Article Text

Abstract
Objective Our aim was to explore the risk of infection with all classes of inflammatory bowel disease (IBD) medications and the impact of these medications on the disease course in a nationwide cohort of patients with IBD.
Design This was a retrospective national cohort study of patients with IBD in the Veterans Affairs Healthcare System. We categorised IBD medication use immediately prior to the COVID-19 pandemic and used survival analysis methods to study associations with SARS-CoV-2 infection, as well as a combined secondary outcome of COVID-19 hospitalisation or COVID-19-related mortality.
Results The analytical cohort of 30 911 patients was primarily male (90.9%), white (78.6%) and with ulcerative colitis (58.8%). Over a median follow-up of 10.7 months, 649 patients (2.1%) were diagnosed with SARS-CoV-2 infection and 149 (0.5%) met the combined secondary outcome. In adjusted models, vedolizumab (VDZ) use was significantly associated with infection relative to mesalazine alone (HR 1.70, 95% CI 1.16 to 2.48, p=0.006). Patients on no IBD medications had increased risk of the combined secondary outcome relative to mesalazine alone (sub-HR 1.64, 95% CI 1.12 to 2.42, p=0.01), however, no other IBD medication categories were significantly associated with this outcome, relative to mesalazine alone (each p>0.05). Corticosteroid use was independently associated with both SARS-CoV-2 infection (HR 1.60, 95% CI 1.23 to 2.09, p=0.001) and the combined secondary outcome (sub-HR 1.90, 95% CI 1.14 to 3.17, p=0.01).
Conclusion VDZ and corticosteroid were associated with an increased risk of SARS-CoV-2 infection. Except for corticosteroids no medications including mesalazine were associated with an increased risk of severe COVID-19.
- inflammatory bowel disease
- COVID-19
- 5-aminosalicylic acid (5-ASA)
- crohn's disease
- ulcerative colitis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
Data on the impact of inflammatory bowel disease (IBD) medications on the risk of SARS-CoV-2 are lacking.
Results from previous studies which have evaluated the impact of IBD medications on the clinical course of COVID-19 need to be validated in different study populations.
What are the new findings?
In a predominantly elderly male population.
Vedolizumab use for IBD was associated with an increased risk of infection with SARS-CoV-2.
Corticosteroid use for IBD was associated with an increased risk of infection with SARS-CoV-2.
Mesalazine use was neither associated with an increased risk of SARS-CoV-2 or severe COVID-19.
How might it impact on clinical practice in the foreseeable future?
This is the first study to link vedolizumab use with the acquisition of SARS-CoV-2.
Contrary to existing literature, mesalazine use was neither associated with an increased risk of severe COVID-19.
This study reaffirms the recommendation that physicians should exercise caution to use corticosteroids for IBD during the SARS-CoV-2 pandemic.
Introduction
The SARS-CoV-2 pandemic is a severe threat to public health with more than 20 million people reported to have been infected in the USA as of 1 January 2021.1 Several factors such as increasing age, cardiovascular disease, chronic lung disease, obesity and diabetes have been identified to increase the risk of severe COVID-19 infection.2 3 Inflammatory bowel disease (IBD), comprising of ulcerative colitis (UC) and Crohn’s disease (CD), is a chronic inflammatory disorder of the gastrointestinal tract of unknown aetiology. IBD is characterised by perturbation of the mucosal immune system and is usually treated with immunomodulatory and/or immunosuppressive medications which can lead to an increased risk of infections.4–6 Additionally, significant molecular intersections between SARS-CoV-2 and IBD-associated intestinal mucosal pathways have been described warranting further insights into potential clinical ramifications of IBD therapies on the risk of SARS-CoV-2 infection.7 8
The incidence of SARS-CoV-2 among all patients with IBD appears to be comparable to that seen in the general population.9–12 However, the impact of drugs used to treat IBD on the risk of infection has not been fully explored. Rather, most studies have examined the course of SARS-CoV-2 infection after the infection is documented. For example, Surveillance Epidemiology of Coronavirus Under Research Exclusion (SECURE-IBD) studied patients diagnosed with infection and not the risk of infection.13 14 Despite major achievements, SECURE-IBD also has certain inherent limitations and it is important to validate the findings in other study populations.
