Article Text

Abstract
Objective We aimed to determine the predictive capacity and diagnostic yield of a 10-fold increase in serum IgA antitissue transglutaminase (tTG) antibody levels for detecting small intestinal injury diagnostic of coeliac disease (CD) in adult patients.
Design The study comprised three adult cohorts. Cohort 1: 740 patients assessed in the specialist CD clinic at a UK centre; cohort 2: 532 patients with low suspicion for CD referred for upper GI endoscopy at a UK centre; cohort 3: 145 patients with raised tTG titres from multiple international sites. Marsh 3 histology was used as a reference standard against which we determined the performance characteristics of an IgA tTG titre of ≥10×ULN for a diagnosis of CD.
Results Cohort 1: the sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) for IgA tTG levels of ≥10×ULN at identifying individuals with Marsh 3 lesions were 54.0%, 90.0%, 98.7% and 12.5%, respectively. Cohort 2: the sensitivity, specificity, PPV and NPV for IgA tTG levels of ≥10×ULN at identifying individuals with Marsh 3 lesions were 50.0%, 100.0%, 100.0% and 98.3%, respectively. Cohort 3: the sensitivity, specificity, PPV and NPV for IgA tTG levels of ≥10×ULN at identifying individuals with Marsh 3 lesions were 30.0%, 83.0%, 95.2% and 9.5%, respectively.
Conclusion Our results show that IgA tTG titres of ≥10×ULN have a strong predictive value at identifying adults with intestinal changes diagnostic of CD. This study supports the use of a no-biopsy approach for the diagnosis of adult CD.
- coeliac disease
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
Paediatric European Society for the Study of Paediatric Gastroenterology, Hepatology and Nutrition guidelines suggest that a diagnosis of coeliac disease (CD) can be made without taking duodenal biopsies.
The latest criteria suggest that a 10-fold increase in IgA antitissue transglutaminase (tTG) antibody levels in combination with EMA positivity is sufficient to make a diagnosis of CD in the absence of duodenal biopsies.
In adults, this approach has not yet been widely adopted into clinical practice, largely due to a lack of international multicentre data and testing in low CD prevalence cohorts.
What are the new findings?
Across three cohorts of adult patients, we have shown that almost all individuals with IgA tTG titres of ≥10×ULN have small intestinal mucosal changes diagnostic of CD (Marsh 3 lesions) on duodenal biopsy.
We show that IgA tTG titres of 10×ULN have 100% specificity at detecting Marsh 3 lesions in a cohort of 532 adults with a CD prevalence of 3.2%.
Finally, we found that an IgA tTG cut-off of 10×ULN performed well at identifying individuals with Marsh 3 lesions using different assays across multiple international sites. However, determining assay-specific thresholds and/or standardisation of tTG assays used with this pathway may help to optimise the accuracy and impact of this approach.
How might it impact on clinical practice in the foreseeable future?
This study supports a change in guidelines towards a no-biopsy approach for the diagnosis of CD within adult gastroenterology services.
Introduction
Coeliac disease (CD) is a common immune-mediated enteropathy, whereby increased immunological sensitivity to dietary gluten results in chronic small intestinal mucosal inflammation in genetically susceptible individuals.1 CD affects ~1% of the global population, but despite its rising prevalence, the majority of patients remain undiagnosed.2 Currently, most patients with suspected CD are screened serologically for antibody positivity, in particular for IgA antibodies to tissue transglutaminase 2 (tTG) and antiendomysial IgA antibodies (EMAs).1 As these serological markers are not 100% specific for detecting intestinal lesions compatible with CD, positive coeliac serology is confirmed by duodenal biopsies demonstrating the hallmark pathological changes of mucosal remodelling, such as villous atrophy, crypt hyperplasia and intraepithelial lymphocytosis.3
However, upper GI endoscopy with biopsies is expensive, with costs relating directly to the procedure and indirectly to the processing and analysing of samples. The procedure is poorly tolerated by many patients4 and carries risks, including sedation complications and although rare in current practice, GI haemorrhage and/or perforation.5 Furthermore, variability exists in the identification of the main histological changes of CD, meaning cases can be missed despite duodenal biopsy sampling.6 7 Therefore, the identification of a non-invasive approach to the diagnosis of CD is of great interest.
