Article Text

Abstract
Objective An international meeting was organised to develop consensus on (1) the landmarks to define the gastro-oesophageal junction (GOJ), (2) the occurrence and pathophysiological significance of the cardiac gland, (3) the definition of the gastro-oesophageal junctional zone (GOJZ) and (4) the causes of inflammation, metaplasia and neoplasia occurring in the GOJZ.
Design Clinical questions relevant to the afore-mentioned major issues were drafted for which expert panels formulated relevant statements and textural explanations.
A Delphi method using an anonymous system was employed to develop the consensus, the level of which was predefined as ≥80% of agreement. Two rounds of voting and amendments were completed before the meeting at which clinical questions and consensus were finalised.
Results Twenty eight clinical questions and statements were finalised after extensive amendments. Critical consensus was achieved: (1) definition for the GOJ, (2) definition of the GOJZ spanning 1 cm proximal and distal to the GOJ as defined by the end of palisade vessels was accepted based on the anatomical distribution of cardiac type gland, (3) chemical and bacterial (Helicobacter pylori) factors as the primary causes of inflammation, metaplasia and neoplasia occurring in the GOJZ, (4) a new definition of Barrett’s oesophagus (BO).
Conclusions This international consensus on the new definitions of BO, GOJ and the GOJZ will be instrumental in future studies aiming to resolve many issues on this important anatomic area and hopefully will lead to better classification and management of the diseases surrounding the GOJ.
- HELICOBACTER PYLORI
- BARRETT'S CARCINOMA
- BARRETT'S OESOPHAGUS
- GASTROESOPHAGEAL REFLUX DISEASE
- GASTRO-OESPHAGEAL JUNCTION
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- HELICOBACTER PYLORI
- BARRETT'S CARCINOMA
- BARRETT'S OESOPHAGUS
- GASTROESOPHAGEAL REFLUX DISEASE
- GASTRO-OESPHAGEAL JUNCTION
Summary box
What is already known about this subject?
Definitions of Barrett’s oesophagus (BO) among guidelines are inconsistent in terms of the minimum length of metaplastic mucosa and of the requirement of intestinal metaplasia (IM, often called specialised columnar metaplasia or specialised IM).
The endoscopic landmarks for identifying gastro-oesophageal junction (GOJ) adopted in these guidelines are discordant, the proximal end of gastric folds (PEGF) on the one hand, the distal end of palisade vessels (DEPV) on the other.
Presence and nature of the cardia type mucosa have been debated.
Classification of cancers arising in the GOJ are ill-defined or confusing.
What are the new findings?
A new definition of BO, which does not require the length criteria nor IM, is proposed.
Preferred use of DEPV as an endoscopic landmark of GOJ is agreed.
Existence of the cardia type columnar mucosa without parietal cells as an innate structure in the limited extent of the GOJ (usually several millimetre of length) is agreed.
A new concept of gastro-oesophageal zone (GOJZ), defined as an area straddling 1 cm proximal and 1 cm distal to the GOJ, is proposed for practical purposes.
Cancers arising in the GOJZ as defined above is proposed as a substitute of the Siewert’s type II cancer in the junctional zone.
How might it impact on clinical practice in the foreseeable future?
Adoption of new definition of BO will help resolving the inconsistencies among the reported results and provide a new platform for future studies.
Use of unified endoscopic landmark (DEPV) observed under proper methodology will reduce the diagnostic inconsistencies of the short (including ultra-short) segment BO.
Limited distribution of the cardia-type epithelium calls for a revamp of the current category of ‘cardia cancer’ or ‘cancer in the cardia’.
Adoption of GOJZ cancer concept will better serve to elucidate the aetiology of cancers arising from this area and to improve the classification for health statistics.
Introduction
In the previous consensus conference held in Kyoto, we have reached a consensus to classify gastritis based on aetiology, Helicobacter pylori-associated dyspepsia, methodologies to evaluate gastritis, and, most importantly, to prevent gastric cancer by prescribing eradication of H. pylori.1 However, the important issue of ‘carditis’ was left untouched, as it requires full discussions on the definition of cardia as well as the definition of gastro-oesophageal junction (GOJ), which is closely linked the definition of Barrett’s oesophagus (BO). Indeed, there are a number of differences in the definition of BO among guidelines published by professional societies2–7 (table 1). To resolve these issues, extensive discussions between specialists with different backgrounds (gastroenterology, pathology and surgery) having expertise on BO and gastric diseases are mandatory. We had a chance to organise the second international consensus meeting dedicated to these issues that have been left in a state of confusion for a long time thanks to financial support from the fund of the Asia Pacific Digestive Week (APDW) held in Kobe in 2016 deposited to the Organisation of Japan Digestive Disease Week (JDDW).
Different definitions of Barrett’s oesophagus
After formulation of the draft for clinical questions (CQ) and statements concerning the issues on GOJ which were amended through two rounds of voting by the faculty members, the draft CQs and statements were further discussed and finalised at the face-to-face meeting again in Kyoto. Fortunately, we could reach consensus on all the important issues including a new conceptual definition of BO, a desirable anatomical landmark for GOJ, a definition of ‘cardiac mucosa’, a new proposal for the gastro-oesophageal junctional zone (GOJZ) concept and unique pathophysiological factors affecting GOJZ, all of which, we hope, will form the basis for future research and thereby improve our understanding, classification and management of the diseases occurring in the area of GOJ.
Method
Consensus development process
Draft plan for CQs and statements were developed by the Japanese faculty members who are experts in the relevant topics. International faculty members were selected from the faculty members who had contributed to international guidelines and from renowned pathologists with extensive publications on the topics. The first drafts of CQs and statements edited and revised by core faculty members (KS, KM, EME-O and PM) were sent to each faculty members who agreed to participate via the internet voting. This internet-based platform to develop consensus based on the Delphi method allowed the faculty members to anonymously choose their level of agreement for each set of CQ and statement. Faculty members were entitled to vote on all set of CQs and statements from the first round of voting. The voting platform was designed for the voters to make any comments and provide references, irrespective of their levels of agreement with the statements. However, when they disagree with the CQs and/or statements, they were obliged to specify their reasons for the objecting. Consensus level was predefined as ≥80% voting either agree (A) or agree with minor reservation (B). The first round of voting involved 27 CQs and statements. Among the 38 faculty members, 37 completed voting. Although all the CQs and statements cleared the consensus threshold of 80% of agreement (A+B), a considerable number of amendments were implemented to omit the redundant CQs and to provide a more logically consistent orders of CQs, based on comments provided by faculty members before the second round of voting. Textural explanations and references attached to support each statement were also revised. For the second round of voting, 23 set of CQs and statements were uploaded to the voting platform, and all the faculty members have completed the voting. Again consensus level was achieved for all the CQs and statements. Further revisions of wording, though minor, were made and presented at the face-to-face meeting.
At the face-to-face meeting, faculty members were asked to vote the evidence level and recommendation to the statements according to the predefined category based on the Grade system,8 9 which rates the quality of evidence into four tiers (high to very low) and the strength of recommendation into three levels (strong, weak and not applicable) (online supplemental table 1A,B).
Supplemental material
Each CQ, statement and supporting evidence was presented by the Japanese faculty member assigned to prepare them, followed by a question and discussion session. Voting at the meeting was accomplished with a key-pad system distributed to faculty members to ensure anonymity, and the polling results were shown on the screen immediately after voting.
One ad-hoc CQ concerning the definition of BO was proposed at the face-to-face meeting in order to facilitate discussions on the entire group of CQs and statements. Although it did not go through the two rounds of internet voting process, adoption of this CQ (initially designated as CQ zero, but renumbered as CQ 1 in this report) was approved and a statement to accompany this CQ was formulated through discussion. Faculty members attending to the meeting were asked to vote to this ad hoc CQ in the same manner as the other CQs, and the wording was modified until the level of agreement was reached. Therefore, this particular CQ did not reflect the opinions of several faculty members who could not attend the meeting. The textual explanation for CQ 1 was prepared by KS and SJS.
Role of the funding sources
This consensus conference was fully supported by a fund from the APDW meeting held in Kobe 2016, which was deposited to the Organisation of JDDW. The funding source also provide assistance in preparatory works, but had no roles in the planning, formulation of CQ, literature search, writing the manuscript, nor decision to submit for publication.
Results
CQ 1
How can we define BO conceptually?
Statement 1
BO is the condition in which a metaplastic columnar mucosa predisposed to neoplasia replaces the squamous mucosa of the distal oesophagus.
Agreement
Strongly agree 97%.
Agree with minor reservation 3%.
Disagree with major reservation 0%.
Strongly disagree 0%.
Quality of evidence
High 72%.
Moderate 28%.
Low 0%.
Very low 0%.
Strength of recommendation
Strong 90%.
Weak 10%.
Not applicable 0%.
Textural explanation
As stated in the Introduction section, diagnostic criteria for BO among international guidelines are discrepant2–7 regarding two major points: the length of metaplastic mucosa required and the requirement for the presence of intestinal metaplasia (IM), previously often denoted as specialised columnar epithelium (SCE) or specialised IM, (SIM) (table 1). As for the length of columnar metaplasia, guidelines by the American Gastroenterological Association (AGA) and the Japan Esophageal Society accept any length of metaplastic change, while other societies require a minimum length of 1 cm of metaplastic mucosa for a diagnosis of BO. One major reason for setting this minimum length threshold presumably is rooted in the reports showing unreliability in identifying columnar metaplasia extending less than 1 cm.10 11 However, even in the cases with longer segments of oesophageal columnar metaplasia, length measurements are imprecise,12 13 raising doubt regarding the reliability of any length requirement. Moreover, the GOJ landmark used to measure the length of oesophageal metaplasia that is advocated in most guidelines, that is, the proximal end of gastric folds (PEGF), also is imprecise (eg, its location varies with respiration and extent of insufflation), making measurements of the length of metaplastic mucosa inaccurate and unreliable (see CQ 2 and 3 for more detailed explanation).
Although a number of reports have shown that the risk of oesophageal adenocarcinoma (OAC) increases with the extent of Barrett’s metaplastic mucosa,14–17 it is important to consider several factors that can confound the interpretation of endoscopic and histologic findings in BO. First, a relative large number of biopsy samples (minimum of eight) is required to demonstrate IM reliably,18 and community endoscopists often do not take so many biopsies in routine clinical practice. Indeed, one study documented poor reproducibility in the finding of IM between two endoscopic examinations performed only 6 weeks apart, even when a fairly large number of biopsy samples were taken (mean 13.6 for the first endoscopy and 11.4 for the second endoscopy) conducted in a short interval (6 weeks).19 Therefore, a substantial proportion of metaplastic oesophageal epithelium containing IM would be missed, and hence cannot be diagnosed as BO. Second, ‘pseudogoblet cells’ are mucinous, gastric foveolar-type columnar cells that have distended cytoplasmic vacuoles that give them a histologic appearance close to goblet cells. Biopsies containing pseudogoblet cells can easily be misinterpreted as IM,20 which has been surmised as a clonal event involving multiple cell lineages.21–23 Third, in biopsies of the GOJ region, it can be difficult to distinguish IM involving the stomach (an atrophic condition frequently caused by chronic H. pylori infection) from IM in the metaplastic oesophageal mucosa, since gastric and oesophageal IM can appear identical even when immunohistochemical staining or with gene expression analyses are employed.24 25 Moreover, IM at the GOJ can exhibit proliferative abnormalities similar to those found in the IM of long-segment BO,26 implying an increased risk for neoplastic changes. Fourth, a longitudinal follow-up study found that a substantial proportion of patients with IM on an initial endoscopy did not have positive IM in a follow-up procedure and, conversely, those without IM at the first endoscopy often had IM found in the follow-up.27 Finally, a number of emerging studies have shown that metaplastic columnar epithelium without IM can have genetic alterations that might predispose to cancer development.28–30 Indeed, several reports have contended that adenocarcinomas can develop in columnar epithelium without IM31–36 (see CQ 21 for more detailed explanation). Collectively, these problems raise a serious concern regarding the validity of the requirement for IM and the minimum length definition of 1 cm as diagnostic criteria for BO. Thus, in this consensus conference, the new definition of BO was created in which both length limitation and the presence of IM were lifted from the definition of BO.