Thus, to better understand the risk of infection with all classes of IBD medications and the impact of medications on disease course, we conducted a retrospective study in a nationwide cohort of patients with IBD in the Veterans Affairs Healthcare System (VAHS). The VAHS is the largest integrated healthcare system in the USA serving more than 9 million veterans every year.15 The VAHS is an apt health system in which to conduct this study as it has established a database of all patients who have tested positive for SARS-CoV-2 and all medication records are maintained in a central pharmacy dataset prior to and postinfection.
Methods
Study design and cohort creation
This was a retrospective cohort study using data from the VAHS. The primary study period extended from 20 January 2020 to 10 December 2020. The focus of the study was on the impact of medications used to treat IBD, which include 5-aminosalicylic acid (5-ASA, ie, mesalazine), corticosteroids, thiopurines (TP) (azathioprine and mercaptopurine) and methotrexate (MTX) (jointly referred to as immunomodulators), anti-tumour necrosis factor agents (anti-TNFs), vedolizumab (VDZ), ustekinumab and tofacitinib.
We identified all patients with either UC or CD diagnosed prior to 20 January 2020 using a previously validated algorithm.16 We obtained inpatient and outpatient International Classification of Diseases, Version 9 and 10, Clinical Modification(ICD-9-CM, ICD-10-CM) diagnosis codes (online supplemental table 1), encounters, procedures, pharmacy and demographic data for the study population. To create a source cohort, we used the following criteria1: ≥1 ICD-9 or ICD-10 diagnosis code for UC and/or CD,2 ≥1 outpatient visit in VA healthcare system,3 at least one outpatient pharmacy claim for any of the IBD medications (ie, mesalazine, TPs, anti-TNF agents and vedolizumab), and4 at leasttwo prescriptions of one distinct medication in the following five IBD medication groups (ie, mesalazine only, TPs, anti-TNF agents, a combination of TPs and anti-TNF, and vedolizumab). We did not include tofacitinib or ustekinumab to define cohort entry as they are not approved as first-line medications in the management of IBD in the VAHS and are primarily used for other medical conditions in the network. To identify patients primarily cared for in the VAHS and thereby minimise misclassification, we only included patients with at least 6 months of VAHS data prior to 20 January 2020. After additionally classifying patients according to their IBD medication use on 20 January 2020 (below), we then excluded patients who were not on any IBD medications in the 3 months prior to 20 January 2020, and who had fewer than five IBD-related diagnoses in the 5 years prior to study entry. The rationale for this exclusion is that these patients were less likely to truly have IBD and be followed in the VAHS. In the primary analysis (below), we performed a sensitivity analysis where the exclusion criteria were relaxed to include fewer than three IBD-related diagnoses in the 5 years prior to study entry.
Supplemental material
Ascertainment of exposures IBD medication categories
From the VAHS data repository, we collected demographic (age, sex, race) and comorbidity data including obesity, hypertension, diabetes mellitus, heart failure, arrhythmia, peripheral vascular disease, chronic obstructive pulmonary disease, chronic liver disease and renal failure. The primary exposure of interest was IBD medication category, which was determined in a 3-month window prior to 20 January 2020. The following mutually exclusive categories were used: mesalazine alone, TP alone, anti-TNF), anti-TNF plus TP, anti-TNF plus MTX, vedolizumab, ustekinumab and tofacitinib. If patients were on none of these medications, they were categorised as ‘no IBD medications’. Use of corticosteroids (prednisone, prednisolone, methylprednisolone) in the 3-month window was classified separately as a binary variable.
Ascertainment of outcomes
The primary outcome was time to SARS-CoV-2 infection, which was determined based on results of PCR testing performed in the VAHS. The secondary outcome was a combined outcome of hospitalisation related to COVID-19 infection or COVID-19-related mortality, defined as death occurring within 90 days of documented infection. This combined outcome was regarded as a surrogate of severe COVID-19 infection.
