
Abstract
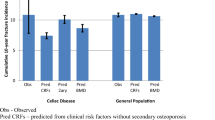
The association of celiac disease with fracture is controversial. Recent studies may have underestimated the impact by studying patients with low fracture risk. Since postmenopausal women are at greatest risk of fracture, we have investigated non-spine fracture occurrence in women ≥50 years with celiac disease. Patients were recruited from hospital and general practice as well as from volunteers, controls from general practice. All completed a questionnaire detailing fracture occurrence. Three hundred and eighty-three female celiac patients and 445 female controls aged ≥50 years at time of study were compared. Mean age was 61.4±7.8 years in celiac patients and 62.7±9.9 years in controls. Celiac patients were lighter but not shorter. Celiac patients displayed greater “all fracture” prevalence (odds ratio [OR], 1.51; confidence interval [CI], 1.13:2.02) and fracture after 50 years (OR, 2.20; CI, 1.49:3.25). Wrist fracture was more frequent (OR, 1.65; CI, 1.12:2.41), but significance was lost once height and weight were taken into account. Celiac patients had more multiple fractures (OR, 2.96; CI, 1.81:4.83). To investigate the association of fracture with time from diagnosis, 324 celiac patients were paired with a control by age. No excess fracture risk was found more than 10 years before diagnosis amongst celiac patients diagnosed after age 50 years, but risk increased in the period from 10 years before diagnosis to 5 years after and remained high more than 5 years after diagnosis ( p<0.05). Wrist fracture only increased in the period more than 5 years after diagnosis ( p<0.05). In women diagnosed before 50 years, no excess fracture risk existed. Fracture risk in female celiac patients >50 years is increased overall but is related largely to the peri-diagnostic period. Wrist fracture risk is partly accounted for by height and weight, but is more common more than 5 years after diagnosis. Celiac testing may be indicated in thin women over 50 years with multiple fractures, and after diagnosis adequate calcium and vitamin D intake should be ensured.
Similar content being viewed by others

References
Kemppainen T, Kroger H, Janatuinen E, Arnala I, Kosma VM, Pikkarainen P, Julkunen R, Jurvelin J, Alhava E, Uusitupa M (1999) Osteoporosis in adult patients with celiac disease. Bone 24:249–255
Pistorius LR, Sweidan WH, Purdie DW, Steel SA, Howey S, Bennett JR, Sutton DR (1995) Coeliac disease and bone mineral density in adult female patients. Gut 37:639–642
Selby PL, Davies M, Adams JE, Mawer EB (1999) Bone loss in celiac disease is related to secondary hyperparathyroidism. J Bone Miner Res 14:652–657
Fickling WE, McFarlane XA, Bhalla AK, Robertson DA (2001) The clinical impact of metabolic bone disease in coeliac disease. Postgrad Med J 77:33–36
Vasquez H, Mazure R, Gonzalez D, Flores D, Pedreira S, Niveloni S, Smecuol E, Maurino E, Bai JC (2000) Risk of fractures in celiac disease patients: a cross-sectional, case-control study. Am J Gastroenterol 95:183–189
Vestergaard P, Mosekilde L (2002) Fracture risk in patients with celiac Disease, Crohn’s disease, and ulcerative colitis: a nationwide follow-up study of 16,416 patients in Denmark. Am J Epidemiol 156:1–10
Thomason K, West J, Logan RF, Coupland C, Holmes GK (2003) Fracture experience of patients with coeliac disease: a population-based survey. Gut 52:518–522
West J, Logan RF, Card TR, Smith C, Hubbard R (2003) Fracture risk in people with celiac disease: a population-based cohort study. Gastroenterology 125:429–436
Walters JR, van Heel DA (2003) Detecting the risks of osteoporotic fractures in Coeliac disease. Gut 52:1229–1230
Vestergaard P, Mollerup CL, Frokjaer VG, Christiansen P, Blichert-Toft M, Mosekilde L (2000) Cohort study of risk of fracture before and after surgery for primary hyperparathyroidism. BMJ 321:598–602
Scott EM, Gaywood I, Scott BB (2000) Guidelines for osteoporosis in coeliac disease and inflammatory bowel disease. British Society of Gastroenterology. Gut 46 [Suppl 1]:1–8
