Article Text

Statistics from Altmetric.com
Host genetics and IBS
Irritable bowel syndrome (IBS) is the most common gastrointestinal disorder but its aetiology remains poorly understood. A genetic link in IBS is supported by familial clustering and a higher incidence in monozygotic twins. In this issue of Gut, Zucchelli et al examined the hypothesis that genes contributing to epithelial barrier integrity, control of mucosal immune responses and interactions with bacteria in the gut are associated with IBS. They tested 30 known susceptibility loci for Crohn's disease in 1992 individuals from two independent case-control cohorts from Sweden and the USA. The Crohn's disease risk allele rs4263839 G in the TNFSF15 gene was significantly associated with an increased risk of both IBS (p=2.2310−5; OR 1.37) and more markedly, constipation predominant IBS (p=8.7310−7; OR 1.79). Furthermore, the polymorphism was shown to be functional with the G allele correlating with higher TNFSF15 mRNA expression in blood and rectal mucosal of healthy individuals (see figure 1). This gene is involved in the regulation of immune and inflammatory responses supporting a role for these pathways in the pathogenesis of IBS. The findings of this study might ultimately lead to improved prognostic and therapeutic strategies (see page 1671).

Association between rs4263839 genotype and TNFSF15 mRNA expression in peripheral blood leucocytes and rectal mucosal biopsies from healthy individuals.
Maternal health and colon cancer
Epidemiological data and animal studies support a protective role for dietary folate and related B vitamins against colorectal cancer, however, recent randomised controlled trials have demonstrated a tumour promoting effect of folate. This paradox may be related to the timing and duration of the exposure. In this issue of Gut, two groups of investigators have assessed the effect of maternal exposure of folate and B-vitamins, respectively, on colon cancer risk. Maternal diet and environmental exposure are becoming increasingly recognised as important determinants of the risk for chronic disease in offspring. In addition to its established role in preventing birth defects, maternal folate supplementation appears to be protective against several paediatric cancers. Ciappio et al found that maternal supplementation with vitamins B2, B6, B12 and folate markedly suppresses intestinal tumourigenesis in mouse offspring (OR 0.18; 95% CI 0.0519 to 0.6308; p=0.009) (see figure 2). Of interest, they found exceedingly mild maternal B vitamin inadequacy increases the likelihood of tumours in offspring acquiring an invasive phenotype. Moreover, Sie et al report that maternal, but not post-weaning, folic acid supplementation at the level equivalent to the average post-fortification total folate intake in North America and to that recommended to women at reproductive age significantly reduced the odds of colorectal cancer by 64% in the offspring (OR 0.36; 95% CI 0.18 to 0.71; p1/40.003). These data indicate that maternal B vitamin and folate supplementation may not only protect offspring against birth defects but also against colorectal cancer in adulthood (see page 1687 and 1695).

