Article Text

Abstract
Introduction Over-the-scope clip (OTSC) has been used recently for primary haemostasis of peptic ulcers. This study aimed to compare the efficacy of OTSC to standard endoscopic therapy in primary treatment of patients with peptic ulcer bleeding that are of size ≥1.5 cm. The target population accounts for only 2.5% of all upper GI bleeders.
Methods This was a multicentre international randomised controlled trial from July 2017 to October 2020. All patients with Forest IIa or above peptic ulcers of ≥1.5 cm were included. Primary outcome was 30-day clinical rebleeding. Secondary endpoints include 3-day all-cause mortality, transfusion requirement, hospital stay, technical and clinical success, and further interventions. 100 patients are needed to yield a power of 80% to detect a difference of −0.15 at the 0.05 significance level (alpha) using a two-sided Z-test (pooled).
Results 100 patients were recruited. Success in achieving primary haemostasis was achieved in 46/50 (92%) and 48/50 (96%) in the OTSC and conventional arm, respectively. Among patients who had success in primary haemostasis, 2/46 (4.35%) patients in the OTSC arm and 9/48 (18.75%) patients in the conventional arm developed 30-day rebleeding (p=0.03). However, in an intention-to-treat analysis, there was no difference in rebleeding within 30 days (5/50 (10%) OTSC vs 9/50 (18%) standard, p=0.23) or all-cause mortality (2/50 (4%) OTSC vs 4/50 (8%) standard, p=0.68; OR=2.09, 95% CI 0.37 to 11.95). There was also no difference in transfusion requirement, hospital stay, intensive care unit admission and further interventions.
Conclusion The routine use of OTSC as primary haemostasis in large bleeding peptic ulcers was not associated with a significant decrease in 30-day rebleeding.
Trial registration number NCT03160911.
- gastrointestinal bleeding
- endoscopy
- bleeding peptic ulcer
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Over-the-scope clip (OTSC) has been shown to decrease recurrent bleeding in 7 days for refractory peptic ulcer bleeding in a randomised controlled trial setting. However, its efficacy as primary haemostasis has yet to be determined.
WHAT THIS STUDY ADDS
This is the first randomised controlled trial using OTSC as primary haemostasis for high-risk bleeding peptic ulcers ≥1.5 cm. It showed that the routine use of OTSC as primary haemostasis cannot decrease 30-day rebleeding in large bleeding peptic ulcers.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This study showed that the routine use of OTSC as primary haemostasis cannot decrease 30-day rebleeding in large bleeding peptic ulcers. However, there may be a role of OTSC in expert hands where OTSC can be successfully applied. It also highlighted that there is a learning curve to the use of OTSC and that salvage after a misplaced OTSC could be challenging.
