Article Text

Abstract
Objective The underlying microbial basis, predictors of therapeutic outcome and active constituent(s) of faecal microbiota transplantation (FMT) mediating benefit remain unknown. An international panel of experts presented key elements that will shape forthcoming FMT research and practice.
Design Systematic search was performed, FMT literature was critically appraised and a 1-day round-table discussion was conducted to derive expert consensus on key issues in FMT research.
Results 16 experts convened and discussed five questions regarding (1) the role of donor and recipient microbial (bacteria, viruses, fungi) parameters in FMT; (2) methods to assess microbiota alterations; (3) concept of keystone species and microbial predictors of FMT, (4) influence of recipient profile and antibiotics pretreatment on FMT engraftment and maintenance and (5) new developments in FMT formulations and delivery. The panel considered that variable outcomes of FMT relate to compositional and functional differences in recipient’s microbiota, and likely donor-associated and recipient-associated physiological and genetic factors. Taxonomic composition of donor intestinal microbiota may influence the efficacy of FMT in recurrent Clostridioides difficile infections and UC. FMT not only alters bacteria composition but also establishes trans-kingdom equilibrium between gut fungi, viruses and bacteria to promote the recovery of microbial homeostasis. FMT is not a one size fits all and studies are required to identify microbial components that have specific effects in patients with different diseases.
Conclusion FMT requires optimisation before their therapeutic promise can be evaluated for different diseases. This summary will guide future directions and priorities in advancement of the science and practice of FMT.
- faecal microbiota transplantation
- donor
- recipient
- bacteria
- virus
- fungi
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
Faecal microbiota transplantation (FMT) is effective in recurrent Clostridioides difficile infections and is potentially beneficial in other microbiota-related disorders.
FMT rectifies the recipient’s intestinal microbial community by introducing micro-organisms associated with a ‘healthy’ state to normalise microbiota composition and function.
What are the new findings?
Variable outcomes of FMT may relate to compositional and functional differences in the recipient’s gut microbiota, and likely donor-associated and recipient-associated physiological, genetic or demographic factors.
Taxonomic composition of donor intestinal microbiota may influence the efficacy of FMT in recurrent Clostridioides difficile infections and UC.
FMT helps establish trans-kingdom equilibrium between gut fungi, viruses and bacteria to promote the recovery of microbial homeostasis.
