Article Text

Abstract
Objective The use of tenofovir (TDF) and entecavir (ETV) in patients with chronic hepatitis B (CHB) has led to a decrease in the incidence of hepatocellular carcinoma (HCC) and liver-related events. However, whether there is a difference between the two agents in the extent of improving such outcomes has not been clarified thus far. Therefore, we aimed to compare TDF and ETV on the risk of HCC and mortality.
Design A total of 7015 consecutive patients with CHB who were treated with TDF or ETV between February 2007 and January 2018 at the liver units of the Catholic University of Korea were screened for study eligibility and 3022 patients were finally analysed. Study end points were HCC and all-cause mortality or liver transplantation (LT) within 5 years after the initiation of antiviral therapy. Propensity score matching (PSM) and inverse probability of treatment weighting methods were used.
Results No difference was observed between TDF and ETV in the incidence rates of HCC in the entire cohort (HR 1.030; 95% CI 0.703 to 1.509, PSM model, p=0.880) and subgroups of patients with chronic hepatitis and cirrhosis. Also, no difference was observed between TDF and ETV in the incidence rates of all-cause mortality or LT in the entire cohort (HR 1.090; 95% CI 0.622 to 1.911, PSM model, p=0.763), and patients with chronic hepatitis and cirrhosis.
Conclusion This study has demonstrated the clinical outcomes in patients with CHB who received TDF or ETV treatment. There was no difference in the intermediate-term risk of HCC and mortality or LT between the two drugs.
- tenofovir
- entecavir
- hepatocellular carcinoma
- hepatitis B
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
The treatment with highly potent antiviral drugs tenofovir (TDF) and entecavir (ETV) for patients with chronic hepatitis B (CHB) has led to a decrease in the incidence of hepatocellular carcinoma (HCC) and liver-related events.
Although there has been no head-to-head randomised controlled trial that directly compared TDF and ETV, virologic, serologic and biochemical responses are reported to be similar but whether there is a difference between the two agents in the extent of decreasing incidence rates of HCC and mortality has not been clarified thus far.
What are the new findings?
No difference was observed between TDF and ETV in the incidence rates of HCC and all-cause mortality or liver transplantation in the entire cohort and in the subgroups of patients with chronic hepatitis and cirrhosis.
How might it impact on clinical practice in the foreseeable future?
HCC develops consistently even after treatment with highly potent antiviral drugs and in patients without cirrhosis, which indicate the importance of regular surveillance for HCC in all patients with CHB.
Introduction
The treatment with highly potent antiviral drugs for patients with CHB has led to a decrease in the incidence of HCC and liver-related events.1 2 The main factors associated with the improvement in such clinical outcomes are reported to be complete virologic (VR) and biochemical responses (BR).3 4 Regression of fibrosis and improved liver function with long-term antiviral treatment, which have been verified in a prospective study, may also be related to the decreased risk of HCC and mortality.5
ETV and TDF, which were approved for use in Korea since 2007 and 2012, respectively, are currently recommended as the first-line therapy in patients with CHB. Both drugs display high genetic barriers with very low rates of resistance and high rates of viral suppression. Although there has been no head-to-head randomised controlled trial that directly compared the two drugs, the rates of HBV DNA suppression, Hepatitis B e Antigen (HBeAg) seroconversion and normalisation of alanine aminotransferase (ALT) are reported to be comparable in treatment-naïve adult patients with CHB and immune-active disease.6
However, recently Choi et al have suggested for the first time that TDF treatment was more effective compared with ETV in lowering the risk of HCC in a propensity score-matched, population-based cohort study.7 On the contrary, Kim et al have reported in their longitudinal observational study that there was no difference between the two drugs.8 The emergence of these conflicting data necessitates additional validation in a large-scale, real-world cohort.
Therefore, we aimed to compare TDF and ETV on the risk of HCC and mortality or liver transplantation (LT) in a propensity-matched, large-scale cohort with follow-up period of 5 years.
Methods
Patients
A total of 7015 patients with CHB who were treated with TDF or ETV between February 2007 and January 2018 at the liver units of the Catholic University of Korea were screened for study eligibility. We have excluded the patients with HCV or HIV infection, antiviral therapy <6 months, HCC or LT prior to or within 6 months after initiation of antiviral therapy, other malignancies at baseline, treatment-experienced patients and patients with decompensated cirrhosis from the analysis. The remaining 3022 patients (1439 with TDF, 1583 with ETV) were finally analysed (figure 1).

