Article Text

Statistics from Altmetric.com
Introduction
Crohn disease is a chronic condition characterised by intestinal inflammation and progressive bowel damage associated with impaired functioning.
In rheumatoid arthritis, which shares some common aetiological pathways and treatments with Crohn disease, treatment goals no longer include symptom control alone, but also alteration of the biological processes underlying synovial inflammation and progressive structural destruction, thereby preventing structural joint damage and functional decline.1 Analogous disease-modifying treatment goals for Crohn disease are currently being conceptualised and may include prevention of structural bowel damage (stricture, fistula, abscess) and impaired gastrointestinal physiology (ie, maintaining normal gastrointestinal physiology).2 3
In order to achieve disease modification, an effective intervention must occur at the right time, that is, before the development of bowel damage and impaired functioning. While it has been said in this context ‘the earlier, the better’, there is no formal definition of early Crohn disease.4 This article will review the rationale for defining early Crohn disease and the rationale for specifically targeting early Crohn disease from both immunopathological and clinical points of view, using rheumatoid arthritis (another chronic, progressive, destructive disease), as an example. We will then propose a definition of early Crohn disease and briefly discuss its potential application in future clinical trials.
Rationale for defining early Crohn disease (see Box 1)
Studies from referral centres have demonstrated that the clinical features of Crohn disease change over time with a decreasing frequency of inflammatory (non-stricturing non-penetrating) disease behaviour and an increasing frequency of stricturing and/or penetrating disease behaviour (disease progression).5 6 Population-based studies have demonstrated that more than 50% of adult patients with Crohn disease develop stricturing or penetrating intestinal complications within 20 years of diagnosis7 and similarly these complications occur in more than 50% of children after a median follow-up of 84 months.8 The development of these complications is associated with a need for surgical resection. Recent population-based studies