
Abstract
Acute nonvariceal upper gastrointestinal (UGI) hemorrhage is a frequent complication associated with significant morbidity and mortality. The most common cause of UGI bleeding is peptic ulcer disease, but the differential diagnosis is diverse and includes tumors; ischemia; gastritis; arteriovenous malformations, such as Dieulafoy lesions; Mallory-Weiss tears; trauma; and iatrogenic causes. Aggressive treatment with early endoscopic hemostasis is essential for a favorable outcome. However, severe bleeding despite conservative medical treatment or endoscopic intervention occurs in 5–10% of patients, requiring surgery or transcatheter arterial embolization. Surgical intervention is usually an expeditious and gratifying endeavor, but it can be associated with high operative mortality rates. Endovascular management using superselective catheterization of the culprit vessel, « sandwich» occlusion, or blind embolization has emerged as an alternative to emergent operative intervention for high-risk patients and is now considered the first-line therapy for massive UGI bleeding refractory to endoscopic treatment. Indeed, many published studies have confirmed the feasibility of this approach and its high technical and clinical success rates, which range from 69 to 100% and from 63 to 97%, respectively, even if the choice of the best embolic agent among coils, cyanaocrylate glue, gelatin sponge, or calibrated particles remains a matter of debate. However, factors influencing clinical outcome, especially predictors of early rebleeding, are poorly understood, and few studies have addressed this issue. This review of the literature will attempt to define the role of embolotherapy for acute nonvariceal UGI hemorrhage that fails to respond to endoscopic hemostasis and to summarize data on factors predicting angiographic and embolization failure.
Similar content being viewed by others

Introduction
Upper gastrointestinal (UGI) bleeding is defined as bleeding originating at the level of the distal esophagus, the stomach, and the duodenum (proximal to the ligament of Treitz). The most common cause of nonvariceal UGI bleeding is peptic ulcer disease, but the differential diagnosis is diverse and includes benign and malignant tumors; ischemia; gastritis; arteriovenous malformations, such as Dieulafoy lesions; Mallory-Weiss tears; trauma; and iatrogenic causes [1, 2]. Effective treatment requires an accurate diagnosis (location and etiology), and unlike lower gastrointestinal bleeds, most patients have undergone endoscopic examination and treatment before their referral to interventional radiology. Of the small group of patients whose bleeding fails to respond to endoscopic therapy, some are treated surgically [3], but increasingly the majority are referred for embolotherapy [4]. Surgery is typically reserved for those patients whose bleeding failed to respond all previous treatments. In such cases, conservative surgical techniques to focus the bleeding source, including vagotomy and pylorotomy in the case of peptic ulcer bleeding, are usually preferred to conventional definitive surgery, which has rebleeding rates ranging from 3 to 29% [3]. Transcatheter arterial embolization (TAE) has been performed for at least three decades and has been shown to be effective at controlling hemorrhage and decreasing mortality [5–10]. However, few published series analyzed factors predicting angiographic and embolization failure. The purpose of this review is to summarize data on outcomes and factors that may influence the outcome of patients who have undergone embolization procedures for acute nonvariceal UGI hemorrhage.
Methods for Literature Review
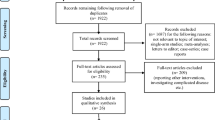
We conducted a review of the English literature and identified case series on embolization for acute nonvariceal UGI bleeding from 1992 to 2009 using PubMed queries. Further bibliography was added by manual searches of reference lists. Studies were selected for review when they had well-defined indications for intervention and offered a detailed description of outcomes, including technical and clinical success rates, rebleeding and reintervention rates, need for surgery to control bleeding, and morbidity and mortality rates. For the assessment of clinical and technical factors affecting success, only studies with statistical analysis of predictors of outcome were included. To avoid selection bias associated with small series, studies with <20 patients and case reports were excluded. Results were tabulated and presented as absolute numbers and percentage. Averages for the outcomes of interest were also calculated. Information on indications, technique, complications, predictors of rebleeding, and a variety of other topics of interest are presented as a narrative to provide a more thorough understanding of the current status and controversial issues related to the endovascular treatment of UGI bleeding.
Indictions for Angiography
TAE as an alternative to surgery for the control of UGI hemorrhage was introduced by Rosch et al. in 1972 [5]. Since then, arterial catheterization has become a useful diagnostic and therapeutic tool in selected populations [11]. The typical candidate patient presents with the following: (1) massive bleeding (transfusion requirement of at least 4 U blood/24 h) or hemodynamic instability (hypotension with systolic pressure <100 mm Hg and heart rate of 100 min−1 or clinical shock secondary to blood loss), (2) bleeding that has failed to respond to conservative medical therapy, including volume replacement, antacids, H2-receptor blocking agents, or proton pump inhibitors, and (3) bleeding that has failed to respond to at least one, and sometimes two, attempts at endoscopic control [12]. At that point, low-risk patients are offered the option of surgical intervention, whereas high-risk individuals are directed toward percutaneous embolotherapy. Finally, endovascular treatment can be used after open intervention has failed and bleeding recurs [9].
