Article Text

Abstract
Objective To evaluate the benefit of mass eradication of Helicobacter pylori infection in reducing premalignant gastric lesions.
Design Mass eradication of H pylori infection was started from 2004 for a Taiwanese population with prevalent H pylori infection, who were >30 years of age. Participants positive for the 13C-urea breath test underwent endoscopic screening and 1-week clarithromycin-based triple therapy. For subjects whose initial treatment failed, 10-day levofloxacin-based triple therapy was administered. The main outcome measures were changes in the prevalence of H pylori infection and premalignant gastric lesions, and changes in the incidence of premalignant gastric lesions and gastric cancer before (1995–2003) and after (2004–2008) chemoprevention using various comparators.
Results The reduction in H pylori infection was 78.7% (95% CI 76.8% to 80.7%), and the estimated incidence of re-infection/recrudescence was 1% (95% CI 0.6% to 1.4%) per person-year. The effectiveness of reducing the incidence of gastric atrophy resulting from chemoprevention was significant at 77.2% (95% CI 72.3% to 81.2%), while the reduction in intestinal metaplasia was not significant. Compared with the 5-year period before chemoprevention and in the absence of endoscopic screening, the effectiveness in reducing gastric cancer incidence during the chemoprevention period was 25% (rate ratio 0.753, 95% CI 0.372 to 1.524). The reduction in peptic ulcer disease was 67.4% (95% CI 52.2% to 77.8%), while the incidence of oesophagitis was 6% (95% CI 5.1% to 6.9%) after treatment.
Conclusions Population-based eradication of H pylori infection has led to a significant reduction in gastric atrophy at the expense of increased oesophagitis. The ultimate benefit in reducing gastric cancer incidence and its mortality should be validated by a further long-term follow-up.
Trial registration number NCT00155389.
- Helicobacter pylori
- gastric cancer
- chemoprevention
- cancer prevention
- endoscopic procedures
- gastro-oesophageal reflux disease
- colorectal cancer screening
- oesophageal cancer
- cancer epidemiology
- statistics
- meta-analysis
- cancer registries
- colonoscopy
- colonic polyps
- colorectal neoplasia
- colonic neoplasms
- colorectal adenomas
- endoscopic polypectomy
- colorectal neoplasm
- endoscopy
- gastric lymphoma
- helicobacter pylori - pathogenesis
- molecular oncology
- gastrointestinal neoplasia
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/3.0/ and http://creativecommons.org/licenses/by-nc/3.0/legalcode
Statistics from Altmetric.com
- Helicobacter pylori
- gastric cancer
- chemoprevention
- cancer prevention
- endoscopic procedures
- gastro-oesophageal reflux disease
- colorectal cancer screening
- oesophageal cancer
- cancer epidemiology
- statistics
- meta-analysis
- cancer registries
- colonoscopy
- colonic polyps
- colorectal neoplasia
- colonic neoplasms
- colorectal adenomas
- endoscopic polypectomy
- colorectal neoplasm
- endoscopy
- gastric lymphoma
- helicobacter pylori - pathogenesis
- molecular oncology
- gastrointestinal neoplasia
Significance of this study
What is already known on this subject?
-
Randomised controlled clinical trials of subjects receiving anti-Helicobacter pylori treatment have not been able to identify a significant reduction in gastric cancer because of the long time period during which gastric lesions are premalignant and the requirement for a large sample size.
-
Mass eradication of H pylori infection has not yet been substantiated with population-based data; as improvements in sanitation and hygiene have contributed to an observed decline in gastric cancer incidence, the benefit of this strategy remains elusive.
What are the new findings?
-
Population-based eradication of H pylori infection substantially reduced the incidence of H pylori infection, gastric atrophy and peptic ulcer disease within the relatively short time period of this study.
-
The re-infection/recrudescence rate of 1% per person-year after intervention is lower than the threshold value for which treatment is not considered to be cost-effective.
-
The intervention does not reduce the incidence of intestinal metaplasia or decrease its histological severity, supporting the ‘point-of-no-return’ theory.
-
The increased incidence of oesophagitis after intervention in a population where gastric atrophy was prevalent establishes a causal relationship between them.
How might it impact on clinical practice in the foreseeable future?
-
Mass eradication of H pylori infection led to a substantial reduction in the incidence of gastric atrophy shortly after implementation, which supports the use of this strategy to prevent gastric cancer in populations where H pylori is endemic and the incidence of gastric cancer is high.
Introduction
Helicobacter pylori is well recognised as a class I carcinogen because long-term colonisation by this organism can provoke chronic inflammation and atrophy,1 ,2 which can further lead to malignant transformation. As treatment of gastric cancer at the symptomatic stage represents a significant medical burden, clinicians have been encouraged to focus on designing preventive strategies instead of multimodal therapies. The role of H pylori eradication in reducing premalignant gastric lesions3–5 and invasive cancers6–10 has therefore gained attention.
The results of previous studies have been inconclusive because the prevalence of H pylori infection varies between countries and the premalignancy phase of gastric cancers is long.11 Although eradication of H pylori has the potential to prevent gastric cancer, a pooled analysis of five randomised controlled trials3–5 ,7 ,8 still revealed an insignificant reduction in cancer risk,12 and the benefit of a microbial-based approach to cancer prevention in a population-wide, real-life setting thus remains unsubstantiated.
Because the transition from inflamed mucosa to atrophic change is a common route to carcinogenesis,1 ,2 the effect of H pylori eradication on the incidence of this early precursor lesion is of interest. This effect can be examined using population-based empirical data, particularly in high-risk areas where virulent strains of H pylori are highly prevalent and premalignant gastric lesions are commonly observed at the start of active intervention. Such evidence would help clinicians target aggressive therapy to susceptible patients and design surveillance programmes for treatment-unresponsive patients.
