Article Text

Abstract
Refractory ascites is a frequent complication of advanced cirrhosis and is associated with hepatorenal syndrome and hepatic hydrothorax. Large volume paracentesis and pleurodesis are regarded as first-line treatments in patients who do not respond adequately to diuretics. These treatments, however, do not prevent recurrence and carry the risk of worsening of the circulatory dysfunction leading to hepatorenal syndrome. The transjugular intrahepatic portosystemic shunt (TIPS) has been proposed as an alternative to paracentesis. TIPS reduces the rate of ascites recurrence mainly due to the reduction in the filtration pressure. In addition, TIPS results in a positive effect on renal function, including hepatorenal syndrome, demonstrated by a rapid increase in urinary sodium excretion, urinary volume, and improvement in plasma creatinine concentration. Furthermore, plasma renin activity, aldosterone, and noradrenalin concentrations improve gradually after TIPS insertion suggesting a positive effect on systemic underfilling, the factor of hepatorenal syndrome. As demonstrated recently in two meta-analyses including five randomised studies, TIPS also improves survival when compared with paracentesis. However, the evidence is based on relatively few studies with only 305 patients included. The positive effects of the TIPS are opposed by an increased frequency and severity of episodes of hepatic encephalopathy which may be reduced by both patient selection and reduced shunt diameter. Based on the present knowledge the recommended hierarchy of treatments for refractory ascites may be reconsidered upgrading TIPS in suitable candidates.
- Ascites
- transjugular shunt
- hepatorenal syndrome
- hydrothorax
- portal hypertension
Statistics from Altmetric.com
Introduction
Refractory ascites is defined by its unresponsiveness to diuretics and characterised by oliguria and reduced urinary sodium excretion. Refractory ascites is also present in patients with tense ascites who do not tolerate diuretic medication due to side effects such as azotaemia, hyponatraemia, hyperkalaemia, or hepatic encephalopathy.1 2 Recidivant ascites recurs three times or more a year despite prescription of diuretics in adequate dosage and recommendation of sodium restriction.1 The occurrence of ascites indicates poor prognosis with a 5-year survival of 50%. If ascites becomes refractory to diuretics 50% of patients die within 1 year.1–3
Hepatorenal syndrome (HRS) is a frequent and most serious complication of refractory ascites. Two types are distinguished: a progressive, severe type 1, and a type 2 which shows a more constant renal dysfunction and is commonly associated with refractory ascites.4 Hepatic hydrothorax is also a consequence of ascites occurring in up to 10% of these patients.5 The mostly right-sided, generally large effusion is caused by transition of fluid from the abdominal cavity into the pleural space due to a leak in the diaphragm. Hepatic hydrothorax often results in permanent hospitalisation and early death.
The treatment of refractory or recidivant and of tense ascites and its associated complications has changed considerably during recent years. Large volume paracentesis (LVP)6 has been shown to be safe, easy to perform, and has the advantages of immediate relief of complaints and reduced duration of hospitalisation.2 7 However, the negative effects of LVP on systemic haemodynamics and renal function often limit its use as a permanent treatment, in particular in patients who are not candidates for liver transplantation and who need life-long paracenteses. For such patients, the transjugular intrahepatic portosystemic shunt (TIPS) offers a treatment option which does not exert negative effects on systemic haemodynamics or renal function.
TIPS (figure 1) was introduced in 1988 as a decompressive interventional treatment of portal hypertension with the primary intention to treat variceal bleeding.8 9 Nowadays, TIPS is mainly being used for the treatment of ascites. Thus, as shown by the German TIPS registry,10 in the past 4 years 68% of patients receiving a TIPS had refractory ascites and only 32% were treated for variceal bleeding.

Schematic illustration of a transjugular intrahepatic portosystemic shunt (TIPS) and shunt angiography.
Pathophysiology of ascites formation and HRS
The hydrostatic pressure in portal hypertension is composed of structural and dynamic components. The structural changes in the cirrhotic liver lead to an increase in its vascular resistance. This is further enhanced by a dynamic and reversible constriction of sinusoids by hepatic stellate cells.11 Another dynamic mechanism of portal hypertension is a defective regulation of the splanchnic arteriolae.12 It combines arterial underfilling with a forward increase in splanchnic capillary pressure and blood flow with increased filtration and lymph formation.
The presently favoured hypothesis on the pathophysiology of cirrhotic ascites formation is the forward-flow theory which is based on the peripheral arterial vasodilatation hypothesis.12–14 Accordingly, sinusoidal hypertension initiates a cascade of events leading to ascites formation, but is itself not the dominant factor in its development.15 Thus, sinusoidal hypertension induces systemic vasodilatation and reduces systemic vascular resistance, which is most evident in splanchnic blood vessels. Splanchnic vasodilatation leads to a forward increase in filtration across splanchnic capillaries.16 The lymphatic system is not capable of returning all the filtered fluid which causes ascites formation. Furthermore, systemic vasodilatation causes central vascular underfilling, which stimulates sodium retaining neurohumoral mechanisms. This triggers sodium retention, water retention (with dilutional hyponatraemia) and renal vasoconstriction, which may lead to hepatorenal syndrome.14 15
Rationale of treatments for refractory ascites, effects and side effects
Paracentesis
With ongoing disease severity acites becomes intractable or refractory to the dietary and diuretic therapy requiring additional measures. Large volume paracentesis (LVP) relieves symptoms rapidly and has few technical complications.7 However, it does not correct the underlying problem leading to ascites formation and, therefore, ascites reappears in almost all patients requiring serial use of paracenteses.