To circumvent the above problems, we feel it is useful to separate a conceptual definition of BO from its diagnostic criteria. As noted above, there can be considerable disagreement among authorities regarding diagnostic criteria requirements, there are limitations in endoscopic and histologic techniques for identifying those criteria, and diagnostic criteria might change with future studies regarding their importance. However, the conceptual definition of BO as the condition in which a metaplastic columnar mucosa predisposed to neoplasia replaces the squamous mucosa of the distal oesophagus need not change. It should be noted that this new concept of BO does not imply that all the BO in this category should undergo surveillance. On the contrary, we do not recommend endoscopic surveillance of ultrashort segment BO (USSBO) with less than 1 cm of columnar metaplasia since an overall risk of developing OAC is very low despite that it has an increased risk per unit area comparable to short segment BO (SSBO) with 1–3 cm of columnar metaplasia (SSBO).37
CQ 2
Which of the two, the distal end of the palisade vessels (DEPV) or the PEGF, is more appropriate anatomical landmark of the GOJ?
Statement 2
Anatomically, the DEPV is more appropriate than the PEGF for defining the GOJ.
Agreement
Strongly agree 71%.
Agree with minor reservation 11%.
Disagree with major reservation 14%.
Strongly disagree 4%.
Quality of evidence
High 36%.
Moderate 39%.
Low 4%.
Very low 21%.
Strength of recommendation
Strong 57%.
Weak 36%.
Not applicable 7%.
Textural explanation
Several landmarks have been used to define the GOJ such as the squamocolumnar junction (SCJ), the PEGF and the DEPV38 (figure 1A, IB). As the SCJ shifts towards proximally when there is columnar metaplasia of the oesophagus39 40 or in rare cases, the SCJ shifts distally into the stomach,41 it cannot be used as an anatomical landmark of the GOJ.

Landmarks of gastro-oesophageal junction (GOJ). (A) Schema of the landmarks used for GOJ. Endoscopic view of the GOJ. (1) palisade vessels, (2) squamocolumnar junctional line (Z line), (3) proximal end of the gastric folds, (4) gastric sling fibres and (5) angle of His. (B) Palisade vessels (thin arrows), squamocolumnar junctional line (Z-line) (arrow heads) and the end of gastric folds (thick arrows) are shown. These three landmarks (distal end of palisade vessels, Z-line and proximal end of gastric folds) are closely aligned with each other in normal subjects. (This endoscopic Image was provided by Prof. MF.).
PEGF has been used by many Western gastroenterologists for defining the GOJ, since 1987, when McClave et al proposed PEGF as an optimal endoscopic landmark for diagnosing the columnar-lined oesophagus.39 Although those investigators described PEGF as a stable landmark in subjects with hiatus hernia, the study included only four normal control subjects. Moreover, the biopsies taken from the PEGF in the control subjects contained junctional-type mucosa (corresponding to cardiac type mucosa), which might not be a gastric mucosa at all (see below). Furthermore, the literature42 provided by the authors to support their contention that PEGF represents the GOJ was not convincing.
It is well known that PEGF can vary with different observation methods and pathologic changes in the stomach. In severe gastric atrophy, for instance, gastric folds can become indistinct. The location of the PEGF is susceptible to change with air insufflation during endoscopic observation (see CQ 3 and 4). In the surgically resected oesophagogastrectomy specimens, Chandrasoma et al reported that oesophageal submucosal glands, an established anatomical hallmark of the oesophagus, were present distal to the PEGF, raising doubts on its validity as a landmark of the GOJ.43 A recent report has presented evidence to support Chandrasoma’s assertion.44 In this large multicentre study, biopsies taken at the PEGF by experienced endoscopists were histologically diagnosed as containing the ‘cardiac mucosa’ in the majority.44 Furthermore, cardiac mucosa at the GOJ was found to be associated with symptoms of GORD and/or oesophagitis, supporting Chandrasoma’s contention that ‘cardiac mucosa’ represent columnar metaplasia of the oesophagus, not the stomach.44
In contrast, DEPV has been shown to mark the anatomical site where the lower oesophageal sphincter (LOS) ends and merges with gastric muscle structures.45 46 This vascular landmark is not altered by oesophageal columnar metaplasia or by gastric pathology such as atrophy or IM. Moreover, DEPV has been used as a landmark for identifying the LOS during per oral oesophageal myotomy for the treatment of achalasia47 48 and palisade vessels (PV) has been used to identify the end of the oesophagus in the resected specimen.49–51 In a recent review, DEPV was deemed more accurate than PEGF as a mucosal landmark for GOJ.52
Another proposed anatomic landmark for the GOJ is the angle of His, which has been used for surgically resected or autopsy specimens. Although the angle of His can be surmised during endoscopy with retroflexed views,38 it can be difficult to determine its precise location if hiatal hernia is present.
CQ3
Which of the two landmarks, DEPV or PEGF, is more appropriate for clinically defining the GOJ?
Statement 3
Clinically, if the DEPV is clearly identifiable, it should be used for defining the GOJ. In case the PV are not identifiable, the PEGF should be used as a landmark of the GOJ.
Agreement
Strongly agree 78%.
Agree with minor reservation 11%.
Disagree with major reservation 11%.
Strongly disagree 0%.
Quality of evidence
High 57%.
Moderate 29%.
Low 14%.
Very low 0%.
Strength of recommendation
Strong 68%.
Weak 32%.
Not applicable 0%.
Textual explanation
As described in CQ2, DEPV is considered a preferred landmark as it is not influenced by epithelial changes53 and it has been validated by anatomical, histologic and in vivo dissection studies (see the textural explanation in CQ2). However, identification of the DEPV requires proper training and appropriate control of air insufflation during endoscopic examinations.54–58 High-resolution endoscopy with image-enhanced modalities may increase the visibility of PV.59 60 Nevertheless, inflammation in the terminal oesophagus can compromise the recognition of this landmark (online supplemental figure 1). In such cases, PEGF can be used as a surrogate landmark for the GOJ. Use of proton pump inhibitors (PPIs) for several weeks prior to endoscopy to resolve the oesophageal inflammation was reported to be beneficial in increasing the diagnostic yield for USSBO.61 In this study, PEGF was used as a landmark for GOJ, but it is possible that this kind of pretreatment may increase the visibility of DEPV in the columnar metaplasia as well. Similarly, therapeutic use of PPIs for GORD was shown to reduce mucosal thickness of the distal inflammatory squamous epithelium,62 and, hence, may facilitate recognition of PV, though this has to be tested in the future.
Supplemental material
To distinguish which landmark is used to define GOJ for research purposes, we propose that endoscopists specify either GOJp (the subscript ‘p’ for palisade vessel) or GOJg (the subscript ‘g’ for gastric folds) is used to define the site when biopsies in this zone are taken. Refer to CQ4 to CQ6 for more detailed description of proper endoscopic methods to observe these landmarks.
CQ 4
What is the most appropriate endoscopic method to identify the DEPV?
Statement 4
White light imaging (WLI) with/without image-enhanced endoscopy (IEE) in both forward and retroflexed views with air insufflation is the most appropriate method for identifying the DEPV.
Agreement
Strongly agree 71%.
Agree with minor reservation 29%.
Disagree with major reservation 0%.
Strongly disagree 0%.
Quality of evidence
High 57%.
Moderate 36%.
Low 7%.
Very low 0%.
Strength of recommendation
Strong 79%.
Weak 21%.
Not applicable 0%.
Textual explanation
Textural explanation for statements 3–5 are combined together (see CQ5).
CQ 5
What is the most appropriate endoscopic method to identify the PEGF?
Statement 5
To clearly identify the PEGF by endoscopy, the air insufflation must appropriately be controlled as excessive air inflation or deflation changes the position and shapes of the PEGF.
Agreement
Strongly agree 89%.
Agree with minor reservation 11%.
Disagree with major reservation 0%.
Strongly disagree 0%.
Quality of evidence
High 78%.
Moderate 18%.
Low 4%.
Very low 0%.
Strength of recommendation
Strong 93%.
Weak 7%.
Not applicable 0%.
CQ6
Can IEE improve visibility of the PV?
Statement 6
IEE can improve the visibility of PV.
Agreement
Strongly agree 72%.
Agree with minor reservation 21%.
Disagree with major reservation 7%.
Strongly disagree 0%.
Quality of evidence
High 21%.
Moderate 57%.
Low 18%.
Very low 4%.
Strength of recommendation
Strong 39%.
Weak 61%.
Not applicable 0%.
Textual explanation for statements 4–6
As mentioned in the explanation for the statements 1 and 2, DEPV is considered a preferable landmark for the GOJ based on the anatomical evidence. However, identification of DEPV depends on the endoscopic observation method, requiring standardisation to ensure reproducibility. For instance, Kusano et al 57 evaluated whether there were differences between American and Japanese endoscopists in the recognition of PV. A total of 82 patients were enrolled in this study. After an appropriate training, both American and Japanese endoscopists identified the GOJ with the DEPV as a landmark in 87.8% (72/82) and 89.0% (73/82) of cases, respectively. In another study, presence of PV was assessed in endoscopic images obtained from Western patients in eight conditions by a panel of six endoscopists from Japan and Netherland.58 The results showed visible PV in 25 patients (100% (95 % CI 87 to 100)) during insufflation of the four available insufflation images per patient, namely, forward approach–WLI–insufflation, forward–narrow band imaging (NBI)–insufflation, retroflexed–WLI–insufflation and retroflexed–NBI–insufflation, whereas PV were recognised in 15 patients (60% (95 % CI 41 to 77)) in the deflated condition of the four desufflation images per patient); p<0.001, suggesting adequate air insufflation for identifying PV.
Endoscopic identification of the PV, however, can be difficult in cases with reflux oesophagitis or BO since inflammation and/or mucosal dysplastic changes may obscure them. Insufficient air inflation can also render them difficult to visualise. Therefore, PEGF has been widely adopted as the landmark for GOJ3 5–7 39 54 63 despite uncertain anatomic evidence as discussed in previous CQs.
It should be noted that the endoscopic observation method appropriate for identifying the PEGF is rather opposite to that of PV; namely, air must be properly deflated by endoscopy as air insufflation flattens the gastric folds obscuring the tips of the folds. However, caution must be exerted not to excessively suck the air, as it may change the position of the PEGF and/or cause artificial plication of the oesophageal mucosa that simulates the gastric folds (pseudogastric folds) (figure 2A–C). This precaution should particularly be taken in patients with columnar metaplasia as the metaplastic mucosa cannot be discriminated by mucosal colour. Also, in patients with dilated distal oesophagus, oesophageal folds can erroneously be interpreted as gastric folds.43 64 Moreover, respiratory movement was shown to affect the position of diaphragm causing separation of the PEGF from the DEPV by deep inspiration.55 56 65 Other factors including heart pulsation and contraction of the LOS may further complicate accurate identification of the GOJ. Therefore, in order to identify the PEGF, standardised endoscopic observations with proper desufflation of air should be applied.

Changes of endoscopic images at the GOJ depending on the different observation conditions. (A) This white light image was taken with deflated condition. Note that oesophageal mucosa on the left side of this image forms as a fold-like configuration, but can be identified as oesophageal mucosa as the whitish colour of the squamous epithelium. Whereas the columnar metaplasia seen at the upper right folds with columnar metaplasia, such a fold-like configuration can be miss-interpreted as PEGF. (B) When the distal end of the oesophagus was inflated with moderate amount of air, the distal end of the gastric folds was clearly recognisable. Although palisade vessels can be seen on the right side of the same fold pointed out in A, they are not visible on the other side of this image, indicating a very short area of metaplastic mucosa. (C) Image taken under further air insufflation during deep inhalation, separation between the PEGF and SCJ became more obvious, partly due to flattening of the gastric mucosa. On the right side of this image, DEPV in the columnar mucosa distal to the squamous epithelium became clearly visible, indicating the presence of metaplastic mucosa in this case. (These endoscopic images were provided by Prof. TG.). DEPV, distal end of palisade vessel; GOJ, gastro-oesophageal junction; PEGF, proximal end of gastric fold; SCJ, squamocolumnar junction.
