Article Text

Abstract
Introduction There is growing evidence for the efficacy and safety for the insertion of self expanding metal stents (SEMS) in the treatment of acute malignant colonic obstruction.1 This allows either palliation or a bridge to surgery in an otherwise acutely unwell patient. Colonic stenting literature quotes technical success rates in excess of 85%.1–4 Our unit has been inserting colonic SEMS since 2006. Prior to this we had extensive experience in therapeutic endoscopy but not in colonic stenting. We have observed a learning curve with colonic stenting that is encouraging for endoscopists who are considering implementing the technique.
Methods All SEMS insertions from July 2006 to December 2011 were analysed retrospectively by examining a combination of endoscopy reports, the CRC database and patient notes. A successful SEMS deployment was defined as: satisfactory radiological and endoscopic evidence of colonic decompression at time of deployment and clinical improvement. All SEMS insertion successes and failures were collated and the data compared in consecutive groups of ten procedures.
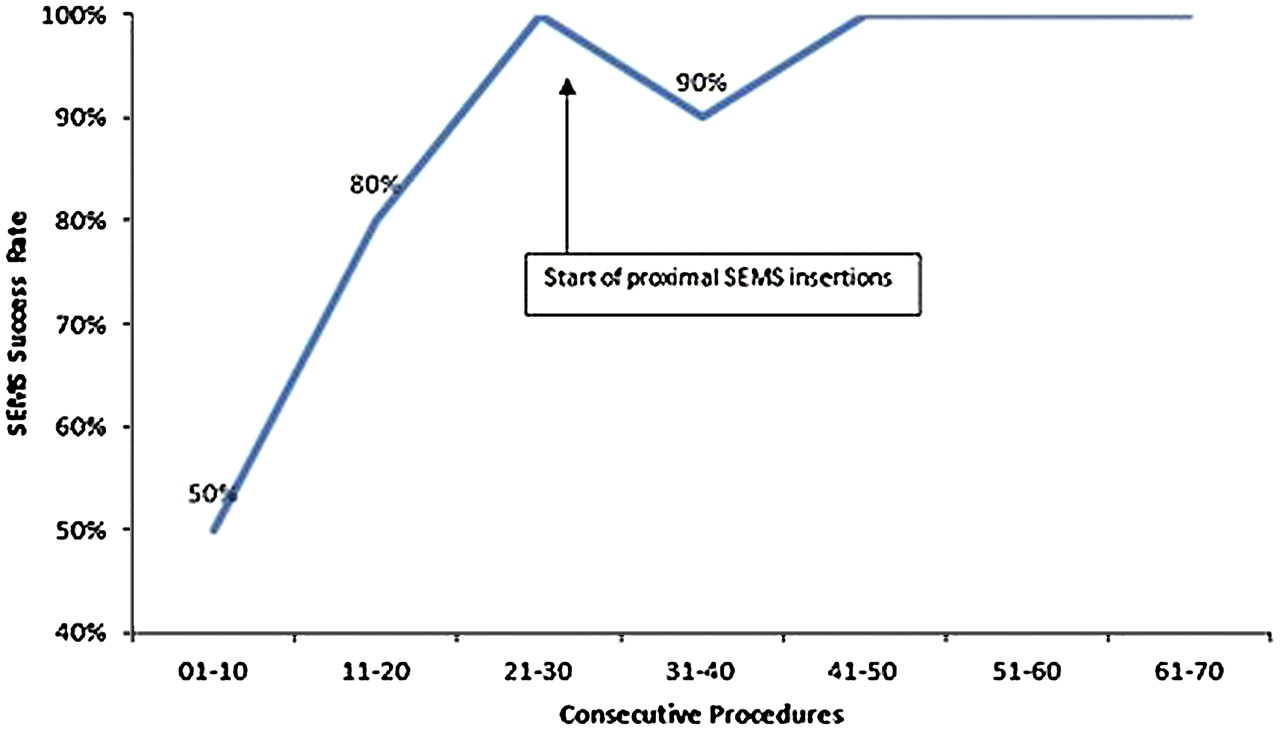
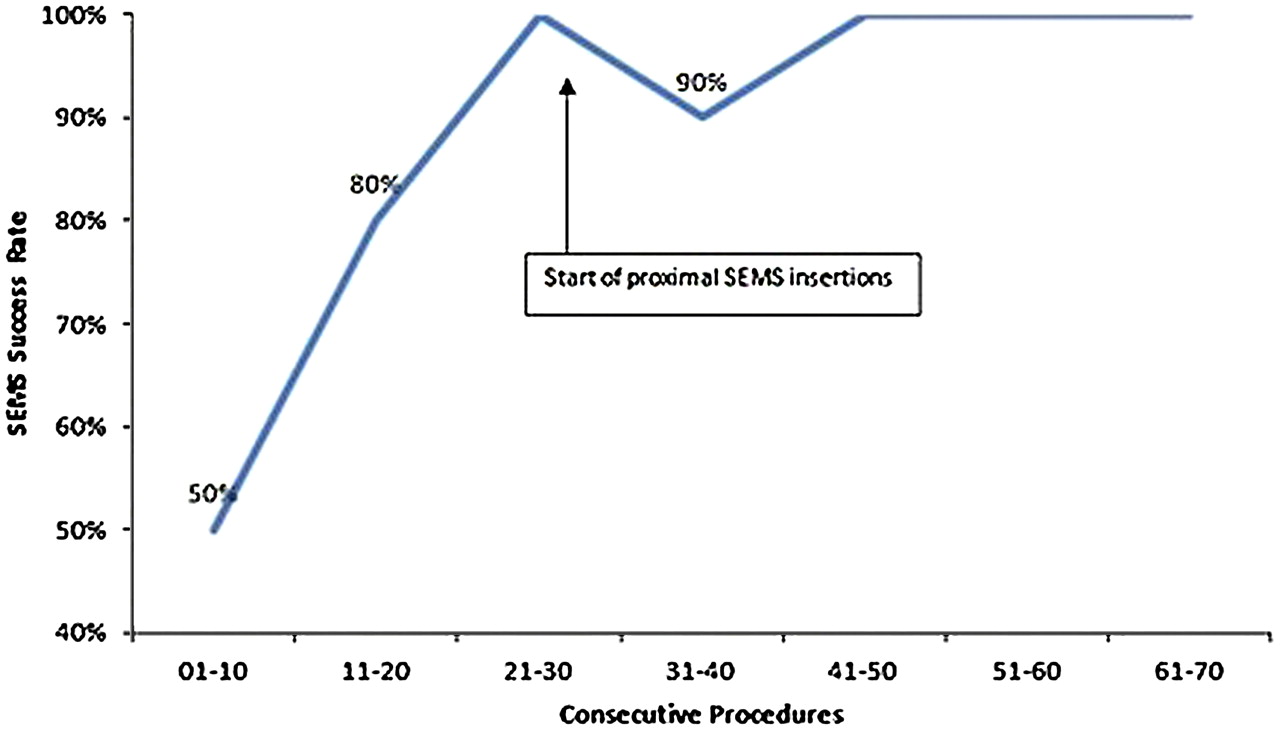
