Article Text

Statistics from Altmetric.com
Climate change is a threat to both public1 and digestive health.2–4 Ironically the delivery of healthcare contributes to global warming by generating waste and emissions. If the global healthcare sector was a country, it would be the fifth highest emitter of greenhouse gases on the planet.5 Healthcare providers6 and the global gastroenterology (GI) community recognise the need to break this cycle. For example, several GI societies have started climate focused action groups or committees, and the British Society of Gastroenterology has produced a first-of-its-kind GI society sustainability blueprint.7 Although promising, these initiatives are recent, geographically piecemeal and possibly limited in their impact since they require buy-in and then implementation of measures to directly address the carbon footprint and waste-related challenges, in addition to the need for goal-directed efforts by healthcare systems and providers.8 The climate crisis requires global, comprehensive, coordinated and urgent action if the GI community is to respond effectively.
Professional societies could make an important contribution to meeting this challenge. The World Gastroenterology Organisation (WGO) is a non-governmental organisation with 117-member GI societies from 108 countries representing over 65 000 gastroenterologists worldwide. The WGO Climate Change Working Group conducted a survey of global GI society leadership to understand their views on climate change, their society’s status, perceived barriers to action, support that might be useful and plans regarding the climate crisis. In this commentary, we provide the results and implications of the survey.
Global surveys of physicians on the issue of climate change have had variably low response rates.9 10 This raises a concern whether the respondents, and responses, are representative. We surveyed the leadership, rather than the membership, of the 117 GI societies who are members of the WGO. Leaders are well positioned to provide insights into their society’s attitudes, are familiar with society structures in place and are likely to have an informed view on what actions might be feasible in the future. The methodology and data from this survey are available as online supplemental file 1. The high response rate in our survey (49%; 57 of 117 societies) supports this approach (see online supplemental information for the methods we used and the survey questions). Given the proportional representation from all geographic areas and economic zones, the results are likely an accurate reflection of senior GI leadership attitudes and beliefs and the structures currently in place in their societies. We cannot exclude the possibility that the respondents are biased towards those who are more concerned about global warming. Another possible limitation of our strategy is that the responses are from a limited number of older, predominantly male, members of the profession whose views may, or may not, represent the attitudes and beliefs of their membership. However, we captured not only the subjective personal beliefs of leadership but also the structures in place in their respective organisations (table 1).
Supplemental material
Overview of the survey results of the global gastroenterology leadership
The majority of responders believe that climate change represents a crisis, with 86% appearing knowledgeable regarding the cause, which is almost entirely anthropogenic. The remaining minority believe that the problem is caused equally by human and natural forces, so there is still work to do on educating GI leaders. This finding is similar to previous surveys where level of knowledge was captured.9–12 A majority of leaders are personally committed to change, and a significant number have already made changes in their personal (49%) and professional (53%) lives. The level of concern did not vary by geographic or economic group, but these personal beliefs and concerns have not resulted in global warming being prioritised by their national societies. The issue receives a low prioritisation ranking in their GI society. Only 9% have a climate working group or committee in place that provides a planning and administrative structure, which would be able to facilitate change. However, 46% of those surveyed indicated that their GI society will likely form a CC working group.
