Article Text

Abstract
Objective To clarify the full range of benefits and adverse consequences of Helicobacter pylori eradication as a strategy for gastric cancer prevention, the community-based intervention trial was launched in Linqu County, China.
Design A total of 184 786 residents aged 25–54 years were enrolled in this trial and received 13C-urea breath test. H. pylori positive participants were assigned into two groups, either receiving a 10-day quadruple anti-H. pylori treatment or lookalike placebos together with a single dosage of omeprazole and bismuth.
Results The prevalence of H. pylori in trial participants was 57.6%. A total of 94 101 subjects completed the treatment. The overall H. pylori eradication rate was 72.9% in the active group. Gender, body mass index, history of stomach disease, baseline delta over baseline-value of 13C-urea breath test, missed medication doses, smoking and drinking were independent predictors of eradication failure. The missed doses and high baseline delta over baseline-value were important contributors in men and women (all Ptrend<0.001). However, a dose-response relationship between failure rate and smoking or drinking index was found in men (all Ptrend<0.001), while high body mass index (Ptrend<0.001) and history of stomach disease were significant predictors in women. The treatment failure rate increased up to 48.8% (OR 2.87, 95% CI 2.24 to 3.68) in men and 39.4% (OR 2.67, 95% CI 1.61 to 4.42) in women with multiple factors combined.
Conclusions This large community-based intervention trial to eradicate H. pylori is feasible and acceptable. The findings of this trial lead to a distinct evaluation of factors influencing eradication that should be generally considered for future eradication therapies.
Trial registration number ChiCTR-TRC-10000979 in accordance with WHO ICTRP requirements.
- GASTRIC CANCER
- HELICOBACTER PYLORI
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
Gastric cancer is a global public health burden, nearly one million new cases are diagnosed each year worldwide, of which 42% cases occur in China.
Helicobacter pylori infection is the main risk factor for gastric cancer, and it was classified as a class I carcinogen for gastric cancer by International Agency for Research on Cancer in 1994.
The Shandong Intervention Trial launched in Linqu in 1995 yielded a 39% reduction in gastric cancer incidence rate after 15 years follow-up.
Benefits and adverse consequences of strategy for gastric cancer prevention by eradication of H. pylori are still in concern in the community setting.
What are the new findings?
The large community-based intervention trial to eradicate H. pylori is feasible and acceptable in a high-risk area of gastric cancer in China. It gained an elimination of 72.9% of H. pylori in such community intervention trial without severe side effects among all the subjects during the entire 30-month trial period.
Gender, body mass index, history of stomach disease, baseline delta over baseline-value of 13C-urea breath test, missed medication doses, smoking and drinking were independent predictors of eradication failure.
How might it impact on clinical practice in the foreseeable future?
The findings of this trial lead to a distinct evaluation of the factors influencing eradication of H. pylori that should be generally considered for future eradication therapies, particularly in a community-based intervention trial.
