Article Text

Abstract
Objective An unmet need exists for a non-invasive biomarker assay to aid gastric cancer diagnosis. We aimed to develop a serum microRNA (miRNA) panel for identifying patients with all stages of gastric cancer from a high-risk population.
Design We conducted a three-phase, multicentre study comprising 5248 subjects from Singapore and Korea. Biomarker discovery and verification phases were done through comprehensive serum miRNA profiling and multivariant analysis of 578 miRNA candidates in retrospective cohorts of 682 subjects. A clinical assay was developed and validated in a prospective cohort of 4566 symptomatic subjects who underwent endoscopy. Assay performance was confirmed with histological diagnosis and compared with Helicobacter pylori (HP) serology, serum pepsinogens (PGs), ‘ABC’ method, carcinoembryonic antigen (CEA) and cancer antigen 19–9 (CA19-9). Cost-effectiveness was analysed using a Markov decision model.
Results We developed a clinical assay for detection of gastric cancer based on a 12-miRNA biomarker panel. The 12-miRNA panel had area under the curve (AUC)=0.93 (95% CI 0.90 to 0.95) and AUC=0.92 (95% CI 0.88 to 0.96) in the discovery and verification cohorts, respectively. In the prospective study, overall sensitivity was 87.0% (95% CI 79.4% to 92.5%) at specificity of 68.4% (95% CI 67.0% to 69.8%). AUC was 0.848 (95% CI 0.81 to 0.88), higher than HP serology (0.635), PG 1/2 ratio (0.641), PG index (0.576), ABC method (0.647), CEA (0.576) and CA19-9 (0.595). The number needed to screen is 489 annually. It is cost-effective for mass screening relative to current practice (incremental cost-effectiveness ratio=US$44 531/quality-of-life year).
Conclusion We developed and validated a serum 12-miRNA biomarker assay, which may be a cost-effective risk assessment for gastric cancer.
Trial registration number This study is registered with ClinicalTrials.gov (Registration number: NCT04329299).
- gastric cancer
- screening
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
Circulating microRNAs (miRNAs) are promising biomarkers for detection of gastric cancer (GC) but previous studies were limited by small cohort sizes and the use of research grade assays.
What are the new findings?
This is the most extensive evaluation of circulating miRNAs as biomarkers for GC detection to date, as measured by both cohort size and technical stringency. A clinical assay based on a panel of 12-miRNA biomarkers was developed, manufactured to clinical standards, and prospectively validated in a multicentre cohort of over 5000 subjects. The assay was more accurate than any existing blood-based diagnostic biomarkers for GC and it could reduce the number of unnecessary upper endoscopy. It was also cost-effective as a screening test for GC.
How might it impact on clinical practice in the foreseeable future?
The serum miRNA biomarker panel can be used as a risk assessment tool for GC before endoscopy. It has the potential to be a cost-effective mass screening tool for GC.
Introduction
Gastric cancer (GC) is the fifth most common cancer and the third-leading cause of cancer deaths worldwide.1 GC mortality is high due to late presentation.2 In high-incidence countries, such as Japan and Korea, mass screening for GC is practiced using photofluorography or, more recently, endoscopy. In these settings, over 50% of GC patients are diagnosed at early stages and their survival is excellent.3 4 However, in most countries, mass screening is neither feasible nor cost-effective because such screening methods are costly and invasive, with poor compliance.4 There is an unmet need for a less invasive and cost-effective GC screening test.
Currently available gastrointestinal tumour markers, including carcinoembryonic antigen (CEA) and cancer antigen 19–9 (CA19-9) are inadequate for GC screening due to their poor sensitivities, especially for early-stage GC.5 Recently, the ABC method, a combination of age, serum anti-Helicobacter pylori (HP) IgG antibody (serology) and pepsinogen (PG) 1 and 2 levels, have shown some promise as a blood test for GC risk stratification in Japan but its clinical performance has varied among different populations.4 6 7
MicroRNAs (miRNAs or miRs) are small non-coding RNAs that regulate gene expression post-transcriptionally.8 Aberrant expression of miRNAs has been implicated in the pathogenesis of many diseases, including cancer.9 10 Cell-free miRNAs have been shown to circulate stably in serum and plasma,11 12 and dysregulation of their expressions correlate with cancer onset and progression, making them attractive biomarker candidates.12 13 However, sensitive and robust detection of these circulating miRNA from clinical samples is challenging due to their small size and low abundance.14 To overcome these challenges, we developed a proprietary miRNA RT-qPCR assay platform with greater sensitivity and reproducibility in detecting circulating miRNAs using small-volume clinical samples.15
The primary aim of this study is to develop a serum panel of miRNA as a non-invasive test that can detect GC of all stages and validate its performance in a large prospective cohort. The secondary aim is to evaluate its cost-effectiveness as a mass screening tool for GC.