Introduction
Acute upper GI bleeding is a common and potentially life-threatening condition. Non-variceal bleeding accounts for more than 80%–90% of the cause with gastroduodenal peptic ulcer being the major cause.1 2 Endoscopic haemostasis has significantly improved the outcome of these patients.3 4 Despite acid suppression and endoscopic treatment, 10%–20% of patients continue to bleed or develop rebleeding.5 Recurrent bleeding remains one of the most important predictors of mortality.6 7 Therefore, it is important to improve methods for endoscopic haemostasis in the high-risk group to prevent rebleeding and thus mortality.
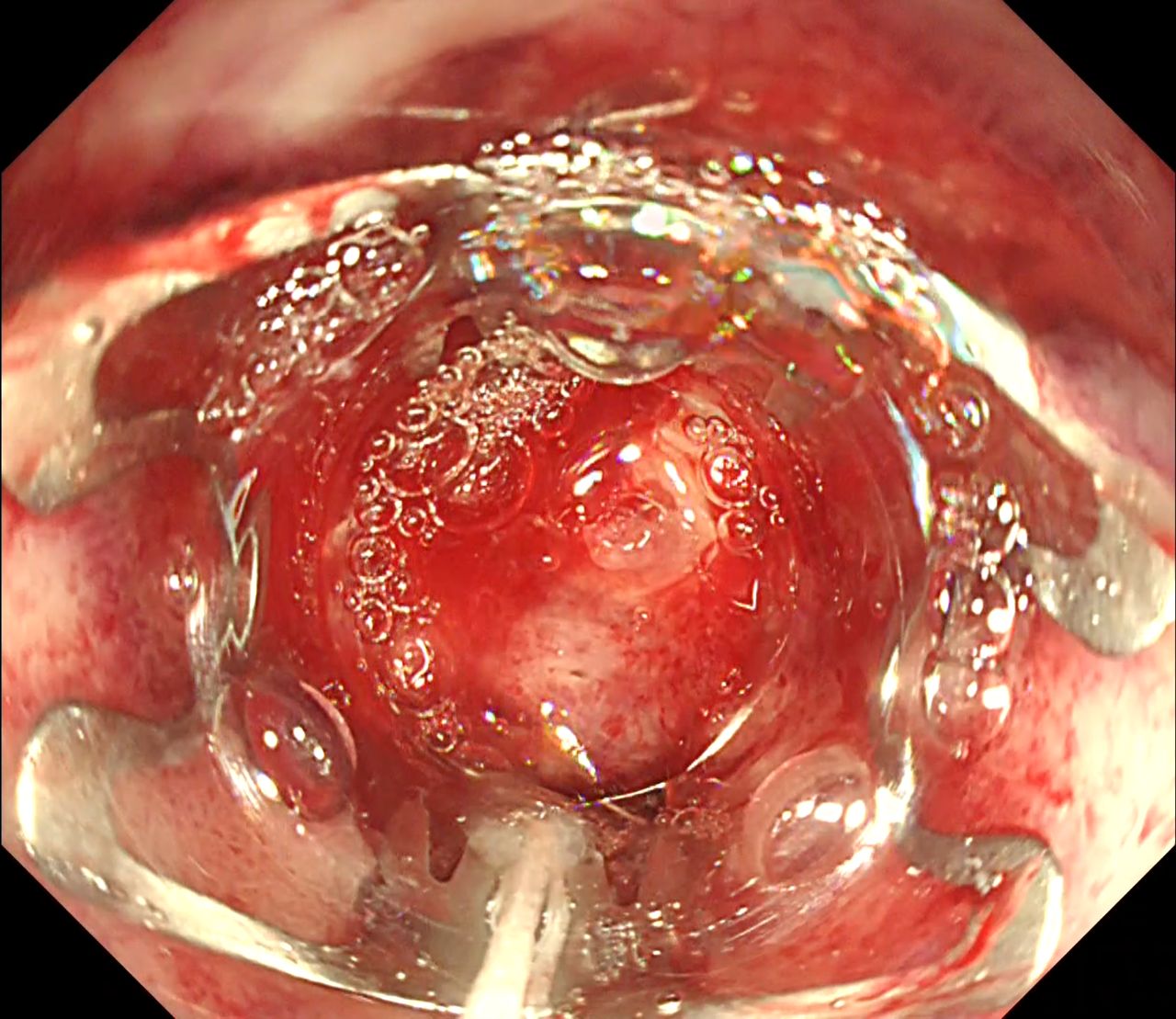
Conventionally, endoscopic haemostasis is achieved by injection therapy, thermocoagulation or mechanical therapy such as haemostatic clips. It is currently recommended in international consensus guidelines to combine at least two techniques for haemostasis in peptic ulcer bleeding.8–10 However, there are limitations to thermocoagulation and conventional haemostatic clips. Application of clips can also sometimes be difficult in chronic ulcers with fibrotic bases. A novel endoscopic clipping device, the over-the-scope clip (OTSC; Oversco Endoscopy AG, Tübingen, Germany), has become available (figure 1). The device provides strong tissue apposition with a larger jaw width and greater strength. In an ex vivo porcine model, the efficacy of OTSC was shown on a validated bleeding model to be superior to other clips.11 Initial case series on OTSC for recurrent peptic ulcer bleeding showed encouraging results,12–17 with rebleeding rates ranging from 0% to 22%. However, data on the use of OTSC on primary haemostasis of peptic ulcers are lacking. In a subgroup analysis of a randomised controlled trial, prophylactic transarterial embolisation (TAE) to peptic ulcers with a size of ≥1.5 cm decreased 30-day rebleeding rate when compared with standard therapy alone.18 In that study, the 30-day rebleeding rate for conventional arm without TAE was up to 23%.18 Therefore, the aim of this study was to compare the efficacy of the OTSC as primary haemostasis to standard therapy in this particular high-risk group of ulcers with a size of ≥1.5 cm. According to these inclusion criteria, the target population accounts for only 2.5% of all upper GI bleeders.

An OTSC being applied over a visible vessel at first part of duodenum. OTSC, over-the-scope clip.