reported that the cumulative risk for first intestinal resection in adults with Crohn disease was 64% at years 30 from diagnosis9 and in children 34% at 5 years from diagnosis.8 These data suggest that Crohn disease, similar to rheumatoid arthritis,10 is a chronic progressive destructive disease and that effective intervention before the onset of bowel damage (stricture, fistula, abscess) may be required to optimise patient outcomes.
Box 1 Rationale for defining early Crohn disease
Crohn disease is a chronic progressive destructive disease.
Approximately one-fifth of adult and paediatric patients already have evidence of a stricturing or penetrating intestinal complications at diagnosis.
Effective intervention before the onset of bowel damage (stricture, fistula, abscess) is required to modify the clinical course of Crohn disease.
Current molecular tools, such as genetic and serological markers, do not allow the identification of subclinical intestinal inflammation with accuracy.
At present, the only way to define early Crohn disease is to use clinical, biological, endoscopic and radiological criteria.
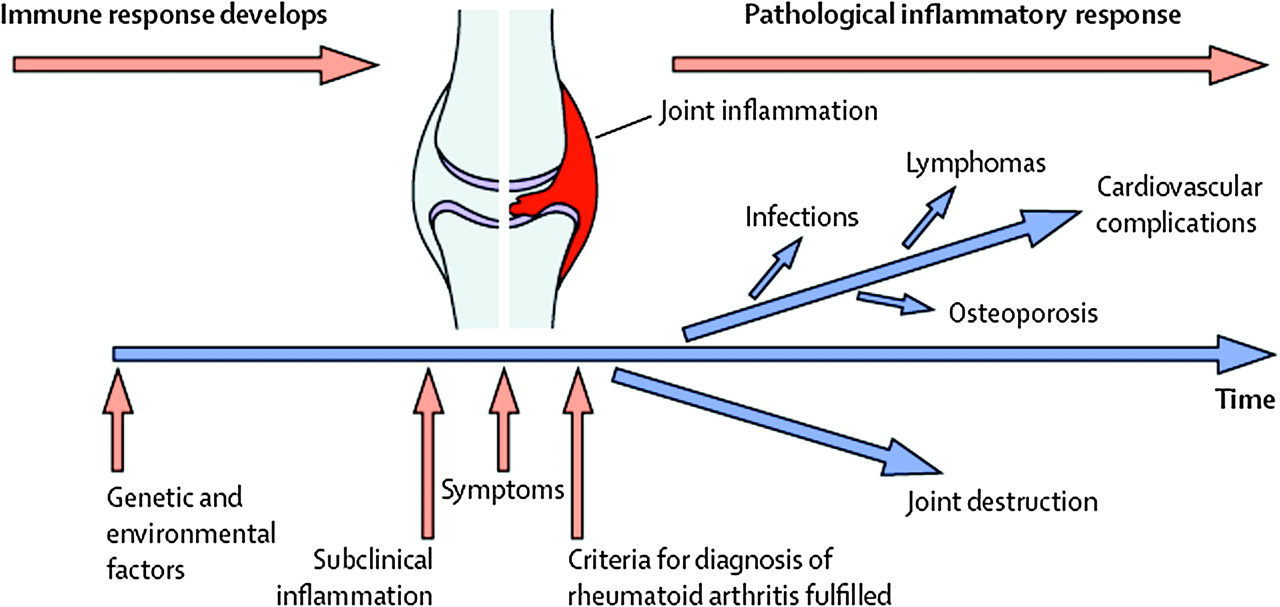
The concepts of ‘a therapeutic window of opportunity’ for early intervention in rheumatoid arthritis and in Crohn disease, aimed at preventing the development of disease complications such as joint or bowel damage, are shown in figures 1, 2.11 The identification of patients with early Crohn disease in clinical practice and for enrolment in clinical trials remains a challenge, as no formal definition exists. In clinical practice, early Crohn disease is usually considered as a newly diagnosed case. This definition may be inadequate to alter the clinical course of Crohn disease, since approximately 20% of adult patients already have evidence of a stricturing or penetrating intestinal complication at diagnosis or within 90 days of diagnosis,7 and disease complications are present in 29% of children at diagnosis.8

Longitudinal course of rheumatoid arthritis (reprinted with permission from Klareskog et al11).

{kind=link}
{kind=link}
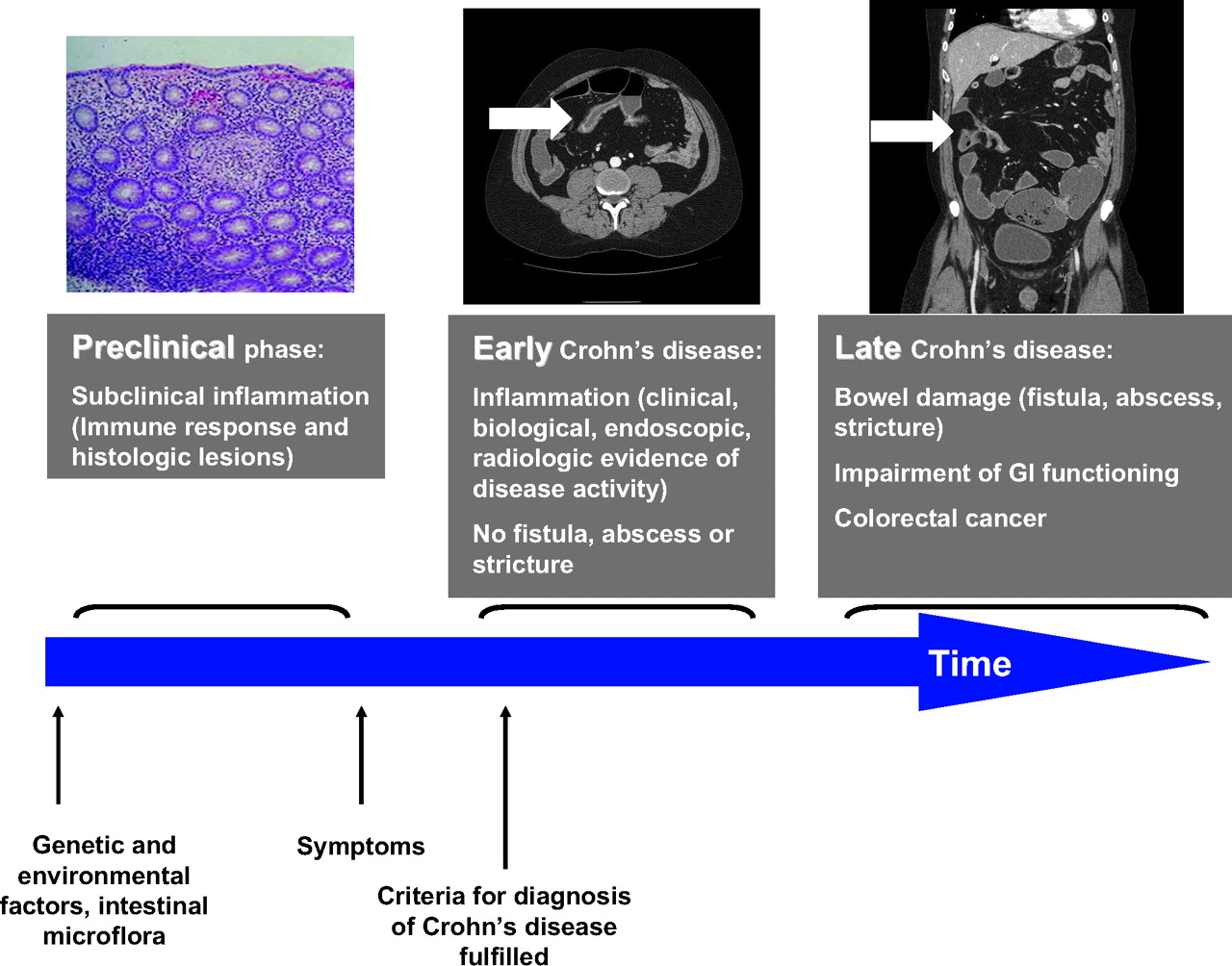
Longitudinal course of Crohn disease; computed tomography enterography showing early (enhancement and increased wall thickness) and late (several loops of small bowel are drawn together with multiple enteroenteric fistulas) lesions in the same patient with Crohn disease (courtesy of D Bruining, Mayo Clinic, Rochester, Minnesota).
