Article Text

Abstract
Objective Antitumour necrosis factor (TNF) drugs impair serological responses following SARS-CoV-2 vaccination. We sought to assess if a third dose of a messenger RNA (mRNA)-based vaccine substantially boosted anti-SARS-CoV-2 antibody responses and protective immunity in infliximab-treated patients with IBD.
Design Third dose vaccine induced anti-SARS-CoV-2 spike (anti-S) receptor-binding domain (RBD) antibody responses, breakthrough SARS-CoV-2 infection, reinfection and persistent oropharyngeal carriage in patients with IBD treated with infliximab were compared with a reference cohort treated with vedolizumab from the impaCt of bioLogic therApy on saRs-cov-2 Infection and immuniTY (CLARITY) IBD study.
Results Geometric mean (SD) anti-S RBD antibody concentrations increased in both groups following a third dose of an mRNA-based vaccine. However, concentrations were lower in patients treated with infliximab than vedolizumab, irrespective of whether their first two primary vaccine doses were ChAdOx1 nCoV-19 (1856 U/mL (5.2) vs 10 728 U/mL (3.1), p<0.0001) or BNT162b2 vaccines (2164 U/mL (4.1) vs 15 116 U/mL (3.4), p<0.0001). However, no differences in anti-S RBD antibody concentrations were seen following third and fourth doses of an mRNA-based vaccine, irrespective of the combination of primary vaccinations received. Post-third dose, anti-S RBD antibody half-life estimates were shorter in infliximab-treated than vedolizumab-treated patients (37.0 days (95% CI 35.6 to 38.6) vs 52.0 days (95% CI 49.0 to 55.4), p<0.0001).
Compared with vedolizumab-treated, infliximab-treated patients were more likely to experience SARS-CoV-2 breakthrough infection (HR 2.23 (95% CI 1.46 to 3.38), p=0.00018) and reinfection (HR 2.10 (95% CI 1.31 to 3.35), p=0.0019), but this effect was uncoupled from third vaccine dose anti-S RBD antibody concentrations. Reinfection occurred predominantly during the Omicron wave and was predicted by SARS-CoV-2 antinucleocapsid concentrations after the initial infection. We did not observe persistent oropharyngeal carriage of SARS-CoV-2. Hospitalisations and deaths were uncommon in both groups.
Conclusions Following a third dose of an mRNA-based vaccine, infliximab was associated with attenuated serological responses and more SARS-CoV-2 breakthrough infection and reinfection which were not predicted by the magnitude of anti-S RBD responses, indicative of vaccine escape by the Omicron variant.
Trial registration number ISRCTN45176516.
- infliximab
- COVID-19
- inflammatory bowel disease
- vedolizumab
- immunosuppression
- vaccination
- biological
Data availability statement
Data are available on reasonable request. The study protocol including the statistical analysis plan is available at www.clarityibd.org. Individual participant de-identified data that underlie the results reported in this article will be available immediately after publication for a period of 5 years. The data will be made available to investigators whose proposed use of the data has been approved by an independent review committee. Analyses will be restricted to the aims in the approved proposal. Proposals should be directed to tariq.ahmad1@nhs.net; to gain access data requestors will need to sign a data access agreement.
This article is made freely available for personal use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Vaccine-induced anti-SARS-CoV-2 spike (anti-S) receptor-binding domain (RBD) antibody responses are attenuated and less durable in infliximab-treated than vedolizumab-treated patients with IBD.
During the delta wave of the COVID-19 pandemic, breakthrough SARS-CoV-2 infection was more common in infliximab-treated than vedolizumab-treated patients, and were associated with lower anti-S RBD antibody concentrations following two doses of SARS-CoV-2 vaccines.
Higher, more sustained antibody concentrations are observed in patients with a history of SARS-CoV-2 infection prior to vaccination, but whether infliximab treatment is linked to increased risk of SARS-CoV-2 reinfection is unknown.
WHAT THIS STUDY ADDS
A third dose of a messenger RNA (mRNA)-based vaccine substantially boosted anti-S RBD antibody responses in infliximab-treated and vedolizumab-treated patients; however, anti-S RBD antibody concentrations remained attenuated in patients treated with infliximab, irrespective of the combination of primary vaccinations received.
There was a diminishing return on anti-S RBD antibody responses with a fourth dose of an mRNA-based vaccine, irrespective of biological type or combination of primary vaccinations received.
Breakthrough infection after a third dose of an mRNA-based vaccine was more common and occurred earlier in infliximab-treated than in vedolizumab-treated patients.Breakthrough infection was not associated with the magnitude of post-third dose vaccine anti-S RBD antibody concentrations.
Reinfection with the B.1.1.529 (Omicron) variant was more common in patients treated with infliximab, compared with vedolizumab, and was predicted by SARS-CoV-2 antinucleocapsid concentrations after initial infection. We did not observe persistent oropharyngeal carriage.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Despite Omicron variant breakthrough infection, vaccines continue to protect against severe illness, hospitalisations and death in infliximab-treated and vedolizumab-treated patients with IBD.
A current correlate of protection from B.1.1.529 (Omicron) infection is unknown and at present there is no role for routine antibody concentration testing against ancestral anti-S RBD.
Vaccination regimens for patients treated with antitumour necrosis factor (TNF) therapy should include at least one dose of an existing mRNA vaccine and booster vaccine doses need to be administered every 4–6 months.
Anti-TNF-treated patients have attenuated responses to vaccination and are at increased risk of breakthrough infection. Whether, in the setting of novel variants of concern, this will translate to an increased risk of severe COVID-19 is unknown.
Introduction
The COVID-19 pandemic has been characterised by successive waves of more transmissible SARS-CoV-2 variants of concern (VOC), culminating most recently in B.1.1.529 (Omicron) and its subvariants BA.2–5 that are able to evade adaptive immunity following prior infection and vaccination. The B.1.1.529 (Omicron) variant of SARS-CoV-2 was designated a variant of concern by WHO on 26 November 2021,1 and BA.4 and BA.5 are now the dominant variants in the UK and are spreading rapidly worldwide. Compared with the ancestral Wuhan strain, B.1.1.529 has >32 mutations including 15 in the spike receptor binding domain (RBD).2 Current COVID-19 vaccines continue to protect against severe illness, hospitalisations and death.3 However, the B.1.1.529 variant is causing high numbers of SARS-CoV-2 breakthrough infection and reinfection because of antigenic escape.4
By suppressing immune responses, immunosuppressive therapies, including biologicals, increase the risk of SARS-CoV-2 infection, persistent nasopharyngeal carriage and viral evolution.5 6 We have recently shown that treatment with the antitumour necrosis factor (TNF) therapies, infliximab and adalimumab, impairs antibody responses following SARS-CoV-2 infection.7 8 Furthermore, we demonstrated vaccine-induced antibody responses are attenuated and less durable in patients treated with infliximab, translating to a 50% increased risk of breakthrough SARS-CoV-2 infection, compared with patients treated with vedolizumab, a gut-selective anti-integrin α4β7 monoclonal antibody.9–11
For patients with IBD treated with immunosuppressive therapies, these findings, along with data from other immunosuppressed patient cohorts,11–13 provided evidence for the prioritisation of third primary SARS-CoV-2 vaccine doses,14 even before the emergence of the B.1.1.529 (Omicron) variant.