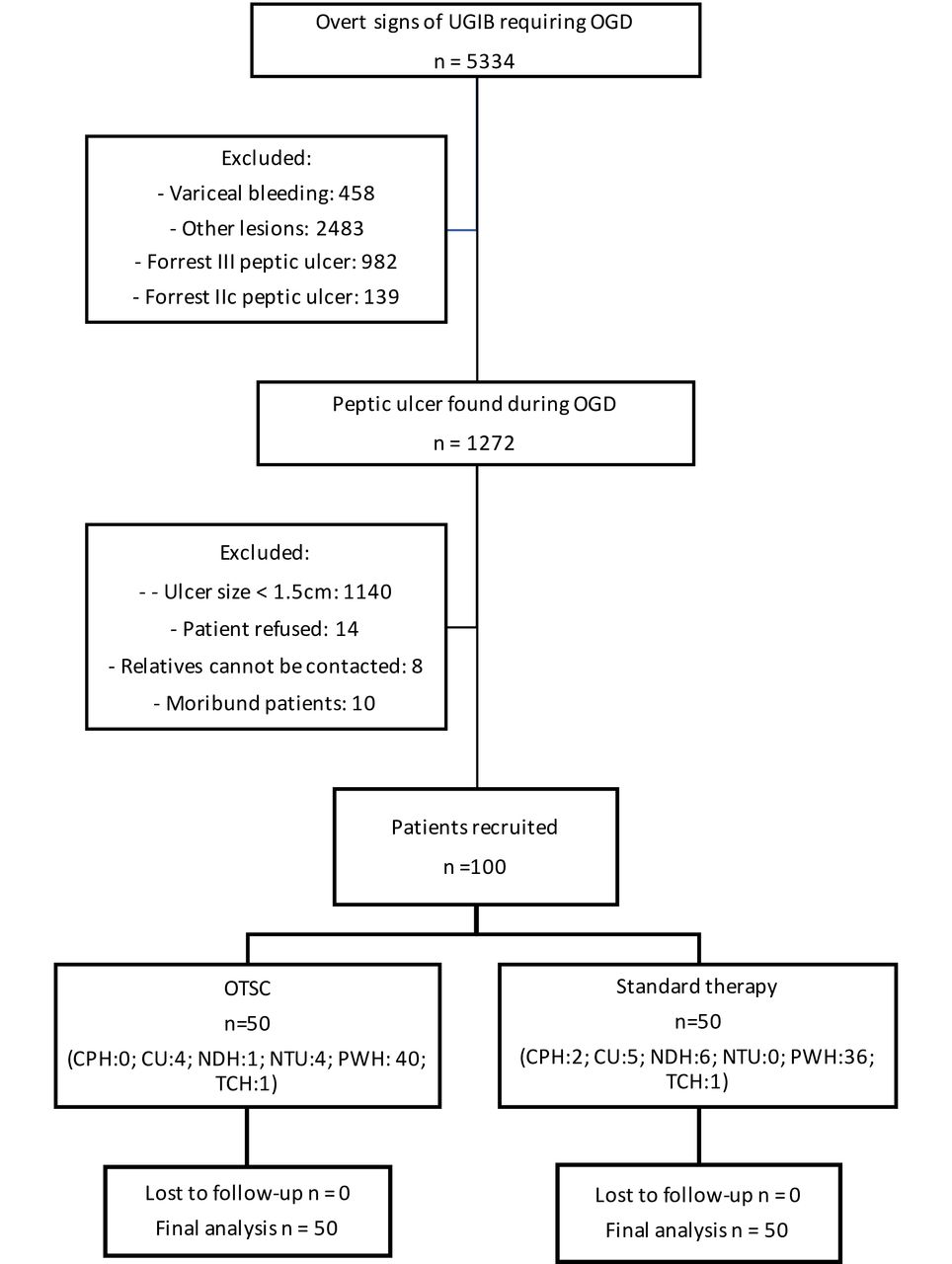
Consolidated Standards of Reporting Trials diagram. CPH, ChengDu 2nd people’s Hospital; CU, Chulalongkorn University; NDH, North District Hospital; NTU, National Taiwan University; PWH, Prince of Wales Hospital; TPH, Taipei Tzu Chi Hospital.

