Article Text

Abstract
Introduction Crohn’s perianal fistulas are challenging for patients and clinicians. Many do not respond to available treatments and despite recommendations by a global consensus, there are currently no specific patient-derived quality of life tools to measure response to treatment. We present a new validated patient-reported outcome measure (PROM) for this complicated disease phenotype.
Methods A draft questionnaire was generated using unstructured qualitative patient interviews on the experience of living with Crohn’s perianal fistula, a nationwide multidisciplinary consensus exercise, a systematic review of outcomes assessing medical/surgical/combined treatment and a patient and public involvement day. Psychometric properties were assessed including construct validity (by comparison with the Hospital Anxiety and Depression Scale (HADS) and the UK Inflammatory Bowel Disease Questionnaire (UK-IBDQ)), and reliability and responsiveness was assessed by test–retest analysis.
Results Data from 211 patients contributed to development of a final 28-item questionnaire. The Crohn’s Anal Fistula Quality of Life (CAF-QoL) demonstrated good internal consistency (Cronbach’s alpha 0.88), excellent stability (intraclass correlation 0.98) and good responsiveness and construct validity, with positive correlation with the UK-IBDQ and HADS.
Conclusion The CAF-QoL scale is ready for use as a PROM in research and clinical practice. It complements objective clinical evaluation of fistula by capturing impact on the patient.
- Crohn's disease
- quality of life
- gastrointestinal fistulae
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. Additional supplementary data assessing the psychometric properties of the CAF-QoL scale are available on request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
There is heterogeneity in outcome measurement in Crohn’s perianal fistula, limiting comparison of treatment options, with no widely accepted gold standard. There is currently no patient-reported outcome measure (PROM) for Crohn’s perianal fistula, representing an unmet need, which was highlighted in a published core outcome set for perianal Crohn’s disease.
What are the new findings?
The development and initial validation of a new PROM for Crohn’s perianal fistula, the Crohn’s Anal Fistula Quality of Life scale.
How might it impact on clinical practice in the foreseeable future?
This new PROM lends itself to utility in clinical trial design for Crohn’s perianal fistulas, enabling consistency in data sets collected in this condition. It also has the potential utility of assessment of disease impact in a clinic setting, to guide stratification of patients according to severity of disease impact and tailor appropriate management.
Introduction
Perianal fistulas occur in a third of all patients with Crohn’s disease (CD).1 They represent a distinct and aggressive phenotype of CD1 2 and often follow a chronic course with symptoms including anal pain and purulent discharge, commonly leading to a severely impaired quality of life (QoL). Crohn’s perianal fistulas are challenging to treat; often complex in nature, they can be refractory to conventional medical treatment strategies such as antibiotics, immunomodulators3 4 and biologic drugs, such as anti-tumour necrosis factor agents.5–9 Surgical treatments fare little better and despite a multidisciplinary approach (ie, concomitant surgical and medical therapies), most patients experience recurrence or persistence. The associated morbidity of the disease and its treatment can have profound effects on patients’ physical and psychosocial well-being.
In clinical trials, success is usually measured by clinical assessment of closure of fistula tracks, sometimes accompanied by radiological assessment of ‘healing’. This is appropriate in trials of treatment with ‘curative intent’, but as most patients do not achieve sustained fistula closure, there is a need to measure any benefit produced by treatments in situations where fistulas do not ‘heal’. Further, it is important to assess additional impacts of any intervention on QoL even if successful ‘healing’ occurs. For example, continence impairment might occur after a ‘curative’ fistulotomy or advancement flap repair. There are also interventions, such as setons, which are not designed to heal fistulas and are performed with intent to ameliorate symptoms rather than cure. QoL assessment may represent the primary outcome in such situations.