We sought to assess if a third dose of an mRNA-based vaccine substantially improved anti-SARS-CoV-2 antibody responses, and if infliximab-treated compared with vedolizumab-treated patients are at increased risk of SARS-CoV-2 breakthrough infection, reinfection or persistent oropharyngeal carriage.
Methods
Study design, population and clinical setting
CLARITY IBD is a UK-wide, multicentre, observational cohort study investigating the impact of biological and/or concomitant immunomodulators on SARS-CoV-2 acquisition, illness and immunity in patients with IBD (www.clarityibd.org).
The overarching aims, study design and sample size calculations have been described previously.8 9 In brief, 7224 consecutive patients were recruited at the time of attendance at infusion units between 22 September 2020 and 23 December 2020 (online supplemental table 1). Patients with a diagnosis of IBD, aged 5 years and over, treated with infliximab or vedolizumab were eligible for inclusion. Follow-up visits coincided with biological infusions and typically occurred 8 weekly.
Supplemental material
Data were linked by National Health Service (NHS) number or Community Health Index to NHS England, Public Health England, Scotland and Wales data who hold dates of vaccine uptake and dates and results of SARS-CoV-2 PCR tests undertaken in the UK. When central data on vaccination were missing, we used patient reports. The alpha and B.1.1.529 (Omicron) variants are characterised by an S-gene deletion which leads to loss of one of the three gene targets employed in the SARS-CoV-2 Taq Path PCR assay15 used by most UK public health laboratories. Therefore, S-gene target failure can be used as a marker of infection with the alpha or the B.1.1.529 (Omicron) subvariants.
In the UK, vaccines were administered to the most clinically vulnerable, and then through progressively lower risk and younger age groups from December 2020. Citizens received either the mRNA-based vaccine, BNT162b2 or the adenovirus-vector vaccine, ChAdOx1 nCoV-19 for the first two doses. From 13 September 2021, patients deemed to be clinically extremely vulnerable, including those with IBD treated with anti-TNF therapies and vedolizumab were offered a third and fourth primary vaccine dose with an mRNA-based vaccine (either BNT162b2 (Pfizer-BioNTech) or mRNA-1273 (Moderna)) at least 8 weeks after their second dose.14
Here, we report anti-SARS-CoV-2 antibody responses after a third primary and fourth dose with an mRNA-based vaccine, rates of SARS-CoV-2 breakthrough infection and reinfection and persistent oropharyngeal carriage.
Outcomes
Participants were eligible for our immunogenicity analysis if they had an anti-SARS-CoV-2 spike (anti-S) RBD antibody test between 14 and 70 days after a third and fourth vaccine dose with an mRNA-based vaccine.
Anti-SARS-CoV-2 antibody assays
To determine antibody responses specific to vaccination, we used the Roche Elecsys anti-S immunoassay alongside the nucleocapsid (N) immunoassay.16 17 This double sandwich electrochemiluminescence immunoassay uses a recombinant protein of the RBD on the spike protein as an antigen for the determination of antibodies against SARS-CoV-2. Sample electrochemiluminescence signals are compared with an internal calibration curve and quantitative values are reported as units (U)/mL, which are identical to WHO’s International Standard (binding antibody units/mL).18
The Roche Elecsys anti-SARS-CoV-2 (N) immunoassay is a sandwich electrochemiluminescence immunoassay that uses a recombinant protein of the nucleocapsid antigen for determination of antibodies against SARS-CoV-2 infection. Using a cut-off index (COI) of 1, the manufacturer reports clinical sensitivity and specificity of 99.5% (95% CI 97.0 to 100) and 99.8% (95% CI 99.7 to 99.9), respectively, >14 days after PCR-confirmed COVID-19. We have previously reported that anti-N antibody responses following SARS-CoV-2 natural infection are impaired in patients treated with infliximab compared with vedolizumab.8 As such, a threshold of 0.12 COI was set using receiver operator characteristic curve and area under the curve analysis of anti-N antibody results from participants 2 weeks following a PCR-confirmed infection to maximise sensitivity and specificity, beyond which patients were deemed to have had prior SARS-CoV-2 infection.
Breakthrough SARS-CoV-2 infection
SARS-CoV-2 infection was defined by a positive PCR test to SARS CoV-2. Breakthrough infection was defined as a SARS CoV-2 infection, diagnosed by positive PCR test, >14 days after a third dose of a SARS-CoV-2 vaccine.
Reinfection with SARS-CoV-2 and persistent oropharyngeal carriage
We defined SARS-CoV-2 reinfection as a recurrence of symptoms compatible with COVID-19, accompanied by a positive PCR test, >90 days after the onset of the primary infection.19
Because PCR positivity may persist for prolonged periods following initial infection and asymptomatic carriage is common, it is difficult to differentiate reinfection from persistent oropharyngeal carriage. To assess the risk of persistent carriage, participants aged 18 years and over with a previous history of confirmed SARS-CoV-2 infection, but without ongoing symptoms, were invited to carry out a home buccal swab test between 20 May 2021 and 7 January 2022.
We used PCR to detect SARS-CoV-2 RNA, and in positive samples, for the presence of envelope (E) and subgenomic RNAs (sgRNA).20 sgRNAs are generated after SARS-CoV-2 enters cells and are poorly incorporated into mature virions and can be used as marker for actively replicating, rather than inactivated or neutralised, virus. Methods have been reported previously.20 In brief, RNA was extracted using the Chemagic Viral DNA/RNA Kit on the Chemagic 360D platform. Viral loads were measured by quantitative real-time PCR for E gene and E-gene-derived sgRNA sequences, respectively. Reactions were performed using the SuperScript One-Step RT-PCR System with Platinum Taq DNA Polymerase (Thermo Fisher, Waltham, USA). Reactions were carried out in 384 well plates on the QuantStudio 12K Flex Real-Time PCR System (Applied Biosystems, Foster City, USA). Probes and primers were obtained from Thermo Fisher (Waltham, USA). E gene and E sgRNA viral loads were determined in relation to known quantities of synthetic standards by standard curve analysis. Synthetic standards consisted of the probe and primer binding sites in a single long oligonucleotide for each of E gene and E gene-derived sgRNA sequences and were obtained from Invitrogen (Waltham, USA).