Introduction
Helicobacter pylori (H. pylori) is a recognised cause of chronic gastritis and peptic ulcer disease, and may play an important role in the etiology of gastric cancer (GC).1 ,2 The development of GC in a subset of H. pylori-infected individuals may be a result of subtle changes in the gastric epithelial cells induced by bacteria and host inflammatory response,3 including DNA alterations and an imbalance between proliferation and apoptosis.4 ,5 In 1994, the International Agency for Research on Cancer has classified H. pylori as a class I carcinogen for GC.6 In 2005, the H. pylori-GC Task Force recommended that for countries with a high risk of GC, the greatest benefit would be gained by eradicating or preventing H. pylori infection in early adulthood.7
Linqu County, an underdeveloped rural region in Shandong Province, was identified to be one of the areas with the highest incidence of GC in China. Since 1983, a series of epidemiological investigations have been conducted in this region to explore aetiology and prevention of this common cancer worldwide.8–12 Indeed, 50–85% of children aged 3–10 years and 67% of the adults in Linqu were infected by H. pylori,9 ,10 and H. pylori infection was a risk factor for progression from atrophic gastritis to intestinal metaplasia, dysplasia and GC.11
Consequently, we conducted a Shandong Intervention Trial in Linqu in 1995.12 ,13 This trial yielded a 40% reduction in the prevalence of advanced gastric lesions as well as a favourable effect on GC after 7 years.12 Moreover, the trial participants were continually followed for an additional 8 years, showing a 39% reduction in GC incidence rate even among older subjects and those with advanced baseline pathology.14 ,15 A meta-analysis with a total of 6695 participants including our trial in Linqu also showed that the relative risk for GC was 0.66 (95% CI 0.46 to 0.95), suggesting that H. pylori eradication is effective in preventing GC.16 However, a recent report from the International Agency for Research on Cancer working group on H. pylori revealed concerns about the generalisability of H. pylori screening and treatment, and possible adverse consequences of programmes applied in the community setting.17
There was a unique opportunity to conduct a large community-based randomised trial in Linqu, which will provide more solid data to evaluate the full range of benefits and adverse consequences of strategy for GC prevention by eradication of H. pylori. In addition, this trial can extensively explore the factors affecting eradication that should be considered for future treatment of H. pylori, particularly in a community setting. The following text reports our detailed design, baseline results and factors influencing H. pylori eradication of this newly initiated community-based randomised trial with 184 786 residents in Linqu.
Methods
This intervention trial was a collaborative investigation between Peking University Cancer Hospital & Institute (PUCI), International Digestive Cancer Alliance and Technische Universität München.
Study population