The only current measure designed to assess Crohn’s perianal fistula activity and its impact on QoL is the Perianal Disease Activity Index (PDAI).10 This clinical assessment tool aims to measure disease activity in patients with Crohn’s perianal fistulas. It assesses pain, restriction of physical and sexual activities, and perianal disease severity (discharge, disease type and induration). Items are scored from 0 (no problem) to 4 (severe problem) on a Likert scale.10–12 Although the PDAI was developed to measure clinical disease activity in patients with ‘perianal disease’, it is not specific to perianal fistula and was not developed using methodology that conformed to accepted principles of evaluative index development.13 A significant limitation to its use as a patient-reported outcome measure (PROM) is the lack of patient involvement in its development, relying instead on QoL issues which physicians believed to be important to patients. Thus, it does not assess the global QoL impact of fistulas on patients, and its relevance to what patients themselves consider as important is unknown. Recent guidelines recommend that improved instruments are needed to score perianal CD fistula activity and impact on QoL.8 In particular, a tool which assesses the impact of fistula(s) on a patient’s QoL and which detects a meaningful change in their QoL after treatment is required. Early exploratory qualitative work demonstrates that the impact of CD perianal fistulas extends far beyond restricting daily and sexual activities14 15 and a patient-centred, patient-derived tool is needed. We aimed to develop and undertake initial psychometric validation of a new QoL scale for patients with CD with perianal fistulas ensuring patients were involved in all phases of development.
Methods
Overview
The study used a three-phase mixed methods design using an exploratory instrument development model16 17 to support a QoL PROM development process.18 Phase 1 used an exploratory qualitative approach19 to create a long list of items. Phase 2 involved cognitive interviews to refine items. Phase 3 subjected the draft PROM to psychometric testing via completion by participants with Crohn’s perianal fistula and completed final item reduction.
Study steering group and patient and public involvement
Members of the study steering group included all relevant stakeholders: a colorectal surgeon with expertise in fistulas, a gastroenterologist with expertise in IBD, IBD specialist nurses (2), researchers with experience in PROM design (3)20 and patient representatives (4). The latter constituted our patient and public involvement (PPI) team and consisted of four members of Crohn’s and Colitis UK (CCUK) charity. All had CD and previous or current experience of living with a perianal fistula. The PPI team helped with analysis and contributed to discussion and development of the preliminary items for the draft questionnaire and final item reduction. The study design was also presented at a dedicated PPI day for critical feedback and to gather suggestions to optimise recruitment and response rates.
Recruitment and sampling
Participants were recruited using purposive sampling from the membership (via advertisement) of collaborating registered patient charities including those specific to IBD/bowel diseases (ForCrohn’s, CCUK, Bowel Disease Research Foundation) and UK-wide patient repositories (UK IBD BioResource). Recruitment also occurred via IBD outpatient clinics, aiming to recruit equal numbers of men and women, with a broad age range.
Selection of participants
Inclusion criteria: Over 16 years; living in the UK; diagnosis of CD with perianal fistula; ability to read, speak and understand English; ability to give informed consent.
Exclusion criteria: Patients with resolved fistulas were excluded from phase 3 and participants contributing to any phase of the study were excluded from contribution to another.
Data collection/generation of a draft PROM
Phase 1: experience interviews/data from outcomes review and consensus exercise
(A) Individual unstructured interviews were conducted face to face or by telephone/video call according to participant preference, to explore the experience of living with CD-related perianal fistula(s) and the impact of the disease and surgical and/or medical treatments on the individual. This facilitated an in-depth understanding of the complex experience of living with Crohn’s perianal fistulas. Interviews were digitally recorded and transcribed verbatim by a professional transcriber. A thematic analysis15 21 22 was undertaken to generate a long list of items for inclusion in the draft PROM. Individual followed by steering group analysis and agreement ensured that findings represented a consensus of the steering group.15 22
(B) To enhance the face and content validity of the questionnaire, we included data from a systematic review of fistula outcome measures and a consensus exercise undertaken to develop a core outcome set (COS) for Crohn’s perianal fistulas.23 The systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines and involved a search limited to studies conducted in adults aged ≥18 years and papers published between 1 January 2010 and 12 July 2016. Reference lists were searched to ensure complete capture. We assessed the results to identify patient-reported outcomes and included these in the long list of items for the draft PROM. The COS involved stakeholder recruitment from across the UK,23 including clinicians (colorectal surgeons, gastroenterologists, radiologists and IBD nurses) and patients, the latter being the primary stakeholders. Qualitative data from patient focus groups (discussing QoL and outcome measurements) in the COS exercise were discussed by the consensus steering group and included in the long list of items for the draft PROM.
