Article Text

Statistics from Altmetric.com
Luminal GI
IBD among US Women: a north versus south divide
Geographical variation according to latitude of residence in the incidence of Crohn's disease (CD) and ulcerative colitis (UC) has been reported in Europe with higher rates for northern countries. There are no comparable data for US and no clear data in relation to risk of CD or UC using time points with more plausible biological latency. Khalili et al provide data based on a geographically diverse population of women enrolled in two large prospective studies in the USA: the Nurses’ Health Study I (NHS) in 1976 and the NHS II in 1989. Information on state of residence at the time of birth, at age 15 years and age 30 years was collected in 1992 in NHS I and in 1993 in NHS II. Reported diagnoses of incident CD or UC to the end of 2003 were confirmed by medical record review. The incidence of CD and UC increased significantly with increasing latitude (p trend <0.01), with residence at age 30 years more strongly associated with risk. Compared with women residing in northern latitudes at age 30, the multivariate adjusted HR for women residing in southern latitudes was 0.48 (95% CI 0.30 to 0.77) for CD and 0.62 (95% CI 0.42 to 0.90) for UC. These interesting data support the importance of biological pathways that mediate these geographical differences in the pathogenesis of IBD and stress the importance of understanding such pathways as a means of modulating risk of incident disease. (see page 1686).
Secukinumab is ineffective for Crohn’s disease
Data from animal models of IBD suggest involvement of interleukin (IL)-17 in CD pathogenesis, and overexpression of IL-17 was observed in intestinal tissue from patients with active CD. Genetic studies found a strong association of IL-23R with susceptibility to CD, thus implicating the IL-23-IL-17 axis in disease pathogenesis. Secukinumab (AIN457), a fully human selective anti-IL-17A monoclonal antibody, has completed phase II trials in psoriasis and rheumatoid arthritis and was found to be safe and efficacious in these patient populations. Hueber et al report the results of a multicentre, double-blind, randomised, placebo-controlled proof-of-concept study involving 59 patients with moderate to severe CD. Patients were assigned in a 2 : 1 ratio to 2×10 mg/kg intravenous secukinumab or placebo. The primary end point was the probability that secukinumab reduces the CDAI by ≥50 points more than placebo at week 6. The results showed that blockade of interleukin-17A was ineffective and was associated with higher rates of adverse events compared with placebo (table 1). This is an important negative study and calls for a better understanding of the inflammatory pathways that underlie CD. (see page 1693).
Primary end point (Bayesian analysis including historical controls)
Insights into a new way to prevent or treat colorectal cancer
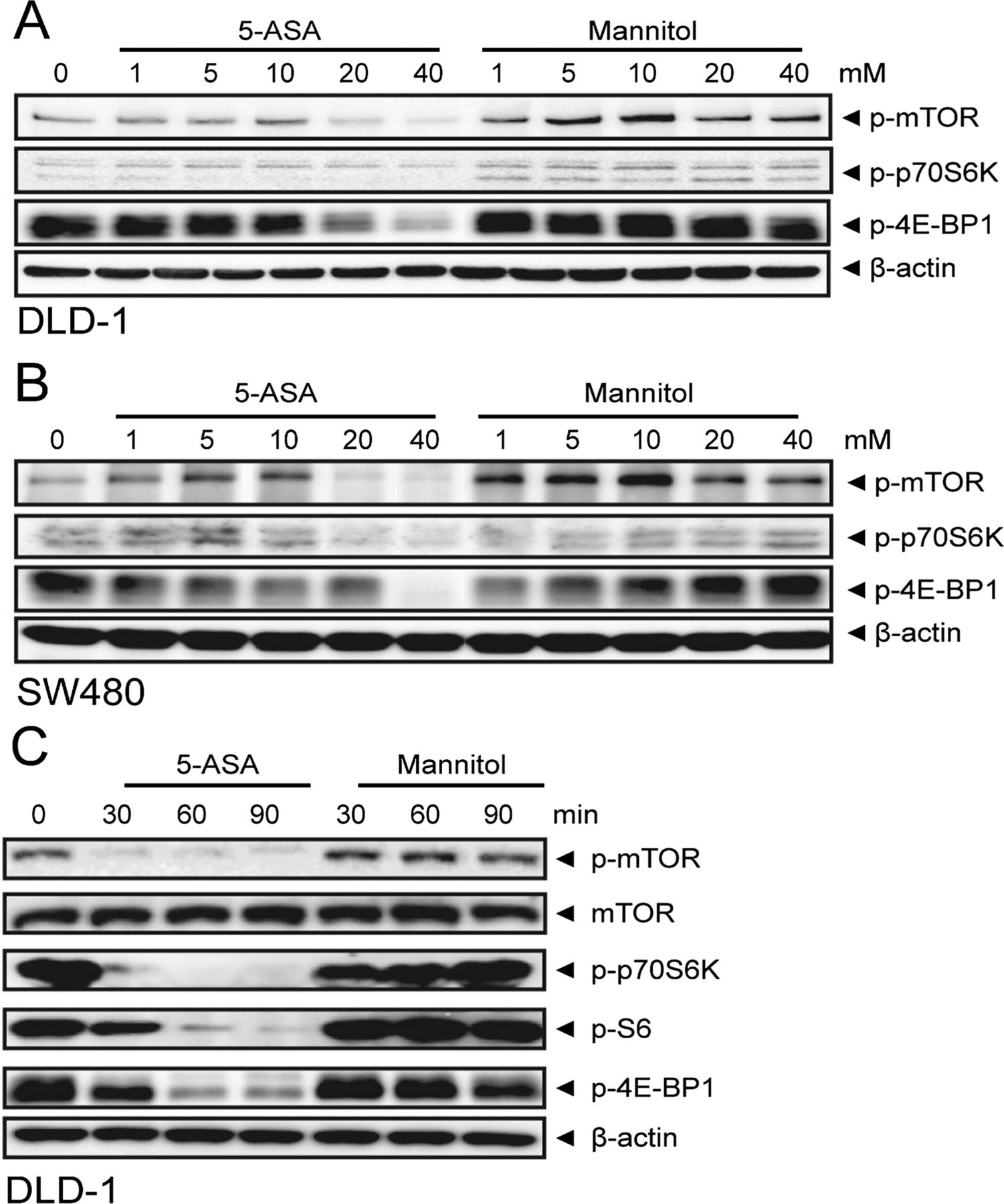
It is well known that inflammatory bowel disease is associated with an increased risk of colon cancer due to chronic inflammation in the colon. The risk of colorectal cancer associated with IBD has decreased recently presumably because of the use of anti-inflammatory medications like 5-aminosalicylic acid (5-ASA). 5-ASA may protect against the development of inflammation associated colorectal cancer, but the molecular mechanism leading to this anti-cancer effect remains to be determined. Baan and colleagues now show that treatment of colorectal cancer with 5-ASA inhibits the mTOR signalling pathway, a key oncogenic pathway in colorectal cancer cells (figure 1). Furthermore, they showed that cancer cell proliferation and mTOR activity depended on PLD, an enzyme that generates phosphatidic acid. Their findings open the door to new treatment options for colorectal cancer. (see page 1708).
5-Aminosalicylic acid (5-ASA) inhibits mTOR signalling in vivo. (A) Immunohistochemistry for phospho-mTOR in two representative colorectal carcinomas before and after a 14 day treatment with 5-ASA enemas. (B) Phospho-mTOR staining intensity for all individual patients (*p<0.05 in Mann Whitney test). (C) Immunohistochemistry for phospho-S6 in two representative patients before and after 5-ASA treatment.
The right time to do a virtual colonoscopy
It is well known that patients presenting with colorectal cancer have a risk of having a second proximal primary cancer or advanced adenoma. However, on occasion the presenting distal cancer can be near-obstructing and can prevent endoscopic evaluation of the proximal colon. This clinical situation led Park and colleagues to study the utility of CT colonography (CTC) for assessing the proximal colon in patients with near-obstructing colon cancer. They definitively studied 248 patients who underwent CTC for proximal colonic evaluation after failed colonoscopy because of a newly diagnosed stenosing colorectal cancer. Impressively, they found that the per-patient and per-lesion CTC detection sensitivities for proximal synchronous cancers were 100% with the corresponding per-patient negative predictive value (NPV) of a negative CTC of 100%. They also found that the per-patient NPV of a negative CTC for advanced adenoma and adenocarcinoma was 97.4% and that the per-lesion positive predictive value was 80%. So, CTC appears to be highly sensitive in detecting synchronous cancers proximal to near-obstructing colorectal cancer, which will help ensure the patient gets the best surgical treatment when he/she goes to the operating room (figure 2). (see page 1716).