Flow diagram for the patient selection process. ETV, entecavir; HCC, hepatocellular carcinoma; LT, liver transplantation; PS, propensity score; TDF, tenofovir.
The two groups were compared using a general model and after propensity score matching (PSM). Besides the analysis of the entire population, we also performed subanalyses after stratification according to the severity of underlying liver disease in order to explore the risk reduction effects of the two drugs in various patient populations. This study was approved by the institutional review board of the Catholic University of Korea (XC19REDI0028H).
Assessment
The patients were regularly examined with abdominal ultrasound (US) and blood tests including complete blood count, blood chemistry, alpha-fetoprotein (AFP) and viral markers HBsAg/Ab, HBeAg/Ab and HBV DNA every 3–6 months. Currently in Korea, abdominal US and AFP every 6 months as surveillance tests for HCC are almost fully reimbursed by the national health insurance for patients infected with HBV, HCV and with liver cirrhosis from any cause. Dynamic CT scan or MRI scan were performed when HCC was suspected in the US or an increase in AFP was observed. TDF became available in Korea from December 2012 and therefore, the analysis was censored at 5 years after the initiation of antiviral therapy.
The end points of this study were HCC and all-cause mortality or LT between the two groups. However, we have also analysed and compared the incidence rates of non HCC-related mortality or LT, and liver-related mortality or LT between the two groups.
Definitions
HCC was defined as a mass sized ≥1 cm showing arterial phase hyperenhancement and washout in four-phase dynamic CT or contrast enhance MRI.9 All-cause mortality included death from any cause during the follow-up period, non HCC-related mortality consisted of all deaths but with the exclusion of HCC-related death and liver-related mortality was defined as death due to complications of liver cirrhosis. The diagnosis of liver cirrhosis was made comprehensively from liver biopsy, abdominal US or fibroscan. For objective evaluation of advanced fibrosis, we also analysed the patients according to aspartate aminotransferase (AST) to Platelet Ratio Index (APRI) score and fibrosis-4 (FIB-4) index. VR was defined as HBV DNA <20 IU/mL and BR was defined as ALT ≤40 U/L.3 10
Statistical analysis
For the comparison of the categorical variables, χ2 test was used and for continuous variables, independent T-test was used. Competing risk analysis was conducted for the interpretation of the cumulative incidence of HCC with death and lost to follow-up considered as competing risks. In order to compare the hazards and cumulative incidence functions between the two groups, proportional hazard model by Fine and Gray for the subdistributions was used. For the analysis of cumulative incidences of mortality or LT, the outcome variables were estimated using the Kaplan-Meier method and comparison of HRs between the two groups was done using the Cox proportional hazard model. Multiple imputation method was used to estimate the missing values, which comprised 0%–4.6% of the baseline laboratory data.
PSM analysis was used to reduce bias by equating the two groups based on the following variables: age, sex, severity of underlying liver disease, APRI, FIB-4 index, diabetes mellitus, hypertension, body mass index, alcohol drinking, oesophageal varix, AST, ALT, total bilirubin, albumin, creatinine, gamma-glutamyl transferase, prothrombin time (PT), platelet count, Child-Pugh score, HBeAg status, HBV DNA and AFP. The PSM was performed using the nearest-neighbour 1:1 matching method with a calliper width of 0.2 of the pooled SD of the logit of the propensity score. Also, for the analyses of all subgroups, new weights were calculated accordingly. Inverse probability of treatment weighting (IPTW) analysis was also carried out using the same variables to confirm the results of the PSM analysis on the cumulative risk of HCC and all-cause mortality or LT. For the analysis of VR, BR and combined VR and BR, we also applied the weighted PSM approach in patients without missing values from year 1 to year 5.
SAS software V.9.4 (SAS Institute) was used for analyses and p values <0.05 were considered to be statistically significant.
