Article Text

Abstract
Objective Anti-drug antibodies (ADA) to anti-tumour necrosis factor (anti-TNF) therapy drive treatment loss of response. An association between intestinal microbial composition and response to anti-TNF therapy was noted. We therefore aimed to assess the implications of antibiotic treatments on ADA formation in patients with inflammatory bowel disease (IBD).
Design We analysed data from the epi-IIRN (epidemiology group of the Israeli IBD research nucleus), a nationwide registry of all patients with IBD in Israel. We included all patients treated with anti-TNF who had available ADA levels. Survival analysis with drug use as time varying covariates were used to assess the association between antibiotic use and ADA development. Next, specific pathogen and germ-free C57BL mice were treated with respective antibiotics and challenged with infliximab. ADA were assessed after 14 days.
Results Among 1946 eligible patients, with a median follow-up of 651 days from initiation of therapy, 363 had positive ADA. Cox proportional hazard model demonstrated an increased risk of ADA development in patients who used cephalosporins (HR=1.97, 95% CI 1.58 to 2.44), or penicillins with β-lactamase inhibitors (penicillin-BLI, HR=1.4, 95% CI 1.13 to 1.74), whereas a reduced risk was noted in patients treated with macrolides (HR=0.38, 95% CI 0.16 to 0.86) or fluoroquinolones (HR=0.20, 95% CI 0.12 to 0.35). In mice exposed to infliximab, significantly increased ADA production was observed in cephalosporin as compared with macrolide pretreated mice. Germ-free mice produced no ADA.
Conclusion ADA production is associated with the microbial composition. The risk of ADA development during anti-TNF therapy can possibly be reduced by avoidance of cephalosporins and penicillin-BLIs, or by treatment with fluoroquinolones or macrolides.
- inflammatory bowel disease
- infliximab
- antibiotics
- TNF-alpha
- intestinal microbiology
Data availability statement
Data are available upon reasonable request. The data used in the study was obtained from the epi-IIRN registry.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
Immunogenicity to anti-tumour necrosis factor (anti-TNF) therapy in patients with inflammatory bowel disease (IBD) is considered a leading cause of treatment loss of response.
The association between intestinal microbial composition and response to anti-TNF therapy is becoming increasingly acknowledged. However, no studies assessed the distinct effect of various antibiotic classes on immunogenicity and response to anti-TNF therapy.
What are the new findings?
The intestinal microbiome plays a key role in anti-drug antibodies (ADA) production.
The risk for ADA development was increased in patients exposed to cephalosporins or penicillin with β-lactamase inhibitors, before or during anti-TNF therapy, while the use of fluoroquinolones or macrolides was associated with a reduced risk of immunogenicity.
In agreement with the human patient data, mice challenged with infliximab and pretreated with cefuroxime demonstrated overall higher ADA levels, while azithromycin, or no antibiotics showed lower ADA levels.
How might it impact on clinical practice in the foreseeable future?
Specific antibiotic classes such as fluoroquinolones, or macrolides can potentially be used to reduce the risk of immunogenicity.
Thoughtful selection of antimicrobial therapy is required in patients with IBD treated with anti-TNF therapy.
Introduction
Anti-tumour necrosis factor (anti-TNF) monoclonal antibodies are an effective and well-established treatment for induction and maintenance of remission in Crohn’s disease and ulcerative colitis.1–5 However, primary non-response to anti-TNF therapy is seen in ~40% of patients with even higher rates of failure to achieve complete remission.6 7 Additionally, the rate of secondary loss of response (LOR) after 12 months of therapy ranges between 23% and 46% for infliximab and adalimumab, with an annual risk of 13% loss of response to infliximab per patient year.8 9 Immunogenicity, which refers to the development of anti-drug antibodies (ADA) is considered as the main factor driving secondary LOR and is likely involved in primary non-response as well.10 11
ADA development is associated with reduction in serum drug levels, reduced treatment efficacy and treatment failure.12 Numerous risk factors for ADA development were recognised, including genetic predisposition,13 drug storage and administration and formation of drug/target complexes.12 14 15 Yet, there is limited understanding of how to predict and mitigate the risk for ADA formation.
