Article Text

Abstract
Histological remission is evolving as an important treatment target in UC. We aimed to develop a simple histological index, aligned to endoscopy, correlated with clinical outcomes, and suited to apply to an artificial intelligence (AI) system to evaluate inflammatory activity.
Methods Using a set of 614 biopsies from 307 patients with UC enrolled into a prospective multicentre study, we developed the Paddington International virtual ChromoendoScopy ScOre (PICaSSO) Histologic Remission Index (PHRI). Agreement with multiple other histological indices and validation for inter-reader reproducibility were assessed. Finally, to implement PHRI into a computer-aided diagnosis system, we trained and tested a novel deep learning strategy based on a CNN architecture to detect neutrophils, calculate PHRI and identify active from quiescent UC using a subset of 138 biopsies.
Results PHRI is strongly correlated with endoscopic scores (Mayo Endoscopic Score and UC Endoscopic Index of Severity and PICaSSO) and with clinical outcomes (hospitalisation, colectomy and initiation or changes in medical therapy due to UC flare-up). A PHRI score of 1 could accurately stratify patients’ risk of adverse outcomes (hospitalisation, colectomy and treatment optimisation due to flare-up) within 12 months. Our inter-reader agreement was high (intraclass correlation 0.84). Our preliminary AI algorithm differentiated active from quiescent UC with 78% sensitivity, 91.7% specificity and 86% accuracy.
Conclusions PHRI is a simple histological index in UC, and it exhibits the highest correlation with endoscopic activity and clinical outcomes. A PHRI-based AI system was accurate in predicting histological remission.
- histopathology
- ulcerative colitis
- inflammatory bowel disease
- computerised image analysis
Data availability statement
Data are available on reasonable request. Computer algorithm code available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
We developed a new simple histological index for UC, Paddington International virtual ChromoendoScopy ScOre Histogic Remission Index (PHRI), which could be successfully implemented into an artificial intelligence (AI) model to detect histological remission.
What is already known on this subject?
Histological activity in UC is associated with poor outcomes and histological remission has been proposed as a treatment target in UC.
Multiple histological indices have been developed to define disease activity, however they have not been widely adopted in clinical practice due to their complexity.
Machine learning models are powerful tools that can complement and support pathologists in their histopathological evaluation.
What are the new findings?
PHRI is a new score based simply on the presence or absence of neutrophils (yes/no) and it provides excellent diagnostic accuracy, the strongest correlation to endoscopic activity among several histological scores, minimal inter-rater variability and excellent prediction of long-term clinical outcome.
An AI algorithm based on PHRI was able to accurately determine histological remission.
Significance of this study
How might it impact on clinical practice in the foreseeable future?
PHRI can help standardise histological assessment of UC in a most practical and easy way.
A machine learning model based on PHRI can further facilitate the histological reading and improve diagnostic performance.
Introduction
Histological assessment plays a critical role in determining inflammatory activity and monitoring treatment response in UC. Histological remission (HR) (also referred as histological healing) is an emerging treatment target and is an important outcome in UC clinical trials due to its association with favourable outcomes.1–10 However, challenges remain on how to incorporate histology into clinical practice mainly due to: (1) the lack of a universal definition of HR to guide pathologists and (2) the lack of a sensitive, easily applicable histological score/index. Ideally, this index would be: (a) informative of and correlated with endoscopic assessment of disease activity, (b) representative of recovery/healing status of damaged mucosa and (c) predictive of disease outcomes.
The histopathological characteristics of UC are those of a chronic active colitis with a relapsing and remitting course, and consist of three fundamental components: (1) active inflammation (‘activity’), which is the neutrophil infiltration in cryptal epithelium as well as in the lamina propria; (2) chronic inflammation, characterised by expansion of mononuclear cell (lymphocyte and plasma cell) infiltrates in the lamina propria, often accompanied by basal plasmacytosis and eosinophilia and (3) cryptal architecture/structure distortion (‘chronicity’), characterised by irregularity and variation of crypts in size, shape, orientation and intercryptal distance, which is the result of mixed repetitive injury and regeneration of crypts.
Over the past decades, >30 histological scores have been developed, although their adoption in clinical practice remains modest.11 12 Similarly, different definitions and criteria of HR have been proposed, ranging from ‘elimination of mucosal ulceration/erosion’ to ‘complete histological normalisation’.1 3 13–18 Almost all investigators now agree that the absence of neutrophilic infiltration (‘neutrophil-free’ mucosa) is the key to a HR definition due to its association with favourable clinical outcomes.2 4 5 19–22 Indeed, two independent international expert panels recently recommended to define HR as the absence of neutrophil infiltration (ie, elimination of histological activity).22 23
With the advent of digital pathology, artificial intelligence (AI) algorithms are increasingly employed into histopathological evaluation and diagnosis, as seen in many imaging-focused fields in medicine. For example, it is being widely introduced in oncopathology using convolutional neural network (CNN)-based learning.24 But, thus far, to the best of our knowledge, no computer-aided diagnosis (CAD) system has been developed to perform histological scoring and assess HR in UC. Part of the reason is that the complexity and mixed subjectivity of the existing histological scores makes it difficult to build and train deep learning algorithm, supervised and unsupervised.
