Article Text

Abstract
Objectives Interval colorectal cancer (CRC) after colonoscopy may affect effectiveness and cost-effectiveness of screening programmes. We aimed to investigate whether and how faecal haemoglobin concentration (FHbC) of faecal immunochemical testing (FIT) affected the risk prediction of interval cancer (IC) caused by inadequate colonoscopy quality in a FIT-based population screening programme.
Design From 2004 to 2009, 29 969 subjects underwent complete colonoscopy after positive FIT in the Taiwanese Nationwide CRC Screening Program. The IC rate was traced until the end of 2012. The incidence of IC was calculated in relation to patient characteristics, endoscopy-related factors (such adenoma detection rate (ADR)) and FHbC. Poisson regression analysis was performed to assess the potential risk factors for colonoscopy IC.
Results One hundred and sixty-two ICs developed after an index colonoscopy and the estimated incidence was 1.14 per 1000 person-years of observation for the entire cohort. Increased risk of IC was most remarkable in the uptake of colonoscopy in settings with ADR lower than 15% (adjusted relative risk (aRR)=3.09, 95% CI 1.55 to 6.18) and then higher FHbC (μg Hb/g faeces) (100–149: aRR=2.55, 95% CI 1.52 to 4.29, ≥150: aRR=2.74, 95% CI 1.84 to 4.09) with adjustment for older age and colorectal neoplasm detected at baseline colonoscopy. Similar findings were observed for subjects with negative index colonoscopy.
Conclusions Colonoscopy ICs arising from FIT-based population screening programmes were mainly influenced by inadequate colonoscopy quality and independently predicted by FHbC that is associated with a priori chance of advanced neoplasm. This finding is helpful for future modification of screening logistics based on FHbC.
- COLORECTAL CANCER SCREENING
- COLORECTAL CANCER
- SCREENING
- COLORECTAL NEOPLASIA
- COLONOSCOPY
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
Screening can reduce the risk of colorectal cancer but the existence of interval cancer (IC) may affect the effectiveness of the screening programme.
Inadequate colonoscopy quality such as low adenoma detection rate (ADR) has been well documented as the main cause of missed ICs but not confirmed in large population-faecal immunochemical testing (FIT)-based screening programmes as yet.
Faecal haemoglobin concentration (FHbC) obtained from FIT-based screening programmes has recently been reported as a predictor for IC, but whether it is a predictor, revealing a chance of advanced colorectal neoplasm, for colonoscopy IC independently of the influence of colonoscopy quality, has never been addressed.
What are the new findings?
We corroborated that inadequate quality of colonoscopy is still a dominant cause of ICs as they preponderated in low ADR (<15%) in FIT-based population screening programmes, allowing for old age, FIT level and baseline colonoscopy with neoplasm.
FHbC is demonstrated as an independent predictor for risk of IC after considering inadequate quality of colonoscopy together with old age and baseline colonoscopy with neoplasm.
How might it impact on clinical practice in the foreseeable future?
The results may be applied for tailored case management and modification of screening logistics based on FHbC in population-FIT-based screening programmes.
Introduction
Colorectal cancer (CRC) is the second leading cause of cancer mortality worldwide, and its incidence is rapidly rising in the Asia-Pacific region.1 Screening for CRC enables early detection of invasive cancers or precancerous neoplastic lesions, thereby reducing their associated mortality.2 ,3 Populations at high risk for CRC can be selected with faecal-based tests, which have proven efficacy.4 Such screening tests have become popular in regions where colonoscopy resources are limited.5 Our recent study demonstrated that population screening with faecal immunochemical testing (FIT) can effectively reduce mortality from CRC.6 Nevertheless, interval cancers (ICs) still occur between screening rounds, either after negative faecal testing or after colonoscopy and studies have shown that ICs after colonoscopy result primarily from lesions missed at colonoscopy and, less often, from biological factors, such as rapidly growing neoplasms.7–10 Therefore, identification of potential risk factors for occurrence of ICs through monitoring the screening programme is of paramount importance. Previous studies have demonstrated that ICs have been closely associated with the quality of colonoscopy and may affect the effectiveness and cost-effectiveness of the entire screening programme.8 ,11–14 Adenoma detection rate (ADR) is one of the most important and well documented indicators that are closely associated with subsequent risk of IC or even CRC death.11 ,13 Nevertheless, to what extent poor quality of colonoscopy makes contribution to occurrence of IC in population-based screening for CRC with FIT has been barely addressed and whether and how risk prediction of ICs resulting from inadequate quality of colonoscopy can be influenced by FIT level remained unclear.