Primary statistical analysis
Descriptive statistics were presented as medians and IQRs for continuous variables and percentages for categorical data. Statistical comparisons among IBD medication categories were made using Wilcoxon rank-sum and χ2 tests, as indicated. Due to small sample size, only descriptive data were presented for the ustekinumab and tofacitinib groups, and they were excluded from subsequent multivariable modelling. Crude incidence rates of SARS-CoV-2 infection, COVID-19 hospitalisation, and COVID-19 mortality were computed for each IBD medication category and corticosteroid use, as well as unadjusted Kaplan-Meier survival plots for SARS-CoV-2 infection (the latter excluding ustekinumab and tofacitinib). Statistical comparisons were made using the log-rank test. Mixed-effects Cox regression analysis was then used to evaluate the impact of IBD medication category on the risk of SARS-CoV-2 infection, adjusting for potential confounders. Time zero was 20 January 2020, and data were right censored at patient death or loss to follow-up (ie, no further clinical encounters in the record system). US geographical region was treated as a random effect, given the variable temporal burden of COVID-19 experienced throughout the country. All demographic and comorbidity data were considered for adjustment in multivariable modelling, using a backward stepwise selection approach to identify a base model. Corticosteroid use was forced into all models given a plausible independent association between the primary exposure and outcome. After the base model was identified, we then created several clinician-directed models where we reintroduced or removed variables based on clinical grounds. Additionally, an interaction term between IBD medication category and steroid use was evaluated. The final model was chosen based on a minimised Bayesian information criterion value. HRs and 95% Cis were reported for each model exposure, and adjusted survival curves were plotted for IBD medication category and corticosteroid use. Given the possibility of informative censoring of non-COVID-19 related deaths, we performed a sensitivity analysis where we treated non-COVID-19-related death as a competing event in the final model, using the Fine and Gray method. In all cases, type 1 error rate of 5% was used for statistical significance. SAS version 9.4 and STATA V.15.1/IC were used for data management and analysis.
Secondary analysis
To evaluate the impact of IBD medication groups on the combined outcome of COVID-19 hospitalisation or COVID-19-related mortality, we used Fine and Gray competing risks regression where death from non-COVID-19-related causes was treated as a competing event. In contrast to the primary analysis above, we chose the Fine and Gray method as the initial analysis approach for the combined outcome due to the greater proportion of non-COVID-19-related mortality events relative to the outcome, and a clearer expectation to violate the assumption of non-informative censoring using standard Cox regression. Estimates were adjusted for the same predictors identified in the primary analysis. Sub-HRs (SHRs) were presented along with 95% CIs. As before, these analyses excluded patients on ustekinumab or tofacitinib due to small sample size. Finally, three additional subgroup analyses were performed, using the above competing risks regression approach1: comparing mesalazine alone to any other IBD medication group (excluding ‘no IBD medications’),2 comparing mesalazine use alone to any anti-TNF use, and3 comparing vedolizumab use to any anti-TNF use.
Patient and public involvement statement
As this was a retrospective cohort study, there was no patient or public involvement or recruitment for this study.
Results
Cohort characteristics
A total 30 911 patients met all inclusion and exclusion criteria. The cohort was primarily male (90.9%), white (78.6%), mostly with UC (58.8%), and with median age 65 years (IQR 50, 73). When stratified by IBD medication category, there were significant differences in patients’ age (eg, median 71 years for mesalazine vs 53 for anti-TNF +TP, p<0.001), IBD diagnosis (eg, 73.2% UC for mesalazine vs 38.5% anti-TNF, p<0.001), and various comorbidities (table 1). Corticosteroid use was more common in patients on vedolizumab (14.3% vs 4.6% for 5-ASA, p<0.001).