Concomitant treatment of an anti-TNF with thiopurines or methotrexate was shown to reduce the development of ADAs, even when added after anti-TNF treatment initiation, or when combined with a second anti-TNF after loss of response to a previous agent,12 16–20 and was suggested as the major protective factor against immunogenicity.21 However, anti-TNF and immunomodulators combination treatment is associated with significant risks including malignancy and opportunistic infections.22–24
It is currently widely accepted that microbial dysbiosis plays an important role in the pathogenesis of inflammatory bowel disease (IBD).25 Moreover, a growing body of evidence demonstrated an association between the intestinal microbial composition and response to anti-TNF therapy.26–29 Of relevance, a recent study demonstrated a functional linkage between antibiotic treatment, the microbial and metabolic milieu and their interaction with the immune system as factors driving immune response towards influenza in a specific immunisation setting.30 This suggests that also in the context of anti-TNF therapy, the intestinal bacterial composition can potentially be manipulated by antibiotics, or faecal transplantation to produce favourable outcomes with respect to immunogenicity and prevention of LOR. Here, we aimed to assess the possible implications of antibiotic treatment on immunogenicity to anti-TNF agents in patients with IBD.
Methods
Cohort analysis
Settings, study population and data
We used data from the epidemiology group of the Israeli IBD research nucleus (epi-IIRN), a validated registry that records all patients with IBD in Israel since 2000–2002. We included data from three of the four health maintenance organisations (HMO), covering 89% of the Israeli population. Patient identification, database curation, available data and data identification and extraction were previously described.31 The patient identification algorithm uses a combination of IBD-related International Classification of Diseases diagnoses codes separately or combined with purchases of IBD-related medications (at least three purchases or at least a 3-month interval from first to last purchase). The algorithm accurately identified and classified patients with IBD from the HMO electronic medical records (sensitivity 89%, specificity 99%, positive predictive value (PPV) 92%, negative predictive value (NPV) 99% for IBD diagnosis and, sensitivity 92%, specificity 97%, PPV 97%, NPV 92% for IBD classification).31 The follow-up period was between 2005, which was the previously validated cut-off year for incidence determination,31 up to 1 January 2019, death or immigration.
We included all patients with IBD who were treated with either infliximab and/or adalimumab who had available ADA levels during the treatment period. In patients who were treated with both infliximab and adalimumab, the first anti-TNF treatment with available ADA levels was selected. Follow-up period started 3 years prior to the first anti-TNF dispensation, up to positive ADA level measurement, or last negative ADA level measurement available.
We analysed demographic details, IBD type and disease duration, laboratory results, previous IBD-related surgeries, hospitalisations with IBD-related diagnoses and additional IBD treatments including 5-aminosalicylic acid (5-ASA) agents, corticosteroids and immunomodulators (table 1). We defined medication use as number and dates of dispensations extracted from HMO databases. Medication data were perceived accurate since medications in Israel are provided almost for free via the HMOs.
Comparison of baseline variables between patients with or without registered dispensations of antibiotics in the year prior to anti-TNF initiation
Exposure and outcome
The six most frequently prescribed antibiotic groups were selected for analysis (online supplemental table 1). Drug dispensations during the pre-defined time periods before first anti-TNF dispensation and up to the last measurement of ADA levels during therapy were summarised. For the survival analysis, at each time point during follow-up medication exposure was assessed for the 3 years prior to the time point.
Supplemental material
The primary outcome was defined as positive serum ADA during the treatment period. Notably, ADA level measurements were performed by several methods, varying with medical insurer, laboratory and time period and were extracted as numeric values. Depending on reference values for each test, numeric values were therefore translated to either ‘low’ or ‘high’ with the latter considered as ADA positive in outcome analysis. The study design is graphically demonstrated in online supplemental figure 1.
Supplemental material
Animal studies
To evaluate the causative effect of antibiotic treatment and the associated gut microbiome dysbiosis on ADA formation, mice were treated with antibiotics and challenged with infliximab. Mice raised in a specific pathogen-free environment (C57BL/6J, female, age 7–8 weeks) were divided into three groups with 25 mice in each group. Two groups received antibiotics—cefuroxime (GSK, Barnard Castle, UK) 0.176 mg/g body weight, or azithromycin (Pfizer, Foster City, USA) 0.088 mg/g body weight in the drinking water, and the third was untreated and served as control. Antibiotic dosages were calculated based on human treatment recommendations adjusted to mouse body weight. A parallel control group consisted of C57BL germ-free (GF) mice (n=5). Mice exclusion criteria were, loss of more than 20% of body weight, or improper infliximab administration, verified by serum drug level determination. Five mice were excluded from the cefuroxime treated group and four from the azithromycin treated group.
