Article Text

Abstract
Immunotherapy strategies targeting immune checkpoints such as the CTLA4 and CD274 (programmed cell death 1 ligand 1, PD-L1)/PDCD1 (programmed cell death 1, PD-1) T-cell coreceptor pathways are revolutionising oncology. The approval of pembrolizumab use for solid tumours with high-level microsatellite instability or mismatch repair deficiency by the US Food and Drug Administration highlights promise of precision immuno-oncology. However, despite evidence indicating influences of exogenous and endogenous factors such as diet, nutrients, alcohol, smoking, obesity, lifestyle, environmental exposures and microbiome on tumour-immune interactions, integrative analyses of those factors and immunity lag behind. Immune cell analyses in the tumour microenvironment have not adequately been integrated into large-scale studies. Addressing this gap, the transdisciplinary field of molecular pathological epidemiology (MPE) offers research frameworks to integrate tumour immunology into population health sciences, and link the exposures and germline genetics (eg, HLA genotypes) to tumour and immune characteristics. Multilevel research using bioinformatics, in vivo pathology and omics (genomics, epigenomics, transcriptomics, proteomics and metabolomics) technologies is possible with use of tissue, peripheral blood circulating cells, cell-free plasma, stool, sputum, urine and other body fluids. This immunology-MPE model can synergise with experimental immunology, microbiology and systems biology. GI neoplasms represent exemplary diseases for the immunology-MPE model, given rich microbiota and immune tissues of intestines, and the well-established carcinogenic role of intestinal inflammation. Proof-of-principle studies on colorectal cancer provided insights into immunomodulating effects of aspirin, vitamin D, inflammatory diets and omega-3 polyunsaturated fatty acids. The integrated immunology-MPE model can contribute to better understanding of environment-tumour-immune interactions, and effective immunoprevention and immunotherapy strategies for precision medicine.
- cancer epidemiology
- cancer Immunobiology
- colorectal carcinoma
- cancer prevention
- molecular pathology
Statistics from Altmetric.com
Introduction
Accumulating evidence indicates that innate and adaptive immunity profoundly influences the evolution of neoplasms.1–3 While cancer comprises transformed neoplastic cells that have accumulated somatic molecular alterations, there is a dynamic interplay of neoplastic and non-neoplastic cells including inflammatory and immune cells. A fraction of somatic mutations may result in the generation of new antigens (neoantigens) that can be recognised as non-self by the immune system. During an individual’s life-course, cells may acquire somatic molecular alterations, and some of these cells undergo clonal expansion, displaying hallmarks of early neoplasia. Many of these cells are likely kept in check or killed by the host immune system before they can develop into clinically detectable tumours. By the time a tumour is detected, it has often acquired mechanisms to suppress immune responses and evade host immune surveillance. These processes are referred to as cancer immunoediting.