Techniques of Angiography and Embolization
Angiography
Diagnostic angiography for UGI bleeding is straightforward and is centered on the anatomy of the celiac artery. Specifically, the celiac artery gives rise to the left gastric artery, which provides branches to the distal esophagus and fundus of the stomach. These branches also communicate with distal branches of the small, short gastric arteries from the splenic artery and branches of the right gastric artery. The latter is usually a small artery that originates from the left or common hepatic artery, but it is often not visualized angiographically. The remainder of the stomach and duodenum are supplied by branches from the gastroduodenal artery (GDA). The superior mesenteric artery (SMA) may supply portions of the duodenum, mostly by way of pancreaticoduodenal anastomoses, which for the most part are important angiographically as a rich collateral supply keeping the stomach and duodenum viable after celiac branch embolization, but it also may be responsible for rehemorrhage after embolotherapy. Anatomic variations in the celiac anatomy, most notably in the origins of the hepatic arteries, occur in at least 50% of the population. Such variations must always be considered when evaluating a patient angiographically for UGI bleeding [13].
In the setting of UGI bleeding, the source for hemorrhage is usually identified by endoscopy. Therefore, angiography is most often performed only as a precursor to transcatheter embolotherapy based on the known vascular supply to the area of abnormality. A positive examination is classically described as extravasation of contrast into the bowel lumen or false aneurysm-like lesion. However, an abnormal blush of the mucosal surface of the UGI tract is indicative of an inflammatory process (gastritis or duodenitis), which, if correlated with endoscopic findings, may also be considered a positive angiographic examination. Angiography in the setting of UGI bleeding is positive for extravasation or abnormal mucosal blush in ≤61% of cases [13]. There is much discussion about the necessity of diagnostic studies before angiography. Computed tomography angiography (CTA) has been used accurately (with a sensitivity up to 86%) in the diagnosis of acute gastrointestinal bleeding and can show the precise location and etiology of bleeding, thereby directing further management [14]. However, the use of this technique necessitates hemodynamic stability.
By the time a patient with an UGI bleeding reaches the interventional suite, he or she should be fluid resuscitated, hemodynamically stable, and have any coagulopathy corrected. Blood products, such as fresh frozen plasma, platelets, or packed red blood cells (RBCs), may also be given intraprocedurally. It is desirable to correct any coagulopathy before embolization because achieving hemostasis depends on technically successful embolization as well as the patient’s ability to clot properly. However, in the case of acute bleeding, arteriography with embolization should be promptly performed and soon followed by coagulopathy correction. A transfemoral approach was used by most investigators in the series we reviewed and involves placement of a 5F sheath in the common femoral artery. A variety of introducers and selective catheters with a smaller caliber can be used to cannulate the celiac artery and obtain access to the common hepatic artery. For selective catheterization by way of the femoral route, the most widely used catheter configurations are the cobra, hook, and short- and long-curve sidewinder with a 4F diameter. Once access is secured, arteriogram is performed to delineate the anatomy and identify contrast extravasation. Selective catheterization for UGI bleeding includes the celiac and superior mesenteric arteries. The initial artery catheterized is the one most suspected of bleeding based on previous imaging or endoscopy, which is, of course, the celiac artery for UGI bleeding. If no extravasation is seen, then superselective angiography is advised, depending on endoscopic findings that offer information on the likely location of the bleeding source: superselective catheterization of the GDA (Fig. 1), the left gastric artery (Fig. 2), or the splenic artery (Figs. 3 and 4) may be performed. A microcatheter is always necessary for a distal and superselective approach to the bleeding as well as to avoid the spasm caused by catheters with a 4F or 5F caliber. Longer injection durations or use of carbon dioxide for contrast medium can also improve sensitivity for small bleeds. CTA is also a good and reliable method to highlight the presence of a bleed in progress and should be performed before any invasive procedure in the absence of hemodynamic instability. Arteriography after superselective cannulation may show extravasation that could have been missed during contrast injection in the main hepatic artery. When a dual supply of the bleeding area is suspected, both arterial sources must be embolized to assure that all of the inflow ceases. This is the typical case of bleeding secondary to an ulcer that erodes into the GDA. Embolization in this case must start distally to prevent persistent “backdoor” hemorrhage from the right gastroepiploic and superior pancreaticoduodenal arteries and then proceed to the proximal side of the erosion.

Typical sandwich embolization in a 73-year-old man with bleeding from a postbulbar duodenal ulcer at endoscopy. A and B Selective angiography of the celiac trunk and superselective arteriogram of the GDA before embolization show no evidence of active bleeding. C Result after blind coil embolization of the distal and proximal GDA (with gelatin sponge placed in the arterial trunk), including the anterior and posterior superior pancreaticoduodenal arteries and the right gastroepiploic artery, to prevent retrograde flow (arrows). No ischemic complications were reported

Bleeding dieulafoy lesion in an 87-year-old man. A and B Extravasation of contrast medium from the left gastric artery at the celiac trunk and superselective angiography indicates continuing bleeding (arrows). C After arterial microcatheterization, bleeding was controlled after embolization of the left gastric artery using a Glubran/Lipidol mixture (1:3) (arrows)

Digital subtraction images of a 37-year-old man with massive hematemesis. A and B Selective angiography shows a bleeding ulcer in the fundus of the stomach. Extravasation of contrast medium from a branch of the left gastroepiploic artery is seen (arrows). C Control angiogram after glue (Glubran) embolization throughout the splenic artery using a 3F microcatheter shows complete and superselective occlusion of the bleeding branch, with no active bleeding. The patient was discharged from the hospital 4 days later

A 68-year-old man with acute hematemesis. A and B Selective and superselective arteriograms showing contrast medium extravasated from a slender branch of the left gastroepiploic artery (arrows). C and D After microcatheterization, superselective coil embolization ensured control of the bleeding (arrows); there were no early or late recurrences
Embolization
In cases of active hemorrhage with extravasation of contrast, the bleeding vessel is identified by superselective catheterization with a microcatheter and embolized with microcoils or glue if arterial flow is not blocked by the microcatheter. If no evidence of bleeding is found on pre-embolization arteriography, then blind embolization, defined as embolization without angiographic proof of extravasation, is advised and is typically guided by endoscopic information regarding the location of the bleeding vessel (Fig. 1). Coils and gelatine sponge are then used in such a situation. Another useful maneuver in this scenario requires clips to be placed around the area of bleeding during pre-embolization endoscopy. The clips remain in position for several hours and allow for an educated guess of the location of the culprit vascular branch [15]. If no extravasation is seen despite the injection of contrast, then the branches terminating to the clip are superselected using microcatheter techniques and embolized. Arteriography at multiple projections is necessary at this step to ensure the relation between the clip and the adjacent branches. Infusion of a fibrinolytic agent, such as t-PA, intra-arterial anticoagulants, or vasodilators, to temporarily increase the rate of hemorrhage during angiography has been tried by some with success, thereby facilitating angiographic identification and localization of the bleeding lesion [16, 17]. Finally, “sandwich” occlusion can be used at the level of the GDA: the catheter is pushed to the origin of the right gastroepiploic artery, and coils are introduced as the catheter is withdrawn to the proximal GDA. Complete embolization of the GDA, which inlcudes proximal and distal embolization and exclusion of its two side branches, is the end point in this case. A selective superior mesenteric arteriogram is made after embolization to ensure that no collateral supply to the bleeding site is present. If extravasation is identified, superselective catheterization of the inferior pancreaticoduodenal artery and the side branch responsible for the collateral circulation is performed with the microcatheter. Embolization with microcoils of the bleeding site is performed as distal as possible.