Patient with a stenosing cancer in the rectum and a 15-mm synchronous cancer with submucosal invasion in the ascending colon. A. Three-dimensional endoluminal view of CTC, showing a 17-mm plaque-shaped sessile lesion with mild surface undulation (arrowheads).
Hepatology
Role of lymphocytes for formation and progression of hepatocellular carcinoma
Hepatocellular carcinoma (HCC) is a typical inflammation-associated cancer. Therefore the role of anti-tumoral immune responses is of great interest but as yet not fully understood. This interesting study from Germany (page 1733) functionally characterised immune responses in the DEN mouse model and also in human HCC. HCC induction was accompanied by hepatic leukocyte infiltration and upregulation of intrahepatic chemokines related to macrophages and to T cells, respectively. These tumour-associated immune responses were further investigated using several knock-out mouse lines. The authors found evidence that T cells prevent initial tumour formation whereas B cells limit HCC growth. Interestingly, T and B cell pathways were differentially regulated in human HCC and associated with patient survival probability (figure 3A,B). Thus, augmentation of anti-tumour adaptive immune cell functions may be an interesting therapeutic approach for HCC.

{kind=link}
{kind=link}
{kind=link}
Cluster analysis of 139 human HCC samples based on genes relevant to T cell (A) or B cell receptor signalling (B) defined two subgroups with different survival probability.