At the end of phase 1, items for inclusion in the PROM (the Crohn’s Anal Fistula Quality of Life (CAF-QoL) scale) were collated using a mixture of questions and statements. Scoring systems (mixture Likert scale/closed-ended ordinal answers) were added following steering group consensus. A background section (16 questions) collected demographic data and disease details (including duration, number of fistulas, medication and surgical history). This section also had an anchor question using a 10-point Likert scale to measure self-reported global rating of fistula status. This enabled transitional analysis on the basis of the participants’ subjective perceptions of their fistula.
Phase 2: cognitive interviews/pretesting of draft PROM
Participants in this phase provided further content validation via four cognitive interview rounds (involving three to four individual interviews per round), to enable participants to refine the questions using think-aloud techniques and verbal probing as they completed the draft PROM. Interviews were digitally recorded and transcribed by a professional transcriber. Following each round of cognitive interviews, items were reviewed by the steering group to ensure any suggested changes were agreed by consensus. Subsequent rounds of interviews were used to confirm acceptability until data saturation was achieved and no new suggestions were received.
Phase 3: testing of the new CAF-QoL PROM
Participants with CD and active (ie, presence of symptoms related to) perianal fistulas were sent the draft CAF-QoL PROM by post or online and asked to complete it again 2 weeks later for test–retest reliability. At the initial administration of the CAF-QoL PROM, participants were also asked to complete a demographic details form, the validated UK-IBDQ24 and the Hospital Anxiety and Depression Scale (HADS).25 Overall and perianal fistula disease activity information was collected on both occasions using a modified version of the Harvey-Bradshaw Index (HBI)26 27 and self-reported global rating of fistula status. This allowed stratification according to change in overall disease activity level between the test and retest analysis and allowed a subanalysis for sensitivity to change in fistula status.
Testing of psychometric properties
Validity
Content validity assessed the applicability, relevance and clarity of question items in order to maximise the accurate completion of the questionnaire. Further to verification of content validity in phases 1 and 2, it was explored by evaluating the levels of missing data per item in phase 3. The overall response rate was analysed to indicate the feasibility of the questionnaire for self-completion.
Construct validity assessed the consistency of the scale with other instruments known to assess similar attributes with good validity and reliability. Two validated outcome measures (UK-IBDQ24 and HADS25) were used as comparators to evaluate the relationships between patients’ reports as these measures cover some similar concepts. Correlation was assessed using Pearson’s correlation coefficient (r).
Reliability
Test–retest reliability (reproducibility or stability) assessed consistency between the two completions of the draft CAF-QoL.28 29 Respondents completing the phase 3 test–retest in whom the IBDQ, HADS and anchor questions indicated stable disease were used to assess reliability.24 30 31 Relevant anchor questions were a general rating of fistula status (on a Likert scale of 0–10) and a question ascertaining whether there had been any flare-up of their fistula (requiring medication, operation or seton) since the previous questionnaire completion. Those who reported no changes (absence of flare-up, <1 point difference on Likert scale and stable overall IBD disease activity as defined by stable HBI scores) were included in the reproducibility analysis. The difference between test and retest responses was appraised using weighted statistics (the weighted kappa method32 33) due to the categorical nature of response options. Kappa is measured on a scale ranging up to a maximum agreement of 1, with values signifying a good (>0.6) and very good (>0.8) strength of agreement.34 Reproducibility of the total CAF-QoL scores for stable patients was also assessed using the intraclass correlation (ICC) coefficient. The ICC is the proportion of total variation in CAF-QoL scores between test and retest completions that is due to variation between respondents (inter-respondent variation), as opposed to variation within respondents (intrarespondent variation). A high agreement between test and retest scores implies little intraparticipant variation and thus an ICC value close to 1 with values exceeding 0.75 generally accepted as a marker of good reproducibility.28
Sensitivity to change
Sensitivity to change (or responsiveness) was assessed in retested patients who reported significant change (ie, three or more points on the Likert scale) in their general rating of fistula status. Comparisons between baseline and retest overall CAF-QoL scores were assessed using mean change between successive completion scores, with a corresponding CI. Changes with p values <0.05 were deemed significant.