Synopsis of Outcomes in Case Series
Procedural and Clinical Outcomes
We identified 15 studies (819 patients, mean age 65 years) on endovascular management of intractable nonvariceal UGI bleeding (Tables 1 and 2). Among them, only seven studies identified factors affecting the success of embolotherapy using statistical analysis (Table 3). Endoscopy had been performed and failed in 99% of patients: significant amount of blood in the stomach, large ulcer size, location of lesion at posterior bulbar duodenum, multiple lesions, and lesser curve were identified as causes for endoscopic failure. The majority of patients treated endovascularly in the series under review had significant comorbidities and was deemed high risk for operative intervention. Endovascular embolization was successful technically in 762 (93%) patients (Table 1). The causes for endovascular technique failure were as follows: difficult vascular anatomy, arterial dissection, vasospasm, false-negatively read angiogram, multiple bleedings, and tumorous bleeding. A variety of embolic materials, including coils, polyvinyl alcohol (PVA) particles, blood clot, Gelfoam, and cyanoacrylate glue were used. The sandwich technique, with placement of embolic material at both sides of the bleeding vessel, was used in most series to minimize the chance of recurrent bleeding caused by rich collaterals. Active extravasation was present at the time of embolization in only 442 (54%) patients. Three factors may contribute to explain this finding. First, superselective catheterization of all potential involved branches was not always performed by all investigators. Second, provocative pharmacoarteriography was almost never carried out. Third, the likelihood of identifying the bleeding source is higher when the arteriogram is performed promptly after bleeding, e.g., in hemodynamically unstable patients, and when CTA performed before angiography shows extravasation. Unfortunately, neither the mean time from hypovolemic shock onset to angiography, nor whether CT was performed before referral for angiography, is specified in most of studies. Consequently, 46% of patients underwent blind embolization guided by the findings on endoscopy or placement of clips around the area of the bleeding vessel. In most cases, gelatin sponge or coils were then used for embolization. From the subgroup that underwent technically successful embolization, 549 (67%) patients responded well clinically and had cessation of bleeding (Table 2).
Thirty-three percent of patients continued to bleed, but almost half of them responded to repeat embolization. The possible causes of failure were not clearly identified in most series, but some investigators reported predictors of rebleeding as the presence of multiple or large duodenal ulcers, gastritis, coagulopathy, or multiorgan failure. Finally, 20% (164) of patients underwent open surgical intervention to definitively manage the bleeding source (Table 2). Major and minor embolization-related complications developed in 9% (74) of patients and included access site complications, dissection of the target vessel, and liver and spleen infarction. The most significant long-term complication was duodenal stenosis in a series by Lang et al. [18], particularly after glue embolization of terminal muscular branches of the GDA (25%). The overall 30-day mortality rate was 28% (229 patients) (Table 2). Unfortunately, it was difficult to extract data with regard to different causes of death and assess their relation with the success of the embolization or the need for a subsequent procedure. Although the mortality rate appears to be as high as in some surgical series for emergent open repair of UGI bleeding, one should keep in mind that the patients treated with embolotherapy had been, on most occasions, turned down for open repair due to significant comorbidities and advanced age. Due to variability in the way the results were reported, and the difficulty in obtaining a precise risk factor profile of the population in these series, it is not possible at present to make comments regarding impact of embolotherapy on mortality. A closer look into this review of outcomes and the individual studies underscores a few important points. First, mortality and complication rates exhibited wide variability among series, further emphasizing the importance of individual expertise and center experience in outcomes. Second, the presence of active extravasation and superselective embolization does not necessarily imply better short-term clinical response, a phenomenon that may be explained by the intermittent nature of the gastrointestinal bleeding and the presence of bleeders that were missed with the very selective embolotherapy. Last, only 20% of the patients who initially underwent embolization finally needed surgical intervention to control recurrent bleeding, indicating that embolotherapy can decrease the incidence of laparotomy in patients presenting with acute UGI bleeding. Surgery was usually performed after failure of second endoscopic hemostasis or embolization procedure at the discretion of the gastroenterologists or surgeons.
