Article Text

Statistics from Altmetric.com
Messages
The approach to paraoesophageal structures and lesions via the oesophagus was initiated by the introduction of peroral endoscopic myotomy (POEM), followed by peroral endoscopic removal of tumours within the muscular layer. We now report a case which suggests that the next step, that is, to remove paraoesophageal tumours not related to the oesophageal wall, would also be possible. This is the case of a 66-year-old male patient with a 4.0×2.0×1.5 cm benign schwannoma from the recurrent laryngeal nerve bulging into the proximal oesophagus, which we removed via a POEM tunnel. The postoperative course was uneventful. Further controlled studies have to show which lesions may be suitable for this expanded approach and also confirm the safety and feasibility of this technique which can be regarded as much less invasive than operative minimal invasive alternatives.
In more detail
Due to the complicated anatomy of the mediastinum, mediastinal masses represent a heterogeneous group of tumours.1 2 Characteristic location of the mass establishes a useful differential diagnosis that aids in planning the diagnostic evaluation. Video-assisted thoracoscopic surgery and conventional open surgery are the currently available treatments for these patients with benign lesions in whom removal is considered to be indicated, also for clarification of the diagnosis.3–5 Traditional surgical approach can be associated with substantial trauma, slower recovery, higher complication rate and decreased postoperative quality of life.
To overcome these disadvantages, we report on a novel technique, transoesophageal endoscopic surgery, for treating mediastinal tumours. This technique takes advantage of the submucosal tunnelling technique popularised by natural orifice translumenal endoscopic surgery (NOTES). NOTES stimulated with the development of POEM and submucosal tunnelling endoscopic resection (STER), the submucosal or ‘third space’ endoscopy combining minimal invasive surgery and endoscopy. Here we present a rare case of schwannoma originated from the recurrent laryngeal nerve, which we removed via transoesophageal endoscopic surgery (figure 1).

Rare case of schwannoma in the mediastinum. (A) During transoesophageal endoscopic surgery: the schwannoma originates from left recurrent laryngeal nerve (yellow arrow) in the mediastinum. (B) Morphology of the tumour: a 4.0×2.0×1.5 cm enveloped nodular mass with necrotic tissues inside.
Patient history
A 66-year-old man was admitted for oesophageal ‘submucosal tumour (SMT)’ found on routine check-up at a local hospital by regular oesophagogastroduodenoscopy (OGD) examination for 1 month. No special for his history, family history or life history. Contrast-enhanced CT of the chest showed a mass located among aorta arch, oesophagus and trachea in the left posterosuperior mediastinum with internal heterogeneity. No metastasis to the lymph nodes or other organs was seen on the CT scan. Endoscopic ultrasound (EUS) revealed it to be heteroechoic and well demarcated, approximately 2.0×1.5 cm in diameter, and located outside the oesophageal wall. OGD exploration at our hospital showed a smooth-elevated bulging lesion 23 cm from the incisors. After a full discussion, transoesophageal endoscopic removal of the tumour was attempted.
Description of technology
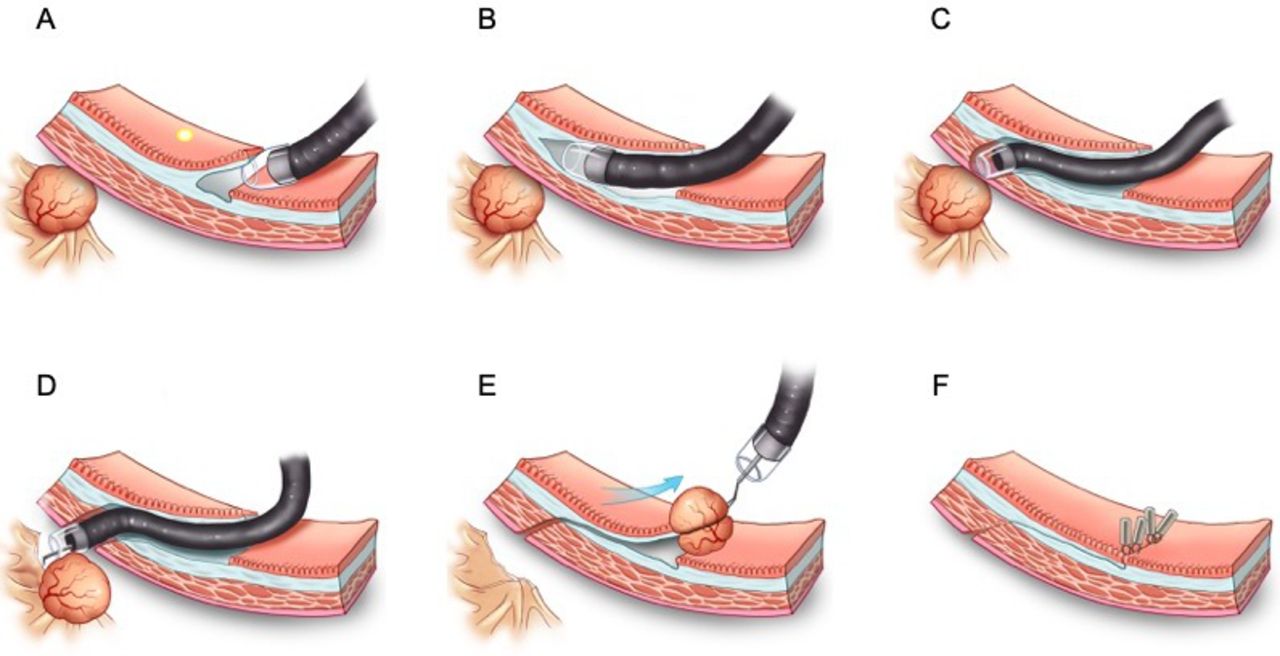
The patient is under general anaesthesia with endotracheal intubation. Prophylactic intravenous antibiotics are introduced 30 min before the procedure. The procedure includes six steps as follows (figure 2):