Although fairly good results in identifying PV have been reported if trained properly under an appropriate air insufflation, improved endoscopic imaging modalities may further facilitate recognition of PV.
NBI is well known as an excellent tool to highlight microvascular details and may, thus, improve visualisation of the PV.66 However, a study comparing high-resolution WLI with NBI did not show difference in identifying DEPV.58
A different modality of image enhancement, called flexible intelligent colour enhancement, may increase the visibility of PV,59 but another report questioned the superiority of this modality over WLI in identifying BO.67 Inconsistent results of the two studies might be explained by the difference in the spectral settings. Thus, further studies are required for validating the utility of this modality.
Recently, a new modality of IEE, linked colour imaging (LCI), was shown to improve visibility of short segment Barrett’s mucosa as compared with WLI in a single-centre retrospective clinical study.60 Intraclass correlation coefficient (ICC) for the inter-rater reliability for LCI compared with WLI was 0.77 (95% CI 0.67 to 0.84). ICC for the intrarater reliability of LCI compared with WLI ranged from 0.45 to 0.57 for trainees and 0.49–0.79 for experts. Intrarater reliability for LCI was ‘moderate’ for trainees and ‘moderate-substantial’ for experts, indicating better visibility even in trainees. Although their study used PEGF as the landmark for GOJ, the visibility of PV was also reported to be superior to WLI. These data support a promising role of LCI for better identification of PV in patients with SSBO, but should be validated in a prospective, multicentre study involving a larger number of subjects under a standardised condition of endoscopic observation. In contrast, however, another modality of IEE, blue laser imaging (BLI) did not show an improvement over WLI on the visibility of BO in this study. More recent reports also described a high rate of diagnosis of SSBO with LCI due to technical enhancement of colour difference.68 69
CQ 7
What is the location of the SCJ in the fully developed fetus?
Statement 7
The SCJ is located at the terminal end of the oesophagus in the fully developed fetus. There is no congenital columnar metaplastic change.
Agreement
Strongly agree 75%.
Agree with minor reservation 21%.
Disagree with major reservation 4%.
Strongly disagree 0%.
Quality of evidence
High 47%.
Moderate 39%.
Low 14%.
Very low 0%.
Strength of recommendation
Strong 68%.
Weak 32%.
Not applicable 0%.
Textual explanation
In the human fetus, the oesophagus is initially lined with simple columnar epithelium, and then ciliated cells appear.70 71 Formation of squamous epithelium becomes evident initially in the middle oesophagus. Ciliated cells disappear after 36 weeks of gestation71 but may persist until birth. During this period of conversion of ciliated epithelium into squamous epithelium, scattered foci of superficial columnar glands (oesophageal cardiac glands) originating from the foetal columnar epithelium develop most prominently in the upper and distal ends of the oesophagus.70 After 20 weeks of gestation, well-defined acidic mucin-positive cardiac glands and pits become recognisable at the SCJ (or Z-line).71 However, more precise cellular composition of these glands was not described in these studies. Zhou et al reported that a transitional zone with the characteristics of cardiac mucosa was universally present between squamous epithelium and oxyntic mucosa in the fetus and neonates.72 In this study, mixed glands containing mucous cells with isolated parietal cells (corresponding to oxyntocardiac gland) appeared at 15 weeks of gestational age when parietal cells in the stomach emerge, indicating the transitional mucosa during prenatal period is predominantly of gastric origin. The proportion of transitional mucosa with pure mucous glands increases after birth. Similarly, Park et al identified the transitional epithelium mucous glands with scattered parietal cells abutted the squamous epithelium in 78% of fetal and paediatric autopsy cases.73 Their autopsy cases, however, only covered cases up to 34 weeks of gestation and only three neonatal (within 1 month after birth) cases were included. Although these studies showed that well-identifiable SCJ is formed by full-term in the fetus, none of them described the location of SCJ in reference to the anatomical landmarks described in CQ 1 and 2 or the angle of His.
De Hertogh et al reported that the tiny area of cardiac mucosa (0.3–0.6 mm) in neonates lie at the same level (in 41-week fetus) or just distal to (0.3 mm at 7 months infant) the GOJ with the angle of His74 as a reference marker. In contrast, Kilgore et al described the SCJ as aligned with the angle of His, which corresponded to the PEGF in paediatric autopsy series (mean age 6.3 years, range 16 days to 18 years).75 In all of their cases, cardiac-type mucosa was present as a narrow zone (mean length of 1.2 mm on the gastric side of the oesophageal squamous epithelium.75 Note that they were prudent enough to use the term ‘cardiac-type mucosa’ instead of ‘cardiac mucosa’. In any event, SCJ aligns with the anatomical GOJ with the angle of His as a reference.
In a detailed anatomical landmark study, the line connecting the DEPV is not straight but is concave and about 5 mm distal to the angle of His on the lesser curvature in adult specimens.76 If similar anatomic relation between the angle of His and DEPV is maintained in neonates, the cardiac-type mucosa might be originated from the oesophageal mucosa at least on the lesser curvature side. However, further detailed histological studies in the fetal and neonatal specimens are required to ascertain if this anatomical relation between DEPV and the angle of His can be replicated in full-term neonates.
CQ 8
Does cardiac mucosa exist in fetuses and infants?
Statement 8
Cardiac mucosa exists in fetuses and infants, but its extent is minimal.
Agreement
Strongly agree 82%.
Agree with minor reservation 18%.
Disagree with major reservation 0%.
Strongly disagree 0%.
Quality of evidence
High 43%.
Moderate 50%.
Low 7%.
Very low 0%.
Strength of recommendation
Strong 50%.
Weak 50%.
Not applicable 0%.
Textual explanation for CQ 8, 9 are combined (see CQ 9).
CQ 9
What are the definition and histological features of cardiac-type mucosa?
Statement 9
Cardiac-type mucosa is histologically defined as mucosa, which consists of a foveolar epithelium with only mucous glands and no parietal cells.
Agreement
Strongly agree 61%.
Agree with minor reservation 39%.
Disagree with major reservation 0%.
Strongly disagree 0%.
Quality of evidence
High 48%.
Moderate 45%.
Low 7%.
Very low 0%.
Strength of recommendation
Strong 55%.
Weak 45%.
Not applicable 0%.
Textual explanation for statements 8 and 9
There has been a controversy as to whether the cardiac mucosa is a normal native constituent or an acquired metaplasia of the oesophageal squamous epithelium.70–73 75–85 Researchers in the University of Southern California (USC) have asserted that the cardiac mucosa develops through metaplastic change of the oesophageal squamous epithelium as a consequence of reflux.79–85 Park et al also demonstrated the presence of the transitional mucosa with oxyntocardiac glands but without pure cardiac glands in fetal and paediatric autopsy materials,73 supporting their concept. However, Chandrasoma, a representative researcher from USC, acknowledged the presence of the cardiac mucosa (mostly oxyntocardiac type) in four out of seven autopsy specimens of infants.79 In contrast, other groups demonstrated the existence of the cardiac mucosa in autopsy studies of fetuses and infants, though its extent was very limited.72 74–77 86 87 For instance, De Hertogh et al 74 identified the cardiac mucosa as containing only mucous glands with a mean length of 1.0 mm (range 0.1–3 mm) and present distal to the squamous epithelium in all autopsy cases of fetuses, neonates and an infant (up to 7 month), but it spanned only 0.3–0.6 mm after birth. The same group confirmed their previous findings that the cardiac mucosa with pure mucous glands (mean length: 0.612 mm, range 0.160–1.308 mm) was present in fetuses, neonates and may grow in length with age, which showed similar cytokeratin staining with the Barrett’s epithelium.86 Derdoy et al 87 reported that cardiac mucosa with pure mucous glands was present in all paediatric autopsy cases including premature babies (mean age: 2.2 years, range: 1 day to 18 years). Zhou et al 72 also showed the presence of a very short stretch of transitional epithelium composed of simple columnar epithelium, pure mucous glands or mixed (oxyntocardiac) glands (mean length: 0.226 mm in foetuses, 0.167 mm in postnatal infants) between the oesophageal squamous epithelium and the gastric oxyntic mucosa in 78% of their series. The rest of their cases (22%) lacked this transitional mucosa in which the oxyntic mucosa directly abutted the squamous epithelium. Therefore, the majority of the autopsy studies involving neonates and infants supported the presence of the cardiac mucosa with pure mucous glands, if not completely circumferential, at the GOJ. Therefore, we agreed that the genuine cardiac mucosa exists as a native structural component at the GOJ, but the mean length is less than 1 mm. Kilgore et al 75 examined the mucosa of the GOJ in paediatric autopsy cases (mean age: 6.3 years, range 16 days to 18 years) and found cardiac-type mucosa with pure mucous gland in all specimens with a mean length of 1.8 mm (range: 1.0–4.0 mm). They also noted that this cardiac-type mucosa was adjacent to the transitional mucosa (cardio-oxyntic mucosa) in 59% cases, while the rest lacked the transitional mucosa and directly faced to the oxyntic fundic mucosa. The maximal length of combined cardiac-type and transitional-type mucosa was 8 mm. Therefore, the cardiac-type mucosa is still less than 5 mm during childhood, indicating that the traditional concept of cardiac mucosa extending several centimetres in the proximal stomach88–90 is false as ‘the cardiac glands’ described in these papers contained parietal cells. Furthermore, this proposal by Hayward not based on tangible data more than half a century ago that the cardiac epithelium, for which his preferred term was the junctional epithelium, occupies about 1 cm to 2 cm of the most distal portion of the oesophagus91 seems to be inappropriate in view of the current concept of the cardiac mucosa but might have been due to a mislabelling of the columnar metaplasia. In contrast, Miyagawa described two types of cardiac glands, one without oxyntic cells and another with oxyntic cells, present in the small area (0.5 cm) of the orifice of the stomach,92 which is consistent with the current observations.
Regarding the GOJ in the adults, Sarbina and colleagues reported the length of cardiac mucosa ranged from 1 mm to 15 mm in surgically resected specimens in adult patients (median 55 years, range 24–82 years) with squamous cell carcinomas.93 Nakanishi et al reported in their series of surgical specimens in patients with oesophageal squamous cell carcinomas (mean age: 63 years, range 46–94 years) that the mean length of the cardiac mucosa in the oesophagus was 4 mm (range 1–26 mm) and that of the gastric side was 13 mm (range 2–64 mm) with the angle of His as a reference point for GOJ.94 More recently, Stojsic et al verified the presence of cardiac-type mucosa in all the adult autopsy cases (mean 59 years) at the angle of His (incisura).95 Although they found areas with pure mucus glands (cardiac-type mucosa), they are always intermingled with the oxyntocardiac-type glands in the same section. The mean length of total transitional mucosa including oxyntocardiac type glands was 6.7 mm (range: 0.927–19.5 mm). As mentioned in CQ6, the line connecting the angle of His lies proximal to the GOJ with the DEPV as a reference,75 the extension of the cardiac-type mucosa in to the gastric lesser curvature side should be minimal, if present.
Since the lengths of the ‘cardiac mucosa’ observed in adults were longer than those of neonates and infants, metaplastic changes, either in the adjacent oesophageal squamous epithelium or in the gastric mucosa would be contributing to this extension of the cardiac-type mucosa.96
Can we discriminate these three types of ‘cardiac mucosa’, namely, the pure cardiac mucosa consisting of mucous glands, the columnar metaplastic mucosa of the oesophagus and the atrophic oxyntocardiac or fundic mucosa devoid of parietal cells or chief cells? Currently, these three-types of mucosa are hardly discernible not only with H&E staining but with mucin histochemistry. Thus, in this consensus, we propose the umbrella term ‘cardiac-type mucosa’ instead of ‘cardiac mucosa’ to be used for describing the mucosa found at the adult GOJ. Indeed, this term has already been used by some of the prescient investigators.75 89
CQ 10
Which direction does the cardiac-type mucosa lengthen?