Methods
Study design and patient cohorts
We conducted a three-phase, multicentre study to discover and validate a panel of serum miRNA biomarkers for GC. In the discovery phase, we measured the expression of 578 circulating miRNAs in a case–control cohort of 472 Singaporean Chinese subjects, including 236 cancer and 236 matched control subjects, to identify candidate biomarker miRNAs as well as candidate multi-miRNA panels. A total of 236 patients with cancer were from the Gastric Cancer Biomarker Discovery Study (GASCAD), which recruited newly diagnosed GC patients. Blood was collected prior to any cancer treatment. Matched control subjects were enrolled through the Gastric Epidemiology and Molecular Genetics Project (GCEP), a prospective cohort study that aimed to identify GC risk factors in the Singapore Chinese population with age 50 or above and to develop a screening algorithm.16 All control subjects received surveillance endoscopy with standardised biopsy protocol at regular intervals and were confirmed to have no GC or high-grade dysplasia based on endoscopy and histological examination. GC patients and controls were matched in ethnicity (Chinese), sex and age (±10 years).
In the verification phase, we confirmed the dysregulation of candidate biomarkers and identified a 12-miR panel in another case–control cohort of 210 Singaporean and Korean subjects, including 94 cancers and 116 matched controls. Blinded biomarker verification was performed with sera specimen from cancer and control subjects recruited from Singapore and Korea. The Singaporean sample set included 20 additional GC patients and 69 matched controls from GASCAD and GCEP cohorts respectively. The Korean sample set included 74 GC patients recruited at Yonsei Cancer Center and 47 controls who were healthy blood donors from Songdang Institute for Cancer Research.
After the verification phase, a clinical grade multivariate index assay based on the 12-miR panel was formulated. Finally, the performance of this 12-miR panel was validated in a prospective cohort of 4566 Singaporean subjects who underwent upper endoscopy for their gastrointestinal symptoms. Patients eligible for inclusions were consecutive adults, between the ages of 40 and 90 years, who were scheduled to undergo gastroscopy based on standard clinical indications at National University Hospital and Tan Tock Seng Hospital in Singapore from 2013 to 2016. A total of 5282 subjects were recruited. Subjects with a history of total or partial gastrectomy were excluded. The presence and absence of GC and high-grade dysplasia were confirmed by endoscopy and histological examinations. Written informed consent was obtained from all participants.
Blood collection and serum processing
Fasting blood samples (20 mL) were withdrawn from each subject via venipuncture and collected in two plain serum tubes (BD vacutainer plus plastic serum tube). The serum tubes were centrifuged at 3000 rpm at 20°C for 10 min. Centrifugation and serum collection was done within 4 hours of blood collection. Serum specimen were aliquoted and stored immediately at −80°C.
MiRNA quantification in discovery and verification phases
The absolute expression (copy numbers) of 578 candidate miRNAs were quantified in each patient and control biospecimen using miRNA-specific RT-qPCR assays (MiRXES, Singapore) via a highly controlled workflow illustrated in online supplemental figure S1. The analytical specificity, reproducibility and sensitivity of the assay and workflow (online supplemental methods) are shown in online supplemental figure S2. Total RNA from 200 µL of patient and control serum specimen was isolated using miRNeasy serum/plasma miRNA isolation kit (Qiagen, Germany). Synthetic miRNA controls were added to samples before RNA isolation, and RT-qPCR to monitor and normalise technical variations throughout the entire workflow (online supplemental methods). Absolute expression of each miRNA was determined in each patient serum sample and normalised across samples using endogenous reference miRNAs (online supplemental methods).
Supplemental material
12-miR assay in validation phase
A central biorepository received all serum specimens. The 12-miR qPCR assay was developed and manufactured in accordance with the ISO13485 medical devices quality management systems (MIRXES, Singapore). Laboratory testing (online supplemental methods) was performed in CAP/ISO-certified laboratories without knowledge of the results of endoscopic and histopathological findings. Eleven GC related miRNAs (miR-140, miR-183, miR-30e, miR-103a, miR-126, miR-93, miR-142, miR-21, miR-29c, miR-424 and miR-181a) were measured together with a reference miRNA (miR-340) (online supplemental methods). All qPCR measurements were performed in duplicates. The assay generated a numerical GC risk score for each sample using the GASTROSmart Software (MIRXES, Singapore) (online supplemental methods). Using the 12-miRNA panel, a cancer prediction score was generated based on the most optimal sensitivity and specificity combination. The risk score was calculated using a linear regression model of the measured expression levels of the 12 miRNAs in the panel. A score of 40 or more was defined as a positive test result.
Other blood-based GC marker assays
Serum biomarkers CEA, CA19-9, anti-HP IgG, PG 1 and PG 2 were also measured. CEA, CA19-9, PG 1/2 ratio, PG index (combining a PG 1 level cut-off and PG 1/2 ratio), and the so-called ‘ABC method’ by combining HP serology and PG 1/2 ratio have previously been proposed as biomarkers for GC screening.4 6 7 17 Serum specimens were qualitatively assayed for HP antibodies with the MP Diagnostics HELICO BLOT 2.1 Western blot kit assay (MP BIOMEDICALS Asia Pacific). PG I and II levels were determined with latex agglutination turbidimetric immunoassay kit (LZ Test ‘Eiken’ PG I and II, Tokyo, Japan). Access CEA and CA19-9 chemiluminescent sandwich immunoassays (Beckman Coulter, USA) were run on the UniCel DxI 800 immunoassay system (Beckman Coulter, USA). All assays were performed without knowledge of the clinical findings.