Mice were subjected to 2 weeks of antibiotic treatment via the drinking water. Thereafter, all mice were challenged with subcutaneous infliximab at 30.75 µg/g body weight equivalent to 2.5 mg/kg in humans after conversion according to the Food and Drug Administration recommendations,32 based on previously studied dosages, which demonstrated a measurable and scalable mouse antibody response.15 Mice were exposed to infliximab by subcutaneous injection after demonstrating a similar, yet more homogeneous response, as compared with intraperitoneal exposure (data not shown). Following 2 weeks, serum samples were collected and ADA levels were determined using a mouse adapted anti-lambda chain ELISA.33 All animal trials were conducted at the Pre-Clinical Research Authority at the Ruth and Bruce Rappaport Faculty of Medicine, Technion—Israel Institute of Technology. Mice were housed in ventilated cages containing five mice each (20°C–23°C, 12 light-hours a day) and fed autoclaved food and sterilised acidic water (pH=3.2±0.2) ad libitum. Mice were given at least 1 week of acclimatisation prior to the experiments. Animal studies were approved by the Technion—Israel Institute of Technology and the Israeli Ministry of Health (Pre-clinical research approval IL-077-06-2020).
Statistical analysis
Analyses were performed using R V.4.0.0 (R foundation for statistical computing). Crude comparison of baseline variables between patients with prior dispensation of any antibiotic in the 3 years prior to anti-TNF initiation and no antibiotic use was performed using Mann-Whitney U test for continuous and ordinal variables, and χ2 test for categorical variables. Medians and IQRs were presented for continuous variables and numbers with percentages for categorical variables. Only variables that were available for at least 75% of patients and were positive in at least 5% of the patient population, respectively, were included for analysis. Among the variables that were included for multivariable analysis (as listed in online supplemental table 1) only serum C reactive protein (CRP) and albumin were not fully available for all patients, in 19.6% and 5.7% of records, respectively. To avoid loss of data, we imputed these records using median values.
We performed univariate survival analysis using the Kaplan-Meier method and tested the association between the use of each antibiotic class during the 3 years prior to investigated anti-TNF initiation and ADA formation using a log-rank statistic. We defined the analysis origin as the time of initiation of anti-TNF and end of follow-up was defined as either first date with positive ADAs or last available negative ADAs measurement. Using the same time origins and endpoints, we performed a multivariable Cox proportional hazards model with a time varying definition for concomitant antibiotic use of each class. Based on prior knowledge and availability of data, we included all available covariates with clinical significance for ADA formation (online supplemental table 1).10 12 14 21 Similar to antibiotic use, concomitant immunomodulatory and corticosteroid use and IBD-related hospitalisations were incorporated as time varying covariates. We calculated Schoenfeld residuals to confirm the proportionality assumption.
To study whether a dose-response relationship exists between antibiotic use and ADA development, we performed a similar multivariable Cox proportional hazards model with antibiotic classes incorporated as continuous variables defined as total number of drug dispensations for the specified time period. We then plotted the regression coefficient estimates for each of the antibiotic classes that were significantly associated with ADA development as dichotomous variables as a function of number of registered drug dispensations. We used generalised additive models with cubic splines to model the non-linear time-varying effect of dispensations of each antibiotic class on ADA formation risk.
To evaluate possible synergistic or antagonising effects of antibiotic combinations, we first selected the antibiotic classes for which a substantial and significant association was observed to ADA development. For each pair from the selected combination, we evaluated Kaplan-Meier estimates and plots tested by a log-rank statistic for the association between the use of either of the antibiotics from the pair, both or none within the 3 years before anti-TNF initiation with ADA development. We also performed a multivariable Cox proportional hazards model with antibiotic classes as described previously with the addition of interaction terms of all possible pairs of the selected antibiotics.
A sensitivity analyses with a 1-year time frame considered for each antibiotic class was performed as well. To assess whether imputation affected the result, we performed a Cox proportional hazards model, with a 3-year time frame, but without CRP and albumin, and an additional analysis that only included patients who had complete data available for all covariates.
A concern for selection bias arose due to the exclusion of patients without available ADA levels. We assessed the extent of this possible bias by a comparison of patients included in our analysis with excluded patients. For the comparison, in the latter group we included only patients that received anti-TNF for at least 14 weeks to avoid analysis of primary non-responders. Additionally, since the two groups substantially varied in the year of initiation of anti-TNF therapy, which is reflected in treatment and management protocols, including considerations of therapeutic drug monitoring, we performed frequency matching for treatment year with a ratio of 1:2. Thus, for each distinct year of treatment initiation in which n patients had available ADA levels, a random sample of 2n patients with the same year of treatment initiation was added to the excluded group for comparison.
In the animal studies, ADA measurements below detection level were substituted for values of one over the square root of two times the detection limit (measurements under 937.5 ng/mL, the detection limit, were substituted with 663 ng/mL). The validity of the substitution was assessed using rules suggested by Helsel.34 Differences in ADA levels between mouse groups were compared using Kruskal-Wallis and Dunn’s test. The p value of the post hoc analysis was adjusted for multiple comparisons using the Benjamini-Hochberg method.
