Article Text

Abstract
Environmental enteric dysfunction (EED) has been recognised as an important contributing factor to physical and cognitive stunting, poor response to oral vaccines, limited resilience to acute infections and ultimately global childhood mortality. The aetiology of EED remains poorly defined but the epidemiology suggests a multifactorial combination of prenatal and early-life undernutrition and repeated infectious and/or toxic environmental insults due to unsanitary and unhygienic environments. Previous attempts at medical interventions to ameliorate EED have been unsatisfying. However, a new generation of imaging and ‘-omics’ technologies hold promise for developing a new understanding of the pathophysiology of EED. A series of trials designed to decrease EED and stunting are taking novel approaches, including improvements in sanitation, hygiene and nutritional interventions. Although many challenges remain in defeating EED, the global child health community must redouble their efforts to reduce EED in order to make substantive improvements in morbidity and mortality worldwide.
- Gastroenterology
- environmental enteropathy
- environmental enteric dysfunction
- Tropical Paediatrics
Statistics from Altmetric.com
Stunting and environmental enteric dysfunction
The Sustainable Development Goals, adopted by the United Nations in September 2015, set the international agenda for global development for the next 15 years.1 Goal #2 aims to end hunger and improve nutrition worldwide, with target 2.2 specifically aiming to reduce stunting. Stunting, broadly speaking, reflects the failure of an individual to reach his or her genetic potential for optimal health, generally measured as capacity for physical activity, cognitive ability and resilience to disease. In the context of global child health, stunting is most readily assessed as linear growth failure and is generally considered to be the most prevalent and pervasive form of undernutrition worldwide.2 This form of growth faltering, as measured by a low height-for-age Z-score, affects at least 25% of children worldwide, and at least 15% of deaths among children under the age of 5 years can be attributed to stunting.3 The causes of stunting are postulated to be multifactorial and include at least (1) inadequate prenatal nutrition and inadequate dietary intake early in life (the so-called ‘first 1000 days’ essential to appropriate growth and development); (2) chronic and repeated acute infections leading to a catabolic inflammatory state; and (3) the chronic intestinal inflammatory condition now known as environmental enteric dysfunction (EED), previously referred to as tropical enteropathy or environmental enteropathy. Given that interventions aimed at reducing or ameliorating stunting by addressing the first two factors (nutrition and recognised infections) have been largely unsuccessful, interventions targeted against EED have gained importance as a means of improving the growth and survival of children throughout the developing world, including through mechanisms such as improved oral vaccine efficacy.4
Given its increasing prominence on the child survival agenda, EED has been the subject of numerous recent reviews5–10 that well delineate its hypothesised pathogenesis and summarise the current state of knowledge. As international bodies have also increased their interest in attacking EED as a means to stimulate improvements in global child morbidity and mortality, the International Atomic Energy Agency held a high-level technical meeting on EED in October 2015.11 Several innovative and promising insights into EED are reviewed here in order to motivate further study and discussion among the global child health community.
New insights into the morphology of EED
