Article Text

Abstract
Introduction The annual cost of alcohol related harm in the UK is 2.7 billion, 78% of which is for acute care (20% and 40% for hospital and A and E admissions respectively)1. Alcohol harm cost NHS Surrey £73m annually with a higher spend per adult than national and regional levels1. Admissions to hospital for alcohol related conditions in Surrey was 12 079 per 1 00 000 (2014/15)2. To address local issues, an alcohol liaison service (ALS) was introduced in 2014. ALS has a prominent role in the education of fellow health care practitioners and in the clinical care of patients with alcohol issues. Here we describe our experience and outcomes
Method The introduction of the ALS prompted a shift in practice in our hospital from fixed dose chlordiazepoxide reducing regimen for all patients at risk of alcohol withdrawal lasting at least 5 days to introduce the CIWA scoring regimen. This was followed by a tailored reducing course calculated on initial dose required to control symptoms. A program of education, training and regular team debriefs allowed a successful transition. Patients with alcohol related presentation are referred to ALS at admission with all requiring CIWA scoring reviewed. There are close links with community teams to foster a seamless transition for those requiring urgent support. Both prospective and retrospective data on all inpatient detoxes and referrals to this service was collected through each clinical encounter and medical records respectively
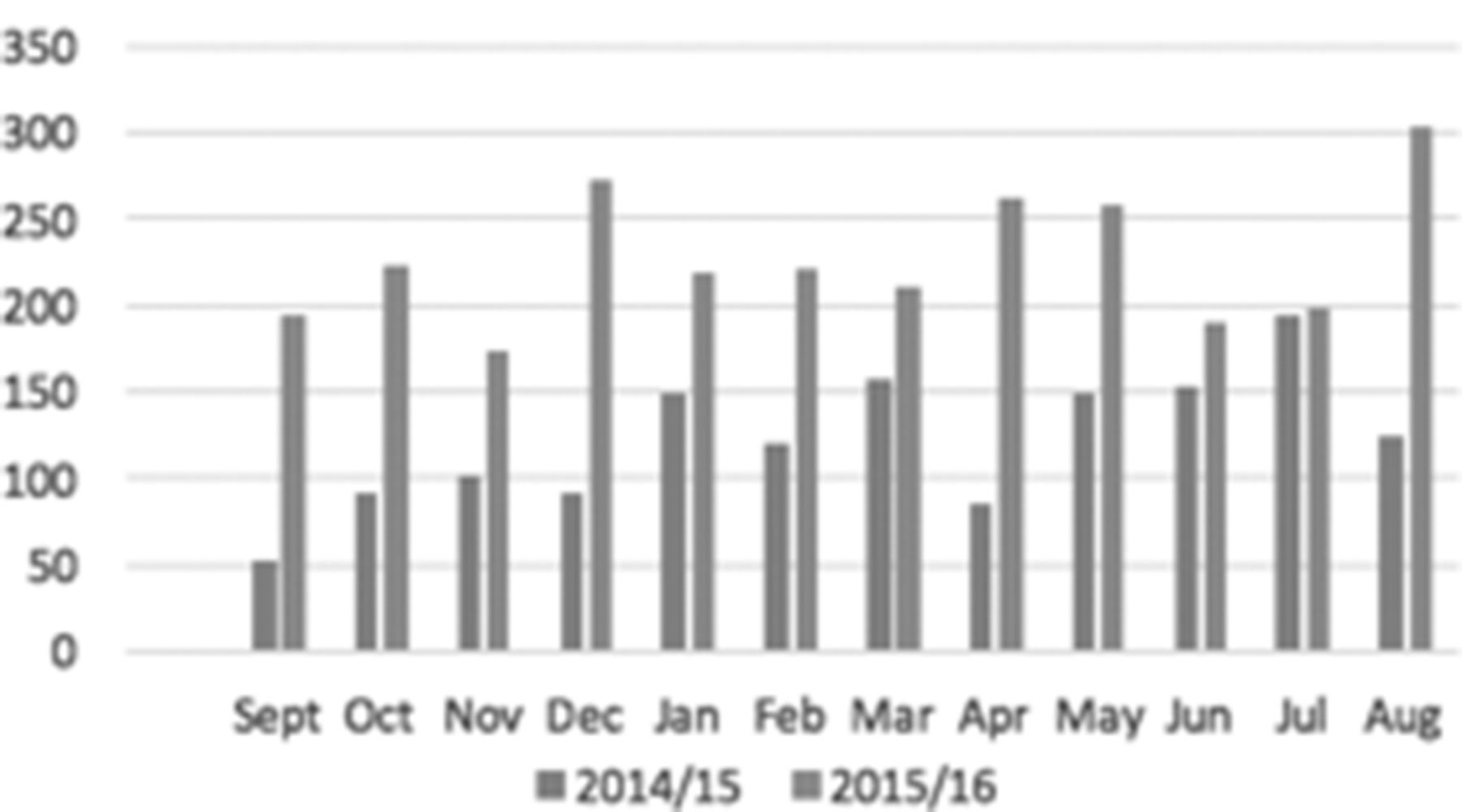
Results The number of referrals received has increased in the 2 years of this service (Fig 1). Data on need for full detox after initial CIWA and length of stay (LOS) [Table 1] reflects the growing presence of the ALS in acute services. We have shown that those admitted with primarily medical problems require, on average, a shorter detox.
{kind=link}
Conclusion The ALS has been successful in changing trust policy and facilitating early discharge without detox where appropriate and reducing length of stay for those with primary alcohol presentations. These patients can now be seen in the ALS dedicated out patient clinic for ongoing support. Interestingly, our results show that patients admitted for non alcohol related problems receive less intense detox compared to their counterparts. This observation merits further study to explore the contributing factors to this. Our future work will also focus on developing care plans for frequent attenders to minimise number of admissions.
References
. National Health Intelligence Service (NHiS) Ltd2014: Alcohol Impact Model
. Local Alcohol Profile - Surrey2017, Public Health England
Disclosure of Interest None Declared
- alcohol misuse