Article Text

Abstract
Iron deficiency anaemia (IDA) is a major cause of morbidity and burden of disease worldwide. It can generally be diagnosed by blood testing and remedied by iron replacement therapy (IRT) using the oral or intravenous route. The many causes of iron deficiency include poor dietary intake and malabsorption of dietary iron, as well as a number of significant gastrointestinal (GI) pathologies. Because blood is iron-rich it can result from chronic blood loss, and this is a common mechanism underlying the development of IDA—for example, as a consequence of menstrual or GI blood loss.
Approximately a third of men and postmenopausal women presenting with IDA have an underlying pathological abnormality, most commonly in the GI tract. Therefore optimal management of IDA requires IRT in combination with appropriate investigation to establish the underlying cause. Unexplained IDA in all at-risk individuals is an accepted indication for fast-track secondary care referral in the UK because GI malignancies can present in this way, often in the absence of specific symptoms. Bidirectional GI endoscopy is the standard diagnostic approach to examination of the upper and lower GI tract, though radiological scanning is an alternative in some situations for assessing the large bowel. In recurrent or refractory IDA, wireless capsule endoscopy plays an important role in assessment of the small bowel.
IDA may present in primary care or across a range of specialties in secondary care, and because of this and the insidious nature of the condition it has not always been optimally managed despite the considerable burden of disease— with investigation sometimes being inappropriate, incorrectly timed or incomplete, and the role of IRT for symptom relief neglected. It is therefore important that contemporary guidelines for the management of IDA are available to all clinicians. This document is a revision of previous British Society of Gastroenterology guidelines, updated in the light of subsequent evidence and developments.
- iron deficiency
- anaemia
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Executive summary of recommendations and practice statements
Background
Iron deficiency anaemia (IDA) is common, and a major cause of morbidity worldwide (evidence quality—high, consensus—100%, statement strength—strong).
IDA can be caused by a range of GI pathologies including cancer, and so GI investigation on an urgent basis should be considered in adults with a new diagnosis of IDA without obvious explanation (evidence quality—high, consensus—85%, statement strength—strong).
Definitions
We recommend that anaemia is defined as a haemoglobin (Hb) concentration below the lower limit of normal for the relevant population and laboratory performing the test (evidence quality—medium, consensus—100%, statement strength—strong).
We recommend that iron deficiency should be confirmed by iron studies prior to investigation. Serum ferritin is the single most useful marker of IDA, but other blood tests (eg, transferrin saturation) can be helpful if a false-normal ferritin is suspected (evidence quality—medium, consensus—92%, statement strength—strong).
We recommend that a good response to iron therapy (Hb rise ≥10 g/L within a 2-week timeframe) in anaemic patients is highly suggestive of absolute iron deficiency, even if the results of iron studies are equivocal (evidence quality—medium, consensus—100%, statement strength—strong).
Initial clinical assessment
We recommend taking a detailed history, as it may provide important clues as to the cause(s) of IDA in the individual case (evidence quality—low, consensus—100%, statement strength—strong).
We recommend that initial investigation of confirmed IDA should include urinalysis or urine microscopy, screening for coeliac disease (CD) and in appropriate cases, endoscopic examination of the upper and lower GI tract (evidence quality—moderate, consensus—85%, statement strength—strong).
CD is found in 3%–5% of cases of IDA, and we recommend that it should be routinely screened for serologically, or on small bowel biopsy at the time of gastroscopy (evidence quality—high, consensus—84%, statement strength—strong).
Age, sex, Hb concentration and mean cell volume are all independent predictors of risk of GI cancer in IDA, and need to be considered as part of a holistic risk assessment. It follows that the cancer risk in iron deficiency without anaemia is low (evidence quality—high, consensus—92%, statement strength—strong).
There are insufficient grounds at present to recommend faecal immunochemical testing for risk stratification in patients with IDA. The evidence base is evolving rapidly, however, and on that basis, this guidance may therefore change (evidence quality—low, consensus—100%, statement strength—weak).
We recommend that in men and postmenopausal women with newly diagnosed IDA, gastroscopy and colonoscopy should generally be the first-line GI investigations. In those not suitable for colonoscopy, CT colonography is a reasonable alternative (evidence quality—moderate, consensus—100%, statement strength—strong).
Follow-up and recurrent IDA
Hb levels normalise with iron replacement therapy (IRT) in most cases of IDA, but IDA recurs in a minority of these on long-term follow-up (evidence quality—low, consensus—92%, statement strength—strong).
Further evaluation of the small bowel
In those with negative bidirectional endoscopy of acceptable quality and either an inadequate response to IRT or recurrent IDA, we recommend further investigation of the small bowel and renal tract to exclude other causes (evidence quality—moderate, consensus—85%, statement strength—strong).
We recommend capsule endoscopy as the preferred test for examining the small bowel in IDA because it is highly sensitive for mucosal lesions. CT/MR enterography may be considered in those not suitable, and these are complementary investigations in the assessment of inflammatory and neoplastic disease of the small bowel (evidence quality—high, consensus—100%, statement strength—strong).
After a negative capsule endoscopy of acceptable quality, we recommend that further GI investigation needs to be considered only if there is ongoing IDA after IRT (evidence quality—high, consensus—100%, recommendation—strong).
We recommend that long-term IRT may be an appropriate strategy when the cause of recurrent IDA is unknown or irreversible (evidence quality—low, consensus—100%, statement strength—strong).
Treatment of IDA
We recommend that IRT should not be deferred while awaiting investigations for IDA unless colonoscopy is imminent (evidence quality—high, consensus—100%, statement strength—strong).
We recommend that the initial treatment of IDA should be with one tablet per day of ferrous sulphate, fumarate or gluconate. If not tolerated, a reduced dose of one tablet every other day, alternative oral preparations or parenteral iron should be considered (evidence quality—medium, consensus—92%, statement strength—strong).
Limited transfusion of packed red cells may on occasion be required to treat symptomatic IDA, in which case IRT is still necessary post-transfusion (evidence quality—high, consensus—100%, statement strength—strong).
We recommend that patients should be monitored in the first 4 weeks for an Hb response to oral iron, and treatment should be continued for a period of around 3 months after normalisation of the Hb level, to ensure adequate repletion of the marrow iron stores (evidence quality—medium, consensus—92%, statement strength—strong).
We recommend that parenteral iron should be considered when oral iron is contraindicated, ineffective or not tolerated. This consideration should be at any early stage if oral IRT is judged unlikely to be effective (see the Treatment section), and/or the correction of IDA is particularly urgent (evidence quality—high, consensus—92%, statement strength—strong).
There is insufficient evidence to support invasive investigation in non-anaemic iron deficiency unless there are additional indications (see the Definitions section), but periodic blood count monitoring is suggested (evidence quality—low, consensus—92%, statement strength—weak).
After the restoration of Hb and iron stores with IRT, we recommend that the blood count should be monitored periodically (perhaps every 6 months initially) to detect recurrent IDA (evidence quality—very low, consensus—85%, statement strength—strong).
Special situations—young women
IDA is common in young women, and major contributory factors include menstrual losses, pregnancy and poor dietary intake (evidence quality—high, consensus—100%, statement strength—strong).
Underlying GI pathology is uncommon in young women with IDA, and so after screening for CD, we recommend that further investigation is warranted only if there are additional clinical features of concern—as detailed in the text (evidence quality—moderate, consensus—92%, statement strength—strong).
If GI investigation in a pregnant woman is deemed necessary prior to delivery, gastroscopy and (after the first trimester) MR enterography are considered safe in pregnancy (evidence quality—low, consensus—91%, statement strength—strong).
Special situations—young men
Confirmed IDA is uncommon in young men, but when found we recommend that it warrants the same investigational algorithm as for older people (evidence quality—moderate, consensus—100%, statement strength—strong).
Special situations—the elderly
Iron deficiency is common in the elderly, and is often multifactorial in aetiology (evidence quality—high, consensus—100%, statement strength—strong).
We recommend that the risks and benefits of invasive endoscopic and alternative investigation(s) are carefully considered in those with major comorbidities and/or limited performance status (evidence quality—medium, consensus—92%, statement strength—strong).
Special situations—specific comorbidities
Functional iron deficiency (FID) is a common contributory factor to the anaemia associated with advanced chronic kidney disease (CKD) (evidence quality—high, consensus—92%, statement strength—strong).
Iron deficiency is common in chronic heart failure (CHF), and is often multifactorial (evidence quality—high, consensus—92%, statement strength—strong).
Parenteral IRT may improve symptoms and quality of life in CHF with FID (evidence quality—moderate, consensus—100%, statement strength—strong).
In the management of iron deficiency associated with CKD or CHF, reference to the appropriate specialist published guidelines is recommended (evidence quality—moderate, consensus—92%, statement strength—strong).
IDA is a common manifestation of IBD, particularly when the disease is active (evidence quality—high, consensus—100%, statement strength—strong).
Intolerance and malabsorption of oral IRT can be particular problems in the treatment of IBD-associated IDA, and parenteral IRT may be required (evidence quality—medium, consensus—100%, statement strength—strong).
Special situations—GI surgery
IDA is common following resection or bypass surgery involving the stomach and/or small bowel, including bariatric surgery (evidence quality—high, consensus—92%, statement strength—strong).
In new presentations of IDA, we recommend that a history of GI or bariatric surgery should not preclude a search for other causes of IDA (evidence quality—low, consensus—85%, statement strength—strong).
Service considerations
We recommend that all service providers should have clear points of referral and management pathways for patients with IDA (evidence quality—low, consensus—100%, statement strength—strong).
To ensure efficient use of resources, we recommend that IDA pathways should be delivered by a designated team led by a senior clinician (evidence quality—low, consensus—100%, statement strength—strong).
We recommend that service providers should aim to have an ambulatory care base for the administration of parenteral iron (evidence quality—low, consensus—100%, statement strength—strong).
Background
1. Iron deficiency anaemia (IDA) is common, and a major cause of morbidity worldwide (evidence quality—high, consensus—100%, statement strength—strong).
2. IDA can be caused by a range of GI pathologies including cancer, and so GI investigation on an urgent basis should be considered in adults with a new diagnosis of IDA without obvious explanation (evidence quality—high, consensus—85%, statement strength—strong).