In March 2011, 347 811 residents aged 25–54 years identified from a roster of 980 villages in 10 townships of Linqu were invited to participate in this trial (figure 1). The PUCI staff helped each village chief to distribute a written message to explain the aim and eligibility of the study, and a Brochure of ‘Helicobacter pylori Infection and Gastric Cancer and Gastric Lesions’ to explain the possibility of risk of H. pylori infection to GC and gastric lesions. Informed consent for participation was obtained from each subject; it was explicitly explained that H. pylori positive residents would be assigned into a high dose or a low dose group, and they are free to stop enrolment and leave the study at any time, and have a right to receive any medical care. Residents with the following conditions were excluded: peptic ulcers, serious medical conditions, undergoing active treatment for cancer, currently or previously on antibiotic therapy for H. pylori infection, history of congestive heart failure, respiratory failure, stroke, seizures, pregnancy, and mental or psychiatric illness.
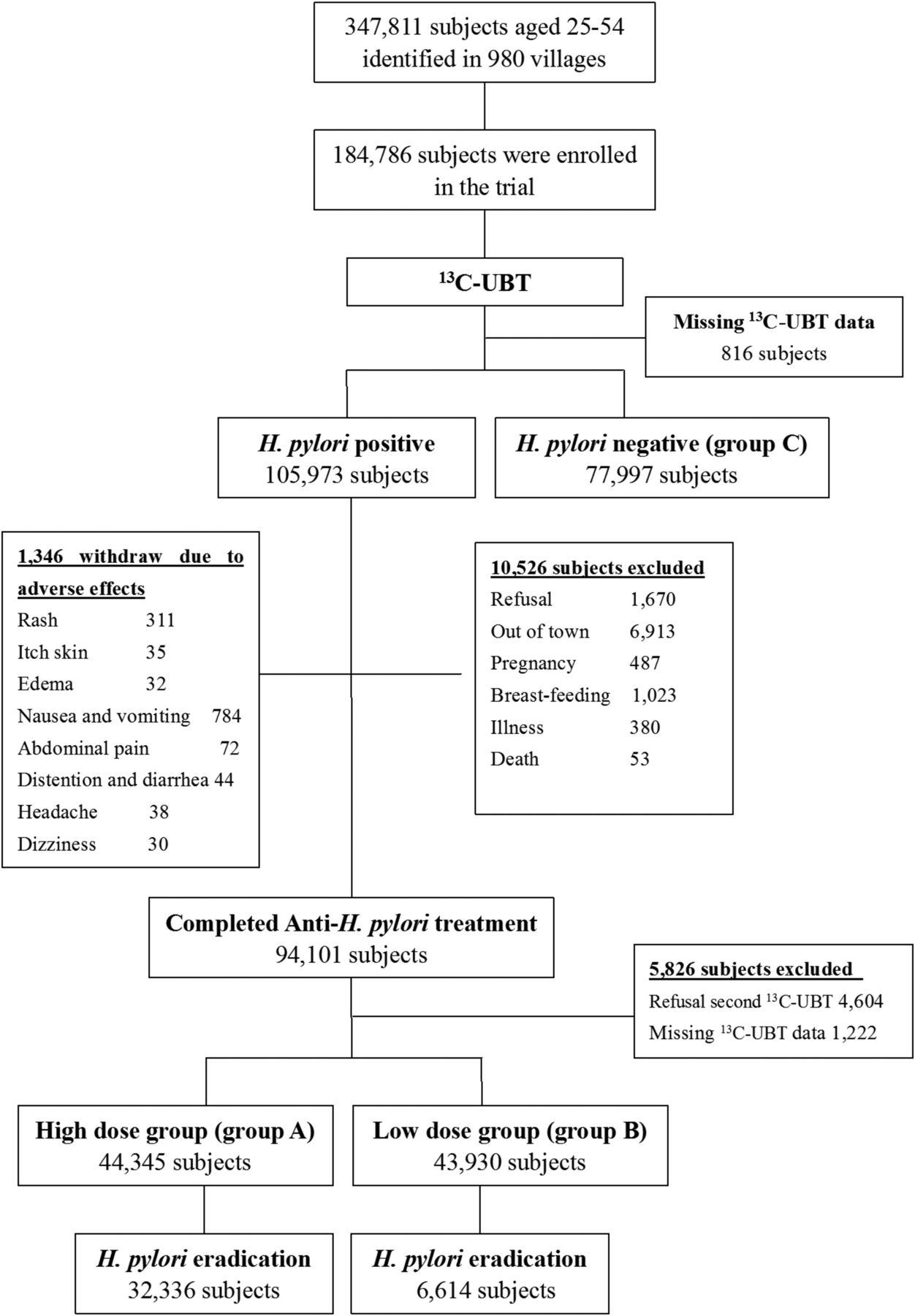
{kind=link}
Participant flow diagram. 13C-UBT, 13C-urea breath test.
A structured questionnaire was used at baseline including items on demographic variables, medical history, family cancer history, stomach disease history (including stomach pain, acid reflux and history of gastritis), occupation, smoking, alcohol drinking and dietary information. All interviews were conducted by trained interviewers using a computerised Data Collection and Management System. We also performed a physical examination in all subjects including measurements of height and body weight. In addition, two 4-mL blood samples were collected from trial participants.
Methodology of 13C-urea breath test
Each subject was requested to swallow a pill containing 75 mg 13C-urea (Min.99 atom %13C, Campro Scientific GmbH, Germany) with 20 ml of water in the morning. Exhaled air was collected in sampling tubes 30 min later. 13CO2 values were determined using a gas isotope ratio mass spectrometer, and delta over baseline-value (DOB) was used to express the difference between 30 min and baseline. The concentration of 13CO2 at 30 min that exceeded the baseline more than 3.8 parts per thousand (>0.38%) was regarded as a positive indicator of H. pylori infection.
Data collection and management system
We developed a data collection and management system, including: (1) Scanning System: scanning participant's ID and printing the individual barcode; (2) Interview System: computerised interviews to collect baseline information; (3) Web-based Data Editing: storing data in a database and integrating it online; and (4) Database Management System: building a database for effective storing and retrieval on demand. Access to the database was limited to authorised researchers of the trial.
Randomisation and blinding
H. pylori positive residents were assigned into two groups using cluster randomisation by village, either receiving high dose therapy (group A) or low dose therapy (group B). H. pylori negative residents were assigned into group C (figure 1). A blocked stratified cluster randomisation scheme in each 10 townships was used. All villages within the township were first ranked by population size in descending order. Double-blinded blocks of six consecutively ranked villages were then identified, and two treatment groups were randomly assigned.