Quantitative faecal immunochemical test (FIT) permits the determination of an optimal cut-off for the faecal haemoglobin concentration (FHbC) based on regional prevalence of CRCs and the available capacity of colonoscopy. The quantitative measurement of FHbC has been described, but is seldom used clinically. It has been reported that FHbC determines a priori chance of an advanced lesion and correlates with the histological severity of colorectal neoplasms detected at colonoscopy.15–17 Our recent studies have demonstrated that FHbC, even when below the determined cut-off, is correlated with the subsequent risk of incident neoplasm.16 ,18 ,19 Since missed neoplasms are the primary cause of IC, it is reasonable to speculate that higher levels of FHbC carry a higher risk of IC after colonoscopy and thereby we can apply it for identification of people at risk of IC under the current quality monitoring framework.
By using large population-based data on subjects who had received colonoscopy after positive FITs in the Taiwanese Nationwide CRC Screening Program, we aimed to corroborate how inadequate quality of colonoscopy makes contribution to the occurrence of IC and to further assess whether FHbC concentration is an independent predictor for IC to influence risk prediction of IC caused by inadequate colonoscopy quality after controlling for patient characteristics and index colonoscopy findings.
Methods
Taiwanese nationwide CRC screening programme and study population
The Taiwanese Nationwide CRC Screening Program was launched in 2004.6 In the programme's inaugural 10 years, biennial FIT was offered to average-risk subjects aged 50–69 years. Those at high risk for CRC, such as hereditary CRC syndromes or IBD, were identified and recommended a direct colonoscopy rather than FIT screening. All data are stored in the central database and screening activities in all municipalities and relevant screening indicators (eg, FIT positive rate, confirmatory examination rate, neoplasm detection rate and presence of IC) are assessed regularly by the government's monitoring and evaluation centre. In this study, subjects who received complete total colonoscopy after positive FITs without detection of CRC at any round of the screening programme during the period 2004–2009 comprise the study cohort, and all subjects were traced longitudinally by linkage to the Taiwan Cancer Registry in order to identify subsequently developed cancers (described below).
FIT and confirmatory colonoscopy after positive tests
One of two FIT kits (OC-SENSOR by Eiken Chemical, Tokyo, Japan, and HM-JACK by Kyowa Medex, Tokyo, Japan) was selected by each municipality based on its own purchasing processes. Faecal testing was conducted with 1-day (single sample) sampling, and faecal haemoglobin cut-off for the two tests was established at 100 ng/mL for the OC-SENSOR and 8 ng/mL for the HM-JACK; both were equivalent to 20 μg Hb/g faeces.20 The mass of faeces collected and volume of the device buffer were claimed as 10 mg and 2 mL, respectively, for OC-SENSOR and 0.5 mg and 1.25 mL, respectively, for HM-JACK. All the patients were asked to collect the faecal sample at home using the collecting stick and store the faecal samples in refrigerators after collection, then submit to certified laboratories in each individual municipality for testing within 1 week. A positive test was defined as a result that was above the defined cut-off for the given test. Test results of FIT were stored in the regional and central government database and reported to all participants by mail and telephone, and participants with positive tests were referred for colonoscopy by certified endoscopists (gastroenterologist or surgeon) within 6 months. The results of the colonoscopies were documented in the hospitals where the procedures were performed and in the government's central database. Endoscopic findings of those who need more than one colonoscopy to clear all detected neoplasms were also traced and documented. The fees for confirmatory colonoscopies were reimbursed by the National Health Insurance, which has a coverage rate of 99.9% of the entire population.
Colorectal neoplasms and hospital-level ADR
All colorectal neoplasms detected and/or resected at index (baseline) colonoscopy that had been triggered by a positive FIT were classified according to the WHO criteria.21 Advanced adenoma was defined as a lesion larger than 10 mm, or a lesion having a villous component or high-grade dysplasia. Advanced neoplasm was defined as advanced adenoma or invasive cancers.
As our screening database could specify the hospital where colonoscopy was performed rather than the individual endoscopist, we calculate the hospital-level ADR in this study.
