Article Text

Abstract
Importance Patients with familial adenomatous polyposis (FAP) are at markedly increased risk for duodenal adenomas and cancer. Combination sulindac and erlotinib was previously shown to reduce duodenal polyp burden but was associated with a relatively high adverse event (AE) rate. Objective: To evaluate if a once weekly dosing schedule for erlotinib intervention improves the AE profile, while still providing efficacy with respect to reduced polyp burden, in participants with FAP. Design, setting and participants: Single-arm trial, enrolling 46 participants with FAP, conducted from October 2017 to September 2019 in eight academic cancer centres.
Exposures Participants self-administered 350 mg of erlotinib by mouth, one time per week for 6 months. Main outcomes and measures: Duodenal polyp burden (sum of polyp diameters) was assessed in the proximal duodenum by esophagogastroduodenoscopy performed at baseline and 6 months, with mean per cent change defined as the primary efficacy outcome of interest. Rate of grade 2–3 AEs was evaluated as a co-primary outcome. Secondary outcomes included changes in total duodenal polyp count, along with changes in lower gastrointestinal (GI) polyp burden and count (for participants examined by optional lower endoscopy).
Results Forty-six participants (mean age, 44.1 years (range, 18–68); women, 22 (48%)) were enrolled; 42 participants completed 6 months of intervention and were included in the per-protocol analysis. Duodenal polyp burden was significantly reduced after 6 months of weekly erlotinib intervention, with a mean per cent change of −29.6% (95% CI, −39.6% to −19.7%; p<0.0001). Similar results were observed in subgroup analyses defined by participants with advanced duodenal polyposis (Spigelman 3) at baseline (mean, −27%; 95% CI, −38.7% to −15.2%; p<0.0001). Post-intervention Spigelman stage was downstaged in 12% of the participants. Lower GI polyp number was also decreased after 6 months of intervention (median, −30.8%; IQR, −47.4% to 0.0%; p=0.0256). Grade 2 or 3 AEs were reported in 71.7% of subjects, with only two experiencing grade 3 toxicity at least possibly related to intervention.
Conclusion In this single-arm, multi-centre trial of participants with FAP, erlotinib one time per week resulted in markedly lower duodenal polyp burden, and modestly reduced lower GI polyp burden, after 6 months of intervention. While AEs were still reported by nearly three-quarters of all participants, these events were generally lower grade and well-tolerated. These findings support further investigation of erlotinib as an effective, acceptable cancer preventive agent for FAP-associated GI polyposis.
Trial registration number NCT02961374.
- polyposis
- familial adenomatous polyposis
- cancer genetics
- chemoprevention
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Patients with familial adenomatous polyposis (FAP) are at markedly increased risk for colorectal and duodenal adenomas and cancer. Multiple studies have shown the cyclooxygenase inhibitors, sulindac and celecoxib, significantly inhibit colorectal adenomatous polyps in patients with FAP but their efficacy in duodenal neoplasia is modest. The present study is designed to evaluate the efficacy and safety of one time per week erlotinib to reduce adenoma burden in the duodenum of participants with FAP.
WHAT THIS STUDY ADDS
In this multi-centre single-arm trial duodenal polyp burden was significantly reduced after 6 months of one time per week erlotinib 350 mg intervention, with a mean per cent change of decrease of nearly 30% (p<0.0001). While adverse events were still reported these events were generally lower grade and well-tolerated.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
These findings support further investigation of erlotinib as an effective, acceptable cancer preventive agent for FAP-associated gastrointestinal polyposis. This strategy may serve to complement current endoscopic and surgical management approaches, with reduced morbidity.
Introduction
Familial adenomatous polyposis (FAP) is an autosomal dominant, genetic cancer syndrome caused by germline mutations in the adenomatous polyposis coli (APC) gene. In its classic form, the disease is characterised by the progressive development of hundreds to thousands of adenomatous polyps in the colorectum and a nearly 100% risk of colorectal cancer if left untreated. Once the burden of colorectal polyposis is beyond endoscopic management, proctocolectomy or (sub)total colectomy is the consensus standard of care. Upper gastrointestinal (GI) polyposis develops in the duodenum in more than 80% of patients with FAP, with duodenal and periampullary cancers occurring in 5%–12% of these patients.1 Unlike colorectal disease, current approaches to prevent duodenal carcinomas through endoscopy (duodenal polypectomy, papillectomy) and or surgery (pancreas-sparing duodenectomy, pancreatoduodenectomy—Whipple) are suboptimal and can be associated with significant morbidity. Additionally, surgical interventions for duodenal polyposis carry higher risk of mortality and morbidity that can markedly affect quality of life.2 3 Thus, there is an urgent, unmet need for improved cancer prevention strategies to delay or interrupt FAP-associated duodenal carcinogenesis.
