospital in the past 5 years and excluded all the patients in whom the scan could assign a cause for a dilated CBD. All patients in whom the MRCP reported a dilated CBD, but the cause was not apparent, were included in the study.
Results: We identified 86 such patients (24 male; 62 female): 11 patients were under 40 years age, 23 between 40 to 60 years, and 52 were more than 60 years age. The indication for MRCP was abdominal pain in 29, abnormal liver function tests (LFTs) in 11, and both in 38 patients. LFTs were done pre-MRCP in 83 patients. The notes of 8 patients could not be obtained. 56 had obstructive and 19 had normal LFTs. 75 patients had some form of imaging prior to MRCP (ultrasound - 66; CT abdomen/pancreas - 7; both - 2). Ultrasound or CT demonstrated dilated CBD in 55 patients, normal in 15 patients and was not commented upon in 5. The results of MRCP were correlated with the indications for imaging, LFT abnormality and pre-MRCP scans. Out of the 75 patients with dilated CBD on MRCP, 29 had evidence of stones/sludge in the gall bladder (GB) and 8 had thickened GB suggestive of cholecystitis in pre-MRCP ultrasound scans. Seven patients had cholecystectomy in the past and the dilated CBD was considered to be normal in that subgroup. Six patients had evidence of chronic pancreatitis with abnormal CBD and pancreatic duct (PD). Five had a CBD stricture, 2 had ampullary stenosis, 4 had metastatic cancer, and 1 had hepatic cystic disease. One was later diagnosed with primary sclerosing cholangitis. True CBD dilatation without a cause was recognised in only 12 patients. The main indication for MRCP in this group was abdominal pain. Seven had normal LFTs and 5 of them had minimally obstructive LFTs (max ALP 133; max GGT 155). The diameter of CBD on MRCP ranged from 7 to 10 mm. These patients were followed up for 2 years. Two patients were suspected to have sphincter of Oddi dysfunction and 2 needed cholecystectomy in the follow-up period; one for chronic cholecystitis and the other for empyema of the GB.
Conclusion: MRCP is a very sensitive investigation in documenting CBD pathology. True dilatation without a cause is uncommon. These might be normal variants and do not herald a sinister pathology as we have observed in our 2 year follow-up period. Sphincter of Oddi dysfunction is an important consideration in this subgroup. Further investigations are needed to find out whether an association between a dilated CBD and abdominal pain is significant.
Service development posters
PW382 ARE WE USING TUMOUR MARKERS APPROPRIATELY?
C. L. Gan, L. Sunder Raj, S. Malik, M. A. Czajkowski. Department of Gastroenterology, Royal Gwent Hospital, Newport, UK
Introduction: Tumour markers are increasingly becoming part of routine investigations nowadays. Currently there are no clear guidelines on their use throughout the UK and the use of tumour markers has rarely been studied properly in the past. To investigate further the use of tumour markers, requests for gastrointestinal tumour markers, i.e. CEA, CA19–9 and AFP, were studied and compared with recommendations made by European Group On Tumour Markers (EGTM) and American Society Of Clinical Oncology (ASCO).
Aims and Methods: All the inpatient and outpatient requests made for CEA, CA19–9 or AFP within Royal Gwent Hospital and St Woolos Hospital between 3 March 2008 and 7 March 2008 were studied prospectively. Medical records and test results from clinical workstations were reviewed to ascertain the indication for their requests.
Results: In total, 140 requests in 81 patients were analysed. 91% of CEA, 98% of CA19–9 and 44% of AFP were requested inappropriately, according to EGTM and ASCO recommendations. 54% of the patients had more than two tumour markers requested. Incidental findings also revealed 3 requests for CA153 and 13 requests for CA125 were made in male patients from our study, which were inappropriate. Most of these inappropriate requests were made to screen for malignancy in patients suspected for cancers of any origin. Medical and surgical departments were equally responsible for these inappropriate requests. Estimated wastage of resources based on test reagents alone exceeded £8000/pa. Also, wastage of consultants’ time, outpatient appointments and unnecessary subsequent investigations were noted but difficult to quantify.
Conclusion: The majority of requests for gastrointestinal tumour markers are inappropriate, according to the international guidelines. This is probably also the case for many hospitals in the UK. A trust wide guideline is now being created to help prevent these inappropriate requests. The findings and recommendations could also apply to other hospitals in the UK in order to improve practice.
PW383 THE YIELD OF ENDOSCOPY IN PATHOLOGY DETECTION IS MUCH HIGHER THAN EXPECTED
C. S. Kothari, N. V. Someren, K. Besherdas. Gastroenterology, Barnet and Chase Farm Hospitals NHS Trust, Enfield, Middlesex, UK
Introduction: The demand for gastrointestinal endoscopy is increasing with a resultant rise in overall costs and waiting lists for endoscopic procedures. Therefore, adherence to appropriate indications for these procedures is essential for the rational use of finite resources. Appropriateness of endoscopy is an important aspect of the Global Rating Scale. There is evidence from published studies from Europe that the proportion of patients with negative endoscopies is increasing.1 Further to development of a new endoscopy referral form and vetting of endoscopy requests by a consultant gastroenterologist, we set out to assess the detection of pathology rate in endoscopies performed within our unit.
Aims and Methods: To determine the pathology detection rate at endoscopy following the introduction of consultant triaging of procedures. In addition to assess any difference in pathology detected in patients being referred for inpatient and outpatient endoscopy. A single centre retrospective analysis of 1500 consecutive patients referred for endoscopy within an associated teaching hospital was performed. All completed referral forms for endoscopy, inpatient or outpatient, were vetted by consultant gastroenterologist for appropriateness of indication. Patients undergoing endoscopy were analysed for detection of pathology.