Cohort characteristics stratified by IBD medication category
Association between IBD medication category and SARS-CoV-2 infection
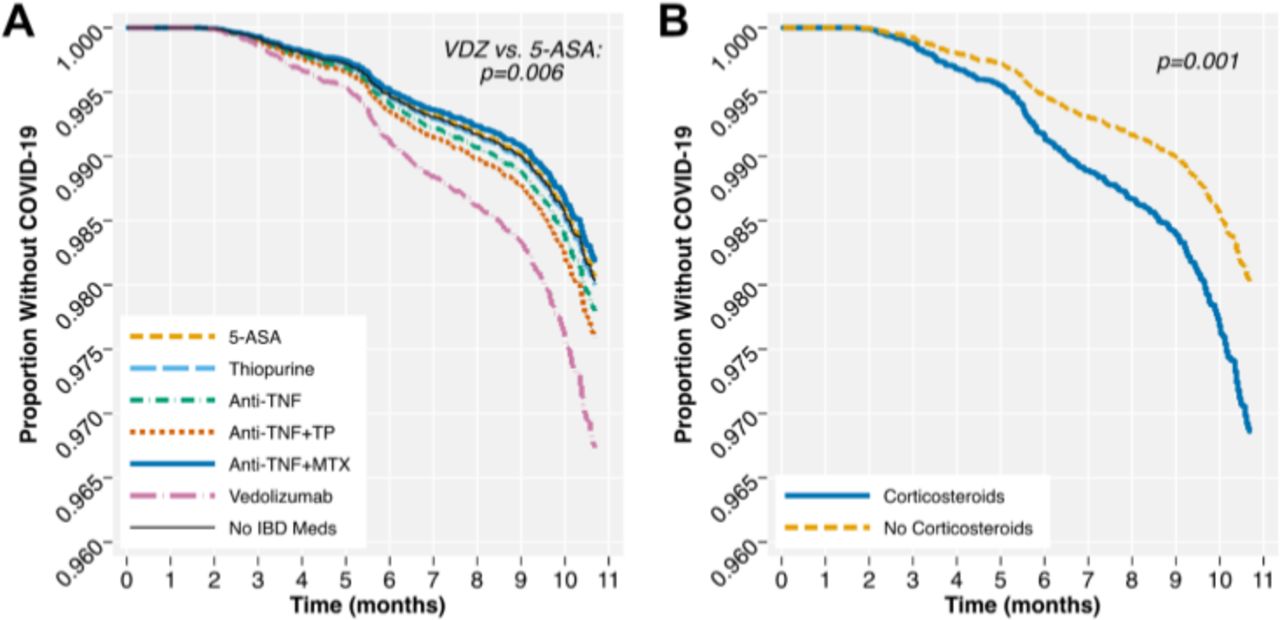
Over a median follow-up of 10.7 months (IQR 10.7–10.7), 649 (2.1%) patients were diagnosed with SARS-CoV-2 infection. The crude incidence rates of infection were highest in patients on vedolizumab (34.53 infections per 10 000 person-months, 95% CI 24.28 to 49.01: table 2). In unadjusted analysis, there were significant differences in SARS-CoV-2 infection by IBD medication category (p=0.02) and by corticosteroid use (p<0.001; online supplemental figure 1). In adjusted mixed-effects Cox regression analysis, there were significant differences in the hazard of SARS-CoV-2 infection for vedolizumab versus mesalazine alone (HR 1.70, 95% CI 1.16 to 2.48, p=0.006), however, there were no significant differences with other IBD medication categories versus mesalazine alone. Corticosteroid use as also associated with an increased hazard of SARS-CoV-2 infection (HR 1.60, 95% CI 1.23 to 2.09, p=0.001; table 3, figure 1). Testing for an interaction term between IBD medication category and corticosteroid use was not significant (p=0.95). In a sensitivity analysis where the exclusion criteria were relaxed, there were no substantive changes to the above results (online supplemental table 2). Finally, in a sensitivity analysis treating non-COVID-19-related mortality as a competing event, there were similarly no changes to the primary results (online supplemental table 3).
Supplemental material
Crude incidence rates* of SARS-CoV-2 infection, COVID-19 hospitalisation, and COVID-19 mortality by IBD medication group and corticosteroid use
Mixed-effects Cox regression model for SARS-CoV-2 infection*†
{kind=link}
Cox-adjusted* survival curves for development of SARS-CoV-2 infection by (A) IBD medication category and (B) corticosteroid use. *Models adjusted for age, race, diabetes mellitus, peripheral vascular disease and obesity, with geographical region treated as a random effect. 5-ASA, 5-aminosalicylic acid; IBD, inflammatory bowel disease; MTX, methotrexate; TNF, tumour necrosis factor; TP, thiopurine; VDZ, vedolizumab.
