Article Text

Statistics from Altmetric.com
We read with great interest the article by van der Meer et al 1 recently published in Gut. They found that a simple algorithm based on demographic and readily available laboratory variables is able to predict long-term prognosis of patients with chronic HCV infection and well-compensated, advanced liver disease. Indeed, in this time and age, an accurate assessment of the outcome of patients with HCV infection and advanced fibrosis is of utmost importance as prognostic subclassification may help prioritise those who are in urgent need of antiviral treatment within an homogeneous group of patients who are equally candidates to therapy. The findings of this study are especially relevant as the results were validated in an independent cohort of patients with similar disease stage.
The parameters identified in this study as predictors of long-term mortality (ie, age, gender, aminotransferases ratio and platelet count) have been previously recognised, alone or in scores, as indicators of advanced histology and prognosis in patients with chronic HCV infection, although patients included in these studies had various degrees of liver fibrosis, and therefore the relevance of some parameters may have been gauged.2 However, the aminotransferase ratio—likely the parameter with the greatest ‘weight’ in the van der Meer score—proved to be a good, short-term prognostic indicator even in patients with liver cirrhosis of viral aetiology and to be correlated with residual liver function.3 Thus, we deemed it of interest to assess whether the mortality score identified in the van der Meer et al study was also able to asses short-term prognosis of patients with established cirrhosis. As new antiviral treatments seem to have high efficacy even in patients with advanced liver disease and decompensated cirrhosis, we felt that an external validation of the mortality score in sicker patients may be of help in refining these patients’ prognosis and assessing urgency for treatment.4
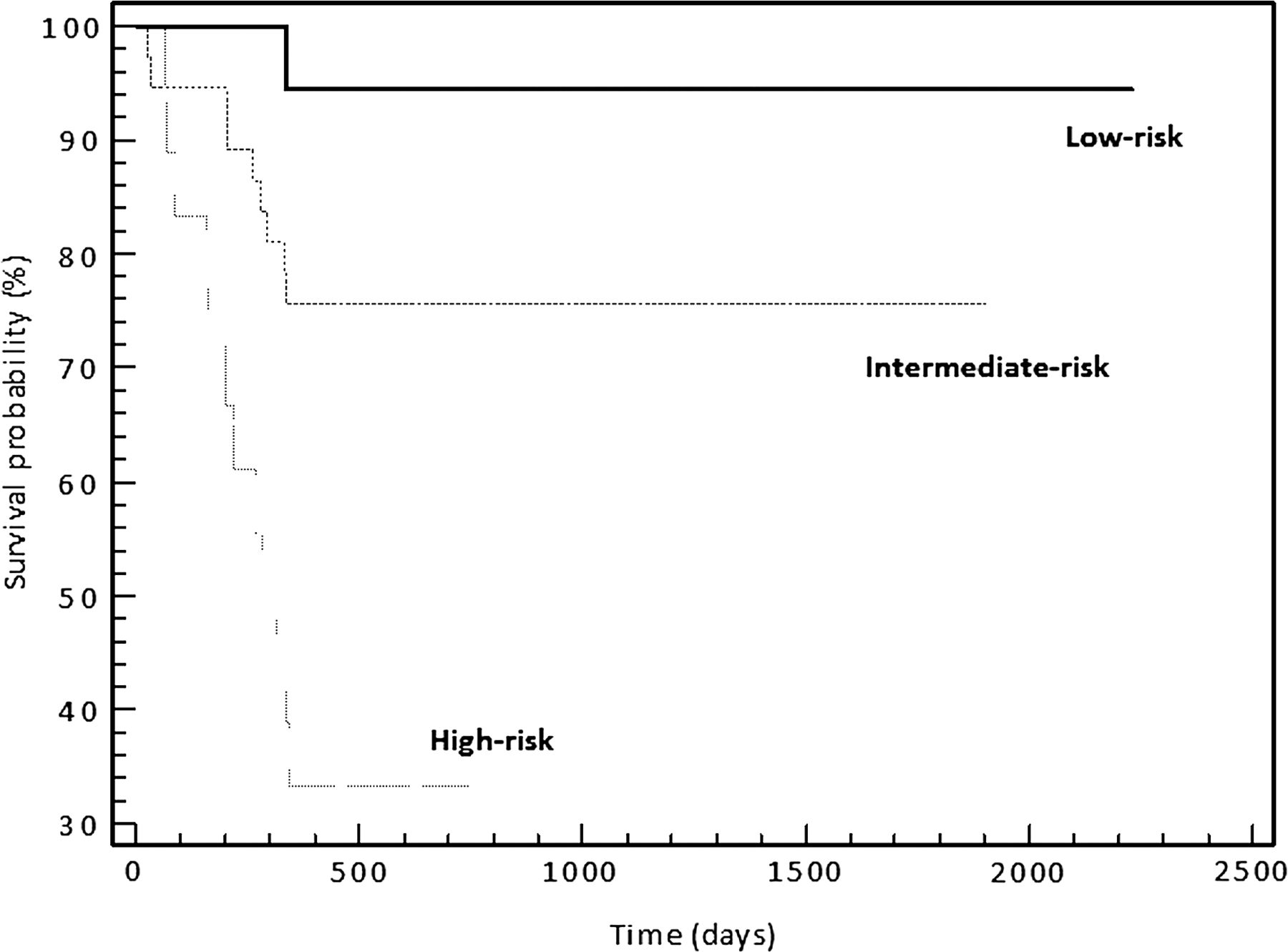
