
Abstract
Background
With the recent, widespread availability of endoscopic hemoclips, it has become common clinical practice to apply hemoclips to some non-bleeding polypectomy sites “prophylactically” to prevent delayed post-polypectomy bleeding (PPB). Few published data support this practice, however.
Aim
The aim of this study was to compare rates of delayed PPB in matched patients who had polypectomies performed with and without the prophylactic placement of hemoclips.
Methods
We reviewed medical records of patients who had elective colonoscopy at our VA Medical Center between July 2008 and December 2009. We identified patients who had hemoclips applied prophylactically (cases) and compared their rate of delayed PPB within 30 days to that of patients who had polypectomy without hemoclipping (controls). Controls were matched 1:1 to cases based on age and on factors known to contribute to the risk of PPB including polyp size, morphology, technique of polyp removal, number of polyps removed, and use of anticoagulants.
Results
We identified 184 patients (cases) who underwent prophylactic hemoclipping and 184 well-matched controls. An average of 3.8 polyps per patient were removed in the case group compared to 3.3 polyps per patient in controls (p = 0.6). Delayed PPB occurred in three patients in the prophylactic hemoclip group and in one patient in the control group (1.6 vs. 0.5 %, p = 0.62).
Conclusions
We found no significant difference in the rate of delayed PPB between patients who had prophylactic hemoclipping of polypectomy sites and a well-matched control group of patients who had polypectomy without prophylactic hemoclipping. These data call into question the expensive practice of prophylactic hemoclipping.
Similar content being viewed by others


Introduction
The reported incidence of post-polypectomy bleeding (PPB) ranges from 0.6 to 8.6 %, and hemorrhage continues to be the most common adverse event of polypectomy [1, 2]. It has become common practice to treat PPB with the application of endoscopic hemoclips, which have become widely available to gastroenterologists only over the past decade. PPB can occur immediately after removal of a polyp, but most reported PPB is delayed, occurring within days after completion of the colonoscopy. In attempts to minimize the risk of delayed PPB, colonoscopists often place hemoclips at non-bleeding polypectomy sites, even though there is little published evidence that supports the efficacy and safety of such “prophylactic” hemoclipping.
Few studies have evaluated the efficacy of prophylactic hemoclipping for preventing delayed PPB. To date, there have only been two published, randomized, controlled trials on prophylactic hemoclipping, with significant differences in study design, and both found no benefit for the practice [3, 4]. In the first study, 413 patients were randomly assigned to receive prophylactic hemoclipping or no prophylactic hemoclipping during colonoscopic polypectomy. The investigators found no significant difference in the incidence of delayed PPB between the two groups, and they concluded that prophylactic hemoclipping did not decrease the rate of delayed PPB [3]. However, the conclusions that can be drawn from this study are limited because most (75 %) of the polyps removed were small (<10 mm) and, therefore, unlikely to bleed. Interestingly, the other of these two studies focused on placing prophylactic hemoclips for pedunculated polyps prior to performing the polypectomy and found that this increased the risk of mucosal burns and perforation [4]. Other studies have shown that polyps >10 mm are 4.5 times more likely than smaller polyp to be complicated by hemorrhage after polypectomy [5]. Furthermore, colonoscopists are more likely to use hemoclips prophylactically for larger polyps.
One retrospective study compared the rate of delayed PPB in patients who had large (≥20 mm) sessile or flat polyps removed colonoscopically with and without prophylactic hemoclipping. The investigators found that the rate of delayed PPB was significantly lower in those who received prophylactic hemoclip placement (1.8 vs. 9.7 % in those not prophylactically hemoclipped; OR 6.0) [6]. The conclusions that can be drawn from this study also are limited, however, both by its retrospective nature and by the fact that the study period spanned the “pre-hemoclip” and “post-hemoclip” eras. During that period, changes in patient and technique-related factors (other than the application of hemoclips) might well have influenced the observed rates of delayed PPB [7].
Some experts have suggested that patients at high risk of PPB, such as those taking anticoagulants, might benefit from prophylactic hemoclipping, but there are few published data to support this opinion [8]. In our retrospective study on the safety of polypectomy in patients taking clopidogrel, we found no significant difference in the rates of PPB between clopidogrel users and nonusers. However, we did find that patients in the clopidogrel group were significantly more likely to have prophylactic hemoclipping performed after polypectomy (22 vs. 10 %, p = 0.0001) [9]. In our prospective study addressing the same issue, five patients in the uninterrupted clopidogrel group experienced delayed PPB even though four of those five had been treated with prophylactic hemoclipping. This observation further calls into question the utility of prophylactic hemoclipping [10].
