Article Text

Statistics from Altmetric.com
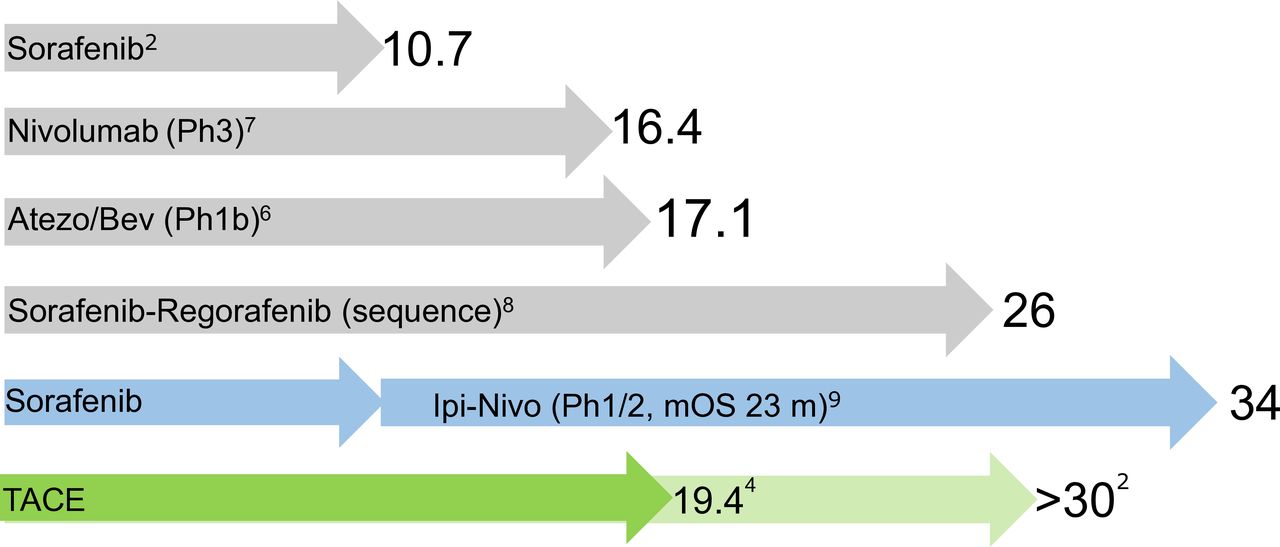
We read with interest the recent Gut roundtable paper by Gerbes et al. As highlighted by these authors, treatment of HCC has rapidly changed1: currently, four tyrosine kinase inhibitors, ramucirumab and two immune checkpoint inhibitors (ICP) are approved in different lines of treatment.2 3 Survival of patients with advanced disease have improved correspondingly, and more progress is expected from the burgeoning of trials of ICP-based combination treatment schemas (figure 1).

Schematic representation of the development in the treatment of advanced-stage HCC based on median overall survival (mOS) data from some recent trials. The arrows are proportional to the reported (grey) or hypothetical (blue) mOS indicated by the respective numbers. The green overlapping arrows represent respectively the real-world and the expected survival (ie, based on the selection of ‘ideal’ candidates for TACE) in BCLC-B patients. The list of trials is not exhaustive and, due to the heterogeneity of patients’ population, not suitable for direct cross-comparison between the trials. Atezo/Bev: combined atezolizumab and bevacizumab; pH, phase of clinical study; TACE, trans-arterial chemoembolisation.
Due to the increasing efficacy of pharmacological treatment, many physicians are inclined to initiate systemic therapy, rather than trans-arterial chemoembolisation (TACE), in patients with more advanced intermediate-stage HCC (patients with more numerous or large lesions) or to switch earlier from TACE to systemic treatment. This propensity is accentuated by studies increasingly highlighting some limitations of the current use of locoregional treatment: median overall survival (mOS) under TACE treatment, expected to amount to over 30 months in well-selected patients, doesn’t exceed 20 months in population-based studies.4 Moreover, repeated TACE are also known to cause some extent of unintended collateral damage to non-tumour liver, since a deterioration of liver function has been observed in up to 30% of patients treated by TACE.5 Liver function being a major determinant of survival in HCC patients, this implies that TACE may not only be unnecessary, but even noxious in ‘non-responders’. With these facts in mind, and with mOS of Barcelona Clinic Liver Cancer (BCLC)-C patients approaching 2 years,6–8 shouldn’t it be expected that this improving effectiveness of systemic treatment would become even more evident in BCLC-B patients, and that systemic agents should be used instead of TACE in this tumour stage (figure 1)?