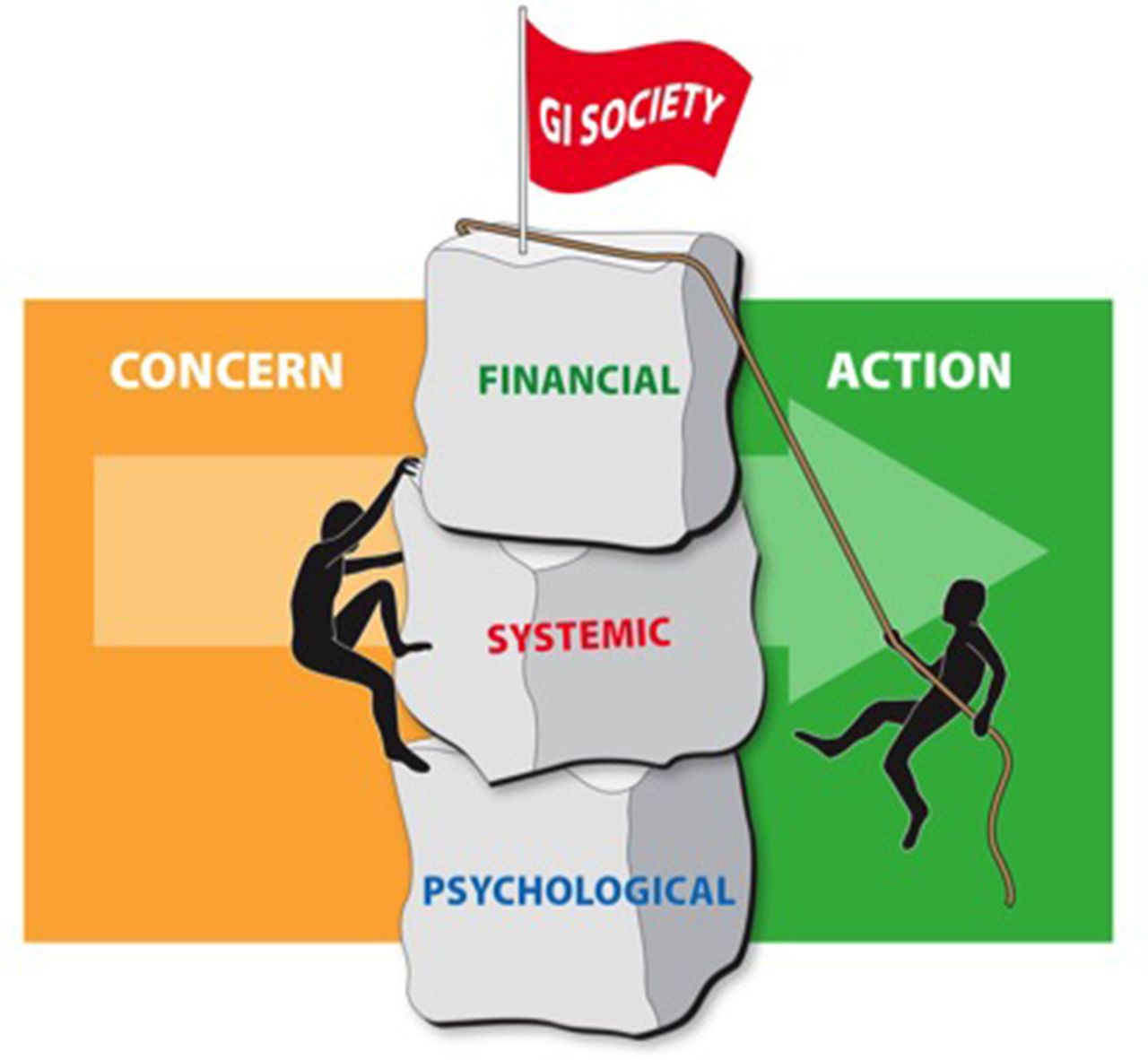
Obstacles to moving from concern to action could be due to prioritisation of systemic issues, psychological13–15 or financial constraints (figure 1). Leadership did provide insights, in both open text and direct questions, into the disconnect between their personal ranking of the crisis and the lack of prioritisation by their society. A lack of awareness and knowledge of the issue and the competing demands of clinical work were the major reasons cited. A smaller number believe that the health sector could not change its practices or was not responsible, that engagement was hindered by lack of organisation and resources, and a lack of advocacy.
{kind=link}
Major barriers for the gastroenterology (GI) societies to move from being concerned to taking action as related to climate change. Three types of obstacles are major impediments to moving from the primary current sentiment of being concerned to take active measures. The three types of barriers are: (1) financial incentives and disincentives, (2) systemic issues such as a lack of knowledge and education on the topic and an absence of an administrative structure and (3) psychological barriers.