The 2012 European Society for the Study of Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) guidelines for the diagnosis of CD challenged the necessity for duodenal biopsies in paediatric patients. They suggested that an IgA tTG antibody titre greater than 10 times the upper limit of normal (ULN), in combination with a positive EMA antibody test and compatible human leucocyte antigen (HLA) genotype, is sufficient to support a diagnosis of CD in symptomatic individuals.8 This eliminates the need for gastroscopy and its associated costs/risks in selected paediatric patients.8 The latest guidelines published this year remove the requirement for the presence of symptoms and HLA testing in the diagnostic pathway.9 This underscores the specificity of a serology-based or ‘no-biopsy’ approach for the diagnosis of paediatric CD.
Studies have evaluated whether this strategy can be applied in symptomatic adult CD.10–21 These studies have suggested that tTG levels of ≥10×ULN could be predictive of CD in adults, and the recently published Finnish national guidelines for the diagnosis of CD have incorporated this diagnostic pathway into their practice.22 However, this approach has not been widely adopted into adult clinical practice or guidelines. Adult gastroenterologists have cited the lack of international, multicentre data including testing in low CD prevalence populations and thus intimated caution.23 Furthermore, there are inconsistencies in the histological diagnosis of CD in the published literature.23 Therefore, the aim of the current study was to assess whether a tTG level of ≥10×ULN could be sufficient for detecting duodenal mucosal abnormalities diagnostic of CD and to determine the diagnostic yield of this approach across different adult cohorts. In doing so, we aimed to address the shortcomings within the adult literature.
Methods
Patients
The study comprised three adult (≥16 years old) cohorts; all individuals included in the study underwent clinical assessment and had IgA tTG serology testing alongside upper GI endoscopy with duodenal biopsies performed.
Cohort 1 comprised a prospective analysis of consecutive adult patients assessed in the specialist CD clinic Royal Hallamshire Hospital, UK, from 2008 to 2019 who had a serum IgA tTG test and duodenal biopsy within 6 weeks of each other, no previous diagnosis of CD, naivety to a gluten-free diet (GFD) and IgA competency. As these individuals were assessed within the specialist coeliac clinic, they were considered as having high clinical suspicion for CD.
Cohort 2 comprised a retrospective analysis of a prospectively recruited (December 2014–January 2017)24 cohort of adults referred for upper GI endoscopy at the Royal Hallamshire Hospital, UK. Patients were recruited prospectively from an endoscopy list that is for the investigation of GI complaints, as well as general and open-access referrals. Those with IgA deficiency, with a previous diagnosis of CD and on gluten restriction prior to diagnosis were excluded from analysis. To reduce the referral bias for CD, patients referred with positive coeliac serology (EMA positivity) in primary care were also excluded from the analysis. As a result, we considered this cohort as having low suspicion for CD.
Cohort 3 comprised a retrospective analysis of adult patients with raised tTG titres from multiple sites, involving 8 countries and comprising 11 laboratories. Cases were identified based on positive coeliac serology and having had appropriate duodenal biopsy sampling. The eight countries included Argentina (n=11), Iran (n=10), Netherlands (n=10), Italy (n=44), Romania (n=10), Turkey (n=10), the USA (n=40) and the UK (n=10). In total, this provided assessments on 145 patients.
Serology and biopsy
All patients from cohorts 1 and 2 underwent serological testing and duodenal biopsy within 6 weeks of each other at the Royal Hallamshire Hospital in the context of a routine clinical service, with the exception that histopathologists were blinded to the serological status of patients from cohort 2. IgA tTG antibody levels were measured by ELISA using the Aeskulisa Diagnostics (Wendelsheim, Germany) kit before December 2014 and the ELiA Celikey (Thermo Fisher, Freiburg, Germany) after December 2014. Results were reported in unit per millilitre using the manufacturer’s supplied reference ranges: 0–15 negative, >15 positive, 0–7 negative and >7 positive, respectively. The highest standard in the assay is 300 and 128 U/mL, respectively, and these were used as upper limits for analysis, irrespective of whether optical density values exceeded this. IgA EMA was detected by immunofluorescence on primate oesophagus sections (Binding Site, Birmingham, UK).