The likely answer is: no. For one, TACE may be effective in treating lesions not responsive to systemic treatment until ‘unTACEable progression’ (a concept most recently applied by Masatoshi Kudo in the TACTICS trial); moreover, TACE might boost the response to immunological agents by causing tumour-specific antigen release. To this regard, with much emphasis put on the ‘abscopal’ effect, and with no exceptions known to us, current studies of combination treatment with TACE are designed to administer immunological agents either during or after TACE.
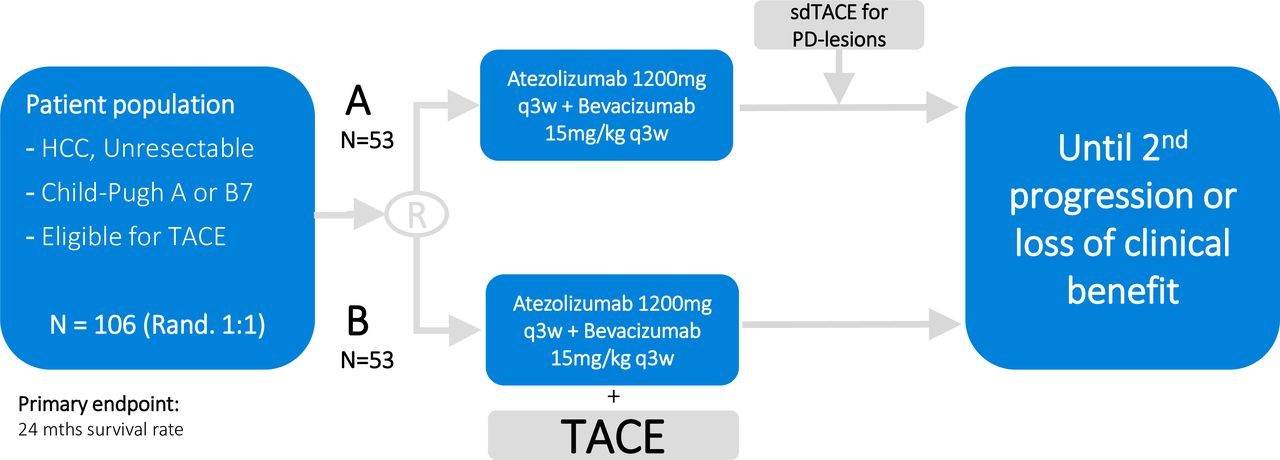
We propose here a novel concept for treatment of intermediate-state HCC by which (1) ICP are initiated first, (2) TACE is performed only on detection of radiological progression, (3) is directed only towards single progressive lesions and (4) repeated until untreatable progression. This study design is implemented in the randomised study DEMAND (EUDRACT 2019-002430-36), where TACE candidates are randomised either to a TACE-‘on demand’ or to a synchronous-treatment arm with atezolizumab/bevacizumab (figure 2).
{kind=link}
{kind=link}
Schematic representation of the DEMAND study, a randomised, two-arm non-comparative phase II study on the efficacy of atezolizumab and bevacizumab (Atezo/Bev) followed by on-demand selective TACE (sdTACE) on detection of disease progression (PD), or of initial synchronous treatment with TACE and Atezo/Bev on 24 months survival rate in the treatment of unresectable hepatocellular carcinoma patients. The use of local ablation is allowed for lesions which cannot be targeted sufficiently selectively by TACE. TACE, trans-arterial chemoembolisation.
This approach is based on the observation that objective response to ICP (expected in approximately one-third of all patients) translates into excellent survival9 and is evident early.10 Delaying the use of TACE to the time-point of progression (should this ever occur) and confining it to targeting of progressive lesions, will altogether reduce the number of patients and the proportion of liver parenchyma exposed to the collateral damage potentially caused by TACE. Most likely, however, this will not lessen the beneficial immunogenic effect of locoregional treatment, which is thought to be independent of the targeted tumour volume (abscopal effect). Initiating ICP first will also leave tumour vessels open to drug delivery and to the access of circulating lymphocytes.
In summary, while systemic treatment alone might soon exceed the real-life benefits of TACE, combination currently likely remains the best option. However, initiating ICP-based systemic treatment first would select treatment-resistant tumour lesions—rather than individuals—as target of TACE. This may not reduce the benefits of the combination but could save liver function, thus translating into a survival benefit and contributing to solve the yearlong dilemma of when to start and stop TACE.
Footnotes
Contributors ENDT has written this manuscript on behalf of the DEMAND study group.
Funding The author has not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests ENDT has served as a paid consultant for AstraZeneca, Bayer, BMS, EISAI, Eli Lilly & Co, Pfizer, IPSEN, and Roche. He has received reimbursement of meeting attendance fees and travel expenses from Arqule, BMS, Bayer, Celsion and Roche and lecture honoraria from BMS and Falk. He has received third-party funding for scientific research from Arqule, AstraZeneca, BMS, Bayer, Eli Lilly and Roche.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; internally peer reviewed.