Multiple studies have shown the cyclooxygenase-1 and cyclooxygenase-2 (COX-1 and COX-2) inhibitors—sulindac and celecoxib, respectively—significantly inhibit colorectal adenomatous polyps.4–6 However, based on available literature, this agent class appears to have much more modest efficacy with respect to duodenal adenomas.7 COX inhibitors are also associated with cardiovascular side effects that have dampened enthusiasm for routine use in sporadic colorectal cancer prevention. Further complicating widespread clinical application, the US Food and Drug Administration’s (FDA) accelerated approval of celecoxib for FAP colorectal disease was voluntarily withdrawn by the manufacturer as postmarketing study intended to verify clinical benefit and required as a condition of approval under accelerated approval (subpart H) was never completed.8
Studies have suggested that somatic APC inactivation and epidermal growth factor receptor (EGFR) signalling promote COX-2 expression and the subsequent development of intestinal neoplasia.9–11 The results of preclinical studies conducted in mouse models and of the phase 2 double-blind placebo-controlled randomised FAP Erlotinib–Sulindac Trial (FAPEST) (NCT1187901) showed that combination COX and EGFR inhibition with sulindac and erlotinib resulted in a profound 69%–71% reduction in duodenal and colorectal polyp burden after only 6 months of treatment.12 However, adverse events (AEs) were common, with an acne-form rash observed in over 80% of participants on active therapy, likely limiting the use of this medical regimen at the dosing schedule applied in this study. Recent studies conducted in subjects with head and neck cancer suggested that the pharmacokinetics of erlotinib may lead to a lower side effect profile when dosed one time per week.13–15 In regards to COX inhibitor use in FAP, the combination of FDA withdrawal of approval of celecoxib, cardiovascular side effect profile and limited efficacy in duodenal polyposis prompted the question whether erlotinib as a single agent would be effective (with fewer adverse effects) in the setting of FAP cancer prevention.
We therefore designed and conducted an National Cancer Institute-sponsored single-arm, multi-centre, phase 2 trial to evaluate the efficacy and safety of 350 mg one time per week erlotinib to reduce adenoma burden in the duodenum of participants with FAP.
Methods
Study design
To further develop the evidence base regarding dosing and safety of erlotinib as a candidate agent for FAP-associated cancer chemoprevention, this study was designed as a single-arm trial of participants with genetically or clinically-confirmed FAP, conducted at eight academic cancer centres from 27 October 2017 to 6 September 2019. Enrolling institutions included Mayo Clinic in Scottsdale, Arizona, USA; Cleveland Clinic, Cleveland, Ohio, USA; University of Michigan, Ann Arbor, Michigan, USA; University of Utah, Salt Lake City, Utah, USA; Mayo Clinic in Rochester, Minnesota, USA; University of Pittsburgh, Pittsburgh, Pennsylvania, USA; University of Puerto Rico, San Juan, Puerto Rico; and University of Texas MD Anderson Cancer Center, Houston, Texas, USA.
All enrolling institutions received local Institutional Review Board (IRB) acknowledgement of the Central IRB approval prior to initiation of enrolment. Prior to screening, all participants underwent informed consent and signed the approved informed consent document.
Eligible participants included men and women aged 18–69 years, of all races and ethnic groups, English-speaking or non-English-speaking with a diagnosis of FAP. Diagnosis of FAP was required to be confirmed genetically (pathogenic/likely pathogenic germline variant in APC) and/or clinically (>100 colorectal adenomas with a family history of FAP). Eligible subjects had documented duodenal disease (Spigelman stage 2 or 3), with no prior history of treatment with or allergy to erlotinib. Other eligibility criteria included willingness to abide by study requirements and discontinue use of non-steroidal anti-inflammatory drugs (NSAIDs) (except the use of ≤81 mg/day or 650 mg/week) and tobacco, no use of potent CYP3/4 inhibitors or inducers, no intercurrent illness or history of invasive malignancy within 3 years prior to screening, no history of upper GI surgery that would preclude evaluation of the first 10 cm of the duodenum, ECOG (Eastern Cooperative Oncology Group) performance status ≤1, adequate bone marrow and organ function, not pregnant or breast feeding, no evidence of high-grade dysplasia or cancer, quantifiable polyp burden and no regular use of drugs that would alter the pH of the GI tract.
