Article Text

Abstract
Objective Microbiome and dietary manipulation therapies are being explored for treating ulcerative colitis (UC). We aimed to examine the efficacy of multidonor faecal microbiota transplantation (FMT) and anti-inflammatory diet in inducing remission followed by long-term maintenance with anti-inflammatory diet in patients with mild-moderate UC.
Design This open-labelled randomised controlled trial (RCT) randomised patients with mild-moderate (Simple Clinical Colitis Activity Index (SCCAI) 3–9) endoscopically active UC (Ulcerative Colitis Endoscopic Index of Severity (UCEIS)>1) on stable baseline medications in 1:1 ratio to FMT and anti-inflammatory diet (FMT-AID) versus optimised standard medical therapy (SMT). The FMT-AID arm received seven weekly colonoscopic infusions of freshly prepared FMT from multiple rural donors(weeks 0–6) with anti-inflammatory diet. Baseline medications were optimised in the SMT arm. Clinical responders (decline in SCCAI>3) at 8 weeks in both arms were followed until 48 weeks on baseline medications (with anti-inflammatory diet in the FMT-AID arm). Primary outcome measures were clinical response and deep remission (clinical—SCCAI <2; and endoscopic—UCEIS <1) at 8 weeks, and deep remission and steroid-free clinical remission at 48 weeks.
Results Of the 113 patients screened, 73 were randomised, and 66 were included in (35—FMT-AID; 31—SMT) modified intention-to-treat analysis (age—35.7±11.1 years; male—60.1%; disease duration—48 (IQR 24–84) months; pancolitis—34.8%; SCCAI—6 (IQR 5–7); UCEIS—4 (IQR 3–5)). Baseline characteristics were comparable. FMT-AID was superior to SMT in inducing clinical response (23/35 (65.7%) vs 11/31 (35.5%), p=0.01, OR 3.5 (95% CI 1.3 to 9.6)), remission (21/35 (60%) vs 10/31 (32.3%), p=0.02, OR 3.2 (95% CI 1.1 to 8.7)) and deep remission (12/33 (36.4%) vs 2/23 (8.7%), p=0.03, OR 6.0 (95% CI 1.2 to 30.2)) at 8 weeks. Anti-inflammatory diet was superior to SMT in maintaining deep remission until 48 weeks (6/24 (25%) vs 0/27, p=0.007).
Conclusion Multidonor FMT with anti-inflammatory diet effectively induced deep remission in mild-moderate UC which was sustained with anti-inflammatory diet over 1 year.
Trial registration number ISRCTN15475780.
- ulcerative colitis
- diet
Data availability statement
Data are available upon reasonable request.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Faecal microbiota transplantation (FMT) is effective in inducing remission in patients with mild to moderate ulcerative colitis (UC).
There is only one small pilot study on the combination of FMT and anti-inflammatory diet in mild to moderate UC which was conducted only until 8 weeks and reported negative outcomes.
The role of anti-inflammatory diet in maintenance of FMT-induced remission has not been explored.
WHAT THIS STUDY ADDS
Faecal microbiota transplantation in combination with anti-inflammatory diet was more effective than optimised standard medical therapy in inducing remission in mild to moderate UC.
Anti-inflammatory diet could sustain the remission until 1 year and was more effective than standard medical therapy alone.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Combination of FMT and anti-inflammatory diet would be an effective and safe therapy for patients with mild to moderate UC.
Microbiome manipulation and dietary interventions may play a major role in the management of inflammatory bowel disease and should be further evaluated.
Introduction
Inflammatory bowel disease (IBD) including ulcerative colitis (UC) has been characterised by gut dysbiosis, although the cause and effect relationship remains an enigma.1 2 The present treatment algorithm for UC targets the dysregulated immune response and is limited by moderate efficacy, side effects (infections and malignancy) and cost, especially in developing countries, where the disease burden of IBD is rising.3–5 Correction of dysbiosis would be a more physiological, cost-effective and safe approach to target the intestinal inflammation, with a potential to alter the dysregulated pathophysiology upstream of the destructive immune response.
Diet is one of the major determinants of the gut microbiome and has been associated with risk as well as disease course of IBD.6 Diet patterns and dietary constituents can have a positive or negative influence on the gut microbiome, and various anti-inflammatory diets have been used with clinical success in patients with Crohn’s disease (CD).7 8 However, the evidence on dietary manipulation strategies in patients with UC is limited, and hence, recommendations cannot be made on diet as primary or adjunct therapy.7–9
Faecal microbiota transplantation (FMT) has been associated with clinical and endoscopic remission in cohort studies and randomised controlled trials (RCTs) in UC.10 11 However, these studies have been heterogeneous in terms of FMT protocol, method of preparation, dose and intensity of FMT, and there is no FMT-based induction RCT from Asia. Diet has a potential to enhance the success of FMT by creating a favourable niche for the engraftment of donor microbiota and by its own anti-inflammatory effect.12 However, except for a recent three-arm study which compared FMT and diet, FMT alone and diet alone in patients with refractory UC, there is no study which has evaluated the combination of diet and FMT in UC.13 Moreover, this study had a small sample size with 17, 19 and 15 patients in each arm, respectively. Further, there is no study which has evaluated the effect of microbiome manipulation through anti-inflammatory diet alone in sustaining FMT-induced clinical response. Donors also have a very important influence on the success rates of FMT,14 and we have shown previously that in a cohort of healthy individuals, rural individuals had a healthier microbiome than urban individuals,15 which formed the basis for recruitment of rural donors in the present study.
Hence, we planned a unique study design of combining FMT from rural donors along with an anti-inflammatory diet for induction, followed by anti-inflammatory diet alone for maintaining remission in patients with mild-moderate UC.
Methods
Patient population
Patients with mild-moderate UC (Simple Clinical Colitis Activity Index (SCCAI) 3–9), aged 18–65 years, following at the IBD clinic, All India Institute of Medical Sciences (AIIMS), New Delhi, India, were included as per the inclusion and exclusion criteria mentioned in table 1.