Interventions
The H. pylori positive subjects received either a 10-day quadruple anti-H. pylori treatment (group A) with omeprazole 20 mg twice daily, tetracycline 750 mg three time a day, metronidazole 400 mg three time a day and bismuth citrate 300 mg twice daily, or lookalike placebos of tetracycline and metronidazole together with single dosages of 20 mg omeprazole and 300 mg bismuth citrate (group B) (see online supplementary table S1).
To reach and maintain a high compliance, all participants took the medications in the house of the village leaders, and PUCI staff monitored the intake of the drugs at 6:00 and 18:00 over the 10-day period. All participants were also required to sign or fingerprint in the medication intake log daily to measure the compliance. Information on adverse events was collected and recorded on the adverse event case report form. All subjects with 10-day treatment underwent a second 13C-urea breath test (13C-UBT) at 45 days after treatment to determine the efficacy of H. pylori eradication. However, 13C-UBT was not performed in those who had not complete anti-H. pylori treatment.
Follow-up procedures and monitoring
The trial participants will prospectively undergo a follow-up for at least 7 years after the treatment. A rapid reporting system has been established in the population-based Cancer Registry in Linqu designated by the Chinese government.18 All new cancer cases are officially required to report to the Cancer Registry through an internet-based reporting system and a standard reporting form. All information on the cancer diagnosis using ICD-10:C00–96 is linked with the data collection and management system of our trial. For quality control, each village chief and village doctor will be responsible to report all cancer cases to the township doctors each month. The staff of PUCI will collect all information on the cancer cases every 3 months from township doctors and link the data with the Cancer Registry in Linqu, and then visit the villages every 6 months to validate the GC diagnosis and monitor the surveillance of each cancer case in the trial. If necessary, the staff will visit the hospital where the GC is diagnosed to obtain the medical files.
Safety related procedures
Participants were informed with a written information sheet by village leaders and PUCI staff and asked to report any potential adverse experiences to the investigator any time during the study. In addition, participants were withdrawn from the study within 24 h of any episodes of ulcer, perforation, upper GI bleeding or any moderate or severe adverse events regardless of whether or not the event resulted from treatment.
Any adverse event/concurrent illness experienced by a subject during any portion of the study was described in detail and fully evaluated by the investigator. Any pertinent information was recorded in the case report form. Any severe side effects were required to be reported to the independent Data and Safety Monitoring Board.
End points and statistical analysis
The primary end point of this trial is the incidence of GC. Secondary end points are GC mortality and other health effects related to H. pylori eradication. If we apply a significance level of 5% and a power of 90% to detect a conservative estimate of at least a 20% reduction of GC risk, we need 625 GC cases in total, 349 in the placebo group and 276 in the active group, according to the estimated incidence rates for each year by age for H. pylori positive individuals in Linqu. The trial will be terminated at any time during the follow-up period if the difference of GC incidence rate between two arms reaches a statistically significant level.
Pearson's χ2 test was used to examine the differences of H. pylori prevalence and H. pylori eradication rate in different sex, age, marriage, smoking and drinking statuses, and the differences of side effects between two groups. An unconditional logistic regression model was applied in the analysis of influence factors for H. pylori eradication by a backward selection with a statistical significance at 0.05. To test the dose effect of smoking and drinking on the H. pylori eradication rate, smoking and drinking indexes were generated, where smoking index= number of cigarettes taken per day×years of smoking and drinking index=dosage of alcohol consumption per week (kg)×years of drinking, respectively. Trend test of linear relationship between body mass index (BMI), baseline DOB, frequency of missed doses, smoking index and drinking index with H. pylori eradication rate were evaluated by unconditional logistic regression analysis adjusting for other risk factors. Furthermore, joint effects were calculated in different combinations of risk factors by logistic regression analysis. All p values were two-sided, and p<0.05 was considered statistically significant. All statistical analyses were carried out using Statistical Analysis System software (V.9.0; SAS Institute, Cary, North Carolina, USA).
Results
The field work of this intervention trial was launched in March 2011 and completed in September 2013 (30 months). A total of 184 786 residents aged 25–54 years from 980 villages were enrolled, accounting for 53.1% of the relevant population of 347 811 in Linqu (figure 1). Apart from refusing participation and meeting exclusion criteria, many migrant farm workers who were absent from home contributed to 53.1% of enrolment of the entire population.