Ascertainment and definition of colonoscopy IC
The screening database was linked to the Taiwan Cancer Registry, from which data regarding incident CRC could be obtained. This cancer registry is a nationwide programme, with a coverage rate of 98.6% and accuracy of greater than 99%. Date of diagnosis can be obtained by matching the computerised data file of the screening programme with the registry's database, using each subject's unique identification number. In this study, we traced incident cases by linking to this registry system until the end of 2012. For some cases that needed more than one clearing colonoscopy to resect multiple or large neoplasms, we traced and merged the endoscopic findings of those multiple colonoscopies with the aid of the reports from regional health bureaus and linkage to the cancer registry.
We adopted the definition of IC after colonoscopy as proposed by the Expert Working Group on interval CRC of the CRC Screening Committee of the World Endoscopy Organization.22 According to this definition and currently recommended postcolonoscopy surveillance intervals, in a FIT-based screening programme, we defined IC as CRCs diagnosed within 3 years after index colonoscopies with the finding of advanced adenoma, within 5 years with the finding of non-advanced adenoma and within 10 years with negative finding.23 After excluding those with missing stage information, we also calculated the attributable proportion of colonoscopy IC of various aetiologies pursuant to the definition by le Clercq et al.24 ‘Colonoscopy IC caused by incomplete resection’ was defined as the proportion of colonoscopy ICs diagnosed in the same anatomical segment as a previously resected advanced adenoma; ‘colonoscopy IC caused by missed lesion’ as the sum of colonoscopy ICs of any size or stage that were diagnosed within 36 months of the index colonoscopy or American Joint Committee on Cancer (AJCC) stage III or IV CRCs that were diagnosed in 36 months and longer without previous advanced adenoma detected in the same segment at the index colonoscopy, and ‘colonoscopy IC caused by newly developed cancer’ as the colonoscopy ICs detected longer than 36 months after the index colonoscopy without features of advanced cancer and without a previous advanced adenoma in the same segment.
Statistical analysis
For IC, follow-up time was computed from the index colonoscopy until the diagnosis of CRC or until the end of 2012 for those who did not have IC based on the abovementioned definition. Person-years were defined as the product of the number of years from index colonoscopy to the occurrence of IC or till the end of 2012 (whichever came first) times the number of study population who were followed up, taking into account the currently recommended postcolonoscopy surveillance interval (3 years, 5 years and 10 years for advanced adenoma, non-advanced adenoma and negative findings at index colonoscopy, respectively) (figure 1). All person-years were used for IC incidence risk estimation and offset for the Poisson regression model. The incidence of IC was calculated and expressed as cancers per 1000 person-years of observation. CRCs detected at baseline and subsequent rounds of screening were considered as screen-detected CRC.

Flow diagram of identification of study population from the nationwide screening cohort.
Poisson regression model was applied to assess the potential risk factors responsible for IC. This model included FHbC (categorised as 20–49 μg Hb/g, 50–99 μg Hb/g, 100–149 μg Hb/g and ≥150 μg Hb/g of faeces), the FIT kit brand, and ambient temperatures when faecal samples were collected and other conventional factors, such as age (dichotomised to 60–69 years vs 50–59 years), gender (male vs female), settings with different ADRs (>30%, 15–30% and <15%) and index colonoscopy findings (normal, non-advanced adenoma, advanced adenoma). As Taiwan is an island that is located in the subtropical-tropical zone, the variation of ambient temperature changes by calendar month. Recent studies, including ours, have demonstrated that ambient temperature might have affected FIT performance; the ambient temperature of when and where individual faecal sample was collected was taken into account in the multivariable analysis.20 ,25 The analyses for the subjects with negative colonoscopy were conducted in the same manner. Factors with statistical significance in the univariate model were further analysed in the multivariate model. Relative risk (RR) and adjusted RR (aRR), and their respective 95% CIs, were calculated.
To test the predictive validity of the current model, we also performed cross-validation by splitting data into two-thirds for deriving the model and a third for validation of the model. The observed number of colonoscopy ICs in the validation data set were compared with the predicted ones that were computed by the application of parameters trained from the derivation data set.
All the statistical analyses were performed with SAS V.9.2 (SAS Institute, North Carolina, USA).