Similar themes emerged in direct questioning. Over 80% of the leaders agreed strongly, or partially, that their societies have more pressing problems than climate change. A similar percentage agreed that they do not have the knowledge to engage, and that it is the responsibility of government (69%) to deal with this or that financial sponsorship for work in this area may be difficult to secure.
Several of the systemic or structural blocks, perhaps with the exception of the demands of clinical work, may be readily correctable. For example, awareness and knowledge can be increased through education programmes. There is evidence that healthcare can reduce its impact and that it has a high environmental impact.5 The misperception that healthcare cannot change can be corrected by education and raising awareness. The current lack of organisation and advocacy can be addressed by creating climate action groups, or climate committees, in national GI societies. It is understandable that societies feel they have more pressing problems, especially in the current pandemic, and it is likely that if leadership did fully grasp the level of threat, that prioritisation would change. A majority also believe that this is an issue for government; however, most governments have not begun to deal effectively with the problem and likely will not until they feel that they have public support, for which the medical profession can play leadership and advocacy roles. Clearly a conversation needs to be had with industry partners, who will also increasingly face demands to reduce their carbon footprint, concerning ways in which sponsorship may be secured.16
A smaller number of leaders identified what may be considered psychological barriers, the lack of an imminent threat, climate change uncertainty (or even denial) and an inability to have an impact on the problem.15 The perception that climate change is not an imminent threat may be partly due to knowledge but may also be a psychologic block known as temporal discounting13 whereby non-imminent threats are not prioritised. Almost equal numbers believe that they can, or cannot, make a difference. Inability to make a difference is a valid reason to not act but it may be a manifestation of what the psychologists term a lack of behavioural control.15 Not engaging because of concerns that engagement may not be effective is a circular argument.
In addition to structural and psychological barriers, there are financial incentives and disincentives at play in current practice. For example, many national societies derive income from annual meetings, which helps support key services they provide to their members, but which for many may have the largest proportional carbon impact within their organisations. The meeting attendance generates income from pharmaceutical and device industry support but also increases travel-related emissions, often from air travel, which can be very significant.17 Notably, over a quarter of GI society leaders in this survey were willing to consider carbon offsets and 70% have plans to move to hybrid models for their annual meeting suggesting that openness to change is already beginning. Some societies might be wary of the financial impact of addressing climate change by total conversion to remote meetings, but anecdotal experience, not captured in our survey, indicates that innovative new models of delivering meetings remotely can be as financially advantageous as traditional meetings. This needs formal study and if the data are validated, might present a compelling argument to consider hybrid meetings as the norm in the future.
Now that these obstacles have been identified, it may be possible to address them. The only action that has already been adopted by a majority is a plan to move to virtual or hybrid meetings. Whether that is due to the pandemic or a response to climate change is unclear. Other strategies, not explored in our survey, have been incorporated into the British Society of Gastroenterology statement on sustainable conferences.18 These include a competitive tendering process for meeting organisers and venues, which include robust sustainability mitigation measures within their operations. Simple measures, which can be adopted readily include a ‘paperless’ meeting at the venue, including course materials, advertising and posters. Delegates, particularly for local or regional meetings, can be encouraged to travel by the most environmentally sustainable method such as train rather than car or air. Industry sponsors can also be encouraged to adopt sustainable operations for these meetings, and these sustainability measures can be emphasised in the marketing of events. Face-to-face meetings have a role to play in building the community of practice and in professional identity formation, which is achieved in part through socialisation.19 They should be retained with the least possible environmental impact.
Moving forward, the situation is more positive with a majority or near-majority of leaders believing that a variety of adaptation and mitigation plans may be acceptable to their societies. Leadership is open to a variety of options regarding improving knowledge, awareness and delivery of education on this issue. While we have identified society meetings and conferences as a major contribution to their carbon footprint, we encourage all societies to critically appraise all of their operations to identify and mitigate against the effects of greenhouse gas emissions.