Overall prevalence of H. pylori in study population
Among 184 786 subjects enrolled in the trial, 183 970 had 13C-UBT results, and 105 973 were H. pylori positive (figure 1; see online supplementary table S2). The overall prevalence of H. pylori in the trial participants was 57.6%, slightly higher in men than in women (59.0% vs 56.4%, p<0.0001). The age-specific prevalence of H. pylori was 59.5% at 25–29 years, similar among those at 30–34 years, 35–39 years and 40–44 years, but a little lower among those at 45–49 years and 50–54 years (57.0% and 54.3%). The prevalence of H. pylori was at a similar level in different townships.
Adverse events
In 1346 subjects reporting moderate side effects, anti-H. pylori treatment was stopped including 916 (2.3%) in group A and 430 (0.98%) in group B (p<0.0001). The proportions of rash (0.43% vs 0.27%, p<0.0001), nausea and vomiting (1.28% vs 0.49%, p<0.0001) were higher in group A than in group B (see online supplementary table S3). No severe side effects or life-threatening events were observed among all the subjects with a 10-day treatment during the entire 30-month trial period.
Compliance and balance in different groups
Among 105 973 H. pylori positive subjects, 94 101 completed the treatment (compliance 88.8%), and 88 275 (compliance 93.8%) finally received the second 13C-UBT after treatment including 44 345 in group A and 43 930 in group B. A total of 11 872 (11.2%) subjects withdrew before or during a 10-day treatment in the 30-month trial period due to pregnancy, breast feeding, illness, being out of town, death, refusal and side effects (figure 1).
The randomisation of the trial participants reached an adequate balance between three groups within strata defined by baseline characteristics of the subjects (table 1). The majority of the subjects were farmers (78.5%, 79.0% and 78.1%, respectively) with education of middle school or less (96.1%, 97.8% and 96.3%, respectively). Smoking and alcohol drinking were frequent among men but not in women. About 10.7% of participants had family history of cancer (11.2%, 10.5% and 10.6%, respectively), and about 33.5% of participants were overweight or obese (BMI ≥25) (33.8%, 34.3% and 32.7%, respectively).
Baseline characteristics of participants in the different groups*
Efficacy of the H. pylori treatment and factors affecting H. pylori eradication
The overall H. pylori eradication rate was 72.9% in group A and 15.1% in group B. As shown in table 2, except for age and BMI level, the H. pylori eradication rate in group A varied by gender, education, marriage, occupation, family cancer history, stomach disease history, smoking and drinking status. Men, subjects with college education, unmarried subjects or widows, smokers and alcohol drinkers, and subjects with family cancer history or stomach disease had lower eradication rates.
Helicobacter pylori eradication rate in group A stratified by baseline characteristics*
We further evaluated the factors influencing the eradication in 43 846 subjects (out of 44 345) with the full data in group A, including 20 878 men and 22 968 women. Among them, 32 268 subjects had successful eradication of H. pylori, and 11 578 had treatment failure. As summarised in table 3, male gender, missed doses, smoking, drinking, history of stomach disease, high BMI, and high baseline DOB were significantly and independently associated with the eradication failure by stepwise multivariate logistic regression analysis. A grade-response association was found between failure rate and smoking index (OR: 1.23 to 1.56, Ptrend<0.001), drinking index (OR: 1.11 to 1.29, Ptrend<0.001), baseline DOB (OR: 1.09 to 1.19, Ptrend<0.001) or missed medication doses (OR: 1.32 to 2.15, Ptrend<0.001). Further stratified analysis by sex showed that high baseline DOB and missed doses were important contributors in men and women. However, a grade-response relationship between failure rate and smoking or drinking indices was only found in men (all Ptrend<0.001), and a history of stomach disease (OR 1.23, 95% CI 1.10 to1.38) and high BMI (Ptrend<0.001) were the significant predictors in women.