Health economic analysis
The overall costs and health benefits of conducting mass screening using the validated miRNA panel relative to current practice of no-screening were estimated for a hypothetical cohort, with assumed health seeking behaviours, disease incidence/progression and associated patient quality-of-life years (QALY) representative of a high-risk population in Singapore (Chinese males of 50–75 years old). We assumed that miRNA test-positive subjects would go on to have a confirmatory endoscopy while test-negative subjects would be followed up in 3 years. Further modelling and parameter uncertainties were addressed using sensitivity analysis. Details of this analysis are provided in online supplemental methods.
Statistical analysis
During the discovery phrase, significantly regulated miRNAs were identified using Student’s t-tests with a false discovery rate (FDR) correction.18 The receiver operating characteristic curve was used to present the performance of individual miRNA or multivariant biomarker panels. A sequential forward floating search (SFFS) algorithm19 was used to optimise the miRNA biomarker panel, with area under the curve (AUC) values as the performance indicator. Multivariate analysis was carried out to construct multi-miR panels with associated algorithms for classifying cancers and controls (online supplemental methods). Multivariate Cox regression analysis of the 12-miR panel and clinical covariates was carried out.
For the prospective validation study, the sample size was calculated based on an expected 2% prevalence of GC in a high-risk symptomatic population and a point estimate of 85% sensitivity based on discovery and verification data. We planned to recruit about 5000 participants to achieve margins of sampling error of approximately 5 percentage points for sensitivity.
The study was reported according to Standards for Reporting of Diagnostic Accuracy Studies 2015 guidelines.20
Results
Identification of GC associated serum miRNA biomarkers
GC-associated serum miRNA biomarkers were identified through retrospective analysis of 472 prospectively collected specimens from GC patients and controls matched by age, sex and ethnicity. Clinicopathological characteristics of the discovery cohort are shown in table 1. The cohort was enriched for early stage GC patients (30.1% stage 1 and 15.3% stage 2) to ensure that it was sufficiently powered to identify biomarkers associated with early stage GC. We systematically evaluated an a priori list of 578 circulating miRNAs using a highly controlled and analytically validated RT-qPCR workflow. Prior to biomarker discovery, the analytical sensitivity, specificity and reproducibility of the miRNA assay and workflow were validated using a combination of synthetic miRNA templates. These assays demonstrated strong discrimination against highly homologous miRNA sequences (online supplemental figure S2A), high concordance in detecting circulating miRNAs in both control and cancer sera (online supplemental figure S2B), and good dynamic range in amplifying and detecting miRNAs with distinct sequences and varying AT content (online supplemental figure S2C).
Discovery cohort clinicopathological characteristics
