Article Text

Abstract
Objective Outside clinical trials, the effectiveness of chromoendoscopy (CE) for long-standing IBD surveillance is controversial. We aimed to assess the effectiveness of CE for neoplasia detection and characterisation, in real-life.
Design From June 2012 to 2014, patients with IBD were prospectively included in a multicentre cohort study. Each colonic segment was evaluated with white light followed by 0.4% indigo carmine CE. Specific lesions' features were recorded. Optical diagnosis was assessed. Dysplasia detection rate between expert and non-expert endoscopists and learning curve were ascertained.
Results Ninety-four (15.7%) dysplastic (1 cancer, 5 high-grade dysplasia, 88 low-grade dysplasia) and 503 (84.3%) non-dysplastic lesions were detected in 350 patients (47% female; mean disease duration: 17 years). Colonoscopies were performed with standard definition (41.5%) or high definition (58.5%). Dysplasia miss rate with white light was 40/94 (57.4% incremental yield for CE). CE-incremental detection yield for dysplasia was comparable between standard definition and high definition (51.5% vs 52.3%, p=0.30). Dysplasia detection rate was comparable between expert and non-expert (18.5% vs 13.1%, p=0.20). No significant learning curve was observed (8.2% vs 14.2%, p=0.46). Sensitivity, specificity, and positive and negative predictive values for dysplasia optical diagnosis were 70%, 90%, 58% and 94%, respectively. Endoscopic characteristics predictive of dysplasia were: proximal location, loss of innominate lines, polypoid morphology and Kudo pit pattern III–V.
Conclusions CE presents a high diagnostic yield for neoplasia detection, irrespectively of the technology and experience available in any centre. In vivo, CE optical diagnosis is highly accurate for ruling out dysplasia, especially in expert hands. Lesion characteristics can aid the endoscopist for in situ therapeutic decisions.
Trial registration number NCT02543762.
- DYSPLASIA
- COLORECTAL CANCER
- ULCERATIVE COLITIS
- INFLAMMATORY BOWEL DISEASE
- COLONOSCOPY
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
Due to the increased risk of dysplasia and colorectal cancer in patients with long-standing IBD, endoscopic surveillance is strongly recommended.
Most neoplastic lesions are endoscopically visible, therefore, targeted biopsies strategy has replaced the classical multiple random biopsies policy for surveillance purposes.
Randomised trials have demonstrated that chromoendoscopy (CE) is superior to white-light endoscopy for the detection of dysplasia
Real-time optical diagnosis has demonstrated its effectiveness for histology prediction in diminutive colorectal tumours.
What are the new findings?
CE with targeted biopsies is superior to white-light endoscopy for dysplasia detection even outside clinical trials.
In vivo optical diagnosis with CE is highly accurate for ruling out dysplasia, especially in expert hands.
Lesions located in the proximal colon, with protruding morphology, loss of innominate lines and neoplastic Kudo pit pattern should be considered as potentially dysplastic.
How might it impact on clinical practice in the foreseeable future?
Our results support the implementation of CE for UC and Crohn's colitis surveillance in clinical practice.
Lack of experience in CE should not be a limitation for its implantation in real-world practice.
The high accuracy of CE optical diagnosis can potentially achieve more cost-effective examinations, by reducing the number of unnecessary biopsies that may optimise the effectiveness of surveillance.
Introduction
The debate over the best method for colorectal cancer (CRC) screening in patients with long-standing IBD is still ongoing.
During the past few decades, mimicry of dysplasia along with the view that IBD-associated neoplasia may occur as a field effect has justified the strategy of screening based on random biopsies.1 Since the arrival of video endoscopes and newer endoscopic technologies such as chromoendoscopy (CE) and high-definition systems, it is now recognised that the majority of IBD-associated dysplasia is visible.2–4 Several randomised, controlled trials show a clear benefit of CE over white-light endoscopy in identifying IBD-associated dysplasia.5 ,6 A meta-analysis of prospective studies showed that the difference in dysplasia detection yield between CE and white light was 7% (95% CI 3.2% to 11.3%).7 Accordingly, many scientific societies currently recommend the use of pancolonic CE with targeted biopsies for IBD CRC surveillance.8–11
Despite compelling evidence from these studies, there is scant data on the effectiveness of this strategy in a clinical setting, outside of clinical trials. The recently published SCENIC consensus11 reinforces the placement of CE as the preferred technique for surveillance of dysplasia in IBD, although some authors12 question the acceptability of SCENIC statement, due to a lack of longitudinal data.
The only published multicentre study is a retrospective analysis from three referral centres in Netherlands over a 14-year period showing that the implementation of CE did not result in a significant increase in the detection of dysplastic lesions.13
Hence, whether the implementation of CE in a clinical setting could achieve the same advantages as previously derived from clinical trials is still unclear. Moreover, the learning curve for CE and its potential benefit in combination with high-definition colonoscopy have not been adequately addressed.
