Article Text

Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
In order to protect endoscopy staff, guidelines recommend pre-endoscopy COVID-19 testing.
WHAT THIS STUDY ADDS
Our retrospective analysis presents no SARS-CoV-2 transmission performing 4543 outpatient endoscopies without pre-procedural testing.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Usage of personal protective equipment together with a vaccination against COVID-19 might be enough to substantially reduce the risk of SARS-CoV-2 transmission to endoscopy staff.
Message
Pre-endoscopy viral real-time PCR (RT-PCR) testing has been recommend by several guidelines in addition to personal protective equipment (PPE). We analysed retrospectively 15 750 GI endoscopies performed by 29 endoscopy staff members in one institution during a 20-month period until December 2021 using PPE and three different test approaches: no testing (n=4543), rapid antigen (RA) testing (n=682) and RT-PCR testing (n=10 465). In addition, 60 endoscopies were performed in patients with proven COVID-19. Not a single staff member became infected with SARS-CoV-2 during the 20 months analysed; vaccination rate of the team was 97%. We suggest that pre-selection of patients with respective questionnaires, vaccination and particularly PPE appear to be sufficient for the prevention of SARS-CoV-2 transmission in GI endoscopy.
In more detail
The outbreak of the COVID-19 pandemic led to dramatic changes in GI endoscopy. Very soon, PPE such as high-filter respiratory masks (FFP2) and water-resistant gowns were recommended by many, if not all national and international societies for prevention of transmission of the virus to staff members.1 2 After the lockdown, when a deceleration of incidence rates was observed, routine procedures were increasingly performed in almost all endoscopic centres. This was mainly related to the fact of growing experience on how to avoid transmission but also on widespread use of tools for viral testing. Since GI endoscopies can be regarded potentially hazardous examinations due to close contact to the patient, it has been therefore suggested that pre-endoscopy viral testing based on RT-PCR-tests should be considered, at least for patients who are not fully vaccinated.3–5 Due to a lack of evidence, RA tests have not been recommended.3
To further gain data on the effectiveness of various prevention measurements (solely PPE, RA test, RT-PCR test), we retrospectively evaluated the transmission rate in a tertiary endoscopy unit in an area with a medium COVID-19 incidence in Germany.
Between 1 May 2020 and 31 December 2021, a total of 15 750 GI endoscopies were performed at the University Hospital of Würzburg. The hospital is spatially divided into a centre for operative medicine (ZOM) and a centre for internal medicine (ZIM). At the ZOM, a negative RT-PCR test was mandatory for all endoscopies. At the ZIM, RT-PCR testing was only necessary for procedures performed in hospitalised patients. In this case, patients received an RT-PCR test at admission and thus before performing the endoscopy. For patients who were scheduled for complex procedures necessitating overnight surveillance, a negative RA test was required starting January 2021.6 Endoscopy was performed directly after the RA test result. For all other ZIM patients who received an endoscopy on an outpatient basis, no test was required. All patients were interviewed on symptoms, contacts to infected persons and recent travelling in high-risk countries before admission. Last but not least, endoscopies were also performed in patients with proven infection (figure 1). Endoscopies were performed using PPE as recommended (FFP2 mask, one pair of gloves, protective eyewear and disposable gowns); in patients with known COVID-19, two pairs of gloves, a disposable hairnet and a water-resistant disposable gown were used for additional protection. The regular endoscopies were performed in negative pressure intervention rooms.