Illustration of the technique. (A) Submucosal injection and mucosal incision. (B) Creation of submucosal tunnel. (C) Full-thickness myotomy. (D) Tumour dissection. (E) Tumour extraction. (F) Closure of mucosal entry.
Step 1: Mucosal incision. A submucosal injection is performed followed by a 2 cm longitudinal mucosal incision made at 5 cm above the tumour site as the tunnel entry.
Step 2: Submucosal tunnelling. A submucosal longitudinal tunnel is created towards the tumour location by using a technique similar to STER between the mucosal and muscular layers.
Step 3: Full-thickness myotomy. It is performed above the estimated location of the mediastinal tumour.
Step 4: Tumour dissection. Dissection of the surrounding tissues is well performed at very close distance to the tumour capsule but still with the aim to achieve an en bloc resection.
Step 5: Tumour extraction. By using a snare, the tumour is extracted from the mediastinum to oesophageal cavity and out of the patient followed by a careful inspection of the submucosal tunnel for any evidence of bleeding sites.
Step 6: The closure of the mucosal incision is achieved by placement of several metallic clips. Any mucosal injury or perforation should also be clipped to avoid mucosal leakage.
Video description
The online supplementary video presents a successful case of removing a schwannoma in the posterosuperior mediastinum by transoesophageal endoscopic surgery with an operative time of 50 min (figure 3). During the procedure, subcapsular enucleation was difficult to realise, sacrificing the nerve is inevitable in this situation in order to resect the tumour completely.
Supplementary video

{kind=link}
{kind=link}
{kind=link}
Transoesophageal endoscopic surgery for treatment of a schwannoma in the mediastinum. (A) Visualisation of a mediastinal tumour under CT of the chest (yellow spot). (B) A smooth elevated lesion 23 cm from the incisors. (C) Submucosal injection and mucosal incision 5 cm proximal to the lesion towards submucosal space. (D) Full-thickness myotomy and clear exposure of the tumour. (E) Tumour dissection and extraction. (F) Completion of tumour resection. (G) Closure of mucosal entry. (H, I) Four-month follow-up OGD and vocal cords evaluations.
Postoperative course
Our patient presented with choke and hoarseness on postoperative day (POD) 1, an endoscopy inspection was done immediately and it showed that the left side of the vocal cord was fixed, the glottis was opening which bears out earlier diagnosis that it is a schwannoma in the mediastinum that originates from left recurrent laryngeal nerve. CT scan showed no abnormality, and the patient was discharged on POD 3. On routine follow-up 4 months later for this patient, his symptom is relieved and epiglottis is oedema but function compensatory, and oesophageal anatomy is recovered.
Comments
The anatomy of the mediastinum involves various important structures like heart, lung, aorta, trachea, oesophagus and other important structures. Transoesophageal endoscopic surgery for mediastinal tumours is a novel technique combining STER and NOTES and uses the narrow submucosal tunnel or ‘third space’ as an operating entry into the mediastinal cavity. It may have the advantage of a much less invasive approach, but also several potential risks should be considered such as potential complications due to the oesophageal approach with opening the lumen with the tunnel technique and violation of vital structures in the mediastinum with the need of urgent surgical salvage. So the correct setting should be determined which this procedure should be performed, possibly in the operating theatre with a surgical backup team.
For these reasons, to ensure the procedure to be efficient, precise and above all safe, utmost care should be taken. All patients should have chest CT and EUS preoperatively to make sure the location of the tumour, including the distance from incisors, direction and its relationship with oesophageal wall, vascular and other important structures. Immediately before dissection, tumour location is reconfirmed by EUS. Our case had a clear-cut bulging in the oesophagus making orientation straightforward. For other cases without bulging seen on luminal endoscopy, more care has to be taken to get the right approach. Possible solutions are injection of India ink or indigo carmine at the tumour site is needed, possibly under EUS guidance. Also preprocedural use of EUS, conventional or perhaps better with a miniprobe, should be considered.
For the procedure itself, as with POEM and STER, a transparent cap is attached to the tip of the gastroscope to improve operative field exposure. Carbon dioxide should be used to avoid overinflation during the operating procedure. Once the operative field is clear, dissection close to the tumour capsule should be done as soon as possible to avoid any unnecessary injury to the surrounding structures. Postoperative monitoring is also important according to the tumour site and its surrounding structures. Repeated postoperative endoscopic inspections and timely supportive treatments were done in this case to save the maximum function after sacrificing the recurrent laryngeal nerve.
Since transoesophageal endoscopic surgery for mediastinal tumour is a high-demanding procedure, both preoperative evaluation and expertise of an experienced endoscopist are essential. Consultation and support of cardiothoracic surgeons and neurosurgeons are also needed in complicated cases. Further clinical studies with a larger number of patients are necessary to confirm the indication, to systemically evaluate its utility and to assess critical surgical parameters such as morbidity, operative time, postoperative stay, postoperative pain and procedure-related adverse events compared with the open approach. Equally importantly, all these cases should be done under study conditions.
Footnotes
PG and QL contributed equally.
Contributors PG and QL contributed equally to this work. PG and QL collected the data and wrote the manuscript. JH, JX, SL, MC, LM, WC, YZ, SC, YZ and LY contributed to clinical review and discussion. PZ designed the study, provided the case and made critical revisions. All authors approved the final version of the manuscript.
Funding This study was funded by the National Natural Science Foundation of China (Grant: 81902394, 81873552 and 81670483).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; internally peer reviewed.