Association between IBD medication category and combined endpoint
Crude incidence rates of COVID-19 hospitalisation stratified by IBD medication category and steroid use are shown in table 2. Of the IBD medications, anti-TNF+MTX use had the highest incidence rate (7.42 per 10 000 person-years, 95% CI 2.79 to 19.77). Of the 649 patients with SARS-CoV-2 infection, 125 (19.3%) were hospitalised and 41 (6.3%) died. A total 149 patients (0.5%) met the combined endpoint of COVID-19 hospitalisation or COVID-19-related death. Non-COVID-19-related death occurred in 881 patients (2.9%) during the follow-up. In competing risks regression analysis, patients on no IBD medications had a significantly increased SHR of the combined outcome as compared with those on mesalazine alone (SHR 1.64, 95% CI 1.12 to 2.42, p=0.01; table 4). No other medication categories were significantly different from the mesalazine alone group (each p>0.05). Corticosteroid use was independently associated with the combined endpoint (SHR 1.90, 95% CI 1.14 to 3.17, p=0.01). Finally, in subgroup analyses, there was no significant difference in the subhazard of the combined endpoint between mesalazine alone and other IBD medications (SHR 0.77,95% CI 0.51 to 1.15, p=0.20), between mesalazine alone and anti-TNF use (SHR 0.80, 95% CI 0.49 to 1.31, p=0.38), or between vedolizumab and anti-TNF use (SHR 1.58, 95% CI 0.63 to 3.97, p=0.33).
Competing risks regression model for combined endpoint of COVID-19 hospitalisation COVID-19 mortality*
Discussion
We investigated the impact of different IBD medications on the risk of acquiring an infection with SARS-CoV-2 and developing severe COVID-19, defined as hospitalisation related to COVID-19 infection or COVID-19-related mortality. Treatment with vedolizumab, when compared with mesalazine, as well as corticosteroids, when compared with not taking corticosteroids, were associated with an increased risk of SARS-CoV-2 infection. Corticosteroid use was also associated with severe COVID-19. However, the use of vedolizumab was not associated with an increased risk of developing severe COVID-19 when compared with mesalazine use alone, and mesalazine use alone was not associated with severe COVID-19 infection when compared with all other IBD medications.
Our results reaffirm the preliminary analysis done by our group in which there were 36 SARS-CoV-2 cases, and which indicated that the use of TP and anti-TNF medications was not associated with development of COVID-19.17 This study includes more than 18-fold greater number of patients with SARS-CoV-2 infection than our prior study, allowing us to generate more precise estimates of risk. Again, we found that immunomodulators and anti-TNF drugs, whether used as monotherapy or in combination, were not associated with an increased risk of COVID-19. Not surprisingly, in this study, corticosteroids use was independently associated with an increased hazard of SARS-CoV-2 infection and severe COVID-19. Perhaps somewhat surprisingly, vedolizumab use was also associated with an increased risk of developing SARS-CoV-2 infection relative to mesalazine use, although not with severe COVID-19. Vedolizumab binds to α4β7 integrin of effector memory cells primarily fending off infections in the mucosa of the intestinal, but also the upper respiratory tract. The latter might be associated with a slightly increased risk of respiratory infections with vedolizumab treatment.18 Those sites by their expression of ACE2, the receptor for SARS-CoV-2, also pose entries for that viral infection, which could be the translational explanation for our finding.19
The number of patients on the newer medications for IBD, tofacitinib and ustekinumab, was low and hence precluded meaningful statistical analysis. However, the crude incidence rates for SARS-CoV-2 infection, COVID-19 hospitalisation, and COVID-19-related mortality did not identify concerning safety signals. As has been previously reported, we found that obesity, diabetes, and peripheral vascular disease were also associated with an increased risk of SARS-CoV-2 infection. The Royal College of General Practitioners also found obesity in addition to chronic kidney disease to be associated with an increased risk of SARS-COV-2.20 African American race was associated with a greater risk of contracting SARS-COV-2 as has been shown in other studies.21