Cancer immunology is a blossoming field that has garnered well-deserved attention because of the success of immunotherapy approaches that target immune checkpoint mechanisms such as the CTLA4 and CD274 (programmed cell death 1 ligand 1, PD-L1)/PDCD1 (programmed cell death 1, PD-1) pathways.4 Many types of cancers misappropriate physiologic immune checkpoint mechanisms to evade immune-mediated recognition and destruction. Notably, blockade of immune checkpoints has proven successful in treating multiple tumour types, underscoring the power of the immune system to keep neoplasia in check. Additional active areas within cancer immunology include the development of cancer vaccines, adoptive cell therapy and immunisation for prevention and therapy.5–8
The immune system and inflammation undoubtedly play an important role in cancer aetiology as indicated by IBD-associated cancers and post-transplant malignancies due to long-term immunosuppression. Hence, primary cancer prevention is possible through the use of the immune system.5 9 Evidence indicates that modifiable factors such as non-steroidal anti-inflammatory drug (NSAID) use, obesity, physical activity, cigarette smoking and systemic vitamin D levels influence cancer risk and outcome as well as immune system function.10–17 Hence, dietary, lifestyle and pharmacological immunomodulators may be used to enhance the immune system for cancer prevention and treatment.
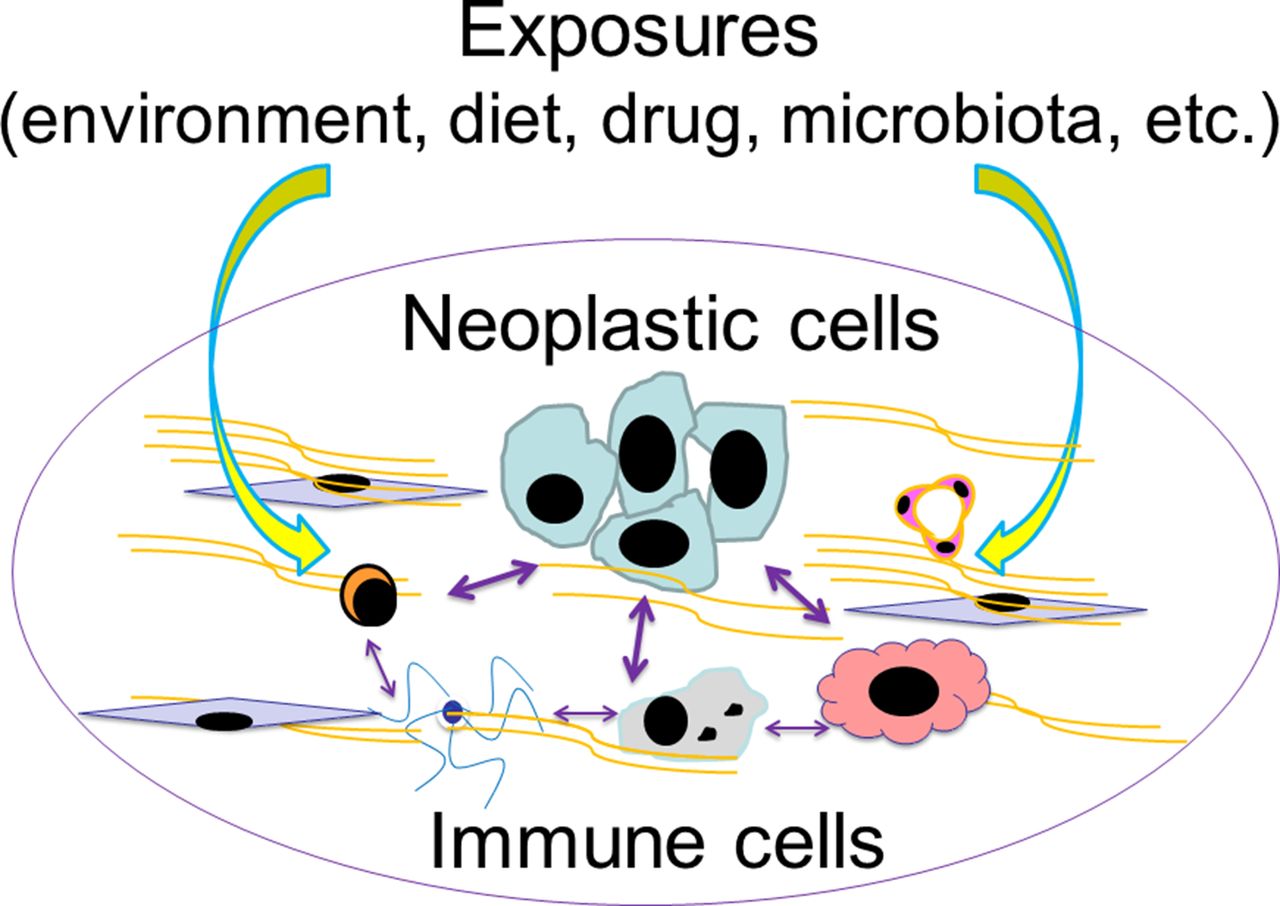
Due to these multifaceted interactions, a comprehensive understanding of neoplasia requires a robust interrogation of the environment (inclusive of the exposome, ie, the totality of the exposures to various exogenous and endogenous factors) given environmental effects on both host immunity and neoplasms (illustrated in figure 1). Expert panels have recommended that integrative transdisciplinary studies of modifiable exposures, tumour characteristics (including tumour omics and immunity) and clinical outcomes are urgently needed to improve strategies for precision prevention and treatment.9 18–21 However, this area of research is still in its infancy. We propose an integrated multilevel analysis of environment, tumour and immunity for improving cancer prevention and treatment. In this review, we discuss values and potentials of new approaches of integrating cancer immunology into pathobiology-based population health science.
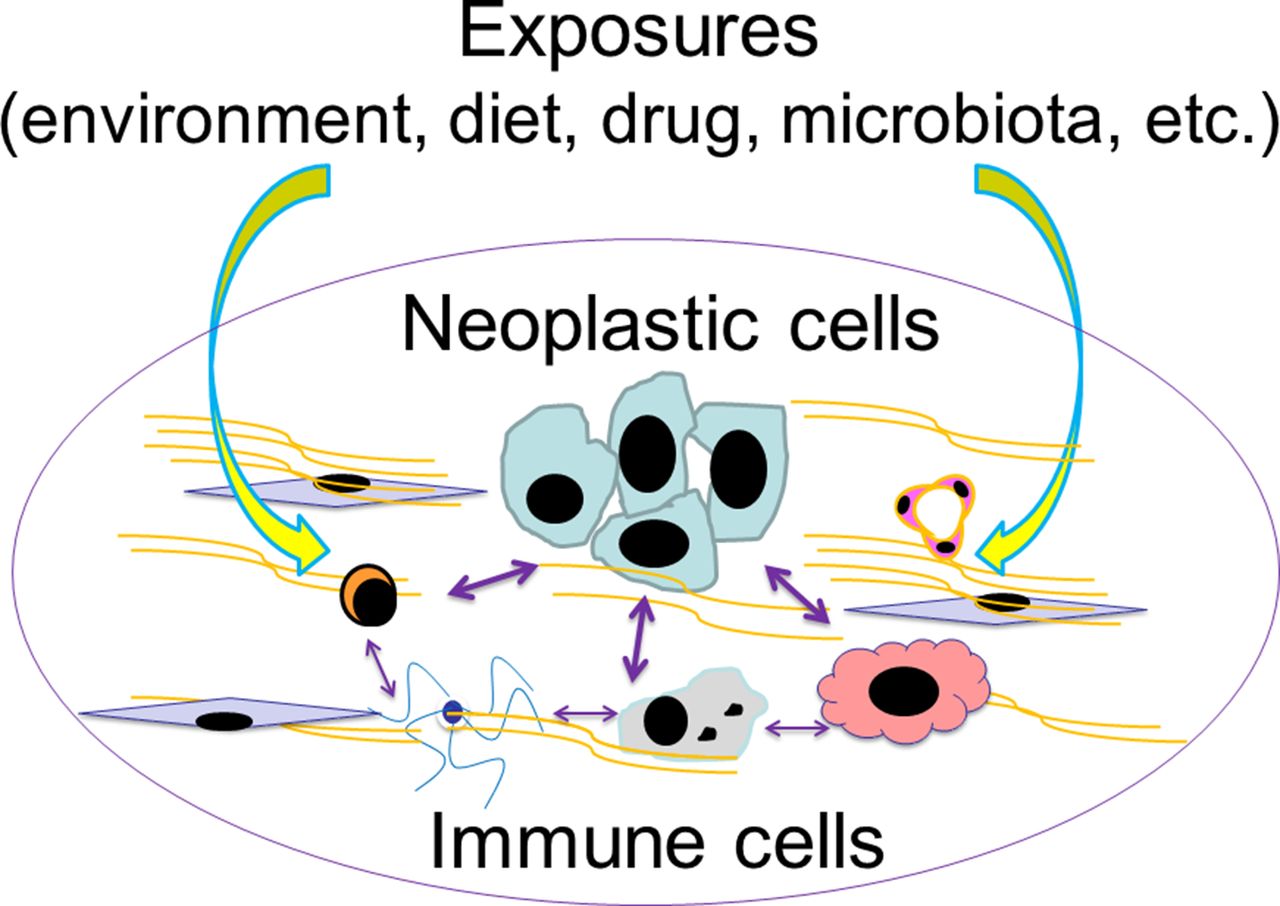
Various exogenous and endogenous factors (collectively called ‘exposures’) influence a tumour that has intrinsic and interacting components of neoplastic cells and the immune system. For simplicity, this does not depict complex interactions between the exposures and between neoplastic cells. There are ample research opportunities to decipher the interactions between these factors and components in human subjects and populations for better understanding of neoplasms. This figure illustrates potentials of integration of immunology and molecular pathological epidemiology.