Statement 10
Cardiac-type mucosa expands proximally due to GORD.
Agreement
Strongly agree 71%.
Agree with minor reservation 29%.
Disagree with major reservation 0%.
Strongly disagree 0%.
Quality of evidence
High 68%.
Moderate 32%.
Low 0%.
Very low 0%.
Strength of recommendation
Strong 82%.
Weak 18%.
Not applicable 0%.
Textual explanation for CQ 9 and 10 is combined (see CQ10).
CQ 11
What is the role of hiatus hernia in the lengthening of cardiac mucosa?
Statement 11
In hiatus hernia, cardiac-type mucosa extends proximally due to reflux.
Agreement
Strongly agree 86%.
Agree with minor reservation 14%.
Disagree with major reservation 0%.
Strongly disagree 0%.
Quality of evidence
High 68%.
Moderate 32%.
Low 0%.
Very low 0%.
Strength of recommendation
Strong 79%.
Weak 21%.
Not applicable 0%.
Textual explanation for statements 10 and 11
As already described in the explanation for CQ7 and 8, several investigators have noted the association of longer cardiac-type mucosa with age, and inflammation at the GOJ,77–83 though not confirmed by others.74 75 87 However, these studies were retrospective observations and, thus, inadequate for establishing the cause–consequence relationship.
Recently, McColl’s and colleagues demonstrated in their elegant prospective studies that the cardiac-type mucosa extends proximally in association with increasing age, central obesity and hiatus hernia in H. pylori-negative healthy volunteers.97 98 In the healthy subjects, however, the LOS function remained intact and thereby limited the regurgitation within the LOS. Thus, the extension was confined within the LOS and further development of BO was prevented. This proximally extended cardiac-type mucosa closely resembled non-IM BO immunohistochemically.99 This association with risk factors predisposing to GOR (age, central obesity and hiatus hernia) and resemblance to BO suggest that this proximal extension of cardiac-type mucosa is due to columnar metaplasia of the most distal oesophageal mucosa secondary to intrasphincteric GOR, which is associated with central obesity and may provoke the columnar metaplasia and consequently promote proximal extension of cardiac-type mucosa in these subjects.97
In contrast, in H. pylori-positive subjects, atrophic changes most frequently progress from the incisura to the proximal corpus mucosa, but also spreads from the GOJ mucosa to a more distal part in some cases.100–103 In a recent study that examined parietal and chief cell density in biopsy specimens, the incisura and the GOJ were the two sites where a highest rate of reduction of both parietal cells and chief cells was observed in patients with H. pylori infection resulting in the longer length of mucosa without parietal cells distal to the GOJ.104 This atrophic loss of parietal and chief cells distal to the SCJ mucosa can be accounted for as the consequence of extensive progression of atrophy from the distal gastric mucosa in the majority but may be due to the isolated atrophic change in the oxyntocardiac or fundic mucosa independent from the atrophic changes in the distal stomach. In a study with surgically resected specimens due to squamous cell carcinoma of the oesophagus, isolated IM below the SCJ was noted in 21% of them, whereas IM were continuous from the distal stomach in the majority (42%). About half of the isolated IM at the SCJ would be oesophageal mucosal origin as indicated by the presence of submucosal oesophageal glands.105 Occurrence of atrophy and IM at the GOJ independent from those of the distal stomach in H. pylori-positive patients was reported in a Western population as well.106 Another recent report investigating a large number of biopsies taken at the GOJ in the US population also demonstrated that IM in three subset of patients, one with columnar metaplasia in the distal oesophagus (BO), second with distal gastric IM and the rest without BO or distal gastric IM (isolated IM at the GOJ).107
It has been well-established that hiatus hernia is a prominent risk factor for BO (according to the traditional definition requiring the presence of SIM) irrespective of the length.108 109 Although more prospective studies showing the cardiac-type mucosa proximally extends with hiatus hernia are required, it would be reasonable to assume that this condition facilitates the proximal extension of the cardiac-type mucosa.
CQ 12
What is the role of impedance and pH monitoring in the analysis of GOJ mucosal pathophysiology?
Statement 12
Currently available impedance and pH monitoring equipment have a limited role for investigating oesophageal junctional mucosal pathophysiology.
Agreement
Strongly agree 66%.
Agree with minor reservation 31%.
Disagree with major reservation 3%.
Strongly disagree 0%.
Quality of evidence
High 38%.
Moderate 55%.
Low 7%.
Very low 0%.
Strength of recommendation
Strong 55%.
Weak 45%.
Not applicable 0%.
Textual explanation
The presence of liquid and/or gas reflux is measured by the oesophageal impedance technique,110 and intraoesophageal acid exposure time is measured by 24-hour ambulatory pH monitoring.111 The combination of these modalities allows us to analyse the effect of acidic, weakly acidic and non-acidic reflux on oesophageal junctional mucosal pathophysiology.112–114
In general, intraoesophageal acid exposure time is known to be associated with the degree of oesophageal mucosal injury.115 Recent studies suggest that mucosal injury is caused by immunological mechanisms triggered by inflammatory mediators or cytokines that are released from oesophageal mucosal cells by stimulation with acid.116 117 There is an argument whether pH monitoring data truly reflect the acidic environment because the pH probe used for 24-hour pH monitoring is placed 5 cm above the GOJ, not at the GOJ itself. However, it is known that the acidic environment 5 cm above the GOJ reflects the true environment at the GOJ well.118 119 It is also known that intraoesophageal acid exposure time (pH <4) results in columnar epithelialisation with increased expression of intestinal differentiation factors such as CDX1, CDX2 and BMP4 in oesophageal epithelial cells and stromal cells, respectively.120 Therefore, measurement of intraoesophageal acid exposure time by 24 hour pH monitoring is useful for analysing oesophageal junctional mucosal pathophysiology as a method of predicting columnar epithelialisation. In fact, it has been reported that intraoesophageal acid exposure time is an important factor determining the length of Barrett’s mucosa.121–123 Regarding liquid and/or gas reflux, not only an acidic environment (pH <4) but also a weakly acidic environment (pH >4) is assumed to affect oesophageal junctional mucosal pathophysiology. It has been reported that a weakly acidic environment (pH >4) enhanced mucosal permeability, which results in dilation of intraepithelial spaces (DIS).124 125 Experimentally, even a weakly acidic environment (pH >4) is known to release inflammatory mediators such as ATP from oesophageal mucosal cells.126 However, the mechanisms of how a weakly acidic, as well as an acidic, environment induces mucosal permeability, mucosal impedance and metaplastic change are unknown.
It has been reported that baseline impedance represents mucosal integrity, which is related to changes of mucosal permeability, tight junctions and DIS.127–130 If mucosal permeability increases, baseline impedance decreases, thereby it can be regarded as a new measure of oesophageal mucosal integrity, though the specific cause of lowering the baseline mucosal integrity cannot be inferred.
In this regard, the pathophysiological roles of bile acids need to be taken into consideration. The Bilitec that detects bilirubin in gastroduodenal refluxate has been used as a surrogate measurement of toxic bile acid. Increased oesophageal exposure of bile refluxate detected with this monitoring has been documented to be associated with the occurrence of Barrett’s mucosa and mucosal injury.131–136 Moreover, development of Barrett’s metaplasia was less frequent in patients with acidic reflux alone, but was more prevalent in those with mixed bile and acid reflux.131–134 136 Even higher bile reflux was observed in patients with complicated BO.137 Clinically, it is also known that the injurious bile acid composition of the refluxate or gastric juice was higher in patients with BO than in patients without.138 139 From these studies, it is thought that bile reflux affects oesophageal junctional mucosal pathophysiology. Since impedance and pH monitoring alone cannot evaluate the bile reflux, they have a limited role for investigating the bile-induced epithelial alterations at the GOJ.
CQ 13
What is the role of high-resolution manometry (HRM) and functional luminal imaging probe (EndoFLIP) planimetry in the evaluation of GOJ pathophysiology?
Statement 13
HRM is useful for evaluating the motor function of the GOJ, whereas functional luminal imaging probe (EndoFLIP) planimetry is useful for evaluating the distensibility of the GOJ.
Agreement
Strongly agree 86%.
Agree with minor reservation 14%.
Disagree with major reservation 0%.
Strongly disagree 0%.
Quality of evidence
High 69%.
Moderate 24%.
Low 7%.
Very low 0%.
Strength of recommendation
Strong 62%.
Weak 38%.
Not applicable 0%.
Textual explanation
Studies have reported techniques and usefulness of HRM in evaluating pathophysiology of oesophageal motor disorders.140–150 A recently introduced functional lumen imaging probe (EndoFLIP) allowed three-dimensional imaging of lumen distensibility in real time and clarified functional and anatomical abnormalities of GOJ in cases with GORD, eosinophilic esophagitis, achalasia and other gastrointestinal motor diseases.151–158 Due to limited availability and suboptimal resolution, however, no detailed study looking into the changes of histologic phenotype at the GOJ mucosa with this instrument has been published.
CQ 14
How can we define a GOJZ to clarify junctional pathologies?
Statement 14
A GOJZ can be defined endoscopically as a transitional segment extending 1 cm either side of GOJ.
Agreement
Strongly agree 69%.
Agree with minor reservation 17%.
Disagree with major reservation 7%.
Strongly disagree 7%.
Quality of evidence
High 21%.
Moderate 45%.
Low 24%.
Very low 10%.
Strength of recommendation
Strong 45%.
Weak 48%.
Not applicable 7%.
Textual explanation
The GOJ is defined as a border between the abdominal oesophagus and the gastric cardia. The GOJ is radiologically recognised by barium swallow as a sharp angulation between the tubular oesophagus and the sac-shaped stomach. This incisura is called angle of His. Angle of His is anatomically created by the collar-sling muscle of the stomach. The collar-sling muscle is the most inner muscle layer of the gastric cardia. The upper margin of the collar-sling muscle is considered as GOJ anatomically in muscle level.91 159–161
The SCJ is an epithelial landmark, which is clearly recognisable by endoscopy as a border of white oesophageal squamous mucosa and salmon pink gastric mucosa. Thus, SCJ seems to be a simple and endoscopically clear landmark of GOJ, but it quite often shifts proximally in pathological conditions like erosive oesophagitis and BO.10 56
The DEPV is an independent and anatomically fixed marker of GOJ (refer to CQ2). Without BO, DEPV corresponds accurately to SCJ.45 53
In most Asian populations, PV are clearly observed during endoscopic examination, but it is not uncommonly obscured in Western populations. In such a situation the PEGF is an alternative visually recognisable indicator. DEPV and PEGF are mostly in the same location, but PEGF is often affected by insufflated air volume at endoscopy (refer to CQ3–5 for detailed explanation).
In the submucosal layer, spindle veins are one of the specific markers of gastric cardia (online supplemental figure 2). When the spindle veins appear in the submucosal tunnel, they mark the beginning of the gastric submucosa.47 48 Spindle veins run vertically and connect both branched vessel (at the level of muscularis mucosae (CM)) and submucosal drainage veins in the gastric cardia. Spindle veins are regarded as a characteristic anatomical landmark during submucosal endoscopy such as POEM (per-oral endoscopic myotomy).
The length of cardiac-type mucosa varies from a few millimetres to a few centimetres in the literature, but as explained in the previous sections above, the extent of this type of mucosa is very limited. Cardiac-type mucosa has its specific histological and immunohistochemical features (refer to CQ 7 to CQ 9).72–75 86 93 94
DEPV and PEGF at mucosal level, spindle veins at submucosal level and upper margin of oblique muscle at muscle level are not exactly at the same position but close to the DEPV (same position to SCJ without BO) with a few centimetre discrepancies. Therefore, GOJ is practically and theoretically recognised as a ‘junctional zone’ including these gaps and variations (refer to CQ 25).