At baseline, endoscopic evaluation with esophagogastroduodenoscopy (EGD) was implemented in a matter consistent with the previous FAPEST study, reported in Journal of the American Medical Association (JAMA).12 16 In brief, a tattoo was placed 10 cm distal to the duodenal bulb to define the ‘evaluable duodenal segment’. All polyps were counted, and each polyp with associated size (as estimated by the performing endoscopist using a closed biopsy forceps of 2.4 mm) was mapped and Spigelman score calculated in the evaluable 10 cm segment at 1-cm intervals. After the counting and mapping was complete, at least one polyp, along with any polyps that were suspicious for high-grade dysplasia or malignancy, were biopsied and sent to the local pathologist for evaluation and Spigelman stage determination. For research purposes, four endoscopic biopsies of grossly normal duodenal mucosa and one (for Spigelman 2) or two (Spigelman 3) endoscopic biopsies of duodenal polyps were obtained from all participants. One biopsy each from normal mucosa and polyp was placed in RNAlater, and the remaining specimens were snap-frozen in liquid nitrogen. Still photos and videos were captured for all procedures though central review was not used to determine the outcome measure as it is not a validated instrument. Individuals with at least 10 cm of rectum or an ileoanal pouch also underwent optional lower GI endoscopies with polyp counting and research biopsy collection. Only subjects who satisfied all inclusion and exclusion criteria advanced to drug intervention (figure 1).
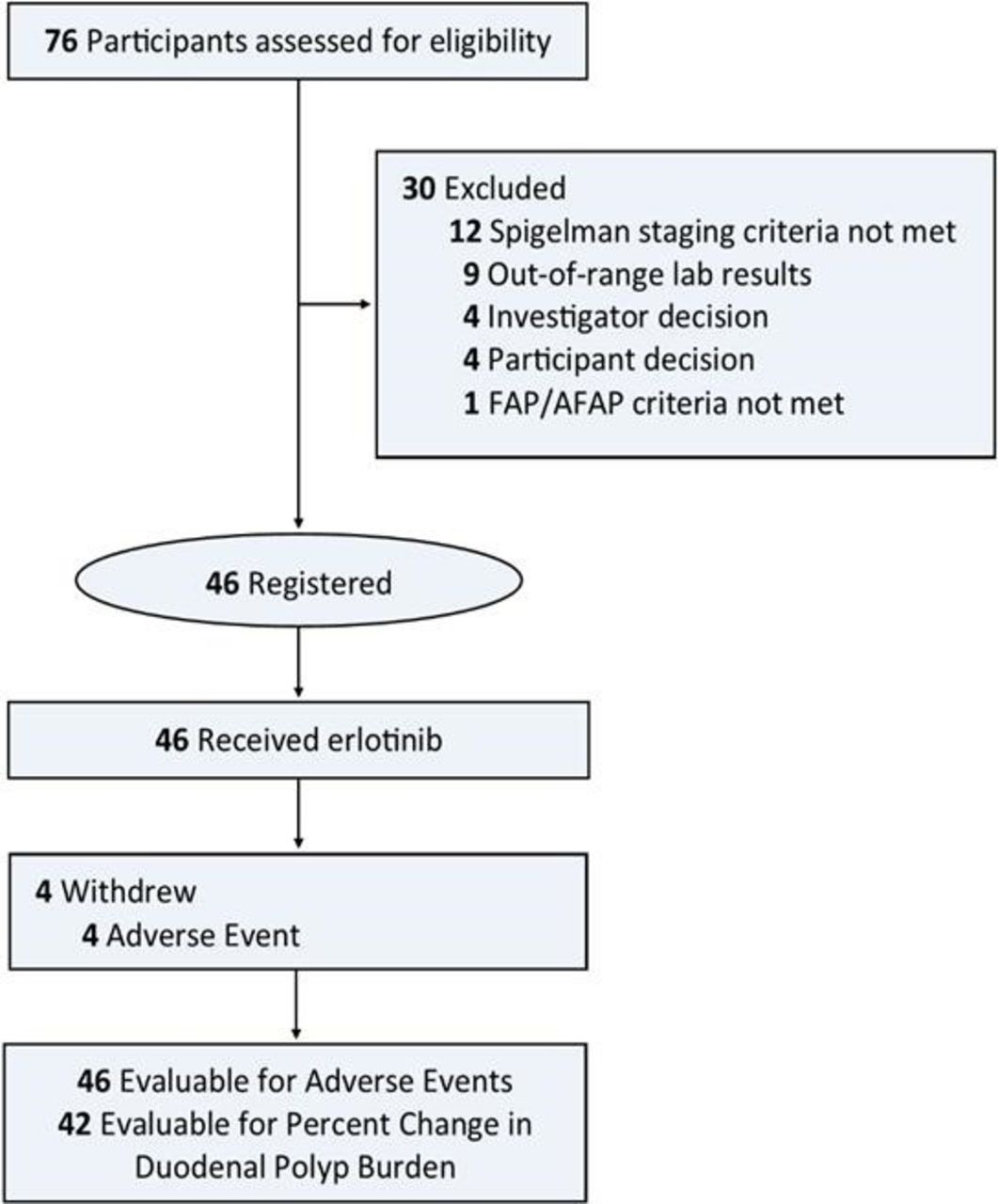
CONSORT (Consolidated Standards of Reporting Trials) flow diagram of subject progress through the clinical trial. AFAP, attenuated FAP; FAP, familial adenomatous polyposis.