Inclusion and exclusion criteria
Study design
This single-centre, prospective, open-labelled RCT randomised patients in 1:1 ratio to FMT and anti-inflammatory diet (FMT-AID) versus optimised standard medical therapy (SMT) arm. Randomisation was held centrally to ensure concealment of allocation. Random numbers were generated by computerised random number schedule (The RAND), and the randomisation list and numbered packing of the intervention was prepared by a person not involved in the study. Randomisation was performed using permuted blocks of 4. Neither the patient nor the investigator giving treatment was blinded. However, endoscopy was done by one investigator, which was then scored by another investigator blinded to the study assignment, and the investigator analysing the data was blinded to the treatment details.
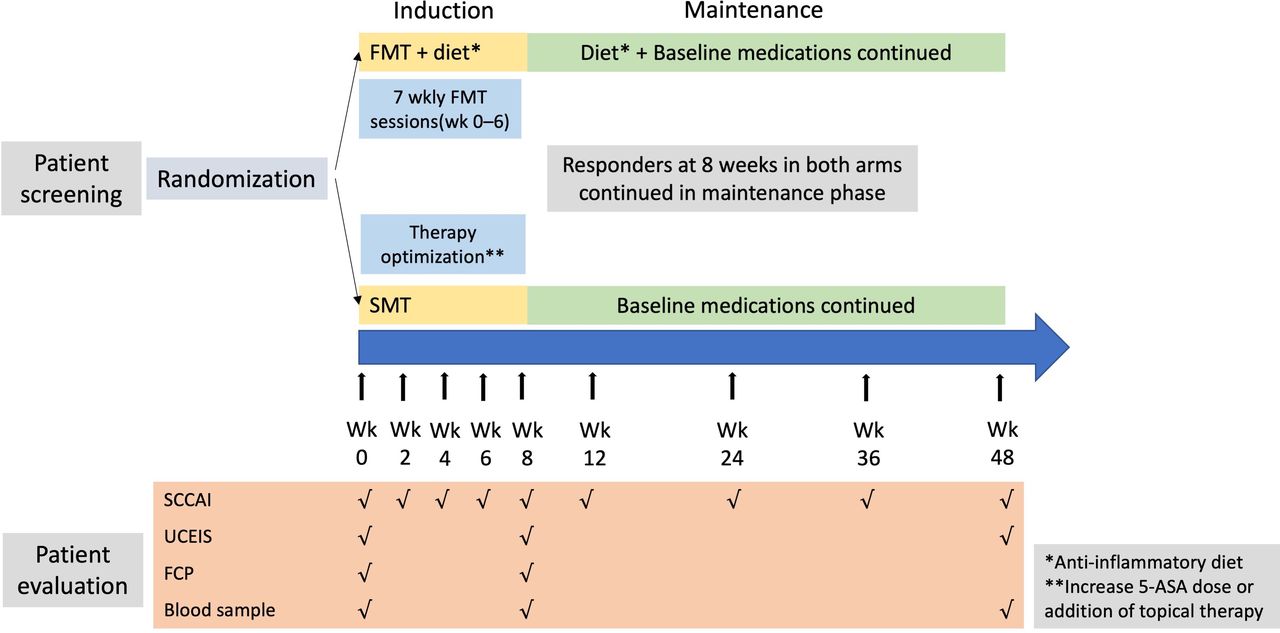
At 8 weeks, patients with clinical response (decline in SCCAI by >3 points) or remission were followed for the next 40 weeks until 48 weeks (figure 1). Patients in the FMT-AID arm continued anti-inflammatory diet in addition to baseline medications, while patients in the SMT arm continued only baseline medications.

Study design for induction and maintenance phase. 5-ASA, 5-aminosalicylic acid; FCP, faecal calprotectin; FMT, faecal microbiota transplantation; SCCAI, Simple Clinical Colitis activity Index; SMT, standard medical therapy; UCEIS, Ulcerative Colitis Endoscopic Index of Severity.
Study duration
Patient enrolment started in September 2019 and was continued until March 2020. However, because of the COVID-19 pandemic and nationwide lockdown which was enforced in last week of March 2020, the trial was withheld until August 2021. No new patient was recruited during this time period, and patients who were ongoing in the trial were followed-up was telephonically (or in person after the lockdown was over) until the trial endpoint was met. The trial was restarted in the month of August 2021 and continued until November 2021. Because of the third wave of the COVID-19 pandemic which started in December 2021, the trial was again withheld in December 2021.
Baseline assessment
All patients underwent a uniform baseline evaluation including clinical, laboratory and endoscopic assessment (see online supplemental methods).
Supplemental material
Intervention and follow-up during induction phase
Faecal microbiota transplantation
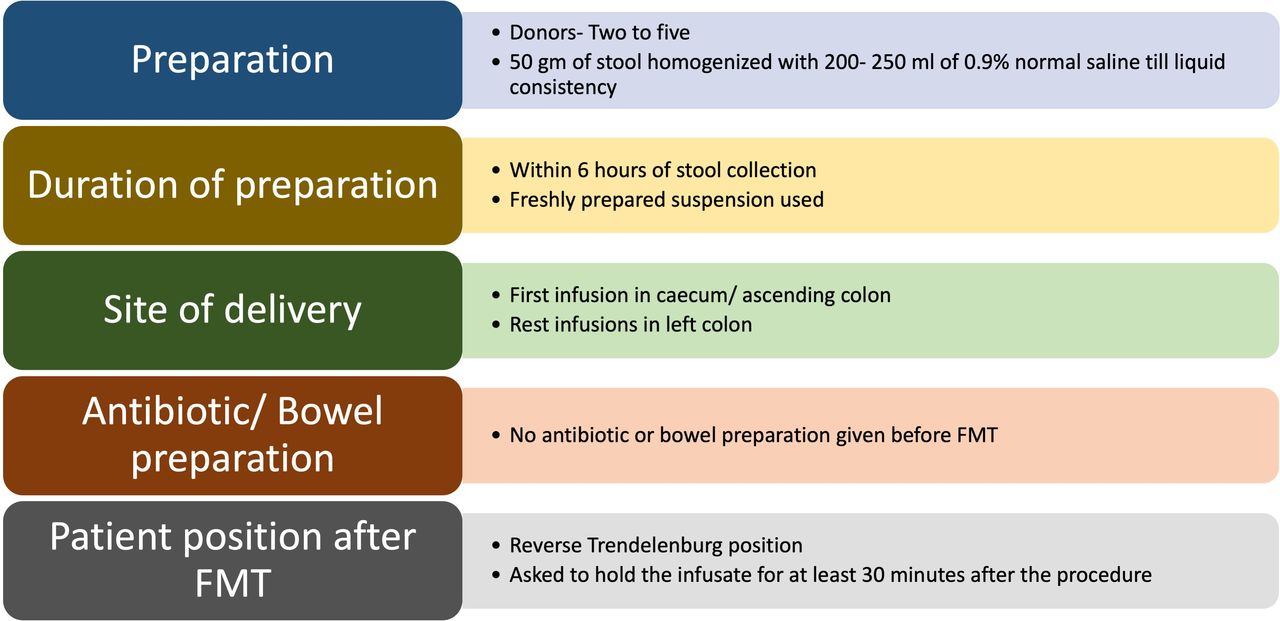
Patients underwent seven weekly sessions (one session per week from week 0 to week 6) of FMT through the colonoscopic route (figure 2). For a few patients, who were recruited immediately before the lockdown (when the trial was withheld), the seven FMT sessions could not be completed. However, these patients were continued in the trial on anti-inflammatory diet. Of these, in three patients, six FMT sessions were completed; in one patient, four FMT sessions were completed; and in two patients, one FMT session was given.