FMT is not a one size fits all strategy, and studies are required to identify microbial components microbiota that have specific effects in patients with different diseases.
How might it impact on clinical practice in the foreseeable future?
Selecting donors based on microbial indicators and/or capability of the donor microbiota to restore specific metabolic disturbances associated with each disease may be important for improved FMT efficacy.
FMT delivery methods and microbial strains need to be rationally designed and tightly controlled taking into account microbial diversity, taxonomic composition and donor–recipient factors.
Background
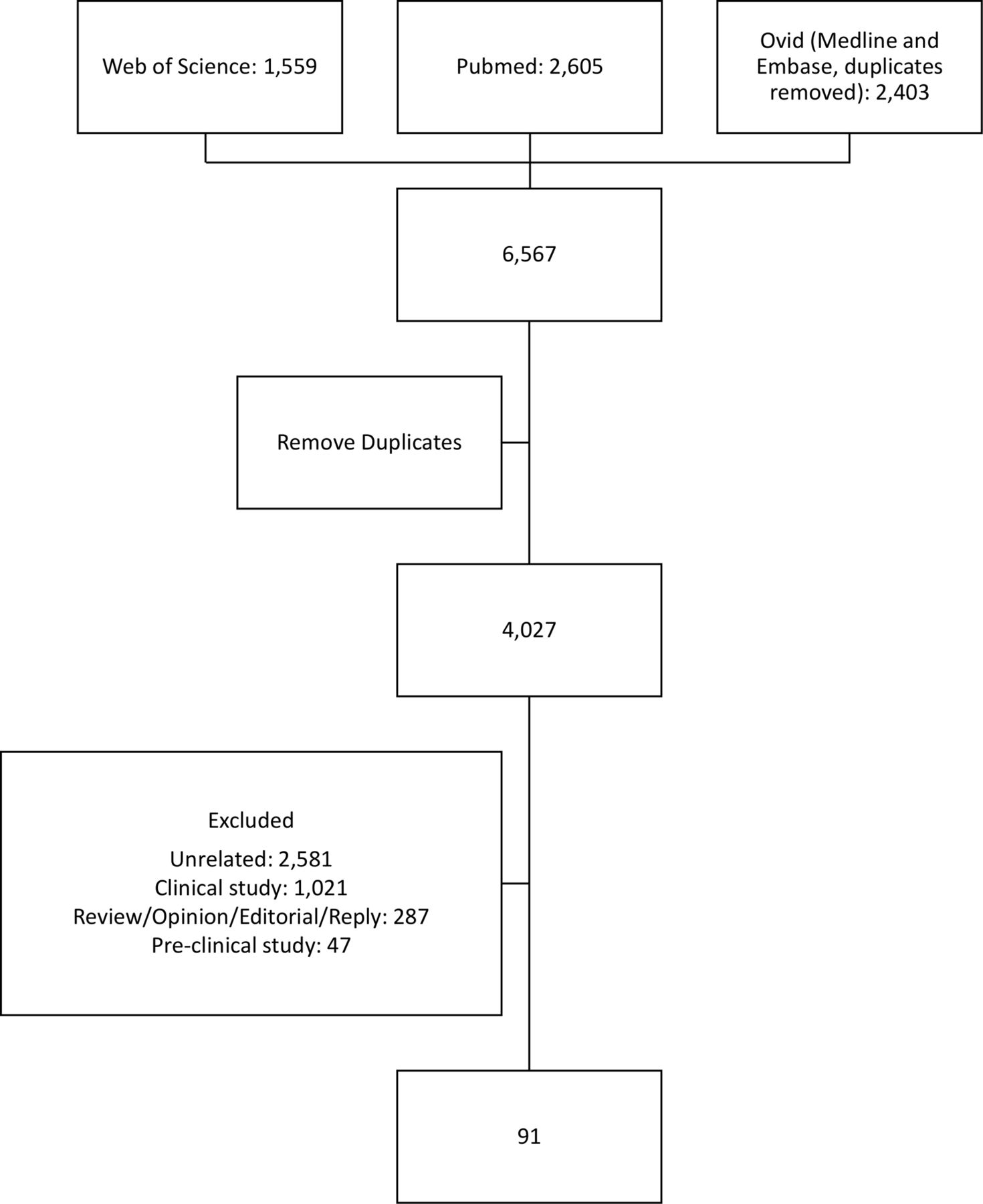
Faecal microbiota transplantation (FMT) has been shown to be a highly efficacious, safe and cost-effective therapy for recurrent Clostridioides difficile infections (CDI).1 2 Beyond CDI, FMT has been investigated as a treatment option in a variety of diseases (GI), including IBD,3–6 IBS,7 hepatic encephalopathy,8 9 autism10 and metabolic syndrome.11 12 Although FMT is potentially effective, substantial heterogeneity in donor selection and FMT application have been reported in studies across different populations.13 According to data submitted to the clinical studies registry in the US National Institutes of Health, over 200 clinical trials of FMT in various diseases are being conducted or have been registered in the past 2 years.14 However, the underlying microbial predictors of therapeutic outcome and active constituent(s) of FMT mediating success remain largely unknown, even in the setting of the most studied recurrent CDI (rCDI). Recently, the term ‘super-donor’ has been proposed to describe donors whose stool results in more successful FMT outcomes compared with stool from ‘regular’ donors.15 This paper aims to review the scientific rationale behind FMT with a main focus on recent advances in our understanding of mechanisms of FMT and factors associated with FMT outcomes across different clinical conditions. It does not intend to cover clinical aspects of FMT, such as indications or outcome, donor screening2 16 or regulations of FMT practice,17 18 as most of these aspects have been extensively reviewed elsewhere. In a frontiers meeting held in Hong Kong, experts within Asia-Pacific presented their views and discussed outlooks pertaining to FMT regarding (1) the role of donor and recipient microbial parameters; (2) concept of keystone species and microbial predictors, (3) methods to assess microbial alterations, (4) possible influence of recipient profile and antibiotics pretreatment on FMT engraftment and maintenance and (5) new developments in FMT formulations and delivery. Detailed methodology is described in online supplementary appendix 1 and figure 1 shows the flow diagram of studies included.
