Article Text

Abstract
Objective Scheduled endoscopic dilatation of dominant strictures (DS) in primary sclerosing cholangitis (PSC) might improve outcome relative to endoscopic treatment on demand, but evidence is limited. Since randomisation is difficult in clinical practice, we present a large retrospective study comparing scheduled versus on-demand endoscopic retrograde cholangiopancreatography (ERCP) based on patient preferences.
Design Between 1987 and 2017, all new patients with PSC had been offered scheduled ERCP with dilatation of a DS if diagnosed; the latter was repeated at defined intervals until morphological resolution, independent of clinical symptoms (treatment group). Patients who refused participation were clinically evaluated annually and received endoscopic treatment only on demand (control group). The primary clinical endpoint was transplantation-free survival. Secondary outcomes were overall survival, bacterial cholangitis episodes, hepatic decompensation of liver cirrhosis and endoscopy-related adverse events.
Results The final study included 286 patients, 133 (46.5%) receiving scheduled ERCP and 153 (53.5%) receiving on-demand ERCP. After a mean follow-up of 9.9 years, the rate of transplantation-free survival was higher in patients receiving scheduled ERCP (51% vs 29.3%; p<0.001), as was transplantation-free survival time (median: 17.9 vs 15.2 years; log-rank: p=0.008). However, the benefit of scheduled ERCP was significant only in patients with the initial (17.1%) or later (45.5%) diagnosis of a DS (17.8 vs 11.1 years; log-rank: p<0.001). IBD (p=0.03), DS (p=0.006), higher Mayo Risk Score (p=0.02) and non-adherence to scheduled endoscopy (p=0.005) were independently associated with transplantation-free survival.
Conclusion In our large retrospective study, regular ERCP with endoscopic balloon dilatation significantly benefits patients with PSC with DS, diagnosed both at initial presentation and during surveillance, even if asymptomatic. Further studies have to find out how to best identify stricture patients non-invasively.
- biliary strictures
- biliary endoscopy
- cholestatic liver diseases
- primary sclerosing cholangitis
- endoscopic retrograde pancreatography
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- biliary strictures
- biliary endoscopy
- cholestatic liver diseases
- primary sclerosing cholangitis
- endoscopic retrograde pancreatography
Significance of this study
What is already known on this subject?
Primary sclerosing cholangitis (PSC) is a chronic cholestatic liver and biliary tract disease with a variable natural history. Reported benefits following endoscopic treatment of dominant strictures (DS) include short-term improvement of symptoms and of liver biochemical tests, as well as a longer predicted survival. The impact on actual long-term survival of scheduled endoscopic treatment independent of symptoms, up to resolution of DS at cholangiography, has not been evaluated thus far.
What are the new findings?
Scheduled endoscopic surveillance and treatment of DS in patients with PSC may reduce hepatic decompensation and biliary infectious complications. Detection rate of DS was higher in patients receiving annual endoscopic retrograde cholangiopancreatography (ERCP) than in those receiving ERCP only in case of overt clinical and/or laboratory signs of biliary obstruction or cholangitis. Subsequently, adherence to scheduled endoscopic therapy in patients with PSC with DS was associated with longer transplantation-free survival compared with patients with on-demand therapy.
How might it impact on clinical practice in the foreseeable future?
In patients with PSC, timely detection and repeated endoscopic therapy for DS up to sustained resolution of biliary obstruction, even in the absence of laboratory or clinical signs of cholangitis, should be performed to prevent chronic liver damage caused by biliary obstruction and infectious complications.
Introduction
Primary sclerosing cholangitis (PSC) is a chronic cholestatic liver and biliary tract disease with a variable natural history.1 2 Clinical symptoms and complications of the disease result from fibrosis and strictures involving extrahepatic and intrahepatic bile ducts.3–6 PSC may have a progressive course, leading to recurrent biliary tract obstruction, recurrent episodes of cholangitis and, ultimately, end-stage liver disease. Biliary obstruction may develop at all levels of the biliary tree, but endoscopic therapy is possible only for large bile ducts and is recommended for strictures described as dominant strictures (DS). At cholangiography, DS are defined as stenoses measuring <1.5 mm in the common bile duct or <1.0 mm in the hepatic ducts.7 8 DS are detected at the initial clinical presentation of PSC in up to one-half of patients and frequently will develop over the course of the disease.9 10 Reported benefits following endoscopic treatment of DS include short-term improvement of symptoms and liver biochemical test results, as well as a longer transplantation-free survival than that predicted using the Mayo clinical risk model.8 9 11–15 Thus, in different guidelines, endoscopic treatment is recommended for suspected DS in patients with PSC who present with symptoms likely to improve following endoscopic treatment.16 17
The impact on actual long-term survival, rather than predicted survival, of scheduled endoscopic treatment independent of symptoms, up to resolution of DS at cholangiography, has not been evaluated thus far. In the present trial, we compared clinical outcome and long-term survival of patients with PSC adhering to a scheduled endoscopic surveillance and treatment programme versus patients with PSC receiving endoscopic diagnosis and therapy on clinical demand only.