Although metaplastic changes of the squamous epithelium exceeding 1 cm from the GOJ as defined in CQ 2 can reproducibly be recognisable as BO, which are supported by several consensus documents, the issue of the cardiac-type mucosa found within 1 cm from the GOJ has been left unsettled. In this consensus, we agreed that all the cardiac-type mucosa found above the GOJ should be considered as BO (refer to CQ 1). However, considering the discrepancies between the various guidelines, the area residing within 1 cm proximal to the GOJ is included in the GOJZ. Thus, oesophageal side of GOJZ includes so-called USSBO.
As for the range on the gastric side, we set the mucosal area within 1 cm from the GOJ (as defined by DEPV) based on the maximum extent of distribution of the cardiac-type gland mucosa in adults to reduce inclusion of pathologies of the gastric fundic mucosa (refer to CQ 9). This new definition of GOJZ is narrower by 1 cm in the gastric side than the well-known Sievert type II definition162 but will substantially eliminate the inclusion of gastric pathology. To estimate the length of GOZ during routine endoscopic examinations, currently available endoscopes have a diameter of approximately 1 cm, which can be used as a reference.
CQ 15
What are the principal causes of inflammation in the GOJZ?
Statement 15
H. pylori infection and GOR are the principal causes of inflammation in the GOJZ.
Agreement
Strongly agree 90%.
Agree with minor reservation 3%.
Disagree with major reservation 7%.
Strongly disagree 0%.
Quality of evidence
High 80%.
Moderate 17%.
Low 3%.
Very low 0%.
Strength of recommendation
Strong 83%.
Weak 17%.
Not applicable 0%.
Textual explanation
H. pylori
Infection causes inflammation in all the gastric mucosa from the gastric cardia, corpus and antrum.104 106 163–169 Inflammation tends to be more intense in the cardia as compared with gastric corpus.104 106 163 H. pylori colonisation in the oesophageal mucosa, which correlated with inflammatory changes, was also reported.170 However, inflammation in the cardia occurs even without H. pylori infection and has been shown to be associated with GOR.44 79 169 171–173 Chronic inflammation of the GOJ mucosa appears to be the immediate consequence of GORD, correlating with endoscopic diagnosis,169 and occurs without H. pylori infection.44 79 169 171
The inflammatory changes can be induced by bile reflux. Indeed, bile reflux gastritis and IM at the cardia are correlated.174 175 Bile acids in low pH milieu are harmful in inducing oxidative and nitrosative stress in oesophageal epithelial cells, leading to DNA damage.176 177
Luminal nitrosative stress derived from dietary components (such as leafy vegetables containing a high amount of nitrates) could be a potential chemical insult to the human GOJ area.178–181 The oesophageal microbiota other than H. pylori may also be involved in the inflammation in the GOJZ.182–189 As Gram-negative microbiota are predominant in the reflux oesophagitis and BO, lipopolysaccharide derived from them may mediate inflammation and metaplasia via activation of Toll-like receptors in the epithelium and inflammatory cells at the GOJZ.190 A number of studies also showed that obesity-induced adipocytokine abnormalities are associated with BO.191–198 The role of these chemical, bacterial and endocrine factors in causing inflammation in the GOJZ should be further investigated.
CQ 16
What is the mechanism and clinical relevance of formation of double MM in the oesophagus?
Statement 16
Double MM is likely the result of inflammation and will guide the pathological staging and clinical management of lesions in the oesophagus.
Agreement
Strongly agree 73%.
Agree with minor reservation 21%.
Disagree with major reservation 3%.
Strongly disagree 3%.
Quality of evidence
High 63%.
Moderate 34%.
Low 3%.
Very low 0%.
Strength of recommendation
Strong 72%.
Weak 28%.
Not applicable 0%.
Textual explanation
Histologically, double MM is a specific feature of BO noted by Takubo et al 199 and has been observed in 71% of 66 histological sections.51 198 Therefore, double MM is considered to be one of the most frequent features specific for BO.200 The lamina propria of the original oesophagus lies within the double MM.201 202 The deep MM is continuous with that of the gastric mucosa and lies beneath the oesophageal squamous epithelium. Smooth muscle fibres of the superficial MM of the columnar epithelial mucosa spread into the lamina propria. The proximal end of the thin MM becomes indistinct and disappears in fibrous tissue deep to the transition zone between the metaplastic columnar epithelium and the original squamous epithelium. The distal end of the superficial MM connects with the deep MM in the GOJZ. Thus, BO should be understood as comprehensive changes that involve the epithelium, lamina propria and MM, rather than a change limited to the epithelium (figure 3). However, no previous studies have investigated whether the columnar epithelium induces the stroma (lamina propria, MM) or vice versa. Although we can see double MM in cases of reflux oesophagitis, invasion by early squamous cell carcinoma, and sclerotherapy in the oesophagus, unlike the MM-associated BO, however, these double MM are seen in a very limited area. Therefore, we can consider that double MM is the result of reactive changes, likely to inflammation.203

Histological features of oesophagus at the gastro-oesophageal junction. In this specimen, histological features unique to the oesophagus are depicted; namely double muscularis mucosa consisting of the superficial muscularis mucosae (m) and the deep muscularis mucosae (M), squamous epithelium (S) and the duct (D) connected to the oesophageal submucosal gland (oesophageal gland proper; ESG). Note the right side of the epithelium is covered by columnar epithelium containing goblet cells. Presence of double muscularis mucosae, and the oesophageal submucosal gland underneath the epithelium indicate that the columnar epithelium is not gastric mucosa but metaplastic oesophageal mucosa. (This histology photo was provided by professor KM.).
CQ 17
Can metaplastic cardiac-type mucosa progress into IM?
Statement 17
Metaplastic cardiac-type mucosa shows molecular evidence of intestinal differentiation and appears to be the precursor of IM.
Agreement
Strongly agree 71%.
Agree with minor reservation 25%.
Disagree with major reservation 4%.
Strongly disagree 0%.
Quality of evidence
High 64%.
Moderate 29%.
Low 7%.
Very low 0%.
Strength of recommendation
Strong 71%.
Weak 25%.
Not applicable 4%.
Textual explanation
Many hypotheses have been reported regarding the cellular origin of BO with IM. These include (1) the columnar epithelium being directly generated from the oesophageal squamous epithelium,204–206 (2) a gastric mucosa creeping theory,207 208 (3) development from the oesophageal glands,209 (4) development from the transitional mucosa at the GOJ,210 (5) a foetal remnant211 and (6) development from bone marrow cells.212 Hattori’s group had shown a sequence of morphological changes of squamous epithelium leading to BO, found a peculiar metaplastic change common to other parts of the gut, and proposed the concept of a ‘gut regenerative cell lineage’ (GRCL).204 The GRCL is characterised by pyloric-foveolar metaplasia with goblet cell metaplasia, which occurs in the regenerative process in response to chronic inflammation.204 213 Columnar metaplasia without goblet cells reportedly has the potential to involve intestinal phenotypes.204 207 214–216 The earliest form of columnar metaplasia resembles gastric mucosal epithelium.204 207 214 217–219 The finding suggests that the cellular origin of the columnar metaplasia in the GOJZ might be similar to BO with IM. A recent report with sophisticated genetic analyses supports that BO originates from gastric cardia.220 It is, therefore, presumed that with time, and ongoing injury and inflammation, the metaplasia then undergoes additional reprogramming, which ultimately results in the development of intestinal differentiation.
CQ 18
Which is the more common metaplastic mucosa in the GOJZ, cardiac or intestinal type?
Statement 18
Metaplastic cardiac-type mucosa is more frequent in the GOJZ.
Agreement
Strongly agree 79%.
Agree with minor reservation 21%.
Disagree with major reservation 0%.
Strongly disagree 0%.
Quality of evidence
High 68%.
Moderate 32%.
Low 0%.
Very low 0%.
Strength of recommendation
Strong 71%.
Weak 29%.
Not applicable 0%.
Textual explanation
From data obtained mainly from biopsy specimens, Barrett’s mucosa has been classified into fundic, cardiac and intestinal types, in what was thought to be the order of arrangement from the distal end.221 However, biopsies in this study were blindly taken by suction method and might have been obtained from the gastric mucosa in hiatus hernia. Therefore, it is questionable that the cellular phenotypes reported in this study truly represented those of BO. Observations of resected specimens have indicated that these types tend to be arranged in an intricate mosaic pattern, especially in SSBO.222 However, it is difficult to judge the mucosal phenotypes as precise proportion of respective metaplasia was not reported, and inclusion of gastric fundic mucosa was suspected in this study. In a more recent study with a large number of biopsy samples taken under direct endoscopic examinations, cardiac-type mucosa without IM was most frequent (45.9%) as compared with IM (14.8%) within 1 cm from the GOJ as judged by PEGF.223 There are a few studies which examined mucin phenotype in the columnar epithelium-lined oesophagus. A study with specimens obtained by endoscopic submucosal dissection showed that the cardiac-type mucosa, the intestinal-type mucosa and a mixture of both types were present in 34.3%, 14.3% and 51.4%, respectively.224 The three epithelial types of columnar metaplastic mucosa were arranged as stated: cardiac in the distal, both cardiac and intestinal type in the middle and intestinal (when present) at the top. Another study from Japan reported that the SSBO predominantly had gastric-type mucin phenotype.225 In a large multicentre study (hisotGERD trial), patients with cardiac-type mucosa at the GOJ were much higher than those with IM.226 It should be noted that columnar, non-IM is a salient feature of paediatric or young patients with Barrett’ epithelium or GOJ.219 227–230 Age-dependent increase in the intestinal metaplastic changes indicates that cardiac-type metaplasia represents the early metaplastic change before IM arises.
Below the GOJ, genuine cardiac mucosa is present in the majority, if not all, of normal subjects. In a Chinese cohort, cardiac-type mucosa was more frequent than IIM in biopsy samples taken just below the GOJ.231 Similarly, IM in the gastric cardia was present in only a minority of patients with or without BO.232 In sum, we can conclude that the cardiac-type mucosa is the predominant metaplasia observed in the GOJZ, although the cellular origins of the metaplastic cardiac-type mucosa might be different depending on the location.
CQ 19
What factors are associated with IM in the GOJZ?
Statement 19
Gastric acid, pepsin, bile, nitrosative stress and H. pylori are associated with IM in the GOJZ.
Agreement
Strongly agree 72%.
Agree with minor reservation 21%.
Disagree with major reservation 7%.
Strongly disagree 0%.
Quality of evidence
High 47%.
Moderate 39%.
Low 14%.
Very low 0%.
Strength of recommendation
Strong 50%.
Weak 50%.
Not applicable 0%.
Textual explanation
Association of mixed acid and bile reflux with BO with the metaplastic mucosal length of over 1 cm has been well documented.130 134 233 Mechanistically, involvement of gastric acid and bile in the development of metaplastic changes were also indicated by experimental studies.234–238 It can be presumed that similar mechanisms are involved in the intestinal metaplastic changes in the GOJZ. In addition, reactive nitrogen species imposed at human GOJZ178 179 could be involved in the development of BO, which was shown in basic experimental studies239 240 although the association in the clinical settings remains to be proved. Since Barrett’s metaplasia is accompanied and preceded by cardiac-type metaplasia, and gene expression and immunohistological patterns between the metaplasia at both sites are similar,99 241 cardiac-type metaplasia may be the precursor of Barrett’s metaplasia with IM. In a longitudinal observational cohort study, progression to macroscopically visible BO was observed in about a quarter of patients with IM at the SCJ, supporting this notion.242 Thus, causative factors for Barrett’s metaplasia (eg, gastric acid, bile, nitrosative stress) could also act as stimuli for development of cardiac-type columnar metaplasia (see also CQ 20 for the risk of neoplasia in the columnar metaplasia).
In subjects with H. pylori infection, but without reflux, however, chronic inflammation due to H. pylori can be a major causative factor for IM in the GOJZ.104 106 243–247 In a large autopsy series, IM at the GOJZ was localised in the gastric side (namely, distal to the PEGF) in more than 90% cases. These cases also had more IM in the distal stomach, indicating a link with H. pylori gastritis.248
As mentioned in CQ14, dysbiosis of the oesophageal microbiota and alterations of adipocytokines might also play a role in the IM.