Supplemental material
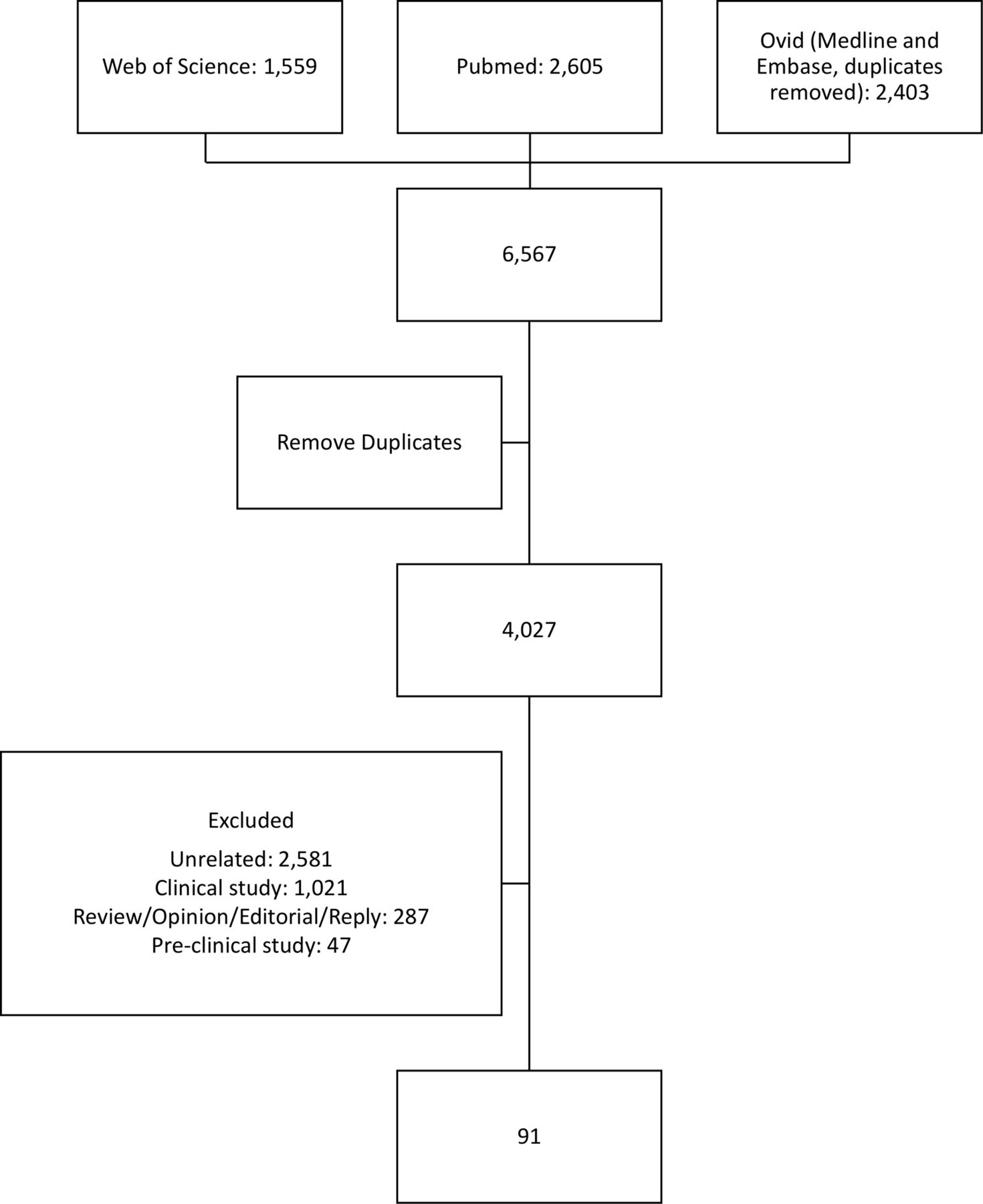
Flow diagram of studies included after systematic search.
Microbiology of FMT
Role of donor-associated microbial parameters in FMT
Recurrent CDI
While current donor screening procedures mainly focus on safety, by excluding known human pathogens, there is no clear agreement on selecting donors based on microbial parameters.16
In a study where 10 paediatric patients with rCDI were treated with FMT from a competitively selected ‘optimal’ universal donor based on high microbial diversity, balanced Bacteroidetes versus Firmicutes and a high concentration of faecal butyrate, all subjects showed no disease recurrence at 10 weeks after treatment.19 This study demonstrated that using markers of the bacterial community profile may be feasible for donor stratification, although larger cohorts inclusive of control populations without specific donor profiling are needed to confirm whether donor stratification improves FMT success rates in rCDI.
Few studies have focused on potential role of viruses as a mediator of FMT efficacy. This is due to complexities in profiling viruses compared with bacteria as viruses lack universal marker genes. To facilitate recovery of virus sequences in metagenomes, virome-enrichment nucleic acid extraction methods have been developed to selectively enrich virus particles from stool. However, these enrichment procedures disrupt inherent virus community by altering their relative numbers. One pilot study of five subjects administered a single jejunal infusion of sterile stool filtrate and all subjects with relapsing CDI recovered, lending support to a role of bacteriophages in FMT efficacy.20 The positive outcome from using non-live bacterial stool filtrates in FMT highlighted the possibility that bacterial fractions of donor gut communities are necessary for successful treatment, although it did not exclude that bacterial-secreted metabolites and cell components such as proteins and RNAs that may exert crucial effects in the recipient. In a survey of enteric bacterial and viral composition in an FMT recipient cured of rCDI, the recipient’s phage community was highly similar to the donor’s following FMT and remained stable for 7 months.21 The viral communities in both donor and post-transplant recipient exhibited comparable diversity and richness. These studies indicate that enteric virome composition could be a key indicator of the clinical outcomes of FMT for rCDI.21 We found that in rCDI patients treated with FMT, all recipients responded to FMT when richness of Caudovirales was higher in donors compared with recipients.22 A separate study of 19 patients with rCDI showed that subjects successfully treated with a single FMT had increased Bacteroidetes and Firmicutes and a complete loss or reduction of Siphoviridae phages. FMT can alter both bacterial and phage composition to resemble the donor.23 Patients requiring multiple FMT showed increased abundances of Enterobacteria phages HK542, mEp237 and phiP27 suggesting that the presence of these Enterobacteria phages may be associated with reduced efficacy.23
The human gut also hosts various fungi and other eukaryotes.24 Fungal communities are commonly profiled using a DNA barcode sequence known as the internal transcribed spacer (ITS),25 but this approach has multiple shortcomings including large variation in copy number among fungal taxa, variable lengths in ITS sequences and fungal cells are harder to lyse during DNA extraction. These factors, combined with a significantly less comprehensive reference database compared with the 16S ribosomal RNA gene, distort relative abundance estimates in fungal community surveys. It was found that higher relative abundances of Saccharomyces and Aspergillus in stool of recipients correlated with successful FMT for rCDI and a high abundance of Candida albicans in donor stool was associated with reduced FMT efficacy.26 Both gut bacteriophages and fungi, particularly C. albicans, affect bacterial community assembly,27–29 potentially influencing FMT effectiveness in rCDI.