Results: Of the 1500 endoscopies, pathology was detected in 927 (62%). Out of a total of 382 inpatients, 252 had a pathology found (65.96%). Out of a total of 1118 outpatients, 675 had a pathology found (60.37%). Pathology included various lesions ranging from benign polyps, ulcers, oesophageal strictures, Mallory Weiss tears to neoplastic growths.
Conclusion: There is a very high pick-up rate of pathologies within our unit in comparison to published reports from Europe of reducing rates of pathology detection. This may well reflect the selection criterion of endoscopy and consultant vetting. Overall, there is a greater chance of inpatients having pathology compared to outpatients although in both groups the pathology pick up rate is greater than 60%.
PW384 THE ONE STOP SWALLOWING SHOP: A BETTER CHOICE FOR SUSPECTED CANCER
D. L. Morris, J. Deacon. Gastroenterology, Queen Elizabeth II Hospital, Welwyn Garden City, UK
Introduction: A succession of cancer targets over the last 5 years have led to streamlining the patient pathway in the management of upper gastrointestinal cancers. The role of the clinical nurse specialist has had a similar impact on the quality of the multidisciplinary care provided. We report on a new combined nurse and consultant led service established to improve patient care and reduce waiting times.
Aims and Methods: A weekly rapid access combined clinic and endoscopy service was established in our District General Hospital, catchment population 250 000. All suspected upper GI cancer 2-week GP referrals from 3 January 2006 to 30 September 2008 were vetted by a consultant gastroenterologist along with all other referrals where dysphagia was a main symptom or suspicion of malignancy raised. Patients were offered a combined assessment with the nurse specialist followed by same morning gastroscopy by a consultant gastroenterologist. Further investigations and management plan were organised according to endoscopic and clinical findings and all malignancies referred directly to the multidisciplinary meeting.
Results: 167 patients (81 male) were seen over 33 months, aged 30 to 98 years. 41 (25%) were 2-week referrals, 116 (69%) urgent and 10 (6%) routine. Dysphagia was the main referring symptom in 120 (72%), dyspepsia in 17 (10%), reflux in 11 (6.6%), and weight loss in 9 (5.4%) patients, respectively. Other symptoms included chest pain, nausea, abdominal pain and pain on swallowing. 23 cancers were diagnosed at endoscopy, 14% of all patients and 18% of those with dysphagia. Including benign disease 34 (20.6%) of all patients had oesophageal strictures. 1 patient had a failed intubation and 1 procedure was abandoned due to food residue.
Conclusion: The rapid access clinic/endoscopy service has done what it states. More than 1/3 of all upper GI cancers are now diagnosed in this clinic enabling direct links into the multidisciplinary team and prompt staging investigations. Patients with benign disease are reassured and discharged directly on treatment reducing need for outpatient follow up. Only 6.7% endoscopies were normal which compares favourably with direct access endoscopy. As 1 in 5 patients seen had oesophageal strictures this is an excellent method of promptly identifying and managing significant pathology. A patient satisfaction survey is underway.
PW385 MORE CANCERS ARE DIAGNOSED IN PATIENTS WITH SYMPTOMS COMPLIANT WITH THE 2 WEEK REFERRAL GUIDANCE THAN ORIGINALLY PREDICTED
G. Masterton, S. Chatterjee, D. Nylander. Gastroenterology, Sunderland Royal Hospital, Sunderland, UK
Introduction: In 2000, the Department of Health (DoH) published guidance for referral of patients with symptoms suggesting cancer, also termed as 2 week referral scheme (2WRS). In this document, it was estimated that there would be 1 cancer for every 15 patients referred with the suggested symptoms.1
Aims and Methods: To assess the proportion of patients referred to medical gastroenterology (MGD) via 2WRS pathway, we performed a retrospective notes audit of referrals over 3 months from 1 April 2007. Notes were recalled in late 2008. From the notes, we obtained information on diagnoses, time from referral to hospital attendance and for those with a diagnosis of cancer, the time to therapy. We also assessed whether patients referred via the 2WRS pathway had the appropriate symptoms as per the DoH guidance.
Results: 1074 referrals were made to MGD of which 221 (21%) were via 2WRS pathway (and all these notes were obtained and viewed). All 2WRS patients were seen within 2 weeks of referral. First hospital contact was outpatient clinic (OPC) in 43%, direct to test in 53% and 4% initially had radiological investigation prior to OPC. In 194 patients (88%) the referral complied with 2WRS. A final diagnosis of cancer was made in 31 patients (sites were oesophageal–4, pancreatic–5, gastric–2, cholangiocarcinoma–2, colorectal–8, hepatoma–1, and others–9). Cancer was suspected at the first point of contact in 97% of these cases. 90% of the cancers were diagnosed within 31 days of referral and 95% were diagnosed and started therapy within 61 days of referral. Gastro-oesophageal reflux disease was diagnosed in 39 patients (18%). 9 patients (4%) were diagnosed with inflammatory bowel disease (ulcerative colitis–2; Crohn’s–4; indeterminate colitis–3). 3 patients were diagnosed as microscopic colitis and 1 had collagenous colitis. 1 patient was diagnosed with coeliac disease. In other patients referred for diarrhoea, the diagnoses were bile salt malabsorption (3), diverticular disease (9), proton pump inhibitor related diarrhoea (2), irritable bowel syndrome (6).
