Article Text

Statistics from Altmetric.com
Message
We describe a novel, fast-track, innovative intestinal wound healing model developed in mice called the ‘colonoscopic leakage model’. This model uses a colonoscopic biopsy grasper to make a controlled transmural perforation in the colon. Similar to other classic anastomotic leakage models, we observed about 50% incidence of peritonitis, although this model is less invasive, faster and avoids intestinal occlusion as well as massive bodyweight loss. Therefore, this preclinical model could be used to test potential therapeutic agents and to investigate the different molecular wound healing mechanisms.
In more detail
Despite significant progress in the medical field, the mechanisms of healing of a wound in the GI tract are still not completely identified, which limits the options for positive interventions at the local level to support the healing processes.
Even though many influencing factors have been studied, it is very challenging to acquire knowledge of the local pathophysiology and to study the impact of different pharmacological and microbiological conditions at the molecular level. To overcome these difficulties, the use of experimental models that help in understanding the local conditions has become indispensable.
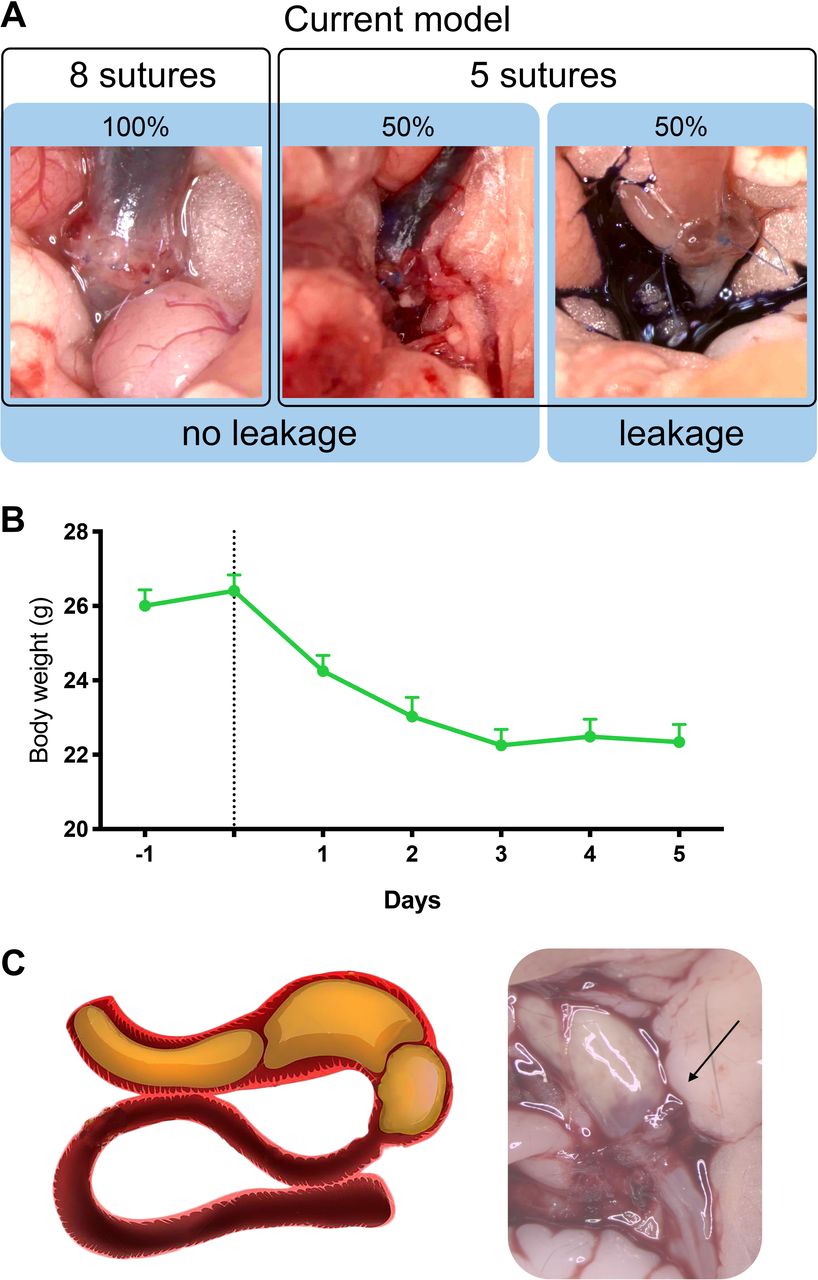
The models proposed in the literature to study the mechanisms of intestinal wound healing are mainly anastomotic leakage models. Among them, the one proposed by Pommergaard et al1 is the most commonly used technique (online supplementary video 1). This rodent model is based on the variation of the number of intestinal anastomotic sutures after segmental colonic resection (5 vs 8 stitches) in order to achieve a probability of 50% of anastomotic leakage (figure 1A and online supplementary videos 2–4) and peritonitis in the anastomotic leakage group.
Supplementary video
Supplementary video
Supplementary video
Supplementary video