Complications
Groin hematomas (3–17%) and contrast-related complications (0.04–12.7%) can occur with the same frequency as in other endovascular procedures [19, 20]. Acute renal failure may occur, and its etiology is multifactorial, related to the contrast injection in the context of hemorrhage and volume depletion. Arterial embolization in the UGI tract above the ligament of Treitz is generally considered very safe because of the rich collateral supply to the stomach and duodenum. However, the risk of significant ischemia after embolization is known to increase in patients with previous surgery within the same area [21] or with embolic agents that can advance far into the vascular bed, such as liquid agents (e.g., tissue adhesives, such as cyanoacrylate) or very small particles (e.g., gelatin sponge powder or calibrated microspheres) [21–24]. Although cases have been reported at the acute phase, postembolization ischemia usually presents as duodenal stenosis at the chronic phase. Lang et al. [18] reported duodenal stenosis in 7 of 28 patients 8 months to 7 years after embolization of terminal vessels, mostly when tissue adhesive was used. In this series, duodenal stenosis after GDA embolization was far less common and occured in only 2 of 29 patients who underwent more proximal GDA occlusion. The high incidence of stenosis of the duodenum, which is attendant on embolization of the terminal vessels of a bleeding site, is thought to be the consequence of severe hypoxia and resultant avascular necrosis. Surgical correction of the stenosis was necessary in 8 patients to address persistent symptoms. Another patient had to undergo multiple balloon dilatations for duodenal stenosis. Balloon dilatations were performed in 1 additional patient after surgical resection and recurrent symptoms of duodenal obstruction.
Inadvertent embolization of the main hepatic artery can result in a broad spectrum of manifestations, ranging from a temporary increase in the liver enzymes to life-threatening hepatic failure, with the latter being more common in the setting of cirrhosis and associated compromise of the portal vein circulation [25]. Inadvertent placement of coils in the main branches of the celiac axis has been reported in ≤ 3.3% of cases [26], usually in keeping with technical difficulty or coil migration. Given the rich collateral circulation, however, coils in the left gastric or splenic artery rarely produce organ-threatening ischemia [27].
Predictors of Outcomes
Factors Affecting Success
Although conclusions from all retrospective studies must be drawn with caution, some investigators have identified several clinical and technical factors that may influence the embolization outcome (Table 3).
Clinical Predictors of Rebleeding
Coagulopathy has been shown to adversely affect the success rate for embolotherapy, with an increase in the odds ratio for clinical failure, which ranges from 2.9 to 19.6 [7, 25–27]. Indeed, Encarnacion et al. [7] first identified the presence or absence of coagulopathy as a major factor affecting embolization outcome. Although the investigator did not consider other technical or clinical variables in their study, they did find that embolization was 2.9 times more likely to fail in patients with coagulopathy, and death from bleeding after embolization was 9.6 times more likely to occur in this group. Despite these odds, the investigators reported successful angiographic bleeding control in 6 of 14 (43%) patients. Similarly, Schenker et al. [27] were able to achieve bleeding control with angiographic embolization in 43 of 93 (46%) patients with coagulopathy. Consequently, although every effort should be made to correct coagulopathy before, during, and after intervention, patients with coagulopathy should by no means be excluded from angiographic treatment for emergent arterial UGI hemorrhage.
Other clinical variables have been identified as predictors of early rebleeding after embolization. Loffroy et al. [26] recently reported their large experience in treating 60 patients with peptic ulcer bleeding. Devascularization was achieved in 57 of 60 patients (technical success of 95%). In 37% (n = 22) of patients, angiography failed to demonstrate contrast extravasation, and therefore blind embolization was performed. This was guided by endoscopic findings before the procedure. Approximately 28% (n = 16) of these patients bled again, and only three had repeat embolization. Of the 16 rebleeding events in this study, 15 occured after embolization of the GDA and its branches. According to the investigator, the abundant collateral circulation in the duodenum probably explained this finding. Interestingly, several of the variables that were studied in this series such as coagulation disorders, a longer time from shock onset to angiography, a larger number of RBC units transfused before angiography, and having ≥2 comorbid conditions were found by univariate analysis to be associated with early rebleeding. In addition, clinical outcomes were significantly influenced by the presence of coagulation disorders (P = 0.027) by multivariate analysis, which was found to predict failure embolization. In addition, the presence of >2 comorbidities and time to angiography >2 days were associated with rebleeding in the univariate analysis, specifically in patients with coagulation disorders. Thus, the ability to achieve bleeding control in critically ill patients seems to depend chiefly on early intervention and severity of the underlying disease. Even if comorbid conditions was not identified as a predictor of rebleeding in the multivariate analysis because of intercorrelation with coagulopathy in this study, recurrence of bleeding was associated with comorbidities in the univariate analysis and probably depends on the clinical setting and whether or not the patient has the ability to clot. Walsh et al. [23] found longer time to angiography (P = 0.01), more total units of packed RBCs (P = 0.03), and previous surgery for bleeding (P = 0.02) to be predictors of embolization failure by multivariate analysis. The study by Poultsides et al. [28] agreed with the earlier findings, indicating that recent duodenal ulcer surgery (P = 0.03) and blood transfusion of > 6 U RBCs before the procedure (P = 0.04) were independent predictors of poor embolization outcome. Last, in the series from Defreyne et al. [29], low hemoglobin concentration (<80 g l−1) and shock were more frequently observed in patients with early failure, which points to the severe and brisk character of UGI hemorrhage. Clinical signs of shock and active bleeding at admission are known risk factors for rebleeding after endoscopic therapy [30]; hence, they are probably risk factors for early recurrence after embolization as well. In this study, corticosteroid intake was also considered to be a statistically significant risk factor for rebleeding after embolization, probably because it retards the wound-healing effect. Corticosteroid use is more often encountered in inpatients with bleeding than in those with primary-referred UGI hemorrhage [31], but it has not yet been reported to be an independent risk factor for rebleeding.