Such a population is found on Matsu Island, located between Taiwan and mainland China, where a two-stage mass screening programme for gastric cancer by endoscopic examination was performed in subjects with positive biomarker results between 1995 and 1998; however, the benefit of this strategy was limited.13
In a further attempt to prevent gastric cancer and reduce its mortality in the Matsu Island population, a population-based H pylori eradication programme was launched in 2004 under the auspices of the Taiwanese Ministry of Health.14 This programme provided the unique opportunity to evaluate the effect of H pylori eradication in reducing premalignant gastric lesions by comparing data from the pre- and post-chemoprevention programme eras (1995–2003 and 2004–2008, respectively) in the same population. Such evaluation was the main objective of the present study. Because early endoscopic detection of gastric cancer may have occurred concomitantly with the chemoprevention programme, our secondary objective was to evaluate changes in the incidence of gastric cancer and cancer-specific mortality. The findings of our longitudinal cohort study were further validated by adjustment for the declining incidence of gastric neoplasm due to improved sanitation and hygiene.
Methods
Study subjects and prevention programmes
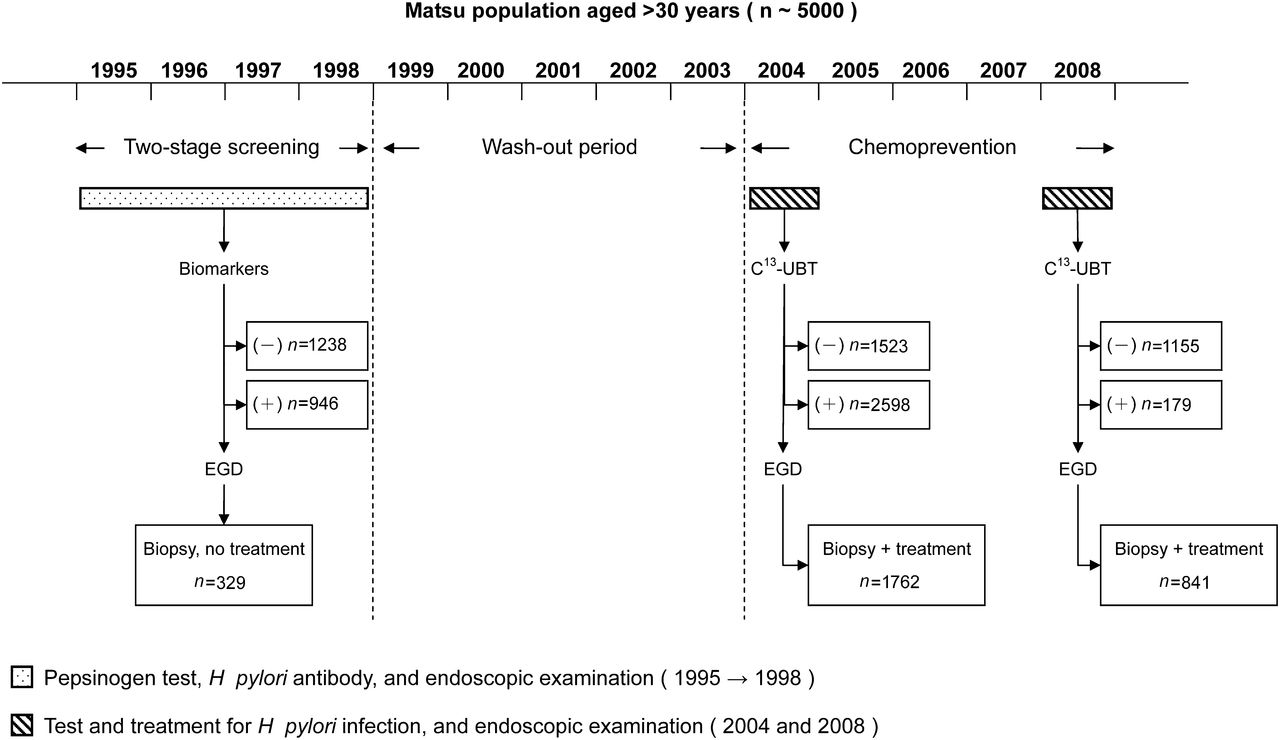
Our target population comprised approximately 5000 residents of Matsu Island (online appendix figure 1), who were >30 years of age and listed in the population registry. Residents of Matsu Island have a high prevalence of H pylori infection, and the annual death rate for gastric cancer was approximately three times that in Taiwan. Because of the high-risk characteristics, a series of mass screening programmes for gastric cancer, including endoscopy and chemoprevention, were implemented (figure 1). Between 1995 and 1998, the prevention programme focused on two-stage mass screening for gastric neoplasia, with an initial biomarker test (according to the level of serum pepsinogen and H pylori antibody) and subsequent endoscopic examination for positive subjects.13 Subjects identified as having a higher risk of gastric cancer were referred for an endoscopic examination. Biopsy specimens were taken from the gastric antrum and corpus for histological assessment. No H pylori treatment was given to these subjects because the evidence remained inconclusive at that time.

Gastric cancer prevention programmes implemented on Matsu Island, in chronological order. EGD, oesophagogastroduodenoscopy; UBT, urea breath test.
From 1999 to 2003, a multiple-disease screening programme was launched that included non-neoplastic (diabetes mellitus, hypertension and hyperlipidaemia) and neoplastic (breast and colorectal cancer) diseases, but not gastric cancer. This programme was called the Matsu Community-Based Multiple Screening Program, and had a design similar to that of a programme in Keelung, the northern-most area of Taiwan.15 Periodic health assessments and services are ongoing. In this multiple-disease screening programme, potential participants were contacted by telephone and received a pamphlet by mail that invited them to attend their local screening centre. Although this programme did not include gastric cancer screening, it offered community residents an incentive to attend screening and comply with treatment. Information collected from each participant included family history, lifestyle factors (eg, smoking and alcohol consumption), anthropometric measurements and biochemical studies (eg, fasting glucose, lipid profile and uric acid). After this multiple-disease screening programme, the local government implemented a chemoprevention programme from 2004 to 2008 under the auspices of Taiwan's Ministry of Health.