LVP has haemodynamic side effects. Shortly after LVP the cardiac output increases and the mean arterial blood pressure decreases by 8–10 mm Hg17 18 together with a further decline of the peripheral and splanchnic vascular resistance.19 Consequently, paracentesis may lead to a further increase in splanchnic blood flow and portal pressure causing an increased filtration rate and rapid ascites re-accumulation.19 In addition, paracentesis aggravates central vascular underfilling with a further activation of the renin–aldosterone and sympathetic nervous systems leading to renal dysfunction and eventually to the hepatorenal syndrome.20 21 This complication is termed as ‘postparacentesis circulatory dysfunction’ which limits the use of LVP in patients with unstable renal function. The infusion of albumin during or shortly after the paracentesis reduces the incidence of postparacentesis circulatory dysfunction from about 50% to 15%.21 22
TIPS
The rationale for TIPS is to decrease the portal pressure and the filtration into the peritoneal space to a level which can be drained by the lymphatic system. Thus, in contrast to diuretics and paracentesis, TIPS may counteract the mechanisms leading to ascites formation.
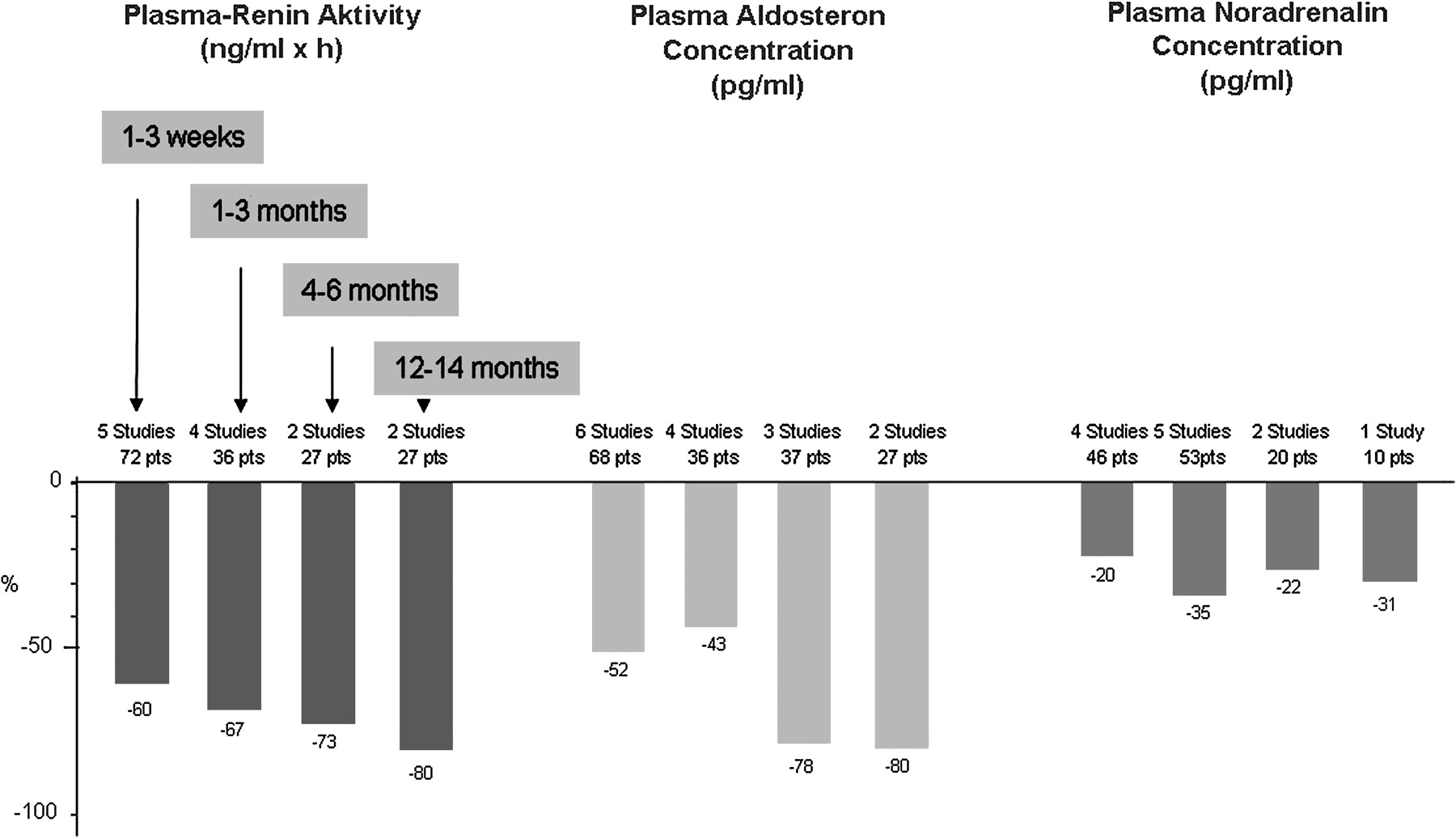
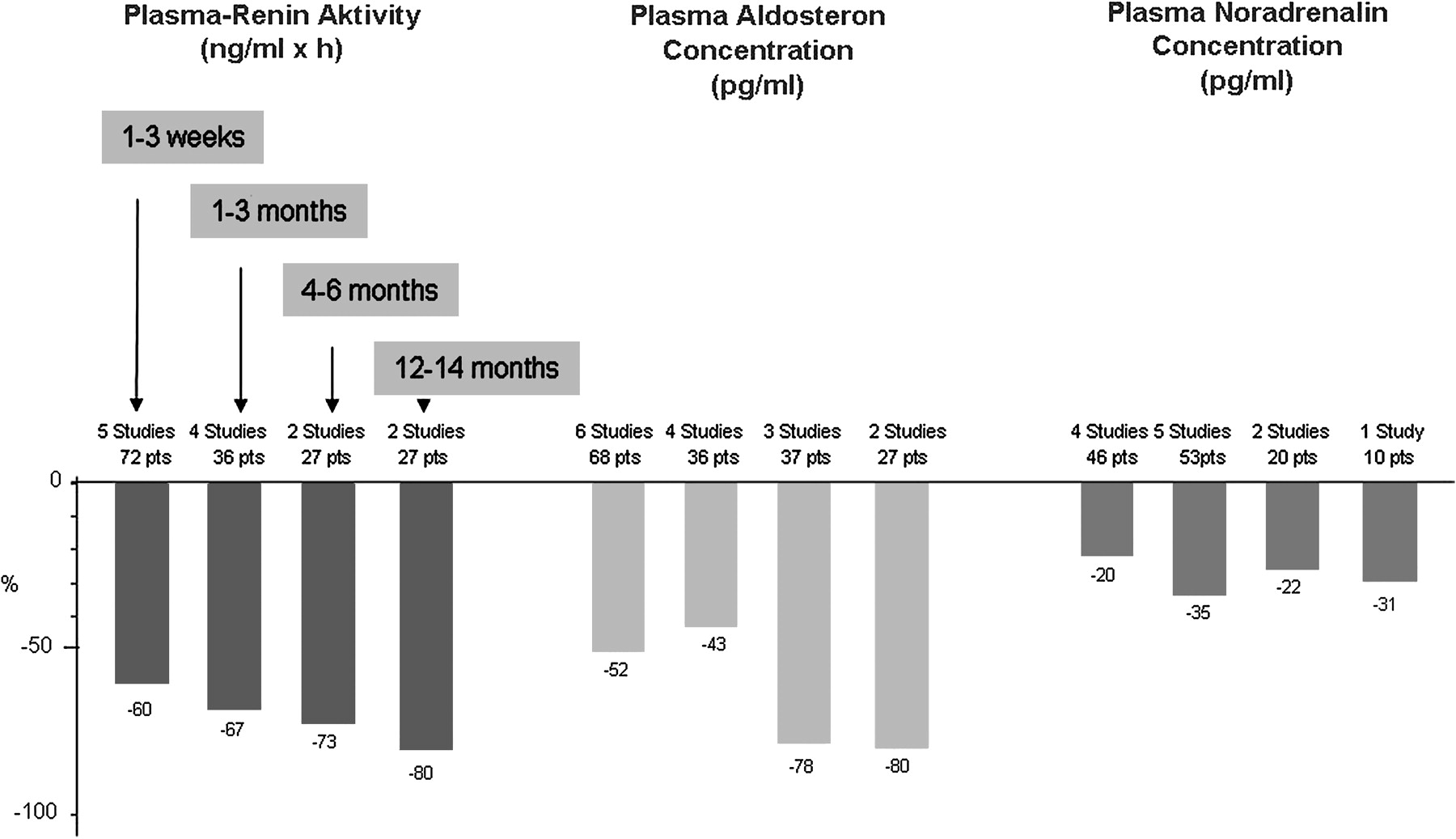