On the other hand, whereas real-time optical diagnosis has clearly demonstrated its effectiveness for differentiating adenomas from hyperplastic polyps in average CRC risk population,14 it has scarcely been studied in the specific setting of IBD. Real-time optical diagnosis can potentially improve the effectiveness of CE by reducing the number of unnecessary biopsies and optimising the endoscopic treatment of IBD-associated neoplasia.
We aimed at evaluating CE plus targeted biopsies strategy effectiveness and learning curve for detection and characterisation of IBD-associated dysplasia in a real clinical setting. Second, we attempted to identify specific endoscopic features that may aid the endoscopist for on-site characterisation of dysplasia.
Patients and methods
Study population and procedures
From June 2012 to June 2014, 15 Spanish centres prospectively recruited all patients aged 18 years or older with clinical, endoscopic and pathological proof of IBD that were referred for dysplasia screening. Eligibility criteria included:
UC proximal to the rectum and Crohn's disease (CD) or indeterminate colitis involving at least a third of the colonic mucosa.
Duration ≥8 years since disease diagnosis, or any duration in patients with concomitant diagnosis of primary sclerosing cholangitis.
Absence of clinical activity: non-invasive 6-point partial Mayo Score15 <3, CD Activity Index16 <150.
Exclusion criteria included: prior colonoscopy within the last 6 months, personal history of CRC, partial or total colectomy, coagulopathy and known allergy to indigo carmine.
Participating individuals completed a short questionnaire concerning their clinical history before undergoing endoscopic examination. Demographic data such as age, sex, cigarette smoking and concomitant primary sclerosing cholangitis or family history of CRC were ascertained.
Procedures were performed with high-definition systems (ie, 180/190 series in combination with EVIS EXERA II-III processors (Olympus, Tokyo, Japan), EC 390 LI scope in combination with Pentax processor (Pentax, Tokyo, Japan) and 590 WL and 590 ZW endoscopes in combination with Fujinon 4400/4450 processors (Fujifilm Medical Systems, USA) or with standard-definition systems (ie, CF-Q160L and CF-Q165L (Olympus, Tokyo, Japan) and Pentax EC 380 LKP (Pentax, Tokyo, Japan)).
Quality of bowel cleansing was graded by each endoscopist following the Boston Bowel Preparation Scale.17 Adequate preparation was defined as a total score ≥6 with no segments <2. Procedures in which the quality of preparation was inadequate were excluded.
Endoscopic disease activity was recorded by the endoscopist following the Mayo Endoscopic Subscore for UC18 and Simplified Endoscopic Activity Score for CD (SES-CD).18 All patients with moderate or severe endoscopic activity (ie, Mayo Endoscopic Subscore ≥2 or SES-CD >5) involving at least one colonic segment were excluded.
The colonoscope was advanced to the caecum. On withdrawal, each segment (ascending colon, transverse colon, descending sigmoid and rectum) was thoroughly washed with a saline solution mixed with N-acetylcysteine and dimethicone and was then scrutinised for lesions in two sequential passes: first, by careful examination with white light at first with maximal insufflation to detect colour changes and then, with minimal insufflation to detect small mucosal surface abnormalities; and subsequently, with CE. For CE, the SURFACE19 guidelines were followed: the lumen was sprayed in a segmental fashion using 0.4% indigo carmine delivered via a specially designed dye spray catheter (Olympus PW-5V1). After allowing a few seconds for the dye to settle onto the mucosal surface, excess pools of indigo carmine were suctioned and the mucosa was then scrutinised. Time to withdraw from the caecum was measured using a stopwatch.
Lesions detected by white light and/or CE were biopsied/removed after the second pass with CE. Moreover, two random biopsy samples were obtained from each segment to assess the presence of microscopic inflammation.
Colonoscopy features previously associated with IBD-associated dysplasia were collected. These comprised scarring, tubular colonic appearance, featureless colon, presence of postinflammatory polyps and colonic strictures.19 Patients were categorised as positive for a feature if any of the previous was documented at colonoscopy.
Endoscopists
Participating centres included both tertiary referral academic centres and local community hospitals.
Endoscopists completed a brief questionnaire designed to evaluate their degree of expertise. This included: adenoma detection rate, number of hours dedicated to endoscopy per week, number of procedures per year and previous experience in CE.
Before the study was initiated, a brief learning set of images incorporated into a slideshow (Microsoft PowerPoint 2003, Microsoft, Redmond, Washington, USA) with a short explanation of morphological characteristics of lesions was sent to all investigators.