Variables
Variables recorded by participants were demographics (age, sex, ethnicity, comorbidities, height and weight, smoking status and postcode), IBD disease activity (PRO2), SARS-CoV-2 symptoms aligned to the COVID-19 symptoms study (symptoms, previous testing and hospital admissions for COVID-19) and vaccine uptake (type and date of primary vaccination). Study sites completed data relating to IBD history (age at diagnosis, disease duration and phenotype according to the Montreal classifications), previous surgeries and duration of current biological and immunomodulator therapy, COVID-19 hospitalisations and deaths. Data were entered electronically into a purpose-designed Research Electronic Data Capture database hosted at the Royal Devon and Exeter NHS Foundation Trust.21 Participants without access to the internet or electronic device completed their questionnaires on paper case record forms that were subsequently entered by local research teams.
Statistical analysis
Statistical analyses were undertaken in R V.4.1.2 (R Foundation for Statistical Computing, Vienna, Austria). All tests were two-tailed and p values <0.05 were considered significant. We included patients with missing clinical variables in analyses for which they had data and have specified the denominator for each variable. Continuous data are reported as median and IQR, and discrete data as numbers and percentages.
Anti-S RBD antibody concentrations are reported as geometric means and SD. T-tests of log-transformed anti-S RBD antibody concentrations were used to compare antibody responses by vaccine type, biological drug type, breakthrough infection and reinfection status. Multivariable linear regression models were used to identify factors independently associated with log anti-S RBD concentration. Based on our previous findings,9 10 a priori, we included age, ethnicity, biological medication and immunomodulator use. Results are presented after exponentiation, so that the coefficients of the model correspond to the fold change (FC) associated with each binary covariate. For age, a cut-off of>60 years was chosen based on graphical inspection of the relationship between age and anti-S RBD antibody concentrations.
We visualised durability of antibody responses by calculating 15-day rolling geometric mean anti-S RBD antibody concentrations. Anti-S RBD antibody half-lives were estimated using an exponential model of decay. Linear mixed models were fit using the lme4 and lmerTest package, with biological treatment and vaccine type as fixed effects and each subject as a random effect. CIs were calculated using likelihood ratios. P values for comparison of half-lives were estimated from the full linear mixed effects model that incorporated vaccine, biological drug and prior SARS-CoV-2 infection status.
Kaplan-Meier curves and Cox proportional hazard regression models were used to identify treatment and vaccine-related factors associated with time to breakthrough infection and reinfection. Multivariable logistic regression analysis was used to identify factors associated with hospitalisation among those with a positive SARS-CoV-2 PCR across the pandemic. Where appropriate, the same analyses were used to compare antibody responses in participants with PCR evidence of SARS-CoV-2 infection at any time prior to vaccination.
Ethics and role of the funding source
CLARITY IBD is an investigator-led, UK National Institute for Health Research COVID-19 urgent public health study, funded by the Royal Devon and Exeter NHS Foundation Trust, Hull University Teaching Hospital NHS Trust, NIHR Imperial Biomedical Research Centre, Crohn’s and Colitis UK (M2021/1), Guts UK and by unrestricted educational grants from F. Hoffmann-La Roche (Switzerland), Biogen (USA), Celltrion Healthcare (South Korea), Takeda (UK) and Galapagos (Belgium). This study was supported by an NCSi programme UKRI award to RB, DA, NP and TA (MR/W020610/1). None of our funding bodies had any role in study design, data collection or analysis, writing or decision to submit for publication.
The sponsor was the Royal Devon and Exeter NHS Foundation Trust. The protocol is available online at https//www.clarityibd.org. The study was registered with the ISRCTN registry, ISRCTN45176516.
Results
Patient characteristics
Between 22 September 2020 and 23 December 2020, 7224 patients were recruited to the CLARITY study from 92 UK hospitals. In our primary immunogenicity analyses, we included 918 infliximab-treated and 442 vedolizumab-treated participants without a history of prior SARS-CoV-2 infection, who had received uninterrupted biological therapy since recruitment and had an antibody test between 14 and 70 days after a third dose with an mRNA-based SARS-CoV-2 vaccine. Participant characteristics are shown in table 1. Additional analyses are presented for 512 infliximab-treated and 185 vedolizumab-treated participants with a history of SARS-CoV-2 infection before the third vaccine dose (table 2).
Baseline characteristics of participants without a history of prior SARS-CoV-2 infection, who received uninterrupted biological therapy since recruitment and had an antibody test between 14 and 70 days after a third dose with an mRNA-based SARS-CoV-2 vaccine
Baseline characteristics of participants with a history of prior SARS-CoV-2 infection, who received uninterrupted biological therapy since recruitment and had an antibody test between 14 and 70 days after a third dose with an mRNA-based SARS-CoV-2 vaccine
Anti-SARS-CoV-2 (S) antibody level following third COVID-19 vaccine
The peak geometric mean (SD) anti-S RBD antibody concentration was higher in recipients of three doses of an mRNA-based vaccine than recipients of two ChAdOx1 nCoV-19 vaccines and a third dose with an mRNA-based vaccine (4085 U/mL (5.1) vs 3275 U/mL (5.5), p=0.016). Geometric mean (SD) anti-S RBD antibody FC between peak antibody concentrations after second and third vaccine doses was greater in recipients of two ChAdOx1 nCoV-19 vaccines, followed by a third dose with an mRNA-based vaccine, compared with recipients of three mRNA-based vaccine doses (FC 11.1 (4.0) vs FC 3.7 (4.1)), p<0.0001 (figure 1).

