Article Text

Abstract
Objective Liver injury has frequently been reported in COVID-19 patients. The clinical relevance of liver injury related to SARS-CoV-2 infection remains unclear with a need for prospective studies on the impact of liver function test (LFT) abnormalities at baseline.
Design Data of 217 patients without pre-existing liver disease prospectively included in the COVID-19 registry of the LMU university hospital were analysed in order to assess the association of abnormal LFT at admission and course of the disease. Severe course was defined as admission to the intensive care unit (ICU) or as COVID-19-related death.
Results Abnormal LFT at baseline was present in 58% of patients, with a predominant elevation of aspartate aminotransferase (AST) (42%), gamma-glutamyltransferase (GGT) (37%) and alanine aminotransferase (ALT) (27%), hypoalbuminaemia was observed in 33%. Elevation of ALT and GGT, as well as hypoalbuminaemia, was associated with higher proportions of patients requiring ICU treatment and mechanical ventilation. After adjusting for age, gender and comorbidities, hypoalbuminaemia combined with abnormal AST or GGT at hospital admission was a highly significant independent risk factor for ICU admission (OR 46.22 and 38.8, respectively) and for a composite endpoint of ICU admission and/or COVID-19-related death (OR 42.0 and 26.9, respectively).
Conclusion Abnormal LFTs at hospital admission, in particular GGT and albumin, are associated with a severe course of SARS-CoV-2 infection.
- COVID-19
- liver function test
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
During infection with SARS-CoV-2 liver injury occurs in a relevant proportion of patients. As yet, mainly elevation of aminotransferases has been described, while abnormalities of cholestatic parameters, that is, gamma-glutamyltransferase and alkaline phosphatase were reported less frequently. Liver function test (LFT) peak levels correlate with severity and/or outcome in COVID-19 patients. However, the association of baseline LFT abnormalities with the course of the disease has not been prospectively evaluated.
What are the new findings?
In our prospective COVID-19 cohort, 58% of patients had LFT abnormalities at the time of hospital admission. Hypoalbuminaemia, in particular in combination with an elevation of aminotransferases or gamma-glutamyltransferase, was highly significant independent risk factors for a severe course.
How might it impact on clinical practice in the foreseeable future?
Patients with hypoalbuminaemia and abnormal aminotransferases or gamma-glutamyltransferase are at high risk for a severe course of COVID-19 disease and should be closely monitored and considered for early intensive care unit admission.
Introduction
COVID-19 predominantly affects the pulmonary tract causing mainly respiratory symptoms,1 however, involvement of other organ systems has been described, including myocarditis, acute kidney injury, neurological abnormalities and acute liver injury.2–4 Especially the latter has been reported for a large proportion of COVID-19 patients with numbers as high as 76% of patients presenting with liver biochemistry abnormalities.5–7 However, the clinical relevance of abnormal liver function tests (LFT) in COVID-19 is still subject of debate.8 9 This especially holds true for the impact of baseline LFT on severity, since the majority of available studies focused on liver injury at peak levels during hospitalisation for COVID-19.10 11
Therefore, we evaluated the proportions of elevated liver enzymes at hospital admission and their association with severe COVID-19 in a prospectively acquired cohort of COVID-19 patients from the University Hospital in Munich.