Study design for evaluation
Because the 1999–2003 multiple-disease screening programme did not include gastric cancer, this 5-year wash-out period before the implementation of chemoprevention eliminated the possible effect of the previous screening conducted between 1995 and 1998. This allowed us to use a ‘before and after’ study design to compare the prevalence of H pylori infection, gastric atrophy, intestinal metaplasia and gastric dysplasia before and after chemoprevention, in order to evaluate the effectiveness of mass eradication of H pylori infection. We also evaluated the effectiveness of our intervention in reducing the incidence of, and mortality from, gastric cancer by comparing the 5-year wash-out period (1999–2003) with the chemoprevention period (2004–2008).
In addition to the before and after study design, data from the two-stage mass screening (1995–1998; biomarker test and endoscopic examination) also formed a historical control to evaluate the effect of chemoprevention on the incidence of gastric atrophy and intestinal metaplasia. However, these estimates of effectiveness would be more conservative than those based on the before and after study design because the historical control group might be influenced by the administration of endoscopy for biomarker-positive subjects.
Chemoprevention
A chemoprevention programme was implemented and appended to the multiple-disease screening programme in 2004. Detailed information on the mass eradication of H pylori infection and the preliminary efficacy of the programme has been given elsewhere.14 In brief, participants positive for the 13C-urea breath test (UBT) underwent endoscopic screening, histological assessment, 1-week clarithromycin-based triple therapy (esomeprazole 40 mg once daily, amoxicillin 1 g twice daily, and clarithromycin 500 mg twice daily) and a confirmatory 13C-UBT. Re-treatment was administered in subjects whose initial treatment failed as indicated by a positive 13C-UBT performed 6–8 weeks after the end of treatment. The re-treatment consisted of 10-day levofloxacin-based triple therapy (esomeprazole 40 mg once daily, amoxicillin 1 g twice daily, and levofloxacin 500 mg once daily) and another confirmatory test. The adverse effects of the antibiotic treatment were considered mild, and none led to premature discontinuation of treatment. No severe adverse effects were observed.14 Endoscopic screening was also administered in an attempt to balance the effects of this tool across the pre- and post-chemoprevention programme epochs.
In 2008, another course of chemoprevention was delivered and new participants were also encouraged to undergo screening and treatment for H pylori infection, endoscopic screening and histological assessment. The first objective of this screening programme was to determine the sustainability of H pylori eradication, so that bacterial re-infection, which has the potential to overturn treatment effectiveness,11 could be ruled out. The second objective was to evaluate the effectiveness of chemoprevention on the outcome measure of gastric atrophy. Finally, the third screening objective was to increase the rate of coverage of H pylori treatment because of a potential increase in the number of eligible subjects.
All participants provided written informed consent. The ethics committee of the National Taiwan University Hospital approved the study (No 940110).
Histological assessment
The biopsy procedure protocol specified sampling of the same locations to maintain consistency. Senior histopathologists who were blinded to the subjects' clinical status performed the histological assessments. Specimens were graded using a categorical construct that included the identification of normal mucosa, superficial gastritis, gastric atrophy (loss of glandular tissue and fibrous replacement) and intestinal metaplasia (presence of goblet cells and absorptive cells), according to the most advanced lesion observed in each set of biopsy samples from each subject. Beginning in 2004, an ordinal scale16 was appended to the categorical construct to rate the severity of each category as none (0), mild (1), moderate (2) or marked (3). Three sub-categories were added to describe the types of inflammatory cell infiltrates: acute inflammation (polymorphonuclear infiltrates), chronic inflammation (lymphoplasmacytic infiltrates) and mucosa-associated lymphoid tissue (lymphoid tissue comprising nodular aggregates). The presence and severity of gastric dysplasia were also graded as none, indefinite for dysplasia (the epithelium was not unequivocally negative or unequivocally dysplastic), low-grade dysplasia (the crowded nuclei were confined to the basal half of the cell and showed only scant mitotic activity) and high-grade dysplasia (the nuclei extended into the luminal aspect of the cell and showed frequent mitotic figures).17
To confirm the reliability of histological assessments, 100 pretreatment samples collected in 2004 were randomly selected for re-evaluation by the same pathologist in 2009. With the categorical construct described above, a substantial level of agreement was observed (κ=0.64; 95% CI 0.51 to 0.77). The weighted κ values for acute inflammation, chronic inflammation, mucosa-associated lymphoid tissue, gastric atrophy and intestinal metaplasia were 0.58 (95% CI 0.48 to 0.68), 0.56 (95% CI 0.39 to 0.73), 0.81 (95% CI 0.73 to 0.89), 0.62 (95% CI 0.49 to 0.74) and 0.74 (95% CI 0.60 to 0.88), respectively.
Statistical analysis
Comparisons of the prevalence of H pylori infection, gastric atrophy, intestinal metaplasia and gastric dysplasia before and after chemoprevention were performed using a risk ratio (RR). Comparisons of the incidence of gastric atrophy, intestinal metaplasia, gastric cancer and cancer-specific mortality before and after chemoprevention were performed using a rate ratio. The effectiveness of H pylori treatment in reducing these outcomes was calculated as: 1−(RR or rate ratio)×100%.
Because premalignant lesions are asymptomatic, histological evaluations conducted during endoscopic screenings were used to identify the number of new cases and the proportion of the population at risk. The number of gastric cancer cases was determined by searching the databases of Taiwan Cancer Registry. The number of gastric cancer deaths was determined by searching the databases of the Department of Health. The number of at-risk subjects was determined by searching the database of the Household Registration Administration System. These data were checked annually by government registration officers to ensure the records were complete and accurate. To evaluate treatment efficacy, the histological severity scores of endoscopies performed in 2004 were compared with those performed in 2008 using the Wilcoxon signed-rank test. We also evaluated the influence of relevant individual factors18 on treatment effectiveness using the backward elimination method in a multivariate logistic regression model.