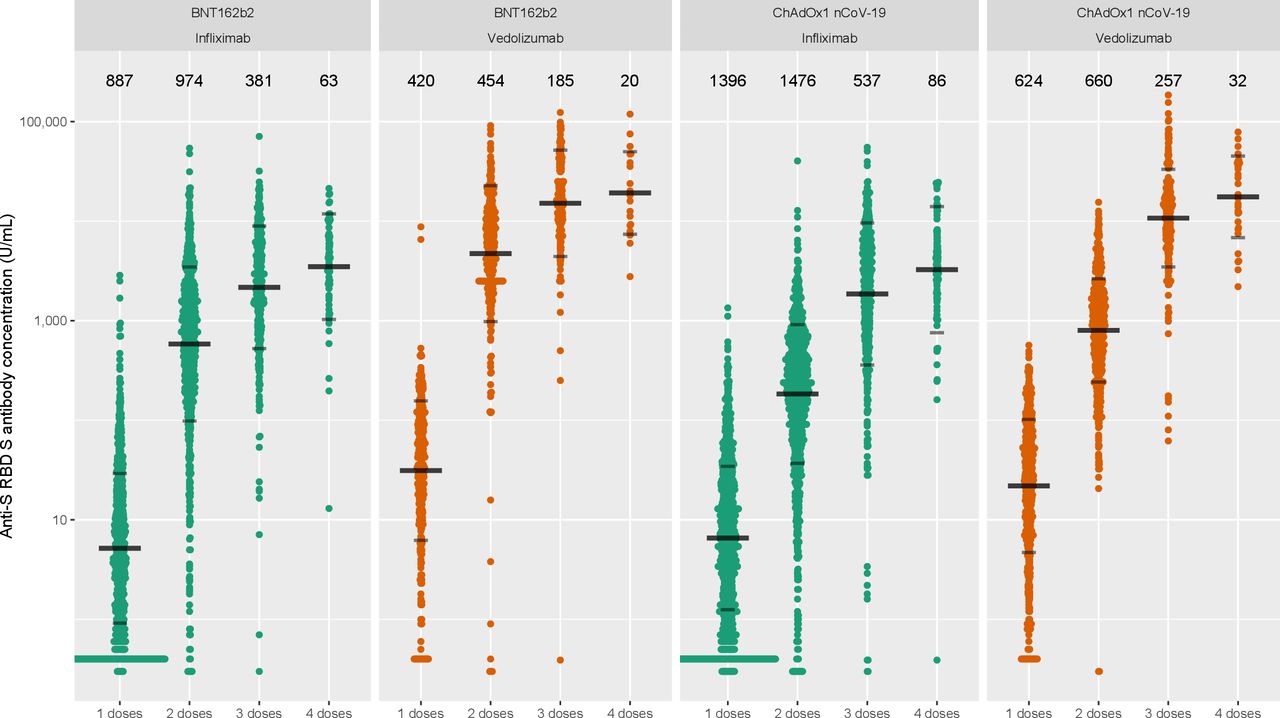
Anti-SARS-CoV-2 spike (anti-S) receptor-binding domain (RBD) antibody concentration stratified by biological therapy (infliximab vs vedolizumab) and type of vaccine. The wider bar represents the geometric mean, while the narrower bars are drawn one geometric SD either side of the geometric mean. The biological treatment infliximab is shown in green and vedolizumab in orange. The number of individuals tested for each group are shown in black at the top of each panel.
Anti-S RBD antibody concentrations were lower in infliximab-treated than vedolizumab-treated patients following a third dose with an mRNA-based vaccine (1978 U/mL (4.7) vs 12 384 U/mL (3.3), p<0.0001), irrespective of whether they had received their first two vaccine doses with the ChAdOx1 nCoV-19 (1856 U/mL (5.2) vs 10 728 U/mL (3.1), p<0.0001) or BNT162b2 vaccines (2164 U/mL (4.1) vs 15 116 U/mL (3.4), p<0.0001) (figure 2).

Rolling geometric mean anti-SARS-CoV-2 spike (anti-S) receptor-binding domain (RBD) antibody concentration over time from the date of the first dose of the SARS-CoV-2 vaccine (week 0) stratified by biological therapy (infliximab vs vedolizumab), vaccine and history of prior SARS-CoV-2 infection. Geometric means are calculated using a rolling 15-day window (ie, 7 days either side of the day indicated). The shaded areas represent the 95% CIs of the geometric means. Each dose of SARS-CoV-2 vaccine is marked out by vertical grey lines and annotated at the bottom of each panel. The biological treatment infliximab is shown in green and vedolizumab is shown in orange. The top panels represent those without prior infection and the bottom panels represent those who have had a prior infection.
Multivariable linear regression analyses in patients without prior SARS-CoV-2 infection confirmed that antibody concentrations were reduced 5.5-fold in infliximab-treated compared with vedolizumab-treated patients after a third dose with an mRNA-based vaccine (FC 0.18 (95% CI 0.15 to 0.21), p<0.0001) (figure 3). Age ≥60 years and methotrexate use were also independently associated with lower anti-S RBD antibody concentrations. Receipt of three doses of an mRNA-based vaccine and a longer interval between second and third vaccine doses were associated with higher anti-S RBD antibody concentrations.

Exponentiated coefficients of linear regression models of log anti-SARS-CoV-2 spike (anti-S) receptor-binding domain (RBD) antibody concentration after a third dose with a messenger RNA-based vaccine. The resultant values represent the fold change of antibody concentration associated with each variable. IBDU, IBD unclassified.
In patients without prior infection, anti-S RBD antibody half-life estimates were shorter in infliximab-treated than vedolizumab-treated patients following three doses of a SARS-CoV-2 vaccine: 37.0 days (95% CI 35.6 to 38.6) vs 52.0 days (95% CI 49.0 to 55.4), respectively. Antibody concentrations following a third vaccine dose were higher in patients with a prior history of SARS-CoV-2 infection (online supplemental figure 1). Among patients with a history of SARS-CoV-2 infection at any point before third vaccination dose, geometric mean (SD) anti-S RBD antibody concentrations were lower in infliximab-treated compared with vedolizumab-treated patients after third vaccination with an mRNA-based vaccine (4059 U/mL (4.7) vs 18 788 U/mL (3.0), p<0.0001).
Anti-SARS-CoV-2 (S) antibody level following fourth COVID-19 vaccine
Anti-S RBD antibody concentrations were lower in infliximab-treated than vedolizumab-treated patients following a fourth dose with an mRNA-based vaccine (3353 U/mL (3.9) vs 18 152 U/mL (2.6), p<0.0001), irrespective of whether they had received two doses of ChAdOx1 nCoV-19 (3257 U/mL (4.3) vs 17 535 U/mL (2.6), p<0.0001) or BNT162b2 (3489 U/mL (3.4) vs 19 183 U/mL (2.6), p<0.0001) vaccines first (figure 1). There was no difference between geometric mean (SD) anti-S RBD peak antibody concentrations following third and fourth doses of an mRNA-based vaccine, irrespective of the combination of primary vaccinations received (figure 2).