CQ 20
Do we have useful molecular markers to predict the progression of metaplastic cardiac-type mucosa to IM?
Statement 20
Although several markers have been proposed, there is no established marker ready for clinical application.
Agreement
Strongly agree 76%.
Agree with minor reservation 24%.
Disagree with major reservation 0%.
Strongly disagree 0%.
Quality of evidence
High 38%.
Moderate 62%.
Low 0%.
Very low 0%.
Strength of recommendation
Strong 52%.
Weak 48%.
Not applicable 0%.
Textual explanation
Although many hypotheses concerning the pathogenesis of GOJ mucosal metaplasia have been proposed, the precise molecular mechanisms of metaplastic change at the GOJ mucosa and the origin of cells from which GOJ metaplastic mucosa forms are not clear. The elevated expression of CDX2, EpCam and villin have been reported at the human GOJ metaplastic mucosa.213 214 249–252 However, increases in these markers were shown in the cardiac-type columnar metaplasia and may be used as predictors for the future development of IM. Trefoil factor 3 (TFF3) is another marker for detecting BO253 employed for non-invasive screening. Unfortunately, TFF3 may not be suitable for identifying the IM at the GOJZ as it was expressed in the cardiac-type mucosa as well as oesophageal submucosal gland.254 255 More recently, gene methylation profile has been explored as diagnostic biomarkers.256–261 Furthermore, microRNA (miR) profiles in the oesophageal mucosa as well as blood unique to BO have been extensively investigated.262–266 Although these newer biomarker panels have advantages of providing more objective measures and several promising results have been reported, their diagnostic performance on differentiating BO with IM from pure columnar metaplasia and on the intestinal metaplastic changes at the GOJZ requires further verification.
CQ 21
Does metaplastic cardiac-type mucosa in the absence of IM in the GOJZ predispose to adenocarcinoma?
Statement 21
Metaplastic cardiac-type mucosa in the absence of IM in the GOJZ appears to have a risk of progression to malignancy.
Agreement
Strongly agree 49%.
Agree with minor reservation 45%.
Disagree with major reservation 3%.
Strongly disagree 3%.
Quality of evidence
High 17%.
Moderate 59%.
Low 21%.
Very low 3%.
Strength of recommendation
Strong 31%.
Weak 66%.
Not applicable 3%.
Textual explanation
The criteria used in the USA suggest that metaplastic columnar epithelium with goblet cells is the main precursor of dysplasia and cancer, and as such, represents the specific subgroup of patients with columnar lined oesophagus at highest risk for neoplastic progression2 267–269 (see also textural explanation for CQ 1). While it is true that most cancers arise in the columnar lined oesophagus with goblet cells, there is indisputable evidence that metaplastic non-goblet columnar mucosa is at risk for cancer.31–35 221 In a recent study by Lavery et al, development of adenocarcinoma from premalignant columnar epithelium without goblet cells was convincingly demonstrated by tracing the clonal origin of cancer across an entire Barrett’s segment via a combination of histopathologic spatial mapping and clonal ordering.36 The non-goblet columnar epithelium, mainly cardiac-type mucosa, shows molecular abnormalities and the potential for neoplastic progression.28–36 218 224 270 A small prospective study also showed that development of adenocarcinoma in patients with the columnar metaplastic mucosa without IM.271 Therefore, metaplastic cardiac-type mucosa without IM is deemed to be an ‘at risk’ condition predisposing to neoplastic transformation.
CQ 22
Can IEE improve the diagnosis of IM in the GOJZ?
Statement 22
IEE with or without magnification can enhance the detection of IM in the GOJZ.
Agreement
Strongly agree 83%.
Agree with minor reservation 17%.
Disagree with major reservation 0%.
Strongly disagree 0%.
Quality of evidence
High 37%.
Moderate 60%.
Low 3%.
Very low 0%.
Strength of recommendation
Strong 53%.
Weak 47%.
Not applicable 0%.
Textual explanation
It has been reported that magnification endoscopy with chromostaining (methylene blue, indigo-carmine, and acetic acid) and IEE such as NBI with magnification or LCI without magnification achieved high degree of accuracy for detection of the IM in BO.60 68 69 272–283 Although evidence is limited, improved diagnostic performance of IEE with or without magnification on the diagnosis of IM in the GOJZ has also been reported.273 283
CQ 23
What should adenocarcinoma arising from the ‘GOJZ’ be named?
Statement 23
We propose to name it ‘GOJZ adenocarcinoma’.
Agreement
Strongly agree 90%.
Agree with minor reservation 10%.
Disagree with major reservation 0%.
Strongly disagree 0%.
Quality of evidence
High 44%.
Moderate 43%.
Low 10%.
Very low 3%.
Strength of recommendation
Strong 67%.
Weak 33%.
Not applicable 0%.
Textual explanation for CQ 23 (see CQ 24).
CQ 24
How is a GOJZ adenocarcinoma defined?
Statement 24
A GOJZ adenocarcinoma is one with its epicentre lying within 10 mm either side of the GOJ.
Agreement
Strongly agree 93%.
Agree with minor reservation 7%.
Disagree with major reservation 0%.
Strongly disagree 0%.
Quality of evidence
High 47%.
Moderate 50%.
Low 3%.
Very low 0%.
Strength of recommendation
Strong 70%
Weak 30%.
Not applicable 0%.
Textual explanation for CQ 23 and CQ 24
A short segment (GOJZ) straddling 1 cm proximal and distal to the GOJ has different spectra of the mucosa (see CQ 14 for the definition of GOJZ). However, the adenocarcinoma is assumed to develop only from the columnar epithelial cells such as the cardiac-type mucosa, specialised metaplastic mucosa, oesophageal cardiac glands (superficial oesophageal glands) and oesophageal submucosal glands, but not from the stratified oesophageal squamous cells. As it is difficult to exactly identify the cellular origin of the epithelium from which the adenocarcinomas in this area originate, an umbrella term ‘GOJZ adenocarcinoma’ is proposed for encompassing them in this meeting.
This new definition of GOJZ adenocarcinoma is distinct from the previous definitions on the adenocarcinoma of the GOJ, often called ‘cardiac cancer’ or ‘cancer in the gastric cardia’. For instance, Misumi et al proposed the definition of cardiac cancers as the tumours having its epicentre residing between 1 cm proximal and 2 cm distal to the GOJ area.284 The justification for his definition was derived from meticulous histological examinations on resected specimens where he showed that the distribution of ‘cardiac glands’ was 2.6 mm above and 6.7 mm below the SCJ on average. In his later report,285 the distribution of the cardiac glands ranged 7.5 mm proximal and 13 mm distal to the SCJ with the mean distance 0.8 mm for the proximal margin and 2.7 mm for the distal margin from the SCJ. Unfortunately, however, the landmark used for judging the GOJ in these studies was the SCJ which was located 0.5 cm to 1 cm proximal to the angle of His. Indeed, the submucosal oesophageal gland, a hallmark of the oesophageal tissue, was depicted in the ‘gastric’ side and several squamous cell carcinomas occurred in the ‘gastric’ side of the junction in these reports, implying the true GOJ lies below the reference line (SCJ) employed for these studies. If the angle of His had been used as the reference line, the distribution of cardiac gland should be less than 5 mm from the true GOJ in the majority of cases, which corroborates well with the ranges described by other anatomical studies (see CQ 7 and 8).
In Europe, Siewert proposed to classify the adenocarcinomas arising in the lower oesophagus to upper stomach into three subclasses (designated as I, II and III according to the location of tumour epicentre) based on his extensive surgical experience162 286 in order to guide to selection of surgical operation. In this Siewert classification, ‘true cardia cancer’, designated as Siewert type II, was defined as a tumour with the epicentre located from 1 cm above to 2 cm below the GOJ, that is, similar to Misumi’s definition. Again, SCJ (Schleimhautgrenze: Z-line) was used as the GOJ in his report, and, hence, the range of the true cardiac-type mucosa of Siewert type II likely was overestimated in the gastric side. Furthermore, as has been discussed in the previous sections (CQ 8 and 9), the cardia mucosa consisted with pure mucous glands (excluding oxyntocardiac glands), if present, is confined within several millimetres distal to the GOJ. Thus, by adopting the concept of GOJZ adenocarcinoma, which narrows the mucosal area by 1 cm in the distal gastric side than the well-recognised Siewert type II adenocarcinoma,162 inclusion of gastric cancer should be reduced (see CQ 25 and CQ 26). Indeed, Ichikura et al proposed a new definition of ‘true cardia carcinoma’ arising within 1 cm from the GOJ (type IIA) as their nodal involvement pattern was different from the subcardia cancer (type IIB, more than 1 cm distal to GOJ).287 Therefore, GOJZ adenocarcinomas corresponding to true cardia carcinoma (type IIA) by Ichikura et al would better reflect clinical features of adenocarcinomas regarding lymphatic spread and provide clearer guidance for selecting surgical management. This new definition pertinent to the histologic evidence on the distribution of the cardia mucosa may offer a practical clinical benefit.
However, this concept would still include adenocarcinomas of heterogeneous origins; those originating from the USSBO, those from the oesophageal submucosal glands, and those from the metaplastic cardiac or oxyntocardiac epithelium and so forth. Nevertheless, this concept will provide a category for the adenocarcinomas arising from the ultrashort segment (<1 cm) columnar epithelium which many guidelines have precluded from the diagnosis of BO due to the length rule of 1 cm. As proposed in CQ 1, however, if lifting the length rule of 1 cm for the diagnosis of BO is internationally agreed on, adenocarcinomas located in the proximal half of the GOJZ should be unified as adenocarcinoma of the oesophagus arising from the Barrett’s epithelium (as defined in CQ 1) in the future.
CQ 25
Are there two distinctive aetiologies of cancer in the GOJZ?
Statement 25
There are two major distinctive aetiologies for GOJZ adenocarcinoma: GORD-related and H. pylori infection.
Agreement
Strongly agree 100%.
Agree with minor reservation 0%.
Disagree with major reservation 0%.
Strongly disagree 0%.
Quality of evidence
High 97%.
Moderate 3%.
Low 0%.
Very low 0%.
Strength of recommendation
Strong 100%.
Weak 0%.
Not applicable 0%.
Textual explanation
(see CQ 26).
CQ 26
Should cancers arising in the GOJZ be classified separately from cancers arising in the rest of the stomach?
Statement 26
Cancer arising in the GOJZ has a mixed aetiology and should be classified separately from cancers arising in the rest of the stomach that are largely due to H. pylori infection.
Agreement
Strongly agree 90%.
Agree with minor reservation 7%.
Disagree with major reservation 3%.
Strongly disagree 0%.
Quality of evidence
High 53%.
Moderate 40%.
Low 7%.
Very low 0%.
Strength of recommendation
Strong 80%.
Weak 20%.
Not applicable 0%.