To validate the effect of chemoprevention while adjusting for influences other than H pylori eradication, such as improvements in sanitation and hygiene, that led to a decline in incidence over time,19 we extrapolated the rate of gastric atrophy by following the time trend from 1995 to 2003 to calculate the expected rate of gastric atrophy during the chemoprevention period using the Poisson regression model. We then compared the expected number of cases with the observed number during the chemoprevention period between 2004 and 2008 to remove the influence of declining incidence by taking into account the effect of calendar year (a proxy variable). Adjustment for the change in incidence and mortality with time was performed for intestinal metaplasia, gastric cancer and death from gastric cancer in a similar manner. The detailed calculations are provided in online appendix table 1.
To validate the impact of intervention on gastric cancer, we used external data from Taiwan Island.20 Trends in the incidence rates of gastric cancer were plotted to examine the change achieved by the chemoprevention programme. The incidence of gastric cancer on Matsu Island was standardised to that in Taiwan, and is presented as a standardised incidence ratio.
Results
Attendance and compliance rates
A total of 4121 participants (1888 men and 2233 women) participated in the chemoprevention programme in 2004, and 1334 (677 men and 657 women) participated in the second round of the programme in 2008. Their mean ages were 49.2 (SD 12.8) and 52 (10.8) years in 2004 and 2008, respectively. Of the 1762 residents who had undergone a baseline histological assessment in 2004, 1169 (66.3%) received a follow-up 13C-UBT in 2008; of these, 1056 (1056/1169, 90.3%) were free from H pylori infection, and 841 (841/1169, 71.9%) underwent a face-to-face interview, endoscopy and histological reassessment.
Reduction in H pylori infection
Of the 841 who underwent histological reassessment, 94 (11.2%) showed persistent H pylori infection. Poor compliance with treatment was confirmed in 33 (3.9%) of the subjects. Thirty-two subjects (3.8%) remained H pylori carriers despite the administration of two courses of triple antibiotic therapy, suggesting the presence of drug-resistant strains. Among the 776 subjects who had previously undergone successful H pylori eradication therapy in 2004, 29 (3.5%) tested positive in 2008. The estimated rate of re-infection/recrudescence was 1% (29/2914; 95% CI 0.6% to 1.4%) per person-year.
At the population level, the prevalence of H pylori infection was 64.8% in 1995, which was close to the 63% prevalence at baseline before the implementation of chemoprevention in 2004. This prevalence had declined to 13.4% in our study population (including 182 new participants) at the time of the H pylori infection survey in 2008. The estimated population-level effectiveness of chemoprevention was thus 78.7% (95% CI 76.8% to 80.7%).