Number of endoscopies performed in relation to pre-endoscopy testing. Asterisk (*) resembles time span January–December 2021.
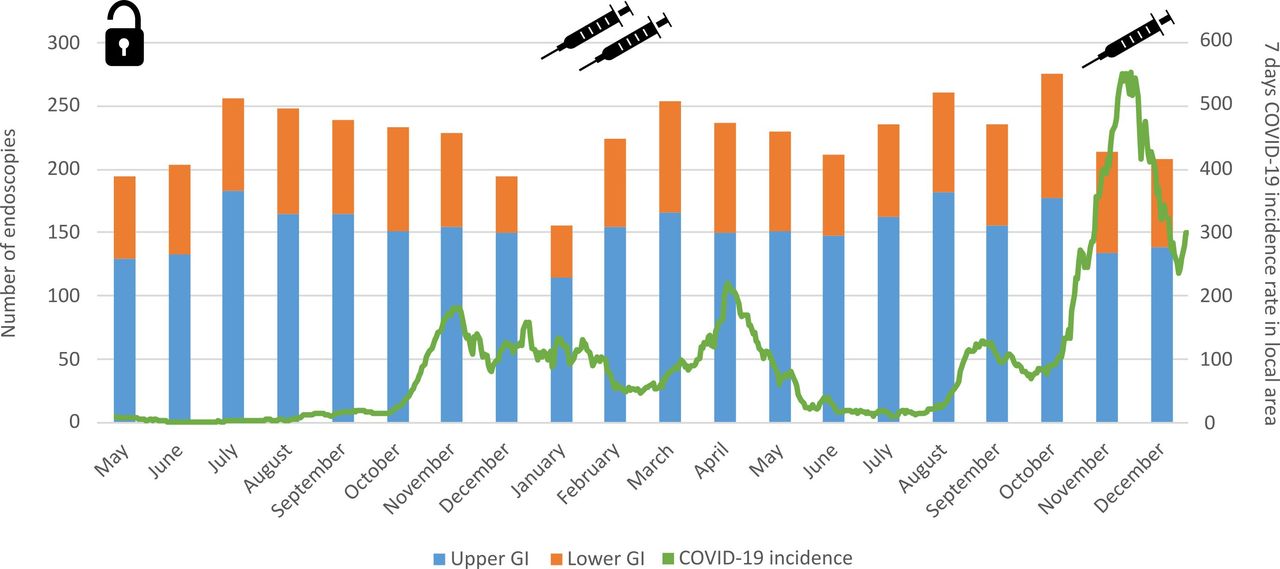
In total, 29 staff members were involved (physicians: 16, assistants: 13). Staff was defined as working in the endoscopy unit for at least 2 days a week for at least 6 months. No routine testing of the endoscopy staff was performed. Of note, not a single infection was detected in any of the staff members during the time period. The internal policy of our hospital is that medical staff must be tested using RT-PCR testing if RA test is positive or symptoms exist. Due to this policy, symptomatic infections would have been detected. This includes the period before and after vaccination of the staff. Vaccination was performed using two dosages of BNT162b2 (Pfizer-BioNTech) in January and February 2021. Booster immunisation was performed with a single dose of BNT162b2 or mRNA-1273 (Moderna) in November and December 2021. Furthermore, mean local 7-day incidence rate was not related to the number of examinations performed in patients with no pre-endoscopic testing (figure 2).

{kind=link}
{kind=link}
Outpatient endoscopies performed in patients without pre-procedural COVID-19 test from May 2020 to December 2021. Symbols represent when lockdown ended and staff was vaccinated.
Comments
Although our data were not part of a randomised prospective study, we were able to demonstrate on a fairly high number of patients that PPE measurements in addition to a short interview for assessment of a patient’s individual risks appear to be highly effective to control transmission of SARS-CoV-2 during endoscopy. Pre-procedural RT-PCR testing or RA testing did not show any additional benefit. Of course, it cannot be excluded that with even higher incidence rates as currently with the Omicron variant, a few cases would have been detected, especially since infections in the private area (school, social life) with this variant seem to be higher. Nevertheless, even then, it would have to be differentiated whether infections were then transmitted from patients to staff.
Apart from PPE, a beneficial effect of vaccination against COVID-19 may be possible as well. This is supported by the fact that even fairly high incidence rates at the end of 2021 did not lead to any transmission of the virus (figure 2). Of interest, it should also be noted that data from the same hospital showed that if a strict RT-PCR testing policy is adhered to, there is a risk of 0.6% that asymptomatic but infected patients are examined, as demonstrated in a previous study of some of the authors.7 Hence, it can be assumed that approximately 30 infected but not tested patients underwent outpatient endoscopies during the examined time period. This highlights again the effectiveness of PPE for avoidance of transmission.
Limitations of our study include the retrospective design and that the lack of systematic testing of the endoscopy staff prevents the exclusion of asymptomatic infections. Additionally, the relatively low COVID-19 incidence in our local area might have positively influenced the risk of transmission. However, even at the end of 2021, when the incidence was increasing, we did not see any higher risk of transmission to endoscopy staff. Another important limitation of our study relates to the new variant Omicron that was dominant in our local area after the analysed time frame.
In summary, our study compares three strategies with different measures. In group 1, endoscopy was performed only with PPE; in group 2, endoscopic examination was done with PPE and after negative RA testing; and in group 3, a negative RT-PCR testing was mandatory before endoscopy was performed. In all three groups, we did not detect a virus transmission. Although this was not a randomised study, data were assessed prospectively with different approaches during an identical time interval. We therefore think that our conclusion is valid (PPE is highly effective for avoidance of SARS-CoV-2 transmission during upper or lower GI endoscopies, depending on local incidence and vaccination status of staff and patients). Current testing strategies should be reconsidered taken into account the additional costs and implications on routine activity.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
The Ethics Committee of the University of Würzburg allowed for retrospective analysis of patients treated at the same centre. Analysis was performed for quality control reasons. Informed consent was obtained for treatment at the centre. No consent was obtained for anonymised analysis of the cases for quality control reasons.
Acknowledgments
Authors like to thank Professor Ulrich Vogel, coordinator of the COVID-19-task force at the hospital, and the whole endoscopy staff for their continuous support during the pandemic and beyond.
Footnotes
Contributors AH and AM—study concept and design. AH, SF, SR, KG and AM—interpretation of results. AM—drafting of the manuscript. AH, SF, SR, KG, TK, C-TG and AM—acquisition of data. AH and AM are responsible for the overall content as guarantors. All authors—critical revision of the article for important intellectual content and final approval of the article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.