Recently, we conducted a prospective international multicentre study to develop the Paddington International virtual ChromoendoScopy ScOre (PICaSSO) endoscopic score,25–27 a new tool for assessing endoscopic activity and remission in patients with UC by using high-definition virtual electronic chromoendoscopy (HD-VCE). The PICaSSO endoscopic score had better correlation than Mayo Endoscopic Score (MES) and UC Endoscopic Index of Severity (UCEIS) with multiple histological scores.27 The current study is distinct, and a step further, from all our previous published studies on PICaSSO endoscopic score, as it focuses on creating a new UC histological score that can be used quickly and easily by histopathologists in clinical practice, as well as in trials, and can be incorporated into an AI algorithm. Using the PICaSSO project as a platform, in the present study we meticulously analysed the mucosal biopsies taken from the same colonic areas assessed endoscopically, with a focus on identifying the specific histopathological component(s) associated with histological-endoscopic correlation and with the risk of adverse clinical outcomes. Ultimately, we aimed to develop a simplified and novel histological score that could accurately reflect microscopic mucosal inflammation and healing, predict clinical outcome, respond to therapy and be readily implementable into a machine learning algorithm and thus easily adopted into clinical practice and trials. Creating a simplified histological score, PHRI, that is an objective histological instrument was the main aim, as current use of histological scores in clinical practice is limited. The primary aim of PHRI was to create a simple ‘neutrophil-only’ histological evaluation that predicted specified clinical outcomes. An additional purpose was that an ideal histological index should go beyond the limit of endoscopic evaluation.
Patients and methods
Study population, endoscopic evaluation and clinical follow-up
A total of 307 patients with UC were prospectively enrolled from 11 centres in Europe and North America into the international multicentre PICaSSO study. The protocol for endoscopic and histological evaluation have been described in details in a previous publication.27 Briefly, each patient underwent white light HD colonoscopy to determine MES and UCEIS,28 29 followed by VCE (iSCAN, Pentax, Japan) to determine PICaSSO score, which comprises mucosal and vascular subscores (PICaSSO Mucosal Score (PMS) and PICaSSO Vascular Score (PVS)).25 27 In the same areas of rectum and sigmoid assessed and video recorded on endoscopy, at least two targeted mucosal biopsies were taken resulting in a total of 614 biopsies for histopathological analysis. Targeted biopsies were taken from the most inflamed area or showing the most representative features of endoscopic remission (ER) determined by PICaSSO.26 All patients were then followed up for at least 12 months with regular clinic visits to document the following prespecified adverse clinical outcomes: (1) hospitalisation as a result of UC relapse, (2) colectomy and (3) initiation or changes in medical therapy for UC flare-up including steroids, immunosuppressants and biologics (after excluding adverse effects, immunogenicity or low drug levels).
Phase I: deep histological analyses and histological-endoscopic-clinical outcome correlations
The H&E-stained glass slides of colorectal biopsies were scanned at 40× (0.25 μm per pixel) using Aperio Digital Pathology Scanning system (Leica Biosystem, Illinois, USA). The HD digitised slides were centrally hosted and read by a group of 6 GI pathologists (XG, MV, VV, DZ, GdH, ESR) experienced in IBD who were blinded to the endoscopic data. For each biopsy from each segment, the worst features were scored applying five different histological scoring schemes—Geboes Score (GS),30 Robarts Histological Index (RHI),31 Nancy Histological Index (NHI),32 extent, chronicity, activity and plus (ECAP) score33 34 and Villanacci Simplified Score (VSS).35 The average values of each score and subscore for both rectum and sigmoid were also separately analysed.
The endoscopic-histological correlation was analysed in multiple steps in order to identify the histopathological features/components that specifically corresponded to the different endoscopic features/patterns of disease activity and remission, as well as predicted the risk of specified clinical outcomes at follow-up.
Phase II: development and assessment of PICaSSO Histologic Remission Index
Based on a solid conclusion from our multistep and comprehensive histological-endoscopic-clinical outcome correlation analyses in the phase I study and following a modified Delphi roundtable discussion between the expert pathologists, the presence of neutrophil infiltration was identified as the key element in UC histopathology that determines the disease activity, mucosal healing and clinical outcome. Subsequently, a novel simplified histological scoring scheme, PICaSSO Histologic Remission Index (PHRI), was proposed, as detailed in table 1. This index takes into account solely the neutrophil infiltration in both epithelium and lamina propria, as illustrated in online supplemental figure 1. Ulcer and erosion were not included because the histological features of ulcers and/or erosions may not always been apparent in the biopsies due to sampling variation. We standardised particularly the criteria of ‘cryptitis’ (any number of neutrophils infiltrating the epithelium of any number of crypt/gland) and ‘crypt abscess’ (cryptitis with any number of neutrophils overflowing into cryptal lumina and any degree of cryptal epithelial cell injury), given that a clear and standardised histological criteria of cryptitis and crypt abscess are still lacking. The pathologists also completed a standardised training module representative of several histological pictures displaying all the histological features before scoring the slides.
Supplemental material
PICaSSO Histologic Remission Index (PHRI)
The new PHRI was then used to re-analyse the aforementioned histological-endoscopic correlations, to compare it with the other five histological indices, and its prediction of clinical outcome at 12 months follow-up. We also explored the additional prognostic benefit of PHRI in further stratifying the risk of disease relapse in patients who were already in ER defined by MES of 0. The PHRI scores of rectum and sigmoid were considered individually as well as combined in the total score (PHRI_total, ie, the sum of PHRI scores of both rectum and sigmoid) or the maximum score (PHRI_max, ie, the higher score between rectum and sigmoid). The latter, PHRI_max, was chosen. If not otherwise specified, the term PHRI refers to the highest score in the examined areas, PHRI_max.