The peri-procedural use of warfarin has been found to increase the risk of PPB, with one study describing a 13-fold increased PPB risk in patients taking warfarin [11]. A report of a case series has suggested that patients whose warfarin is stopped for 36 h before colonoscopy have low rates of PPB when prophylactic hemoclips are applied, but the conclusions that can be drawn from this small, retrospective study in regard to the utility of prophylactic hemoclipping also are very limited [12].
The aim of our study was to compare the risk of PPB in patients who had undergone prophylactic hemoclipping (during a period when hemoclips were readily available and widely used) with a well-matched group of patients (i.e. with similar risk factors for PPB) who did not have prophylactic hemoclipping.
Methods
Study Design
We performed a retrospective case–control study on patients who underwent elective colonoscopy with polypectomy at the Dallas VA Medical Center from July 2008 to December 2009. This study was approved by our institutional review board in August 2011.
Identification of Cases and Controls
We reviewed our endoscopy database (ProVationMD) on all patients who underwent colonoscopy with polypectomy at the Dallas VA Medical Center from July 2008 to December 2009. Cases were identified as patients who had prophylactic hemoclip placement after polypectomy (defined as hemoclip placement after polypectomy in the absence of acute bleeding). Potential controls were patients who had polypectomy with no hemoclip placement.
Data Collection
Patients’ medical records were reviewed for data on age, sex, race and comorbidities including coronary artery disease, congestive heart failure, atrial fibrillation, cerebrovascular disease, diabetes, lung and renal disease. We also noted whether patients were prescribed any medications that might increase the risk of bleeding including aspirin, non-steroidal anti-inflammatory drugs (NSAIDs), thienopyridines (clopidogrel, prasugrel), warfarin and heparin, and whether these medications were stopped prior to the procedure. We also recorded data on the date of the procedure, indication for the procedure, findings, and placement of hemoclips. We collected data on other factors that might influence the risk of PPB including polyp size, morphology, histology, removal technique and number of polyps removed. Adverse events related to the colonoscopy (during and up to 30 days after) were noted.
Post-polypectomy Bleeding
The primary outcome was delayed PPB, which was defined as the occurrence of rectal bleeding within 30 days of the procedure that resulted in hospitalization and/or treatment.
Delayed PPB was determined after careful review of multiple sources of information. The medical record was reviewed to identify visits with primary care providers, specialty clinic notes, emergency room visits and any hospitalizations during at least the period of 30 days after the colonoscopy. Moreover, it is standard practice at our Medical Center to call patients within 48 h of colonoscopy to assess for post-procedural events. These calls are documented in the medical record, and these records were also reviewed.
For patients identified with delayed PPB, additional data were collected on time to onset of bleeding after colonoscopy, hospitalization, number of hospitalization days, blood transfusion and treatment measures such as repeat colonoscopy, angiography or surgery.
Case Matching
Patients identified as cases (those who had prophylactic hemoclipping) were matched 1:1 to control patients based on age and on factors that might independently contribute to the risk of PPB including polyp size, morphology (sessile or pedunculated), technique of removal (hot snare, cold forceps, cold snare), number of polyps removed, and use of anticoagulation (clopidogrel, warfarin, heparin).
Data Analysis
In comparing data on cases and controls, a Fisher’s exact test was used for categorical variables, and a Mann–Whitney test was used for continuous variables. Post-hoc power analysis was done with a McNemar’s test using SAS. All authors had access to the study data and have reviewed and approved the final manuscript.
Results
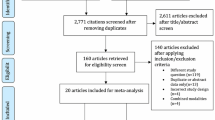
A total of 2,081 patients were identified as having undergone colonoscopy with polypectomy during the observation period. Among these, 184 were identified as having prophylactic hemoclipping after polypectomy (cases). The 184 cases were matched 1:1 with controls who had similar age, polyp size, morphology, technique of removal, number of polyps removed, and anticoagulant usage.
Baseline Characteristics
Table 1 shows that there were no significant differences between cases and controls in regard to average age (63.7 years in the cases vs. 64.9 years in the controls), gender (182 of 184 in both groups were male), ethnicity, co-morbid diseases, anti-coagulant or anti-platelet usage, and pertinent laboratory values.