Pazianas M, Butcher GP, Subhani JM, Finch PJ, Ang L, Collins C, Heaney RP, Zaidi M, Maxwell JD ( 2004) Calcium absorption and bone mineral density in celiacs after long-term treatment with gluten-free diet and adequate calcium intake. Osteoporos Int Jun 17 [Epub ahead of print]
Taranta A, Fortunati D, Longo M, Rucci N, Iacomino E, Aliberti F, Facciuto E, Migliaccio S, Bardella MT, Dubini A, Borghi MO, Saraifoger S, Teti A, Bianchi ML (2004) Imbalance of osteoclastogenesis-regulating factors in patients with coeliac disease. J Bone Miner Res 19:1112–1121
Cummins AG, Penttila IA, Labrooy JT, Robb TA, Davidson GP (1991) Recovery of the small intestine in coeliac disease on a gluten-free diet: changes in intestinal permeability, small bowel morphology and T-cell activity. J Gastroenterol Hepatol 6:53–57
Crofton RW, Glover SC, Ewe SW, Baggett PJ, Moat NA, Mills CF (1983) Zinc absorption in celiac disease and dermatitis herpetiformis: a test of small intestinal function. Am J Clin Nutr 38:706–712
Molteni N, Bardella MT, Vezzoli G, Pozzoli E, Bianchi P (1995) Intestinal calcium absorption as shown by stable strontium test in Coeliac disease before and after gluten-free diet. Am J Gastroenterol 90:2025–2028
Sategna-Guidetti C, Grosso SB, Grosso S, Mengozzi G, Aimo G, Zaccaria T, Di Stefano M, Isaia GC (2000) The effects of 1-year gluten withdrawal on bone mass, bone metabolism and nutritional status in newly diagnosed adult Coeliac disease patients. Aliment Pharmacol Ther 14:35–43
Companion T, Kroger H, Anatine E, Anal I, Lamberg-Allardt C, Karkkainen M, Kosma VM, Julkunen R, Jurvelin J, Alhava E, Uusitupa M (1999) Bone recovery after a gluten-free diet: a 5-year follow-up study. Bone 25:355–360
Bai JC, Gonzalez D, Mautalen C, Mazure R, Pedreira S, Vazquez H, Smecuol E, Siccardi A, Cataldi M, Niveloni S, Boerr LA, Maurino E (1997) Long-term effect of gluten restriction on bone mineral density of patients with Coeliac disease. Aliment Pharmacol Ther 11:157–164
O’Loughlin PD, Morris HA (1998) Oestrogen deficiency impairs intestinal calcium absorption in the rat. J Physiol 511 (Part 1):313–322
Heaney RP, Recker RR, Stegman MR, Moy AJ (1989) Calcium absorption in women: relationships to calcium intake, estrogen status, and age. J Bone Miner Res 4:469–475
Gonzalez D, Sugar E, Gomez JC, Oliveri MB, Gomez Acotto C, Vega E, Bagur A, Mazure R, Maurino E, Bai JC, Mautalen C (2002) Is it necessary to screen for celiac disease in postmenopausal osteoporotic women? Calcif Tissue Int 71:141–144
Mather KJ, Meddings JB, Beck PL, Scott RB, Hanley DA (2001) Prevalence of IgA–antiendomysial antibody in asymptomatic low bone mineral density. Am J Gastroenterol 96:120–125
Ismail AA, O’Neill TW, Cockerill W, Finn JD, Cannata JB, Hoszowski K, Johnell O, Matthis C, Raspe H, Raspe A, Reeve J, Silman AJ (2000) Validity of self-report of fractures: results from a prospective study in men and women across Europe. EPOS Study Group. European Prospective Osteoporosis Study Group. Osteoporos Int 11:248–254
Ivers RQ, Cumming RG, Mitchell P, Peduto AJ (2002) The accuracy of self-reported fractures in older people. J Clin Epidemiol 55:452–457
Honkanen K, Honkanen R, Heikkinen L, Kroger H, Saarikoski S (1999) Validity of self-reports of fractures in perimenopausal women. Am J Epidemiol 150:511–516
Hadjivassiliou M, Chattopadhyay AK, Davies-Jones GA, Gibson A, Grunewald RA, Lobo AJ (1997) Neuromuscular disorder as a presenting feature of Coeliac disease. J Neurol Neurosurg Psychiatry 63:770–775
Williams SF, Mincey BA, Calamia KT (2003) Inclusion body myositis associated with celiac sprue and idiopathic thrombocytopenic purpura. South Med J 96:721–723
Acknowledgements
Funding was obtained from Procter and Gamble Pharmaceuticals and from the Bone Disease Foundation
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Davie, M.W., Gaywood, I., George, E. et al. Excess non-spine fractures in women over 50 years with celiac disease: A cross-sectional, questionnaire-based study. Osteoporos Int 16, 1150–1155 (2005). https://doi.org/10.1007/s00198-004-1822-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-004-1822-z