Technical Predictors of Rebleeding
Blind Embolization
Blind embolization is also controversial. Because massive bleeding is often intermittent [32], most groups have adopted a policy to embolize on the basis of endoscopic findings even in situations where no extravasation is seen angiographically [33]. In the series from Aina et al. [25], Loffroy et al. [26], and Padia et al. [34] there was no difference of outcome between patients who underwent blind embolization and those who underwent embolization after a bleeding site had been demonstrated angiographically. Other researchers have also advocated the practice of endoscopy-directed blind embolization [6, 35, 36]. Based on the findings from the literature and our own experience, we believe that blind embolization is appropriate. The GDA should be embolized using the sandwich technique, in which both ends of the artery are filled with coils to avoid retrograde bleeding from the superior mesenteric circulation. If there is suspicion that smaller muscular branches terminating to a clip are the culprits, then those should be embolized with any of the materials available.
Marking with a Metallic Clip
Eriksson et al. [15] reported a series of ten patients who were referred for embolotherapy after failed endoscopic attempt to control bleeding from acute duodenal ulcer. To guide the endovascular treatment, the endoscopists marked the site of bleed with clips placed at the junction of the ulcer and the adjacent normal mucosa. In eight patients hemostasis was achieved after embolization, whereas surgical intervention was necessary in the other two patients. The clips accurately guided the endovascular intervention in six patients who had no evidence of contrast extravasation at the time of angiography. This was of particular importance in three patients: in two patients, the culprit vessel was a supraduodenal artery without connection to the GDA, whereas one patient had bleeding from erosion into the inferior pancreaticoduodenal artery that was arising from the SMA. Marking with a metallic clip can assist with localization of the vessel feeding the bleeding ulcer even if there is no contrast medium extravasation after injection with the catheter in the common hepatic or the main trunk of the GDA. This is also important when the bleeding artery arises separately from the proper hepatic artery or the GDA. Superselective angiography guided by clip position has better chances to demonstrate the extravasation, making blind coil placement unnecessary, thus increasing the efficacy of the procedure and decreasing the risk of coil misplacement and inadvertent hepatic embolization [15, 26]. The only limitation of this technique is the need for around-the-clock availability of an experienced interventionalist and gastroenterologist, which is easy to achieve only in high-volume medical centers.
Choice of Embolic Agent
More controversial is the influence of the type of embolic agent on the clinical outcome. It is generally accepted that embolic therapy is superior to vasopressin infusion for the treatment of UGI hemorrhage from gastroduodenal ulcers [11]. The choice of the best embolic agent is still debatable. In most series, this choice was at the discretion of the interventional radiologist, according to his or her own experience, material availability, angiographic findings, and capability to perform superselective catheterization of the bleeding vessel. Coils alone inserted in the GDA or superselectively in the pancreaticoduodenal arteries have been used with success by several investigators [35, 37, 38]. Lang et al. [18] compared several embolic agents in a series of 57 patients. They achieved the best results in terms of safety and efficacy with the use of autologous blood clot for proximal gastroduodenal embolization and tissue adhesive for occlusion of the distal vasculature of the GDA. These investigators reported a 40% rate of duodenal stricture when tissue adhesives were used, a finding that may be related to the fact that tissue adhesives were used to embolize terminal muscular branches and not to the choice of embolization agent. The same group reported that a high rate of bleeding recurrence was observed when PVA particles or Gelfoam were used alone. Similarly, Encarnacion et al. [7] achieved a low success rate (62%) in their series, which included mostly patients embolized with gelatin sponge alone. These data confirm that the use of gelatin sponge as the only embolic agent guarantees only short-term results and should probably be avoided. Good results were also reported with cyanoacrylate [39, 40] and with the combination of gelatin sponge and coils [41]. Toyoda et al. [40] reported that the time for TAE using n-butyl cyanoacrylate was significantly faster than for TAE procedures that do not use n-butyl cyanoacrylate. This is important particularly in cases of massive bleeding that require urgent hemostasis, especially in patients with coagulopathy. Loffroy et al. [41] reported early clinical success in 22 (64.7%) of 34 patients treated by sandwich embolization of the GDA using coils released distally and proximally in combination with gelatin sponge placed in the arterial trunk. However, because most of these series included small study populations, no statistical conclusions can be drawn from these data. Finally, Aina et al. [25] compared embolization with coils alone versus a combination of coils and PVA particles or Gelfoam. Multivariate regression analysis in his study showed an association between the use of coils alone and the incidence of bleeding recurrence in patients with coagulopathy, a finding that supports the use of PVA or Gelfoam in association with coils when choosing a strategy for this subgroup of patients. Loffroy et al. [26] also demonstrated that the use of coils as the only embolic agent was significantly associated with early rebleeding in both univariate and multivariate analysis (P = 0.03 and 0.022, respectively). These findings may be explained by the fact that almost all of rebleeding events occured after coil embolization of the GDA and that most of these patients underwent sandwich embolization without coiling of the arterial trunk of the GDA. It is well known that successful embolization with spirals depends on their number. They concluded that coils probably should not be used as the only embolic agent but rather in association with Gelfoam, particles, or glue for the treatment of gastroduodenal hemorrhage, especially when using the sandwich technique. Otherwise, the choice of embolic agent does not seem to affect clinical response or recurrence rates.