Textual explanation for CQ25 and CQ26
Several studies have consistently documented the distinct pathways leading to the GOJ adenocarcinoma as defined by Siewert type II,162 based on the differences in several pathophysiological factors such as gastric acid secretion,288 reflux esophagitis or columnar metaplasia of the oesophagus,289 290 H. pylori infection,289–291 gastric atrophy288–293 and IM.291 294 Furthermore, different biological and oncogenic alterations have been observed among these tumours.295 296 This evidence strongly suggests that the adenocarcinomas arising in the GOJ have two distinct aetiologies, one associated with hypersecretion of gastric acid and reflux oesophagitis, and another with gastric acid hyposecretion and advanced gastric atrophy. It has to be remembered, however, that a subset of patients with the Siewert’s type II adenocarcinomas retained acid hypersecretion despite of H. pylori infection.297
Considering the tumour locations, it was reported that superficial adenocarcinomas located above the GOJ judged by the DEPV associated with reflux oesophagitis with lower grade of gastric atrophy while those below the junction had less reflux oesophagitis with more advanced gastric atrophy.298 This observation was supported by Uedo et al who reported that Siewert-type II adenocarcinomas at T1 stage could be separated according to the tumour location: those above the GOJ were more associated with GORD while those below the GOJ were associated with H. pylori infection and atrophy.299 Thus, adenocarcinomas arising in the proximal segment of the GOJZ had similar aetiology with OAC. In contrast, the majority of GOJZ adenocarcinomas arising from the distal segment below GOJ had more mucosal background akin to gastric adenocarcinomas caused mainly by H. pylori infection, at least in East Asia. However, simple aetiological dichotomy of the adenocarcinoma may not be appropriate. In Yamada’s report,293 81% of gastritis positive group had reflux oesophagitis, which was similar to the non-gastritis group, although SSBO in gastritis-positive group was 36%, significantly less than that of non-gastritis group (72%). In Uedo’s data, 31% of patients classified into ‘atrophy’ group were of closed types (CII and CIII), according to Kimura and Takemoto’s classification300 without endoscopic atrophy in the vicinity of GOJ. Moreover, GORD symptoms and SSBO were present in 52% and 41%, respectively, in the ‘atrophy’ group,299 indicating the reflux-induced mucosal changes occurred in a substantial proportion of the ‘atrophy’ subgroup. These findings corroborated well with the report by Inomata et al.297
Collectively, adenocarcinomas arising in the GOJ are assumed to have at least three aetiological subgroups, the first one with high gastric acid secretion accompanied with reflux in the absence of H. pylori infection, the second with high gastric acid secretion, positive reflux, mild atrophy with H. pylori infection (similar to those with duodenal ulcer) and the third with low gastric acid secretion, negative reflux and extensive gastric atrophy with positive H. pylori infection (figure 4). In patients with autoimmune gastritis with extensive corpus atrophy may be an additional subgroup belonging to the third type, but data for the neoplastic changes at GOJZ in AIG are scarce and, thus, require further study.

{kind=link}
{kind=link}
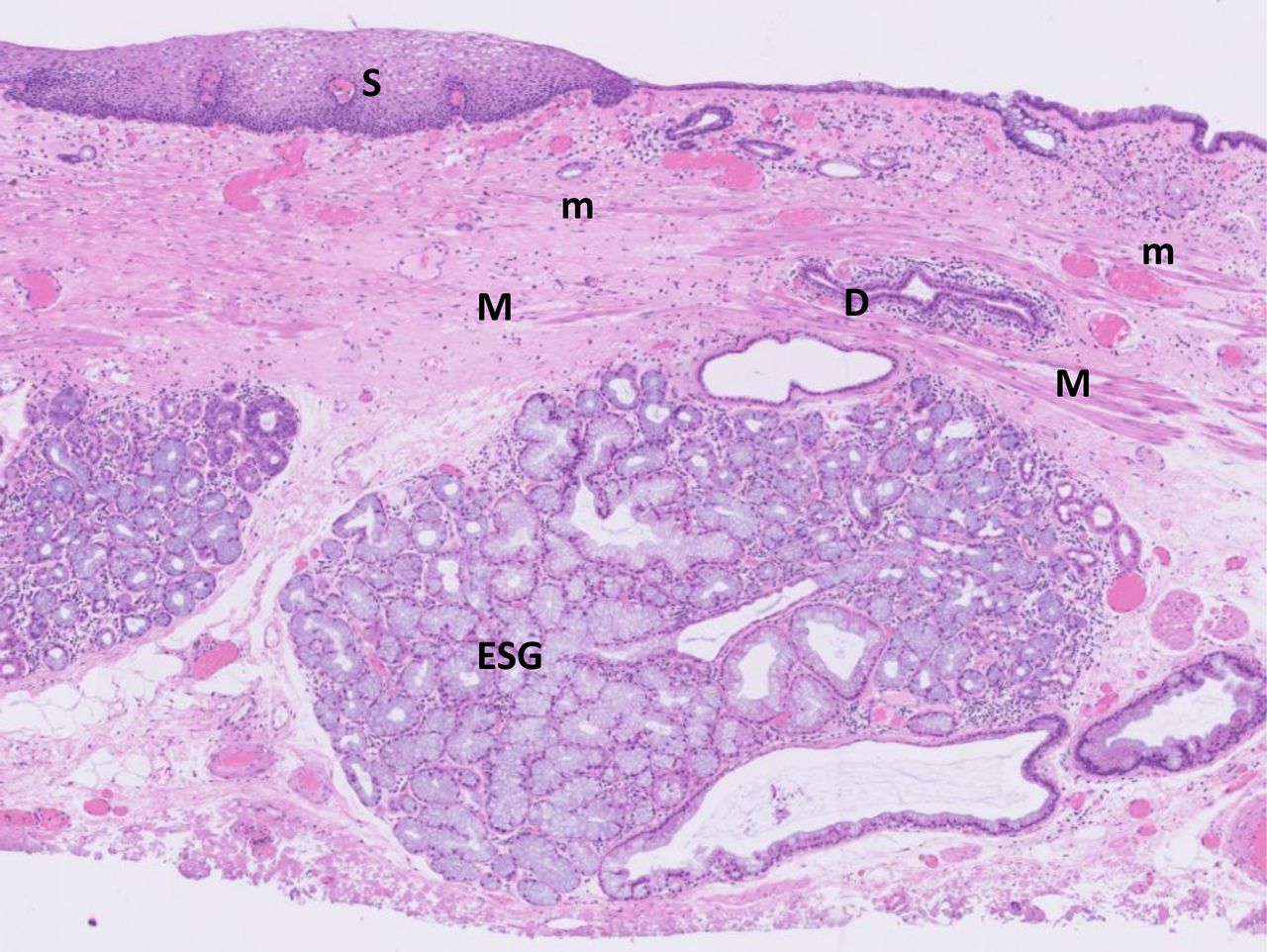{kind=link}
{kind=link}
Pathophysiological mechanisms of columnar metaplasia at the gastro-oesophageal junction zone (GOJZ). Two independent mechanisms, gastroduodenal reflux in high gastric acidity (type I) and hypo- or achlorhydria due to advanced atrophy caused by H. pylori infection (type II) were postulated for causing columnar metaplasia at the GOJZ. Type I may be subdivided further into two subtypes, gastroduodenal reflux in H. pylori-negative patients without gastric atrophy (type Ia), and gastroduodenal reflux in H. pylori-positive patients with mild gastritis limited in the antrum (type Ib). Nitrosative and oxidative stress occurring at the GOJ may also contribute the inflammation. In H. pylori-positive subjects, inflammation around the GOJ may be higher than the gastric corpus and can be a cause of atrophic and/or intestinal metaplastic change. However, more frequent pattern of gastric atrophy is pangastritis progressing from the distal stomach toward proximal direction. Theoretically autoimmune gastritis (AIG) may involve GOJZ. However, detailed investigation on histological changes at the GOJZ in AIG is scarce, and hence this hypothetical subtype is not depicted in this figure. Curved black arrows indicate reflux (gastric acid and bile acid). Vermillion areas indicate inflammations and/or metaplasia caused by these factors.
Although Siewert defined the adenocarcinoma arising from the mucosa between 1 cm above and 2 cm below the GOJ as ‘true cardia adenocarcinoma’ (Siewert type II), true cardiac mucosa was shown to span only a much narrower area than that defined by Siewert type II cancer (see CQ 8 and CQ 9). Therefore, the distal mucosa beyond this narrow area of the true cardia mucosa should be considered as the gastric fundic mucosa. Logically, the adenocarcinoma arising from the gastric mucosa should be classified as gastric cancer, not junctional adenocarcinoma nor carcinoma of the cardia. By adopting more strict definition for the adenocarcinoma arising in the GOJ (CQ 23 and CQ24), we would better delineate the aetiology of the junctional adenocarcinomas by excluding proximal gastric cancers.
CQ 27
What molecular events lead to neoplasia arising in the GOJZ?
Statement 27
Many genetic and epigenetic abnormalities have been described in GOJZ neoplasia, but the exact mechanisms remain unclear.
Agreement
Strongly agree 93%.
Agree with minor reservation 7%.
Disagree with major reservation 0%.
Strongly disagree 0%.
Quality of evidence
High 62%.
Moderate 38%.
Low 0%.
Very low 0%.
Strength of recommendation
Strong 69%.
Weak 31%.
Not applicable 0%.
Textual explanation
As described in the previous CQs, adenocarcinomas arising in GOJZ have different aetiologies and likely originate from various cancer stem cells. For this reason, no simple account on the molecular pathogenesis of the neoplasia arising in the GOJZ would be possible. However, with the advent of rapid advancement of sequencing technology, substantial data have been accumulated to analyse the molecular abnormalities of the OAC.301–310 These reports verified that alterations of p53 and p16 INK4a as the most frequent early genetic events as documented earlier.311–316 Importantly, such genetic changes were shown to be present in the Barrett’s stem cells.317 Between the two, p53 may play a more important role in the progression to cancer by underpinning the generation of clonal diversity,307 317 a significant factor for this transition. A longitudinal study also demonstrated that p53 lesions increased the risk of progression to cancer (OR=13.8 with 95% CI 3.2 to 61.0, p<0.001)), whereas p16 INK4a lesions did not.318 Interestingly, these new data revealed the presence of multiple clones with different molecular alterations in the precancerous Barrett’s epithelium303 304 even in the same patients, not to mention among the different patients, suggesting a complexity of molecular pathways leading to cancer.
Since adenocarcinomas arising from USSBO were included in some of these studies,301 305 306 310 318 we may assume that the molecular events leading to neoplasia should resemble with OAC in this subset of GOJZ adenocarcinomas. Although some differences between OAC and cancer in the cardia were noted in earlier studies,319–322 a number of genetic changes observed in the adenocarcinoma in the cardia have also been shared with OAC.304 305 Furthermore, a large-scale comparative genomic analysis of OAC revealed a similarity not only with the adenocarcinoma in the GOJ area but also with the chromosome instable subset of gastric adenocarcinoma, predominantly located in the proximal stomach.308 Another report also demonstrated similar transcriptome profiles of intestinal type of the three subtypes of GOJ adenocarcinomas defined by Siewert, in which Asian cohort was also included.309
Except for some particular chromosomal sites susceptible to DNA damages (fragile sites such as FHIT or WWOX locus),323 324 chromosomal instability occurs in a late stage of oesophageal carcinogenesis, often accompanied with gene amplification of growth factor receptors such as ERBB2 (HER2) and EGFR.303–305 324 In some cases, massive catastrophic chromosomal aberrations, such as chromothripsis and breakage-fusion-bridge events, precipitate cancerous changes.304 324 325 Similar major chromosomal aberrations were shown in the cardia cancer and associated high-grade dysplasia as well.306 308 Collectively, we may assume that the overall genetic landscape of GOJZ adenocarcinomas defined in this consensus would remain similar to that of the OAC.310
In addition to these genetic mutations and chromosomal changes, epigenetic abnormalities such as methylations have been shown in BO and OAC.308 310 326–331 Recent comprehensive methylome analyses identified multiple subtypes with distinctive relations to transcriptional and chromosomal changes,327–331 implying the presence of diverse carcinogenic routes with complex interactions between genetic and epigenetic changes. Other epigenetic changes occurring in non-coding RNA, such as miR and long non-coding RNAs, have been documented as early as the mucosa with reflux oesophagitis, which are progressively diversified from Barrett’s mucosa, dysplasia to adenocarcinoma by methylation and chromosomal number variation,332–339 adding further layer of complexity in the genetic changes leading to neoplasia.
Further investigations are required for unravelling the precise temporal relationship and causal mechanisms involved in the alterations between genetic alterations and neoplastic progression with a careful consideration on tumour localisation.
It should be of note that the role of H. pylori infection, one of the major culprits assumed to invoke inflammatory changes in the GOJZ, has not been linked to the serial genetic pathways leading to the GOJZ adenocarcinomas. Despite being a major aetiologic factor in gastric carcinogenesis, the role of H. pylori in genetic changes was ill defined across the major genetically classified subsets of gastric cancers,340 likely due to the lack of information on the infection status. Future studies on genetic changes in the GOJZ adenocarcinoma should incorporate this important aetiological factor.