Reduction in gastric atrophy
As shown in table 1, the prevalence of gastric atrophy was 59.9% (95% CI 57.6% to 62.2%) in 2004 (immediately before chemoprevention) and 13.7% (95% CI 11.4% to 16%) in 2008 (after chemoprevention), yielding a RR of 22.8% (95% CI 18.8% to 27.7%; p<0.01) and an effectiveness of 77.2% (95% CI 72.3% to 81.2%) in reducing gastric atrophy (a power of 99% to detect a difference at an α=0.05 level of significance).
Changes in the prevalence of gastric and oesophageal lesions before and after mass eradication of Helicobacter pylori infection
Using historical control data from the two-stage endoscopic screening (1995–1998), we determined that the annual rate of gastric atrophy significantly declined from 8.2% (95% CI 6% to 10.3%) per person-year before chemoprevention to 3.5% (95% CI 1% to 6.1%) after chemoprevention, yielding a rate ratio of 0.434 (95% CI 0.194 to 0.951; p=0.02). With adjustment for the effect of the ∼6% annual decline in the incidence of gastric atrophy, the reduction in the incidence of gastric atrophy in our study population was 61.1% (95% CI 18.5% to 81.5%; see online appendix table 1 for detailed calculation). This finding was further supported by substantial reductions in the severity scores for acute inflammation, chronic inflammation, gastric atrophy and mucosa-associated lymphoid tissue after treatment (online appendix table 2).
Changes in intestinal metaplasia, gastric dysplasia, gastric cancer and gastric cancer-specific mortality
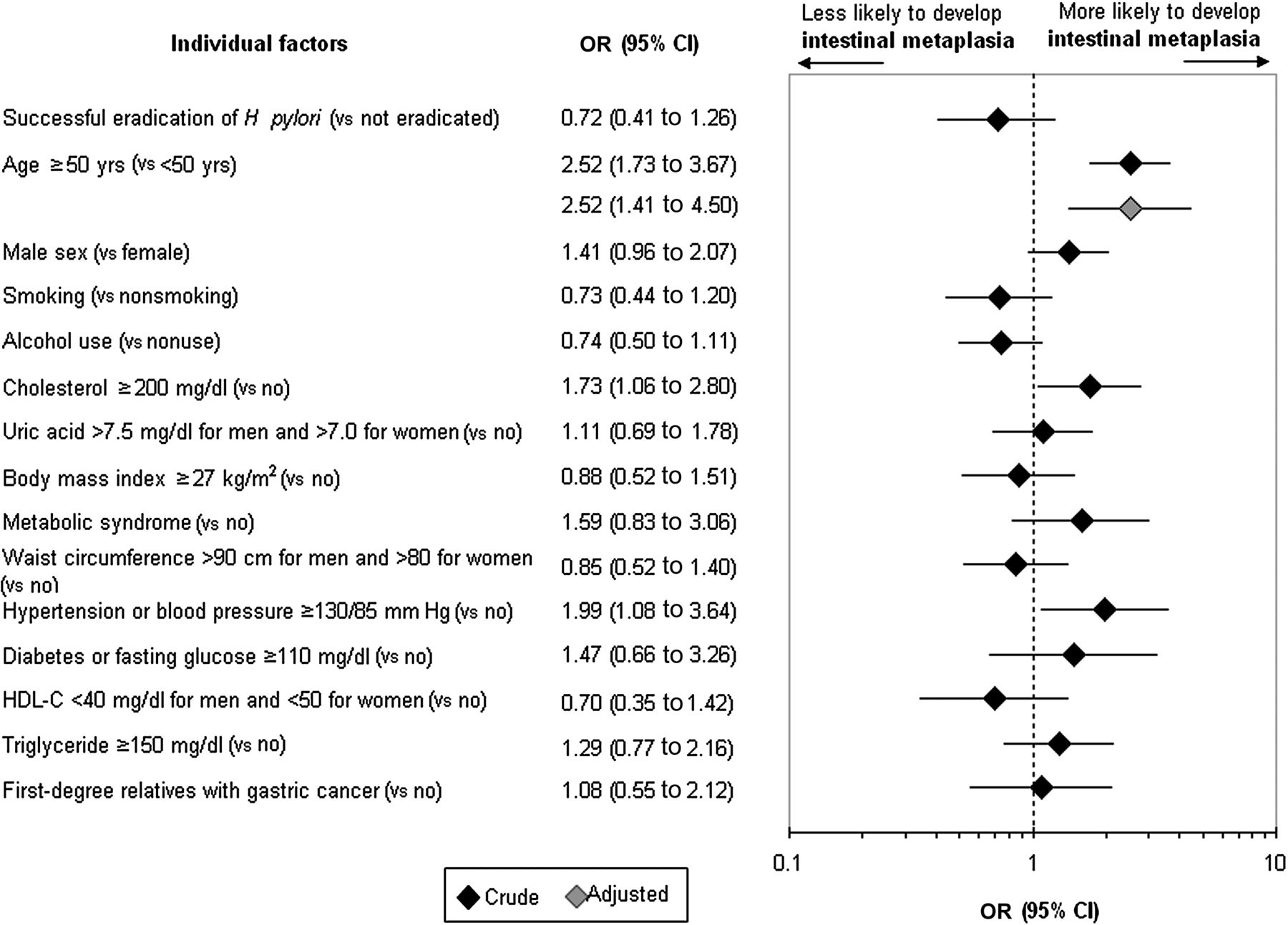
The prevalence of intestinal metaplasia was higher after chemoprevention (38.9%; 95% CI 35.6% to 42.2%) than before (31.7%; 95% CI 29.5% to 33.9%). The incidence of intestinal metaplasia was 6.1% (95% CI 5% to 7.1%) and 4.7% (95% CI 3.1% to 6.2%) per person-year after and before chemoprevention, respectively. After adjustment for the effect of declining incidence, no reduction in intestinal metaplasia was seen. These results are consistent with the histological findings, which indicated no change in the severity score for intestinal metaplasia (online appendix table 2). The identification of individual factors associated with histological responses showed that successful eradication of H pylori was associated with a significant reduction in severity scores, which was modified by age (online appendix table 3). Specifically, older subjects were more likely to develop intestinal metaplasia despite chemoprevention (figure 2).
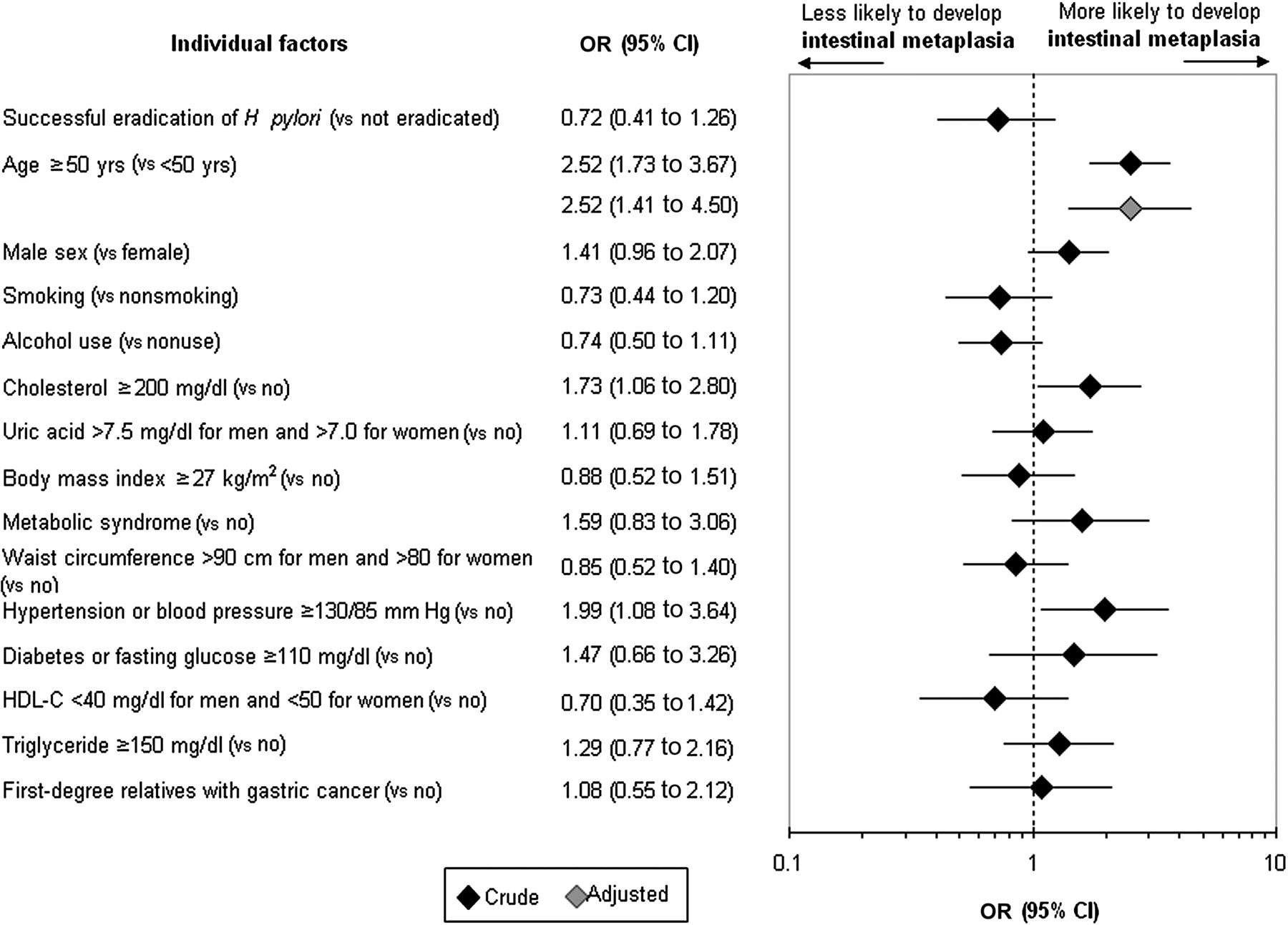
Individual factors associated with the occurrence of intestinal metaplasia after chemoprevention. The multivariate model adjusted for all variables is shown in the forest plot. HDL-C, high-density lipoprotein cholesterol.