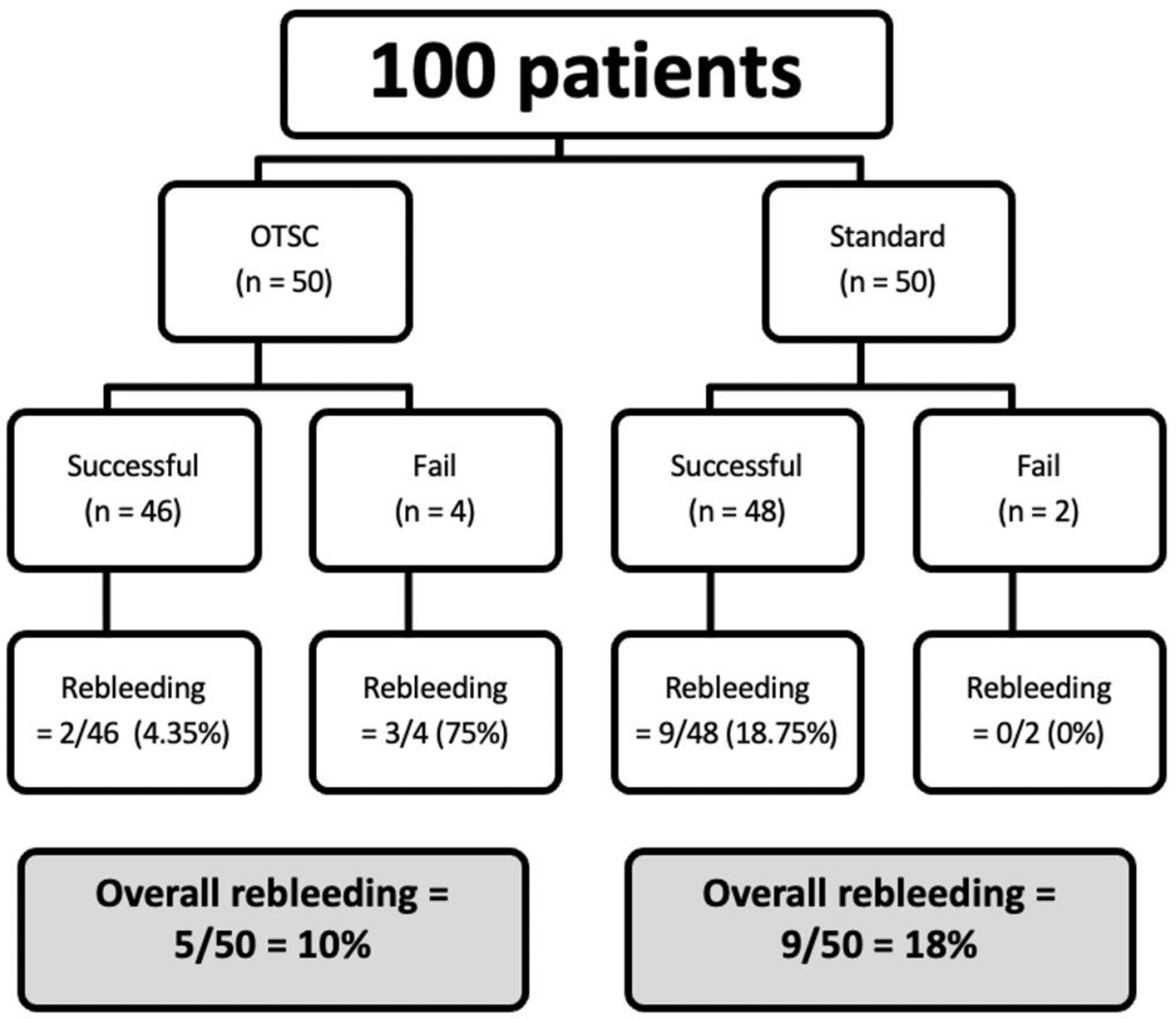
Participant flow diagram with clinical rebleeding rates. OTSC, over-the-scope clip.
Methods
Trial design
This was an open-labelled multicentre international randomised controlled trial comparing OTSC with standard endoscopic therapy for primary treatment of patients with peptic ulcer bleeding that are at high risk of rebleeding. Recruited patients were randomised to receive OTSC or standard endoscopic therapy.
Participants
The inclusion criteria included actively bleeding peptic ulcers (Forrest Ia and Ib), ulcers with a non-bleeding visible vessel or Forrest IIa ulcer with a size of ≥15 mm. Patients aged below 18 with peptic ulcer with concomitant perforation, tumour bleeding, variceal bleeding, stricture of the oesophagus, stomach or pylorus that could not be dilated to allow passage of a 11 mm endoscope or an 11 mm OTSC; patients who are pregnant or lactating; and moribund patients or patients with terminal malignancy or end-stage non-malignant conditions, in whom life expectancy is less than 30 days, were excluded.
Participating centres include the Chinese University of Hong Kong (Hong Kong), North District Hospital (Hong Kong), Chulalongkorn University (Thailand), National Taiwan University (Taiwan), Taipei Tzu Chi Hospital (Taiwan) and ChengDu Second People’s Hospital (China). All procedures were performed by expert endoscopists defined as having performed more than 20 endoscopic haemostatic procedures with OTSC. Research staff screened all patients presented with upper gastrointestinal bleeding (UGIB) requiring esophagogastroduodenoscopy (EGD) at the endoscopy centre and obtained consents. On confirmation on EGD that patients fitted the inclusion criteria, randomisation was performed.
Interventions
Standard therapy group
Haemostasis was achieved (according to clinical practice) by combining two standard treatment options. Possibilities included injection with diluted epinephrine solution (1:10 000–1:20 000) with the application of standard clips or the use of a contact thermal coagulation technique (heater probe 25 J four continuous pulses per station). The decision to for the type of standard therapy was decided by the endoscopist.