Cancer immunology and precision medicine
The immune system is complex, consisting of many different and interacting cell types, which include (but are not limited to) T cells, B cells, NK cells, dendritic cells, macrophages, mast cells, polymorphonuclear neutrophils, eosinophils, basophils and other lymphoid and myeloid cells. While the importance of immunity for cancer is well recognised, the complexities of the immune system make its measurement and evaluation challenging in the clinical setting. Hence, clinical testing on tumour immunity have lagged behind tumour molecular testing for which the guidelines have been well developed.22 The clinical implications of the abundance and activities of various immune cell types in tumour tissue may vary in different tumour types. For example, intratumoural FOXP3 + regulatory T cells (Tregs) may have a different prognostic significance in different tumour types.23 24 In addition, heterogeneity in immune cell distribution and action can be influenced by local tumour cells, stroma and microenvironmental factors, including the microbiota.25 Spatial heterogeneity of the immune response poses further challenge when analysis is performed on small biopsy specimens rather than large resection specimens.
Despite these challenges, there are ample opportunities to develop clinically useful cancer immunology assays. For instance, international efforts have recently started to standardise immune cell analysis in cancer tissue; one of such efforts is the ‘immunoscore’ project,26 27 with an independent proof-of-principle study.28 In addition, a comprehensive evaluation of tumour immunity necessitates analyses of both tumour and immune cells.29 A number of tumour molecular analyses have been used in clinical practice, and tumour immunity evaluation can add prognostic information beyond tumour molecular features.24 30 For example, high-level microsatellite instability (MSI) and a high neoantigen load in colorectal cancers have been associated with a robust immune response and favourable clinical outcomes.31–34 MSI-high phenotype or mismatch repair deficiency predicts response to PDCD1 (PD-1) immune checkpoint blockade.35 36 Since May 2017, the US Food and Drug Administration (FDA) has approved use of the anti-PDCD1 (PD-1) antibody pembrolizumab for MSI-high or mismatch repair-deficient solid tumours regardless of primary organ site of tumour (https://www.fda.gov/drugs/informationondrugs/approveddrugs/ucm560040.htm; last visited on 5 December 2017). This represents the first FDA approval of a drug indication based solely on tumour molecular testing without consideration of primary body or organ site. Thus, MSI status (or mismatch repair protein expression) is now an established predictive biomarker of GI cancers for response to immune checkpoint inhibition.
Regarding other immune-related tumour markers, analyses of immune checkpoint pathways have become common for targeted immunotherapies. Some tumours express immune checkpoint ligands, including CD274 (PD-L1) and PDCD1LG2 (PD-L2), to suppress antitumour immunity.2 These ligands can bind to the T cell surface receptor PDCD1 (PD-1) and downregulate the immune response. In multiple cancers including melanoma, renal cell carcinoma, lung carcinoma, gastric carcinoma, lymphomas and other malignancies, blockade of the immune checkpoint pathway provides an effective treatment strategy. Accumulating evidence indicates that activation of the PI3K signalling pathway (by EGFR mutation, PTEN loss, PIK3CA mutation, etc) can upregulate CD274 expression in various tumour types.37–40 These tumour molecular features can be combined with immune cell status in tumour tissues, to subclassify tumours for precision intervention strategies.41 42 In addition to the immune checkpoint ligand-receptor interactions, some cancers have been shown to upregulate certain metabolic enzymes including IDO1 (indoleamine 2,3-dioxygenase 1), TDO2 (tryptophan 2,3-dioxygenase) and ARG1 (arginase 1) that can skew the immune response to suppress antitumour immunity.43–47 IDO1 expression in cancers has been associated with the levels of T cell infiltrates.48 49 Evidence also suggests that enhanced tumour cell metabolism depletes specific nutrients in the tumour microenvironment, which in turn, can suppress immune response and lead to tumour progression.50
To accelerate translation of our growing knowledge about cancer immunology into precision medicine, further efforts are needed to develop integrative tumour molecular pathology and immunity tests that can be useful for clinical and public health practices. To ensure rigour and reproducibility of these efforts, we cannot overemphasise the importance of data sciences, including epidemiology. The field of epidemiology primarily concerns methods of designing studies and analysing biomedical health data. Essentially, all clinical studies explicitly or implicitly rely on epidemiological principles to ensure the internal and external validity of results. Misuse or failure to properly use epidemiological and statistical principles is one of major reasons for non-reproducible study findings.51 Hence, the epidemiological principles must be properly used in clinical and translational research studies to promote robust evidence-based precision medicine.