Phase III: validation of PHRI
To validate PHRI, the same pathologists assessed 50 digital slides (about half quiescent and half active UC) and scored PHRI and the other five selected indexes. The validation cases were randomly selected and relabelled by a non-pathologist investigator from the same study group. The pathologists were blinded to clinical and endoscopic information and performed the histological scoring independently.
Phase IV: development of AI algorithm
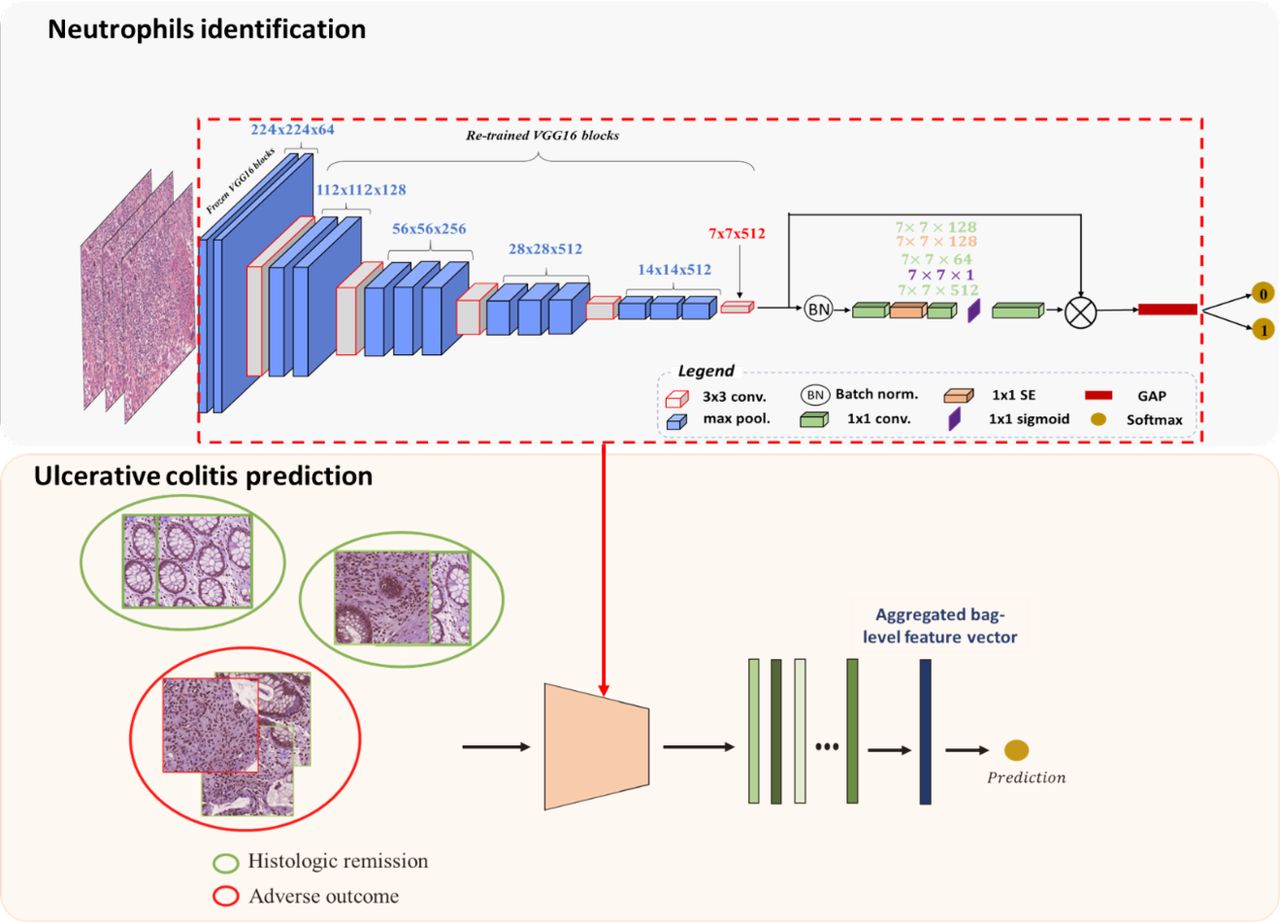
In this exploratory study we included 138 biopsies, randomly selected from the study collection, that were representative of different grades of inflammation from the 614 collected in the whole study. We developed a CNN classifier to detect the neutrophils in whole slide images (WSIs) and classify them into either histological remission or non-remission based on the presence of neutrophils. The detailed design of the CNN is reported in the AI online supplemental appendix. Briefly, a first model identified patches (areas of the WSI) containing neutrophils, while a second model, using a multiple instance learning approach, combined the features of each patch in the slide into a final dichotomous result (presence or absence of active disease) following the PHRI (figure 1).
Supplemental material

Framework of the proposed deep learning approach. The framework is composed of two models with different but related tasks. The first model predicts patches with neutrophils using a pretrained architecture in histological images. The second model uses the feature extractor and the feature refinement used by the first model to the prediction of UC at the patient level. GAP, global average pooling; SE, squeeze and excitation (feature refinement).