Current concepts of Crohn disease pathogenesis suggest a complex interplay between the host susceptibility genes,12 the host intestinal microbiological flora and the environment, resulting in an increased immunological response towards microbiological and self antigens,13 followed by the development of subclinical intestinal inflammation that can be considered as the earliest form of Crohn disease14 (figure 2). In one serum bank study, the presence of anti-Saccharomyces cerevisiae antibody (ASCA) in asymptomatic Israeli military recruits was associated with a subsequent diagnosis of Crohn disease after a median delay of 38 months.15 Increased immune reactivity to the intestinal microbiological flora has also been associated with an increased risk of intestinal complications in patients with Crohn disease.16
Overall, the preclinical stages of Crohn disease remain unexplored, and the question ‘when does Crohn disease start?’ remains unanswered. Currently, it is not possible to identify individuals at risk of developing Crohn disease, and current molecular tools, such as genetic markers (nucleotide-binding oligomerisation domain containing (NOD2), interleukin (IL)-23 receptor, etc), do not allow the identification of subclinical intestinal inflammation with accuracy. Thus, at present, the only way to define early Crohn disease is to use clinical, biological, endoscopic and radiological criteria (figure 2).
Rationale for early intervention in Crohn disease: lessons from rheumatoid arthritis (see Box 2)
Immunopathological evidence
Rheumatoid arthritis is a systemic autoimmune disorder primarily affecting the synovium of peripheral joints.17 Patients with early rheumatoid arthritis have significantly elevated synovial concentrations of IL-2, IL-4, IL-13 and IL-17 as compared with those with established rheumatoid arthritis.18 Later in the disease course of rheumatoid arthritis, increased production of interferon-gamma (IFN-γ) in synovial fluid has been reported.19–21 These data indicate a transient T-helper 2 (Th2) disease phenotype in the early phase of rheumatoid arthritis, with a shift towards a Th1 disease phenotype in the late phase of disease.
