Article Text

Statistics from Altmetric.com
H pylori and the acid pump
H pylori infection causes gastritis and transient hypochlorhydria, which may progress after decades to a gastric cancer phenotype. CagA positive strains increase cancer risk but their effect on acid secretion is poorly understood. Acid secretion is mediated by the catalytic α subunit of parietal cell H, K-ATPase (HKa). Saha et al sought to identify bacterial genes involved in HKa repression and to assess their impact on acid secretion. AGS cells transfected with an HKa promoter construct or human gastric body biopsies were infected with wild-type (wt) or isogenic mutant (IM) strains. AGS cell HKa promoter activity, and biopsy HKa mRNA, protein and H+ secretory activity were measured. The authors showed that the H pylori cag PAI genes cagL, cagM and cagE are implicated in repression of HKa transcription following acute infection, and that this repression is reflected in markedly diminished HKa translation and ensuing H, K-ATPase activity in H pylori-infected gastric biopsies (see figure 1figure 1). The study demonstrates a novel model that allows controlled exposure of human gastric mucosa to different H pylori strains and refined pharmacological interventions to dissect the affected cellular signalling pathways. See page 874.

H pylori represses H, K-ATPase a subunit (HKa) levels in human gastric biopsies. Open bars represent mock-infected biopsies, and shaded bars represent patient-matched infected biopsies.
Gata4 deletion in mice induces bile acid absorption in the proximal small intestine
Resection of the terminal ileum often results in bile acid malabsorption due to loss of the ileal-specific bile acid transporter (ASBT) and therapeutic options are limited. In this study, the authors hypothesised that reduction of GATA4 activity, a transcription factor expressed in the small intestine except in the distal ileum, restricting expression of the ASBT transporter results in an induction of bile acid transport in the proximal small intestine which in turn could be sufficient to restore bile acid absorption and homeostasis after ileocaecal resection. Their experiments in mice show that a reduction of intestinal GATA4 activity results in an induction of ASBT expression, bile acid absorption, and expression of bile acid-responsive genes in the proximal small intestine, and a reduction of luminal bile acids in the terminal ileum. Proximal induction of Asbt in Gata4 mutant mice corrected this bile acid malabsorption. They conclude that reduction of intestinal GATA4 activity induces bile acid absorption in proximal small intestine which in turn would be sufficient to correct bile acid malabsorption caused by ileocaecal resection. See page 888.

Bile acid pool size, as determined by the total bile acid content in liver, gall bladder and small intestine, is lower in Wt-control mice that underwent ileocaecal resection as compared to sham-operated mice. Bile acid pool size in G4Δex2 and G4ap mice that underwent ICR remained similar to the sham-operated mice.
Partial inhibition of the proteasome by bortezomib or deletion of the immunosubunit LMP7 attenuates experimental colitis
Inflammatory bowel disease is characterised by chronic relapsing inflammation of the gut. Increased proteasome activity, associated with the expression of immunoproteasomes, enhances pro-inflammatory signalling and thus promotes inflammation in IBD patients. In this study, the authors explored if modulation of the proteasomal activity may be a suitable therapeutic approach. They induced DSS colitis in lmp7-/- mice lacking the immunoproteasome-subunit LMP7 and in wildtype mice (WT) treated with the proteasome inhibitor bortezomib. They found that compared to WT mice, lmp7-/- mice developped significantly attenuated colitis. Treatment with bortezomib revealed furthermore a dose-dependent amelioration of DSS-induced inflammation. The secretion of proinflammatory cytokines and chemokines was reduced and neutrophil infiltration as well as expansion of Th1 and Th17 T cells were diminished. They conclude that reduction of the proteasome activity either by partial inhibition with bortezomib or by specifically targeting the immunoproteasome-subunit LMP7 is a suitable therapy of intestinal inflammation. See page 896.

Flow cytometric analysis of the frequency of Th1 T cells (CD4+IFNg +) (A) or Th17 (CD4+ IL-17+) (C) cells in LPMCs shows reduced numbers of Th17 and Th1 T cells in DSS-treated lmp7-/- mice.
Tumour biology and survival in colon cancer
The immune system plays an important role in colorectal cancer development and progression and predicting survival based on markers of tumour biology is becoming a reality. In this study, Simpson et al studied expression of intra-tumoural T cells (ITTC), interferon-γ receptor (IFNGR1) and nSTAT-1 in a large, well-characterised cohort of CRC patients. They showed that expression of these markers was correlated with MHC-1 expression, survival and standard clinico-pathological criteria. The presence of high ITTC correlated with an improved survival compared to low ITTC with a mean survival difference of 16.3 months. Patients whose tumours had high ITTC and nSTAT1 survived 20 months longer than patients whose tumours had low ITTC and no nSTAT1. A mean survival advantage of 26.1 months was seen in patients whose tumours had strong MHC-1 expression and high ITTC over those who had weak MHC-1 and low ITTC. They conclude that patients with ITTC, nSTAT1 and strong MHC-1 tumour expression (all markers of an intact tumour immune system) have improved survival and may benefit from immunotherapy, whereas loss of these markers identifies patients whose tumours have escaped immunosurveillance and are unlikely to benefit from immunotherapy. See page 926.