Item reduction: questionnaire refinement
Factor analysis (FA) with principal axis factoring extraction and varimax rotation were used to determine individual dimensions or subscales of the CAF-QoL and to refine the number of items.35 The internal reliability (ie, correlation between different items) was determined using Cronbach’s alpha (values exceeding 0.7 indicate good consistency).28 The strength of association between individual questions was assessed using Pearson’s correlation coefficient. Those with strong associations (correlation coefficient >0.75) were reviewed by the steering group to achieve consensus on excluding questions deemed to duplicate information and those unlikely to change with intervention. Contentious items were discussed, and consensus agreed on exclusion of questions following review of those with missing data from a majority of participants (regardless of fistula status), questions with poor test–retest agreement (suggesting unreliability), questions with strong associations with others (ie, suggesting duplicated themes) and questions with poor spread of response.
Results
A total of 211 participants with Crohn’s perianal fistula were involved in the three study phases (table 1). Most participants (~60%) reported having IBD for longer than 10 years and over 80% had experienced Crohn’s perianal fistulas for at least 1 year. Fewer than 15% had a stoma (temporary or permanent).
Participant characteristics
Devising and pretesting the draft CAF-QoL scale: phases 1 and 2
Twelve interviews were conducted (median of 43 min, range 18–145 min) achieving apparent data saturation. Three broad themes emerged: burden of symptoms, burden of treatment and impact on emotional, physical and social well-being (figure 1). Each included several subthemes, with considerable interplay between these.15 The impact of perianal fistula(s) on patients with CD was intense and wide reaching, negatively affecting intimate, close and social relationships and causing losses in life and work-related opportunities.36 Data from the qualitative interviews were combined with those from the COS exercise which involved more than 230 stakeholders from across the UK,23 including 80 patients with Crohn’s perianal fistula. Data from the COS included the systematic review of patient-reported outcomes, qualitative data from patient focus groups and the final list of core outcomes. An original long list of 45 items was collated for the draft PROM and these were reviewed by the steering group, reducing these to 35 items following elimination of repetition and overlap. Those retained were grouped under three domains (A–C) mirroring the broad themes described above and converted into questions (Domain A—symptoms) and statements (Domain B—treatment and Domain C—QoL impact). Likert scales were adopted measuring frequency (0–4) in domain A, and degree of agreement (Likert scales 0–4) in domains B and C. The questions and statements were phrased to ensure that positive answers (indicating good QoL) were always at the lower end of the Likert scale, and higher scores indicated worse QoL. Pretesting occurred during cognitive interviews (n=15; average questionnaire completion time was 9 min) and no additional items were suggested for inclusion.

Thematic depiction of the experiences of living with Crohn’s anal fistula Themes are located in the central circles with the subthemes in the peripheries
Testing the CAF-QoL: phase 3
Patient sample
The test data consisted of responses from 184 patients. Three (1.6%) were excluded due to excessive missing data leaving 181 CAF-QoL questionnaires for analysis. The retest data had a response rate of 79% (143/181) completing the questionnaire.
Data spread and completeness
Results of the test data indicated that the majority of responses were spread across the available categories, demonstrating that the questionnaire can discriminate between patients with a range of symptoms and concerns. There were little missing data with fewer than 1% of respondents missing sporadic responses. Most questions were applicable to the majority of respondents. Some questions had ‘not applicable’ responses. These were the questions relating to presence of seton or side effects of medication and was highest for the question relating to presence of a stoma (not applicable to 83% of respondents). Analysis of the association between questions demonstrated that there were no ‘perfect’ correlations, with no correlation coefficient over 0.9. Therefore, no questions were perfectly duplicating information. However, there were some strong associations between questions (correlation coefficient >0.8), and these were considered for item reduction.