Conclusion: Despite initial concerns, the 2WRS predicted about double the original proportion of cancers estimated by DoH (1 cancer for every 7.1 referrals in this group). The majority (88%) of patients referred via this pathway were compliant with 2WRS. The majority of patients without cancer were found to have organic rather than functional disorders. In our trust, all patients referred to MGD with 2WRS were seen within 2 weeks of referral and 95% of those with cancer started treatment within 61 days.
PW386 APPROPRIATENESS OF THE “STRAIGHT TO TEST” GASTROSCOPY REQUEST FOR PATIENTS WITH SUSPECTED GASTROINTESTINAL CANCERS
1I. Amin, 2P. Steer, 2R. Madhotra. 1Gastroenterology, Milton Keynes General Hospital, Milton Keynes, UK, 2Gastroenterology, Milton Keynes Hospital NHS Trust, Milton Keynes, UK
Introduction: In our experience “Straight to Test” upper GI cancer assessment service is efficient, safe, and cost-effective in establishing early diagnosis of and appropriate management in patients with new diagnosis of gastrointestinal cancer. However, the “Straight to Test” service carries a risk of being used inappropriately and adds further workload to our endoscopy units. In the UK the National Institute for Health and Clinical Excellence (NICE) has provided guidelines for requesting urgent endoscopy in patients with suspected gastrointestinal cancer.
Aims and Methods: The aim of this study is to evaluate appropriateness of the urgent gastroscopy referrals for suspected gastrointestinal cancer in our endoscopy unit at Milton Keynes General Hospital. Between December 2005 and March 2008 all consecutive patients with requests for urgent gastroscopy from their general practitioners under “Straight to Test” rule were evaluated for their appropriateness and followed until final diagnosis. Data were collected prospectively. Each endoscopy request was blindly analysed by a single observer and compared against the current NICE recommendations and categorising them into Appropriate or Inappropriate. Percentage of cancer diagnosis and other endoscopic diagnosis were calculated in both population groups.
Results: A total of 509 referrals were studied prospectively. The mean age was 66.7 years. Commonest clinical category for referrals was dyspepsia 342 (67%), followed by dysphagia 230 (45%). Weight loss, iron deficiency anaemia and jaundice was seen in 40%, 17%, and 4%, respectively. Using NICE guidelines 54 (10.6%) referrals were found to be inappropriate and 453 (88.9%) were in keeping with recommended guidelines. No cancers were diagnosed in the Inappropriate group. In the Appropriate group 69 (15%) patients were diagnosed with cancer. Gastric ulcer, duodenal ulcer and oesophageal ulcer was seen in 7, 4 and 8 patients, respectively in Appropriate group compared to one gastric ulcer and no duodenal ulcer or oesophageal ulcer in Inappropriate group. Reasons for inappropriate referrals included: long duration of symptoms greater than 12 months 18 (31%), anaemia not investigated before referring 13 (22%), dyspepsia under 55 without alarm symptoms 9 (16%), vomiting without alarming symptoms 4 (7%), and miscellaneous 6(10%).
Conclusion: A significant number of patients are referred for cancer assessment outside the recommended guidelines. Patients referred outside the guidelines generally have a low risk of being diagnosed with cancer or significant gastrointestinal pathology. A significant number of endoscopies could be avoided if the primary care physicians strictly adhere to professional guidelines. Modifying our referral form will further aim to reduce the inappropriate requests.
PW387 AN AUDIT OF NURSE PRESCRIBING IN GASTROENTEROLOGY
I. Mason, T. Vaghjiani, O. Epstein. Gastroenterology, Royal Free Hospital, London, UK
Introduction: After identifying the need for independent nurse prescribing in a series of audits of nurse led outpatient services, the Clinical Nurse Specialist (CNS) qualified as an independent prescriber. This audit is the first review of the nurse prescribers practice since qualification.
Aims and Methods: All outpatient prescriptions over a 3 month period were reviewed. The prescriptions were generated in the Nurse Led Dyspepsia, Coeliac and Inflammatory Bowel Disease clinics. Results were reviewed by the designated medical practitioner and the specialist gastroenterology pharmacist.
Results: A total of 89 prescriptions were given. Total of 147 items (mean 1.6 per prescription) and 30 different named drugs were prescribed. Proton pump inhibitors (PPI) were the most commonly prescribed. Omeprazole was the main PPI of choice (95%) as per local guidelines. Two prescribing errors were identified: 1. A methotrexate prescription for 1 week instead of 4 weeks; 2. Calcichew D3 should be prescribed as Calcium D3 forte.
Conclusion: This audit found that independent nurse prescribing had been implemented effectively and safely into the CNS practice. There was no prescribing identified that was inappropriate. No serious prescribing errors were identified.
PW388 GUT-DIRECTED HYPNOTHERAPY IN A DISTRICT HOSPITAL SETTING SIGNIFICANTLY IMPROVES THE SYMPTOMS OF PATIENTS WITH IRRITABLE BOWEL SYNDROME
G. G. Robins, L. A. Reed, S. M. Kelly, A. J. Turnbull, J. L. Turvill, S. J. Smale. Gastroenterology, York Hospital, York, UK
Introduction: Irritable bowel syndrome (IBS) is a chronic disorder affecting 10–20% of the population, with such patients making up to 50% of gastroenterology referrals.1 Recent UK guidelines recommend consideration of hypnotherapy for these patients in primary care,2 but there is sparse information on its use in an integrated secondary care setting. York Hospital serves a population of approximately 280,000 and set up an IBS nurse specialist-led hypnotherapy service in July 2006.