Anaemia affects about a third of the global population and is a major cause of morbidity worldwide.1 2 Iron deficiency is one of the dominant causes, and the resulting anaemia (iron deficiency anaemia (IDA)) has a point prevalence of 2%–5% among adult men and postmenopausal women in the developed world.3–5
IDA is the most common form of anaemia seen in primary care in the UK. It is estimated to account for more than 57 000 emergency admissions to UK hospitals each year, costing the National Health Service (NHS) more than £55 million per annum.6
While menstrual loss is commonly the cause of IDA in premenopausal women, IDA in adult men and postmenopausal women is often due to chronic blood loss from the GI tract.4 5 7–12 IDA may be the first presenting manifestation of colonic or oesophago-gastric carcinoma, highlighting the importance of swift and complete investigation. There are however many other recognised causes of IDA (table 1) including malabsorption (most commonly from coeliac disease (CD) in the UK), poor dietary intake, blood donation, gastrectomy and use of non-steroidal anti-inflammatory drugs (NSAIDs). IDA is often multifactorial, and dual pathology (ie, significant disease in both upper and lower GI tract) is found in 1%–10% of cases—this should be particularly considered in the older patient.4 5 7–12
Pathological disorders associated with iron deficiency anaemia
IDA may present in primary care, or across a range of specialties in secondary care, and historically the management of IDA was often suboptimal—with investigation being slow, inadequate or incomplete.13–15 Over recent years, however, the recognition that IDA may reflect serious underlying GI pathology has resulted in increasing involvement of gastroenterology services. IDA may now account for 10% or more of all gastroenterology referrals, and a typical district hospital unit in the UK with a catchment of 250 000 may have in excess of 400 IDA referrals per annum.16 17
Scope
The objective of these guidelines is to summarise contemporary evidence on the diagnosis and management of IDA in adults, and to provide recommendations based on this in the light of developments since the original publication in 2000, last updated in 2011.18 The guidelines are primarily intended for health professionals in primary and secondary care in the UK, though many aspects are relevant to health services elsewhere in the world.
Method
These guidelines were commissioned by the British Society of Gastroenterology (BSG) in 2018, following a proposal approved by the Clinical Standards and Services Committee. They were developed in accordance with the BSG guideline process (revised version 2018) and the Agree II instrument.19 20
A committee of 13 members was convened from interested individuals representing a range of disciplines including gastroenterology, haematology, specialist nursing and patient groups, under the co-chairmanship of AFG and NB. Two lay members on the Guideline Committee represented patients and the general public. Following discussion of the scope and purpose of the guidelines and the key issues, a formal literature search was undertaken by the National Guidelines Centre using all subcategories of the term “iron deficiency anaemia”. Leads were identified to oversee the writing of section drafts based on a review of the relevant literature, and to produce draft sets of recommendations relevant to each section: Definitions—WT; Initial assessment—JS; Coeliac disease and further evaluation—RS; Treatment—ILPB; Special situations—MP, NB, AFG; Service considerations—RL. JS led on collating the consensus statements and editing the section drafts into a unified guideline document.
These recommendations were subject to three rounds of anonymised consensus voting by the full committee in an eDelphi exercise during 2020 using an online platform (ECD Solutions, Columbus, USA). Recommendations were modified in the light of feedback from previous rounds, and those reaching a consensus of over 80% were incorporated into the final document.
For each statement, section leads provided a grading of the quality of the supporting evidence, and the strength of the recommendation—these assessments were all ratified by the co-chairs. The quality of the supporting evidence was semi-quantified using the GRADE system (high, moderate, low, very low).21 The recommendation strength (strong, weak) was based on the evidence quality, but as in many cases this was low or very low, a range of other factors were considered including (as appropriate) the degree of consensus, the perceived risk/benefit balance, patient views, resource costs and expert opinion.
Information regarding evidence quality, eDelphi consensus and recommendation strength is summarised for each statement in the executive summary. The final document was read and approved by all members of the guideline committee, and formally assessed and approved by the Clinical Services and Standards Committee of the BSG.
Definitions
3. We recommend that anaemia is defined as a haemoglobin (Hb) concentration below the lower limit of normal for the relevant population and laboratory performing the test (evidence quality—medium, consensus—100%, statement strength—strong ).
4. We recommend that iron deficiency should be confirmed by iron studies prior to investigation. Serum ferritin is the single most useful marker of IDA, but other blood tests (eg, transferrin saturation) can be helpful if a false-normal ferritin is suspected ( evidence quality—medium, consensus—92%, statement strength—strong ).
5. We recommend that a good response to iron therapy (Hb rise ≥10 g/L within a 2-week timeframe) in anaemic patients is highly suggestive of absolute iron deficiency, even if the results of iron studies are equivocal ( evidence quality—medium, consensus—100%, statement strength—strong ).
Anaemia
The WHO defines anaemia as a haemoglobin (Hb) concentration below 130 g/L in men over 15 years of age, below 120 g/L in non-pregnant women over 15 years of age and below 110 g/L in pregnant women in the second and third trimester.2 22 The diagnostic criteria for anaemia in IDA vary between published studies.7–12 The normal range for Hb also varies between different populations in the UK. It is reasonable to use the lower limit of the normal range for the laboratory performing the test to define anaemia, but these should be aligned with the WHO defined lower limits.2
There is little consensus as to the level of anaemia that requires investigation. The National Institute for Health and Care Excellence (NICE) referral guidelines in the UK for suspected lower GI cancer suggest that IDA with an Hb concentration <110 g/L in men or <100 g/L in non-menstruating women warrants fast-track referral.23 These cut-off values will however miss some cases of colorectal cancer, especially in men.24 25 It is therefore advised that investigation should be considered at any level of anaemia in the presence of iron deficiency, though the case is stronger in those with more severe degrees of anaemia, as they are more likely to have serious underlying GI pathology.11 24 25
Iron deficiency
Automated cell counters provide measurements of the changes in red cells that accompany iron deficiency including reduced mean cell Hb (MCH)—hypochromia; and reduced mean cell volume (MCV)—microcytosis.26 MCH is probably a more reliable marker of iron deficiency as it is less dependent on storage and the counting machine used, and a reduction is seen in both absolute and functional iron deficiency (FID). MCH may also be more sensitive for iron deficiency than MCV.27 Both microcytosis and hypochromia lose sensitivity for iron deficiency in the presence of chronic disease, thalassaemia or vitamin B12/folate deficiency.28
The specificity of MCV and MCH for iron deficiency is limited, as microcytosis and hypochromia also occur in many haemoglobinopathies (such as thalassaemia, when the MCV is typically reduced out of proportion to the level of anaemia), in sideroblastic anaemia and in some cases of anaemia of chronic disease. To prevent unnecessary GI investigation, Hb electrophoresis is recommended in those with microcytosis and normal iron studies, particularly if there is an appropriate ethnic background.
The serum markers of iron deficiency include low ferritin, low transferrin saturation, low iron, raised total iron-binding capacity, raised red cell zinc protoporphyrin, increased serum transferrin receptor (sTfR), low reticulocyte Hb (Retic-Hb) and raised percentage hypochromic red cells. Serum ferritin (SF) is the most specific test for iron deficiency in the absence of inflammation. An SF level of <15 µg/L is indicative of absent iron stores, while SF levels of less than 30 µg/L are generally indicative of low body iron stores. The lower limit of normal for most laboratories, therefore, lies in the range 15–30 µg/L.29–31
As SF is an acute phase protein, however, apparently normal levels may occur with iron deficiency in the context of an inflammatory disease process.26 An SF cut-off of 45 µg/L has been suggested as providing the optimal trade-off between sensitivity and specificity for iron deficiency in practice.32 An SF value above 150 µg/L is unlikely to occur with absolute iron deficiency, even in the presence of inflammation.33
In summary, an SF <15 µg/L is highly specific for iron deficiency (specificity 0.99). A cut-off of 45 µg/L provides a respectable specificity of 0.92, and figures below this may warrant consideration of GI investigation, especially in the context of a chronic inflammatory process with anaemia.
The sTfR concentration is a good marker of iron deficiency in otherwise healthy subjects,34 but it can also be raised where there is increased erythropoietic drive such as with haemolytic anaemias, thalassaemias and Hb E29—and most UK hospitals do not provide this test. The [sTfR/log10 ferritin] ratio may provide superior discrimination to either test on its own, particularly in chronic disease.35
A therapeutic trial of oral iron replacement therapy (IRT) for 2–4 weeks may aid with the diagnosis of IDA, but is dependent on compliance. A ≥10 g/L rise in Hb over a 2-week period is highly sensitive for absolute iron deficiency.36 While further tests to confirm iron deficiency are occasionally necessary, estimation of iron concentration in bone marrow is invasive, often subjective and difficult to justify in most cases.
After excluding thalassaemia carriage, low Retic-Hb provides evidence of iron restriction, and should be considered in the laboratory work-up of anaemia particularly where there is chronic renal impairment.37 Retic-Hb is reported to be a more reliable marker of iron restriction than sTfR in healthy blood donors.38 An early indicator of response to iron therapy in IDA is provided by a rising Retic-Hb on day 4,39 similar to the observation of a falling percentage of hypochromic red cells in response to therapy.40 An algorithm for the diagnostic approach to IDA is suggested in figure 1.