We also evaluated the impact of IBD medications on the clinical outcomes of COVID-19 infection, as assessed by risk of the combined endpoint of COVID-19 hospitalisation or COVID-19-related mortality. Unlike SECURE-IBD, we did not look at ICU care or ventilator use. The primary reason was that in many VA hospitals as in other hospitals, the Medical and Surgical ICU were converted to COVID-19 patient holding areas. Thus, a relatively stable patient with COVID-19 could also be placed in the ICU making it difficult to ascertain whether a patient was in the ICU secondary to his medical condition. As the management of COVID-19 has evolved over time, the indications for ventilator use have also changed and thus it may not be the best indicator for disease severity especially in cohorts using recent data. We found that while there was a significantly increased incidence of SARS-CoV-2 infection with vedolizumab, this did not translate to an increased incidence of severe COVID-19, although this could reflect reduced statistical power for this outcome. Additionally, relative to other IBD medication categories, mesalazine use alone was not associated with an increased rate of severe COVID-19. There were also no differences in risk between mesalazine use alone and1 anti-TNF use or2 other IBD medication groups pooled together. However, patients on no IBD medications had a significantly increased risk of severe COVID-19 infection relative to mesalazine use alone. These results are in contrast to SECURE-IBD, which identified an increased risk of severe COVID-19 infection associated with mesalazine use. There are several possible explanations for this difference. First, there is possible reporting bias as the practitioners may be reporting their sickest patients, a limitation that the authors have noted. Second, our analysis accounts for the competing risk of non-COVID-19-related death, which was common in this population. Failure to account for this competing event in analyses would be expected to bias cumulative incidence estimates as well as associated relative effect sizes. Finally, our results are in accordance with previous research suggesting that mesalazine products are not associated with an increased risk of infections.5 Our data support the position that mesalazine products should be continued during the pandemic period where indicated, as they are the mainstay of treatment in stable UC patents.22
We found that corticosteroids use was independently associated with an increased risk severe COVID-19 infection (SHR 1.90, 95% CI 1.14 to 3.17, p=0.01). These findings are consistent with SECURE IBD which also showed that corticosteroids use was associated with more severe outcomes among COVID-19 patients.13 Similar results were also described in the rheumatological literature where corticosteroids use was associated with an increased risk of hospitalisation.23 In view of the increased risk of acquiring SARS-CoV-2 infection and developing a more severe COVID-19 disease course, the initiation of corticosteroids for the management of IBD should be carefully considered especially among high-risk patients who are older and have comorbidities. Our findings are not in line with the results from the Oxford Recovery Trial (NCT04381936) which states that low-dose dexamethasone reduces death by up to one-third in hospitalised patients with severe respiratory complications of COVID-19.24 The discrepancy in the findings could mainly be due to the differences in the impact of corticosteroids on the various stages of the COVID-19 disease. At the time of the initial infection with SARS-CoV-2, steroids are postulated to have a deleterious impact on the viral clearance or immune response while during later stages of the disease when the cytokine storm is more prevalent as in severely ill patients, steroids may decrease the magnitude of the immune response.25
The major strength of our study was the use of a nationwide cohort of IBD patients followed in the VAHS, serving approximately 9 million veterans every year.15 Every patient in the VAHS has an SARS-CoV-2 status determination in the electronic health record (positive, negative or not tested), even if diagnosed outside the VA. The VA has developed a central database which updates all SARS-CoV-2 diagnosis, hospitalisations and deaths among other features. However, there is a possibility that testing and hospitalisations outside the VA may not have been completely recorded leading to under reporting of events. Since we evaluated every patient followed in the VA, we were not impacted by reporting bias. Another strength of our study was the use of the nationwide VA Pharmacy records for gathering data regarding medications. The VA has a central pharmacy that is, if a patient used multiple VA centres during the course of his/her follow-up, data regarding all the medication prescriptions will be recorded in the central VA pharmacy, thus decreasing the chance of missing prescribed medications. Lastly, as previously highlighted, we had almost 650 patients making it the second largest IBD cohort of patients with SARS-CoV-2.