Within 4 weeks after TIPS urinary sodium excretion and serum creatinine improve significantly and, in combination with diuretics, can normalise within 6–12 months (figure 2).23–38 This is associated with a gradual increase in urinary volume and glomerular filtration rate.25 37 In addition, serum sodium concentration increases gradually.25 28 33 As shown in figure 3, the plasma renin activity, aldosteron and noradrenalin concentrations decreased significantly during 4–6 months of follow-up by 80%, 80% and 31%, respectively.25 26 28 32 33 36 37 This indicates an improvement of the circulatory dysfunction which is demonstrated in figure 4. Opening of the shunt leads to a sudden increase of the cardiac preload with an increase of the central venous pressure by 100% from an average of 5.7–11.6 mm Hg.39 40 This is accompanied by a major increase of the cardiac output from 7.8–11.5 l/min and a decrease in the total systemic vascular resistance by 35%.39

Effects of a transjugular intrahepatic portosystemic shunt (TIPS) on urinary sodium excretion and creatinine concentration. Data are extracted from 16 studies.23–38

Effects of a transjugular intrahepatic portosystemic shunt (TIPS) on systemic hemodynamics. Data are obtained from nine studies.39–45
After a few hours, the haemodynamic changes return towards pre-TIPS conditions with a mild persisting increase in the cardiac output by about 1 l/min and a decreased total vascular resistance by about 20% for the following months.39–44 As demonstrated in two studies with 12 months follow-up37 40 cardiac output and peripheral vascular resistance return to the pre-TIPS levels.