Procedure of faecal microbiota transplantation (FMT).
Donors for FMT
Healthy rural adults between 18 and 45 years were screened through a questionnaire (online supplemental table 1), and those fulfilling the questionnaire underwent stool and blood tests to rule out possible transmissible infections including multidrug-resistant organisms in the stool (through antimicrobial resistant (AMR) gene testing in faecal samples).16 The donors underwent regular screening with the questionnaire and investigations every 12 weeks. When the trial was restarted in August 2021 in addition to the screening measures described above, donors were also screened to rule out COVID-19 infection (see online supplemental methods and online supplemental table 2).
Supplemental material
Diet
Patients in the FMT-AID arm were administered an anti-inflammatory diet (online supplemental table 3a) rich in dietary constituents that expand T-regulatory cells, promote healthy microbiota and improve the intestinal barrier, and poor in dietary constituents that cause dysbiosis or have negative effect on intestinal barrier.17–28 The major diet principles which were followed were avoidance of gluten-based grains,17 dairy products of any kind and margarine (curd was allowed),18 processed and red meat,21 27 food additives,22 23 and refined sugars,27 and increased intake of fresh fruits and vegetables,24 fermented foods, AhR (aryl hydrocarbon receptor) ligand-rich vegetables (cruciferous vegetables)25 and polyphenols (activate AhR).26 However, the evidence on association between majority of food components and proinflammatory or anti-inflammatory effects is mostly derived from preclinical models or epidemiological studies. Patients were prescribed a diet chart accordingly (online supplemental table 3b) and were counselled to adhere to the diet protocol. Regular telephonic interviews were conducted by an IBD dietitian (MF) to ensure compliance to diet. Dietary adherence was assessed as per the flow given in the online supplemental methods.
In addition to FMT and diet, patients were continued on their baseline medications. Those on steroids received a steroid taper of 5 mg every 2 weeks.
Control arm
Patients in the SMT arm were continued on their baseline medications along with optimisation of their therapy, which consisted of increase in 5-aminosalicylic acid (5-ASA) dose and/or addition of topical therapy (topical 5-ASA or topical steroids in those already on topical 5-ASA). The dose of topical steroids was increased in patients on both topical 5-ASA and topical steroids.
Follow-up
Clinical assessment with SCCAI was done at 0, 2, 4, 6 and 8 weeks in both arms. Dietary adherence was assessed at 0, 2, 6 and 8 weeks in the intervention arm (figure 1). Endoscopic assessment was done at baseline and 8 weeks in both arms, and the colonoscopic examination was carried out until the area of most severe inflammation as per the previous colonoscopy. Endoscopic videos were scored by an independent investigator blinded to the study assignment. Blood and stool samples for FCP measurement were collected at 8 weeks.
Intervention and follow-up during the maintenance phase
Clinical responders at the end of 8 weeks were followed at 12, 24, 36 and 48 weeks (figure 1). Clinical disease activity (SCCAI) was assessed at all visits, dietary adherence in the FMT-AID arm was assessed at weeks 12, 24, 36, and 48, and endoscopic assessment was done at 48 weeks.
Study endpoints
The endpoints for study were assessed at 8 weeks for the induction phase and 48 weeks for maintenance phase, or treatment failure if earlier than 8 or 48 weeks. Treatment failure was defined as an increase in SCCAI by >3 points with rectal bleeding score >1, requirement for oral steroids and lack of improvement (decline in SCCAI by <3 points at 4 weeks, for induction phase only). Patients were withdrawn from the study on treatment failure in any arm.
Outcome measures
Primary
The primary outcome measure for induction phase was a combination of clinical (SCCAI <2) and endoscopic (UCEIS <1) remission (deep remission), and the co-primary outcome was clinical response (decline in SCCAI by >3 points) at 8 weeks. The primary outcome measure at 48 weeks was deep remission and maintenance of steroid-free clinical remission (maintenance of clinical remission without any requirement of steroids, and steroid taper in those on steroids at induction).
Secondary
The secondary outcome measures included endoscopic remission and response (decline in UCEIS by 2 points) at 8 weeks, combination of clinical remission and endoscopic response at 8 weeks, clinical remission and response at 24 and 48 weeks, maintenance of steroid-free clinical response at 48 weeks (maintenance of clinical response without any requirement of steroids, and steroid taper in those on steroids at induction), endoscopic remission and response at 48 weeks, and adverse events at 12 and 48 weeks. Adverse events were assessed according to common criteria for adverse events (CTCEA) (online supplemental methods).
Statistical analysis
Sample size
For the induction trial, the sample size was based on 28% endoscopic remission rate, as reported in previous studies on 5-ASA dose escalation in patients with UC who relapsed or had active disease on standard dose 5-ASA.29 Assuming 25% higher remission rates in the FMT-AID arm, with 90% power, alpha of 0.05 and drop-out rate of 10%, a total of 150 patients would be required for the desired outcome. However, due to slow recruitment because of the COVID-19 pandemic, the trial stopped recruiting patients in December 2021.