Results
Baseline characteristics
A total of 3022 patients were analysed with 1439 patients on TDF and 1583 patients on ETV in the general model. Following PSM, a total of 2740 patients were analysed with 1370 patients on TDF and 1370 patients on ETV. After PSM, the mean age of the patients was 47 years, 58% were male and 34% of the patients had cirrhosis. Fifty-nine per cent of the patients were positive for HBeAg, and the median HBV DNA was 6.4 log IU/mL (table 1). For subanalyses, the baseline characteristics of the chronic hepatitis and patients with cirrhosis were individually evaluated and analysed in detail after PSM (online supplementary tables 1, 2). The median and mean follow-up period of the two groups were 36.4 and 36.6 months in the TDF group, and 60 and 51.5 months in the ETV group, respectively.
Supplemental material
Baseline characteristics—entire cohort (general model and PSM model)
Hepatocellular carcinoma
HCC developed in a total of 134 patients during follow-up with 50 patients (3.5%) in the TDF group and 84 patients (5.3%) in the ETV group in general model. After propensity matching, HCC developed in 47 patients (3.4%) in the TDF group and 64 patients (4.7%) in the ETV group. There was no difference in the cumulative incidences of HCC in the general model and after PSM (figure 2A and B). The 5-year cumulative incidence rates were 5.587% in the TDF group and 5.459% in the ETV group (HR 0.912; 95% CI 0.638 to 1.303; p=0.613) in the general model, and 5.292% in the TDF group and 4.816% in the ETV group (HR 1.030; 95% CI 0.703 to 1.509; p=0.880) after PSM (table 2).

Cumulative incidences of HCC. (A) Entire cohort, general model. (B) Entire cohort, PSM model. (C) Chronic hepatitis patients, general model. (D) Chronic hepatitis patients, PSM model. (E) Liver cirrhosis patients, general model. (F) Patients with liver cirrhosis, PSM model. The 5-year cumulative incidence rates according to each antiviral drug are expressed in percentages in the figure. HCC, hepatocellular carcinoma; PSM, propensity score matching.
Comparison of incidence of HCC and death or LT
Also in patients with chronic hepatitis, no difference was observed (figure 2C and D) with 5-year cumulative incidence rates of 1.861% in the TDF group and 1.727% in the ETV group (HR 1.031; 95% CI 0.481 to 2.211; p=0.937) in the general model, and 1.725% in the TDF group and 1.890% in the ETV group (HR 0.923; 95% CI 0.420 to 2.028; p=0.841) after PSM.
No difference was observed in patients with cirrhosis (figure 2E and F) with 5-year cumulative incidence rates of 12.658% in the TDF group and 12.196% in the ETV group (HR 0.916; 95% CI 0.613 to 1.369; p=0.669) in the general model, and 12.171% in the TDF group and 11.471% in the ETV group (HR 0.956; 95% CI 0.614 to 1.488; p=0.842) after PSM.
In addition, for objective evaluation of advanced fibrosis, we performed subanalyses according to APRI score and FIB-4 index. No difference was observed in the risk of HCC between TDF and ETV in patients depending on the APRI score, and the FIB-4 index score, respectively (online supplementary figures 1, 2). IPTW analysis also showed that there was no difference in the risk of HCC between the two groups (online supplementary figure 3). We also performed PSM analysis with year 1 VR, year 1 BR and year 1 combined VR and BR as matching covariates, respectively. No difference in the incidence rates of HCC was observed in all cases (online supplementary figure 4).
Supplemental material
Supplemental material
Supplemental material
Supplemental material
In the multivariate analyses of the patients with chronic hepatitis and cirrhosis, the usage of either TDF or ETV was not associated with HCC. The factors associated with HCC development after univariate and multivariate analyses according to subgroups are shown in online supplementary tables 5 and 6.
All-cause mortality or LT
A total of 59 patients died or received LT during follow-up with 22 patients (1.5%) in the TDF group and 37 patients (2.3%) in the ETV group in general model. After propensity matching, death or LT occurred in 20 patients (1.5%) in the TDF group and 28 patients (2.0%) in the ETV group. There was no difference in the cumulative incidences of mortality or LT in the general model and after PSM (figure 3A and B). The 5-year cumulative incidence rates were 2.406% in the TDF group and 2.929% in the ETV group (HR 1.052; 95% CI 0.614 to 1.804; p=0.853) in the general model, and 2.317% in the TDF group and 2.512% in the ETV group (HR 1.090; 95% CI 0.622 to 1.911; p=0.763) after PSM (table 2).