Methods
Study design and patient selection
From March 2020 to July 2020 275 patients were prospectively included in the Registry of the LMU Klinikum (CORKUM, WHO trial ID DRKS00021225). Inclusion was based on the diagnosis or suspicion of COVID-19. The detailed inclusion criteria were: (1) patients and members of the hospital staff with a positive test for SARS-CoV-2 or a highly likely SARS-CoV-2 infection based on typical radiological findings, respiratory symptoms, absence of a more likely diagnosis and negative testing for influenza and respiratory syncytial virus; (2) patients and members of the hospital who have a high risk of more severe COVID-19 due to known comorbidities or treatments, in particular immunosuppression, underlying malignant disease or underlying cardiovascular and/or pulmonary conditions; (3) patients and members of the hospital with initial suspicion of SARS-CoV-2 infection who were tested negative for SARS-CoV-2. Written informed consent was obtained from each patient or their respective legal representatives in case the patient was unable to give informed consent, and from each member of the hospital included in the study. In case informed consent was not obtained, eg, due to fulminant course of disease, data were used in an anonymised and aggregated way only. Patients and the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research. Out of the 275 patients included until July 2020, 235 were diagnosed with SARS-CoV-2 infection using reverse-transcriptase PCR of nasopharyngeal swab specimens in the accredited diagnostic laboratories at the Pettenkofer-Institute, Munich, as previously described.12 Patients without available baseline liver chemistry results (n=14) or with underlying chronic liver disease (n=4) were excluded from the analysis leaving 217 patients for analysis (figure 1). Patient history including gender, age and underlying medical conditions were recorded. Laboratory tests including liver enzymes were performed on admission and repeatedly until discharge. Values at admission as well as respective minimal and peak values were obtained via automated data extraction tools. LFT analysis included aspartate aminotransferase (AST), alanine aminotransferase (ALT), alkaline phosphatase (ALP), gamma-glutamyltransferase (GGT), total bilirubin (TBIL) and albumin. Further analyses included C reactive protein (CRP) and interleukin 6 (IL-6). In case the patient had been transferred from another hospital, laboratory values from the initial admission were extracted from the patients’ files. Endpoints for severe COVID-19 were defined as admission to the intensive care unit (ICU), COVID-19-related death and a composite endpoint for severe COVID-19 comprising both ICU admission and COVID-19-related death. In case of missing single liver biochemistry values at the time of admission, we calculated the proportions of patients reaching each endpoint according to the numbers of patients for whom the respective laboratory parameters were available. The Charlson Comorbidity Index which is based on age and comorbidities was calculated.13

Flow chart of patient inclusion.
Statistical analysis
Statistical analyses were performed using SPSS V.26 (IBM). Categorical variables are presented as number and percentage (n (%)). Continuous variables are presented as median (range). After testing for normal distribution, parametric or non-parametric tests (χ2 test or Mann-Whitney U test) were applied. To analyse the association between LFT abnormalities and the severity of disease a hierarchical binary logistic regression analysis was conducted adjusting for age, gender, arterial hypertension, diabetes, coronary artery disease and previous myocardial infarction, which are risk factors that have previously been identified to have a high association with severity,14 and also showed association with severity in our cohort (online supplemental table 1). Furthermore, logistic regression was performed adjusting for gender and the Charlson Comorbidity Index. Pearson’s correlation was applied to calculate a relationship between the liver biochemistry abnormalities and inflammatory parameters at admission. Receiver operating characteristic (ROC) curves were calculated using SPSS to evaluate a cut‐off value for albumin that could distinguish best between severe and non-severe COVID-19 and the respective sensitivity and specificity values.
Supplemental material
Results
Clinical characteristics
The baseline clinical characteristics of COVID-19 patients from our cohort are summarised in table 1. The median age was 63 years and 66% were male. The most prevalent underlying medical conditions were arterial hypertension, diabetes mellitus type II, coronary artery disease and chronic kidney disease.
Clinical characteristics in patients with COVID-19
Clinical course and outcome
Out of the 217 patients with SARS-CoV-2 infection that were included in our cohort, 36% required treatment in the ICU and 32% underwent mechanical ventilation. The total fatality rate was 14.7%, mostly related to COVID-19 (table 2). Median time from hospital admission to ICU admission was 1 day. Twenty-seven out of 77 patients (35%) were admitted to the ICU on the same day of admission, while the majority of the ICU patients had an interval of two or more days from admission and 15 of 77 (19%) an interval of a week or more.