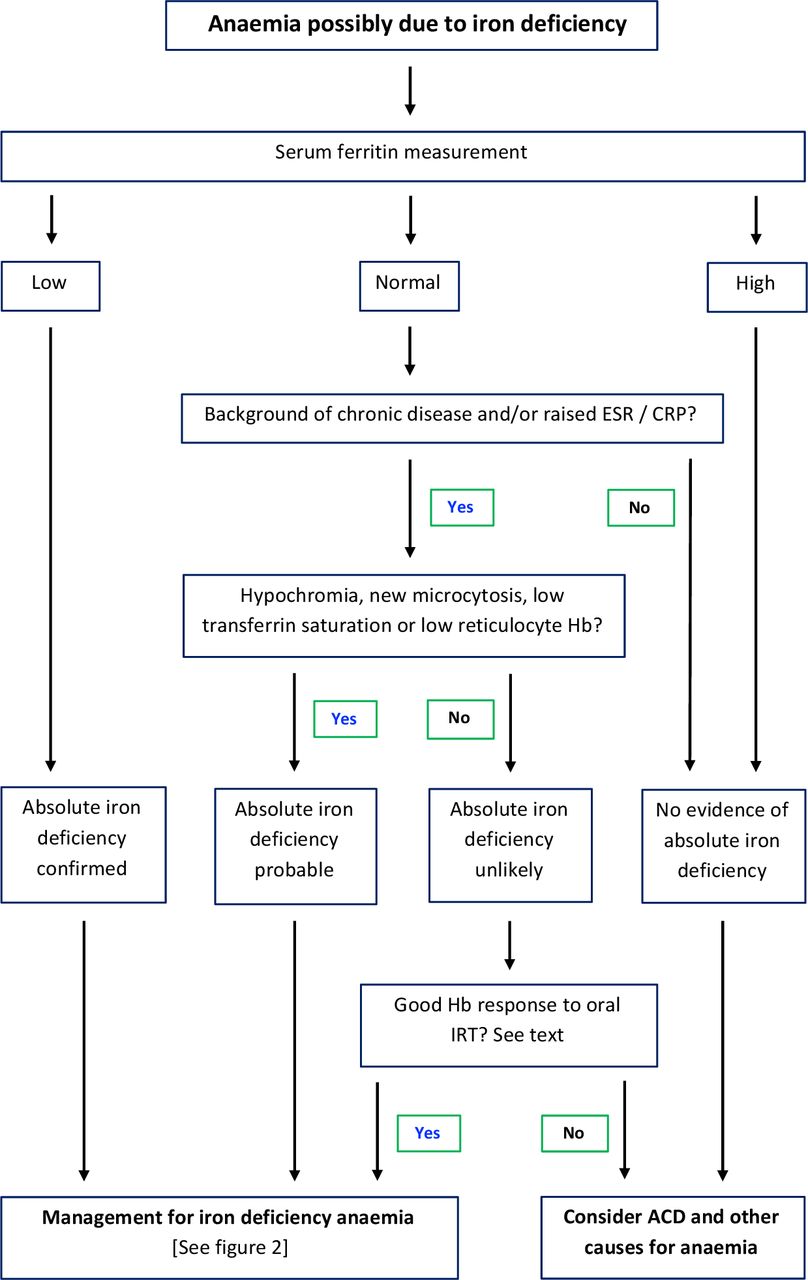
Algorithm for the diagnosis of iron deficiency anaemia. ACD, anaemia of chronic disease; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; Hb, haemoglobin; IRT, iron replacement therapy.
Functional iron deficiency
Absolute iron deficiency describes a situation where body iron stores are inadequate to meet demands, while in FID the supply of iron for erythropoiesis is inadequate despite apparently normal iron stores in cells of the monocyte-macrophage system. This restrictive effect is modulated by hepcidin, which also limits iron absorption through the gut mucosa.
A common clinical setting for FID is CKD, where parenteral iron therapy facilitates the response to administered erythropoietin to correct anaemia. FID is also one element of the anaemia of chronic disease, occurring in many chronic inflammatory conditions such as rheumatoid arthritis and IBD. A detailed discussion of the complex pathogenesis of the anaemia of chronic disease is beyond the scope of these guidelines.
An area of difficulty is establishing whether patients with presumed FID (with raised inflammatory markers and an SF in the normal range) have reduced iron stores indicative of absolute deficiency. When attributing anaemia to FID, it is important to consider whether there is sufficient evidence of a chronic illness. Evidence from studies in CKD suggests that in the absence of thalassaemia, the percentage of hypochromic red cells and Retic-Hb are superior to transferrin saturation in predicting the response to intravenous iron therapy.41 A transferrin saturation of <20% is indicative of iron restriction, particularly in thalassaemia carriers.41
Similar evidence that low Retic-Hb is an independent marker of iron restriction in the non-CKD setting,42–44 and for example provides a reliable marker of iron stores in patients with IBD.45 A very low hepcidin level is more commonly seen in absolute than FID, and may therefore indicate the probability of a response to oral IRT,46 but few UK laboratories offer this test. A good haematological response to a trial of oral iron suggests absolute iron deficiency rather than FID.
Given that chronic inflammatory conditions are common and that SF values may therefore be difficult to interpret, it is important to use additional clinical and laboratory information when considering whether further GI investigations are warranted. Clinical features (eg, bowel-related symptoms), inflammatory markers (eg C-reactive protein (CRP)), transferrin saturation, red cell hypochromia and response to oral IRT can all be helpful in this complex clinical setting.
Non-anaemic iron deficiency
The development of anaemia from iron deficiency goes through an initial phase where body iron stores are depleted resulting in hypoferritinaemia, but the Hb concentration is still within the normal range (non-anaemic iron deficiency (NAID)). For example, in a study of young women with menorrhagia, over half had reduced iron stores but only 25% were actually anaemic.47
The overall prevalence of significant underlying GI pathology, and in particular of GI malignancy, is low in NAID.25 In the absence of other pointers, GI investigation generally is not warranted in premenopausal women since the cause is likely to be menstrual blood loss and/or recent pregnancy (see the Special situations section). The threshold for investigation of NAID should however be low in men, postmenopausal women, and those with GI symptoms or a family history of GI pathology.
Initial clinical assessment
6. We recommend taking a detailed history, as it may provide important clues as to the cause(s) of IDA in the individual case ( evidence quality—low, consensus—100%, statement strength—strong ).
7. We recommend that initial investigation of confirmed IDA should include urinalysis or urine microscopy, screening for coeliac disease (CD) and in appropriate cases, endoscopic examination of the upper and lower GI tract ( evidence quality—moderate, consensus—85%, statement strength—strong ).
8. CD is found in 3%–5% of cases of IDA, and we recommend that it should be routinely screened for serologically, or on small bowel biopsy at the time of gastroscopy ( evidence quality—high, consensus—84%, statement strength—strong ).
9. Age, sex, Hb concentration and mean cell volume are all independent predictors of risk of GI cancer in IDA, and need to be considered as part of a holistic risk assessment. It follows that the cancer risk in iron deficiency without anaemia is low ( evidence quality—high, consensus—92%, statement strength—strong ).
10. There are insufficient grounds at present to recommend faecal immunochemical testing for risk stratification in patients with IDA. The evidence base is evolving rapidly, however, and on that basis, this guidance may therefore change. ( evidence quality—low, consensus—100%, statement strength—weak ).
11. We recommend that in men and postmenopausal women with newly diagnosed IDA, gastroscopy and colonoscopy should generally be the first-line GI investigations. In those not suitable for colonoscopy, CT colonography is a reasonable alternative ( evidence quality—moderate, consensus—100%, statement strength—strong ).
Service provision
IDA is a common clinical problem with fairly clear diagnostic criteria, a degree of case homogeneity, and straightforward algorithms for treatment and investigation.48 These features make the condition eminently suitable for streamlined management in dedicated nurse-led IDA clinics, as have been developed in a number of units around the UK.49–51 An algorithm for the management approach to IDA is suggested in figure 2.
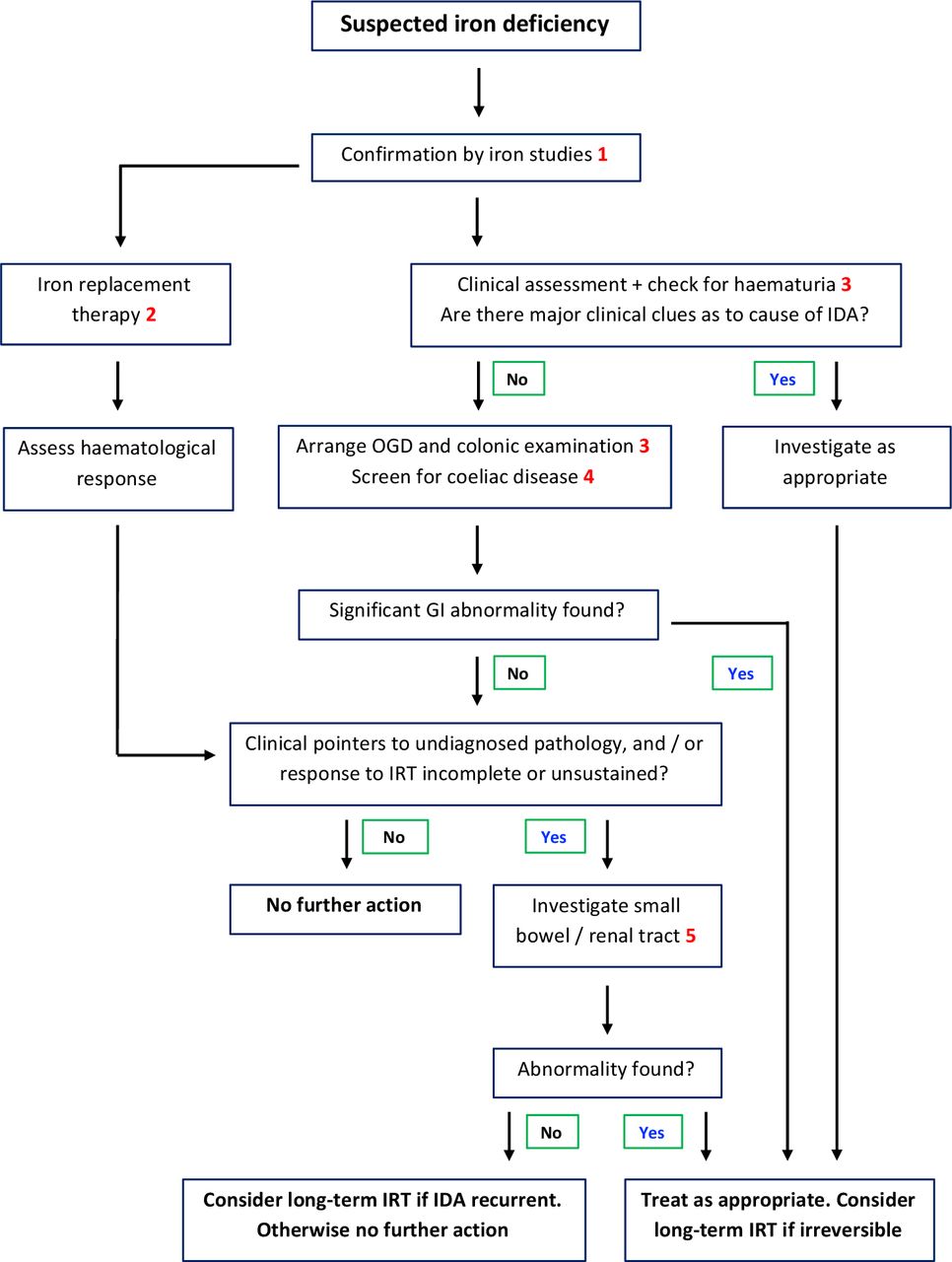
Algorithm for the management of IDA. Section reference key: 1—diagnosis, 2—treatment, 3—clinical assessment, 4—coeliac disease, 5—further evaluation. IDA, iron deficiency anaemia; IRT, iron replacement therapy; OGD, oesophago-gastroduodenoscopy.