Results
Of the 46 303 patients with IBD recorded in the epi-IIRN registry, 1946 were ever treated with infliximab or adalimumab and had available ADA levels during the treatment (54.7% adalimumab and 45.3% infliximab). Overall, positive ADAs were measured in 363 patients (18.6%). Median follow-up time from anti-TNF treatment was 651 (IQR 1175) days.
Most baseline factors including age, gender, body mass index, IBD subclass, surgery registries or hospitalisations prior to anti-TNF initiation, type of anti-TNF analysed, concomitant use of immunomodulators and various laboratory values were comparable between patients with or without antibiotic use in the 3 years prior to anti-TNF initiation (table 1). Most antibiotic prescriptions were for approximately 1 week. Notably, patients who had registered dispensations of antibiotics prior to anti-TNF initiation had longer intervals to their first and last antibody measurements. This variation was consistent across all antibiotic classes and could be explained by a higher probability of any intervention with longer follow-up periods (online supplemental table 2). Past anti-TNF therapy with a different agent was more prevalent in patients with antibiotic dispensations prior to anti-TNF initiation although drug monitoring results were not available for these patients during that time period (table 1).
An increased hazard of ADA development was noted in patients who used cephalosporins or penicillins with β-lactamase inhibitors (penicillin-BLI) and reduced risk of ADA formation with use of fluoroquinolones, metronidazole and macrolides, with early risk divergence for most classes (all p<0.05 vs non-treated group, by log-rank test) (figure 1). Multivariable Cox proportional hazards model adjusted for time-fixed and time varying factors demonstrated that commonly prescribed antibiotic classes are significantly and differentially associated with the risk of ADA formation which were overall in agreement with the univariate analysis results (table 2 for primary and secondary variable effects and, online supplemental table 1 for assessment of the Schoenfeld residuals, figure 2 for primary exposure variables). Cephalosporin, or penicillin-BLI use before or during anti-TNF treatment was associated with ADA formation (HR 1.96; 95% CI 1.58 to 2.43 and HR 1.38; 95% CI 1.11 to 1.71, respectively). In contrast, fluoroquinolone or macrolide use reduced the risk of ADA formation (HR 0.20; 95% CI 0.11 to 0.33 and HR 0.38; 95% CI 0.17 to 0.86, respectively).

Kaplan-Meier curves of cumulative risk of ADA development for prior use of different antibiotic classes. Tick marks represent censoring and shaded area represent 95% CI. Plot is limited to first 2000 days of follow-up. A p value for the log-rank test is presented in each plot. ADA, anti-drug antibodies; BLI, β-lactamase inhibitors.

Multivariable-adjusted HRs (represented by blue points) for anti-drug antibodies development for use of various antibiotic classes during anti-tumour necrosis factor therapy. HRs are presented on a log10 scale. Black lines represent 95% CIs. BLI, β-lactamase inhibitors.
Multivariable adjusted HRs for ADA development during anti-TNF therapy
A similar analysis with antibiotic use incorporated as continuous time dependent variables defined as total dispensations demonstrated a similar trend whereby total macrolide use seemed to reduce risk, but this analysis did not reach statistical significance (HR 0.63; 95% CI 0.38 to 1.06 for each additional dispensation) (table 2). When modelling the effect of number of dispensations for each class, we observed a positive increasing association between increasing number of dispensations of cephalosporins and penicillin-BLIs and ADA development risk and an inverse association mostly with increasing number of dispensations of fluoroquinolones (figure 3).