Clinical course and outcome in patients with COVID-19
LFT abnormalities
Liver biochemistry abnormalities of any kind (including ALT, AST, GGT, ALP and TBIL) at the time of admission were detected in 125 patients (58%). Elevation of ALT and AST at the time of hospital admission was observed in 27% and 42%, respectively (table 3). Most of the patients had mild elevation of ALT (n=40/59, 68%) and AST (n=67/91, 74%) below two times the upper limit of normal (ULN). Regarding elevation of liver biochemistry at respective peak levels, ALT and AST elevation was found in 64% and 72% of patients with relatively high proportions presenting with pronounced elevation of ALT and AST of five times or more ULN (17% and 14% of all patients, respectively).
Proportion of patients with abnormal LFT at hospital admission and at respective peak levels
Association of liver biochemistry abnormalities at admission with severe COVID-19
COVID-19 patients who required ICU treatment showed significantly higher baseline levels of AST, ALT, GGT and TBIL (p<0.05) and peak levels of AST, ALT, TBIL, GGT and ALP (p<0.001) as well as significantly lower albumin levels at baseline and respective nadir (p<0.001; online supplemental table 2). Patients with severe COVID-19 as defined by ICU admission and/or a COVID-19-related fatal outcome showed significantly lower albumin levels at baseline and respective minimal levels (p<0.001) and significantly higher baseline levels of TBIL and AST (p<0.05) as well as significantly higher peak levels of AST, TBIL, GGT and ALP (p<0.001; online supplemental table 2).
Supplemental material
AST and ALT elevation at hospital admission were associated with higher rates of ICU admission and mechanical ventilation (table 4): 50% of patients with abnormal AST and 51% with abnormal ALT but only 27% or 31% with normal AST or ALT at hospital admission were transferred to the ICU. The OR for ICU treatment for patients with AST elevation at baseline was 2.68 (95% CI 1.50 to 4.80) and 2.35 (95% CI 1.26 to 4.36) for patients with ALT elevation (online supplemental table 3). AST elevation was associated with a significantly increased risk of severe COVID-19 (OR 2.2; 95% CI 1.25 to 3.87). However, neither AST nor ALT abnormalities at admission were related to mortality (p>0.05; table 4).
Supplemental material
Clinical course in patients with COVID-19 according to LFT abnormality at hospital admission
TBIL elevation at admission was associated with significantly higher all-cause mortality and mortality rate related to COVID-19 (OR 4.56; 95% CI 1.21 to 17.39; online supplemental table 3), but not with the risk of ICU admission nor mechanical ventilation (table 4). Patients with ALP elevation at admission were more likely to require extracorporeal membrane oxygenation (18% vs 3%, p=0.004). However, rates of ICU admission rate, mechanical ventilation and mortality were not different (data not shown).
GGT at admission was associated with higher rates of ICU admission and mechanical ventilation: 45% of patients with GGT elevation at baseline required ICU treatment, while only 30% of patients with normal GGT did (OR 1.96; 95% CI 1.10 to 3.50; online supplemental table 3). However, no association with all-cause mortality or COVID-19-related death was observed (table 4).
Hypoalbuminaemia was associated with a significantly higher risk for severe COVID-19: The composite endpoint of ICU admission and/or COVID-related mortality was reached in 80% of patients with initial albumin deficiency but only in 26% patients with normal albumin at admission (p<0.001; table 4). Baseline hypoalbuminaemia or AST elevation was associated with a shorter time from hospital admission to ICU admission, while no association was observed for the other LFT. Hypoalbuminaemia was also associated with significantly higher mechanical ventilation and mortality rates (table 4). Twenty-three per cent of patients with baseline hypoalbuminaemia had a COVID-19-related fatal outcome, while only 9% of patients with normal albumin levels did (p<0.05; table 4). Therefore, the risk of a severe course of COVID-19 in patients with albumin deficiency at baseline was significantly increased: OR for ICU admission was 12.71 (95% CI 6.00 to 26.92), while the OR for the composite endpoint for severe COVID-19 was 11.86 (95% CI 5.59 to 25.17; online supplemental table 3).