History and examination
Clinical assessment of a subject with IDA may reveal manifestations of anaemia (eg, breathlessness, fatigue, heart failure) and on occasion more specifically of iron deficiency (such as angular stomatitis, glossitis, koilonychia, restless legs syndrome, pagophagia (a craving for ice), blue sclerae). A personal or family background of GI disease may provide a clue as to the cause of IDA. A family history of true iron-refractory IDA is rare, but if given may suggest a genetic disturbance of the pathway controlling iron absorption.52
Even if present, abdominal symptoms are not a reliable guide to the presence, nature or location of underlying GI pathology.16 Physical examination is generally unremarkable, but may on occasion provide the diagnosis, for example, in hereditary haemorrhagic telangiectasia.
There are many potential contributors to a negative iron balance, leading to IDA (see table 1). Particular risk factors that should be sought include chronic overt blood loss (eg, nosebleeds, menstruation), blood donation, inadequate dietary intake, long-term NSAID usage and previous resectional or bypass surgery of the GI tract. More recently it has been recognised that long-term proton pump inhibitor(PPI) therapy may contribute to the risk of iron deficiency,53 presumably as a result of impaired absorption secondary to hypochlorhydria, and that IDA is common in endurance athletes—the mechanism is uncertain, but high hepcidin levels may contribute.54 Iron deficiency is however often multifactorial, and so the presence of one or more of these risk factors should not necessarily be a deterrent to further GI investigation, particularly in older age groups.
Preliminary investigations
CD is a relatively common cause of IDA17 55 56 and should be routinely excluded in all age groups (see the later section). Renal tract pathology, in particular renal cell carcinoma,57 is a well-recognised though uncommon cause of IDA due to chronic blood loss, and so all subjects presenting with unexplained IDA should at least be checked for microscopic haematuria. Urine dipstick testing and mid-stream urine (MSU) analysis have limited sensitivity and specificity for renal tract pathology, but nevertheless, after exclusion of infection, a persisting positive result is an indication for urological investigation.
Imaging of the GI tract
How to investigate
Standard practice is to examine the upper and lower GI tracts at gastroscopy and colonoscopy respectively, and many units undertake both procedures at the same session.10 17 32 This approach is more efficient than separate procedures and, given the patient is already prepared, simplifies the decision to proceed to colonoscopy if there are abnormalities of uncertain relevance to IDA in the upper GI tract. Given that most series have revealed some cases with dual unrelated pathology, the recommendation is to defer colonoscopy only if an upper GI cancer is found. Overall, investigation of the GI tract in IDA reveals potentially significant pathology in about a third of cases16 17 58—there is a myriad of recognised GI causes, as outlined in table 1.
CT colonography is an acceptable alternative to colonoscopy,59 60 and may be preferable in certain clinical situations, such as in the presence of major comorbidities. The advantage of CT colonography is that it is less invasive, does not require sedation and provides limited imaging of the other viscera. The disadvantage is that it does not identify more subtle mucosal pathology such as vascular malformations, and there may be some circumstances where a colonoscopy is subsequently required to obtain histology, remove a polyp, or insert a tattoo prior to laparoscopic resection.
There is a limited place for contrast CT without bowel preparation in those with IDA and major comorbidities including frailty, accepting that this will only identify relatively gross pathology, and will miss some cancers. The value of investigating those where the outcome is unlikely to affect management does however need to be carefully considered (see the Special situations section). There is no longer a role for contrast fluoroscopy in the investigation of the upper and lower GI tract in IDA.
Atrophic gastritis is a recognised contributor to the development of IDA, probably because of the impairment of iron absorption that accompanies all causes of achlorhydria.5 In support of this, subgroup analysis of a small study has suggested that atrophic gastritis may be commoner in those without a definite alternative explanation for IDA than in those with.61 Helicobacter infection has also been weakly associated with the risk of developing IDA,62 though it is unclear whether this reflects the effect of related pathologies such as peptic ulceration or atrophic gastritis. The same meta-analysis suggested that Helicobacter eradication does not improve the Hb response to IRT.62 It, therefore, remains to be established whether the cost of routine gastric biopsies in IDA is justified, given that the results are unlikely to directly alter management.32
Who to investigate
The investigation of IDA potentially involves a considerable workload with a relatively low yield, and so there is a strong case for targeting valuable investigational resources. Cancer is by far the most serious pathology underlying IDA, but even following previous guidelines advising investigation of males and postmenopausal women, cancer is only found in 8%–10% of cases11 17 58—and the majority of investigations reveal no other significant abnormalities either.
It is also important to bear in mind that premenopausal women do on occasion develop cancer in the GI tract, and that cancer is not the only GI pathology underlying IDA. There is therefore sometimes justification for investigating younger women—particularly if the IDA is severe or recurrent, and disproportionate to perceived menstrual losses (see the Special situations section).
There is now evidence that individuals with IDA can be stratified for the risk of underlying GI cancer based on a set of simple and objective clinical variables—specifically age, sex, MCV and Hb concentration.11 25 The IDIOM App63 has been developed to provide a swift estimate of GI cancer risk in IDA, which may help inform the patient discussion as to the potential benefit of investigation. Further refinement of the risk stratification process with the incorporation of additional clinical variables may allow the identification of sizeable subgroups who can safely avoid invasive procedures altogether.25
Role of faecal immunochemical testing
The introduction of faecal immunochemical testing (FIT) for trace quantities of blood in the stool has provided a major step forward in risk stratification for those presenting with clinical features that are potentially due to colorectal cancer (CRC), and the value of it has been demonstrated in a series of large observational studies.64–69 FIT is currently recommended by NICE for determining whether IDA in the under-60 age group warrants fast-track referral23 –while this suggestion is logical, the evidence base is limited.
The place of FIT in risk stratification for the IDA population as a whole—either as a stand-alone or in conjunction with established tools—remains to be established. There are reasons for caution about a FIT-based triage system for IDA. First, CRC accounts for only a minority of the pathology found on the investigation of IDA, particularly in those under 60. Second, data from six recently published studies of real-world experience confirm that even at the low detection threshold of 10 µg/g, the sensitivity of FIT for CRC ranges from 83% to 91%.64–69 Furthermore, although numbers are small, there is the suspicion that IDA may be over-represented in the FIT negative CRC subgroup, accounting for 32 (40%) of the 81 pooled cases. The data are summarised in table 2. This conclusion is supported by a meta-analysis of the few IDA-specific studies in the published literature, which yielded a sensitivity of 83% of FIT for CRC, with concerns that this may be an over-estimate due to publication bias.70
Summary of recent real-world studies of the performance of quantitative FIT in the prediction of colorectal cancer (CRC) in adults with clinical pointers to this diagnosis, showing data for FIT-negative cancers with IDA (reference 68 assessed all-cause anaemia rather than confirmed IDA)
Currently therefore we are unable to advocate the use of FIT for risk stratification or colorectal cancer exclusion in IDA, though this view may change with the appearance of a stronger evidence base. While it seems logical to consider the result of FIT in the overall assessment of the risk serious organic disease, safety netting is still required to ensure that serious pathology is not missed. BSG guidance will be updated as further evidence for the role of FIT in IDA is evaluated, and a BSG Association of Coloproctology of Great Britain and Ireland (ACPGBI) guidelines group has recently been commissioned to assess this.
Coeliac disease and IDA
CD is found in 3%–5% of subjects investigated for unexplained IDA as demonstrated by studies from the UK, Europe, USA and Middle East.17 55 Duodenal biopsy histology remains the gold standard for exclusion or confirmation of the diagnosis. Coeliac serology—anti-tissue transglutaminase (tTG) or antiendomysial antibody—is however a useful screening test.32 71 72 A prospective study of 2000 referrals for gastroscopy (all indications including anaemia, mean age 56 years) with parallel serology and histology yielded both a sensitivity and a specificity of tTG IgA antibody for CD of 90.9%, with a negative predictive value of 99.6%.73
With emerging evidence on the reliability of serology with an anti-tTG IgA titre of greater than 10× the upper limit of normal,74 the BSG has issued interim guidance on a ‘no biopsy’ protocol in patients under the age of 50 years during the COVID-19 pandemic, provided they have no alarm symptoms. An updated guideline on the diagnosis of CD in adults is expected in 2022.
Retrospective studies suggest that antibody-negative CD accounts for about 2% of the total coeliac population,75 76 though this may be an under-estimate due to ascertainment bias (seronegative subjects are less likely to get a biopsy), and the true figure may be nearer 10%.56 73 As standard serological screening tests are IgA-based, apparently seronegative CD can result from IgA deficiency. This only accounts for a minority of antibody-negative cases however,56 71 and screening for it may not be cost-effective as the result only marginally changes the probability of CD.
As the relative prevalence of seronegative CD is highest in the elderly,56 75 77 the sensitivity of coeliac serology for CD falls with age. This has importance in the investigation of IDA, where the incidence is highest in the elderly, and the median age at presentation is over 70.17 As the sensitivity of serology for CD can be as low as 74% in coeliacs presenting with IDA,56 it may be that an age-related approach to investigation is most appropriate.
In a younger patient with IDA, where the sensitivity of serology for CD is high and the risk of other serious pathology low, a check on coeliac serology may be all that is required, with gastroscopy and biopsy only if the result is positive. Other factors of course may influence the need for further investigation—colonoscopy, for example, should be considered in those with a strong family history of colorectal cancer.
In an older subject with IDA, the sensitivity of serology for CD is rather lower, while the probability of other pathology and in particular GI malignancy, is much higher, and dual pathology is more common.17 So a more appropriate approach in this situation might be bidirectional endoscopy (BDE) with duodenal biopsy to exclude CD.
Presentation of CD in later life is well recognised,56 78–81 and indeed the seroprevalence of undiagnosed CD is similar to that in younger age-groups.82 CD in the elderly may however be more likely to present with manifestations of malabsorption, including IDA.78 79 81 There is conflicting evidence as to whether a diagnosis of CD over the age of 50 confers an increased cancer risk relative to the general population of the same age,83 84 but the possibility of a concurrent GI neoplasm should always be considered. Older patients with CD and IDA and any patient with alarm features should be considered for BDE, but no specific age or Hb cut-off can be recommended due to lack of published evidence.
Follow-up and recurrent IDA
12. Hb levels normalise with iron replacement therapy (IRT) in most cases of IDA, but IDA recurs in a minority of these on long-term follow-up ( evidence quality—low, consensus—92%, statement strength—strong ).
16. We recommend that long-term IRT may be an appropriate strategy when the cause of recurrent IDA is unknown or irreversible ( evidence quality—low, consensus—100%, statement strength—strong ).