Statistics
Statistical Software R (R Core Team, https://www.R-project.org/) was used. The strength of the correlation of continuous and categorical variables was measured with Spearman’s (ρ) correlation coefficient. Coefficients of 0.8–1.0 were considered as ‘very strong’, 0.6–0.79 as ‘strong’, 0.4–0.59 as ‘moderate’ and 0.2–0.39 as ‘weak’. Spearman’s correlations were compared by drawing 100 bootstrap samples for each pair of variables and computing the corresponding quantiles. Wilcoxon and Fisher’s exact tests were used to determine the differences between continuous and binary distributions, respectively. For area under the receiver operating characteristic curve analysis, we used R-package pROC (https://CRAN.R-project.org/package=pROC). Predictive modelling was performed by R-package CARRoT (https://CRAN.R-project.org/package=CARRoT). Details are reported in the statistical online supplemental appendix.
The Cox proportional hazard model was used to calculate the probability of survival without specified clinical outcomes for different cut-offs of PHRI. The difference between groups of patients was assessed by HR test and survival analysis implemented via R-package survival (https://CRAN.R-project.org/package=survival).
To assess the inter-rater agreement of the histological scorings, we used one-way intraclass correlation (ICC) coefficient by means of R package irr (http://cran.r-project.org/package=irr). In order to test the hypothesis of the ICC being >0.5 against the alternative, we needed a minimum of 40 histology images to reach the power of 0.8 with a type I error of 0.05.36 According to Landis and Koch benchmarks,37 ICC of <0.2, 0.2 to 0.4, >0.4 to ≤0.6, >0.6 to 0.8 and >0.8 was considered ‘poor’, ‘fair’, ‘moderate’, ‘good’, ‘substantial’ and ‘almost perfect’, respectively. Results of all statistical tests were considered significant at p<0.05. Statistical power was computed in the PICaSSO endoscopic and histological study recently published27 based on correlation of PICaSSO endoscopic score and histological scores compared with standard MES and also on specified clinical outcome rates and a sample size of 302 was determined.
The diagnostic performance of the AI CAD for the detection of active UC was reported as sensitivity (SE), specificity (SP), positive predictive value (PPV), negative predictive value (NPV) and accuracy (ACC).
Results
Six hundred fourteen biopsies from 307 patients with UC were analysed. One hundred sixty-eight (54.7%) patients were in ER as defined by MES 0, while the others had endoscopically active disease at the time of study. None of the patients was on topical therapy or had Montreal E1 disease. Two hundred seventy (88%) patients completed follow-up for 12 months. The detailed demographic data of the study subjects are shown in table 2.
Demographic data of study subjects
Phase I: neutrophils as the key determinant in histological-endoscopic-clinical correlation
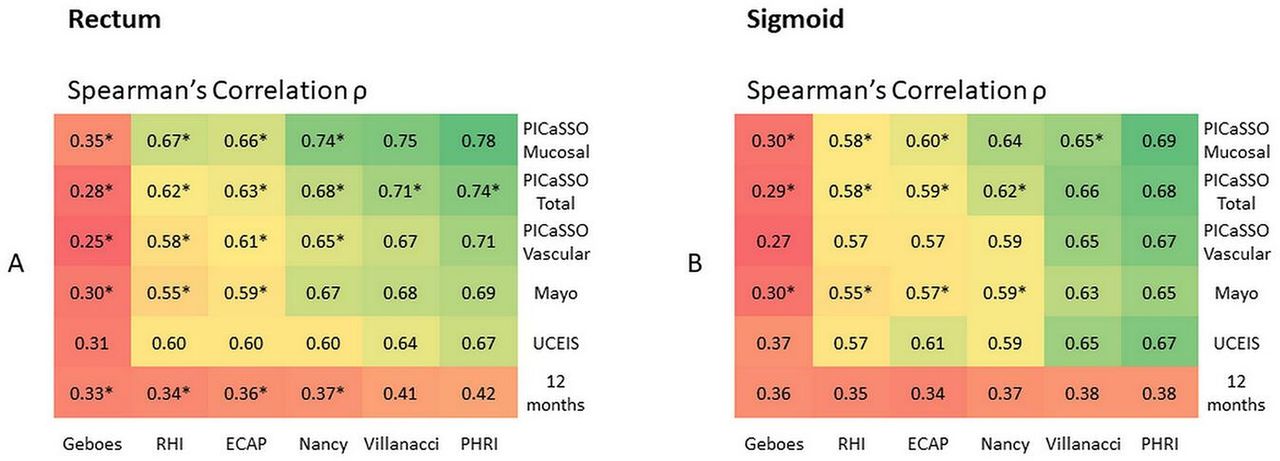
All five histological indices (VSS, RHI, NHI, GS and ECAP) correlated strongly with all of the endoscopic scores in the same regions of bowel (rectum and sigmoid colon) (Spearman’s ρ=0.55–0.78), as illustrated by the heatmaps (figure 2). All histological indices also showed a weak to moderate correlation with the prespecified adverse clinical outcomes at 12 months (ρ=0.34–0.42) (figure 2).