During the intervention phase, participants self-administered 350 mg erlotinib by mouth, one time per week at approximately the same day/time each week, for a period of 6 months. Erlotinib (FDA IND (Investigational New Drug) exemption 108086) was provided by the National Cancer Institute’s Division of Cancer Prevention through a contract with the drug manufacturer. Drug compliance was assessed by pill count review of participant diaries. Safety evaluations, including laboratory assessment (blood, urine and pregnancy tests) were performed during and at the end of the intervention. A repeat EGD and lower endoscopy, with polyp mapping and research biopsy collection identical to the baseline procedure took place, after which polyps were cleared and reviewed by the local pathologist, per institutional standards of good clinical practice.
Primary endpoints
There were two co-primary endpoints. The first co-primary endpoint was defined as the mean per cent change in duodenal polyp burden (which is based on the sum of diameters from all polyps from baseline to 6 months post-intervention), as evaluated during EGD. Endoscopic evaluations were performed within 30 days before intervention with erlotinib was initiated (month 0) and 6 months after intervention was initiated (month 6). The hypothesis was that weekly erlotinib would significantly reduce duodenal polyp burden after 6 months of intervention.
The second co-primary endpoint was defined as the rate of grade 2/3 Cancer Terminology Criteria for Adverse Events (CTCAE) V.4 AEs. The hypothesis was that weekly erlotinib would significantly reduce the grade 2/3 AE rate compared with previously reported data from the FAPEST trial.12
Secondary endpoints
Secondary endpoints included: (1) absolute and per cent change in duodenal polyp number; (2) duodenal polyp burden stratified by Spigelman stage; (3) duodenal polyp burden in the subset of participants with a genetic diagnosis; (4) absolute and per cent change in colorectal polyp number and burden from baseline to month 6. For the secondary endpoint involving the colorectum, the length of the lower intestine remaining was stratified into two groups: ileal pouch-anal anastomosis or rectal remnant in those with an ileorectal anastomosis. To evaluate the safety and tolerability of weekly erlotinib, all participants were evaluated for toxicity from the time of their first dose of erlotinib.
Statistical analyses
With 35 evaluable subjects, we estimated 81% power to detect a mean per cent decrease in polyp burden of 15% compared with baseline based on a paired t-test with two-sided significance level of 0.05. The power calculation assumed an effect size of 50% and a SD of 30%.
With respect to the grade 2/3 AE co-primary endpoint, 35 evaluable patients would yield 83% power to detect a reduction in the grade 2/3 AE rate from 50% to 25%, assuming a two-sided significance level of 0.05 and using an exact test for a single proportion. With at least 35 eligible patients, at least 80% power was estimated for both primary endpoints (polyp burden and AEs), per protocol. In total, 42 evaluable participants were enrolled, thus meeting the accrual target needed for achieving acceptable statistical power.
For the primary analysis assessing the mean per cent change in duodenal polyp burden, we used a paired t-test because the per cent change distribution was approximately normally distributed. For the grade 2/3 AE primary analysis, a one-sample exact test for a single proportion was conducted assuming 50% for the null hypothesis. In the event that a continuous secondary endpoint was found not to be approximately normally distributed, the paired Wilcoxon Signed-Rank test was used; otherwise, the paired t-test was used. Analyses were performed using SAS V.9.4 (SAS Institute). No adjustment was made for performing multiple tests. P values are two-sided and p values <0.05 were considered statistically significant.
The complete study protocol is available in online supplemental appendix 1.
Supplemental material
Results
Demographic characteristics
From 27 October 2017 to 6 September 2019, a total of 76 individuals were evaluated for eligibility, and 30 were excluded as they did not meet the inclusion/exclusion criteria or declined to participate (figure 1). After the baseline endoscopy 46 participants were enrolled and started intervention.