The effect of TIPS on renal haemodynamics has been investigated in six studies 28 29 32 33 37 45 showing normalisation after a follow-up of 12 months. Recently46 it was demonstrated that TIPS results in an improved renal blood flow together with an upward and leftward shift of the renal blood flow/renal perfusion pressure relationship curve which represents the renal autoregulation by the sympathetic nervous system. Accordingly, a significant reduction in norepinephrine levels was observed. It was, however, not normalised and was significantly higher than normal and similar to that in patients with diuretic-responsive ascites. The effect on the norepinephrine concentration and renal blood flow was directly related to the portosystemic pressure gradient. These results support a previous study of the same group showing that opening and occlusion of the TIPS channel exerts a rapid effect on renal blood flow.31 The authors concluded that the findings support the existence of a previously postulated hepato- or porto-renal reflex.47
With respect to the hepatic blood flow, TIPS leads to a reduction in the portal perfusion of the liver, dependent on the shunt diameter and the degree of the portal pressure reduction. In most patients a reduction of the portal pressure by about 50% results in a complete loss of the hepatic portal blood flow seen at angiography. Accordingly, duplex sonography after the TIPS commonly shows retrograde flow direction or stagnant flow in the intrahepatic portal branches indicating an abolished portal perfusion of the liver. This is counter-balanced by an immediate increase in the arterial blood flow as demonstrated by Duplex sonography48 and endoluminal flow measurements during the TIPS procedure.49 The calculated average arterial liver perfusion per minute increased from 599±100 ml/min before to 749±161 ml/min after TIPS. The effect occurred within seconds after opening the shunt and disappeared also within seconds after its balloon occlusion.
With respect to other complications related to portal hypertension a meta-analysis50 comparing TIPS with paracentesis investigated three frequent complications which occurred during the follow-up: gastrointestinal bleeding, spontaneous bacterial peritonitis (SBP) and HRS. Among patients allocated to TIPS gastrointestinal bleeding occurred in 13 subjects (8%), SBP in three (2%), and HRS in seven (4.6%), respectively. Among patients allocated to paracentesis, gastrointestinal bleeding occurred in 20 subjects (12.7%), SBP in five (3%), and HRS in 20 (12.7%), respectively. The overall rate of portal hypertension-related complications was significantly lower in the TIPS group than in the paracentesis group (23/149, 15% vs 45/156, 28%; p=0.005).
TIPS may also have a positive effect on quality of life. One study including 21 patients with refractory or recidivant ascites rated quality of life, fatigue and physical performance on a scale (range 0–100) before and 3 and 6 months after TIPS implantation.51 In addition, quality of life was determined by the QoL index (range 0–10) introduced by Spitzer. Patients' ratings on the self-assessment scale increased significantly from 35±25 to 64±28. Similarly, the Spitzer index significantly improved from 6.9±2.0 to 8.3±2.1. However, a randomised study on refractory ascites did not show a difference of quality of life between the TIPS and the paracentesis groups.52
Malnutrition and protein wasting is seen in most patients with cirrhosis and refractory ascites and has a negative effect on survival.53 54 In contrast to paracentesis, which leads to a protein loss of about 200 g per 10 litres ascites removed, TIPS improves the protein metabolism and nutrition. Three studies show a significant improvement in dry weight, total body nitrogen, total body fat and total body protein55–57 (figure 5). This is in agreement with our findings of an increase in body weight despite resolution of ascites.58 The reasons for the positive effects of TIPS on nutrition are not known. One reason may be an increase in the systemic insulin concentration bypassing now the liver. Another reason may lie in the disappearance of the ascites which may lead to an improved appetite and absorption of nutrients.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Effects of a transjugular intrahepatic portosystemic shunt (TIPS) on nutrition.56 Twenty-one patients were studied before and 6 months after TIPS. Body weight, muscle mass, body cell mass, resting energy expenditure and energy intake increased significantly while fat mass did not change significantly. In a subgroup of 16 patients followed over a 12-month period the parameters further improved (not demonstrated).
The drawbacks of TIPS are an increased incidence of hepatic encephalopathy (HE) and the negative effect on liver function. HE occurs in about 30% of patients after TIPS.59 60 Factors associated with the development of encephalopathy that can be used for patient selection are advanced age, liver or renal failure, and a history of encephalopathy before TIPS insertion.61–63 Encephalopathy usually becomes clinically apparent 2–3 weeks after TIPS insertion and then declines (as measured by the portosystemic encephalopathy index) at 6 months in bare but not in covered stents.59 60 63 Thus, shunt stenosis with time may reduce the incidence of HE.
As demonstrated in a meta-analysis of individual patient data50 the cumulative probability of developing a first episode of HE during follow-up was not different between TIPS and paracentesis groups (p=0.36 by log-rank) and a similar result was found for the development of severe HE (p=0.46 by log-rank). By contrast, when the average number of episodes-per-patient was considered, patients allocated to TIPS had significantly more episodes of HE with regard to both, total number of episodes (1.13±1.93 vs 0.63±1.18, p=0.006) and number of severe episodes (0.68±1.0 vs 0.24±0.50, p=0.008). Independent predictors of post-TIPS HE were baseline mean arterial pressure (MAP) (HR 0.93, CI 0.89–0.98; p=0.004), model of end stage liver disease (MELD) score at baseline (HR 1.068, CI 1.006 to 1.13; p=0.032), and post-TIPS porto-systemic pressure gradient (HR 0.93, CI 0.87 to 0.99; p=0.048). An explanation for the correlation of baseline MAP with HE may be that a low MAP reflects poor liver and brain perfusion together with advanced disease. This is confirmed by the finding that the increase in hepatic arterial blood flow after TIPS has a potential predictive value of postprocedural HE and mortality.64 With respect to the MELD score, the INR and bilirubin concentration reflect liver function and the creatinine concentration the haemodynamic impact of the liver disease similar to the MAP. Theoretically, the combination of bilirubin and MAP or the MELD score may both be promising predictors for HE in patients with cirrhosis with and without a TIPS. Unfortunately, the study by Salerno50 does not provide thresholds with lower or higher probabilities of HE after TIPS. However, with a mean MAP of 87 mm Hg and a mean MELD score of 12.5 values of <80 mm Hg or above 15 may be regarded as risk indicators for HE.