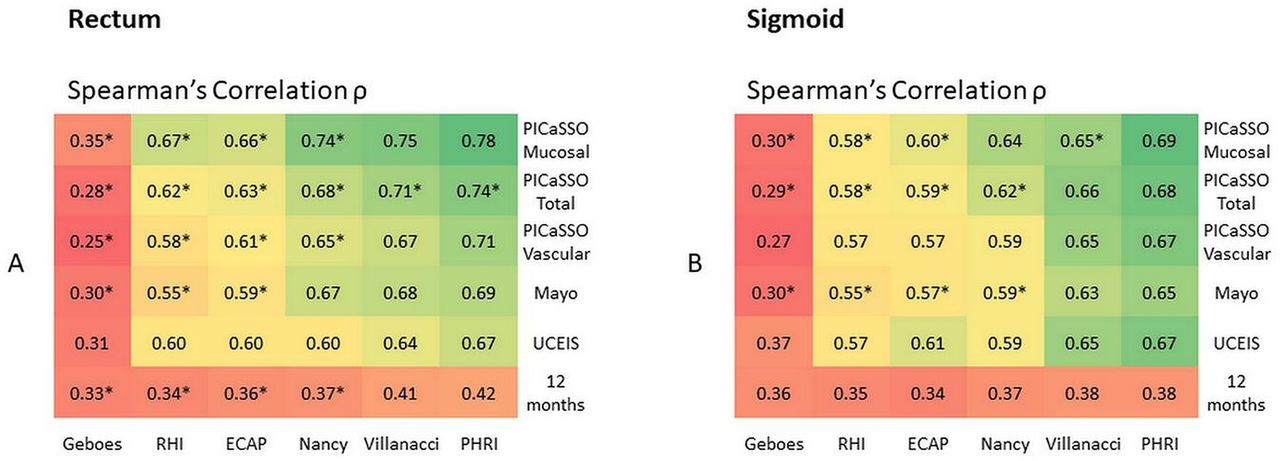
PICaSSO Histologic Remission Index (PHRI) correlation. Histological-endoscopic correlation demonstrated by heatmaps showing Spearman’s correlation coefficients between different histological and endoscopic scores in the rectum (A) and in the sigmoid (B) and between the endoscopic-histological scores and the specified clinical outcomes at 12 months (0.8–1.0: very strong correlation, 0.6–0.79: strong, 0.40–0.59: moderate, 0.2–0.39: weak) (*p<0.05 as compared with PHRI with regard to the correlation strength in the same category of correlation analysis). ECAP, extent, chronicity, activity and plus; PHRI, PICaSSO Histologic Remission Index; PICaSSO, Paddington International virtual ChromoendoScopy ScOre; RHI, Robarts Histological Index; UCEIS, UC Endoscopic Index of Severity.
Looking further into the correlations between the various histopathological components (online supplemental table 1) and endoscopic scores (represented by the mucosal and vascular subscores of PICaSSO score), the neutrophil infiltration in the lamina propria and in epithelium, especially that in lamina propria and the combination of both, generally showed the strongest correlation (ρ=0.60–0.76), as compared with the other histological features that also showed correlation to some degree (moderate to strong, ρ=0.43–0.64) (p<0.05) (figure 3). Similarly, neutrophil infiltration also showed a stronger correlation, although overall weak/moderate (ρ=0.40–0.45), with clinical outcomes at 12 months compared with other histological features (ρ=0.24–0.37) (p<0.05) (figure 3).
Supplemental material

Correlation of histopathological components. Heatmaps showing the correlations of histopathological components with PICaSSO endoscopic subscores and with the rates of 12-month adverse outcomes in all patients. Biopsies from the rectum (A) and the sigmoid (B) (0.8–1.0: very strong correlation, 0.6–0.79: strong, 0.40–0.59: moderate, 0.2–0.39: weak) (*p<0.05 as compared with neutrophils in the lamina propria, !p<0.05 as compared with and total neutrophils infiltration and #p<0.05 as compared with neutrophils in epithelium, with regard to the correlation strength in the same category of correlation analysis) (neutrophils total: neutrophil infiltration in both lamina propria and epithelium). PICaSSO, Paddington International virtual ChromoendoScopy ScOre.
Phase II: PHRI for histological-endoscopic and clinical outcome correlations
PHRI correlated best with endoscopic disease activity
PHRI correlated strongly with the endoscopic scores, and the strength of its correlation was the best among all the histological indices (p<0.05) (figure 2).
Correlation of PHRI with specified clinical outcomes and relapse risk
For the entire cohort, the PHRI showed a similar moderate correlation with the specified adverse clinical outcomes at 12 months (ρ values around 0.4). Additionally, the average PHRI scores were significantly higher in those who had specified adverse clinical outcomes at 12 months than in those with no events (online supplemental table 2, online supplemental figure 4).