Molecular pathological epidemiology—integrating molecular and population-level science
Although molecular pathology analyses had been used in epidemiological research on non-communicable diseases since the 1990s, a more complete integration of pathology and epidemiology occurred only relatively recently.52 Molecular pathology has become a major subfield of pathology with molecular pathology diagnostics now playing a routine part in clinical practice. By virtue of advances in molecular pathology, disease classification systems have transformed patient treatment and management. Molecular pathological information can also transform epidemiology. Advances in molecular pathology have enabled testing of targeted epidemiological hypotheses based on biological mechanisms. This trend necessitates the development of new research frameworks and analytic methodologies to decipher disease at both the molecular and population levels.52
In parallel with this trend, the integration of molecular pathology and epidemiology has led to the emergence of the transdisciplinary field of ’molecular pathological epidemiology (MPE)'.53–56 The MPE approach aims to connect potential risk factors to the molecular pathology of disease. As outcome variables, MPE research deals with disease incidence and mortality as well as health conditions and biomarkers that can predict future disease development or manifestations.57–59 Figure 2 illustrates the general approach that is typically taken for MPE research, using immune analysis as an example. The conceptual and practical rationale for hypothesis testing in MPE research has been described in detail elsewhere.55 60 61 Statistical analysis methods have been developed to test hypotheses on aetiological heterogeneity between disease subtypes in various study design settings,60–69 and to address missing data in MPE research.70 The paradigm of MPE has been widely recognised in the literature.71–113 Its relevance has been discussed in well-established scientific society meetings,114–117 and in the International MPE Meeting Series.118 119

Hypothesis testing in molecular pathological epidemiology (MPE) in a study of immune subtypes of disease A, with the simplest binary subtyping (subtypes B and C). Note that disease subtyping systems are often more complicated than simple dichotomy. Hypothesis testing #1 or #2 is on the relationship between an exposure of interest and each subtype. In this illustration, the exposure is hypothesised to prevent subtype B. Hypothesis testing #3 is unique to MPE, and concerns on a difference (heterogeneity) between the relationships of the exposure with the immune subtypes B and C.
The MPE approach can contribute to precision medicine. Aspirin has been associated with reduction of colorectal cancer incidence and mortality.120–125 MPE analyses of patient survival have suggested potential of aspirin as a therapeutic agent specifically for PTGS2 (cyclooxygenase-2)-overexpressing colorectal cancers,126 127 PIK3CA-mutated colorectal cancers128–130 and CD274 (PD-L1)-low colorectal cancers.131 Some of these markers may be used to select patients for aspirin therapy. Because these MPE analyses have been based on observational cohorts, prospective clinical trials have been ongoing.76
MPE analyses to assess cancer incidence can also contribute to precision prevention.11 13 21 132–134 Although colonoscopy screening has been associated with lower incidence of colorectal cancer, it may be less effective for MSI-high, CpG island methylator phenotype (CIMP)-high and BRAF-mutated colorectal cancers as high levels of MSI and CIMP and BRAF mutations are common features of postcolonoscopy (or interval) colorectal cancers.135–138 MPE studies have shown that smoking is associated with increased risk of MSI-high, CIMP-high and BRAF-mutated colorectal cancers.139–143 These lines of evidence may raise a question whether tobacco smokers may need improved colonoscopy or other screening procedures. It is expected that future MPE analyses can reveal additional links of certain risk factors and specific disease subtypes, which will contribute to the development of precision prevention strategies.
Moreover, MPE is a versatile method-based discipline that can enhance other scientific fields by means of developing unique analytical frameworks and methodologies. For instance, MPE can be integrated into social science144 and pharmacology.145 In particular, integration of pharmacology and MPE can decipher the influence of common medications on incidence and progression of disease subtypes.128 146–149 Similarly, integration of immunology and MPE can also be achieved as detailed below.
MPE helps establish causality
Epidemiological associations between lifestyle factors and cancer risks are relatively weak because traditional epidemiological studies generally use overall organ-specific cancers as a single outcome, and controversies have existed on causality in many of the associations.54 By means of connecting an exposure to specific molecular pathology, MPE research can provide pathogenic insights, and determine the strength of the association for the specific subtype, thereby helping establish causality.54 150 MPE research can reveal hidden structures of causal relationships, which may not be observed in conventional epidemiological research.150 For example, in the so-called obesity paradox, obesity is associated with better clinical outcome among patients with a disease that is caused (at least in part) by obesity. Such paradoxical findings on obesity lead to confusion and questions on causality of the relationship, hindering the development of public health measures for obesity prevention. On the other hand, MPE research can provide unique insights into paradoxical observations. For example, studies on renal cell carcinoma have shown such paradoxical findings.151 MPE research has shown that obesity is associated with FASN-non-expressing subtype of renal cell carcinoma, which in turn is associated with better clinical outcome compared with FASN-overexpressing subtype.152 Hence, MPE research can potentially decipher paradoxical findings in conventional epidemiological research.150
It is also important to acknowledge limitations of observational studies in establishing causality. Hence, in addition to rigorous study design and analyses, the importance in acquiring multiple lines of evidence from research using different experimental biological models and different study settings, including experimental clinical trials, should be recognised.
Integrating immunology into MPE
In this section, we discuss the integration of cancer immunology and MPE.
The scientific link between MPE and immunology
MPE research addresses the interpersonal heterogeneity of disease processes and pathogenesis.53 118 As the unique disease principle153 154 indicates, a pathological process in each person is uniquely influenced by a combination of exogenous and endogenous factors, and their interactions with both disease cells and normal cells including immune cells. It is assumed that individuals with diseases that share similar molecular pathological features also share similar aetiologies.153 Accordingly, subclassification of patients based on similarities (and dissimilarities) of pathological and immunological markers may enable researchers to link putative risk factors to specific pathologies, including altered immune status. Ample evidence indicates an influence of tumour molecular pathological alterations on immune response to tumour, and an influence of immune status on biological aggressiveness and progression of tumour.24 26–29 155 156 Exogenous and endogenous factors can modify the biological nature of a given tumour that has intrinsic and interacting components of neoplastic cells and the immune system (figure 1). In this sense, immunology can be considered an integral part of MPE at the conceptual level, with the potential for providing valuable new insights when integrated into MPE at the practical level.
In addition, the importance of immunity analysis in human tissue cannot be overemphasised, because even the best animal models cannot fully recapitulate the human immune system or complex diseases.157 Hence, experimental immunology research on model systems need to be corroborated and augmented by human tissue and population research and vice versa.