Results
Demographics of study cohort and IC subjects
The flow of identifying study population is demonstrated in figure 1. After excluding ineligible subjects with incomplete colonoscopy and baseline diagnosis of CRC or IBD at index colonoscopy, a total of 29 969 subjects who underwent complete colonoscopy constituted the study cohort and a total of 162 ICs were identified during the study period. The mean subject age was 59.8 years (SD=5.8) and 13 339 subjects (44.5%) in the whole study cohort were male; and mean subject age was 60.6 years (SD=5.4) and 91 subjects (56.2%) in the IC cases were male. Demographics such as FHbC, number of subjects that received colonoscopy in settings with different ADRs, and index colonoscopy findings of the whole cohort and IC cases are shown in table 1. The association of FHbC and the diagnostic yields of index colonoscopy (screen-detected adenoma and cancers) are demonstrated in online supplementary table S1.
Demographics of the study population (n=29 969) and interval cancer (IC) cases (n=162)
IC and IC rates
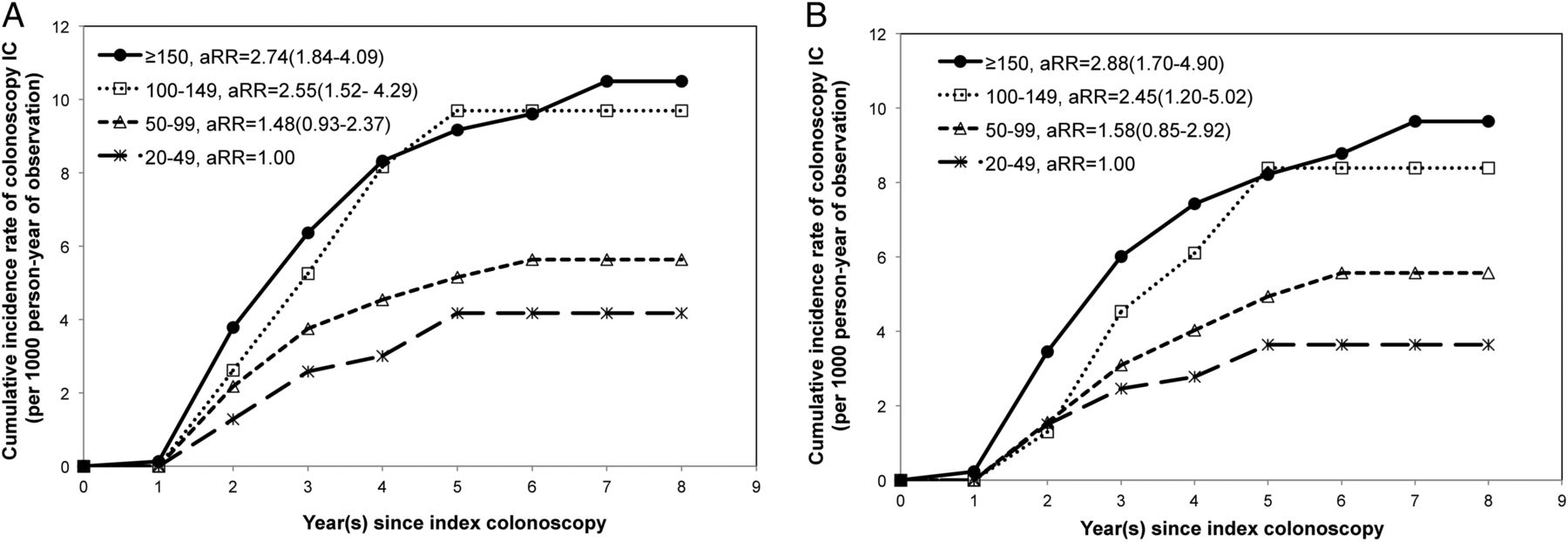
The overall incidence rate of IC was 1.14 per 1000 person-years of observation in the whole cohort and 0.94 per 1000 person-years of observation in subjects with negative colonoscopy. The IC rates in association with age group, gender, FHbC, hospital-level ADR and index colonoscopy findings are shown in table 2 and the association between FHbC and the risk of IC in the whole study cohort and those with negative index colonoscopy is demonstrated in figure 2. The distribution of stage and anatomical location of the lesions are listed in online supplementary tables S2 and S3.
IC rates of the whole cohort and subjects with negative colonoscopy in relation to various factors
{kind=link}
{kind=link}
Risk of colonoscopy interval cancer (IC) in association with FHbC. (A) Overall cumulative risk of colonoscopy IC in the whole study cohort. (B) Cumulative risk of colonoscopy IC in subjects with negative index colonoscopy. FHbC, faecal haemoglobin concentration (unit: μg Hb/g faeces).