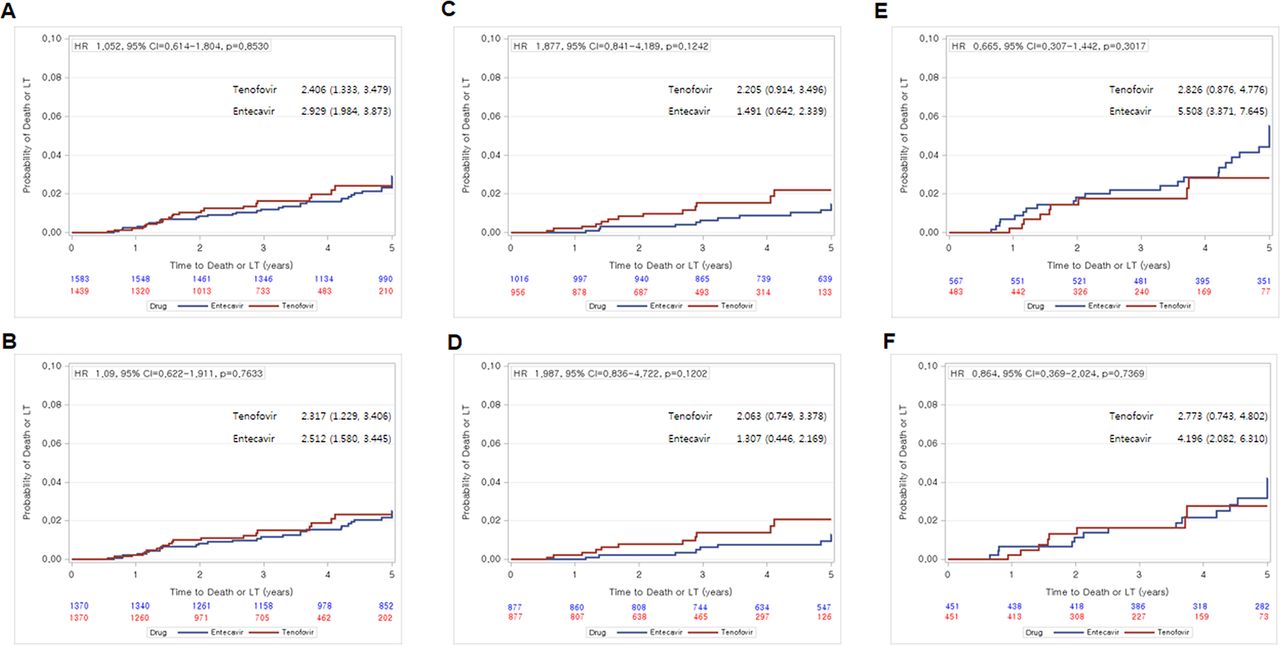
Cumulative incidences of death or LT. (A) Entire cohort, general model. (B) Entire cohort, PSM model. (C) Patients with chronic hepatitis, general model. (D) Patients with chronic hepatitis, PSM model. (E) Patients with liver cirrhosis, general model. (F) Patients with liver cirrhosis, PSM model. The 5-year cumulative incidence rates according to each antiviral drug are expressed in percentages in the figure. LT, liver transplantation; PSM, propensity score matching.
Also in patients with chronic hepatitis, no difference was observed (figure 3C and D) with 5-year cumulative incidence rates of 2.205% in the TDF group and 1.491% in the ETV group (HR 1.877; 95% CI 0.841 to 4.189; p=0.124) in the general model, and 2.063% in the TDF group and 1.307% in the ETV group (HR 1.987; 95% CI 0.836 to 4.722; p=0.120) after PSM.
No difference was observed in patients with cirrhosis (figure 3E and F) with 5-year cumulative incidence rates of 2.826% in the TDF group and 5.508% in the ETV group (HR 0.665; 95% CI 0.307 to 1.442; p=0.302) in the general model, and 2.773% in the TDF group and 4.196% in the ETV group (HR 0.864; 95% CI 0.369 to 2.024; p=0.737) after PSM.
IPTW analysis also showed that there was no difference in the risk of all-cause mortality or LT between the two groups (online supplementary figure 3). We additionally performed detailed PSM analyses on non HCC-related mortality or LT, and liver-related mortality or LT. The results showed that there were no differences in all end points regarding mortality or LT (online supplementary figures 5, 6). The full details of the patients who experienced liver-related deaths or LT are summarised in online supplementary table 4.