Sample size calculation for maintenance phase was not done as no study exists on the role of diet in the maintenance of FMT-induced clinical response. We also expected different numbers at the end of induction phase in both arms, which precluded us from sample size calculation.
The continuous variables were expressed as mean±SD or median (IQR) depending on normal or non-normal distribution, and categorical variables were expressed as percentages. Continuous variables were compared with Student’s t-test or Mann Whitney U test, and categorical variables were compared with χ2 test or Fisher’s exact test (for values<5). Pairwise comparison between baseline and week 8 continuous variables was done with Wilcoxon rank-sum test, and for categorical variables with McNemar’s test. A p value<0.05 was considered as statistically significant. All statistical analysis was performed with SPSS statistical software (V.28).
A modified intention-to-treat analysis (mITT) was performed, and patients who received even a single session of FMT in the intervention arm, or treatment optimisation in the control arm, were included. Patients who withdrew from the trial before 8 weeks due to treatment failure were considered as clinical as well as endoscopic non-responders. Of patients with treatment failures in the FMT-AID arm, six discontinued FMT before seven sessions at a median of three (two to four) sessions (online supplemental table 4). For patients whose endoscopy at 8 weeks could not be done during the lockdown, the following protocol was followed: Patients without any further endoscopy (either in the FMT arm or the SMT arm) were excluded from analysis of endoscopic and composite outcomes. For patients in the FMT arm, whose FMT sessions were withheld before seven sessions before the lockdown, the last endoscopic score was carried forwards at 8 weeks (online supplemental table 4).
Donor microbiome and metabolite analysis
The details on donor microbiome and metabolite analysis have been mentioned in online supplemental methods.
Patient and public involvement statement
Patient and public involvement was not included in the design and conduct of the research.
Results
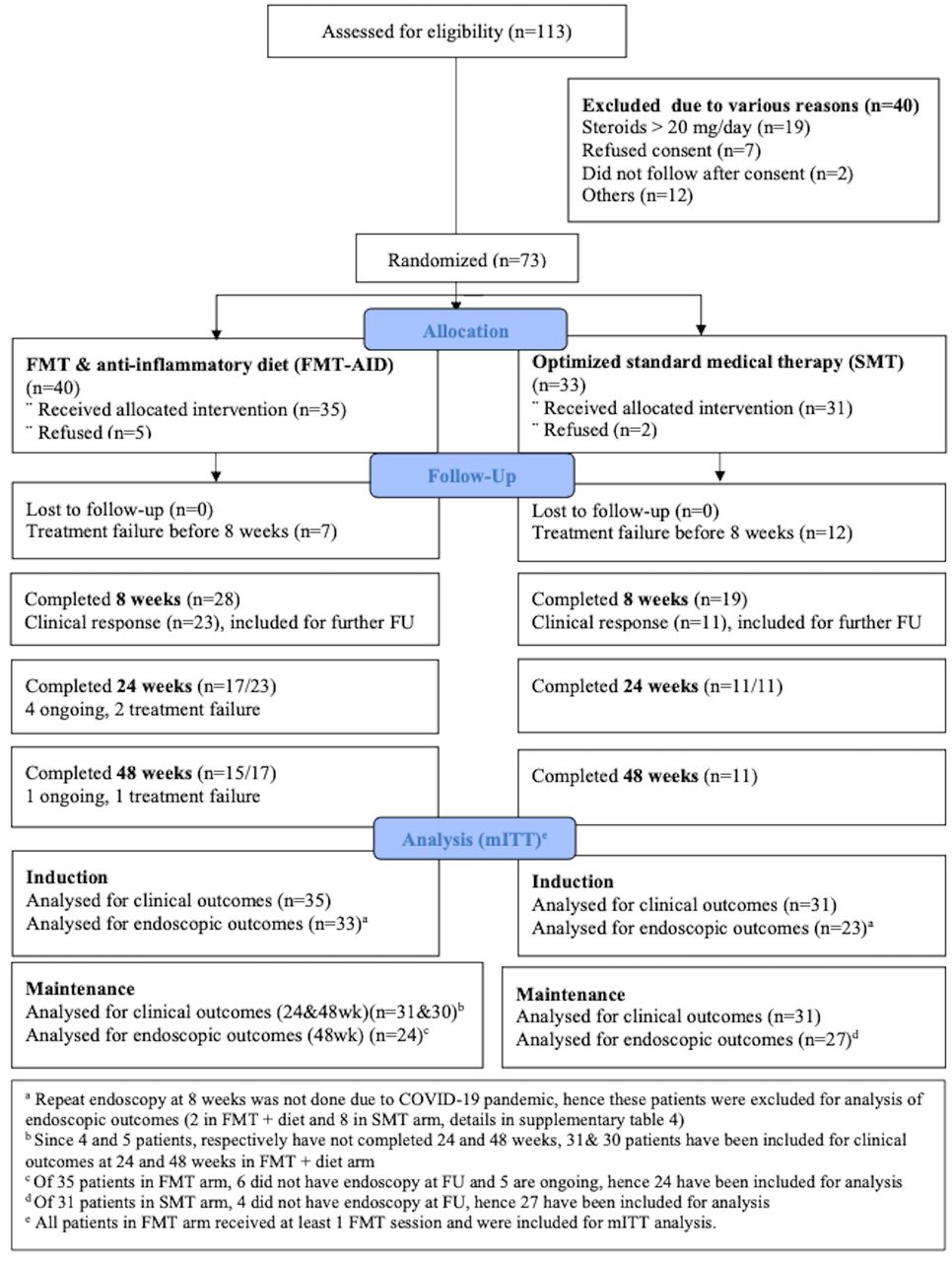
A total of 113 patients were screened for eligibility, of which 40 were excluded due to various reasons (figure 3), and 73 were randomised (40 in the FMT-AID arm and 33 in the SMT arm). After randomisation, 5 patients in the FMT-AID arm and 2 patients in the SMT arm withdrew consent and were excluded; finally, 35 and 31 patients were considered for mITT analysis, respectively.