Supplemental material
Supplemental material
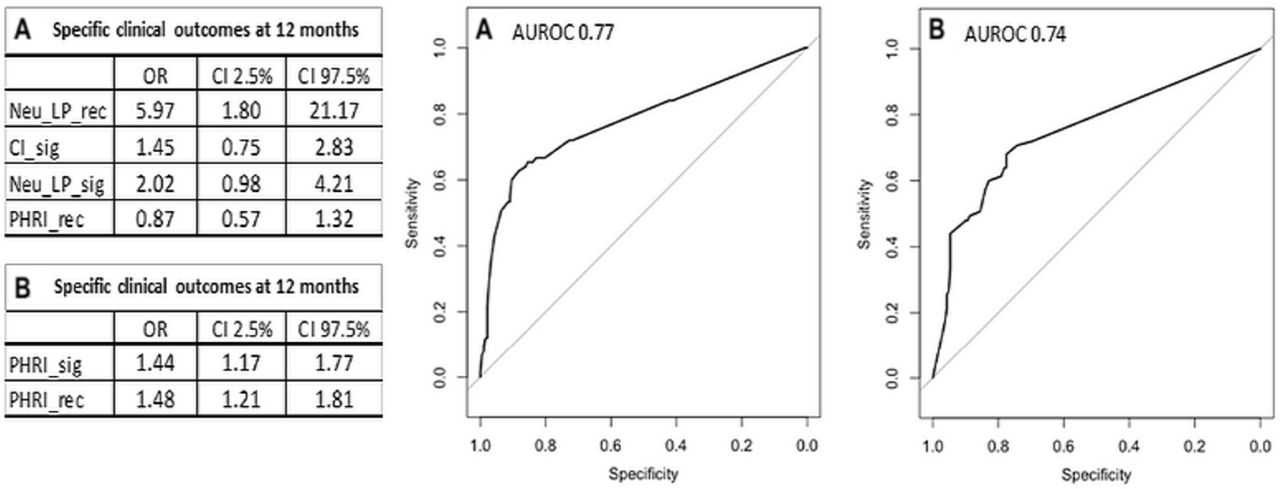
Furthermore, we performed a multivariable logistic regressions to explore whether other histological features (chronic inflammation, basal plasmacytosis and eosinophilia) could improve PHRI prediction of specified clinical outcomes. We found that the addition of none of these histological features further improved PHRI prognostic outcome ability (figure 4).

Receiver operating characteristic (ROC) curve and Paddington International virtual ChromoendoScopy ScOre Histogic Remission Index (PHRI) thresholds to predict specified clinical outcomes and histological remission (HR). AUROC, area under the receiver operating characteristic curve; CI, chronic inflammation; Neu-LP, neutrophil infiltration in lamina propria; Neu-Epi, neutrophil infiltration in epithelium; PHRI_rec, PHRI scores of rectum; PHRI_sig, PHRI scores of sigmoid.
Patients with PHRI >0 compared with those with PHRI=0 had significantly more negative clinical events (outcomes) at 12 months (48.65% (54/111) vs 13.91% (21/151), p<0.00001), as shown in online supplemental figure 4C. In addition, analysis by receiver operating characteristic (ROC) curve, as shown in online supplemental table 3A, the best cut-off values of PHRI for predicting the specified clinical outcomes at 12 months in the entire cohort was 1 (≤1 vs >1).
Supplemental material
Cox proportional hazards curves of PHRI in predicting specified clinical outcome
We then further analysed with the Cox proportional hazards curves by using value 0 or 1 as the cut-off score of PHRI (or individual PHRI of rectum or sigmoid), the patients’ event rates of specified clinical outcomes during 12 months follow-up were significantly stratified, as shown in figure 5A and B. The predictive power of PHRI in any form were almost the same.

Cox proportional hazard curves of Paddington International virtual ChromoendoScopy ScOre Histogic Remission Index (PHRI) in stratifying risk of specified clinical outcomes up to 12 months of follow-up. A and B for all patients, C for Mayo Endoscopic Score 0 patients. (A) Using PHRI=0 (blue) vs >0 (red). (B) Using PHRI ≤1 (blue) vs >1 (red). (C) 12 months of follow-up, using PHRI=0 (blue) vs >0 (red).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Original images (first column), annotation of the pathologist (second column) and class activation maps (CAMs) (third column). Note that in this case, the first row corresponds to the lamina propria while the second row corresponds to the surface of the epithelium.
Subgroup analysis of patients with only endoscopic remission
When we singled out the patients who were in ER as defined by MES 0, the histological-endoscopic-clinical outcome correlations became weak in all aspects. In the phase I of the study, for this particular subpopulation of patients, of whom only a few had residual mild neutrophil infiltration in colorectal biopsies (5.7% with neutrophils in lamina propria and 5.4% in epithelium), the correlations between histological and endoscopic scores (represented by PICaSSO mucosal score and PICaSSO vascular score) (ρ<0.30) and between histological scores and specified clinical outcome (indicative of relapse in this particular patient population) both became weak or near zero (ρ=0–0.12) (online supplemental figure 2). Nevertheless, neutrophil infiltration was the single histological feature that remained correlated, although weakly (slightly over 0.1) (online supplemental figure 3).
Supplemental material
Supplemental material
In the phase II of the study, in patients in ER (MES 0), of which only 10.9% had PHRI >0 (presence of neutrophilic infiltration) and 89.1% had PHRI of 0 (no neutrophilic infiltration), the correlation between PHRI and endoscopic scores also turned to be much weaker (ρ=0.24–0.36) (online supplemental table 4). However, PHRI still appeared generally superior to most of the other histological indices (p<0.05), as represented by their correlation with PICaSSO score and its mucosal and vascular subscores (online supplemental figure 2). Moreover, the correlation between PHRI scores and prespecified clinical outcomes was also very weak, but still performed better than the other histological scores (p<0.05) (online supplemental figure 2 and online supplemental table 4). Consistent with this, patients with PHRI >0 seemed to have a higher disease relapse rate at 12 months, as compared with those with PHRI 0 (11.76% (2/17) vs 9.3% (12/129)), although the differences did not reach statistical significance (p>0.05) (online supplemental figure 4D). Lastly, the best cut-off value of PHRI for predicting the relapse at 12 months in patients in ER seemed to be 1 (≤1 vs >1), although further analysis with Cox proportional hazards curves failed to satisfactorily stratify the patients’ relapse risk (figure 5C).