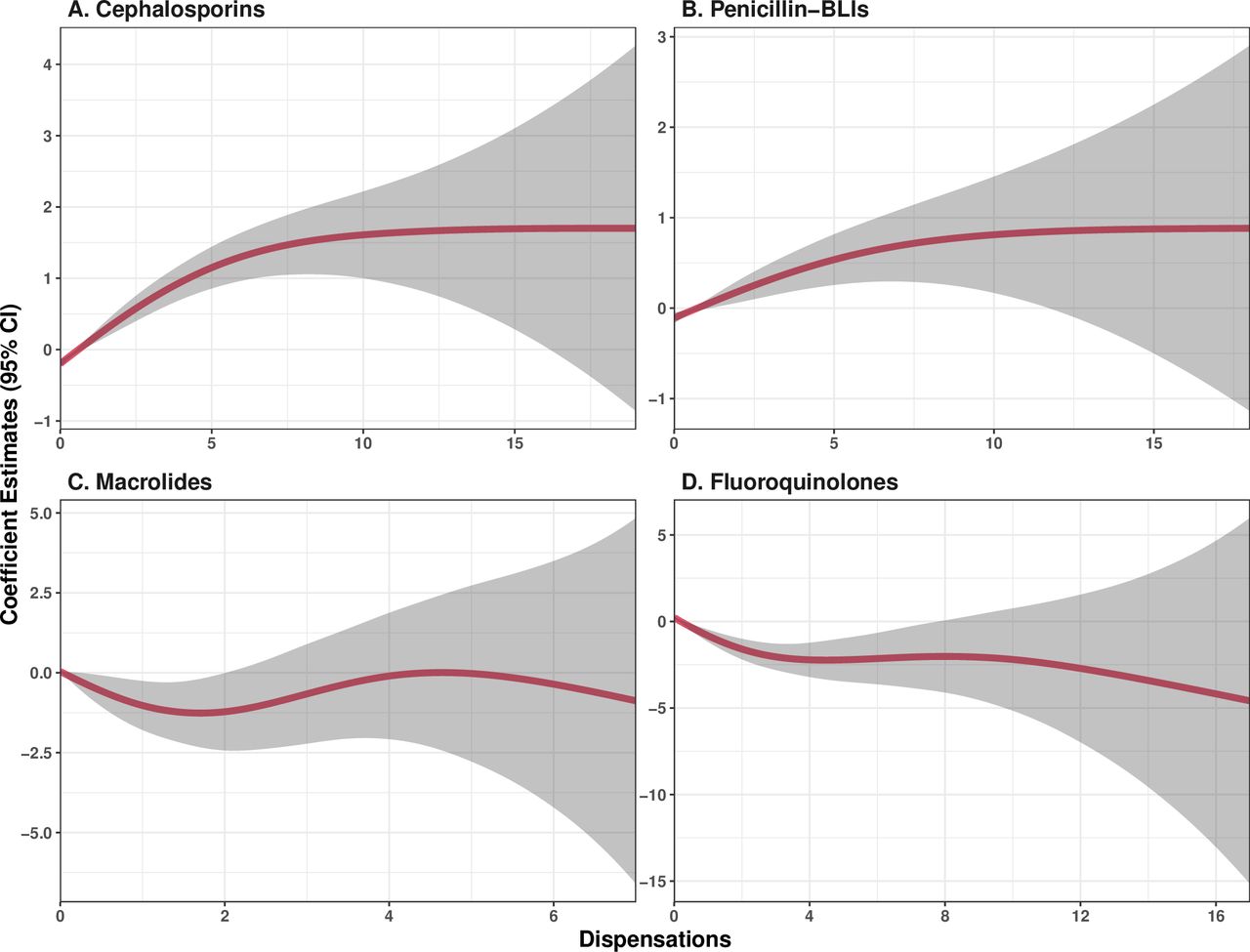
Estimated adjusted regression coefficients for a range of number of dispensations for cephalosporins (A); penicillin-BLIs (B); macrolides (C); and fluoroquinolones (D). Shaded areas represent 95% CIs. BLIs, β-lactamase inhibitors.
Patients who used both cephalosporins and penicillin-BLIs had higher rates of ADA development compared with patients who used either alone (figure 4). Although a very small group of patients used both fluoroquinolones and macrolides, none developed ADA during their follow-up period (figure 4). Patients who were treated with both pro and anti-immunogenic, demonstrated a mixed effect with immunogenicity rates similar to controls. In a multivariable analysis with multiple interaction terms only the interaction between cephalosporins and penicillin-BLIs were significant with an HR of 1.56 (95% CI 1.01 to 2.42) suggesting some synergistic effect of these classes on immunogenicity (online supplemental table 3).

Kaplan-Meier curves with risk tables of cumulative risk of ADA development for prior use of combinations of pairs from cephalosporins, penicillin-BLIs, macrolides and fluoroquinolones. Tick marks represent censoring and shaded areas represent the 95% CI. The plot is limited to the first 2000 days of follow-up. A p value for the log-rank test is presented in each plot. ADA, anti-drug antibodies; BLI, β-lactamase inhibitors.
Multivariable analysis with alternate definitions of antibiotic use revealed qualitatively similar results (online supplemental table 4). The most noteworthy difference was loss of significance of the effect of macrolide use on ADA formation, probably due to the smaller sample size in this analysis. Similar effect sizes were revealed by additional analyses that assessed the possible influence of data imputation (online supplemental table 5).
A comparison between patients included in the analysis, and a frequency matched group on year of treatment initiation of patients without available ADA levels in the epi-IIRN database, revealed differences, mainly in adalimumab and thiopurine use (online supplemental table 6).