Periconceptional maternal B vitamin supplementation suppresses tumour occurrence, while depletion promotes tumour invasiveness in the small intestine of Apc1638N offspring. (A) Tumour incidence (percentage of mice with tumours). (B) Tumour grade (number of tumours per mouse) in 8-month-old Apc1638N mice. Groups with different letters are significantly different (p<0.05). Maternal diets, CTRL, control; VBD, vitamin B deficient; VBS, vitamin B supplemented. N1/445, 27 and 24 mice/group respectively (from 9 to 15 l). WT, wild-type.
More evidence for a connection between diabetes and colon cancer
Epidemiological studies have implicated type 2 diabetes (T2D) as a risk factor for colorectal cancer. In addition, genetic association studies have identified genetic risk variants for colorectal cancer. Previous genetic association studies of colorectal cancer have examined a few of the T2D risk variants for their impact on colorectal cancer but mostly in small study populations. Le Marchand's research team has found in examining 19 established T2D risk variants in a large case control study of colorectal cancer nested in a Multiethnic Cohort study that genetic variants for T2D that also impact the risk of colorectal cancer. Since similar patterns of associations were observed with adjustment for diabetes status and body mass index suggesting the underlying effects of these T2D risk variants may operate through pathways separate from those for diabetes. Importantly, if these variants are confirmed to be associated with colorectal cancer, they could be used to improve risk prediction models and, ultimately, personalise indications for colorectal cancer screening (see page 1703).
Hepatology
Vitamin D inhibits liver fibrosis
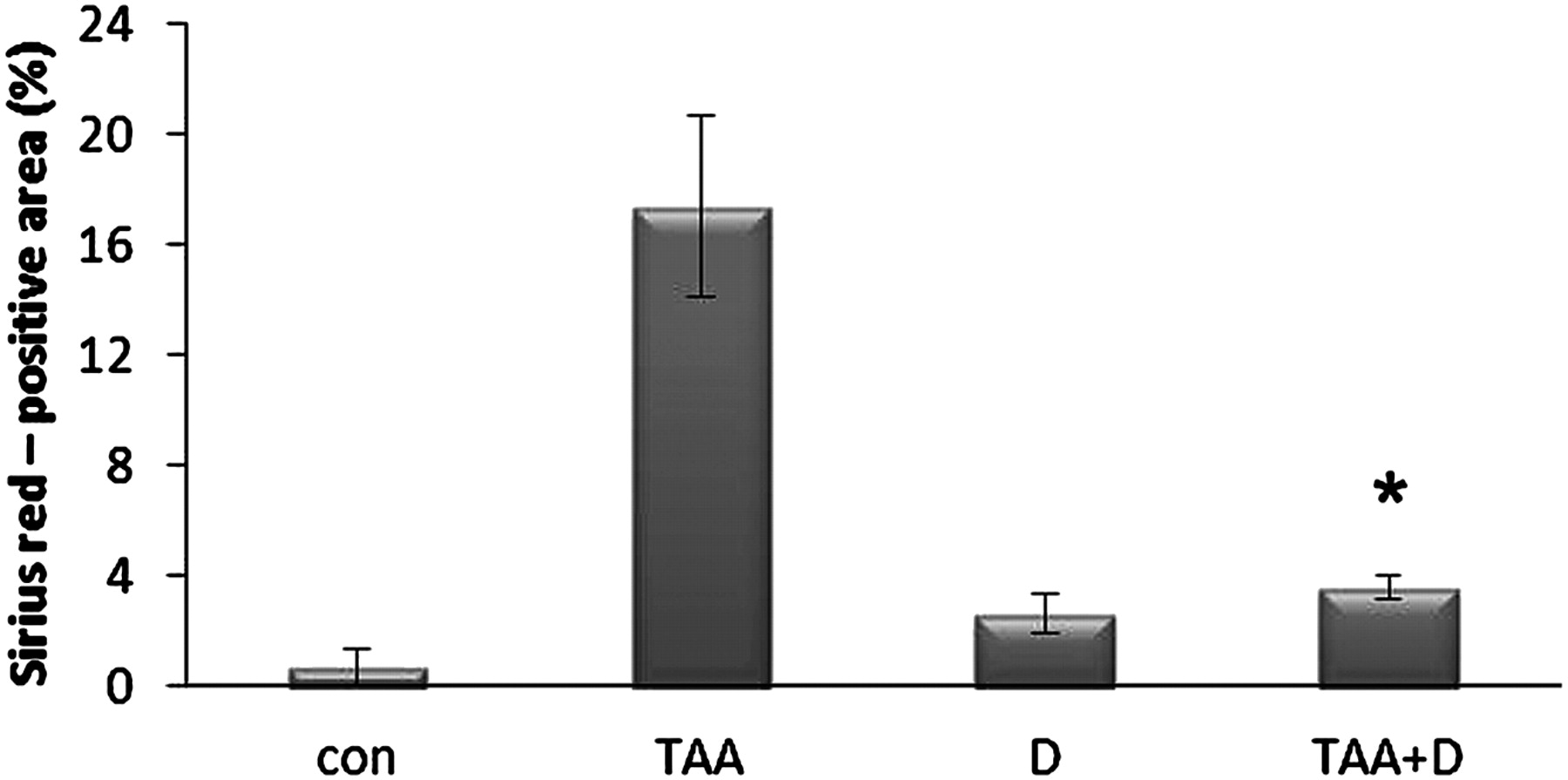
Liver fibrosis remains a great clinical challenge with few treatments available. Proliferation of hepatic stellate cells and activation of profibrogenic pathways are the key players and consequently prime targets for prevention of fibrosis. Vitamin D deficiency has been associated with advanced fibrosis. This interesting investigation from Israel found marked antifibrotic and antiproliferative effects of vitamin D in cultures of rat stellate cells. Moreover, fibrosis was attenuated by vitamin D in an in-vivo model (see figure 3). Thus, vitamin D administration may represent an interesting strategy to prevent progression of fibrosis (see page 1728).
{kind=link}
{kind=link}
{kind=link}
Vitamin D inhibits collagen deposition in rats with TAA induced fibrosis. *p<0.05 versus TGF-β.
Nonalcoholic fatty liver is a risk factor for coronary heart disease, but not a predictor of outcome
Nonalcoholic fatty liver disease (NAFLD) is presumably the most common liver disease. NAFLD is characterised by an increase of proinflammatory cytokines and by insulin resistance and often accompanied by diabetes and the metabolic syndrome. This large, prospective study from Hong Kong found that fatty liver, diagnosed by simple ultrasound, was a risk factor for coronary heart disease independent of other demographic or metabolic factors (see table 1). However, in patients with coronary heart disease NAFLD was not predictive of cardiovascular death, myocardial infarction or the need for further coronary intervention. Still, in patients with NAFLD the presence of coronary heart disease should always be considered (see page 1721).
| Factors | Univariate analysis | Multivariate analysis | ||
| OR (95% CI) | p Value | OR (95% CI) | p Value | |
| Fatty liver | 3.07 (2.09 to 4.51) | <0.001 | 2.31 (1.46 to 3.64) | <0.001 |
| Age (years) | 1.03 (1.02 to 1.05) | <0.001 | 1.05 (1.03 to 1.07) | <0.001 |
| Male gender | 2.44 (1.66 to 3.60) | <0.001 | 2.60 (1.65 to 4.09) | <0.001 |
Coronary heart disease is clearly associated with fatty liver
Linked Articles
- Colon
- Neurogastroenterology
- Hepatology
- Colon
- Colon
- Hepatology