Inflammatory bowel disease
In IBD, a small study of 14 refractory patients (8 UC, 6 Crohn’s disease (CD)) reported that higher bacterial species richness in donors and a higher number of transferred phylotypes were associated with successful transplantation.30 In addition, stool of donors with a high bacterial richness, a high relative abundance of Akkermansia muciniphila, unclassified Ruminococcaceae and Ruminococcus spp were more likely to induce remission.31 In a randomised controlled trial (RCT) of FMT in UC, increased relative abundances of Eubacterium hallii and Roseburia inulivorans in UC were the strongest and most consistent associations with positive clinical outcomes. Functional analyses demonstrated that Eubacterium and Roseburia contributed to increases in beneficial metabolic pathways.32 For instance, E. hallii maintains microbial metabolic health and homeostasis via short-chain fatty acid production. In contrast, the presence of Fusobacterium in UC was associated with FMT failure.32 Reduced relative abundances of Clostridium cluster XIVa and increased Bacteroidetes were reversed by FMT, mainly in responders.33 Sustained remission was associated with butyrate-producing organisms, and relapse was associated with Proteobacteria and Bacteroidetes.33 It has also been suggested that remission rates could be enhanced by pooling stools from multiple donors to increase microbial diversity.5 34
A low eukaryotic virus richness before FMT in patients with UC was associated with FMT success.35 These studies showed that phages in donor stool were associated with FMT efficacy in CDI, whereas eukaryotic viruses appeared to be more relevant in UC, suggesting that virome interactions may be disease specific. Although phages may play a role in efficacy, the experimental designs of many studies did not exclude the possibility that these viruses were purely enriched alongside bacterial hosts, as whole donor stools including bacteria were transplanted into recipients.
Other diseases
With improvements in high-throughput DNA sequencing technology, it is now possible to study long-term engraftment of donor bacterial strains.36 In a study into metabolic syndrome, multiple recipients of a single donor showed extensive coexistence of donor and recipient faecal bacterial strains up to 3 months after FMT. Furthermore, recipients receiving the same donor stool displayed large variation in microbiota transfer, indicating that individuals vary in their microbiome engraftment and donor–recipient compatibility.37 These examples indicate that strain level differences between microbial taxa could offer a key to understanding why certain strains are more efficacious relative to others, and that these genomic differences can be used to optimise donor selection. Recent work has evaluated the temporal variation in bacteriome and virome after FMT. In a small pilot study of three patients with carbapenem-resistant Enterobacteriaceae who had successful decolonisation after FMT, viral communities varied substantially over time whereas intensive trans-kingdom correlations between viruses (Caudovirales) and bacteria (Ruminococcaceae) were significantly depleted in recipients after FMT, particularly with the interaction between Klebsiella-specific bacteriophages and Ruminococcaceae species weakened.38 In acute graft versus host disease (GvHD), a series of FMTs altered the gut bacterial, fungal and viral communities in a patient with GvHD. Engraftment of donor-derived fungi occurred instantly after a single FMT and persisted up to 4 months39. Moreover, FMT reduced an over-represented fungus Fusarium oxysporum and Torque teno virus in parallel with an increase in fungal diversity and abundance of Caudovirales bacteriophages. While these data do not directly address the role of fungi in FMT, it suggests that FMT helps establish trans-kingdom equilibrium between gut fungi, viruses and bacteria to promote recovery.39 Although the clinical value of donor selection based on stool microbial community profiles remains to be established, incorporation of steps to assess stool community composition is technically feasible. Since microbial community composition, richness and diversity remained a distinct characteristic of each donor, a single assessment of stool composition during donor selection is likely sufficient to represent samples collected in subsequent months.40
Table 1 summarises donor and recipient stool compositions and factors associated with improved FMT efficacy.