A summary of the demographic characteristics of the enrolled subjects is shown in table 1. The 46 participants enrolled in this study had a mean age of 44.1 years (SD, 13.90 years); 47.8% were women; 93.5% were white. The majority of participants (87%) had a genetic diagnosis of FAP with a confirmed APC mutation and nearly 70% had Spigelman 3 duodenal disease. Other descriptive factors, including enrolling institution, use of any aspirin or NSAIDs at baseline and body mass index, are presented in table 1.
Baseline demographic characteristics of participants (N=46)
Outcomes
Four participants withdrew before the endpoint endoscopy. Thus, 42 participants completed the study with pre-intervention and post-intervention endoscopy results and were included in the per-protocol analysis of duodenal polyp burden.
Primary outcome: duodenal polyp burden
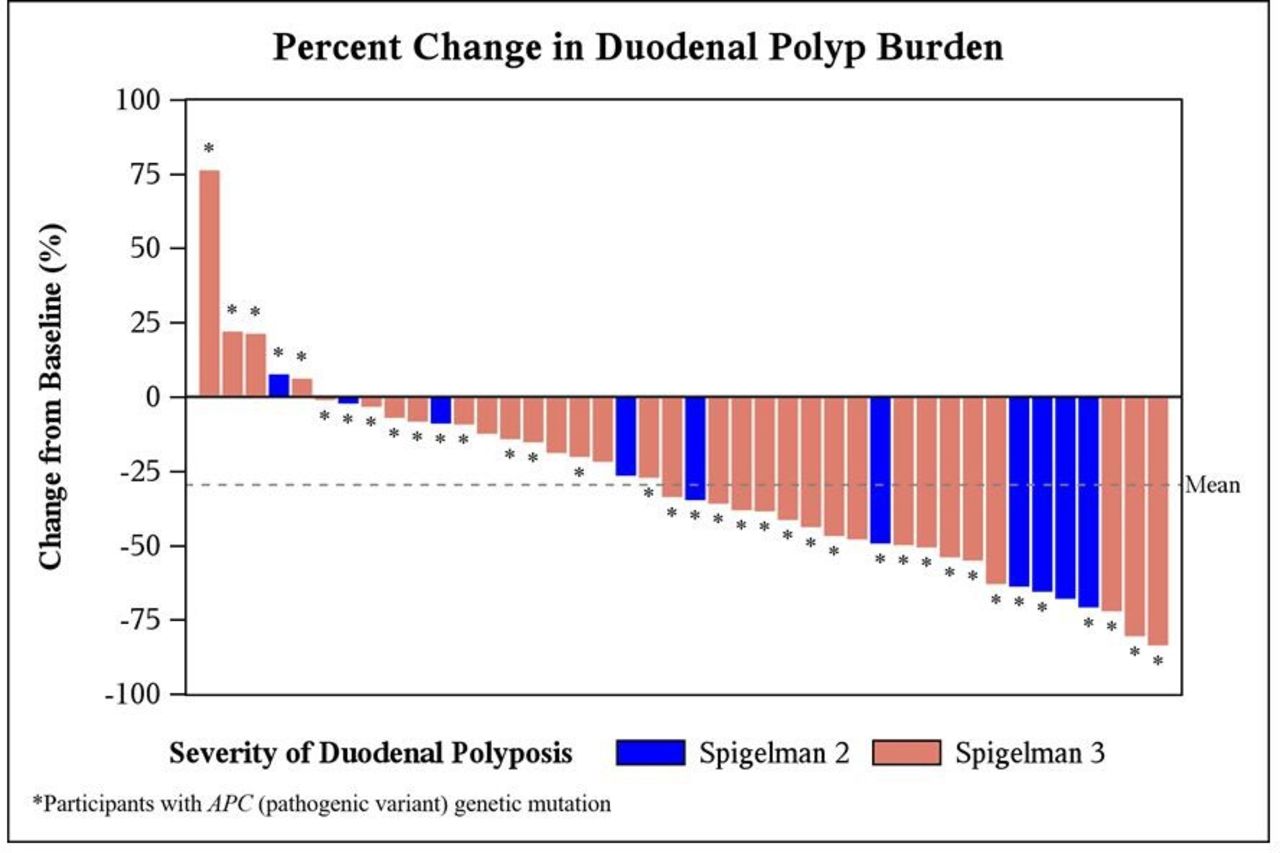
The mean polyp burden at baseline was 137.2 mm and at month 6 was 97.2 mm (median polyp burden at baseline was 107 mm and month 6 median was 81 mm) (tables 2 and 3). There was a 40 mm (64.4) mean (SD) decrease in total duodenal polyp burden from baseline to 6 months post-intervention, which represented a 29.6% (31.9%) mean (SD) decrease from baseline (95% CI, −39.6% to −19.7%; p<0.0001) (table 2 and figure 2). Overall, 37 (88.1%) and 5 (11.9%) subjects were found to have reduced and increased duodenal polyp burdens, respectively. Online supplemental table 1a and b shows results restricted to the population with a confirmed APC germline mutation.