Factors Affecting Survival
In general, the mortality rate of patients with UGI hemorrhage from gastroduodenal ulcers who do not respond to conservative therapy ranges from 17% to 43% in surgical series [42, 43]. Factors influencing mortality include advanced age, trauma or sepsis, recent major operation, lung or liver disease, and massive blood transfusions [43, 44]. After embolization in patients too sick to undergo open intervention, the mortality rate of patients with UGI hemorrhage is rather similar and varies between 10 and 45%. One explanation may be the fact that most patients treated with embolization are often significantly older and have more comorbidities than those managed surgically. A number of factors have been identified as influencing postembolization mortality. One of the most important and frequently encountered is the absence of early recurrent bleeding, especially after superselective embolization of a vessel with contrast extravasation on initial angiography. Patients with angiographic extravasation exhibit a marked decrease in mortality when embolization is successful compared with patients requiring surgery after failed embolization (38 vs. 83% mortality rate) [45]. A strong correlation has been seen between coagulopathy, clinical failure, and mortality after embolization: patients with impaired coagulation profile are 3 times more likely to rebleed after initially successful embolization and 10 times more likely to die as a result of bleeding compared with those having normal coagulation status [7, 25]. Rescue surgery after a failed attempt for embolization has a high mortality that exceeds even the 50% death rate with emergency surgery [46, 47]. In other series, underlying medical problems, such as cirrhosis and malignancy, have a major impact on the mortality rate. Finally, in the presence of multisystem organ failure, a clinical successful embolization appears to offer the only chance for survival. In the series from Schenker et al. [27], the mortality was 96% in patients with multisystem organ failure who did not respond to embolization versus 31% in those who did respond.
Topics of Interest
Long-Term Follow-Up
Long-term results in 57 patients who underwent angiography and embolization for bleeding from the UGI tract have been published by Lang et al. [18]. Control of bleeding was accomplished in 52 of 57 patients. Superselective terminal muscular branch embolization was as effective as embolization of the main GDA. In 8 of these patients, a second catheter-based intervention was necessary within 30 days to completely stop the hemorrhage. Notably, 29 of the 52 patients who were embolized successfully bled again during the follow-up period (3 months to 7 years after the initial embolization procedure) at the level of the GDA, indicating the need for aggressive long-term risk factor modification and treatment for the underlying peptic ulcer disease. Long-term bleeding control was more likely in the subgroup of patients who underwent superselective terminal muscular branch embolization compared with patients who underwent embolization of the main GDA trunk (53 vs. 27%, P = 0.084). Long-term success in this series was related to the embolic material used. For occlusion of the muscular branch arteries, 6-cyanoacrylate had the highest success rate, whereas for occlusion of the main GDA, epsilon-aminocaproic acid–induced blood clot was superior to other materials (coils, gelatin sponge particles, or PVA particles).
Embolization Versus Surgery
To date, no controlled trial has compared angiographic embolization with surgery as a salvage procedure for failed endoscopic therapy. The wide array of alternatives for the treatment of UGI bleeding after endoscopic failure make the decision of when to resort to emergency surgery more difficult, especially in patients with risk factors for recurrent bleeding and death, which are also related to high surgical risk. Law et al. [48], in a randomized controlled study, showed no differences in bleeding control between a second endoscopic treatment and surgery after initial endoscopic treatment failure for bleeding peptic ulcers. During endoscopy, active bleeding, large ulcer size, location of ulcer at posterior bulbar duodenum, and lesser curve have been identified as predictors for endoscopic failure [49]. Embolotherapy may be particularly attractive in such a setting because it is not as invasive as surgery and has few complications [7, 50]. Another advantage of TAE is that most patients with recurrent bleeding after initial treatment with surgery or TAE can be effectively treated with TAE, thus avoiding a second surgical procedure [51].
Two retrospective comparisons showed at least similar efficacy in terms of rate of rebleeding, morbidity, and mortality. Ripoll et al. [50] retrospectively analyzed the outcome of 70 patients with refractory peptic ulcer bleeding. Thirty-one patients underwent angiographic embolization, and 39 patients were managed with surgery. Although patients receiving angiographic embolization were 10 years older and more patients had heart disease, the incidence of recurrent bleeding (29 vs. 23%) and mortality was similar (26 vs. 21%). Another retrospective comparison study by Eriksson et al. [51] included 40 patients who underwent angiographic embolization and 51 patients who underwent surgery after failed endoscopic therapy. The angiographic embolization group was older and had more comorbidity. Thirty-day mortality was lower in the angiographic embolization group (3 vs. 14%).
Conclusion
Managing massive bleeding from the UGI tract remains a challenge. A multidisciplinary team of skilled endoscopists, intensive care specialists, experienced UGI surgeons, and interventional radiologists all have a role to play. The past three decades have seen enormous advances in endovascular device development and treatment of a wide variety of hemorrhagic conditions. The safety and efficacy of transcatheter embolization for the treatment of life-threatening acute nonvariceal UGI bleeding is now widely accepted and is considered the gold standard for endoscopy-refractory patients. Embolization may be effective for even the most gravely ill patients for whom surgery is not a viable option, even when extravasation is not visualized by angiography. As described in this review, several clinical and technical factors must be known by interventional radiologists because they may influence the clinical outcome of embolotherapy in such setting. Specifically, every effort should be made to perform embolization early after bleeding onset and to correct coagulations disorders. In addition, it seems that careful selection of the embolic agents according to the bleeding vessel may play a role in a successful outcome.
