Article Text

Statistics from Altmetric.com
Clinical presentation
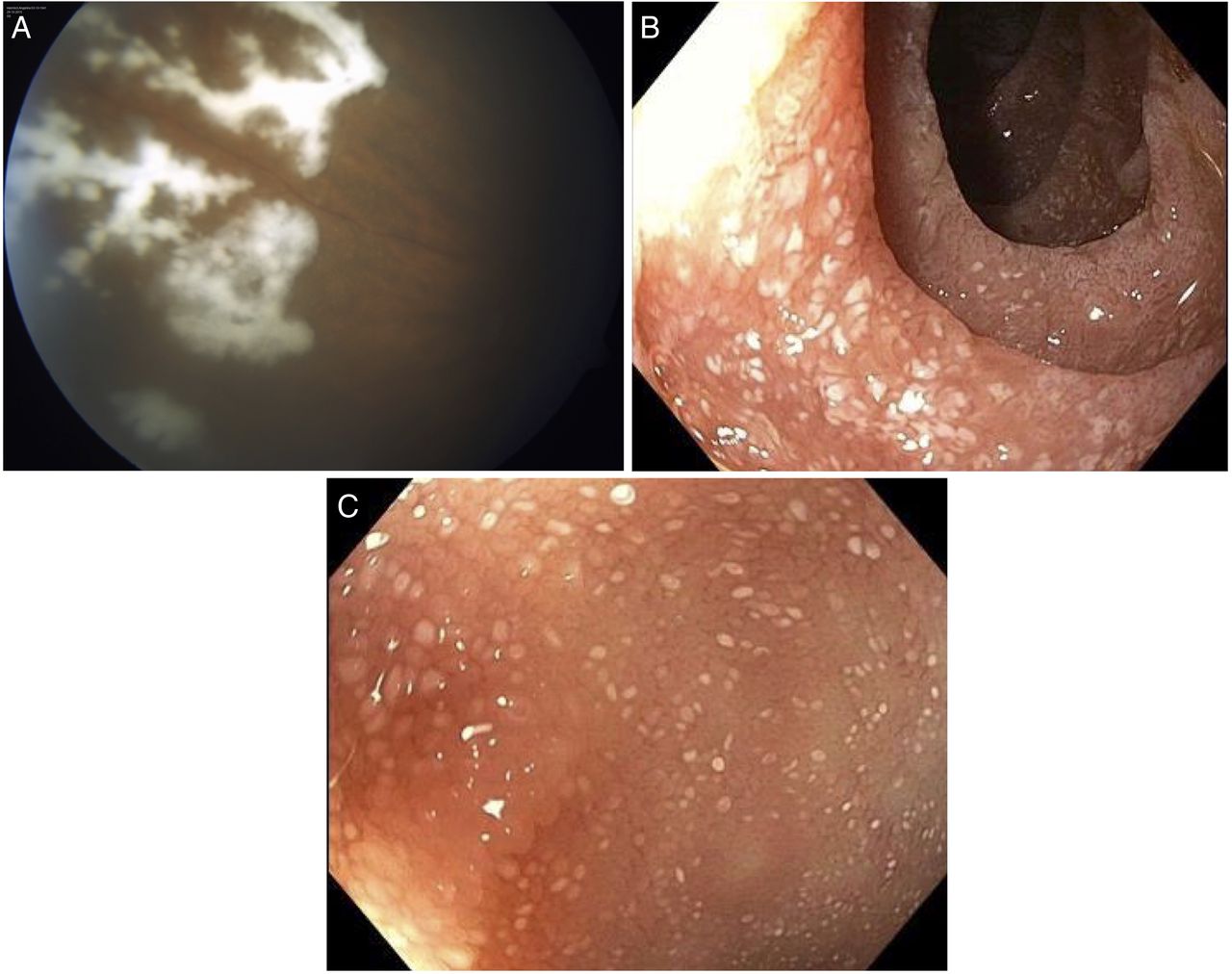
A 74-year-old woman was admitted to the ophthalmology department with progressive vision loss, vitreous clouding and suspected endogenous endophthalmitis. Bilateral eye problems had started several weeks before and grew worse under oral prednisolon therapy. After admission, progressive vitreous haze was diagnosed (figure 1A). A diagnostic vitrectomy was performed for microbiological testing.

Assessment of the left eye before vitrectomy. Preretinal ‘white material’ was visible on ophthalmoscopy within the vitreous cavity (A). Endoscopic view into the second part of the duodenum (B) and the terminal ileum (C), showing ragged erythematous mucosa and lymphangiectasia.
The patient was also presented with watery diarrhoea that had started 6 months ago. Bowel movements were independent of food ingestion and occurred also during the night; furthermore, the patient reported weight loss of 6–7 kg, epigastric pain, latent nausea and deterioration of general well-being. An incomplete gastroenterological assessment had been performed elsewhere, including microbiological testing of stool samples, blood tests, chest X-ray, abdominal CT and colonoscopy without intubation of the terminal ileum. Apart from microcytic anaemia (haemoglobin level=8.2 g/L; mean corpuscular volume=76.0 fl), there had been no pathological findings.
Over the last 20 years, the patient had been treated with immunosuppressants (methotrexate, ethanercept, tocilizumab) for seronegative polyarthritis that necessitated knee replacement in 2006. Treatment with tocilizumab was stopped 2 months before admission at our hospital, but a prednisolone maintenance therapy was continued throughout and even increased to treat the deteriorating uveitis.
An oesophagogastroduodenoscopy and ileocolonoscopy were performed (figure 1B, C).
Question
What is the diagnosis, and how was it confirmed?