Supplemental material
{kind=link}
{kind=link}
Per-protocol analysis of percent change in total sum of diameters of duodenal polyps for each participant.
Change in duodenal polyp burden from baseline
Change in duodenal polyp number from baseline
Primary outcome: adverse effects
Grade 2 or 3 AEs were reported in 71.7% of subjects, which was a significantly more than the expected null hypothesis rate of 50% (p=0.0032). Intervention with one time per week erlotinib for a 6-month period was generally well-tolerated. However, four participants withdrew from the study due to drug-induced adverse effects (grade 3 rash acneiform, grade 2 infections (hand, foot and mouth disease), grade 1 fatigue and grade 1 rash acneiform). No grade 4 events were reported during intervention. The most common AE was an erlotinib-induced acneiform-like rash, which occurred in 56.5% of the participants (n=26). The rash was managed with topical cortisone and/or clindamycin therapy. Additional erlotinib-induced AEs reported included oral mucositis (6.5%, n=3), diarrhoea (50%, n=23) and nausea (26.1%, n=12). Study-related AEs are summarised in table 4.
Incidence and severity of adverse events, at least possibly related to intervention (observed in 5% or more of participants or grade 2 or higher toxicity. Presented as number (%) of individuals)
Secondary outcome analyses
In a subgroup analysis of participants with confirmed germline APC mutation FAP (n=36), the mean (SD) per cent decrease in duodenal polyp burden after 6 months of intervention was 29.1% (33.61%) (95% CI, −40.5% to −17.8%; p<0.0001) and among those with severe duodenal disease (Spigelman 3, n=32) the mean (SD) per cent decrease in duodenal polyp burden was 27% (32.7%) (95% CI, −38.7% to −15.2%; p<0.0001) (online supplemental table 1a and table 2). Similar results were present in those of both genders or median age and in those with and without an acneiform rash (table 2).
For total duodenal polyp count, there was a mean (SD) decrease of nearly 13 (23) polyps 6 months post-intervention, which represented a 10.7% (16.8%) decrease from baseline (95% CI, −15.9% to −5.4%; p=0.0002) (table 3). Subgroup analysis confirmed similar findings in participants with a confirmed germline APC mutation (online supplemental table 1b), Spigelman 3 disease and a genetic diagnosis.
In assessing Spigelman stage pre-intervention and post-intervention we found that of the 42 participants evaluable for the primary endpoint, 36 (85.7%) reported the same Spigelman stage at baseline and endpoint, 1 (2.4%) reported an increase in Spigelman stage from 2 to 3 and 5 (11.9%) reported a decrease in Spigelman stage from 3 to 2 between baseline and endpoint, however this was not statistically significant (p=0.1025).
Compared with baseline, at 6 months, the median (IQR) per cent change in the number of lower GI polyps was (−30.8 (−47.4 to 0.0); p=0.0256) however, the median (IQR) per cent change in lower GI polyp burden was not significantly different (0.0 (0.0 to 25.0); p=0.7031) (online supplemental table 2).
Study safety
Study agent adherence assessed by pill count diaries was available for 43 (93.5%) of 46 participants. Of those who started intervention, 3 (6.5%) of 46 participants had erlotinib dose reduction to 175 mg per week. Erlotinib dose reductions included two cases of grade 2 rash acneiform, and one case of grade 2 infections and infestations (hand, foot and mouth disease). There were three participants for whom erlotinib was temporarily discontinued due to concerns for grade 2–3 acneiform rash (n=2) and grade 2 oral mucositis (n=1). When symptoms improved, erlotinib was re-escalated as tolerated.
Discussion
FAP portends a heritable, systemic predisposition to cancer and the ultimate goal of cancer preventive intervention is to interrupt the development of neoplasia, need for surgery and ultimately death from cancer,1 17 with an acceptable AE profile. In this single-arm, multi-centre, phase II cancer prevention clinical trial, one time per week erlotinib effectively reduced the duodenal polyp burden and polyp number in participants with FAP. This effect was significant after only 6 months of therapy and was observed in those with either Spigelman 2 or Spigelman 3 duodenal polyp burden. Though only 12% of patients noted a decrease in Spigelman stage from 3 to 2 associated with therapy, the majority of patients (86%) had stable disease while on treatment. Though adverse effects were commonly reported, participants generally did not require dose modification of the erlotinib intervention. While promising, further investigation of the chemopreventive benefits from erlotinib or similar agents require further investigation.