Of 578 serum miRNAs quantified, 191 miRNAs were detected in more than 90% of the subjects (expression levels ≥500 copies/mL of serum) (online supplemental table S1); 75 of the 191 miRNAs were differentially expressed between cancer patients and matched controls (FDR corrected p<0.01) (online supplemental table S2). Of the 75 dysregulated miRNAs, 68 were novel discoveries; 51 were upregulated and 24 downregulated (online supplemental tables S2 and S3). An expression heatmap of the dysregulated miRNAs showed the majority of GC subjects clustered closely (figure 1A). Many of these miRNAs were positively correlated (Pearson correlation coefficient (r) >0.6) (figure 1B), suggesting potential co-regulation in miRNA expression. Among the dysregulated miRNAs, miR-142–5 p (upregulated) and miR-99b-5p (downregulated) exhibited the highest AUC, at 0.71 and 0.67, respectively (online supplemental figure S3A). Seven miRNAs were found to be differentially expressed (FDR corrected p<0.05) in the three histological subtypes (diffuse, intestinal and mixed) of GC (online supplemental figure S4). Thirty-six miRNAs were differentially regulated at various stages of GC (FDR corrected p<0.01) (online supplemental figure S3B and table S4).
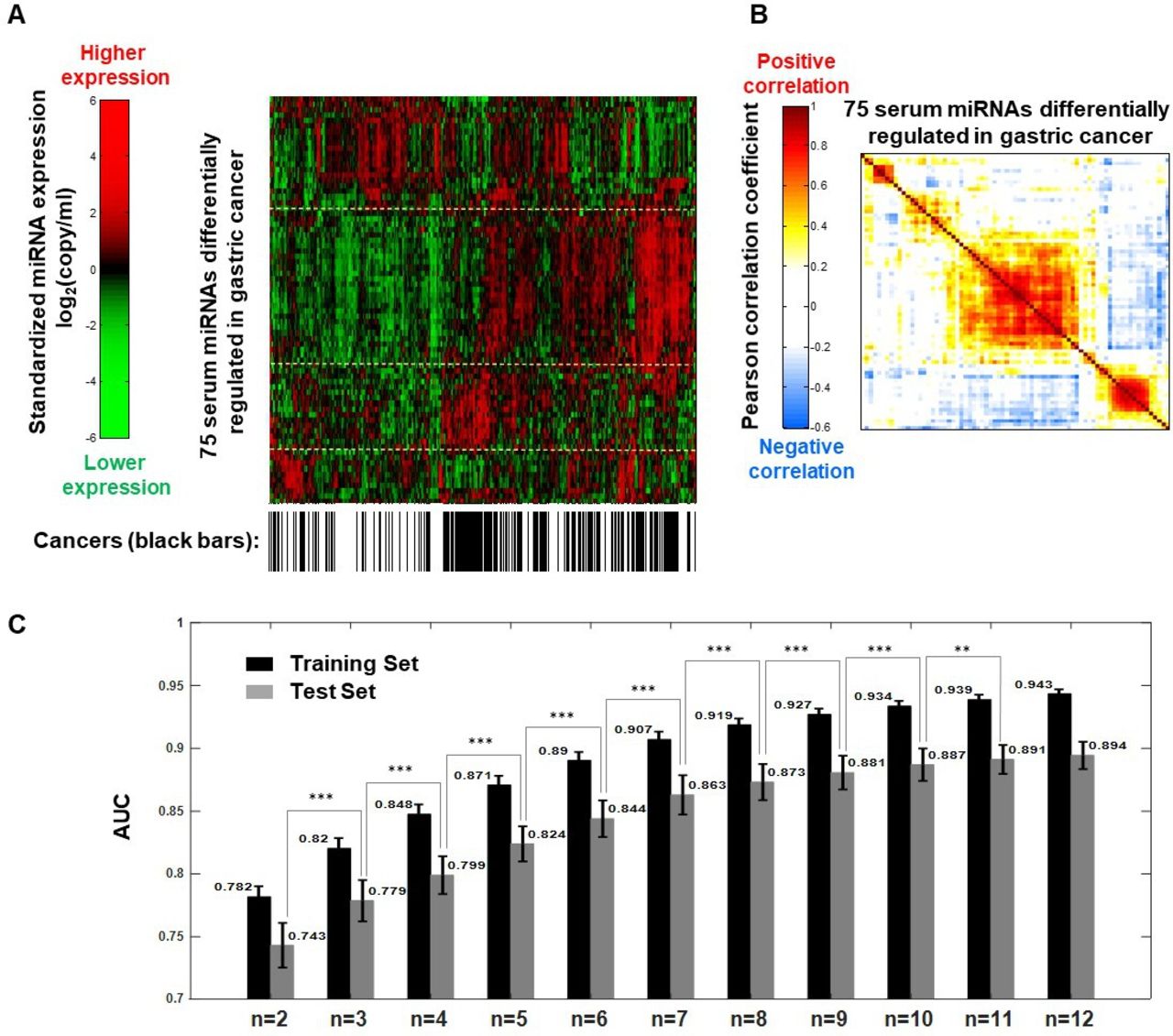
Identification of candidate miRNA biomarkers and multi-miRNA biomarker panels for gastric cancer detection. (A) Heat-map showing expression levels of serum miRNAs that were differentially regulated in gastric cancer. The full list can be found in in online supplemental table S2; absolute miRNA expression levels (copy/mL) of miRNAs were presented in log2 scale and standardised to zero mean. Hierarchical clustering was carried out for both dimensions (miRNAs and samples) based on Euclidean distance. (B) Correlation in expression levels between differentially regulated miRNAs. Pearson’s linear correlation coefficients were calculated between all 75 miRNAs that were identified to be differentially regulated in gastric cancer (online supplemental table S2). (C) Gastric cancer detection accuracy of multi-miRNA biomarker panels with 3–10 miRNAs as determined by mean area under ROC curve (AUC). Biomarker panels were tested in the discovery cohort. Two hundred iterations of a cross-validation process were carried out by dividing the Discovery cohort into two data sets: training and testing. Error bars indicate SD. Statistical significance of difference in AUC was determined using Student’s t-test (one sided, **p<0.01; ***p<0.001). AUC, area under the curve; miRNA, micro-RNA.
Next, we developed and tested multi-miRNA biomarker panels with high AUC in distinguishing cancer from controls using cross-validation. The discovery cohort was partitioned into equally sized training and test sets matched for cancer stage, subtype, age, gender and ethnicity.21 We derived multi-miRNA biomarker panels in training set using SFFS and SVM and tested the panel performance in the test set. The composition of the miRNA panels included a combination of miRNAs that were individually significant and non-significant between GC and matched controls. An improvement in AUC was observed when number of miRNAs in the panel increased but plateaued at 12-miRNAs. The median AUC values for a 12-miRNA panel were close to 0.90 in the test set, with a spread between the 25th and 75th percentile of <0.05 (figure 1C). Incorporating more miRNAs into the panel did not significantly improve AUC. Multivariate Cox regression analysis showed that the 12-miRNA biomarker panel was independent of clinical covariates in detecting GC (online supplemental table S5).
Verification of miRNA biomarker panel
We verified the performance of individual miRNAs and the 12-miR panel in two independent retrospective case–control cohorts of 89 subjects from Singapore and 121 subjects from Korea (table 2). We observed good correlations in individual miRNA expression fold-changes between the discovery cohort and each of the two verification cohorts (figure 2A).