The TIPS diameter, which can be adjusted during the TIPS intervention, correlates inversely with the portosystemic pressure gradient after TIPS, the remaining portal liver perfusion and the liver function. In patients at risk for HE according to the parameters mentioned, a smaller shunt diameter may be less harm and should therefore be preferred.
Treatment of HE is medical in most of the cases and consists of controlling any precipitating factor, lactulose and non-absorbable antibiotics (neomycin or rifaximin).60 62 If medical therapy fails, the TIPS diameter can be reduced or the shunt occluded.65–67 In this situation one should be assured that the patient's quality of life benefits more from improving HE than it worsens by the re-accumulation of ascites. Fortunately, in a series of 1000 patients, the need for shunt reduction for debilitating HE was only 3%.68
Deterioration of liver function after TIPS is indicated by an increase of serum bilirubin concentration.42 69 Its magnitude depends on the baseline liver function. As demonstrated, a bilirubin concentration of >3 mg/dl was closely correlated with mortality (RR: 5.4, 95% CI: 1.4 to 10.2).70 The finding is confirmed by showing that an elevated pre-TIPS bilirubin is a powerful independent predictor of 30-day mortality after TIPS creation with a 40% increased risk of death for each 1 mg/dl increase above 3.0 mg/dl.71 Therefore, a bilirubin concentration above 3 mg/dl can be regarded as a relative and above 5 mg/dl as an absolute contraindication for TIPS implantation for refactory ascites.72
To prevent both deterioration of liver function and HE the shunt diameter and the degree of reduction of the portosystemic pressure gradient should be moderate. As demonstrated recently, 25 of 27 patients who developed hepatic encephalopathy after TIPS implantation had a pressure gradient of <12 mm Hg.73 Thus, in patients with a higher risk of HE and poor liver function (ie, bilirubin concentration above 3 mg/dl) the portosystemic pressure gradient should be decreased with great caution.
Technical aspects of TIPS
Complications
Although many serious complications have been reported and summarised,74 no prospective study on technical complications has been published so far. The estimated technical success rate is reported in the range of 93–100% and procedure-related mortality is very low (<1%) and mainly due to intra-abdominal bleeding.74 Technical complications comprise mispuncture of the carotid artery (2%), the hepatic artery and the bile ducts (6% each), and rupture of the liver capsule (6%).10 Clinical consequences of these technical complications are rare. Many interventional radiologists consider TIPS insertion more difficult and possibly accompanied by more complications in patients with refractory ascites. This, however, is not our experience.10 To avoid procedural problems, as much ascites as possible should be removed before TIPS. This facilitates the access to a suitable hepatic vein and improves the patient's respiratory function.
Temporary cardiac complications such as arrhythmia if the catheter enters the right atrium or right ventricle are often seen but rarely serious. In the presence of cirrhotic cardiomyopathy the haemodynamic changes upon TIPS may lead to manifest cardiac dysfunction seen in a few patients after TIPS insertion.75 Therefore an ejection fraction below 50% has been regarded as a relative and below 40% as an absolute contraindication for TIPS. Since the ejection fraction of patients with cirrhosis is usually greater than 60%76 only few patients will be precluded from TIPS. As shown recently, cardiac diastolic dysfunction may also play a role in a patient's survival after TIPS.77 In particular, a reduced E/A ratio predicted a poorer survival after TIPS.
A complication which was encountered mainly in the early 1990s is anaemia due to haemolysis. It is probably due to mechanical damage of erythrocytes when passing with a high velocity of up to 2 m/s through the wire mesh of the stent.74 The complication is now rare and limited possibly because of improved stents. This is also true for the stent migration into the right heart or lungs which is almost abandoned by the use of self-expandable nitinol stents.
As with any intravenous intervention, systemic infection or septicaemia may not be avoided completely. In the experience of the authors and based on previous studies74 antibiotics are not needed in general. They may, however, be indicated after complicated and long-lasting procedures with a great number of guide wire and catheter exchanges.
Shunt failure
Shunt insufficiency is frequent with bare stents and occurs in 50–80% during 1 year of follow-up.74 In many cases it may be due to bile duct involvement which may lead to ‘endotipsitis’ followed by intimal proliferation and thrombosis. It can be prevented by introducing covered stents and reduced by subcutaneous low molecular weight heparin for 4 weeks possibly together with trapidil and ticlopidin for 12 months.78 Our present practical approach in patients receiving bare stents is the adapted application of up to 2000 U of heparin intravenously during stent implantation followed by low molecular weight heparin subcutaneously during the index hospitalisation and a platelet aggregation inhibitor (eg, acetyl salicylic acid 100 mg/day for at least 6 months) in patients with platelet count >100 000/μl.