During gastroscopy, at least four quadrantic biopsies were taken from the second part of the duodenum (D2) and one from the duodenal bulb using the single bite technique (21% of patients from cohort 1 had >1 D2 biopsy only). The histopathology department at this site had significant experience in CD diagnosis. Duodenal mucosal changes were assessed using the Marsh criteria; Marsh 3 lesions were classified based on evidence of increased intraepithelial lymphocytes, crypt hyperplasia and villous atrophy.3 25 The most severe histological grade detected on biopsy was recorded and used for analysis. Unless otherwise stated, a diagnosis of typical CD was based on positive coeliac serology and Marsh 3 histology on duodenal biopsy. Seronegative CD was diagnosed in individuals with Marsh 3 lesions and supporting CD risk factors and/or response to a GFD; non-coeliac causes of villous atrophy were ruled out in these individuals.
Individuals from cohort 3 had IgA tTG titres measured by ELISA assays in routine clinical use at each site, including ARUP Laboratories (Utah, USA), QuantaLite (Inova Diagnostics, San Diego, California), Eu-tTG (Eurospital, Italy), Euroimmune (Luebeck, Germany) and ELiA Celikey (Thermo Fisher, Freiburg, Germany). Each individual had four to six duodenal biopsies sampled during upper GI endoscopy. A diagnosis of CD was made locally by expert gastroenterologists taking into consideration serology and duodenal biopsy results.
Ethical consideration
All identifiable medical information was removed, and all analyses were performed using anonymised data. See below for full details.
Statistical analysis
Data handling was conducted using spreadsheets in Microsoft Excel (2016); statistical analysis and graph construction were performed using GraphPad Prism V.7 (GraphPad Software, San Diego, California, USA). To enable comparison of tTG levels between different assays, tTG levels were normalised by expression as a multiple of the ULN—defined as the lowest value that was considered abnormal for each assay.19 Where indicated, receiver operating characteristic (ROC) curves were constructed, and area under the curve (AUC) was calculated to determine the accuracy of tTG levels at predicting villous atrophy. Analysis of variance or Kruskal-Wallis test, with appropriate post hoc analysis, was used to compare Marsh grades with tTG titres. A p value of <0.05 was considered statistically significant.
Results
Cohort 1: patients assessed in the specialist CD clinic
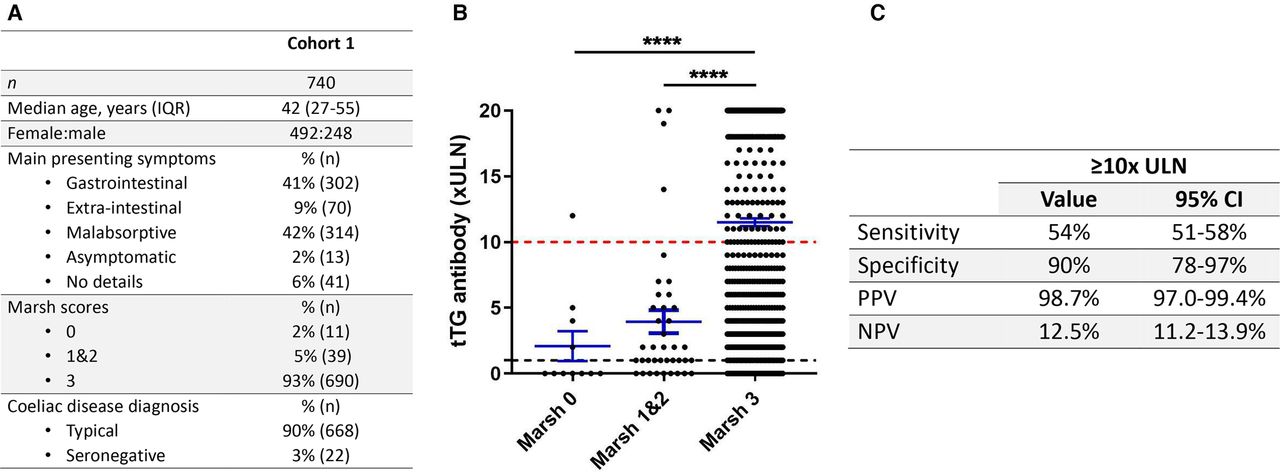
A total of 740 patients fulfilled the criteria and were included in cohort 1. The prevalence of CD in this cohort was 93% (690/740 patients). Patient demographics and clinical details are listed in figure 1A. Altogether, 380/740 (51%) had tTG titres of ≥10×ULN. Marsh 3 lesions were detected in 375/380 (98.7%) of those with tTG titres of ≥10×ULN (figure 1B). Of the 740 patients, 360 (49%) had tTG titres of <10×ULN; of those, 315/360 (87.5%) had Marsh 3 lesions, 35/360 (9.7%) had Marsh 1–2 lesions and 10/360 (2.8%) had Marsh 0 lesions on duodenal biopsy. Based on this, the positive predictive value (PPV) of tTG values of ≥10×ULN at predicting mucosal abnormalities with villous atrophy was 98.7% (97.0%–99.4%) (figure 1C). Five patients had tTG titres of ≥10×ULN without detectable villous abnormalities (ie, Marsh<3 lesions); the demographic and clinical characteristics of these patients are shown in table 1. All five patients had symptoms of malabsorption and/or were EMA positive and all were positive for the HLA DQ2/8 genotype. All patients were started on a GFD and subsequently, tTG titres decreased.