Supplemental material
Phase III: validity and reliability of PHRI
The inter-rater agreement among pathologists on all of the histological scores was excellent, as reflected by ICCs: RHI 0.77 (95% CI 0.69 to 0.85), NHI 0.85 (95% CI 0.79 to 0.90), GS 0.82 (95% CI 0.75 to 0.88), ECAP 0.87 (95% CI 0.82 to 0.92), VSS 0.77 (95% CI 0.71 to 0.86) and PHRI 0.84 (95% CI 0.78 to 0.90). The differences between the ICCs of each index were not statistically significant. Overall, interobserver agreement for PHRI was almost perfect, although not necessarily significantly superior to the other histological indices. The breakdown of ICC on each of the histological components of different histological indices were also analysed. For any given histological score, we had the best agreement on assessment for the neutrophil-related parameters, as shown in online supplemental table 5.
Supplemental material
Phase IV: convolutional neural network classifier able to detect neutrophils
We divided our cohort in two sets, training and testing, with similar patient characteristics to avoid overfitting our system and ensuring its generalisability. Seventy per cent of the biopsies were used to train the model and 30% to test it. To train the proposed models and optimise the hyperparameters involved, 15% of the training set was used as validation. In the testing set, our CAD to detect neutrophils had SE 0.71, SP 0.95, PPV 0.85, NPV 0.89 and accuracy 0.88, these results were in line with those of the validation cohort (see table 3). Figure 6 shows the class activation maps to highlight the regions of interest at patch-level in which the proposed model focused to predict the samples. The highlighted regions match with the areas containing neutrophils. For the histological remission prediction, the diagnostic performance, expressed as the same characteristics, was 0.78, 0.92, 0.88, 0.85 and 0.86, respectively (see table 3).
Classification results reached during the validation and the test stage with the neutrophil identification model and the activity of UC prediction
Discussion
We developed a novel and simpler HR index for UC, the PHRI, that correlates well with endoscopic disease activity and with clinical outcomes and it can be easily implemented into a CNN model. The development process of this histological index differs from that of existing scores. PHRI was the result of a joint collaboration between pathologists and endoscopists aiming to develop a histological score aligned to the endoscopic score and going beyond endoscopic evaluation.27 Our work has several strengths. First, the histological study was part of a large international multicentre prospective study with the precise focus on endoscopic-histological-clinical correlation. We included a large number of matching biopsies taken immediately after and exactly from the same areas where endoscopic assessment was performed, rather than limiting the comparison to a patient-level. Second, instead of including multiple diagnostic features as in other histological indices, we limited the PHRI to one parameter only, neutrophil infiltration (active inflammation), the single factor identified by multiple comparative analyses, to be most relevant to both endoscopic features and clinical outcomes. Our independent finding echoes the study by Pai et al 21 and is consistent with a gathering consensus on the importance of neutrophils in the definition of disease activity and HR.
The most notable advantage of PHRI is its simplicity. PHRI requires only identifying the presence or absence of infiltrating neutrophils within the lamina propria and glandular epithelium, in a straightforward dichotomous way of ‘yes or no’ (present or absent). It also avoids the usual activity grading (eg, mild, moderate and severe) by arbitrary visual scale or estimate of percentage values, which is somewhat subjective. As found by other investigators and shown by our own inter-rater agreement data, the assessment for neutrophils has always been the most reproducible characteristic.38 39 Presence of ulceration/erosion, often included in other indexes, was eliminated from PHRI as we considered it a potential source of variability with little contribution to the score’s accuracy. Indeed erosions/ulcers might not be visible on biopsy histology,22 the distinction between the two is not always possible and, more importantly, patients with erosions/ulcers inevitably have more extensive neutrophilic infiltration anyway. Adopting this simplified ‘neutrophil-only’ approach, we expect that the histological readings would be maximally objective and reproducible. The addition of other histological components that also had some degree of impact on endoscopic features and/or clinical outcomes did not add significant benefit from a practical point of view and would have instead complicated the development of the AI algorithm. We feel that compared with the other currently available histological scores, PHRI is the easiest to apply in daily practice as a universal histological indicator and quantitative measurement (grading tool) of disease activity in UC. table 1
Another advantage is that PHRI makes it easier to perform histological scoring on multiple biopsies from different segments of colon in patients with extensive colitis, to achieve an entire assessment and generate a global (total, maximum, or average) score per colon. This approach would appreciate the globality and increase the overall accuracy of the histological assessment.
In our analysis, we found that the PHRI scores of rectum and sigmoid were similar in terms of their correlation with endoscopy and prediction of clinical outcome. In addition, the highest score and the total score of PHRI (PHRI_max and PHRI_total) had the same value of application and significance. Therefore, it is our preference to set the global score as the highest/worst score among all biopsies (PHRI_max) or simply the score of the histologically worst biopsy only, considering that the total number of biopsies being taken and the extent of disease vary in different patients and different clinicians. Finally, the successful development of a computer-aided UC histological diagnosis and scoring system based on PHRI, to the best of our knowledge the first in the field of IBD, supports the notion that a simplified score is readily implementable into an AI model. This may complement rapidly advancing development of AI systems for endoscopic scoring of UC, including prediction of histology from endoscopic scores by a number of authors including us.40–48 Although preliminary, these findings are particularly promising in light of the rapid integration of CAD systems into clinical practice. The potential benefits of this change are extraordinary, but their discussion exceeds the objectives of our study.