Kaplan Meier graph showing the difference in survival probability between patients whose tumours have a) low (≤15 cell/mm2) and high (>15 cell/mm2) intra-tumoral T cell (ITCC); p=0.006. b) have sparse, moderate or dense stromal T cell infiltration p=0.167.
Fatty liver can be dangerous
Nonalcoholic fatty liver disease (NAFLD) presumably is the most frequent liver disorder. Fatty liver with inflammation (NASH) is a risk factor for cirrhosis and hepatocellular carcinoma. Thus, a key issue in hepatology is whether simple steatosis without inflammation may also progress to severe liver injury as has recently been suggested for children in this journal (Gut 2009;58:1538–1544). The present prospective study from Hong Kong provides important novel information. Using protocol biopsies at 3 years interval they found disease progression towards NASH in half of the patients with simple steatosis. Reduction of body mass index was a good predictor of stable NAFLD. As important clinical consequences patients with simple steatosis should be followed-up and moderate weight reduction seems to prevent progression towards NASH. See page 969.
Quantitative liver function tests revisited
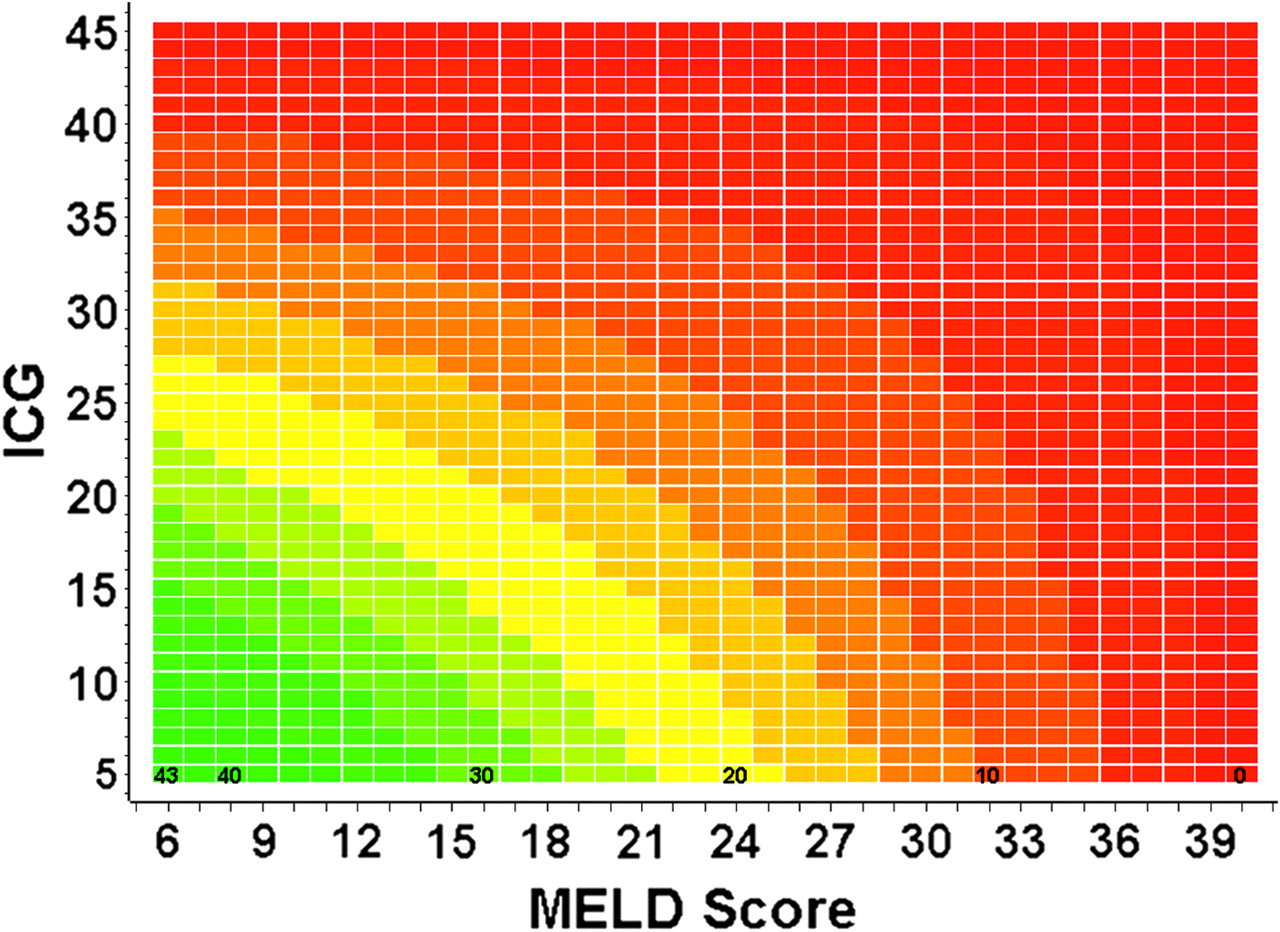
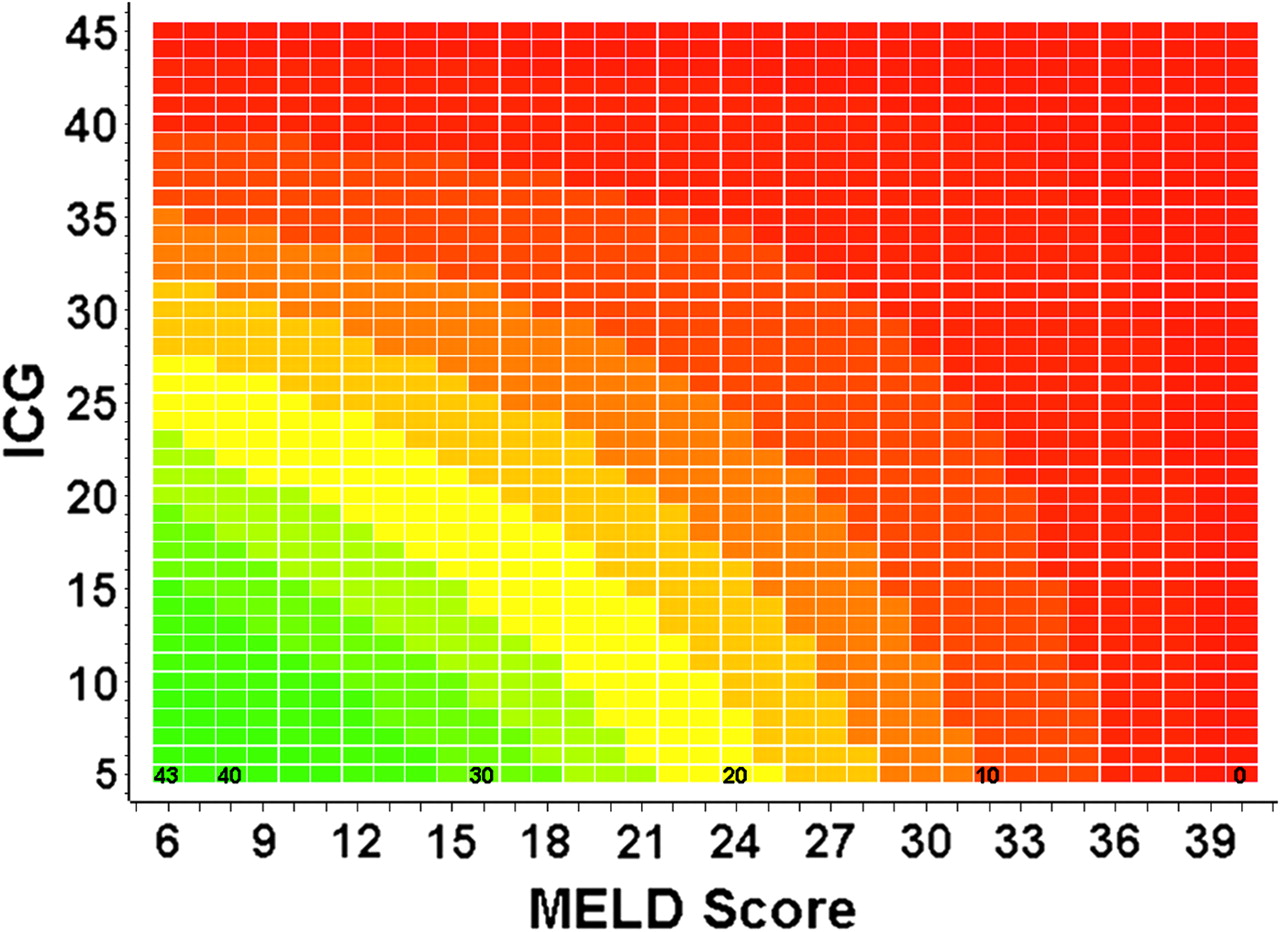
The heyday of quantitative liver function tests was quite a while ago. Nowadays simple non-invasive scores such as the MELD score are generally used to assess the severity of liver disease and to predict short-term survival. These scores, however are far from being perfect and modifications such as the MELD-Na, incorporating serum sodium have been suggested. This careful and thorough study from Halle compared the prognostic accuracy of MELD and Pugh scores, hepatic-venous pressure gradient and four different liver function tests in 395 patients with cirrhosis, 74 of whom had a TIPS inserted during the same hospital stay. ICG clearance, reflecting liver blood flow turned out superior to the other liver function tests in predicting one year survival. A newly constructed MELD-ICG was slightly superior to MELD and MELD-Na, respectively, particularly in patients with a MELD score between 10 and 30 and in patients undergoing TIPS. Now the score shall be prospectively evaluated in a large trial using a new non-invasive technique to assess ICG (see figure 5). See page 963.
{kind=link}
Modification of MELD score by ICG.
Linked Articles
- Inflammatory bowel disease
- Hepatology
- Hepatology
- Small bowel
- Helicobacter pylori
- Colon