Shunt insufficiency does not necessarily indicate the need for shunt revision. Shunt revision is indicated in patients who fail initial response or who have recurrence of ascites. With the availability of stents covered with polytetrafluoroethylene (Goretex), long-term patency rates of 80–90% have been described.79 80
Shunt diameter, type of stent
The diameter of the shunt is crucial for effects and side effects.50 73 The decision of the individual shunt diameter ranging between 7 and 12 mm needs consideration of all aspects of the liver disease and the patient's biomedical characteristics. It should therefore be the result of a clinical judgement before the intervention. As demonstrated in patients with variceal bleeding,81 the reduction of the pressure gradient must not always reach the 12 mm Hg threshold. The same is possibly true for the treatment of ascites. As ascites formation begins within a wide range of porto-systemic pressure gradient ranging from about 12–40 mm Hg (mean of 24 mm Hg),24 the therapeutic reduction to below 12 mm Hg which is almost always efficient,73 is not always necessary.82 A smaller reduction of the gradient by about 25–50% fits better to the individual requirements and showed promising results with a 1-year response rate of 93%.82 Thus, in most patients it may be advisable to implant a 10 mm stent but dilate it to only 6–8 mm. In cases of insufficient response further dilatation can be performed.
As for the shunt diameter, the choice of the stent type is also a decision with clinical relevance which should be discussed before the intervention. In a patient with a higher risk of shunt-related complications such as age over 60 years, bilirubin around 3 mg/dl, presence of some degree of encephalopathy or with a poor prognosis, uncovered stents may be preferred because they allow spontaneous narrowing in case of worsening of liver function or HE. In contrast, patients with a low risk of complications or with Budd–Chiari syndrome may have a covered stent a priori to avoid unnecessary revisions. A randomised study including patients with varices and ascites found a better survival with the covered stent graft.83 This may, however, not apply to ascites patients who did not show a correlation between shunt failure and survival.50 In patients with Budd–Chiari syndrome covered stents can provide better results.84 85 The effects and side effects of the treatments are summarised in box 1.
Large volume paracentesis may deteriorate hyperdynamic circulation and renal function in particular when performed without adequate substitution of albumin.
TIPS corrects central vascular underfilling and improves renal function, but has a higher frequency of hepatic encephalopathy.
Side effects depend on the diameter of the shunt and on the reduction of the hepatic–venous pressure gradient which should be adjusted according to risk factors.
Covered stents may offer improved patency and yield better results in selected patients.
TIPS versus paracentesis: survival and efficacy
Survival
Five randomised studies from France,29 Germany,58 Spain/USA,86 USA/Canada,52 and Italy87 have been published which showed poorer, similar or improved survival with TIPS (table 1). Several reasons could be identified to explain these variations including differences in technical skills, patient selection and data analysis.
Two-year survival rates of randomised studies comparing transjugular intrahepatic portosystemic shunt (TIPS) and paracentesis
Table 2 summarises three technical quality parameters of the TIPS procedure: success rate of the TIPS intervention, reduction of the portosystemic pressure gradient and rate of secondary patency. The first study published in 199629 differs considerably with respect to technical success (77%), reduction in pressure gradient (6 mm Hg), and the rate of secondary TIPS patency (46%). As demonstrated by D'Amico et al88 the technical variables correspond to the ORs for mortality suggesting that technical disability was the reason for the poor outcome of TIPS in the French study.29 Therefore, the French study should be regarded as an outlier. It should be borne in mind that this was the first study, and therefore the experience with TIPS was limited.
Variables assessing technical quality of the transjugular intrahepatic portosystemic shunt (TIPS) intervention88
Second, selection of patients may have influenced the results. About 40–60% of patients screened were included in the trials with the exception of the American study52 which included only 21% of the source population.89 Selection also depends on inclusion and exclusion criteria. It can be biased due to unbalanced criteria favouring one of the two treatment arms. Thus, the use of different inclusion and exclusion thresholds for the bilirubin and creatinine concentrations may be a source of bias (table 3). Both parameters are equally important as markers for liver or kidney function. Since the TIPS may worsen liver function (but improve kidney function) and the paracentesis worsens kidney function (but has no effect on liver function) one should request similar concentrations of bilirubin and creatinine to provide equal chances for the treatment arms and to avoid a selection bias. As shown in table 3 all studies disfavoured the TIPS groups by including patients with much higher bilrubin than creatinine concentrations. The Spanish study86 allowed inclusion of patients with a bilirubin concentration as high as 10 mg/dl, which is a clear contraindication for a portosystemic shunt. On the other hand, in the American study52 inclusion and exclusion conditions selected patients with an almost normal renal function but with severe liver dysfunction, a fine condition for the paracentesis arm but a clear disadvantage for the TIPS arm.90
Inclusion and exclusion threshold values for bilirubin and creatinine concentrations
Third, survival analysis in all studies was performed according to the method described by Kaplan and Meier. However, studies differ in providing transplant-free survival. This is of particular importance when the time to transplantation differs between the groups. In the two studies providing the time to transplantation,52 87 TIPS patients had a much longer time to transplantation than did paracentesis patients. Unfortunately, the American study52 did not present a transplant-free survival analysis although this trial included the highest proportion of transplanted patients.
Four meta-analyses of these five studies88 91–93 have been published and are summarised in table 4. Surprisingly, they show different results although the calculations were done on an identical body of data.
Meta-analyses comparing transjugular intrahepatic portosystemic shunt (TIPS) with paracentesis
The first study91 lacks sophisticated statistical evaluation and calculation of heterogeneity. The second analysis92 provides relative risks which are not identical to the commonly used ORs and thus is difficult to compare. Considering survival, heterogeneity between the studies was found but authors made no effort to investigate and eliminate its source. A meta-analysis by the Cochrane Institute93 is hampered by incorporating incorrect data of the Italian publication.87 This is why their OR for survival differs from the other meta-analyses. The best meta-analysis was performed by D'Amico.88 It identified the French study as the source of heterogeneity of survival probabilities. After eliminating this study as an outlier, heterogeneity disappeared. Actuarial rates of survival were clearly different between groups favouring TIPS (POR 0.74).