Donor and recipient stool compositions and factors associated with improved FMT efficacy
Microbial predictors of FMT success: how to study them
To understand how gut microbial communities are involved in FMT and whether key micro-organisms can be manipulated to improve therapeutic outcomes, studies have used 16S ribosomal RNA gene-based amplicon sequencing to characterise the gut microbiota of FMT donors and recipients. In successful cases of treating UC and rCDI, general trends observed in the recipients’ gut community profiles are the following: (1) increased bacterial community diversity following FMT,3 41 42 (2) community profiles more closely resembling donor profiles,41–43 (3) decrease in certain bacterial taxa including Proteobacteria and Fusobacteria and (4) a corresponding increase in key Firmicutes and Bacteroidetes taxa.33 41–44 In patients with metabolic syndrome, lower initial faecal microbiota diversity before FMT in the recipients was predictive of metabolic improvement on treatment.11 12 In addition to donor-derived microbial populations that persist in the recipient, some microbial populations that flourish post-FMT are undetectable in donor or recipient pretransplantation. Taken together, these findings indicate that micro-organisms from donors engraft in recipients, potentially colonising and/or creating conditions that repress disease-associated micro-organisms. This change in the gut environment could create conditions that allow microbial populations below detection thresholds in pre-FMT samples to flourish and repopulate the gut, helping to restore diseased gut communities to a ‘healthy’ state. Although most FMT studies have used 16S rRNA profiling, 16S sequences do not contain sufficient resolution to inform whether the same microbial species or strains are found in both donors and recipients. An increasing number of studies now use shotgun metagenomics (sequencing of bulk DNA) in which total extracted DNA is sequenced without preselection for any marker genes. Given the strong influence of environment on human gut microbiota composition45 and a high functional redundancy among gut microbial taxa,46 it is highly likely that FMT success is mediated by functionality of gut micro-organisms in addition to phylogeny. Using gene-centric metagenomics, community functionality is traditionally assessed by sequencing bulk DNA and then comparing the resultant sequences to gene orthology databases such as the Clusters of Orthologous Groups47 and Kyoto Encyclopedia of Genes and Genomes.48 Genome-centric metagenomics has been widely used in environmental microbiology but is not yet commonplace in human gut microbiome studies.49 50 To date, the use of shotgun metagenomics screening to predict FMT success in CDI and other diseases is mostly confined to academic research due to its cost and timescale. Nevertheless, information gained from this research can be instrumental in formulating clinical trials, such as guiding primer designs for screening a list of beneficial and negative micro-organisms and viruses. Table 2 illustrates the different methods to characterise microbial parameters in FMT. Figure 2 illustrates the potential mechanism of FMT.
Methods to study microbial parameters in FMT

Potential mechanisms of faecal microbiota transplantation (FMT). Potential mechanisms of FMT include direct interaction or competition between donor and recipient gut microbiota to achieve homeostasis, effect of donor microbiota on the host immunity and effect of microbiota on modulating host metabolism and physiology. Competitive niche exclusion is a plausible mechanism behind the therapeutic effects of FMT in the treatment of Clostridioides difficile infections (CDI) by introducing competitors and/or modifying the diseased gut environment to the detriment of Clostridioides difficile. For example, introduction of non-toxigenic C. difficile strains can reduce the recurrence of CDI in subjects.1 Another competition-based strategy harnessed by gut micro-organisms is the production of bacteriocins.2 Quorum sensing systems have also been detected in C. difficile and are known to affect toxin expression profiles in other coexisting micro-organisms. FMT can alter host bile acid metabolism concomitant with alterations to gut microbiota composition. In CDI, a consistent metabolic signature with reduced primary bile acids and increased secondary bile acid production capacity has been reported after FMT. FMT restores Firmicutes phylum bacteria and secondary bile acid metabolism,3 providing a prime example of FMT re-establishing normal gut microbiota and host metabolism. FMT also has the ability to restore gut microbiota and mucosal immunity and systemic immunity of the host. In mice models of colitis, FMT reduced colonic inflammation and initiated a simultaneous activation of different immune pathways, leading to interleukin (IL-10) production by innate and adaptive immune cells including CD4+ T cells, invariant natural killer T (iNKT) cells and antigen-presenting cells (APC), and reduced the ability of macrophages, monocytes and dendritic cells to present MHCII-dependent bacterial antigens to colonic T cells.4 These results demonstrate the immunomodulating capability of FMT to therapeutically control intestinal homeostasis and highlight FMT as a valuable therapeutic option in immune-related pathologies. For instance, a reconstitution of the gut microbiome and a relative increase in the proportion of Foxp3+ regulatory T cells within the colonic mucosa were potential mechanisms through which FMT could abrogate immune check point inhibitors associated toxicity.5 online supplementary file 1 Please refer to Appendix 3 for references. iNKT, invariant natural killer T; MHCII, major histocompatibility complex class II.