23. After the restoration of Hb and iron stores with IRT, we recommend that the blood count should be monitored periodically (perhaps every 6 months initially) to detect recurrent IDA ( evidence quality—very low, consensus—85%, statement strength—strong ).
IDA should be treated with IRT as detailed in the Treatment section, and if the initial investigation reveals the cause, it should obviously be addressed as appropriate. However, the majority of individuals presenting with unexplained IDA will have negative BDE, no evidence of CD, no other symptoms, and a complete and sustained haematological response to IRT. In this situation, the outlook is generally favourable,4 32 51 85–88 and there is no need for further investigation other than a periodic blood count after completion of IRT to check for recurrent IDA. In an era of limited resources, we would suggest checks at perhaps 3, 6, 12 and 24 months.
Further investigation is however warranted if there is any evidence of active undiagnosed pathology. Pointers to this possibility include symptoms such as ongoing weight loss or chronic unexplained diarrhoea, persistently elevated inflammatory markers and the persistence or recurrence of IDA. Persistent IDA describes the situation where there is haematological evidence of ongoing iron deficiency despite adequate IRT, while in recurrent IDA the haematological abnormalities resulting from iron deficiency resolve with IRT, only to reappear at a later date.
Depending on the circumstances, further investigation may involve repeat BDE, particularly if the original procedures were felt to have provided inadequate views or to be outdated. Detailed imaging of the small bowel is an important element of further assessment (see the Small bowel section). Finally, formal imaging of the renal tract should be considered regardless of the result of testing for microscopic haematuria, in view of the recognised association of renal cell carcinoma with IDA.57
Depending on the definition employed, IDA proves to be recurrent in the medium term in 12%–25% of cases following previous negative BDE and a complete response to IRT.17 88 Recurrent IDA will respond in most cases respond to further IRT.
There are no established algorithms for the investigation of recurrent IDA, but our recommendation is to follow the principles outlined earlier. In particular, repeat BDE is advised if the previous investigations are outdated. There is no validated definition of this, but a threshold of 2 years has been suggested on the basis of limited evidence.17
The diagnostic yield of small bowel examination by capsule endoscopy (CE) is high in recurrent IDA unexplained by adequate imaging of the upper and lower GI tract (see the Small bowel section). The most common findings are vascular malformations (sometimes single but more commonly multiple) and Crohn’s disease, though tumours account for a small percentage of cases.17 89
The prevalence depends on definitions, but in a significant minority of cases of recurrent IDA, no convincing cause is found despite comprehensive investigation of the GI and renal tracts. Long-term IRT is an appropriate management strategy when the cause of recurrent IDA is unknown or where it is irreversible, for example, secondary to atrophic gastritis or previous GI surgery.
Further evaluation of the small bowel
13. In those with negative bidirectional endoscopy of acceptable quality and either an inadequate response to IRT or recurrent IDA, we recommend further investigation of the small bowel and renal tract to exclude other causes ( evidence quality—moderate, consensus—85%, statement strength—strong ).
14. We recommend capsule endoscopy as the preferred test for examining the small bowel in IDA because it is highly sensitive for mucosal lesions. CT/MR enterography may be considered in those not suitable, and these are complementary investigations in the assessment of inflammatory and neoplastic disease of the small bowel ( evidence quality—high, consensus—100%, statement strength—strong ).
15. After a negative capsule endoscopy of acceptable quality, we recommend that further GI investigation needs to be considered only if there is ongoing IDA after IRT ( evidence quality—high, consensus—100%, statement strength—strong ).
CE is now the first-line test for assessment of the small bowel in the setting of covert bleeding/IDA, as it has a higher diagnostic yield than radiology.90–92 A pooled diagnostic yield of 66.6% (95% CI 61% to 72%) has been reported in a systematic review of CE in IDA.93 Angioectasia, Crohn’s disease and NSAID enteropathy are common findings,17 89 94–96 and factors such as transfusion dependence, increasing age and comorbidity all positively influence the diagnostic yield.97 A longer small bowel transit time on CE is also associated with a higher yield,96 98 so the possibility of missed pathology should be considered when transit is unduly rapid.
The pathology found on CE is actually within reach of standard gastroscopy in up to 28% of cases.99 100 Such lesions include in particular Cameron’s ulcers, gastric antral vascular ectasia and vascular anomalies high on the lesser curve. Repeating gastroscopy prior to CE in all patients is not cost-effective,101 102 but should be considered on an individual case basis, particularly if views were previously poor or there has been a major time lapse since the last gastroscopy. Similarly, lesions may be missed in the right colon, particularly in the elderly and when preparation has been suboptimal.97 102
While the pick-up rate for small bowel pathology is significantly higher in the elderly, there is emerging evidence of the value of CE in younger age groups with IDA, though with differences in aetiology.89 103 A retrospective European cooperative study of 220 cases under the age of 50 revealed significant pathology in 32%, neoplastic in 5%.104 On multivariate analysis, a low MCV and weight loss were independent predictors of significant pathology.104
The rebleeding potential is low following a negative CE, and a conservative approach can in general be followed.105 CE does however have a miss rate, importantly for small bowel tumours.106 Indications warranting additional investigation after a negative CE may include a further Hb drop of >40 g/L, and a change in presentation from occult to overt bleeding.105 In the context of suspected small bowel bleeding including IDA, there is limited evidence to support repeating CE after an initial negative study in cases where there remains a strong suspicion of undiagnosed pathology, with a yield of up to 45%.107 108
Device-assisted enteroscopy (DAE), an endoscopic technique that allows deep intubation of the small bowel, provides the option for endoscopic biopsy and/or therapy, but this is an invasive procedure, and the need for it should be directed by the findings on CE. Predictably, the diagnostic yield of double-balloon enteroscopy is significantly higher if preceded by a positive CE than a negative one.109
Vascular lesions (angioectasia) are a common finding on CE, particularly in the elderly, and cohort studies have demonstrated that endoscopic ablation may reduce rebleeding rates and transfusion requirements.110 111 There are however no randomised controlled trials, and a systematic review has suggested that the rebleeding rate after ablation of small bowel angioectasia is not dissimilar to that of historical (untreated) controls.112 As angioectasia is a benign condition, conservative management with long-term IRT is therefore a reasonable alternative—particularly in the context of non-intrusive IDA and/or significant comorbidity.
The majority of small bowel lesions underlying IDA are subtle vascular or inflammatory abnormalities, undetectable by conventional radiology. CT enterography (CTE) does however have a role in delineating small bowel tumours seen on CE, and the combination of arterial venous and phases is helpful in characterising vascular small bowel tumours and detecting metastases. In addition of course, CTE may reveal evidence of other neoplasia underlying IDA, such as lymphoma or tumours of the renal tract.
Most series in the published literature on studies comparing CTE and small bowel endoscopy have combined cases of IDA and overt small bowel bleeding. Meta-analyses have concluded that CTE and CE/DAE are best considered complementary investigations.113 114 CTE may have a higher yield for tumours, although this is a tentative conclusion due to small numbers.115
Treatment of IDA
17. We recommend that IRT should not be deferred while awaiting investigations for IDA unless colonoscopy is imminent ( evidence quality—high, consensus—100%, statement strength—strong ).
18.We recommend that the initial treatment of IDA should be with one tablet per day of ferrous sulphate, fumarate or gluconate. If not tolerated, a reduced dose of one tablet every other day, alternative oral preparations or parenteral iron should be considered ( evidence quality—medium, consensus—92%, statement strength—strong ).
19. Limited transfusion of packed red cells may on occasion be required to treat symptomatic IDA, in which case IRT is still necessary post-transfusion ( evidence quality—high, consensus—100%, statement strength—strong ).
20. We recommend that patients should be monitored in the first 4 weeks for an Hb response to oral iron, and treatment should be continued for a period of around 3 months after normalisation of the Hb level, to ensure adequate repletion of the marrow iron stores ( evidence quality—medium, consensus—92%, statement strength—strong ).
21. We recommend that parenteral iron should be considered when oral iron is contraindicated, ineffective or not tolerated. This consideration should be at any early stage if oral IRT is judged unlikely to be effective (see text), and/or the correction of IDA is particularly urgent ( evidence quality—high, consensus—92%, statement strength—strong ).
22. There is insufficient evidence to support invasive investigation in non-anaemic iron deficiency unless there are additional indications (see text), but periodic blood count monitoring is suggested (evidence quality-low, consensus-92%, statement strength-weak).
23. After the restoration of Hb and iron stores with IRT, we recommend that the blood count should be monitored periodically (perhaps every 6 months initially) to detect recurrent IDA ( evidence quality—very low, consensus—85%, statement strength—strong ).
The treatment of iron deficiency aims to (i) restore normal circulating Hb levels, (ii) replenish body iron stores, (iii) improve quality of life and (iv) improve physiological function. Successful IRT should achieve all of these outcomes.36 116–118 An algorithm providing an overview of the treatment of IDA is shown in figure 3, and the elements of this are discussed in more detail below.

{kind=link}
{kind=link}
{kind=link}
Overview of treatment algorithm for IDA. IDA, iron deficiency anaemia; IRT, iron replacement therapy.
Oral IRT
It is usual to start treatment for IDA as soon as the diagnosis has been confirmed by laboratory investigation, so that the treatment and investigation of IDA proceed in parallel. There is usually a beneficial rise in Hb within 2 weeks of commencing oral IRT.36 Oral iron preparations often stain the stools and may cause constipation, so it is usual practice to pause these prior to bowel preparation for colonoscopy. Therefore, if a patient is to be investigated for IDA within 2 weeks, it would be appropriate to delay treatment until after the colonoscopy has been completed. There is no need to withhold oral iron before gastroscopy or CT colonography.
Traditionally oral iron salts were taken as split dose, two or three times a day. More recent data suggest that lower doses and more infrequent administration may be just as effective, while probably associated with lower rates of adverse effects. In addition, it may be inconvenient for some people to find three periods during the day to take iron on an empty stomach.
Various oral iron preparations are available in the UK (table 3). Traditional oral iron salts (ferrous sulfate, ferrous gluconate and ferrous fumarate) are inexpensive, effective, safe and readily available—and they remain the standard therapies for IDA. Their use is supported by considerable clinical experience and observational data. In a pooled analysis of trial data, 72.8% of patients with IDA demonstrated a satisfactory response to an oral iron formulation, defined as an Hb rise of >10 g/L within 2 weeks, though rates of normalisation of Hb were lower with continued bleeding or clinically evident GI disease.36
A comparison of oral iron preparations available in the UK (February 2021)
A Cochrane analysis in 2014 highlighted that the reviewed trials were of poor quality, but concluded that in comparison to placebo oral IRT significantly improves Hb levels in IDA, and probably reduces blood transfusion requirements.119 When given in standard doses there do not appear to be important differences in efficacy or adverse events,119 although side effects may be lower with less than daily dosing.120 Modified release preparations (table 3) release iron in the more distal small bowel beyond the areas of most active assimilation—they do not enhance iron absorption121 122 or reduce side effects,123 and their use is not recommended.
