Article Text

Statistics from Altmetric.com
Clinical presentation
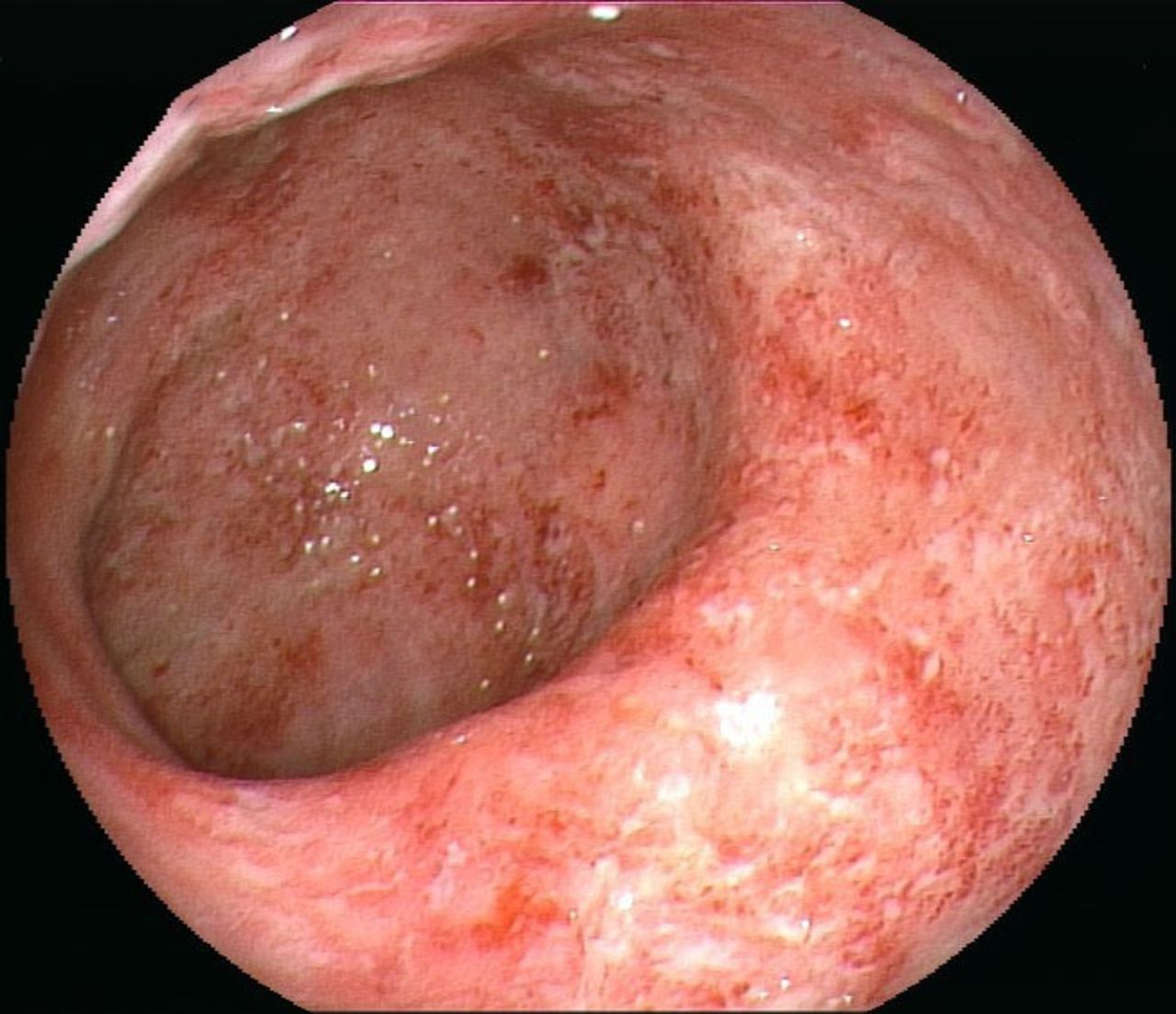
A 41-year-old female patient was admitted to hospital with bloody stool and diarrhoea for 2 months, accompanied with fever, left earache, obvious saddle-nose deformity and red eyes for 2 weeks. She had history of repeated multiple sore joints for 6 months and hearing impairment in the left ear for 4 months. Laboratory tests showed elevated white cell count (WBC) of 15.57×10ˆ9/L, neutrophil of 76.8% and C reactive protein (CRP) of 95.4 mg/L. Haemoglobin was decreased at 94 g/L. Antineutrophil cytoplasmic antibody was negative. Colonoscopy showed diffuse inflammation and ulcers in the left-sided colon (figure 1). Histological findings from sigmoid colon showed chronic inflammation without vasculitis appearance. CT enterography revealed left-sided colon inflammation (figure 2). MRI of the internal auditory canal showed left middle ear mastoiditis (figure 3). Physical examination found swollen left auricle and obvious saddle-nose deformity (figure 4). Treatment of mesalamine, antibacteria and eye drops was started with subsequent symptomatic improvement (bloody stool improved, fever and swollen auricle disappeared), paralleled by a reduction in WBC to -5.0×10ˆ9/L (normal differential) and CRP to 20 mg/L. But earache, red eyes, saddle-nose deformity and sore joints still persisted. And she gradually appeared complete hearing loss in her left ear.

Diffuse inflammation and ulcers in the sigmoid colon.

CT view of thick-walled left-sided colon with rich blood vessels and lymphadenopathy.

MRI of left middle ear mastoiditis.

Saddle-nose deformity.
Question
What is the diagnosis?
Answer
The colon lesions were diagnosed as ulcerative colitis (UC). After comprehensive assessment, the symptoms of earache, saddle-nose deformity, red eyes, sore joints and hearing loss were diagnosed as relapsing polychondritis (RP). After 1 week of oral prednisone (30 mg/day) treatment, earache and red eyes disappeared, sore joints improved, but saddle-nose deformity and hearing loss had no improvement, and floppy eared gradually appeared. The dose of prednisone was gradually reduced when she was discharged from hospital and treatment of oral mesalazine was sustained. Three months later, colonoscopy showed endoscopic remission of UC (figure 5). She had no earache and sore joints, but saddle-nose deformity, cauliflower-like left ear (figure 6) and hearing loss persisted.

Endoscopic remission in the sigmoid colon.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cauliflower-like left ear.
RP is a rare autoimmune rheumatic disorder characterised by episodic inflammation of cartilaginous tissue throughout the body.1 Typical presenting features include chondritis of the nasal bridge, auricular cartilage, ocular inflammation and involvement of the tracheobronchial tree.2 To date, diagnosis of RP is mainly based on typical clinical findings. UC with RP is rarely reported.3 Treatment for PR is usually with steroids and immunosuppressive drugs, but there are no standardised treatment options. The patient in our study is a rare example of UC with RP who responds to oral steroid.
Ethics statements
Patient consent for publication
Footnotes
Contributors MC performed the endoscopy, prepared the endoscopic figures and wrote the manuscript. ZL collected medical history, prepared the CT and MRI figures. XL revised the manuscript carefully. All authors contributed to the care of the patient.
Funding The case was funded by National Natural Science Foundation of China, Grant Number: 81600443, 81873554.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.