Lesions
After indigo carmine staining, lesions were carefully inspected and morphological characteristics were recorded in a specific data sheet. This data sheet included 11 items previously selected from literature such as: size, location, morphology based on Paris classification,20 other specific morphology features (ie, regular or irregular shape, well or poorly demarcated borders, carpet lesion morphology), abnormal vascularisation, friability, ulcerated or velvety surface, disruption of innominate lines and Kudo pit pattern when possible.21 Lesion shape was grouped into protruding (pedunculated—Paris 0–Ip or sessile—Paris 0–Is) and flat lesions (Paris 0–II and laterally spreading tumours—LST) and Kudo pit pattern was subdivided into non-neoplastic (Kudo I and II) and neoplastic (Kudo III–V).
Investigators were asked to make a prediction of the lesion histology prior to resection, based on seven categories: CRC, sporadic adenoma, dysplasia associated lesion or mass (DALM), adenoma like dysplasia (ALM), pseudopolyp, hyperplastic polyp or ‘other’ (scarring changes, quiescent inflammation or normal mucosa). Furthermore, investigators were asked to classify lesions as endoscopically resectable or unresectable. For analysis purposes optical diagnoses were grouped into two groups: dysplasia (including CRC, sporadic adenoma, DALM and ALM) and non-dysplasia (including pseudopolyp, hyperplastic polyp and other).
All detected lesions were removed irrespective of the histology presumption. Only polyps ≤4 mm in the rectosigmoid colon that were ascertained as hyperplastic polyps and those clearly suggestive of pseudopolyps were not removed. Lesions <5 mm were resected using biopsy forceps. Pedunculated polyps or sessile polyps ≥5 mm were resected using polypectomy snare. Protruding non-pedunculated polyps and flat lesions ≥5 mm were resected by endoscopic mucosal resection technique. After lesion removal, two samples were obtained at perilesional mucosa to rule out surrounding and/or multifocal dysplasia.
Histology was used as the gold standard. Biopsies were processed and stained using standard methods, and were subsequently evaluated by experienced GI pathologists. Neoplastic changes were classified according to the Vienna classification.22 Histological outcome was classified into: normal, inflammation, hyperplasia, low-grade dysplasia (LGD), high-grade dysplasia (HGD) or adenocarcinoma. The HGD group included intramucosal carcinoma and carcinoma in situ.
Although no histology centralised review was performed, all specimens showing dysplasia were revised by an independent pathologist, and in the event of interobserver disagreement a consensus was reached.
For analysis purposes, only those lesions located within diseased areas were included and classified into two groups: (1) Dysplasia, which included: LGD, HGD and invasive carcinoma and (2) Non-dysplasia, which included: hyperplastic polyps, sessile serrated polyps without dysplasia, pseudopolyps, scarring tissue, and other unspecific and non-neoplastic mucosal changes.
Outcome measures
Endoscopist experience and learning curve
Endoscopists were classified into two groups according to their previous experience in CE technique: (1) CE-expert group: composed of endoscopists who had performed ≥20 previous CE-based IBD surveillance procedures and (2) CE-non-expert group: composed of endoscopists with scarce (<10 procedures) or no prior experience in CE technique. Learning curve was evaluated among the CE-non-expert endoscopists who performed at least 20 consecutive procedures during the 2 years of inclusion period.
Dysplasia detection yield and dysplasia detection rate
Dysplasia detection yield was defined as the proportion of lesions containing dysplasia or invasive CRC in relation to the total number of biopsied/removed lesions. This parameter was used to compare white-light effectiveness and CE effectiveness.
Dysplasia detection rate was defined as the proportion of patients who had at least one dysplastic lesion or invasive CRC in relation to the total number of screened patients. This parameter was used to evaluate the role of experience and the learning curve.
Statistical analysis
Statistical analysis was performed using SPSS V.20.0 (IBM, Somers, New York, USA). Quantitative variables were expressed as medians and IQRs, or means± SDs. Categorical variables were expressed as total number and frequencies (%). Quantitative variables were analysed using the Student's t-test or Mann-Whitney test, and qualitative variables were analysed using the χ2 test. Univariate binary logistic regression was performed for selecting variables associated with the presence of IBD-associated neoplasia. For multivariable logistic regression analyses, only candidate variables with p values ≤0.05 on univariate analysis were used in the final multivariate model. We included ORs with 95% CIs to quantify the magnitude of the association. Diagnosis accuracy and CI for all features were derived from 2×2 tables. Outcome parameters were sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV) and overall accuracy.
Results
Patients and procedures
A total of 350 patients were included in the study. Study flow chart is represented in figure 1. Detailed demographic and clinical patients’ characteristics are shown in table 1. A majority of patients had UC (78%) and extensive disease (83.1%). The vast majority (70.3%) presented with at least one high-risk feature for IBD-associated dysplasia23 (ie, primary sclerosing cholangitis, first-degree family history of CRC <50 years old and/or extensive colitis with previous severe activity). Nineteen (5.4%) patients had a personal history of dysplasia. In all of them, dysplastic lesions had been removed by endoscopy.