EED is a chronic inflammatory state of the duodenum and jejunum. The normal architecture of this portion of the digestive tract is a forest of fluffy, undulating villi that are protected from the luminal contents by a thick barrier of mucus (figure 1). Most nutrient absorption occurs in this area of the digestive tract. The pathological changes that occur in EED have heretofore been visualised only on intestinal specimens obtained from the host by endoscopic biopsy. The villi are broad and short and the mucosa is seen to be flattened with increases in the crypt depth between villi, such that a scalloped appearance is seen on endoscopy, not dissimilar to the early stages of coeliac disease. The surface area available for nutrient absorption and active uptake is markedly reduced, correlating with the decreased absorption of essential fats, carbohydrates and vitamins.8
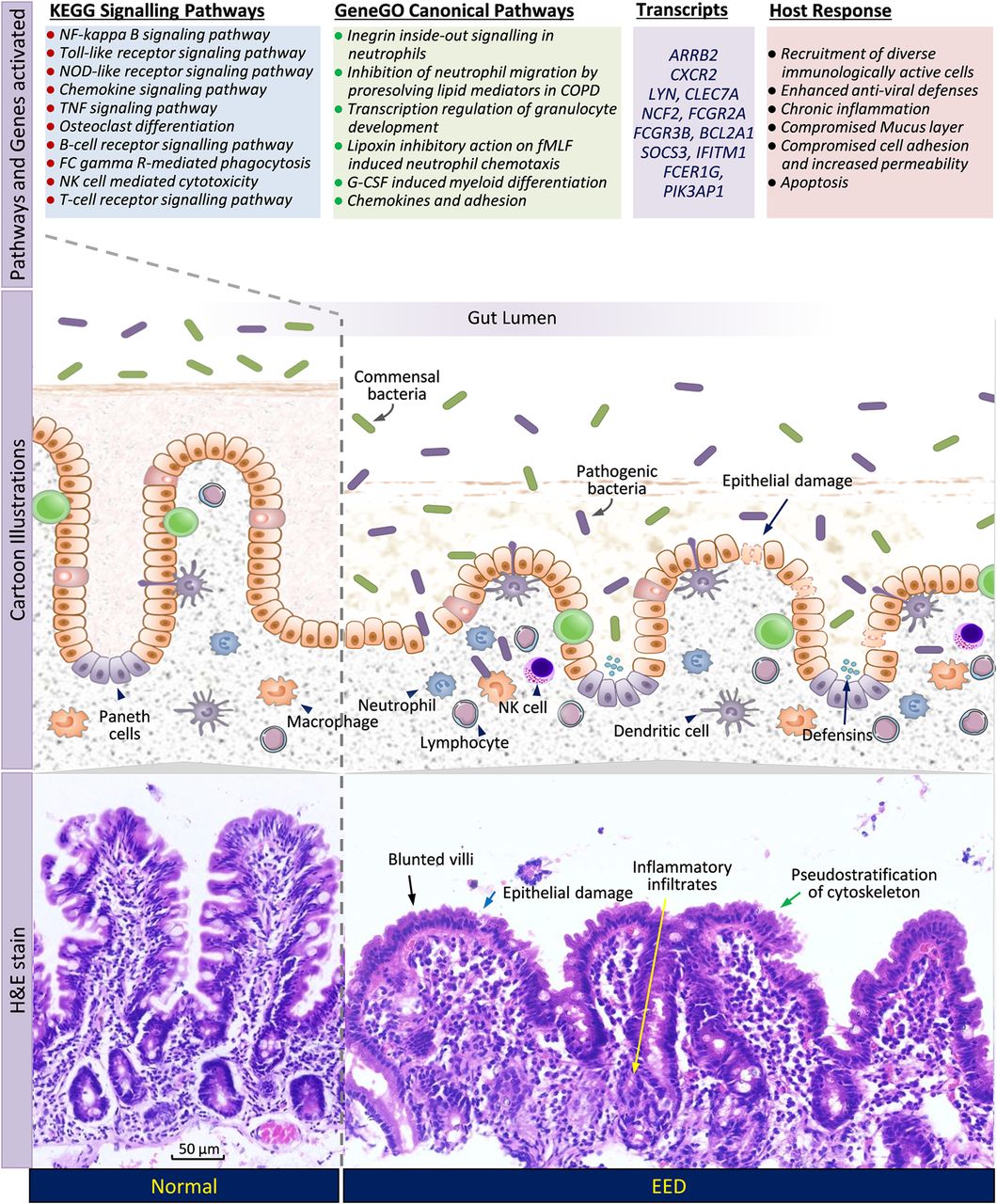
List of pathways, transcripts and host responses activated in environmental enteric dysfunction, juxtaposed with a schematic diagram of cellular interactions and histological photographs of damaged intestinal mucosa.
Novel recent work using confocal laser endomicroscopy in adult volunteers with EED in Zambia has demonstrated this dynamic pathology in a way never previously visualised. In these experiments, after the infusion of intravenous fluorescein dye, bright plumes of this dye are seen leaking out of the damaged epithelial matrix and into the gut lumen (figure 2).12 Experience from animal studies and from studies in inflammatory bowel disease have demonstrated that when these types of defects occur there is in fact a bidirectional reflux.13 Serum lipopolysaccharide levels in these individuals are correlated with the degree of visualised cell shedding. Innumerable micro-erosions are visible in these studies, associated not just with the efflux of fluorescein but with the loss of nutrient absorptive capacity, which was further demonstrated by an impaired uptake of zinc in these patients as well.

{kind=link}
{kind=link}
Confocal laser endomicroscopy image from an adult with environmental enteric dysfunction, demonstrating villous blunting and shortening, along with two plumes of fluorescein dye extruding through epithelial defects.
These striking in vivo findings validate and extend the previously established in vitro histological findings of compromised small intestinal integrity, which puts the child at risk for increased exposure and translocation of a spectrum of microbes and toxins into the systemic circulation. This area of the intestine is not well adapted to routinely experience such a chronic microbial assault as evidenced by the highly activated CD4+ and CD8+ lymphocytes found in histological specimens from children with EED.5
Host transcriptome and metabolomic profiles in children with EED
Despite these striking morphological findings, EED does not have a specific and easily measurable clinical case definition, which limits understanding of its epidemiology and makes assessing therapeutic interventions challenging. Given the invasiveness and cost of endoscopy, especially among children in the developing world where EED is most prevalent and morbid, a variety of biomarkers have been used to assess gut function and integrity.5 ,9 ,10 ,14–17 The most commonly used method for measuring enteropathy remains the tedious dual sugar absorption test, which involves an overnight fast, followed by the consumption of a precise volume of solution containing known quantities of one or more dissolved sugars (most commonly used are lactulose and mannitol), and then subsequent collection of several hours of urine and precise quantification of the amounts of these sugars excreted.14 Since these sugars are not metabolised once absorbed, their relative amounts in the urine provide information about (a) whether there is a relative increase in the amount of the large sugar (eg, lactulose) that has crossed a disrupted gut barrier and also (b) whether there is a relative decrease in the amount of the small sugar (eg, mannitol) actively transported across a diminished absorptive surface area.14 Given how labour-intensive and time-consuming this test is, novel biomarkers for EED are actively being sought.