Finally, the inappropriate survival analysis in the American study52 was overcome by Salerno et al50 who analysed individual patient data. Their findings with respect to survival/mortality are summarised in table 5. After excluding the French study and analysing transplant-free survival, TIPS patients were found to live significantly longer than the patients treated with paracentesis. TIPS also improved the estimated transplant-free survival in patients with MELD scores between 10 and 20 suggesting that even patients with severe disease may benefit from TIPS. In a multivariate analysis, factors predicting mortality were older age (HR 0.61, 95% CI 0.41 to 0.91, p=0.015), high bilirubin levels (HR 1.22, 95% CI 1.029 to 1.048, p=0.022), low sodium concentration (HR 0.95, 95% CI 0.92 to 0.99, p=0.03), and TIPS (HR 0.61, 95% CI 0.41 to 0.91, p=0.015).
Transplant-free 1- and 2-year survival probabilities and estimated 12-month mortality according to various MELD scores after TIPS or paracentesis treatment
Treatment efficacy
A recent analysis of the literature on TIPS for refractory ascites including 16 studies showed a complete response in 51%, complete and partial response not requiring paracenteses in 68% of the patients.94 The five randomised studies discussed before29 52 58 86 87 show a mean response to TIPS in 76% of patients. As shown in the meta-analysis by Salerno50 recurrence of tense ascites occurred in 42% of patients allocated to TIPS and 89% of patients allocated to paracentesis (p<0.0001). Recurrence is mostly due to shunt insufficiency and can be effectively treated by TIPS revision. Accordingly, the average number of paracenteses-per-patient was significantly lower in patients allocated to TIPS (1.6±3.5 vs 7.1±8.8; p<0.0001) whereas allocation to paracentesis resulted in an independent association to recurrence of ascites (OR 11.67, 95% CI 6.2 to 21.9).
Treatment of hepatorenal syndrome
The definition of HRS was elaborated in 19961 and updated in 2007.4 Accordingly, type 1 HRS is a rapidly progressive disease defined by doubling of initial serum creatinine concentrations to a level greater than 226 mmol/l (2.5 mg/dl) in less than 2 weeks. HRS type 1 usually occurs within the setting of an acute deterioration of circulatory function characterised by arterial hypotension and activation of endogenous vasoconstrictor systems. Hospital mortality is as high as 90%. Type 2 HRS is characterised by moderate renal failure with serum creatinine concentrations between 1.5 mg/dl and 2.5 mg/dl with a steady or slowly progressive course. It appears spontaneously, but can also follow a precipitating event and is typically associated with refractory ascites. Treatment of HRS has changed in the recent years considerably. Specific pharamological therapy includes plasma expansion using albumin and vasoconstrictors such as terlipressin.
Vasoconstrictor therapy
Terlipressin in combination with albumin is the most widely studied pharmacological treatment for patients with type 1 HRS. Complete response occurs in approximately 40% of patients treated for a maximum of 15 days with terlipressin and albumin and is associated with improved survival.4 95
TIPS
Numerous studies in patients with refractory ascites including the five randomised studies show that TIPS improves renal function and haemodynamic variables. Even patients with cirrhosis and parenchymal kidney disease may benefit from TIPS.35 Many patients with HRS type 1, however, suffer from advanced hepatocellular insufficiency with serum bilirubin exceeding 5 mg/dl, a clear contraindication for TIPS. However, mortality after liver transplantation is higher in patients transplanted with HRS than in those without HRS.96This may argue in favour for TIPS in transplantation candidates. A recent study confirms this contention.97 It showed that TIPS improves post-transplant graft and patient survival significantly possibly due to an improved pre-transplant renal function and portal blood supply of the graft.
Only a few studies have assessed the role of TIPS for the treatment of HRS in a total of 61 patients.33 36 38 98 Brensing et al36 treated 31 non-transplantable patients (14 type 1 and 17 type 2) and found that renal function improved following TIPS. One- and 2-year survival rates were 20% for type 1 and 70% and 45%, respectively, for type 2 HRS. However, due to a bilirubin cut-off of 10 mg/dl, nine patients had to be excluded from TIPS. Liver failure was one of the most frequent causes of death following TIPS. Guevara et al33 reported on seven patients with type 1 HRS showing a significant improvement in serum creatinine, blood urea nitrogen, glomerular filtration rate and renal plasma flow by TIPS. Three patients survived by more than 3 months. As shown by Wong et al98 TIPS may also have a role in maintaining patients who initially respond to vasoconstrictor treatment. Fourteen patients with type 1 HRS were treated using a combination of midodrine, octreotide and albumin. Medical therapy for 14 days improved renal function in 10/14 patients with mean serum creatinine significantly decreasing from 233 μmol/l to 112 μmol/l. Five responders were then treated with TIPS and showed further improvement in renal function (mean glomerular filtration rate: 96±20 ml/min at 12 months). Testino et al38 reported the effects of TIPS in 18 patients with type 2 HRS and a Child–Pugh score of 10–12 awaiting transplantation. All patients improved with respect to ascites and renal function.