When hypoalbuminaemia was combined with elevation of any other LFT, the risk of ICU admission was markedly increased with the highest OR observed for the combination of hypoalbuminaemia and abnormal GGT (OR 35.79; 95% CI 8.16 to 157.04; online supplemental table 3). Combination of hypoalbuminaemia and TBIL elevation was associated with a ninefold risk increase for COVID-19-related mortality (online supplemental table 3).
Association of abnormal baseline liver functions tests and COVID-19 disease severity by multivariable logistic regression
Since LFT abnormality of any kind, of AST, ALT, TBIL and GGT as well as hypoalbuminaemia and the combination of hypoalbuminaemia with those parameters showed the strongest association with a severe course of the disease, a multivariable logistic regression was performed adjusting for age, gender and relevant comorbidities with the highest individual OR for severe COVID-19. Logistic regression had shown that confounding variables with risk increase of severe COVID-19 were age (OR 1.03, p<0.0001), arterial hypertension (OR 2.69; p=0.001), diabetes (OR 2.36, p=0.009), coronary artery disease (OR 2.36, p=0.014) and previous myocardial infarction (OR 3.03, p=0.024; online supplemental table 1). Male gender was also associated with a tendency to a higher risk in our cohort, although statistical difference was not reached (OR 1.79, p=0.06; online supplemental table 1). Table 5 shows that also after adjustment, liver biochemistry abnormalities of any kind, AST, ALT, GGT and albumin at admission correlated strongly with a higher risk of ICU admission. The OR for the composite endpoint for severe COVID-19 was 2.51 (95% CI 1.30 to 4.82) for liver biochemistry abnormality of any kind, 2.54 (95% CI 1.33 to 4.84) for AST and 2.10 (95% CI 1.07 to 4.11) for baseline ALT elevation. GGT elevation was also associated with a twofold risk increase for ICU admission (OR 2.06; 95% CI 1.08 to 3.92). TBIL elevation did not correlate with ICU admission rates but was an independent risk factor for COVID-19-related death (OR 4.80; 95% CI 1.14 to 20.16). Hypoalbuminaemia was associated with a significantly increased risk of ICU admission (OR 13.95; 95% CI 5.72 to 34.03) and the composite endpoint for severe COVID-19 (OR 9.95; 95% CI 4.40 to 22.78). Strinkingly, when albumin deficiency and elevation of AST, ALT, GGT or of any liver parameter at admission were combined a more than 20-fold risk increase of ICU admission was observed with the highest OR detected for the combination of hypoalbuminaemia and AST (OR 46.22, p<0.001) and of hypoalbuminaemia and GGT (OR 38.82, p<0.001). The combination of hypoalbuminaemia and TBIL elevation at admission on the other hand was associated with a nearly 10-fold risk increase for COVID-19-related death. Furthermore, we performed logistic regression adjusting for gender and the Charlson Comorbidity Index, which is used for the risk stratification of hospitalised COVID-19 patients,15 and similar results were obtained (online supplemental table 4). Any liver biochemistry abnormality, elevation of AST, ALT and GGT as well as hypoalbuminaemia remained strongly associated with ICU admission, while liver biochemistry abnormality of any kind, AST elevation and hypoalbuminaemia were independent risk factors for the composite endpoint of severe COVID-19. In addition, hyperbilirubinaemia (OR 4.22) as well as hypoalbuminaemia alone (OR 2.69) or in combination with any liver biochemistry abnormality (OR 2.82) or TBIL elevation (OR 10.61) was associated with an increased risk of COVID-19-related death (online supplemental table 4).