OTSC group
Haemostasis was achieved by application of the OTSC. Pretreatment with diluted epinephrine solution (1:10 000) injection and the use of the anchor device was optional.
Postendoscopy treatment
All patients were treated with proton pump inhibitor infusion for 72 hours (80 mg+8 mg/hour) after endoscopic haemostasis according to international guidelines.10 19 Oral proton pump inhibitor was prescribed for 6–8 weeks after the procedure. Helicobacter pylori was eradicated based on rapid urease test or histology results. Antithrombotic drugs for cardiovascular disease or prevention of thromboembolic event were resumed 3–5 days after index endoscopy. Clinical outcomes were recorded for 30 days.
Outcomes
The primary endpoint was clinical rebleeding within 30 days. Clinical rebleeding was defined as fresh haematemesis, fresh melena, haematochezia, signs of hypovolaemic shock (systolic blood pressure of <90 mm Hg and pulse rate of >110 beats/min), or a drop in haemoglobin of >=2 g/dL per 24 hours despite adequate transfusion. Rebleeding was confirmed by an immediate endoscopy showing fresh blood in the stomach or active bleeding from a previously seen ulcer. A clinical rebleeding was independently reviewed by an adjudication panel. Secondary endpoints included death from all causes within 30 days of therapy, transfusion requirement within 30 days of therapy, hospital and intensive care unit (ICU) stay, failure of achieving primary haemostasis and further interventions required, such as repeat endoscopy, surgery or TAE. Failure of achieving primary haemostasis was defined as persistent bleeding despite application of therapy in the randomised arm with the need for additional endoscopic therapy.
Sample size estimation and statistical analysis
In a recent randomised controlled trial on prophylactic transarterial embolisation to peptic ulcers with high rebleeding risk, the rebleeding rate for ulcers 1.5 cm or greater in size was 23.3%.18 Based on this result, the rebleeding rate of the included high-risk patients with standard treatment in this study was estimated to be 23%. At the time of planning of the study, there were only scanty case reports and series on the efficacy of OTSC in primary treatment of bleeding peptic ulcers. The average rebleeding rate following application of the OTSC in the literature was 5%.12–17 Therefore, OTSC was assumed to reduce the rebleeding rate from 23% to 5%. Using a two-sided log-rank test with 5% significance level, 100 patients are required to achieve 80% power. Since the primary outcome was 30-day clinical rebleeding, it was decided to be a short-term endpoint, so a 0% dropout rate was assumed.
Randomisation and blinding
Informed consent was obtained before endoscopy for eligible patients. Once the endoscopist confirmed that the patient fulfilled inclusion criteria, the patient was randomised with an online randomisation form in the form of a computer-generated random sequence in blocks of 10. The method of haemostasis was performed according to the allocation. In patients whoare incapable of consent, consent from their legal representatives was obtained. It was not possible to blind the endoscopist, given the different therapies required during the endoscopy. Also, given the objective outcomes measured, blinding was deemed not necessary. On technical failure of haemostasis of the randomised group, other methods of haemostasisws allowed, including crossover to the other group, TAE or surgery.
Statistical analysis
The data were analysed with intention-to-treat analysis. χ2 test was used to calculate the rates of recurrent bleeding while the Kaplan-Meier method with the log-rank test was used to compare differences in death within 30 days after randomisation. The effect of OTSC as compared with that of standard therapy was calculated with relative risks and the corresponding 95% CI. The χ2 test (or Fisher’s exact test when appropriate), Student’s t-test and Mann-Whitney U test were used to compare categorical, parametric and non-parametric data, respectively. All tests of significant were two-tailed, and a p value of <0.05 was considered statistically significant. Statistical analyses were performed using SPSS V.24.0 statistical software.
Results
From July 2017 to Oct 2020, a total of 100 patients were recruited, 50 patients in each arm. The Consolidated Standards of Reporting Trials diagram and patient flow diagram are shown in figures 2 and 3. There were no cases lost to follow-up. There were 5 ulcers with spurters, 16 oozing ulcers, 74 ulcers with visible vessels and 5 with adherent clots. There was no difference in the Forrest classification of the ulcers between the two groups (p=0.14). There was no significant difference between the two groups in terms of age, gender, use of anticoagulants, renal failure and American Society of Anesthesiologists (ASA) grading. Out of the 50 patients in each group, 19/50 (38%) ulcers were located in the stomach, and 31/50 (62%) were located in the duodenum for the OTSC group, while 24/50 (48%) ulcers were located in the stomach and 26/50 (52%) were located in the duodenum for the conventional arm (p=0.31). The mean size of the ulcer was 1.81 (SD 0.45) cm and 2.03 (SD 0.74) cm for the OTSC and conventional arm, respectively (p=0.15). The aforementioned results are available in table 1. For the standard therapy group, there were 48/50 patients who had dual therapy: 33 patients had epinephrine injection and heater probe application; 15 patients had epinephrine injection and through-the-scope endoclips were applied. Two patients had triple therapy done (epinephrine injection, heater probe application and endoclips). The mean epinephrine injection was 6.50 (SD 6.05) millilitre and the median of endoclips applied was 2(ag 1–5).