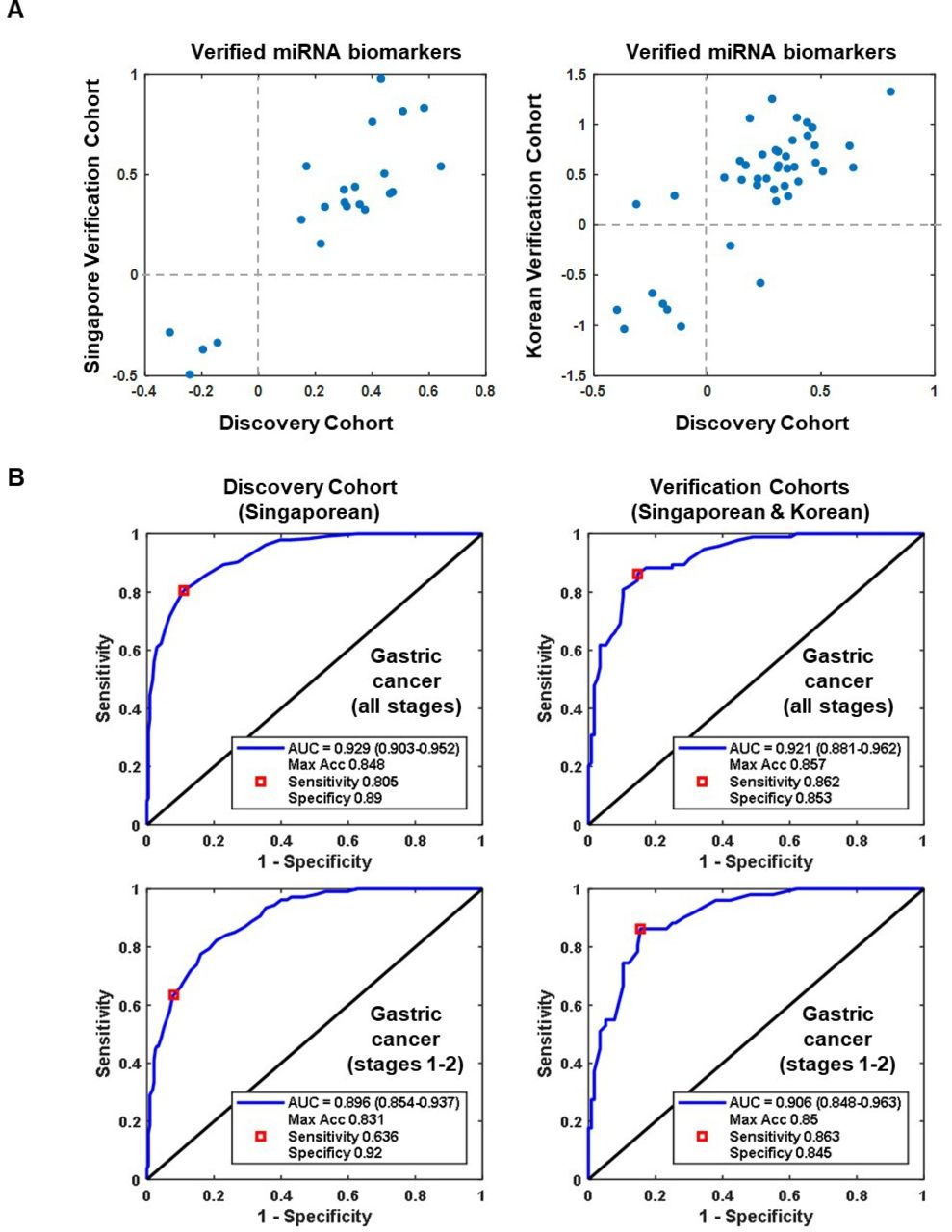
Verification of gastric cancer miRNA biomarkers and multi-miRNA biomarker panel detection accuracy in independent cohorts. (A) Correlation in expression level fold changes (cancer over control) of verified miRNA biomarkers between the discovery cohort and verification cohorts. (B) Receiver operating characteristics (ROC) curves for the 12-miRNA biomarker panel in detecting all gastric cancers (A) and early stage (stage 1–2) cancers (B). Area under the ROC curve (AUC) used to determine gastric cancer detection accuracy. Maximum classification accuracy is determined to occur at the point indicated by the red box. The sensitivity and specificity at this point is shown. miRNA, micro-RNA.
Verification cohort clinicopathological characteristics
Similarly, the 12-miR panel identified through the discovery cohort showed consistency in the verification cohorts. The panel was able to discriminate GC from matched controls with AUC 0.93 (95% CI 0.90 to 0.95) in discovery cohort and 0.92 (95% CI 0.88 to 0.96) in the verification cohort. When comparing early-stage GC (stages 1–2) from matched controls, the panel achieved AUC 0.90 (95% CI 0.85 to 0.94) in the discovery cohort and 0.91 (95% CI 0.85 to 0.96) in the verification cohort (figure 2B). The verified 12-miR panel (miR-140, miR-183, miR-30e, miR-103a, miR-126, miR-93, miR-142, miR-21, miR-29c, miR-424, miR-181a and miR-340) was thus finalised and developed into a clinical assay in accordance with the ISO13485 medical devices quality management system for prospective validation.
Prospective validation of the 12-miR assay
Study population
The 12-miR assay, with a prespecified prediction algorithm, was validated in a large prospective validation cohort of Singaporean patients (figure 3). The clinicopathological characteristics are shown in table 3. A total of 5282 participants underwent endoscopy, and had serum collected for testing with the 12-miR assay and other serum-based biomarker tests that have been suggested for GC detection (HP serology, PG 1/2 ratio, PG index, ABC method, CEA and CA19-9). 597 subjects were excluded from miRNA analysis due to sample quality issues. Of the remaining 4685 samples assayed, 4570 (97.5%) yielded valid test results. The remaining samples did not yield valid results due to invalid expression ranges or were excluded from data analysis due to incomplete clinical information. Altogether, 4566 participants had results that could be fully analysed for the 12-miR assay, HP serology, CEA and CA19-9 tests. A total of 133 samples were excluded from PG 1/2 analysis because patients had renal failure which affects PG levels. A total of 4433 patients had results for the PG tests which could be analysed. A total of 115 biopsy-proven GC was found by endoscopy (prevalence, 2.5%). Another 10 participants were found to have gastric high-grade dysplasia.