Methods
Study population and design
In this retrospective analysis in patients with PSC we evaluated the effect of a scheduled endoscopic surveillance and treatment regimen maintained over 30 years. From May 1987 through January 2017, a total of 429 patients with confirmed PSC were considered for inclusion in the study, 143 of whom were excluded. Ten patients declined to participate in the study, 96 patients were evaluated for liver transplantation due to advanced-stage PSC at first visit and 14 patients had malignancies at the first visit (11 cholangiocarcinoma [CCA], 1 hepatocellular carcinoma, 2 colorectal carcinoma). Fifteen patients were lost to follow-up and were not considered in the final evaluation. In eight patients, the diagnosis of PSC was not confirmed. Thus, the final study cohort consisted of 286 patients and all of them were followed up until June 2017. During the first visit, all patients were recommended to participate in a scheduled endoscopic surveillance programme. This programme comprised diagnostic endoscopic retrograde cholangiopancreatography (ERCP) at yearly intervals and endoscopic treatment of identified DS up to morphological resolution (figure 1) (the scheduled group). Patients who refused participation in this scheduled endoscopic programme were monitored at least annually (clinical evaluation, serum liver test and liver imaging) and received endotherapy only if required (on-demand group). This was considered necessary in the case of pruritus, jaundice, acute bacterial cholangitis or suspected obstructive cholestasis on imaging, in line with the clinical symptoms. This applied also to an increase of serum bilirubin and/or alkaline phosphatase by 20% or more, although no absolute cut-offs were defined. In the scheduled group, despite minor adaptations in the treatment interval and minor changes of endoscopic techniques during the study period, the aim of endoscopic treatment, namely morphological resolution of the stricture, and endoscopic surveillance, namely ERCP at yearly intervals, was sustained throughout the study period. Physical examination, biochemical blood tests, sonographic examination of the liver or MRI/MR cholangiopancreatography (MRCP) (since 2002) were performed at entry and at least once per year in all patients. The introduction of MRI/MRCP was primarily intended to detect focal lesions (CCA surveillance) and parenchymal changes and to gain experience in the biliary assessment, but the method has not yet been applied and validated for the detection of DS. Originally, a liver biopsy was taken in all patients at entry into the study. Since in PSC liver biopsies are of only limited clinical value, starting from 2001 a liver biopsy was no longer considered a prerequisite for entry into the study. All biopsies were read blindly. In altogether 137 patients the diagnosis was confirmed by biopsy. Up to 1995, all patients were treated with ursodeoxycholic acid (UDCA) (Dr Falk, Freiburg, FRG) 750 mg/day (9–15 mg/kg/day). Since cholestasis may lead to reduced absorption of UDCA14 and increasing evidence has shown that higher doses may be more effective,9 10 starting in 1995 the patients were treated with an increased dose of 750–1250 mg/day (14–17 mg/kg/day) and starting from 2001 with 1000–1750 mg/day (18–21 mg/kg/day). Liver transplantation or death was considered as the combined primary endpoint. Allocation of liver graft changed during the study period. Since 2003 liver grafts were allocated according to the Model of End Stage Liver Disease (MELD) score via Eurotransplant, with the option of an exceptional MELD for patients with PSC. Secondary outcomes consisted of occurrence of procedure-related complications, occurrence of events associated with decompensation of liver function/cirrhosis including variceal bleeding, ascites, spontaneous bacterial peritonitis, hepatorenal syndrome and hepatic encephalopathy. Occurrence of episodes of acute bacterial cholangitis and hospitalisation due to cholangitis were also considered secondary endpoints. Cholangitis was defined as fever and/or abdominal pain and jaundice, or in case all of the components of the triad were not present, additional laboratory data and imaging findings supporting inflammation and biliary obstruction. The Mayo Risk Score (MRS) was calculated as follows: MRS (R)=(0.0295 * (age in years)) + (0.5373 * LN(total bilirubin in mg/dL)) − (0.8389 * (serum albumin in g/dL)) + (0.5380 * LN(AST in IU/L)) + (1.2426 * (points for variceal bleeding)).

Protocol for scheduled endoscopic surveillance and therapy. Endoscopic surveillance was performed at yearly intervals. In case of detection of dominant stricture, repeated balloon dilatation was performed until sustained resolution of biliary obstruction was achieved. ERC, endoscopic retrograde cholangiography.
Endoscopic procedures, surveillance and scheduled dilation
At entry, the biliary system was visualised by ERCP in each patient. ERCP was performed under conscious sedation using a therapeutic duodenoscope. Standardised cannulation of the common bile duct and endoscopic sphincterotomy was performed as previously described.18 19 DS was defined as a stenosis of the common duct with a diameter smaller than 1.5 mm or a stenosis of a hepatic duct (within 2 cm of the bifurcation) with a diameter smaller than 1.0 mm.19 For reasons of practicability, biliary catheters were used during the procedures as references for stenosis size. In disputable (borderline) cases a decision for the intervention was favoured.
In patients in whom DS were identified after passing of a guidewire, stepwise balloon dilations of the strictures starting from 12 F or 18 F were performed. Common bile duct DS were dilated up to 24 F, whereas DS of the hepatic ducts up to 2 cm proximal to the bifurcation were dilated to a maximum of 18 F. Bile duct diameter upstream and downstream of the DS was taken into account when selecting balloon diameter to avoid dilation to more than the duct diameter. In the beginning of the study, in a minority of patients (n=5), a plastic stent (10 F) was placed for 1–2 weeks in addition to dilation, but this approach was stopped thereafter. All patients were kept overnight in the hospital and received antimicrobial prophylaxis according to our internal institutional standard. The peri-interventional antibiotic regimen was identical for all patients. The standard regimen in our institution was intravenous mezlocillin; in the case of known allergy to penicillins, ciprofloxacin was used and individually adapted according to corresponding bile culture if possible.