Demographic and clinical details of patients with tTG titres≥10×ULN where villous abnormalities were not detected on duodenal biopsies

(A) Demographic and clinical details of the patients in cohort 1. GI symptoms include abdominal pain, dyspepsia, dysphagia, nausea, vomiting, bloating and constipation; extraintestinal symptoms include ataxia, headache, dizziness, fatigue, joint pain and skin rash; malabsorptive symptoms include diarrhoea, haematinic deficiencies with/without anaemia and weight loss. (B) Normalised tTG titres against Marsh grade in patients from cohort 1. Horizontal bar represents the mean; error bars denote SE of the mean. Black dotted line represents 1×ULN threshold; red dotted line represents 10×ULN threshold. Comparisons between groups made with Kruskal-Wallis and post hoc Dunn test. (C) Performance characteristics of tTG titres of 10×ULN at predicting villous atrophy. ****P<0.0001. tTG, tissue transglutaminase; ULN, upper limit of normal; PPV, positive predictive value; NPV, negative predictive value.
Two different tTG assays were used to test tTG titres in cohort 1 over the study period; we next evaluated the differences between these two assays. To do this, we divided the cohort into two, based on the tTG assay used (cohort 1A, Aeskulisa Diagnostics; cohort 1B, ELiA Celikey). The demographics of individuals included in cohort 1A and 1B are detailed in figure 2A. Analysis of tTG titres showed that there were differences in the predictive power of the two tests, such that applying a 10×ULN cut-off had a PPV of 98.1% (95.7%–99.1%) for Marsh 3 lesions in cohort 1A, but a PPV of 100% in cohort 1B (figure 2B–D). Notably, the very high tTG titres in patients with Marsh<3 lesions were recorded using the Aeskulisa assay (figure 2B).

(A) Demographic and clinical details of the patients in cohorts 1A and 1B. (B) tTG titres against Marsh grade in patients from cohort 1A. (C) tTG titres against Marsh grade in patients from cohort 1B. Horizontal bar represents the mean; error bars denote SE of the mean. Black dotted line represents 1×ULN threshold; red dotted line represents 10×ULN threshold. Comparisons between groups were made with analysis of variance and post hoc Tukey test. (D) Performance characteristics of tTG titres of 10×ULN at predicting villous atrophy. **P<0.01, ****P<0.0001. tTG, tissue transglutaminase; ULN, upper limit of normal; PPV, positive predictive value; NPV, negative predictive value.
Cohort 2: patients referred for upper GI endoscopy
A total of 778 patients were included in cohort 2. Ten patients had IgA deficiency; 91 patients were already consuming a GFD and/or had a diagnosis of CD; 1 patient had clinical features in keeping with a relapse of known small bowel Crohn’s disease; and 23 individuals had incomplete testing or missing information, and so these individuals were excluded from further analysis. Of the remaining cohort, 121 patients had positive EMA testing in primary care, and so these were excluded from further analysis.
Therefore, 532 patients were included in the analysis stage. The prevalence of CD in this cohort was 3.2% (17/532 patients). Patient demographics and clinical details are presented in figure 3A. 18/532 patients had Marsh 3 lesions identified on duodenal histology, 15 patients (2.8% of the cohort) were diagnosed with typical CD; 2 patients (0.4% of the cohort) had seronegative CD; and 1 patient (0.2% of the cohort) was diagnosed with non-coeliac seronegative villous atrophy.