Results 70 SEMS insertions were attempted in 62 patients. Each procedure is carried out endoscopically with radiological guidance by a gastroenterologist. Ten (14.3%) of the stents were proximal to the splenic flexure. The overall success rate for SEMS deployment was 88.6% (n=62). Abstract PTU-264 figure 1 shows the success rates improvement with the number of procedures carried out. 7 of the 8 failures occurred in the first 20 procedures carried out in our unit. Reasons for unsuccessful procedures are failure to traverse stricture with guidewire (n=5), stent slippage (n=2) and poor bowel prep & excessive looping (n=1). Overall complications rates were low. There were two perforations (2.9%), one of which underwent emergency surgery while the other was managed conservatively. Restenosis occurred in two patients (2.9%) and tumour overgrowth occurred in 1 (1.4%).
{kind=link}
Conclusion SEMS technology is now readily available and is a safe and effective means of treating malignant colonic obstruction. As with all new techniques there is a learning curve associated with its implementation. We have shown that the learning curve is surmountable and that potentially any unit could offer a colonic SEMS service.
Competing interests None declared.
References 1. Vemulapalli R, Lara LF, Sreenarasimhaiah J, et al. Dig Dis Sci 2010;55:1732–7.
2. Manes G, de Bellis M, Fuccio L, et al. Arch Surg 2011;146:1157–62.
3. Foo C, Poon JT, Law WL. Colorectal Dis 2010;13:549–54.
4. Olubaniyi BO, McFaul CD, Yip VSK, et al. Ann R Coll Surg Eng 2008;91:55–8.