CONSORT (Consolidated Standards of Reporting Trials) chart of the study. FMT, faecal microbiota transplantation; FMT-AID, faecal microbiota transplantation with anti-inflammatory diet; FU, follow-up; SMT, standard medical therapy.
Baseline clinical, demographic, laboratory and endoscopic characteristics
The mean age of the entire cohort was 35.7±11.1 years, 60.1% patients were male, median disease duration was 48 (IQR 24–84) months and 34.8% patients had pancolitis. The median SCCAI and UCEIS at enrolment were 6 (IQR 5–7) and 4 (IQR 3–5), respectively.
Baseline characteristics were comparable between the FMT-AID and SMT arms (table 2). The use of concomitant and previous medications was also similar (table 2). Only 3 (8.6%) and 2 (6.5%) patients in the FMT-AID and SMT arms were on oral steroids at enrolment, respectively (table 2). Five patients in each group were steroid naïve. For patients in the SMT group, the treatment was optimised as follows: topical steroid was added in 4 patients, topical 5-ASA with topical steroid was added in one patient, and dose of topical steroid was increased in 26 patients.
Comparison of baseline clinical, demographic, endoscopic and laboratory characteristics between patients who received FMT-AID versus those who received optimised SMT
Patients continued on their baseline medications until 8 and 48 weeks, no patient required oral steroids, and there was no change in medication intake until last follow-up (online supplemental table 5).
Donor selection
Thirty-six potential rural donors were screened with donor personal interview and health questionnaires. Subsequently, 20 donors passed the questionnaire, of which 13 were finally selected (online supplemental figure 1). No donor carried AMR gene in the stool sample (online supplemental figure 2). The stool from these donors were pooled for preparation of faecal infusate, and the number of donors pooled varied from 2 to 5 (online supplemental table 6).
Supplemental material
Supplemental material
Baseline, 8 weeks and 48 weeks dietary intake
The dietary intake at baseline in terms of macronutrients, different food groups and micronutrients was comparable (table 3), except for significantly lower intake of wheat, insoluble fibre and thiamine in the FMT-AID group. At 8 weeks, the FMT-AID group had a significantly higher intake of curd, AhR ligand-rich foods, fermented foods and ascorbic acid, and a significantly lower intake of energy, total fat, milk and milk products, processed foods, thiamine, pantothenic acid, biotin, iron and sulphated amino acids than the SMT group (table 3). However, when compared with baseline, at 8 weeks, there was a significant decline only in the intake of total fat, wheat, milk and milk products, processed foods, sulphated amino acids, and an increase in intake of ascorbic acid, curd and total polyphenols (online supplemental table 7). The intake of other vitamins and minerals was comparable. The intake of total fibre was less in the FMT-AID group than the SMT group at baseline and 8 weeks, although the difference was not statistically significant (table 3), while that between baseline and 8 weeks in both groups was similar (online supplemental table 7). The soluble fibre intake was similar between the two groups at baseline and 8 weeks (table 3), and between baseline and 8 weeks in both groups (online supplemental table 7). However, the ratio of soluble fibre to energy intake was significantly high in the FMT-AID group at 8 weeks, in comparison with both baseline intake and SMT group at 8 weeks (p<0.001 for both). At 48 weeks, the dietary differences between FMT-AID and SMT arms and between FMT-AID arm at baseline and 48 weeks was similar to that observed at 8 weeks, except for minor differences (online supplemental table 8).
Comparison of dietary intake at baseline and 8 weeks between patients who received FMT-AID versus those who received optimised SMT
The intakes of energy, protein, fat and micronutrients with respect to recommended daily allowance has been mentioned in the online supplemental table 9.
Adherence to diet at 8 and 48 weeks
Qualitative adherence
At 8 weeks, 84.6% patients were highly adherent, and 15.4% patients were moderately adherent. At 48 weeks, 66.7% patients were highly adherent, and 33.4% patients were moderately adherent.
Quantitative adherence
The adherence to individual food groups at 8 and 48 weeks is mentioned in the online supplemental table 10. At 8 weeks, 65.4% patients were highly adherent, and 34.6% patients were moderately adherent. At 48 weeks, 64.2% patients were highly adherent, and 35.8% patients were moderately adherent. No patient was poorly adherent or non-adherent throughout the study duration. The average high (>80%) adherence to prohibited food groups at 8 and 48 weeks was 92.3% and 71.4%, respectively.
Efficacy outcomes 8, 24 and 48 weeks (mITT analysis)
All patients were assessed for clinical outcomes at 8 weeks. Thirty-three and twenty-three patients in the FMT-AID and SMT arms were assessed for endoscopic and composite outcomes, respectively, as 2 and 8 patients in the FMT-AID and SMT arms did not have repeat endoscopy due to the COVID-19 pandemic (online supplemental table 4).