Our study is not without its limitations. First, due to the retrospective nature of our study, data regarding potential confounders may be missing. Furthermore, prescriptions filled outside the VA may be incomplete. However, we believe that such a bias would be minimal as empirically veterans have a strong adherence in using the VA pharmacy.26–28 Second, as this study was done in the VAHS, there are inherent external validity considerations, such as a predominantly male cohort. Our patient population also had a higher median age as compared with the average IBD population, thus limiting our ability to report on younger IBD patients with a short disease duration. However, due to the fact that SARS-CoV-2 is more likely to elicit clinical and symptomatic disease with increasing age, our patient population may be particularly sensitive to observe signals on the effect of concomitant disease medications on the risk of SARS-CoV-2 infection and severity. Furthermore, patients are not proactively screened for SARS-CoV-2 but rather tested when symptomatic or for preventative measures such as before an elective procedure. As the reason for testing remains elusive, our patient population might be biased toward symptomatic COVID-19 patients and might miss a substantial proportion of asymptomatic patients. Therefore, our results are primarily reflective of the risk of patients acquiring symptomatic SARS-CoV-2 infection, that is, COVID-19 disease. Third, there is the possibility of medication exposure misclassification, in particular with corticosteroids. Patients prescribed a given medication may have later discontinued the medication during the course of follow-up, either under the direction of a physician or by personal choice during the pandemic. It is difficult to capture such changes, however, this bias would likely have the impact of minimising differences between groups, and therefore, the results observed in this study may be conservative. Furthermore, our results regarding steroid use are consistent with prior literature regarding the impact on COVID-19 infection, lending validity to our findings.14 Fourth, our measure of medication exposure was based on prescriptions for oral and self-injected medications that were dispensed and administration of infused medications. However, we cannot be certain that all patients continued to take their prescribed medications during the pandemic. As such, our results should be interpreted with knowledge of this limitation. Fifth, although we were unable to measure disease activity, we did adjust for recent steroid use, a surrogate for active disease. Were the results of the analyses appreciably biased by active disease, we would have expected to see positive associations with most of the medication classes relative to mesalazine alone, not just vedolizumab. Thus, it seems unlikely that failure to adjust for disease activity would explain the observed association between vedolizumab exposure and risk of infection. Finally, in the secondary analysis of severe COVID-19 infection, there may be centre-level variation in hospitalisation criteria, which could potentially bias estimates or make them less generalisable to other settings where hospitalisation criteria differ. However, in the aggregate of the 170-centre network of VAHS sites, which reflect both community-based and academic-affiliated centres, we would expect the impact of this bias to be minimal.
In conclusion, using a large nationwide VA database comprising of predominantly elderly male population, we found that vedolizumab and corticosteroids use for IBD were associated with an increased risk of SARS-CoV-2 infection. To our knowledge, this is the first study to link vedolizumab with acquisition of SARS-CoV-2 infection, even though it was not associated with clinically severe COVID-19 infection resulting in hospitalisation or death. In our study, mesalazine was neither associated with SARS-CoV-2 infection nor with worse outcomes. Furthermore, our findings support the prevailing opinion that physicians should be cautious in using corticosteroids for IBD management during the SARS-CoV-2 pandemic.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
NK and NM are joint first authors.
WR and JDL are joint senior authors.
Correction notice This article has been corrected since it published Online First. The joint first author and joint senior author statements have been added.
Contributors NK has participated in funding acquisition, study supervision, study concept and design, acquisition of data, analysis and interpretation of data, drafting of the manuscript, and critical revision of the manuscript for important intellectual content. NM data has participated in study concept and design, acquisition of data, statistical analysis, analysis and interpretation of data and drafting of the manuscript. CT has participated in acquisition of data and drafting of the manuscript. WR has participated in study concept and design, analysis and interpretation of data, drafting of the manuscript and critical revision of the manuscript for important intellectual content. JDL has participated in study concept and design, statistical analysis, analysis and interpretation of data, drafting of the manuscript and critical revision of the manuscript for important intellectual content.