Breakthrough SARS-CoV-2 infection following three doses of vaccine
Incident SARS-CoV-2 infection across the entire CLARITY IBD cohort are shown in figure 4. Overall, 15.0% (393/2619 (95% CI 13.6% to 16.4%)) patients had a breakthrough infection after the third vaccine dose. S-gene target failure, indicative of infection with the B.1.1.529 (Omicron) variant, was observed in 74.9% (128/171) of those patients with breakthrough infection for whom PCR gene detection patterns were available.

Proportion of patients with SARS-CoV-2 infection, stratified by biological therapy (infliximab vs vedolizumab) and S-gene target failure (SGTF) over time. Proportion of PCR-positive SGTF infection shown in orange.
Univariable factors associated with time to breakthrough infection are shown in online supplemental table 2. Younger age, infliximab treatment, concomitant thiopurine and lack of exposure to steroids were associated with a shorter time to breakthrough infection. In a multivariable model including anti-S RBD antibody concentrations, infliximab treatment, compared with vedolizumab treatment, and younger age, but not antibody responses, were significantly associated with a shorter time to breakthrough infection (figure 5).
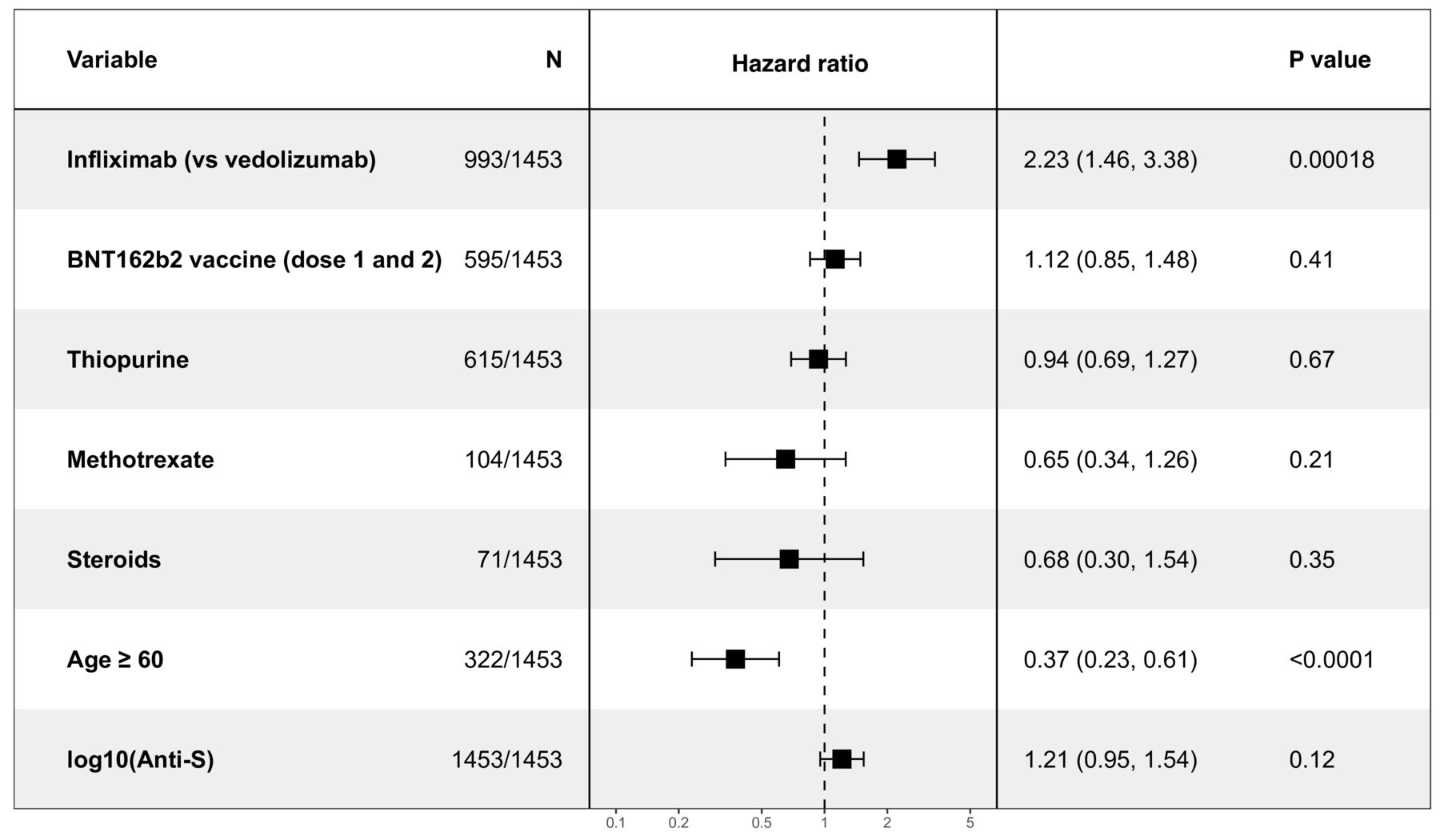
Coefficients of cox proportional hazards models of time to breakthrough infection after a third dose with a messenger RNA-based vaccine. The resultant values represent the hazard ratio for breakthrough infection associated with each variable.
SARS-CoV-2 reinfection and persistent carriage
In our analyses of reinfection, we included 757 infliximab-treated and 274 vedolizumab-treated participants who had at least 91 days of follow-up following a first positive PCR test while treated with their original biological. Overall, 12.5% (129/1031 (95% CI 10.5% to 14.7%)) patients had a reinfection with SARS-CoV-2. S-gene target failure was observed in 83.6% (56/67) patients for whom PCR gene detection patterns were available.
Time to reinfection was shorter in infliximab-treated than vedolizumab-treated patients (HR 2.10, 95% CI 1.31 to 3.35, p=0.0019). Reinfection was associated with SARS-CoV-2 anti-N antibody level 2–10 weeks after the first PCR-confirmed infection. For every 10-fold rise in anti-N RBD antibody concentration, we observed a 0.73-fold (95% CI 0.56 to 0.95, p=0.02) reduction in hazard of reinfection. Reinfection was not associated with SARS-CoV-2 anti-S antibody level 2–10 weeks after the third vaccine dose.