The absorption of oral iron salts is significantly impaired if taken with food. Taking iron with meals can reduce bioavailability by up to 75%.124 This necessitates iron being taken either in the fasting state first thing in the morning or in periods between meals during the day. It is not clear how soon after oral iron food can be taken, but the inhibitory effect of tea on iron absorption dissipates within 60 min.125 Despite previous suggestions of benefit,121 coadministration of vitamin C with oral IRT is not recommended—a recent large randomised controlled trial has confirmed that it neither enhances the haematological response or rate of iron loading, nor diminishes side effects.126
Iron absorption from oral preparations is determined by a complex interplay involving total body iron stores, erythropoietic activity of the bone marrow, recent exposure of the small intestine to iron and systemic inflammation.35 127–131 Hepcidin is the most important inhibitor of iron absorption. Hepcidin levels follow a diurnal pattern and increase after oral iron intake, impairing fractional absorption of subsequent doses.131 132
Short-term studies of iron-depleted but otherwise healthy women have shown that oral doses of 60 mg elemental iron stimulate increased hepcidin levels for the next 24 hours, thus reducing subsequent iron absorption by 35%–45%.131 As a consequence, the overall absorption of iron from 60 mg of elemental iron taken once a day was similar to that from 60 mg two times a day. Therapy with low dose oral iron has been reported to be successful and safe in elderly patients with IDA—a daily dose of 15 mg of elemental iron was as effective as 50 mg or 150 mg in terms of the Hb response, with a lower incidence of adverse effects.133
There are limited data on outcomes at lower dosage frequencies. Alternate day dosing leads to a significantly increased fractional iron and total iron absorption in iron-depleted healthy women.132 134 Fractional iron absorption was significantly higher with alternate day administration of 100 mg or 200 mg elemental iron compared with daily dosing.134 Importantly, the overall iron absorption from 200 mg on alternate days was almost twice that from the equivalent dosage of 100 mg on consecutive days.134 In a randomised trial comparing treatment regimes in subjects with IDA, 60 mg elemental iron two times a day produced a faster rate of Hb rise than 120 mg on alternate days (ie, half the equivalent daily dose), though similar Hb increments were seen with alternate day dosing after the same total dose had been given, with a significantly lower prevalence of nausea.120
Intermittent oral iron (defined as less frequently than daily) has been reported to be at least as effective as daily dosing in raising Hb levels in young women and during pregnancy, although less effective in boosting iron stores in the short-term.135 136 Intermittent oral iron is associated with a lower incidence of GI adverse events in pregnant women (relative risk 0.56; 95% CI 0.37 to 0.84).137
The optimal drug, dosage and timing of oral IRT for adults with IDA are not clearly defined, and the effect of alternate day therapy on compliance and ultimate haematological response are unclear. Based on the available literature, a once daily dose of 50–100 mg of elemental iron (eg, one ferrous sulfate 200 mg tablet a day) taken in the fasting state may be the best compromise option for initial treatment. Whatever agent and regimen are chosen, it is essential to monitor the initial haematological response, and modify as appropriate with apparent therapeutic failure.
The best option for patients with significant intolerance to oral IRT (usually GI disturbance) is also unclear. Depending on the individual, oral ferric maltol, alternate day oral iron and parenteral iron are all options. The standard practice of switching to a different traditional iron salt is not supported by evidence.
Ferric maltol is a relatively new preparation, which is licenced for the treatment of IDA of any cause.138 139 In patients with inactive IBD, previous intolerance to or failure of traditional iron salts and moderate IDA (Hb >95 g/L), 12 weeks of treatment with ferric maltol normalised the Hb in 63%–66% of cases.138 140 GI side effects and overall rates of treatment cessation were comparable to placebo.138 Due to a relatively low iron content, the rate of iron loading is comparatively slow with ferric maltol, but iron loading and tolerance were maintained during a year of active treatment, with normalisation of Hb in 89% of cases.139 Although more expensive than traditional iron salts, ferric maltol is considerably less expensive than parenteral irons.
Blood transfusion is rarely required to treat IDA, first because most patients with slowly developing anaemia adapt to the resulting physiological stress. Second, as parenteral iron reliably produces a clinically meaningful Hb response with a week, it should always be considered as an alternative. Transfusion should therefore be reserved for those with severe symptomatic and/or circulatory compromise. If used, packed red cells should be transfused in accordance with established good practice guidelines,141 and a target Hb of 70–90 g/L (80–100 g/L in those with unstable coronary artery disease) would be reasonable. Since a unit of packed red cells contains about 200 mg of elemental iron, it will not replenish the iron store deficit in severe IDA, and so restrictive transfusion should be followed by adequate iron replacement.
There should be a prompt and measurable haematological response to the initiation of IRT, and early monitoring should detect those patients not responding to or intolerant to oral iron. Failure to respond to oral iron has many causes including non-compliance, malabsorption, systemic disease, bone marrow pathology, haemolysis, continued bleeding and concurrent deficiency of vitamin B12 or folic acid.
The absence of an Hb rise of at least 10 g/L after 2 weeks of daily oral IRT is strongly predictive of subsequent failure to achieve a sustained haematological response (sensitivity 90.1%, specificity 79.3% for adequate subsequent response).142 In this situation, parenteral iron is more effective than continuing traditional oral therapy.142
Logistically it may be difficult to arrange monitoring 2 weeks after starting oral IRT in all cases. Indeed because of the lower doses of iron used in alternate day regimens, a 28-day review may be more appropriate.132 At this point, a rise in Hb of 20 g/L or into the normal range would be accepted as an adequate response.36 Whichever monitoring regimen is used, intolerance and/or ineffectiveness should be managed promptly and appropriately.
For patients with intolerance or failure of Hb response at the 2–4 weeks point, alternate day traditional iron salts (if not already used) or ferric maltol may be alternatives to parenteral iron on those with mild-moderate anaemia (Hb >95 g/L). The tolerability and response should be assessed, and failure of the Hb to rise by 10 g/L at 4 weeks for alternate day iron, or 6 weeks for ferric maltol, indicates the need for parenteral IRT.132 140
Regular Hb monitoring is recommended to ensure an ultimately satisfactory response. The optimal interval is not clear, but every 4 weeks until the Hb is in the normal range seems reasonable. After normalisation of the Hb, oral iron needs to be continued to replenish the iron stores. Traditionally it has been recommended that oral iron is continued for 2–3 months to do this. However, the duration required and indeed the appropriate measure of true iron repletion are both unclear. In healthy, almost iron-replete subjects, 2 months of continued iron was considered sufficient.143 However, in patients with chronic disease, continuing blood loss, impaired absorption or GI inflammatory disease (where iron is lost from the GI mucosa), it is likely that a longer period would be required.
Parenteral IRT
Parenteral IRT replenishes body iron stores more quickly than oral IRT. However, for the majority of patients with IDA, this is not translated into a clinical benefit in terms of rise in Hb.144–147 The Hb response to parenteral and oral iron is typically similar,148 or marginally faster with parenteral iron—for example, 0.7 g/L higher after 23 days treatment in postoperative cases.149 A course of oral 200 mg ferrous sulfate once a day was as effective as a single ferric carboxymaltose infusion in restoring Hb after a GI haemorrhage.147 Therefore, the oral route is generally preferred on the grounds of cost and convenience with comparable efficacy.
The intravenous route for IRT may however be preferable from the outset in those with ongoing significant bleeding, malabsorption due to GI disease, the combination of iron deficiency and anaemia of inflammation, or issues with administration (eg, severe dysphagia) or compliance.149 150 Parenteral iron may also be indicated in those failing to respond to oral IRT due to intolerance, pharmacodynamic failure or continued bleeding. Intravenous IRT has been shown to be superior to continuing oral therapy in cases with IDA that failed to show a significant Hb rise with oral IRT (defined as an increase of 10 g/L or more after 2 weeks),36 or had ongoing menorrhagia.117
A variety of parenteral iron preparations are available in the UK (table 4), and these all have the advantage of providing a much greater iron load per dose than oral iron. They all are more expensive than traditional oral iron preparations, and there are additional associated costs relating to the facilities, staffing and equipment required for administering infusions. Some preparations (ferric carboxymaltose), iron derisomaltose (previously iron isomaltoside 1000) and (low molecular weight) iron-dextran can effectively replenish total body iron stores in one or two infusions. Iron sucrose requires multiple infusions because the maximum dose per administration is 200 mg. Iron-dextran is rarely used, as the much longer time required for infusion (4–6 hours) means this is much less convenient than the other total dose preparations, which can be given over 15–40 min.
A comparison of intravenous iron preparations available in the UK (February 2021)
The dose of parenteral iron may be calculated using the original Ganzoni formula.151 Modifications using a lower target Hb level (130 g/L) have also been used.145 Overall the different intravenous iron formulations appear equivalent in terms of the ultimate haematological response and safety,152 but the total dose preparations provide more rapid replenishment of body iron stores,116 146 153 154 usually in just one or two infusions. Monitoring for a satisfactory Hb response after 2–4 weeks should be undertaken, and then as outlined below.
Treatment of NAID
The efficacy of IRT for NAID (also termed isolated hypoferritinaemia) is unclear. There are limited studies in adults, with a variety of inclusion criteria and outcomes. A meta-analysis of these concluded that NAID was not significantly associated with physiological impairment assessed objectively by VO2 max or respiratory exchange ratio max (RERmax), and that IRT did not significantly improve either these parameters or maximal heart rate.155 There is however evidence that IRT may provide subjective improvement of fatigue, mental quality of life and subjective cognitive function in premenopausal women.156–160 Therefore, given the safety of the available iron preparations, it would be reasonable to offer treatment for NAID if symptomatic.
Monitoring after IRT
The optimal follow-up protocol after IRT remains to be established, but given the possibility of recurrent IDA indicating underlying disease, and the prevalence of persistent anaemia after IRT seen in some real-world studies,161 periodic monitoring is advised. Once the Hb has reached the normal range, a check blood count 3-monthly for 12 months and then 6-monthly for 2–3 years would be reasonable. Although SF is a reliable measure of total body iron stores, there are insufficient data to recommend routine ferritin monitoring.