Baseline demographic and clinical characteristics of all patients
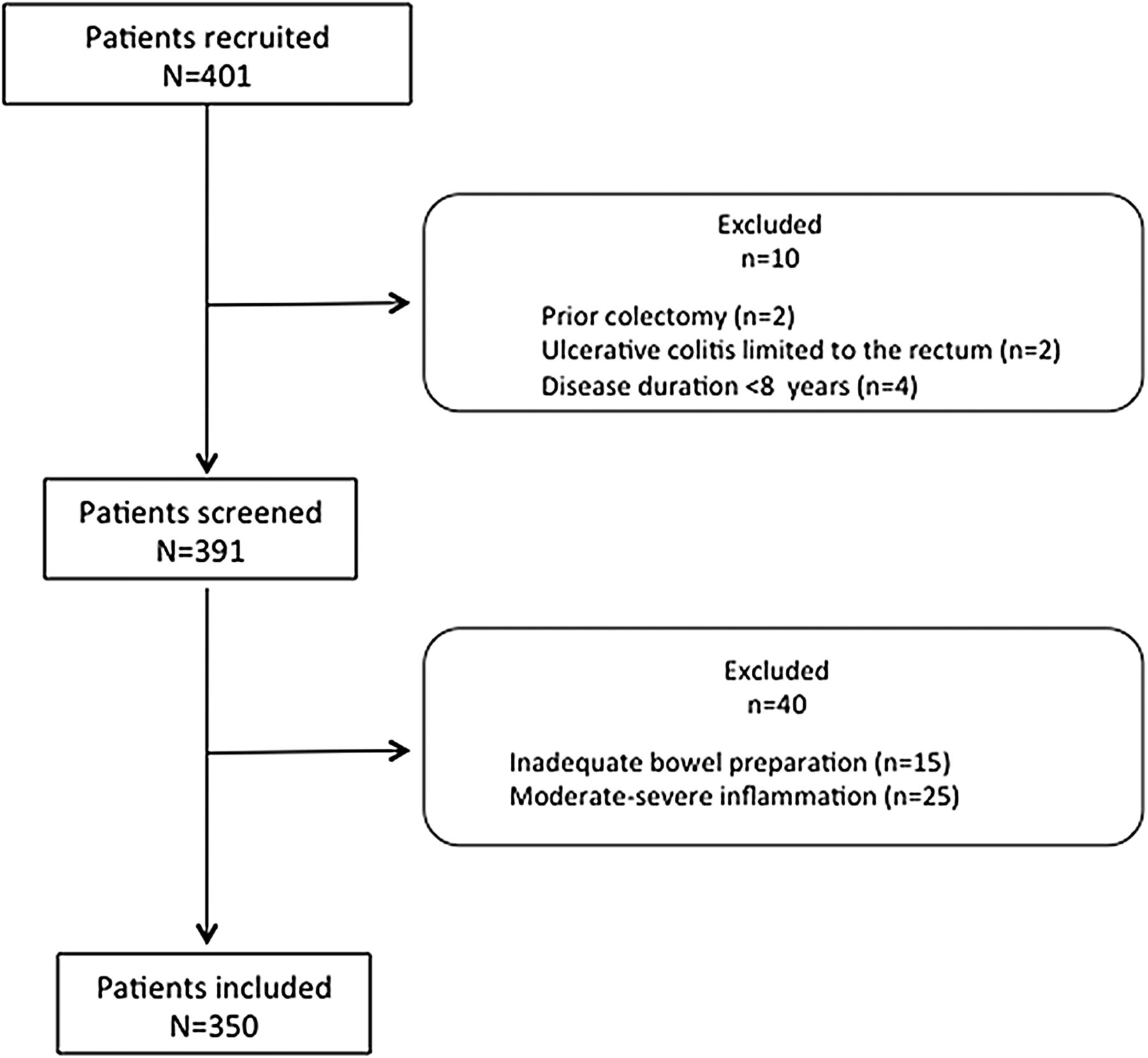
Flow chart of patients evaluated for the study.
At the time of screening colonoscopy, 185 (52.8%) patients were treated with oral aminosalicylates, 81 (23%) with immunomodulators, 27 (0.7%) with antitumour necrosis factor therapy and 57 (23.5%) with combination therapy.
Colonoscopies were performed with standard-definition scopes in 145 cases (41.5%) and with high-definition scopes in 205 (58.5%). Regarding colonic appearance: 178 (51%) patients presented with scars, 129 (37%) presented with pseudopolyps, 72 (20.6%) had a tubular colon, 54 (12.8%) had a featureless colon and 24 (7%) colonic strictures.
In 213 (61%) patients at least one lesion was biopsied or removed. The median of lesions biopsied/removed per patient was 2 (1–4).