These beneficial effects of TIPS on renal function are difficult to reconcile with the findings by Malinchoc et al99 who observed a (negative) correlation between the creatinine concentration before TIPS and survival after TIPS, a fact which was well recognised in the MELD scoring system. Accordingly, an elevated creatinine concentration should be a negative predictive factor for the survival after TIPS. However, numerous studies24 58 including the meta-analysis by Salerno,50 failed to show a correlation between the pre-TIPS creatinine concentration and post-TIPS survival. The positive effect of TIPS on renal function explains that the MELD score underestimates survival following TIPS for refractory ascites.100
In summary, TIPS can improve renal function in type 1 and 2 HRS and eliminate ascites. However, the data are limited and survival may not be improved in patients with poor liver function. Thus, TIPS is indicated in selected patients with HRS and/or in candidates for liver transplantation.
Treatment of hepatic hydrothorax
Hepatic hydrothorax occurs in approximately 5% of patients with advanced cirrhosis. It is defined as the presence of pleural fluid (usually greater than 500 ml) without the presence of primary cardiac or pulmonary disease.5 It is mostly right-sided (85%), combined with ascites, and due to direct passage of peritoneal fluid via diaphragmatic leaks. The treatment modalities for hepatic hydrothorax consist of medical therapy, repeated pleuracenteses, pleurodesis, permanent chest tube, surgical repair of the diaphragmatic leak, peritoneo-venous shunts, and TIPS.5 101
TIPS for hepatic hydrothorax has been investigated in seven non-controlled studies102–108 and several case reports. The results of studies including at least 10 patients are summarised in table 6. Overall, 198 patients (predominantly Child–Pugh B and C) were included. The mean complete and partial (not requiring thoracenteses) response rates were 65% and 15%, respectively. Thus, an overall clinically relevant response was found in about 70% of patients. The average 30-day mortality rate was around 20%. The 1-year survival, given in two studies,105 108 was 64% and 48%, respectively. Survival was correlated with response, age <60–65 years, and the MELD score.
Transjugular intrahepatic portosystemic shunt (TIPS) for the treatment of hepatic hydrothorax
These studies are uncontrolled and most of them are retrospective. Since patients with refractory hydrothorax are relatively rare, a randomised comparison with other treatment options may not be feasible. Repeated thoracenteses are probably not an acceptable alternative if required frequently.109 Pleurodesis is rarely helpful due to rapid re-accumulation of the pleural effusion and to side effects. Results of pleurodesis may be improved by the addition of continuous positive airway pressure which may keep the pleural space dry.110 However, data are limited to case reports. According to a recent report using a permanent chest tube in 17 patients with hepatic hydrothorax, this treatment should be disregarded.111 Sixteen of the 17 patients had severe complications including acute kidney injury (11 patients), pneumothorax (seven patients) and empyema (five patients). Six patients (35%) died within 3 months while six of seven patients who received a TIPS for hepatic hydrothorax survived. Finally, the video-assisted thoracoscopy (VATS) for repair of the diaphragmatic leak with or without additional pleurodesis may be an alternative to the TIPS treatment. However, the overall success rate was only 48% and mortality was 40% within 40 days of follow-up.112
In summary, compared with other treatment options, TIPS seems to provide a high rate of response and rather good long-term survival. In addition, TIPS is the only treatment option which also treats the refractory ascites, the source of the hepatic hydrothorax.
Conclusions
TIPS seems to be the treatment of choice for patients with ascites requiring repeated and frequent paracenteses. To reduce shunt-related complications such as deterioration of liver function and hepatic encephalopathy, patients should be selected according to hepatic function (bilirubin <3 mg/dl). In patients not fulfilling these criteria TIPS may be justified when it is considered vital because of the severity of the symptoms or when liver transplantation is scheduled.
TIPS may also be the treatment of choice in patients with refractory ascites accompanied by HRS type 2. As demonstrated in numerous studies, normalisation of renal function can often be achieved. In accordance with the guidelines of the International Ascites Club,4 TIPS can not be recommended for patients with HRS type 1 due to lack of sufficient data. In many patients with type 1 HRS TIPS is contraindicated because of the concurrence of severe hepatic failure. However, TIPS may be used after vasoconstrictor therapy to stabilise renal function and possibly improve the outcome of liver transplantation.
Numerous studies unanimously recommend TIPS for the treatment of hepatic hydrothorax. However, due to the lack of comparative trials the recommendations are of minor evidence suggesting that treatment should better be based on individual needs and local facilities.
Most patients with refractory ascites, HRS or hydrothorax have advanced liver disease with a higher risk of TIPS-induced complications. Therefore, the diameter of the stent-shunt which determines the reduction of the portosystemic pressure gradient, should be chosen carefully. The same is true for the type of stent which may be uncovered in patients at higher risk and covered in those with a lower risk of shunt-related complications. A stepwise enlargement of the stent diameter may help to prevent complications. Liver transplantation should be discussed for patients with severe complications of cirrhosis such as massive ascites, HRS or hepatic hydrothorax. The place of TIPS in the treatment of refractory ascites and its limitations are summarised in box 2.
TIPS improves survival in well selected patients with ascites requiring repeated and frequent paracenteses.
Patients with a bilirubin concentration <3 mg/dl, an age <65 years and no history of hepatic encephalopathy benefit most from TIPS.
TIPS may be useful as a bridge to transplantation in selected patients with HRS.
Several uncontrolled studies recommend TIPS for the treatment of hepatic hydrothorax.
References
Footnotes
Competing interests None.
Provenance and peer review Commissioned; externally peer reviewed.