Immunopathological studies in both animals and humans have also demonstrated that cytokine profiles change during the clinical course of Crohn disease.22–24
Box 2 Rationale for early intervention in Crohn disease
Immunopathological evidence supports the concept of early intervention in Crohn disease.
Subgroup analyses of large randomised placebo-controlled trials suggested that tumour necrosis factor antagonists (adalimumab, certolizumab pegol) may be more effective in patients with disease duration less than 1 or 2 years.
Many adverse effects may occur at a lower frequency among patients with early rheumatoid arthritis treated with tumour necrosis factor antagonists.
A formal definition of early Crohn disease is needed to develop new therapeutic strategies aimed at modifying the clinical course of the disease.
In experimental murine models of colitis and ileitis, early disease is characterised by Th1 immune responses with upregulation of IL-12 and IFN-γ, whereas a Th2 phenotype (IL-4 and IL-13) is observed when disease enters the chronic phase.25 26
Whether data from animal models of spontaneous colitis or ileitis could be extrapolated to human Crohn disease has only recently been investigated. Kugathasan et al demonstrated that mucosal T cells derived from colonoscopic biopsies from children with early Crohn disease that were conditioned with IL-12 mounted a Th1 response characterised by elevated concentrations of IFN-γ, a phenotype that was not observed in mucosal T cells from patients with late disease.24 In addition, the colonic mRNA concentrations of IL-12 and IL-12Rβ2 chain were higher in early than late Crohn disease.24 In another human study, early endoscopic recurrence of Crohn disease 3 months after ileal resection was associated with a significant increase in IL-4 mRNA concentration and a concomitant decrease in IFN-γ mRNA concentration.23 In contrast, a significant increase in IFN-γ concentration was observed in chronic ileal lesions, together with a marked decrease in IL-4 concentration.23
Disease-specific changes also occur in the expression of adhesion molecules and their ligands,27 such as the chemokine receptor 9 (CCR9), a highly specific receptor expressed by T cells migrating selectively to the digestive tract.28
The results from these immunopathological studies suggest some potential targets for therapeutic intervention in patients with early Crohn disease, including tumour necrosis factor-alpha (TNF-α) inhibition with infliximab, adalimumab or certolizumab pegol, and chemokine receptor CCR9 inhibition with CCX282-B.14
Evidence from clinical trials
The first randomised controlled trials in patients with early rheumatoid arthritis were conducted more than 30 years ago.29 30 Clinical response, progression of disability and erosive damage are now all routinely assessed in early rheumatoid arthritis trials.30 Results from recent large trials have demonstrated that combination therapy with TNF-α antagonists and methotrexate prevents disability and radiographic damage in early rheumatoid arthritis.31–35 The BeSt (Dutch acronym for Behandel-Strategieën, ‘treatment strategies’) study enrolled 508 patients with early rheumatoid arthritis and compared four different treatment strategies36: (1) sequential monotherapy; (2) step-up combination therapy; (3) initial combination therapy with prednisone and methotrexate; and (4) initial combination therapy with infliximab and methotrexate. After 4 years of treatment, joint damage progression remained significantly lower after initial combination therapy compared with initial monotherapy.37
Safety is an important concern when treating patients with disease-modifying drugs. A potential caveat regarding early use of highly effective combination therapy treatment strategies is the possibility of overtreatment, as some patients will have a mild disease course. All the studies in rheumatoid arthritis showed a tendency for more adverse events with combination therapy independently from disease duration, but the differences between studies are small.30 Interestingly, a pooled analysis of clinical trials with TNF antagonists in patients with early rheumatoid arthritis suggested that many adverse effects occur at a lower frequency among patients with early disease.38 Patients with early rheumatoid arthritis in general are younger, use concomitant medications less frequently and have less comorbidity than individuals with longstanding rheumatoid arthritis. Whether early intervention with highly effective therapy that is disease-modifying may reduce the risk of adverse events is unknown.