Baseline demographics and ulcer characteristics of the two groups
Clinical rebleeding
Clinical rebleeding occurred in 5/50 (10%) cases in the OTSC and 9/50 (18%) in the conventional arm. In the intention-to-treat analysis, there was no statistically significant difference (p=0.23, OR=1.98, 95% CI 0.61 to 6.38). The Kaplan-Meier curve for 30-day clinical rebleeding with log-rank test is shown in figure 4. Success in achieving primary haemostasis was achieved in 46/50 (92%) and 48/50 (96%) in the OTSC and conventional arm, respectively. Among patients who had success in primary haemostasis, 2/46 (4.35%) patients in the OTSC arm rebled within 30 days, while 9/48 (18.75%) patients in the conventional arm developed rebleeding (p=0.03) (figure 5). Two cases in the conventional arm failed primary haemostasis and required OTSC as salvage. Both did not rebleed. Four cases in the OTSC arm failed primary haemostasis. Persistent bleeding was noted after OTSC application in all four cases from the base of the ulcer. In two cases, the OTSC was applied to cover half of the bleeding vessel. OTSC was applied at the end of the vessel in two other cases but still persistent oozing from the base. For all four cases, additional epinephrine injection and heater probe were used as salvage. Three out of four (75%) rebled and required TAE. The one case that did not rebleed had empirical TAE performed. All four of these ulcers were located in the junction between the first and second parts of the duodenum table 2
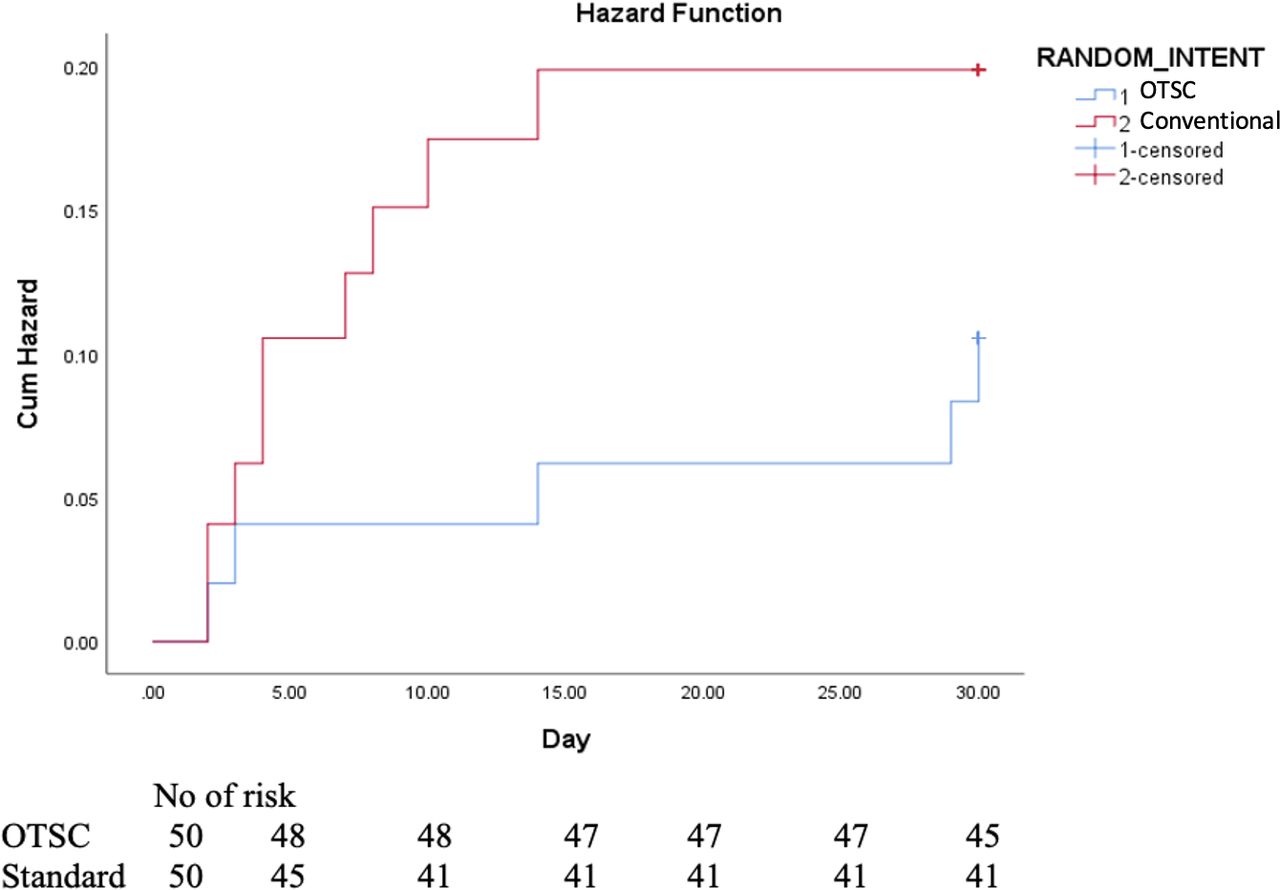
Kaplan-Meier curve showing the clinical rebleeding in 30days (log-rank test, p=0.23). OTSC, over-the-scope clip.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan -Meier curve showing clinical rebleeding within 30 days of therapy in patients who had technical success. (log rank test who had technical success. (log RANK-rank test, pp=0.03)). OTSC, over-the-scope clip.