Endoscopists
Fifteen gastroenterologists from different hospitals participated in the study, 11 from tertiary academic hospitals and 4 from local community centres. A median of 19 (14–30) patients were screened per endoscopist.
Endoscopists had previously performed a median of 800 (IQR: 600–900) procedures per year and their median adenoma detection rate in symptomatic, CRC surveillance or positive faecal immunological test patients was 41% (IQR: 36–47). Previous experience in IBD screening among endoscopists was variable: six (40%) had previously performed ≥20 IBD-screening procedures using CE-targeted biopsies, six (40%) had never performed CE but had performed ≥20 not supervised IBD-screening endoscopies using white-light and random biopsies, and three (20%) did not have any previous experience in IBD screening (see online supplementary table S1).
supplementary tables
Lesions
From a total of 637 lesions, 40 were excluded as they were located in non-affected segments of the colon (ie, patients with left-sided colitis or proctosigmoiditis). Thus, 597 lesions were included in the analysis (see figure 2). Morphological and histological lesion characteristics are shown in table 2. Main characteristics of lesions detected by white-light endoscopy and CE are represented in online supplementary table S4.
Baseline endoscopic and histological lesion characteristics
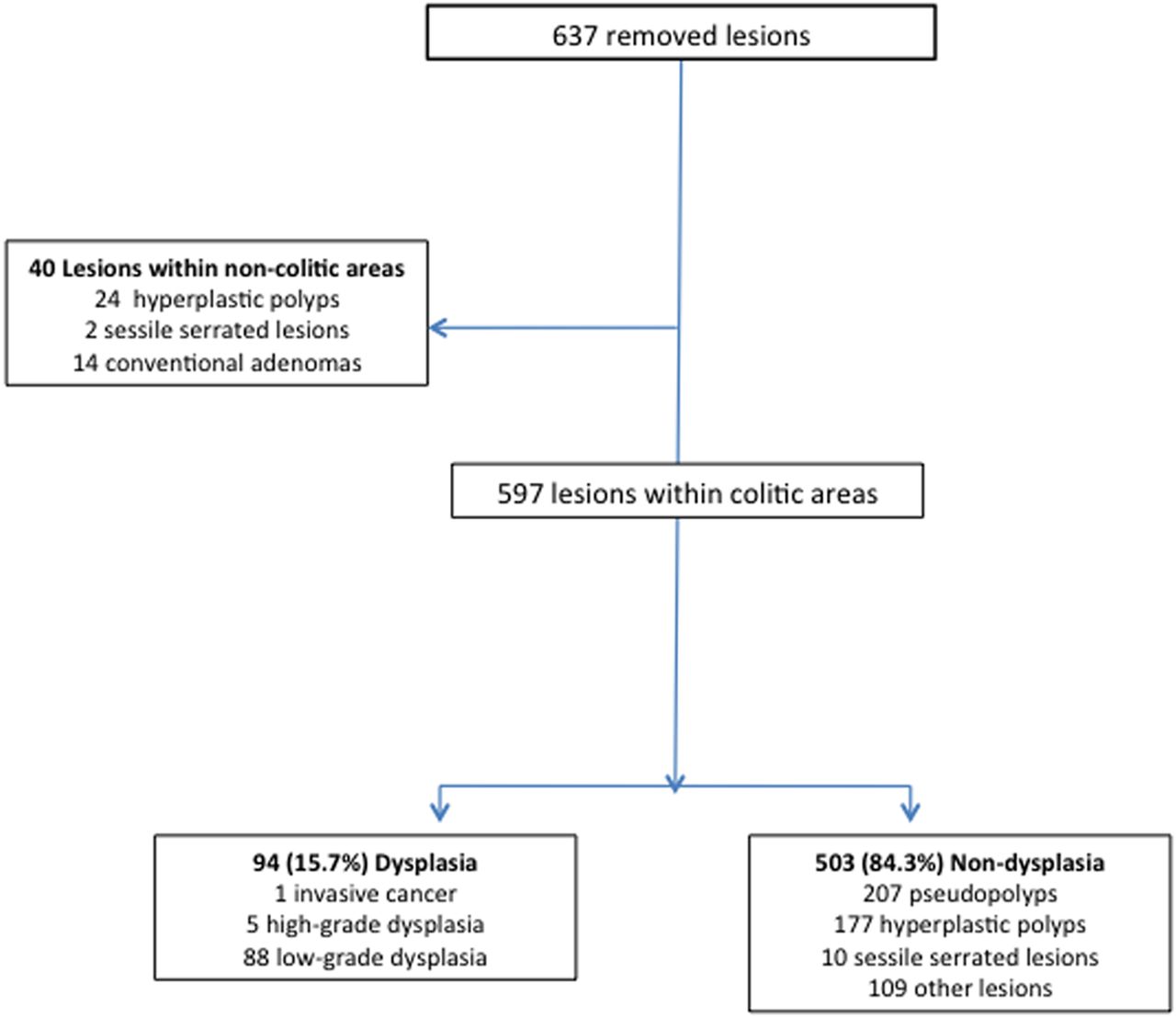
Flow chart and classification of removed lesions.