Clinical predictors of FMT
Several clinical factors have been reported to be associated with failure of FMT in rCDI. In a prospective study of 64 patients with rCDI treated with FMT by colonoscopy, severe CDI and inadequate bowel preparation were independent predictors of failure after single faecal infusion.51 A multicentre study showed that predictors of early FMT failure included severe or severe-complicated CDI, inpatient status during FMT and previous CDI-related hospitalisation were associated with early FMT failure.52 In a RCT of patients with active UC, those with disease for less than 1 year appeared to have better outcomes after FMT.3
Optimising FMT protocols
Donor–recipient matching
It is recognised that differences in microbiome composition between individuals and diseases could contribute to variations in response to FMT.53 Furthermore, host genetic factors such as differences in innate immune responses or environmental factors, such as diet, xenobiotic exposure and microbial interactions may also play a role in shaping FMT responses between donor and recipient.15 OpenBiome, a public stool bank in the USA published an investigation into the selection criteria of universal donors based on faecal butyrate concentration, microbial diversity metrics and ratio of Firmicutes to Bacteroidetes which yielded good FMT outcomes for rCDI, but there was no formal comparison of these selection criteria against standard donor selection whereby microbiota composition or metrics were not taken into account for FMT.19 Donor–recipient matching for FMT may not be as critical for CDI because of high efficacy even without specific matching, but is likely important for other conditions including UC and IBS in which response rates remain modest and variable (approximately 30%–40%).7 54 For example, when gut microbiota profiles of different donors were compared, it was found that microbial diversity was a predictor for FMT success in UC.31 While current evidence suggests that FMT efficacy can be improved by carefully selecting donors based on their gut microbiota content and that ‘one stool does not fit all’, the specific parameters for implementing a selection criteria are still unknown. Alterations in microbiota may also not be the only factor contributing to disease status or development. An individual’s response to FMT may predominantly depend on the capability of the donor’s microbiota to engraft and reverse the microbial community dysbiosis associated with a specific disease phenotype; these factors need to be investigated in future studies.
Apart from using whole faecal transplants, one approach which removes donor-dependent effects is to provide patients with a defined cocktail of micro-organisms confirmed to be beneficial for disease resolution. For example, providing IBD patients with a targeted microbiota-based formulation containing only butyrate producers may be a logical and safer alternative to whole faecal transplantation. Precision approaches have been trialled in CDI but with mixed results.55 56 It may be that the donor microbial community as a whole plays a stronger role in driving FMT success than critical species in isolation. Nevertheless, targeted bacteriotherapy approaches should be investigated as a way of circumventing risks associated with administering whole faecal material.
Recipient microbial profiling prior to FMT
The criteria that denote an ‘optimal recipient’ for receiving FMT are not clear, although there are several studies describing correlations between gut microbiota composition of recipients and FMT outcomes. In a study of patients with UC receiving FMT, the presence of Fusobacterium in recipient stool was associated with FMT failure.32 In another study of subjects with metabolic syndrome, responders had lower initial faecal microbiota diversity, higher relative abundances of Subdoligranulum variabile and Dorea, and lower relative abundances of Eubacterium ventriosum and Ruminococcus torques.11 In a study using oral administration of encapsulated faeces for rCDI, faecal samples of patients before FMT had low diversity and relative abundances of Firmicutes and Bacteroidetes, and a high relative abundance of members of the Proteobacteria, specifically Enterobacteriaceae. Following FMT, subjects who developed recurrence of CDI had greater relative abundances of Enterobacteriaceae and did not show resolution of dysbiosis.57 While it is not immediately clear how resident microbial communities in recipients influence FMT outcome, since diverse microbial taxa have been associated with unsuccessful FMT, it is postulated that they form a ‘barrier’ against uptake of donor microbial populations by creating competition for ecological niches and/or resources.
Pretreating recipients with antibiotics before FMT
Not all studies adopt the use of antibiotics prior to FMT and data remain controversial. Consistent with concept of species competition resulting in reduced FMT success, use of antibiotics prior to FMT may help alter resident gut microbiota in recipients to increase FMT efficacy. This is supported by a meta-analysis of human studies and two studies in mice showing that pretreatment with antibiotics may enhance FMT efficacy.58–60 The inference based on these data is that antibiotics eliminate competition from resident micro-organisms by freeing previously occupied ‘niches’. For instance, combination therapy of FMT and antibiotics was more effective than antibiotic cocktails or FMT therapy alone in restoring Bacteroidetes diversity in UC.61 In another study, patients with UC received FMT capsules containing purified Firmicutes spores (SER-287) with killed bacteria, parasites, fungi and viruses. A subset of recipients received vancomycin pre-FMT, which resulted in higher rates of clinical remission compared with recipients without vancomycin,62 63 providing further support for the ‘ecological niche’ hypothesis. Future studies should specifically assessed the role of antibiotics prior to FMT in different conditions and its cost-effectiveness.