CQ 28
Can IEE improve diagnostic yields of early adenocarcinoma arising in the GOJZ?
Statement 28
IEE with or without magnification is likely to improve diagnostic yields of early adenocarcinoma arising in the GOJZ.
Agreement
Strongly agree 86%.
Agree with minor reservation 14%.
Disagree with major reservation 0%.
Strongly disagree 0%.
Quality of evidence
High 59%.
Moderate 38%.
Low 3%.
Very low 0%.
Strength of recommendation
Strong 69%.
Weak 31%.
Not applicable 0%.
Textual explanation
There is no study focusing on endoscopic diagnosis of early adenocarcinoma arising in the GOJZ alone. Because GOJ is located between the distal oesophagus and the proximal stomach, the evidence obtained in the Barrett’s neoplasia and early gastric cancer would be inferred for early adenocarcinoma arising in the GOJZ. Regarding the Barrett’s neoplasia, early studies did not provide evidence for increased interobserver agreement or increased yield to identifying early neoplasia,341 a more recent meta-analysis, however, revealed IEE (both chromoendoscopy and equipment-based IEE) with or without magnification increased the diagnostic yield for detection of neoplasia by 34% in comparison with WLI.342 There was no significant difference between chromoendoscopy and equipment-based IEE in the subanalysis. The American Society for Gastrointestinal Endoscopy (ASGE) recommended acetic acid chromoendoscopy and NBI, which met the thresholds (per-patient sensitivity of >90%, negative predictive value of >98%, specificity of >80%) set by the ASGE preservation and incorporation of valuable endoscopic innovations (PIVI).343 To further enhance diagnostic reproducibility among different endoscopists, endoscopic classifications of Barrett’s neoplasia by using NBI with magnification have been established.344 345 However, the PIVI thresholds achieved by these techniques were on the diagnostic performance on detected lesions, but their capability of detecting neoplastic lesions in surveillance endoscopy was not confirmed. Indeed, Boerwinkel et al concluded that these advanced imaging techniques did not significantly increase the number of patient with a diagnosis of early neoplasia compared with high-definition white light endoscopy.346 Other IEE modalities, iScan Optical Enhancement system, BLI and LCI also demonstrated improved visualisation of neoplasia in BO,67 68 347–349 but their utility in neoplasia surveillance in BO requires further validation. In an attempt to achieve more stable, higher diagnostic performance in detecting neoplasia in patients with BO, artificial intelligence (AI) technologies have been reported,350 351 which is expected to be introduced in clinical practice in the near future.
In terms of early gastric cancer, a meta-analysis for the characterisation of early gastric cancer revealed advantages of NBI with magnification over WLI with pooled sensitivity and specificity of 0.83 versus 0.48 and 0.96 versus 0.67, respectively.352 The classification system based on surface mucosal and vessel pattern is well established.353 In recent well-designed controlled studies, however, the second-generation NBI was not superior to high-definition WL endoscopy in detecting early GC.354 355 In contrast, considerably higher performance in detecting gastric neoplasia with another IEE modality, LCI has been reported from different institutions and countries,356–358 indicating promising role of this IEE in early gastric cancer surveillance.
As shown in the detection of Barrett’s neoplasia, a number of studies have reported highly accurate diagnostic capability in the diagnosis of early gastric cancer with AI technologies,359–363 and their introduction to real clinical practice to assist endoscopists will be available soon.
Considering the limitation and difficulty in adhering to the current Seattle protocol for detecting neoplasia even in patients with a shorter length of BO,364 these AI technologies coupled with IEE are expected to facilitate the detection of neoplastic lesions arising not only in the GOJZ but also in the long-segment BO.
Discussion
A number of controversial issues regarding the GOJ area have been left unresolved until today. These include the definition of BO in terms of length criteria and of the requirement for SCE (IM), the definition of GOJ and the question on the existence of the cardia mucosa as an innate epithelium. In order to resolve these issues, a critical starting point should be the definition of the GOJ applicable to our clinical practice with endoscopic diagnosis, as we cannot determine the exact length of BO nor the extent of the cardia mucosa unless we decide the point to separate oesophagus from stomach.
Two criteria, PEGF and DEPV, have been utilised so far for the definition of the GOJ. Although these definitions have inherent shortcomings, in this consensus meeting we adopted DEPV as a more appropriate landmark for defining GOJ, since it has a more valid anatomical basis as the landmark. It has to be remembered, however, that a proper observation method with appropriate air insufflation is required to identify this landmark, often neglected in the past. Recent advanced endoscopic image enhanced technology may also facilitate the identification of this landmark. In order to facilitate the adoption of DEPV as the landmark for GOJ, an illustrative manual showing the technical details for proper observation method is planned. We hope that the feasibility of DEPV as the standard landmark of the GOJ is verified by international multicentre prospective studies with or without IEE.
Regarding the definition of BO that has been discrepant among international guidelines, we adopted a new definition in which both length definition and requirement of specialised columnar metaplasia (ie, IM) were abolished. The length threshold for diagnosis of BO has historically been changed, and the 1 cm of length threshold adopted in some of the current guidelines is set not on explicit scientific basis but on technical reasons such as poor reproducibility of the endoscopic diagnosis and dubious clinical significance. However, adenocarcinomas arising from the USSBO and/or GOJZ are increasing in Japan.365 These adenocarcinomas arising from USSBO are designated as Barrett’s adenocarcinomas in Japan and possibly in the USA (according to the AGA guidelines when IM is coexisted in the short (less than 1 cm) segment of columnar metaplasia). However, adenocarcinomas occurring in the GOJZ have been classified under GOJ adenocarcinomas separate from OAC (Barrett’s adenocarcinoma) according to the ICD-11 classification366 or IARC’s classification of digestive tract tumours.367 In this consensus meeting, we still have retained the concept of GOJZ adenocarcinoma considering internationally accepted clinical practice and disease classification systems, but theoretically adenocarcinomas arising from the USSBO should be classified under OAC in the future. As for the requirement of IM for defining BO, recent evidence indicates that columnar metaplasia without IM entails elevated risk of neoplastic changes. Problems of sampling error and inconvenience of random sampling are another reason to lift this requirement. Indeed, a very recent provocative study with sophisticated genetic analyses presented evidence that BO may originate from gastric cardia,220 a step forward to unify the proximal segment of GOJZ as BO.
In close relation to the issue of columnar metaplasia of the oesophagus is the controversy on the nature of cardiac mucosa, whether it is an innate mucosa or a metaplastic changes of oesophageal squamous epithelium. In this consensus, we agreed that cardiac epithelium with pure mucous glands does exist as an innate mucosa between squamous epithelium of the oesophagus and gastric oxyntic mucosa based on a detailed review of the literature. However, the genuine cardiac mucosa, thus defined, only spans less than 10 mm, and may not be circumferential in some cases. Therefore, the cardia cancer, most widely adopted definition by Siewert type II, which included adenocarcinomas located 2 cm distal to the SCJ, need to be redefined in order to avoid inclusion of the proximal gastric cancers in this category. Therefore, the distal range from the GOJ (defined as DEPV) of adenocarcinomas arising from the subjunctional mucosa was decreased to 1 cm. In clinical practice, however, it is often difficult to identify the precise mucosal origin of the adenocarcinomas of the GOJ, we propose the concept of GOJZ spanning 1 cm proximal and 1 cm distal to the GOJ and adenocarcinomas arising from the GOJZ as GOJZ adenocarcinomas. As mentioned previously, this GOJZ adenocarcinoma can develop from several cellular origins, such as metaplastic oesophageal mucosa, oesophageal cardiac glands, oesophageal submucosal glands, genuine cardia glands, transitional oxyntocardiac glands and metaplastic oxyntic mucosa. Further refined definition of GOJZ adenocarcinomas, in particular, separation of Barrett’s adenocarcinomas from this concept should be addressed to avoid duplication. Nevertheless, this new definition of GOJZ adenocarcinomas will better serve to clarify aetiological factors contributing to neoplasia arising at this particular zone, by principally eliminating proximal gastric cancers due to H. pylori infection. At present, we admit that adoption of new concept of GOJZ requires wider recognition and practice implementation. For which, it is planned that this concept is discussed at the consensus meeting held at the 15th international gastric cancer congress 2023. As for the major pathoaetiological factors, gastroduodenal reflux, nitrosative stresses and microbiota including H. pylori infections have been proposed. Although advanced atrophy caused by H. pylori can contribute to proximal gastric cancer, a majority of them may be excluded by this new concept. However, two lines of evidence showing that the metaplastic changes can take place in the cardia region independent from the distal stomach, and H. pylori can infect metaplastic oesophageal mucosa suggest that three major pathoaetiologies, hyperacidity with reflux and/or oxy- and nitrogen-radicals, hyperacidity and H. pylori infection and hypoacidity due to advanced atrophy caused by H. pylori infection. Thus, the conventional idea that H. pylori infection might be protective in the development of BO is too simplistic, since acid hypersecretion similar to the situation seen in duodenal ulcer can take place in H. pylori infection and damage the GOJ mucosa. It is also possible that other microbiota may contribute to the inflammation and progression to neoplastic transformation of this zone.
Considering the remarkable advancement of imaging technology combined with AI, this will facilitate identification of dysplastic changes or early cancers arising from the GOJZ which can be managed with minimally invasive endoscopic therapy. It is important for all the endoscopists to describe the exact location of the neoplasms in relation to GOJ, presence or absence of BO, and aetiological factors such as GORD, gastric mucosal atrophy, and H. pylori as described above.
Although major issues have been resolved by this interdisciplinary expert consensus, the concepts adopted, and their usefulness, await further validation in the real world. In other words, we recognised a huge area of interesting research themes regarding the issues surrounding the GOJZ are wide open to us. Thus, we do hope this consensus document will play a role in promoting our understanding of the complex pathophysiology of the GOJZ, thorough which better prevention and management on the diseases in the GOJZ can be offered.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
Authors are indebted to Drs Junichi Akiyama, Chika Kusano, Sachiyo Nomura, Yuto Shimamura and Shizuki Takemura for their excellent clerkship for recording the documents at the consensus meeting. We also thank Ms. Emiko Dan and Mr. Hiroyuki Yasui, of the Organization of Japan Digestive Disease Week for their business support, and Mr. Masayoshi Umemura and Mr. Kenya Morimoto of Omura Printing Co. Ltd for developing the internet-based voting system. Excellent secretarial and operation support given by Ms. Hiroko Eto, Ms. Aki Iiyama and Mr Tadashi Komada from Japan Convention Services Inc. is greatly appreciated.
References
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @emadelomar
Contributors KS and MK planned and organised the meeting. PM, KELM, EME-O rearranged the CQ and statements prepared by the Japanese faculty members. Japanese faculty members did literature search and wrote the draft the statements for their allocated CQs. KS finalised the whole manuscript from the drafts prepared by the Japanese faculty members and updated the literature except textural explanation for CQ1, which was jointly written with SJS. All the authors contributed to develop consensus document by voting and providing their comments. They also contributed to revise the manuscript prepared by KS by constructive proposals. SJS and EME-O did editing of the manuscript.
Funding The cost of this meeting was provided by the fund from the APDW meeting in Kobe 2016 deposited to the account of the Organization of JDDW. We also thank Professor Daniel Sifrim, The London School of Medicine and Dentistry Queen Mary, University of London, Professor Nicholas J Shaheen, University of North Caroline School of Medicine and Professor Parakrama Chandrasoma, University of Southern California Medical Center for their contributions during the consensus development.
Competing interests KS serves as an advisor for Fujifilm Medical Co. and received a lecture fee from Fujifilm Medical Co. MF received lecture fee from Olympus Medical Systems Co. and Fujifilm Medical Co. He also received research grant from Olympus Medical Systems Co, Fujifilm Medical Co. and HOYA Pentax Co. HI serves as an advisor for Olympus Medical Systems Co. HM received a lecture fee from Fujifilm Medical Co. GT and HT received lecture fees from Olympus Medical Co. and Fujifilm Medical Co. Other authors have declared no competing interests regarding this manuscript
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.