Clinical rebleeding within 30 days
There was also no difference in early rebleeding, defined as within 72 hours of the index procedure (p=1.00, OR=1.53, 95% CI 0.25 to 9.59)
Secondary endpoints
Table 2 summarised the findings of the secondary endpoints. The all-cause mortality was 2/50 (4%) and 4/50 (8%) in the OTSC and conventional arm, respectively (p=0.68, OR=2.09, 95% CI 0.37 to 11.95). In the OTSC arm, one patient died of multiorgan failure. The other patient had a known intracranial haemorrhage, who presented with cardiac arrest with massive melaena 1 day after endoscopy. The patient died despite cardiopulmonary resuscitation. For the conventional arm, there was one patient who died of rebleeding. The patient presented with massive melaena and cardiac arrest. Cardiopulmonary resuscitation was given and the patient was revived. Emergency laparotomy with open surgical application was performed. The patient subsequently died of ischaemic bowel and multiorgan failure. The other three patients died of medical causes including respiratory failure, multiorgan failure and hospital-acquired pneumonia. A mean of 3.13 (S 3.64) units of blood was transfused in the OTSC group, and a mean of 2.90 (D4.07) units was required for the conventional group (p=0.31). Hospital stay and need for ICU admission were also similar. Six per cent of the OTSC group required further intervention compared with 2% in the standard arm. Three patients in the OTSC group required further TAE after endoscopic haemostasis. One was done after primary failure of OTSC with further epinephrine injection and heater probe, but haemostasis was deemed insecure. Empirical TAE was performed and there was no rebleeding. The other two were performed due to clinical rebleeding. One bleeding stopped; the other rebled and had multiple sessions of endoscopic haemostasis. One case in the conventional arm required emergency surgery, but the patient died of ischaemic bowel and multiorgan failure.
Subgroup analysis
There is no difference in the subgroup analysis on location of ulcer (gastric vs duodenal, p=0.28–1.00), patients with renal failure (p=0.25–0.47) or patients on anticoagulation (p=0.15–1.00).
Discussion
In bleeding peptic ulcers of more than or equal to 15 mm in size, OTSC for primary haemostasis did not decrease 30-day clinical rebleeding when compared with standard therapy. Although there was no statistical difference between the rebleeding rates (10% vs 18% for OTSC and standard therapy, respectively; p=0.234), this may be due to an underestimation of the sample size leading to type II error. The failure rate of achieving primary haemostasis was 8% (4/50) in the OTSC group. All four ulcers were located at the junction of D1/2, which is notoriously difficult for haemostasis. At the D1/2 junction, the scope position is unstable and the direction of the instruments is often not located at an optimal angle. Moreover, these are large fibrotic ulcers which increased difficulty of application to the base. In two out of the four cases of failed primary haemostasis, there was persistent oozing despite end on application of the OTSC. This was probably due to the fibrotic base. This illustrated that it is technically demanding to apply an OTSC clip, especially in fibrotic ulcers at the junction between the first and second portions of the duodenum. Also, in situations of persistent bleeding despite OTSC application, endoscopic salvage was made even more challenging due to the presence of the OTSC clip and resulted in a high rate of rebleeding (3/4 (75%)). TAE is often required for salvage. A learning curve is associated with the successful use of the OTSC, and technical expertise is mandatory in the application. Moreover, careful preapplication assessment is necessary to avoid misfire because rebleeding rate after misfire is exceptionally high and endoscopic salvage is not possible in most situations. On the contrary, where primary haemostasis was successful, OTSC significantly decreased clinical rebleeding when compared with standard therapy. In the 46 cases (92%) of successful application of the OTSC, the rebleeding rate was only 4.35% when compared with 18.75% with conventional therapy (p=0.03). This suggests that OTSC has its role in decreasing rebleeding.