Mouse model study
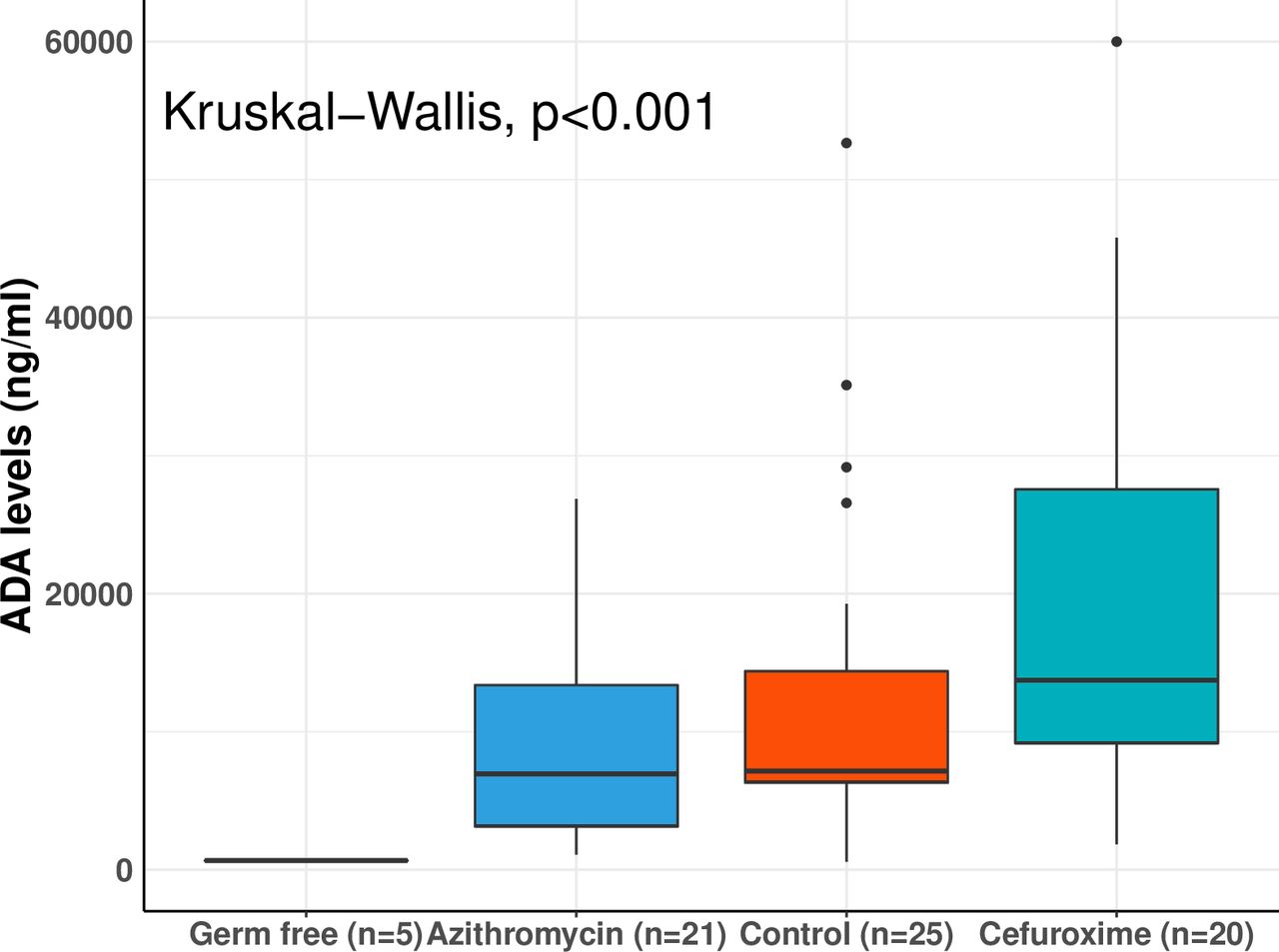
To test whether the human observations were merely associated with ADA production, or whether antibiotics were causative and whether the effect was driven by antibiotic-induced dysbiosis or chemical effect by the drug, we exposed antibiotic-treated and GF mice to infliximab. ADA levels were determined in 71 mice 2 weeks following infliximab injection. Mouse groups consisted of 25 controls with no pretreatment, 21 mice pretreated with azithromycin, 20 mice pretreated with cefuroxime and 5 GF mice. Significant differences in ADA levels were observed between groups (p<0.001 by Kruskal-Wallis) (figure 5). Consistent with the human observations, a trend for higher ADA levels in cefuroxime pretreated mice and lower ADA in azithromycin pretreated mice as compared with the control group, and significant differences in median ADA levels between cefuroxime and azithromycin pretreated mice were noted (13 732 ng/mL vs 6948 ng/mL, respectively, adjusted p=0.04; figure 5, and online supplemental table 7), suggesting a direct causative effect of the antibiotics in agreement with the human effects. GF mice produced no detectable antibodies, indicating the importance of the intestinal flora for antibody production and suggesting that the observed antibiotic effects were at least in part mediated through their effects on the intestinal flora (figure 5 and online supplemental table 7).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mean anti-drug antibodies levels in mice treated with anti-tumour necrosis factor and prior cefuroxime (n=20), azithromycin (n=21) or no antibiotic (regular control, n=25, or germ-free, n=5). ADA, anti-drug antibodies.