The attributable proportion of colonoscopy IC with various aetiologies was 1.9% (2/105) for colonoscopy IC caused by incomplete resection, 84.8% (89/105) for colonoscopy IC caused by missed lesion and 13.3% (14/105) for colonoscopy IC caused by newly developed cancer.
Multivariable analysis
The results of the Poisson regression analysis are illustrated in table 3. It showed that subjects with older age (aRR=1.49, 95% CI 1.09 to 2.04), subjects that received colonoscopy in settings with ADRs lower than 15% (aRR=3.09, 95% CI 1.55 to 6.18), subjects with non-advanced adenoma only (aRR=1.52, 95% CI 1.06 to 2.18) and advanced adenoma (aRR=1.87, 95% CI 1.19 to 2.96) at initial colonoscopy were associated with increased risk of IC, and a stepwise increment in IC risk associated with increased FHbC, with aRR ranging from 1.48 (95% CI 0.93 to 2.37) in those with 50–99 μg Hb/g faeces, 2.55 (95% CI 1.52 to 4.29) in those with 100–149 μg Hb/g faeces, to 2.74 (95% CI 1.84 to 4.09) in those with 150 μg Hb/g faeces or greater.
Association of various risk factors and interval cancer after colonoscopy in study population
In subjects with negative colonoscopy, receiving colonoscopy in settings with ADRs lower than 15% was still the strongest risk factor of colonoscopy IC (aRR=3.61, 95% CI 1.33 to 9.81) and a stepwise increment in IC risk, along with increased FHbC, was also observed, with aRR ranging from 1.58 (95% CI 0.85 to 2.92) in those with 50–99 μg Hb/g faeces, 2.45 (95% CI 1.20 to 5.02) in those with 100–149 μg Hb/g faeces, and 2.88 (95% CI 1.70 to 4.90) in those with 150 μg Hb/g faeces or more after adjustment for other conventional risk factors. The cross-validation based on the two-thirds derivation data set and a third validation data set showed no significant difference between the observed and predicted numbers of colonoscopy IC (p=0.76) (see online supplementary table S4).
Discussion
While quality of colonoscopy and FHbC have been investigated simultaneously using large Taiwanese population-based screening for CRC with FIT, we confirmed inadequate quality of colonoscopy (such as low ADR) is still the main cause responsible for the risk of IC. We also demonstrated that FHbC, independently of quality of colonoscopy, is also a significant predictor for IC in subjects who received complete colonoscopy after positive FIT in this Taiwanese Nationwide Screening Program. Both findings are supported by the results that the incidence of IC was the highest in those with ADR lower than 15% followed by high FIT level. It would not be surprising to confirm the important contribution to IC as a result of inadequate quality of colonoscopy in a population-FIT-based screening programme. The novel finding in our study is pertaining to the independent role of FIT level played in occurrence of IC. We found that in addition to the established factors such as ADR, age and the presence of neoplasms at the baseline colonoscopy, FHbC was positively associated with subsequent risk of developing IC. Moreover, even in the subjects with negative colonoscopy, a high baseline FHbC was also associated with a significantly higher risk of developing IC in the subsequent years. Our results are consistent with previous studies demonstrating the significance of conventional risk factors, and shed a light on finding a solution for identifying subjects who are at risk of colonoscopy IC. We believe that the findings of this study can be used to adjust screening logistics in order to improve the effectiveness of CRC screening programmes. IC after colonoscopy is attributable mainly to two possible mechanisms: operational (endoscopic or clinical setting) and biological (patient or neoplasm) factors.26 Recognition of operational factors is important because they may be addressed, perhaps with improved logistics of screening. Previous studies on colonoscopy IC, or the so-called postcolonoscopy CRC, have demonstrated some operational risk factors that were associated with the risk of colonoscopy IC: population studies from Canada and USA showed that the completion rate of colonoscopy, polypectomy rate, hospital level and endoscopist specialty were associated with the risk of colonoscopy IC.8 ,10 ,27–29 A study from Germany showed that colonoscopy-related factors (incomplete examination, incomplete resection of neoplasms and poor bowel preparation) accounted for 41.1% of developing CRCs after colonoscopy.30 Recent studies have also shown that a low ADR of individual endoscopists is an independent risk factor for colonoscopy IC.11 ,13 These operational factors are identifiable and modifiable through monitoring or auditing of endoscopy personnel and techniques. Various quality indicators and benchmark thresholds have been proposed in national and professional society guidelines.31–33 The other potential explanation for the occurrence of IC is pertaining to biological factors. Previous studies have shown that subjects with baseline findings of advanced neoplasm or more than three synchronous neoplasms were more likely to have incident advanced adenoma or invasive cancer in the subsequent years.34–36 Regarding biological factors, certain