This trial is built on preclinical data showing a beneficial role for EGFR inhibition in FAP along with a prior phase 2 clinical trial involving combination blockade of COX and EGFR.12 16 The murine studies showed a greater than 85% decrease in the progression of intestinal microadenomas through genetic or biochemical inhibition of EGFR tyrosine kinase activity in the ApcMin/+ mouse model of FAP.11 18 A preliminary phase 2 double-blind placebo-controlled randomised trial (FAPEST, NCT01187901) conducted in Spigelman 1 and 2 patients with FAP showed that combination of COX and EGFR inhibition with sulindac and erlotinib resulted in a 38% reduction in median duodenal polyp burden after 6 months of therapy in the active therapy arm.12 The current trial expands on these findings by showing that EGFR inhibition alone (independent of COX inhibition with sulindac) can lead to significant duodenal polyp regression similar in magnitude to that seen with combination therapy with erlotinib and sulindac. These findings are consistent with prior studies which have shown that sulindac (COX inhibition) alone or in combination with other agents has not been effective in reducing duodenal polyposis,7 19–21 highlighting the importance of the EGFR pathway in duodenal neoplasia development in FAP. The present study not only confirms the results of the prior single centre FAPEST trial but also expands by using multiple centres throughout the USA for generalisability and involves participants with greater severity of duodenal disease (Spigelman stage 2–3) than the prior study which represents the population likely to benefit from this therapy in real world use. While compelling, the favourable chemopreventive effects observed to date from erlotinib must be correlated with decreased GI cancer risk in patients with FAP to confirm clinical utility as a potential strategy to reduce or delay the need for more aggressive endoscopic or surgical interventions. Patients with Spigelman stage 4 were not included based on the historical data of an up to 30% risk of duodenal cancer and current standard of care recommendations for consideration of surgical duodenectomy within 6 months.
Our study found a more modest decrease in lower GI polyp number as compared with the prior FAPEST trial using combination sulindac and erlotinib.16 Several investigators have described regression of colorectal adenomatous polyps in patients with FAP who received sulindac or celecoxib alone. Regression of rectal adenomas following therapy with sulindac was demonstrated in two placebo-controlled trials, however no patient had complete remission and rapid recurrence as observed after discontinuation of sulindac.4 5 22 Similarly, a modest reduction in colorectal polyp number was achieved with 6 months of celecoxib therapy.6 The FAPEST trial reported a 69% net change in colorectal polyp number after 6 months of dual erlotinib and sulindac therapy compared with placebo.16 Taken together with our findings, this suggests that colorectal (lower GI) polyp development in FAP maybe more dependent on COX signalling than EGFR pathways, further highlighting the difference between duodenal and colorectal neoplasia in FAP.
Along with the encouraging reductions in duodenal and lower GI polyp burden observed in our study, AEs were frequently reported, although within limits of tolerability for most. Overall, the grade 2–3 adverse event rate was 72%, similar to that expected from standard of care use of this medication in oncology practice. The most notable AEs were acneiform cutaneous rash in 26 participants (56%) and oral mucositis in 3 participants (7%). Only two participants had grade 3 AEs at least possibly related to intervention—one case each of acneiform rash and infectious enterocolitis. One time per week administration of erlotinib (350 mg) did not seem to mitigate the AE rate compared with the prior FAPEST study which employed daily dosing of erlotinib (50 mg per day) and reported acneiform rash in 68% and oral mucositis in 32% in the treatment group. A recent study using a murine model of FAP (APC-mutation polyposis in rat colon, Pirc) suggested that an optimal low dose strategy (using a human equivalent of erlotinib 125 mg one time per week plus daily sulindac) led to significant tumour inhibition in the colon and small intestine while minimising skin toxicity and gastric ulceration.23
To reduce potential bias and interobserver variability, the baseline and 6-month endoscopy were performed by the same endoscopist for all study participants. The endoscopist was not blinded as to whether it was a baseline or endpoint procedure since the placement or existing presence of a tattoo would make it impossible. Advanced imaging methods (including narrow band imaging and chromoscopy) were not used though all centres used high-definition endoscopy. Central video review was not performed as an outcome measure as it is not a validated measure of polyp regression in FAP trials.