Ninety-four out of 597 lesions harboured dysplasia resulting in a dysplasia detection yield of 15.7%.
Among these 94 dysplastic lesions: 88 had LGD, 5 HGD and 1 was an invasive CRC. All the lesions with HGD were polypoid, well demarcated and were completely removed by endoscopy. Within the 88 lesions with LGD, 53 (60%) were polypoid and the rest were flat. All of them were removed by endoscopy except one: a 30 mm LST detected in a 35-year-old woman with pancolonic disease. This poorly demarcated lesion was located within a postinflammatory stenotic area. Kudo pit pattern was unable to be assessed. The lesion was considered unresectable and the patient was referred for surgery. Surgical specimen confirmed the diagnosis of LGD.
One invasive CRC was observed in a 40-year-old man who had been diagnosed with extensive UC at 14 years of age. This CRC was identified within a well defined 10 mm depressed lesion (Paris 0–IIc) with Kudo V pit pattern. The patient underwent a total colectomy with ileorectal anastomosis. Surgical specimen showed a pT1N0 adenocarcinoma.
As for non-targeted biopsies, neither perilesional samples nor random samples obtained to assess inflammatory activity showed dysplasia.
All patients with a dysplastic lesion that was completely removed by endoscopy were submitted to a 6–12-month surveillance CE, following our national guidelines. After 2–4 years follow-up, none of them has presented with a CRC nor has been submitted to surgery because of dysplasia or CRC.
Factors related with dysplasia detection and learning curve
Dysplasia was detected in 56/350 screened patients resulting in a dysplasia detection rate of 16%: 50/223 (18.3%) in patients with UC and 6/66 (8.3%) in patients with CD. Detection rate for LGD, HGD and CRC was 13.1%, 1.4% and 0.2%, respectively. Dysplasia detection rate was comparable between standard-definition procedures and those performed with high definition (27/145 (18.6%) vs 31/205 (15.1%), p=0.38). Similarly, it was comparable between CE-expert (n=6) and CE-non-expert (n=9) endoscopists (12.7% vs 16.2%, p=0.46), with similar withdrawal times (37.4±5.3 vs 36.1±12.8 respectively, p=0.83) (table 3).
Detection and optical diagnosis performances in relation to CE expertise
In order to assess the effect of learning curve for dysplasia detection, we compared the first third to the last third of procedures. Baseline patient and colonoscopy characteristics were similar in both subgroups. There was a trend to improve the dysplasia detection rate over time (12.5% vs 18.5%, respectively, p=0.18) (see online supplementary table S1). We also analysed the learning curve among five CE-non-expert investigators who performed at least 20 procedures during the study. When the first third of procedures were compared with the last third of procedures, we observed that three endoscopists had increased their dysplasia detection rate from 0% to 10%, 20% and 33%, respectively. However, dysplasia detection rate remained unchanged for the other two endoscopists (0% and 11%, respectively).
Diagnostic yield of CE for dysplasia detection
CE identified 409 additional lesions in addition to the 188 detected with white light. This resulted in an incremental detection yield for CE of 68.5% (95% CI 64.8% to 72.2%).
The invasive CRC and 39 dysplastic lesions were detected with white-light endoscopy. CE added 54 new dysplastic lesions: 53 LGD and 1 HGD. Therefore, CE-incremental detection yield for dysplasia was 57.4% (95% CI 47.5% to 67.3%): 60.2% (95% CI 50.2% to 69.1%) for LGD and 20% (95% CI 15.4% to 40.6%) for HGD.
The CE-incremental detection yield was comparable between standard-definition and high-definition procedures for both the total number of lesions (65.3% vs 70.7%, p=0.10) and for dysplasia (51.5% vs 52.3%, p=0.30) (see online supplementary table S3). Similarly, the CE-incremental detection yield for dysplasia was similar for CE-expert and CE-non-expert endoscopists (66.6% vs 53.7%, p=0.48).
Accuracy of optical diagnosis
Investigators correctly classified 455/503 non-dysplastic and 66/94 dysplastic lesions. Conversely, 48/503 non-dysplastic lesions were assessed as dysplasia, whereas 28/94 dysplastic lesions were assessed as non-dysplasia. As a result, sensitivity, specificity, PPV and NPV for dysplasia optical diagnosis were 70% (95% CI 61% to 79%), 90% (95% CI 88% to 93%), 58% (95% CI 49% to 67%) and 94% (95% CI 92% to 96%), respectively. The global accuracy value for ‘on site’ optical diagnosis was 87.4% (95% CI 82% to 93%) (see figures 3 and 4).