Supplemental material
Association of abnormal liver test results with severity of the COVID-19 infection adjusted for age, gender and comorbidities
ROC analysis for albumin
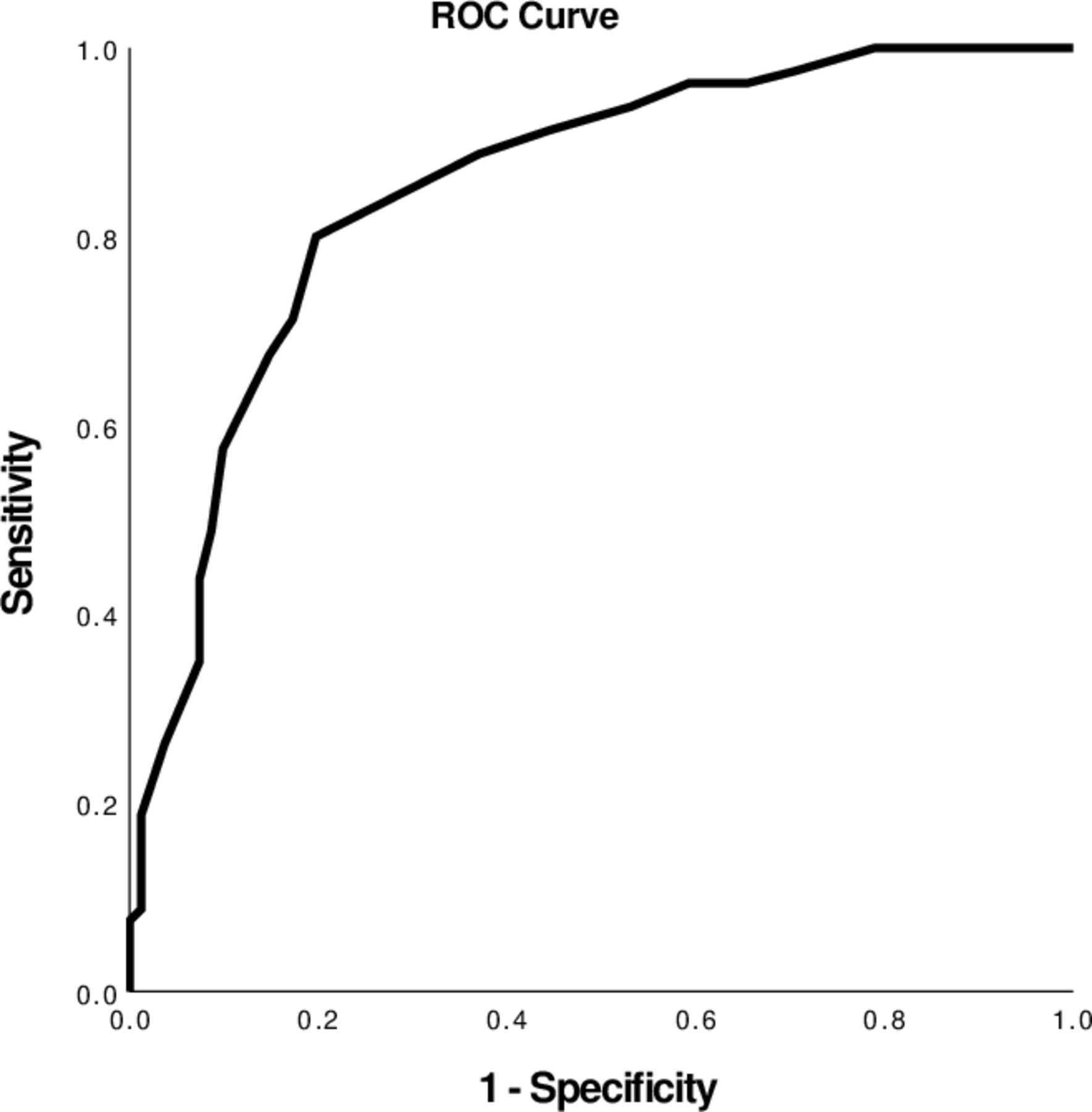
Since particularly hypalbuminaemia was strongly associated with poor outcome, an ROC analysis was performed. Albumin at admission showed the best differentiation at 3.55 g/dL with sensitivity and specifity for the composite endpoint ICU admission and/or COVID-19-related death of 80%, respectively (area under receiver operating characteristic (AUROC) 0.85; figure 2).