Discussion
Here we report an effect of antibiotic therapy on the risk of anti-TNF ADA formation in patients with IBD, during, or prior treatment. An increased risk was noted in patients treated with cephalosporins or penicillin-BLIs. In contrast, fluoroquinolone or macrolide use was associated with reduced immunogenicity in a dose-dependent manner further supporting the validity of the associations. Moreover, drug combination analysis pointed to a possible synergism for immunogenicity risk with both cephalosporins and penicillin-BLIs. Mouse experiments supported the human population-based analysis and suggested that the effect is causal and mediated by the microbiome.
This is the first large scale study that extensively evaluated the effect of different antibiotic classes on immunogenicity of anti-TNF therapy. In support of the findings, the association of antibiotics with immunogenicity was recently suggested in a study performed by the European consortium ABIRISK. The study showed that antibiotic use during therapy reduced the risk of ADA formation after multivariable adjustment.35 However, in the ABIRISK study, antibiotic groups were not differentiated and substantial heterogeneity of patients and types of treatments limited the interpretation of the finding.
Although the nature of infliximab immunogenicity in mice and humans may differ, the parallel antibiotic effect suggests similar immune mechanisms. Combined with the long-term effect of therapy, where patients were exposed to antibiotics long before anti-TNF treatment and the mixed effects of sequential treatments, the most likely explanation for the results would be an effect of treatment on the microbiome. Furthermore, in agreement with the results in our murine model, Ruiz et al 36, demonstrated that macrolide treatment in GF mice did not alter the effect of the GF status itself as assessed by ileal gene expression suggesting the effect was mediated through the microbiome.
The association we observed between the immunogenicity enhancing effect of cephalosporins and penicillin-BLIs, with possible synergism between classes, can also be explained by specific alterations of the microbiome. Previous studies evaluated the role of the microbiome as a biomarker for prediction of response to anti-TNF therapy.29 Several, which profiled the microbiota of patients with IBD prior to and during anti-TNF treatment observed a higher baseline abundance of the Clostridiales order in anti-TNF responders.27 37 38 A large systematic review that summarised the effect of multiple antimicrobial agents on the composition of the intestinal microbiota concluded that cephalosporins and penicillin-BLIs mostly caused a decrease in abundance of Clostridium species,39 which might suggest that the effect of cephalosporins and penicillin-BLIs seen in our analysis could be explained by the specific dysbiosis caused by these agents supporting ADA formation and its ramifications on response to anti-TNF therapy.
The association we found between macrolides and reduced immunogenicity concurs with the reduction in inflammatory activity seen with macrolide therapy.40 The use of a synthetic non-antibiotic macrolide has been shown to reduce intestinal inflammatory activity in mice with induced colitis.41 Additionally, pretreatment with azithromycin resulted in reduced antibodies to pneumococcal vaccine in mice.42 Anti-inflammatory properties of fluoroquinolones with suppression of TNFα levels were also demonstrated.43
An additional observation was the long-term effect of antibiotic treatment extending up to 3 years post treatment. In support of such possibility, a previous study performed in mice demonstrated a prolonged effect of macrolides in pups which received the treatment through their nursing dams.36 In that study, a single treatment course induced prolonged disruption of microbial network and ileal immune milieu and was associated with reduced secretory IgA production.
Our results also suggest the reversibility of the antibiotic effect. Patients treated with both ADA stimulating and ADA suppressing antibiotics responded similarly to controls. This observation may conceivably result from effects of treatment on bacterial metabolism, or balance between bacterial populations enhancing or supporting ADA formation and should be further investigated.
The data suggest that fluoroquinolones and macrolides could possibly be used to reduce immunogenicity to biological therapy without risks associated with immunosuppressive therapy. The current study suggests that specific microbial manipulation may serve as a tool to modify immunogenicity which is preferably turned on for protective immunisations and off for biological therapy.