Safety of IRT
GI adverse effects (such as nausea, diarrhoea, constipation) are much commoner with oral preparations, and there is no convincing evidence for the superiority of any of the readily available traditional iron salts.162 163 GI side effects are significantly commoner with oral ferrous sulfate than placebo (OR 2.32 (95% CI 1.74 to 3.08)) or parenteral iron (OR 3.05 (95% CI 2.07 to 4.48)), and there is no dose–effect relationship over the range 50–400 mg of elemental iron per day.123 Despite the high prevalence of mild side-effects, the rates of discontinuation in clinical trials due to adverse events are relatively low (0%–24%), though higher than rates of discontinuation of parenteral iron (0%–18%).126 144 145 149 164 165 Discontinuation of oral IRT seems to be commoner in observational and population studies, with reported rates of up to 40%.166 167
Infusion-related reactions are uncommon with modern intravenous iron preparations, but hypersensitivity-type and infusion reactions (approximate incidence—0.5%) are commoner than with oral iron or placebo.152 Serious adverse reaction rates are low, however, and similar for oral and parenteral iron preparations.168
Caution is advised regarding the use of parenteral iron in the context of acute and chronic infection, although studies have consistently shown no significant increase in clinically important infective episodes associated with the use of parenteral IRT.152 168 169 Infection should not be regarded as a contraindication to parenteral IRT if the risk/benefit assessment favours treatment of the anaemia, though it should be withheld in those with ongoing bacteraemia.
Hypophosphataemia has been reported with all parenteral iron preparations. This seems to relate to the molecules complexed to the iron, rather than the iron itself. Rates of hypophosphataemia are higher with ferric carboxymaltose (58%) than with iron derisomaltose (4%) or iron sucrose (1%), but the clinical importance of this has not been established. Most of the episodes are biochemically moderate (serum phosphate in the range 0.32–0.64 mmol/L) and asymptomatic, and resolve without the need for intervention.170 171 However, because of the rare association with hypophosphataemic osteomalacia, the Medicines and Healthcare products Regulatory Agency issued a recommendation in 2020 advising that serum phosphate levels should be monitored in those with risk factors for hypophosphataemia, and in those receiving long-term or multiple high-dose infusions of ferric carboxymaltose.172
Special situations
Young women
24. IDA is common in young women, and major contributory factors include menstrual losses, pregnancy and poor dietary intake ( evidence quality—high, consensus—100%, statement strength—strong ).
25. Underlying GI pathology is uncommon in young women with IDA, and so after screening for CD, we recommend that further investigation is warranted only if there are additional clinical features of concern—as detailed in the text ( evidence quality—moderate, consensus—92%, statement strength—strong ).
26. If GI investigation in a pregnant woman is deemed necessary prior to delivery, gastroscopy and (after the first trimester) MR enterography are considered safe in pregnancy ( evidence quality—low, consensus—91%, statement strength—strong ).
The prevalence of IDA in otherwise healthy premenopausal women is 5%–12%.173 174 It usually reflects some combination of dietary insufficiency, menstrual losses, and increased demand for iron in pregnancy and breastfeeding.175
Multiple studies have analysed the yield of GI investigation in young women with IDA.176–183 As CD is found in up to 4% of cases, all premenopausal women with IDA should be considered for serological screening. Malignant tumours can occur in otherwise asymptomatic premenopausal women, but they are extremely uncommon—two studies suggesting a higher prevalence182 183 have been criticised on the grounds of selection bias.
In general, therefore IDA in young women is not an indication for endoscopic investigation. There are however various situations where direct endoscopic investigation of premenopausal women with IDA may be appropriate. These include11 25:
Age over 50—as age is a strong predictor of the risk of malignancy in IDA.
Non-menstruating women—for example, following hysterectomy.
Associated red flag symptoms, as outlined in NICE referral guidelines.23 24 184
Indications of a major genetic risk of GI pathology—for example, colorectal cancer affecting two first-degree relatives, or one first-degree relative affected before the age of 50 years.
Recurrent or persistent IDA which appears disproportionate to other potential causes of iron deficiency such as menstrual losses—accepting that this is usually a rather subjective judgement.
Mild IDA is common in pregnancy.22 175 IRT should be encouraged, but there is no need for endoscopic investigation unless there are pointers to the presence of underlying GI pathology in the history or on coeliac serology. If further investigation prior to delivery is felt to be warranted, gastroscopy, duodenal biopsy and MR enterography are considered safe for mother and fetus in pregnancy, though the National Radiological Protection Board considers it prudent to avoid MRIs in the first trimester. There are insufficient data on the safety of colonoscopy in pregnancy, and because of the potential to cause serious adverse events, it should be only be considered for the most pressing of indications.185
Young men
27. Confirmed IDA is uncommon in young men, but when found we recommend that it warrants the same investigational algorithm as for older people ( evidence quality—moderate, consensus—100%, statement strength—strong ).
IDA is relatively uncommon in young men, but the yield of pathology on examination of the GI tract is considerably higher than in women of the same age.25 186 IDA in young men therefore generally warrants the same investigational algorithm as described for older people, unless a convincing explanation for it is evident.
The elderly
28. Iron deficiency is common in the elderly, and is often multifactorial in aetiology ( evidence quality—high, consensus—100%, statement strength—strong ).
29. We recommend that the risks and benefits of invasive endoscopic and alternative investigation(s) are carefully considered in those with major comorbidities and/or limited performance status ( evidence quality—medium, consensus—92%, statement strength—strong ).
Anaemia is common in older people, affecting more than 20% of those over the age of 85 years, and more than 50% of residential/nursing home residents. The aetiologies responsible for anaemia in this age group are complex, and often multiple. Iron deficiency is however a contributory factor in about half of cases, sometimes associated with deficiencies of vitamin B12 and/or folate. Anaemia in older patients has been shown to contribute to worsening of physical performance, cognitive function and frailty.187–190
Iron deficiency in the elderly has many potential contributory causes including poor diet, reduced iron absorption, occult blood loss, medication (eg, aspirin) and chronic disease (eg, CKD, CHF). Blood loss from mucosal lesions may be compounded by concurrent antiplatelet/anticoagulant therapy. Older patients are more likely than younger ones to have more than one contributing cause. The diagnosis can be confirmed by measurement of ferritin and transferrin saturation, though the former may be difficult to interpret in the presence of coexisting inflammatory conditions.
Evaluation of the upper and lower GI tract should be considered if IDA has been confirmed, though CT colonography may be a more attractive alternative to colonoscopy for some older individuals. The prevalence of malignancy and of dual unrelated pathology in this age group strengthens the case for imaging both the upper and lower GI tract.17 However, the potential risks and benefits of invasive investigation should be carefully weighed up in older adults, particularly those who are frail, have significant comorbidities or reduced life expectancy. Furthermore, these considerations should be discussed with each patient and his/her family, taking their views into account.
As in other age groups, the cause of IDA cannot always be established despite thorough investigation. Oral iron administration remains the standard first-line treatment in most patients, but parenteral iron is a convenient and relatively safe alternative if oral iron is not tolerated.
Specific comorbidities
30. Functional iron deficiency (FID) is a common contributory factor to the anaemia associated with advanced chronic kidney disease (CKD) ( evidence quality—high, consensus—92%, statement strength—strong ).
31. Iron deficiency is common in chronic heart failure (CHF), and is often multifactorial ( evidence quality—high, consensus—92%, statement strength—strong ).
32. Parenteral IRT may improve symptoms and quality of life in CHF with FID ( evidence quality—moderate, consensus—100%, statement strength—strong ).
33. In the management of iron deficiency associated with CKD or CHF, reference to the appropriate specialist published guidelines is recommended ( evidence quality—moderate, consensus—92%, statement strength—strong ).
34. IDA is a common manifestation of IBD, particularly when the disease is active ( evidence quality—high, consensus—100%, statement strength—strong ).
35. Intolerance and malabsorption of oral IRT can be particular problems in the treatment of IBD-associated IDA, and parenteral IRT may be required ( evidence quality—medium, consensus—100%, statement strength—strong ).
Several chronic disorders such as CKD, CHF and IBD are associated with iron deficiency. While the cause of iron deficiency in these conditions is often multifactorial, altered production of hepcidin and ferroportin is thought to be a major contributory factor. Nevertheless, the presence of iron deficiency should be actively sought because IRT may improve patient outcomes.191 The assessment and management of iron deficiency in these conditions do have certain nuances, and consultation with detailed published guidelines is therefore recommended. Similar clinical considerations apply to other inflammatory disorders such as rheumatoid arthritis.
Chronic kidney disease
Anaemia is a frequent complication of CKD. CKD is a potential cause for anaemia in anyone with a glomerular filtration rate (GFR) of less than 60 mL/min/1.73m2. As the prevalence of anaemia increases with deteriorating renal function, CKD is especially likely to be the cause of anaemia when the GFR is less than 30 mL/min/1.73m2. The investigation and management of anaemia in CKD is a complex area, and readers are advised to consult specific guidelines relevant to UK practice published by NICE and the Renal association for more detailed recommendations.41 192 193
The causes are anaemia in CKD are multifactorial. Iron deficiency is a major element, but multiple other mechanisms (eg, haemolysis, plasma cell dyscrasias) may also contribute towards the development of anaemia, hence the requirement for detailed haematological investigation. The causes of iron deficiency in CKD are also multifactorial. Renal failure itself contributes, but this may also be compounded by reduced iron intake, reduced iron absorption and blood loss via either the GI tract or other routes such as dialysis and phlebotomy.194
Assessment of iron deficiency in CKD can be difficult. Measurement of ferritin and transferrin saturation may be helpful, but the interpretation of results is not the same as in patients who do not have CKD. Specifically, absolute iron deficiency in CKD has been defined as transferrin saturation ≤20%, with SF ≤100 µg/L (in predialysis and peritoneal dialysis patients) or ≤200 µg/L (in haemodialysis patients).194
Patients with CKD may of course also have GI pathology underlying their confirmed iron deficiency. The decision about the need for endoscopic evaluation of the upper and lower GI tract in CKD can be difficult, and should ideally be made in conjunction with a nephrologist. However, the majority of CKD patients with confirmed IDA warrant GI investigation as long as they are fit enough to undergo these procedures.