The prevalence of indefinite dysplasia and low-grade dysplasia was higher after chemoprevention (15.2% (95% CI 12.8% to 17.6%) and 2% (95% CI 1.1% to 2.9%), respectively) than before (8.1% (95% CI 6.8% to 9.4%) and 0.3% (95% CI 0% to 0.6%), respectively). Screening detected two gastric cancers during 1995–1998, four in 2004, and one in 2008. Taking into account participants who did not attend the screening programmes but presented with symptomatic disease, changes in the incidence of gastric cancer over time are shown in the figure 3. Case numbers, person-years and standardised incidence ratios are presented in online appendix table 4. The annual incidence of gastric cancer on Matsu Island was high before 2004 and declined slowly with time. After the first round of chemoprevention in 2004, a marked peak in gastric cancer incidence was observed, followed by a pronounced and rapid decline. In contrast, external data obtained from Taiwan Island, where no active intervention occurred, were relatively constant over the same period (lower curve of figure 3).
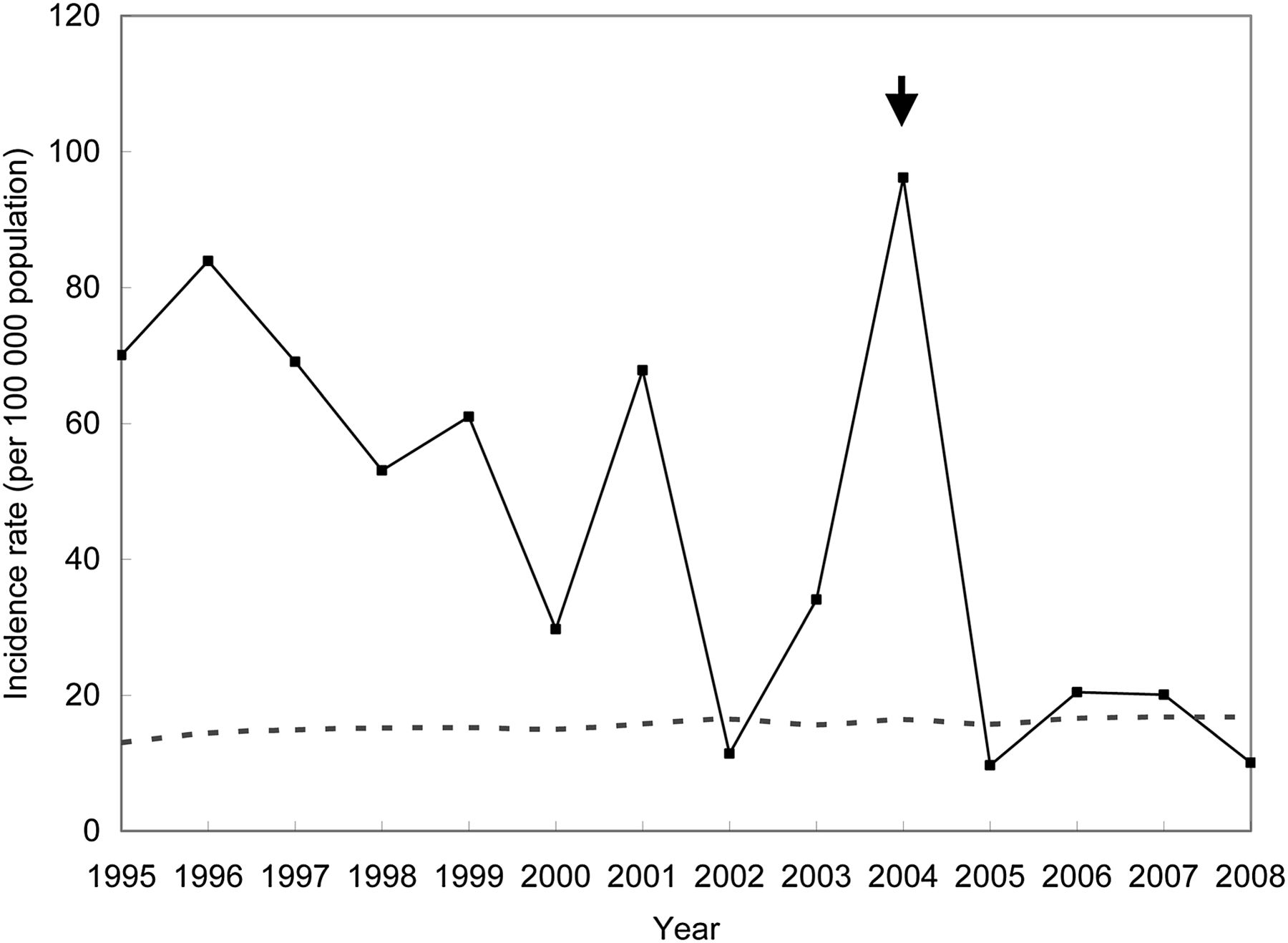
Incidence of gastric cancer between 1995 and 2008, correlated with mass eradication of Helicobacter pylori infection. The trend in gastric cancer incidence over time is represented by the solid line for subjects on Matsu Island and by the dotted line for residents of Taiwan. The closed arrow indicates the start of the chemoprevention programme in 2004, involving endoscopic screening and H pylori treatment.