Supplemental material
Supplemental material
In the multivariate analyses of the patients with chronic hepatitis and cirrhosis, the usage of either TDF or ETV was not associated with mortality or LT. The factors associated with all-cause mortality or LT after univariate and multivariate analyses according to subgroups are shown in online supplementary tables 7 and 8.
Virologic and biochemical responses
TDF showed higher VRs after PSM at years 4 and 5 (figure 4A and B). There were no differences in the VRs at years 1, 2 and 3 with 76.2% VR in the ETV group and 81.7% VR in the TDF group at year 1. However, at years 4 and 5, significantly higher VRs were observed in the TDF group. At year 5, the VRs were 91.6% in the ETV group and 97.7% in the TDF group (p=0.001) after PSM.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Virologic and biochemical responses. (A) Virologic response, general model. (B) Virologic response, PSM model. (C) Biochemical response, general model. (D) Biochemical response, PSM model. (E) Combined virologic and biochemical response, general model. (F) Combined virologic and biochemical response, PSM model.
The rates of BR were similar between the two groups but slightly higher tendency was observed in the ETV group (figure 4C and D). There were no differences at years 1, 3, 4 and 5 between the two groups after PSM with BRs of 82.3% and 89.7% in the ETV group, and BRs of 76.7% and 86.8% in the TDF group at years 1 and 5, respectively. However at year 2, higher BR was observed in the ETV group with 86.2% in the ETV group and 81% in the TDF group (p=0.046) after PSM.
No difference was observed in the rates of combined VR and BR from year 1 to year 5. After PSM, the rates of combined VR and BR were 66.8% and 82.9% in the ETV group and 62.6% and 83.2% in the TDF group at years 1 and 5, respectively (figure 4E and F).
Discussion
This large-scale, PS-matched cohort study explored the comparative risk reduction effects of TDF and ETV on HCC, mortality and LT. No difference was observed between TDF and ETV in the 5-year cumulative risk of HCC development and all-cause mortality or LT. There were no differences between the two groups in the general model, after PSM, and in subgroups of patients with chronic hepatitis and cirrhosis.
Hepatic carcinogenesis consists of complex multistep processes including chronic inflammation, angiogenesis, HBV integration and metabolic, oxidative injuries leading to genetic errors and mutations over a substantial period of time.11 12 Also, in various clinical studies, factors such as age, sex, degree of liver fibrosis and higher HBV DNA in the long term have been reported to be associated with HCC in patients infected with HBV.13 14 For example, Chen et al and the REVEAL-HBV study group have reported that HBV DNA higher than 10 000 copies/mL during a long mean follow-up of 11.4 years was a strong predictor of HCC.15 Therefore, considering the high potency and low resistance rates of ETV and TDF, the effects of the two drugs on HBV suppression and thus HCC risk reduction are highly likely to be similar especially in short or intermediate terms. Correspondingly in our data, the rates of HCC did not differ between the two groups, although PS-matched VRs were slightly higher in the TDF group at years 4 and 5. The similar rates of HCC development despite the differences in VR may have been related to the relatively short duration of higher VR, the strict VR definition of 20 IU/mL or yet unidentified causes such as environmental, lifestyle, or metabolic factors. Moreover, the rates of BR and combined VR and BR were comparable between the two groups.
Our results were contradictory to the article recently published regarding this issue. Choi et al have suggested that TDF treatment was associated with a significantly lower risk of HCC during 4 years of follow-up.7 The notable differences between the two studies were observed in parameters of PSM and baseline characteristics of the patients. Their population-based cohort had comparatively smaller number of PSM parameters with no HBV DNA and laboratory parameters of liver function such as bilirubin, albumin, platelet counts and PT. Also, in their validation cohort, higher proportion of 58% had baseline cirrhosis compared with 34% in our study. It is difficult to exactly determine whether these differences in study design and baseline characteristics have led to different conclusions. However, in our study, we have tried to include all necessary variables known to be associated with the prognosis of patients with HBV for PSM and performed meticulous subgroup analyses according to the severity of underlying liver disease. Especially, we aimed to be as objective as possible in defining patients with advanced liver fibrosis or cirrhosis by using three different indices. All of the results from the detailed subgroup analyses were consistent and showed that 5-year cumulative risk of HCC were not different between the two groups.