The management of iron deficiency in the context of CKD is beyond the scope of these guidelines and is discussed in detail elsewhere.41 192 193 Treatment is usually initiated and monitored by the nephrology team. In brief, oral iron replacement may be tried in patients who are predialysis. However, intravenous IRT is required if this is not tolerated or ineffective, or if dialysis has been commenced. Other treatments for anaemia such as erythropoietin may also be needed, but these should be managed by the nephrology team.
Chronic heart failure
Evidence of some degree of iron deficiency, as defined by an SF <100 µg/L and/or a transferrin saturation of <20%, is found in 40%–70% of cases with CHF.195–198 The causes are again multifactorial with malabsorption, malnutrition and GI blood loss (potentially exacerbated by anticoagulants or antiplatelet agents) all potentially contributing. In addition, the chronic inflammatory state present in many patients with CHF can lead to increased hepcidin release by the liver, resulting in reduced iron absorption/mobilisation.
Patients with CHF should be screened for iron deficiency by measurement of ferritin and transferrin saturation.195–198 Endoscopic evaluation of the upper and lower GI tract should be considered if they have evidence of absolute iron deficiency (see the Definitions section) to exclude treatable GI causes. Decisions about the need for and safety of endoscopic evaluation should ideally be made in conjunction with the cardiology team.
The majority however have FID rather than absolute iron deficiency. Nevertheless, both forms of ID are associated with reduced functional capacity, impaired quality of life and poorer prognosis in CHF.191–194 Patients who meet the above criteria for iron deficiency in this condition should therefore be considered for intravenous IRT,195 as this has been shown to have prognostic benefit in meta-analyses.196 197 No prognostic benefit has been demonstrated for oral iron, and this is best avoided as in CHF it may be poorly absorbed due to gut oedema, and is frequently associated with side-effects.195 Specific guidelines should be consulted for detailed recommendations about the investigation and management of iron deficiency in this patient group.198
Inflammatory bowel disease
A third of patients with active IBD are estimated to have iron deficiency, though other mechanisms including vitamin B12 and folate deficiency, marrow suppression due to the anaemia of chronic disease, and overt blood loss may all contribute to the anaemic state.199 SF levels of up to 100 µg/L in the presence of inflammation may still reflect iron deficiency,200 and so an estimate of transferrin saturation may be helpful. The absorption of oral iron may be impaired by the systemic inflammatory process,148 201 as well as by small bowel involvement and/or previous surgery, and this may favour intravenous IRT in some cases.164
Current European guidelines suggest that oral IRT in patients with IBD should contain no more than 100 mg elemental iron a day.200 Intravenous iron is indicated for those who are intolerant of oral iron and have moderate to severe IDA (Hb <100 g/L).148 164 200 Optimising nutritional and pharmacological management to bring active IBD into remission would be expected to help improve IDA metrics and response to iron therapy.200 201
It has been suggested that patients with IBD and IDA should be monitored for recurrent iron deficiency every 3 months for at least a year after correction, and periodically thereafter.200 Recurrent IDA may indicate persistent intestinal inflammatory activity even in the face of clinical remission and normal inflammatory biomarkers.200
GI surgery
36. IDA is common following resection or bypass surgery involving the stomach and/or small bowel, including bariatric surgery ( evidence quality—high, consensus—92%, statement strength—strong ).
37. In new presentations of IDA, we recommend that a history of GI or bariatric surgery should not preclude a search for other causes of IDA ( evidence quality—low, consensus—85%, statement strength—strong ).
Resection or bypass surgery involving the stomach and/or small bowel generally predisposes to IDA.202 This includes the expanding population with a history of bariatric surgery, including sleeve gastrectomy. Reduced nutritional intake and malabsorption are probably the major underlying mechanisms,203 and therefore IDA in this situation may occur in the context of other nutritional deficiencies—in particular of vitamin B12.
The prevalence of IDA depends on the specific diagnostic criteria employed, but it is found in approximately a quarter of subjects 2 years following Roux-en-Y gastric bypass, and is markedly commoner in women,204–206 and in those with preoperative evidence of low iron stores.202 The figure for sleeve gastrectomy is probably lower.202 207
Predictably, the yield of other causative lesions on BDE is lower in individuals with IDA and a history of GI surgery than in those without.208 Nevertheless, it is unsafe to automatically attribute IDA to previous surgery without excluding other possibilities, particularly in those at risk of underlying GI malignancy—bearing in mind that partial gastrectomy may predispose to the later development of cancer in the gastric remnant.209
Without supplementation, the percentage prevalence of IDA tends to increase over the first 10 postoperative years.203–206 Long-term oral IRT is often effective, though because of underlying malabsorption this is not always the case, and intravenous therapy may be required.210 211
Service considerations
38. We recommend that all service providers should have clear points of referral and management pathways for patients with IDA ( evidence quality—low, consensus—100%, statement strength—strong ).
39. To ensure efficient use of resources, we recommend that IDA pathways should be delivered by a designated team led by a senior clinician ( evidence quality—low, consensus—100%, statement strength—strong ).
40. We recommend that service providers should aim to have an ambulatory care base for the administration of parenteral iron ( evidence quality—low, consensus—100%, statement strength—strong ).
Organisation
IDA has a considerable impact on referrals for urgent investigation for suspected cancer and non-elective services. This is due to the prevalence of IDA in the population, difficulty in distinguishing IDA from other causes of anaemia, and in some areas the absence of a dedicated referral pathway for the management of anaemia. In many hospitals IDA is no longer the prime interest of haematology, so becoming an ‘orphan’ condition without clinical leadership. This can lead to duplication of services, prolonged referral pathways and inappropriate investigation.212
Anaemia is common in elderly patients and those with multiple comorbidities. The anaemia of chronic disease can mimic IDA, and in a study of fast-track referrals with suspected IDA, the diagnosis was confirmed in only 11% of cases.213 Therefore it is important to establish at an early stage that anaemia is due to iron deficiency. Fortunately, artificial intelligence or smart testing algorithms embedded within red cell laboratory analysers (reflex testing) are now available and can include specific recommendations for further management to primary care,214 including referral to a dedicated electronic IDA clinical assessment service which supports appropriate clinical interaction between primary and secondary care before any further investigation.215 Given the increasing fragmentation of care across providers, this should include a facility for interrogating electronic healthcare records for any previously documented diagnosis of IDA, and the results of prior investigations including oesophago-gastroduodenoscopy, colonoscopy and CT colonography.
For a dedicated IDA service to deliver highly effective care, the four essential components are1 confirmation of IDA,2 timely access to appropriate investigation (if not already investigated)3 ensuring appropriate IRT (with long-term therapy when needed) and4 strong clinical leadership.49–51 216
IDA services can also provide an alternative pathway for patients found to have more severe anaemia, and who otherwise might have been referred for emergency hospital admission. Estimates based on data from Hospital Episode Statistics 2017 suggest that up to 97 781 patients are admitted in England each year with IDA as the primary diagnosis, which is 72% higher than in 2012. Similar increases over the same period are seen for non-elective hospital spells (days in hospital) with IDA as a secondary diagnosis.
Costs associated with IDA
The estimated costs incurred by the NHS in the management of IDA in secondary care in England rose from £65.8 million in 2012/2013 to £90.6 million in 2017/2018.217 The vast majority of these costs arose from patient management—outpatient or emergency inpatient referral, and subsequent investigation—rather than from treatment of the iron deficiency. Clearly, treatment costs following the diagnosis of CD for example are very different to those associated following occult GI blood loss in patients taking anticoagulants. Few studies have analysed the investigation and management costs of IDA, but it is recognised from data collected as part of the national blood transfusion audits that costs arising from unnecessary emergency hospital admission could be substantially reduced if alternative patient referral pathways were readily available to support ambulatory care.217
While most oral iron supplements are cheap, they are not always well-tolerated, often due to GI side-effects. Newer oral iron supplements are better tolerated, but more expensive (table 3). Intravenous IRT is often necessary for patients with comorbidities which impair iron absorption. While there are several studies reporting the cost-effectiveness of intravenous iron preparations in comparison to oral IRT for specific conditions such as CKD, CHF and IBD, it is the associated comorbidity which accounts for the improved cost-effectiveness of intravenous iron in these circumstances.218
Patient summary
Iron is a nutrient essential to life. It is used in the body to produce many cellular proteins, and an important one is Hb, the oxygen-binding protein found in red blood cells. A shortage of iron in the body prevents the production of these proteins, and so one of the major consequences is that the rate and quality of red cell production in the bone marrow is reduced—a condition called IDA.
IDA is common worldwide, and can result in many symptoms including extreme fatigue and breathlessness. It can generally be diagnosed by simple blood tests, and remedied by treatment with IRT given by mouth or injection.
There are many causes of iron deficiency, including a poor dietary intake, and failure to absorb dietary iron in the upper bowel. Because blood is iron-rich, it can also result from the gradual loss of blood from the body over the course of a long period—and this is a common cause of IDA.
Studies have shown that about a third of adults over the age of 50 with IDA in the UK have an underlying bleeding abnormality, most commonly in the stomach or lower bowel. In about a third of these, the abnormality proves to be a cancer. It is therefore recommended that unexplained IDA in this age group is investigated by examining these areas, even if there are no other relevant symptoms. This is usually done by endoscopy, though CT scanning is an alternative for assessing the lower bowel.
Research recommendations
Diagnosis
New digital approaches to identifying IDA.
Investigation
FIT and risk stratification in IDA.
Role of screening for atrophic gastritis by histology or serology (eg, Gastropanel).
The role of newer diagnostic modalities for example, colon capsule.
Treatment
Optimal dosage regimes for oral IRT.
Optimal target of treatment with oral IRT.
Role of newer iron salts (eg, ferric maltol) when traditional salts have failed.
Optimal place of intravenous iron in acute and chronic settings.
The role of laboratory investigations in predicting non-response to oral IRT.
Special situations
Appropriate investigative strategies in menstruating women.
Epidemiology, investigation and treatment of NAID.
Ethics statements
Patient consent for publication
References
Footnotes
JS and NB are joint first authors.
Twitter @nijbhala, @gastrolivuni, @drreenasidhu1, @UKGastroDr, @bodgoddard
Correction notice This article has been corrected since it published Online First. Affiliation number 6 and table 4 have been updated.
Contributors All coauthors contributed material for and amendments to the original draft, and approved the final version for submission.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests ILPB: Vifor advisory board, Pharmcosmos advisory board; PI for Feraccru studies. RL: Vifor Advisory Board, NHS England advisor. MP: Trio Medicines (research funding); IPSEN, Advanced Accelerator Applications, Mayoly Spindler laboratories (consultancies). AMV, WT, RS, CK, DC, NB, SS, AFG, JS: none declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.