Limitations
This single-arm, phase II trial further supports the cancer preventive potential of erlotinib in FAP. However, the study has some limitations. Because the study measured polyp regression, it is unknown if erlotinib would be effective in preventing the emergence of new duodenal adenomas. This issue has previously arisen in a paediatric FAP trial that suggested sulindac may be ineffective in preventing the emergence of colonic adenomas in children with FAP. Without long-term follow-up data, the durability of the effect of erlotinib, the potential to develop resistance to the drug, and whether patients ultimately undergo fewer surveillance endoscopies and/or surgery or develop fewer cancers related to polyp regression are unknown. The long-term impact of erlotinib cancer prevention with respect to clinical and economic outcomes related to FAP-associated duodenal polyp management requires further investigation. Erlotinib can be associated with rare and serious adverse effects, such as interstitial lung disease,24 25 though no such effects were encountered in the present study. Notably, this study was not designed to directly assess the effects of erlotinib versus erlotinib +sulindac combination therapy. Rather, the erlotinib intervention regimen and co-primary endpoints were defined to further clarify the cancer preventive potential, and acceptability, of this promising candidate agent. Polyps may have also been removed at baseline if deemed necessary and appropriate for clinical care and this could potentially limit result to less advanced polyps. The role of erlotinib in management of ampullary polyps, which patients with FAP are at high risk for developing, was not specifically assessed. Due to the length of a standard endoscope used in this trial, examination of the distal duodenum (fourth portion of duodenum) was not specifically evaluated and thus could underestimate the polyp burden in some patients with FAP. Use of erlotinib also necessitated significant changes in lifestyle for safety including cessation of smoking, avoiding sun exposure and acid reducing medications which may limit its broad use in the FAP population outside of a clinical trial. In addition, the acneiform rash associated with erlotinib, while manageable during this study may limit more widespread use of this agent. Future trials may consider using next generation EGFR inhibitors which have lesser side effect profile. The results of this study should not be generalised to the broader population of sporadic GI tract neoplasia without appropriately designed clinical trials in those cohorts and the likely adverse effects would outweigh the benefits when applied to average risk groups.
Conclusions
Among participants with FAP, the use of erlotinib one time per week alone resulted in lower duodenal polyp burden after 6 months of therapy. Reported side effects were generally lower grade, and well-tolerated. However, even with the dosing schedule applied in this study, AEs were relatively common, and may still limit the clinical application of erlotinib for cancer prevention in some patients with FAP. This study provides novel, informative data that warrant investment in additional evaluation of erlotinib and/or similar EGFR inhibitors to further clarify the preferred dose, duration, risk:benefit ratio and potential drug combination(s) with merit for clinical application to prevent or regress FAP-associated carcinogenesis. If existing data are confirmed and extended through future research, this strategy has the potential for substantial impact on clinical practice by decreasing, delaying or augmenting endoscopic and surgical interventions as the mainstay for duodenal cancer prevention in this high-risk patient population.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the Cancer Prevention and Control Central Institution Review Board (CPC CIRB) of the National Cancer Institute. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors gratefully acknowledge the clinical study coordinators at the participating organisations: Lori Bergstrom, Megan Keener, Kadyn Kimball, Jessica Hernandez-Marrero, Deanne Nash, Samantha Goode, Lynda Dzubinski, Theosevia Demertzis, Larette Castleberry, Erika Koeppe, Diane Weber, Ramona Lansing, Hennie Hasson, Deanne Nash, Valerie Sepeda, Carrie Mays, Mayra Tornel Fernandez, Cateka Tsosie, Dr Kenneth Boucher and Dr Randall Burt. The authors acknowledge the Mayo Clinic Cancer Prevention Network for their assistance with study design, administration and manuscript preparation.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Correction notice This article has been corrected since it published Online First. The order of authors has been corrected.
Contributors NJS, ER, AU, GD, LMR, ES and PJL planned the study. NF, RPM and DZ biostatistical support and conducted data analyses. CAB, ES, PK, RD, MC-C, EV, GM, NB, ST, DKT, MS and MW led execution of the study at the participating sites. All authors contributed to drafting, reviewing and finalising the manuscript. NJS is the guarantor of the paper.
Funding This work was sponsored by the National Cancer Institute, Division of Cancer Prevention (contract no. HHSN261201200042I).
Competing interests PJL serves as Chief Medical Officer for Screening at Exact Sciences through a contracted services agreement with Mayo Clinic. PJL and Mayo Clinic have contractual rights to receive royalties through this agreement; Exact Sciences. JS is a consultant for Janssen Research and Development, Recursion Pharmaceuticals and Cancer Prevention Pharmaceuticals. CAB is a consultant for SLA pharma, Freenome, and has received research support from Janssen Pharmaceuticals, Cancer Prevention Pharmaceuticals, Ferring Pharmaceuticals and Emtora Biosciences. EV has a consulting or advisory role with Janssen Research and Development and Recursion Pharma and has received research support from Janssen Research and Development.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.