How can immunology be integrated into MPE?
MPE research has been most commonly applied to neoplastic diseases.55 Neoplastic diseases provide us with clonally expanded cells for molecular analyses in both clinical practice and MPE research settings. However, analyses of immunity status in tumour tissue have been uncommon in epidemiology despite the important role of immunity in cancer. This is in part because immune cell assessment in tumour tissue has not been a common clinical test, and it remains a considerable challenge to accurately and reproducibly evaluate the interactions between the tumour and immune cells. Furthermore, in a typical population-scale research setting, it is not always practical or feasible to incorporate detailed characterisation of tumours beyond information present in medical records. Assessment of immune cells in tumour tissue currently requires considerable effort from a pathologist. Hence, the integration of immunological assessment of tissue into epidemiological studies remains limited.
Likely, the most commonly used immune-related analysis method in epidemiology settings is germline genetic testing. For example, specific HLA genotypes have been associated with risks for certain autoimmune disorders, including ankylosing spondylitis, rheumatoid arthritis and multiple sclerosis. Numerous genes and gene variants (including those in HLA loci) play roles in immune response to various antigens including microbial proteins and tumour neoantigens. Analysis of immune cells and inflammatory markers in peripheral blood specimens is another method that can provide information on systemic inflammation and immune status and is commonly used in epidemiological research. Nonetheless, germline genetic and peripheral blood analyses yield only limited information on the status of interactions between tumour and immune cells in the local tumour microenvironment. Immune cells in the normal colon mucosa and colorectal cancer tissue show substantial phenotypic differences compared with the same immune cell type isolated from the peripheral blood from the same individual.158 159 Hence, analysis of immune cells in the relevant tissue is essential to understand immune cells in the tumour microenvironment.160 Importantly, integrative multilevel analyses (including omics technologies) of available biospecimens, including germline DNA, peripheral blood cells, circulating molecules, microbes, neoplastic cells and immune cells in the local microenvironment can provide a better, holistic view of immune status within an individual and in relation to a tumour, compared with analysis of any single source of information. Ultimately, the full integration of immunology into MPE will help us gain considerable insights into cancer as a disease of immune dysfunction.
Integrative ‘immunology-MPE’ research model
As discussed above, the integration of immunology and MPE is a natural extension of MPE. It can generate insights into how lifestyle, dietary, genetic, microbial and environmental exposures influence disease processes through impacting the immune system and disease-immune interactions. Although data are currently scarce in this emerging area, this field is expected to expand in light of the increasing importance of cancer immunology. Figure 3 illustrates the multilevel framework of immunology-MPE research. Assessment of immunity can be performed using multilevel and multidimensional approaches, using germline genotypes, immune biomarkers in blood or other body fluids and normal and disease tissues of interest to evaluate the immune status in the tissue microenvironment. Immunology-MPE can and should synergise with basic experimental immunology, as these two research models offer complementary strengths (table 1).

Overview of research designs to integrate immunity analyses into the framework of molecular pathological epidemiology. The word ‘exposures’ is broadly used as an epidemiological term for variables that can causally influence disease incidence, status or outcome. Immunity assessments include germline genotyping of immune-related genes, analyses of immunity status in disease tissue and analyses of biomarkers on tissue, blood and/or other body fluids as intermediary phenotypes. Intermediary phenotypes refer to phenotypes that are thought to precede full-blown disease phenotypes or subsequent clinical outcome (eg, mortality), and can be typically assessed in radiological images, biopsy tissue, peripheral blood or other body fluids. Intermediary phenotype variables can be used as exposures or outcomes in epidemiological terms.
Comparisons of basic experimental immunology and immunology-molecular pathological epidemiology (MPE)
Research on GI neoplasms, especially colorectal carcinoma, has considerable relevance in this emerging immunology-MPE area. GI neoplasms represent exemplary diseases to use this integrative research model. The digestive tract, especially the colon and rectum, has rich microbiota and immune tissues and is accessible by endoscopies. It is also sensitive to tumour-promoting effects of inflammation, as illustrated by the link between IBD and colorectal cancer. Furthermore, the external environment, including immune-related lifestyle factors, appears to have a stronger role in the development of GI cancers compared with many other types of malignancies. Colorectal cancer is a molecularly heterogenous group of neoplasms,161–168 which are influenced by exogenous and endogenous factors and immune response to tumour.54 169–172 Epigenetics can mediate effects of exposures on tumour plasticity and phenotypes.153 173–178 The continuum of differences in clinical and molecular characteristics of colorectal neoplasms according to bowel subsites is compatible with the interactive roles of the microbiota and immunity in colorectal carcinogenesis.179–191 As immunoediting appears to be a common event during colorectal carcinogenesis, a subset of colorectal carcinomas have been shown to overexpress CD274 (PD-L1)31 192–201 and PDCD1LG2 (PD-L2).202 However, immune checkpoint blockade has not been shown to be effective against most colorectal carcinomas, except for MSI-high (mismatch repair deficient) tumours.156 203 204 There are thus ample opportunities for the development of effective interventions, including immunoprevention and immunotherapy strategies against colorectal cancer.204 205
Colorectal cancer has been commonly studied in MPE research.54 206 207 There is an increasing trend of assessments of immune response to colorectal carcinoma, in addition to tumour molecular analyses, in the context of large-scale population-based studies.194 208–219 Table 2 lists proof-of-principle immunology-MPE studies on potential aetiological factors that may influence incidence of immune subtypes of cancer; below, we highlight several notable findings.