Few studies have been performed in patients with early Crohn disease. Two trials have evaluated the use of early surgical intervention.39 40 This idea has limited appeal because it permanently alters the gastrointestinal physiology and function. Both observational and placebo-controlled trials have suggested that azathioprine and 6-mercaptopurine may be more effective when administered to children and adolescents early in the course of their disease.8 41 A small controlled trial demonstrated that 6-mercaptopurine significantly reduced the need for prednisone and was more effective than placebo for maintenance of clinical remission.41 In a population-based study from northern France, the use of immunosuppressive therapy in paediatric patients was associated with a decreased risk for surgery.8 Moreover, azathioprine was introduced earlier in the course of disease in patients not undergoing surgery than in patients requiring surgery.8 In adults, experience from a referral centre suggested that despite increasing use of azathioprine in Crohn disease over time, it did appear not to change surgical rates.42 However, these results should be interpreted with caution because less than 10% of patients followed during this period received azathioprine before surgery, the study was not designed to investigate the impact of azathioprine on surgery rates, and many of the patients likely received azathioprine later in the disease course.42
Subgroup analyses from placebo-controlled trials with TNF antagonists have also suggested that patients with early Crohn disease may experience greater efficacy than patients with established disease.43–45 One small randomised trial suggested that combination therapy with azathioprine and anti-TNF therapy may be more effective in patients with early Crohn disease. However, no definite conclusions can be drawn from this study, as efficacy results at 2 years were negative, and the authors used an empirical definition of early Crohn disease.46
Collectively, these observations suggest that the development of a formal definition of early Crohn disease is needed to facilitate the development of new therapeutic strategies.
Proposal for a definition of early Crohn disease for use in clinical trials (see Box 3)
Example of rheumatoid arthritis
Early rheumatoid arthritis is defined by the American College of Rheumatology (formerly, the American Rheumatism Association) 1987 revised criteria47 as a disease duration of ≤2 years, age ≥18 years, and active disease with ≥6 of 66 swollen joints, ≥6 of 68 tender joints, and either an erythrocyte sedimentation rate ≥28 mm/h or a global health score of ≥20 mm on a 0–100 mm visual analogue scale, where 0 is the best and 100 is the worst (table 1). This definition has been widely used in recent disease modification trials in rheumatoid arthritis such as the BeSt study,36 even though significant variations in the definition of disease duration exist. The time frame of early rheumatoid arthritis ranged up to 5 years in some studies.49 50 At this time, ‘early rheumatoid arthritis’ is defined as ≤6–24 months of symptoms.50 The median duration of symptoms at the time of enrolment in most early rheumatoid arthritis cohorts was 5–8 months.50–53 Very early rheumatoid arthritis has been defined with a maximum duration of symptoms of 12 weeks.50 54 Currently, the American College of Rheumatology and the European League Against Rheumatism are in the process of defining new criteria for rheumatoid arthritis that will allow earlier diagnosis and treatment of patients in both clinical practice and clinical trials.55
Box 3 Main points of the proposed definition of early Crohn disease (patient must fulfil all criteria without any exception)
Adult or paediatric patient with an established diagnosis of Crohn disease.
Clinical and biological, endoscopic or radiological evidence of disease activity or positive faecal markers.
No impairment of gastrointestinal function (normal faecal continence, no oral or parenteral vitamin or mineral supplementation and no nutritional support since diagnosis).
No bowel damage (stricture, fistula, abscess) on computed tomography or MRI.
Disease duration less than 2 years.
Being naïve to potential disease-modifying agents.
Not having undergone Crohn disease-related surgery or therapeutic endoscopic procedures.
Proposal for a definition of early Crohn disease and comparison with the definition of early rheumatoid arthritis by the American College of Rheumatology47
Defining early Crohn disease
In the study by D'Haens et al,46 early Crohn disease was defined by the investigators as ‘a diagnosis within 4 years in patients who had not previously received corticosteroids, antimetabolites or biological agents’. This empirical definition did not take into account bowel damage or impaired gastrointestinal functioning. A definition that is more analogous to the American College of Rheumatology definition of early rheumatoid arthritis may better define an early disease population.
