Article Text

Statistics from Altmetric.com
Introduction
A 62-year-old man was incidentally found to have a massive splenomegaly during his admission for a right-sided pneumonia. A contrast-enhanced CT of the neck, thorax, abdomen and pelvis revealed a massive splenomegaly that measured 26 cm in the craniocaudal span, with no hepatomegaly, lymphadenopathy or suspicious mass. Thalassaemia screen was negative and peripheral blood film did not show any abnormal cells or spherocytes. A bone marrow examination was normal as well. Liver cirrhosis, though less likely the cause of massive splenomegaly, was excluded by a normal transient elastography.
Full blood count showed microcytic hypochromic anaemia with haemoglobin of 94 g/L. He reported neither gastrointestinal symptoms nor weight loss. Upper gastrointestinal endoscopy and colonoscopy were done to evaluate his anaemia. No significant finding was seen during the upper gastrointestinal endoscopy. In the colonoscopy, numerous diminutive polyps were noted throughout the colon, particularly at the ileocaecal valve and caecum (figures 1 and 2). Cold biopsies were performed on the smaller (1–2 mm) polyps at the caecum, while cold snare polypectomies were performed to the larger ones in the rest of the colon (figures 3 and 4).

Endoscopic view of the ileocaecal valve.

Close up endoscopic view of the caecal wall under (A) white light, (B) narrow-band imaging.

Endoscopic view of an ascending colon polyp.

Endoscopic view of a transverse colon polyp.
Question
What is the diagnosis?
Answer
These polypoidal lesions are multiple lymphomatous polyposis. Lymphomatous polyps are usually dome shaped and appear subepithelial with smooth and glistening surfaces. The subepithelial appearance is thought to be due to the abnormal lymphoid aggregates starting from lamina propria or submucosa of the gastrointestinal wall.1 Lymphomatous polyposis has a reported frequency of 4%–9% among all different endoscopic patterns of gastrointestinal lymphoma.2 Morphologically, these polyps can sometimes be mistaken for hyperplastic polyps.
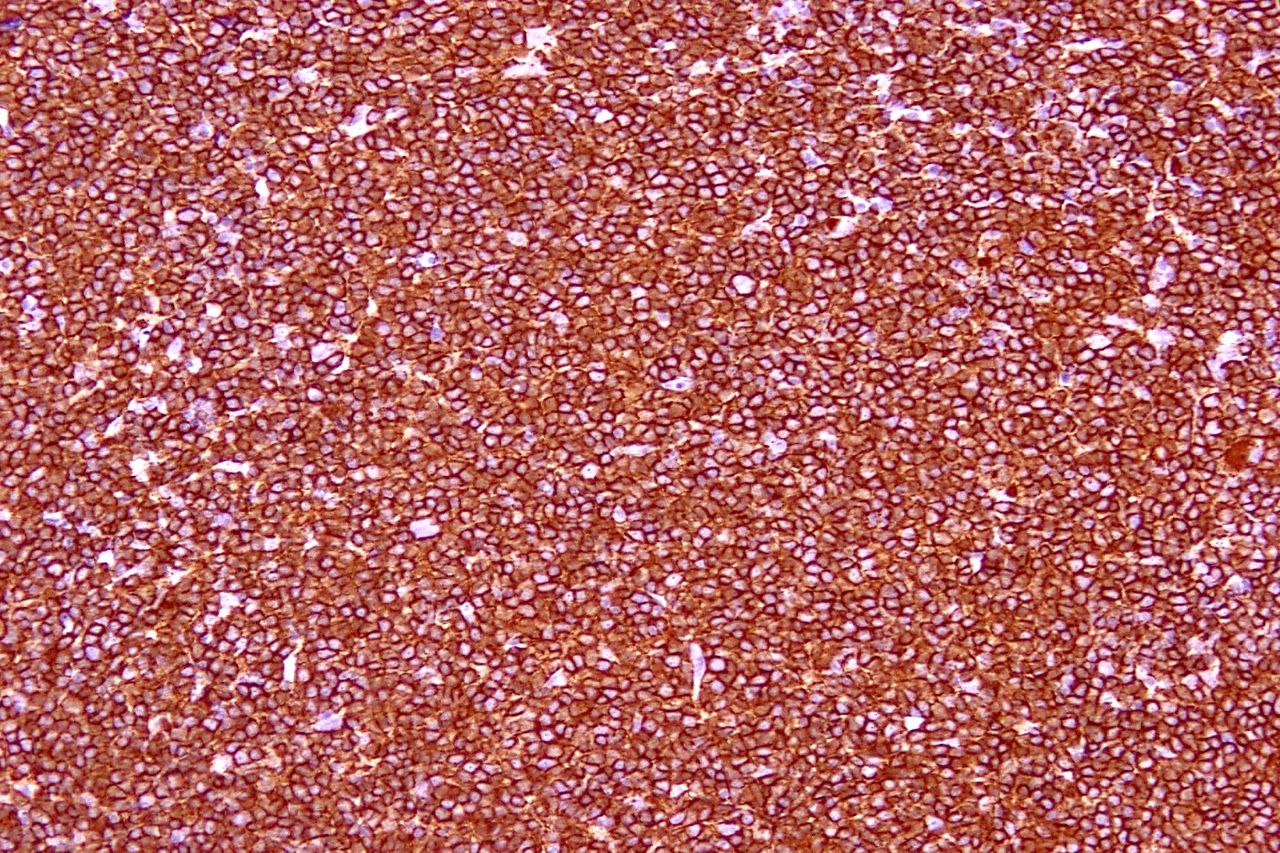
Gastrointestinal mantle cell lymphoma (MCL) was diagnosed as the histology from the colonic specimens demonstrated neoplastic small CD20+ B cells (figure 5) that coexpressed CD5, CD43 and cyclin-D1 (figure 6), while being negative for CD10, BCL-6 and CD23. Fluorescence in situ hybridisation revealed t(11;14)(q13;q32) mutation—the characteristic mutation in MCL. The patient was treated with an intensive rituximab-based chemotherapy.

Histology of the colonic lesions (H&E stain, original magnification ×100).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cyclin-D1 immunohistochemical stain (original magnification ×200).
The gut has the largest collection of immune cells in the body. Gastrointestinal lymphoma constitutes 10%–15% of all non-Hodgkin’s lymphoma (NHL) and 30%–40% of all extranodal NHL, making gastrointestinal tract the most common site for extranodal disease.3 In patients with isolated splenomegaly without lymphadenopathy, and a negative bone marrow examination, it is worth considering bidirectional gastrointestinal endoscopy, especially in the presence of anaemia or gastrointestinal symptoms, before embarking on more invasive procedures like splenic biopsy or diagnostic splenectomy.
Ethics statements
Patient consent for publication
Footnotes
Contributors JLH drafted and edited the manuscript. CV provided overall clinical supervision and edited the manuscript. RL performed the endoscopic procedures and edited the manuscript. CD provided help with histology component of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; internally peer reviewed.