Immunology–molecular pathological epidemiology (MPE) studies on possible aetiological factors and incidence of neoplasia subgroups classified by immune response to tumour
One study, using resources of the Nurses’ Health Study (NHS) and the Health Professionals Follow-up Study (HPFS), showed that a higher intake of marine omega-3 polyunsaturated fatty acids (ω-3 PUFA, rich in fish) was associated with a lower risk of colorectal cancer containing high-density FOXP3+ cells in tissue, but not with risk of colorectal cancer containing low-density FOXP3 + cells.220 Possibly, ω-3 PUFA may downregulate the function of FOXP3 + Treg cells, thereby enhancing the antitumour function of effector T cells even in the presence of abundant FOXP3 + cells.220 Consistent with this hypothesis, an in vitro experiment using coculture of naïve CD4 + T cells and colonic FOXP3 + Treg cells revealed that exposure to high ω-3 PUFA concentrations led to downregulation of FOXP3 + cell function, which resulted in increased naïve CD4 + T cell proliferation.220 As exemplified by this study,220 immunology-MPE research can synergise with basic experimental immunology research.
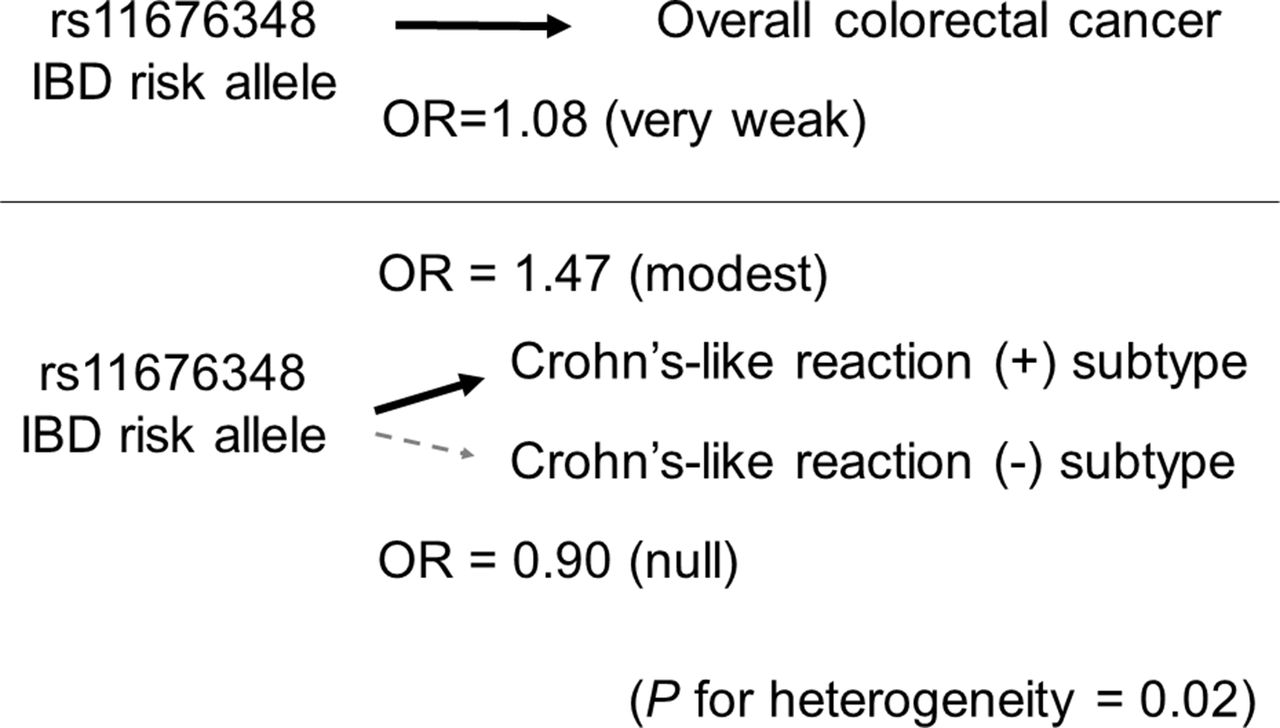
A second study221 based on the Genetics and Epidemiology of Colorectal Cancer Consortium (GECCO) examined whether risk alleles for IBD identified by genome-wide association studies (GWAS) might be associated with colorectal cancer risk (figure 4). Although risk alleles for IBD, a well-established colorectal cancer risk factor, are conceivably also risk alleles for colorectal cancer, none of GWAS-identified IBD risk alleles was detected as a risk allele for colorectal cancer by agnostic GWAS.222 Using over 25 000 cases and controls, one IBD risk allele (rs11676348) was associated weakly with colorectal cancer with an OR (per allele) of 1.08 (95% CI 1.04 to 1.12)221; notably with this effect size, this polymorphism was not detected by an agnostic GWAS approach. Interestingly, when immune response to colorectal cancer was examined, the rs11676348 allele was associated with colorectal cancer exhibiting Crohn’s-like lymphoid reaction (with the OR 1.47; 95% CI 1.01 to 2.13) but not with cancer exhibiting no Crohn’s-like reaction.221 Crohn’s-like lymphoid reaction refers to transmural lymphoid aggregates that mimic Crohn’s disease (one manifestation of IBD).208 As Crohn’s-like reaction is associated with MSI-high colorectal carcinoma,208 the differential association of the rs11676348 allele according to MSI status was examined, revealing a consistent differential association of the rs11676348 allele with MSI-high tumours, but not with non-MSI-high tumours, in two independent datasets within GECCO.221 Possible heterogeneity of aetiological associations according to cancer immune subtypes may explain why the rs11676348 polymorphism is only weakly associated with colorectal cancer overall. This approach enables us to find many uncovered risk alleles for various diseases. This study221 represents a proof-of-principle analysis of the GWAS-MPE approach54 and immunology-MPE research.

Illustration of the molecular pathological epidemiology approach using tumour immunity status. The germline DNA polymorphism rs11676348 is a risk allele for IBD. Because IBD is a risk factor for colorectal cancer, the rs11676348 polymorphism is considered to be a risk factor for colorectal cancer. The Genetics and Epidemiology of Colorectal Cancer Consortium study showed the OR estimate of 1.08 per rs11676348 risk allele, indicating a very weak association with overall colorectal cancer.221 When colorectal cancer was classified by immune response features, the association of the risk allele was stronger (OR estimate of 1.47 per risk allele) and specific for colorectal cancer subtype with Crohn’s-like lymphoid reaction, but not for subtype without Crohn’s-like lymphoid reaction.