Aims and Methods: The primary aim of this study is to assess prospectively symptom change in IBS patients referred to this service. By definition these patients have failed to respond to conventional advice and medications for IBS. A course of hypnotherapy typically entails 5–7 sessions over 6–12 weeks. Patients are assessed at each session to check ongoing suitability, in terms of compliance with therapy (use of hypnosis CD at home between sessions) and stable mental state. All patients were asked to fill out a Hospital Anxiety and Depression Scale (HADS) pre-therapy, 3 months post- and 6 months post-finishing hypnotherapy. This is a validated Likert-scale based questionnaire that assesses psychological symptoms in two domains – anxiety (HADA) and depression (HADD). A score of 11+ in either domain indicates “probable presence” of mood disorder. A score of 8–10 is borderline. Patients were also asked to complete visual analogue scales from 1–100 on the severity of the following symptoms: pain intensity (PI), pain frequency (PF), bloating (B) and urgency (U). Pre- and post-hypnotherapy scores were compared by the relevant statistical method (Student’s paired t-test or Wilcoxon signed ranks test). All p values are two-tailed.
Results: 62 patients (male 8, female 54) with a mean age (SD) of 40.6 (15.1) years have been referred to this service as of March 2008.
Conclusion: An IBS nurse specialist-led hypnotherapy service significantly improves short-term patient outcomes in a secondary care setting. Longer-term data is needed to determine whether this benefit is sustained.
PW389 IMPACT OF CAPSULE ENDOSCOPY IN THE MANAGEMENT OF IRON DEFICIENCY ANAEMIA
M. Guerra del Rio, M. Mortimer, D. Kerajiwal, L. Baldwin, Y. Miao. Gastroenterology, Ipswich Hospital NHS Trust, Ipswich, UK
Introduction: Establishing a diagnosis for recurrent iron deficiency anaemia (IDA) in the absence of gastric or colonic pathology is difficult. A number of alternative investigations including barium follow through (BaFT) is available. However, the diagnostic yield is small and frequently patients undergo repeated inconclusive tests. Following recent National Institute for Health and Clinical Excellence (NICE) guidelines, capsule endoscopy has been gaining wide acceptance as a diagnostic tool.
Aims and Methods: To evaluate the impact of the introduction of capsule endoscopy (CE) services in our hospital in the diagnosis and management of patients with recurrent IDA. A retrospective analysis of patients with recurrent IDA and negative upper GI and lower GI endoscopy was undertaken. CE was introduced in our unit in June 2004. From July 2005 a patency capsule has been used. Three patient groups were identified : Group A n = 22 Jan 2003 to June 2004 (patients who had BaFT only); Group B n = 24 June 2004 to March 2007 (patients who had a BaFT followed by CE); and Group C n = 19 July 2005 to July 2007 (patients who had a patency capsule followed by CE). Patients were identified via a diagnostic imaging database and a gastroenterology CE database. Results of the investigations were independently reviewed. Hospital case notes were obtained and the number of alternative investigations was determined.
Results: 65 patients were identified (25M: 40F, mean age 57.7 years (range 31 to 88)) with IDA and negative OGD and negative colonoscopy. CE findings included vascular lesions (angiodysplasias Group A 9 (37.5%) Group B 4 (21.0%), venous ectasias A 1 (4.1%), multiple vascular malformations A 1 (4.1%), multiple telangiectatic lesions A 1 (5.2%)) or ulceration (A 6 (25%), B 4 (21%)) Findings were classified as negative, positive, suspicious or incomplete (see table). The total number of investigations needed to establish diagnosis in IDA was 83 in group A, 135 in B and 90 in C, leading to an index mean diagnostic investigation per patient of 2.8 (A), 5.6 (B), 4.7(C).
Conclusion: Use of capsule endoscopy increases the diagnostic yield as compared to BaFT leading to a definite diagnosis in 63% of patients. Replacement of BaFT with CE as a third line investigation reduces the number of diagnostic investigations needed to establish diagnosis. Therefore, use of CE has significant impact in improving outcomes in the investigation of recurrent IDA.
PW390 BISPECTRAL INDEX MONITORING DURING CONSCIOUS SEDATION IN ENDOSCOPIC RETROGRADE CHOLANGIOPANCREATOGRAPHY
1P. Kennedy, 2D. Adjogatse, 1N. Kumar, 1E. A. Russo, 1N. Powell, 1D. Bansi, 1A. Thillainayagam, 1P. Vlavianos, 1D. Westaby. 1Gastroenterology, Hammersmith Hospital, London, UK, 2Gastroenterology, St Mary’s Hospital, London, UK
Introduction: Patient sedation is often cited as a cause for procedure failure during endoscopic retrograde cholangiopancreatography (ERCP). While general anaesthesia is an option to overcome patient intolerance, it is not common practice in the UK. Bispectral Index (BIS) measurement during conscious sedation has been adopted as a tool to monitor the depth of consciousness during procedures.
Aims and Methods: The purpose of this study was to evaluate whether BIS monitoring during conscious sedation in ERCP impacted on sedation doses administered for 300 consecutive ERCPs. Data were analysed retrospectively through procedure reports. We compared 150 procedures performed with BIS monitoring and 150 without. Where BIS monitoring was employed, a score of <80 was considered moderate sedation and guided commencement of the procedure. Patients with low or poor signal quality were excluded from the study.
Results: There were no significant differences in patient demographics in patients monitored by BIS compared to unmonitored patients. There was no significant difference between the median dose of midazolam administered to patients monitored by BIS (median 5 mg, range 0–12 mg) compared to unmonitored patients (median 5 mg, range 1–14 mg). Similarly, there was no statistically significant difference between the median dose of fentanyl in BIS monitored patients (median 100 mg, range 25–200 mg) compared to unmonitored patients (median 100 mg, range 0–200 mg). Only 1 in 150 patients required reversal of sedation in the unmonitored patients compared to 0 in 150 in the BIS monitored group.