Only patients with evidence of clinical and biological disease activity will be considered as having early active Crohn disease. The Crohn Disease Activity Index (CDAI) is a validated instrument which is used to measure disease activity in clinical trials.56 The cut-off value of 220 points is generally chosen to distinguish moderate to severely active Crohn disease.56 In a Scandinavian population-based study, the mean and median C-reactive protein (CRP) concentration at diagnosis were 51 and 33 mg/l (range 0–266 mg/l).57 A total of 25% of patients (44/176) had a CRP level below 10 mg/l at diagnosis. In order to limit the risk of including patients with symptoms related to functional disorders, a cut-off value of 10 mg/l seems reasonable. Because some patients may have active Crohn disease with normal CRP concentrations despite abnormal small-bowel radiographic imaging,58 59 significant endoscopic or radiological evidence (CT or MRI bowel enhancement60 61) of disease activity can be included in the definition as an alternative to the CRP concentration cut-off value. Patients with large coalescent and deep ulcerations covering more than 10% of the mucosal area of at least one segment of the colorectum will be considered as having endoscopic evidence of active inflammation.62 When available, active disease may be detected by using faecal markers, such as faecal calprotectin or lactoferrin.59
We propose that both paediatric and adult patients with Crohn disease can be included in the definition of early Crohn disease. First, about 10% of Crohn disease is diagnosed in childhood.8 63 Second, Crohn disease results in paediatric-specific complications, such as growth failure and delayed puberty.64 65 Third, in a population-based study from France, disease complications were already present in 29% of children at diagnosis, and disease progression led to a cumulative incidence of disease complication of 59% during a median follow-up of 7 years8 with a cumulative incidence of surgery of 34% at 5 years from diagnosis.8 Overall, the consequences of Crohn disease can severely impair physical and social functioning (disability66) in paediatric patients.67
Patients with early Crohn disease should be naïve to drugs that are potentially disease-modifying. These drugs include azathioprine, 6-mercaptopurine, methotrexate and biological agents, such as TNF-α antagonists and natalizumab. Corticosteroids are not effective for maintaining remission.68 Therefore, the use of oral corticosteroids without steroid-dependent disease is not an exclusion criterion from the definition of early Crohn disease. However, patients should not have previously been steroid-dependent (defined as being unable to reduce corticosteroids below the equivalent of prednisolone 10 mg/day or budesonide below 6 mg/day within 3 months of starting corticosteroids, without recurrent active disease, or who have a relapse within 3 months of stopping corticosteroids69) or have received intravenous steroids. Because mesalamine and antibiotics have no or little efficacy in treating Crohn disease and are not disease-modifying agents, their use will be permitted.2
Crohn disease is known to be a transmural disease with progression from inflammatory disease to complications of stricture, fistula and abscess. Hence, the evaluation of the whole intestinal wall is required in Crohn disease, and a combination of both colonoscopic examination of the mucosa of the terminal ileum and colon, and radiographic or magnetic-resonance examination of the small bowel will be necessary to demonstrate the presence of inflammation and the absence of complications in patients with early Crohn disease. While high-quality CT is available in almost all centres managing patients with Crohn disease, there is still a limited access to MRI. MRI is preferred when both techniques are available because of the risks of exposure to ionising radiation from serial CT examinations in patients with Crohn disease, especially those under the age of 35 years.70 71 Several studies now indicate that MRI is accurate for detecting disease activity and assessing disease severity in Crohn disease.61 72 In other cases, CT will be performed. In a Norwegian population-based study, at the time of diagnosis, 121 (61%) had non-stricturing non-penetrating disease, 55 (28%) had stricturing complications, and 24 (12%) had penetrating complications.73 In Olmsted County, Minnesota, USA, 19% of Crohn disease patients had already experienced penetrating or stricturing complications within the first 90 days of diagnosis, and fully half of all patients had experienced an intestinal complication 20 years after diagnosis.7 To be considered as early Crohn disease, patients should undergo gastrointestinal imaging, and no fistulas (including perianal fistulas), abscesses or strictures (defined as wall thickening and luminal narrowing with prestenotic dilatation—defined as a diameter greater than the normal diameter of the small bowel or colon) should be found. In addition, there should be no history of Crohn disease-related surgery, including minor or major surgical procedures (intestinal resection, stricturoplasty, diverting procedure, fistulectomy, fistulotomy, drainage of abscess, placement of seton(s)), and no history of any endoscopic balloon dilation of a Crohn disease stricture. For studies that have the primary aim of preventing bowel damage, as opposed to preventing both bowel damage AND maintaining normal gastrointestinal physiology (see below), it might be reasonable to consider including patients who have had a previous surgical resection and have recurrent inflammatory disease without strictures, fistulas or abscesses. However, such patients should not be designated as having early Crohn disease.