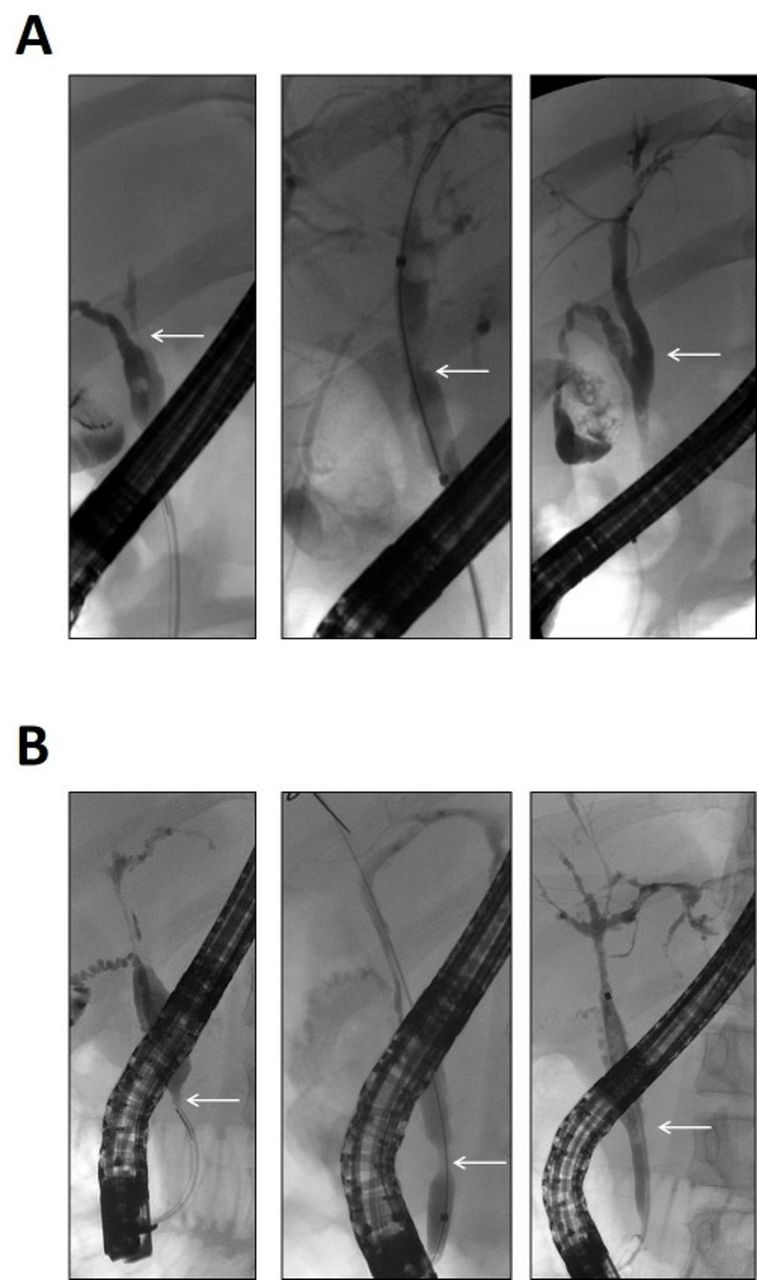
Balloon dilation was repeated until success, as assessed by opening of the stricture on repeat cholangiography, at 4-week intervals until 2006. Since 2006, the protocol was slightly modified with repetition of the dilation after 4 weeks, 3 months and 6 months up to morphological resolution. Subsequently, patients underwent diagnostic ERCP at yearly intervals. In case of worsening of cholestasis or clinical symptoms or acute cholangitis, ERCP was performed as soon as possible, independently from the protocol. Morphological resolution was defined as either no more detectable sign of previous stricture on cholangiography (figure 2A), or only a slight narrowing of the bile duct as residuum of the previous stricture (figure 2B), but in all cases an unhindered passage of biliary catheters and unobstructed passage of contrast medium through the balloon-dilated biliary segment were minimum requirements. Recurrence of DS was defined as diagnosis of a biliary stricture after a time interval of more than 3 months after the last intervention. In case of recurrent or newly developed DS, the scheduled protocol was restarted (figure 1). Procedure-related complications were recorded as secondary outcomes including cholangitis, bleeding, perforation and pancreatitis. The criteria to diagnose post-ERCP pancreatitis were according to the 1991 consensus report by Cotton et al.20
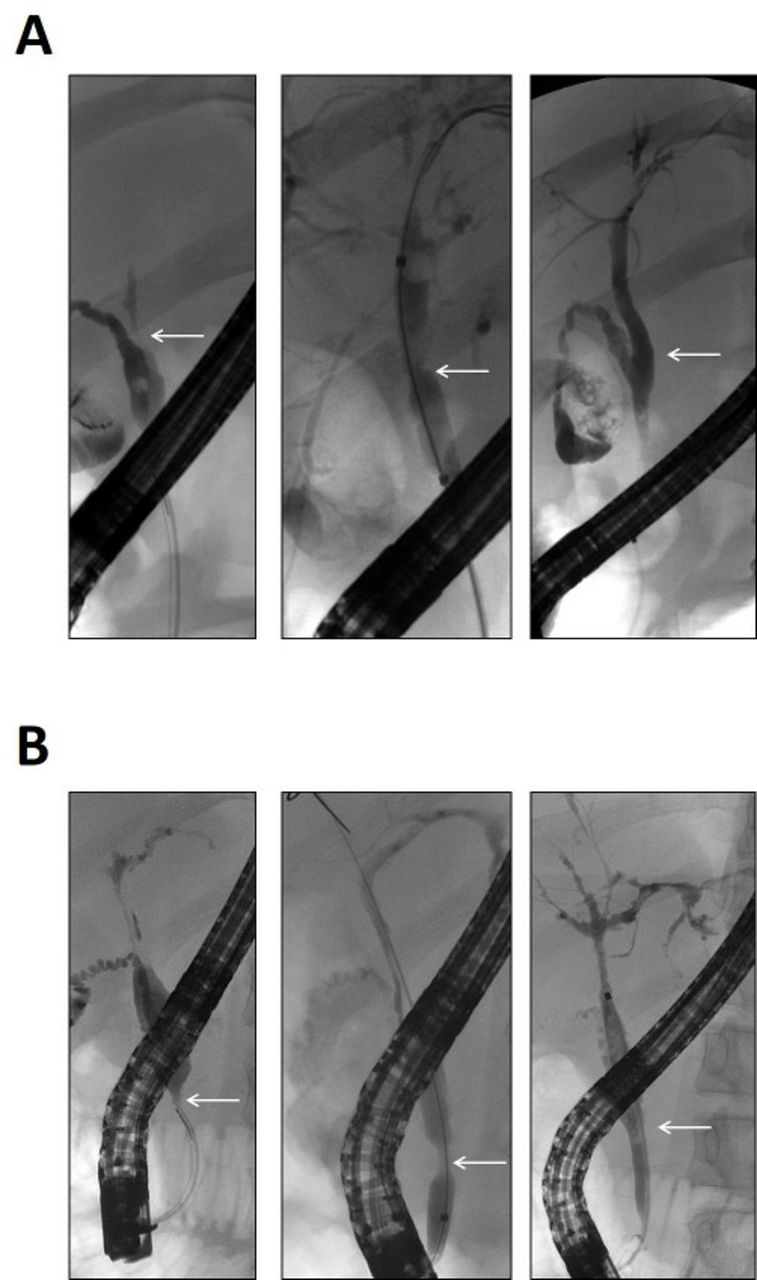
Endoscopic treatment until morphological resolution of dominant stricture. (A) White arrow indicates a dominant stricture of the common hepatic duct (left panel), repeated balloon dilation was performed (middle panel), until no more sign of previous stricture on cholangiography was detectable (right panel). (B) White arrow indicates a dominant stricture of the common bile duct with additional dilation of the upstream segment (left panel). Repeated balloon dilation was performed (middle panel) and finally only a slight narrowing of the bile duct as residuum of the previous stricture and regression of the upstream dilation was demonstrated (right panel).
All patients were offered participation in this programme. For the retrospectively performed analysis patients were allocated to the scheduled group if they adhered to the scheduled surveillance and interventions until the end of the study period. Of the 133 patients in the treatment group all but 12 patients (9.0%) adhered consequently to our scheduled intervals. The remaining 12 patients prolonged the interval beyond our scheduled intervention during the surveillance period marginally (weeks to months), but returned to frequently endoscopic surveillance thereafter. Patients were allocated to the on-demand group if they or transferring physicians decided to perform endoscopic diagnosis and treatment only on clinical demand, or treatment of DS was terminated after clinical improvement but not completed up to morphological resolution.