While this survey focused on the role GI societies might play and identifying hurdles they face, there is a wider context. At COP26 in Glasgow, 50 countries committed to sustainable, low emission health systems.20 If planning for that change includes the activities of professional societies, as may be the case, then novel incentives to deliver sustainable, low emission professional societies strategies may emerge. Professional societies may be held, or hold themselves, accountable for their carbon footprint within a national framework striving to decrease environmental impact. That change would radically alter the approach to overcoming obstacles. There will also be opportunities, especially in those countries that have committed, to connect with national government agencies and other medical organisations, to contribute to research and best practice development.
Global GI leadership is deeply concerned about the issue of climate change. While this concern has not yet translated into widespread action, the indications are that the profession is on the cusp of change. That change will be accelerated by increasing the awareness of society members. GI societies can play a critical role in educating their membership, leading by example, reducing the environmental impact of their operations such as travel, increasing advocacy for solutions and related research funding, and by informing and supporting politicians trying to lead change. However, removing barriers and educating membership may not be sufficient. The underlying psychological barriers described above will also need to be addressed.
As concrete next steps, we suggest that all GI societies establish climate action committees, working groups or task forces, and place this topic as a regular feature of their education programmes. At this stage, raising awareness should be the priority. Those who do not feel that they have the expertise can be assured that a growing global support group is available, which is willing to help. In addition to raising awareness, we also need to urgently explore novel framing of the education message and to remove financial incentives that promote environmental harm.
On a historical note, it was scientist, innovator and women’s rights activist, Eunice Newton Foote, who speculated in 1856 that changing the proportion of carbon dioxide in the atmosphere would change its temperature.21 Fast forward 166 years later, we in GI are well positioned, should we choose to do so, to build on her work. It is in all our interests to actively cooperate and generate an effective global response to this emerging crisis.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
We greatly appreciate and thank all the gastroenterology society leaders and colleagues who took the time to reply to our survey and provide open comments. We thank Jim Melberg for his administrative support of the World Gastroenterology Organisation (WGO) Climate Change Working Group, and Kristopher Morrow for assistance with the figure preparation. We acknowledge the contributions of the members of the WGO Climate Change Working Group, in addition to the authors: Naima Amrani, Mohammed V University, Morocco; Lars Aabakken, Oslo University Hospital, Norway; Raja Affendi Raja Ali, National University of Malaysia, Malaysia; Mario Reis Alvares-da-Silva, Universidade Federal do Rio Grande do Sul, Brazil; David Armstrong, McMaster University, Canada; Sedat Boyacioglu, Baskent University, Turkey; Ye Chen, Southern Medical University, China; Reda Elwakil, Ain Shams University, Egypt; Kwong-Ming Fock, Duke-NUS Medical School and Changi General Hospital, Singapore; Saeed S. Hamid, Aga Khan University, Pakistan; Vivek Kaul, University of Rochester Medical Center, United States; Harshit Khara, Geisinger Medical Center, United States; Govind Makharia, All India Institute of Medical Sciences, India; Finlay Macrae, Royal Melbourne Hospital, Australia; Reza Malekzadeh, Tehran University of Medical Sciences, Iran; Elias Makhoul, Holy Spirit University of Kaslik Byblos, Lebanon; Chris J. Mulder, Amsterdam UMC, The Netherlands; Mathieu Pioche, Hospices civils de Lyon, France; Alejandro Piscoya, Universidad San Ignacio de Loyola, Peru; Mai Ling Perman, Fiji National University, Fiji; Quang Trung Tran, Hue University, Vietnam; Eduardo Rodrigues-Pinto, Centro Hospitalar São João, Porto, Portugal; Anahita Sadeghi, Tehran University of Medical Sciences, Iran; Roque Sáenz, Universidad del Desarrollo, Chile; Jean-Christophe Saurin, Hôpital Edouard Herriot, France; Amna Subhan Butt, Aga Khan University, Pakistan; Kaichun Wu, Xijing Hospital of Digestive Diseases, China; Yeong Yeh Lee, Universiti Sains Malaysia, Malaysia.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors DL led on development of the survey, with methodological and content contributions from all of the other authors. DL led on the writing of the manuscript, with edits, amendments, and final approval from all of the other authors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.