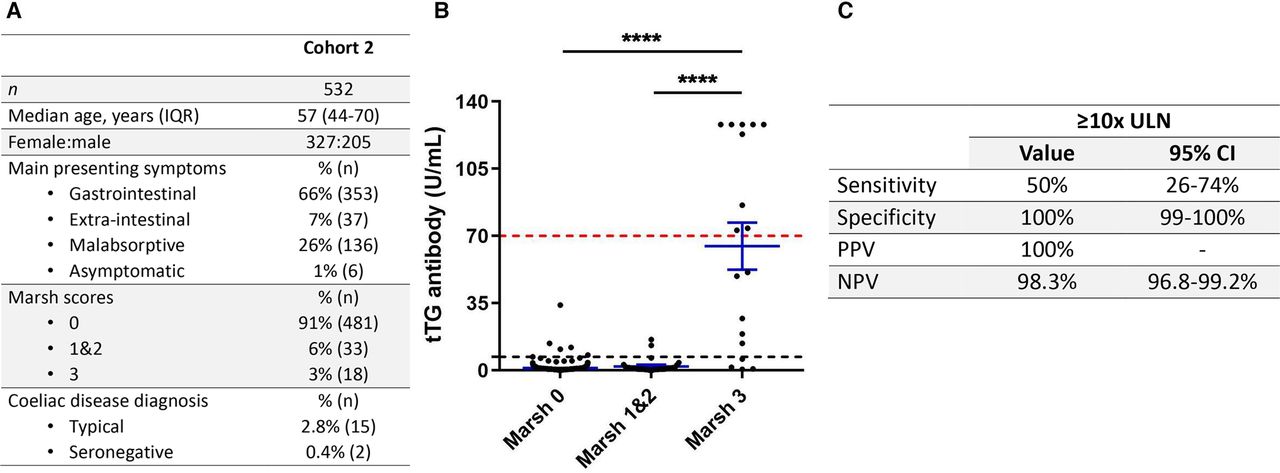
(A) Demographic and clinical details of the patients in cohort 2. GI symptoms include abdominal pain, dyspepsia, dysphagia, nausea, vomiting, bloating and constipation; extraintestinal symptoms include ataxia, headache, dizziness, fatigue, joint pain and skin rash; malabsorptive symptoms include diarrhoea, haematinic deficiencies with/without anaemia and weight loss. (B) tTG titres against Marsh grade in patients from cohort 2. Horizontal bar represents the mean; error bars denote SE of the mean. Black dotted line represents 1×ULN threshold; red dotted line represents 10×ULN threshold. Comparisons between groups were made with analysis of variance and post hoc Tukey test. (C) Performance characteristics of tTG titres of 10×ULN at predicting villous atrophy. ****P<0.0001. tTG, tissue transglutaminase; ULN, upper limit of normal; PPV, positive predictive value; NPV, negative predictive value.
The ELiA Celikey was used to measure tTG levels in all patients in cohort 2. Altogether, 9/532 (1.7%) had tTG titres of ≥10×ULN. Marsh 3 lesions were detected in 9/9 (100%) of those with tTG titres of ≥10×ULN (figure 3B). All individuals (9/9) with tTG titres of ≥10×ULN were EMA positive. Of the 532 patients included, 523 (98.3%) had tTG titres of <10×ULN; of those, 9/523 (1.7%) had Marsh 3 lesions; 33/523 (6.3%) had Marsh 1–2 lesions; and 481/523 (92.0%) had Marsh 0 lesions on duodenal histology. Thus, the PPV of tTG values of ≥10×ULN at predicting individuals with Marsh 3 lesions was 100% (figure 3C).
ROC analysis showed an AUC of 0.9179 for tTG values at predicting Marsh 3 histology (figure 4A). Based on this analysis, the optimal threshold of tTG titres was 5.9×ULN (tTG titres of >41.5 U/mL) (figure 4B). Reducing the threshold to this level increased the sensitivity of this approach from 50% to 61%. These results demonstrate that tTG titres of 10×ULN have excellent specificity at detecting Marsh 3 lesions in a cohort of predominantly symptomatic adult patients with a low suspicion/prevalence of CD. Reducing the tTG threshold increased the number of individuals who would have benefited from this strategy, without compromising the predictive value of this approach.

(A) Receiver operating characteristic curve analysis of tTG values against Marsh 3 histology in cohort 2. (B) Performance characteristics of tTG titres×5.9 ULN at predicting Marsh 3 lesions. tTG, tissue transglutaminase; ULN, upper limit of normal; PPV, positive predictive value; NPV, negative predictive value.