Conclusion: There was no difference in the dose of sedation administered to patients monitored by BIS compared to unmonitored patients. Likewise, BIS monitoring did not reduce the frequency of oversedation measured by the need to administer reversal agents. Although BIS permits an objective measure of the effects of conscious sedation, it appears that it does not influence the dose of sedative administered, above and beyond normal clinical judgement.
PW391 PROCESS MAPPING IS A VALUABLE TOOL TO IDENTIFY IMPROVEMENTS IN ENDOSCOPY SERVICES FOR UPPER GASTROINTESTINAL HAEMORRHAGE IN A DISTRICT GENERAL HOSPITAL
1P. J. Basford, 1T. M. Trebble, 2S. Courtney, 1R. W. Bowers, 1N. Gildeh. 1Gastroenterology, Queen Alexandra Hospital, Portsmouth, UK, 2Practice Transformation Team, Queen Alexandra Hospital, Portsmouth, UK
Introduction: Process mapping is a system of healthcare audit relating to a specified patient journey and is a key component of performance management. The aims of mapping are to identify areas of potential service improvement. Upper gastrointestinal haemorrhage (UGIH) is a common cause of acute medical admission and continues to place a significant demand on resources within the acute hospital setting. Endoscopy is an effective mode of diagnosis and treatment for UGIH. We investigated the patient journey in a busy district general hospital through a process mapping exercise.
Aims and Methods: Information about the process relating to admission, initial management, transfer to and treatment in the endoscopy unit was obtained through direct interview of clerical, nursing and medical staff. The individual steps were assessed with respect to maximum and minimum estimated times, delays and limitations to patient flow and the transfer of information. The journey was visualised diagrammatically on a process map, allowing analysis of the individual steps in terms of the overall process time, contribution to the outcome, duplication of work and coordination between departments. Further analysis was undertaken with respect to urgency of the procedure.
Results: 53 steps were identified in the patient journey from admission to completion of treatment within the endoscopy unit. The total process time ranged from 6 hours 21.5 mins (minimum in urgent cases) to 6 days, 8 hours and 2 mins (maximum in non-urgent cases). Delays in the process ranged from 4 hours 13 mins to 6 days 4 hours 2 mins. The proportion of overall process time representing active management (value score) varied from 49.1% to 3.1%. The principle contributory factors to delay in the patient journey identified by the process mapping included: patient stratification, access to endoscopy timeslots and portering services. Inherent system delays also occurred due to parallel flow of patient related information and unnecessary duplication of history taking, examination and assessment. Early specialist gastroenterological review allowed effective patient stratification. Delays awaiting endoscopy could be associated with patients remaining nil by mouth for more than 48 hours.
Conclusion: Process mapping is a useful tool for identifying areas for service improvement and increased efficiency for acute endoscopy for patients presenting with UGIH. Changes to the process may have benefits in terms of utilisation of hospital resources and the patient experience.
PW392 GUIDED SELF-MANAGEMENT FOR PATIENTS WITH ULCERATIVE COLITIS AND CROHN’S DISEASE
S. Gethins, T. Duckett, C. Shatford, R. R. J. Robinson. Gastroenterology, Leicester General Hospital, Leicester, UK
Introduction: The NHS plan proposed that health professionals should be supporting self care initiatives. A landmark study from Manchester in 2001 highlighted the benefits of self-management in patients with chronic ulcerative colitis. Our aim was to evaluate the potential of using the self-management programme in patients with stable inflammatory bowel disease (IBD) attending secondary care.
Aims and Methods: Patients (pts) with stable IBD were recruited from the out-patients. Eligibility criteria: Diagnosis of IBD >12 months, stable on first line medical-management, in remission (defined by Walmsley/HBI scores). Exclusion criteria: on immunosuppressants, steroid use in the last 6-months, admission for active IBD in the last 12-months, complicated disease, e.g. fistula/short bowel, etc. Suitable pts were recruited by the specialist nurse in clinic and provided with a personalised management plan.
Results: 148 pts recruited (114 = UC, 28 = Crohn’s, 4 = indeterminate) (male = 76, female = 72, age range 20–80 years). No suitable patient refused to participate. 2 pts have been re-referred for treatment changes (one as a result of abnormal bloods (letter from GP) and one not responding to plan.) One pt was brought in for investigations due to ongoing flare-up.
Conclusion: Our results suggest a self-management programme is possible for large numbers of patients with IBD and appears to be popular with patients. The programme should lead to significant improvements in the efficiency of gastroenterology out-patients clinics. The views of patients is now being sought.
PW393 THE “ONE-STOP” CLINIC FOR PRISONERS WITH HEPATITIS C: AN INNOVATIVE APPROACH
1S. Masson, 1M. Hewett, 2D. Jones, 2B. Docherty, 1S. Saksena. 1Hepatology, University Hospital of North Durham, UK, 2County Durham PCT, Durham Prison Services, Durham, UK
Introduction: In order to provide more equitable healthcare for prisoners, an integrated care pathway (ICP) for the management of chronic hepatitis C virus (HCV) in the Durham prison cluster was established. Central to this, we created a novel “one-stop” clinic entailing a single visit to secondary care, during which the complete assessment, clinical investigations and counselling could be undertaken, prior to initiating therapy where appropriate.