Anastomotic leakage model. (A) The anastomotic leakage model is feasible with an anastomotic leakage and peritonitis of 40%–50%. The tightness and the absence of stenosis are verified postoperatively. (B) Bodyweight drop of over 15% with little to no recovery after 5 days. (C) Representative images of intestinal obstruction occurring in more than half of the operated mice.
This model, which we adapted to our laboratory settings in order to achieve the same outcome, is feasible and reproducible; however, during our research we identified a number of significant shortcomings that limit the use of this model for potential transversal clinical approaches. The most important limitations were that the surgery is extremely time-consuming, very invasive (ie, significant loss of weight and no recovery within 7 days), the intestinal transit is seriously affected and the occurrence of occlusions is very high (figure 1B and 1C). Altogether, these drawbacks make the model inadequate to perform local interventions and study changes at molecular level.
In order to address these weaknesses, we set up a new intestinal wound healing model, using colonoscopy and a grasper, which we called the ‘colonoscopic leakage model’ (figure 2). A detailed description is provided, including video documentation of the colonoscopy procedure (online supplementary videos 5 and 6 and online supplementary material and methods).
Supplementary video
Supplementary video
Supplemental material

{kind=link}
{kind=link}
Colonoscopic leakage model. (A) Representative perforation visualised by endoscopy. (B) Weight loss is very limited, and mice reach their preoperative body weight in less than 5 days. (C) The percentage of peritonitis is 40%–50% at 7 days postintervention. The subject’s mortality before the selected endpoint (ie, 7 days) is between 10% and 19%. (D) Histological visualisation of the wound healing area using a serial slicing method.
Similar to the anastomotic leakage rodent model described by Pommergaard et al,1 we are creating a controlled transmural perforation in a normal vascularised colon. However, in our method, instead of using a laparoscopic method, we used a colonoscopy system combining a high-resolution camera with a rigid examination sheath that enables local manipulation through an endoscopic sheath working channel. A transmural biopsy is performed during a colonoscopy with the aid of a grasper passed through the working channel of the colonoscopic system (online supplementary video 5). Working under direct visual control, we are able to precisely determine the site of the perforation of the colonic wall (figure 2A). Besides this visual confirmation (online supplementary video 6), successful perforation is also objectivated by the immediate occurrence of a pneumoperitoneum and instantaneous inflation of the whole abdominal cavity. The deflation of the peritoneal cavity is obtained by intraperitoneal introduction of a needle for a few seconds (online supplementary material and methods). Performing the whole procedure takes less than 10 min (ie, six times faster than the anastomosis model).
Additional advantages include a fast recovery of the mice, with mice displaying normal behaviour as soon as the anaesthetics wear off, and a low use of painkillers without the necessity of using opiates. Weight loss is also very limited, and mice reach their preoperative body weight in less than 5 days (figure 2B). Importantly, we did not observe any signs of intestinal occlusion, therefore ensuring a normal bowel movement after the procedure.
After 7 days of follow-up, our model resulted in 40%–50% incidence of peritonitis, which is perfectly in line with what was obtained using the anastomotic leakage model (figure 2C).
To characterise the levels of inflammatory response within our test subjects, we also developed a peritonitis severity score (figure 2C), ranging from 0 (no peritonitis) to 4 (peritonitis affecting the whole abdominal cavity and that led to death before the end of the 7-day period) (online supplementary material and methods).
Using this model, changes at a local level can be studied using complementary techniques: colonic sites of interest can be isolated and used to measure molecular biology markers (eg, via quantitative PCR or western blot), or the area of perforation can be prepared for histological analysis. Such microscopical evaluation grants a deep morphological characterisation when using different staining protocols (ie, H&E for general morphology, Alcian blue for mucus layer, immunohistochemistry). This approach also has the advantage of comparing different sections of the colon, and that combining several serial sections into a two-dimensional reconstruction can provide a broad overview of the healing process around and at the perforation site (figure 2D).
Comments and conclusions
Intestinal wound healing is influenced by a number of factors. While microbiota-independent environmental factors have already been well studied,2 more and more studies suggest that the local intestinal microenvironment, shaped by the resident microbiota, significantly influences the cicatrisation progress of an intestinal wound.3 Little research has been done so far in this respect, compared with the potential benefits that this could bring. Indeed, being able to study the local conditions of a wound during healing, including the evolutions in host–microbial relations, has the potential to help develop specific local interventions that have beneficial effect on recovery.
The current anastomotic leakage model described in literature, although feasible and reproducible, was not satisfying for our research purposes as it presented many unacceptable limitations. The newly developed colonoscopic leakage model is more suitable to study the different intestinal wound healing stages.
As a consequence, this model has a clear potential for clinical use. It might be used to study the local intestinal wound healing, for example after iatrogenic colonic perforation due to extended polypectomy (ie, endoscopic submucosal dissection), or the local cicatrisation mechanisms following a surgical colonic anastomosis. It may offer clinicians an easy model to study intestinal cicatrisation under a variety of different conditions, such as during treatment with different pharmacological compounds, during nutritional interventions, after modification of the microbiota (eg, faecal material transplantation), but also in numerous pathologies that impact the local microenvironment, such as autoimmune diseases.
Acknowledgments
We are very grateful to Anthony Puel for excellent technical help.
Footnotes
Twitter @MicrObesity
RB and MVH contributed equally.
Contributors RB, MHV and PDC: study concept and design of the study. RB and MVH performed the experiments. PDC supervised the experiments. RB, MVH and PDC analysed the experiments. RB, MHV and PDC wrote the manuscript. PDC provided funding. All authors provided intellectual input. All authors critically revised and approved the manuscript.
Funding This work was supported by the FRFS-WELBIO under grant WELBIO-CR-2017C-02 and WELBIO-CR-2019C-02R. PDC is a recipient of the Funds Baillet Latour (Grant for Medical Research 2015).
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; internally peer reviewed.