Polypectomy Data
A total of 236 polyps that were prophylactically hemoclipped were removed from the 184 cases. The average size of these polyps was 12.4 mm. Most of the prophylactically clipped polyps were sessile, and most were removed with hot snare (Table 2).
Between the two cohorts, a total of 1,311 polyps were removed including 701 (236 hemoclipped, 465 not hemoclipped) in the prophylactic hemoclip group and 610 (all not hemoclipped) in the control group (Table 3). An average of 3.8 polyps per patient were removed in the prophylactic hemoclip group compared to 3.3 polyps per patient in the controls (p = 0.6). There were no significant differences between the groups in regard to number of polyps removed, polyp size, morphology, location, removal technique or adenomatous histology, but the frequency of “other” non-adenomatous polyps was slightly but significantly lower in the prophylactic hemoclip group (8 vs. 12 %, p = 0.02) (Fig. 1).

Details of patients included in hemoclip group and matched controls
Post-polypectomy Bleeding
There were three delayed PPBs in the group that had prophylactic hemoclipping and one delayed PPB in the control group, a difference that was not statistically significantly (1.6 vs. 0.5 %, p = 0.62, OR 3.0, 95 % CI 0.31–29.4). Characteristics of the patients who experienced delayed PPB are summarized in Table 4. Note that two of the four delayed PPBs occurred in patients taking anticoagulants (one warfarin, one clopidogrel), and all four occurred in patients whose polyps were removed with a hot snare. Three of the four bleeding polyps were sessile. None of the four patients with delayed PPB required angiography or surgery, and all recovered without further sequelae.
Discussion
With the recent, widespread availability of endoscopic hemoclips, the practice of prophylactic hemoclipping to prevent delayed PPB has become frequent, even though there are few published data to support the efficacy of the practice. Of the two prospective, randomized studies addressing this issue, one was limited by the small size of polyps removed and the low rates of PPB and the other, which was specifically focused on pedunculated polyps, was stopped early due to increase in complications from hemoclip placement; neither showed a significant benefit for prophylactic hemoclipping [3, 4]. Conversely, a retrospective review of the practice of one expert colonoscopist revealed that the rate of delayed PPB declined significantly after starting the practice of prophylactic hemoclipping for large (>2 cm) polyps [6]. Consequently, the efficacy of prophylactic hemoclipping remains disputed.
In our study, we matched 184 patients who had prophylactic hemoclipping of polypectomy sites to 184 controls who had similar polypectomies but without hemoclipping. The two groups were well matched for the known risk factors that might contribute to PPB, including anticoagulant use, polyp size, polyp number, technique used for polypectomy, and polyp morphology. There were three delayed PPBs in the patients who underwent prophylactic hemoclipping (1.6 %) and one delayed PPB in the matched control group (0.5 %). Although this difference was not statistically significant, it is interesting that the rate of delayed PPB was higher in the patients who had prophylactic hemoclipping than in the controls. Among the four patients who experienced delayed PPBs, one on warfarin and one on clopidogrel bled from smaller polyps (7 and 8 mm, respectively), while the delayed PPBs in the other two patients not taking anticoagulants involved larger polyps (15 and 25 mm). This supports that notion that anticoagulants increase the risk of delayed PPB, even for small polyps. Unfortunately, the small number of delayed PPBs in our study precludes a meaningful subgroup analysis to assess the effect of prophylactic hemoclipping on the incidence of PPB in patients on anticoagulants. Notably, all four delayed PPBs in our study were readily controlled without surgery or angiography, and no patient had any long-lasting sequelae.
Our study has several limitations. The major limitation is in its retrospective nature. Although the cases and controls were well matched for known risk factors for delayed PPB, the criteria for applying hemoclips were not mandated prospectively. Consequently, there may have been differences between the cases and controls regarding the endoscopic appearance of the polypectomy sites, or regarding other unquantifiable or undocumented factors that cannot be discerned by a retrospective review. However, with our matched analysis, we attempted to control for all known factors for PPB to minimize this confounder. Another study limitation is that the colonoscopies were performed by multiple endoscopists whose polypectomy techniques and criteria for applying prophylactic hemoclips might vary. Finally, the overall incidence of delayed PPB was small, which limits the study’s power. Nevertheless, our observed rate of PPB is comparable to those described in other studies [3, 9, 10]. Moreover, based on our post hoc power analysis, a study designed to confirm the small difference in the rate of PPB that we observed between our cases and controls with 80 % power would require approximately 3,000 patients total, which is logistically difficult. Further, it is unlikely that our study missed a large difference between the groups, because it was sufficiently powered to detect a difference in the rate of delayed PPB of at least 10 % between the groups. Despite these limitations, the strength of the study lies in the careful matching of cases and controls in regard to risk factors for delayed PPB such as polyp size, removal technique and anticoagulation use, in order to isolate the effect of hemoclipping on PPB.