A third study based on the NHS and the HPFS showed that high-level plasma vitamin D was associated with a lower risk of colorectal cancer with high-level lymphocytic infiltrates, but not with risk of colorectal cancer with low-level lymphocytic infiltrates.223 Hence, the cancer preventive effect of vitamin D appears to be stronger for cancer with high-level lymphocytic infiltrates.223 Some immune cells are capable of converting 25-hydroxyvitamin D [25(OH)D] to bioactive 1α,25-dihydroxyvitamin D3 [1,25(OH)2D3], which may prevent neoplastic progression in individuals who can elicit high-level lymphocytic response to emerging tumours.223
Translation into immunoprevention and immunotherapy
The integration of immunology and MPE can drive future research and clinical practice, to generate population-based evidence and novel insight for the development of effective immunotherapy and immunoprevention strategies. Immunoprevention (or immunoprophylaxis) embraces the use of immunomodulators and prophylactic vaccines. For example, the aforementioned research on ω-3 PUFA and vitamin D suggests their roles in preventing cancer through immune mechanisms. If replicated, the findings of this immunology-MPE study may provide the rationale for the use of nutritional supplementation for cancer immunoprevention. Identification of a dietary, lifestyle or pharmacological factor that can effectively improve outcomes in a specific disease subtype (classified by immune status) may lead to an effective immunotherapeutic strategy for that subtype. Hence, in addition to targeted immunotherapeutic agents, immunomodulators may have a role in clinical immuno-oncology practice. A recent study has shown that use of aspirin is associated with better clinical outcome in colorectal cancers that do not overexpress the CD274 (PD-L1) immune checkpoint ligand, but not with outcome in CD274 (PD-L1)-overexpressing cancers, suggesting a possible synergistic effect of immune checkpoint blockade and aspirin.131 Hence, immunology-MPE research has substantial roles in the development and refinement of strategies of immunoprevention and immunotherapy.
Challenges
Challenges exist in the emerging immunology-MPE field. Some of those are relevant to the field of MPE as previously described.54 First, sample size is generally limited based on biospecimen availability, which can also lead to selection bias. Hence, investigators should make efforts to increase sample size and reduce sample selection bias in MPE research. In addition, a causal inference method such as inverse probability weighting can be used to reduce selection bias due to specimen availability.131 224 225 Second, MPE research uses disease subtyping (ie, multiple disease subtypes), hence inherently facing the issue of multiple hypothesis testing. To address the multiple hypothesis testing issue, it has been recommended that investigators set a heterogeneity test comparing subtype-specific associations as primary hypothesis testing.55 Proper utilisation and practice of statistical analysis can also mitigate this weakness. Third, there are measurement errors in bioassays. Hence, it is critical to ensure assay validity and performance. These challenges affect generalisability of findings. Currently, the studies described in table 2 represent rare examples of immunology-MPE research, for which a replication analysis may not easily be conducted. To increase overall sample size, statistical power and robustness of findings, a consortium should be formed to pool data from multiple studies. It may also be feasible to synthesise population health registries into global-scale MPE databases in the future.226
There are also challenges specific to the emerging field of immunology-MPE. While integration of tumour molecular pathology into epidemiology has been progressing since the 1990s,145 integration of cancer immunology into epidemiology has lagged behind due to several reasons. Importantly, the immune system and its interactions with tumour are inherently complex. Hence, it is very challenging to develop a standardised laboratory test for detailed phenotyping and precise measurement of immune status in the tumour microenvironment. For this reason, it is difficult to implement detailed analyses of tumour-immune interactions in clinical settings and large-scale studies. Nonetheless, the emerging field of immunology-MPE can address this unmet need. Tackling many unanswered questions on effects of exposures on tumour-immune interactions are important in our efforts to improve our understanding of cancer and develop strategies for cancer prevention and treatment. Indeed, efforts to perform cancer immunity analyses using tissue resources in population-based studies have been ongoing. A number of analytic methods that use high-throughput tumour omics platforms to assess tumour-immune cell interactions are available.227 Infiltrates of various immune cell types can be quantified using transcriptome profiling of tumour tissue that contains immune cells.228 229 In addition, DNA or RNA sequencing-based methods targeting T cell receptor genes (such as TRB; T cell receptor β)230–233 may have considerable potential in large-scale population-based studies. Data analysis methods such as network analysis can be applied to tumour immune response data in a large-scale study.189 There is also an opportunity to incorporate digital pathology and image analysis technologies on tissue specimens. In vivo microscopic technologies, which can be used together with endoscopies,234 235 will revolutionise biomedical and population studies of neoplasms, especially premalignant lesions.21 85 236–239 As various omics analysis platforms have recently been applied to single cell analyses,240 there are open opportunities to use single cell analyses on a large number of cells (including immune cells) within a tumour in a large number of people; however, there exist considerable challenges in cost and feasibility of such a study.
In addition, there is a scarcity of interdisciplinary experts and education programmes integrating areas of epidemiology, pathology and immunology. This scarcity causes difficulty in planning and execution of transdisciplinary research including immunology-MPE projects. The scarcity of interdisciplinary experts is both a cause and consequence of the paucity of interdisciplinary training programmes. While population health scientists need education in immunology and pathobiology, wet laboratory scientists also need education in study design, epidemiology and statistics. Development of an interdisciplinary education system in public health and medical schools has been proposed to bridge this gap.52 Such a new system should encompass pathology and epidemiology, and naturally integrate immunology, considering its importance in many human diseases.