subcategories of colorectal neoplasms are more difficult to detect by colonoscopy and/or carry a higher risk of invasiveness and progression than do others. Studies from Japan and the US veteran population, and our prior study, have shown that non-polypoid neoplasms carry a significantly higher risk of unfavourable histology and invasiveness at a relatively smaller size than do polypoid neoplasms.37–39 Another subcategory of the lesion, the sessile serrated adenoma, has recently attracted attention since it may be responsible for as high as 28% of colonoscopy ICs.40 Those lesions are more difficult to be detected during colonoscopy, even if they have already become invasive, owing to the non-polypoid and subtle morphology and detection of such subtle lesions requires complete and high-quality colonoscopy, and, although their contribution to the incidence of ICs and tendency to bleed remains unclear, early invasive cancers arising from such lesions might be missed on initial colonoscopy. According to the results of this study, after controlling for the aforementioned operational factors, we found a stepwise increment of the risk of developing IC along with the increased level of FHbC. Such an association can be caused by either operational or biological factors. Our ancillary analysis showed that the higher the level of FHbC, the higher the likelihood of detecting advanced adenoma or invasive cancers, which is consistent with a previous Dutch study conducted by Hol et al17 (see online supplementary table S1). The highest incidence of IC was observed in the lowest ADR setting followed by those with high baseline FHbC (table 2), and a similar trend in the multivariate analysis (table 3); it is therefore reasonable to speculate that certain significant neoplasms might have been missed at index colonoscopy in subjects with high baseline FHbC levels even if colonoscopy yielded negative or only non-significant finding. Our speculation is also supported by the estimation of an attributable proportion of 84.8% for colonoscopy ICs being caused by missed lesions.
Our finding on FHbC as a predictor for IC may provide a potential opportunity for applying FHbC to screening programmes under the current quality-monitoring (ADR) or risk stratification (index colonoscopy finding) framework. This might be accomplished by intensive referral of cases with high FHbC values (above 150 μg Hb/g of faeces) to hospitals or endoscopists with better performance (high complete colonoscopy rate, high ADR) where there may be a lower risk of IC after colonoscopy. We can also consider offering a second-look colonoscopy for those who had high FHbC even after a complete colonoscopy with negative or non-significant findings. As a third of our FIT-positive subjects (equivalent to 1–2% of the overall screening population) had FHbCs above this level, tailored referral of this subgroup of subjects or offering second-look colonoscopy seems feasible, taking into account the overall FIT-positive rate of 4% in our programme, although accessibility or geographical barriers may need to be overcome. In this context, offering second-look colonoscopy for at least those subjects with poor bowel preparation or incomplete exam at the initial colonoscopy with very high FHbC may help capture missed lesions but minimise the stress put on the currently constrained colonoscopy capacity. In addition, another FIT before the next round of screening may be prescribed for this subgroup of subjects, thus increasing the chance of triggering another colonoscopy. This approach is also applicable to colonoscopy-based screening programmes by adding a FIT within the colonoscopy surveillance interval, an addition that may help in detecting missed or incompletely resected advanced neoplasms as reported by Lane et al.41 Finally, as demonstrated by the current study, missed lesions comprise more than 80% of colonoscopy ICs, implementation of quality certification for all participating colonoscopists for screening colonoscopy and regular audit of important quality indicators under the framework of screening programme, is crucial. Further cooperation of the professional societies and the government is mandatory.
Our study has several strengths. First, its large population of subjects participating in a nationwide screening programme provides sufficient power and more accurate estimation of the IC risk by various factors. Second, all FITs were conducted in accredited laboratories under regular audit, and all FHbC measurements were stored in the government's central database. Third, we conducted separate analyses on a negative colonoscopy cohort, so the results can be applied to colonoscopy-based screening programmes as well as to FIT-based programmes. High FHbC may imply the existence of undetected advanced neoplasms or even invasive cancers, and dedicated management of those cases may facilitate prompt detection of these significant lesions and improve the effectiveness of the screening programme. Finally, all colonoscopy ICs were identified based on the National Cancer Registry, which was linked to our screening database and has a coverage rate of 98.6%.