Moreover, HCC is the primary cause of death in patients with CHB taking up 30%–40% of all causes.16 17 Correspondingly in our data, of the 59 patients who died during follow-up, 21 patients (35%) died due to HCC. However in the article by Choi et al, differences in the risk of HCC between the two drugs were observed in both nationwide and validation cohorts but no difference was observed regarding death or transplant. Difference in the risk of HCC but no difference in mortality indicates that more patients may have died in the TDF group than the ETV group due to other reasons such as other malignancies or decompensation events which are the second and third most common causes of death in patients with CHB.17 Collectively, it is our opinion that discrepancy between the risk of HCC and death or transplant and the difference between the two drugs in the risk of HCC development in the article by Choi et al should be further evaluated.
In addition, no difference in the rates of all-cause mortality or LT was observed between the two groups. Our results were consistent with the results from the randomised, observational study of entecavir to assess long-term outcomes (REALM) study, which was conducted for 10 years with average follow-up period of 7 years that showed no difference between ETV and non-ETV antivirals in overall malignant neoplasm, deaths and HCC.18 We also analysed non-HCC-related mortality and liver-related mortality to show in detail that there was no difference between the two groups. We also observed with interest that only a very few patients with chronic hepatitis or compensated cirrhosis died or received LT (eight patients, 0.3%) due to liver-related events other than HCC after treatment with highly potent antivirals such as ETV or TDF in the intermediate term.
Virological on-therapy remission and maintained virologic response (MVR) are both very important in patients with CHB to reduce decompensation events, HCC and improve survival. However, unlike decompensation events which are basically associated with inflammatory processes in the liver, the development of HCC requires multifactorial carcinogenesis over a substantial period of time. Therefore, in patients who receive highly potent antiviral drugs such as TDF or ETV, the sole difference in VR, particularly under strict VR definition, may not be sufficient to incur difference in the risk of HCC in short or intermediate terms. Our opinion is in line with two previous reports. Papatheodoridis et al have shown that VR did not significantly affect the incidence of HCC during a median follow-up of 4.7 years.19 Also, Jang et al have reported that MVR was not an independently significant predictor of HCC but was associated with survival in patients with HBV-related decompensated cirrhosis in their 10-year observation study.3 Presumably in some patients, even full virologic suppression may not be sufficient to overcome the already established carcinogenic processes such as HBV integration, genomic instability and completely eliminate the possibility of HCC.
There were a few limitations in this study. First, it was not a long-term but an intermediate-term study, although the follow-up period of 5 years is the longest so far regarding this issue, a long-term study of >10 years would be able to draw more definitive conclusions. Second, this study was carried out without randomisation and retrospectively which may have resulted in selection bias but we tried to minimise such limitation by PSM and IPTW analyses. Third, we did not thoroughly investigate patient adherence to antiviral therapy which may have influenced the VR, especially in the ETV group.20 The strengths of this study were that it was a large-scale, real-world, propensity-matched cohort with >7000 consecutive patients screened, and >3000 patients analysed. In addition, we have performed detailed subgroup analyses which made our data more reliable. Finally, we have investigated for the first time, PS-matched VR, BR and combined VR and BR every year during the follow-up period, which was essential for the explanation of the clinical outcomes considering that this study aimed to compare the effects of two antiviral drugs.
In conclusion, this study has demonstrated the clinical outcomes in patients with CHB who received TDF or ETV treatment. There was no difference in the intermediate-term risk of HCC and all-cause mortality or LT between the two drugs.
Acknowledgments
The authors would like to thank the Department of Biostatistics of the Catholic Research Coordinating Center for statistical consultation.
Footnotes
SWL and JHK contributed equally.
Presented at This study was previously presented as part of a poster presentation at The International Liver Congress 2019.
Contributors SWL, JHK, JWJ: study concept and design, writing of the manuscript, data collection, statistical analysis and interpretation of the data. HLL, SHY, HCN, PSS: data collection and management. SWN, SHB, JYC, SKY, NIH: patient management and critical revision.
Funding This study was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Science, ICT and Future Planning (NRF-2019R1A2C1009439).
Competing interests None declared.
Patient consent for publication Waiver of informed consent was obtained from the institutional review board of the Catholic University of Korea due to the retrospective nature of this study.
Ethics approval This study was approved by the institutional review board of the Catholic University of Korea (XC19REDI0028H).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.