Of note, 3.1% (68/2185) participants with an initial positive SARS-CoV-2 PCR had a further positive test between 15 and 90 days later. To investigate whether participants shed replication-competent virus beyond 14 days, 207 adult patients with SARS-CoV-2 infection (positive RT-PCR from nasopharyngeal swabs) within the previous 90 days were sent kits in the post to carry out a home buccal swab test for a SARS-CoV-2 RT-PCR. One hundred sixty-eight patients returned the kits and three were positive for SARS-CoV-2, 16, 26 and 28 days after a positive PCR test. None of these samples tested positive for E gene or E gene-derived subgenomic RNA indicating non-replicating virus.
Overview of all COVID-19 infections, hospitalisations and deaths in the CLARITY cohort
In a Cox proportional hazards model of all infections across the entire CLARITY cohort, there were independent protective effects of prior infection and vaccination on the risk of SARS-CoV-2 infection. We observed a significant interaction between biological use and vaccination, whereby the protective effect of vaccination on the risk of infection was reduced in patients treated with infliximab compared with vedolizumab, irrespective of vaccine type (figure 6). No interaction was seen between biological type and the protective effect of prior infection (figure 7).

Kaplan-Meier graphs comparing the time to PCR-confirmed SARS-CoV-2 infection following a third dose of vaccine, stratified by biological therapy and vaccine type. Infliximab-treated patients are represented in green (those who received BNT162b2 for their first two doses) and purple (those who received ChAdOx1 nCoV-19 for their first two doses), and vedolizumab-treated patients in orange (those who received BNT162b2 for their first two doses) and pink (those who received ChAdOx1 nCoV-19 for their first two doses). The number of participants at each time point are displayed in black at the bottom of each figure. P values are calculated using log-rank test.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cox proportional hazards model of factors associated with the risk of SARS-CoV-2 infection. The resultant values represent the HR of the risk of developing SARS-CoV-2 infection for each variable independently, and the interaction between biological treatment and prior infection, and biological treatment and each vaccine dose.
Overall, 26/2186 (1.2%) patients had been hospitalised with COVID-19 after a median of 2.5 (IQR 0–8) days following a positive PCR test. Univariable analyses demonstrated that hospitalisation was associated with treatment with vedolizumab, older age, higher BMI, comorbid heart disease, diabetes, lung disease and cancer and having had fewer than two vaccine doses. Multivariable logistic regression confirmed that hospitalisation with COVID-19 was independently associated with older age (per decade: OR 1.69, 95% CI 1.28 to 2.25, p<0.0001) and a history of cancer (OR 113.63, 95% CI 14.12 to 1125.64, p<0.0001), whereas having at least two doses of SARS-CoV-2 vaccine (OR 0.24, 95% CI 0.10 to 0.56, p=0.0011) was protective (online supplemental figure 2).
There were 15 deaths in the CLARITY cohort, 3 were due to COVID-19. Two deaths occurred in unvaccinated participants and one in a participant who had received two vaccine doses. The vaccinated patient had no comorbidities and received his last vedolizumab dose 3 weeks prior to testing positive for SARS-CoV-2.
Discussion
Key results
After primary vaccination, anti-SARS-CoV-2 spike antibody concentrations were highest in the recipients of three doses of an mRNA-based vaccine. Infliximab treatment was associated with attenuated, less durable anti-SARS-CoV-2 antibody responses and a twofold increase in subsequent breakthrough SARS-CoV-2 infection. Unlike earlier in the pandemic, during the B.1.1.529 (Omicron) wave, magnitude of SARS-CoV-2 ancestral spike antibody concentrations did not predict protective immunity. Anti-SARS-CoV-2 antibody concentrations were higher and more sustained in participants with prior SARS-CoV-2 infection compared with those without prior infection. Reinfection occurred predominantly during the B.1.1.529 (Omicron) wave, was more common in infliximab-treated than vedolizumab-treated patients and were predicted by SARS-CoV-2 anti-N concentrations. We did not observe persistent oropharyngeal carriage. Hospitalisations and deaths remained uncommon.
Interpretation
In keeping with the original vaccine trials,22 23 after two vaccine doses, the highest anti-S RBD antibody concentrations were observed in recipients of the BNT162b2 vaccine. However, a third dose of an mRNA-based vaccine substantially improved responses in patients who had previously received the ChAdOx1 nCoV-19 vaccine, in support of previous studies demonstrating the benefit of heterologous booster vaccinations.24 25 Few published studies have reported the impact of biological and immunomodulator drugs on anti-SARS-CoV-2 antibody responses after three or four doses of a COVID-19 vaccine in patients with IBD.26
Previous observational studies following one or two doses of a SARS-CoV-2 vaccine showed that most patients mount a serological response.27–32 Drawing conclusions across studies, however, is limited by differences in study sample size, control populations, the numbers and types of vaccines administered and the assays and seroconversion thresholds adopted to define response. Perhaps unsurprisingly then, results regarding the impact of specific biological and/or immunomodulator drugs are contradictory. Those studies that were adequately powered concluded that anti-TNF monotherapy attenuates serological responses, which are further impaired by combination immunomodulator use and in particular by methotrexate.8 9 11 Our half-life estimates suggest that further booster doses may be required for infliximab-treated patients without prior infection, after about 4 months to maintain antibody concentrations above peak prethird dose concentrations.10 Based on our postfourth dose antibody responses, however, there appears to be a ceiling effect on peak anti-S RBD antibody concentrations, irrespective of biological type or combination of primary vaccinations received.
Overall, vaccination continued to provide protective immunity during the B.1.1.529 (Omicron) wave. However, breakthrough SARS-CoV-2 infection occurred more commonly and earlier in infliximab-treated than vedolizumab-treated patients. Because infliximab does not increase the risk of SARS-CoV-2 infection prior to vaccination, the increased risk of breakthrough infection observed here is likely mediated by attenuated vaccine responses. Our findings that antinucleocapsid concentrations predict reinfection reflects the conserved nature of the SARS-CoV-2 nucleocapsid sequence. In contrast, the spike sequence has rapidly evolved from the ancestral Wuhan Hu-1 strain sequence used in currently available vaccines. This is likely to explain why the anti-S-RBD antibody concentrations does not predict the risk of breakthrough infection with the omicron variant. In the age of VOCs, no reliable serological correlate of protection currently exists making routine anti-S RBD antibody testing to assess vaccine responses of limited utility, although it remains a useful marker demonstrating an immune response to vaccination.