Prospective validation of 12-miR biomarker assay for detection of gastric cancer. Flow chart of prospective validation study design prepared in accordance with Standards for Reporting of Diagnostic Accuracy Studies guidelines. miR, micro RNA, NC, negative control; QR, quantitative reference.
Prospective validation cohort clinicopathological characteristics
Assay performance
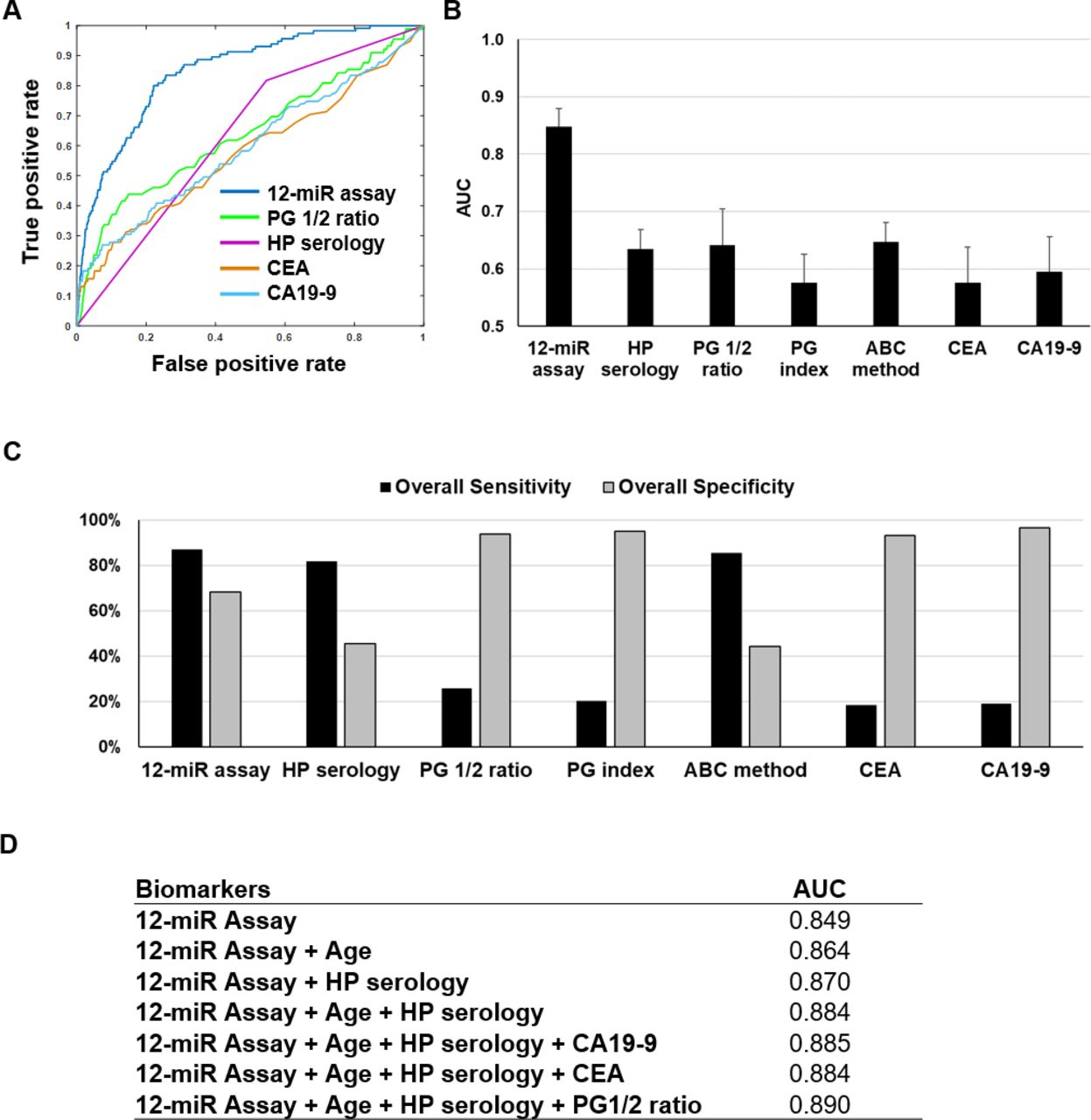
The 12-miR distinguished GC from matched normal controls with AUC 0.848 (95% CI 0.809 to 0.880) (figure 4A). This GC detection accuracy was higher than HP serology (AUC 0.635, 95% CI 0.594 to 0.668), PG 1/2 ratio (AUC 0.641, 95% CI 0.567 to 0.705), PG index (AUC 0.576, 95% CI 0.540 to 0.626), ABC method (AUC 0.647, 95% CI 0.60 to 0.681), CEA (AUC 0.576, 95% CI 0.512 to 0.638) or CA19-9 (AUC 0.595, 95% CI 0.535 to 0.656) (figure 4A,B).