Aims and Methods: We describe an innovative approach in providing access to clinical investigations and treatment for prisoners with HCV in our “one-stop” clinic. On reception, all prisoners are offered confidential testing for blood borne viruses. All HCV antibody positive patients are offered a PCR test; those who are PCR positive are offered an appointment in the “one-stop” clinic. Prisoners are transferred to the University Hospital for the “one-stop”. In a single visit, they are first seen by a hepatology clinical nurse specialist who obtains a clinical history and examination, routine blood tests and offers counselling regarding harm reduction and the rationale and risks of therapy. They attend for abdominal ultrasound before a final review with the consultant, with further discussion and decisions about treatment. Patients eligible for treatment are then offered further counselling and treatment is delivered to the prison where subsequent monitoring is undertaken.
Results: During 15 months, 60 (37 male, 23 female) prisoners who tested positive for HCV RNA were referred to our service. These included patients with genotype 1 (n = 34), 2 (n = 4) and 3 (n = 22). Risk factors for disease acquisition were intravenous drug use (IVDU) (n = 54, 90%), tattoos done in prison (n = 2, 3.3%), deliberate self-harm with shared blades (n = 2, 3.3%), and unknown (n = 2, 3.3%). The median time from referral to “one-stop” clinic appointment was 6.9 weeks (range 3–14). Of those referred, the majority attended (n = 53, 88%), though a small number of these (n = 6, 10%) required a second visit to hospital for radiological imaging, for logistical reasons. The vast majority (n = 51, 96%) were deemed eligible and have been offered treatment; only 2 were ineligible on grounds of psychiatric illness. So far, 35 prisoners have been treated through this pathway, with 4 due to start soon; a further 11 have declined treatment for various reasons.
Conclusion: With the introduction of the “one stop clinic”, prison referrals can be managed in a timely fashion, enabling adherence with the forthcoming 18-week referral to treatment target, while minimising the pressures on the associated burden of time, security and cost for both healthcare and prison services. We believe this to be an effective management strategy, and a novel and appropriate initiative in this high risk group.
PW394 ENDOSCOPIC BALLOON GASTROSTOMY WITH GASTROPEXY: MORBIDITY AND MORTALITY 28 DAYS POST INSERTION
1Y. Pasha, 1D. G. Walker, 2M. Baulf, 1Y. Chen, 1J. Nightingale, 1S. M. Gabe. 1Lennard-Jones Intestinal Failure Unit, UK, 2Wolfson Endoscopy Unit, St Mark’s Hospital, London, UK
Introduction: In oropharyngeal malignancy, placement of endoscopic balloon gastrostomy with gastropexy is preferable to traditional percutaneous gastrostomy. This avoids seeding malignancy along the gastrostomy tract and is paramount for patients undergoing potentially curative surgery.
Aims and Methods: The aim of the study was to assess the 28 day outcome of patients post PEG-gastropexy insertion. Patients were identified over a 1 year period and an assessment was carried out 28 days post-insertion. For each patient the clinical notes, histology and microbiology were reviewed. All complications were recorded. Main outcome measures were survival and development of complications (pain, infection, bleeding, malposition).
Results: Over a one year period, PEG-gastroplexy was attempted in 15 patients using a Freka gastrostomy tube (Pexact®). The patients' median age was 58 (range 38–81). All patients had oropharyngeal malignancy (11 male: 4 female) and required post-operative/radiotherapy feeding. Insertion was successful in 14 patients (93%). The single procedure failure was due to inability to visualise the introducer needle. 8/15 were placed under general anaesthesia (GA), prior to surgery and 7/15 inserted with midazolam sedation. The abdominal operator was a consultant (7/15), nurse endoscopist (5/15) or specialist registrar (3/15). 28-day survival was 100%, 43% were uncomplicated. There were 3 major complications; 2 patients developed pneumonia (1 had sedation and 1 had GA) and 1 patient had serious haemorrhage post procedure (the patient had anti-phospholipid syndrome, and bleeding occurred despite prior clotting correction; repeat endoscopy (within 24 hours) showed no active bleeding). Minor complications included: 2 minor bleeding episodes at insertion, requiring no action, and 1 gastrostomy-site infection (Day 9, Staphylococcus aureus and mixed anaerobes, treated with Augmentin). 2 tubes were inadvertently removed by patients (days 11, 14) but both were replaced at the bedside without further complication or subsequent infection.
Conclusion: Gastropexy can be performed by nurse endoscopists, specialist registrars and consultants, with sedation or GA. There is an acceptable 28-day survival and serious complication rate. Longer follow-up is necessary to examine incidence of seeding along the gastrostomy tract.
Trainees posters
PW395 TRAINING IN PRACTICAL PROCEDURES REQUIRED FOR GENERAL INTERNAL MEDICINE ACCREDITATION: WHAT IS THE PERCEPTION AND EXPERIENCE OF GASTROENTEROLOGY SPECIALIST REGISTRARS?
1C. P. Selinger, 2X. McFarlane. 1Department of Gastroenterology, Royal Albert Edward Infirmary, Wigan. UK, 2Department of Gastroenterology, North Manchester General Hospital, Manchester, UK
Introduction: Gastroenterology trainees are expected to be competent in performing the following practical procedures required for their General Internal Medicine (GIM) accreditation: central venous lines (CVP) (with or without ultrasound guidance), arterial lines, chest drains, ascites drains, lumbar punctures, invasive temporary cardiac pacemakers and DC cardioversion.
Aims and Methods: The aim of this survey was to evaluate the experience and self-assessed competence and confidence of all Gastroenterology Specialist Registrars (SpR) of the North Western Deanery. Data were collected via an online survey. This included number of procedures performed (overall and within the last year) and a trainee’s self-assessment of their own Confidence Score and Competence Score on a scale of 0 to 10. Satisfactory experience was defined as ⩾10 procedures overall. Confidence and Competence Scores of ⩾7 were deemed satisfactory.