As the pandemic evolved, reinfection with the new VOC has become more frequent. Similar to the situation in the general population, in this study, prior to the emergence of B1.1.529 (Omicron), breakthrough infection and reinfection with COVID-19 were relatively uncommon in our vaccinated population. Thereafter, treatment with infliximab was associated with a twofold increased risk of reinfection compared with treatment with vedolizumab that was predicted by the immune responses at the time of the initial infection. While we observed that 3.1% of our patients tested positive for SARS-CoV-2, 15–90 days after their index diagnosis, we did not observe persistent oropharyngeal carriage of replication-competent virus in our substudy. Our findings may be limited by our sample size, however, against this, in the general population 13% of immunocompetent participants had evidence of persistent carriage of live virus.20 However, and unlike Davies et al, we undertook this work during a low prevalence phase of the pandemic when the delta variant was dominant, and relied on cross-sectional rather than sequential testing with a longer interval between first and last PCR tests.
Despite the increased risk of breakthrough and recurrent SARS-CoV-2 infection in patients treated with infliximab, hospitalisations and deaths were reassuringly uncommon. This is likely to reflect the effectiveness of vaccination and the lower virulence of the B1.1.259 (Omicron) variant. Moreover, anti-TNF therapy may prevent severe illness through inhibition of systemic inflammatory response associated with severe COVID-19.33 34 While hospitalisations were uncommon, a large number of infected patients risk a high burden of long COVID-19 in a population who already experience increased rates of fatigue, cognitive dysfunction and mood disorders than the general population.35 36 Several groups have suggested that anti-TNF therapy protects patients from severe COVID-19 illness.37 Because long COVID-19 has been linked to more severe initial disease,38 further work is needed to understand the effect of anti-TNF therapy on the prevalence and biology of long COVID-19.
Limitations and generalisability
We acknowledge the following limitations. First, our sample size although larger than similar studies, did not allow us to determine the effectiveness of vaccination against breakthrough infection with specific SARS-CoV-2 variants. Second, we have not been able to evaluate the impact of biological therapy on immunity that follows infection independent of vaccination, as only 5% of patients were unvaccinated at latest follow-up. Finally, we only assessed anti-S RBD antibody responses to infection, while a comprehensive appraisal of protective immunity would incorporate analysis of specific T cell immunity.
Anti-TNF drugs are used to treat a number of other immune-mediated inflammatory disease, which together affect about 3%–7% of Western populations including rheumatoid arthritis, ankylosing spondylitis, psoriatic arthritis, psoriasis, hidradenitis suppurativa and uveitis. Our findings are likely to be generalisable to other anti-TNF drugs including adalimumab, certolizumab, golimumab and etanercept and across these other disease indications. Recent data from the VIP study suggests that anti-SARS-CoV-2 antibody responses following vaccination are also impaired in patients with IBD treated with other systemic immunosuppressant drugs, including tofacitinib, and allowing for sample size constraints, ustekinumab.11
As a consequence of attenuated and less durable immunity, the potential benefits of vaccination against the risk of SARS-CoV-2 breakthrough infection and reinfection were reduced by infliximab treatment. The growing immunity in the population will potentially accelerate antigenic evolution, increasing the risk of reinfection and potentially for higher disease severity in reinfected patients.39 Patients with attenuated responses to vaccination should be considered vulnerable to future more virulent SARS-CoV-2 variants.
Strategies that bypass the negative effect of the anti-TNF on vaccine-induced immune responses are now required. Further work is needed to assess whether the next generation of anti-SARS-CoV-2 vaccines, temporarily withholding immunomodulators at the time of vaccination40 and/or timing booster doses towards the end of an anti-TNF treatment cycle when drug levels are lowest7 may induce greater immunogenicity. In the meantime, anti-TNF patients should be prioritised for booster vaccine doses with an mRNA-based vaccine.
Conclusion
Following a third dose of anti-SARS-CoV-2 mRNA-based vaccine, infliximab treatment was associated with attenuated serological responses, and breakthrough SARS-CoV-2 infection and reinfection. Breakthrough infection was not predicted by the magnitude of anti-S RBD responses, indicative of vaccine escape by the B1.1.529 (Omicron) variant.
Data availability statement
Data are available on reasonable request. The study protocol including the statistical analysis plan is available at www.clarityibd.org. Individual participant de-identified data that underlie the results reported in this article will be available immediately after publication for a period of 5 years. The data will be made available to investigators whose proposed use of the data has been approved by an independent review committee. Analyses will be restricted to the aims in the approved proposal. Proposals should be directed to tariq.ahmad1@nhs.net; to gain access data requestors will need to sign a data access agreement.
Ethics statements
Patient consent for publication
Ethics approval
The Surrey Borders Research Ethics committee approved the study (REC reference: REC 20/HRA/3114) in September 2020. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
CLARITY IBD is a UK National Institute for Health Research (NIHR) Urgent Public Health Study. The NIHR Clinical Research Network supported study set-up, site identification and delivery of this study. This was facilitated by Professor Mark Hull, the National Speciality Lead for Gastroenterology. We acknowledge the contribution of our Patient Advisory Group who helped shape the trial design around patient priorities. Our partners, Crohn’s and Colitis UK (CCUK), continue to support this group and participate in Study Management Team meetings. We thank Professor Graham Cooke and Dr Katrina Pollock for their helpful discussions and review of the data. Laboratory tests were undertaken by the Exeter Blood Sciences Laboratory at the Royal Devon and Exeter NHS Foundation Trust. The Exeter NIHR Clinical Research Facility coordinated sample storage and management. Tariq Malik and James Thomas from Public Health England, Guy Stevens, Katie Donelon, Elen de Lacy from Public Health Wales, Johanna Bruce and Eva Lahnsteiner from Public Health Scotland and the team from NHS Digital Access Request Service supported linkage of central SARS-CoV-2 PCR test results with study data. Roche Diagnostics Limited provided the Elecsys Anti-SARS-CoV-2 immunoassay for the study. The Department of Microbiology at the Royal Devon and Exeter NHS Trust performed SARS-CoV-2 PCR and antibody tests, and subgenomic experiments were performed by the RNA-mediated disease mechanism group at the University of Exeter.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @DrNickKennedy, @nchanchlani1, @SimengLin, @PANTSresearch, @T_J_McDonald, @miRNAgirl, @Merlin_Davies, @klaartjekok, @DrChrisLamb, @drailsahart, @NA, @charlie_lees, @BoytonRosemary, @Daltmann10, @ibdseb, @NickPowellLab, @JamesGoodhand1, @tariqahmadIBD
NAK and MJ contributed equally.
NP, JRG and TA contributed equally.
Correction notice This article has been corrected since it published Online First. Gramatical errors have been amended in the abstract, key messages and discussion.