Statistical analysis
Calculations were carried out using PASW Statistics V.22 (IBM, Armonk, New York, USA). Frequencies were compared using the χ2 test or the Fisher’s exact test, where appropriate. Continuous data were compared using the non-parametric Wilcoxon rank-sum test. Actuarial transplantation-free survival was estimated using a Kaplan-Meier product limit estimator. Differences between the actuarial estimates were tested using the log-rank test. Factors that independently affected the risk of reduced transplantation-free survival were determined using Cox proportional HR models with simultaneous adjustment for gender, age at diagnosis, presence of IBD, presence of DS, presence of PSC with features of autoimmune hepatitis (AIH), MRS at baseline, number of endoscopic interventions and non-adherence to scheduled endoscopy. Statistical significance was set at p<0.05.
Consent
Written informed consent for clinical and laboratory data acquisition and analysis was obtained from each patient at entry into the study. Data acquisition and evaluation was approved by the local ethics committee of Heidelberg University (S-043/2011) and conformed to the ethical guidelines of the Declaration of Helsinki, as reflected in an a priori approval by the institution’s human research review committee. Informed consent for endoscopic intervention was obtained before each ERCP.
Results
Baseline characteristics
The final study cohort consisted of 286 patients with confirmed PSC. All patients were treated with UDCA (9–21 mg/kg/day). One hundred and thirty-three (46.5%) of them adhered to our proposed protocol (scheduled) and 153 (53.5%) received ERCP if DS was suspected (on demand). Table 1 reports baseline characteristics of the entire study cohort and the subgroups. At entry into the study no clinical or laboratory differences were detectable. The number of patients with DS at first diagnosis was equal between both groups (27 [20.3%] vs 22 [14.4%], p=0.2). Morphology of DS at entry into the study was also equally distributed between both groups (scheduled: extrahepatic 17 [63.0%], intrahepatic 10 [37.0%] vs on demand: extrahepatic 13 [59.1%], intrahepatic 9 [40.9%]; p=0.8) (online supplementary table 1) and we could not detect any significant difference between both groups with regard to histological stage at first presentation (online supplementary table 2).