Item reduction
Nine questions were removed from the final CAF-QoL (see online supplemental appendix 1 for item reduction overview). Three questions pertaining to symptoms (domain A) were removed. Two of these had very little spread in response categories, with low SD, and responses were grouped towards the lower end of the Likert scale (indicating minimal relevance to most respondents). These questions related to the use of painkillers and the association of urinary tract infections to the fistula. One question relating to the use of pads or gauze for the discharge from the fistula was removed due to strong association with the preceding question on fistula discharge, with consensus decision that there was probable overlap in the item being assessed. Four questions relating to fistula treatment (domain B) were removed due to poor spread and poor test/retest agreement (in those reporting no change in global fistula status). Two questions relating to QoL impact (domain C) were removed. These questions involving fistula effect on intimacy and career progression were found to be strongly associated with other questions (correlation coefficient >0.83), replicating themes.
Supplemental material
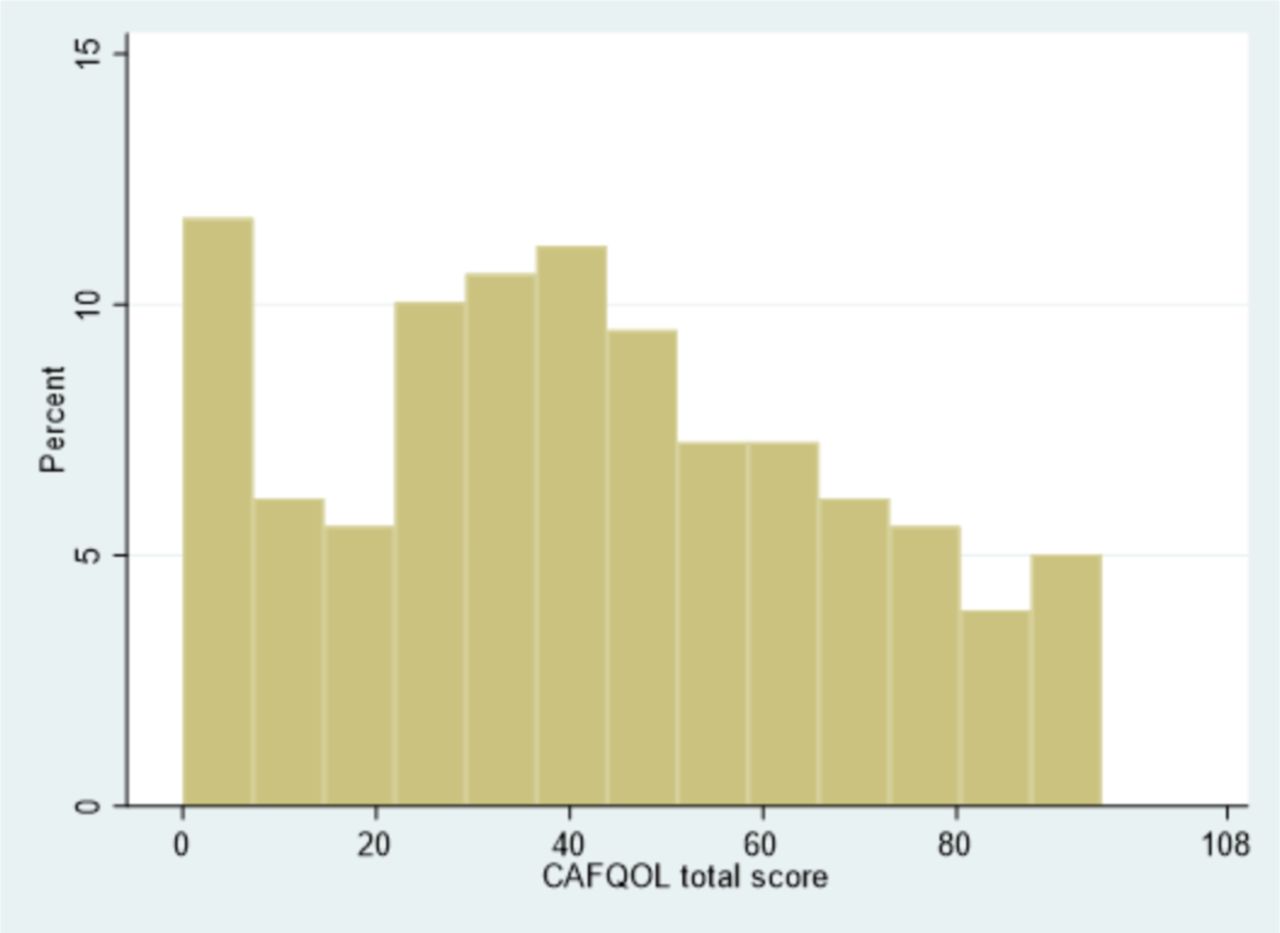
The final version of the questionnaire included 28 items, 27 of which were scored from 0 to 4, plus one free-text question (figure 2), giving a score range of 0–108. Data from 181 respondents demonstrated scores of 0–95 (possible range 0–108), as depicted in figure 3. Scores were approximately normally distributed with a mean score of 42.0, and an SD of 26.0.

The Crohn's Anal Fistula Quality of Life (CAF-QoL) scale. © London North West University Healthcare NHS Trust 2020. © Imperial College Innovations Ltd 2021. All rights reserved. Individuals or organisations wishing to reuse the Crohn’s Anal Fistula Quality of Life (CAF-QoL) scale should contact Manish Patel – Imperial College London at nhsinfo@imperial.ac.uk.
{kind=link}
{kind=link}
{kind=link}
Histogram of total CAFQOL scores. CAF-QoL, Crohn’s Anal Fistula Quality of Life.
Internal consistency and FA
Cronbach’s alpha was 0.88, demonstrating a good degree of internal consistency among the individual items. An FA was performed to determine if the score naturally broke down into different subscales. Only one factor was found to be significant, encompassing the majority of questions, indicating no subscales.