Funding This study was supported by an unrestricted research grant from Pfizer Pharmaceuticals.
Disclaimer Pfizer has no role in the study concept and design, acquisition of data, analysis of the data, interpretation of the data, and preparation of the manuscript.
Competing interests NK has received an unrestricted research grant from Pfizer, Luitpold and Takeda Pharmaceuticals as well as Samsung BioEpis. NM and CT have nothing to disclose regarding conflicts of interest. WR has served (1) as a speaker for Abbott Laboratories, Abbvie, Aesca, Aptalis, Astellas, Centocor, Celltrion, Danone Austria, Elan, Falk Pharma, Ferring, Immundiagnostik, Mitsubishi Tanabe Pharma Corporation, MSD, Otsuka, PDL, Pharmacosmos, PLS Education, Schering-Plough, Shire, Takeda, Therakos, Vifor, Yakult, (2) as a consultant for Abbott Laboratories, Abbvie, Aesca, Algernon, Amgen, AM Pharma, AMT, AOP Orphan, Arena Pharmaceuticals, Astellas, Astra Zeneca, Avaxia, Roland Berger, Bioclinica, Biogen IDEC, Boehringer-Ingelheim, Bristol-Myers Squibb, Cellerix, Chemocentryx, Celgene, Centocor, Celltrion, Covance, Danone Austria, DSM, Elan, Eli Lilly, Ernest & Young, Falk Pharma, Ferring, Galapagos, Genentech, Gilead, Grünenthal, ICON, Index Pharma, Inova, Intrinsic Imaging, Janssen, Johnson & Johnson, Kyowa Hakko Kirin Pharma, Lipid Therapeutics, LivaNova, Mallinckrodt, Medahead, MedImmune, Millenium, Mitsubishi Tanabe Pharma Corporation, MSD, Nash Pharmaceuticals, Nestle, Nippon Kayaku, Novartis, Ocera, OMass, Otsuka, Parexel, PDL, Periconsulting, Pharmacosmos, Philip Morris Institute, Pfizer, Procter & Gamble, Prometheus, Protagonist, Provention, Quell Tx, Robarts Clinical Trial, Sandoz, Schering-Plough, Second Genome, Seres Therapeutics, Setpointmedical, Sigmoid, Sublimity, Takeda, Therakos, Theravance, Tigenix, UCB, Vifor, Zealand, Zyngenia, and 4SC, (3) as an advisory board member for Abbott Laboratories, Abbvie, Aesca, Amgen, AM Pharma, Astellas, Astra Zeneca, Avaxia, Biogen IDEC, Boehringer-Ingelheim, Bristol-Myers Squibb, Cellerix, Chemocentryx, Celgene, Centocor, Celltrion, Danone Austria, DSM, Elan, Ferring, Galapagos, Genentech, Grünenthal, Inova, Janssen, Johnson & Johnson, Kyowa Hakko Kirin Pharma, Lipid Therapeutics, MedImmune, Millenium, Mitsubishi Tanabe Pharma Corporation, MSD, Nestle, Novartis, Ocera, Otsuka, PDL, Pharmacosmos, Pfizer, Procter & Gamble, Prometheus, Sandoz, Schering-Plough, Second Genome, Setpointmedical, Takeda, Therakos, Tigenix, UCB, Zealand, Zyngenia and 4SC, and (4) has received research funding from Abbott Laboratories, Abbvie, Aesca, Centocor, Falk Pharma, Immundiagnostik, MSD'. JDL has served as a consultant for Merck, AbbVie, Lilly, Janssen, Johnson & Johnson Consumer, and Takeda; has served on Data Safety Monitoring Boards for Pfizer, Gilead, and UCB; and has received research support from Takeda and Nestle Health Science.
Patient consent for publication Not required.
Ethics approval Data were collected using pre-existing electronic patient records in the VISTA CAPRI database post an Institutional Review Board (IRB) approval from the Corporal Michael J Crescenz VA Medical Center, Philadelphia, Pennsylvania, USA.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available. A retrospective cohort study. Deidentified data may be available from the corresponding author on request by the journal but identified data will not be available due to HIPAA rules.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.