Article Text

Statistics from Altmetric.com
We read with great interest the recent publication by Barlass et al in which morphine was demonstrated to aggravate the severity of acute pancreatitis (AP) and delay pancreatic regeneration. These results indicated the risk of morphine use in AP-associated pain treatment.1 Similar to their observation, we found another interesting phenomenon that hypertriglyceridaemia (HTG), a prevalent metabolic disorder, delayed pancreatic regeneration after AP in mice and patients. Moreover, the delayed regeneration process could be ameliorated by lipid-lowering therapy.
Two models of HTG (drug induced: poloxamer 407 (P407) and gene modified: glycosylphosphatidylinositol-anchored high-density lipoprotein-binding protein 1 (GPIHBP1) deficiency) were employed to explore the effect of HTG on AP repair. AP induced by caerulein infusion in both normal triglyceride (NTG) mice and HTG mice caused pancreatic acinar cell necrosis. The injured pancreas was reconstructed in 3 days and recovered its normal architecture in 7 days in the NTG mice (figure 1A–C). However, we observed reduced morphological recovery in the HTG mice, especially in the severe HTG mice that presented with prolonged necrosis until 7 days (figure 1A–C, online supplementary figures 1–3). Furthermore, the key cellular responses involved in AP repair, including the fibroinflammatory response and acinar cell proliferation,2 were significantly delayed in the HTG mice (online supplementary figures 4–6). The above results suggested the possibility that the repair process associated with AP may be impeded by HTG.
Supplementary file 1
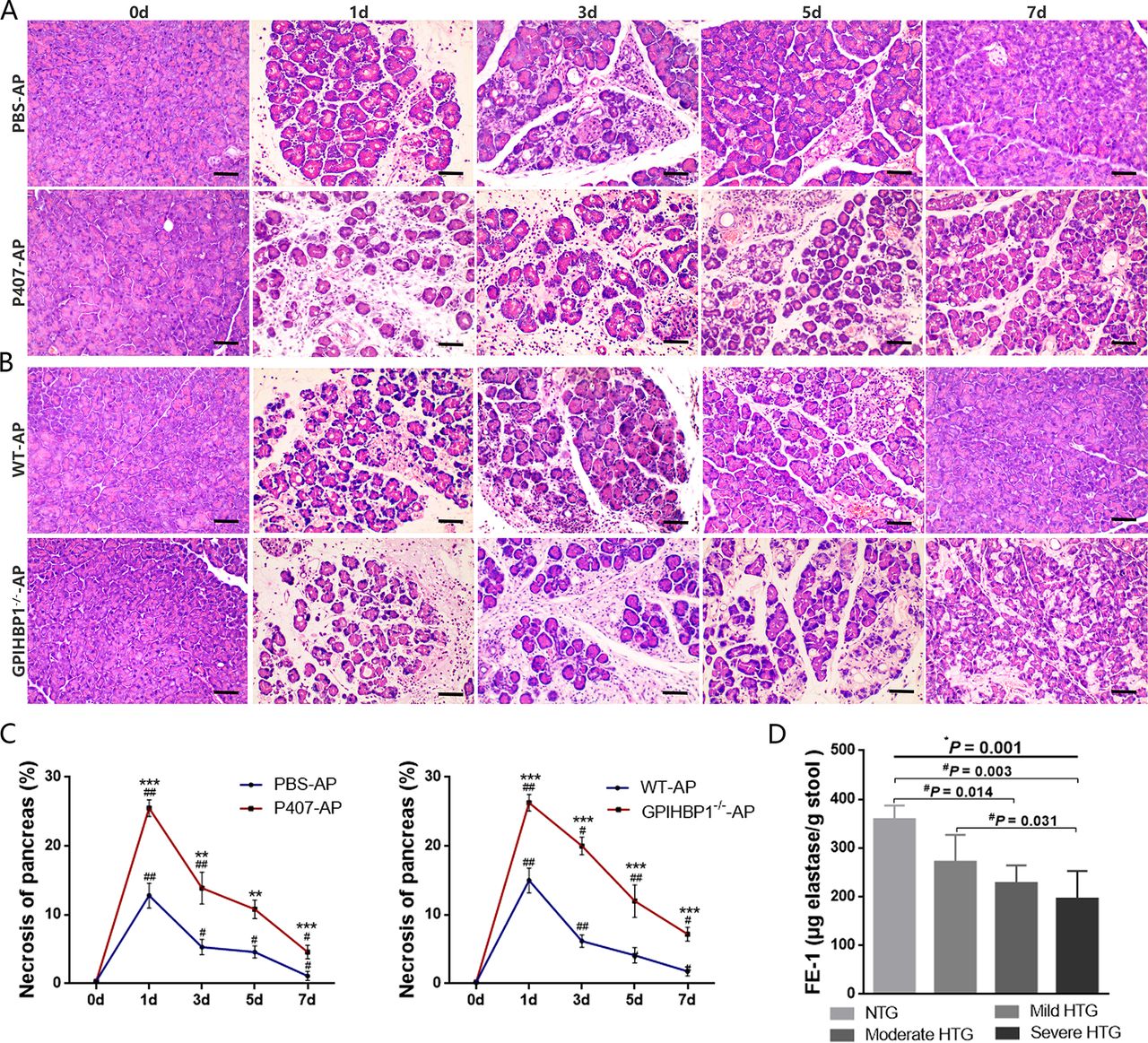
HTG inhibits pancreatic repair after caerulein-induced AP. (A) Representative histological changes in the pancreas of the P407-AP group (the HTG mice) and the phosphate buffer saline (PBS)-AP group (the NTG mice). HTG was induced using 0.5 g/kg P407 in the P407-AP group. The PBS-AP group was administered PBS instead of P407 in the same amount and duration. Scale bar: 50 µm. (B) Representative histological changes in the pancreas of the GPIHBP1−/−-AP group (the HTG mice) and the WT-AP group (the NTG mice). Scale bar: 50 µm. (C) Quantification of the necrotic area as a percentage of the total pancreatic sections at different time points (n=10 per group). *P<0.05, **P<0.01, ***P<0.001 vs control group; #P<0.05, ##P<0.01 vs prior time points. (D) Comparison of the FE-1 levels between the HTG categories in the patients with severe AP (n=11 for NTG, n=37 for mild HTG, n=11 for moderate HTG and n=14 for severe HTG). *One-way ANOVA for the trend was significant. #The Bonferroni test for post hoc analysis was significant. AP, acute pancreatitis; FE-1, faecal elastase 1; GPIHBP1, glycosylphosphatidylinositol-anchored high-density lipoprotein-binding protein1; HTG, hypertriglyceridaemia; NTG, normal triglyceride; P407, poloxamer 407; WT, wild type.