The findings of this study have potentially important implications for the practice of delivering healthcare in today’s era of cost consciousness. A single hemoclip costs approximately $150 [13]. Thus, even the application of one hemoclip substantially increases the cost of colonoscopy. At our VA hospital alone, a review of our endoscopy database revealed that we spend approximately $64,000 per year on hemoclips used for prophylactic purposes.
In summary, we found no significant effect of prophylactic hemoclipping of polypectomy sites on the risk of delayed PPB. Indeed, the rate of delayed PPB was higher in patients who had prophylactic hemoclipping, although this difference was not statistically significant. Our findings do not support the routine performance of this expensive and common clinical practice, and highlight the need for a definitive, prospective trial on this issue.
References
Kapetanos D, Beltsis A, et al. Postpolypectomy bleeding: incidence, risk factors, prevention and management. Surg Laparosc Endosc Percutan Tech. 2012;22:102–107.
Fatima H, Rex D. Minimizing endoscopic complications: colonoscopic polypectomy. Gastrointest Endosc Clin N Am. 2007;17:145–156.
Shioji K, Suzuki Y, et al. Prophylactic clip application does not decrease delayed bleeding after colonoscopic polypectomy. Gastrointest Endosc. 2003;57:691–694.
Quintanilla E, Castro JL, Rábago LR, et al. Is the use of prophylactic hemoclips in the endoscopic resection of large pedunculated polyps useful? A prospective and randomized study. J Interv Gastroenterol. 2012;2:183–188.
Watabe H, Yamaji Y, et al. Risk assessment for delayed hemorrhagic complication of colonic polypectomy: polyp related factors and patient related factors. Gastrointest Endosc. 2006;64:73–78.
Liaquat H, Rohn E, Rex DK. Prophylactic clip closure reduced the risk of delayed postpolypectomy hemorrhage: experience in 277 clipped large sessile or flat colorectal lesions and 247control lesions. Gastrointest Endosc. 2013;77:401–407.
Edmundowicz SA. To clip or not clip: is that the question? Gastrointest Endosc. 2013;77:408–409.
Kaltenbach T, Soetikno R. Endoscopic resection of large colon polyps. Gastrointest Endosc Clin N Am. 2013;23:137–152.
Feagins LA, Uddin F, et al. The rate of post-polypectomy bleeding for patients on uninterrupted clopidogrel therapy during elective colonoscopy is acceptably low. Dig Dis Sci. 2011;56:2631–2638.
Feagins LA, Iqbal R, Harford W, et al. Low rate of post-polypectomy bleeding among patients who continue thienopyridine therapy during colonoscopy. Clin Gastroenterol Hepatol. 2013;11:1325–1332.
Hui A, Wong R, et al. Risk of colonoscopic polypectomy bleeding with anticoagulants and antiplatelet agents: analysis of 1357 cases. Gastrointest Endosc. 2004;59:44–48.
Friedland S, Sedehi D, Soetikno R. Colonoscopic polypectomy in anticoagulated patients. World J Gastroenterol. 2009;15:1973–1976.
Parikh N, Zanocco K, Keswani RN, Gawron AJ. A cost efficacy decision analysis of prophylactic clip placement after endoscopic removal of large polyps. Clin Gastroenterol Hepatol. 2013;11:1319–1324.
Acknowledgments
This work was supported by the Office of Medical Research, Department of Veteran’s Affairs.
Conflict of interest
Dr. Feagins has received research funding from Altheus Therapeutics for an unrelated project. Dr. Spechler is a consultant for Torax Medical Inc., Ironwood Pharmaceuticals Inc., and Takeda Pharmaceuticals Inc.; however, none of these are relevant to this article. A.D.N. and R.I. have nothing to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Feagins, L.A., Nguyen, A.D., Iqbal, R. et al. The Prophylactic Placement of Hemoclips to Prevent Delayed Post-polypectomy Bleeding: An Unnecessary Practice? A Case Control Study. Dig Dis Sci 59, 823–828 (2014). https://doi.org/10.1007/s10620-014-3055-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-014-3055-0