Supplementary file 1
Supplementary file 2
Clinical baseline characteristics of patients according to endoscopic surveillance strategy
Endoscopic interventions and success rate
At entry into the study all patients received ERCP for confirmation of PSC diagnosis and balloon dilatation if DS was detected. In total, more than 1800 ERCPs with approximately 600 balloon dilatations were performed in our cohort. In 179 (62.6%) patients, DS was diagnosed. Forty-nine (17.1%) patients had DS at the first diagnosis; the remaining 130 (45.5%) patients developed DS during the course of disease. Patients in the scheduled group had more diagnostic and therapeutic ERCPs compared with the on-demand group (average number of ERCPs with no DS: scheduled 6 [range: 2–17] vs on demand 1 [range 1–3]; DS at first diagnosis: scheduled 18 [range: 2–23] vs on demand 3 [range 1–8]; DS during course of disease: scheduled 18 [range: 1–27] vs on demand 3 [range 1–11] [online supplementary table 3]). On average, two (range: 1–8) sequential balloon dilatations were necessary to resolve DS. Recurrent DS was detected in 76 patients (scheduled: 49 [48.5%] vs on demand: 27 [34.6%]; p=0.07). While frequency of symptomatic DS at first presentation was comparable between both cohorts (scheduled: 17 [12.8%] vs on demand 22 [14.4%]) the detection rate of new DS during the course of disease was higher in the scheduled group compared with the on-demand group (74/133 [55.6%] vs 56/153 [36.6%]; p=0.001). Mean time until first detection of DS was 5.0 years (range: 0.9–23.5 years), mean number of ERCPs until first detection of DS was 3.9 (range: 1–15). In 12 (9.0%) patients in the scheduled group, endoscopic therapy became necessary before the scheduled ERCP due to acute cholangitis. In all cases, a new DS was diagnosed and dilatations according to our programme were started again. With exception of the first diagnostic ERCP to confirm the diagnosis of PSC, in the on-demand group, the most common indications for ERCP were acute bacterial cholangitis (54 [35.3%]), jaundice (31 [20.3%]) and pruritus (13 [8.5%]).
Supplementary file 3
Clinical endpoints
At the end of the study period, 117 (40.9%) patients reached a primary clinical endpoint. Fifty-five (19.2%) patients died and 82 (28.9%) underwent liver transplantation. The number of clinical endpoints differed significantly between subgroups. In the scheduled group, 39 (29.3%) patients reached a clinical endpoint (33 orthotopic liver transplantation [OLT, 24.8%]; 6 [4.5%] death), compared with 78 (51.0%) in the on-demand group (49 OLT [32.0%]; 29 [18.9%] death; p<0.001). CCA was diagnosed in 22 (7.7%) patients, of which 7 (5.3%) were in the scheduled group and 15 (9.8%) were in the on-demand group (p=0.1). Causes of death were primarily liver related with decompensation of liver function (scheduled: 0 [0.0%] vs on demand: 14 [9.2%]) and CCA (scheduled: 5 [3.8%] vs on demand: 13 [8.5%]). Three patients died due to IBD-associated colon carcinoma (scheduled: 1 [0.8%] vs on demand: 2 [1.3%]) (figure 3).
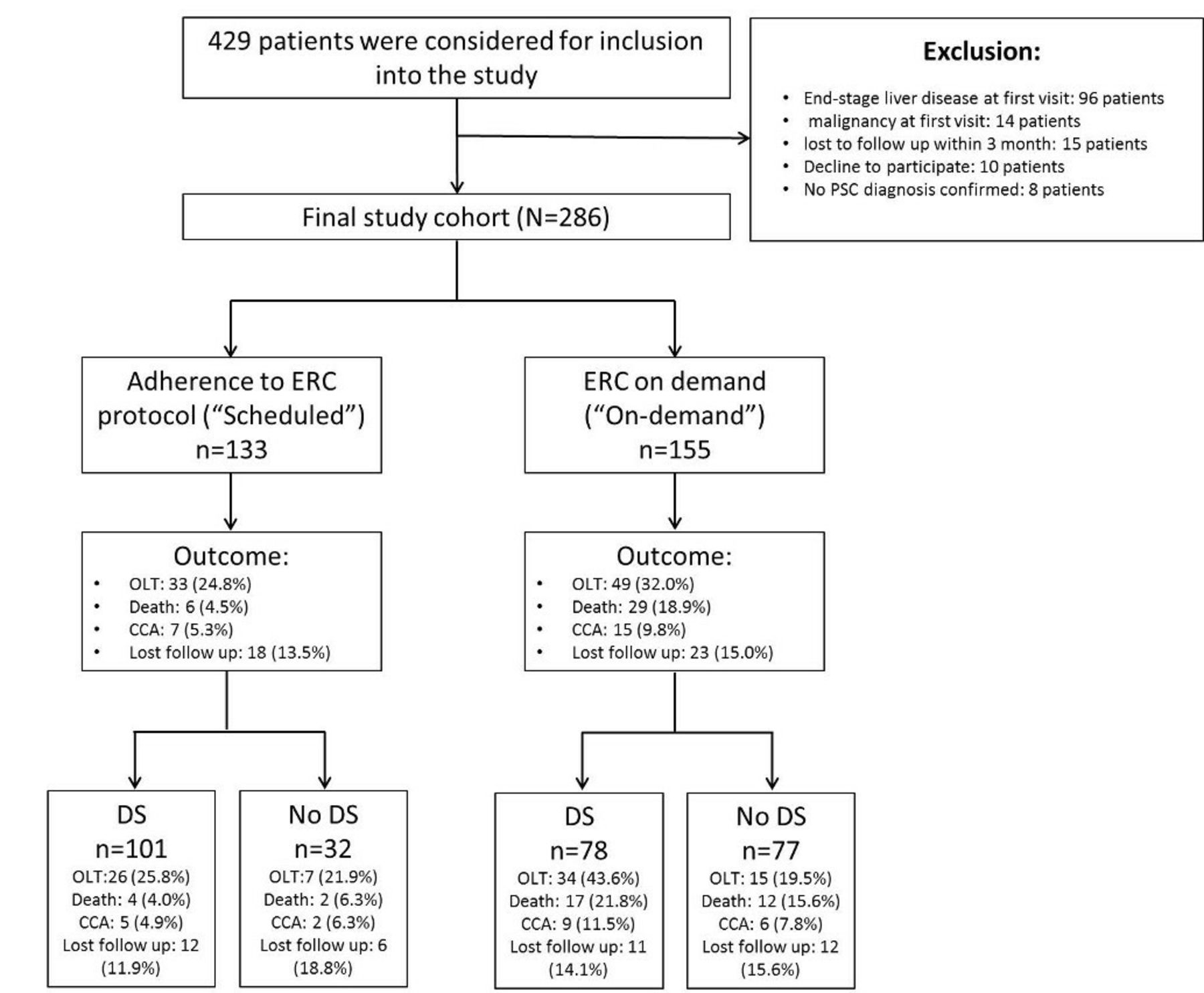
Flow chart. CCA, cholangiocarcinoma; DS, dominant stricture; OLT, orthotopic liver transplantation; PSC, primary sclerosing cholangitis.
Secondary outcomes
Overall survival was higher in the treatment group compared with the control group (30.2 years vs 22.5 years, p<0.001). While we found comparable laboratory parameters at baseline, cholestasis parameters showed increasing differences during the further course of disease between both groups. As shown in the online supplementary table 4A–C, alkaline phosphatase (AP), gamma glutamyl transferase (GGT) and serum bilirubin values remain almost stable within the first 5 years in the scheduled group, whereas it increased in the on-demand group. With regard to infectious complications associated with PSC, more patients developed recurrent bacterial cholangitis with need for hospitalisation and antibiotic therapy in the on-demand group (scheduled: 23 [17.3%] vs on demand: 53 [34.6%]; p=0.001). Furthermore, hepatic decompensation occurred more often and earlier in the course of disease in the on-demand group during the course of disease with more life-threatening complications, for example, variceal bleedings (scheduled: 13 [9.8%] vs on demand: 34 [22.2%]; p=0.005; online supplementary table 5).