{kind=link}
{kind=link}
Receiver operator characteristic (ROC) curve for albumin as the most discriminating factor regarding the composite endpoint ICU admission and/or death. ICU, Intensive care unit.
Correlation with inflammatory markers
To investigate whether liver injury at admission and its association with poor outcome was predominately caused by more severe disease states with higher levels of inflammation, we analysed the correlation between LFT and inflammation markers (CRP and IL-6) at baseline (table 6). The only relevant correlation found was between albumin and CRP (r=−0.58, p<0.001). A weak correlation was also observed for GGT and IL-6 (r=0.15, p=0.048) and albumin and IL-6 (r=−0.18, p=0.037), while ALT, AST, ALP and TBIL did not correlate with any of the inflammation markers at baseline.
Pearson’s correlation coefficients between CRP, IL-6 and liver function tests at admission
Discussion
SARS-CoV-2 has infected more than 85 million people worldwide causing severe strains on healthcare systems.16 Therefore, a better understanding of risk factors for more severe courses has become particularly important. A wide array of data is available now showing that male gender, age and comorbidities such as arterial hypertension and diabetes mellitus type II correlate with worse outcomes and more severe COVID-19 infections.17 In addition, it has become evident that liver injury is present in a relevant proportion of patients during SARS-CoV-2 infection and might also correlate with worse outcomes.6 18 Even cases of acute liver failure have been described.5 19 However, the mechanism behind liver injury in SARS-CoV-2 and its clinical relevance remain a subject of debate. Importantly, the association between liver damage in COVID-19 patients and poor outcomes has only been evaluated retrospectively in the majority of studies, prospective studies on the clinical characteristics of COVID-19 patients are still scarce.20 21 Furthermore, the available reports mainly focus on liver injury occurring during hospitalisation, while reports on an elevation of liver parameters at admission and analyses of the effect of baseline liver parameters on outcome and severity are rare.11 22 The correlation of LFT at the time of admission with severity is therefore less clear but of great clinical importance. We here present novel data on the association of LFT at the time of admission and course of the disease in a prospectively collected and well-characterised cohort of 217 COVID-19 patients.
At the time of hospital admission, liver biochemistry abnormalities of any kind were observed in 58% of all COVID-19 patients included. Forty-two per cent of patients had elevation of AST, 37% of GGT, 27% of ALT, 10% of ALP and 5% of TBIL, respectively. The finding that GGT was one of the predominantly elevated liver-specific parameters is in contrast to the majority of available data. While Aghemo et al reported GGT elevation in 36.2% of patients,23 the many studies so far have reported an elevation of serum aminotransferase rather than of GGT and ALP,4 however, largely without providing data on ALP and/or GGT, respectively.20 24–33
Our findings of frequently abnormal GGT at admission might indicate that SARS-CoV-2 could directly cause liver injury. Various causes have been proposed for liver injury in COVID-19 patients such as the cytokine storm in severe COVID-19 with a consecutive multiorgan damage, ischaemic hepatitis following cardiac, circulatory and/or respiratory failure, mechanical ventilation-induced disturbance of the venous return especially if high end-expiratory positive pressures are needed and drug-induced liver injury.34–36 Additionally, direct viral effects on the liver have been discussed,18 35 37 38 since the ACE2, which has been identified as the receptor through which SARS-CoV-2 mainly infects the host cells,39 is not only expressed in pulmonary tissue but also in a subset of cholangiocytes. Expression in hepatocytes, however, is low.37 40 41 Therefore, it has been hypothesised, that SARS-CoV-2 could induce bile duct damage, followed by hepatocyte injury. However, several publications report elevation of serum aminotransaminases rather than of ALP or GGT,7 35 42 as it would be expected if biliary damage was the main mechanism of liver injury. Thus, our observation that GGT levels are elevated in a relevant proportion of patients at the time of admission