As discussed above, future therapeutic goals for Crohn disease may include not only a reduction in bowel damage but also maintaining normal gastrointestinal physiology.2 Thus, in addition to absence of structural damage and surgical loss of bowel, patients with early Crohn disease should have a normal gastrointestinal function, which consists of normal faecal continence (history of only one episode of incontinence is sufficient to exclude the patient from the definition of early Crohn disease), no requirement for oral or parenteral vitamin or mineral supplementation (ie, vitamin B12, folate, fat-soluble vitamins, etc), and no requirement for nutritional support (enteral nutrition supplementation or parenteral nutrition) since diagnosis. Iron supplementation for iron-deficiency anaemia due to gastrointestinal blood loss is acceptable for inclusion as early Crohn disease.
As suggested by subgroup analyses of large randomised placebo-controlled trials, TNF-α antagonists may be more effective in patients with disease duration less than 1 or 2 years.43 44 Ideally, 1 year should be part of the definition of early Crohn disease, when the economic burden of the disease and efficacy of TNF antagonists are maximal.43 74 Similarly to rheumatoid arthritis,47 a disease duration <2 years is more realistic and will allow the identification of a sufficient number of patients with early Crohn disease, particularly in clinical trials, without including those with longstanding disease. However, in the future, consideration should be given to developing a definition of very early Crohn disease (possibly ≤12 weeks, which is the definition used for very early rheumatoid arthritis).
Our proposal for a definition of early Crohn disease is shown in table 1.
Discussion
Both immunopathological and clinical evidence indicates that early intervention may be a prerequisite for demonstrating the efficacy of drugs that are potentially disease-modifying in patients with Crohn disease. A Europe-wide population-based cohort showed that total and hospitalisation costs were much higher in the first year after diagnosis than in subsequent years.74 A Markov chain analysis of this Europe-wide population-based cohort revealed that surgery accounted for 63% of total healthcare costs in first year, rising to 90% after 6 years of follow-up75 Clinical trials that identify therapies that change this clinical course are needed. Defining early Crohn disease is a prerequisite to undertaking such trials.
Functional and structural damage are increasingly being taken into account in assessing the impact of chronic diseases on the individual, as well as the effectiveness of treatments to impact on the natural course of the disease, including multiple sclerosis76 77 and rheumatoid arthritis.36 We have proposed here a definition taking account both concepts. This article is not a consensus document and should be regarded as a position paper. The next step will involve defining early Crohn disease during a consensus conference involving national and international experts in the field. After the testing and validation phases, this definition may be used in clinical trials and to evaluate drugs for disease modification of Crohn disease. Clinical trials using this definition of early Crohn disease will also help in defining patients who might benefit from early treatment initiation, thus limiting the risk of overtreatment of patients with minimal or inactive disease on one hand and patients who already have irreversible complications on the other. Finally, such clinical studies will evaluate whether specific therapeutic regiments are cost-effective in the treatment of Crohn disease by improving quality of life, reducing hospitalisation, surgeries and other interventions,78 and preventing both bowel damage (stricture, fistula, abscess) and impaired gastrointestinal physiology.
References
Footnotes
Competing interests None.