In order to carry this out, we reassessed the prognosis of the patients with HCV infection included in our previous study applying the mortality score identified in the van der Meer et al, study according to the formula: Rm=(6×age in years)−(platelet count per 109/L)+(258.8×log10(aspartate aminotransferase (AST)/alanine aminotransferase (ALT)))+(64.5 for male patients).1 ,3 We studied 73 patients (52 men, 71.2%) with HCV-related cirrhosis whose median age was 54 years (range, 34–81 years). Median aminotransferase ratio was 1.22 (range, 0.57–3.30) and median platelet count was 75×109/L (range, 29–238×109/L). In our cohort, the predictive accuracy for mortality of this score, as assessed by mean values of the C-statistic, was 0.789 (95% CI 0.677 to 0.876). We calculated the interquartile ranges for the Rm and categorised patients into three subgroups: low-risk (Rm<263.0), intermediate risk (263.0≤Rm≤369.5), and high-risk of mortality (Rm>369.5). In these three groups the 1-year mortality rates were 5.5%, 24.3% and 66.7%, respectively, with a statistically significant different survival among groups (p<0.0001, figure 1). All in all, we found that the mortality risk score proposed by van der Meer et al for assessing long-term prognosis of patients with HCV and advanced fibrosis proved to be an accurate predictor of short-term prognosis in patients with HCV and advanced liver disease as well. In our cohort, different score cut-offs for subclassification of patients’ prognosis were the reflex of more advanced disease with higher aminotransferase ratio and lower platelet counts.

{kind=link}
Kaplan–Meier survival curves of patients with advanced liver disease and chronic HCV infection, subdivided into three groups according to the mortality risk score (Rm): low-risk (Rm<263.0), intermediate risk (263.0≤Rm≤369.5) and high-risk of mortality (Rm>369.5).
To conclude, we feel that the mortality score proposed by van der Meer et al is a useful tool for predicting both short-term and long-term prognosis of patients with HCV infection and advanced liver disease, and its implementation in clinical practice may be a valuable aid so as to improve patient management.
Footnotes
Contributors EGG conceived the study, performed statistical analysis and drafted the manuscript. VS revised the manuscript.
Competing interests None.
Provenance and peer review Not commissioned; internally peer reviewed.