Admittedly, our work has a few limitations. First, our patients’ follow-up protocol did not include the endoscopic and histological reassessments at 12 months (not standard of care in all centres), and second it only lasted 12 months, whereas some clinical outcomes might be observed even after 36 months.49 Third, we did not follow-up patients using patient-reported outcomes similar to other studies1 15 as symptoms do not relate well to histology or endoscopy. Fourth, we have not yet tested sufficiently the global score of PHRI throughout different regions of the entire colon in patients with pan-colitis, although we did include two sites (rectum and sigmoid) in the present study which recruited a diverse cohort of patients. We recruited patients as part of standard of care and this included flexible sigmoidoscopy or colonoscopy. External validation in large cohort in the context of specific clinical trials is necessary and will be conducted as the next step. Lastly, some histological interpretations were challenging and required further discussion (details in histological appendix). An unsolved issue remains the suboptimal performance of all the current histological indices for patients who have reached ER where residual neutrophils are lacking or scarce. In this particular patient population histological indices, including our new PHRI, lose correlation with either endoscopic scores or with relapse rate. The predictive power of PHRI in assessing the relapse risk in these patients was also limited, although a biopsy finding of PHRI >0 in patients who are otherwise in ER would still be of interest. By using a different histological scoring, Narula et al also failed to show the significance of the impact of histological activity on the relapse in this subpopulation of patients.50 The reasons for this shortfall may be several. First, the small number of cases with histological but not endoscopic activity (only 10% had PHRI >0 in our patients) underpowered the analysis. Second, the heterogeneous distribution of residual inflammation in treated UC might have generated an underestimation of disease activity. Third, the recurrence of UC is not simply arising from the minimal residual inflammation but is the result of the reactivation of dysregulated mucosal immunological mechanisms.
Nonetheless, in our opinion, as compared with any of the other histological indices, PHRI is the simplest one, while it is also most objective and sensitive. Since a pathologist needs only to identify neutrophils, which is a part of routine in reading biopsy slides as clinical histopathological evaluation, one can have the PHRI score immediately without making additional effort and spending extra time. Thus, the PHRI score can also be easily included into the pathology reports, which would be something that infrequently happen at present. Therefore, we believe that PHRI can be applied efficiently in clinical practice.
In conclusion, PHRI is a simple and reproducible histological index that correlates strongly with endoscopic activity and predicts clinical outcomes in UC. It is therefore ideally suited for adoption in clinical practice as well as for consideration in clinical trials and central readouts if further validated to fulfil requirements of US Food and Drugs Administration or European Medicines Agency requirements. We suggest using a PHRI cut-off of 0 to define HR, and a cut-off of 1 to stratify low vs high risk of adverse outcomes. The dichotomous nature of PHRI (ie, presence or absence of neutrophils) allowed the development of machine learning algorithm with high diagnostic accuracy for detection of the disease activity and HR in UC. Further studies are ongoing to validate the deep learning-based computer-aided classifier before it can be adopted in clinical practice.
Data availability statement
Data are available on reasonable request. Computer algorithm code available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Ethics approval was obtained from West Midlands Research Ethics Committee (17/WM/0223) and institutional ethics committees of all centres. All patients gave informed consent to participate in the study.
Acknowledgments
The authors would like to acknowledge Dr Zainab Abdawn for her help in retrieving and digitalising histological slides.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @IBDdoc
XG, AB, RdA and VV contributed equally.
Correction notice This article has been corrected since it published Online First. Author affiliations have been updated and figures 2 and 3 replaced.
Contributors XG: study conception and design, data acquisition, analysis and interpretation of data, drafting of the manuscript, critical revision of manuscript for important intellectual content. AB, ELS, MATM, GA, RP, RK, EG: analysis and interpretation of data, critical revision of manuscript for important intellectual content, statistical analysis. VV: study conception and design, data acquisition, analysis and interpretation of data, critical revision of manuscript for important intellectual content. RdA: study conception, analysis and interpretation of data, critical revision of manuscript for important intellectual content. MV, GdH, DZ, PB, JGF, MG, BH, ML, AP-B, LP, TR, GET, RB: data acquisition, analysis and interpretation of data, critical revision of manuscript for important intellectual content. TLP: analysis and interpretation of data, drafting the manuscript, critical revision of manuscript for important intellectual content. UNS, GM: data acquisition, critical revision of manuscript for important intellectual content. SD: critical revision of manuscript for important intellectual content. VN, SG: study conception and design, analysis and interpretation of data, drafting of the manuscript, critical revision of manuscript for important intellectual content. MI: study conception and design, concept of AI for histological scoring, data acquisition, analysis and interpretation of data, drafting of the manuscript, critical revision of manuscript for important intellectual content and guarantor of the study.
Funding MI and SG are funded by the NIHR Birmingham Biomedical Research Centre at the University Hospitals Birmingham NHS Foundation Trust and the University of Birmingham.
Disclaimer The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.