As another challenge, funding mechanisms also need to be adapted and optimised to fairly evaluate transdisciplinary science. The current peer-review system relies on evaluations of research proposals by researchers most of whom are experts in traditional disciplines. In addition, funding agencies (such as US National Institutes of Health and Cancer Research UK) have organisational structures mainly based on traditional disciplines, typically disease-based disciplines (but not method-based disciplines). Therefore, it is plausible that transdisciplinary research proposals may not be duly evaluated in light of their potential paradigm-shifting impact. Indeed, transdisciplinary research has been associated with lower funding success despite its stronger scientific impact compared with traditional discipline-bound research.241
Opportunities and future directions
There are ample opportunities, given the importance of immunity in cancer, evidence for immunomodulatory roles of many exposures and the early rising phase of the immunology-MPE field. Thus far, only a limited number of studies have been conducted in the area, and hence, novelty of the integrative immunology-MPE approach remains relatively high. In addition, new methodologies of immune cell analyses can be incorporated in research. For instance, in vivo pathology technologies are promising tools that can expand the immunology-MPE model as discussed above.
Combining tumour tissue assessment with analyses of normal tissue and other biospecimens including peripheral blood, sputum, urine and other body fluids can add new dimensions to immunology-MPE research. For instance, immune cell analyses such as multicolour flow cytometry can be performed on those body fluid specimens. In addition, omics approaches, such as epigenomic, transcriptomic, proteomic and metabolomic analysis of circulating peripheral blood cells (and/or plasma),242–245 may enable multilevel studies on the status of the immune system, and together with tissue analyses, improve our understanding of influences of the systemic and local immune system status on cancer development and progression. It should be noted that circulating peripheral blood cells consist of many different cell types, and those omic data on circulating cells substantially depend on cellular compositions and their activation status. Recent advances in liquid biopsy provide new approaches to repeatedly and non-invasively interrogate the dynamic evolution of the molecular profiles of human cancers, through analyses of circulating tumour cells (CTCs), circulating tumour DNA (ctDNA) and exosomes containing various biomolecules.3 246–251 Dysregulation of immune regulators has been detected in CTCs,252 and mutational profile in ctDNA has been suggested as a useful marker for monitoring immunotherapy response.253 Therefore, applications of liquid biopsies can lead to new approaches for studying the dynamics of the tumour-immune-environmental interaction.
As another opportunity, microbiology can be integrated into immunology-MPE research. Microorganisms have been the most important targets of the immune system during human evolution. Therefore, an improved understanding of microbes and their interactions with the immune system can advance broad areas of immunology and medicine. Accumulating evidence indicates that microorganisms play important roles in classical infectious diseases and many chronic diseases, including cancer.254–256 For example, many microorganisms have been implicated in tumourigenesis, including Epstein-Barr virus, HBV, HCV, HIV, human papillomavirus, human T-lymphotropic virus, polyoma viruses, Fusobacterium nucleatum, Helicobacter pylori, Schistosoma hematobium, among others. Notably, there is an intriguing link between the gut microbiota, including F. nucleatum and colorectal cancer.172 257–264 F. nucleatum may suppress the adaptive T cell response,265 and this immunosuppressive property may function in a way similar to the immune checkpoint in colorectal cancer. Supporting this, the amount of F. nucleatum in colorectal carcinoma has been inversely associated with CD3 + cell density in tumour.266 The abundance of F. nucleatum in colorectal cancer tissue has been associated with the serrated neoplasia pathway,236 267–270 a fibre-poor diet271 and unfavourable clinical outcomes.272 273 A recent study has shown persistence of F. nucleatum in metastatic colorectal tumour.274 The gut microbiota is a key factor in intestinal diseases and diseases in distant body sites, and even systemic diseases through their influences on metabolisms and immunity.254 Analyses of microbiota can be conducted using oral swab, stool and normal and tumour tissue,275–277 and integrated into immunology-MPE research.
Emerging evidence indicates inter-related links between drugs, nutrition, microbiota, immunity and tumour evolution. Data from integrative research can be used for drug repurposing.278 Studies have shown that the gut microbiota has a profound effect on the efficacy of cancer chemotherapy and immunotherapy.279–283 Frequent use of antibiotics has been associated with an increased risk of colorectal adenomas.284 Combined with pharmacological, nutritional, social and behavioural sciences,144 149 285–287 effects of medications, nutrients, socioeconomic status and other exposures on tumour-microbe-immune interactions can be examined.
Conclusions
Given the unquestionable importance of the immune system in health and disease, immunology needs to be fully integrated into pathobiological population health science such as MPE. This integration, which has the potential to facilitate the realisation of precision medicine, has been hindered by the complex nature of the immune system and difficulty in developing standardised laboratory methods to assess tumour-immune interactions. Nonetheless, these technical challenges can be surmounted, and research efforts have started to integrate tumour immunology into MPE. To foster this integration, we must develop transdisciplinary education systems and new funding mechanisms. In the next decade, recognised as a discrete scientific field, immunology-MPE will play an increasingly important role in medicine and health sciences, as this field represents one of the priority areas in cancer research.288 Immunology-MPE research will provide novel evidence for roles of the immune systems in health and diseases at a population scale. Figure 5 illustrates a roadmap of integrative immunology-MPE research in order for us to realise precision medicine and exert clinical impact. Ultimately, integrative immunology-MPE research will offer new insights for the development of intervention strategies harnessing the immune system towards precision prevention and treatment.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Roadmap of integrative immunology-molecular pathological epidemiology (MPE) to precision medicine. Three themes are set to start integrated immunology-MPE research and accomplish three specific aims. Based on data from research for the three specific aims, strategies 1 through 3 will help us implement, monitor and optimise tumour immunity testing for clinical use.
References
Footnotes
Contributors RN, MG, WSG and MS contributed equally. SO developed the main concept of the manuscript. SO, AIP, UP and RN wrote grant applications. All authors contributed to review and revision, and approved the final manuscript.
Funding This work was supported in part by grants from the USA National Institutes of Health (R35 CA197735 (to SO), K07 CA172298 (to AIP), U01 CA137088 (to UP) and K07 CA190673 (to RN)) and Nodal Award (to SO) from the Dana-Farber Harvard Cancer Center.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.