Formulating FMT preparations and delivery procedures
New developments in FMT delivery
There is interest in developing convenient, easy-to-administer FMTs as current infusions are delivered via endoscopy (eg, colonoscopy or nasojejunal), enema or colonic transendoscopic enteral tubing (TET).64–66 Oral capsules has been developed showing efficacy comparable to delivery by colonoscopy regardless of whether fresh, frozen or lyophilised stools were used.67–69 However, frequency of doses and optimal overall duration is still unclear as study parameters were not directly comparable across different studies. So far, studies on oral capsule-based FMTs in chronic diseases have been limited to short-term outcomes (up to 8 weeks). The next steps must evaluate parameters such as dosage frequency and total treatment duration, as well as long-term response (years) of the recipient’s gut microbiota.
Factors to consider in FMT formulations, preparations and delivery
Fresh, frozen or lyophilised (freeze-dried) stool
Figure 3 summarise FMT preparations, formulations and delivery methods. Although FMT infusions prepared from fresh or frozen stool may have comparable efficacy,70 71 various studies reported a decline in microbial viability in frozen stool. FMT oral capsules frozen up to 1 year were associated with a CDI resolution rate of 88%,69 comparable to the widely reported 90% resolution rate for this condition. Quantitative PCR analyses showed statistically significant decreases in Bifidobacterium and Lactobacillus abundances in frozen and lyophilised FMT samples stored for 9 months.72 An RCT estimated rCDI remission rates associated with the use of fresh, frozen or lyophilised stools at 100%, 83%, and 78%, respectively, when delivered by colonoscopy.73 In CD, contrasting results have been reported whereby one study reported increased clinical improvement and remission using fresh stool compared with frozen specimens,74 while a meta-analysis found no significant difference in clinical remission rates between fresh and frozen FMT preparations.75 These observations raise the question about whether viability of micro-organisms in frozen stools is important for FMT success; in a pilot study of four patients, lyophilised sterile faecal filtrates and whole stool achieved similar efficacy for rCDI.76

{kind=link}
{kind=link}
{kind=link}
For faecal microbiota transplantation (FMT) administration, lower GI delivery can be achieved through enema or colonoscopy, whereas upper GI delivery is through infusion via gastroscopy or via nasoenteric tubes. Oral capsules are non-invasive and is an ideal delivery method for FMT. Formulation to improve delivery, ensuring organism survival and ensure colonisation along the GI tract are needed.6 An encapsulation technique based on a water-in-oil emulsion can provide better insulation of FMT material from GI environment.7 One potential solution is the use of bile absorbent resins.The use of bile acid binding agents such as cholestyramine, when combined with Vcaps HPMC capsules, provided a 1700-fold increase in freeze-dried and rehydrated Lactobacillus casei in a simulated intestinal fluid containing 1% bile.8 Alternatively, a layer-by-layer encapsulation approach using mucoadhesive polysaccharides, chitosan and alginate has been shown to improve cytoprotection, bioavailability and engraftment of Bacillus coagulans in porcine and human intestines.9 Capsule design content release is dependent on intestinal stimuli.10 Other approaches include genetic engineering, for example, Escherichia coli engineered to bind to colorectal cancer cell receptors and catalyse production of molecules with anticancer activity.11 This novel approach can be considered for FMT if constituent strains that contribute to clinical efficacy are identified. They can then be engineered to improve binding and colonisation in the gut of FMT recipients.Please refer to Appendix 3 for references.(online supplementary file 1)
Aerobic or anaerobic preparations
Many bacterial populations in the human gut are obligate or facultative anaerobes, whose viability may depend on how FMT infusions are prepared. Comparisons conducted in rCDI subjects using aerobically and anaerobically prepared FMT infusions showed similar efficacy,77 but comparisons have not been undertaken in other indications.78 In a study of 73 active UC, treatment with 1 week of anaerobically prepared donor FMT resulted in higher steroid-free remission rates at 8 weeks compared with autologous FMT (32% vs 9%).6 The role of anaerobic FMT preparation in preserving anaerobes is consistent with the peptide nucleic acid sequencing analyses which showed that anaerobic preparation better preserves obligate anaerobes such as Faecalibacterium prausnitzii, an anti-inflammatory commensal bacterium whose absence is correlated with active IBD.79
FMT dose amount and frequency
For traditional FMT delivery via enema and colonoscopy, most studies report the use of approximately 50 g of donor stool. The basis for this is unclear, but a systematic review reported that the amount used had little impact on rCDI resolution rates. However, when less than 50 g of stool was administered, the relapse rate was fourfold higher (4% compared with 1%).80 A recent meta-analysis also confirmed that faecal amount ≤50 g was associated with lower efficacy rates after a single infusion in rCDI.81 In IBD, approximately 50 cm3 faecal microbiota after filtration and centrifugation from stool was used. To determine the dosage required for oral FMT capsules, a comparative cohort analysis comparing clinical cure rates between 22.5 and 45 g of stool found little difference.82 No studies have investigated direct comparison of different FMT dosing for IBD; however, a study has evaluated enriching microbiota from the stool for the treatment of IBD.65 Generally there is limited information to guide current practice related to FMT stool dose and frequency of administration.13 Stool mass varies among donors.43 A more objective method to standardise FMT dosage such as microbial richness and diversity remains to be tested.