Outcomes at 8 weeks
Clinical outcomes
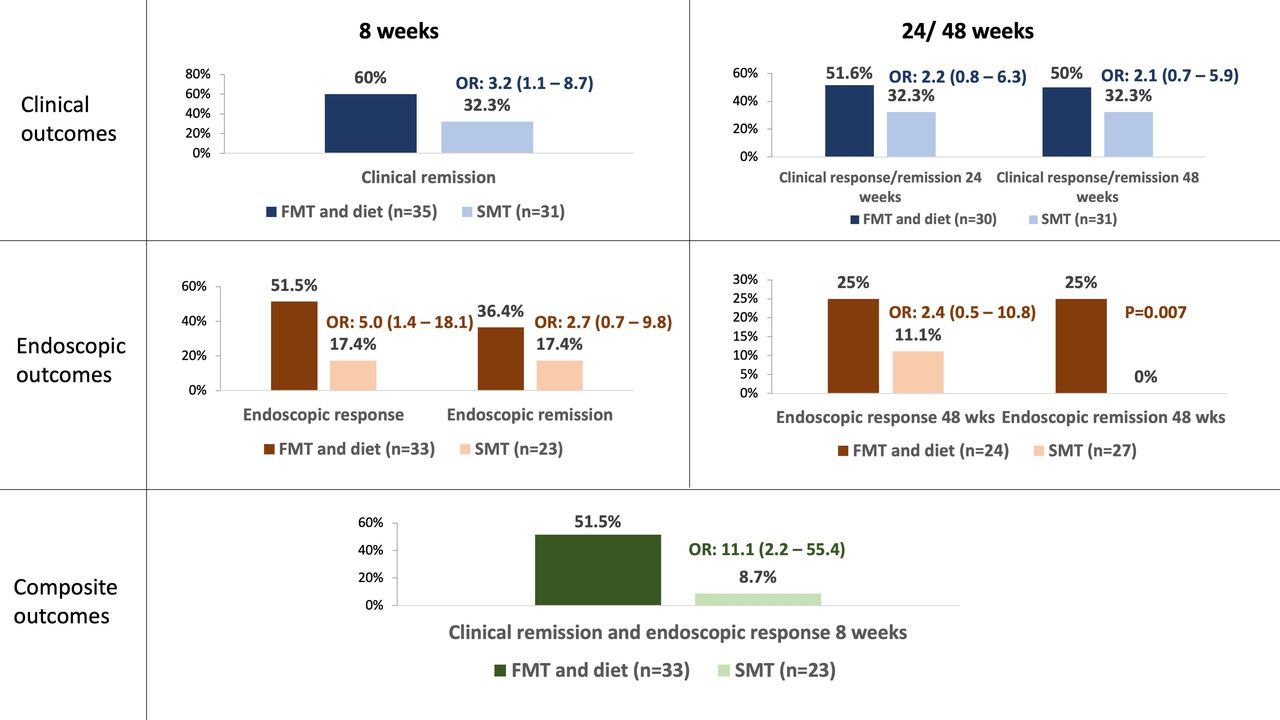
Both clinical response (23/35 (65.7%) vs 11/31 (35.5%), p=0.01, OR 3.5 (95% CI 1.3 to 9.6)) and clinical remission (21/35 (60%) vs 10/31 (32.3%), p=0.02, OR 3.2 (95% CI 1.1 to 8.7)) were significantly high in the FMT-AID arm than the SMT arm (figure 4 and table 4).

Comparison of primary outcomes at 8 and 48 weeks between patients who received faecal microbiota transplantation and anti-inflammatory diet (FMT-AID) versus those who received optimised standard medical therapy (SMT).
Comparison of 8 weeks’ outcomes between patients who received FMT-AID versus those who received optimised SMT
Endoscopic outcomes
The endoscopic response was significantly higher in the FMT-AID arm (17/33 (51.5%) vs 4/23 (17.4%), p=0.012, OR 5.0 (95% CI 1.4 to 18.1)). Although endoscopic remission was also higher, difference was not statistically significant (12/33 (36.4%) vs 4/23 (17.4%), p=0.15, OR 2.7 (95% CI 0.7 to 9.8)).
Composite outcomes
Deep remission (12/33 (36.4%) vs 2/23 (8.7%), p=0.03, OR 6.0 (95% CI 1.2 to 30.2)) (figure 4) and a combination of clinical remission and endoscopic response were also significantly high in the FMT-AID arm (17/33 (51.5%) vs 2/23 (8.7%), p=0.001, OR 11.1 (95%CI 2.2 to 55.4)).
Biomarker outcomes
Twenty and ten patients in the FMT-AID and SMT arms, respectively, had paired FCP samples at baseline and 8 weeks. Although the median FCP at 8 weeks was comparable, the delta FCP (change from baseline to week 8 FCP) and proportion of patients with FCP <50 μg/g was higher in the FMT-AID arm, although the difference was not statistically significant (table 4). Because of dropouts due to the COVID-19 pandemic, more patients with FCP results available in the SMT arm had a clinical response than the entire cohort (6/10 (60%) vs 11/31 (35.5%)).
Outcomes at 24 and 48 weeks
Clinical outcomes
Twenty-three clinical responders in the FMT-AID arm and 11 in the SMT arm entered the maintenance phase. Of 23 patients in the FMT-AID arm, 17 and 15 patients completed 24 and 48 weeks follow-up (FU), respectively, of which 16 and 15 patients were in clinical response/remission. Hence, overall clinical remission/response at 24 and 48 weeks was 51.6% (16/31) and 50% (15/30), respectively (4 and 5 patients, respectively, are ongoing, have not completed 24 and 48 weeks FU).
In the SMT arm, all 11 patients completed 24 and 48 weeks FU. Overall clinical remission and response rate at 24 and 48 weeks was 32.3% (10/31).
Although the clinical response and remission at 24 and 48 weeks were higher in the FMT-AID arm, the difference was not statistically significant (figure 5 and table 5). Overall, three and one patients in the FMT-AID and SMT arm relapsed by 48 weeks, respectively.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comparison of secondary outcomes at 8 and 48 weeks between patients who received faecal microbiota transplantation and anti-inflammatory diet (FMT-AID) versus those who received optimised standard medical therapy (SMT).
Comparison of 24 and 48 weeks’ outcomes between patients who received FMT-AID versus those who received optimised SMT
Endoscopic outcomes
Endoscopic outcomes at 48 weeks could be assessed for 24 patients in the FMT-AID arm and 27 patients in the SMT arm (online supplemental table 4). Six patients were in endoscopic remission at 48 weeks in the FMT-AID arm, and none in the SMT arm (6/24 (25%) vs 0/27, p=0.007). Of the 12 patients in endoscopic remission at 8 weeks, outcomes were available for 7 patients at 48 weeks, of which 4 maintained endoscopic remission (55.5%). Although endoscopic response was also higher in the FMT-AID arm, the difference was not statistically significant (6/24 (25%) vs 3/27 (11.1%), p=0.28).
Composite outcomes
The result for deep remission at 48 weeks was similar to endoscopic outcome and was significantly higher in the FMT-AID arm (6/24 (25%) vs 0/27, p=0.007).
Steroid-free clinical remission and response at 48 weeks were similar to clinical remission and response, as only five patients were on steroids at enrolment and all could taper steroids before 8 weeks. No patient who had remission or response at 48 weeks required steroids.