Supplementary file 5
Supplementary file 5
Complications
Complications calculated per patient included post-ERCP pancreatitis (13 occurrences in 11 patients, 3.8%, treated by conservative routine measures), bacterial cholangitis (eight occurrences in five patients; 1.8%) and bile duct perforation (one occurrence in one patient; 0.3%). We could not detect any difference between the scheduled and on-demand groups concerning complication rates. Although there was a trend for higher complication rates during the first ERCP, this effect was not statistically significant (online supplementary table 6). All complications could be managed by conservative treatment. No patient died due to complications associated with endoscopic procedures.
Supplementary file 6
Transplantation-free survival
The median transplantation-free survival in our study cohort was 16.7 years. Patients in the scheduled group had significantly longer transplantation-free survival compared with patients in the on-demand group (5-year survival rate: 84% vs 67%; 10-year survival rate: 69% vs 50%; 20-year survival rate: 40% vs 25%). Analysis of time to event (event defined as transplantation or death) showed significant difference between both groups (17.9 vs 15.2 years; log-rank: p=0.008; figure 4A). Further subgroup analysis revealed superior survival due to scheduled endoscopic intervention only in patients with the presence of DS (17.8 vs 11.1 years; log-rank: p<0.001; figure 4B), whereas in patients without DS, transplantation-free survival was not affected by scheduled endoscopic surveillance (21.0 vs 18.7 years; log-rank: p=0.8; figure 4C). When considering only death as endpoint superior survival was found for the scheduled group in the entire study cohort and the subgroup of patients with DS (entire cohort: 28.3 vs 21.9 years; log-rank: p=0.001; DS at first diagnosis: 28.3 vs 18.2 years; log-rank: p<0.001) (online supplementary figure 1A–C). When handling death as competing risk due to transplantation (online supplementary figure 2A–C), no difference between the scheduled and on-demand groups was seen (online supplementary figure 3A). However, subgroup analysis confirmed superior OLT-free survival due to scheduled endoscopic intervention only in patients with DS (online supplementary figure 3B,C). The subgroup of patients with DS at first diagnosis showed also improved transplantation-free survival for patients with adherence to our proposed protocol (17.8 vs 12.1 years; log-rank: p=0.02) (online supplementary figure 4A). If patients with DS at first diagnosis were excluded from analysis the beneficial effect of scheduled endoscopic intervention persists for the whole study cohort and patients with development of DS during the course of disease (entire cohort: 18.7 vs 16.3 years; log-rank: p=0.03; DS during course of disease: 16.8 vs 9.6 years; log-rank: p<0.001) (online supplementary figure 4B–D). Despite mild adaptions of endoscopic treatment and dosing of UDCA we could confirm the beneficial effect of our scheduled approach during the entire course of the study, although the proportion of patients adhering to our protocol was higher in the last decade of our study (1987–2005: scheduled 57/173 [32.9%] vs 2006–2017: scheduled 76/113 [67.3%]; p=0.001) (online supplementary figure 5A,B).