With the before and after design, the 5-year average incidence of gastric cancer on Matsu Island declined from 40.3 (95% CI 20.6 to 60.0) to 30.4 (95% CI 15.0 to 45.7) per 100 000 person-years in 1999–2003 and 2004–2008, respectively. The rate ratio was 0.753 (95% CI 0.372 to 1.524) and the intervention effectiveness was 24.7% (p=0.21). However, the 5-year average gastric cancer mortality increased from 20.1 (95% CI 6.2 to 34.1) to 26.3 (95% CI 12.0 to 40.6) per 100 000 person-years in 1999–2003 and 2004–2008, respectively. The rate ratio was 1.31 (95% CI 0.541 to 3.151).
Rate ratios were determined by extrapolating the expected rate (based on a historical control from 1995 to 2003) as opposed to the observed number during the period of chemoprevention (2004–2008). This method yielded a rate ratio of 1.40 (95% CI 0.845 to 2.325) for gastric cancer and 3.94 (95% CI 2.288 to 6.785) for death from gastric cancer. The increase in gastric cancer cases was mainly due to early detection through mass endoscopic screening.
Effect of H pylori eradication on peptic ulcer disease and the oesophagus
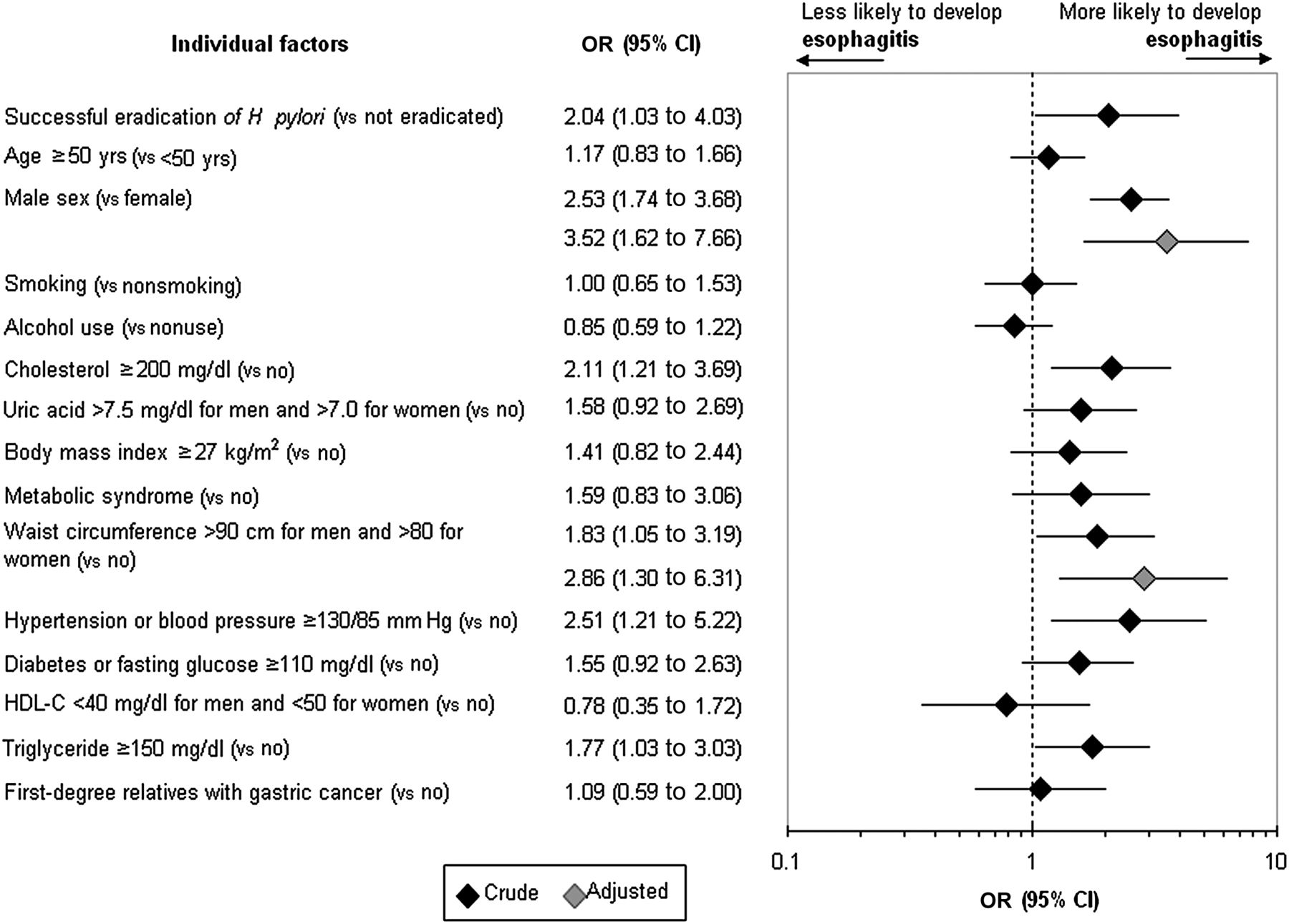
The prevalence of active peptic ulcer decreased during 2004–2008 from 11% to 3.6%, yielding a RR of 32.6% (95% CI 22.2% to 47.8%; p<0.01) and an effectiveness of 67.4% (95% CI 52.2% to 77.8%). However, the prevalence of endoscopic oesophagitis increased from 13.7% to 27.3% (p<0.001), yielding an annual incidence of 6% (163/2723; 95% CI 5.1% to 6.9%) per person-year. Among individuals with oesophagitis at baseline, H pylori treatment actually increased the severity of the condition (p<0.001). Two of these subjects developed histologically confirmed Barrett's oesophagus. Male sex and large waist circumference were associated with the development of oesophagitis after H pylori treatment (figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Individual factors associated with the occurrence of endoscopic oesophagitis after chemoprevention. The multivariate model adjusted for all variables is shown in the forest plot. HDL-C, high-density lipoprotein cholesterol.