Gastric cancer detection accuracy of 5-miR biomarker assay compared with other serum-based biomarker tests. (A) ROC curves for 12-miR assay, PG 1/2 ratio, HP serology, CEA, and CA19-9 for detection of gastric cancer. (B) AUC for 12-miR biomarker assay compared with HP serology, PG 1/2 ratio, PG index, ABC method, CEA, and CA19-9 tests. Bars show 95% CI (C) Overall sensitivity and associated specificity of GC detection using the 12-miR assay (both high sensitivity and high specificity cut-offs), HP serology, PG 1/2 ratio, PG index, ABC method, CEA, and CA19-9 tests. (D) Combinations of biomarker tests with optimal AUC for detecting gastric cancer. AUC, area under the curve; CA19, cancer antigen 19; CEA, carcinoembryonic antigen; HP, Helicobactor pylori; miR, micro-RNA; PG, pepsinogen.
The 12-miR assay identified 100 of 115 GC detected by endoscopy, for an overall sensitivity of 87.0% (95% CI 79.4% to 92.5%) at a specificity of 68.4% (95% CI 67.0% to 69.8%). The 12-miR assay achieved the highest sensitivity among the serum-based biomarker tests (figure 4C). PG, CEA and CA19-9 tests had higher than 90% specificity but lower than 30% sensitivity for GC detection. GC detection accuracy with the 12-miR assay can be improved by including patient’s age, HP serology and PG 1/2 ratio (figure 4D). Using this combination, AUC was improved to 0.884, with specificity of 69.4% at sensitivity of 87.0%. GC detection sensitivity of the 12-miR did not vary significantly by cancer stage, gender and ethnicity but tends to be higher in older patients, larger tumour and intestinal-type GCs (figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Detection sensitivity of 12-miR assay by gastric cancer stage and clinicopathological characteristics. Detection sensitivity at 68.4% specificity according to (A) gastric cancer stage, (B) age range, (C) tumour size, (D) histological subtype (Lauren classification), (E) gender and (F) ethnicity. miR, microRNA.
To detect 115 GC cases in a symptomatic population, 4566 gastroscopies were carried out. Therefore, 40 gastroscopies will be required to detect one case of GC if no biomarker test were used. In comparison, only 15 endoscopies will be required if the 12-miR assay result was used to select patients for endoscopy in the same population. The positive predictive value (PPV) of using the 12-miR assay is 6.7% while the negative predictive value (NPV) is 99.5%. The assay had minimal cross-reactivity with other common cancers including those of the gastrointestinal tract (online supplemental table S6 and figure S6).
Health economic analysis
Using an assumption of compliance reflective of the existing screening programmes in Asia (45%), the number needed to screen (NNS) with the 12-miR assay in order to detect one case of GC was calculated to be 489 annually. Mass screening with the 12-miR assay can increase early-stage GC detection rate to 40 per 100 cancers identified, compared with 30 per 100 in current practice (table 4). Overall, mass screening using the 12-miR assay added costs of USD 175 per subject. The ratio of additional cost to additional health gains, or the incremental cost-effectiveness ratio is USD44 531/QALY, which is cost-effective in the local context, compared with the WHO-CHOICE threshold of approximately USD50 000/QALY (table 5). We anticipate that actual compliance for mass screening is likely to be significantly higher for a non-invasive test compared with endoscopy.
Results of base-case analysis for mass screening for Singapore Chinese Males (50–75 years)
Cost-effectiveness of mass screening using 12-miR assay in conjunction with endoscopy
Discussion
In recent years, miRNAs have been investigated as promising GC biomarkers because many solid tumours exhibit dysregulation of miRNA expression.13 Patients with cancer exhibit aberrant expression of circulating miRNAs in biofluids such as blood.22 23 However, change in miRNA expression in blood is less readily detected than changes in tissue due to multiple tissue sources for circulating miRNA and multiple physiological or pathological conditions affecting miRNA quantities. It is also technically challenging to detect miRNAs because of their small size. Previous studies exploring circulating miRNAs as GC biomarkers have shown promising proof-of-concept results but remain largely inconclusive, possibly due to small cohort sizes (n=6 to 570),24–26 and the use of research grade assays.27
To the best of our knowledge, this is the most extensive evaluation of circulating miRNAs as biomarkers for GC detection as measured by both cohort size and technical stringency. We quantified the absolute expression of 578 serum miRNAs in 682 cancer patients and control subjects using a comprehensive biomarker detection platform that incorporated important advances that were designed to overcome the biological and technical challenges inherent in detecting circulating miRNA. Sixty-eight novel serum miRNAs associated with GC were discovered. Subsequently, we used multivariant data analysis to develop a 12-miR assay that discriminated between GC patients and matched high-risk controls with high accuracy (AUC >0.93). A clinical grade 12-miR assay was then manufactured in accordance with the ISO13485 medical devices quality management systems and validated in a prospective cohort of 4566 patients. Depending on cut-off used, detection sensitivity reached 87% while specificity was as high as 93.9%. The assay could detect GC with high sensitivity across all age groups, genders, ethnicities and tumour stages. The serum 12-miR assay performed significantly better than any of the conventional blood-based biomarker tests. Its performance can be further enhanced by combining with age and HP serology to achieve an AUC of 0.884. Furthermore, we demonstrated the clinical specificity of the 12-miR assay against seven other prevalent cancers, including lung, breast, colorectal, liver, oesophageal, prostate and bladder cancer. We used a multivariate panel, instead of solitary miRNA biomarkers, to overcome low detection accuracy attributed to tumour heterogeneity.12
In the symptomatic study population, the 12-miR assay has a NNS to detect one cancer of 15, comparing favourably with NNS of 40 with unselected gastroscopy in the same population. While it is not the intent of the 12-miR assay to replace endoscopic evaluation, we believe this assay provides a useful option for symptomatic patients who might not be keen on initial endoscopic screening. The 12-miR assay is also a potential tool for mass screening. In this scenario, NNS was 489 annually which compares favourably with prostate-specific antigen, a common serum-based screening test for prostate cancer.28 If used for mass screening, the 12-miR assay is also capable of detecting more early-stage GCs than current practice. Furthermore, a blood-based test is expected to have better population compliance compared with a scope-based evaluation. In countries with high prevalence of GC, and with endoscopic screening programmes, such as South Korea, the 12-miR assay can enhance overall compliance among the population subset who decline endoscopy. In countries with intermediate prevalence of GC and no current screening programmes, such as Singapore, the 12-miR assay can be implemented as a screening test with endoscopic examinations for those with positive 12-miR assay results.