Reliability (agreement between test and retest scores)
Sixty-nine patients of the 143 retest respondents (48%) met the criteria for disease stability (as defined by ≤1 point difference between test/retest scores on global self-rating of fistula status, and stable disease on HBI and no fistula flare between test/retest completion). Weighted kappa was >0.7 for all items, demonstrating very good agreement. The mean difference between the retest and test measurements (calculated as retest minus test) was −0.6 with an SD of 6.0. The agreement between test and retest scores was also examined using ICC method. This method gave an ICC value of 0.98 (95% CI 0.96 to 0.99). This high value demonstrated very good agreement between the test and retest scores.
Sensitivity to change
In order to examine the change in CAF-QoL total score between test and retest in specific groups of patients, three groups were examined relating to patients with ‘stable’, ‘improving’ and ‘worsening’ global fistula rating (table 2). In patients with stable disease there was no significant change in CAF-QoL scores between the two time points. CAF-QoL scores decreased significantly at the retest time point in those with improved disease, by an average of 4 units. Conversely in those with worsening global fistula rating scores increased significantly between time points, by a mean of 7 units.
Changes in CAF-QoL score from test to retest
Association with other health-related measures
Assessment of the agreement between the total CAF-QoL scores and other health-related measures (UK-IBDQ/HADS) used Pearson’s correlation (table 3). The results demonstrated significant positive correlations between the total CAF-QoL score and each of the other measures. Higher CAF-QoL scores were associated with higher levels of anxiety and depression, and also worse IBDQ scores.
Association between CAF-QoL scores and other health scores
Discussion
The CAF-QoL questionnaire scale has demonstrated good reliability, internal consistency and face/content validity. The robustness of the questionnaire is confirmed through the rigorous developmental process, with participants with Crohn’s perianal fistula contributing throughout, as participants and on the steering group. This has ensured that the language is straightforward, using lay terms that increase readability and enable accurate interpretation, and that the content is relevant to patients.