One promising area of exploration is the assessment of the human host transcriptome in stool samples.18 Using a novel method to isolate even very low copy numbers of host mRNA, the host transcriptome was profiled and revealed a panel of 51 transcripts significantly associated with stunting and EED (figure 1). These include chemokines known to stimulate T-cell proliferation, a number of immunoglobulin fragments, several interferon-induced proteins and activators of neutrophils and B-cells. The transcripts mapped to 12 canonical pathways involved in cell adhesion and gut integrity and to host responses against a spectrum of bacterial, viral and parasitic pathogens. This approach of evaluating the host immune and inflammatory responses to specific environmental insults that have not been precisely identified paves the way for the possibility of using one or more of these host transcripts as an improved and more clinically relevant biomarker for EED, and may open up understanding of pathophysiology for design of novel interventions.
In terms of ease of obtaining biological samples under difficult field conditions, identifying serum markers of gut inflammation and breakdown may be an ideal approach. There may be positive or negative alterations in essential metabolites involved in gut function and integrity, nutrient absorption, energy metabolism and those involved in growth and differentiation. Identifying these changes may even provide more specific information about the pathophysiological cascade responsible for and stemming from EED. Given the altered absorption and metabolism of various micronutrients and macronutrients in EED,8 it might be anticipated that levels of specific amino acids,19 cell membrane components, neurotransmitter precursors, compounds involved in mitochondrial function and components of zinc homeostasis20–22 may differ based on the severity of EED. Studies exploring the metabolome are still in early stages but may have profound implications for future work in EED.
Reducing EED with novel water, sanitation and hygiene and nutritional interventions
Prior attempts to improve EED in children via a variety of medical interventions have unfortunately been disappointing, without the discovery of marked ‘game changing’ improvements likely to lead to significant reductions in stunting or overall childhood mortality. These have been previously reviewed elsewhere9 ,10 and more recent trials have not fundamentally changed this conclusion,23–25 although a small recent trial of the anti-inflammatory medication mesalazine shows some promise.26 This general lack of demonstrated benefit may be due to the ongoing challenge of not yet having a perfect biomarker or case definition for EED. Nevertheless, our deficiencies in treatment and prevention of EED have led to an emphasis on more novel and comprehensive interventions to decrease EED.
There is a strong epidemiological link between EED and poor sanitation, exposure to animal faeces,16 lack of access to soap and water for hand and face washing,27 and consumption of contaminated food and water.28–31 These associations lead to the hypothesis that poor sanitation facilitates a constant exposure to microbes in the small intestine, provoking the chronic inflammatory state and defective integrity of the gut observed in EED. Two very large multicentre clinical studies, water, sanitation and hygiene (WASH) Benefits32 and the Sanitation Hygiene Infant Nutrition Efficacy (SHINE) Trial,33 are now underway to test whether household-level and community-level improvements in water supplies and sanitation facilities can lead to improved child growth and decreased EED. These studies should provide ample opportunities to better understand EED and stunting over the next several years as results become available.
Aside from WASH interventions, nutritional interventions to ameliorate EED are being studied, taking advantage of the natural anti-inflammatory and microbiome-modifying properties of specific nutrients and foods. Trials using specific amino acids such as arginine and glutamine,34 proteins such as lactoferrin and lysozyme,35 and legumes as supplementary foods for children during their period of weaning36 all have potential for demonstrating improvements in EED and stunting. Foods, either genetically modified or natural, that are high in growth factors that reduce apoptosis, enhance enterocyte proliferation and stimulate villous growth are prime targets for investigation. The recent development of a novel mouse model of EED37 should also be of great benefit in facilitating less expensive and more ethically feasible preclinical studies of such interventions.
Conclusions
Much has been learned about EED in the last decade, and recent technical developments in endomicroscopy and genomics are opening up further avenues for research into the pathobiology of and treatments for this condition. The transcriptomic approach to identification of specific inflammatory and repair pathways involved in EED provides hope that specific manipulation of these pathways in the not-too-distant future may be a possibility for prevention and treatment. A high-priority research area is the identification of a biomarker or panel of biomarkers that can be obtained without excessive labour or cost in the field; application of 21st-century -omics technology may well be able to provide this. The outcomes of ongoing and upcoming trials evaluating the impact of sanitation and nutritional interventions need to be evaluated carefully and applied in operational settings to reduce EED and stunting if they show promise. Areas that we largely remain ignorant about are the local microbiome of the small intestine and how it differs in children with and without EED, the role that the in utero and early infancy environments play in the development of EED and what role the colon plays, with its large, dynamic and diverse microbiota. Given the large role EED plays in physical and cognitive stunting and child survival worldwide, these issues and many more are sure to occupy an important place on the global child health landscape.
References
Footnotes
Contributors IT, PK, NS and MJM designed the review, wrote it, reviewed and approved its contents.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.