Supplementary file 7
Supplementary file 8
Supplementary file 9
Supplementary file 10
Supplementary file 11

{kind=link}
{kind=link}
{kind=link}
![[gutjnl-2018-316801supp007.jpg]](https://gut.bmj.com/content/gutjnl/68/12/2170/DC7/embed/inline-supplementary-material-7.jpg?download=true){kind=link}
![[gutjnl-2018-316801supp008.jpg]](https://gut.bmj.com/content/gutjnl/68/12/2170/DC8/embed/inline-supplementary-material-8.jpg?download=true){kind=link}
![[gutjnl-2018-316801supp009.jpg]](https://gut.bmj.com/content/gutjnl/68/12/2170/DC9/embed/inline-supplementary-material-9.jpg?download=true){kind=link}
![[gutjnl-2018-316801supp010.jpg]](https://gut.bmj.com/content/gutjnl/68/12/2170/DC10/embed/inline-supplementary-material-10.jpg?download=true){kind=link}
![[gutjnl-2018-316801supp011.jpg]](https://gut.bmj.com/content/gutjnl/68/12/2170/DC11/embed/inline-supplementary-material-11.jpg?download=true){kind=link}
{kind=link}
Kaplan-Meier analysis. Kaplan-Meier estimation confirmed the significant difference in transplantation-free survival between scheduled (red) and on-demand groups (blue) (17.9 vs 15.2 years; log-rank: p=0.008) (A). Further subgroup analysis revealed superior survival due to scheduled endoscopic intervention only in patients with the presence of DS (17.8 vs 11.1 years; log-rank: p<0.001) (B), whereas in patients without DS, transplantation-free survival was not affected by scheduled endoscopic surveillance (21.0 vs 18.7 years; log-rank: p=0.8) (C).
Univariate and multivariate analysis
To determine the factors that might influence transplantation-free survival, univariate and multivariate analyses were performed for the following baseline factors: gender, age at diagnosis, presence of IBD, presence of DS, presence of PSC with features of AIH, MRS at baseline, number of endoscopic interventions and non-adherence to scheduled endoscopy. In univariate analysis, age at first diagnosis, the presence of DS, MRS and non-adherence to scheduled endoscopy were statistically significantly associated with reduced transplantation-free survival. Multivariate analysis confirmed presence of DS, presence of IBD, MRS and non-adherence to scheduled endoscopy as independent risk factors for poor outcome (table 2).
Cox regression analysis
Data show prospective factors for longer survival until liver transplantation or death. In univariate analysis, age at first diagnosis, presence of DS, MRS and non-adherence to scheduled endoscopy were associated with reduced actuarial transplantation-free survival. In multivariate analysis, presence of DS, presence of IBD, MRS and non-adherence to scheduled endoscopy reached significance (p<0.05).
Discussion
In the present study in a large cohort of patients with PSC, we evaluated the outcome of an endoscopic surveillance and treatment programme with a follow-up of almost 30 years. We implemented a strategy for treatment of DS with repeated balloon dilatation until morphological resolution, independent of clinical symptoms. This approach is in disagreement with the recommendations of the American College of Gastroenterology and European Society of Gastrointestinal Endoscopy/European Association for the Study of the Liver, which suggest performing endoscopic treatment of DS only in patients with pruritus and/or cholangitis to relieve symptoms.16 17 After therapeutic success, defined as morphological resolution of DS, ERCP for diagnostic purposes was repeated at yearly intervals and the dilatation programme was initiated again if recurrent or newly developed DS occurred, again independent of clinical symptoms or cholestatic enzyme levels. In patients adherent to our proposed scheduled endoscopic surveillance and treatment programme, we observed a markedly increased transplantation-free survival compared with that in patients who underwent ERCP only on demand in case of proven or suspected obstructive cholestasis or cholangitis. This effect was especially pronounced in patients with DS, whereas in patients without DS, endoscopic surveillance had no significant impact on survival. The observed survival of our entire cohort was comparable to a recently reported Dutch population21 and considerably better than values reported in earlier series.22–25 The fact that, in our series, systematic endoscopic intervention in patients with DS compensated for the prognostic disadvantage in the survival rate among patients without DS is of particular importance. Complications of PSC are a direct result of fibrosis and strictures affecting intrahepatic and extrahepatic bile ducts.26 Recurrent biliary tract obstruction and recurrent episodes of cholangitis may accelerate progression of the disease. Thus, earlier detection of DS and treatment before infectious complications occurred might explain the improvement in transplantation-free survival in our study. With regard to this, we found a lower rate of recurrent episodes of cholangitis in patients adhering to our proposed protocol. Whereas all patients in the on-demand group received endoscopic treatment only in case of overt bacterial cholangitis, in the scheduled group less than 10% of patients experienced episodes of bacterial cholangitis between the scheduled endoscopic intervals. This could also explain the significantly lower frequency and later appearance of cirrhosis-related complications.