Multivariable logistic regression analysis on the influence factors for Helicobacter pylori eradication rate
We were also interested in assessing the joint effect of risk factors for failure of H. pylori eradication. The joint effect was more evident and stronger in subjects with combined multiple risk factors (table 4). For men, H. pylori eradication failure rate was up to 48.8% in subjects with high baseline DOB, missed doses, smoking and drinking, with a 2.87-fold (95% CI 2.24 to 3.68) increased risk of eradication failure compared with reference group. However, for women, the risk of eradication failure was more pronounced in subjects with high baseline DOB, history of stomach disease and missed doses (OR 2.67, 95% CI 1.61 to 4.42).
Joint effect analysis of the influence factors for Helicobacter pylori eradication rate
Discussion
In Linqu County, a high-risk area of GC in China, more than 50% of 347 811 eligible population aged 25–54 years participated in this trial, indicating an excellent feasibility and acceptance. This largest trial so far provides the unique opportunity to clarify whether and how to implement strategies for preventing GC by eradication of H. pylori in a large community setting.
We are one of the first groups to study the effects of treatment of H. pylori on GC and its precursors. Our Shandong Intervention Trial and another 2×2 factorial designed, randomised controlled trial in Linqu indicated that H. pylori eradication is effective in preventing GC and progression of gastric lesions.12 ,14 ,15 ,19 However, the sample size in those trials was relatively small and insufficient for estimation of the overall benefits and possible adverse consequences in the community-based eradication scheme. With the large sample size of 184 786 subjects in this trial, we will achieve more power to directly detect the impact on the incidence of GC. In addition, it permits evaluation of the impact of reduction of GC and early preventive treatment among young adults aged 25–34 years in the trial, because we found that 50% of children at 3 years to 85% at 10 years were infected with H. pylori in Linqu and gastritis is very common in young adults.8 ,9 Moreover, the longitudinal outcomes indicated that H. pylori infection primarily enhanced the transition from superficial gastritis to atrophy, indicating that the inhibition of progression of gastric lesions in young adults might be a critical strategy.
We evaluated earlier several schemes of H. pylori treatment, including a dual or triple eradication therapy in Linqu, yielding an unsatisfactory eradication rate (64–69%).12 ,20 However, two trials reported that a bismuth-based quadruple therapy eradicated H. pylori infection by 93% and 88%, respectively.21 ,22 Another clinical trial using the same regimen in 7 days and 10 days also showed high rates of eradication of H. pylori.23 To assess the efficacy of this 10-day quadruple therapy and its safety in Linqu population, we conducted a placebo-controlled pilot study with 277 subjects in one village before this large trial, and H. pylori eradication rates were 76.7% by intention-to-treat (ITT) analysis and 83.3% by per-protocol (PP) analysis.24 Our experiences showed that elimination of 72.9% of H. pylori in this community-based treatment has been relatively successful. Besides strict monitoring and good compliance of treatment, low resistance to tetracycline (3.5% in China),25 which has not been widely used for more than 20 years in China, may be beneficial in H. pylori management. Although a high rate of resistance to metronidazole was found in China and Asia,25 ,26 the combined resistance to tetracycline and metronidazole was only 5.32% in Linqu population (data not shown). Moreover, the cost of this regimen is much lower than triple therapy with omeprazole, amoxicillin and clarithromycin management.
In this large trial, we found 15.1% of the subjects in group B turned to be negative in 13C-UBT assessments at 45 days after the therapy. There are several possible explanations for this result. 13C-UBT may give some false negative results (up to 5%), particularly for those with values only slightly above the diagnostic threshold of 13C-UBT (possibly caused low density of H. pylori in the gastric mucosa). In addition, bismuth or omeprazole might have an impact on the eradication of H. pylori. Indeed, several studies have shown that a single dosage of 20 mg or 40 mg omeprazole can achieve about a 10–50% H. pylori eradication rate,27 ,28 and bismuth salts are partially effective in suppressing and eradicating H. pylori as monotherapy (eradication rates ranging from 0 % to 32%),29 ,30 although H. pylori recurrence appeared more frequently in those patients. Omeprazole reduces the stomach acid which can inhibit H. pylori urease and therefore might change H. pylori activity, representing a direct effect on H. pylori. Omeprazole has also been found to have a number of anti-inflammatory actions that are independent of their effects on gastric acid secretion.31 Bismuth may have an anti-H. pylori action by a number of mechanisms including inhibition of cell wall synthesis, cell membrane function and protein synthesis.32 In addition, bismuth has been suggested to decrease the development of H. pylori resistance to antibiotics.32 In the future, it will be interesting to re-evaluate the status of those subjects who turned to negative in the low dose group as well as the possibility of H. pylori recurrence in the two treatment arms.