Collaborators Contributors to the CLARITY IBD study—please see supplemental file for all names.
Contributors NAK, JRG, CB, SS, NP and TA participated in the conception and design of this study. CB was the project manager and coordinated patient recruitment. RN and TJM coordinated all biochemical analyses and central laboratory aspects of the project. NAK, MJ, NC, SL, CB, LWH, MD, KBK, CAL, PJS, AH, RCP, CWL, RB, DA, SS, NP, JRG and TA were involved in the acquisition, analysis or interpretation of data. CA and SM performed SARS-CoV-2 variants characterisation analysis and interpretation. LWH and MD performed and interpreted RNA and subgenomic analyses. Data analysis was done by NAK. Drafting of the manuscript was done by NAK, MJ, NC, SL, JRG and TA. TA and RB obtained the funding for the study. All the authors contributed to the critical review and final approval of the manuscript. NAK, NP, JRG and TA have verified the underlying data. TA is the guarantor of the article.
Funding SL is supported by a Wellcome GW4-CAT fellowship (222850/Z/21/Z). NC acknowledges support from CCUK. CAL acknowledges support from the NIHR Newcastle Biomedical Research Centre and the support of the Programmed Investigation Unit at Royal Victoria Infirmary, Newcastle upon Tyne. CWL is funded by a UKRI Future Leaders Fellowship. RB and DA are supported by MRC (MR/W020610/1, MR/S019553/1, MR/R02622X/1 and MR/V036939/1), NCSi4P, NIHR EME NIHR134607 and NIHR COV-LT2-0027, Innovate UK SBRI894, NIHR Imperial BRC Institute for Translational Medicine and Therapeutic, Cystic Fibrosis Trust SRC (2019SRC015) and Horizon 2020 Marie Skłodowska-Curie Innovative Training Network (ITN) European Training Network (No 860325). NP is supported by the NIHR Imperial Biomedical Research Center (BRC). We acknowledge the study co-ordinators of the Exeter Inflammatory Bowel Disease Research Group: Marian Parkinson and Helen Gardner-Thorpe for their ongoing administrative support to the study. This research used data assets made available by National Safe Haven as part of the Data and Connectivity National Core Study, led by Health Data Research UK in partnership with the Office for National Statistics and funded by UK Research and Innovation (research which commenced between 1 October 2020 and 31 March 2021 grant ref MC_PC_20029; 1 April 2021 and 30 September 2022 grant ref MC_PC_20058). This study was supported by an NCSi programme UKRI award to RB, DA, NP and TA (MR/W020610/1). The sponsor of the study was the Royal Devon and Exeter NHS Foundation Trust.
Competing interests NAK reports grants from F. Hoffmann-La Roche, grants from Biogen, grants from Celltrion Healthcare, grants from Galapagos, non-financial support from Immundiagnostik, during the conduct of the study; grants and non-financial support from AbbVie, grants and personal fees from Celltrion, personal fees and non-financial support from Janssen, personal fees from Takeda, personal fees and non-financial support from Dr Falk Pharma, outside the submitted work. SL reports non-financial support from Pfizer, non-financial support from Ferring, outside the submitted work. LWH declares an interest in SENISCA as founder and Chief Scientific Officer. KBK reports personal fees from Janssen, personal fees from Takeda, personal fees from PredictImmune, personal fees from Amgen, outside the submitted work. CAL reports grants from Genentech, grants and personal fees from Janssen, grants and personal fees from Takeda, grants from AbbVie, personal fees from Ferring, grants from Eli Lilly, grants from Pfizer, grants from Roche, grants from UCB Biopharma, grants from Sanofi Aventis, grants from Biogen IDEC, grants from Orion OYJ, personal fees from Dr Falk Pharma, grants from AstraZeneca, outside the submitted work. PJS reports speaker fees and advisory board sponsorship from Janssen, Celltrion, AbbVie, Tillotts Pharma, Galapagos, Amgen, Dr Falk Pharma and Takeda outside the submitted work. AH reports personal fees from AbbVie, personal fees from Allergan, personal fees from BMS, personal fees from Celltrion, personal fees from Dr Falk Pharma, personal fees from GSK, personal fees from Takeda, personal fees from Pfizer, personal fees from Janssen, personal fees from Galapogos, personal fees from AstraZeneca, outside the submitted work. RCP reports acting as consultant, advisory board member, speaker or recipient of educational grant from Dr Falk Pharma, Ferring, Janssen, Pharmacosmos and Takeda, outside the submitted work. CWL reports personal fees from AbbVie, personal fees from Janssen, personal fees from Pfizer, personal fees from Takeda, grants from Gilead, personal fees from Gilead, personal fees from Galapagos, personal fees from Iterative Scopes, personal fees from Trellus Health, personal fees from Celltion, personal fees from Ferring, personal fees from BMS, during the conduct of the study. RB and DA are members of the Global T cell Expert Consortium and have consulted for Oxford Immunotec outside the submitted work. SS reports grants from Takeda, AbbVie, Amgen, Tillots Pharma, personal fees from Jaansen, Takeda, Galapagos, Celltrion, Dr Falk Pharma, Tillots Pharma, Cellgene, Pfizer, Pharmacocosmos, outside the submitted work. NP reports personal fees from Takeda, personal fees from Janssen, personal fees from Pfizer, personal fees from Bristol-Myers Squibb, personal fees from AbbVie, personal fees from Roche, personal fees from Lilly, personal fees from Allergan, personal fees from Celgene, outside the submitted work; and NP has served as a speaker/advisory board member for AbbVie, Allergan, Bristol-Myers Squibb, Celgene, Dr Falk Pharma, Ferring, Janssen, Pfizer, Tillotts Pharma, Takeda and Vifor Pharma. JRG reports grants from F. Hoffmann-La Roche, grants from Biogen, grants from Celltrion Healthcare, grants from Galapagos, non-financial support from Immundiagnostik, during the conduct of the study. TA reports grants and non-financial support from F. Hoffmann-La Roche, grants from Biogen, grants from Celltrion Healthcare, grants from Galapagos, non-financial support from Immundiagnostik, during the conduct of the study; personal fees from Biogen, grants and personal fees from Celltrion Healthcare, personal fees and non-financial support from Immundiagnostik, personal fees from Takeda, personal fees from ARENA, personal fees from Gilead, personal fees from Adcock Ingram Healthcare, personal fees from Pfizer, personal fees from Genentech, non-financial support from Tillotts Pharma, outside the submitted work.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the 'Methods' section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.