Our study has several limitations also. First, although we standardised the two FIT kits in terms of μg Hb/g of faeces, as recommended by the international expert working group, the two kits may not be equal in detectability of cancer or precancerous lesions.20 ,42 Second, we used hospital-level ADR as the surrogate for variations in endoscopists’ performance, although this criterion likely does not fully reflect the performance of each individual endoscopist. Results from more objective characterisation of endoscopist and colonoscopy quality, such as endoscopist-level ADR and quality of bowel cleansing, are warranted and may provide useful clues for intervention. In our programme, all endoscopists performing colonoscopy for FIT-positive subjects are now obligated to report the findings using a standardised reporting format, which includes several necessary items relevant to quality indicators. A regular monitoring system of colonoscopy quality indicators is also under construction now and further improvements can also be anticipated in the future. Third, we included only subjects with complete colonoscopy in our analysis to highlight the potential role of FHbC in warning that significant neoplasm might have been missed even after a thorough colonoscopy. It is, however, intriguing to know whether FHbC could also play a role to put up a red flag among FIT-positive subjects with incomplete colonoscopy. We demonstrated the results of the ancillary analysis by including subjects with incomplete colonoscopy (see online supplementary table S4) and it showed similar results even controlling for completeness of colonoscopy. Finally, one may argue that the FHbC is just the result of bleeding from neoplastic lesions that were detected at the index colonoscopy, and the association between FHbC and the risk of future colonoscopy IC can be explained simply by the endoscopic findings per se. However, our results revealed significant impact of FHbC after controlling for various endoscopic factors. We speculate that the high value of FHbC may not be caused only by detected neoplasms, but also by undetected significant neoplasms including invasive cancer in subjects who had negative or only non-advanced neoplasms detected at index colonoscopy. Moreover, in the analysis of the subjects with negative colonoscopy, we observed a similar association of FHbC and subsequent risk of colonoscopy IC, which further support our speculation.
In summary, we corroborated from the FIT-based population screening programme that inadequate colonoscopy quality (indicated by lower ADR) is still the main cause responsible for the risk of colonoscopy IC, and FHbC, independently of quality of colonoscopy, is also a significant predictor for IC in subjects who received complete colonoscopy after positive FIT. In addition to a generalised quality control plan or audit action, the results showed that dedicated FHbC-based management of screenees may be helpful and can be applied to adjust screening logistics in order to decrease ICs and improve the effectiveness of CRC screening programmes.
Acknowledgments
The authors thank the clinicians, endoscopists and public health workers in the individual municipalities who participated in this nationwide colorectal cancer screening programme. The authors also thank professor Hsiu-Hsi Chen for providing constructive advice during the process of study design and data analysis.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
The preliminary results of this study were presented during the Research Forum, Digestive Disease Week 2014 (May 6, 2014, Chicago, Illinois, USA; Abstract # 1896191).
Contributors Conception and design of the study: SY-HC, H-MC, Y-CL, S-LC, SL-SC, AM-FY, JC-YF; generation, collection, assembly, analysis and/or interpretation of data: H-MC, S-LC, SL-SC, AM-FY, SY-HC, D-CC and JC-YF; drafting or revision of the manuscript: SY-HC and H-MC; critical revision of the manuscript for important intellectual content; approval of the final version of the manuscript: all authors; administrative, technical or material support: S-LC, SL-SC, H-MC, AM-FY, SY-HC, JC-YF, D-CC, Y-CL, M-SW, C-KC, W-FH and S-TC; study supervision: H-MC; H-MC had the final responsibility for the decision to submit for publication.
Funding This study was supported by the Health Promotion Administration, Ministry of Health and Welfare (A1011119 and A1021227), and Ministry of Science and Technology (MOST 102-2314-B-182-028-MY3). The funding source had no role in study design, data collection, analysis, or interpretation, report writing, or the decision to submit this paper for publication.
Competing interests None declared.
Ethics approval This study was approved by the Health Promotion Administration of the Ministry of Health and Welfare prior to data retrieval and analysis.
Provenance and peer review Not commissioned; externally peer reviewed.