Many clinical studies have confirmed that HTG exacerbates the severity and prognosis of AP,3 but the effect of HTG on pancreatic regeneration in patients is still unknown. Here, we conducted a 1-year follow-up study (online supplementary figure 7, supplementary table 1) to investigate the influence of serum triglyceride (TG) levels on pancreatic recovery in patients with severe AP. Obtaining pancreas samples from patients with AP is difficult. Given that the exocrine function of the pancreas is injured after AP resulting in gradual recovery,4 faecal elastase-1 (FE-1), a hallmark of pancreatic exocrine function, was measured to indirectly evaluate pancreas regeneration.5 We found that FE-1 levels decreased with an increase in serum TG levels (P trend <0.001; figure 1D).
We further investigated whether the observed results are reversible by treating HTG with TG-lowering agents after the onset of AP. Fenofibrate, the most common agent used clinically for decades, was repeatedly administered 6 hours after the initial injection of caerulein (figure 2A). Compared with 100 mg/kg/day and 100 mg/kg/twice daily of fenofibrate, 100 mg/kg/three times a day fenofibrate significantly lowered serum TG levels in the HTG-AP mice in 3 days (figure 2B, online supplementary figure 8). Histopathological examination showed no difference in pancreatic morphology between the HTG-AP and fenofibrate-treated groups at 1 day and 3 days, indicating that fenofibrate had no effect on the severity of early-stage AP (figure 2C,D). Progressively, compared with the control group, the 100 mg/kg/three times a day fenofibrate-treated HTG group had reduced necrosis and enhanced expansion of acinar cells at 5 days, while the other two dosages had no comparable effect (figure 2C,D, online supplementary figure 8A,C). In addition, this improvement was not observed in the NTG mice (online supplementary figures 9–10).

{kind=link}
{kind=link}
Fenofibrate promotes pancreatic recovery in HTG mice after caerulein-induced AP. HTG was induced using 0.5 g/kg P407 in the P407-AP group. (A) Timetable of fenofibrate administration (100 mg/kg/three times a day by gavage 6 hours after the initial injection of caerulein). (B) Serum TG and TC levels of HTG mice at different time points after AP induction (n=10 per group). (C) Quantification of the necrotic area as a percentage of the total pancreatic sections after AP induction (n=10 per group). (D) Representative histological changes in the pancreas. Scale bar: 50 µm. *P<0.05, **P<0.01, ***P<0.001 vs control group; #P<0.05, ##P<0.01 vs prior time points. AP, acute pancreatitis; GPIHBP1, glycosylphosphatidylinositol-anchored high-density lipoprotein-binding protein1; HTG, hypertriglyceridaemia; P407, poloxamer 407; TC, total cholesterol; TG, triglyceride.
In conclusion, we demonstrate that HTG is a risk factor for a delay in AP regeneration, which can be reversed by intensive fenofibrate administration after the onset of AP. Whether TG-lowering therapy is necessary after AP is controversial.6 Our present results may provide a new perspective for clinical practice.
Footnotes
NY, BL and YP contributed equally.
Contributors NY, BL and YP performed experiments, analysed data, prepared figures and wrote the manuscript. JT collected patients’ information and evaluated data of human samples. GeL edited the manuscript. WL and GuL conceived the study, supervised and directed experiments, analysed data, provided funding and edited the manuscript.
Funding This work was supported by the National Natural Science Foundation of China (no. 81570584), Key Research and Development Program Foundation of Jiangsu Province of China (no. BE2015685) and Postdoctoral Science Foundation of China (2014M562664).
Disclaimer The views expressed in the submitted manuscript are our own and not an official position of the institution or funder.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The Ethics Committee of Jinling Hospital.
Provenance and peer review Not commissioned; externally peer reviewed.
Correction notice This article has been corrected since it published Online First. Figure 1 has been updated.