There is limited evidence in the literature on QoL in patients with anal fistula. Reported patient assessment of interventions highlights that patients have concerns with regard to anal fistulas and the treatment options; however, data collection is often rudimentary, involving patient satisfaction or incontinence.37 38 The absence of a validated PROM means patients’ concerns are often expressed based on clinicians’ perspectives and this was highlighted in an Australian study by Wong et al 39 comparing surgeon and patient preferences for surgical operations for idiopathic anal fistulas. The different cure and incontinence rates for each procedure were quoted for the patients to consider and their preferences explored. A clear mismatch was reported between what the surgeons and patients felt were important QoL issues. For example, 91% of surgeons versus 25% of patients nominated continence as an important QoL issue.39 The study demonstrated the potential assumptions made by clinicians with regard to the impact of fistula surgery on patients’ QoL. More recently, Ferrer-Marquez et al 40 developed a QoL questionnaire in patients with (non-Crohn’s) anal fistula; however, major limitations of this study were the testing on a small sample (n=54) of Spanish-speaking patients, and crucially patients were not included in the initial development of the questionnaire. There is no objective patient-centred disease scoring tool for Crohn’s perianal fistula and this results in an inability to quantify adequately the effect of Crohn’s fistulas on psychosocial well-being and has led to calls to address the unmet need for a disease-specific PROM.41
Study strengths and limitations
The strength of the study lies in its design, incorporating a literature review, consensus exercise, patient focus groups and individual patient interviews19 (unstructured and cognitive) to inform the item generation. Recruitment of participants occurred via nationwide charities, hospitals and social media, ensuring a broad sample of those with experience of Crohn’s perianal fistulas. The involvement of patients both as participants and in the steering group ensured their voice was central to every stage of the process, facilitating creation of a true PROM. This is often lacking in PROM development.42 Another strength was the diversity of stakeholders in the steering group (patient representatives, gastroenterologist, colorectal surgeon, specialist nurses, qualitative researchers) while ensuring that patient input was always prioritised.
Limitations include the absence of data collected on other manifestations of perianal CD which often coexist with fistulas. This was a deliberate decision based on a consensus view to create a fistula-specific PROM. Another potential limitation was the lack of access to exact data, for example, MRI and other anatomic fistula data for participants recruited via charities. However, the large number of patients contributing to the CAF-QoL as well as the recruitment strategy (ie, recruited from various locations and not just tertiary centres) means that a spread of fistula/inflammatory characteristics is to be expected. Furthermore, patients reported different levels of symptoms at different points in the process (the basis of the test–retest phase) and were asked to describe the longitudinal history of their fistula during the interview stage so we would expect variation in fistula ‘phenotype’. Regarding analysis, respondents with temporary defunctioning stomas as opposed to following proctectomy did not have separate analyses assessing the influence of either intervention on QoL. The group consensus was that such patients might well have different priorities, goals and symptoms, and separate analysis might have contributed to a score which was useful for neither group. During the data collection, those with stomas had no CD-specific marker of disease activity pertaining to looser stool, and the HBI question on diarrhoea may have been ambiguous for these patients. However, only 14.6% (31/211) of the entire study cohort and 25/184 (13.6%) of the test–retest respondents had stomas and we made the assumption that disease activity might affect the fistula symptoms less in defunctioned patients, and thus not compromise the integrity of the score. In the analysis process, there were fewer numbers in the sensitivity to change/responsiveness analysis and a self-reported global fistula rating was used as a marker to assess transition in fistula status due to absence of a widely accepted/reliable clinical measure. Indeed, responsiveness and stability calculations were limited by the fact that there is no true gold standard to define a change in disease state. However, use of subjective transition questions is an accepted technique used in several outcome measure studies and can be advantageous in assessment of QoL because it directly addresses patients’ perceptions of change over time and is short and simple.24 29–31
Clinical usefulness and future direction
Assessing QoL in patients with IBD is an important component of medical and surgical management and clinical decision-making, and the last decade has seen a rapid increase in the number of measures to assess the QoL in patients with IBD.43 There was previously no validated outcome measure that captured the patients’ evaluation of the effect of interventions for Crohn’s perianal fistulas on their well-being. This has importance in the face of elusive cure/non-sustained fistula closure, and is equally valuable as a secondary outcome measure for determining the impact of interventions in studies with curative intent, and as a primary outcome in studies of disease or symptom-ameliorating interventions.44 The CAF-QoL is the first disease-specific PROM in Crohn’s perianal fistula developed with a patient-centred methodology. Completion takes about 9 min on average and can be done with the clinician present or independently by the patient, with the goal of assessing the benefit of interventions in clinical trials, both medical and surgical, as well as defining disease impact and severity in the clinical setting to aid decision-making. It may also play a role in highlighting changing concerns and priorities that arise for patients between remission and relapse, which may guide individualised patient advice and support. Future research will include validation of its use in clinical trials, measuring the CAF-QoL scale scores and determining if scores correlate with fistula activity levels and what constitutes a clinically significant response.