Answer
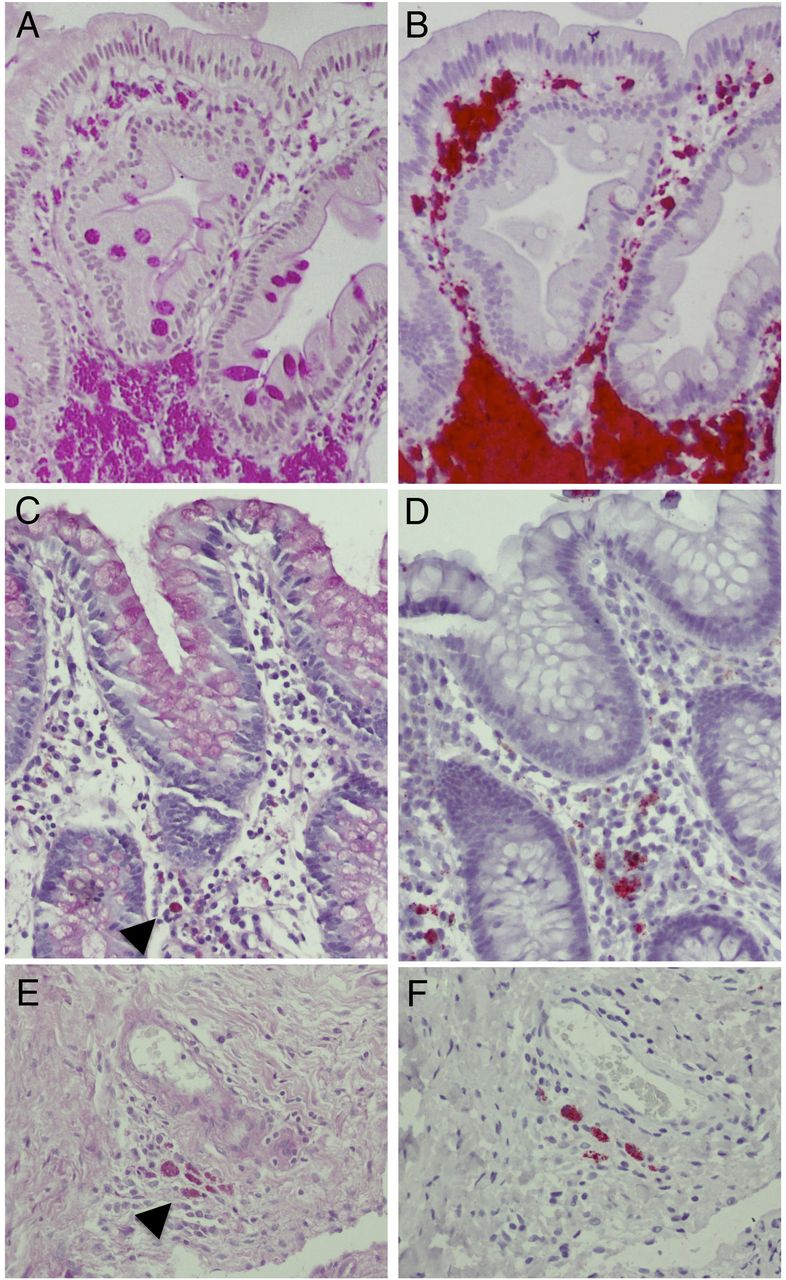
Ragged erythematous intestinal mucosa and lymphangiectasia are macroscopic signs of Whipple's disease. Histological examination of duodenal biopsies revealed villus atrophy with patchy periodic acid–Schiff (PAS) staining, most prominent in the submucosa (figure 2A, C), and verification by positive Tropheryma whipplei-specific immunostaining (figure 2B, D).
{kind=link}
{kind=link}
Periodic acid–Schiff (PAS) staining (A, C and E) and Tropheryma whipplei-specific immunohistochemistry (B, D and F) in duodenum biopsies (A–D) at the time of diagnosis and a synovial biopsy (E and F) of the left knee taken 9 years before. Panels A and B show strong staining with sickle particle-containing (SPC) cells typical for initial diagnosis of Whipple’s disease, while panels C and D display a biopsy with only faintly stained macrophages demonstrating the patchy affection of the tissue. Faintly stained PAS-positive areas are indicated by arrowheads, and positive anti-T. whipplei immunostaining appears in bright red. Histological changes consistent with Whipple's disease were also found in biopsies taken from the terminal ileum (not shown).
However, positive PCR and sequencing for T. whipplei-specific 16S rDNA from the vitrectomy specimen established the diagnosis even before this.
Symptomatic eye involvement, mostly uveitis, is rare in Whipple's disease. Approximately 40 cases have been described in the literature.1 ,2 It is indicative for central nervous system (CNS) involvement in our case. CNS involvement is frequent in Whipple's disease:3 In our cohort of 222 patients in Berlin, 22% presented with neurological symptoms and 42% had positive PCR findings from cerebrospinal fluid. However, only one additional presentation with T. whipplei uveitis (without vision loss) was observed in our cohort.
Long-standing seronegative arthralgia is often the first symptom of Whipple's disease and may precede other manifestations for years:4 in our case, retrospectively, T. whipplei was found to be present in a synovial specimen from left knee replacement surgery performed 9 years before the current presentation (figure 2E, F).
Our patient was treated with intravenous ceftriaxone for 2 weeks and is currently under a 1-year regimen of cotrimoxazole (twice daily) orally. In accordance with our general experience, treatment resolved the diarrhoea quickly, the patient gained weight and joint problems were reduced.
Footnotes
KHW and UP contributed equally.
Contributors UBB and KHW: wrote and designed the manuscript and figures; UP: provided the ophthalmological care and image; AF: performed the endoscopies; VM and TS: performed histological staining and provided data from their patient cohort; TM: coordinated the diagnostic steps.
Competing interests None.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.