Cohort 3: international multicentre cohort
A total of 145 patients were included in cohort 3. The prevalence of CD in this cohort was 92% (133/145 patients). Demographic and clinical characteristics are included in figure 5A. Of the 145 patients included, 42 (29.0%) had tTG titres of ≥10×ULN, of which 40/42 (95.2%) patients had Marsh 3 lesions on duodenal biopsy (figure 5B). One hundred three of the 145 patients (71.0%) had tTG titres of <10×ULN; of those, 93/103 (90.3%) patients had Marsh 3 lesions; 6/103 (5.8%) patients had Marsh 1–2 lesions; and 4/103 (3.9%) had Marsh 0 lesions on duodenal biopsy. Based on this, the predictive value of using a 10×ULN threshold at detecting individuals with Marsh 3 lesions was 95.2% (84.6%–98.7%) (figure 5C). Two patients that had tTG titres of ≥10×ULN without villous abnormalities both had Marsh 2 lesions on duodenal biopsy and were diagnosed with CD. Interestingly, tTG titres did not reach the 10×ULN threshold across three sites, despite 56 individuals having Marsh 3 lesions across these sites. Therefore, a uniform tTG threshold of 10×ULN may exclude many true positive cases.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Demographic and clinical details of the patients in cohort 3. GI symptoms include abdominal pain, dyspepsia, dysphagia, nausea, vomiting, bloating and constipation; extraintestinal symptoms include ataxia, headache, dizziness, fatigue, joint pain and skin rash; malabsorptive symptoms include diarrhoea, haematinic deficiencies with/without anaemia and weight loss. (B) Normalised tTG titres against Marsh grade in patients from cohort 3. Horizontal bar represents the mean; error bars denote SE of the mean. Black dotted line represents 1×ULN threshold; red dotted line represents 10×ULN threshold. Comparisons between groups made with Kruskal-Wallis and post hoc Dunn test. (C) Performance characteristics of tTG titres of 10×ULN at predicting villous atrophy. **P<0.01. tTG, tissue transglutaminase; ULN, upper limit of normal; PPV, positive predictive value; NPV, negative predictive value.
Discussion
Altogether this study included 1417 patients; 431/1417 (30%) patients had tTG titres of ≥10×ULN, of which 424 (98%) patients had Marsh 3 lesions on duodenal biopsy and were diagnosed with CD. This study addresses the concerns raised by the adult gastroenterology community and supports a change in guidelines towards a no-biopsy approach for the diagnosis of CD in adults.
We identified Marsh 3 histology as our primary reference standard across all cohorts because (1) small intestinal mucosal remodelling, in keeping with Marsh 3 histology, represents the hallmark pathological changes in CD26; (2) few studies in the adult literature have reported on the predictive capacity of tTG titres of ≥10×ULN against Marsh 3 histology; rather, a clinical diagnosis of CD (based on the constellation of appropriate symptoms, serology and associated risk factors, in the absence of villous abnormalities) has been used as a reference standard by many27; and (3) few studies have included appropriate details regarding the location (including the duodenal bulb) and interpretation of biopsies.28 By contrast, our centre in Sheffield, UK, has published extensively on the matter of duodenal biopsy sampling in adult CD.29–32
In taking this approach, initially, we evaluated the predictive value of tTG titres of ≥10×ULN against the presence of Marsh 3 histology in patients seen in the specialist CD clinic (cohort 1). Most individuals within this cohort were diagnosed with CD, which reflects a high referral bias and pretest probability for CD in this cohort. This aligns with many previous studies, which have also assessed the diagnostic accuracy of tTG titre multiples of the ULN in high pretest probability/disease prevalence populations (CD prevalence >70%).10 12–14 16 18 In accordance with these previous studies, we found that a tTG titre threshold of 10×ULN accurately identified individuals with Marsh 3 lesions.