Although ERCP has been regarded as the standard of reference in diagnosing PSC, MRI is now recommended as a first-line non-invasive imaging method for patients with suspected PSC that offers comparable accuracy.27–30 In addition, MRI may be useful to confirm the symptom-driven indication for endoscopic intervention, to exclude focal parenchymal changes and to enable imaging-based guidance to minimise the risk of ERCP-related complications.17 On the contrary, for MRI, there is modest agreement regarding surveillance and detection of DS in PSC.31 This may be explained in part by the fact that the definition of DS derives from ERCP studies, which cannot be readily transferred to cholangiograms obtained using MRI. The most important conclusion of our trial is that only patients with DS had a benefit from scheduled ERCP, but the imaging method for effective DS diagnosis was not the subject of the study. Recent studies suggest an only moderate agreement between ERCP and MRI/MRCP in assessing presence and severity of biliary strictures.32 In view of this, it is most important that the MRI PSC Working Group of the International PSC study group propose definitions and minimum technical requirements for the detection of DS in MRI, emphasising the need to identify strictures that may require endoscopic intervention. The detection rate of DS in patients with on-demand endoscopy was significantly lower than that in patients with regularly scheduled endoscopy. Thus, in view of the fact that even frequent assessment of clinical status and laboratory parameters does not indicate the presence of DS, the development of reliable, non-invasive methods for detection of DS is all the more important. Especially in patients without the initial diagnosis of DS surveillance with MRCP probably in combination with other non-invasive markers might allow timely detection of new DS during the course of disease.
In the majority of published studies, balloon dilation was the preferred approach for treatment of DS, and stents were inserted only in a minority of patients.7 11 12 33 34 With the exception of a very small minority of patients in the beginning of our study, we also applied the dilation method exclusively, due to complications associated with stenting.14 This approach is supported by an European multicentre randomised trial comparing single-balloon dilation versus short-term stenting. The final analysis of this study showed no difference in outcome, but it did show a higher serious adverse event rate in the stent group.35
ERCP in patients with PSC carries an increased risk of complications, especially pancreatitis, cholangitis and extravasation of contrast due to dilation, but not all studies show an increased risk in PSC.36–40 The overall complication rate in our trial was within the lower range of that reported in our previous trials, and all adverse events could be managed by conservative treatment. Patients with PSC were only treated by experienced endoscopists and sphincterotomy was performed in all patients, which might have improved cannulation in follow-up ERCPs, consequently reducing the risk for peri-interventional complications. Thus, even our concept of a diagnostic ERCP at yearly intervals for the early detection of DS seems justified, at least until non-invasive MRI methods become more reliable.
Several limitations of our study must be taken into account. Our study was not randomised regarding endoscopic therapy, which is a limitation and might reduce the validity of the results. The lack of randomisation might have caused a selection bias towards more compliant patients in clinically stable condition choosing frequent surveillance at our department. However, as we excluded patients with advanced liver disease due to our exclusion criteria, we could not identify differences in laboratory values or clinical risk factors, such as age at first diagnosis, presence of IBD, presence of DS at first diagnosis, or MRS between groups at first presentation. Furthermore, frequency and location of DS at first presentation and histological stage was comparable between both groups. In patients with DS at first diagnosis, the beneficial effect of scheduled endoscopic interventions was similar to that in patients with development of DS during the course of disease.
As stated in the Methods section, the dosing of UDCA (administered to all patients) changed during the course of the study period. The favourable effect of adequate UDCA treatment has been reported in several other studies before and might also account for a substantial improvement in long-term survival in our cohort. Different dosing might had also an influence on variable disease progression. With respect to Hawthorne effect we found no differences in the adherence to drug intake, as all our patients received UDCA in both groups Furthermore, while UDCA dosing was changed over time, we found constant beneficial effect of endoscopic treatment during all study decades. Concerning maturation bias we compared the proportion of patients adhering to our protocol or not over the course of time. Indeed we found a significantly higher proportion of patients adhering to our protocol in the last decade of our study with beneficial effect of our endoscopic programme in both time frames.
In summary, in patients with PSC, timely detection and endoscopic therapy for DS up to morphological resolution, even in the absence of laboratory or clinical signs of obstructive cholestasis, seems to prevent chronic liver damage caused by biliary obstruction and infectious complications, leading to a significant improvement in actual survival.
References
Footnotes
Contributors CR, ASt and PS designed the study. Data collection was conducted by CR, TH, PK-P, ASc, RK, ASt, DNG and PS. Data analysis and interpretation was performed by CR, TB, ASt, DNG and PS. CR, TB, ASt and PS drafted the article. TH, PK-P, ASc, RK and DNG performed critical revision of the article. All authors approved the final version to be published.
Funding The study was supported by a grant from ’Deutsche Forschungsgemeinschaft (DFG)' to CR (RU 1936/1-2) and DNG (GO 1971/1-2).
Competing interests None declared.
Ethics approval Local ethics committee of Heidelberg University (S-043/2011).
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Obtained.