Studies demonstrated that the efficacy of H. pylori eradication depended upon a number of factors. Smoking can stimulate gastric acid secretion, decrease gastric blood flow and mucus secretion, and thus might reduce the delivery of antibiotics to gastric mucosa.33 ,34 Alcohol drinking can affect H. pylori eradication at different levels, such as gastric emptying and acid secretion.35 Our study showed that smoking and drinking habits were the most important contributors to the eradication failure in men, consistent with previous studies.33–35 We also found that the high baseline DOB, as a potential indicator for H. pylori growth in the stomach, was an important predictor for eradication failure, confirming the findings of former study.36 It would be tempting to speculate that high H. pylori load was associated with eradication failure and more severe gastritis, therefore, those subjects might benefit from extended therapies (duration from 10 days to 14 days). In our study, we found a grade-response association between BMI level and eradication failure in women, providing new evidence and suggesting that extended therapies should be recommended for those with high BMI. Several studies showed that H. pylori eradication rates increased with the severity of inflammation and activity, and decreased with the severity of atrophy.37 Although we didn't conduct an endoscopic screening before enrolment, our previous endoscopic survey in Linqu showed that chronic atrophic gastritis was nearly universal in the adult population.8 In spite of a very good compliance of treatment, we identified that missed doses were an important predictor for eradication failure, particularly for women with more than three missed doses, indicating that patients require detailed information. In addition, we found that missed doses were more common among those with college education due to busy daily work (4.00% vs 2.75% among those with primary school education, p=0.005), corresponding with a lower eradication rate (69.3%) in those subjects. Together, the results indicate that more attention should be paid to environmental and patient-specific factors to increase the successful eradication of H. pylori and thus improve prevention and control of GC development.
The prevalence of H. pylori declined from 67.1% in 1995, to 63.2% in 2002 and 57.6% in 2011/2013 among the residents in Linqu, consistent with the consensus of the second Asia-Pacific conference of H. pylori management, which states that a decline in prevalence of H. pylori appears to parallel economic improvement within a particular country.38 The infection of H. pylori is acquired at very young age of 3 years and is highly associated with parental, particularly maternal infection, suggesting person-to-person transmission is the most plausible route of H. pylori infection in Linqu.39 Moreover, drinking shallow water is associated with H. pylori infection.40 The sanitation system improved in the past 18 years, which may account for the annual reduction of 0.54% prevalence in this region. However, a higher prevalence of H. pylori infection in patients who developed GC was found in our previous cohort study in Linqu (76.5% in the GC group vs 54.8% in the superficial gastritis group),10 ,41 and the crude mortality rate of GC in Linqu has not significantly declined over the past decades. Beside H. pylori, our series of epidemiological studies in Linqu suggested that dietary and other environmental risk factors as well as interaction with H. pylori infection may also play important roles in GC development.11 ,42
H. pylori eradication might be associated with the development of gastro-oesophageal disease and esophageal adenocarcinoma. A negative association between the prevalence of H. pylori and the severity of GORD has been demonstrated in epidemiological studies.43 However, several cohort studies and randomised controlled trials of the effects of H. pylori eradication on GORD are inconclusive.43 ,44 A recent meta-analysis demonstrated that eradication of H. pylori was related to the higher risk of developing GORD in Asian studies.44 In contrast, no such risk has been reported by Western studies.45 However, two recent large-scale cohort studies in Korea produced inconsistent results.46 ,47 In addition, our previous endoscopic surveys revealed that GORD was rare and oesophageal adenocarcinoma was uncommon in Linqu,48 therefore, the risk of increasing GORD and oesophageal adenocarcinoma may be minor in comparison with the benefits of a 20–40% of reduction in GC incidence in Linqu.