However, the pretest probability/disease prevalence within a cohort can influence the PPV of a diagnostic test.33 This means that as the disease prevalence increases, the more likely it is that a positive test represents a true positive case.33 The predictive value of the 10×ULN threshold in adults has less commonly been evaluated in more general clinical scenarios where the disease prevalence of CD is considered <10%.11 28 33 Sugai et al previously demonstrated that a tTG titre threshold of around 7×ULN had a 100% PPV for CD in an adult cohort with a CD prevalence of 3.3%.11 More recently, Fuchs et al demonstrated that a tTG titre threshold of 10×ULN was accurate at identifying individuals with Marsh 3 lesions across adult cohorts with different pretest probabilities for CD.28 However, in this study, the low CD pretest probability cohort included only older (>50 years) adults.28 Furthermore, the performance characteristics of the 10×ULN tTG threshold in a more general clinical scenario have been estimated, but not studied.33
Therefore, to confirm and extend these findings, we next sought to determine the predictive capacity of the 10×ULN threshold against the presence of Marsh 3 lesions on duodenal biopsy in a cohort of individuals considered as low suspicion for CD (cohort 2). Low suspicion was determined on the basis that, in those referred for upper GI endoscopy, the referral bias for CD was removed by excluding those who tested positive for CD in primary care. Indeed, the prevalence of CD in this population was 3.2%, which aligns with the local prevalence of CD in symptomatic adults in primary care (3.6%).34 These results demonstrate that tTG titres of ≥10×ULN are equally good at predicting Marsh 3 lesions in the setting of both low and high disease pretest probability/prevalence and complement previous work that this diagnostic pathway can be used in adults with different risk levels for CD.11 28 Importantly, while these data support the use of the biopsy avoidance approach in adults, we still advocate that suspected cases with tTG titres exceeding the 10× threshold are referred to a gastroenterologist for assessment, rather than the diagnosis of CD being made in primary care. In addition, these data were generated in adult cohorts within secondary and tertiary care settings, and thus, these results do not apply to screening the general population for a diagnosis of CD. These are important considerations to ensure that patients receive the correct diagnosis and to prevent the inappropriate institution of a GFD, which has been raised as concerns regarding this approach by some.23 35
One of the major challenges in implementing this diagnostic pathway is the variability and lack of standardisation between tTG assays.36 The inability to compare tTG results accurately between different assays increases the chances of misdiagnosis if a uniform threshold is used. In adults, there is a lack of data evaluating this in a multicentre international setting. To address this, we evaluated the 10×ULN threshold across multiple sites/countries and multiple assays (cohort 3). The PPV of the 10×ULN threshold at detecting Marsh 3 lesions dropped from nearly 99% across cohorts 1 and 2 at our UK centre to 95.2% in a multicentre international setting. This raises the concern that sole reliance on this as a marker for CD will lead to a false-positive diagnosis in around 1 in 20 cases.
Across all cohorts, the diagnostic performance of this pathway is based strictly on the presence of Marsh 3 histology. The PPV in all three cohorts increased to >99%, where both Marsh 2 and Marsh 3 lesions are accepted as CD. It is widely accepted that in the setting of relevant symptoms/high baseline risk of CD, raised serological markers, HLA DQ2/8 positivity and/or response to a GFD, the diagnosis of CD can be established in the absence of villous effacement. Indeed, this situation may represent a false-negative histology rather than a false-positive serology28 due to a variety of reasons, including incorrect histological interpretation, which can vary in 10%–25% of cases between independent evaluations6 7 and/or patchy disease.32 Additionally, individuals with symptomatic CD may present with subtle villous abnormalities that fall within the scope of microscopic enteritis, which may lead to diagnostic inaccuracy.37
In comparison with the datasets that have evaluated the tTG IgA cut-off at ≥10×ULN included in the latest paediatric ESPGHAN guidelines, 2/30 reported a PPV of <95%; 7/30 had a PPV between 95% and 99%; and 21/30 reported a PPV of >99% for detecting Marsh 3 lesions.9 In studies where Marsh 2 or Marsh 3 duodenal lesions were accepted for a diagnosis of CD, the PPV was >97% in all studies.9 Thus, based on the current study, the performance characteristics of this diagnostic pathway in adults with different risk levels for CD or in a multicentre international setting is at least comparable with the studies included within the paediatric guidelines.