References
Huang C, Lichtenstein DR (2003) Nonvariceal upper gastrointestinal bleeding. Gastroenterol Clin North Am 32:1053–1078
Rollhauser C, Fleischer DE (2004) Nonvariceal upper gastrointestinal bleeding. Endoscopy 36:52–58
Schoenberg MH (2001) Surgical therapy for peptic ulcer and nonvariceal bleeding. Langenbbecks Arch Surg 386:98–103
Defreyne L, De Schrijver I, Decruyenaere J et al (2008) Therapeutic decision-making in endoscopically unmanageable nonvariceal upper gastrointestinal hemorrhage. Cardiovasc Intervent Radiol 31:897–905
Rosch J, Dotter CT, Brown MJ (1972) Selective arterial embolization. A new method for control of acute gastrointestinal bleeding. Radiology 102:303–306
Funaki B (2002) Endovascular intervention for the treatment of acute arterial gastrointestinal hemorrhage. Gastroenterol Clin North Am 31:701–713
Encarnacion CE, Kadir S, Beam CA et al (1992) Gastrointestinal bleeding: treatment with arterial embolization. Radiology 183:505–508
Lang EV, Picus D, Marx VM et al (1990) Massive arterial hemorrhage from the stomach and lower esophagus: impact of embolotherapy on survival. Radiology 177:249–252
Ljungdahl M, Eriksson LG, Nyman R et al (2002) Arterial embolisation in management of massive bleeding from gastric and duodenal ulcers. Eur J Surg 168:384–390
Holme JB, Nielsen DT, Funch-Jensen P et al (2006) Transcatheter arterial embolization in patients with bleeding duodenal ulcer: an alternative to surgery. Acta Radiol 47:244–247
Gomes AS, Lois JF, McCoy RD (1986) Angiographic treatment of gastrointestinal hemorrhage: comparison of vasopressin infusion and embolization. AJR Am J Roentgenol 146:1031–1037
Parente F, Anderloni A, Bargiggia S et al (2005) Outcome of non-variceal acute upper gastrointestinal bleeding in relation to the time of endoscopy and the experience of the endoscopist: a two-year survey. World J Gastroenterol 11:7122–7130
Miller M Jr, Smith TP (2005) Angiographic diagnosis and endovascular management of nonvariceal gastrointestinal hemorrhage. Gastroenterol Clin North Am 34:735–752
Chua AE, Ridley LJ (2008) Diagnostic accuracy of CT angiography in acute gastrointestinal bleeding. J Med Imaging Radiat Oncol 52:333–338
Eriksson LG, Sundbom M, Gustavsson S et al (2006) Endoscopic marking with a metallic clip facilitates transcatheter arterial embolization in upper peptic ulcer bleeding. J Vasc Interv Radiol 17:959–964
Sandstede J, Wittenberg G, Schmitt S et al (1997) The diagnostic localization of acute gastrointestinal bleeding in a primarily negative angiographic finding. Rofo 166:258–259
Johnston C, Tuite D, Pritchard R et al (2007) Use of provocative angiography to localize site in recurrent gastrointestinal bleeding. Cardiovasc Intervent Radiol 30:1042–1046
Lang EK (1992) Transcatheter embolization in management of hemorrhage from duodenal ulcer: long-term results and complications. Radiology 182:703–707
Goodney PP, Chang RW, Cronenwett JL (2008) A percutaneous arterial closure protocol can decrease complications after endovascular interventions in vascular surgery patients. J Vasc Surg 48:1481–1488
Katayama H, Yamaguchi K, Kozucka T, Takashima T, Seez P, Matsuura K (1990) Adverse reactions to ionic and nonionic contrast media. A report from the Japanese committee on the safety of contrast media. Radiology 175:621–628
Shapiro N, Brandt L, Sprayregan S et al (1981) Duodenal infarction after therapeutic Gelfoam embolization of a bleeding duodenal ulcer. Gastroenterology 80:176–180
Rosch J, Keller FS, Kozak B et al (1984) Gelfoam powder embolization of the left gastric artery in treatment of massive small-vessel gastric bleeding. Radiology 151:365–370
Walsh RM, Anain P, Geisinger M et al (1999) Role of angiography and embolization for massive gastroduodenal hemorrhage. J Gastrointest Surg 3:61–65
Loffroy R, Guiu B, Cercueil JP et al (2009) Endovascular therapeutic embolisation: an overview of occluding agents and their effects on embolised tissues. Curr Vasc Pharmacol 7:250–263
Aina R, Oliva VL, Therasse E et al (2001) Arterial embolotherapy for upper gastrointestinal hemorrhage: outcome assessment. J Vasc Interv Radiol 12:195–200
Loffroy R, Guiu B, D’Athis P et al (2009) Arterial embolotherapy for endoscopically unmanageable acute gastroduodenal hemorrhage: predictors of early rebleeding. Clin Gastroenterol Hepatol 7:515–523
Schenker MP, Duszak R Jr, Soulen MC et al (2001) Upper gastrointestinal hemorrhage and transcatheter embolotherapy: clinical and technical factors impacting success and survival. J Vasc Interv Radiol 12:1263–1271
Poultsides GA, Kim CJ, Orlando R III et al (2008) Angiographic embolization for gastroduodenal hemorrhage: safety, efficacy, and predictors of outcome. Arch Surg 143:457–461