There are limitations of this assay. First, the 12-miR panel had high sensitivity but moderate specificity. We chose a risk score cut-off giving high sensitivity by design to minimise false negatives since this blood test served as a prescreening test for GC. Patients with positive test results will undergo endoscopy to confirm the diagnosis. Thus, this blood assay may reduce the reliance on endoscopy. Any test will have false negatives and it does not supplant clinical review and consideration for endoscopy if symptoms persist. It is not the intent of the 12-miR assay to replace endoscopic evaluation, we believe this assay provides an option for patients who might not be keen on initial endoscopic screening, and adds to the current cancer evaluation tool armamentarium, just as the stool DNA test is an option for colon cancer screening. Second, most controls in this study were patients with gastrointestinal symptoms referred to hospital clinics. Care should be taken when applying these findings to the general population. This 12-miR assay has obtained regulatory approval in Singapore and post-market surveillance data being gathered will clarify the PPV and NPV in different clinical settings, including in the general population. To date, the NPV in the general population is encouraging (data not shown). Furthermore, the study population is entirely Asian. Future studies in other populations should be considered. Finally, the roles that these GC-associated circulating miRNAs play in GC development and progression have not been defined through functional studies. Some of these miRNAs were shown to promote cancer metastasis and modulate tumour immune environment, additional mechanistic studies in cell and animal models are required.29 30
In conclusion, we have developed and validated a serum miRNA biomarker panel assay as a risk assessment tool for detecting GC. This assay is a useful adjunct in the armamentarium for cancer screening and has the potential to be a cost-effective mass screening tool for GC.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The studies were approved by Domain Specific Review Board (DSRB) of the National Healthcare Group, Centralised Institutional Review Board (CIRB) of Singapore Health Services, Institutional Review Board (IRB) of National University of Singapore, Yonsei Cancer Center and Songdang Institute for Cancer Research.
Acknowledgments
We would like to thank all our participants and the investigators from Yonsei Cancer Centre, NUH and TTSH hospitals, investigators from the Singapore Gastric Cancer Consortium (SGCC), the NUHS Tissue Repository, NUH Lab Medicine as well as the staff of all participating clinics, laboratories and research institutes for their contributions to the study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors JBYS, KGY, H-PT, JY, CTY, PCKG, JL, KPL, MH, CK, FZ and WPY participated in the design and performance of the study, review of results, analysis and discussion. JBYS, CK, JL, SYR, HCC, JR, CKC, ST and AS enrolled subjects for the study and contributed clinical data. HPT, LZ, RZ, RK and JY analysed the data and RK performed the cost-effective analysis. The manuscript was drafted by JBYS, KGY, H-PT, LZ, YCT, RK, JY and reviewed by all authors. All authors read and approved the final manuscript.
Funding The Singapore Gastric Cancer Consortium (SGCC) is a national translational research group comprising clinicians and scientists working in gastric cancer research from academic medical centres, universities, hospitals and research institutes across Singapore. It receives funding from the National Research Foundation Singapore under its Translational and Clinical Research (TCR) Flagship Programme and Open Fund-Large Collaborative Grant (OF-LCG), administered by the Singapore Ministry of Health’s National Medical Research Council. This study was supported by the Bedside & Bench grant (NMRC/BnB/0014b/2014) and the Translational and Clinical Research grant administered by Singapore Ministry of Health’s National Medical Research Council (NMRC/TCR/009-NUHS/2013, NMRC/TCR/001-NUS/2007) and RIE2020 Centre Grant (CG) Programme (NMRC/CG/M005/2017_NCIS), as well as the COT and GAP grants administered by Singapore A*STAR Exploit Technology.
Competing interests KGY, JBYS, WPY, HPT, LZ, RZ and FZ were coinventors in the patent application 'Serum MicroRNA Biomarker for the Diagnosis of Gastric Cancer'. HPT, LZ and RZ are founders and shareholders of MiRXES. LZ, RZ and YCT are employees of MiRXES. HCC received grants from Lilly, GSK, MSD. Merck-Serono, BMS-Ono, Taiho outside the submitted work. The rest of authors declare no competing interests.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.