On sensitivity analysis (by considering patients with incomplete FMT sessions (due to pandemic) as treatment failures or excluding them) of endoscopic and composite outcomes at 8 and 48 weeks, the trend and statistical significance of results was similar to outcomes presented above. However, the proportion of patients with FCP <50 μg/g at 8 weeks became significantly higher in the FMT-AID arm on sensitivity analysis (online supplemental table 11).
Adverse events
The overall adverse events at 8 weeks were similar between FMT-AID and SMT arms (26 (74.3%) vs 27 (87.1%), p=0.19) (table 6). All adverse events were grade 1 or 2 according to CTCAE. Common adverse events were mild pain abdomen, bloating/flatulence, diarrhoea and worsening of disease activity. No patient had any serious adverse event including hospitalisation or death. Beyond 8 weeks, no new safety signals were reported and no serious adverse event was observed in patients who continued follow-up until 48 weeks.
Comparison of adverse events at 8 weeks between patients who received FMT-AID versus those who received optimised SMT
Predictors of response to FMT
More patients who had clinical remission in the FMT-AID arm had mild disease severity (16/21 (76.2%) vs 5/14 (35.7%), p=0.02, OR 5.7 (95% CI 1.3 to 25.4)) and left-sided colitis (15/21 (71.4%) vs 7/14 (50%), p=0.19, OR 2.5 (95% CI 0.6–10.3)). Median FCP (309 (281– 476) vs 479.6 (336.9–538.7) μg/g, p=0.15, OR 0.99 (95% CI 0.99 to 1.0)) and past immunomodulator use (47.6% vs 78.6%, p=0.07, OR 0.25 (95% CI 0.059to 1.2)) was also lower in patients with clinical remission, although the difference was not statistically significant. All patients who were steroid naïve had clinical remission. There was no difference in other parameters (table 7), and baseline or 8 weeks dietary intake (online supplemental table 12). Because we used multiple donors per pool for FMT, the donor effect could not be precisely evaluated. However, with a 2×2 contingency table approach, donors 3, 10, 11 and 13 were associated with significantly better response (online supplemental table 13).
Clinical predictors of induction remission to faecal microbiota transplantation and anti-inflammatory diet at 8 weeks
Donor microbiome analysis
The β diversity index on permutational multivariate analysis of variance (PERMANOVA) test was significantly different between the donors associated with better response than other donors (online supplemental figure 3). Analysis of differentially abundant bacteria revealed significant enhancement of beneficial bacterial members such as Eubacterium rectale, Dorea, Roseburia, Faecalibacterium prausnitzii, Blautia, Bifidobacterium, etc, in donors associated with significantly better response, while other donors had an enhanced abundance of pathobionts such as Enterococcus, Haemophilus parainfluenzae, Acinetobacter, Pseudomonas, Veillonella, etc (online supplemental figure 4). The principal component analysis biplot strengthened the positive co-occurrence patterns between the beneficial bacteria listed above with the beneficial donors and their faecal butyrate levels (online supplemental figure 5).
Supplemental material
Supplemental material
Supplemental material
Discussion
FMT from rural donors with an anti-inflammatory diet was more effective than the optimised SMT in inducing clinical and deep remission in patients with mild-moderate UC. Deep remission at 48 weeks was also significantly better in the FMT-AID arm, suggesting that anti-inflammatory diet could sustain the FMT-AID-induced endoscopic and clinical remission. FMT was safe and no serious adverse events were reported. The minor adverse events were similar to that reported by other RCTs.13 30–33
The major strength of our study was a unique protocol combining two microbiome manipulation strategies: FMT and diet. While both were used for induction of remission, the effect was maintained only with diet, which adds novelty to the study design. Moreover, it also makes the approach more acceptable and practical for patients as they can practise the modified diet at home and avoid hospital visits for repeat FMTs. The adherence to modified diet was maintained until 48 weeks, suggesting the acceptability of this approach to patients. This is the first induction RCT on FMT from Asia, which represents an ethnically different population, and where the disease burden of IBD is rising.4 5 Moreover, the study also provides a low cost, safe alternative for IBD physicians in resource-limited settings. Although FMT was more efficacious in steroid naïve patients with relatively mild disease severity, patients with steroid-dependent disease and immunomodulator experienced patients also responded.
There are certain other novel findings. The study design was different from previous RCTs, as the comparator arm here was optimisation of medical therapy, rather than a true placebo, while, except for one, previous RCTs have either included placebo or autologous FMT as a comparator arm.13 30–34 This accounted for relatively higher clinical/endoscopic remission and response rates in the comparator arm compared with previous RCTs (which reported positive results with FMT). These results are in contrast to a recent three-arm RCT which compared FMT, FMT and diet, and diet alone in patients with mild-moderate refractory UC (CRAFT-UC trial).13 Patients who received only diet had the best outcomes as compared with FMT arms, which reported outcomes equivalent to placebo arms of successful RCTs. Possible reasons for discrepancy between ours and the CRAFT-UC trial could be due to differences in patient population and FMT protocol. Only two patients in our study had received biologics, and only 7.5% patients were on steroids at enrolment, in contrast to the CRAFT-UC study, where about 30% patients were on steroids, 35% patients were on biologics and 55% patients were refractory to biologics, indicating a more aggressive and refractory patient population. Regarding FMT protocol, we used multiple donors and seven FMT sessions over 6 weeks, while in the CRAFT-UC study, single donor with three FMT sessions (one colonoscopic, and two 100 mL enemas on days 0, 2 and 14) were used, indicating a relatively more intense FMT protocol spread over a longer duration in our study. The recently published LOTUS trial was also terminated prematurely due to the COVID-19 pandemic, and it reported results similar to our study.33
In the present study, 15 out of 18 responders at 8 weeks maintained clinical remission and response until 48 weeks, and 6 were in deep remission. The maintenance response rate in the present study is quite high as compared with the non-FMT maintenance arm of the LOTUS trial, possibly due to the effect of modified diet. Similarly, in the other induction RCTs, patients who sustained remission for or beyond 12 months either resumed FMT or modified their diet.33 35 In a maintenance RCT of FMT versus placebo, although eight weekly FMT led to better steroid-free clinical remission (statistically insignificant), endoscopic and histological remission than placebo, two-thirds of patients in the placebo arm also maintained clinical remission until 48 weeks, against other studies in which no maintenance microbial manipulation was practised.36 However, in this study, induction duration was prolonged until 22 weeks, which could have accounted for this discrepant effect. In another case series from India, majority of responders relapsed at a median of 14.8 months after induction FMT, and the relapse duration was shorter in patients who did not receive maintenance FMT.37
The dietary intake at baseline was comparable between the two groups, while at 8 weeks, in the FMT-AID group, diet was significantly different from baseline in terms of recommended (curd, AhR ligand-rich foods, fermented foods and polyphenols) and prohibited food items and nutrients (milk, processed foods, wheat, total fat and sulfated amino acids). The intake of soluble fibre was comparable both at baseline and 8 weeks, possibly due to the high fibre content of regular Indian diet,38 39 and the non-vegetarian food intake was also minimal in both groups because of the mixed diet pattern of most patients. The anti-inflammatory diet tried to promote the soluble fibre intake, as evidenced by higher ratio of soluble fibre to total energy intake in the FMT-AID arm. The intake of soluble fibre was promoted to increase short chain fatty acids which are fuel for the intestinal epithelial cells, enhance the gut barrier and modulate the gut immunological environment,24 while the food texture was softened to limit insoluble fibre. In addition to increasing fibre intake, we also restricted proinflammatory diet such as dairy, gluten, red meat and processed food, and increased intake of fermented foods and AhR ligand-rich foods which could also have led to clinical benefit.