could be an indication for direct SARS-CoV-2-mediated liver damage via the affection of cholangiocytes. Since baseline liver parameters and not peak levels were regarded, potential alternative causes of liver injury, such as a cytokine storm, which rather occurs in later phases of the infection,43 liver damage induced by mechanical ventilation, prone positioning or vasopressor therapy and drug-induced liver injury caused by the medication used to alleviated SARS-CoV-2 infection or its side effects, are rather unlikely. Yet, since patients who are admitted due to COVID-19 per se have a more severe disease than patients that can be treated in outpatient care, more severe inflammation might have contributed to liver injury. To address this issue, we performed a correlation analysis, which showed that the only liver parameter that correlated significantly with both CRP and IL-6 was albumin. GGT did not correlate with CRP, while a weak correlation was observed with IL-6. An inflammatory-syndrome-driven liver injury as the cause of elevated liver enzymes is therefore less likely, while more severe inflammation might have contributed to albumin deficiency. The latter is feasible since hypoalbuminaemia can be the consequence of a capillary leak syndrome induced by severe inflammation, which can lead to extravasation of albumin.44 However, other LFT abnormalities were not influenced to a significant degree by severe inflammation adding evidence that liver injury at admission was not merely a reflection of more severe inflammatory responses. Our findings are contractionary to Da et al who showed a significant association between liver injury and IL-6.45 However, in their work liver injury was defined as AST and/or ALT above three times ULN at any given time during hospitalisation. Applying this definition causes two issues from our point of view: peak values are highly influenced by procedures and treatments during the full period of hospitalisation, for example, vasopressor therapy, ventilation, antibiotics, all of which were over-represented in patients with liver injury in their study.45 Furthermore, by defining liver injury as ALT or AST elevation, patients who have a predominant AST elevation might be declared as having liver injury. However, AST can be elevated due to various extrahepatic causes, for example, myositis and cardiomyopathy, which have also been described in COVID-19 patients.46 47
Interestingly, liver biochemistry abnormalities at admission had an impact on severity and outcome. AST, ALT and GGT elevation at baseline were associated with higher rates of ICU admission and requirement for mechanical ventilation, while TBIL elevation at admission was associated with higher rates of COVID-19-related deaths. In addition, hypoalbuminaemia was associated with higher rates of ICU admission and COVID-19-related mortality.
After adjusting for age, gender and relevant comorbidities, we observed a significantly increased risk of ICU admission if any liver parameter was abnormal. The highest risk increase was observed for hypoalbuminaemia with 14 times higher odds for ICU admission. Strinkingly, when elevation of ALT and hypoalbuminaemia at admission were combined, we observed a 20-fold risk increase for ICU admission and a 12-fold risk increase for the composite endpoint of ICU admission and/or COVID-19-related death. Moreover, the combination of GGT elevation and hypoalbuminaemia was associated with very pronounced increase of ICU admission or the composite endpoint for severe COVID-19 (OR 38.82 and 26.85, respectively). The same applied for AST elevation in combination with hypoalbuminaemia, for which an OR of 46.22 and 42.04, respectively, was observed for ICU admission or the composite endpoint of ICU admission and/or COVID-19-related death. Hyperbilirubinaemia, although rare at admission, on the other hand was an independent risk factor for COVID-19-related death also after adjustment for comorbidities, gender and age. When hyperbilirubinaemia and hypoalbuminaemia were combined the association with COVID-19-related mortality was even higher, showing a nearly 10-fold risk increase. These results were comparable when adjustment was performed for gender and the Charlson comorbidity index, which indicates that the associated between liver injury at admission and poor outcome was not predominately caused by higher frailty of patients with abnormal LFT.