Results: 23 of 32 (76.6%) of trainees took part. 47.8% of participants were in their first and second year of SpR training. The vast majority of trainees showed satisfactory levels of experience, confidence and competence with chest drains, ascites drains, CVP lines, lumbar puncture and DC cardioversion. Only 43.8% used ultrasound guidance when inserting CVP lines. 20% of trainees had little experience (<5), and low confidence and competence with arterial lines. Levels of confidence and competence were low (average scores of 4.47 and 4.53) for cardiac pacemaker insertion and 39.1% trainees had little experience (<5) in performing this procedure. Most SpRs performed <5 of each procedure within the last year.
Conclusion: Most trainees have adequate experience and competence in the practical procedures required for GIM accreditation. Three problems were identified: 1. Ultrasound guidance for CVP line insertion is commonly not used despite NICE guidance. 2. Most trainees perform repeat procedures ⩽five times a year. 3. Regarding invasive temporary cardiac pacemakers, competence, confidence and experience are poor. The majority of hospitals within this Deanery do have Cardiologists on call; this skill may no longer be relevant. To improve shortcomings, structured training may be required for some trainees. All SpRs should be encouraged to seek opportunities to maintain interventional skills.
PW396 HOW USEFUL IS YOUR CUSUM AND COMPLETION RATE?
B. J. Colleypriest, D. Gavin, G. Longcroft-Wheaton, P. F. Marden. Gastroenterology, Royal United Hospital, Bath, UK
Introduction: CUmulative SUM (cusum) is a technique to monitor change in an outcome. All colonoscopists are required to maintain a 90% caecal intubation and a cusum can facilitate the monitoring of this. Increasingly, an endoscopist’s completion rate as reflected by their cusum is used as a quality indicator to assess and compare competence. For cusums to be compared the input data have to be standardised. Currently there is minimal guidance as to what constitutes a completed examination and can lead to inaccuracy of cusums.
Aims and Methods: The aim of this study was to assess variation in cusum calculation among trainee colonoscopists presented with a uniform set of endoscopy scenarios. An anonymous questionnaire was distributed to all trainee gastroenterologists in the Severn and Peninsula Deaneries. SpRs were asked questions concerning their knowledge of national standards, use of and opinions about cusums. To assess variation in cusum calculation, a set of 12 common scenarios was outlined, and trainees were asked how they would be scored. The options were 1 (complete examination), 0 (incomplete), or to discount from the cusum calculation.
Results: An 80% response rate was achieved. 92% of SpRs had attended an accredited training course but only 54% kept a cusum. 83% knew the required standard for caecal intubation. In 67% of scenarios there was considerable disagreement in scoring.
Conclusion: Our results show an unacceptable variability in the way trainee gastroenterologists complete their cusums, reflecting disparate interpretation of a complete examination. Given this discrepancy in input data used to calculate a cusum, it is currently not a tool that can be used to compare competence. For cusums to become standard quality indicators, discretion and subjectivity need to be removed from its calculation. Detailed guidelines from JAG and BSG are needed to describe what constitutes a complete or failed colonoscopy. Only then will it become a useful standardised tool, to assess the competence of trainees’ colonoscopy practice.
PW397 ATTITUDES OF UK GASTROENTEROLOGY TRAINEES TO RESEARCH AND OUT OF PROGRAMME EDUCATION
1E. N. Fogden, 2A. Holt, 3H. Ellison, 4G. Sadler, 5D. G. Thompson, 6M. A. Hull, 1M. J. Brookes. 1Department of Gastroenterology, Royal Wolverhampton Hospital NHS Trust, Wolverhampton, UK, 2The Liver Unit, University Hospitals Birmingham NHS Foundation Trust, Birmingham, UK, 3IT Department, British Society of Gastroenterology, UK, 4Department of Gastroenterology, St George’s Healthcare NHS Trust, London, UK, 5School of Medicine, University of Manchester, Manchester. UK, 6Leeds Institute of Molecular Medicine, University of Leeds, Leeds, UK
Introduction: Changes in training have meant that career pathways and progression have changed significantly. A recruitment crisis in academic medicine exists with up to 10–20% of UK academic posts being vacant. This has been addressed by the Walport report recently; however, these changes may have implications for trainees wishing to undertake a period of research or out-of-programme experience (OOPE) in non-academic training posts.
Aims and Methods: The aim was to determine trainees’ experience of OOPE and evaluate perceived barriers to undertaking a period of OOPE and through a national survey of trainees in gastroenterology.
Results: 56.7% (n = 274) of trainees responded, 71.2% (n = 195) male and 28.8% (n = 79) female. 85.0% (n = 233) trainees expressed a desire to undertake OOPE; 38.3% (n = 105) wanted to undertake a PhD and 40.5% (n = 111) an MD. 49.6% (n = 136) were currently in or had previously undertaken OOPE; 44.8% PhD (n = 61) and 41.9% (n = 57) MD, predominantly in clinical or biological science. The percentage success rate for clinical fellowship applications was up to 29.9%, however this was dependent on gender and training region. 21.9% (n = 60) of trainees wish to become NHS general physicians, 37.6% (n = 103) NHS gastroenterologists or hepatologists, 31.4% (n = 86) NHS gastroenterologists or hepatologists with an academic interest, and 8.8% (n = 24) wanted to become an academic. 93.8% (n = 257) of trainees felt a postgraduate degree would make them more competitive at NHS consultant interview. 50% of trainees rated a PhD or MD as most valuable OOPE for improving future career prospects, with 17.3% rating endoscopy fellowships as most valuable. 83.8% of final year trainees had undertaken research or OOPE. 54.4% had completed their OOPE at the time of survey and 47.3% of this group had received their degree.