The retrospective nature of the analysis is a potential drawback. Therapeutic drug monitoring (TDM) was inconsistent in our cohort, and we did not have information regarding the indication for TDM performance. A selection bias might have occurred from the analysis of only patients with available ADA levels. Factors that underlie the referral for therapeutic drug monitoring might be associated with the risk of ADA development and antibiotic treatment. These concerns were addressed and reduced by several measures. Primarily, various antibiotic classes, our main analysed exposures, are used mainly for non-IBD related indications, less often for IBD-related complications, yet mostly not to address biological treatment failure. Factors that might underlie decisions of ADA level measurement or the measurement site are not expected to affect antibiotic class selection and, most importantly its effect on immunogenicity. HMO based laboratory test locations are spread geographically across Israel and the site of ADA levels measurement is usually selected according to the patient and physician familiarity and convenience. Therefore, we believe that our cohort represents a random sample of patients that undergo TDM. The quantitative assessment of a possible selection bias revealed that while baseline variables were overall comparable between groups, a notable difference was observed in thiopurine use. This difference could be explained by increased awareness of the physician to immunogenicity which coincides with referral for TDM, or by an unstable disease course. However, this difference was relatively modest, and all effects were adjusted for thiopurine use.
Antibiotics are usually taken in the same day or within a few days from dispensation date, a period which is negligible by comparison to the duration of follow-up of patients in our cohort. Hence the possibility of an immortal time bias due to meaningful misclassification of the exposures is substantially diminished.
We noted a substantial variation in first and last antibody measurement times between patients with and without antibiotic dispensations of all analysed classes. As these differences were consistent across all antibiotic classes, the possibility of a differential bias is reduced. Antibiotics that were administered in hospitals were not available in our registry. Nevertheless, hospitalisations with an IBD-related diagnosis were incorporated as a covariate in the multivariable survival analysis and did not disclose a significant association with the outcome. Additionally, no particular indication for prescription of a specific antibiotic is expected to induce a bias. Importantly, the indication for antibiotic use may differ from the effect on immunogenicity. For example, perforating complications and perianal sepsis are commonly treated with either penicillin-BLIs or ciprofloxacin/metronidazole. These treatments have a similar effect on disease pathogenesis yet had opposite effects on immunogenicity. Another major limitation is the inability to adjust exposure to antibiotics to type and severity of the infection for which they were prescribed which may be a substantial confounder for ADA development. Yet, the antibiotic groups that were found to be significantly associated with immunogenicity are indicated and prescribed for a diverse range of infections. The considerable effects on immunogenicity were demonstrated in a time fixed and time dependent manner of antibiotic use and with several alternative definitions of antibiotic exposure.
Further studies involving detailed analysis of the antibiotic effects on the human microbiome and immune milieu are needed, as well as comparative experiments with other medications used to reduce immunogenicity.
Data availability statement
Data are available upon reasonable request. The data used in the study was obtained from the epi-IIRN registry.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by an institutional review board (0134–17-SZMC).
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @yiskaw
YG and SF contributed equally.
Correction notice This article has been corrected since it published Online First. The order of authors have been corrected.
Contributors YG and SF contributed equally to this work. YC, YK, YG and SF conceived and designed the study. YG, CF and GF processed and analysed the data. SF, SG-V, AB, SP and NG-Z performed animal data acquisition and analysis. YC provided data interpretation. YC, YG and SF drafted and revised the manuscript with input from all authors. SG-V, YLW, RK, ID, NG-Z and SSS-O critically reviewed the manuscript and revision. CF, GF, YLW, SG, RK, NL, ID and YC were involved in the data collection process for the epi-IIRN registry.
Funding This work was partially supported by the Leona M. and Harry B. Helmsley Charitable Trust (grant number G-2018PG-CD009). This work was partially supported by a grant from the Israeli Ministry of Science and Technology (MOST, grant number 3-15520).
Competing interests YC received research grants, speaker and advisory fees from AbbVie; speaker and advisory fees from Janssen; grant, speaker and advisory fees from Takeda and consultancy fees from CytoReason. SSO received grant funding from Takeda, holds equity and receives consultancy fees from CytoReason. SG-V declares CytoReason advisory fees for last 3 years. RK received consultation fee, research grant, royalties or honorarium from Takeda and Pfizer. ID received consultation fee, research grant or honorarium from Janssen, AbbVie, Takeda, Pfizer, Roche/Genentech, Celgene/BMS, Arena, Neopharm, Gilead, Gallapagos, Celltrion, Ferring, Falk Pharma, MSD, DSM, Cambridge Healthcare, Sublimity, Sangamo, Nestle, Wild bio, Food Industries Association, Integran Holdings, Abbott, Altman Research
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.