Our results are contradictory to earlier studies that showed no independent association of baseline LFT abnormalities and severity.5 48 49 The discrepancies might be due to the retrospective nature of those studies and differences in data collection. For instance, Zhou et al only adjusted for age and gender but not comorbidities,32 while Cai et al did not evaluate the influence of liver parameters separately nor did they analyse the association between hypoalbuminaemia and severity.5 On the other hand, some studies have observed an association between abnormal LFT and severity,10 11 42 yet, there are methodical issues that should be addressed. Phipps et al and Lei et al evaluated the association only between peak ALT levels and severity but did not analyse the association for baseline ALT, GGT nor albumin.10 11 Furthermore, exclusion of patients with previous liver disease was not universally conducted confounding the analyses.10 11
In summary, we could show in a prospective cohort of COVID-19 patients without previous liver disease that relevant proportions of patients present with abnormal LFT at hospital admission. These baseline LFT, in particular the combination of AST, ALT or GGT elevation and hypoalbuminaemia are associated with a more severe course of infection with higher risk of ICU treatment. In addition, we exhibit the impact of hypoalbuminaemia in SARS-CoV-2-infected patients for the first time in a prospective cohort in line with recent retrospective analysis.50 51 We found that hypoalbuminaemia on admission correlated strongly with more severe SARS-CoV-2 infections, even after adjusting for other risk factors such as age, gender and relevant comorbidities. With a cut-off of 3.55 mg/dL, which is the lower limit of normal in our laboratory institute, albumin could differentiate between less and more severe cases with a sensitivity and specificity of 80%, respectively.
Our study has limitations. Only patients who presented or were referred to our University Hospital serving as the regional tertiary care centre were included in the study. Thus, there is a potential bias towards more severe COVID-19 cases. It can, therefore, not be fully excluded that LFT elevation at admission might represent a more severe course of SARS-CoV-2 infection with multiorgan affection including hepatobiliary inflammation. However, regardless of the cause of liver injury at the time of admission, we show a strong association between severity and liver parameters at admission rather than peak values, which can help to guide clinical decisions early in the course of the disease. Further strengths of our study are the prospective data collection, the exclusion of patients with underlying chronic liver disease and the adjustment for relevant cofounding risk factors for severe COVID-19.
In conclusion, we present data showing a significant correlation of elevation of baseline LFT, including GGT, as well as hypoalbuminaemia with more severe courses of SARS-CoV-2 infections. Thus, baseline hypoalbuminaemia when combined with other abnormal LFT in particular with abnormal AST or GGT should be regarded as a red flag indicating a more severe course of the disease and could support clinical decisions regarding closer monitoring and intensive care of patients with COVID-19.
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
Ethics statements
Ethics approval
The study protocol conforms to the ethical guidelines of the Declaration of Helsinki and was approved by the ethics committee of the Faculty of Medicine, LMU Munich (Project Number 20–245). Written informed consent was intended from each patient or their respective legal representatives in case the patient was unable to give informed consent, and from each member of the hospital included in the study. In case informed consent was not obtained, eg, due to fulminant course of disease, data were used in an anonymised and aggregated way only.
Acknowledgments
We wish to acknowledge the excellent help and support by all the healthcare workers and students during this COVID-19 pandemic, who helped to treat patients and to collect data for the COVID-19 Registry of the LMU Klinikum (CORKUM). We would like to thank all CORKUM investigators and staff. The authors thank the patients and their families for their participation in the CORKUM registry.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors SW: data collection, first draft of the manuscript. JCH, CS and MM: supervision of COVID-19 Registry of the LMU Klinikum (CORKUM), data collection and revision of the manuscript. JM and ALG: Supervision and revision of the manuscript.
Funding SW received funding from the Friedrich-Baur-Institution.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.