OTSC was first used for peptic ulcer bleeding in the setting of recurrent bleeding after initial endoscopic haemostasis. The initial case series for recurrent bleeding from our centre showed clinical effectiveness of 77.8%.13 Two out of nine patients developed rebleeding requiring TAE. A multicentre German randomised trial (STING-1 study) on the use of OTSC in refractory peptic ulcer bleeding showed that OTSC was more effective than standard therapy with less recurrent bleeding within 7 days (15.2% vs 57.6%, p<0.001).20 In a retrospective analysis on the experience of OTSC for primary haemostasis in 67 patients by the Mayo Clinic, high-risk ulcers were included. High-risk ulcers were defined as vessels greater than 2 mm in size, deep, penetrating or excavating fibrotic ulcers and those who fail other endoscopic treatment.21 The clinical success rate was 81.3%, and patients with coronary artery disease have an increased risk of rebleeding even after OTSC, suggesting a need for escalating therapies. The results of this study are similar to those of the current study. In the current study, the clinical success rate of the OTSC group was 90% and that of the conventional arm was 82%. Both studies included large fibrotic ulcers, suggesting that even with OTSC, there is still a 10%–20% chance of rebleeding. In the first randomised controlled trial for primary haemostasis by Jensen et al, 53 patients with bleeding peptic ulcers and Dieulafoy’s lesions were randomised to receive either OTSC or standard treatment. Recurrent bleeding occurred in only 1 of 25 (4%) patients treated by OTSC compared with 8 of 28 (28.6%) in the standard treatment group (p=0.017).22 Although this study did show a significant decrease in rebleeding in the OTSC group, the sample size was relatively small; the study included both ulcers and Dieulafoy’s lesion; and the rebleeding rate for the standard arm was exceptionally high.
There are several limitations of this study. The first is an underestimation of the sample size leading to a type II error. The OTSC group had a 10% rebleeding rate when compared with a predicted 5%. The 5% rebleeding rate was estimated according to published case cohort and is in fact, similar to the study by Jensen et al.22 However, our study included only giant ulcers, which may explain the higher rebleeding rate. Also, there may be publication bias leading to an underestimation of the rebleeding rate. The second is the technical failure rate for OTSC was high. Endoscopists with experience of more than 20 cases of OTSC for haemostasis were included. To date, there are no studies regarding the learning curve of OTSC application. The optimal cut-off point for an experience endoscopist for OTSC is still undetermined. Although this study did not show significant results, it reflected on the real-life scenario on the use of OTSC in giant ulcers. Technical success of OTSC application was associated with decreased rebleeding, suggesting that OTSC may be beneficial in selected cases.
This study showed that the routine use of OTSC as primary haemostasis in large bleeding peptic ulcers was not associated with a significant decrease in 30-day rebleeding. However, there may be a role of OTSC in expert hands where OTSC can be successfully applied. It also highlighted that there is a learning curve to the use of OTSC and that salvage after a misplaced OTSC could be challenging.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Joint Chinese University of Hong Kong-New Territories East Cluster Clinical Research Ethics Committee (CREC reference number 2016.711-T). The participants gave informed consent to participate in the study before taking part.
References
Footnotes
Twitter @sunnyheiwong, @wingyanjoyce, @RashidLui
Correction notice This article has been corrected since it published Online First. The second affiliation has been corrected.
Contributors SC is the principal investigator and author responsible of this project and she is from Prince of Wales Hospital, Hong Kong. She was responsible for study design, running of the study, coordination with other overseas centres, data analysis, interpretation and write-up of the manuscript. RP and RR are the coinvestigators in Chulalongkorn University, Bangkok, Thailand. They were responsible for case recruitment, performance of the procedures and data collection in their centre. HPW and YTK are the coinvestigators from National Taiwan University, Taiwan. They were responsible for case recruitment, performance of the procedures and data collection in their centre. JHC is the coinvestigator of Taipei Tzu Chi Hospital, Taiwan, and was responsible for case recruitment, performance of the procedures and data collection in their centre. AYBT, RSYT, HCY, SKKN, SW, JWYM, HC, LL, RNL and MW are the coinvestigators in Prince of Wales Hospital, Hong Kong. They were responsible for case recruitment, performance of the procedures and data collection. EKN and PWYC were the advisors of this project, responsible for overseeing the project, final data analysis and manuscript approval. SC is responsible for the overall content as the guarantor.
Funding This study is supported by the Health and Medical Research Fund of the Food and Health Bureau, Government of Hong Kong Special Administrative Region.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.