
Summary
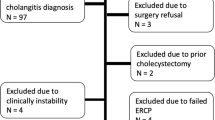
Laparoscopic cholecystectomy (LC) has become the primary surgical treatment for symptomatic cholelithiasis. In conjunction with the dramatic rise in LC there has been an increase in the number of endoscopic retrograde cholangiopancreatographies (ERCPs) performed. For this study, the records of patients referred to the surgical endoscopy department between January 1991 and February 1992 were reviewed. Seventy-seven ERCPs were performed in conjunction with LC. The indications for ERCP included jaundice or a history of jaundice, gallstone pancreatitis, a suspicious filling defect on either ultrasound or intraoperative cholangiogram, abnormal liver function tests, cholangitis, or postoperative bile leak. Sixty-two procedures were performed prior to LC and 15 procedures after LC. Forty-two patients were female (54.5%) and the patients ages ranged from 14 to 92 years (mean 54.1 years). Of the 62 patients having ERCP preoperatively 35 patients (56.5%) had no evidence of common bile duct (CBD) stones and underwent LC as planned. Twenty-three patients were found to have CBD stones, of which six were referred for an open cholecystectomy and CBD exploration, because of large multiple CBD stones or the presence of a large duodenal diverticulum. Seventeen patients had their CBD cleared endoscopically, and four patients were not successfully cannulated.
Fifteen patients had ERCP after LC. There were two patients with CBD injuries who were referred for surgical correction. Two patients had leakage from the cystic duct stump, and four patients had CBD stones, all of whom were successfully treated with endoscopic sphincterotomy. There were four patients who had a normal postoperative ERCP and two patients who could not have their CBD cannulated.
There were no mortalities, but there were four cases of complications. Two patients had bleeding after stone extractions, and they required blood transfusions. One patient developed cholangitis from stenosis of the papilla after an endoscopic sphincterotomy, and one patient developed pancreatitis which resolved with conservative treatment. There is an increasing role for ERCP and sphincterotomy in patients undergoing LC. ERCP carries an inherent morbidity and therefore routine ERCP is not justified. However, with the proper suspicion of CBD stones a preoperative ERCP is indicated prior to a planned laparoscopic cholecystectomy.
Article PDF
Similar content being viewed by others


References
Allen B, Shapiro H, Way LN (1981) Management of recurrent and residual common duct stones. Am J Surg 142: 41–47
Arregui ME, Davis CJ, Arkush AM, et al (1992) Laparoscopic cholecystectomy combined with endoscopic sphincterotomy and stone extraction or laparoscopic choledochoscopy and electrohydraulic lithotripsy for management of cholelithiasis with choledocholithiasis. Surg Endosc 6: 10–15
Berci G, Sackier JM (1991) The Los Angeles experience with laparoscopic cholecystectomy. Am J Surg 161: 382–384
Berci G, Sackier JM, Paz-Partlow M (1991) Routine or selected intraoperative cholangiography during laparoscopic cholecystectomy. Am J Surg 161: 355–360
Binmoeller KF, Katon RM, Shneidman R (1991) Endoscopic management of postoperative biliary leaks: review of 77 cases and report of two cases with biloma formation. Am J Gastroenterol 86: 227–231
Broughan TA, Sivak M, Hermann RE (1985). The management of retained and recurrent bile duct stones. Surgery 98: 746–751
Cotton PB (1984) Endoscopic management of bile duct stones (apples and oranges). Gut 25: 587–597
Davidoff AM, Pappas TN, Murray EA, et al. (1992) Mechanisms of major biliary injury during laparoscopic cholecystectomy. Ann Surg 215: 196–202
Davidson BR, Neoptolemos JP, Carr-Locke DL (1988) Endoscopic sphincterotomy for common bile duct calculi in patients with gallbladder in-situ considered unfit for surgery. Gut 29: 114–120
Ghazi A, Washington M (1989) Endoscopic retrograde cholangiopancreatography, endoscopic sphincterotomy, and biliary drainage. Surg Clin North Am 69: 1249–1274
Goldin E, Katz E, Wengrower D, et al. (1990) Treatment of fistulas of the biliary tract by endoscopic insertion of endoprostheses. Surg Gynecol Obstet 170: 418–423
Hunter JG (1992). Laparoscopic transcystic common bile duct exploration. Am J Surg 163: 53–58
Jacobs M, Verdeja JC, Goldstein HS (1991) Laparoscopic choledocholithotomy. J Laparoendosc Surg 1: 79–82
Leese T, Neoptolemos JP, Baker AR, et al. (1986) Management of acute cholangitis and the impact of endoscopic sphincterotomy. Br J Surg 73: 988–992
Lillemoe KD, Yeo CJ, Talamini MA, et al. (1992) Selective cholangiography, current role in laparoscopic cholecystectomy. Ann Surg 215: 669–676
Miller BM, Kozarek RA, Ryan JA, et al. (1988) Surgical versus endoscopic management of common bile duct stones. Ann Surg 207: 135–141
Moosa AR, Easter DW, Van Sonnenberg E, et al. (1992) Laparoscopic injuries to the bile duct. Ann Surg 215: 203–208
Neoptolemos JP, Carr-Locke DL, Fossard DP (1987) Prospective randomized study of preoperative endoscopic sphincterotomy versus surgery alone for common bile duct stones. Br Med J 294: 470–474
Neoptolemos JP, London NJ, Slater ND (1986) A prospective study of ERCP and endoscopic sphincterotomy in the diagnosis and treatment of gallstone acute pancreatitis. Arch Surg 121: 697–702
Neugebauer E, Troidl H, Spangenberger W, et al. (1991) Conventional versus laparoscopic cholecystectomy and the randomized controlled trial. Br J Surg 78: 150–154
Shapiro SJ, Gordon LA, Daykhovsky L, et al. (1991) Laparoscopic exploration of the common bile duct: Experience in 16 selected patients. J Laparoendoscopic Surg 1: 333–341
Siegel JH (1981) Endoscopic papillotomy in the treatment of biliary tract disease. Dig Dis Sci 16: 1057–1064
Spaw AT, Reddick EJ, Olsen DO (1991) Laparoscopic laser cholecystectomy: analysis of 500 procedures. Surg Laparosc Endosc 1: 2–7
Stain SC, Cohen H, Tsuishoysha M, Donovan AJ (1991) Choledocholithiasis, endoscopic sphincterotomy or common bile duct exploration. Ann Surg 213: 627–634
Stiegmann GV, Goff JS, Mansour A, et al. (1992) Precholecystectomy endoscopic cholangiography and stone removal is not superior to cholecystectomy, cholangiography, and common duct exploration. Am J Surg 163: 227–230
Stoker ME, Leveillee RJ, McCann JC, et al. (1991) Laparoscopic common bile duct exploration. J Laparoendosc Surg 1: 287–293
Surick BG, Ghazi A (1992) Endoscopic papillotomy while the gallbladder is in-situ. Am Surg 58: 657–660
The Southern Surgeons Club (1991) A prospective analysis of 1518 laparoscopic cholecystectomies performed by Southern U.S. surgeons. N Engl J Med 324: 1073–1078
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Surick, B., Washington, M. & Ghazi, A. Endoscopic retrograde cholangiopancreatography in conjunction with laparoscopic cholecystectomy. Surg Endosc 7, 388–392 (1993). https://doi.org/10.1007/BF00311726
Issue Date:
DOI: https://doi.org/10.1007/BF00311726