Although the intake of some macro (fat and protein) and micronutrients was less in the FMT-AID arm than the SMT arm at 8 weeks, the average energy and protein intake was more than 80% of recommended daily allowance (online supplemental table 9). Further, when compared with baseline, although the total fat intake in the FMT-AID arm was less at 8 weeks, which could have accounted for reduction in total calories, the intake of other macronutrients and micronutrients (except ascorbic acid which was higher) was similar to baseline (online supplemental table 7). Like our study, a recent study on UC exclusion diet in children with active UC also showed reduction in total energy and fat intake at 8 weeks.40 The patients in our study did well and there was no evidence of malnutrition in any patient.
Disease severity was a significant predictor of response to FMT. Other statistically non-significant factors predicting response were low baseline FCP, disease extent (left-sided colitis) and past immunomodulator use (lesser in responders). Interestingly, all steroid naïve patients responded to FMT. Similar findings were corroborated in two recent studies from India,37 41 while results on predictors in other RCTs have been heterogeneous. Similar to the study by Costello et al, we also could not find any association between baseline diet and response to FMT.30 We used rural donors for FMT based on our previous observation that rural healthy donors have a better gut microbiome signature. However, we could not demonstrate the superiority of rural donors in this study due to lack of a control arm with different types of donors. Further, because of donor pooling, we could not precisely evaluate the donor effect, although few donors demonstrated superiority over others.
The study also has some limitations. We did not include a placebo and it was an open-labelled trial which could influence clinical outcomes. However, the endoscopic videos were scored by an independent investigator blinded to the study assignment. We could not achieve the desired sample size due to suspended recruitment during COVID-19-related restrictions. However, even with the limited numbers our primary outcomes were met, and we could demonstrate definite superiority of FMT and diet over optimised SMT. Although we demonstrated clinical and endoscopic response at 8 weeks, the FCP-based response was not significant. This discrepancy arose due to limited number of faecal samples available for FCP analysis at 8 weeks. However, even with these numbers the delta FCP and proportion of patients with FCP <50 μg/g was higher in the FMT-AID arm, although the difference was not statistically significant (table 4). Further on sensitivity analysis, the FCP response became significantly higher in the FMT-AID arm. Similar to FCP, the COVID-19 pandemic also restricted the endoscopy at 8 weeks. However, we controlled for this by carrying forward the latest available UCEIS (according to the last FMT session) in the FMT arm. A sensitivity analysis considering patients with absent endoscopy as treatment failure also demonstrated significant deep remission at 8 weeks and did not affect the overall results of study. The ‘superdonor’ effect could not be evaluated because of the pooled donor protocol. Although we combined diet with FMT, absence of FMT alone and diet alone arms precluded us to evaluate the individual effect of diet or FMT on microbiome or disease activity. Although we demonstrated a beneficial role of anti-inflammatory diet, there is heterogeneity with respect to dietary constituents and their proinflammatory or anti-inflammatory effects, which requires further work. A typical example would be exclusive enteral nutrition which has demonstrated the best efficacy in IBD, yet is devoid of fibre and contains additives, adding to the uncertainty for the role of specific dietary components in IBD activity.42 Although on quantitative analysis high dietary adherence was present in 65% patients, as per qualitative analysis, 84.6% and 66.7% patients were highly adherent at 8 and 48 weeks. Further, on quantitative analysis, adherence was more than 90% and 70% for excluded food items, and the intake of recommended food items (AhR ligand-rich food and curd) was significantly higher at 8 and 48 weeks. Adherence rates in our study match the CRAFT-UC trial13 and a recent RCT comparing Mediterranean diet with specific carbohydrate diet in CD.43 Hence, we believe that the adherence rates in our study were reasonable and in agreement with published literature. Moreover, we have used two methods to assess adherence, which adds strength to the study.
To conclude, a combination of FMT and anti-inflammatory diet was effective in inducing clinical and endoscopic remission in patients with mild-moderate UC. Further, continuation of anti-inflammatory diet alone was effective in maintaining the clinical and endoscopic remission in these patients.
Supplemental material
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by AIIMS ethics committee (ethics number: IEC/51/1/2019). Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors SK: Data curation, data analysis and manuscript writing and editing. SV: Data collection, data analysis and manuscript editing. SK, PK, BK, PS, KK, KS, PD, GKM: Manuscript review and editing. MF: Diet data collection, curation and analysis. MKS, MV: Sample collection, storage, and manuscript review and editing. AB, MM: Microbiome analysis. VA: Study concept and design, funding acquisition, study supervision, data analysis,manuscript writing, editing and guarantor of the article.
Funding Indian Council of Medical Research: Center for Advanced Research and Excellence in Intestinal Diseases awarded to Professor Vineet Ahuja (grant number: 55/4/11/CARE-ID/2018-NCD-II).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.