Defreyne L, Vanlangenhove P, De Vos M et al (2001) Embolization as a first approach with endoscopically unmanageable acute nonvariceal gastrointestinal hemorrhage. Radiology 218:739–748
Choudari CP, Rajgopal C, Elton RA et al (1994) Failures of endoscopic therapy for bleeding peptic ulcer: an analysis of risk factors. Am J Gastroenterol 89:1968–1972
Zimmerman J, Meroz Y, Siguencia J et al (1994) Upper gastrointestinal hemorrhage: comparison of the causes and prognosis in primary and secondary bleeders. Scand J Gastroenterol 29:795–798
Sos TA, Lee JG, Wixson D et al (1978) Intermittent bleeding from minute to minute in acute massive gastrointestinal hemorrhage: arteriographic demonstration. AJR Am J Roentgenol 131:1015–1017
Morris DC, Nichols DM, Connell DG et al (1986) Embolization of the left gastric artery in the absence of angiographic extravasation. Cardiovasc Intervent Radiol 9:195–198
Padia SA, Geisinger MA, Newman JS et al (2009) Effectiveness of coil embolization in angiographically detectable versus non-detectable sources of upper gastrointestinal hemorrhage. J Vasc Interv Radiol 20:461–466
Toyoda H, Nakano S, Takeda I et al (1995) Transcatheter arterial embolization for massive bleeding from duodenal ulcers not controlled by endoscopic hemostasis. Endoscopy 27:304–307
De Wispelaere JF, De Ronde T, Trigaux JP et al (2002) Duodenal ulcer hemorrhage treated by embolization: results in 28 patients. Acta Gastroenterol Belg 65:6–11
Ledermann HP, Schoch E, Jost R et al (1998) Superselective coil embolization in acute gastrointestinal hemorrhage: personal experience in 10 patients and review of the literature. J Vasc Interv Radiol 9:753–760
Van Vugt R, Bosscha K, Van Munster IP et al (2009) Embolization as treatment of choice for bleeding peptic ulcers in high-risk patients. Dig Surg 26:37–42
Goldman ML, Freeny PC, Tallman JM et al (1978) Transcatheter vascular occlusion therapy with isobutyl 2-cyanoacrylate (bucrylate) for control of massive upper gastrointestinal bleeding. Radiology 129:41–49
Toyoda H, Nakano S, Kumada T et al (1996) Estimation of usefulness of N-butyl-2-cyanoacrylate-lipiodol mixture in transcatheter arterial embolization for urgent control of life-threatening massive bleeding from gastric or duodenal ulcer. J Gastroenterol Hepatol 11:252–258
Loffroy R, Guiu B, Mezzetta L et al (2009) Short- and long-term results of transcatheter embolization for massive arterial hemorrhage from gastroduodenal ulcers not controlled by endoscopic hemostasis. Can J Gastroenterol 23:115–120
Kim B, Wright HK, Bordan D et al (1985) Risks of surgery for upper gastrointestinal hemorrhage: 1972 versus 1982. Am J Surg 149:474–476
Larson G, Schmidt T, Gott J et al (1986) Upper gastrointestinal bleeding: predictors of outcome. Surgery 100:765–773
Silverstein FE, Gilbert DA, Tedesco FJ et al (1981) The national ASGE survey on upper gastrointestinal bleeding. II. Clinical prognostic factors. Gastrointest Endosc 27:80–93
Dempsey DT, Burke DR, Reilly RS et al (1990) Angiography in poor-risk patients with massive nonvariceal upper gastrointestinal bleeding. Am J Surg 159:282–286
Welch CE, Rodkey GV, von Ryll Gryska P (1986) A thousand operations for ulcer disease. Ann Surg 204:454–467
Wheatley KE, Dykes PW (1990) Upper gastrointestinal bleeding: when to operate. Postgrad Med J 66:926–931
Lau JYW, Sung JJY, Lam Y et al (1999) Endoscopic retreatment compared with surgery in patients with recurrent bleeding after initial endoscopic control of bleeding ulcers. N Engl J Med 340:751–756
Cheung FKY, Lau JYW (2009) Management of massive peptic ulcer bleeding. Gastroenterol Clin N Am 38:231–243
Ripoll C, Banares R, Beceiro I et al (2004) Comparison of transcatheter arterial embolization and surgery for treatment of bleeding peptic ulcer after endoscopic treatment failure. J Vasc Interv Radiol 15:447–450
Eriksson LG, Ljungdahl M, Sundbom M, Nyman R (2008) Transcatheter arterial embolization versus surgery in the treatment of upper gastrointestinal bleeding after therapeutic endoscopy failure. J Vasc Interv Radiol 19:1413–1418
Loffroy R, Guiu B, Cercueil JP et al (2008) Refractory bleeding from gastroduodenal ulcers: arterial embolization in high-operative-risk patients. J Clin Gastroenterol 42:361–367
Larssen L, Moger T, Bjornbeth BA et al (2008) Transcatheter arterial embolization in the management of bleeding duodenal ulcers: a 5.5-year retrospective study of treatment and outcome. Scand J Gastroenterol 43:217–222
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Loffroy, R., Rao, P., Ota, S. et al. Embolization of Acute Nonvariceal Upper Gastrointestinal Hemorrhage Resistant to Endoscopic Treatment: Results and Predictors of Recurrent Bleeding. Cardiovasc Intervent Radiol 33, 1088–1100 (2010). https://doi.org/10.1007/s00270-010-9829-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00270-010-9829-7