The currently available PDAI was developed to measure clinical disease activity in patients with ‘perianal disease’ and despite its use in clinical trials,41 it is not specific to perianal fistula. It was strongly considered for adjunctive use in this study, but we elected to go with a pragmatic recruitment strategy that obviated the need for clinical assessment of all patients (including those recruited via charities for questionnaire testing), which would have otherwise been required to ensure robust completion of the PDAI.
Future studies will use PDAI in addition to CAF-QoL (we hope) to enable comparison. There is also ongoing work to aiming to improve the objective measures available for assessing perianal fistula disease activity (eg, using MRI13). In addition, a comprehensive classification for Crohn’s perianal fistulas, which integrates all elements that are important for medical and surgical management, is required and may need to incorporate a combination of diagnostics (endoscopy/MRI/endoanal ultrasound) and examination under anaesthesia to ensure robustness. Ongoing refinement and validation of CAF-QoL will ultimately aid the utility of this PROM alongside an objective clinical outcome measure, both of which are necessary tools in the evaluation of perianal fistula. The CAF-QoL scale will also need translation into different languages and cross-cultural validation to aid international dissemination.
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. Additional supplementary data assessing the psychometric properties of the CAF-QoL scale are available on request.
Ethics statements
Ethics approval
The study was approved by King’s College London (ref: HR-16/17-4421) and the UK Health Research Authority (ref: 17/LO/1563). Informed consent was collected prior to data collection. Participants chose which phase of the study they wanted to be involved in.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @KSahnan
Correction notice This article has been corrected since it published Online First. A copyright line has been added to figure 2.
Contributors All authors have contributed substantially to this manuscript design/delivery. AH, CN, JW, OF and RKP were involved in the design of the study. AV, RS, DM and SM served as patient and public involvement and gave critical input and refinements to design. SOA and LD carried out patient interviews. SOA, KS, TW, PT, CN, AH, NY, AV, RS, SM and DM performed independent qualitative analysis of audio transcripts. SOA and PB performed statistical analysis. SOA, KS, PT and LD wrote the article. CN, AH, JW, OF and NY reviewed the article drafts providing refinements and steer. All authors reviewed and approved the final draft.
Funding The study was supported by the Bowel Disease Research Foundation (BDRF; DES008).
Competing interests KS, PJT and SOA have received honoraria from Takeda for sitting on an advisory board. PJT has received honoraria from Takeda for speaking at a symposium. LD: speaker fees from Janssen and AbbVie; consultancy fees from GL Assessments. CN: speaker’s fees from Takeda, Tillots Pharma and Ferring Pharmaceuticals. ALH has served as a consultant, advisory board member or speaker for AbbVie, Atlantic, Bristol Myers Squibb, Celltrion, Falk, Ferring, Janssen, MSD, Napp Pharmaceuticals, Pfizer, Pharmacosmos, Shire and Takeda. She also serves on the global steering committee for Genentech.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.