The high tTG threshold recommended by the paediatric community in part is included to control for tTG assay variation.36 We found that for some tTG assays, a lower cut-off may retain diagnostic specificity but increase the sensitivity of this approach. In contrast, the 10×ULN threshold may not eliminate all false-positive cases across all assays. Therefore, a uniform threshold may hinder the clinical impact and accuracy of the no-biopsy approach in adult patients. Other studies have reported similar findings of differences in the optimal tTG thresholds and performance characteristics of different assays.14 19 28 This does not imply that one assay is inferior to the other nor that using tTG threshold values in this manner is not appropriate, rather that the threshold ULN cut-off should be specific to the tTG assay, as there is currently no way to accurately standardise tTG results across different assays.38 Therefore, local validation of assay specific thresholds and/or limiting the use of this pathway to certain tTG assays may help to optimise the clinical impact and accuracy of this approach.
The latest ESPGHAN guidelines no longer consider either the presence of symptoms or HLA typing as mandatory in this diagnostic pathway.9 HLA typing has been shown to add no diagnostic value in this pathway in children or adults, and testing is costly and not widely available.9 28 Therefore, the HLA status of individuals was not specifically evaluated in this study. In addition, while each cohort comprised predominantly symptomatic adults, we did not specifically evaluate symptomatology in this study. Current ESPGHAN guidelines recommend confirming tTG titres with EMA positivity in a second blood sample.9 EMA status was not evaluated in all patients in the present study. While EMA positivity has been shown to enhance the predictive capacity of the biopsy avoidance approach, EMA testing incurs a high cost and is labour intensive, and the interpretation is subjective.35 For these reasons, some centres have stopped performing EMA tests.17 Therefore, including EMA testing in this algorithm may lead to poor uptake of this pathway in some areas. Alternative strategies have been suggested, including simultaneous tTG measurements28 or testing for deamidated gliadin peptides (DGPs) alongside tTG titres, the latter of which has shown promise in both adult and paediatric cohorts.11 39 Further adult studies are awaited to address the place for DGPs in this algorithm.
Finally, it is noteworthy that the applicability of the biopsy avoidance approach is not as straightforward in adults as it is in children. Indeed, it should be stressed there are a number of reasons that a biopsy should still be performed in adults, particularly if there are ‘red flag’ signs/symptoms, such as, but not limited to, persistent dyspepsia in those aged ≥55 years, weight loss, severe malnutrition, dysphagia and unexplained iron deficiency anaemia.40–42 Some of these presentations align with those of adult CD; this underscores the importance of assessment by a gastroenterologist before a diagnosis of CD is made in the absence of a duodenal biopsy. In addition, a biopsy should also be considered in cases of discordance between serology and risk, and in borderline cases.27 Moreover, individuals with persistent symptoms despite adherence to a GFD require duodenal biopsy sampling, as tTG titres provide no information regarding histological improvement after introduction of a GFD.43
In conclusion, our data show that anti-tTG titres of ≥10×ULN perform well at identifying adults with intestinal changes associated with CD. This study supports a no-biopsy strategy in adult gastroenterology services. This approach has implications in reducing the cost, risk and caseload associated with diagnostic endoscopy in adult CD. However, local validation of assay-specific thresholds would enable this approach to have the greatest impact on adult patients.
Data availability statement
No data are available.
Ethics statements
Ethics approval
The Sheffield arm of the study (cohorts 1 and 2) was approved by the Yorkshire and the Humber Sheffield Research Ethics Committee, under registration numbers 14/YH/1216 and STH15416, respectively. Data relating to the multicentre cohort were previously approved by the research and development/audit departments of countries involved and were fully approved by the ethical committee of the Research Institute for Gastroenterology and Liver Disease, Shahid Beheshti University of Medical Science Tehran (protocol IR.SBMU.RIGLD.REC.1395.87) or the Columbia University Irving Medical Center Institutional Review Board (protocol IRB-AAAB0960).
References
Footnotes
Contributors HAP analysed the data and wrote the original manuscript. KR and DSS conceived the study, collected the data and edited the manuscript. SAR, ML, LJSM and EMRB recruited patients and helped collect and collate the data. JB, GB, HJB, AC, MD, MHD, AE, AG, PHRG, MWJ, SI, BL, AL, RM, HMS, MR-N, DR, IS, AS, UV, VV, GW and SC helped collect/generate the data. All authors approved the final version of the manuscript.
Funding BL is supported by The Louis and Gloria Flanzer Philanthropic Trust.
Competing interests DSS receives an educational grant from Dr Schär (a gluten‐free food manufacturer). PHRG serves on the advisory board of ImmusanT, Cellimmune and ImmunogenX, and is an unpaid member of Nima’s Scientific Advisory Board. The remaining authors disclose no conflicts.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.