Conclusion: The majority of trainees expressed a desire to undertake OOPE and a proportion wish to maintain some academic interest. With changes in training it is likely that career aspirations may change in the future.
PW398 GENDER INEQUALITIES IN ACADEMIA IN UK GASTROENTEROLOGY TRAINEES
1E. N. Fogden, 2A. Holt, 3H. Ellison, 4G. Sadler, 5D. G. Thompson, 6M. A. Hull, 1M. J. Brookes. 1Department of Gastroenterology, Royal Wolverhampton Hospital NHS Trust, Wolverhampton, UK, 2The Liver Unit, University Hospitals Birmingham NHS Foundation Trust, Birmingham, UK, 3IT department, British Society of Gastroenterology, UK, 4Department of Gastroenterology, St George’s Healthcare NHS Trust, London, UK, 5School of Medicine, University of Manchester, Manchester, UK, 6Leeds Institute of Molecular Medicine, University of Leeds, Leeds, UK
Introduction: 60% of medical graduates are female yet women are under-represented in academic medicine. Only 11% of professors and 36% of lecturers are women (2007 CMHS staffing report). 1 in 5 medical schools have no female professors. Studies from the US report that compared to their male counterparts, female GI academics have lower levels of NIH funding, have less laboratory space, publish less and a salary gap exists which increases with age. UK initiatives are in place to address the under-representation of women in academic medicine and include the Athena project and the Women in Academic Medicine (WAM) project.
Aims and Methods: A national survey of trainees in gastroenterology was carried out to determine trainees’ experience of Out-of-Programme Experience (OOPE), their success at research fellowship applications, and evaluate perceived barriers to undertaking a period of OOPE.
Results: 56.7% (n = 274) of trainees responded, 71.2% (n = 195) male and 28.8% (n = 79) female. Overall, 85.0% (n = 233) trainees expressed a desire to undertake OOPE, 38.3% (n = 105) wanted to undertake a PhD and 40.5% (n = 111) an MD. 49.6% (n = 136) were currently in or had previously undertaken OOPE (43.5% of females and 52.8% males.) The majority of OOPE completed or in progress was in clinical or biological sciences with 44.8% studying for a PhD (n = 61) and 41.9% (n = 57) an MD. Fewer women studied for PhD (38% F, 47% M) and MDs (38% F, 43% M). Fewer women wished to pursue careers in academia (6.3% F, 9.7% M) or NHS posts with academic interest (29% F, 44% M.) The overall success rates for all clinical fellowship applications was up to 29.9%; however, there were marked differences in the rates of success in fellowship applications to the major funding bodies, dependent on gender (see table). The number of applications per trainee was less in females (1: 1 F and 1.2:1 M for table). In applications to prefunded posts the success rates were similar (66% F, 59% M) but the number of applications per head was lower (1.16:1 F, 1.68:1 M).
Conclusion: This survey demonstrates significant gender inequalities in academic gastroenterology at the trainee level, particularly with regards to rates of success in fellowship applications to the major funding bodies.
PW399 ENDOSCOPIC MUCOSAL RESECTION/ENDOSCOPIC SUBMUCOSAL DISSECTION (EMR/ESD) MODEL : DEVELOPMENT OF A FIRST UK TISSUE MODEL FOR PRACTICAL TRAINING IN ADVANCED ENDOSCOPY
R. Mead, M. D. Duku, P. Bhandari. Gastroenterology, Queen Alexandra Hospital, Portsmouth, UK
Introduction: Endoscopic techniques are evolving rapidly removing larger deeper, and previously un-resectable lesions with advanced endoscopic mucosal resection (EMR) and endoscopic submucosal dissection (ESD) techniques. These procedures are, however, technically challenging, associated with an increased level of risk, and require a considerable learning curve. There are simulators or models available, but not all are suitable, and most are not practical for training of this type. With the wider background of decreasing doctor hours and trainee time in endoscopy units this means that currently there is no ability to train in these procedures even in specialist centres.
Aims and Methods: We aimed to develop a model that accurately mimicked the human situation, could re-create the upper and lower gastrointestinal tract (GIT), allowed training of advanced endoscopic techniques, had readily accessible components, minimal cost, and rapid accessibility to fit in with training opportunities. A study of the legislation to understand the regulations, and licensing requirements for the proposed approaches was completed. A risk assessment of the cleaning and disposal process, using current guidelines and legislation was completed. Local components were assessed and trialled in combination and alone, to achieve a functional and practical model. Modification to the initial model was made to overcome difficulties, and improve the simulation accuracy during the evaluation trials.
Results: We have developed a working accurate therapeutic endoscopy tissue model of the oesophagus, stomach and colon. We have performed evaluations of dye spray, electrocautery marking, injection, snare, duette, cap and snare, ESD, and clipping in over 40 procedures, using fresh and frozen tissues. Initial components and approaches have been modified to achieve accurate reproduction of the normal human GIT. The model can be available at less than 24 hours notice, with minimal costs, and components that can either be re-used, or disposed of as necessary. All components are from local suppliers, and require minimal skill to assemble. Problems remain with the duette kit in the oesophagus, stomach, and colon, and sub-mucosal injection of the stomach is challenging. However, other ESD and EMR techniques are very realistic and safe.
Conclusion: We have developed a model allowing all trainees the opportunity to practice and refine their EMR and ESD skills, achieving competency before live patient cases. This approach could teach most therapeutic upper and lower GI techniques as part of a skills training programme.