FMT delivery routes
Traditional/endoscopic FMT delivery
Traditional delivery routes of FMT include enema or colonoscopy, or gastroscopy or nasoenteric tubes.83 Colonic TET has been used in specific centre in China.84 In delivery through the lower GI tract, there is a trade-off between reliable delivery (ie, stool retention) and invasiveness of the procedure. Delivery through enemas, colonoscopy, gastroscopy and nasoenteric tubes have comparable efficacy.71 Aspiration pneumonia and regurgitation are potential adverse events associated with gastric route FMT.
Oral capsules
In an RCT, the performance of FMT delivered via oral capsules containing frozen faecal material was equal to delivery by colonoscopy in rCDI.67 Oral FMT capsules are prepared by mixing stools with a cryoprotectant (eg, glycerol), followed by double or triple encapsulation to protect the FMT material from gastric milieu. Capsule shells can be selected depending on the intended released site, with commercially available shells usually targeting gastric (FMTgr) or colonic release (FMTcr). A comparison between FMTgr and FMTcr capsules reported improved remission rates for treatment of rCDI using colonic release capsules (81% vs 75%), presumably due to the lower exposure of FMT material to chemical and enzymatic degradation.82 Various modifications can also be made to the capsule contents, such as used frozen oral capsules containing spores isolated from stool of healthy donors resulting in a 97% rCDI cure rate.85 Another trial that used lyophilised faecal matter in oral capsules reported the same remission rate as enema delivery in rCDI subjects,86 although there was reduced acquisition of Bacteroidia and Verrucomicrobia in patients treated with lyophilised oral capsules. RBX7455, a lyophilised non-frozen room temperature oral FMT capsule reported 90% primary treatment efficacy for rCDI.87 Similarly, CP101, also based on lyophilised faecal matter, was as effective in low dose as high doses of 24–27 capsules, achieving 88% clinical success for rCDI treatment.69 In another double-blind, placebo-controlled trial, 58 UC subjects were randomised to receive an 8-week treatment of either SER-287 (a mix of spores from members of the Firmicutes phylum) or placebo. Patients who achieved clinical remission after treatment with SER-287 exhibited decreased expression of UC-related genes and increased expression of non-IBD genes.88
Conclusion
Considerable effort is being put into identifying factors that contribute to FMT success. While the vast majority of FMT studies are related to treatment of rCDI, a growing body of clinical evidence showed FMT efficacy in non-rCDI indications. Unlike rCDI in which there is a clear gut microbiota dysbiosis, the aetiology of other chronic conditions, such as IBD, IBS and obesity show stronger genetic and environmental predispositions. FMT success may depend more heavily on the capability of the donor microbiota to restore specific metabolic disturbances associated with each disease. Therefore, for FMT to become more effective, its delivery methods and microbial strains need to be rationally designed and tightly controlled taking into account important factors contributing to clinical success (eg, bacterial abundances, taxonomic composition, pretreatment with antibiotics, etc). Further characterisation of super-donors will result in the development of more refined FMT formulations to help standardise therapy and reduce variability in patient responses. In parallel, continued optimisation of FMT protocols, including a shift toward capsule-based delivery will help combat longevity issues associated with FMT and create a more patient-friendly alternative to current disease management strategies.
Supplemental material
References
Footnotes
Contributors SCN, MAK, FKLC planned the meeting and established the main topics. WT and TZ performed the systematic search. All panel members were involved in presenting the literature in a Frontiers meeting in Hong Kong in June 2018. All panel members provided supporting evidence and drafted the text of discussion relevant to their topic. SCN, TZ and YKY wrote the initial draft of the manuscript. All panel faculties read and revised the manuscript for important intellectual content and approved the final manuscript. CJO, VM and KS are representatives of APAGE and NO is representative of APSDE.
Funding Funding from the Center for Gut Microbiota Research, Faculty of Medicine, The Chinese University of Hong Kong to support the Frontiers Meeting in Hong Kong, and Martin Ho (Imperial College London) for his input in the section on new deliveries of FMT.
Competing interests FZ invented the concept of GenFMTer and TET and devices related to it.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.