A slightly elevated lesion (Paris IIa) in a patient with long-standing colitis. Colonoscopy revealed a well delineated, regular and small polyp located at sigmoid colon. The lesion has a type II Kudo pit pattern and disrupts innominate lines. This type of lesion was well documented as hyperplastic lesion.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
A neoplasia-associated lesion in a patient with long-standing UC. This sessile polyp (Paris Is) is well delineated and detectable without chromoendoscopy. Chromoendoscopy helps to characterise it. It has a type IV Kudo pit pattern and can be easily distinguished from the other small sessile polyps located at the upper left part of the same image, which correspond to pseudopolyps.
As it is shown in table 3, there was a trend for better accuracy among CE-expert versus CE-non-expert endoscopists (90% vs 85.5%, p=0.09). CE-expert endoscopists were better at ruling out dysplasia than CE-non-experts (specificity: 94.4% vs 87.9%, respectively; p=0.01).
Endoscopic features associated with dysplasia
A summary of the morphological characteristics and their distribution in both groups of lesions (dysplasia and non-dysplasia) are represented in table 4.
Endoscopic features predictive of dysplasia. Results of univariate and multivariate analyses
Results of univariate statistical analysis showed that four features were associated with dysplastic histology: location at proximal colon, protruding morphology (Paris 0–Ip and 0–Is), loss of innominate lines and neoplastic pit pattern (IIIs, IIIL, IV and V). Some examples of these features are shown in figures 3 and 4. Subsequent multivariate analysis confirmed that these four features were independent predictors of dysplastic histology. The individual rates of these independent predictive features in terms of sensitivity, specificity, PPV, NPV and accuracy are also represented in table 5.
Accuracy of significant lesion characteristics for prediction of dysplasia
When we combined these four independent predictors of dysplastic histology, sensitivity was 10% (95% CI 14% to 16%) and NPV 86% (95% CI 83% to 88%). The global accuracy value of this combination was 85% (95% CI 82% to 89%).
Discussion
This multicentre, prospective cohort study has shown that CE with targeted biopsies is an effective strategy for IBD-associated dysplasia detection even outside clinical trials and in CE-non-experts hands. In vivo optical diagnosis with CE is highly accurate for ruling out dysplasia, especially in CE-expert hands. Lesions located proximal to the splenic flexure, with protruding morphology, loss of innominate lines or neoplastic Kudo pit pattern (IIIs, IIIL, IV and V) should be considered as potentially dysplastic and removed en bloc.
Consistent with previous data from several controlled trials, our results also demonstrated a considerable increase in dysplasia detection rate with CE-targeted biopsies compared with white-light targeted biopsies: 68.5% of all lesions and 57.4% of dysplastic ones were identified only after dye spraying. However, recent evidence on the value of CE in surveillance colonoscopy for IBD is contradictory. Whereas several well designed randomised trials and two single-centre studies with long-term follow-up have demonstrated a superiority of CE,5–7 ,24–30 a recent retrospective multicentre study has failed to demonstrate this benefit in real life.13
The main strength of the present study is that it has been prospectively performed in a real-life scenario, including expert and non-expert endoscopists in the use of CE, from academic and community-based hospitals, and including consecutively all patients with IBD referred for dysplasia screening. Therefore, our results can be generalised to the overall patient population with IBD and healthcare centres. Dysplasia detection rate of 16% is similar to the rate reported in previous studies.5 ,6 ,25–30 Interestingly, in this prospective consecutive series of patients from nine different centres, 70% of patients presented a high-risk feature for dysplasia. Whereas in 40% of patients no lesions were found, in the remaining 60% one out of four patients presented with IBD-associated neoplasia including an early CRC. Thus, surveillance with CE in high-risk patients is highly proficient in a real-life scenario.
A practical question about the use of CE is whether this technique can be implemented across all practice settings and performed by CE-non-expert endoscopists. Although the staining method is easy to learn and does not require any special technical skill, experience maybe required to identify subtle lesions. Based on the general consensus, scientific societies have recommended that CE-targeted biopsy strategy should be used by expert hands. We analysed the effect of CE technique experience in dysplasia detection and showed that dysplasia detection rate was comparable between CE-expert and CE-non-expert endoscopists (12.7% vs 16.2%, p=0.46). Hence, the beneficial effect of this technique on dysplasia detection was not related with CE expertise. In accordance with a previous study evaluating a CE learning curve, ours suggests that experience should not be a limitation for its implantation in real-world practice.31
Another important topic would be to establish to what extent CE is still necessary for improving dysplasia detection when using high-definition availability. A previous retrospective study showed that high definition was superior to standard definition when using white light.32 To date, only preliminary data have suggested a benefit of CE even with the use of high-definition scopes.31 In the present study we have shown that the incremental detection yield of CE was comparable between standard-definition and high-definition procedures for both, the total number of lesions (65.3% vs 70.7%) and IBD-associated dysplastic ones (51.5% vs 52.3). In light of these results, the use of CE should also be recommended when using high-definition systems.