Our large-scale trial has several strengths compared with previous trials. First, it is a prospective, randomised, placebo-controlled trial with good quality control in a well-organised high-risk population. The large sample size could increase the power and the possibility of observation strata. Second, the high treatment compliance might enhance the reliability of the trial, and using a data collection and management system could avoid errors occurring during the data collection and management processes. In addition, an excellent balance of variables in the three groups indicated a high quality implementation of this large trial.
This large-scale trial has also several potential limitations. One of the limitations is that the low dose group is not a pure placebo group due to ethical considerations, and participants assigned to the low dose regimen are expected to suffer from the disadvantage of developing more GCs. However, efforts were made to obtain maximal benefits for each trial participant. During the follow-up period, participants are eligible to receive any medical care including anti-H. pylori treatment. They also have a right and an equal chance to participate in the endoscopy screening program for early detection of GC, which is free of charge and designed by the Chinese Ministry of Health in an endoscopy centre of Linqu County Hospital each year. In the mean time, participants will be closely followed by PUCI staff and township/village doctors, who are responsible for local medical care. They will contact the participants closely to discover any symptoms of gastric diseases every 3 months and decide/suggest if the participant needs to receive the treatment or requires further examination in Linqu County Hospital. We will systematically collect the medical care information of participants through the medical insurance, and adjust the effect of treatment by stratified analysis at the end of the trial. If this unique trial reveals a beneficial effect on GC risk by eradication of H. pylori, we will provide treatment to the subjects in the low dose arm at the end of the trial period. Second, the cluster randomisation design could reach a slightly lower efficacy than the individual randomisation. However, it is difficult, if not impossible, to randomise each individual in such a large sample size trial.
In conclusion, to prevent the burden of one million new GC cases each year in the world, we initiated a large-scale intervention trial, representing more than 50% of adults aged 25–54 years in 980 villages in Linqu. This important trial will finally answer many remaining questions and evaluate the cost-benefit in GC prevention strategy. Importantly, we identified and confirmed several risk factors affecting eradication, helping to improve the personalised efficacy of the therapy in the future, particularly in a community-based treatment.
Acknowledgments
The authors thank the trial participants, field staff and government of Linqu for supporting this large trial, the Wei-fang Centre for Disease Control (CDC) for their support in biospecimen storage collected in this trial, and the Beijing Double-Crane Pharmaceutical for donation of the bismuth-based quadruple medicines and its placebo in the trial. The authors also thank members of the Scientific Committee Drs G Tytgat (Chairmen), SD Xiao, JE Geenen, P Malfertheiner, F Bazzoli, D Forman and ZW Dong, and the Data Safety Monitoring Committee Drs KC Wu, YH Hu, F Megraud and WJ Blot for guidance and overseeing of this trial. In addition, the authors thank Dr Ruanren Hu for consultation of the trial randomisation.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
K-fP and LZ contributed equally.
Contributors All authors directly participated in the planning, execution or analysis of the study. All authors have read and approved the final version submitted. All authors accept responsibility for its content. Study organisation was by W-cY and MC, and W-cY designed the study. W-cY, MC, K-fP, Lian Z, RS, MG, MB, MV, MQ and SS supervised the execution of the study. J-lM, W-dL, J-xW, Lei Z, L-fZ, ML, R-yL, L-hW, TZ and W-xG were responsible for the field administration and data collection. K-fP, KU and Lei Z performed the statistical analyses. W-cY, MC, K-fP, RS and MG drafted the manuscript.
Funding This research was supported in part by grants from Key International S&T Cooperation Project (2010DFB30310), National Basic Research Program of China (973 program 2010CB529303), a grant from Peking University Cancer Hospital & Institute, China, and International Office BMBF (CHN 11/021), DZIF German Centre for Infection Research, München, Germany.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The project was approved by the Institutional Review Board of PUCI and collaborating institutions.
Provenance and peer review Not commissioned; externally peer reviewed.