Discussion
The present study demonstrated the application of mass eradication of H pylori infection to a population in a small area with highly endemic H pylori infection and a high incidence of gastric cancer. Shortly after the implementation of treatment, significant reductions in H pylori infection (79%) and gastric atrophy (77%) occurred. This remarkable effectiveness for atrophy (61%) persisted after adjustment for the effect of the declining incidence, possibly due to improvements in sanitation and hygiene. However, this intervention was unable to effectively arrest the occurrence, or decrease the histological severity, of intestinal metaplasia and also gastric dysplasia. In reference to the point-of-no-return theory7 and the long period during which lesions are premalignant, we reason that a substantial chemoprevention-mediated reduction in gastric atrophy would lead to a further reduction in the incidence and mortality of gastric cancer, provided that the follow-up period is sufficiently long and the Correa pathway is held.1 This hypothesis should be verified by continuous follow-up of this cohort.
Our study lends support to the notion that H pylori eradication affects the natural course of carcinogenesis based on the successful prevention of gastric atrophy, a notion that has been advocated by previous decision-analysis studies.11 ,21–25 Indeed, substantial benefit can be derived from any treatment that prevents inflamed mucosa from undergoing atrophic changes.2 Such optimism is supported by the findings of population-based studies that sought to prevent the occurrence of other cancers.26 ,27 Our short-course chemoprevention regimen13 ,28 can be applied in national or regional eradication programmes, as it has been in other endemic H pylori infection areas in Latin America.29 This is particularly true because the treatment efficacy and sustained reduction in H pylori infection achieved by the programme were both higher than previously reported.3 ,5 ,7 The 1% per person-year re-infection/recrudescence rate is in agreement with previous estimates11 ,22 ,24 and falls below the threshold value for the loss of cost-effectiveness.11
Previous randomised controlled trials have been constrained by the fact that cancer prevention benefits are realised decades later. During this long quiescent period, the improvements in sanitation and hygiene may contribute to the observed decline in gastric cancer incidence. However, this decline occurs at a relatively slow pace in high-risk areas and populations. Despite a relatively small population, our study confirmed that active intervention can shorten this process. Regarding gastric cancer, our findings should be interpreted and compared with the results of previous randomised controlled trials only with great caution. The reduction in the incidence of gastric cancer observed in our study is partly attributable to early endoscopic detection in subjects with H pylori infection and partly due to improvements in sanitation and hygiene, but not due to the mass eradication of H pylori. However, the substantial reduction in gastric atrophy strongly supports the use of such programmes to prevent gastric cancer in H pylori-endemic areas.30 An additional benefit from this strategy is that the prevalence of peptic ulcer disease declined substantially after the intervention.
Our study has clarified each individual factor so as to determine which type of surveillance is appropriate after eradication of H pylori infection.31 In addition, our study investigated the potential side effect of mass eradication of H pylori, which has been scarcely addressed before. Cross-sectional studies have suggested that the widespread eradication of H pylori may lead to unforeseen dangers, such as increases in gastro-oesophageal reflux32 and childhood asthma.33 In support of this argument, the prevalence of endoscopic oesophagitis was found to double after treatment in the present study. Although a reduction in cancer risk may outweigh this potential drawback, further preventive strategies should be designed for this emerging disease.34
The major limitation of this study is that it was not a randomised controlled trial that generated groups with comparable baseline profiles to validate the effects of the studied treatment. Ethical considerations in this high-risk area precluded us from adopting such a study design. In addition, it is impracticable to assess the efficacy of chemoprevention in reducing premalignant lesions on the basis of a control group that did not undergo endoscopic examination in order to detect asymptomatic premalignant lesions or gastric cancers. Our use of data derived from the two-phase mass screening as a historical control renders the results more conservative than those based on a before and after study design because the effects of declining incidence have been taken into account. We therefore believe that our findings probably approximate the results of a randomised controlled trial. The second limitation is that we did not collect data on the change in antimicrobial resistance related to our widespread antibiotic treatment, which should be monitored in the ongoing third round of intervention. Third, although the effect of chemoprevention on gastric atrophy has been demonstrated, this does not guarantee a similar reduction in the incidence of gastric cancer. A meaningful result will only be obtained after a longer follow-up period. We estimated that, if gastric cancer incidence continues to follow-up the current trend, a significant risk reduction of 47% would be observed in 2015.
In summary, we have demonstrated that mass eradication of H pylori infection was associated with a significant reduction in gastric atrophy within a relatively short study period, in parallel with an increase in gastro-oesophageal reflux. Whether a meaningful reduction in gastric cancer can be achieved following the Correa pathway should be verified in a further long-term follow-up study in this region, which has a high prevalence of H pylori infection and a high incidence of gastric cancer.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data Supplement 1 - Online Appendix
Footnotes
-
Funding This study was supported by research grants from the Bureau of Health Promotion, Department of Health, Taiwan (DOH97-TD-M-113-95002), the National Science Council (NSC96-2314-B-002-092-MY3 and 99-2314-B-002-132-MY3), and the National Taiwan University Hospital (98-P21 and 99-P06). The funding source had no role in study design, data collection, analysis or interpretation, report writing or the decision to submit this paper for publication.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval The study protocol was approved by the institutional review board of National Taiwan University Hospital.
-
Provenance and peer review Not commissioned; externally peer reviewed.