CE with targeted biopsies allows us to consistently reduce the number of lesions that need to be biopsied/removed. However, most of these lesions are not significant in terms of CRC prevention, rendering surveillance colonoscopies in patients with IBD a discouraging resource-intensive labour. Furthermore, for optimal management of these patients, it is recommended to remove all dysplastic lesions en bloc and take biopsies from surrounding mucosa to rule out ‘invisible’ dysplasia. Because of chronic inflammation, endoscopic management of dysplasia is associated to a higher rate of complications.33 Consequently, a better prediction of histology in real time would allow to increase the efficiency of surveillance endoscopy. We evaluated real-time optical diagnosis accuracy by asking the researchers to classify each lesion in one out of seven categories before removal. Surprisingly, both CE-expert and CE-non-expert endoscopists were highly accurate for ruling out dysplasia (NPV=94%). Consequently, once a lesion is detected by a highly accurate technique such as CE, if the endoscopist (expert or non-expert in CE) is confident of the benign nature of the lesion, the probability of having a dysplasia is marginal (6%). On the other hand, as sensitivity for dysplasia diagnosis was low (70%), it seems reasonable to keep taking biopsies or removing every single lesion, unless there is a high level of certainty that the lesion is not dysplasia. Finally, we aimed to identify objective endoscopic characteristics that might assist endoscopists in dysplasia differentiation by recording a wide list of features. Proximal location, loss of innominate lines, polypoid morphology and neoplastic Kudo pit pattern were found to be independent predictors of dysplastic histology. Therefore, the presence of any of these four features would indicate that the lesion is highly suspicious of dysplasia and therefore should be treated as it.
Our study has some limitations. Although the study more closely reflects real life than a randomised controlled trial, its external validity to a general practice scenario maybe burdened by some elements. First, it is possible that endoscopists had performed the procedure more diligently than in routine clinical practice and this might result in a bias favouring the technique. Also, CE contribution to dysplasia detection may be overestimated because of a second-look effect and a performance bias. However, previous cross-sectional and randomised trials have already compared white-light endoscopy with CE showing similar results to ours. Then, withdrawal time in the study is not representative of real life since the back-to-back design and the need to carefully characterise lesions before removal might have entailed a longer procedure time. On the other hand, the study design doesn't allow answering whether extra random biopsies might still be useful in this setting. However, based on previous evidence showing the marginal yield of random biopsies,26 ,28 especially when using CE,5 ,34 we believe that this is not a main clinical issue, as reflected by current guidelines.8–11 Finally, because of a relatively small sample size, comparisons between endoscopists and techniques are weak and should be interpreted with caution.
In conclusion, our results show that outside clinical trials CE is an effective technique for IBD-associated dysplasia detection, even if using high-definition technology and in CE-non-expert hands. On the other hand, it allows ‘real-time’ optical diagnosis that might help to optimise lesion management. Future studies should evaluate if this surveillance strategy impacts on patients’ survival and quality of life.
Acknowledgments
The authors thank Erwin Sanabria for his initial commitment to the project.
References
Footnotes
Twitter Follow Antonio López-Serrano at @alopezserrano, Marco Álvarez González at @dralvarez96 and Luis Hernandez at @fingusmingus
Collaborators The EndoCAR group is a research group of the Asociación Española de Gastroenterología (AEG) and Sociedad Española de Endoscopia Digestiva (SEED) interested in endoscopy for patients with high-risk colorectal cancer conditions.
Contributors Study concept and design (MP); acquisition of data (SC, SM, AL-S, AZG-G, MIV, JCM-G, JDT, LM, MAÁ, LH, LDC, JG, IP, PV, MB-B, JA, BP, MLC, ER, MC and MJ); statistical analysis and interpretation of data (SC and MP); drafting of the manuscript (SC and MP); critical revision of the manuscript for important intellectual content (MLC, ER and MP).
Funding This work was supported by grants from the Instituto de Salud Carlos III (PI12/01481); Fundación Científica Asociación Española Contra el Cáncer (GCB13131592CAST) and Agència de Gestió d'Ajuts Universitaris i de Recerca (2014SGR135). This work was co-funded by the European Regional Development Fund (ERDF). Centro de Investigación Biomédica en Red de Enfermedades Hepáticas y Digestivas (CIBEREHD) is funded by Instituto de Salud Carlos III.
Competing interests MP is consultant for Norgine, Iberia.
Patient consent Obtained.
Ethics approval Institutional review boards at each participating institution.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement There are no meaningful additional unpublished data from the study. Eventually, other secondary data would only be used by investigators of the study under the supervision of the principal investigator.
Research reporting checklists The present article follows the STARD guidelines for research reporting of observational studies.